Embed Size (px)
Citation preview

Evolutionary and Ecological Perspectives on “Systems” Diseases
using Agent-based Modeling
Swarmfest 2014
Notre Dame University South Bend, IN, June 30, 2014
Gary An, MD
Associate Professor of Surgery Department of Surgery
University of Chicago, Chicago, IL

Disclosure
• Consultant for Immunetrics
• Mathematical Modeling of Sepsis and Execution of In-silico clinical trials

U.S. FDA ���“Critical Path” Document
• March 2004 “Innovation or Stagnation”

Wandling and An, WJ Emer Surg, 2010

Organ Function

Organ Function
Cell Cell Cell
Cell
Cell
Cell Cell

Organ Function
Cell Cell
Cell
Cell Cell
Cell
Cell
m
m m
m m
m m m
m
m m
m
m
m
m
m
m
m
m m
m
m
m m
m
m
m
m m
m
m
m
m
m
m
m m m
m
m
m
m
m
m
m
m
m m
m
m m
m
m
m m
m
m m
m m
m
m m m
m
m m
m
m
m m
m
m
m
m
m m
m
m
m
m
m
m
m
m
m
m
m m
m
m
m m

Vertical and
Parallel Coupling

The Translational Dilemma

Traditional Scientific Cycle
Scientific Cycle in Data-Rich, High-throughput Environment
Increasing Dimensionality of
Data
Increased Complexity “Systems Diseases”

What are “Systems” Diseases? • Disorders of Control Structures =>
Generate Abnormal and Undesirable States
• Disordered Responsiveness
• “Brittle” rather than “Fragile”
• Resulting Disease States are Robust because of remaining control structures => Hard to Treat
• Examples: Cancer, Sepsis, Diabetes, Autoimmune Diseases, anything having to do with inflammation, all major health problems today…

Data
Hypotheses
Identification of Correlation
• Statistics • Clustering • Networks • Identify
Relationships • “Curve-fitting”
• Static
Evaluation of Causation
• Experiment (Wet lab or In-
silico) • Test Mechanisms
• “Curve-creation” • Dynamic
Scientific Process
• Cyclical • Iterative
NOTE: Hypothesis are always incomplete!
The emphasis here is Knowledge as opposed to Data

Jorge Luis Borges: ���“On Exactitude in Science” “In that Empire, the Art of Cartography attained
such Perfection that the map of a single Province occupied the entirety of a City, and the map of the Empire, the entirety of a Province. In time, those
Unconscionable Maps no longer satisfied, and the Cartographers Guilds struck a Map of the Empire
whose size was that of the Empire, and which coincided point for point with it. The following
Generations, who were not so fond of the Study of Cartography as their Forebears had been, saw that
the vast Map was Useless...”

Karr, et al. A Whole-Cell Computational Model Predicts Phenotype from Genotype.
Cell 150(2):389-401, 20 July 20, 2012
• Mycoplasm genitalium: 525 genes (E. coli has 4288) • Cluster of 128 computers
• 10 hours runtime for 1 cell division • Generates 0.5 GB data
What? �Science is selective
Abstraction!�Abstraction is the pathway
to Theory!�

The Problem with Biology " Almost completely empirical: “My system is
different!”
" Infinite Regress => “Just give me more detail!”
" The Questions of Science: " What? = Data " How? = Mechanism " Why?* = Contextualize
The output of Science is Knowledge

The “What” of Biology
" “What?” = Description
" Phenotype = Data concerning a particular state
" All data goes to defining a phenotype
" Agnostic to scale

The “How?” of Biology " How? = Mechanism
" Means by which one phenotype arises from another
" Dynamic interpretation of data
" Scale becomes important because mechanisms don’t necessarily commute (Sequence of Events Matters!)

