Embed Size (px)
Citation preview
Documenta Ophthalmologica 71: 321-328, 1989. �9 1989 Kluwer Academic Publishers. Printed in the Netherlands.
Evoked potential and preferential looking correlates of the oblique effect in 3-month-old infants
SAMUEL SOKOL, ANNE MOSKOWITZ & VIRGINIA HANSEN Department of Ophthalmology, New England Medical Center, 750 Washington Street, Boston, MA 02111, USA
Abstract. Sensitivity for vertical and horizontal gratings is higher than for obliquely oriented gratings, a phenomenon known as the oblique effect. We compared visual evoken potential and preferential looking estimates of the oblique effect in nonastigmatic 3-month-old infants and found that orientation effects occurred more frequently by visual evoked potential measure than by preferential looking.
Introduction
An adult's visual sensitivity is greater to vertically or horizontally oriented gratings than to obliquely oriented gratings [1]. This phenomenon has been shown to exist electrophysiologically by using both amplitude [2] and lat- ency [3] of the pattern visually evoked potential (VEP). Amplitude is larger and latency is shorter for vertical gratings than for oblique gratings. Recent- ly we reported that the oblique effect as measured with the pattern VEP first appears in human infants at around 3 months of age [4]. Infants show larger VEP amplitude and/or shorter VEP latency for vertically-oriented gratings than for obliquely-oriented gratings. In the present study we compared VEP and preferential looking (PL) estimates of the oblique effect in 3-month-old infants.
Methods
Subjects. VEP and PL data were obtained from 13 infants ranging in age from 11 to 13 weeks. Each infant came twice within a one-week period; half were tested with the VEP first and half with PL first. All infants had less than 1 diopter of cylindrical refractive error by near retinoscopy [5].
VEP recording. Square-wave grating patterns ranging in spatial frequency from 0.63 to 5 c/deg, in one-octave increments, were generated by a black and white Conrac monitor. The mean luminance of the screen was
322
1.5 log cd/m 2 and the contrast was 0.84; the stimulus field subtended 11 ~ and the gratings were phase-alternated at a rate of 3.75 rev/sec. Vertical and left oblique gratings were presented to the infants. The left oblique orientation was produced by rotating the yoke of the monitor. Binocular VEPs were recorded with an active electrode attached to the scalp 1 cm above the inion on the midline. One ear served as reference and the other ear as ground. Signals were amplified with a gain of 20,000 and low- and high-frequency bandpass of 1 and 35 Hz. Amplified signals were averaged by a minicom- puter and a software program with an artifact rejection routine. During VEP recording the infant sat on the parent's lap at a distance of 100 cm from the TV monitor. An observer monitored the infant's fixation and operated a remote-control switch to start and stop averaging. If the infant looked away from the screen, averaging was stopped and restarted when the infant resumed fixation. Because of its low variability bond within and between subjects, we used VEP latency as an index of the oblique effect; we measured the peak latency of the first positive component [3, 6, 7].
Psychophysics. The apparatus used to obtain preferential looking data was similar to that described by Leehey and associates [8]. The stimuli were slides of black and white square-wave gratings ranging in spatial frequency from 0.63 to 5 c/deg in one-octave increments. The mean luminance, contrast, and field size of the slides were matched to that of the TV monitor used for the VEP recording. On each trial a vertical and an oblique grating of the same spatial frequency were paired. During testing, the infant sat on the parent's lap centered between the two stimulus targets at a distance of 100 cm from the partition. An observer looking through a peephole from behind the partition made a forced choice judgment of which side the infant preferred. An experimenter operated the slide projectors and recorded the observer's response. Each infant's percentage of preference for vertical and for oblique gratings was determined for each spatial frequency, with a minimum of 12 and a maximum of 25 trials per spatial frequency. The side of presenttion of vertical and oblique was counterbalanced.
