Embed Size (px)
Citation preview

EVIDENCE REPORT
Guidelines for the Screening, Treatment and Monitoring of Lupus Nephritis in Adults
Working Group
UCLABevra H. Hahn, MD (Rheum)
Jennifer M. Grossman, MD (Rheum)Maureen McMahon, MD (Rheum)
W Dean Wallace, MD (Path)Karandeep Singh, MD (Nephrology)
Soo-In Choi, MD (Rheum)Justin Peng, MD (Rheum)
Mazdak Khalighi, MD (Path)Maneesh Gogia, MD (Rheum)John FitzGerald, MD (Rheum)Alan Wilkinson, MD (Renal)
Suzanne Kafaja, MD (Rheum)William J Martin, MD (Rheum)
Christine Lau, MD (Nephrology)Sefali Parikh, MD (Nephrology)
Mohammad Kamgar, MD (Nephrology)Anjay Rastogi, MD (Nephrology)
Weiling Chen, MA (Rheum)Cheryl C Lee, BA (Rheum)Rikke Ogawa (Librarian)
UCLA-HarborGeorge A. Karpouzas, MD (Rheum)
UCLA and Cedars-SinaiDaniel Wallace, MD (Rheum)
OklahomaJoan T. Merrill, MD (Rheum)
UCSFJinoos Yazdany, MD (Rheum)
David Daikh, MD (Rheum)
Special thanks to Rosalind Ramsey-Goldman, MD and Niloo Nobkht, MD

Table of Contents
Abbreviations
1. Introduction
2. Guideline Development Methodsa. Methodology
1. Rationale and Development of a uniform Lupus Nephritis Definition2. Search Strategy3. Study Selection Based on Title and Abstracts4. Selection of Studies Based on Full Text of Articles5. Quality Assessment
b. Data Extraction and Synthesis1. Rating the Strength of Evidence2. RAND/UCLA Appropriateness Method Using the Task Force Panel (TFP)
c. Definition of Key Term
3. Evidence for Screening, Treatment and Monitoring of Lupus Nephritis in Adults
a. Screening Summary - Pathology1. Role of the Renal Biopsy in Lupus Nephritis2. Correlation of Outcome and Biopsy Findings3. Vascular and Tubulointerstitial Disease in Lupus Nephritis
b. Treatment and Monitoring1. Randomized Control Trials2. Cohort Studies
c. End Stage Renal Disease1. When to Consider Transplant2. Graft and Patient Survival3. Immunosuppressive Medications4. Predictors of Outcome After Transplant5. Summary
d. Pregnancy in Lupus Nephritis Patients1. Maternal/Fetal Outcomes of Pregnancy in Women with SLE2. Relationship of Drugs Used to Treat Nephritis and Outcome of Pregnancy
in Lupus Nephritis
4. Biomarkers in SLE Nephritisa. Anti-dsDNA and Complementb. Anti-dsDNAc. Anti-C1Qd. Complement
5. Adjunctive Therapies to Delay Progression of Renal Damage and Development of Co-Morbid Conditions

6. Socio-Economic Costs and Impact of Lupus Nephritisa. Overview of incidence, economic impact and risk factors of lupus nephritisb. Cost of Lupus Nephritisc. Cost Effectiveness Analysis of Specific Treatments
1. IV Cyclophosphamide vs Steroids alone2. Mycophenalate Mofetil vs IV Cyclophosphamide
Tables1. Task Force Panelists2. ISN/RPS 2003 Classification of Lupus Nephritis3. Renal Pathology Scoring System4. Studies of Poor Prognostic Findings based on Renal Biopsy5. RCT Inclusion/Exclusion Criteria and Jadad Scores6. Cohort Studies Inclusion/Exclusion Criteria and Newcastle-Ottawa Scale7. End Stage Renal Disease/Renal Transplantation Articles8 Summary of Commonly Used Medications’ Teratogenic Effects9 Use of Anti-DNA antibodies for prognosis among SLE patients
APPENDICESA. Search StrategyB. Abstraction Tool – Abstracts C. Abstraction Tool – RCT ArticlesD. Abstraction Tool – Cohort ArticlesE. Case Scenarios
REFERENCES

ABBREVIATIONS
ACR American College of RheumatologyANA Anti-nuclear antibodyAnti-dsDNA Anti-double strand Deoxynucleic AcidARA American Rheumatism AssociationAZA AzathioprineCPH Cr CreatinineCR Complete ResponseCrCl Creatinine ClearanceCYC CyclophosphamideD DayG GramHpf High Power FieldISN/RPSKG KilogramIV IntervenousLE Lupus ErythematosusMG MiligramMTX MethotrexatePOPR Partial ResponsePred PrednisoneProt ProteinRBC Red Blood CellserCr Serum CreatinineSLE Systemic Lupus ErythematosusU UrineWBC White Blood CellWHOWk WeekYr Year

1. Introduction
Important clinical advances have been made since the last ACR guidelines on diagnosis and management of SLE were published in 1999 (1). Those advances include a) improved histologic classification of subsets in renal biopsies (2), b) better management strategies to reduce renal damage (3), c) improved instruments to measure disease activity, damage, flare, and response to therapies ACR response criteria 2004 (4-9) and d) introduction of new treatments with evidence for equal or better response rates and less toxicity compared to the “standard” therapies reviewed in the 1999 (1). The promise of biologic therapies is now on the near horizon with very recent reports of successful clinical trials in lupus (e.g. Belimumab (10)) and lupus nephritis (e.g. ALMS (11)). In addition, the methodology underlying guidelines for medical therapy has improved dramatically (see for example the 2008 ACR guidelines for treatment of rheumatoid arthritis (12). Therefore, it is timely for the ACR to issue updated guidelines for screening, treatment and monitoring in people with lupus nephritis.
The purpose of this systematic review generated evidence-based report is to help develop clinical scenarios to be used for guideline development utilizing a collaborative effort with a working group (WG) and core expert panel (CEP) of clinicians and methodologists.
2. Guideline Development Methods
a. Methodology
Rationale and Development of a uniform Lupus Nephritis DefinitionAfter many discussions, the working group defined diagnosis of Lupus Nephritis as one that meets ACR criteria (persistent proteinuria and/or cellular casts) or in the opinion of a trained rheumatologist or nephrologist.
Search StrategyWe conducted a systematic review of randomized controlled trials and large cohort studies for the therapies identified by the CEP that have been used in treatment of Lupus Nephritis. The therapies chosen were selected on the basis of their availability to be used in treatment of lupus nephritis. Therapies currently in development and not yet available on the market were not reviewed. The search strategy is outlined in Appendix A, and briefly, used Medline (through PubMed) by applying MeSH headings and relevant keywords with references through 1/22/2010. The search was updated on August 8, 2010.
Study Selection Based on Titles and AbstractsOur search was limited to human studies, published in English, and having abstracts. We excluded all review articles. The initial literature search identified 10418 potential interest citations. Two reviewers screened each title and abstract for relevance to the specific aims.
The articles were excluded if:Study population not specific for lupus nephritis (e.g. lupus, autoimmune disease)Case series, Review articles, Meta-analysisStudy population consists of all patients less than age 16Study therapy is not currently commercially available
For randomized clinical trial, articles were excluded if total number of lupus nephritis patients in the study were less than 30.
For cohort studies, articles were included using the following criteria:-if treatment has already been studied in randomized clinical trial, the cohort study must
have either higher number of patients and/or longer study duration- if treatment has not been studied in randomized clinical trial but is or will anticipated to
be commercially available (e.g. rituximab, stem cell)
Selection of Studies Based on Full Text of ArticlesAt the screening phase, all articles identified through the searches for lupus nephritis were reviewed independently by two physicians using a structured form (Appendix B). A third reviewer reconciled discordant results and any disagreements between reviewers. For Randomized Clinical Trials and Cohort Studies, the principal investigators reviewed the results and made final acceptance.
Accepted Randomized Clinical Trials, articles were then reviewed and the relevant data abstracted using a standardized data abstraction forms (Appendix C). The full text of all the articles was reviewed and data abstracted by two reviewers. For Cohort Studies, full text of all the articles was reviewed and data abstracted by at least one reviewer with more than 50% of the articles undergoing duplicate independent data abstraction and reconciliation to ensure consistency and accuracy. (Appendix D – cohort study abstraction form). The principle investigator adjudicated discrepant results in both.
Accepted articles in pathology, renal transplant and end stage renal disease articles, pregnancy, biomarker, and socio-economic quality of life were sent to designated reviewers.
Data were entered into an Excel Spreadsheet.
Quality AssessmentThe quality of RCTs was assessed using the Jadad instrument (13). The Jadad scale ranges from 0-5 based on points given for randomization, blinding, and accounting for withdrawals and dropouts. The quality of the cohort Studies was assessed using the New Castle-Ottawa Quality Assessment Scale (14). The New Castle-Ottawa scale ranges from 0 – 9 stars based on points given for selection, comparability and exposure.
b. Data Extraction and Synthesis
Rating the Strength of EvidenceFor each recommendation, the strength of evidence will be assigned using the method from the American College of Cardiology (15) and/or EULAR/ESCIST (16-17) after the Task Force Panel meeting when the recommendations are developed.
RAND/UCLA Appropriateness Method using the Task Force Panel (TFP)The RAND/UCLA methodology (18-20) incorporates elements of the nominal and Delphi methods. The task force panelists received the evidence report and case scenarios (see Appendix E), illustrating the potential key permutations for each guidelines, instructions for grading scenarios and definitions of all variables and agreed upon thresholds and branch points by email. They were asked to use the evidence to rate the appropriateness of the clinical scenarios permutations. Using a 9-point Likert scale to rate each scenario permutation, the first set of ratings occurred before and a second set of ratings after a group meeting. Disagreement was defined when > 1/3 of the panelists rated a scenario in the lowest tertile of theappropriateness (1-2-3) and > 1/3 of the panelist rated the same scenario in the upper tertile (7-8-9). In the absence of disagreement, a median rating in the lowest tertile classified a scenario
permutation as “inappropriate” and a median rating in the upper tertile classified a scenario as appropriate. Those scenario permutations rating in 4-5-6 together with those with disagreement were classified as “uncertain.” Dispersion of the scores provided the degree of agreement
The anonymous ratings of the 1st round of ratings were reviewed with the panelists at each meeting. Through discussion of definitions and scenario, the reasons for the uncertain category were identified and resolution of discrepancies were attempted by modification of the scenarios,clarification of definitions, or acknowledgement of discordance between clinical practice experience and the medical literature.
Please see Table 1 for list of Task Force Panelists.
Definition of Key Term
DEFINITION OF LUPUS NEPHRITIS DIAGNOSISLupus Nephritis is defined as one that meets ACR criteria (persistent proteinuria and/or cellular casts) or in the opinion of a trained rheumatologist or nephrologist.
Evidence for the Screening, Treatment and Monitoring of Lupus Nephritis in Adults.
a. Screening Summary - Pathology
ROLE OF THE RENAL BIOPSY IN LUPUS NEPHRITISThe purpose of the renal biopsy and the significance of its findings in the treatment of lupus nephritis (LN) have been extensively debated despite, or because of, numerous studies evaluating renal biopsy findings in patients with systemic lupus erythematosus. In an effort to better characterize the specific pathologic findings in lupus-related renal disease, the World Health Organization (WHO) developed a classification system for lupus nephritis in 1974. Over the years this system has been modified and recently, in 2003, adapted into a new classification system under the auspices of the International Society of Nephrology and the Renal Pathology Society (2, 21). The lupus classification is based solely on glomerular disease and does not incorporate vascular or tubulointerstitial changes. As with the WHO system, the ISN/RPS classification has six classes: minimal mesangial LN (class I), mesangial LN (class II), focal LN (class III), diffuse LN (class IV), membranous LN (class V), and sclerosing LN (class IV). Classes III and IV are further characterized by the presence of active or chronic lesions and class IV is subdivided into segmental (IV-S) or global (IV-G) glomerular disease (see Table 2). Some studies have since shown improved interobserver reproducibility with this system (22-23).However the clinical significance of each of these classes and subclasses has been a source of investigation and debate. To evaluate acute and chronic changes a semi-quantitative activity and chronicity grading system was published by the National Institute of Health (NIH) and has been used in many studies (24) (see table 2). However, this grading system is not uniformly applied and has been shown to have poor reproducibility by some authors (25). With the wealth of literature from different cohorts of patients from all over the world over the last 30 years, it is not surprising that there are often contradictory findings in similarly structured studies (see Table 3).
The primary role of the renal biopsy is to provide information to guide treatment. Historically, the proliferative lesions (class III and IV LN) have been regarded as clinically more severe and require immunosuppressive therapy (26-28). It has been recognized that these classes have wide variability in activity and chronicity and the exact point at which immunosuppression should be started or increased has been widely investigated. A review of the literature demonstrates a

