Embed Size (px)
Citation preview

Nallamothu, Robert Lee Page II, Joseph E. Parrillo, Pamela N. Peterson and Chris WinkelmanFrederick G. Kushner, Jeffrey T. Kuvin, Jose Lopez-Sendon, Dorothea McAreavey, Brahmajee
David A. Morrow, James C. Fang, Dan J. Fintel, Christopher B. Granger, Jason N. Katz,Scientific Statement From the American Heart Association
Care Unit and the Emerging Need for New Medical Staffing and Training Models : A Evolution of Critical Care Cardiology: Transformation of the Cardiovascular Intensive
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation published online August 14, 2012;Circulation.
http://circ.ahajournals.org/content/early/2012/08/14/CIR.0b013e31826890b0.citationWorld Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

AHA Scientific Statement
Evolution of Critical Care Cardiology: Transformation ofthe Cardiovascular Intensive Care Unit and the Emerging
Need for New Medical Staffing and Training ModelsA Scientific Statement From the American Heart Association
David A. Morrow, MD, MPH, FAHA, Chair; James C. Fang, MD, FAHA; Dan J. Fintel, MD;Christopher B. Granger, MD, FAHA; Jason N. Katz, MD, MHS; Frederick G. Kushner, MD, FAHA;
Jeffrey T. Kuvin, MD; Jose Lopez-Sendon, MD; Dorothea McAreavey, MD;Brahmajee Nallamothu, MD, MPH, FAHA; Robert Lee Page II, PharmD, MSPH, FAHA;
Joseph E. Parrillo, MD; Pamela N. Peterson, MD, MSPH, FAHA; Chris Winkelman, RN, PhD; on behalf ofthe American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation,
Council on Clinical Cardiology, Council on Cardiovascular Nursing, and Council on Quality of Care andOutcomes Research
Critical care, defined as the diagnosis and management oflife-threatening conditions that require close or constant
attention by a group of specially trained health professionals,is inherent to the practice of cardiovascular medicine. Thedemand for cardiovascular critical care is increasing with theaging of the population and is reflected by trends in the use ofcritical care in general.1 Between 2000 and 2005, althoughthe total number of hospital beds in the United States declinedby 4.2%, the number of critical care beds increased by 6.5%and the annual costs attributed to critical care increased by44%, representing 13.4% of hospital costs.2 Projections forthe next 15 years suggest that the need for critical care willincrease markedly in the United States and globally.1,3–5 Forexample, in Canada, a 57% increase in the need for criticalcare beds is anticipated during that period.5
Concurrent with increases in demand, the medical demo-graphics of general and cardiac critical care have evolvedtoward a patient population with an increasing number ofcomorbid medical conditions who require more prolongedand more technologically sophisticated invasive support. As aresult, the delivery of critical care is advancing substantiallyin its complexity. Moreover, accumulating evidence has
indicated that outcomes are better when critical care isprovided by specially trained providers in a dedicated inten-sive care unit (ICU).6–9 In the context of this evolution,provision of optimal care in the contemporary cardiac ICU(CICU) presents a different set of challenges and requires anexpanded set of skills compared with 10 years ago. Cardio-vascular medicine has lagged behind other medical disci-plines that have met the “critical care crisis”4 with ICU-focused innovations in organization, training, and qualityimprovement. Therefore, the American Heart AssociationCouncil on Cardiopulmonary, Critical Care, Perioperative andResuscitation, the Council on Clinical Cardiology, the Councilon Cardiovascular Nursing, and the Council on Quality of Careand Outcomes Research have sponsored this writing group toformulate a roadmap to meet the changing needs of the popu-lation with cardiovascular disease requiring critical care.
Evolution of the CICU
Early History of Critical Care CardiologyIn the early 1960s, after the successful implementation ofopen- and then closed-chest defibrillation10–12 and the intro-
The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outsiderelationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are requiredto complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
This statement was approved by the American Heart Association Science Advisory and Coordinating Committee on June 5, 2012. A copy of thedocument is available at http://my.americanheart.org/statements by selecting either the “By Topic” link or the “By Publication Date” link. To purchaseadditional reprints, call 843-216-2533 or e-mail [email protected].
The American Heart Association requests that this document be cited as follows: Morrow DA, Fang JC, Fintel DJ, Granger CB, Katz JN, Kushner FG, KuvinJT, Lopez-Sendon J, McAreavey D, Nallamothu B, Page RL 2nd, Parrillo JE, Peterson PN, Winkelman C; on behalf of the American Heart Association Councilon Cardiopulmonary, Critical Care, Perioperative and Resuscitation, Council on Clinical Cardiology, Council on Cardiovascular Nursing, and Council on Qualityof Care and Outcomes Research. Evolution of critical care cardiology: transformation of the cardiovascular intensive care unit and the emerging need for newmedical staffing and training models: a scientific statement from the American Heart Association. Circulation. 2012;126:●●●–●●●.
Expert peer review of AHA Scientific Statements is conducted by the AHA Office of Science Operations. For more on AHA statements and guidelinesdevelopment, visit http://my.americanheart.org/statements and select the “Policies and Development” link.
Permissions: Multiple copies, modification, alteration, enhancement, and/or distribution of this document are not permitted without the expresspermission of the American Heart Association. Instructions for obtaining permission are located at http://www.heart.org/HEARTORG/General/Copyright-Permission-Guidelines_UCM_300404_Article.jsp. A link to the “Copyright Permissions Request Form” appears on the right side of the page.
(Circulation. 2012;126:00-00.)© 2012 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIR.0b013e31826890b0
1 by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

duction of the first continuous electrocardiographic monitor-ing, the first coronary care units (CCUs) were formed withthe premise that rapid identification and termination ofperi-infarction arrhythmias could dramatically alter the natu-ral history of acute myocardial infarction (MI).13,14 Theearliest CCUs opened almost simultaneously in 1962 in theUnited States and Europe, providing electrical cardioversionand resuscitation care for patients with MI in a single unitcontinuously staffed by specially trained personnel. WhenDesmond Julian, at the time a senior medical registrar of theRoyal Infirmary of Edinburgh (Scotland), presented his novelconception of the CCU to the British Thoracic Society in1961,13 he enumerated 4 basic mandates that have withstoodthe test of time: (1) Continuous electrocardiographic moni-toring linked to alarms, (2) rapidly initiated cardiopulmonaryresuscitation and defibrillation, (3) personnel trained to man-age specialized equipment within a single unit, and (4) skillednurses empowered to independently initiate resuscitation. Asis the case today, nurses “properly indoctrinated in electro-cardiographic pattern recognition, and qualified to interveneskillfully with a pre-rehearsed and well-disciplined repertoireof activities in the event of cardiac arrest” were at theforefront of delivery of care in the early CCU.15 These sameprinciples were described concurrently by Morris Wilburne inan abstract describing a CCU with an “organized programand step-by-step plan of resuscitation” submitted to theAmerican Heart Association annual meeting in 1961.16 In thelate 1960s, the next phase of development of the CCU wasushered in by Bernard Lown and colleagues at the Peter BentBrigham Hospital in Boston, MA, who described a shift fromresuscitation at the time of an arrest to monitoring for earlysigns of clinical change and prevention of a cardiac arrest.15
A precedent for admitting a broader group of patients withsuspected acute MI to a dedicated CCU was established, anda rapid proliferation of CCUs throughout industrialized coun-tries ensued.
The advent of CCUs was temporally associated with andoften credited for a substantial decrease in the in-hospitalmortality rate after MI from 30%–40% in the 1950s to15%–20% in the 1970s.14,17–19 For example, Killip andKimball, in their landmark article on acute MI management,described a nearly 20% decline in the post-MI mortality rateafter implementation of their CCU.17 By 1980, the majorcause of death related to MI had shifted from arrhythmias toventricular failure. New bedside monitoring techniques suchas pulmonary artery catheterization and echocardiographyallowed evaluation of cardiac performance peri-MI, whichled to the characterization of hemodynamic subsets withprognostic and pathophysiological implications for patientmanagement.20 Albeit based on observational data, the avail-able evidence substantiated the vision of Julian and othersthat meaningful improvements in outcomes could beachieved by management of patients within the specializedenvironment of the CCU.21–23
Evolving Demographics and Emergence of theContemporary CICUDespite this evidence of a favorable impact of CCUs overtheir first 2 to 3 decades and the continued decline in case
fatality with MI, at least 1 descriptive study has shownnegligible subsequent improvements in the overall mortalityrate since the 1980s in a major academic CCU.24 The findingsfrom this24 and other studies identified a dramatically chang-ing demographic profile of the patient population in thecontemporary CCU. The proportions of the elderly, women,and minorities admitted to the CCU have all increasedsteadily over the past several decades. Likewise, chronicillnesses, including diabetes mellitus, hypertension, renaldysfunction, and obstructive lung disease, now commonlycoexist with cardiovascular illness in today’s CCU, whichleads to greater case-mix and escalating illness severity.25
Moreover, competitive demand for ICU beds has resulted intriage of lower-risk patients to non-ICU settings. On abroader scale, the aging of the US population, acute andchronic sequelae of nonfatal MI, and a rising frequency ofcomplications of invasive devices have amplified the fre-quency and morbidity of multiorgan dysfunction duringcritical illness.26 At the same time, emerging technologies andimproved therapeutics have altered the natural history ofcritical illness in some groups of patients previously consid-ered unsalvageable, thereby increasing the length of stay, riskof iatrogenic complications, and resource consumption.
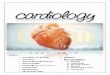
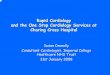
As a result of each of these trends, the medical andprocedural issues that determine outcome in the contempo-rary CCU are often ones that require substantial expertise ingeneral critical care medicine.26 For example, CCUs nowappear strikingly similar to general medical and surgicalICUs with respect to patient characteristics, resource utiliza-tion, and mortality rates.27 Moreover, overall medical com-plexity dominates the outcomes of patients in the modernCCU.28 In an analysis of trends over 2 decades of academicCCU care, Katz and colleagues24 observed a marked increasein the prevalence of sepsis and acute renal failure complicat-ing acute and chronic cardiovascular conditions in the CCU.Not surprisingly, this pattern was also associated with anincrease in the use of bronchoscopy and renal replacementtherapy, along with an increase in the proportion of patientsrequiring prolonged mechanical ventilation and a relativedecrease in the use of cardiovascular procedures (Figure1).24,25,29 Each of these findings underscores the evolutionfrom the earliest CCUs, focused on the management of acuteMI, into the modern CICU, equipped to meet the complexcritical care needs of the patient with cardiovascular disease(Figure 2).
Advanced Technologies and Special Populations inthe CICUThe development of new technologies has heavily influencedthe practice of critical care in cardiovascular medicine (Fig-ure 2). As a result, physicians in the modern CICU must beexperienced in managing the use and complications of ad-vanced medical technologies, including noninvasive andinvasive hemodynamic monitoring tools, complex modes ofmechanical ventilation, renal replacement therapies, imagingguidance for bedside vascular procedures, methods for induc-tion of therapeutic hypothermia, and mechanical circulatorysupport. In addition, the growing populations of patients withsevere pulmonary hypertension and advanced structural heart
2 Circulation September 11, 2012
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

disease merit particular consideration in the formulation of ablueprint to meet the expanding needs of the CICUpopulation.
Advanced Heart Failure and MechanicalCirculatory SupportAlthough the rate of admissions to the CICU for ST-segment–elevation MI has been decreasing over time, thenumber of heart failure admissions has been escalating.24,30
Patients with acute heart failure syndromes and end-stageheart failure can now be stabilized emergently with the use ofmechanical circulatory support devices and extracorporeallife support. As such, management of severe heart failure byuse of advanced pharmacological agents (eg, intravenousinotropes, vasopressors, and vasodilators) and technologies(intra-aortic balloon counterpulsation, percutaneous and sur-gically implanted ventricular assist devices, extracorporealmembrane oxygenation, and renal replacement therapies) hasbecome a major focus of the CICU and requires a well-
coordinated multidisciplinary approach that involves heartfailure specialists and CICU staff. Percutaneous supportmeasures are being used with increasing frequency for themanagement of acute cardiogenic shock and to supporthigh-risk percutaneous interventions and electrophysiologyprocedures.31,32 Such patients are highly susceptible to pro-gressive critical illness, often develop multiorgan dysfunc-tion, and consume substantial clinical resources. Some largecenters have developed specialized “heart failure ICUs” tocare for this growing population. Optimal management of thispopulation of patients and the technology itself requires thatthe providing clinicians are experienced in the appropriateselection of candidates for implantation, the correct use ofsuch devices, and the early recognition or anticipation ofcomplications related to such devices.
Therapeutic Hypothermia in Cardiac ArrestThe care of patients with out-of-hospital cardiac arrest hasimproved significantly since the inception of the early CICU.
Relative Change in Odds of Diagnosis or Procedure
-7%
13%
26%
23%
0%
-4%
11%
6%
-10% -5% 0% 5% 10% 15% 20% 25% 30%
STEMI
NSTEMI
Sepsis
Liver Failure
PCI
IABP
Bronchosopy
Mechanical Ventilation
STEMI
PA line
Figure 1. Temporal trends in dischargediagnoses and critical care procedureswithin the Duke University Coronary CareUnit from 1989 to 2006. Data from Katz etal.24 STEMI indicates ST-segment–eleva-tion myocardial infarction; NSTEMI, non–ST-segment–elevation myocardial infarc-tion; PCI, percutaneous coronaryintervention; and PA, pulmonary artery.
Rapid Resuscita�on
Preven�ve Interven�on
Comprehensive Cri�cal Care
• Mechanical circulatory support• Therapeu�c hypothermia• Advanced modes of ven�la�on • Renal replacement therapy• Invasive & non-invasive monitoring
• Therapy for advanced heart failure• Interven�ons for pulmonary HTN• Protocols for pa�ent safety
• Advanced nursing prac�ce• Mul�disciplinary team-based care• Performance improvement• Heavy use of informa�on technology
• Rapid defibrilla�on
• Nurses as 1st responders
• Post-MI care
• Rapid defibrilla�on• An�arrhythmia therapy• Expanded pharmacotherapy
• Specialized nursing
• Post-MI care• Suspected acute ischemia
Advances in technology
Advances in training & organiza�on
Advances in medical care
Changes in popula�on
• Focus on STEMI pa�ent • All ACS and heart failure • Complex CV disease, severe comorbidity
Figure 2. Evolution of the cardiac inten-sive care unit. Advances in technology,medical care, critical care unit organiza-tion, and changes in the patient popula-tion have contributed to evolution of thecontemporary cardiac intensive care unitfrom a coronary care unit focused onrapid resuscitation to a unit providingcomprehensive critical care for patientswith cardiovascular diseases. MI indicatesmyocardial infarction; STEMI, ST-seg-ment–elevation myocardial infarction;ACS, acute coronary syndrome; HTN,hypertension; and CV, cardiovascular.
Morrow et al The Evolution of Critical Care Cardiology 3
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