Definition of an oblique effect. To establish whether an individual infant exhibited a VEP oblique effect, we first obtained an estimate of the within- session variance for 2.5 c/deg vertical gratings by recording 6 to 10 blocks of VEPs (64 accumulations per block) from each of six nonastigmatic infants. Vertical gratings were presented throughout the course of one session for each infant, with a 1 to 2-minute break between each block of VEP recording. The mean latency and the 99% confidence interval were calculated for each infant. Since we did not obtain repeated measures for
323
oblique gratings, we assumed that the variance for oblique was equal to that for vertical and used twice the vertical standard error in our calculations of the confidence interval. So the data could be compared across subjects, each infant's 99% confidence interval was then converted to a 99% aniso- tropy interval using the formula of Gwiazda and associates [9]: (log ver- tical - log oblique)/log 2, where vertical was the mena latency obtained for vertical gratings and oblique was the mean latency for vertical _+ the 99% confidence interval. A mean anisotropy interval for the six infants was then calculated.
For each of the infants in the experiment, an anisotropy score for latency was calculated, again using the formula (log vertical - log oblique)/log 2. In these calculations, vertical was the latency for vertical gratings and oblique
\
was the latency for obliquely oriented gratings. Each infant's anisotropy score was then compared with the 99 % anisotropy interval. An infant whose score fell within the 99% anisotropy interval did not show an orientation effect. A score equal to or less than the lower 99% anisotropy interval indicated that an oblique effect was present, i.e., latency was shorter for vertical gratings than for oblique gratings. A score equal to or greater than the upper 99% limit indicated a reverse effect, i.e., latency was significantly shorter for the oblique grating.
For PL the percentage of preference for vertical and for oblique was tallied for each spatial frequency. The percentage of preference that was significantly different from chance was determined for each infant by bino- mial probability rules. This ranged from 83% for 12 trials per spatial frequency to 72% for 25 trials per spatial frequency [10].
Results
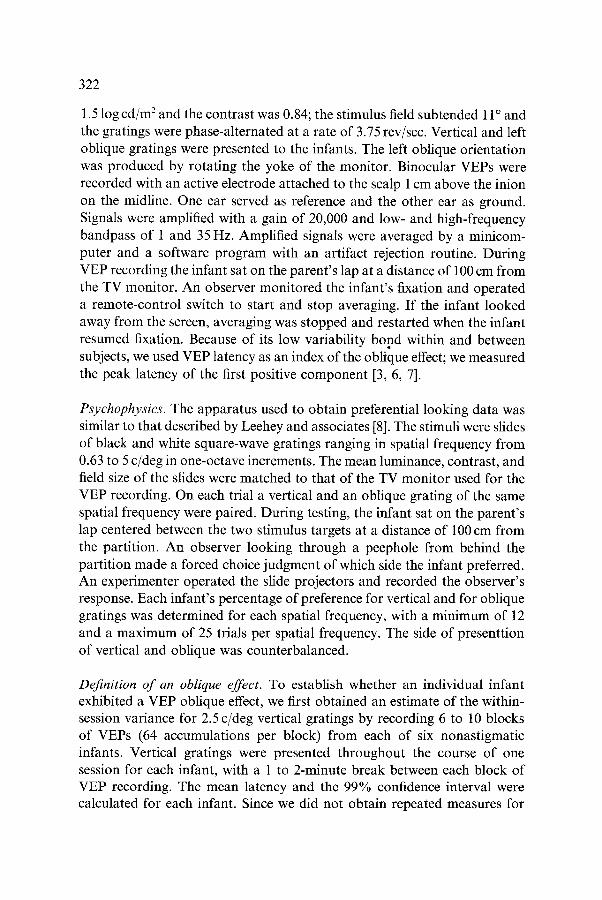
Figure 1 shows VEP records and percentage of preference for vertically and obliquely oriented gratings for one infant. At 5 and 2.5 c/deg, VEP latency was longer for oblique gratings than for vertical gratings, but there was no significant behavioral preference. At 1.25 c/deg, latency was not significantly different for the two orientations, but the infant showed a significant prefer- tence for obliques. At 0.63 c/deg, neither the VEP nor PL showed an effect.