lack of consensus regarding which lesions respond to therapy and at what point treatment should be initiated. Nevertheless, many studies have shown cellular crescents, glomerular necrosis with karyorrhectic debris, subendothelial deposits, and tubulointerstitial inflammation all correlate with acute renal insufficiency and demonstrate a response to immunosuppressive therapy (29-34).
The corollary to the activity index is the chronicity index. Beyond a certain point, it is futile to attempt aggressive therapy. The point at which renal scarring precludes improvement by treatment has been investigated and should always be an important consideration in the evaluation of the renal biopsy. Sclerosing lupus nephritis (class VI) with 90% or greater glomerular sclerosis has consistently been shown to have poor prognosis or no response to treatment (35). In one study, patients younger than 23 with any form of renal scarring have been found to be at 50% risk for renal failure at 8 years (24). Furthermore, numerous studies have found each chronicity marker, specifically global and/or segmental glomerulosclerosis, fibrous crescents, tubular atrophy and interstitial fibrosis, to be individual risk factors for renal failure and in combination indicate very high risk (29, 36-40). Chronic lesions have poor prognostic implications even in the setting of normal renal function (41).
The specific lesions and threshold of activity that require treatment have been investigated. Studies have shown no or limited response to immunosuppressive treatment in patients with mesangial lupus nephritis (class I and class II). However this should be considered in light of data revealing 50% of patients with class II lupus nephritis have no evidence of renal disease (42). Patients with subepithelial deposits only (class V) have minimal improvement of serum creatinine when treated with immunosuppressive therapy, but may improve proteinuria (43-45).In the setting of combined proliferative LN (class III or IV) and membranous LN (class V), the proliferative process dominates the clinical picture and is a better indicator of response to treatment (46).
There are several findings on the renal biopsy that can strongly suggest lupus as the etiology of the glomerulonephritis. These include “full house” deposition of immunoglobulins and complements (IgG, IgA, IgM, C1q and C3) demonstrated by immunofluorescence microscopy and tubuloreticular structures in endothelial cells seen by electron microscopy (47).Nevertheless, there are no features that are pathognomonic for lupus nephritis and it is recommended in the ISN/RPS classification system to defer the diagnosis of lupus nephritis in the absence of collaborating clinical evidence (21). Of course, the renal biopsy is also an important diagnostic tool to detect non lupus-related renal diseases or, rarely, subclinical lupus nephritis (42).
CORRELATION OF OUTCOME AND BIOPSY FINDINGSThe strongest risk factors for renal failure are primarily chronic changes, especially tubulointerstitial scarring and glomerular sclerosis. In some studies high activity indices especially the presence of cellular crescents, have also correlated with renal failure or death (32, 41, 48-50). However, mild to moderately active proliferative lesions have stronger correlation with acute renal insufficiency than chronic renal failure. This may be a reflection of treatment intervention and not a true picture of the natural disease course. One study found chronic renal insufficiency, as defined by doubling serum creatinine, was predicted by >50% crescents or moderate to severe tubulointerstitial scarring (51) (see Table 4 for composite data indicating poor renal prognosis from multiple studies).
VASCULAR AND TUBULOINTERSTITIAL DISEASE IN LUPUS NEPHRITIS

Vascular lesions are not a component of the lupus nephritis classification systems. However, there are a variety of vascular injuries that may be concurrent with the glomerular disease and may or may not be associated with the underlying lupus. The vascular lesions include nephrosclerosis, uncomplicated immune complex deposits, non-inflammatory necrotizing vasculopathy (lupus vasculopathy), vasculitis and vascular thrombosis (52). Nephrosclerosis is more common in older patients or patients with hypertension. Different studies have found no change or mild reduction in renal survival in the setting of nephrosclerosis and concurrent LN in older patients. Uncomplicated immune complex deposits are due to deposition of circulating lupus-related immune complexes. This finding has not been shown to have clinical significance. Lupus vasculopathy is most commonly seen in active class III and class IV lupus nephritis. Lupus vasculopathy is a poor prognostic finding as demonstrated by one study that found 68.1% renal survival at 5 years in patients with this lesion (53). Concurrent vasculitis is rare and is frequently associated with ANCA antibodies. Vascular thrombosis may indicate thrombotic microangiopathy and in the setting of lupus is often associated with antiphospholipid antibodies. Studies evaluating vasculitis and vascular thromboses in the setting of lupus nephritis have demonstrated increase in glomerular sclerosis and reduced renal survival (31, 53).
Tubulointerstitial inflammation is most commonly present with class III or IV LN and associated with immune complex deposits in 73% of cases (54). This suggests immune complex deposits cause most but not all cases of tubulointerstitial inflammation. The role of tubulointerstitial scarring as an independent risk factor for chronic renal failure has previously been discussed(24, 41).
b. TREATMENT AND MONITORING
Randomized Controlled Trials (RCT)In Randomized Controlled Trials, 31 peer-reviewed articles and 3 abstracts were abstracted based on selection criteria. Treatments inclusion/exclusion criteria are listed in Table 5. Jadadscore was calculated indicating the quality assessment of the article.
Therapies comparison include prednisone PO and IV, cyclosporine, cyclophosphamide PO and IV, azathioprine, plasmapheresis, mycophenolate mofetil, leflunomide, rituximab, belimumab, and tocilizumab. Data abstracted include therapies in which all study participants are on, biopsy data, duration of the study, average lupus and lupus nephritis duration, intervention arms, endpoints, and adverse reactions.
Data are compiled into an excel sheet that includes Intervention and Outcome (I-O) and a separate sheet including Adverse Events (AEs). Yellow highlights indicate statistically significant parameter within treatment arm from baseline to after treatment. Orange highlights indicate statistically significant parameter between treatment arms.
Cohort StudiesIn Cohort studies, 25 peer-reviewed articles were abstracted based on commercially available therapies, large # cohorts or long duration of the study. Newcastle-Ottawa Scale is calculated indicating the quality assessment of the article. Please see Table 6.
Therapies comparison include rituximab, stem cell, anti-malarial, cyclosporine, cytoxan, immunosuppressives, azathioprine, mycophenolate mofetil, leflunomide.
Data are compiled into an excel sheet that includes Intervention and Outcome (I-O) and a separate sheet including Adverse Events (AEs). Yellow highlights indicate statistically

