Embed Size (px)
Citation preview
Excellence in end of life care –
is it possible?
Dr Suzanne Kite
Leeds Teaching Hospitals NHS Trust
RCP London, 10 November 2015

Leeds Teaching Hospitals NHS Trust
What does excellent look like?
Well described:
Ambitions for Palliative & End of life Care 2015
One Chance to Get it Right 2014
NICE Quality standards for EoLC 2011
GMC EoLC guidance 2010
CQC – eg Frimley Park, ‘outstanding’
“The whole care team on the ward were excellent. Mum was with them for nearly 8 weeks and they formed a bond with her and were able to help her on her final journey with dignity and respect.
After mum passed away two of the doctors who had delivered the majority of her care spoke to me and made me feel much better because they had understood and acted on her behalf and within her wishes. It was comforting to me and my family.
The communication throughout was open and clear. We knew exactly what was happening and it was given in clear language we could understand. I have a lot of admiration for the role they undertake. It wasn't just clinical it was personal and they have my sincere thanks and gratitude”.
Patient experience
And caring for the family…
“Ward X were wonderful – discrete yet available,
cups of tea were plentiful, and (nurse) and (nurse)
were terrific at the time of mums death”
“We were very well cared for in the two days
before the death. In hospital conditions it was
impossible to better the care”

What have we done?
Education
Partnership working and integration
Building leadership and infrastructure
Continuous quality improvement
Networking
Settings standards and assurance
….. fostered a culture
Education
With thanks to Lesley Charman
Education – what we’ve learned so far:
Local ownership
Building clinical end of life care champions
link nurses
senior clinicians development programme
Understanding behavioural change
Working relationship with HEYH
Embedding within organisational learning
Menu of learning opportunities
Partnership working
Longstanding close working relationship between
specialist palliative care providers, acute and
community trusts, primary care & commissioners.
Includes:
Five year strategies
Marie Curie Delivering Choice Programme 2006-9
Health Needs Analysis 2013
Commissioning Strategy 2014

Palliative Care Ambulance
Building leadership and infrastructure
Developed:
an EoLC Operational Team
a management triumvirate of doctor, nurse, and a
manager senior enough to have influence and
perspective and WITH ENOUGH TIME to do some of the
detail
a wider EoLC group drawn from relevant clinical areas
across the trust - strategy & action plan
Clearer Executive leadership
Started small.

Waiting area for relatives visiting the
mortuary, 2011

New waiting room, 2012


New entrance to Bereavement Suite

Continuous quality improvement
‘The most important single change in the NHS in
response to this report would be for it to become, more
than ever before, a system devoted to continual
learning and improvement of patient care, top to
bottom and end to end’ (Berwick, 2013)
‘Give the people of the NHS career-long help to learn,
master and apply modern methods for quality control,
quality improvement and quality planning’ (Berwick, 2013)
Model for improvement
A framework for accelerating improvement, based
on three fundamental questions:
What are we trying to accomplish?
How will we know that a change is an improvement?
What changes can we make that will result in
improvement?
Combined with the Plan-Do-Study-Act (PDSA)
cycle.