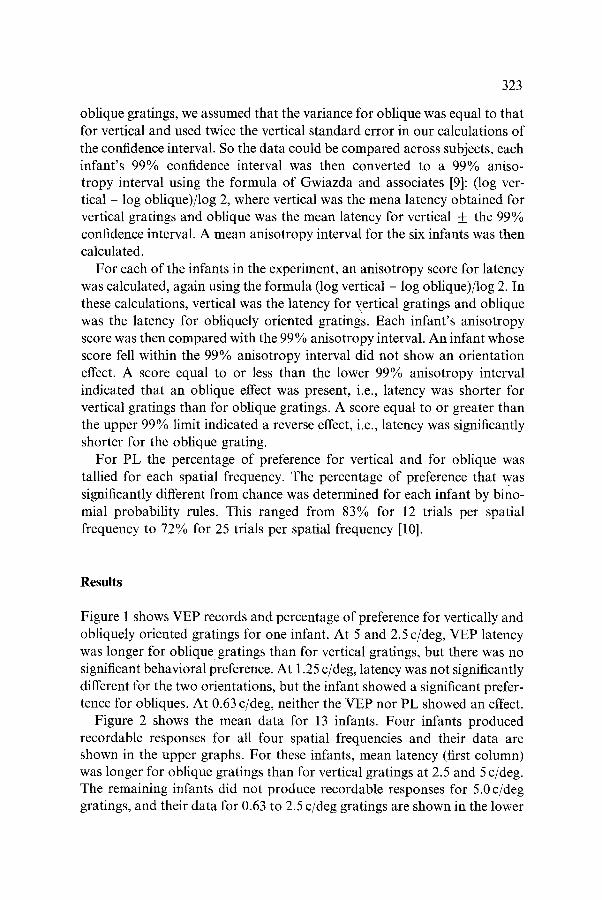
Figure 2 shows the mean data for 13 infants. Four infants produced recordable responses for all four spatial frequencies and their data are shown in the upper graphs. For these infants, mean latency (first column) was longer for oblique gratings than for vertical gratings at 2.5 and 5 c/deg. The remaining infants did not produce recordable responses for 5.0 c/deg gratings, and their data for 0.63 to 2.5 c/deg gratings are shown in the lower
324
5.Oc/d
67%
o 33%
1.25 c/d
2.5 c/d 0.63 c
s8% ~%
~% ~%
~ m
Fig. 1. VEP waveforms and PL percentage of preference for one infant for vertical and oblique gratings.
depths. For these infants mean latency was longer for obliquely oriented gratings at 2.5 c/deg. For both groups the mean latency difference between vertical and oblique gratings for individual subjects (second column) was largest at 2.5 c/deg. The PL data (third column) showed that there was no preference at any spatial frequency for either group of infants.
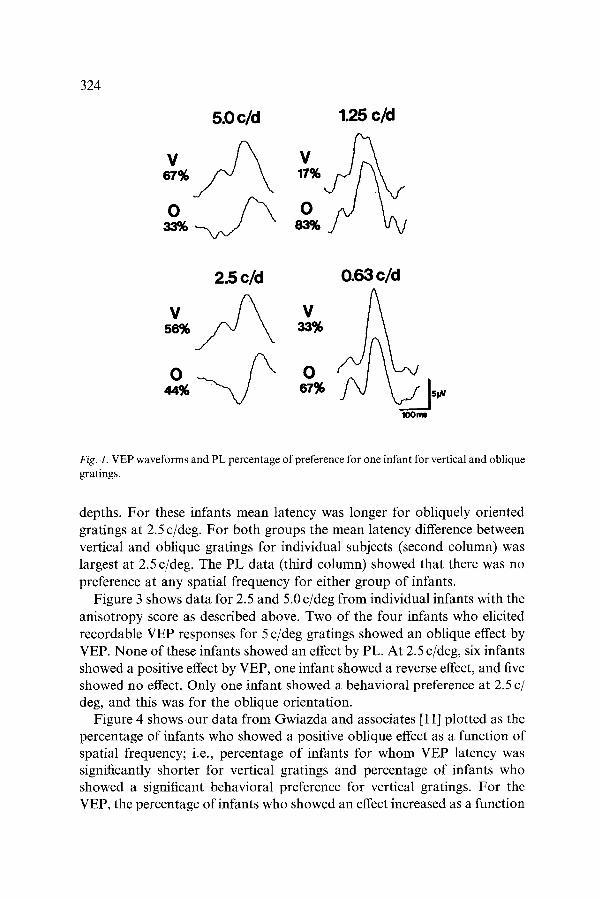
Figure 3 shows data for 2.5 and 5.0 c/deg from individual infants with the anisotropy score as described above. Two of the four infants who elicited recordable VEP responses for 5 c/deg gratings showed an oblique effect by VEP. None of these infants showed an effect by PL. At 2.5 c/deg, six infants showed a positive effect by VEP, one infant showed a reverse effect, and five showed no effect. Only one infant showed a behavioral preference at 2.5 c/ deg, and this was for the oblique orientation.