significant parameter within treatment arm from baseline to after treatment. Orange highlights indicate statistically significant parameter between treatment arms.
c. End Stage Renal Disease
When to consider transplantExpert opinion suggests that clinical activity of lupus should be quiescient before transplantation, with quiescence achieved without cytotoxic agents or more than 10 mg of prednisone daily. Clinically active lupus typically improves with the development of chronic kidney disease but may not do so in some patients, particularly African American women. It is the degree of clinical activity, and not the presence or absence of serologic markers of disease activity, that should determine transplant candidacy. Patients who are heavily immunosuppressed during the course of their native kidney disease may be at increased risk for post-transplantation opportunistic infections, lymphoma, and avascular necrosis (55).
When lupus nephritis results in end stage renal disease, dialysis must be given consideration. There is some evidence to suggest that patients who receive peritoneal dialysis have better post-transplant graft outcomes as compared to those receiving hemodialysis (56). However, candidacy for peritoneal dialysis requires the presence of some residual kidney function, and as that is lost hemodialysis is usually required to achieve sufficient clearance.
The timing for transplantation is not an issue for those without donors. However, if there is ready access to a living related kidney donor, preemptive transplantation is generally a good option. One small study found that dialysis greater than 25 months may be associated with worse graft survival in transplant recipients (57), while other studies (58-59) found no association between duration of dialysis and graft outcomes. A study reviewing USRDS data over a several-year period (56) found no difference in recipient mortality in patients receiving hemodialysis prior to transplant versus no dialysis prior to transplant, although there was a trend towards worse graft outcomes in patients not receiving any dialysis (hazard ratio 1.3, p = 0.055).
Graft and patient survivalOnce a decision has been made to proceed with transplant, there is an abundance of data to suggest that kidney transplantation in patients with lupus nephritis is associated with outcomes generally equivalent to transplant recipients with other underlying etiologies (58-66). Living-related kidney transplants appear to be associated with better graft and recipient outcomes as compared to deceased donor kidney transplants (60).
One-, three-, and five-year rates of graft survival reported in the literature range from 68.8-93.6%, 56-84%, and 33-89%, respectively. Weighted mean 1-, 3-, and 5-year graft survival based on number of transplants per study was 85.1%, 60.9%, and 43.9%, respectively. One-,three-, and five-year rates of kidney transplant recipient survival reported in the literature range from 86.5-99.2%, 61-97.2%, and 36-96%, respectively. Weighted mean 1-, 3-, and 5-year patient survival based on number of transplants per study was 93.3%, 70.1%, and 53.5%, respectively.
Though subclinical recurrence of lupus nephritis may be common on routine surveillance biopsies (67), the prevalence of recurrent lupus nephritis was found to be only 2.4% in analysis of multi-year UNOS data (68), with risk factors for recurrence including African American race, female gender, and younger age.
Immunosuppressive medications
The use of calcineurin inhibitors, mycophenolate mofetil/mycophenolic acid, and azathioprine is considered the mainstay of immunosuppressive therapy in all kidney transplant recipients. Therefore, it is not surprising that the use of these drugs has been associated with improved outcomes in kidney transplant recipients with lupus nephritis. Recipients with lupus nephritis who were not treated with a calcineurin inhibitor had an 89% greater risk of graft failure and an 80% greater risk of death. Those who did not receive either mycophenolic acid or azathioprine had a 41% increased risk of graft failure and a 66% increased risk of death (56).
Predictors of outcome after transplantRisk factors for graft failure include multiple pregnancies, multiple blood transfusions, a greater comorbidity index, higher body weight, age, African American race of the donor or recipient, prior history of transplantation, greater PRA levels, lower level of HLA matching, deceased donors, and hemodialysis in pretransplant period. Risk factors for recipient death include higher recipient and donor age, prior transplantations, and higher rate of pretransplant transfusions(56).
SummaryIn summary, kidney transplantation for lupus nephritis should be treated similarly to kidney transplantation for other causes of renal failure. Ideally, lupus should be clinically quiescent at the time of transplant. Peritoneal dialysis should be chosen over hemodialysis as a bridge to transplantation if a living-related kidney donor is not readily available. Graft and patient survival in kidney transplant recipients with lupus nephritis are generally on par with non-lupus-related kidney transplant recipients. The presence of lupus should not influence choice of immunosuppressive medications. Certain factors can be predictive of worse graft and recipientoutcomes. Please see Table 7 for Summary of End Stage Renal Disease/Renal Transplantation Articles.
d. Pregnancy in Lupus Nephritis Patients
Maternal/Fetal outcomes of pregnancy in women with SLE. We identified one systematic review/ meta-analysis that examined pregnancy outcomes in patients with Systemic Lupus Erythematosus and Lupus Nephritis (69). This review yielded 37 studies which fulfilled study entry criteria, including 29 studies that were case series, five case-control studies, and three cohort studies. Twelve studies were prospective, and 25 studies were retrospective. 34 studies had data for active nephritis at the time of conception, whereas 33 reported data from patients with historic nephritis. Overall, the studies included a total of 1842 patients and 2751 pregnancies.
Random-effects analytic methods were used to evaluate pregnancy complication rates. Overall, the induced abortion rate was 5.9%; when these pregnancies were excluded, fetalcomplications included spontaneous abortion (16%), intra-uterine growth restriction (12.7%), stillbirth (3.6%), and neo-natal deaths (2.5%). Among live births, the preterm birth rate was 39.4%. The definitions used to determine these outcomes were not clarified in the manuscript.
The most frequent maternal complications included lupus flare (25.6%), hypertension (16.3%), nephritis (16.1%) (no specification given regarding frequency of new disease vs. recurrence), and pre-eclampsia (7.6%). Severe complications, including eclampsia, stroke, and maternal death were observed in <1% of subjects. Maternal deaths occurred because of opportunistic infections, sepsis, flares of lupus nephritis, and renal impairment.
Random-effects meta-regression analysis was performed to assess the effects of nephritis on pregnancy outcomes. Active nephritis was significantly associated with maternal hypertension and preterm birth, whereas a history of nephritis was significantly associated with hypertension and pre-eclampsia. After controlling for hypertension, the association between active nephritis and preterm birth was still statistically significant.
Nine papers of thrity-seven correlated renal histology with maternal and/or fetal outcomes. Among these studies, there was no statistically significant association seen between histologic subclass and the rate of unsuccessful pregnancy or any pregnancy complication.
Relationship of Drugs Used to Treat Nephritis and Outcome of Pregnancy in Lupus NephritisWe did not identify any randomized controlled studies that examined the use of medications to treat lupus nephritis in pregnancy. We did identify one retrospective case series that correlated outcomes of pregnancy with treatments of lupus (70). In this study, there were no differences in outcome seen between patients treated with prednisolone alone, prednisolone plus azathioprine, and those who received no treatment. 21/23 pregnancies in women taking azathioprine were successful. A summary of data from MICROMEDEX regarding known information about the teratogenic effects of commonly used medications in lupus nephritis is presented in Table 8.
4. BIOMARKERS IN SLE NEPHRITIS
Biomarkers can be defined as a genetic, biological, biochemical or molecular events whose alternations correlate with disease development or manifestations and can be measured in the laboratory (71). Many different types of biomarkers have been, or are being evaluated, including but not limited to genetic tests, RNA microarray profiles, cytokine profiles, autoantibody profiles and flow cytometry assays of B cell subsets. This is an evolving field with numerous promising candidates (reviewed by Mok, CC (72). This evidence report will focus on anti-dsDNA, C3, C4 and anti-C1q as they are easily measured, readily available and frequently evaluated in patients with SLE. Recommendations for the use of biomarkers in SLE will require updating as additional scientific data and clinical feasibility is reported.
Articles for the evidence report came from four sources; recent reviews (72-74), the evidence report for Quality Measures in SLE, kindly provided by Jinoos Yazdani, MD, expert identified articles, and articles from the RCT, CCT and cohort searches as described in the methods section.
Anti-dsDNA and complementThere is no direct evidence from prospective controlled trials that checking SLE specific laboratory tests, such as anti-dsDNA and complements (versus not checking these laboratories) will improve patient outcomes. However, several of these assays are part of the diagnostic criteria for SLE, have been shown to have prognostic significance, and may assist with disease monitoring (discussed under "indirect evidence" below).
With regard to monitoring of anti-dsDNA antibodies and complements, two randomized controlled trials have directly addressed the question of whether SLE flares can be decreased by responding to changing titers of these assays with escalation of immunosuppressive therapy(75-76). Although the morbidity associated with prophylactic escalations of corticosteroids have made enthusiasm for these trials somewhat limited, both trials (discussed below), did demonstrate that flares in a subset of patients can be decreased.

The first study by Dutch investigators (76) performed block randomization of patients with anti-dsDNA antibodies by whether patients experienced a flare in the previous 2 years, and by two immunosuppression maintenance regimens (stable treatment with glucocorticoids and another immunosuppressive or decreasing glucocorticoid dosage versus no immunosuppressive agents). Early treatment with prednisone 30 mg/day when patients in the treatment arm experienced a 25% rise in anti-dsDNA titers reduced the incidence of major and minor flares.
A more recent randomized study by Tseng et al.(75) followed 154 patients monthly for up to 18months. During follow-up, 41 patients were characterized as having serological flares (elevation of both anti-dsDNA level by 25% and the C3a level by 50% over the previous 1-2 monthly visits). Using a double-blind design, half of these patients received 30 mg/day of prednisone or a placebo for two weeks, followed by a taper over the ensuing 2 weeks. A statistically significant reduction in flares in the group receiving prednisone was observed. However, this study also illustrated that the positive predictive value for these biomarkers for clinical flares in SLE was suboptimal, and that many patients would be over-treated if the serological cutoffs used in this study were used.
Anti-dsDNAAnti-dsDNA antibodies have high specificity for SLE and are found in up to 70% of patients at some point in the course of the disease. Several lines of indirect evidence support the utility of checking anti-dsDNA antibodies at baseline (at a minimum) in patients with SLE. These include:
1) Evidence that these antibodies correlate with disease activity
2) Evidence that in a subset of patients, anti-dsDNA antibodies may precede disease exacerbations
3) Evidence that the presence of these antibodies may identify patients with an increased chance of specific severe disease manifestations over time, such as glomerulonephritis.
Each of these is discussed below.
Kavanaugh et al., as part of the American College of Rheumatology Ad Hoc Committee on Immunologic Testing, issued guidelines for the use of the anti-DNA antibody testing in 2002 (77).Using a systematic review of the literature, they calculated sensitivities, specificities, and likelihood ratios for anti-DNA testing in SLE. The results are adapted in Table 9.
As illustrated in Table 9, the positive likelihood ratios of 4.14 (disease activity), 1.7 (renal involvement), and 1.7 (renal activity) show that the presence of anti-DNA can influence the likelihood of important disease parameters. These overall effects are small, but significant. The general conclusion from these data is that anti-DNA antibodies remain an important clinical tool in the management of SLE. However, the specific weighted means are likely prone to error given the immense heterogeneity in studies given different definitions of disease activity and differing patient populations.
The systematic review of the literature performed by Yazdany and colleagues yielded a number of other relevant studies as well:
1) Additional studies demonstrating that anti-dsDNA antibodies correlate with disease activity in SLE were identified (78-86). However, clinical-serological discordance (i.e.

clinical quiescence, but high anti-dsDNA antibodies or vice versa) has also been described in a subset of patients (87-89).
2) Many studies have shown that rising anti-dsDNA antibody titers may predict disease flares in a subset of SLE patients (83, 89-96), particularly renal flares(97-101). However, a few negative studies have also been reported (102-104), and some studies show anti-dsDNA antibody levels actually decrease in the midst of a flare (92-94).
3) A few studies have shown that anti-dsDNA antibodies early in disease increase the chance of the development of certain disease manifestations, such as glomerulonephritis (81, 105-107), and that these antibodies may be associated with poorer renal outcomes (108-110).
Not all studies support the use of routine antiDNA testing. Esdaile and colleagues found the sensitivity for anti-dsDNA detecting a flare as assessed by SLEDAI was 50% and the specificity was less than 75% with positive and negative likelihood ratios near 1.0 (111).
Anti-C1QThe use of anti-C1q as a biomarker in lupus nephritis was recently reviewed by Mok in 2010(72). To summarize, anti-C1q antibodies are present in 20-44% of lupus patients with most studies showing an association of these antibodies with renal disease. A review by Sinico et al noted that anti-C1q correlated with active renal disease with a sensitivity ranging from 44%-100% and a specificity of 70-92% (112).
Two recent prospective studies have been published. In one study of 70 patients with SLE prior to a diagnosis of SLE , 15 developed renal disease all with positive anti-C1q, 93% with anti-dsDNA while 45% without renal disease had anti-C1q and 73% were antiDNA positive (112).The median follow up for patients who had not developed nephritis was 13 years (range 2-17). In this study, anti-C1Q did not correlate with antiDNA.
Moroni and colleagues studied the relationship of antiC1q antibodies in SLE in 228 patients followed for an average of 6 years (113). Elevation of anti-C1q predicted renal flares with a sensitivity of 80.5% and specificity of 71%. This was only marginally better than antiDNA and complement levels. This study suggested that all four tests combined together had a good negative predictive value while antiC1q combined with C3 and C4 yielded the best results for positive predictive value. Anti-C1q was not as informative in patients with membranous GN as 46% of flares occurred in anti-C1q negative patients.
Not all studies support the use of routine antiC1Q testing. Esdaile and colleagues found the sensitivity for anti-C1q detecting a flare as assessed by SLEDAI was 50% and the specificity was less than 75% with positive and negative likelihood ratios near 1.0 (111).
Anti-C1q antibodies are not necessarily specific for SLE as they can be seen in 0-3% in children and up to 18% in elderly individuals (114). They can also be seen with infections.
ComplementThe relationship of complement to SLE is complex and research in this area is ongoing. Despite the limitations of applying this potential biomarker longitudinally to all SLE patients (such as variations in synthesis, genetic deficiencies and varied extravascular distribution) (115-116), evidence supports obtaining baseline values for complements with available assays as a minimal standard of care.

