Embed Size (px)
Citation preview

J. ELECTROCARDIOLOGY, 10 (1) 1977 67-70
Evolutionary Changes in the Electrocardiogram of Severe Progressive Hypothermia
BY ROBERT THOMPSON, M.D., MAJ MC,* JOHN RICH, M.D., MAJ MC,t FRANK CHMELIK, M.D., MAJ MC** AND WILLIAM NELSON, M.D., COL MCt t
SUMMARY A patient is reported who developed pro-
gressive hypothermia during therapy for adult respiratory distress syndrome. Electro- cardiographic changes (sinus bradycardia, prolonged PR interval, prolonged QTc inter- val, "Osborn waves") were documented and correlated with body temperature. The sig- nificance of these changes is discussed and the relationship between the degree of hypo- thermia and the presence of "Osborn waves" is noted.
P r e v i o u s a u t h o r s h a v e d e s c r i b e d the characteristic ECG changes produced in pa- tients~-5, 7-10 and experimental animals 3,7 by hypothermia . However , these reports con- cerned either rapidly produced hypothermia as an aid to surgery T M or ECG changes after accidental hypothermia. 1,4,s This report con- ce rns e v o l u t i o n a r y e l e c t r o c a r d i o g r a p h i c changes as severe hypo the rmia developed over a 48 hour period.
CASE REPORT A 20 year old Caucasian male was admitted
with left lower lobe pneumonia. After initial improvement, acute respiratory distress with bilateral pulmonary infiltrates developed on
From the Department of Medicine, US General Leonard Wood Army Hospital, Ft Leonard Wood, Missouri, and the Department of Cardiology, Fitz- simons Army Medical Center, Denver, Colorado. *Department of Internal Medicine, Riverside Hos- pital, Columbus, Ohio. tDepartment of Cardiology, Miami Valley Hos- pital, and Wright State University School of Medicine, Dayton, Ohio. **University of Illinois, School of Medicine, Rockford Illinois. t t Division of Cardiovascular Medicine, University of Nebraska Medical Center, Omaha, Nebraska. Opinions stated in this article are strictly those of the authors and should not be construed as official views or as reflecting the official views of the U.S. Army. Reprint requests to: John M. Rich, M.D., Car- diovascular Laboratory, Miami Valley Hospital, 1 Wyoming Street, Dayton, OH 45409.
the 14th hospital day. Artificial venti lat ion was required due to persistent hypoxemia and the development of the adult respiratory dis- tress syndrome. He was treated with volume cycled respirator (Ohio 560*), high percentage oxygen delivery, antibiotics and continuous posi t ive p re s su re brea th ing . His hosp i ta l c o u r s e w a s c o m p l i c a t e d b y b i l a t e r a l pneumothoraces and the development of a t r a c h e o e s o p h a g e a l f i s t u l a w h i c h m a d e adequate venti lat ion impossible. Hypother- mia deve loped on the 33rd hosp i t a l day (36.4~ 97.6~ and electrocardiographic ab- normalities were apparent by the 35th hospi- tal day (35.6~ 96~ The patient expired on the 38th hospital day.
Autopsy revealed pulmonary changes con- sistent with adult respiratory distress syn- drome. The t racheoesophageal f is tula was 1 cm in diameter. Gross and light microscopic examinations of the heart were normal.
MATERIALS AND METHODS Temperatures were recorded using a rectal
probe. ECGs, blood gases and blood chemis- tries were obtained using s tandard methods. E lec t rocard iographic m e a s u r e m e n t s were made from rhythm strips of lead 11. Hear t rates were calculated from the mean o f l0 R-R intervals from the rhythm strips and the QTc was calculated using Bazett 's formula.
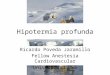
RESULTS Table I summarizes the ECG rhythm strips
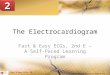
of Fig. 1. There was a progressive slowing of heart rate during the period of hypothermia, but prolongation of the PR and QTc intervals did not occur until 25.6~ Small but definite "Osborn waves ''7 were present, even at 35.6~ but did not become marked unti l approxi- ma te ly 26.7~ was reached. The t e rmina l r h y t h m seen in the strips marked G was probably idioventr icular ending wi th ven- tr icular fibrillation. Previous rhy thms had been s inus b radycard ia and no a t r ia l ar- rhythmias were noted. Fig. 2 shows a full ECG (except for the lateral precordial leads which could not be obtained because of a chest
* Ohio Medical Products, Chicago, Ill.