Since landmark trials demonstrated the benefits of therapeutichypothermia,33,34 rapid implementation of cooling has beenrecommended for all eligible patients who remain comatoseafter successful restoration of spontaneous circulation afterventricular fibrillation or pulseless ventricular tachycardia.Whether cooled invasively or through external methods, theuse of induced hypothermia mandates a carefully orchestratedplan with substantial resource requirements. Patients treatedwith hypothermic techniques commonly require specializedmonitoring, prolonged mechanical ventilation, and extendedICU care. From a critical care perspective, those with cardiacarrest are frequently unstable, at risk for end-organ injury,and particularly vulnerable to infectious complications, in-cluding severe pneumonia. Prognostication regarding neuro-logical recovery after therapeutic hypothermia has evolvedsuch that longer time may be required to determine a lowchance of recovery. Although often challenging, such prog-nostication is central to medical decision making after re-warming.35 Multidisciplinary clinical collaboration and expe-rienced clinical management are important to improveoutcomes for such patients. As therapeutic hypothermiabecomes applied more broadly, the evolution of the CICUmust anticipate the growing needs of the heterogeneous groupof patients with restoration of spontaneous circulation aftercardiac arrest.36
End-of-Life Care in the CICUAs a consequence of greater disease severity and expandedsupportive technologies within the CICU, end-stage diseasestates have become commonplace. Coordination of end-of-life care, including discussions with patients and families,decision making about deactivation of devices such as inter-nal defibrillators, ethics consultation, pain management, andsymptom relief, is now a central part of compassionate care inthe CICU.37 Family members consistently emphasize theimportance of effective communication in the intensive careenvironment and most often rank communication aboveclinical skills when assessing physician quality of care.38,39
Better communication reduces psychological trauma symp-toms, depression, and anxiety; shortens ICU length of stay;and improves the experience during terminal care.40,41 There-fore, a focus on family communication during the delivery ofcritical care is an essential element of best practice in theCICU.41 The CICU staff must also be familiar with optionsfor palliative interventions and services to provide effectivetransitions in care.
Important Trends in Critical Care: LessonsLearned From General Medical and
Surgical ICUsSignificant technical, medical, and organizational advanceshave changed the face of general critical care medicine. Theevidence underlying these advances has originated almostentirely from applied research conducted in general medicaland surgical ICUs; however, this progress bears lessons vitalto the continued maturation of the contemporary CICU andtherefore will be discussed in detail in this section beforeturning back to the CICU in “Roadmap for the Future inCritical Care Cardiology.” In particular, 3 major evidence-
based trends in critical care medicine can be identified: (1) Afocus on interventions to optimize patient safety, driven bythe recognition that ICU-related complications are a majordeterminant of outcomes; (2) a shift toward staffing modelsand structures of ICU coverage that place emphasis oninvolvement of dedicated intensivists, with advanced trainingand/or experience in critical care; and (3) recognition of theimportance of integrated multidisciplinary care with coordi-nated activities of physicians, nurses, respiratory therapists,pharmacists, nutritionists, social workers, and consultants.
Notably, despite the increase in admissions of elderlypatients with complicated medical conditions to generalICUs, there has not been an increase in ICU mortality rates,which provides indirect evidence for steady improvement inthe quality of ICU care.1,42 Moreover, these improvements inclinical performance, tied to patient safety and quality of care,have been recognized as important not only by ICU personneland hospitals but also to accrediting and public agencies.43
The evidence supporting each of these trends will be re-viewed within this section, with a particular focus on staffingmodels that have been developed and investigated in thegeneral critical care environment.
Patient Safety and Preventive PracticesInfections and other complications of the multitude of inva-sive methods for monitoring and treatment used routinely inthe ICU have attracted substantial attention as potentiallypreventable causes of morbidity and mortality in patientsreceiving critical care. Sepsis remains a significant cause ofdeath in the ICU44 and is related to an aging population,indwelling devices such as vascular and urinary catheters,prolonged intubation with mechanical ventilation, and moreprevalent immunosuppressive therapy.44–46 Prudent use ofinvasive devices is essential to reduce sepsis and its attendantmorbidity and mortality.47–49 When invasive devices arenecessary, experienced operators should use rigorous proto-cols for sterile catheter placement and maintenance. Suchprotocols can substantially reduce catheter- and central line–related bloodstream infections (CLABSI or CLABI).50 Otherinterventions that may reduce ICU-related complicationsinclude restrictive blood transfusion strategies,51,52 measuresto prevent and contain Clostridium difficile infections, anddaily awakening of patients from sedating medications toreduce the duration of both mechanical ventilation and lengthof stay in the ICU.53
Additional improvements in patient safety have becomepossible through technical advances in noninvasive ICUmethods. For example, noninvasive mechanical ventilationhas reduced intubation- and ventilator-associated pneumonia(VAP) rates for selected patients with pulmonary edema orhypercarbic respiratory failure.54 Critical care providers arenow trained in these and other important techniques, such asultrasound methods that are now widely used in ICUs toassist in line placement and other percutaneous proceduressuch as thoracentesis.55,56 Noninvasive methods for hemody-namic assessment continue to be refined.57,58 Lastly, the roleof intelligent information systems in the ICU has grown,providing new opportunities for decision support, safety
4 Circulation September 11, 2012
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

flags, and tools for improved communication and qualityimprovement.
Physician Staffing Patterns and Clinical OutcomesEach of the interventions described in the preceding sections,including procedural practices, noninvasive methods, andsafety and communication protocols, contribute to a complex-ity of the ICU environment that requires experience andexpertise. Because of this complexity, organizational andstaffing models for the ICU have been a focus of research incritical care medicine. The results of this research havemotivated an ongoing global shift in the predominant struc-ture and clinical operations in ICUs to place value onproviding an experienced, multidisciplinary team, led by anICU-based physician skilled in critical care medicine (the“dedicated intensivist”).
Open Versus Closed ICUsIn the United States, several organizational models for ICUsexist: Open, semi-open (hybrid), and closed. In an open ICU,patients are admitted or transferred and subsequently man-aged by their individual physicians, without routine assess-ment by an intensivist. The admitting attending physician,however, may seek consultation from relevant subspecialists.By comparison, in a closed ICU, an ICU-based physicianevaluates all admissions and assumes primary responsibilityfor all aspects of patient care. In a semi-open ICU, in whichthe structure lies somewhere between the open and closedmodels, patients are admitted under the care of a primaryattending physician, with ICU-based intensivists available forconsultation and comanagement at the discretion of theprimary attending physician.
In multiple observational studies, compared with openICUs, closed medical and surgical ICUs have reported lowermorbidity and mortality without an increase in resourceutilization.59–62 In a rigorously performed meta-analysis of 27observational studies of critically ill adults and children thatcompared outcomes in open versus closed ICUs, closedICUs, which by design provide high-intensity staffing (asdiscussed in “Intensivist Versus Nonintensivist Coverage”),were associated with reduced hospital and ICU mortality andwith reduced use of resources and length of stay.9 The
potential influence of unidentified selection or publicationbiases, as well as confounding factors, such as from temporalchanges in mortality, must be considered in these observa-tional studies with principally historical controls. Neverthe-less, better outcomes reported in closed ICUs may plausiblybe related to the presence of an intensivist directing care, toimproved overall consistency of care and collaboration be-tween team members inherent to the closed-unit environment,or to both elements contributing to more sophisticated patientmanagement. In one retrospective study of outcomes in openand closed ICUs simultaneously managed by the same groupof faculty intensivists, mortality was lower in the closedsystem, without a significant increase in cost.63 This findingsuggests that the superior outcomes observed in closed ICUsare related to aspects of closed ICU care that are not providedsolely by the availability of a consulting intensivist. Someexperts have suggested that team care should be adopted asan alternative term to a closed ICU to emphasize the benefitsof integrated multidisciplinary care of critically ill patients.64
Intensivist Versus Nonintensivist CoverageThe results of more than 10 nonrandomized studies indi-cate that ICUs managed by intensivists achieve superiorclinical outcomes, including reduced length of stay andassociated costs,65,66 length of mechanical ventilation,60
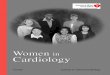
and mortality.6 –9,61,67,68 In the majority of these studies,high-intensity ICU physician staffing has been defined asmandatory intensivist consultation or a closed ICU andcompared with low-intensity staffing, defined as no intensiv-ist or elective intensivist consultation. In a meta-analysis ofthese studies, high-intensity ICU physician staffing wasassociated with a 39% lower ICU mortality rate (relative risk,0.61; 95% confidence interval, 0.50–0.75) and 29% lowerhospital mortality (relative risk, 0.71; 95% confidence inter-val, 0.62–0.82), as well as reduced ICU and hospital length ofstay (Figure 3).8
Limitations to this evidence should be recognized. Themajority of studies of ICU staffing models were conducted�10 years ago, were relatively small in size, and hadnonrandomized designs. In addition, in one analysis of a largeadministrative data base of ICU patients, hospital mortalitywas actually higher for patients managed by intensivists.69
Se�ngICU Mortality Rate
Rela�ve Risk (95% CI)OR L95 U95 p-value
Med/Surg 0.48 0.32 0.72 <0.001
Med/Surg 0.69 0.52 0.91 0.009
Surgical 0.60 0.49 0.73 <0.001
Medical 0.82 0.61 1.10 0.19
Surgical 0.42 0.20 0.89 0.024
Medical 0.71 0.54 0.94 0.015
Surgical 0.54 0.26 1.11 0.094
Pediatric 0.53 0.17 1.65 0.27
Med/Surg 0.61 0.41 0.91 0.017
Medical 0.59 0.44 0.79 <0.001
Surgical 0.15 0.05 0.47 0.001
Pediatric 0.38 0.27 0.53 <0.001
Medical 1.44 1.00 2.07 0.049
0.61 0.50 0.75 <0.001
0.1 0.2 0.5 1 2Favors High-
IntensityFavors Low-
Intensity
N
439
625
667
2409
274
1389
177
262
1656
2959
426
619
349
12251Overall
Figure 3. Meta-analysis of 13 studies ofhigh-intensity vs low-intensity intensivecare unit (ICU) staffing with an outcomemeasure of ICU mortality. The setting indi-cates the type of ICU (medical or surgical[Med/Surg]). N denotes the sample size;OR, odds ratio for mortality with high-intensity vs low-intensity staffing; L95,lower 95% confidence interval; and U95,upper 95% confidence interval. Data arefrom Pronovost et al9 with permission ofthe publisher; individual citations for eachstudy are provided in that reference.Copyright © 2002, American MedicalAssociation. All rights reserved.
Morrow et al The Evolution of Critical Care Cardiology 5
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

However, in that study, the majority of the ICUs includedwere open units with elective intensivist consultation.70 Forthese reasons, multicenter, well-controlled (such as cluster-randomized) outcome studies would be valuable to rigorouslytest the hypothesis that intensivist-based ICU care confersboth a survival benefit and economic savings.71 Other studieswould also be useful to tease out the multiple factors thatinfluence ICU outcomes and costs, including severity ofillness, divergent therapeutic approaches, increasing physi-cian workload,72 and patient insurance status.73
Despite the limitations to these data, the overall consisten-cy of the available evidence and the rational basis forimproved outcomes with enhanced experience, which is acentral tenet of medical and procedural training, are compel-ling. Intensivists may improve outcomes through commonpractices, provision of urgent therapy, familiarity with acuteconditions usually seen only in the critical care setting,facilitation of multidisciplinary care, increased use ofevidence-based measures for prevention of complications,and provision of an ICU leadership role.7,71,74,75 Intensivistsare more likely to implement newer care technologies76 androutinely introduce basic improvements, such as a reductionin use of central lines50 or use of simple and effectivechecklists.77 Lengthy ICU stays have been associated withlack of access to an intensivist.78 Taken together, there is astrong rationale for systems that are built on a pivotal role fordedicated intensivists.
Twenty-Four-Hour In-House Intensivist CoverageIn the United States, intensivists have traditionally providedICU coverage during daytime business hours, with an esti-mated availability of intensivist care during night hours of�10% of ICUs.79 Many critically ill patients are admitted toICUs during off hours, and if proper and rapid therapy isdelivered, mortality may be similar to daytime admis-sions.80–82 However, some studies suggest that patients ad-mitted to the ICU during off hours have higher mortality evenafter adjustment for severity of illness.83–87 This evidence hasled to consideration of continuous (“24/7”) intensivist care.At least 4 observational studies report that introduction of24-hour in-hospital intensivist coverage of the ICU wasassociated with lower mortality,88–90 fewer complications,and reduced hospital length of stay.91,92
Although nocturnal intensivist coverage has been associ-ated with shorter hospital length of stay and lower overallcost for the sickest patients, this may not necessarily be thecase for less severely ill patients.93 Some experts have arguedthat 24/7 (24 hours per day, 7 days per week) intensiviststaffing itself does not reduce mortality or length of stay.71 Anumber of factors could account for the differences inmortality rates seen when times of ICU admission arecompared, such as differences in illness severity for patientsadmitted at night and general system issues such as lowerlevels of medical, nursing, and administrative staffing duringoff hours.86,90
One study raised the hypothesis that the presence oftraining programs in many academic centers may adverselyimpact care94 and that 24/7 attending physician oversight mayprove advantageous. Another benefit is that the intensivist
can continue to educate residents during evening hours. Suchnew educational opportunities may become especially valu-able as resident duty hours are restricted or further reduced.95
However, 24-hour in-hospital intensivist coverage has beenreported to reduce job satisfaction and produce “burnout” ina manner that is correlated with the increased number of nightshifts on duty.96 Introduction of continuous in-hospital inten-sivist coverage therefore requires a balanced assessment ofeach of these issues within an individual healthcare system.
TelemedicineBecause of the obvious impact on staffing and workforcecomposition necessitated by 24-hour coverage schemes, amajority of ICUs in smaller hospitals may be unable tosupport such a model. Care by remote supervision from anintensivist using information technology–supported or video-assisted monitoring may help to resolve this issue and lowercosts.97 Telemedicine can increase intensivist availabilitythrough information technology–based communication andprovide direct intensivist input when a physician is notimmediately available at the bedside. Such a system may useintelligent algorithms to monitor physiological and laboratorydata, identify concerning trends or results, and reduce errorsthat could result in adverse outcomes.98–100
Evidence showing benefits from use of telemedicine inICUs has supported promise for the strategy, but findingshave not been uniformly positive. Observational studiescompared with historic controls have reported reductions inlength of stay and mortality in the ICU and hospital, fewercomplications, improvements in best practices and quality ofcare, and a positive financial impact.98,100–103 However, otherstudies have described no significant change in mortality ormorbidity after implementation of an electronic ICU.104,105 Inone meta-analysis, there was lower mortality and length ofstay within the ICU after implementation of telemedicine butno difference in hospital mortality or overall length of stay.106
These inconsistent findings could be explained by crossovereffects between comparator groups or differences in applica-tion of the telemedicine model itself.105 Moreover, telemedi-cine as a monitoring tool is likely to be effective only in thecontext of other important interventions to improve qualitycare. Issues of cost, reimbursement, and legal and ethicalfactors arise with consideration of telemedicine. The scopeand extent of coverage, proper licensure of participatingphysicians, development of accurate performance measures,lack of direct physician contact, and related job satisfactionare significant but not insurmountable hurdles toimplementation.107–109
Telemedicine may be considered an adjunct to the currentICU system to alleviate the impact of a shortage of intensiv-ists that is not likely to be resolved in the near future.Telemedicine may be especially useful for remotely locatedICUs and could improve physician efficiency in the manage-ment of very large or multiple ICUs.
Physician Workforce IssuesAn estimated 25% of all US ICUs have an intensivist whomanages most (�80%) of the patients, and �50% of all ICUshave no intensivist at all.79 Because of this lack of staffintensivists, a large number of US hospitals employ hospital-
6 Circulation September 11, 2012
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