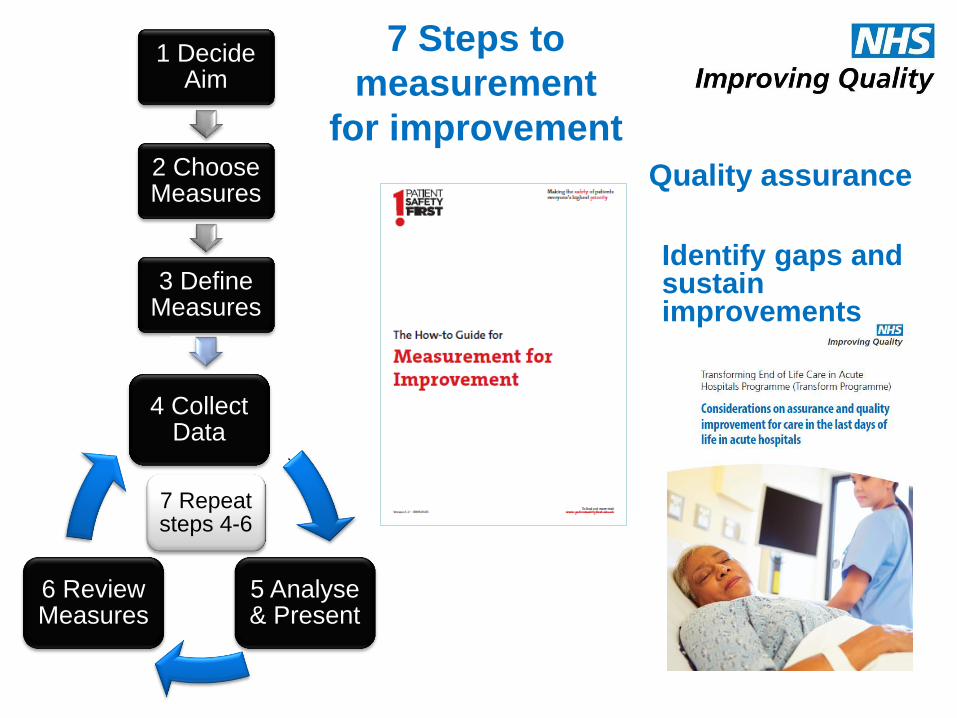
7 Repeat steps 4-6
7 Steps to
measurement
for improvement
1 Decide Aim
2 Choose Measures
3 Define Measures
4 Collect Data
5 Analyse & Present
6 Review Measures [2]
Identify gaps and sustain improvements
Quality assurance
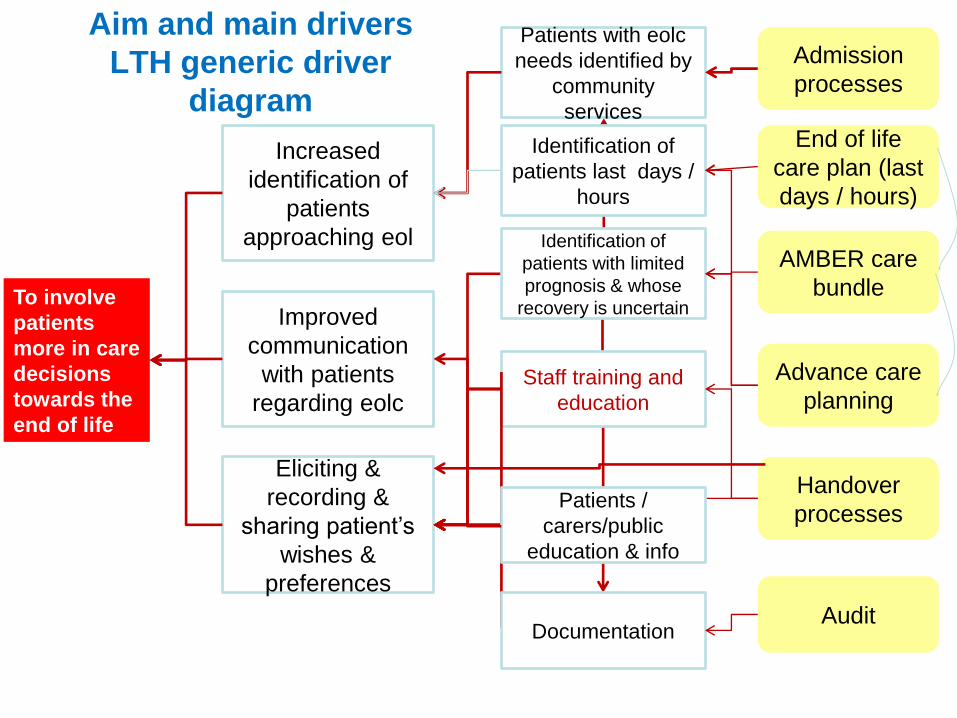
To involve
patients
more in care
decisions
towards the
end of life
Increased
identification of
patients
approaching eol
Improved
communication
with patients
regarding eolc
Eliciting &
recording &
sharing patient’s
wishes &
preferences
Patients with eolc
needs identified by
community
services
Staff training and
education
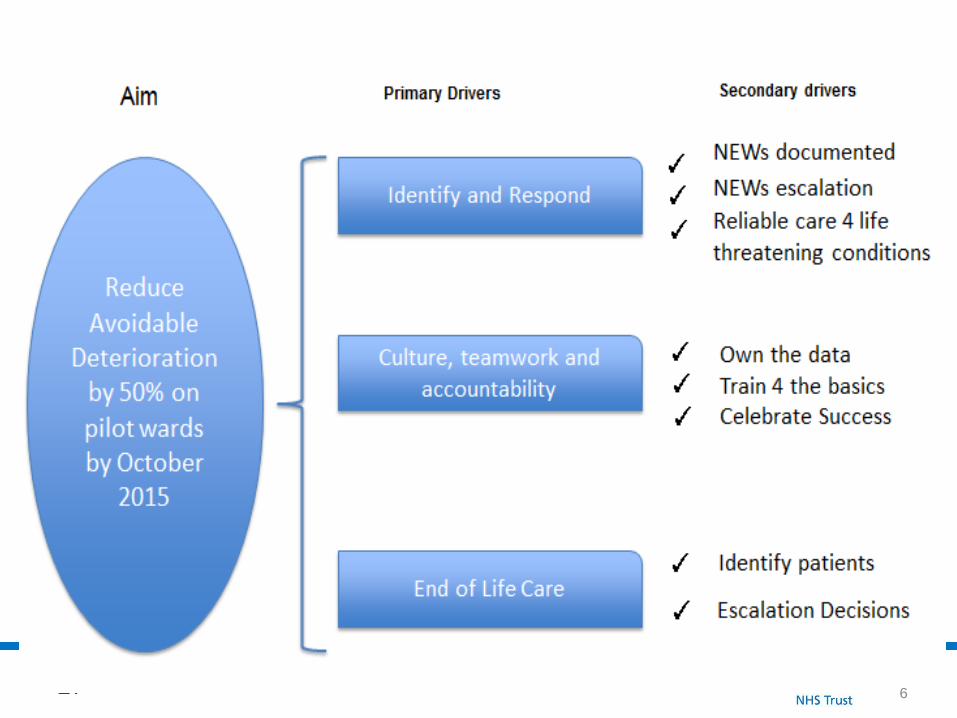
Aim and main drivers
LTH generic driver
diagram
Identification of
patients last days /
hours
Identification of
patients with limited
prognosis & whose
recovery is uncertain
Patients /
carers/public
education & info
Documentation
Admission
processes
Handover
processes
AMBER care
bundle
End of life
