Embed Size (px)
Citation preview
Evolving strategies for preserving the
pulmonary valve during early repair of tetralogy
of Fallot: mid-term results
Vladimiro Vida, MD, PhD
Pediatric and Congenital Cardiac Surgery Unit
University of Padua Medical School

Disclosures
Nothing to disclose

Background
Tetralogy of Fallot (TOF) repair has become nowadays a
standard routine practice
Al Habib HF, Jacobs JP, Mavroudis C, et al. Contemporary patterns of management of tetralogy of Fallot: data from the
Society of Thoracic Surgeons Database. Ann Thorac Surg. 2010 Sep;90(3):813-9.
Sarris GEE, Comas JV, Tobota Z, et al. Results of reparative surgery for tetralogy of Fallot: data from the European
Association for Cardio-Thoracic Surgery Congenital Database. Eur J Cardiothorac Surg. 2012 Nov;42(5):766-74.
Stellin G, Milanesi O, Rubino M et al. Repair of tetralogy of Fallot in the first six months of life: transatrial versus
transventricular approach. Ann Thorac Surg 1995;60:588–S591.
Correction via a right ventriculotomy with
RVOT TAP reconstruction remains the
most frequent approach
Many institutions have adopted, since many
years, a trans-atrial approach (TA) which
has become with time their preferred
standard procedure

• Commonly in any technique, when the use of TAP is necessary
- PVR with chronic volume overload
- Progressive RV dilation and dysfunction
- Impaired functional capacity
Background 1
PV cusps augmentation plasty
- limits an immediate PV regurgitation
- improves short-term clinical outcomes
Early PV cusp deterioration is expected
with a progressive PVR, in the long-term.
Development of different
PV preservation
techniques

Our PV preservation technique
(since 2007 in selected patients)
• Intra-operative PV balloon dilation during TA TOF repair
• Initial indication: less severe forms (PV Z score ≥-3)
• Current indication: PV Z-score ≥ 4
Vida VL, Padalino MA, Maschietto N, Biffanti R, Anderson RH, Milanesi O, Stellin G. The balloon dilation of the pulmonary valve
during early repair of Tetralogy of Fallot. Catheter Cardiovasc Interv. 2012 Nov 15;80(6):915-21.


PV Z-score: -3.6
4 mm 6 mm
10 mm
At 2D: 5.5 mm Z-score= -3.6
8- 10 mm
“In-series” PV balloon dilation
Additional PV plasty

Additional PV plasty after balloon dilation
“De-lamination”: to increase the PV leaflet’s coaptation surface
1) PV leaflets repair 1) PV leaflets “de-lamination”
2) PV leaflets resuspension 2) PV leaflets patch augmentation
3) PV leaflets re-suspension
Simple PV plasty Complex PV plasty

Aim of the study
To assess effectiveness, early and mid-term results of the PV
preservation technique by balloon dilation in pts with TOF
mainly focusing on:
1) PV function and growth
2) RV function
Controls: patients treated with a standard TA repair (with TAP) during the
same time interval

Patients June 2007 – December 2012
69 PATIENTS
+
Reason for PV preservation failure:
1) tearing of the hinges of the PV leaflets due to over-sizing of the
balloon catheter (n=3)(early in our experience)
2) very low PV Z-score (<-4)(n=2).
5 Conversions to TA
repair
34 PV preservation
success (49%)
30 Control TA
repair
39 PV preservation
attempts
- PTFE cusp (n=23)
- CorMatrix cusp (n=10)
- Autologous pericardium cusp (n=1)
- Pulmonaty homograft cusp (n=1)