ists to provide ICU care.79,110 Importantly, if universal ICUcoverage by intensivists were to become an objective, theexisting workforce would be insufficient to provide suchcoverage.1,79,111,112
Efforts to increase the size of the intensivist workforcehave been supported by professional societies, for example,with the recent proposal that emergency medicine residentstrain in critical care113 and subsequent approval of thepathway by the Accreditation Council for Graduate MedicalEducation (ACGME). Moreover, a pathway for dual certifi-cation of cardiologists in critical care medicine and cardio-vascular medicine is already in place and is discussed indetail below (“A Model for Training in Critical Care Cardi-ology”). In addition, to manage the expanding demand forintensivists in the face of a constrained workforce, there isalso a need to explore more basic organizational changes,including regionalization of services, establishment of proto-cols for care, greater nighttime use of other medical personnelor physician extenders, better information technology sys-tems, and consideration of telemedicine in some settings.114
This need may be heightened in some academic settingsbecause of concurrent restrictions to trainee work hours.115
Multidisciplinary CareAttention to the organizational environment in the ICU isessential to ensure the best practice of critical care medi-cine.2,116–118 Specialized critical care nurses are essential tohigh-quality ICU care (as discussed in “Nursing, AdvancedPractice Providers, Pharmacy, and Other Staffing for CI-CUs”). In addition, as the medical complexity of the patientpopulation has increased, so too has the complexity ofpharmacotherapy, with increased potential for adverse drugevents and drug-drug interactions. The addition of pharma-cists to the critical care team has been associated with lowerrates of adverse drug events and complications related to drugtherapy, lower mortality rates in the ICU, and shorter lengthof hospital stay.119–121 As the profession of pharmacy hasmoved from a product-focused to a patient-focused one,pharmacists have been successful in protocol developmentand implementation, therapeutic drug monitoring, adversedrug event surveillance and reporting, orchestration of clini-cal trials, and provision of drug information within the ICUsetting.122 Nutritional management of critically ill cardiovas-cular patients, particularly those with multiple coexistingdisorders, is challenging. Dieticians evaluate dietary intake,formulate tailored nutritional delivery, and help patients toattain or maintain optimal nutritional status. Physical thera-pists identify and treat impairments in strength, range ofmotion, and potential adverse functional outcomes fromprolonged critical illness.123–125 Prolonged immobility in theICU can lead to ICU-acquired weakness and other neuromus-cular impairment.126 Promotion of early mobility and physi-cal therapy in critically ill patients, including those withongoing mechanical ventilation, is feasible and safe127,128 andhas been associated with reductions in the incidence ofpulmonary complications, delirium, the number of ICU andhospital days, and subsequent readmissions.127,129,130 Socialworkers contribute to the care of the complex cardiovascularpatient through counseling and case management, ensuring
that patient and family goals are communicated and incorpo-rated in transitions and discharge plans.131
Quality Improvement in the ICU
Quality Measures in the ICUGiven the high mortality rate, increased resource utilization,and potential for iatrogenic complications, ICUs have been afocus of quality assessment and improvement activities. Inparticular, the multiple levels of interprofessional andprofessional-patient communications in an ICU result ingreater potential for gaps in such exchanges. Successfulquality assessment requires the quantification of relevantmetrics. Donabedian’s model of quality improvement guidesquality assessment and includes evaluation of structure (howcare is organized), process (care delivered), and outcomes(results achieved).132 Others have adapted this model toinclude culture (collective attitudes and beliefs of caregivers),which is particularly relevant in the ICU given the manyindividuals involved in the care of each patient and thenecessary communication and collaboration.133
Quality assessment initiatives in the ICU have traditionallyfocused on outcomes, particularly on mortality rates. Anumber of prediction models or acuity adjustment scores areavailable for ICU or hospital length of stay and mortality,such as the Acute Physiology and Chronic Health Evaluation(APACHE), Simplified Acute Physiology Score (SAPS),Mortality Probability Model (MPM), and Sequential OrganFailure Assessment (SOFA).134,135 With such models, anacuity adjustment score can be applied to compare the actualmortality in an ICU and the mortality predicted by the model(eg, the standardized mortality rate), which provides a bench-mark for comparison.136 However, how this and other criticalcare predictive models perform in patients with primarycardiovascular disorders is less explored. In addition, manyrisk models developed among cardiovascular patients (suchas risk scores in patients with MI) do not include measures ofgeneral medical illness and may underestimate risk in patientswith severe medical comorbid conditions.
The rate of CLABI has become an important outcomemeasure of morbidity in the ICU. Such infections can bemeasured in a systematic manner, and focused interventionshave been shown to prevent them. Examples of other processmeasures that are now widely integrated into ICU practiceinclude appropriate sedation guidelines, prevention of VAP,stress ulcer prophylaxis, and deep vein thrombosis prophy-laxis. Structural measures (organization of care) include thepresence of intensivists, higher nurse-to-patient ratios, andpharmacist presence during rounds.
Regulators, accreditors, and professional societies havealso adopted or developed quality measures and data collec-tion tools. The Joint Commission developed a set of 4measures (VAP prevention, ulcer prophylaxis, deep veinthrombosis prophylaxis, and CLABI) and 2 test measures(ICU length of stay, hospital mortality for ICU patients)specific to the ICU. The measure set was unique in that it wassetting-specific rather than condition-specific and that the 2test measures required clinical data collection instead ofrelying completely on administrative data for risk adjustment.These measures were rigorously tested and reviewed by a
Morrow et al The Evolution of Critical Care Cardiology 7
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

technical advisory panel but were suspended in 2005 beforebeing implemented because of prioritization of surgical-related care. The measures remain in the Joint CommissionMeasure Reserve Library,137 and it is likely that these orsimilar measures will be implemented in the future asexternal benchmarks of quality in the ICU.
Benchmarking and Public Reporting ofPerformance DataCollection and reporting of ICU performance data have beenencouraged by local initiatives, professional cooperatives,and accreditors but to date are not required in the UnitedStates.138,139 Performance can be evaluated by comparing anICU against itself over time, against other comparable ICUs,or to other benchmarks such as best practice.140 Feedback isintended to then drive performance improvement. In addition,there are many medical domains in which performance andbenchmarking are now publicly reported, allowing consumersand stakeholders access to the information. Beginning inearly 2012, the Centers for Medicare and Medicaid Servicesbegan publically reporting CLABI rates in ICUs throughoutthe United States.141 This reporting initiative presents datathat are predominantly voluntarily reported to the Centers forDisease Control and Prevention’s National Healthcare SafetyNetwork. In addition, mandatory reporting of VAP exists inat least 3 states (Oklahoma, Washington, and Pennsylva-nia).141 It is anticipated that ICU-based metrics such as VAPand CLABI rates will ultimately be subject to more wide-spread mandated public reporting. In some instances, perfor-mance may be tied to payment. From a cardiovascular criticalcare perspective, acute MI and heart failure core measure setsare already benchmarked and publically reported as hospitalquality measures.142–145 In addition, established continuousquality improvement efforts such as the American HeartAssociation’s Get With The Guidelines quality program inheart failure, stroke, resuscitation, and coronary artery diseasehave well-developed in-hospital modules. Although thesemeasures are condition- rather than setting-specific, a numberof these measures are relevant to the CICU setting.
External Expectations for ICU StaffingOn the basis of the strong association between ICU structure,the presence of an intensivist, and patient outcomes, a numberof groups external to individual hospital systems or medicalprofessional societies have articulated goals for staffing ofICUs. For example, Leapfrog, a business group that promotes“big leaps” in healthcare safety, quality, and customer valuethrough voluntary hospital surveys, has proposed that ICUsshould be closed units with a board-certified intensivistpresent during the day and an intensivist immediately avail-able by pager in off hours.146 Furthermore, Leapfrog recom-mends that all ICU admissions should be managed or coman-aged by intensivists. Financial estimates have suggested thatsuch a model would reduce hospital costs significantly andshould be adopted by hospital administrators.147 Althoughtheir methods are not universally accepted as ideal, Leapfrogis one example of the growing number of organizationsrecognizing and promoting healthcare quality, as well assetting external expectations toward these ends. Anotherprofessional group, the Committee on Manpower for the
Pulmonary and Critical Care Societies, has suggested that�80% of ICU patients be under the care of full-timeintensivists.79
Roadmap for the Future in CriticalCare Cardiology
These key lessons from general critical care medicine de-tailed in the preceding section, including the well-foundedfocus on patient safety, the more favorable outcomes whencare is delivered by clinicians with advanced skills in criticalcare medicine, and the value of structured multidisciplinarycare, are vital to the continued maturation of the CICU. In thecontext of a growing interest of business entities, consumerfocus groups, and public agencies tasked with improving thequality of ICU care, there is an imperative for the cardiovas-cular community to develop a pathway to respond to the“critical care crisis.” Not only is this effort in the best interestof patients, but some of these changes will likely becomeexternally mandated.
The substantial evidence accumulated over the past 30years in critical care medicine may be used to guide the nextphase of evolution of the CICU. Although these data werederived predominantly in general ICUs, they provide the bestavailable information on which to base rational judgments indeveloping a roadmap for advancing practice in the CICU. Inparticular, the available data suggest that the open model fororganization and staffing of CICUs that is prevalent in theUnited States may not provide the best possible outcomes inthe setting of current practice and patient demographics in theCICU.
Potential Models of Physician Staffing inthe CICUAlthough the advanced expertise of the cardiovascular spe-cialist is essential to providing optimal care for patients withacute cardiovascular diseases, the increasingly challengingand extensive medical comorbid disease of patients cared forin the CICU has created a need for clinicians skilled ingeneral critical care medicine. Thus, increasing the availabil-ity of clinicians with general critical care skills is an impor-tant objective for sustaining and advancing the quality of carein the modern CICU. A pathway toward achievement of thisgoal must also take into account the diversity of needs andresources across varied settings, including rural environ-ments, community-based hospitals, and major tertiary referralcenters. As such, to be successful, the organization andstaffing of the CICU must be individualized to the caresetting. Nevertheless, the writing group believes that accessto clinicians who have specialized skills in critical care isimportant for all settings in which cardiovascular critical careis provided. The writing group also finds that the evidencesupports a closed structure with staffing by dedicated cardiacintensivists (as discussed below in “Dedicated Cardiac Inten-sivists”) as a preferred approach for the advanced CICU(level 1 CICU, “Proposal for Categorization of CICUs”).However, we present first a model of shared responsibilitythat is more broadly applicable to the current predominantstructure and diverse care environments of CICUs in theUnited States.
8 Circulation September 11, 2012
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

Shared Responsibility With Consulting IntensivistsThe most flexible organizational paradigm is a semiopen unitin which cardiologists and a general intensivist comanageeach patient or selected patients in the CICU. This structurealso is most adaptable for CICUs that care for patients withboth higher and lower severity of illness, such as low-riskpatients with suspected acute coronary syndrome or hemody-namically stable arrhythmias (level 2 or 3 CICU, “Proposalfor Categorization of CICUs”). Within this model, the writinggroup favors a structure in which an experienced intensivisttakes primary responsibility for the care of each critically illpatient in the CICU (eg, patients with multiorgan dysfunctionor those requiring mechanical ventilation), with ongoingcollaborative comanagement by the cardiologist. However, acollaborative model with a primary cardiovascular specialistwith close, daily consultative care by a dedicated intensivistmay be most appropriate in some health systems. In somesettings with limited physician resources, this approach mightinclude accessibility of a consulting intensivist via a tele-medicine program.
Under this approach, physician leadership of the CICUmight include both a cardiologist and an intensivist boardcertified in critical care medicine working collaboratively.Key principles guiding the development of this structureinclude high-intensity involvement of an intensivist, coordi-nation of an experienced multidisciplinary team, establishedpreventive programs for complications of ICU care (VAP,stress ulcers, and CLABI), and meaningful quality improve-ment initiatives. The major advantage of the shared respon-sibility model is that it can be adapted to a broad array ofstaffing environments, including smaller community-basedhospitals where the CICU might be combined with a generalmedical intensive care unit or where critical care staff are fewin number or supported by other disciplines such as anesthe-sia critical care. Its success is dependent on effective collab-oration between the cardiologist and intensivist in creating aunified plan for care of the critically ill patient with cardio-vascular disease.
Dedicated Cardiac IntensivistsThe creation of a staffing model with dedicated cardiacintensivists is an alternative approach. The cardiac intensivistmust have well-developed expertise in both general criticalcare and cardiovascular medicine. Such skills may have beendeveloped through clinical experience focusing in cardiaccritical care, as has been formalized in Europe (“The CICU:Models in Other Countries”) or through formal advancedtraining in general critical care (“Training Programs inCardiovascular Medicine and Critical Care”). Leapfrog hassuggested that intensivists must maintain their skills throughat least 6 weeks of full-time ICU care each year.146 Ideally,the cardiac intensivist will function within a closed CICUmodel, in which the intensivist, while caring for patients inthe CICU, provides care exclusively in the ICU, is present atall times during daytime hours, and when not present on-siteis available for consultation with suitably skilled team mem-bers who are on-site. This model can be adapted to provide24-hour in-hospital intensivist coverage if desired.
This innovative paradigm more directly matches the needscreated by the dramatic changes in the CICU since itsinception 50 years ago. This model has the advantage ofproviding for the most seamless direction of complex carethrough the leadership of a single physician who takesprimary responsibility for the patient. In this model, theICU-based physician is experienced in coordinating a largemultidisciplinary team that is integral to the functioning ofthe advanced contemporary CICU. The writing group alsoreaffirms the value of primary responsibility for managementof patients whose dominant medical problem is cardiovascu-lar residing with a clinician with advanced skills in cardio-vascular disease.
Because of the need for full-time staffing by cardiacintensivists despite a limited workforce, this model is notlikely to be suitable for many community-based hospitals;however, it is likely to be the optimal model for the largetertiary referral center. Widespread implementation of thismodel to meet the needs of existing CICUs would require anincrease in the number of cardiologists with advanced expe-rience or training in critical care cardiology and would likelybenefit from an increase in the number of cardiovascularclinicians with formal training in critical care cardiology.Such a broadly trained critical care cardiologist would beideally suited for leadership and staffing of the level 1 CICU,the most advanced CICU (“Proposal for Categorization ofCICUs”).
Integration With Other ICUsAnother possible structure for CICUs would be to combinethe CICU patients with surgical or medical ICU patients,producing a multidisciplinary unit that manages a very broadarray of patients. Such a CICU would require leadership fromcardiology, critical care medicine, surgical critical care,and/or anesthesia critical care. This combined ICU couldhave some geographic segmentation of surgical, medical, andcardiovascular patients into pods, with flexibility to overlapbeds depending on patient demand. This model provides theflexibility to mitigate the impact when specialty ICU bedavailability does not allow appropriate triage of patients toparticular ICUs. This model would be similar to some ICUsformed in Europe and other parts of the world.
“Service Line” ICUsThis solution also has the potential to best serve the expand-ing group of patients with advanced heart disease who requirecomplex care for chronic heart disease and acute managementfor cardiogenic shock, percutaneously placed ventricularsupport devices, or extended mechanical hemodynamic sup-port from surgically placed devices while awaiting destina-tion therapies. With this approach, a more disease-centric (orservice line) model of care can be delivered, which alsocenters the care around the patient rather than the therapiesprovided. In this paradigm, a CICU would care for all patientswith advanced heart disease throughout the entire course oftheir critical illness. Importantly, the entire spectrum of theircare, including hemodynamic guided therapy, before andafter cardiovascular surgery, before and after complex car-diovascular procedures, and palliative services, would be
Morrow et al The Evolution of Critical Care Cardiology 9
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