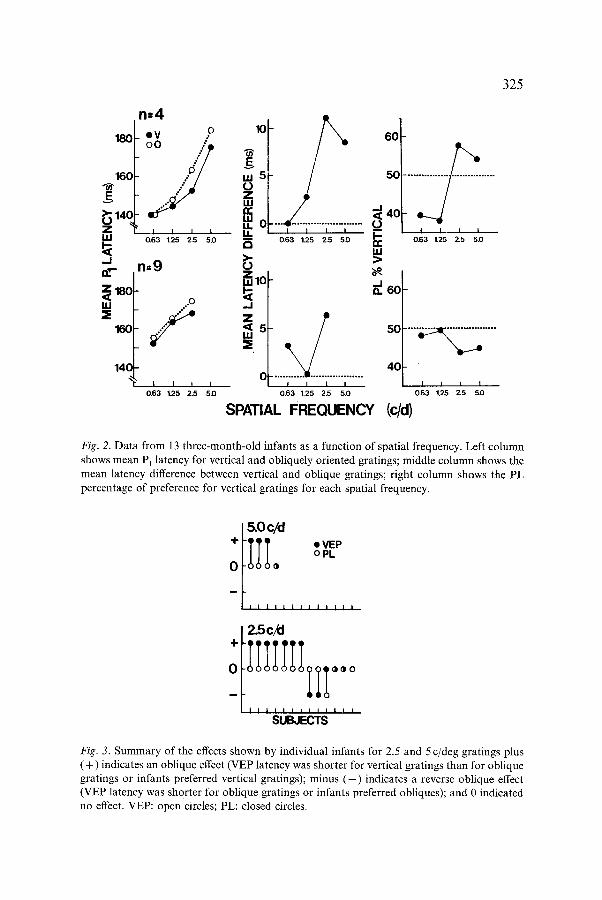
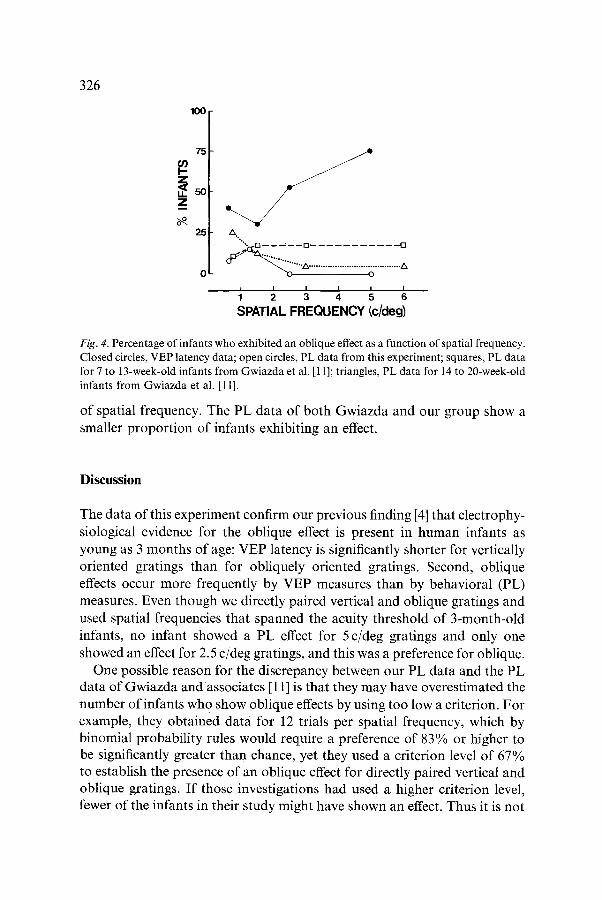
Figure 4 shows our data from Gwiazda and associates [11] plotted as the percentage of infants who showed a positive oblique effect as a function of spatial frequency; i.e., percentage of infants for whom VEP latency was significantly shorter for vertical gratings and percentage of infants who showed a significant behavioral preference for vertical gratings. For the VEP, the percentage of infants who showed an effect increased as a function
325
180
160
14( Z LU
. J I~,r--
Z 180 < lu =E
160
140
n=4 o I V
I I l I 0.63 1.25 2.5 5.0
n=9
/ I I I i
0.63 125 2.5 5.0
10
u.15 0 Z ILl ,'v- ILl U..O IJ.
Z m 10
. J Z
5
C
60
5C
. . . . . . . . ~ 4 0 I I I I L - -
0.63 1.25 2.5 5.0 1,1.1 > Z~ ,_1 a. 60
I I I I 0.63 1.25 25. 5.0
SPATIAL FREQUENCY
50
" ~ . . . . .
I I I I 0.63 1.25 25. 5.0
4 0
I I I I 0.63 1.25 25. 5D
{c/d)
Fig. 2. Data from 13 three-month-old infants as a function of spatial frequency. Left column shows mean P~ latency for vertical and obliquely oriented gratings; middle column shows the mean latency difference between vertical and oblique gratings; right column shows the PL percentage of preference for vertical gratings for each spatial frequency.
/5.0c/d
i I i i I i i i |
/2.5c/d
++o,,, SUBJECTS