67

68 T H O M P S O N ET AL
TABLE I ECG Measurements Corresponding to Rhythm Strips in Figure i
ECG A B C D E F G
Hospital Day 18 33 35 35 36 37 Time 0600 0645 0600 1808 0600 0600 Temperature 38.1 ~ C 36.4 ~ C 35.6 ~ C 33.3 ~ C 30 ~ C 25.6 ~ C
(101.8 ~ F) (97.6 ~ F) (96 ~ F) (92 ~ F) (86 ~ F) (78 ~ F) Rate 106 105 85 70 58 37 Rhythm NSR NSR NSR NSR NSR NSR QT c .40 .38 .43 .46 .45 .55 PR .12 .11 .12 .12 .12 .20 QRS .08 .06 .08 .08 .08 .10 "Osborn waves" No No Yes Yes Yes Yes pH 7.33 7.44 7.48 7.25 - - P02 (ram Hg) 77 55 53 45 - - PC02 (mm Hg) 49 43 52 77 - - K+ 4.9 4.6 3.9 - - -
38 0818
U nrecordable
Column A measurements are for rhythm strip A, etc.
l f
ZI
_LI
Jl
I : !1~ ' - - I I I L I
"- I " - ~ i J
Fig. 1. Rhythm strips of lead 11 labeled A-G correspond to the time noted in Table 1. '~Osborn waves" are noted with x's. Strip G, taken a few minutes before death, shows onset of idioventricular rhythm and then ventricular fibrillation.
J. ELECTROCARDIOLOGY, VOL. 10, NO. 1, 1977

ECG CHANGES IN HYPOTHERMIA 69
tube) at a rectal temperature of 25.6~ dem- onstrat ing characteristic "Osborn waves."
DISCUSSION Characteristic ECG changes of hypother-
mia including sinus bradycardia, prolonga- tion of PR and QTc intervals and the ~'Osborn wave" (J point elevat ion) have been de- scribed. ~ With rapidly induced hypother- mia, a high incidence of atrial fibrillation w i t h d e c r e a s i n g t e m p e r a t u r e had been noted. 3 Ventricular fibrillation has also been thought to be a danger with hypothermia, al- though the incidence of this a r rhythmia is probably over-estimated. ~4
Accidental or disease-induced hypothermia produces ECG changes similar to intentional hypothermia. 4,6's'9 However, disease-induced hypothermia may take place over days. In this case, we were able to document the evolu- tion of the ECG changes as hypothermia oc- curred over a period of two days. When hypothermia is a gradual process, if our case is typical, small "Osborn waves" are the only early abnormality noted. They appeared with
mild hypothermia and gradually increased in size as the temperature fell. PR and QTc in- t e rva l p ro longat ion did not appear un t i l 26.7~ (80~ was reached.
The exact etiology of the "Osborn wave" is not known. Conflicting data exist with regard to the relationship of arterial pH to the pres- ence of the J point elevation in the hypo- thermic experimental animal. Osborn 7 felt tha t these electrocardiographic changes were related to acidosis frequently found in severe hypothermia, while Emslie-Smith 2 found no such relationship. Our data suggest tha t '~Os- born waves" may be d i r ec t ly r e l a t e d to hypothermia and not to acidosis, as small J point elevations were found at a temperature of 96~ when the pH was 7.48. However, the large "Osborn waves" were seen at a pH of 7.25 and the possible additive effect of acidosis to hypothermia cannot definitely be excluded as the cause of these electrocardiographic changes in humans. Whether the acidosis re- sulted from a direct effect of the hypothermia or was in part related to pulmonary insuffi- ciency, in this case, is not clear.
Myocardial fat ty metamorphosis has been
II
lU
R
L
F
l i I [ i l i II _ ~ t t t II [ I I I I I i l l I l i l l l l l l l '
I I I I I I t l I t I I I l l l l l l l l l l l l l l
I l l l I [ [ . l [
1 [ 1 1 1 | [ ~ _ ] H i I I i ~ I I I I I i I !
l i l l l l l l l I F ~
i l i l i l l i l t l l l [ l l I I I I I I I ]
I I I I I I I I I l l l l i l l L l l l l l l l l a
r I
I '
VI
V2
Fig. 2. Full ECG taken one day prior to death with body temperature 25.6~ (78~ rectally. Lateral precordial leads are not available due to position of a chest tube.