provided in a single ICU. Specialized heart failure units arean example of such an approach.
Nursing, Advanced Practice Providers, Pharmacy,and Other Staffing for CICUsFrom the inception of the first CCUs, specialized nursing hasbeen a foundation of excellence in cardiology critical care.Cardiovascular specialty certification is available to regis-tered nurses with experience in cardiac patient care148 or as asubspecialty after achieving certification as a critical carespecialist as either a registered nurse or advanced practicenurse (ie, nurse practitioner or clinical nurse specialist).149
Certification among nurses has been associated with highquality of care, high patient satisfaction, and potential forimproved reimbursement.150,151 Moreover, the integration ofadvanced practice providers (nurse practitioners and physi-cian assistants) into the cardiac critical care team can improvepatient outcomes, including reduced length of stay anddecreased complications, particularly among the chronicallycritically ill population.152–154 Advanced practice providerswith specific training and experience in cardiac conditionscontribute to cost-effective care, improved staffing, andcontinuity of care.
Among pharmacists, additional specialty certification incardiology is available to those who are board certified inpharmacotherapy through the Board of Pharmaceutical Spe-cialties and have additional training or advanced experiencein cardiology. These pharmacists can petition the Board ofPharmaceutical Specialties for the credential of Added Qual-ifications in Cardiology.155,156 Additionally, postdoctoral spe-cialized residency training and fellowships exist for pharma-cists in cardiology and critical care medicine who have alsocompleted a first-year general practice residency after grad-uation with a doctor of pharmacy degree.157
Although there is less information about the effects ofspecialty certification on patient care for other cardiac careteam members, certifications are available to physical thera-pists (cardiac and pulmonary care).158 Dietitians, respiratorytherapists, and social workers do not have specialty cardio-vascular certification but may benefit from developed exper-tise based on continuity of experience in a CICU.
Proposal for Categorization of CICUsBecause it is not necessary nor possible for all healthcareenvironments to support an advanced closed CICU withfull-time intensivist staffing, the writing group recognizesthat a variety of organizational models with different levels ofprofessional and technological resources will be used to carefor patients. The writing group has proposed a schema fordescribing the level of care offered by the CICU within thestructure of the individual healthcare system (Table 1). Thisnomenclature is similar to the American College of Surgeonstrauma center verification.159,160 In the trauma center classi-fication system, centers must not only meet specific criteriaestablished by the American College of Surgeons but alsopass a site review by a verification review committee. Theofficial designation as a trauma center is determined byindividual state law provisions, with the level varying accord-ing to the specific capabilities, ranging from level I being the
highest to level III as the lowest category in most states. Alevel I trauma center provides comprehensive trauma care(immediate availability of specialized surgeons, anesthesiol-ogists, and other clinical staff, as well as all necessaryresuscitation equipment), with a minimum number of majortrauma patients per year; serves as a regional resource; andprovides leadership in education, research, and system plan-ning. Analogously, we propose to define levels of CICUs asfollows.
Level 1 CICUThe level 1 CICU is capable of management of all cardio-vascular conditions and major noncardiovascular comorbidconditions. This unit may contain advanced heart failurepatients dependent on percutaneous ventricular assist devicesand in some circumstances patients who have undergonesurgical ventricular assist device placement or cardiac trans-plantation. The level 1 CICU has all forms of invasive andnoninvasive monitoring capabilities, and advanced technolo-gies will be available to support the cardiovascular systemand manage patients with refractory shock or resuscitatedcardiac arrest. Patient care in this setting would be of highintensity, with management by full-time intensivists, eithercardiac intensivists or general intensivists working collabora-tively with cardiologists. The level 1 CICU is designed tocare for patients with primary cardiovascular problems orthose in whom underlying cardiac disease is sufficientlysevere that it presents imminent risk in the context of anothermedical illness. Therefore, a primary role of cardiovascularspecialists is optimal. Physicians with specialized skills incritical care are available at all times and may be on-sitecontinuously. An on-site nursing director is present, andnurse-to-patient ratios would be expected to be 1:1 or 1:2.Pharmacy, nutrition, and respiratory therapy services wouldcomplete the multidisciplinary CICU team. Access to inter-ventional cardiology and cardiac surgical support is expected.In a level 1 CICU, resident and/or fellow training programswould usually be present, and there would typically be acommitment to perform clinical and translational research.Physician leadership ideally would be provided by a cardiacintensivist or codirectorship with a cardiologist and generalintensivist. A level 1 CICU would be the likely paradigm formost large tertiary medical centers.
Level 2 CICUThe level 2 CICU is capable of providing the initial evalua-tion and management of most acute cardiovascular conditionsand medical comorbid conditions. All invasive and noninva-sive monitoring is available. Mechanical hemodynamic sup-port is available but limited to non–ventricular assist devices,including intra-aortic balloon counterpulsation. Advancedmedical interventions such as continuous venovenous hemo-filtration may not be available. A level 2 CICU should haveprotocols in place to provide for initiation of therapeutichypothermia in survivors of cardiac arrest. Physician staffingfor CICU patients is generally by cardiologists, and intensiv-ists are available for consultation or comanagement of com-plex patients. The unit may be combined with a generalmedical or surgical ICU. A nursing director is designated, andnurse-to-patient ratios are usually 1:1 to 1:3. Training of
10 Circulation September 11, 2012
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

residents and clinical research may be present. Transfer to alevel 1 CICU should be considered for patients requiringadvanced hemodynamic support; for patients under consider-ation for high-risk valvular, coronary, or heart failure surgery;and for patients with intractable arrhythmias or refractorymultiorgan system dysfunction.
Level 3 CICUThe level 3 CICU is the lowest-level CICU. The level 3 CICUshould have the capacity to manage respiratory failure,administer vasopressors and inotropes for hypotension, andprovide immediate resuscitation of cardiac arrest but may befocused on the care of patients with suspected acute coronarysyndrome, heart failure without shock, and hemodynamically
stable arrhythmias. The latter group of patients, for example,those with suspected acute coronary syndrome or stablearrhythmias, may be cared for on cardiac step-down telemetryunits in hospitals with level 1 or level 2 CICUs. Like the level2 CICU, the level 3 CICU may be combined with a generalmedical ICU. Noninvasive monitoring and echocardiographyare available. Invasive monitoring and mechanical hemody-namic support are not usually provided in this unit. Cardiol-ogy service admission or consultation is expected for man-agement of patients admitted with primary cardiac conditionsto this unit. Critical care primary or consultative services areavailable. Nurse-to-patient ratios are usually 1:2 to 1:3.Patients who develop the need for mechanical hemodynamicsupport or advanced medical interventions not available in
Table 1. Levels of Cardiovascular ICUs
Level Patient PopulationMonitoringTechnology Therapeutic Technology Physician Leadership
Physician PatientManagement
Nursing/OtherPersonnel
EducationPrograms Research
1 All CV diagnoses All invasive andnoninvasive
cardiacmonitoring
IABP Cardiac intensivist orcardiologist
(nonintensivist) andgeneral intensivist
High-intensity management:All care directed by
intensivist (cardiac orgeneral), or intensivist
consultation
NursingDirector
Usually residentand fellow
training programs
Commitment toperform clinical
research
Most comorbidities PA catheter Percutaneous orimplantable VADs
Intensivist available at alltimes
RN-to-patientratio 1:1 or
1:2
Advanced heartfailure
Echocardiography Mechanical ventilation May be 24/7 in-hospitalintensivist
STEMI primary PCIcapable
Therapeutichypothermia
May includepost-CV surgery
Continuous renalreplacement
Interventional cardiologyavailable 24/7
Cardiac surgery readilyaccessible
2 Initial diagnosis andmanagement of
most CV conditions
All invasive andnoninvasive
cardiacmonitoring
IABP and/or othernon-VAD devices
Cardiologist orintensivist
Intensivist (cardiac orgeneral) available at all
times
NursingDirector
May be residentsor fellow training
programs
May conductresearch
May be STEMIprimary PCI capable
PA catheter Mechanical ventilation RN-to-patientratios 1:1 to
1:3
Transfer to level 1ICU if patient
remains unstable
Echocardiography Therapeutichypothermia initiation
Coronaryangiography
available on-siteor via transfer
Interventional cardiologyaccess preferable
Cardiac surgery accesspreferable
3 Initial diagnosis andmanagement of
commoncardiovascular
conditions (usuallylow complexity),
respiratory failure
Noninvasive andsome invasivemonitoring (eg,arterial lines)
Mechanical ventilation Cardiologist orintensivist
Cardiology admission orconsultation; intensivist is
available at all times
NursingDirector
Transfer to level 1or 2 ICU if unstable
Echocardiography RN-to-patientratio 1:2 to
1:3
Other cardiovascular care units that are not cardiac ICUs include chest pain units for low-risk patients with chest symptoms and intermediate-care step-down units.Specialized units for advanced heart failure are described in the text.
ICU indicates intensive care unit; CV, cardiovascular; IABP, intra-aortic balloon pump; PA, pulmonary artery; VAD, ventricular assist device; RN, registered nurse;24/7, 24 hours per day, 7 days per week; STEMI, ST-segment–elevation myocardial infarction; and PCI, percutaneous coronary intervention.
Morrow et al The Evolution of Critical Care Cardiology 11
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

the level 3 CICU should be transferred promptly to anappropriate center with a level 1 or 2 CICU. Selection of theappropriate timing and destination of transfer for the patientwith refractory illness is an important aspect of overallmanagement in the level 3 CICU.161,162
The writing group acknowledges the frequent presence ofother specialized cardiovascular care units that are not ICUs.For example, chest pain units or clinical decision units havebeen developed in many health systems to facilitate rapiddiagnosis and triage of patients with possible acute ischemicheart disease and may identify patients who warrant transferto a CICU.
The CICU: Models in Other CountriesOther regions of the world have already made formal recom-mendations for staffing of CICUs. The European Society ofCardiology (ESC) Working Group for Acute Cardiac Carehas recommended that intensive cardiac care units (ICCUs)be directed by board-certified cardiologists specially trainedand accredited as acute cardiac care specialists, includingtraining in the general intensive care unit.163 The ESCworking group recommended that intensive cardiac care unitshave 24/7 coverage by physicians skilled in acute cardiaccare, with attending cardiologists available for consultationand assistance. The ESC panel concluded that ICU nurses areas important as ICU physicians for optimal patient care in anintensive cardiac care unit. The ESC panel advocates the ICUteam concept to include physicians, nurses, respiratory ther-apists, pharmacists, social workers, dieticians, physical ther-apists, and other ancillary staff.163
Training Programs in CardiovascularMedicine and Critical Care
A roadmap to keep pace with evolution of the contemporaryCICU must include enhanced training to ensure developmentof the basic skills necessary to provide care in this setting, aswell as opportunities for advanced training in critical carecardiology for those who intend to specialize as a cardiacintensivist.
General Cardiovascular TrainingCardiovascular fellowship training offers comprehensive,hands-on education in a variety of aspects of cardiovascularpatient care. Fellowship education is composed of bedside,didactic, simulation, and other learning opportunities.164 TheACGME training plan is based on the 6 core competencies,which include medical knowledge, patient care, profession-alism, communication and interpersonal skills, practice-basedlearning and improvement, and systems-based practice,which are meant to provide structure and standardization toall programs.165 The American College of Cardiology Foun-dation Recommendations for Training in Adult Cardiovascu-lar Medicine Core Cardiology Training (COCATS) also helpto standardize the fellowship training process by definingtraining levels, in which level 1 indicates the most basictraining level and level 3 indicates the highest traininglevel.166 COCATS is largely based on procedural numbersand time spent in training to assess level of competency.According to COCATS, fellowship training in cardiovascular
medicine should include 9 months in nonlaboratory clinicalpractice, a portion of which is typically spent in the CICU.Present-day critical care training in cardiovascular trainingprograms is varied. All programs expose the trainees tocritically ill patients, but the structure and duration of timespent by cardiology fellows caring for patients in the ICUsetting depends on the structure of the hospital, departments,and training programs. At the present time, there are nospecific ACGME or COCATS guidelines or recommenda-tions for critical care training within cardiovascular fellow-ship training. Although some programs offer fellows dedi-cated fellowship training months in the ICU, with complexpatient populations and experienced staff and physicianteachers, others have modest ICU exposure for fellows.Given the complexity of present-day cardiology patients,fellows are generally exposed to a variety of critically illpatients; however, some fellows may have more limitedexperience with mechanical support, ventilator management,renal replacement therapy, and other advanced therapieslimited to the CICU setting.
There are impediments to the expansion of critical caretraining during general cardiology fellowship. Fellow dutyhours are increasingly scrutinized, and more time in the ICUis likely to further impact training time. In addition, cardiol-ogy training programs need to be cognizant of the expandingneed for exposure to new areas such as advanced cardiacimaging, including magnetic resonance imaging and com-puted tomography imaging. In light of the rapid changes inenvironment and technology that are increasingly unique tothe CICU, trainees in cardiovascular medicine must haveopportunities to participate in the care of critically ill patientswith cardiovascular disease so as to build basic (COCATSlevel 1 or 2) competency in this area. However, given theconstraints imposed by the essential exposure to a broad baseof clinical practice, trainees in general cardiovascular medi-cine are not likely to be able to acquire additional exposure tocritical care medicine in the present training paradigm. Assuch, there is ample rationale for the development of oppor-tunities for advanced training in critical care cardiology (level3 competency).
A Model for Training in Critical Care CardiologyThe progressively increasing severity of illness, the rapidemergence of new technologies, the crucial role of experiencein mitigating the risk of iatrogenic CICU complications, andthe overall complexity of the CICU environment each pointtoward value in developing training pathways for selectedcardiovascular trainees who wish to acquire advanced skillsin critical care medicine and critical care cardiology inparticular. Moreover, the obvious shortfall in intensivistsavailable to meet the needs of staffing models endorsed bythis writing group adds to the rationale for establishingavenues by which to train cardiac intensivists.
Existing Pathway for Dual Certification inCardiovascular and Critical Care MedicineCurrent ACGME recommendations require 3 years of train-ing in cardiovascular disease, of which at least 24 months isfull-time clinical training, to meet the American Board of
12 Circulation September 11, 2012
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

