Embed Size (px)
Citation preview

Social Science Research 41 (2012) 1515–1528
Contents lists available at SciVerse ScienceDirect
Social Science Research
journal homepage: www.elsevier .com/locate /ssresearch
Examining fear and stress as mediators between disorder perceptionsand personal health, depression, and anxiety
Danielle Wallace ⇑Arizona State University, School of Criminology and Criminal Justice, 411 N. Central Ave., Room 600, Phoenix, AZ 85050, United States
a r t i c l e i n f o a b s t r a c t
Article history:Received 29 September 2011Revised 29 May 2012Accepted 18 June 2012Available online 25 June 2012
Keywords:HealthMental healthDisorderFear of crime
0049-089X/$ - see front matter � 2012 Elsevier Inchttp://dx.doi.org/10.1016/j.ssresearch.2012.06.005
⇑ Fax: +1 602 496 2366.E-mail address: [email protected]
Research examining the effect of neighborhoods on personal health has often focused onneighborhood disorder, or visual cues in neighborhoods perceived as personally threaten-ing or noxious. Neighborhood disorderliness is thought to elevate individuals’ fear of crime,thereby negatively impacting personal and mental health. Unfortunately, the pathwaysbetween disorder, fear of crime, and health have yet to be established. This study examinesthe pathways between neighborhood disorder, fear of crime, and three health outcomes.Using the Community, Crime and Health Survey, this study employs structural equationmodeling to examine how general (being afraid of walking alone) and offense-specific fearof crime (being afraid of specific crimes) mediate the relationship between individuals’ dis-order perceptions and self-rated health, depression and anxiety. Results show that fear ofcrime does mediate the relationship between disorder perceptions, self-rated health anddepression, though the mediating pathways are weak. This study suggests that the disor-der-fear of crime-health nexus should be re-examined theoretically.
� 2012 Elsevier Inc. All rights reserved.
1. Introduction
Neighborhood conditions have long been acknowledged as having a direct impact on individual health (Chadwick, 1842).Recent literature, though, has focused on the indirect ways in which neighborhoods affect an individual’s health, such as com-mercial decline (Browning et al., 2006) or neighboring behavior (Ross and Jang, 2000). For example, one such study finds thatsocial isolation, or residents’ inability to move out of a neighborhood combined with neighborhood poverty leads to high lev-els of psychological distress (Ross et al., 2000). Unfortunately, connecting neighborhood social dynamics to a person’s healthcan be challenging; understanding how neighborhoods and their social environments are difficult to test and have yet to befully theorized (MacIntyre and Ellaway, 2003). This is not due, however, to a lack of academic interest, but rather a deficiencyof data. Only recently has data become available that captures both neighborhood social characteristics, such as social isola-tion or collective efficacy, and a throng of individual health measures using sampling strategies suitable for neighborhoodmodeling (for example, see Cagney et al., 2009 or Sampson and Raudenbush, 1999). Until most recently, scholars have beenleft to hypothesize about the indirect pathways between neighborhoods and health, rather than empirically test them.
One such case is the relationship between neighborhood disorder and health. Neighborhood disorder is the visual, phys-ical and social conditions in a neighborhood environment that are seen as threatening or noxious (Sampson and Raudenbush,1999). Disorder has been associated with a slew of negative, physical and mental health outcomes for individuals, such ascoronary risk factors, heart disease mortality, low birth weight, smoking, morbidity, psychological stress, heavy drinking,feelings of powerlessness, physical decline, depression, all-cause mortality, and self-reported health (Cutrona et al., 2000;
. All rights reserved.

1516 D. Wallace / Social Science Research 41 (2012) 1515–1528
Geis and Ross, 1998; Hill et al., 2005a; Linares et al., 2001; Lowenkamp et al., 2003; Ross and Jang, 2000; Ross and Mirowsky,2001; Sampson and Raudenbush, 2004). The majority of work, investigating the relationship between disorder and health,suggests that the relationship is mediated through fear of crime – specifically, perceiving your environment as disorderedgenerates fear of crime which in turn leads to negative physical and mental health consequences (Geis and Ross, 1998; Ha-ney, 2007; Jackson and Stafford, 2009; Latkin and Curry, 2003; Ross, 1993, 2000a; Ross and Jang, 2000; Ross and Mirowsky,2001; Ross et al., 2000, 2001; Wen et al., 2006). Yet, no studies to date have established the pathways between disorder, fearof crime, and health.
Furthermore, recent research has brought to light methodological issues surrounding how individuals perceive and inter-act with neighborhood disorder; as a result, the relationship between disorder, fear of crime, and health is called into ques-tion. Specifically, several studies have shown that individuals perceive and interpret disorder differently (Hipp, 2010; Katzet al., 2011; Latkin et al., 2009; Sampson and Raudenbush, 2004; Taylor, 2009; Wallace, forthcoming; Wallace et al., forth-coming). As a result, the theorized interpretive meanings behind disorder cues, particularly those that convey the potentialfor criminal victimization, may not be what individuals read into disorder cues (Wallace, forthcoming). If disorder is indeedinterpreted differently, specifically if it is interpreted in ways that does not generate fear of crime, then the path betweendisorder and health breaks down. As a consequence, the pathways between disorder, fear of crime, and health need to beestablished so that current and future work in this arena is valid.
In response to this lacuna in research, the aim of this study is to establish whether fear of crime indeed mediates the rela-tionship between disorder, health and mental health. Thus, the primary research question of this study is, simply, does fearof crime mediate the relationship between individual disorder perceptions and health? If disorder perceptions do engender afear response, then the relationship between disorder and health outcomes should be stable. However, if disorder percep-tions do not produce fear of crime, then the relationship between disorder and health is in question. Using structural equa-tion modeling, this study considers that measures of fear of crime mediate the relationship between disorder perceptionsand measures of self-rated health, depression, and anxiety.
The bulk of research studying the health consequences of neighborhood disorder suggests a strong relationship betweendisorder perceptions, fear of crime, and negative health consequences; however, that relationship is predicated on individ-uals’ perceptions of disorder generating a negative emotional response (i.e., fear of crime). A large part of the emotions, stressand health literature focuses on how individuals’ perceptions of their personal situation can be more powerful predictors ofhealth (Singh-Manoux et al., 2005). For example, subjective social status is considered a more precise measure of one’s socialposition because it includes individuals’ past, current, and future prospects in their evaluation of social position (Singh-Man-oux et al., 2005). As a result, subjective social status is a better means of assessing how one’s social position impacts healthbecause it takes into consideration how individuals’ understandings of their relative social position. Similarly, by exploringthe relationship between individuals’ disorder perceptions, not objective neighborhood conditions, and personal health, thisstudy enables us to understand how perceptions impact emotionally based fear responses, and how they ‘‘gets under theskin’’ to effect health. While we know that neighborhoods are associated with health, we do not precisely know why (Mac-Intyre and Ellaway, 2003). The approach of this paper will enable one of those effects, the psychosocial response to neigh-borhood conditions, to be tested.
2. Literature review
Neighborhood disorder is one means of conceptualizing the effects that deleterious aspects of the neighborhood environ-ment have on personal health. Neighborhood disorder can be seen as visual cues in the neighborhood environment, whichsignal to residents that they may become a victim of crime and that the neighborhood does not have the ability to mobilizeto ameliorate its problems (Hunter, 1978, 1985; Taylor, 2001). Conversely, when defined in terms of social control, effec-tively, disorder constitutes visual signals that the norms of what is considered appropriate physical and social controls ofthe neighborhood have been violated (Bursik and Gramsmick, 1993; Skogan, 1990). Disorder can take both physical and so-cial forms. Specifically, physical disorder includes ‘‘the deterioration of urban landscapes, for example, graffiti on buildings,abandoned cars, broken windows, and garbage in the streets’’ (Sampson and Raudenbush, 1999, p. 604), while social disorderis behavior by individuals on the street that can be construed as threatening (Sampson and Raudenbush, 1999; Woldoff,2002). If disorder is considered a continuum (Sampson and Raudenbush, 1999), social disorder is generally considered amore severe type of disorder; its presence conjures fear in residents and eventually withdrawal from community life (Bursikand Gramsmick, 1993; Sampson and Raudenbush, 1999; Skogan, 1990; Taylor and Covington, 1993; Wilson and Kelling,1982). What makes disorder different from other neighborhood conditions related to health is its ability to have both directand indirect effects on health.