Although not part of the diagnostic criteria for SLE, depressed complement levels may add to the clinical information traditionally used to diagnose the disease. In addition, literature spanning several decades points to the following generalizations:
1) Depressed complements or complement split products roughly correlate with some aspects of disease activity in SLE (85, 115-116), such as renal disease (81, 117-119),
2) Decreasing complements and complement split products can predict flares in some patients (94-96, 99-101, 120-121) and
3) Hypocomplementemia may also be associated with poorer outcomes over time (99, 122).
Not all studies support the use of routine complement testing. Esdaile and colleagues found the sensitivity for C4 detecting a flare as defined by SLEDAI was 50% and the specificity was less than 75% with positive and negative likelihood ratios near 1.0 (111). For C3, the likelihood ratio for a positive test was near 2.0, suggesting that it may be more helpful.
5. ADJUNCTIVE THERAPIES TO DELAY PROGRESSION OF RENAL DAMAGE AND DEVELOPMENT OF CO-MORBID CONDITIONS
Several partly-preventable factors contribute to progressive renal damage, particularly in the setting of proteinuria. These include adaptive hyperfiltration (relatively normal glomeruli increase in size and function in response to damage in other glomeruli, which probably leads to glomerular sclerosis), systemic hypertension, accelerated atherosclerosis, hypovolemia and exposure to nephrotoxic drugs or dyes. Therefore, management of lupus nephritis includes not only the control of SLE but also attention to these other issues, particularly since lupus nephritis tends to flare and/or to persist, making progression to end stage renal disease fairly common over a course of 25 years. The recommendations discussed below are available from the National Kidney Foundation and UpToDate (123-124).
Treatment with an angiotensin converting enzyme inhibitor (ACE) or angiotensin II receptor blocker (ARB) is recommended for any patient with glomerular disease and proteinuria persistent beyond 3 months, and/or patients with glomerular renal disease who are hypertensive. ACE and ARB are more effective in delaying decline of renal function if initiated before serum creatinine levels reach 1.2 mg/dL in women and 1.5 mg/Dl in men. There are two goals of ACE/ARB treatment: a) proteinuria lower than 1000 mg per 24 hours, and b) blood pressure lower than 130/80, with some authorities encouraging an even lower number if proteinuria exceeds 1000 mg per 24 hours. Data are stronger for effectiveness of ACE/ARB therapies in slowing decline of renal function in chronic kidney disease, compared to low protein diets. However, if proteinuria cannot be reduced below 1000 mg/24 hours with ACE/ARB, diet intervention should be considered. A 60% reduction in proteinuria from baseline may be the best achievable outcome. If ACE/ARB are not adequate for control of hypertension, loopdiuretics should be added. ACE/ARB reduce glomerular perfusion; an increase in serum creatinine is common after instituting these agents; an increase of 35% over 2 to 4 months is acceptable if stable. Hyperkalemia is also a potential adverse effect. Both serum Cr and K+ should be assayed at regular intervals after initiation of ACE/ARB therapies.
Other preventable causes of decline in renal function include dehydration for any reason (vomiting, diarrhea, infections, over-diuresis) and administration of potentially nephrotoxic drugs (aminoglycoside antibiotics, NSAIDs, radiographic contrast materials including gadolinium, etc), and these should be avoided when possible.
Metabolic disorders can accompany chronic kidney disease and cause organ damage, such as metabolic acidosis, hyperphosphatemia, hyperparathyroidism, hyperkalemia, and malnutrition

due to anorexia. Guidelines for detection and management of these problems are available (123-124).
Management of hyperlipidemia is also required as a measure to lower cardiovascular disease risk associated both with SLE and with chronic kidney disease CKD. The most common lipid abnormality in CKD is hypertriglyceridemia, which should be treated by diet and appropriate medication. CKD is considered an independent risk factor for coronary heart disease; thus the LDL-cholesterol should be kept below 100 mg/dL (2.6 mmol/L), and some authorities recommend a level less than 70 mg/dL. Statin therapies are usually required to reduce LDL-cholesterol levels. One randomized controlled study shows that patients with SLE who have undergone renal transplantation have significantly fewer cardiovascular events than similar patients on placebo (125).
Anemia of CKD may require treatment; see references (123) and (124).
Planning for renal replacement therapy, discussed in another section, should begin when GFR, falling steadily, reaches a level below 30 mL/min/1.73 M2. Planning for placement of shunts which require months to mature, for identifying and typing potential living donors, etc require time and participation of multiple medical teams. Uremic symptoms are common when GFR falls below 15 mL/min. Uremic symptoms usually requiring immediate dialysis include volume overload that cannot be controlled medically, pericarditis/pleurisy, hypertension that cannot be controlled medically, platelet dysfunction with active bleeding, acute peripheral neuropathy or encephalopathy, and hyperkalemia that cannot be controlled medically.
Prevention of infection and screening for malignancies are additional concerns in managing patients with lupus nephritis receiving chronic immunosuppression. Prospective studies of immunization with influenza or pneumococcal vaccines suggest that they are safe and relatively effective in terms of antibody titers induced (patients on high doses of immunosuppressives are less likely to respond than those on lower doses). Otherwise, systematic prospective studies addressing efficacy and safety of preventing infections and screening for malignancies in SLE patients are not available. A recent USA study (126) showed that administration of influenza/pneumococcal vaccines occurs in approximately 60% of SLE patients, as does routine screening for malignancy (mammograms, cervical smears, colon screening).
6. SOCIO-ECONOMIC COSTS AND IMPACT OF LUPUS NEPHRITISThere have been several studies that address the socio-economic costs of lupus nephritis. Pharmaceutical companies have sponsored many of these studies. However, the studies demonstrate similar findings that the additional cost of lupus nephritis over lupus without nephritis or non-lupus conditions is significant. Additional studies have examined the relative cost-effectiveness of different nephritis treatments with strong evidence supporting cycophosphamide over prednisone mono-therapy for the treatment of severe lupus nephritis (127) and mycophenalate mofetil to be more cost-effective than cyclophosphamide (128).
Overview of incidence, economic impact and risk factors of lupus nephritis
Ward described the incidence of end stage renal disease (ESRD) due to systemic lupus ertythematosus using US Renal Data System, a national population-based registry of all patients receiving renal replacement therapy for ESRD (129). The 2004 incident rate was 4.9per million in 2004. Women had higher rates than did men (7.6 vs. 2.0), African-American

higher than either Hispanic or Caucasian (20.3 vs. 5.8 vs. 3.0). Patients with lower socio-economic status had higher rates than those with high socio-economic status (5.2 vs. 3.8).
Other authors have supported the findings of higher rates of lupus nephritis among African-Americans (130-132). Poverty may account for some of this explanation (131, 133). In a population based ecological study, Ward reported that lower socio-economic areas had higher incidence of endstage renal disease due to SLE (129) suggesting that limited access to care results in poorer SLE renal outcomes. However, Petri attributed the race differences due to other factors including adherence (physician reported) and type of medical insurance (134).Contreras supported the association of poverty and lupus nephritis (132). In an interesting study on race using genetic markers and patient questionnaires from the LUMINA study (135),Fernandez portioned out the contribution of race and socio-economic factors on risk of lupus nephritis. Through logistic modeling, ethnicity explained 7.6% of the variation observed. The ethnicity component could be further broken down into admixture vs. socio-economic status variables.
Ward reported that Lupus patients were as likely to get living related transplants but less likely to get cadaveric renal transplants and more likely to stay on transplant lists longer than other patients with ESRD. Female gender and African-American patients were more prevalent proportions than other causes of renal failure (136).
Cost of Lupus Nephritis
Carls and colleagues described the direct and indirect costs of SLE and SLE nephritis using a large commercial database that contains data on medical and pharmaceutical claims to calculate direct medical costs (2005 US$) and data on employee absenteeism and short-term disability (137). The project was co-authored by the Health and Productivity Divisions, Thomas Healthcare and Bristol-Myers Squibb, UCSF Institute for Health and Productivity and Emory University, Rollins School of Public Health.
Of the 17 million enrollees, 6269 patients with lupus were identified based on at least inpatient or at least 2 outpatient medical claims. Of these SLE patients 592 had nephritis. Lupus nephritis patients’ direct and indirect medical costs totaled $58,389 and $5,806 versus Lupus patients without nephritis $15,447 and $5,714 versus $6,819 and $5,093 (for controls matched to lupus patients without nephritis). Compared to 11 other chronic care conditions, lupus nephritis was associated with the highest medical costs (driven primarily by direct medical costs).
Clarke and colleagues (138) used a cohort of 6 Canadian and US clinics that collected prospective self-reported patient data on health resource utilization and lost work. Patients’ direct and indirect medical expenditures were estimated using patient self reported health utilization and work reported absenteeism. All costs were expressed in terms of 2002 Canadian dollars. Bristol-Myers Squibb supported funding.
Of the 715 patients, 89% had no renal disease. Stratifying patients by the SLICC renal damage count, patients with higher scores had higher direct and indirect medical costs. Patient with no renal disease had median direct and indirect costs of $14K and $46K versus patients whose SLICC renal damage = 3 with costs of $90K and $77K.
Li and colleagues (139) conducted a similar study using Medicaid patients. The study was authored and supported by funding from Bristol-Myers Squibb. Using at least 2 outpatientclaims or at least 1 inpatient claim, 20,125 SLE patients were identified and 2,298 patients with continuous enrollment during the 5-years follow-up. Patients with lupus nephritis had significantly higher direct medical costs ($27,463) than either lupus patients without nephritis

($13,014) or matched controls ($9,258). When nephritis patients were stratified by presence of ESRD, costs for patients with ESRD ($47,660) were significantly higher than costs for patients without ESRD ($18,002). Li also demonstrated that costs increased significantly over the years for lupus patients (particularly for those patients with ESRD).
Pelletier and colleagues used a large US commercial insurance clams dataset to examine cost of lupus nephritis (140). The study was supported and co-authored by Genetech. Of the 15,590 SLE patients identified, 1068 had nephritis. One-third of the patients (30.3%) with nephritis were hospitalized during the year while only 13.6% of the SLE patients without nephritis were hospitalized. Costs across all medical areas of care (e.g. laboratory, outpatient, emergency department, infusions) were higher among patients with nephritis totaling $30,652 vs. $12,029 (in 2008 US$) per patient. Costs directly attributable to SLE were $6,991 and $2,489 respectively.
Cost effectiveness analyses of specific treatments
Intravenous Cyclophosphamide vs. Steroids aloneIn a 1994 NIAMS funded study, McInnes and colleagues reported that cyclophosphamide plussteroids was cost-savings compared to steroids alone, attributable to the significant costs of higher rates of ESRD for patients treated with steroids alone (127). All costs were reported in 1998 dollars. When looking at costs projected over 10 years for a hypothetical cohort of 1130 SLE nephritis patients (annual estimate of incident nephritis), the expected total costs of patients treated with steroids alone would be $65 million (more than 99% of that cost coming from the care for the 50% of patients projected with ESRD). In contrast, the cost of providing care for patients treated with cyclophosphamide was $14 million with only 5% of patients progressing to ESRD. Even though the analysis was over-simplified the magnitude of the cost-savings is clear. (As an example, they have all of the 5% of patients treated with cyclophosphamide progressing to ESRD in year 3.)
Mycophenalate Mofetil vs. Intravenous CyclophosphamideIn a study funded and co-authored by Aspreva, Wilson and colleagues analyzed quality adjusted life-years by treatment type (128). Based on 2.7 g of MMF vs. 750 mg/m2 of cyclophosphamide costs and quality of life were derived for a hypothetical cohort of 10,000 simulated patients. Algorithms were detailed to include crossover patients, expected outcomes, as well as major and some minor adverse infections. The expected cost in 2005 £ for MMF vs. cylophosphamide over 24-weeks was £1,388 vs. £2,994. MMF also had superior quality of life scores with 0.26 QALYs vs. 0.22 QALYs therefore resulting in cost-saving (dominance) of MMF yielding a cost-savings of £41,205 per QALY. The typical willingness to pay for a QALY is £25 -£35 thousand (equivalent to $50 – $70 thousand). Using sensitivity analyses to vary outcomes the confidence interval around the £41,205 per QALY even with poorer outcomes, there was 81% probability that the cost per QALY would be less than the willingness to pay for QALY.