Internal Medicine requirement for certification in cardiovas-cular medicine. For critical care medicine, the ACGMEsuggests a minimum of 12 months of clinical training. TheAmerican Board of Internal Medicine presently recognizes apathway for dual subspecialty training and certification incardiovascular disease and critical care medicine (Table 2).Because of the overlapping elements of the curriculum andclinical experience within these 2 training pathways, 6months of cardiovascular clinical training may be appliedtoward the critical care medicine training requirements.Therefore, overall, this pathway for dual certification requires4 years of fellowship with a minimum of 30 months ofclinical training, of which 6 months of clinical training mustbe in critical care medicine within a critical care trainingprogram accredited by the ACGME. This total period oftraining is commensurate with training in other cardiovascu-lar subspecialties, such as electrophysiology. Functionally,trainees seeking dual certification have typically done sothrough application to an ACGME-accredited 1-year programin critical care medicine before or on completion of theircardiovascular training program.
A summary of the curriculum and current training require-ments for dual board certification in cardiovascular diseaseand critical care medicine is provided in Tables 2 and 3. Thiscurriculum builds on elements already included in the car-diovascular medicine training requirements and expands the
exposure of the trainee to aspects of management of respira-tory failure, acute renal failure, sepsis, and multiorgan systemfailure that are prevalent in the modern CICU. In addition,more broad procedural skills are established, such as perfor-mance of bronchoscopy and placement of chest tubes. Thisenhanced expertise should well equip the cardiac intensivistto manage the broad range of medical problems encounteredin the CICU. However, the writing group also supports thevalue of establishing more innovative pathways for trainingin critical care cardiology that tailor the critical care medicineexperience to develop expertise that the practitioner is likelyto apply in the CICU.
Adaptation and Innovation in Critical CareCardiology TrainingThe writing group recognizes 2 approaches toward develop-ing enhanced training opportunities in critical care cardiology(Table 3). The first adapts and formalizes the existingpathway for dual certification toward providing the medicalknowledge and patient practice experience for a fellow tobecome a cardiac intensivist with the requisite skills neces-sary to work effectively in a CICU. Building on the currentgeneral critical care medicine training requirements for com-bined certification, a tailored program for the cardiac inten-sivist would integrate options for rotations in the cardiacsurgical intensive care unit, emphasize focused experiences
Table 2. Existing Training Requirements for Dual Certification in CVD and Critical Care Medicine
Criterion Details CVD Critical Care
Eligibility criteria Completion of 3 years of accredited CVD fellowship and certification by the ABIM �
Training within a critical care fellowship program in a department of medicine �
Training requirements Completion of 24 mo of full-time clinical training in an accredited fellowship incardiovascular medicine
�
Completion of 12 mo of accredited clinical fellowship training in critical care medicine �
Up to 6 months of critical care medicine experience in CVD and critical care medicinetraining can be applied to admission for both examinations
� �
Minimum total full-time clinical training for dual certification in CVD and critical caremedicine of 30 mo (total training time 48 mo)
� �
Procedural competency Cardioversion; electrocardiography, including ambulatory monitoring and exercisetesting; echocardiography; insertion and management of temporary pacemakers; andleft-sided heart catheterization and diagnostic coronary angiography
�
Advanced cardiac life support (ACLS) � �
Placement of arterial, central venous, and pulmonary artery balloon flotation catheters � �
Calibration and operation of hemodynamic recording systems � �
Airway management and endotracheal intubation �
Ventilator management and noninvasive ventilation �
Insertion and management of chest tubes; thoracentesis �
Proficiency in use of ultrasound to guide central line placement and thoracentesisstrongly recommended
�
Additional areas of knowledgeand practical experience
Indications, contraindications, complications, and limitations of the following procedures:
Intra-aortic balloon pump �
Pericardiocentesis � �
Transvenous pacemaker insertion � �
Continuous renal replacement therapy and hemodialysis � �
Fiber-optic bronchoscopy �
CVD indicates cardiovascular disease; ABIM, American Board of Internal Medicine.
Morrow et al The Evolution of Critical Care Cardiology 13
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

or elective rotations in advanced heart failure and pulmonaryhypertension, and include expanded exposure to complexadult congenital heart disease and percutaneous/surgical cir-culatory assistance devices. Additional research and electivetime would also provide an opportunity to develop specificskills in epidemiology, conduct outcomes research in clinicaltrials, or explore laboratory-based and translational researchin areas of interest relevant to cardiovascular critical care.The training program would be staffed by faculty in cardio-vascular medicine and critical care medicine and requireformative and summative evaluations as required by theACGME. At present, such training is accredited only ifprovided within an ACGME-approved 1-year critical careprogram. In 2011, of the 187 training programs in cardiovas-cular disease, only 31 had associated 1-year programs incritical care medicine at the same institution/program. In thefuture, working collaboratively with faculty from both criticalcare medicine and cardiovascular medicine, the organizationof program leadership in some centers may optimally residewithin the cardiovascular medicine training program, withaccreditation of the integrated program by the ACGME. InEurope, such cardiac intensivist training has already been im-plemented by the European Board for the Specialty of Cardiol-ogy with a formal curriculum and detailed COCATS-typetraining to ensure clinical and procedural competence.167–169
The second approach is substantially farther from existingprogrammatic options, involving the development of a dis-crete, dedicated program for training a cardiac intensivistwith requisite skills to function expertly in the CICU, cardiacsurgical ICU, or other general ICU. In this framework fortraining, a 4-year curriculum drawing from both cardiovas-cular and critical training requirements from the AmericanBoard of Internal Medicine would be formulated and enablean even broader experience in general critical care medicinebut would substitute elective rotations in this domain forsome of the cardiovascular clinical training requirement(Table 3). On the basis of input from certifying authorities,the training would require documentation of clinical experi-ences and procedural competence to certify dual proficiencyin critical care medicine and noninvasive and invasivecardiology.
Recently, a leadership group within the American Board ofThoracic Surgery has discussed the development of a criticalcare certification pathway for the perioperative care ofcardiothoracic surgery patients.170 If such a program were tobe developed, it would provide an additional opportunity fora cardiovascular intensivist to develop skills that would beuseful in the CICU, a cardiothoracic surgical ICU, or acombined unit (“Integration With Other ICUs”). Given thatmost subspecialty ICUs in the United States are located in
Table 3. Proposed Models for Training in Critical Care Cardiology
Current Pathway for DualCertification
Tailored Program for Dual-CertificationCritical Care Cardiology
Possible Dedicated TrainingProgram in Critical Care Cardiology
Clinical, mo
CVD
Noninvasive 7 7 7
Vascular 2 2 2
Catheterization laboratory 4 4 4
Electrophysiology 2 2 2
Nonlaboratory clinical practice* 9 9 (Inclusive of below) 6 (Inclusive of below)
Advanced heart failure … Focused experience Focused experience
Pulmonary hypertension … Focused experience Focused experience
Outpatient continuity clinic 36 36 36
Critical care
MICU or CICU 3 to 6 3 to 6 4 to 6
Nonmedical ICU† 3 to 6 1 to 3 3 to 6
Cardiothoracic surgery ICU … 2 to 3 2 to 3
Research and elective, mo 12 to 18 12 to 18 12 to 18
Total months of training 48 48 48
Program faculty and leadership Separately managed programsin CVD and critical care
medicine
Integrated faculty and collaborative leadershipfrom CV medicine and critical care medicine
Integrated faculty and collaborativeleadership from CV medicine and
critical care medicine
Program accreditation Separate accredited programs:CV medicine
Critical care medicine (1-yprogram)
Accredited programs in CV medicine andcritical care medicine exist within system
Either the critical care medicine or CV medicineprograms may have 1-y accredited program in
critical care cardiology
Integrated program in critical carecardiology with single accreditation
CVD indicates cardiovascular disease; MICU, medical intensive care unit; cardiovascular; CICU, coronary intensive care unit; ICU, intensive care unit; and CV,cardiovascular.
*Ward, consult, CICU.†Nonmedical patients, including surgical intensive care unit, burns, transplant, and neurological ICU or equivalent.
14 Circulation September 11, 2012
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

regional academic centers,79 such a CICU would likely beformed as a collaborative multidisciplinary academic unit thatwould include cardiologists, cardiac intensivists, medical orsurgical intensivists, and anesthesiologists.
Assessing CompetencyDemonstration of proficiency is important for all medicaldisciplines and has been the focus of professional societies,individual medical systems, and independent organizationssuch as the American Board of Internal Medicine that seek tocertify that physicians possess the knowledge, skills, andattitude necessary to provide excellent care. Verification ofinitial training and continued competency is crucial to main-taining conformance to established standards of care and maybe of particular importance for those engaged in the care ofthe most severely ill patients who require critical care. Suchassessment should follow a clearly established program andconsider knowledge, skills, and attitude. The detailed curric-ulum and mechanisms for verification of competency devel-oped by the ESC may serve as a model for similar efforts inthe United States.169 The establishment of opportunities forcontinuing medical education and reassessment of profi-ciency is also important and would be enhanced by expansionof existing programs and development of new programsaimed at critical care cardiology in particular.
At present, mechanisms exist for assessment, certification,and recertification of these elements in both cardiovascularmedicine and critical care medicine through the AmericanBoard of Internal Medicine/American Board of MedicalSpecialties Maintenance of Certification program. Futuredeliberations may consider whether there is a value todeveloping processes for maintenance of certification incritical care cardiology, such as through a certification incardiovascular diseases with “recognition of focused prac-tice,” as is being developed for hospital medicine.171 Thecriteria for such a pathway include (1) that the disciplineincludes large numbers of internists who focus their practicein that discipline and (2) that there is evidence that focusingpractice in the discipline improves patient care and thatrecognition of focused practice would serve an importantsocietal need for the discipline. It is reasonable to argue thatthe latter criterion is already met.
Research Directions for CriticalCare Cardiology
The breadth and volume of cardiovascular research hasoutpaced many other medical specialties over the past de-cades and has made an enormous impact on improving careand outcomes, including among patients cared for in emer-gency and critical care settings. Randomized trials of revas-cularization in cardiogenic shock,172 use of left ventricularassist devices in end-stage heart failure,173 use of pulmonaryartery catheters,174 use of intra-aortic balloon pumps in MI,175
and therapeutic hypothermia for out-of-hospital cardiac ar-rest176 are examples of research restricted to the critical caresetting with patients with primary cardiovascular conditions.However, there has been relatively little research focusing onthe evolution of critical care cardiology to include patientswith multisystem organ dysfunction. There are also important
opportunities to study how staffing models, provider training,team composition, and electronic systems, including decisionsupport, may impact process and outcomes. Moreover, thereis a need for investigation of structured approaches toenhance communication and facilitate transitions between theCICU and external providers inside and outside the hospital.The important research into building regional systems of carefor acute MI with integration of emergency medical systems,community hospitals, and specialized tertiary care centerscould be extended to other critical care conditions. As well,recent work in the treatment of hyperglycemia177 andshock178 and previous randomized studies of the routine useof pulmonary artery catheters179 have highlighted the impor-tance of prospective, well-controlled clinical investigation ingeneral critical care medicine and the impact that it may havein the CICU. End-of-life care and level-of-care decisions bypatients and families are other areas that have undergonesome study180 but need more investigation.
As electronic medical records and evolving coding ofpatient conditions allow more sophisticated analysis of vari-ous aspects of care and outcomes, there will be new oppor-tunities to characterize critically ill cardiovascular patients.This will only be possible with standardized definitions andaccurate coding, as well as multicenter collaboration. Re-search networks in general critical care medicine, such as theCanadian Clinical Trials Group, the ARDS (Acute Respira-tory Distress Syndrome) Network, and the US Critical Illnessand Injury Trials Group, have served to advance the agendaof research in critical care. These models, combined with therich history and expertise of cardiovascular researchers inconducting large clinical trials, could be used to buildimportant evidence to improve care for this understudiedpopulation. With an increasing proportion of healthcaredollars going into care during the last months of life, much ofthis in intensive care units, research into efficient use ofresources is also warranted.
SummaryNo longer is the cardiac ICU merely a “coronary” observationunit for peri-infarction complications. Rather, the contempo-rary CICU is an ICU for complex patients with cardiovascu-lar disease who become critically ill and who are more proneto major systemic complications, including renal failure,respiratory failure, thrombosis, bleeding, catheter-related in-fections, ventilator-acquired pneumonia, and multiorgan dys-function.24,26,29,30 Coincident with significant increases innoncardiovascular critical illnesses, the use of advancedsupportive technologies, both cardiovascular and noncardio-vascular, has increased and requires specialized expertise thatis not in the realm of common experience for the generalclinical cardiologist.24 Together, these changes mark a steadyevolution toward progressively greater complexity of theenvironment in the CICU.
In the opinion of this writing group, this transformationnecessitates innovative approaches to the staffing, structure,and training behind the contemporary CICU. In particular, wehave proposed evidence-based staffing models that are adapt-able to the variety of clinical settings in which cardiovascularcare is provided and adhere to the tenet that the availability of
Morrow et al The Evolution of Critical Care Cardiology 15
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

experienced cardiac intensivists, either as primary caregiversor as consultants, is central to the optimal delivery ofadvanced cardiac critical care. Such specialized skills mayhave been acquired through experience or formal advancedtraining. The writing group also reaffirms the value ofprimary responsibility for management of patients whosedominant medical problem is cardiovascular residing with aclinician with advanced skills in cardiovascular disease. Wehave described a classification system that could be formal-ized to characterize the capabilities and resources of theindividual CICU or health system, with the 2 highest levels(level 1 and level 2) requiring the availability of intensivistsand specialized multidisciplinary teams. In particular, thewriting group concluded that the evidence supports a closed
structure staffed by dedicated cardiac intensivists as a preferredapproach for the level 1 CICU. The writing group also finds thatsuccessful implementation of such models will require thedevelopment of new pathways for training of cardiologists withadvanced skills in critical care cardiology. We have proposedadaptations to existing training models that tailor them towarddeveloping the skills of a cardiac intensivist, and we have raisedthe possibility of more substantial restructuring of training in thefuture. These proposals may be a useful starting point for ameaningful dialogue between the major stakeholders in trainingand certification of such specialists. The future of cardiovascularcritical care medicine is rapidly evolving, with an opportunity toimprove the education and skills of clinicians and the care oftheir patients.
Disclosures
Writing Group Disclosures
Writing Group Member Employment Research GrantOther Research
SupportSpeakers’
Bureau/HonorariaExpert
WitnessOwnership
InterestConsultant/
Advisory Board Other
David A. Morrow Brigham & Women’sHospital/HarvardMedical School
None None None None None None None
James C. Fang University HospitalsCase Medical Center
None None None None None None None
Dan J. Fintel NorthwesternMemorial Faculty
Foundation
None None None None None None None
Christopher B. Granger Duke UniversityMedical Center
Astellas†; AstraZeneca†;Boehringer Ingelheim†;
Bristol-Myers Squibb†; CSK†;GlaxoSmithKline†; Medtronic
Foundation†; Merck†; Pfizer†;Sanofi-Aventis†; The
Medicines Co†
None None None None AstraZeneca*; BoehringerIngelheim†; Bristol-Myers
Squibb†; GlaxoSmithKline*;Hoffmann-La Roche*;
Novartis*; Pfizer*; Roche*;Sanofi-Aventis†; The
Medicines Co*
None
Jason N. Katz University of NorthCarolina
None None None None None None None
Frederick G. Kushner Heart Clinic ofLouisiana
None None None None None None None
Jeffrey T. Kuvin Tufts Medical Center None None None None None None None
Jose Lopez-Sendon Hospital UniversitarioLa Paz, Madrid, Spain
None None None None None None None
Dorothea McAreavey National Institutes ofHealth
None None None None None None None
Brahmajee K.Nallamothu
University of Michigan NIH* None None None PrescriptionSolutions*
Abbott Vascular* None
Robert Lee Page II University of ColoradoSchool of Pharmacy
and Medicine
None None None None None None None
Joseph E. Parrillo Cooper UniversityHospital
None None None None None None None
Pamela N. Peterson Denver HealthMedical Center
None None None None None None None
Chris Winkelman Case WesternReserve Universityand MetroHealthMedical Center
NIH* None AACVPR* None None None None
This table represents the relationships of writing group members that may be perceived as actual or reasonably perceived conflicts of interest as reported on the DisclosureQuestionnaire, which all members of the writing group are required to complete and submit. A relationship is considered to be “significant” if (1) the person receives $10 000or more during any 12-month period, or 5% or more of the person’s gross income; or (2) the person owns 5% or more of the voting stock or share of the entity, or owns$10 000 or more of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
*Modest.†Significant.
16 Circulation September 11, 2012
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