Neighborhoods and health researchers typically discuss the link between neighborhood disorder and health as either anenvironmental or psychophysiological one. Disorder may impact health in the following ways: either (1) disorder has a di-rect effect on health by creating a noxious neighborhood environment that is detrimental to health, or (2) disorder has anindirect effect on health as a personal stressor that is also injurious to health. When considered as part of a noxious environ-ment, disorder is seen as a measure of the ambient urban environment that become biological stressors or environmentalhazards (Cagney et al., 2009; Ewart and Suchday, 2002). Here, disorder is operationalized slightly outside of the traditional,more criminological, conceptions mentioned earlier. Physical cues such as odor and noise are included as signs of incivility

D. Wallace / Social Science Research 41 (2012) 1515–1528 1517
and urban decay (Cagney et al., 2009; Ewart and Suchday, 2002). In this way, disorder is thought to touch the individual di-rectly (Cagney et al., 2009; Ewart and Suchday, 2002).
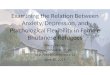
In its indirect form, when disorder is considered a personal stressor, it is due to the psychophysiological response disorderis theorized to produce (Ross and Mirowsky, 2001). From this perspective, disorder is seen to impact health by generatingpsychophysiological responses, such as fear of crime, that erode an individual’s health either through a psychophysiologicalresponse or by impacting an individual’s willingness to engage in health-protective behaviors (Ross, 2000a; Ross and Mirow-sky, 2001). The generation of a psychophysiological response through disorder begins when individuals perceive disorder intheir neighborhood. Once individuals perceive disorder as threatening, it generates fear of crime, or a ‘‘negative emotionalreaction generated by crime or symbols of crime’’ (LaGrange et al., 1992, p. 73). When individuals fear crime, or have that‘‘negative emotional reaction’’ (LaGrange et al., 1992), their fight or flight response is activated (Ross and Mirowsky,2001). The fight or flight response is the body’s way of coping with threatening situations and environments (Memmleret al., 1996), which, when threatened activates individuals’ endocrine systems releases adrenaline to enable them to combatthe threat or flee (McEwen, 2000; Memmler et al., 1996). There are detrimental effects to health when the fight or flight re-sponse is regularly activated. For example, chronic stress can exacerbate chronic illness, or assist in the thickening of arteries(McEwen, 2000). People who live in disorderly neighborhoods experience more frequent, and more intense, activation of thestress response, through fear of crime, and are thus more likely to have negative health consequences (Ross and Mirowsky,2001). Fig. 1 displays the theoretical pathways between disorder, fear of crime and health. In extreme situations, the pres-ence of disorder can have life threatening effects. In his book, Heat Wave, Eric Klinenberg (2002) demonstrates that neigh-borhoods with high crime and disorder coupled with little social capital and neighborly connectedness had much higherlevels of heat wave related mortality. Additional research examining the 1995 Chicago Heat Wave concluded that neighbor-hood commercial decline, including disorder cues such as burnt out or boarded buildings, also contributed to heat wave mor-tality (Browning et al., 2006; Klinenberg, 2002).
In addition to the fight or flight response, disorder and fearfulness can impact personal behavior. Once fearful, individualsbegin to feel and act differently towards engaging in neighborhood life, often withdrawing into their homes (Cagney et al.,2009; Ross, 1993; Ross and Mirowsky, 1999, 2001; Taylor, 2001; Wilson and Kelling, 1982). Neighborhood withdrawal thenleads to reduced levels of neighborhood-level social cohesion and social control (Taylor, 2001), which is also shown to havenegative health effects. Fearfulness also impacts individuals’ willingness to engage in health protective behaviors, such aswalking (Cagney et al., 2009; Ross, 1993, 2000a).
The link between disorder perceptions and mental health is slightly different than stated above. A significant amount ofresearch shows that disorder impacts mental health, such as heightening depression (Latkin and Curry, 2003; Ross, 2000b),mistrust (Ross and Jang, 2000; Ross et al., 2001), powerlessness (Geis and Ross, 1998; Ross et al., 2001), reducing overall psy-chological well-being (Hill and Angel, 2005; Hill et al., 2005a; Ross et al., 2000), and even self-esteem (Haney, 2007). Theperception of disorder and fear of crime can weigh heavily on individuals, as the research noted above shows, and can easilyreduce psychological well-being in a multitude of ways. Haney (2007) suggests that ‘‘blighted and decaying neighborhoodsare read as disinvestments both by residents and the city governments, and therefore, these images are internalized andincorporated into residents’ psychological makeup’’ (p. 968). Others suggest that ‘‘the daily stress associated with livingin a neighborhood where neighbors are not trustworthy, and danger, trouble, crime, are common may produce feelings ofdepression’’ (Ross and Mirowsky, 2000, p. 178). Thus, the relationship between mental health and disorder has a differentprocess than that of general health; here the stress response that is generated by disorder perceptions and fear of crimenot only wears on the body but also on the mind. As a consequence, disorder, fear of crime, and the stress response theyactivate are internalized by the individual, thereby affecting mental health.
There are some distinctions in the fear of crime literature that are important to note for this study. The link between fear ofcrime and health outcomes, particularly psychological ones, is long standing. In the past, scholars note that fear generates re-sponses from the endocrine system that are potentially harmful (Sarnoff and Zimbardo, 1961). Ferraro (1995) notes, ‘‘fear acti-vates a series of complex bodily changes alerting the actor to the possibility of danger’’ (p. 24). However, fear of crime itself isnot a singular concept. Ferraro (1995) suggests that fear of crime is an interaction between the individual’s levels of reference,whether at a more general abstraction or personal level, and the evocation of a negative emotional fear based response.
Typically, fear of crime is specified in two ways: general fear of crime and offense specific fear of crime (Ferraro, 1995;Roundtree and Land, 1996; Warr and Stafford, 1983). On the one hand, general fear of crime represents the emotional
Disorder Perceptions
General Fear of Crime
Offense-Specific Fear of Crime
Self-Rated Health, Depression, or
Anxiety
Fig. 1. The theoretical model showing the paths between disorder perceptions and the health outcomes.

1518 D. Wallace / Social Science Research 41 (2012) 1515–1528
response from the individual that is generated in a more diffuse way and referent to the over all likelihood of being a victimof crime (Warr and Stafford, 1983). On the other hand, offense specific fear of crime extracts which fears trouble individualsthe most in conjunction with their emotional responses of fear of being a victim of specific crimes (LaGrange and Ferraro,1987; Roundtree and Land, 1996; Warr and Stafford, 1983). Warr and Stafford (1983) state that not all crimes generate equallevels of fear in individuals; the crimes that generate the strongest levels of offense specific fear of crime typically involvepersonal property and stranger attack. As a result, fear of crime can be measured in ways that tap a more generalized emo-tional response (‘‘How afraid are you to walk alone in your neighborhood?’’), to a more targeted emotional response to fear ofa specific crime (‘‘How fearful are you of your home being burgled?’’) (Warr and Stafford, 1983).
The range of emotional responses produced by fear of crime has implications for the ability to produce health conse-quences. General fear of crime taps into a person’s general emotional response to safety in their neighborhood. Here, fearof crime is seen as the ‘‘negative emotional reactions generated by crime or symbols associated with crime’’ (Ferraro andLaGrange, 1987, p. 73). In this case, fear of crime is seen as a constant, low-level stressor, that while still harmful, mightnot produce the strong bodily response in individuals that offense-specific fear of crime would. On the contrary, offense-spe-cific fear of crime, where one distinctly fears being a victim of a particular crime, such as assault, robbery, or rape, is incident-based (Roundtree and Land, 1996). Here, individuals who report being fearful of particular crimes most likely are referencinga particular instance or threat they have experienced in the neighborhood that made them fearful. Due to this, offense-spe-cific fear of crime may be more likely to produce the endocrine response readily linked to fear.