Table 1 – Task Force Panelists
Jo H. M. Berden, MD**Professor of Nephrology
Radboud University Nijmegen Med Ctr
Nijmegen, THE NETHERLANDS
Rosalind Ramsey-Goldman, MD*
Professor of MedicineNorthwestern University
Chicago, ILLINOIS
Chi-Chiu Mok, MD*Chief of Rheumatology
Tuen Mun and Pok Oi HospitalHONG KONG
Jill P. Buyon, MD*Professor of Medicine
NYU / Hospital for Joint DiseasesNew York, NEW YORK
Frederic A. Houssiau, MD, PhD*
Professor and HeadRheumatology
Universite Catholique LouvainBrussels BELGIUM
Liz Shaw-StablerExecutive Director
Center for Lupus Care, Inc.Inglewood, CALIFORNIA
Gabriel Contreras, MD**Associate Professor of Medicine
Div of NephrologyUniversity of MiamiMiami, FLORIDA
David A. Isenberg, MD, FRCP*Professor
Center for Rheumatology Research
University College of London London ENGLAND
Brad Rovin, MD**Professor of MedicineDivision of Nephrology
The Ohio State UniversityColumbus, OHIO
Karen H. Costenbader, MD, MPH*
Assistant Professor of MedicineRheumatology Immunology &
AllergyHarvard Med School / Brigham Boston, MASSACHUSETTS
Kenneth C. Kalunian, MD*Professor of Medicine
Center for Innovative TherapyUCSD School of Medicine
La Jolla, CALIFORNIA
Murray B. Urowitz, MD, FRCPC*
Professor in MedicineThe Toronto Western Hospital
Toronto, CANADA
Mary Ann Dooley, MD*Associate Professor of Medicine
NephrologyUniversity of North Carolina
Chapel Hill, NORTH CAROLINA
Susan Manzi, MD, MPH*Chair, Department of MedicineWest Penn Allegheny Health
SystemPittsburgh, PENNSYLVANIA
David Wofsy, MD*Professor of Rheumatology
Arthritis-ImmunologyVA Medical Center / UCSF
San Francisco, CALIFORNIA
Peng Thim Fan, MD*Rheumatologist, Community
PracticeNorth Hollywood, CALIFORNIA
* = Rheumatology ** = Nephrology *** = Pathology

Table 2.
ISN/RPS 2003 Classification of Lupus Nephritis
Class I Minimal mesangial lupus nephritisClass II Mesangial proliferative lupus nephritisClass III Focal lupus nephritisa
Class III (A) Active lesions: focal proliferative lupus nephritisClass III (A/C) Active and chronic lesions: focal proliferative and sclerosing lupus nephritisClass III (C) Chronic inactive lesions with glomerular scars: focal sclerosing lupus nephritis
Class IV Diffuse lupus nephritisbClass IV-S (A) Active lesions: diffuse segmental proliferative lupus nephritisClass IV-G (A) Active lesions: diffuse global proliferative lupus nephritisClass IV-S (A/C) Active and chronic lesions: diffuse segmental proliferative and sclerosing lupus nephritisClass IV-G (A/C) Active and chronic lesions: diffuse global proliferative and sclerosing lupus nephritisClass IV-S (C) Chronic inactive lesions with scars: diffuse segmental sclerosing lupus nephritisClass IV-G (C) Chronic inactive lesions with scars: diffuse global sclerosing lupus nephritis
Class V Membranous lupus nephritisClass VI Advanced sclerotic lupus nephritis
Adapted from Weening et al. (21)

Table 3.
Renal Pathology Scoring System
Activity Index Chronicity IndexGlomerular Abnormallties
1. Cellular proliferation 1. Glomerular sclerosis2. Fibrinoid necrosis, karyorrhexis 2. Fibrous crescents3. Cellular crescents4. Hyaline thrombi, wire loops5. Leukocyte infiltration
Tubulointerstitial Abnormalities1. Mononuclear-cell infiltration 1. Interstitial fibrosis
2. Tubular atrophy
All parameters are scored from 1-3 in terms of severity.Fibrinoid necrosis and cellular crescents are weighted by factorof 2. Maximum score of activity index is 24, of chronicity index is 12
Adapted from Austin et al. (24)

Table 4. Studies of Poor Prognostic Findings based on Renal Biopsy
Study Poor prognostic findings N YearAustin et al. (24) 50% renal failure at 8 years in high risk group (CI
1+ in pts age 8-23 or CI 5+ in pts 24-61) 102 1983
Austin et al. (36) 25% of class IV developed renal failure at 10 years follow up. Chronicity markers are individual risk factors for renal failure and very high risk factor in combination.
102 1984
Austin et al. (51) >50% crescents or moderate/severe interstitial fibrosis at high risk for doubling creatinine
64 1995
Banfi et al (53) Renal vascular lesions (Lupus vasculopathy, vasculitis, thrombosis, nephrosclerosis) 5 & 10year survival of 74.3% and 58% in pts with RVL vs 92% and 83.3% in pts without RVL
285 1991
Blanco et al. (48) Vascular hyalinosis, glomerular sclerosis, fibrous crescents and CI >3
85 1994
Contreras et al (141) chronicity index >/= 2 213 2005Esdaile et al (142) Tubulointerstitial fibrosis/atrophy 87 1989Esdaile et al. (33) Class IV LN Marked subendothelial immune
deposits87 1991
Faurschou et al (35) Class III, Class VI lupus nephritis 100 2010Hill et al. (143) Presence of tubular macrophages,
karyorrhexis/fibrinoid necrosis, cellular crescents71 2001
Kojo et al. (39) Cellular crescents, fibrous crescents, segmental sclerosis
99 2009
Magil et al (144) Presence of karyorrhexis 45 1988Makino et al. (30) Karyorrhexis associated with response to high
dose steroids60 1993
Miranda et al. (31) Glomerular thrombosis strongly associated with crescents, glomerular necrosis and increased AI
108 1994
Moroni et al (145) CI > 2 93 2007Mosca et al. (26) AI 9+, CI 4+ 81 1997Nossent et al (38) AI 12+, CI 4+ 116 1990Parichatikanond et al (37)
>25% sclerotic glomeruli, >25% tubular atrophy, >25% interstitital mononuclear, infiltrate
81 1997
Yokoyama et al. (23) Class IV(S &G), ESRF in patients with IV(S or G) vs I, II, III, V (40.9% vs 2.6%)
60 2004
AI = activity index, CI = chronicity index, RVL = renal vascular lesion, LN = lupus nephritis

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Tabl
e 5.
RC
T In
clus
ion/
Excl
usio
n C
riter
ia a
nd J
adad
Sco
res
Pred
niso
ne (P
red)
vs
Cyc
loph
osph
amid
(CYC
) IV
vs C
yclo
spor
in (C
SA)
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
Jada
d Sc
ore
Aus
tin e
t al,
NIH
, US
A20
09(4
4)
Dia
gnos
is o
f SLE
by
the
AC
R, a
rena
l bio
psy
that
sh
owed
typi
cal l
upus
mem
bran
ous
neph
ropa
thy
(LM
N) b
y lig
ht a
nd e
lect
ron
mic
rosc
opy,
>=
2g;/d
pr
otei
nuria
, age
>=1
2 ye
ar, i
nfor
med
con
sent
End
ocap
illar
y pr
olife
ratio
n or
sub
endo
thel
ial
elec
tron-
dens
e de
posi
ts c
hara
cter
istic
of
prol
ifera
tive
lupu
s ne
phrit
is, c
linic
al o
r his
tolo
gic
evid
ence
of n
onlu
pus
rena
l dis
ease
, cyt
otox
ic d
rug
or C
sA u
se ru
ing
the
30d
perio
d be
fore
stu
dy e
ntry
, cy
toto
xic
drug
or C
sA u
se fo
r >2w
k du
ring
the
10
wk
perio
d be
fore
stu
dy e
ntry
, cyt
otox
ic d
rug
or C
sA
use
for >
10 w
k at
any
time
in th
e pa
st, r
equi
rem
ent
for c
ortic
oste
roid
s in
dos
age
>20
mg/
m2
body
su
rface
are
a pe
r day
of p
redn
ison
e (o
r equ
ival
ent)
for c
ontro
l of e
xtra
rena
l dis
ease
at t
he ti
me
of s
tudy
en
try, a
ctiv
e or
chr
onic
infe
ctio
n (in
clud
ing
HIV
in
fect
ion)
, pre
exis
tent
mal
igna
ncy,
pre
gnan
cy in
fe
mal
e pa
tient
s, n
ursi
ng m
othe
rs, f
emal
e pa
tient
s w
ho w
ere
not p
ract
icin
g bi
rth c
ontro
l, a
sing
le
func
tioni
ng k
idne
y, in
sulin
-trea
ted
diab
etes
, GFR
<2
5ml/m
in p
er 1
.73m
2 bo
dy s
urfa
ce a
rea
at s
tudy
en
try, a
nd h
isto
ry o
f alle
rgy
or to
xici
ty to
cy
clop
hosp
ham
ide
or C
sA.
1
Cyc
losp
orin
(CSA
) vs
Cyc
loph
osph
amid
e (C
YC) I
VA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
eZa
vada
et a
l, C
YCLO
FA-
LUN
E s
tudy
, C
zech
R
epub
lic,
2010
(146
)
Dia
gnos
is o
f SLE
(mee
ting
4 cr
iteria
of t
he A
CR
), re
nal b
iops
y do
cum
entin
g lu
pus
neph
ritis
acc
ordi
ng
to W
HO
or I
SN
/RPS
as
prol
ifera
tive
glom
erul
onep
hriti
s cl
ass
III (f
ocal
) or I
V (d
iffus
e);
clin
ical
act
ivity
as
defin
ed b
y pr
esen
ce o
f at l
east
2
of th
e fo
llow
ing:
abn
orm
al p
rote
inur
ia (m
ore
than
Trea
tmen
t with
CP
H o
r Cyc
losp
orin
eve
r bef
ore,
tre
atm
ent w
ith o
ther
imm
unos
uppr
essi
ve d
rugs
or
high
-dos
e gl
ucoc
ortic
oids
with
in th
e la
st 3
mon
ths,
pe
rsis
tent
ele
vatio
n of
ser
um c
reat
inin
e (>
=140
mic
rom
ol/l)
, pre
gnan
cy o
r lac
tatio
n, b
one
mar
row
insu
ffici
ency
with
cyt
open
ias
not
3