References1. Angus DC, Kelley MA, Schmitz RJ, White A, Popovich J Jr; Committee
on Manpower for Pulmonary and Critical Care Societies (COMPACCS).Caring for the critically ill patient: current and projected workforcerequirements for care of the critically ill and patients with pulmonarydisease: can we meet the requirements of an aging population? JAMA.2000;284:2762–2770.
2. Halpern NA, Pastores SM. Critical care medicine in the United States2000–2005: an analysis of bed numbers, occupancy rates, payer mix,and costs. Crit Care Med. 2010;38:65–71.
3. Adhikari NK, Fowler RA, Bhagwanjee S, Rubenfeld GD. Critical careand the global burden of critical illness in adults. Lancet. 2010;376:1339–1346.
4. Ewart GW, Marcus L, Gaba MM, Bradner RH, Medina JL, ChandlerEB. The critical care medicine crisis: a call for federal action: a whitepaper from the critical care professional societies. Chest. 2004;125:1518–1521.
5. Hill AD, Fan E, Stewart TE, Sibbald WJ, Nauenberg E, Lawless B,Bennett J, Martin CM. Critical care services in Ontario: a survey-basedassessment of current and future resource needs. Can J Anaesth. 2009;56:291–297.
6. Reynolds HN, Haupt MT, Thill-Baharozian MC, Carlson RW. Impact ofcritical care physician staffing on patients with septic shock in a uni-versity hospital medical intensive care unit. JAMA. 1988;260:3446–3450.
7. Pollack MM, Katz RW, Ruttimann UE, Getson PR. Improving theoutcome and efficiency of intensive care: the impact of an intensivist.Crit Care Med. 1988;16:11–17.
8. Brown JJ, Sullivan G. Effect on ICU mortality of a full-time critical carespecialist. Chest. 1989;96:127–129.
9. Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT,Young TL. Physician staffing patterns and clinical outcomes in criticallyill patients: a systematic review. JAMA. 2002;288:2151–2162.
10. Beck CS, Pritchard WH, Feil HS. Ventricular fibrillation of longduration abolished by electric shock. J Am Med Assoc. 1947;135:985.
11. Zoll PM, Linenthal AJ, Gibson W, Paul MH, Norman LR. Terminationof ventricular fibrillation in man by externally applied electric coun-tershock. N Engl J Med. 1956;254:727–732.
12. Lown B, Amarasingham R, Neuman J. New method for terminatingcardiac arrhythmias: use of synchronized capacitor discharge. JAMA.1962;182:548–555.
13. Julian DG. Treatment of cardiac arrest in acute myocardial ischaemiaand infarction. Lancet. 1961;2:840–844.
14. Julian DG. The history of coronary care units. Br Heart J. 1987;57:497–502.
15. Lown B, Fakhro AM, Hood WB Jr, Thorn GW. The coronary care unit:new perspectives and directions. JAMA. 1967;199:188–198.
16. Fye WB. Resuscitating a Circulation abstract to celebrate the 50thanniversary of the coronary care unit concept. Circulation. 2011;124:1886–1893.
17. Killip T 3rd, Kimball JT. Treatment of myocardial infarction in acoronary care unit: a two year experience with 250 patients. Am JCardiol. 1967;20:457–464.
18. Braunwald E. Evolution of the management of acute myocardial infarc-tion: a 20th century saga. Lancet. 1998;352:1771–1774.
19. Lee TH, Goldman L. The coronary care unit turns 25: historical trendsand future directions. Ann Intern Med. 1988;108:887–894.
20. Forrester JS, Diamond G, Chatterjee K, Swan HJ. Medical therapy ofacute myocardial infarction by application of hemodynamic subsets(first of two parts). N Engl J Med. 1976;295:1356–1362.
21. Stern MP. The recent decline in ischemic heart disease mortality. AnnIntern Med. 1979;91:630–640.
22. Goldman L, Cook EF. The decline in ischemic heart disease mortalityrates: an analysis of the comparative effects of medical interventions andchanges in lifestyle. Ann Intern Med. 1984;101:825–836.
23. Rotstein Z, Mandelzweig L, Lavi B, Eldar M, Gottlieb S, Hod H. Doesthe coronary care unit improve prognosis of patients with acute myo-cardial infarction? A thrombolytic era study. Eur Heart J. 1999;20:813–818.
24. Katz JN, Shah BR, Volz EM, Horton JR, Shaw LK, Newby LK, GrangerCB, Mark DB, Califf RM, Becker RC. Evolution of the coronary careunit: clinical characteristics and temporal trends in healthcare deliveryand outcomes. Crit Care Med. 2010;38:375–381.
25. Quinn T, Weston C, Birkhead J, Walker L, Norris R; MINAP SteeringGroup. Redefining the coronary care unit: an observational study ofpatients admitted to hospital in England and Wales in 2003. QJM.2005;98:797–802.
26. Katz JN, Turer AT, Becker RC. Cardiology and the critical care crisis:a perspective. J Am Coll Cardiol. 2007;49:1279–1282.
27. Groeger JS, Guntupalli KK, Strosberg M, Halpern N, Raphaely RC,Cerra F, Kaye W. Descriptive analysis of critical care units in the UnitedStates: patient characteristics and intensive care unit utilization. CritCare Med. 1993;21:279–291.
28. Teskey RJ, Calvin JE, McPhail I. Disease severity in the coronary careunit. Chest. 1991;100:1637–1642.
29. Valente S, Lazzeri C, Sori A, Giglioli C, Bernardo P, Gensini GF. Therecent evolution of coronary care units into intensive cardiac care units:the experience of a tertiary center in Florence. J Cardiovasc Med.2007;8:181–187.
30. Casella G, Cassin M, Chiarella F, Chinaglia A, Conte MR, Fradella G,Lucci D, Maggioni AP, Pirelli S, Scorcu G, Visconti LO; BLITZ-3Investigators. Epidemiology and patterns of care of patients admitted toItalian Intensive Cardiac Care units: the BLITZ-3 registry. J CardiovascMed (Hagerstown). 2010;11:450–461.
31. Dixon SR, Henriques JPS, Mauri L, Sjauw K, Civitello A, Kar B,Loyalka P, Resnic FS, Teirstein P, Makkar R, Palacios IF, Collins M,Moses J, Benali K, O’Neill WW. A prospective feasibility trial inves-tigating the use of the Impella 2.5 system in patients undergoinghigh-risk percutaneous coronary intervention (the PROTECT I Trial):initial U.S. experience. JACC Cardiovasc Interv. 2009;2:91–96.
32. Miller MA, Dukkipati SR, Mittnacht AJ, Chinitz JS, Belliveau L, KoruthJS, Gomes JA, d’Avila A, Reddy VY. Activation and entrainmentmapping of hemodynamically unstable ventricular tachycardia using apercutaneous left ventricular assist device. J Am Coll Cardiol. 2011;58:1363–1371.
33. The Hypothermia After Cardiac Arrest Study Group. Mild therapeutichypothermia to improve the neurologic outcome after cardiac arrest
Reviewer Disclosures
Reviewer EmploymentResearch
GrantOther Research
SupportSpeakers’
Bureau/ Honoraria Expert WitnessOwnership
InterestConsultant/
Advisory Board Other
Gerasimos Fillipatos Evangelismos Hospital, Athens, Greece None None None None None None None
Mike Kontos Virginia Commonwealth University/Medical College of Virginia
NIH* None AstraZeneca* Plaintiff, postoperative MI* None AstraZeneca* None
Steve Pastores Memorial Sloan-Kettering CancerCenter
None None None None None None None
Ileana L. Piña Case Western Reserve University None None None None None None None
Cathy Ryan University of Illinois at Chicago None None None None None None None
C.A. Sivaram University of Oklahoma None None Medtronic* None None Medtronic* None
This table represents the relationships of reviewers that may be perceived as actual or reasonably perceived conflicts of interest as reported on the DisclosureQuestionnaire, which all reviewers are required to complete and submit. A relationship is considered to be “significant” if (1) the person receives $10 000 or moreduring any 12-month period, or 5% or more of the person’s gross income; or (2) the person owns 5% or more of the voting stock or share of the entity, or owns$10 000 or more of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
*Modest.
Morrow et al The Evolution of Critical Care Cardiology 17
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

[published correction appears in N Engl J Med. 2002;346:1756]. N EnglJ Med. 2002;346:549–556.
34. Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G,Smith K. Treatment of comatose survivors of out-of-hospital cardiacarrest with induced hypothermia. N Engl J Med. 2002;346:557–563.
35. Lurie K, Davis S, Olsen J, Oakes D, Holm SO, Gillquist D, Lick C,Yannopoulos D, Gold B. Awakening after cardiac arrest and post-resuscitation hypothermia: are we pulling the plug too early? Circu-lation. 2010;122:A47. Abstract.
36. Neumar RW, Barnhart JM, Berg RA, Chan PS, Geocadin RG, LuepkerRV, Newby LK, Sayre MR, Nichol G; on behalf of the American HeartAssociation Emergency Cardiovascular Care Committee, Council onCardiopulmonary, Critical Care, Perioperative, and Resuscitation,Council on Clinical Cardiology, Council on Epidemiology and Pre-vention, Council on Quality of Care and Outcomes Research, andAdvocacy Coordinating Committee. Implementation strategies forimproving survival after out-of-hospital cardiac arrest in the UnitedStates: consensus recommendations from the 2009 American HeartAssociation Cardiac Arrest Survival Summit. Circulation. 2011;123:2898–2910.
37. Montagnini M, Smith H, Balistrieri T. Assessment of self-perceivedend-of-life care competencies of intensive care unit providers. J PalliatMed. 2012;15:29–36.
38. Molter NC. Needs of relatives of critically ill patients: a descriptivestudy. Heart Lung. 1979;8:332–339.
39. Hickey M. What are the needs of families of critically ill patients? Areview of the literature since 1976. Heart Lung. 1990;19:401–415.
40. Levin TT, Moreno B, Silvester W, Kissane DW. End-of-life communi-cation in the intensive care unit. Gen Hosp Psychiatry. 2010;32:433–442.
41. Ahrens T, Yancey V, Kollef M. Improving family communications atthe end of life: implications for length of stay in the intensive care unitand resource use. Am J Crit Care. 2003;12:317–323.
42. Lerolle N, Trinquart L, Bornstain C, Tadie JM, Imbert A, Diehl JL,Fagon JY, Guerot E. Increased intensity of treatment and decreasedmortality in elderly patients in an intensive care unit over a decade. CritCare Med. 2010;38:59–64.
43. Clancy CM. The intensive care unit, patient safety, and the Agency forHealthcare Research and Quality. Am J Med Qual. 2006;21:348–351.
44. Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsisin the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–1554.
45. Friedman G, Silva E, Vincent JL. Has the mortality of septic shockchanged with time. Crit Care Med. 1998;26:2078–2086.
46. Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J,Pinsky MR. Epidemiology of severe sepsis in the United States: analysisof incidence, outcome, and associated costs of care. Crit Care Med.2001;29:1303–1310.
47. Chang R, Todd Greene M, Chenoweth CE, Kuhn L, Shuman E, RogersMA, Saint S. Epidemiology of hospital-acquired urinary tract-relatedbloodstream infection at a university hospital. Infect Control HospEpidemiol. 2011;32:1127–1129.
48. Kollef MH. Prevention of ventilator-associated pneumonia or ventilator-associated complications: a worthy, yet challenging, goal. Crit CareMed. 2012;40:271–277.
49. O’Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, HeardSO, Lipsett PA, Masur H, Mermel LA, Pearson ML, Raad II, RandolphAG, Rupp ME, Saint S; Healthcare Infection Control Practices AdvisoryCommittee (HICPAC). Summary of recommendations: guidelines forthe prevention of intravascular catheter-related infections. Clin InfectDis. 2011;52:1087–1099.
50. Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, CosgroveS, Sexton B, Hyzy R, Welsh R, Roth G, Bander J, Kepros J, GoeschelC. An intervention to decrease catheter-related bloodstream infections inthe ICU [published correction appears in N Engl J Med. 2007;356:2660].N Engl J Med. 2006;355:2725–2732.
51. Corwin HL, Gettinger A, Pearl RG, Fink MP, Levy MM, Abraham E,MacIntyre NR, Shabot MM, Duh MS, Shapiro MJ. The CRIT Study:anemia and blood transfusion in the critically ill: current clinical practicein the United States. Crit Care Med. 2004;32:39–52.
52. Carson JL, Grossman BJ, Kleinman S, Tinmouth AT, Marques MB,Fung MK, Holcomb JB, Illoh O, Kaplan LJ, Katz LM, Rao SV, RobackJD, Shander A, Tobian AA, Weinstein R, Swinton McLaughlin LG,Djulbegovic B. Red blood cell transfusion: a clinical practice guidelinefrom the AABB. Ann Intern Med. 2012:E-429.
53. Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption ofsedative infusions in critically ill patients undergoing mechanical ven-tilation. N Engl J Med. 2000;342:1471–1477.
54. Brochard L. Mechanical ventilation: invasive versus noninvasive. EurRespir J Suppl. 2003;47:31s–37s.
55. Labovitz AJ, Noble VE, Bierig M, Goldstein SA, Jones R, Kort S, PorterTR, Spencer KT, Tayal VS, Wei K. Focused cardiac ultrasound in theemergent setting: a consensus statement of the American Society ofEchocardiography and American College of Emergency Physicians.J Am Soc Echocardiogr. 2010;23:1225–1230.
56. Blaivas M, Kirkpatrick A, Sustic A. Future directions and conclusions.Crit Care Med. 2007;35(suppl):S305–S307.
57. Konings MK, Grundeman PF, Goovaerts HG, Roosendaal MR, HoeferIE, Doevendans PA, Rademakers FE, Buhre WF. In-vivo validation ofa new non-invasive continuous ventricular stroke volume monitoringsystem in an animal model. Crit Care. 2011;15:R165.
58. Critchley LA, Lee A, Ho AM. A critical review of the ability ofcontinuous cardiac output monitors to measure trends in cardiac output.Anesth Analg. 2010;111:1180–1192.
59. Carson SS, Stocking C, Podsadecki T, Christenson J, Pohlman A,MacRae S, Jordan J, Humphrey H, Siegler M, Hall J. Effects of orga-nizational change in the medical intensive care unit of a teachinghospital: a comparison of “open” and “closed” formats. JAMA. 1996;276:322–328.
60. Multz AS, Chalfin DB, Samson IM, Dantzker DR, Fein AM, SteinbergHN, Niederman MS, Scharf SM. A “closed” medical intensive care unit(MICU) improves resource utilization when compared with an “open”MICU. Am J Respir Crit Care Med. 1998;157(pt 1):1468–1473.
61. Ghorra S, Reinert SE, Cioffi W, Buczko G, Simms HH. Analysis of theeffect of conversion from open to closed surgical intensive care unit.Ann Surg. 1999;229:163–171.
62. van der Sluis FJ, Slagt C, Liebman B, Beute J, Mulder JW, Engel AF.The impact of open versus closed format ICU admission practices on theoutcome of high risk surgical patients: a cohort analysis. BMC Surg.2011;11:18.
63. Hackner D, Shufelt CL, Balfe DD, Lewis MI, Elsayegh A, BraunsteinGD, Mosenifar Z. Do faculty intensivists have better outcomes whencaring for patients directly in a closed ICU versus consulting in an openICU? Hosp Pract (Minneap). 2009;37:40–50.
64. Pronovost PJ, Holzmueller CG, Clattenburg L, Berenholtz S, MartinezEA, Paz JR, Needham DM. Team care: beyond open and closedintensive care units. Curr Opin Crit Care. 2006;12:604–608.
65. Dimick JB, Pronovost PJ, Heitmiller RF, Lipsett PA. Intensive care unitphysician staffing is associated with decreased length of stay, hospitalcost, and complications after esophageal resection. Crit Care Med.2001;29:753–758.
66. Hanson CW 3rd, Deutschman CS, Anderson HL 3rd, Reilly PM, Beh-ringer EC, Schwab CW, Price J. Effects of an organized critical careservice on outcomes and resource utilization: a cohort study. Crit CareMed. 1999;27:270–274.
67. Li TC, Phillips MC, Shaw L, Cook EF, Natanson C, Goldman L. On-sitephysician staffing in a community hospital intensive care unit: impact ontest and procedure use and on patient outcome. JAMA. 1984;252:2023–2027.
68. Manthous CA, Amoateng-Adjepong Y, al-Kharrat T, Jacob B,Alnuaimat HM, Chatila W, Hall JB. Effects of a medical intensivist onpatient care in a community teaching hospital. Mayo Clin Proc. 1997;72:391–399.
69. Levy MM, Rapoport J, Lemeshow S, Chalfin DB, Phillips G, Danis M.Association between critical care physician management and patientmortality in the intensive care unit. Ann Intern Med. 2008;148:801–809.
70. Rubenfeld GD, Angus DC. Are intensivists safe? Ann Intern Med.2008;148:877–879.
71. Kahn JM, Hall JB. More doctors to the rescue in the intensive care unit:a cautionary note. Am J Respir Crit Care Med. 2010;181:1160–1161.
72. Tarnow-Mordi WO, Hau C, Warden A, Shearer AJ. Hospital mortalityin relation to staff workload: a 4-year study in an adult intensive-careunit. Lancet. 2000;356:185–189.
73. Lyon SM, Benson NM, Cooke CR, Iwashyna TJ, Ratcliffe SJ, Kahn JM.The effect of insurance status on mortality and procedural use in crit-ically ill patients. Am J Respir Crit Care Med. 2011;184:809–815.
74. Fuchs RJ, Berenholtz SM, Dorman T. Do intensivists in ICU improveoutcome? Best Pract Res Clin Anaesthesiol. 2005;19:125–135.
18 Circulation September 11, 2012
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