There is a plethora of research revealing the link between fear and health (Jackson and Stafford, 2009; Ross and Jang,2000; Stafford et al., 2007); for instance, Jackson and Stafford (2009) show that there is a recursive relationship between fearof crime and individuals’ health. Individuals with lower health tend to be more worried about crime due to perceived vul-nerability (Killias, 2000; Stafford et al., 2007), while that worry only serves to further diminish health (Jackson and Stafford,2009). Early work differentiates between general and offense-specific fear of crime (Ross, 1993). Ross (1993) demonstrateswith structural equation modeling that fear of crime has a negative effect on health protective behaviors, namely walking,which mediate the effect that fear of crime has on personal health.
However, there is little research that looks at the causal relationship between disorder, fear of crime, and personal andmental health. There have been three studies that explore the pathways between these variables, via structural equationmodeling, though none directly study the relationship stipulated above. Ross (1993) shows that fear of victimization impactshealth and is primarily mediated by psychological distress and walking. While this study shows the direct link between fearand health, disorder is not considered. Haney (2007) shows that disorder perceptions mediate the relationship betweenneighborhood poverty and self-esteem, and suggests that a degraded urban environment is readily internalized by individ-uals. Hill et al. (2005a,b) show that neighborhood disorder is associated with poor health; furthermore, the relationship ismediated by the psychological (i.e., anxiety) and physical distress (e.g., difficulty breathing). Lastly, Hill and Angel (2005) findthat there is an association between disorder and the negative health behavior of drinking, and that association is mediatedby anxiety and depression. While these two studies show that disorder impacts health and health behaviors, the operation-alization of disorder is questionable since the disorder scales include variables that cannot exclusively be considered disor-der. Due to the inconsistencies in the measurement of disorder, there is currently only ancillary evidence that there is adirect relationship between disorder and physical and mental health, as mediated by fear of crime.
3. Data and methods
3.1. Data
This study utilizes the first wave of the Community, Crime and Health (CCH) Surveys (Ross and Britt, 1995, 1998). The goal ofthe CCH is to understand and explain the links between neighborhoods, crime, and physical and mental well-being (Ross and Britt,1995, 1998). The CCH is a probability sample of Illinois households. Respondents were interviewed by telephone and were se-lected trough a prescreened random digit dial technique (Ross, 2000a; Ross and Jang, 2000). This technique reduced the numberof non-eligible contacts (i.e., businesses and nonworking phone numbers), decreases the standard errors when compared to thosecalculated with the Mitofsky–Waksberg methods, while simultaneously producing a sample with similar demographic charac-teristics (Ross, 2000a; Ross and Jang, 2000). Once contact was made, the individual within the household with the most recentbirthday was selected for the interview (Ross, 2000a; Ross and Jang, 2000). Additionally, only English speaking adults were inter-viewed (Ross, 2000a; Ross and Jang, 2000). Lastly, as many as 10 calls were made to contact a respondent, and up to 10 calls weremade to complete interviews (Ross, 2000a; Ross and Jang, 2000). Wave 1, which is employed in this study, was collected in 1995,had a response rate of 73% (Ross, 2000a; Ross and Mirowsky, 1999, 2001). While the CCH contains neighborhood-level (censustract) information, it is important to note it was not cluster sampled, making hierarchical modeling untenable. Since the CCH em-ployed a random-digit dial sampling technique, this strategy resulted in small numbers of respondents per census tract (on aver-age, less than two individuals per tract). The final sample size after data cleaning for this study is 1773.
3.2. Dependent and independent variables
Self-rated health is assessed by asking respondents, ‘‘Would you say your health is very poor, poor, satisfactory, good orvery good?’’ Self-rated health is measured on a five-point scale, where 0 is ‘‘Very Poor,’’ 1 is ‘‘Poor,’’ 2 is ‘‘Satisfactory,’’ 3 is

D. Wallace / Social Science Research 41 (2012) 1515–1528 1519
‘‘Good,’’ and 4 is ‘‘Very Good.’’ However, nearly 85% of the sample rates their health as either good or very good; the remain-ing 15% rate their health as satisfactory, poor, or very poor. To address this, self-rated health was collapsed into a dummyvariable where 0 represents ‘‘Very Poor, Poor, and Satisfactory’’ self-rated health, while 1 represents ‘‘Good and Very Good’’self-rated health.1 Self-rated health is a valid measurement of health status (Browning and Cagney, 2002; Goldstein et al., 1984;Wilson and Kaplan, 1995), with strong predictive validity for morbidity (Ferraro et al., 1997) and disability (Idler and Benyamini,1997).
The respondents’ mental health is measured by assessing respondents’ levels of depression and anxiety. Depression is acombination of reduced mood and physiological symptoms of melancholy (Mirowsky and Ross, 1989; Ross et al., 2000). Inthis study, depression is measured using a smaller, seven-item version of the Center for Epidemiological Studies DepressionScale (CESD; Ross and Mirowsky, 1984). The items include the following: (1) had trouble getting or staying asleep, (2) feltthat everything was an effort, (3) felt that you just could not get going, (4) had trouble keeping your mind on what you weredoing, (5) felt sad, (6) felt lonely, and (7) felt you could not shake the blues? For each of the above questions, respondentswere asked how many days out of the week they felt that particular way. The average of the above questions constitutes thedepression scale. The mean response for the depression scale is 0.668. The anxiety scale is a three-item scale and is replicatedfrom previous studies looking at neighborhoods and health (Hill et al., 2005b; Ross et al., 2000). The anxiety scale is the aver-age score from the following variables, ‘‘how many days a week are you,’’ (1) worried a lot about little things, (2) felt tense ofanxious, and (3) felt restless. The mean response for the anxiety scale is 1.717. Both scales are quite reliable; the depressionscale has an alpha of 0.76, while the anxiety scale has an alpha of 0.79.
Many studies distinguish the effect that disorder has on physical and mental health by differentiating the level at whichdisorder impacts the individuals, be it as a neighborhood condition or individuals’ perceptions of disorder. When disorder isconsidered a neighborhood condition, it influences health and mental health by generating fear of crime in individuals. Inthis sense, disorder is ideally measured through objective assessments of disorder (see Sampson and Raudenbush, 1999).More often, disorder is an aggregate of individual perceptions under the assumption that individuals perceive disorder objec-tively, thus making an aggregate measure, such as a neighborhood average of disorder perceptions, reflects the ‘‘on theground’’ reality (Ross and Mirowsky, 1999). While neighborhood perceptions of disorder are generally thought of to be accu-rate assessments of objective neighborhood conditions (Ross and Mirowsky, 1999; Sampson and Raudenbush, 1999), extantresearch has shown that this is not always the case. Research has demonstrated that both personal characteristics (Hipp,2010; Sampson and Raudenbush, 2004; Wallace, forthcoming), and neighborhood characteristics (Sampson and Rauden-bush, 2004) influence disorder perceptions. Furthermore, bias in perceptions remains even when the ecological unit is highlyconstrained (Hipp, 2010). Therefore, when dealing with individual outcomes and disorder, it is often more appropriate toconsider the effect perceptions of disorder have on individuals’ outcomes given that they more readily reflect emotionalresponses.2
Similar to many other surveys, disorder is measured in the CCH survey by asking the respondents if they agree with aseries of questions surrounding problems typically experienced in neighborhoods (Ross, 2000a; Ross and Mirowsky,1999). Of concern in this study are four disorder questions, specifically, perceptions of abandoned buildings, graffiti, vandal-ism, and people hanging out; these questions form the disorder perception scale. Each respondent was asked to rate howstrongly they agree or disagree with the following statements: there are a lot of abandoned buildings in my neighborhood,there is a lot of graffiti in my neighborhood, vandalism is common in my neighborhood, and there are too many people hang-ing out. Each cue is coded from 0 ‘‘Strongly Disagree,’’ 1 ‘‘Disagree,’’ 2 ‘‘Agree,’’ and 3 ‘‘Strongly Agree.’’ In previous research,this scale has been shown to be highly reliable (Ross and Mirowsky, 1999). Disorder is operationalized as a latent variableusing the above cues. The measurement model shows good fit to the data with RMSEA = 0.065, CFI = 0.998 and TLI = 0.998.