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Cyc
losp
orin
(CSA
) vs
Cyc
loph
osph
amid
e (C
YC) I
VA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
e50
0mg
of p
rote
in in
a 2
4-h
urin
e sp
ecim
en),
abno
rmal
mic
rosc
opic
hem
atur
ia, o
r C3
hypo
com
plem
ente
mia
(the
latte
r tw
o w
ere
defin
ed
acco
rdin
g to
the
norm
s in
the
labo
rato
ries
of th
e pa
rtici
patin
g ce
nter
)
attri
buta
ble
to S
LE, a
nd s
ever
e co
exis
ting
cond
ition
s, s
uch
as in
fect
ion,
live
r dis
ease
, act
ive
pept
ic u
lcer
,etc
.
Pred
niso
ne (P
red)
vs
Aza
thio
prin
e (A
ZA) v
s C
yclo
phos
pham
ide
(CYC
)A
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
e
Ste
inbe
rg a
nd
Dec
ker,
NIH
, US
A,
1974
(147
)
Dia
gnos
is o
f SLE
by
crite
ria o
f AR
A, o
ne o
f the
cr
iteria
requ
ired
was
pos
itive
LE
cel
l tes
t in
the
cour
se o
f the
dis
ease
, kid
ney
dise
ase
unac
coun
ted
for b
y ot
her p
atho
logi
c pr
oces
ses,
with
at l
east
one
of
the
follo
win
g: re
d ce
ll ca
sts
in a
fres
h ce
ntrif
uged
ur
ine
sedi
men
t; ce
llula
r cas
ts a
nd e
ither
hem
atur
ia
(20
RB
C/h
pf) o
r pyr
uia
(20
WBC
/hpf
), pr
otei
nuria
of
at le
ast 1
g/24
hr,
or th
e co
mbi
natio
n of
hig
h se
rum
tit
ers
of a
nti-D
NA
bin
ding
act
ivity
, low
ser
um
com
plem
ent a
nd a
pos
itive
rena
l bio
psy,
rena
l bi
opsy
dem
onst
ratin
g di
ffuse
glo
mer
ulon
ephr
itis
with
at l
east
a p
ortio
n of
all
glom
erul
i inv
olve
d.
A m
ajor
infe
ctio
n w
ithin
the
prec
edin
g 2
wee
ks.
Pre
gnan
cy.
Imm
unos
uppr
essi
ve th
erap
y w
ithin
2
mon
ths.
Sev
ere
liver
dis
ease
. A h
isto
ry o
f hy
pers
ensi
tivity
to a
stu
dy d
rug,
or a
ser
um
crea
tinin
e gr
eate
r tha
n 4.
0mg%
(cre
atin
ine
clea
ranc
e <2
0ml/m
in)
4
Car
ette
et a
l, N
IH, U
SA
,19
83(1
48)
Dia
gnos
is o
f SLE
by
ARA
pre
limin
ary
crite
ria,
posi
tive
lupu
s er
ythe
mat
osus
cel
l tes
t, an
d ki
dney
di
seas
e un
acco
unte
d fo
r by
othe
r pat
holo
gic
proc
esse
s w
ith a
t lea
st o
ne o
f the
follo
win
g: r
ed
cell
cast
s in
a fr
esh
cent
rifug
ed u
rine
sedi
men
t; ce
llula
r cas
ts a
nd e
ither
hem
atur
ia (t
en
eryt
hroc
ytes
per
hig
h po
wer
fiel
d) o
r pyu
ria (t
en
leuk
ocyt
es p
er h
igh
pow
er fi
eld)
in th
e ab
senc
e of
in
fect
ion;
pro
tein
uria
of a
t lea
st 1
g/d
or t
he
com
bina
tion
of h
igh
seru
m D
NA
bin
ding
act
ivity
, lo
w s
erum
com
plem
ent a
nd re
nal b
iops
y re
sults
co
nsis
tent
with
lupu
s gl
omer
ulon
ephr
itis
A m
ajor
infe
ctio
n w
ithin
the
prec
edin
g 2
wee
ks,
preg
nanc
y, im
mun
osup
pres
sive
ther
apy
with
in 2
m
onth
s, s
ever
e liv
er d
isea
se, a
his
tory
of
hype
rsen
sitiv
ity to
a s
tudy
dru
g, o
r a s
erum
cr
eatin
ine
grea
ter t
han
4.0m
g% (c
reat
inin
e cl
eara
nce
<20m
l/min
)
1
Aus
tin e
t al,
Dia
gnos
is o
f SLE
as
defin
ed b
y A
RA
, clin
ical
or
Cre
atin
ine
clea
ranc
e co
nsis
tent
ly le
ss th
an 2
0ml
1

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Pred
niso
ne (P
red)
vs
Aza
thio
prin
e (A
ZA) v
s C
yclo
phos
pham
ide
(CYC
)A
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
eN
IH, U
SA
,19
86(1
49)
hist
olog
ic e
vide
nce
of a
ctiv
e lu
pus
glom
erul
onep
hriti
s, a
nd in
form
ed c
onse
nt to
all
aspe
cts
of th
e st
udy.
per m
inut
e, m
ajor
infe
ctio
n w
ithin
2 w
eek
s of
stu
dy
entry
, pre
gnan
cy, a
leuk
ocyt
e co
unt o
f les
s th
an
2000
per
cub
ic m
illim
eter
, cyt
otox
ic-d
rug
ther
apy
with
in e
ight
wee
ks, a
nd s
ensi
tivity
to th
e st
udy
drug
Ste
inbe
rg a
nd
Ste
inbe
rg,
NIH
, US
A,
1991
(150
)
Dia
gnos
is o
f sys
tem
ic lu
pus
eryt
hem
atos
us a
nd
clin
ical
/his
tolo
gic
evid
ence
of a
ctiv
e lu
pus
glom
erul
onep
hriti
s.
Cre
atin
ine
clea
ranc
e co
nsis
tent
ly <
20m
l/min
ute,
pr
esen
ce o
f a m
ajor
infe
ctio
n w
ithin
the
prev
ious
2
wee
ks, p
regn
ancy
, whi
te b
lood
cel
l cou
nt
<200
0/m
m3,
trea
tmen
t with
a c
ytot
oxic
dru
g w
ithin
th
e pr
evio
us 8
wee
ks, o
r kno
wn
sens
itivi
ty to
any
st
udy
drug
.
2
Gro
otsc
holte
n et
al,
Net
herla
nds
Nep
hrol
ogy,
20
06(1
51)
The
pres
ence
of >
=4 A
CR
crit
eria
for S
LE, a
ge 1
8 to
60
year
s, c
reat
inin
e cl
eara
nce
(Coc
kcro
ft-G
ault)
>2
5ml/m
in, a
nd b
iops
y-pr
oven
pro
lifer
ativ
e LN
. Fo
r pa
tient
s al
read
y kn
own
to h
ave
prol
ifera
tive
LN, t
hela
st re
nal b
iops
y ha
d to
be
perfo
rmed
less
than
one
ye
ar b
efor
e. P
atie
nts
with
WH
O-c
lass
IV o
r Vd
LN
wer
e el
igib
le w
hen
they
had
sig
ns o
f act
ive
neph
ritis
or a
det
erio
ratio
n of
rena
l fun
ctio
n.
Pat
ient
s w
ith W
HO
-cla
ss II
I or V
c LN
had
to m
eet
both
crit
eria
.
Pat
ient
s w
ith m
embr
anou
s LN
WH
O-c
lass
Va
or V
b w
ere
excl
uded
.. D
eclin
e in
rena
l fun
ctio
n (m
ore
than
30%
incr
ease
in s
erum
cre
atin
ine)
dur
ing
treat
men
t with
cyt
otox
ic im
mun
osup
pres
sive
age
nts
in th
e m
onth
bef
ore
incl
usio
n. A
ctiv
e in
fect
ion.
M
alig
nanc
y <5
yea
rs b
efor
e ra
ndom
izat
ion.
P
regn
ancy
or r
efus
al to
use
relia
ble
cont
race
ptiv
es
durin
g th
e fir
st 2
.5 y
ears
of t
reat
men
t. C
hron
ic
activ
e or
per
sist
ing
hepa
titis
or c
irrho
sis
of th
e liv
er,
activ
e pe
ptic
ulc
er, l
euko
cyto
peni
a (<
3.0x
10 9
/l) o
r th
rom
bocy
tope
nia
(<10
0 x
10 9
/l), w
ith s
uppr
esse
d bo
ne m
arro
w (a
s sh
own
in a
bon
e m
arro
w
aspi
rate
). K
now
n al
lerg
y fo
r aza
thio
prin
e or
cy
clop
hosp
ham
ide.
2
Pred
niso
ne (P
red)
vs
Cyc
loph
osph
amid
e (C
YC) I
VA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
e
Bou
mpa
s et
al
, NIH
, US
A19
92(1
52)
Pat
ient
s ha
d 4
or m
ore
crite
ria fo
r SLE
and
sev
ere
lupu
s ne
phrit
is d
efin
ed b
y a
neph
ritic
urin
e se
dim
ent a
nd im
paire
d re
nal f
unct
ion
with
a
crea
tinin
e cl
eara
nce
betw
een
25 a
nd 8
0 m
l per
m
in.
If cr
eatin
ine
clea
ranc
e w
as h
ighe
r tha
n 80
ml
per m
in, t
he c
andi
date
had
to h
ave
very
act
ive
rena
l his
tolo
gy w
ith c
resc
ents
or n
ecro
sis
in m
ore
Pre
gnan
cy o
r had
rece
ived
cyt
otox
ic d
rug
ther
apy
for m
ore
than
10
wee
ks a
t any
tim
e, a
ctiv
e in
fect
ions
, ins
ulin
-dep
ende
nt d
iabe
tes,
or p
revi
ous
mal
igna
ncy.
2