The “Why” of Biology
" Why? can lead to a teleological trap of Final Cause
" Luckily, Final Cause in Biology = Evolution
" Evolution = Diversity + Fitness + Selection + Persistence
" Generally Taboo! => Leads to vitalism, “just-so” stories, Creationism, etc.
" But “Why?” is also a pathway to Theory => Suggests a meta-process

M&S in Bioscience: Path to Theories
" Follow M&S Community’s Standard of Progressive Tiers of Validation " Face validity must come first!
" Discovery rather than Engineering* " Plausibility versus Prediction
" Prediction is not the end-all/be-all, and not even desirable => Biology not mature enough
" Robust Models => Building “Theories” " Rapid iteration with experimentalists

The Importance of “Dynamics” • Dynamic => System evolves over time
• Mechanistic => Approximations of Cause and Effect
• Need to capture movement from Health to Disease…
■ Disease as a specific Dynamic State
Same underlying processes => Different conditions => Different behaviors =>
Different Phenomena => Heterogeneity

Basic Insights from Dynamic Modeling Approach
• “Health” is a dynamic steady state => this is not trivial to model
■ Biological systems and “Health” are very robust => it takes a lot to irrevocably disrupt them
■ Consequently the reaction of the system needs to be vigorous to be effective
■ “Design Principles” => Survival, Selection, Economy and Evolution

Types of Dynamic Computational Modeling
• Equation based methods
• Ordinary Differential Equations (ODE)
• Shifts in variables/measurements over time
• Partial Differential Equations (PDE)
• Shifts in variables/measurements over time and space
• Stochastic Models (Gillespie Algorithm)
• Models that incorporate probability and randomness into component behavior

Another Approach: ���Agent Based Modeling (ABM)
• Object Oriented => Components of the system => Agents
• Rule Based => Mechanisms • Spatial => Virtual World • Intrinsic Stochastics => Heterogeneity • Agent interactions => Population Behavior
=> System Behavior • “Dynamic Knowledge Representation” • Qualitative versus Quantitative

Crossing the Translational Divide with ABM
Organism
Organs
Cell types
Tissues
Molecular mechanisms
Agent Populations Mucosa, epithelium, bone marrow
Rules for the Model Signal Cascades/Gene Regulation
Actors/Agents of the Model Gut flora, colonizing pathogens, dendritic cells, macrophage, epithelial cells, goblet cells
Aggregate Agent Populations Gut (Intestinal epithelium, lumen /
brush border, vasculature, microbiota)
Dynamic, In-‐Silico ABM of Patient The Surgical Patient

Cancer: What is it? • Disordered Cells with Disordered Growth
• Disordered from What? • Failure of Cellular Control Structures
• Cancer is a product of Multicellular Organisms
• Failure Points are related to evolutionary development of multicellularity
• Resultant Cancer behavior akin to unicellular organisms
• Different Evolutionary Strategies • Implications for Cancer behavior

Proposed Generative Hierarchy for Cancer
• 1st Order Process: Promotion of Genetic instability/plasticity • Genetic damage/DNA base pair alterations that
accumulates and not just the regulation of the gene expression network.
• 2nd Order Process: Functional Deficits manifest at the individual cell level. • Proliferation, loss of mortality, impaired DNA damage repair,
loss of migration inhibition. • Loss of evolutionarily generated control structures required
to maintain the integrity of multicellular organisms. • 3rd Order Process: Multicellular effects evident in the
behavior of the tumors as a population of cells. • Angiogenesis, interactions with the stroma, immune evasion,
and release of potentially metastatic cells • Hijacking of "normal" processes present in multicellular
organisms

Source of Damage? • External Sources:
• Radiation, Toxins, Infections • Endogenous:
• Inflammation • Orqanismal Response to Damage • Multi-cellular Organisms • Evolutionarily Conserved • Pathway to Adaptive Immunity • Known Association with Cancers
• Can we contextualize oncogenesis in inflammatory milieu?