Fig. 3. Summary of the effects shown by individual infants for 2.5 and 5c/deg gratings plus ( + ) indicates an oblique effect (VEP latency was shorter for vertical gratings than for oblique gratings or infants preferred vertical gratings); minus ( - ) indicates a reverse oblique effect (VEP latency was shorter for oblique gratings or infants preferred obliques); and 0 indicated no effect. VEP: open circles; PL: closed circles.
326
100
75
25 zx.. o
I I I l I I 1 2 3 4 5 6
SPATIAL FREQUENCY (c/deg)
Fig. 4. Percentage of infants who exhibited an oblique effect as a function of spatial frequency. Closed circles, VEP latency data; open circles, PL data from this experiment; squares, PL data for 7 to 13-week-old infants from Gwiazda et al. [11]; triangles, PL data for 14 to 20-week-old infants from Gwiazda et al. I11].
of spatial frequency. The PL data of both Gwiazda and our group show a smaller proportion of infants exhibiting an effect.
Discussion
The data of this experiment confirm our previous finding [4] that electrophy- siological evidence for the oblique effect is present in human infants as young as 3 months of age: VEP latency is significantly shorter for vertically oriented gratings than for obliquely oriented gratings. Second, oblique effects occur more frequently by VEP measures than by behavioral (PL) measures. Even though we directly paired vertical and oblique gratings and used spatial frequencies that spanned the acuity threshold of 3-month-old infants, no infant showed a PL effect for 5 c/deg gratings and only one showed an effect for 2.5 c/deg gratings, and this was a preference for oblique.