J. ELECTROCARDIOLOGY, VOL. 10, NO. 1, 1977

70 THOMPSON ET AL
reported in pat ients who were hypothermic at dea th2 The exact relation of this pathologic lesion to the "Osborn wave" is uncertain. As ~'Osborn waves" are frequently reversible on warming the patient, 2'~'7'9 it would seem un- l ikely tha t pathologic changes such as ne- crosis or fat ty metamorphosis would be their cause. The fact tha t our patient 's hear t was normal microscopically lends credence to the supposition tha t hypothermia (with the pos- sible additive effect of acidosis) causes elec- trophysiologic changes in the myocardium, producing "Osborn waves" without causing irreversible pathologic changes in the myo- cardium.
Marshall 11 documented electrophysiologic changes in the rabbit a t r ium where she noted prolongation of both the depolarization and repolarization phases of the intracel lular ac- t ion po ten t i a l when the p r e p a r a t i o n was cooled. These data suggest tha t the prolonga- tion of the QTc (repolarization) is directly re- lated to hypothermia. Our data do not resolve the cause of prolongation of the QTc in the h u m a n hear t , as o ther potent ia l apparen t causes of a prolonged QTc 12 such as hypo- kalemia or hypocalcemia were not excluded when hypothermia became severe.
Prolongation of the PR interval has also been noted with severe hypothermia 9 and was seen when our pat ient ' s body t empera tu re reached 25.6~ (78~ This may be the direct effect of hypothermia on AV junctional con- duction. Gould ~3 has recently reported pro- longation of the A-H interval when cooled fluid was infused over the area of the junc- tional tissue of pat ients while recording their His bundle potentials.
The "Osborn wave" is not pathognomonic of hypothermia, as it has been reported in acute cardiac ischemia as well. '~ Also, it cannot be used to specifically quant i ta te the degree of hypothermia in a patient . Our data, as well as tha t of others, ~'4'6'9 suggest, though, tha t large "Osborn waves" are usually found with body tempera tures below 29.4~ (85~ Clements emphasizes the importance of this ECG find- ing in evaluat ion of an unrecordable tempera- ture measured with the rout ine rectal ther-
mometer which only records to 34.4~ (94~ In this situation, the ECG finding of large "Osborn waves" would be evidence for severe hypothermia and the appropriate therapeutic steps could be rapidly taken.
Acknowledgment: We wish to express our grateful appreciation to Mrs. Polly Applegate for aid in typ- ing this manuscript.
REFERENCES
1. REE, M J: Electrocardiographic changes in ac- cidental hypothermia. Br Heart J 26:566, 1964
2. EMSLIE-SMITH, D, SLADDEN, G E AND SWIRLING, G R: The significance of changes in the elec- trocardiogram in hypothermia. Br Heart J 21:343, 1959
3. SCHWAB, R H, LEWIS, D W, KILLOUGH, J H AND TEMPLETON, J Y: E lec t roca rd iog raph ic changes occurring in rapidly induced hypo- thermia. Am J Med Sci 248:290, 1964
4. TREVINO, A, RAZI, B AND BELLER, B M: The characteristic electrocardiogram of accidental hypothermia. Arch Int Med 127:470, 1971
5. HICKS, E H, MCCORD, M C AND BLOUNT, S G, JR: Electrocardiographic changes during hypo- thermia and circulatory occlusion. Circulation 13:21, 1956
6. CLEMENTS, S D AND HURST, J W: Diagnostic value of electrocardiographic abnormalities observed in subjects accidentally exposed to cold. Am J Cardiol 29:729, 1972
7. OSBORN, J J: Experimental hypothermia; Res- piratory and blood pH changes in relation to cardiac function. Am J Physiol 175:389, 1953
8. FERNANDEZ, J P, O'ROURKE, R A AND EWY, G A: Rapid external rewarming in accidental hypothermia. JAMA 212:153, 1970
9. DUGUID, H, SIMPSON, R G, AND STOWERS, J M: Accidental hypothermia. Lancet 2:1213, 1961
10. WYNNE, N A, FULLER, J A, SZEKELY, P: Elec- trocardiographic changes in hypothermia. Br Heart J 22:642, 1960
11. MARSHALL, J M: Effects of low temperatures on transmembrane potentials of single fibers of the rabbit atrium. Circ Res 5:664, 1957
12. SURAWICZ, B: Relationship between electro- cardiogram and electrolytes. Am Heart J 73:814, 1967
13. GOULD, L AND REDDY, CVR: Effect of cold isotonic glucose infusion on A-V nodal conduc- tion. J Electrocardiol 9:23, 1976
J. ELECTROCARDIOLOGY, VOL. 10, NO. 1, 1977