care plan (last
days / hours)
Audit
Advance care
planning
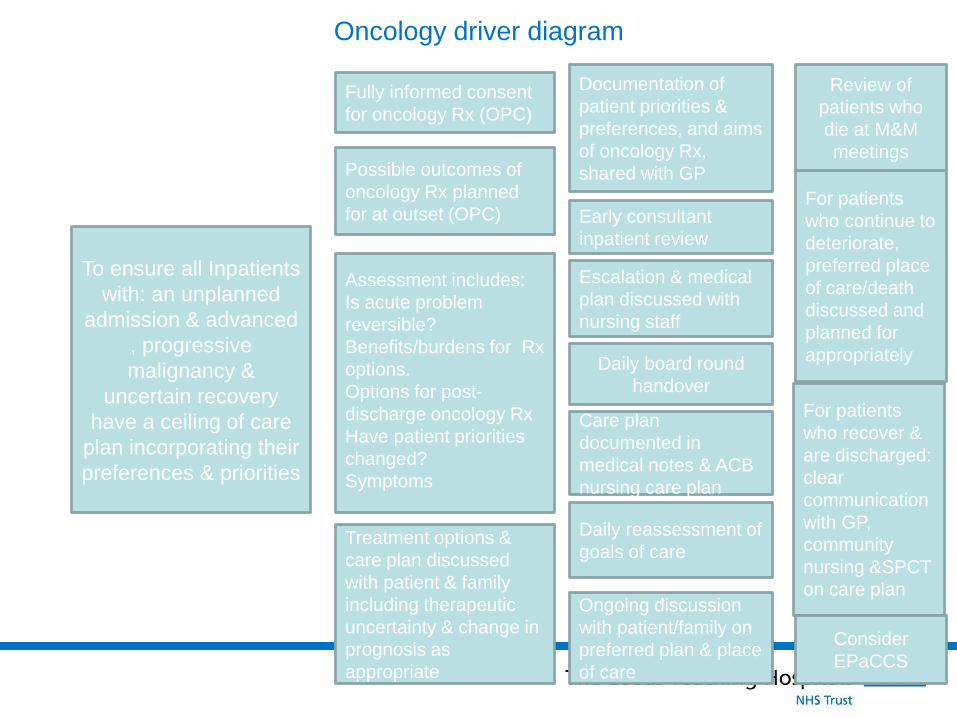
Oncology driver diagram
To ensure all Inpatients
with: an unplanned
admission & advanced
, progressive
malignancy &
uncertain recovery
have a ceiling of care
plan incorporating their
preferences & priorities
Fully informed consent
for oncology Rx (OPC)
Possible outcomes of
oncology Rx planned
for at outset (OPC)
Assessment includes:
Is acute problem
reversible?
Benefits/burdens for Rx
options.
Options for post-
discharge oncology Rx
Have patient priorities
changed?
Symptoms
Treatment options &
care plan discussed
with patient & family
including therapeutic
uncertainty & change in
prognosis as
appropriate
Documentation of
patient priorities &
preferences, and aims
of oncology Rx,
shared with GP
Early consultant
inpatient review
Escalation & medical
plan discussed with
nursing staff
Care plan
documented in
medical notes & ACB
nursing care plan
Daily reassessment of
goals of care
Ongoing discussion
with patient/family on
preferred plan & place
of care
For patients
who recover &
are discharged:
clear
communication
with GP,
community
nursing &SPCT
on care plan
For patients
who continue to
deteriorate,
preferred place
of care/death
discussed and
planned for
appropriately
Review of
patients who
die at M&M
meetings
Daily board round
handover
Consider
EPaCCS
Measurement/evaluation
National VOICES Survey of bereaved carers(‘12+’13)
Annual LTH bereaved families’ survey
Biannual national eolc audits
Annual trustwide mandatory medical audit
Outpatient clinic letter audit
Feedback from training
ONS/HES data
CQC visit
Complaints/compliments/incidents
Clinical practice
Challenges in end of life care measurement
for improvement
often can’t ask patients directly
multiple care settings, overlapping initiatives
requires triangulation/ synthesis of multiple data sources
waiting for data supplied by others ….