One possible reason for the discrepancy between our PL data and the PL data of Gwiazda and associates [11] is that they may have overestimated the number of infants who show oblique effects by using too low a criterion. For example, they obtained data for 12 trials per spatial frequency, which by binomial probability rules would require a preference of 83% or higher to be significantly greater than chance, yet they used a criterion level of 67% to establish the presence of an oblique effect for directly paired vertical and oblique gratings. If those investigations had used a higher criterion level, fewer of the infants in their study might have shown an effect. Thus it is not
327
a case of our PL estimates being too low but of theirs being too high. If we apply their 67% criterion to our data, two infants showed a preference for verticals at 5 c/deg, three infants showed a preference for obliques at 2.5 c/ deg, and two infants showed a preference for verticals and four for obliques at 1.25 c/deg. One could, of course, argue that our sample of infants simply did not have a preference for verticals (or obliques), regardless of the number of trials, but many of these same infants showed an effect by VEP measures.
Another point regarding the VEP and PL comparisons of our study is that the VEP stimuli were phase-alternated while the PL stimuli were stationary. Whether better agreement between the two techniques would have occurred with phase alternating gratings in the PL study remains to be determined.
The magnitude of the oblique effect is small. There is considerable variab- ility between subjects and the pattern of the effect cannot be described simply as one of the main axis orientations versus 45 ~ left or right obliques. For example, Mayer [12] using psychophysical techniques found eight dif- ferent types of oblique contrast curves in a group of young children and adults and concluded that there is no unitary type of oblique effect. More recently, Wattam-Bell and associated [13] found VEP evidence for vertical and horizontal anisotropy in 6-week-old infants. Future VEP or PL studies of orientation specificity in infants should study a greater number of orienta- tions and use many more trials.
Acknowledgements
This research was supported in part by NEI-00926, BRSG SO7-RR05598- 20 and a Research to Prevent Blindness Senior Scientific Investigation award.
References
1. Appelle S. Perception and discrimination as a function of stimulus orientation: the 'oblique effect' in man and animals. Psychol Bull 1972; 78: 266-78.
2. May JG, Cullen JK, Moskowitz-Cook A, Siegfried JB. Effects of meridional variation on steady-state evoked potentials. Vision Res 1979; 19: 1395-1401.
3. Moskowitz A, Sokol S. Developmental changes in the human visual system as reflected by the latency of the pattern reversal VEP. Electroencephalogr Clin Neurophysiol 1983; 56: 1-12.
4. Sokol S, Moskowitz A, Hansen V. Electrophysiological evidence for the oblique effect in human infants. Invest Ophthalmol Vis Sci 1987; 28: 731-5.
328
5. Mohindra I. A noncycloplegic refraction technique for infants and young children. J Am Optometric Assoc 1977; 48: 518-23.
6. Sokol S, Jones K. Implicit time of pattern evoked potentials in infants: an index of maturation of spatial vision. Vision Res 1979; 19: 747-55.
7. Moskowitz A, Sokol S. Effect of stimulus orientation on the latency and amplitude of the VEP. Invest Ophthalmol Vis Sci 1985; 26: 246-8.
8. Leehey SC, Moskowitz-Cook A, Brill S, Held R. Orientational anisotropy in infant vision. Science 1975; 190: 900-2.
9. Gwiazda J, Scheiman M, Held R. Anisotropic resolution in children's vision. Vision Res 1984; 24: 527-31.
10. Freund JE. Modern Elementary Statistics. 2nd Ed. Englewood Cliffs, N.J.: Prentice-Hall, 1960.
11. Gwiazda J, Brill S, Mohindra I, Held R. Infant visual acuity and its meridional variation. Vision Res 1978; 18: 1557-64.
12. Mayer MJ. Non-astigmatic children's contrast sensitivities differ from anisotropic pat- terns of adults. Vision Res 1983; 23: 551-60.
13. Wattam-Bell J, Braddick OJ, Marshall G, Atkinson J. Development and anisotropy of the orientation-specific VEP. Invest Ophthalmol Vis Sci 1987; 28 (Suppl): 5.
Address for correspondence: S. Sokol, Dept. of Ophthalmology, Box 820, New England Medical Center, 750 Washington Street, Boston, MA 02111, USA.