75. Kahn JM, Brake H, Steinberg KP. Intensivist physician staffing and theprocess of care in academic medical centres. Qual Saf Health Care.2007;16:329–333.
76. Kirkland LL, Parham WM, Pastores SM. Approaching hospital admin-istration about adopting cooling technologies. Crit Care Med. 2009;37(suppl):S290–S294.
77. Weiss CH, Moazed F, McEvoy CA, Singer BD, Szleifer I, Amaral LA,Kwasny M, Watts CM, Persell SD, Baker DW, Sznajder JI, WunderinkRG. Prompting physicians to address a daily checklist and process ofcare and clinical outcomes: a single-site study. Am J Respir Crit CareMed. 2011;184:680–686.
78. Higgins TL, McGee WT, Steingrub JS, Rapoport J, Lemeshow S, TeresD. Early indicators of prolonged intensive care unit stay: impact ofillness severity, physician staffing, and pre-intensive care unit length ofstay. Crit Care Med. 2003;31:45–51.
79. Angus DC, Shorr AF, White A, Dremsizov TT, Schmitz RJ, Kelley MA;Committee on Manpower for Pulmonary and Critical Care Societies(COMPACCS). Critical care delivery in the United States: distributionof services and compliance with Leapfrog recommendations. Crit CareMed. 2006;34:1016–1024.
80. Luyt CE, Combes A, Aegerter P, Guidet B, Trouillet JL, Gibert C,Chastre J. Mortality among patients admitted to intensive care unitsduring weekday day shifts compared with “off” hours. Crit Care Med.2007;35:3–11.
81. Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, SuppesR, Feinstein D, Zanotti S, Taiberg L, Gurka D, Kumar A, Cheang M.Duration of hypotension before initiation of effective antimicrobialtherapy is the critical determinant of survival in human septic shock. CritCare Med. 2006;34:1589–1596.
82. Meynaar IA, van der Spoel JI, Rommes JH, van Spreuwel-Verheijen M,Bosman RJ, Spronk PE. Off hour admission to an intensivist-led ICU isnot associated with increased mortality. Crit Care. 2009;13:R84.
83. Bell CM, Redelmeier DA. Mortality among patients admitted to hos-pitals on weekends as compared with weekdays. N Engl J Med. 2001;345:663–668.
84. Cavallazzi R, Marik PE, Hirani A, Pachinburavan M, Vasu TS, LeibyBE. Association between time of admission to the ICU and mortality: asystematic review and metaanalysis. Chest. 2010;138:68–75.
85. Cram P, Hillis SL, Barnett M, Rosenthal GE. Effects of weekendadmission and hospital teaching status on in-hospital mortality. Am JMed. 2004;117:151–157.
86. Ensminger SA, Morales IJ, Peters SG, Keegan MT, Finkielman JD,Lymp JF, Afessa B. The hospital mortality of patients admitted to theICU on weekends. Chest. 2004;126:1292–1298.
87. Uusaro A, Kari A, Ruokonen E. The effects of ICU admission anddischarge times on mortality in Finland. Intensive Care Med. 2003;29:2144–2148.
88. Blunt MC, Burchett KR. Out-of-hours consultant cover and case-mix-adjusted mortality in intensive care. Lancet. 2000;356:735–736.
89. Goh AY, Lum LC, Abdel-Latif ME. Impact of 24 hour critical carephysician staffing on case-mix adjusted mortality in paediatric intensivecare. Lancet. 2001;357:445–446.
90. Netzer G, Liu X, Shanholtz C, Harris A, Verceles A, Iwashyna TJ.Decreased mortality resulting from a multicomponent intervention in atertiary care medical intensive care unit. Crit Care Med. 2011;39:284–293.
91. Gajic O, Afessa B, Hanson AC, Krpata T, Yilmaz M, Mohamed SF,Rabatin JT, Evenson LK, Aksamit TR, Peters SG, Hubmayr RD, WylamME. Effect of 24-hour mandatory versus on-demand critical care spe-cialist presence on quality of care and family and provider satisfaction inthe intensive care unit of a teaching hospital. Crit Care Med. 2008;36:36–44.
92. Kumar K, Zarychanski R, Bell DD, Manji R, Zivot J, Menkis AH, AroraRC; Cardiovascular Health Research in Manitoba Investigator Group.Impact of 24-hour in-house intensivists on a dedicated cardiac surgeryintensive care unit. Ann Thorac Surg. 2009;88:1153–1161.
93. Banerjee R, Naessens JM, Seferian EG, Gajic O, Moriarty JP, JohnsonMG, Meltzer DO. Economic implications of nighttime attending inten-sivist coverage in a medical intensive care unit. Crit Care Med. 2011;39:1257–1262.
94. Pollack MM, Cuerdon TT, Patel KM, Ruttimann UE, Getson PR,Levetown M. Impact of quality-of-care factors on pediatric intensivecare unit mortality. JAMA. 1994;272:941–946.
95. Burnham EL, Moss M, Geraci MW. The case for 24/7 in-house inten-sivist coverage. Am J Respir Crit Care Med. 2010;181:1159–1160.
96. Embriaco N, Azoulay E, Barrau K, Kentish N, Pochard F, Loundou A,Papazian L. High level of burnout in intensivists: prevalence and asso-ciated factors [published correction appears in Am J Respir Crit CareMed. 2007;175:1209–1210]. Am J Respir Crit Care Med. 2007;175:686–692.
97. Sapirstein A, Lone N, Latif A, Fackler J, Pronovost PJ. Tele ICU:paradox or panacea? Best Pract Res Clin Anaesthesiol. 2009;23:115–126.
98. Breslow MJ, Rosenfeld BA, Doerfler M, Burke G, Yates G, Stone DJ,Tomaszewicz P, Hochman R, Plocher DW. Effect of a multiple-siteintensive care unit telemedicine program on clinical and economicoutcomes: an alternative paradigm for intensivist staffing [publishedcorrection appears in Crit Care Med. 2004;32:1632]. Crit Care Med.2004;32:31–38.
99. Groves RH Jr, Holcomb BW Jr, Smith ML. Intensive care telemedicine:evaluating a model for proactive remote monitoring and intervention inthe critical care setting. Stud Health Technol Inform. 2008;131:131–146.
100. Rosenfeld BA, Dorman T, Breslow MJ, Pronovost P, Jenckes M, ZhangN, Anderson G, Rubin H. Intensive care unit telemedicine: alternateparadigm for providing continuous intensivist care. Crit Care Med.2000;28:3925–3931.
101. Lilly CM, Thomas EJ. Tele-ICU: experience to date. J Intensive CareMed. 2010;25:16–22.
102. McCambridge M, Jones K, Paxton H, Baker K, Sussman EJ, EtchasonJ. Association of health information technology and teleintensivistcoverage with decreased mortality and ventilator use in critically illpatients. Arch Intern Med. 2010;170:648–653.
103. Lilly CM, Cody S, Zhao H, Landry K, Baker SP, McIlwaine J, ChandlerMW, Irwin RS; University of Massachusetts Memorial Critical CareOperations Group. Hospital mortality, length of stay, and preventablecomplications among critically ill patients before and after tele-ICUreengineering of critical care processes. JAMA. 2011;305:2175–2183.
104. Morrison JL, Cai Q, Davis N, Yan Y, Berbaum ML, Ries M, SolomonG. Clinical and economic outcomes of the electronic intensive care unit:results from two community hospitals. Crit Care Med. 2010;38:2–8.
105. Thomas EJ, Lucke JF, Wueste L, Weavind L, Patel B. Association oftelemedicine for remote monitoring of intensive care patients with mor-tality, complications, and length of stay. JAMA. 2009;302:2671–2678.
106. Young LB, Chan PS, Lu X, Nallamothu BK, Sasson C, Cram PM.Impact of telemedicine intensive care unit coverage on patient out-comes: a systematic review and meta-analysis. Arch Intern Med. 2011;171:498–506.
107. Dorman T. Telecardiology and the intensive care unit. Crit Care Clin.2001;17:293–301.
108. Fine SH, Loheide L, Swanson-Kazely A, Clarke RL, Simpson K.Assessing the benefits of teleintensivist coverage in the ICU. HealthcFinanc Manage. 2010;64:84–88.
109. Stafford TB, Myers MA, Young A, Foster JG, Huber JT. Working in aneICU unit: life in the box. Crit Care Nurs Clin North Am. 2008;20:441–450.
110. Hyzy RC, Flanders SA, Pronovost PJ, Berenholtz SM, Watson S,George C, Goeschel CA, Maselli J, Auerbach AD. Characteristics ofintensive care units in Michigan: not an open and closed case. J HospMed. 2010;5:4–9.
111. Krell K. Critical care workforce. Crit Care Med. 2008;36:1350–1353.112. Parshuram CS, Kirpalani H, Mehta S, Granton J, Cook D; for the
Canadian Critical Care Trials Group. In-house, overnight physicianstaffing: a cross-sectional survey of Canadian adult and pediatricintensive care units. Crit Care Med. 2006;34:1674–1678.
113. Huang DT, Osborn TM, Gunnerson KJ, Gunn SR, Trzeciak S, KimballE, Fink MP, Angus DC, Dellinger RP, Rivers EP; Society of CriticalCare Medicine; American College of Emergency Physicians; Society ofAcademic Emergency Medicine; Council of Emergency Medicine Res-idency Directors; Emergency Medicine Residents Association. Criticalcare medicine training and certification for emergency physicians. CritCare Med. 2005;33:2104–2109.
114. Nguyen YL, Kahn JM, Angus DC. Reorganizing adult critical caredelivery: the role of regionalization, telemedicine, and communityoutreach. Am J Respir Crit Care Med. 2010;181:1164–1169.
115. Pastores SM, O’Connor MF, Kleinpell RM, Napolitano L, Ward N,Bailey H, Mollenkopf FP Jr, Coopersmith CM. The AccreditationCouncil for Graduate Medical Education resident duty hour new stan-dards: history, changes, and impact on staffing of intensive care units.Crit Care Med. 2011;39:2540–2549.
Morrow et al The Evolution of Critical Care Cardiology 19
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