PV anatomy
PV dilation group
(n=34)
Standars TA group
(n=35) p value
Unicuspid (n=4 pts) - 4 (100%)
0.001 Bicuspid (n=59 pts) 28 (47.4%) 30 (52.6%)
Tricuspid (n=6 pts) 6 (100%) -
Median preoperative PV Z-score p value
Unicuspid (n=4 pts) -4.26 (-2.97 - -4.98)
0.0004 Bicuspid (n=59 pts) -3.2 (-0.95 - -5.62)
Tricuspid (n=6 pts) -1.73 (-1.19 - -2.44)
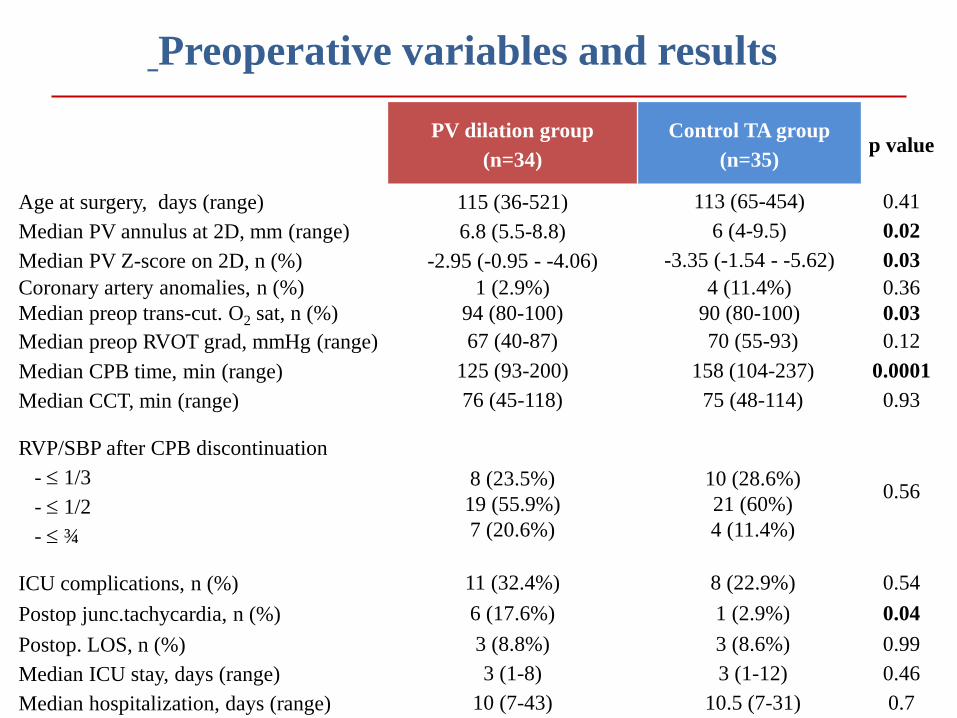
Preoperative variables and results
PV dilation group
(n=34)
Control TA group
(n=35) p value
Age at surgery, days (range) 115 (36-521) 113 (65-454) 0.41
Median PV annulus at 2D, mm (range) 6.8 (5.5-8.8) 6 (4-9.5) 0.02
Median PV Z-score on 2D, n (%) -2.95 (-0.95 - -4.06) -3.35 (-1.54 - -5.62) 0.03
Coronary artery anomalies, n (%) 1 (2.9%) 4 (11.4%) 0.36
Median preop trans-cut. O2 sat, n (%) 94 (80-100) 90 (80-100) 0.03
Median preop RVOT grad, mmHg (range) 67 (40-87) 70 (55-93) 0.12
Median CPB time, min (range) 125 (93-200) 158 (104-237) 0.0001
Median CCT, min (range) 76 (45-118) 75 (48-114) 0.93
RVP/SBP after CPB discontinuation
- 1/3
- 1/2
- ¾
8 (23.5%)
19 (55.9%)
7 (20.6%)
10 (28.6%)
21 (60%)
4 (11.4%)
0.56
ICU complications, n (%) 11 (32.4%) 8 (22.9%) 0.54
Postop junc.tachycardia, n (%) 6 (17.6%) 1 (2.9%) 0.04
Postop. LOS, n (%) 3 (8.8%) 3 (8.6%) 0.99
Median ICU stay, days (range) 3 (1-8) 3 (1-12) 0.46
Median hospitalization, days (range) 10 (7-43) 10.5 (7-31) 0.7

“In-series” PV balloon dilation n=15 / 35 patients (44%)
PV Z-score -2.29 (-0.95 - -3.74) -3.56 (-2.28 - -4.06)
Single BD
n=20 pts
“In-series” BD
n= 15 pts
p=0.002

Simple PV plasty
n=4 pts
Additional PV plasty after balloon dilation (n=18 pts, 53%)
Complex PV plasty
n=14 pts
PV Z-score -2.34 (-1.52 - -2.78) -3.5 (-2.28 - -4.06)
p=0.01