constant reorganisation of NHS
improvement methodology better suited to technological
interventions than to interpersonal aspects of care (Conry
2012)

Key learning
“Improving end of life care” is too generic
Need ‘SMART’ aims
Ownership by clinicians vital
Demonstrating an impact for specific
interventions is difficult
Now focussing on embedding eolc within other
initiatives eg:
Deteriorating patient workstream
Mortality review programme
27 6
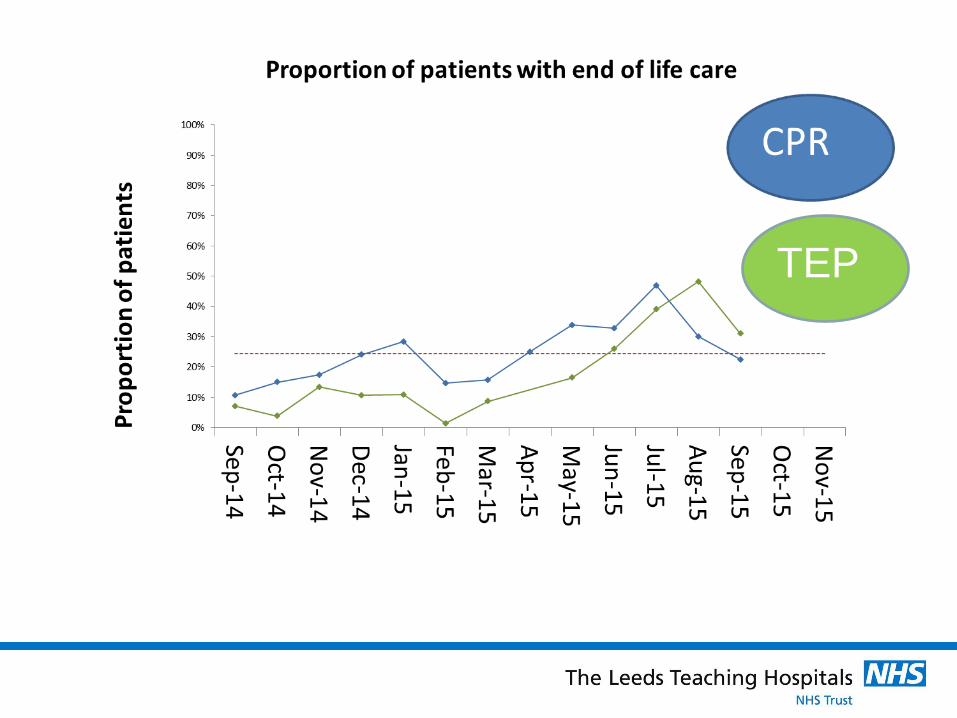
TEP
Networking
For example:
Transform programme – pilot site in 2011
DH EPaCCS pilot, 2011
Regional Acute Hospitals Group, 2012-15
And informally
Setting standards and assurance
EoLC group drawn from relevant clinical areas across the trust &
embedded in quality and governance processes of trust including:
linkage to commissioning strategy, risk register
annual work plan
reporting to Board
Executive leadership.
Quality assurance provided directly to clinical areas:
Annual LTH bereaved families’ survey
Biannual national eolc audits
Annual trustwide mandatory medical audit
CQC visit
Complaints/compliments/incidents
Clinical practice
What next?
Palliative care and interstitial lung disease project:
6/12 SPCT consultancy model, June-Dec 2015
1PA SPC Consultant time
Aims to improve access to palliative care:
Upskill respiratory team
Improve information sharing and access
Establish greater links between the respiratory team and hospital
+ community palliative care teams
Method:
Identify unmet patient needs, and address
Identify staff training needs, develop bespoke education
Develop relevant business cases as necessary
In conclusion
Excellence in end of life care is ‘Everybody’s business’
Listen, and engage with people.
Tailor approach to your environment.
Create management capacity and a
“ culture firmly rooted in continual improvement”(Berwick,
2013)
With thanks to:
Palliative Care Team and
Elizabeth Rees, Lead Nurse EoLC
Dr Fiona Hicks
Karen Henry
Christopher Stothard, EoLC Nurse
Claire Iwaniszak, EoLC Nurse
Deborah Borrill, EoLC Discharge Facilitator
Dr Adam Hurlow
Lesley Charman
Kathy Gibson
Dr Suzie Gillon
Dawn Marshall, Deputy Chief Nurse
Susannah Shouls
And the many others who have contributed across the acute trust and city
References
The How-to Guide for Measurement for
Improvement, www.patientsafetyfirst.nhs.uk
Conry MC, A 10 year systematic review of
interventions to improve quality of care in
hospitals, BMC Health Services Research 2012,
12:275





