3.3. Mediating variables
Literature shows that fear of crime can be either general or offense-specific (Roundtree and Land, 1996; Warr and Staf-ford, 1983). Questions such as ‘‘I am afraid to walk alone at night’’ tap into general feelings of fear (Roundtree and Land,1996). On the other hand, having respondents note how many days a week they are fearful of a specific offense or occurrencegives estimates of the negative emotions related to fear that are produced by fear of specific crime (LaGrange et al., 1992;Roundtree and Land, 1996; Warr and Stafford, 1983). Keeping with this, this study differentiates between general fear ofcrime and offense-specific fear of crime. The CCH measures fear of crime with a series of variables that both types of fear
1 Collapsing a five-category self-rated health variable into a dummy variable has been done in other studies where there is a skewed distribution of self-ratedhealth (Millunpalo et al., 1997). Where there is concern over placing ‘‘Satisfactory’’ together with ‘‘Poor’’ and ‘‘Very Poor’’, the category of ‘‘satisfactory’’ issimilar to ‘‘fair’’ in the self-rated health variables used in the studies mentioned above. Additionally, research has shown that regardless of the specification, theself-rated health measure and the effects it elicits are typically robust to the specification of the health categories measured in the variable. Lastly, as arobustness check, the models presented here were run with a different specification of self-rated health – namely where 1 also contained ‘‘satisfactory’’ – andthe results were no different than the final models presented.
2 Given that this study deals with constructs, particularly disorder, which could be measured at the neighborhood level, nesting the data into individual andneighborhood levels may be appropriate. Unfortunately, the data, and how it was sampled restricts the analysis to one level. The CCH survey was not clustersampled; instead it was a random digit dial of residents in the state of Illinois. When nested, there, on average, are less than two people per neighborhood,which is untenable for a nested analysis. Neighborhood conditions were modeled as a control in earlier models; however, they had no effect and whereremoved for parsimony.

1520 D. Wallace / Social Science Research 41 (2012) 1515–1528
of crime. First, general fear of crime is assessed by asking respondents how much they agree or disagree with the statement,‘‘I am afraid to walk alone at night.’’ Here, 0 is Strongly Disagree while Strongly Agree is 3. On the other hand, offense-specificfear of crime is assessed through two variables that tap into a respondent’s levels of fear. Respondents are asked ‘‘in the pastweek, how many days have you feared. . .’’ being robbed, attacked or injured, or your house being broken into. Unfortunately,responses assessed through the two variables, offense-specific fear of crime are highly skewed. A strong majority of respon-dents report never being fearful, of either offense in the past week, and a substantial minority report being fearful all thetime. While it is best to include all information available, because the distribution of these variables are so skewed, they havebeen collapsed into dummy variables, where 1 indicates that the respondent has been fearful of being robbed, attacked orinjured or having their house being broken into at least one time in the past week. Appendix A shows the distributions of thetwo offense-specific fear of crime variables prior to being recoded as dummies.
3.4. Control variables
A battery of individual characteristics serves as controls. They include race, sex, age, having children, income, employ-ment, education level, chronic disease, and smoking. First, race is a dummy variable ‘‘non-white’’ where 1 represents thatthe respondent is not white, while 0 is White. Sex is measured by the dummy variable Female, where 0 is Male and 1 is Fe-male. Age is measured as a linear variable; the average age in the sample is 43. The variable ‘‘Kids’’ is a dummy variablesdenoting whether the respondent has children. Income is the respondents’ reported family income in dollars. A significantproportion of the initial sample (approximately 716 respondents of the initial sample of 2482) did not provide informationon their family income. Of the 716 respondents in the original sample that were unwilling to report the income in dollars,328 were willing to report their income as a categorical variable. As a result, 388 respondents remained without any incomeinformation; therefore, their income values where imputed. To impute income for the remaining respondents, the respon-dents who reported their income as a category were mid-point coded, meaning the midpoint of the income category theyreported became their income in dollars. Income was imputed using the set of controls discussed below. Due to missing dataon other variables, imputed income was used for only 229 respondents in the final sample. Analyses were run comparingindividuals who had their income score imputed, versus those whose score was not; results showed little difference betweenindividuals who did and did not have their income scores imputed. Also, the income variable is centered. Full-Time Employ-ment is a dummy variable denoting that the respondent works full-time. Education is by a dummy variable representing NoHigh School Diploma. To control for the impact that a chronic disease may have on health, included is a variable that des-ignates whether or not the individual has a chronic disease (1 – Yes, 0 – No). If the respondent reports that they have beentold by a doctor that they have any of the following diseases, they receive a score of 1 on this variable: heart disease, highblood pressure, lung cancer, breast cancer, other type of cancer, diabetes, arthritis, osteoporosis, allergies or asthma, or diges-tive problems. An additional dummy variable is included for whether or not the respondent smokes.3 Finally, both disorderperceptions and health have the potential to be impacted by neighborhood conditions. I tested whether neighborhood charac-teristics, specifically concentrated disadvantage, residential stability and percent Black, have an effect on disorder perceptionsand health. I found that these neighborhood level variables do not have an effect on either disorder perceptions or health. In theinterest of parsimony, these variables are not included in the models presented here. Table 1 shows the summary statistics forall the independent variables and individual controls. Lastly, Fig. 2 displays the full SEM that was modeled while Figs. 3–5 showthe trimmed SEMs for the three dependent variables.
4. Results
This study endeavors to understand the effects that individuals’ disorder perceptions and fear of crime have on their self-rated health and mental health. To do this, I employ structural equation modeling for binary variables using MPLUS 5.0(Muthen and Muthen, 1998–2007). MPLUS allows for fitting models that contain binary and categorical variable, which isof issue here. First, a measurement model is constructed which uses confirmatory factor analysis to estimate the disorderperception scale. Next, three SEM models are fitted to estimate the relationship between disorder perceptions and health,depression, and anxiety, and to assess whether the two fear of crime variables mediate the above relationships.
To develop the measurement model, I employ a small disorder scale based off of Ross and Mirowsky’s (1999) disorderscale. The scale created here includes only the physical and social disorder measures from Ross and Mirowsky’s (1999).4
The measurement model in this study has good model fit (see Table 2 for the standardized and unstandardized estimates ofthe measurement model). All variables in the scale loaded highly onto the factor and are statistically significant. This model
3 In the coming models, smoking is modeled on health. However, it is worth noting that smoking behavior has the potential to impact individuals’ disorderperceptions. Individuals’ routine activities related to smoking may potentially increase their exposure to disorder, thus potentially increasing individuals’disorder perceptions. To assess if this is the case, I ran models where smoking was included as a variable to control for disorder perceptions; smoking is notsignificantly related to disorder. As a result, I excluded it from the paths leading to disorder, but retained smoking as a path effecting health.
4 The disorder scale used by Ross and Mirowsky (1999) has four domains: physical disorder, social disorder, physical order, and social order. Excluded fromthis scale are the measures of social and physical order, as well as ‘‘My neighborhood is noisy’’, ‘‘I’m always having trouble with my neighbors’’ and ‘‘There is alot of crime in my neighborhood.’’ While these questions may load highly onto their disorder scale, they do not sit closely to the definition of disorder being avisual phenomenon and thus were excluded from the scale.

Fear of being robbed, attacked or injured
Fear of home being broken into
Afraid of walkingalone at night
Self -Rated HealthDisorder Perceptions
Graffiti
Vandalism
Abandoned Buildings
Hanging Out
Non-white
Female Age
Kids
Family Income
No High School
Diploma
Non-white
Female Age
Kids
Family Income
Employment
No High School
Diploma
Chronic Disease
Smoke
Employment
Fig. 2. The full SEM model for the dependent variables self-rated health, depression, and anxiety.
Fear of being robbed, attacked or injured
Fear of home being broken into
Afraid of walking
alone at night
Self-Rated HealthDisorder
Perceptions
Graffiti
Vandalism
Abandoned Buildings
Hanging Out Chi-Square = 216.48
df = 34, p < 0.000 CFI = 0.973 RMSEA = 0.055
-0.236***
0.073*
0.916***
0.731***
0.808***
0.890***
0.239***
0..330***
0.671***
Fig. 3. The SEM showing standardized coefficients for the trimmed path model between disorder and health.