1st Order Genetic Instability/
Plasticity
2nd Order Functional Consequences/
Deficits at Individual Cell Level
3rd Order Multicellular/Population
Effects
Adaptation
Environmental Damage
(Inflammatory Milieu)
Therapy Targets
Development of Resistance
X
Fitness Frame Shift To
Colony Behavior
Cancer Cell “Colony”

Base Inflammation Model
• ABM of Global Systemic Inflammation, circa 1990
• Endothelial/Blood interface
• Activation/Propagation of Inflammation
• Endothelial Cells and White Blood Cells
• Reproduces Dynamics of Pathophysiology
• Very Abstract!
An, Shock 2001 and An, Critical Care Medicine 2004

Model of Global Inflammation, circa 1990
Cell types Endothelial cells,neutrophils, monocytes,TH0, TH1, TH2, bacteria,white blood cell generativecells
Cell Receptors andFunctions
L-selectin, E/P-selectin,CD-11/18, ICAM, TNFr, IL-1r, adhesion, migration,respiratory burst,phagocytosis, apoptosis
Mediators Endotoxin, PAF, TNF, IL-1,IL-4, IL-8, IL-10, IL-12, IFN-g, sTNFr, IL-1ra, GCSF


Phenotypically “Healthy” Cell
DNA Damage = Basal-DNA _Damage Rate
+ ROS
If Residual Damage in
1/5 Precancerous/10000 Genes
Intrinsic DNA Repair
_+
Functional Abnormality in 1. Suppression of Proliferation
2. Suppression of Migration 3. Apoptosis
4. DNA Damage Repair 5. Overexpression Proliferation
If DNA Integrity < Cell- Cycle Arrest
Threshold
Cell Cycle Arrest: Decreased Metabolism w/
Enhanced DNA Repair Stays Until Repair or
Replication
“Silent” Mutation
If Residual Damage Present by Replication Threshold
Generationally Propagated
Mutation
Y
Y
Y N
N
N

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 2 3 4 5 6 7 8 9
Healthy Outcome Microtumors Cancers
42 43 44 45 46 47 48 49 50
Basal-DNA-Damage-Rate

0
10
20
30
40
50
60
70
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Incr
easi
ng S
yste
m D
amag
e
Initial Injury Number 50 75 100 125 150 175 200 225 250 275 300 325 350 375 400 425 450 100 475 500
Evidence of Sustained Inflammation

0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Incr
easi
ng R
eact
ive
Oxy
gen
Spe
cies
Initial Injury Number 50 75 100 125 150 175 200 225 250 275 300 325 350 375 400 425 450 100 475 500
Persistent Reactive Oxygen Species

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 2 3 4 5 6 7
Healthy Outcome Microtumors Cancers
150 200 250 300 350 400 450
Initial Injury Number

1 2 3 4 5 6 7
Acc
umul
ated
DN
A D
amag
e (x
106
Uni
t-les
s Va
lue)
0
2
4
6
8
10
12
150 200 250 300 350 400 450 Initial Injury Number
Accumulated DNA Damage/tumor cell

1 2 3 4 5 6 7
Acc
umul
ated
DN
A D
amag
e (x
105
Uni
t-les
s Va
lue)
0
5 10
30 35
150 200 250 300 350 400 450
15
20
25
40 45
Initial Injury Number
Accumulated DNA Damage/microtumor cell

Implications for Cancer Treatment
• Addressing 2nd and 3rd Order Processes need to account for effect on 1st Order Process • Alteration in Selective Forces/Fitness
Functions • Less Disordered: Less immune response but
less evolutionary forcing • More Disordered: Immune response, but
generates more evolutionary forcing • Eradicative Therapies => Increased
Evolutionary Forcing • Environmental Control versus Eradication