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Pred
niso
ne (P
red)
vs
Aza
thio
prin
e (A
ZA) v
s C
yclo
phos
pham
ide
(CYC
)A
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
eth
an 2
5% o
f glo
mer
uli.
Ren
al b
iops
ies
wer
e ev
alua
ted
by li
ght a
nd e
lect
ron
mic
rosc
opy.
Gou
rley
et a
l, N
IH, U
SA
,19
96(1
53)
Pat
ient
s ha
d to
hav
e bo
th g
lom
erul
onep
hriti
s an
d a
diag
nosi
s of
sys
tem
ic lu
pus
eryt
hem
atos
us.
Glo
mer
ulon
ephr
itis
was
def
ined
as
a se
dim
ent o
n tw
o or
mor
e ur
ianl
yses
that
sho
wed
eith
er 1
0 or
m
ore
eryt
hroc
ytes
per
hig
h-po
wer
fiel
d or
er
ythr
ocyt
e or
leuk
ocyt
e ca
sts
(with
out e
vide
nce
of
infe
ctio
n) o
r bot
h, p
lus
hist
olog
ic e
vide
nce
of a
ctiv
e pr
olife
rativ
e lu
pus
glom
erul
onep
hriti
s on
a re
nal
biop
sy s
peci
men
obt
aine
d w
ithin
3 m
onth
s of
stu
dy
entry
(pro
vide
d th
at a
bio
psy
coul
d be
don
e sa
fely
).
Rec
eipt
of c
ytot
oxic
dru
g tre
atm
ent f
or m
ore
than
2
wee
ks d
urin
g th
e 6
wee
ks b
efor
e st
udy
entry
or
rece
ipt o
f cyl
opho
spha
mid
e th
erap
y fo
r mor
e th
an
10 w
eeks
at a
ny ti
me;
rece
ipt o
f pul
se th
erap
y w
ith
corti
cost
eroi
ds d
urin
g th
e 6
wee
ks b
efor
e st
udy
entry
; nee
d (a
t the
tim
eof
stu
dy e
ntry
_ fo
r ora
l co
rtico
ster
oids
in d
osag
es g
reat
er th
an 0
.5m
g of
a
pred
niso
ne e
quiv
alen
t per
kilo
gram
of b
ody
wei
ght
per d
ay to
con
trol e
xtra
rena
l dis
ease
; act
ive
or
chro
nic
infe
ctio
n; p
regn
ancy
; the
pre
senc
e of
onl
y on
e ki
dney
; ins
ulin
-dep
ende
ntdi
abet
es m
ellit
us;
and
alle
rgy
to m
ethy
pred
niso
lone
or
cylo
phos
pham
ide.
2
Pred
niso
ne (P
red)
vs
Cyc
loph
osph
amid
e (C
YC) P
OA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
e
Don
adio
et
al, M
ayo,
U
SA
,19
76(1
54)
Clin
ical
dia
gnos
is o
f SLE
and
fulfi
lled
4 or
mor
e of
th
e cr
iteria
for t
he c
lass
ifica
tion
of S
LE a
s de
velo
ped
by th
e A
RA
Com
mitt
ee o
n D
iagn
ostic
an
d Th
erap
eutic
Crit
eria
. Se
rolo
gic
conf
irmat
ion
of
the
dise
ase
was
als
o re
quire
d, b
ased
on
findi
ng o
f a
posi
tive
LE-c
ell p
repa
ratio
n an
d an
AN
A in
a ti
ter
>= 1
:32
–or
if a
pos
itive
LE
-cel
l pre
para
tion
was
no
t obt
aine
d, o
n fin
ding
two
doub
tful p
ositi
ve (f
or
exam
ple,
rose
ttes
of n
eutro
phils
or n
ucle
olys
is) a
nd
an A
NA
titer
>=
1:32
. In
add
ition
, wor
king
crit
eria
defin
ing
prog
ress
ive
lupu
s gl
omer
ulon
ephr
itis
on
the
basi
s of
rena
l ins
uffic
ienc
y ba
sed
eith
er o
n re
duce
d in
itial
cre
atin
ine
clea
ranc
e to
less
than
80
ml/m
in p
er 1
.73m
2 or
on
a 25
% re
duct
ion
in
crea
tinin
e cl
eara
nce
as c
ompa
red
to in
itial
Cyc
loph
osph
amid
e ha
d be
en u
sed
in th
e pa
st o
r if
othe
r im
mun
osup
pres
sive
dru
gs h
ad b
een
used
w
ithin
6 m
onth
s of
ent
ry in
to th
e st
udy.
2
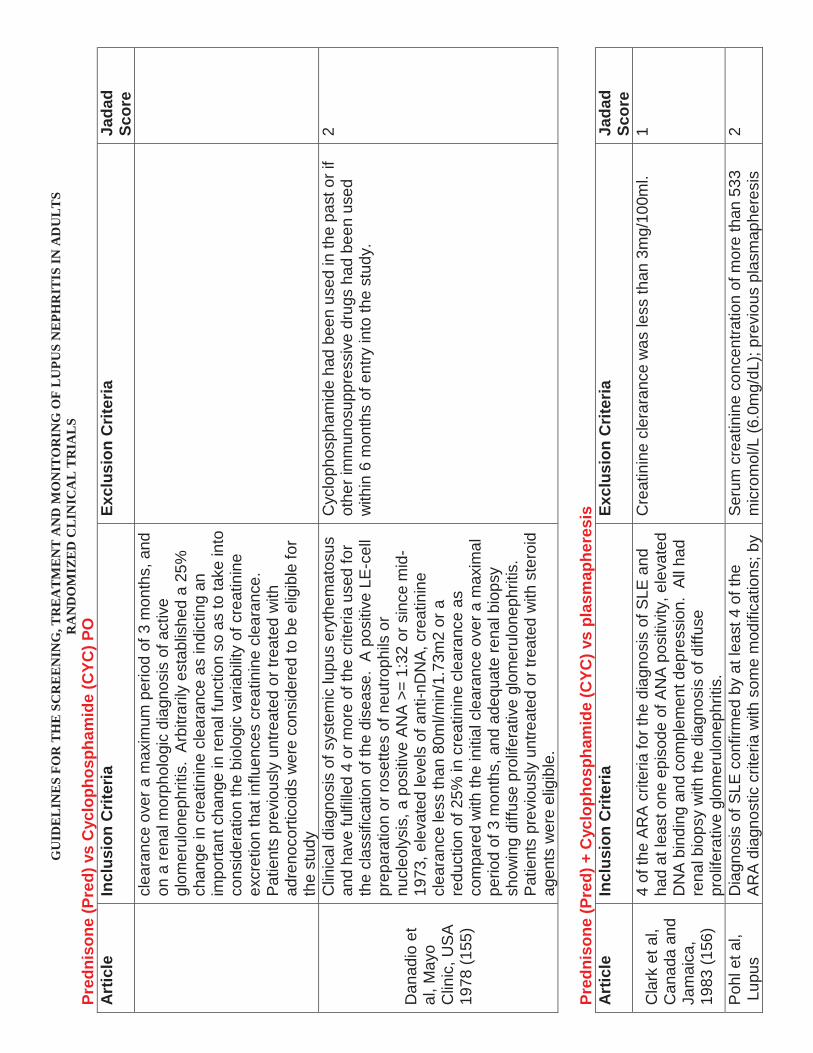
GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Pred
niso
ne (P
red)
vs
Cyc
loph
osph
amid
e (C
YC) P
OA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
ecl
eara
nce
over
am
axim
um p
erio
d of
3 m
onth
s, a
nd
on a
rena
l mor
phol
ogic
dia
gnos
is o
f act
ive
glom
erul
onep
hriti
s. A
rbitr
arily
est
ablis
hed
a 25
%
chan
ge in
cre
atin
ine
clea
ranc
e as
indi
ctin
g an
im
porta
nt c
hang
e in
rena
l fun
ctio
n so
as
to ta
ke in
to
cons
ider
atio
n th
e bi
olog
ic v
aria
bilit
y of
cre
atin
ine
excr
etio
n th
at in
fluen
ces
crea
tinin
e cl
eara
nce.
P
atie
nts
prev
ious
ly u
ntre
ated
or t
reat
ed w
ith
adre
noco
rtico
ids
wer
e co
nsid
ered
to b
e el
igib
le fo
r th
e st
udy
Dan
adio
et
al, M
ayo
Clin
ic, U
SA
19
78(1
55)
Clin
ical
dia
gnos
is o
f sys
tem
ic lu
pus
eryt
hem
atos
us
and
have
fulfi
lled
4 or
mor
e of
the
crite
ria u
sed
for
the
clas
sific
atio
n of
the
dise
ase.
A p
ositi
ve L
E-c
ell
prep
arat
ion
or ro
sette
s of
neu
troph
ils o
r nu
cleo
lysi
s, a
pos
itive
AN
A >
= 1:
32 o
r sin
ce m
id-
1973
, ele
vate
d le
vels
of a
nti-n
DN
A, c
reat
inin
e cl
eara
nce
less
than
80m
l/min
/1.7
3m2
or a
re
duct
ion
of 2
5% in
cre
atin
ine
clea
ranc
e as
co
mpa
red
with
the
initi
al c
lear
ance
ove
r a m
axim
al
perio
d of
3 m
onth
s, a
nd a
dequ
ate
rena
l bio
psy
show
ing
diffu
se p
rolif
erat
ive
glom
erul
onep
hriti
s.
Pat
ient
s pr
evio
usly
unt
reat
ed o
r tre
ated
with
ste
roid
ag
ents
wer
e el
igib
le.
Cyc
loph
osph
amid
e ha
d be
en u
sed
in th
e pa
st o
r if
othe
r im
mun
osup
pres
sive
dru
gs h
ad b
een
used
w
ithin
6 m
onth
s of
ent
ry in
to th
e st
udy.
2
Pred
niso
ne (P
red)
+ C
yclo
phos
pham
ide
(CYC
) vs
plas
map
here
sis
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
Jada
d Sc
ore
Cla
rk e
t al,
C
anad
a an
d Ja
mai
ca,
1983
(156
)
4 of
the
AR
A c
riter
ia fo
r the
dia
gnos
is o
f SLE
and
ha
d at
leas
t one
epi
sode
of A
NA
pos
itivi
ty, e
leva
ted
DN
A b
indi
ng a
nd c
ompl
emen
t dep
ress
ion.
All
had
rena
l bio
psy
with
the
diag
nosi
s of
diff
use
prol
ifera
tive
glom
erul
onep
hriti
s.
Cre
atin
ine
cler
aran
ce w
as le
ss th
an 3
mg/
100m
l.1
Poh
l et a
l,Lu
pus
Dia
gnos
is o
f SLE
con
firm
ed b
y at
leas
t 4 o
f the
A
RA
dia
gnos
tic c
riter
ia w
ith s
ome
mod
ifica
tions
; by
Ser
um c
reat
inin
e co
ncen
tratio
n of
mor
e th
an 5
33
mic
rom
ol/L
(6.0
mg/
dL);
prev
ious
pla
smap
here
sis
2

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Pred
niso
ne (P
red)
+ C
yclo
phos
pham
ide
(CYC
) vs
plas
map
here
sis
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
Jada
d Sc
ore
Nep
hriti
s C
olla
bora
tive
Stu
dy G
roup
, N
IH, U
SA
,19
91(1
57)
curre
nt re
nal b
iops
y ev
iden
ce o
f sev
ere
lupu
s gl
omer
ulon
ephr
itis
(WH
O C
lass
III o
r IV
with
mor
e th
an 5
0% o
f glo
mer
uli i
nvol
ved
or c
lass
V w
ith
supe
rimpo
sed
diffu
se o
r sev
ere
segm
enta
l pr
olife
ratio
n)
for a
ny re
ason
; a h
isto
ry o
f ste
roid
psy
chos
is;
curre
nt p
regn
ancy
; a h
isto
ry o
f neo
plas
m w
ithin
the
prev
ious
5 y
ears
; a n
eutro
phil
coun
t of l
ess
than
1500
/mm
3; o
r age
of l
ess
than
16
year
s.
Lew
is e
t al,
Lupu
s N
ephr
itis
Col
labo
rativ
e G
roup
, US
A,
1992
(158
)
16 y
ears
of a
ge o
r old
er; d
iagn
osis
of S
LE a
s de
fined
by
AR
A a
nd a
qua
lifyi
ng re
nal b
iops
y.P
regn
ancy
, ser
um c
reat
inin
e co
ncen
tratio
n ab
ove
530
mic
rom
ol p
er li
ter (
6mg/
dL),
prev
ious
trea
tmen
t w
ith p
lasm
aphe
resi
s, a
his
tory
of p
rimar
y m
yoca
rdia
l dis
ease
, a h
isto
ry o
f can
cer w
ithin
the
past
5 y
ears
, pre
dnis
one-
asso
ciat
ed p
sych
osis
, pe
ptic
ulc
er d
isas
e, a
nd a
ctiv
e liv
er d
isea
se.
3
Cyc
loph
osph
amid
e (C
YC) I
V vs
Cyc
loph
osph
amid
e (C
YC) P
OA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
e
Mok
et a
l, H
ong
Kon
g,
2001
(159
)
Fulfi
lled
at l
east
4 o
f the
AC
R c
riter
ia fo
r the
cl
assi
ficat
ion
of S
LE a
nd h
ad D
PGN
(WH
O C
lass
IV
a or
IVb)
dia
gnos
ed a
nd tr
eate
d in
two
larg
e re
gion
al h
ospi
tals
in H
ong
Kon
g (Q
ueen
Mar
y an
d Te
n M
un H
ospi
tals
) bet
wee
n 19
95 a
nd 1
998
wer
e in
clud
ed in
this
stu
dy.
Ref
used
CYC
trea
tmen
t or i
n w
hom
rena
l bio
psy
show
ed s
igni
fican
t scl
eros
is o
r chr
onic
cha
nges
but
w
ithou
t act
ivity
wer
e ex
clud
ed.
0
Hig
h-D
ose
Cyc
loph
osph
amid
e (C
YC) I
V vs
Low
Dos
e C
yclo
phos
pham
ide
(CYC
) IV
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
Jada
d Sc
ore
Hou
ssia
u et
al
, Eur
o-Lu
pus
Nep
hriti
s Tr
ial,
2002
(160
)
Dia
gnos
is o
f SLE
acc
ordi
ng to
the
AC
R c
riter
ia,
age
>= 1
4 ye
ars,
bio
psy
prov
en p
rolif
erat
ive
lupu
s gl
omer
ulon
ephr
itis
(WH
O C
lass
II, I
V, V
c, o
r Vd)
, an
d pr
otei
nuria
>= 5
00m
g in
24
hour
s.
Pat
ient
s w
ho h
ad ta
ken
CYC
or A
ZA d
urin
g th
e pr
evio
us y
ear o
r had
take
n >=
15m
g/da
y pr
edni
sone
(o
r equ
ival
ent)
durin
g th
e pr
evio
us m
onth
wer
e ex
clud
ed (e
xcep
t for
a c
ours
e of
glu
coco
rtico
ids
for
a m
axim
um o
f 10
days
bef
ore
the
refe
rral).
Oth
er
excl
usio
n cr
iteria
wer
e re
nal t
hrom
botic
m
icro
angi
opat
hy, p
reex
istin
g ch
roni
c re
nal f
ailu
re,
preg
nanc
y, p
revi
ous
mal
igna
ncy
(exc
ept s
kin
and
cerv
ical
intra
epith
elia
l neo
plas
is),
diab
etes
mel
litus
,
2