D. Wallace / Social Science Research 41 (2012) 1515–1528 1521
was evaluated several ways for goodness of fit. First, the chi-square for the model is 17.618, with 2 degrees of freedom, and issignificant. The loadings of the variables in the scale are quite high, ranging from 0.72 to 0.92. Next, the Root Mean Square Errorof Approximation (RMSEA) is 0.06 and the Comparative Fit Index (CFI) is 0.99. While the RSMEA is slightly higher than thethreshold of 0.05 that is generally suggested for good model fit, the CFI is well within the range of good model fit. Therefore,the measures included in the disorder perception scale are good indictors of the latent concept of disorder.
4.1. Fear of crime as a mediator between disorder perceptions and self-rated health
In the first SEM, I explore whether general and offense-specific fear of crime mediates the relationship between disorderperceptions and health. Fig. 3 shows the path diagram with standardized coefficients. Model 1 in Appendix B displays the fullresults for the model. There are a few exogenous variables that significantly impact disorder perceptions, namely non-whitesand individuals with higher income perceive more disorder, and individuals without a high school diploma perceive less.Several exogenous variables predict self-rated health. Non-whites, females, younger individuals, those without a high schooleducation, those with chronic illnesses, and smokers are less likely to rate their health positively. Conversely, individualswith children or an above average income are more likely to rate their health positively.
As for the relationship between disorder and fear, higher levels of disorder perceptions are significantly related to higherlevels of all three fear levels of crime variables. As for health, disorder perceptions negatively impact self-rated health, mean-ing, people with higher perceptions of disorder are less likely to rate their health positively. However, not all the fear of crime

Fear of being robbed, attacked or injured
Fear of home being broken into
Afraid of walking
alone at night
DepressionDisorder
Perceptions
Graffiti
Vandalism
Abandoned Buildings
Hanging Out Chi-Square = 216.46
df = 34, p < 0.000 CFI = 0.973 RMSEA = 0.055
-0.063*
0.239***
0.127***
0.095***
0.330***
0.239***
0.671***
0.916***
0.890***
0.808***
0.732***
Fig. 4. The SEM showing standardized coefficients for the trimmed path model between disorder and depression.
Fear of being robbed, attacked or injured
Fear of home being broken into
Afraid of walking
alone at night
AnxietyDisorder
Perceptions
Graffiti
Vandalism
Abandoned Buildings
Hanging Out
Chi-Square = 216.40 df = 34, p < 0.000 CFI = 0.974 RMSEA = 0.055
0.132***
0.120***
0.239***
0.120***
0.671***
0.916***
0.890***
0.808***
0.732***
Fig. 5. The SEM showing standardized coefficients for the trimmed path model between disorder and anxiety.
1522 D. Wallace / Social Science Research 41 (2012) 1515–1528
variables predicts health; only the general fear of crime variable, afraid to walk alone at night, does. Here we see that peoplewho say they are more afraid to walk alone at night rate their health more positively; however, the significance is moderate(p < 0.10) and the coefficient is small (0.073).
To test whether fear of crime, whether general or offense specific, mediates the relationship between disorder perceptionsand health, I explore the indirect effects of fear of crime on health. A variable is a mediator when it accounts for some of theassociation between the predictor (disorder) and the outcome (self-rated health, and later depression and anxiety; Baron andKenny, 1986; Simons et al., 2007, 2006). To establish if a variable mediates a relationship, the following conditions must bemet: (1) the predictor and outcome must be statistically related, (2) the mediating variable is statistically related to both thepredictor and outcome, and (3) when controlling for the effect of the mediating variable, the effect should reduce the directrelationship between the predictor and outcome (Baron and Kenny, 1986). As before, SEM was used to establish whether fearof crime, both general and offense-specific, has a mediating effect on the relationship between disorder perceptions andhealth. Table 3 displays the results from the test of the indirect effect on each of the three SEMs that were run with the threeoutcomes (self-rated health, depression, and anxiety). Looking at the first model in Table 3, disorder has a strong, direct im-pact on health. However, for fear of crime, only general fear of crime mediates the relationship between disorder and health,and the indirect effect is small and only moderately significant (p < 0.10); this is also shown in Fig. 1. This suggests disorderdoes influence levels of general fear of crime, which in turn has a negative impact on health. The model fit estimates aregood; while the chi-square is significant (v2 = 216.400, df = 34, p < 0.01), the CFI is 0.974 and the RMSEA is 0.055. While thesemodel fit statistics are not perfect, they do show that the model is a decent fit.
4.2. Fear of crime as a mediator between disorder perceptions and mental health
Appendix C shows the results of the SEMs that test whether general and offense-specific fear of crime mediates the rela-tionship between disorder perceptions and depression (Model 2) and anxiety (Model 3). Figs. 4 and 5 show the trimmed path

Table 1Summary statistics for all variables.
Mean/percentage Standard error
Health measuresSelf rated health 86.4% –Anxiety 1.717 0.043Depression 0.668 0.025
Disorder scaleAbandoned buildings 0.543 0.014Vandalism 0.745 0.016Graffiti 0.606 0.015Hanging out 0.809 0.019
General fear of crimeAfraid to walk alone at night 0.854 0.018
Offense specific fear of crimeFear of being robbed, injured, or attacked 5.5% –Fear of home being broken into 8.0% –
Non-white 14.4% –Female 58.0% –Age 43.38 0.385Have children 85.2% –Family income 0.149 1.830Employment 60.9% –No high school diploma 6.9% –Chronic disease 63.5% –Smoker 25.0% –
n = 1773
Table 2Measurement model for the latent disorder measure.
Question Unstandardized estimate Standardized estimate
Abandoned buildings 1.000 0.816Vandalism 1.312 0.880Graffiti 1.731 0.926Hanging out 0.732 0.719
n = 1773.
Table 3Significance of the indirect effects of the fear of crime variables between disorder perceptions and health outcomes.
Standardized estimate SE t
Model 1: Disorder perceptions to self-rated health �0.209*** 0.057 �3.695Indirect effects
Walk alone at night 0.117* 0.026 1.690Fear of being robbed attacked or injured 0.089 0.007 0.956Fear of home being broken into 0.054 0.009 0.252
Model 2: Disorder perceptions to depression �0.063* 0.029 �1.660Indirect effects
Walk alone at night 0.064*** 0.013 3.774Fear of being robbed attacked or injured 0.037*** 0.005 6.257Fear of home being broken into 0.042*** 0.006 5.488
Model 3: Disorder perceptions to anxiety 0.008 0.055 0.839Indirect effects
Walk alone at night 0.024 0.027 0.247Fear of being robbed attacked or injured 0.031*** 0.008 5.048Fear of home being broken into 0.040*** 0.011 4.768
n = 1773.��p < 0.05.*** p < 0.01.* p < 0.10.
D. Wallace / Social Science Research 41 (2012) 1515–1528 1523

1524 D. Wallace / Social Science Research 41 (2012) 1515–1528
diagrams with standardized coefficients for these models; coefficients for the exogenous variables are suppressed. Beginningwith the relationship between disorder perceptions and depression, there are no exogenous variables that significantly pre-dict disorder perceptions. On the other hand, several of the controls predict depression. Non-white, females, people withouta high school diploma, those with chronic diseases and smokers have higher depression scores, while younger individuals,people with high family income, and those who are employed full time report lower depression scores. As with the previousmodel, disorder perceptions strongly predict all fear of crime variables, specifically, higher disorder perceptions equate tohigher levels of fear of crime. Additionally, all of the fear of crime variables predict depression, and the two offense-specificfear of crime variables have a stronger relationship to depression. Disorder does predict depression, though the relationshipis only moderately significant (p < 0.10).
When examining the mediating effects in Table 3 in Model 2, we see that disorder not only has a direct effect on depres-sion (though it is small and only moderately significant), its effect is also mediated by the three fear of crime variables. Fur-thermore, the model fit is also adequate. The previous model, the chi-square is significant (v2 = 216.464, df = 34, p < 0.01), theCFI is 0.973 and the RMSEA is 0.055.