Spectrum of Host Pathogen Interactions
1. TECHNICAL PROPOSAL OVERVIEWHealthcare Associated Infections: A compelling clinically relevant targetThe greatest challenge facing the American healthcare system related to infectious disease is to control and prevent infections that occur during and long after the process of hospitalization and exposure to extreme medical interventions. Managing these healthcare associated infections (HAIs) is of paramount importance in the face of escalating medical interventions applied to an increasingly aging and vulnerable population. The healthcare associated pathogens (HAPs) that cause these infections persist within anatomic sites such as the gut, naso-oropharynx and skin and cause recurrent infections within highly variable latent periods. While there has been enormous effort to control these infections with antibiotics, environmental control measures, and immune enhancing drugs, there is compelling evidence that persistent and recurring HAIs are increasing in number. We assert that this is because most current strategies for managing infections focus primarily on either the host or the pathogens, and therefore do not a d d r e s s t h e c r i t i c a l interactions between the host and pathogens that define the clinical course of an infection. The host-pathogen interaction (HPI) is itself a set of dynamic and complex processes, and should be treated as a d is t inct ent i ty and subject for study. More specifically, we assert that being able to characterize the HPI associated with HAIs requires a new systems-level perspective consistent with an ecological and evolutionary viewpoint. For instance, current strategies of microbial control focused on eradication only trigger natural selection processes operating in an evolutionary context leading to adaptations that nullify attempted eradication measures; the development of multidrug-resistant HAPs is an obvious example of this phenomenon. Furthermore, we believe that extreme medical interventions on the host represent seismic shifts in environmental and microenvironmental conditions, leading to massive disturbances in previously stable and persisting HPI ecosystems that push HAPs towards virulent and pathogenic trajectories, which result in cascading micro-ecological collapse, systemic disease and death. We propose to study and characterize the HPI that affects the occurrence, course, and outcome of persistent and recurrent HAIs in patients undergoing extreme medical interventions by incorporating uniquely clinically relevant animal models, comprehensive detailed high-throughput analysis, cutting-edge informatics integration and contextualization of data, and innovative modeling and simulation capabilities into a Research Center that will provide these integrated capabilities to the research and clinical community at large.The approach of our research center, the Host Pathogen Interactions associated with Healthcare Associated Pathogens (HPIHAP) Center, is a tightly integrated methodology consisting of an iterative repeating cycle of computational modeling, experimental
O
OH
OH
OHHO
HO
O
OH
OH
OHHO
HO
Host Metabolism
Host Regulation
O
OH
OH
OHHOHOO
OH
OH
OHHOHO
Host Signaling
Pathogen Metabolism
Pathogen Regulation
Pathogen Signaling
Micro-environment
PathogenicInfection
Health
Benign
Host-Pathogen Interaction
Hea
lthca
re A
ssoc
iate
dH
ost S
tres
sH
ealthcare Associated
Pathogen Virulence
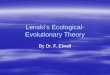
Figure 1. Escalation of hostility in host-pathogen interactions: bidirectional molecular effects of host stress and pathogen virulence leading to healthcare associated infections.
2

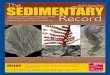
Clostridium difficile Infection (CDI) • 2nd most common hospital related infections • 15-25% of all infectious diarrhea in U.S. • 14,000 deaths in U.S. • Pathophysiology:
• Follows systemic antibiotic treatment • Depletion of baseline intestinal microbiome • C. difficile has an inert spore form and a toxin
producing germinated form • Treatment
• Anti-CDI antibiotics • Fecal microbial Transplant (FMT)

Commensal Microbes
Fecal Microbial
Transplant
C. difficile Spores
C. difficile Germinated
TCA DCA Hepatic Production
Antibiotics
Nutrient Competition
Germination
Sporulation
Induced by Nutrient Scarcity
Intestinal Lumen

A B C
D E
CDIABM Baseline Health
CDI
CDI Toxin View
CDI Taurocholate
CDI Deoxycholate

Total System Damage from Parameter Sweep Resource Replenish Rate

End Commensal Population from Parameter Sweep Resource Replenish Rate

End Total C. difficule Spores and Germinateds from Parameter Sweep Resource Replenish Rate

End Count C. difficile Germinated from Parameter Sweep Resource Replenish Rate

End Count C. difficile Spores from Parameter Sweep Resource Replenish Rate

What does this all get you? If Model Behavior matches real world observations ⇒ The “Thought Experiment” is a Plausible representation of the “real world” ⇒ Look for ways to “break” it
If Model Behavior does not match real world observations ⇒ Re-examine underlying assumptions ⇒ Utilize Modularity for differential fitness ⇒ Science Progresses via Hypothesis Nullification
“It ain't what you don't know that gets you into trouble. It's what you know for sure that just ain't so.” -- Mark Twain

Using Context to Constrain " Need to limit the possible interpretations
of data " Need to limit the possible configurations
of mechanism " Pathway to Theory => “Why it must be
so”
" Theory is what guides Mapping " Interpretation of cross-platform results " Personalization => Generation of State

The Translational Goal " Exercise Control
" Actionable Knowledge
" Establish Sufficient Trust, not Ontological Truth
" Look for conserved functions and architectures => Theories
" There are no Shortcuts
But we can accelerate the cycle...