Echocardiographic evaluation at discharge
PV dilation group
(n=34)
Standars TA group
(n=35) p value
Degree of TR, n (%)
Grade 1 (mild)
Grade 2 (moderate)
Grade 3 (severe)
30 (91.2%) 3 (8.8%)
-
33 (94.3%) 2 (5.7%)
-
0.48
Median RVOT gradient, mmHg (range) 29 (18 – 50) 25 (12 – 50) 0.18
RVOT gradient grade, n (%)
Grade 1 (<20 mmHg)
Grade 2 (20 – 40 mmHg)
Grade 3 (>40 mmHg)
1 (2.9%) 30 (88.2%)
3 (8.8%)
7 (20%) 26 (77.1%)
1 (2.9%)
0.07
Degree of PVR*, n (%)
Grade 1 (none-mild)
Grade 2 (moderate)
Grade 3 (severe)
30 (88.2%) 4 (11.8%)
-
14 (40%) 9 (25.7%) 12 (34.3%)
0.0001
* Grothoff M, Spors B, Abdul-Khaliq H, Gutberlet M: Evaluation of postoperative pulmonary regurgitation after surgical repair of
tetralogy of Fallot: Comparison between doppler echocardiography and mr velocity mapping. Pediatr Radiol. 2008; 38: 186-191

Follow-up
PV dilation group
(n=34)
Standars TA group
(n=35) p value
Follow-up time, days (range)
432 (189 – 1940)
711 (189 – 1492)
0.08
Reoperations, n (%)
1* (2.9%)
1** (2.8%)
0.9
Both with a residual peak RVOT gradient
> 50 mmHg
Both required additional RVOT muscle
bandle resection, TAP + PTFE PV cusp
interposition

Echocardiographic evaluation at follow-up (>6 months)
PV dilation group
(n=30)
Standars TA group
(n=32) p value
Degree of TR, n (%)
Grade 1 (mild)
Grade 2 (moderate)
Grade 3 (severe)
30 (100%)
-
-
32 (100%)
-
-
0.99
Median RVOT gradient, mmHg (range) 23.5 (8 – 40) 22 (7 – 45) 0.85
RVOT gradient grade, n (%)
Grade 1 (<20 mmHg)
Grade 2 (20 – 40 mmHg)
Grade 3 (>40 mmHg)
18 (60%)
12 (40%)
-
18 (56%)
12 (38%)
2 (6%)
0.37
PV Z-score, n (range) -0.1 (-0.3 - +0.7) - -
Degree of PVR, n (%)
Grade 1 (none-mild)
Grade 2 (moderate)
Grade 3 (severe)
24 (80%)
6 (20%)
-
8 (25%)
11 (35%)
13 (40%)
<0.0001

p=0.003
55% (42-70) 50% (40-63)
PV dilation group Standard TA group
Echocardiographic evaluation at follow-up RV fraction of area change
Horton KD, Meece RW, Hill JC: Assessment of the right ventricle by echocardiography: A primer for
cardiac sonographers. J Am Soc Echocardiogr. 2009; 22: 776-792.
Anavekar NS, Gerson D, Skali H, Kwong RY, Yucel EK, Solomon SD: Twodimensional assessment of right
ventricular function: An echocardiographic-mri correlative study. Echocardiography. 2007; 24: 452-456.

PVR and RV function at follow-up Linear regression analyis

Limitations
-Retrospective evaluation
-Mid-term follow-up
- RV function assessment by 2D echo
- Still on a learning curve phase

Conclusions
The PV function can be preserved by balloon dilation during early TA TOF repair
and this contributes to better preserve RV function.
We have recently further expanded the applicability of such a technique to patients
with an increasingly smaller PV annulus (PV Z-score ≥ 4)(being the in-series balloon
dilation and a more aggressive PV plasty strategy important key points).
In case the total valve preservation cannot be achieved the conversion to standard TA
repair can be easily performed.

E-E2)(PV Z-score -3 - -3.5)
PV leaflet’s de-lamination
and re-suspension plasty
Our current PV preservation
surgical protocol
A-C) common pathway including
“protective” commissurotomy and
balloon dilation of the pulmonary valve
annulus.
D-D1)(PV Z-score -3)
Additional PV plasty, for
repairing accidental leaflet’s
tears during balloon dilation,
and leaflet’s re-suspension.
F)(PV Z-score -3.5 - -4)
Additional PV leaflets’s
patch augmentation and
re-suspension plasty.





