Testing the mediating effect of fear of crime on the relationship between disorder perceptions and anxiety in Model 4does not show much promise. Several exogenous variables predict disorder perceptions: non-whites and individuals withouta high school diploma perceive more disorder, while individuals with a higher family income perceive less. Several exoge-nous variables also predict anxiety. Females, those with a chronic disease, and who smoke, report higher levels of anxiety,while conversely, individuals who are younger and have a higher family income report lower anxiety. Furthermore, disorderperceptions strongly predict all three of the fear of crime variables. However, there is no direct relationship between disorderperceptions and anxiety. Therefore fear of crime cannot mediate the relationship between disorder and anxiety.
When testing the indirect effects (Table 3), we see that there is no direct effect between disorder and anxiety. There aresignificant, indirect effects between the two offense-specific fear of crime variables and anxiety. As with the previous mod-els, the model fit is also adequate: the chi-square is significant (v2 = 216.488, df = 34, p < 0.01), the CFI is 0.973 and theRMSEA is 0.055.
To sum up, these results suggest that fear of crime does mediate the relationship between self-rated health and depres-sion, though not anxiety. Furthermore, the indirect effect between fear of crime and self-rated health and the direct effectbetween disorder and depression are moderately significant. While this work does show the presence of a disorder – fearof crime – health link, is a weak one.
5. Discussion
MacIntyre and Ellaway (2003) wisely note that ‘‘one of the main problems in the study of neighborhoods and health is thelack of development of theories about plausible social, psychological, and biological links between specific features of theneighborhood and specific health outcomes’’ (p. 34). The goal of this analysis has been clarify some of these links by explor-ing the mediating relationship that two distinct measures of fear of crime have between disorder and the health measures.Because structural equation modeling, effectively, is a test of how well the observed patterns in the dataset match the the-oretical patterns suggested by the researcher (Gau, 2010), by using SEM, this study can establish if the proposed relationshipbetween disorder and health, as well as fear of crime as a possible mediator to that relationship, is a valid one.
In general, the findings of this study show that both general and offense specific fear of crime do mediate the relationshipbetween disorder and health or mental health; however, there are some caveats. First, while fear of crime does mediate therelationship between disorder and health, some of the mediating effects were weak. The same applies with depression:while all types of fear of crime have a positive (i.e., increasing) impact on depression, there is only a small and negative directlink between disorder perceptions and depression. For the dependent variable of anxiety, on the other hand, fear of crime inany form is not a mediator. Thus, while the pathways have been confirmed, at least between depression and health, theseresults suggest a need for more research to reaffirm this link. Secondly, when testing whether fear of crime mediates therelationship between disorder and depression, offense-specific fear of crime had stronger associations with depression thangeneral fear of crime. Thus, it is important to think about fear of crime in multiple ways when linking fear and health.
Given the prevalence of the association between disorder fear and health in extant research, why are the mediating path-ways in this study present, but weak? Conceivably, the most straightforward explanation is how this study conceptualizedand operationalized disorder. Here, when compared to other studies, disorder was defined as simply the visual cues within aneighborhood that signal the potential for crime, victimization, and general neighborhood problems. This definition is clo-sely tied to the original definitions of disorder offered by criminologists in the late 1970s and early 1980s (see Wilson andKelling, 1982; Garofalo and Laub, 1978). However, there are several studies which examine this relationship that have con-ceptualized disorder in other ways, resulting in differing findings. Indeed, some studies include indictors of disorder that arenot strictly disorder, such as having trouble with neighborhoods or noise (for examples of this, see Hill and Angel, 2005; Hillet al., 2005a,b, and Ross and Mirowsky, 1999). The unfortunate part of these scales is that items nested in these scales aretightly related to the issues of social control, social disorganization, and many of the other neighborhood characteristics, wellknown to be associated with the structural neighborhood conditions related to the presence of disorder. In the end, whendisorder perceptions include questions that tie into other neighborhood concepts related to both health and the prevalence

D. Wallace / Social Science Research 41 (2012) 1515–1528 1525
of disorder in a neighborhood, it becomes difficult to disassociate the direct effect that disorder has on health from otherneighborhood constructs.
This does not mean that disorder is unrelated to health, but rather, that future research should be conscious of how dis-order is defined and measured. Cagney et al. (2009) note that while many studies have constructed measurements that ad-dress how neighborhood processes impact individual health, tests of the reliability and validity of such measures arevirtually non-existent. For neighborhoods and health researchers, disorder is conceptualized and categorized in the sameway for health contexts as it is for sociological or criminological contexts, specifically, that disorder generates fear of crime.The weak paths uncovered in this study may be evidence that disorder means something different in the health context.When defined according the criminological or sociological definitions, disorder conveys to individuals that no one caresabout their community, including its residents; thus, people may withdraw into their homes and be less willing to be naturalguardians of public space, thereby allowing minor infractions of neighborhood norms to persist and potentially generatecrime (Sampson and Raudenbush, 1999; Taylor, 2001; Wilson and Kelling, 1982). Perhaps only in the sense that disorderconveys a potential for criminal victimization (as evidenced through the effects of offense-specific fear of crime) does thismeaning equate to health, where the risk of criminal victimization activates the stress response and thus diminishes health.The results presented here demonstrated this via the significant paths between offense-specific fear of crime and depression.Additionally, the activation of the stress response needs to be relatively frequent to have the deleterious effect on health thatdisorder and fear of crime are supposed to trigger. Fortunately, for the majority of individuals, the activation of the stressresponse as a result of disorderly neighborhood environments and fear of crime is a relatively low baseline event. Thus, dis-order and its effect on fear of crime may not function in the ways that have been previously thought.
Movement towards a health-specific conceptualization of disorder is already underway. Two studies, the Chicago Neigh-borhood and Disability Study and the Baltimore Memory Study, both aimed at studying older adults, establish valid disorderscale that include disorder cues relevant to older adults (Cagney et al., 2009), such as poor lighting, noise, and unmaintainedsidewalks. When putting this scale into play, results show that disorder negatively predicts the likelihood of engaging in pro-health behaviors (i.e., walking; Mendes de Leon et al., 2009). Other research has suggested that disorder is not explicitly dis-order, but rather environmental stressors (Ewart and Suchday, 2002) and show its relationship to anger, depression, and ahost of other mental health problems.
These findings have consequences for public policy and neighborhood renewal aimed at reducing disorder as a means toameliorate health problems in a community. Policies and programs, such as order-maintenance policing, aimed at generaldisorder reduction as a means to reduce fear may not ameliorate residents’ health. Of more concern, for public policy, isthe conceptual slipperiness of disorder. Policies aimed at disorder reduction need to be cognizant of how they want to impacthealth—be it through reducing environmental stressors that induce fear or addressing the problem of social control in a com-munity. Health policies intending to improve the health of neighborhood residents would do best to understand first whataspects of disorder, from an environmental stance, impact health. These results also suggest, via the significance of offense-specific fear of crime, that policies aimed at lowering one’s fear of specific crimes may also ameliorate health.
One of this study’s major strengths was employing a dataset which facilitated creating, two distinct fear of crime mea-sures and a valid disorder perception scale. The CCH is designed to explore how neighborhoods impact individuals’ personalhealth in a multitude of dimensions. Using the CCH enabled me to construct diverse fear of crime measures, not often in-cluded in surveys that assess health. However, just as the dataset offers several strengths to this study, its use also createssome limitations. First, the models employed did not effectively control for objective neighborhood conditions of disorder.While there is significant evidence that individuals’ perceptions of neighborhood conditions may play as important a role inindividuals’ health (Wen et al., 2006), nonetheless it is important to control for objective conditions of the neighborhood thatmay also contribute to personal health. Unfortunately, how the survey was sampled did not allow for hierarchical, or within-neighborhood effects modeling. In the future, studies that explore fear of crime, disorder and health need to have bettermeans to control for neighborhoods. Additionally, the self-rated health measure assesses what the respondent perceivestheir health to be; it certainly may be the case that the respondent over or underestimates the quality of their health. Whilethere are studies showing that self-rated health is a powerful estimate of individual health, there is always the potential forindividual bias. The dataset is relatively dated given that is was collected in 1995. Additionally, all the categories of self-ratedhealth would preferably have been modeled; however, there was little variation in this variable, the result being a dichot-omous outcome. Health is also measured in a multiplicity of ways. While self-rated health is a valid measure of health, thereare many dimensions of health that are not considered here. Finally, the dataset would have ideally included a stress scale.Given the theorized nature of the relationship between disorder perceptions and health, without biomarkers it is impossibleto truly measure the stress response that disorder perceptions and fear of crime induce.