Proposed Process Flow
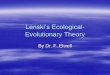
development of the Web Portal, user interfaces and visualization techniques, see Section 2.11.2 and 2.8.4. Our iterative integrated approach to understanding host-pathogen interactions is shown in Figure 2A and consists of the following processes:A. Execution of a series of experiments on clinically relevant animal models with well-defined,
highly-specific phenotypes to produce a repetitive sampling of the HPI over the course of disease progression.
B. Concurrently utilize a combination of high-throughput technologies to generate a diversity of high quality experimental data about the molecular components of the HPI. These technologies include the Functional Genomics Core (FGC) using RNA-Seq and ChIP-Seq, the Quantitative Proteomics Core (QPC) for undirected protein discovery and Micro-western Proteomics Core (MWPC) for targeted characterization of host and pathogen proteins, and the Metabolomics and Lipidomics Core (MLC).
C. Des ign and imp lementa t ion o f an Informatics Core (IC) that will develop and maintain a database, integrated knowledge base and Web Portal. The IC will collect and integrate experimental data from the BACs, track sample preparation with associated workflow metadata, extract and integrate HPI knowledge from external databases and literature, track in silico experiments with provenance metadata, provide data analysis visualization, and publicly disseminate all HPIHAP Center generated data and resources.
D. Design and implementation of a Modeling and Simulation core (MSC) that will develop and maintain the software architecture for an in silico experimental workflow. This workflow includes a “modeling sandbox” that augments hypothesis-driven investigation through semi-automated translation of HPI knowledge into computational models for simulation and analysis. The MSC will provide an ensemble of predictive mathematical modeling methods for understanding the dynamic behaviors and functions of HPI networks, investigating putative new molecular pathway interactions, analyzing potential effects of perturbations and interventions, and designing new biological experiments.
E. Utilize human cells that are infected by HAP to investigate and validate predicted molecular pathway mechanisms, trajectories and outcomes from computationally evaluated hypotheses, perturbations and interventions. The use of human cells provides a bridge from the molecular pathways discovered in our clinically relevant animal models to our eventual clinical human samples. These experiments will produce additional samples for the high-throughput technologies of process B and comprises one layer of the multi-layered iterative cycle of computational modeling, experimental validation and data analysis.
F. Design and execute additional experiments on clinically relevant animal models with perturbations and interventions from computationally evaluated hypotheses of the HPI. These experiments will produce additional samples for the high-throughput technologies of process B as well as perform in vivo confirmation of disease progression and outcome from the predictive mathematical models. This process comprises the second layer of the multi-layered iterative cycle of computational modeling, experimental validation and data analysis.
G. Calibrate our predictive mathematical models to the high-throughput data measurements from normal and pathological human samples. Computational investigation of these models will identify the clinically contextual dynamics and trajectories of particular disease states. Differences between model behavior that generates normal versus pathologic states will
O
OH
OH
OHHO
HO
O
OH
OH
OHHO
HO
Host Metabolism
Host Regulation
O
OH
OH
OHHOHOO
OH
OH
OHHOHO
Host Signaling
Pathogen Metabolism
Pathogen Regulation
Pathogen Signaling
Micro-environment
Clinically RelevantAnimal Models
High-throughputBio-analysisTechnologies
A
InformaticsCoreBC
HumanSamples
Infected HumanCell Cultures
Modeling and Simulation Core
HPIHypotheses
Simulation
In SilicoWorkflow
DE
F
G
Integrated Approach to Host-Pathogen Interactions
Figure 2A. Integrated Approach
6

“Knowledge Ecologies:” Science as Evolution
An, Science Translational Medicine, 2010

Finis






















![[gl0202.doc] The Ecological-Evolutionary Typology of Human](https://img.pdfslide.us/doc/110x75/587f320e1a28ab74298bc70f/gl0202doc-the-ecological-evolutionary-typology-of-human-.jpg)