116. Afessa B. Intensive care unit physician staffing: seven days a week, 24hours a day. Crit Care Med. 2006;34:894–895.
117. Gajic O, Afessa B. Physician staffing models and patient safety in theICU. Chest. 2009;135:1038–1044.
118. Kim MM, Barnato AE, Angus DC, Fleisher LA, Kahn JM. The effect ofmultidisciplinary care teams on intensive care unit mortality [publishedcorrection appears in Arch Intern Med. 2010;170:867]. Arch Intern Med.2010;170:369–376.
119. Leape LL, Cullen DJ, Clapp MD, Burdick E, Demonaco HJ, Erickson JI,Bates DW. Pharmacist participation on physician rounds and adversedrug events in the intensive care unit [published correction appears inJAMA. 2000;283:1293]. JAMA. 1999;282:267–270.
120. MacLaren R, Bond CA, Martin SJ, Fike D. Clinical and economicoutcomes of involving pharmacists in the direct care of critically illpatients with infections. Crit Care Med. 2008;36:3184–3189.
121. Kane SL, Weber RJ, Dasta JF. The impact of critical care pharmacistson enhancing patient outcomes. Intensive Care Med. 2003;29:691–698.
122. Horn E, Jacobi J. The critical care clinical pharmacist: evolution of anessential team member. Crit Care Med. 2006;34(suppl):S46–S51.
123. Zanni JM, Korupolu R, Fan E, Pradhan P, Janjua K, Palmer JB, BrowerRG, Needham DM. Rehabilitation therapy and outcomes in acute respi-ratory failure: an observational pilot project. J Crit Care. 2010;25:254–262.
124. Schweickert WD, Pohlman MC, Pohlman AS, Nigos C, Pawlik AJ,Esbrook CL, Spears L, Miller M, Franczyk M, Deprizio D, Schmidt GA,Bowman A, Barr R, McCallister KE, Hall JB, Kress JP. Early physicaland occupational therapy in mechanically ventilated, critically illpatients: a randomised controlled trial. Lancet. 2009;373:1874–1882.
125. Pohlman MC, Schweickert WD, Pohlman AS, Nigos C, Pawlik AJ,Esbrook CL, Spears L, Miller M, Franczyk M, Deprizio D, Schmidt GA,Bowman A, Barr R, McCallister K, Hall JB, Kress JP. Feasibility ofphysical and occupational therapy beginning from initiation ofmechanical ventilation. Crit Care Med. 2010;38:2089–2094.
126. Nordon-Craft A, Schenkman M, Ridgeway K, Benson A, Moss M.Physical therapy management and patient outcomes following ICU-acquired weakness: a case series. J Neurol Phys Ther. 2011;35:133–140.
127. Hodgin KE, Nordon-Craft A, McFann KK, Mealer ML, Moss M.Physical therapy utilization in intensive care units: results from anational survey. Crit Care Med. 2009;37:561–566.
128. Senduran M, Malkoc M, Oto O. Physical therapy in the intensive careunit in a patient with biventricular assist device. Cardiopulm Phys TherJ. 2011;22:31–34.
129. Needham DM, Korupolu R, Zanni JM, Pradhan P, Colantuoni E, PalmerJB, Brower RG, Fan E. Early physical medicine and rehabilitation forpatients with acute respiratory failure: a quality improvement project.Arch Phys Med Rehabil. 2010;91:536–542.
130. Morris PE, Griffin L, Berry M, Thompson C, Hite RD, Winkelman C,Hopkins RO, Ross A, Dixon L, Leach S, Haponik E. Receiving earlymobility during an intensive care unit admission is a predictor ofimproved outcomes in acute respiratory failure. Am J Med Sci. 2011;341:373–377.
131. Carr DD. Building collaborative partnerships in critical care: the RNcase manager/social work dyad in critical care. Prof Case Manag.2009;14:121–132.
132. Donabedian A. The quality of care: how can it be assessed? JAMA.1988;260:1743–1748.
133. Berenholtz SM, Pronovost PJ. Monitoring patient safety. Crit Care Clin.2007;23:659–673.
134. Breslow MJ, Badawi O. Severity scoring in the critically ill: part 1:interpretation and accuracy of outcome prediction scoring systems.Chest. 2012;141:245–252.
135. Minne L, Abu-Hanna A, de Jonge E. Evaluation of SOFA-based modelsfor predicting mortality in the ICU: a systematic review. Crit Care.2008;12:R161.
136. Terblanche M, Adhikari NK. The evolution of intensive care unit per-formance assessment. J Crit Care. 2006;21:19–22.
137. National Hospital Quality Measures—ICU. October 3, 2010. http://www.jointcommission.org/national_hospital_quality_measures_-_icu/.Accessed April 16, 2012.
138. Higgins TL. Quantifying risk and benchmarking performance in theadult intensive care unit. J Intensive Care Med. 2007;22:141–156.
139. Paragon Critical Care Quality Implementation Program. ParagonCritical Care Quality Implementation Program. http://www.sccm.org/Professional_Development/Quality_Initiatives/Pages/Paragon/aspx.Accessed December 21, 2011.
140. Woodhouse D, Berg M, van der Putten J, Houtepen J. Will bench-marking ICUs improve outcome? Curr Opin Crit Care. 2009;15:450–455.
141. Magill SS, Fridkin SK. Improving surveillance definitions for ventilator-associated pneumonia in an era of public reporting and performancemeasurement. Clin Infect Dis. 2012;54:378–380.
142. Spertus JA, Eagle KA, Krumholz HM, Mitchell KR, Normand SL;American College of Cardiology/American Heart Association TaskForce on Performance Measures. American College of Cardiology andAmerican Heart Association methodology for the selection and creationof performance measures for quantifying the quality of cardiovascularcare. J Am Coll Cardiol. 2005;45:1147–1156.
143. Peterson ED, DeLong ER, Masoudi FA, O’Brien SM, Peterson PN,Rumsfeld JS, Shahian DM, Shaw RE. ACCF/AHA 2010 positionstatement on composite measures for healthcare performance assess-ment: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures(Writing Committee to Develop a Position Statement on CompositeMeasures). Circulation. 2010;121:1780–1791.
144. Bonow RO, Bennett S, Casey DE Jr, Ganiats TG, Hlatky MA, KonstamMA, Lambrew CT, Normand SL, Pina IL, Radford MJ, Smith AL,Stevenson LW, Burke G, Eagle KA, Krumholz HM, Linderbaum J,Masoudi FA, Ritchie JL, Rumsfeld JS, Spertus JA. ACC/AHA clinicalperformance measures for adults with chronic heart failure: a report ofthe American College of Cardiology/American Heart Association TaskForce on Performance Measures (Writing Committee to Develop HeartFailure Clinical Performance Measures). Circulation. 2005;112:1853–1887.
145. Krumholz HM, Anderson JL, Brooks NH, Fesmire FM, Lambrew CT,Landrum MB, Weaver WD, Whyte J, Bonow RO, Bennett SJ, Burke G,Eagle KA, Linderbaum J, Masoudi FA, Normand SL, Pina IL, RadfordMJ, Rumsfeld JS, Ritchie JL, Spertus JA. ACC/AHA clinical per-formance measures for adults with ST-elevation and non–ST-elevationmyocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures(Writing Committee to Develop Performance Measures on ST-Elevationand Non–ST-Elevation Myocardial Infarction). Circulation. 2006;113:732–761.
146. Leapfrog Group. Fact Sheet: ICU physician staffing (IPS). http://www.leapfroggroup.org/media/file/Leapfrog-ICU_Physician_Staffing_Fact_Sheet.pdf. Accessed April 16, 2012.
147. Pronovost PJ, Needham DM, Waters H, Birkmeyer CM, Calinawan JR,Birkmeyer JD, Dorman T. Intensive care unit physician staffing:financial modeling of the Leapfrog standard. Crit Care Med. 2004;32:1247–1253.
148. American Nurses Credentialing Center. Certification: cardiac-vascularnursing. http://www.nursecredentialing.org/NurseSpecialties/CardiacVascular.aspx. Accessed December 1, 2011.
149. American Association of Critical-Care Nurses. Cardiac medicine &cardiac surgery subspecialty certifications. http://www.aacn.org/wd/certifications/content/subspecial.pcms?menu�certification. AccessedDecember 1, 2011.
150. Valente SM. Improving professional practice through certification.J Nurses Staff Dev. 2010;26:215–219.
151. Kendall-Gallagher D, Aiken LH, Sloane DM, Cimiotti JP. Nurse spe-cialty certification, inpatient mortality, and failure to rescue. J NursScholarsh. 2011;43:188–194.
152. Fry M. Literature review of the impact of nurse practitioners in criticalcare services. Nurs Crit Care. 2011;16:58–66.
153. Broers CJ, Sinclair N, van der Ploeg TJ, Jaarsma T, van Veldhuisen DJ,Umans VA. The post-infarction nurse practitioner project: a prospectivestudy comparing nurse intervention with conventional care in a non-high-risk myocardial infarction population. Neth Heart J. 2009;17:61–67.
154. Kleinpell RM, Ely EW, Grabenkort R. Nurse practitioners and physicianassistants in the intensive care unit: an evidence-based review. Crit CareMed. 2008;36:2888–2897.
155. Saseen JJ, Grady SE, Hansen LB, Hodges BM, Kovacs SJ, Martinez LD,Murphy JE, Page RL 2nd, Reichert MG, Stringer KA, Taylor CT. Futureclinical pharmacy practitioners should be board-certified specialists.Pharmacotherapy. 2006;26:1816–1825.
156. Haines ST, Andrus MR, Badowski M, Bradbury MM, Canales AE,Cavanaugh JM, Koval PG, Lee MW, Marrs JC, Michael Nash J, Ott CA,Robbins Williams A, Wham DL. Board certification of pharmacistspecialists. Pharmacotherapy. 2011;31:1146–1149.
20 Circulation September 11, 2012
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from

157. Murphy JE, Nappi JM, Bosso JA, Saseen JJ, Hemstreet BA, HalloranMA, Spinler SA, Welty TE, Dobesh PP, Chan LN, Garvin CG,Grunwald PE, Kamper CA, Sanoski CA, Witkowski PL; AmericanCollege of Clinical Pharmacy. American College of Clinical Pharmacy’svision of the future: postgraduate pharmacy residency training as aprerequisite for direct patient care practice. Pharmacotherapy. 2006;26:722–733.
158. American Board of Physical Therapy Specialists Web page. http://www.abpts.org/home.aspx. Accessed December 1, 2011.
159. Smith J, Plurad D, Inaba K, Talving P, Lam L, Demetriades D. Are alllevel I trauma centers created equal? A comparison of American Collegeof Surgeons and state-verified centers. Am Surg. 2011;77:1334–1336.
160. DiRusso S, Holly C, Kamath R, Cuff S, Sullivan T, Scharf H, Tully T,Nealon P, Savino JA. Preparation and achievement of American Collegeof Surgeons level I trauma verification raises hospital performance andimproves patient outcome. J Trauma. 2001;51:294–299.
161. Bosk EA, Veinot T, Iwashyna TJ. Which patients and where: a quali-tative study of patient transfers from community hospitals. Med Care.2011;49:592–598.
162. Iwashyna TJ, Courey AJ. Guided transfer of critically ill patients: wherepatients are transferred can be an informed choice. Curr Opin Crit Care.2011;17:641–647.
163. Hasin Y, Danchin N, Filippatos GS, Heras M, Janssens U, Leor J, NahirM, Parkhomenko A, Thygesen K, Tubaro M, Wallentin LC, Zakke I;Working Group on Acute Cardiac Care of the European Society ofCardiology. Recommendations for the structure, organization, andoperation of intensive cardiac care units. Eur Heart J. 2005;26:1676–1682.
164. National Resident Matching Program. http://www.nrmp.org/. AccessedNovember 1, 2011.
165. Kuvin JT. Accreditation council for graduate medical education ini-tiatives improve the education of cardiology fellows. Circulation. 2008;118:525–531.
166. Beller GA, Bonow RO, Fuster V. ACCF 2008 recommendations fortraining in adult cardiovascular medicine Core Cardiology Training(COCATS 3) (revision of the 2002 COCATS Training Statement). J AmColl Cardiol. 2008;51:335–338.
167. European Board for the Specialty of Cardiology. Curriculum for acutecardiac care subspecialty training in Europe. www.escardio.org/communities/working-groups/acute-cardiac-care/documents/esc-curriculum-training-intensive-acc-europe.pdf. Accessed April 16, 2012.
168. Fradella G, De Luca L, Tubaro M, Lettino M, Conte MR, Geraci G,Casella G. Clinical competence in intensive cardiac care units: frompractical needs to training programs [in Italian]. G Ital Cardiol (Rome).2010;11:6–11.
169. Danchin N, Filippatos G, Goldstein P, Vranckx P, Zahger D, eds. TheESC Textbook of Intensive and Acute Cardiac Care. Oxford, UnitedKingdom: Oxford University Press; 2011.
170. Katz NM. The evolution of cardiothoracic critical care. J Thorac Car-diovasc Surg. 2011;141:3–6.
171. Cassel CK, Reuben DB. Specialization, subspecialization, and subsub-specialization in internal medicine. N Engl J Med. 2011;364:1169–1173.
172. Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD,Buller CE, Jacobs AK, Slater JN, Col J, McKinlay SM, LeJemtel TH.Early revascularization in acute myocardial infarction complicated bycardiogenic shock: SHOCK Investigators: Should We EmergentlyRevascularize Occluded Coronaries for Cardiogenic Shock. N EnglJ Med. 1999;341:625–634.
173. Rose EA, Gelijns AC, Moskowitz AJ, Heitjan DF, Stevenson LW,Dembitsky W, Long JW, Ascheim DD, Tierney AR, Levitan RG,Watson JT, Meier P, Ronan NS, Shapiro PA, Lazar RM, Miller LW,Gupta L, Frazier OH, Desvigne-Nickens P, Oz MC, Poirier VL; Ran-domized Evaluation of Mechanical Assistance for the Treatment ofCongestive Heart Failure (REMATCH) Study Group. Long-term use ofa left ventricular assist device for end-stage heart failure. N Engl J Med.2001;345:1435–1443.
174. Binanay C, Califf RM, Hasselblad V, O’Connor CM, Shah MR, SopkoG, Stevenson LW, Francis GS, Leier CV, Miller LW; ESCAPE Inves-tigators and ESCAPE Study Coordinators. Evaluation study of con-gestive heart failure and pulmonary artery catheterization effectiveness:the ESCAPE trial. JAMA. 2005;294:1625–1633.
175. Patel MR, Smalling RW, Thiele H, Barnhart HX, Zhou Y, Chandra P,Chew D, Cohen M, French J, Perera D, Ohman EM. Intra-aortic ballooncounterpulsation and infarct size in patients with acute anterior myo-cardial infarction without shock: the CRISP AMI randomized trial.JAMA. 2011;306:1329–1337.
176. Nolan JP, Morley PT, Vanden Hoek TL, Hickey RW. Therapeutichypothermia after cardiac arrest: an advisory statement by the advancedlife support task force of the International Liaison Committee on Resus-citation. Circulation. 2003;108:118–121.
177. NICE-SUGAR Study Investigators, Finfer S, Chittock DR, Su SY, BlairD, Foster D, Dhingra V, Bellomo R, Cook D, Dodek P, Henderson WR,Hebert PC, Heritier S, Heyland DK, McArthur C, McDonald E, MitchellI, Myburgh JA, Norton R, Potter J, Robinson BG, Ronco JJ. Intensiveversus conventional glucose control in critically ill patients. N EnglJ Med. 2009;360:1283–1297.
178. De Backer D, Biston P, Devriendt J, Madl C, Chochrad D, Aldecoa C,Brasseur A, Defrance P, Gottignies P, Vincent JL; SOAP II Investi-gators. Comparison of dopamine and norepinephrine in the treatment ofshock. N Engl J Med. 2010;362:779–789.
179. Wiener RS, Welch HG. Trends in the use of the pulmonary arterycatheter in the United States, 1993–2004. JAMA. 2007;298:423–429.
180. SUPPORT Investigators. A controlled trial to improve care for seriouslyill hospitalized patients: the study to understand prognoses and pref-erences for outcomes and risks of treatments (SUPPORT) [publishedcorrection appears in JAMA. 1996;275:1232]. JAMA. 1995;274:1591–1598.
KEY WORD: AHA Scientific Statements � cardiovascular diseases �critical care � heart-assist device � resuscitation
Morrow et al The Evolution of Critical Care Cardiology 21
by guest on August 21, 2012http://circ.ahajournals.org/Downloaded from