6. Conclusion
This study demonstrates the presence of weak paths between disorder, fear of crime and three health outcomes. Whenusing an operationalization of disorder consistent with criminological and sociological conceptualizations (Sampson andRaudenbush, 1999; Skogan, 1990; Wilson and Kelling, 1982), the relationship between disorder and health, particularlyself-rated health and anxiety, fades. These findings suggest that the relationship between disorder and health is very sensi-tive to how disorder and health are conceptualized. The relationship may be more robust if disorder is conceptualized as a

1526 D. Wallace / Social Science Research 41 (2012) 1515–1528
biological stressor or environmental hazard. Current work which contextualizes disorder scales for the population of interest(see Cagney et al., 2009, for an example) is situated to more accurately assess how disorder impacts health for particularindividuals. Future research needs to re-conceptualize disorder as health-related disorder to more accurately understandthat relationship between disorder, fear of crime, and health.
Appendix A
Frequency distributions for offense specific fear of crime variables.
No. of days per week
Feared being robbed,attacked, or injuredFeared home being brokeninto
f
% f %0
1676 95 1631 92 1 30 2 19 1 2 19 1 38 2 3 5 0 15 1 4 4 0 5 0 5 7 0 10 1 6 0 0 2 0 7 32 2 53 31773
1773Appendix B
Standardized regression coefficients relating fear of crime to the endogenous and exogenous variables for self-ratedhealth models.
Model 1
Exogenous variables
Disorder Walk alone atnightFear of beingattacked
Fear of home break in
HealthNon-white
0.248*** �0.069***Female
0.073 �0.108***Age
�0.241 �0.241***Children
0.080 0.080*Family income
0.077*** 0.077**Full time employment
0.061 0.061 No high schooldiploma
�0.059*** �0.059*Chronic disease
�0.279***Smoker
�0.099***Disorder
0.671*** 0.239*** 0.330*** �0.236***Walk alone at night
0.073*Fear of being attacked
�0.002 Fear of home break in �0.036***
Chi-square 216.400 df 34 CFI 0.974 RMSEA 0.055n = 1773.*** p < 0.01.** p < 0.05.* p < 0.10.

D. Wallace / Social Science Research 41 (2012) 1515–1528 1527
Appendix C
Standardized regression coefficients relating fear of crime to the endogenous and exogenous variables for mental healthmodels.
Model 2 M
odel 3Exogenous variables
Disorder W alkalone atnightFear ofbeingattacked
Fear ofhomebreakin
Depression D
isorder Walkalone atnightFear ofbeingattacked
Fhb
ear ofomereak
in
A
nxietyNon-white
0.248 0.066*** 0 .248*** � 0.005 Female 0.032 0.108*** 0 .032 0 .085***Age
0.037 �0.118*** 0 .037 � 0.245***Children
�0.017 �0.024 � 0.017 0 .020 Family income �0.208 � 0.133*** � 0.208*** � 0.074***Full time employment
0.022 �0.058** 0 .022 0 .006 No high schooldiploma
0.126 0.042** 0 .126*** 0 .030Chronic disease
0.136*** 0 .126***Smoker
0.068*** 0 .053***Disorder
0 .671*** 0.239*** 0.330*** �0.063* 0.671*** 0.239*** 0 .330*** 0 .008 Walk alone at night 0.095*** 0 .035 Fear of being attacked 0.154*** 0 .132***Fear of home break in
0.127*** 0 .120***Chi-square 216.464*** 216.488***
Df
34 3 4 CFI 0.973 0 .973 RMSEA 0.055 0 .055 n = 1773 n = 1773*** p < 0.01.** p < 0.05.* p < 0.10.
References
Baron, R.M., Kenny, D.A., 1986. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statisticalconsiderations. Journal of Personality and Social Psychology 51, 1173–1182.
Browning, C.R., Cagney, K.A., 2002. Neighborhood structural disadvantage, collective efficacy, and self-rated physical health in an urban setting. Journal ofHealth and Social Behavior 43, 383–399.
Browning, C.R., Wallace, D., Feinberg, S.L., Cagney, K.A., 2006. Neighborhood social processes, physical conditions, and disaster-related mortality: the case ofthe 1995 Chicago heat wave. American Sociological Review 71, 661–678.
Bursik, R.J., Gramsmick, H.G., 1993. Neighborhoods and Crime: The Dimensions of Effective Community Control. Lexington Books, Lanham.Cagney, K.A., Glass, T.A., Skarupski, K.A., Barnes, L.L., Schwartz, B.S., Mendes de Leon, C.F., 2009. Neighborhood-level cohesion and disorder: measurement
and validation in two older adult urban populations. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 64B, 415–424.Cutrona, C.E., Russell, D.W., Hessling, R.M., Brown, P.A., Murry, V., 2000. Direct and moderating effects of community context on the psychological well-
being of African American Women. Journal of Personality and Social Psychology 79, 1088–1101.Ewart, C.K., Suchday, S., 2002. Discovering how urban poverty and violence affect health: development and validation of a neighborhood stress index.
Health Psychology 21, 254–262.Ferraro, K.F., 1995. Fear of Crime: Interpreting Victimization Risk. State University of New York, Albany.Ferraro, K.F., Farmer, M.M., Wybraniec, A., 1997. Health trajectories: long-term dynamics among black and white adults. Journal of Health and Social
Behavior 38, 38–54.Garofalo, J., Laub, J.H., 1978. The fear of crime: broadening our perspectives. Victimology 3, 242–253.Gau, J.M., 2010. Basic principles and practices of structural equation modeling in criminal justice and criminology research. Journal of Criminal Justice
Education 21, 136–151.Geis, K.J., Ross, C.E., 1998. A new look at urban alienation: the effect of neighborhood disorder on perceived powerlessness. Social Psychology Quarterly 61,
232–246.Goldstein, M.S., Siegel, J.M., Boyer, R., 1984. Predicting changes in perceived health status. American Journal of Public Health 74, 611–614.Haney, T.J., 2007. ‘‘Broken windows’’ and self-esteem: subjective understandings of neighborhood poverty and disorder. Social Science Research 36, 968–
994. http://dx.doi.org/10.1016/j.ssresearch.2006.07.003.Hill, T., Angel, R., 2005. Neighborhood disorder, psychological distress, and heavy drinking. Social Science & Medicine 61, 965–975. http://dx.doi.org/
10.1016/j.socscimed.2004.12.027.Hill, T.D., Ross, C.E., Angel, R.J., 2005a. Neighborhood disorder, psychophysiological distress, and health. Journal of Health and Social Behavior 46, 170–186.Hill, T.D., Ross, C.E., Angel, R., 2005b. Neighborhood disorder, psychophysiological distress, and health. Journal of Health and Social Behavior 46, 170–186.Hipp, J.R., 2010. Resident perceptions of crime and disorder: how much is ‘‘Bias’’, and how much is social environment differences?�. Criminology 48, 475–
508.

1528 D. Wallace / Social Science Research 41 (2012) 1515–1528
Hunter, A., 1978. Symbols of Incivility. American Society of Criminology, Dallas.Hunter, A., 1985. Private, parochial, and public social orders: the problem of crime and incivilities in urban communities. In: Suttles, G. et al. (Eds.), In The
Challenge of Social Control: Essays in Honor of Morris Janowitz. Ablex Publishing Corporation, Norwood, pp. 231–242.Idler, E., Benyamini, L.Y., 1997. Self-rated health and mortality: a review of twenty-seven community studies. Journal of Health and Social Behavior 38, 21–
37.Jackson, J., Stafford, M., 2009. Public health and fear of crime: a prospective cohort study. British Journal of Criminology 49, 832–847.Katz, C.M., Wallace, D., Hedberg, E.C., 2011. A longitudinal assessment of the impact of foreclosure on neighborhood crime. Journal of Research in Crime and
Delinquency. http://dx.doi.org/10.1177/0022427811431155.Killias, M., 2000. Different measures of vulnerability in their relation to different dimensions of fear of crime. British Journal of Criminology 40, 437–450.Klinenberg, E., 2002. Heat Wave: A Social Autopsy of Disaster in Chicago University of Chicago Press. Chicago.LaGrange, R.L., Ferraro, K.F., 1987. Assessing age and gender differences in perceived risk and fear of crime. Criminology 27, 697–719.LaGrange, R.L., Ferraro, K.F., Supancic, M., 1992. Perceived risk and fear of crime: the role of social and physical incivilities. Journal of Research in Crime and
Delinquency 29, 311–334.Latkin, C.A., Curry, A.D., 2003. Stressful neighborhoods and depression: a prospective study of the impact of neighborhood disorder. Journal of Health and
Social Behavior 44, 34–44.Latkin, C.A., German, D., Hua, W., Curry, A.D., 2009. Individual-level influences on perceptions of neighborhood disorder: a multilevel analysis. Journal of
Community Psychology 37, 122–133.Linares, L.O., Heeren, T., Bronfman, E., Zuckerman, B., Augustyn, M., Tronick, E., 2001. A meditational model for the impact of exposure to community
violence on early child behavior problems. Child Development 72, 639–652.Lowenkamp, C.T., Cullen, F.T., Pratt, T.C., 2003. Replicating Sampson and Groves’s test of social disorganization theory: revisiting a criminological classic.
Journal of Research in Crime and Delinquency 40, 351–373.MacIntyre, S., Ellaway, A., 2003. Neighborhoods and health: an overview. In: Kawachi, I., Berkman, L. (Eds.), Neighborhoods and Health. Oxford University
Press, New York, pp. 20–42.McEwen, B.S., 2000. Allostasis and allostatic load: implications for neuropsychopharmacology. Neuropsychopharmacology 22, 108–124.Memmler, R.L., Cohen, B.J., Wood, D.L., 1996. The Human Body in Health and Disease, eight ed. Lippincott Williams and Wilkins, New York.Mendes de Leon, C.F., Cagney, K.A., Bienias, J.L., Barnes, L.L., Skarupski, K.A., Scherr, P.A., Evans, D.A., 2009. Neighborhood social cohesion and disorder in
relation to walking in community-dwelling older adults: a multilevel analysis. Journal of Aging and Health 21, 155–171.Millunpalo, S., Vuori, I., Oja, P., Pasanen, M., Urponen, H., 1997. Self-rated health status as a health measure: the predictive value of self-reported health
status on the use of physician services and on mortaility in the working age population. Journal of Clinical Epidemiology 50, 517–528.Mirowsky, J., Ross, C.E., 1989. Social patterns of distress. Annual Review of Sociology 12, 23–45.Muthen, L.K., Muthen, B.O., 1998-2007. Mplus Users Guide, fifth ed. Muthen and Muthen, Los Angeles, CA.Ross, C.E., 1993. Fear of victimization and health. Journal of Quantitative Criminology 9, 159–175.Ross, C.E., 2000a. Walking, exercising, and smoking: does neighborhood matter? Social Science & Medicine 51, 265–274.Ross, C.E., 2000b. Neighborhood disadvantage and adult depression. Journal of Health and Social Behavior 41, 177–187.Ross, C.E., Mirowsky, J., 1984. Components of depressed mood in married men and women: the center for epidemiological studies’ depression scale.
American journal of epidemiology 119, 997–1004.Ross, C.E., Britt, C., 1995, 1998. Survey of Community, Crime, and Health, 1995, 1998, United States.Ross, C.E., Mirowsky, J., 1999. Disorder and decay: the concept and measurement of perceived neighborhood disorder. Urban Affairs Review 34, 412–432.Ross, C.E., Jang, S.J., 2000. Neighborhood disorder, fear and mistrust: the buffering role of social ties with neighbors. American Journal of Community
Psychology 28, 401–420.Ross, C.E., Mirowsky, J., 2001. Neighborhood disadvantage, disorder, and health. Journal of Health and Social Behavior 42, 258–276.Ross, C.E., Reynolds, J.R., Geis, K.J., 2000. The Contingent meaning of neighborhood stability for residents’ psychological well-being. American Sociological
Review 65, 581–597.Ross, C.E., Mirowsky, J., Pribesh, S., 2001. Powerlessness and the amplification of threat: neighborhood disadvantage, disorder, and mistrust. American
Sociological Review 66, 568–591.Roundtree, P.W., Land, K.C., 1996. Perceived risk versus fear of crime: empirical evidence of conceptually distinct reactions in survey data. Social Forces 74,
1353–1376.Sampson, R.J., Raudenbush, S.W., 1999. Systematic social observation of public spaces: a new look at disorder in urban neighborhoods. American Journal of
Sociology 105, 603–651.Sampson, R.J., Raudenbush, S.W., 2004. Seeing disorder: neighborhood stigma and the social construction of ‘‘Broken windows’’. Social Psychology Quarterly
67, 319–342.Sarnoff, I., Zimbardo, P.G., 1961. Anxiety, fear, and social affiliation. Journal of Abnormal Social Psychology 62, 356–363.Simons, R.L., Simons, L.G., Chen, Y.-F., Brody, G.H., Lin, K.-H., 2007. Identifying the psychological factors that mediate the association between parenting
practices and delinquency. Criminology 45, 481–517.Simons, R.L., Simons, L.G., Burt, C.H., Drummund, H., Stewart, E.A., Brody, G.H., Gibbons, F.X., Cutrona, C.E., 2006. Supportive parenting moderates the effect
of discrimination upon anger, hostile view of relationships, and violence among African American boys. Journal of Health and Social Behavior 47, 373–389.
Singh-Manoux, A., Marmot, M.G., Alder, N.E., 2005. Does subjective social status predict health and change in health status better than objective status?Psychosomatic Medicine 67, 855–861.
Skogan, W.G., 1990. Disorder and Decline: Crime and the Spiral of Decay in American Neighborhoods. University of California Press, Berkeley.Stafford, M., Chandola, T., Marmot, M., 2007. Association between fear of crime and mental health and physical functioning. American Journal of Public
Health 97, 2076–2081.Taylor, R.B., 2001. Breaking Away from Broken Windows: Baltimore Neighborhoods and the Nationwide Fight Against Crime, Grime, Fear and Decline.
Westview Press, Boulder, CO.Taylor, R., 2009. Potential Models for Understanding Crime Impacts of High or Increasing Unoccupied Housing Rates in Unexpected Places, and How to
Prevent Them, US Department of Justice.Taylor, R.B., Covington, J., 1993. Community structural change and fear of crime. Social Problems 40, 374–397.Wallace, D., forthcoming. A test of routine activities and neighborhood attachment explanations for bias in disorder perceptions. Crime & Delinquency.
doi:10.1177/0011128711426538.Wallace, D., Hedberg, E.C., Katz, C.M., in press. The impact of foreclosures on neighborhood disorder before and during the housing crisis: testing the spiral of
decay. Social Science Quarterly.Warr, M., Stafford, M., 1983. Fear of victimization: a look at proximate causes. Social Forces 61, 1033–1043.Wen, M., Hawkley, L.C., Cacioppo, J.T., 2006. Objective and perceived neighborhood environment, individual SES and psychosocial facots, and self-rated
health: an analysis of older adults in Cook County, Illinois. Social Science & Medicine 63, 2575–2590.Wilson, I.B., Kaplan, S., 1995. Clinical practice and patients’ health status: how are the two related? Medical Care 33, AS209–AS214.Wilson, J.Q., Kelling, G.L., 1982. Broken windows: the police and neighborhood safety. The Atlantic Monthly 127, 29–38.Woldoff, R.A., 2002. The effects of local stressors on neighborhood attachment. Social Forces 81, 87–116.