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Hig
h-D
ose
Cyc
loph
osph
amid
e (C
YC) I
V vs
Low
Dos
e C
yclo
phos
pham
ide
(CYC
) IV
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
Jada
d Sc
ore
prev
ious
ly d
ocum
ente
d se
vere
toxi
city
to
imm
unos
uppr
essi
ve d
rugs
, and
ant
icip
ated
poo
r co
mpl
ianc
e w
ith th
e pr
otoc
ol.
Myc
ophe
nola
te M
ofet
il (M
MF)
+ T
acro
limus
vs
Cyc
loph
osph
amid
e (C
YC) I
VA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
e
Bao
et a
l, N
anjin
g,20
08(1
61)
Elig
ible
pat
ient
s w
ere
eith
er g
ende
r and
bet
wee
n 12
and
60
yr o
f age
; pro
vide
d w
ritte
n in
form
ed
cons
ent;
diag
nosi
s of
SLE
acc
ordi
ng fo
r AC
R
(199
7); s
how
ed a
n SL
E d
isea
se a
ctiv
ity in
dex
>=12
; had
a d
iagn
osis
of C
lass
V+I
V LN
acc
ordi
ng
to IS
N/R
PS 2
003
clas
sific
atio
n of
LN
, with
a
path
olog
ic c
hron
ic in
dex
(CI)
<4 p
rove
d by
ligh
t, im
mun
oflu
ores
cenc
e, a
nd e
lect
ron
mic
rosc
opy
with
in 3
wk
befo
re e
nrol
lmen
t; an
d ex
hibi
ted
over
t pr
otei
nuria
(>=1
.5g
of p
rote
in in
a 2
4-h
urin
e sp
ecim
en) w
ith o
r with
out a
ctiv
e ur
inar
y se
dim
ent
(any
of u
rine
sedi
men
t RB
C c
ount
>10
x 1
0 4/
ml o
r w
hite
blo
od c
ells
> 5
per
hig
h-po
wer
fiel
d or
red
cell
cast
s in
the
abse
nce
of in
fect
ion
or o
ther
cau
ses.
Ser
um c
reat
inin
e >
3.0m
g/dl
(265
.2 m
icro
lmol
/L) o
r es
timat
ed C
reat
inin
e cl
eara
nce
<30m
l/min
per
1.
73m
2 on
repe
ated
test
ing;
live
r fun
ctio
n w
ith A
LT,
AS
ST, o
r bilir
ubin
gre
ater
than
twic
e th
e up
per l
imit
of th
e re
fere
nce
rang
e; a
bnor
mal
glu
cose
m
etab
olis
m, d
efin
ed a
s a
fast
ing
(i.e.
, no
calo
ric
inta
ke fo
r at l
east
8 h
) pla
sem
a gl
ucos
e le
vel >
6.1
m
mol
/L a
nd/o
r a 2
-h p
lasm
a gl
ucos
e le
vel >
7.8
m
mol
/L; k
now
n hy
pers
ensi
tivity
or c
ontra
indi
catio
n to
any
com
pone
nts
of th
ese
regi
men
s; u
se o
f CTX
, M
MF,
or t
acro
limus
with
in th
e pa
st 1
2 w
k;
preg
nanc
y or
lact
atio
n; li
fe-th
reat
enin
g co
mpl
icat
ions
suc
h as
cer
ebra
l lup
us; o
r oth
er
seve
re c
oexi
stin
g co
nditi
ons
prec
ludi
ng
imm
unos
uppr
essi
ve th
erap
y or
con
ditio
ns re
quiri
ng
intra
veno
us a
ntib
iotic
ther
apy.
2
Myc
ophe
nola
te M
ofet
il (M
MF)
vs
Cyc
loph
osph
amid
e (C
YC) I
VA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
e
Hu
et a
l, N
anjin
g,
2002
(162
)
Pat
ient
s ha
s SL
E d
iagn
osis
acc
ordi
ng to
AR
A
crite
ria; u
rinal
ysis
sho
wed
act
ive
urin
e se
dim
ents
,pr
otei
nuria
>2g
/d; r
enal
bio
psy
revi
ewed
lupu
s ne
phrit
is W
HO
IV w
ithin
3 m
onth
s pr
ior t
o th
e st
udy
Sev
ere
com
plic
atio
n su
ch a
s in
fect
ion,
leuc
open
ia,
hear
t fai
lure
or m
alfu
nctio
n of
the
cent
ral n
erve
sy
stem
or l
iver
-1
Ong
et a
l, M
alay
sia,
2005
(163
)
SLE
fulfi
lling
AR
A c
riter
ia w
ith W
HO
Cla
ss II
I or I
V
lupu
s ne
phrit
is, a
ged
16 y
ears
or o
lder
Ser
um c
reat
inin
e m
ore
than
200
mic
rom
ol/L
, whi
te
bloo
d ce
ll co
unt <
3.5
x 1
0 9
L, e
vide
nce
of m
ajor
in
fect
ion,
his
tory
of c
ance
r, al
coho
l or s
ubst
ance
2

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Myc
ophe
nola
te M
ofet
il (M
MF)
vs
Cyc
loph
osph
amid
e (C
YC) I
VA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
eab
use,
act
ive
pept
ic u
lcer
dis
ease
, pre
gnan
t or
lact
atin
g w
omen
, kno
wn
alle
rgy
to M
MF
or
cycl
opho
spha
mid
e an
d us
e of
stu
dy d
rugs
in th
e pr
eced
ing
6 m
onth
s.
Gin
zler
et a
l,U
SA
,20
05(1
64)
SLE
mee
ting
4 cl
assi
ficat
ion
crite
ria o
f the
AC
R;
rena
l bio
psy
docu
men
ting
lupu
s ne
phrit
is a
ccor
ding
to
the
clas
sific
atio
n of
WH
O II
I, IV
, or V
; clin
ical
ac
tivity
as
defin
ed b
y on
e or
mor
e of
the
follo
win
g:
inci
denc
e de
crea
se in
rena
l fun
ctio
n (s
erum
cr
eatin
ine,
>1m
g/dL
(88.
4 m
icro
mol
/L),
prot
einu
ria
(def
ined
as
mor
e th
an 5
00m
g of
pro
tein
in a
24-
hur
ine
spec
imen
), m
icro
scop
ic h
emat
uria
(def
ined
as
>5
red
cells
per
hig
h po
wer
-fiel
d) o
r the
pr
esen
ce o
f cel
lula
r cas
ts, i
ncre
asin
g pr
otei
nuria
w
ith ri
sing
leve
ls o
f ser
um c
reat
inin
e, a
ctiv
e ur
ine
sedi
men
t (he
mat
uria
or c
ellu
ar c
asts
), or
ser
olog
ic
abno
rmal
ity (a
nti-D
NA
ant
ibod
ies
or
hypo
com
plem
ente
mia
). T
hose
with
Cla
ss II
I or V
lu
pus
neph
ritis
wer
e re
quire
d to
hav
e a
seru
m
crea
tinin
e le
vel g
reat
er th
an 1
mg/
dL o
r pro
tein
uria
gr
eate
r tha
n 2g
in a
24-
h ur
ine
spec
imen
.
Cre
atin
ine
clea
ranc
e of
less
than
30m
l /m
in, s
erum
cr
eatin
ine
on re
peat
ed te
stin
g gr
eate
r tha
n 3m
g/dL
(2
65.2
mic
rolm
ol /L
), se
vere
coe
xist
ing
cond
ition
s pr
eclu
ding
imm
unos
uppr
essi
ve th
erap
y or
co
nditi
ons
requ
iring
intra
veno
us a
ntib
iotic
ther
apy,
pr
ior t
reat
men
t with
myc
ophe
nola
te m
ofet
il,
treat
men
t with
intra
veno
us c
yclo
phos
pham
ide
with
in th
e pa
st 1
2 m
onth
s, m
onoc
lona
l ant
ibod
y th
erap
y w
ithin
the
past
30
days
, or p
regn
ancy
or
lact
atio
n.
2
Wan
g et
al,
Nan
jing,
2007
(165
)
AR
A c
riter
ia o
f SLE
, 18-
50 y
rs o
f age
; urin
e pr
otei
n >=
1g/
24h
with
act
ive
urin
e se
dim
ent;
seru
m
crea
tinin
e <3
mg/
dL (2
65m
icro
lmol
/L) o
r cre
atin
ine
clea
ranc
e >=
30m
L/m
in, b
iops
y pr
oven
ISN
/RP
S
Cla
ss IV
with
exc
eptio
n of
sup
erim
pose
d m
embr
anou
s ch
ange
s an
d N
NV
lesi
on s
how
n in
ar
terio
les
and
inte
rlobu
lar a
rterie
s an
d th
e pr
opor
tion
of g
lom
erul
ar s
cler
osis
<50
% a
nd
chro
nic
inde
x <4
.
Ser
um c
reat
inin
e >=
3 m
g/dL
or c
reat
inin
e cl
eara
nce
<30m
L/m
in; p
ropo
rtion
of g
lom
erul
ar
scle
rosi
s >=
50%
, chr
onic
ity in
dex
>=4
with
sev
eral
re
nal t
ubul
e-in
ters
titia
l fib
rosi
s; p
rimar
y or
se
cond
ary
imm
unod
efic
ienc
y, e
spec
ially
leuk
ocyt
e co
unt o
f <=2
x 1
9 9
L; a
ny c
linic
ally
sig
nific
ant
infe
ctio
n, p
regn
ancy
or l
acta
tion,
act
ive
type
B o
r C
hepa
titis
, tub
ercu
losi
s an
d th
e re
ceip
t of C
TX,
MM
F, o
r oth
er c
ytot
oxic
dru
gs w
ithin
the
past
3
mon
ths
3
App
el e
t al,
ALM
S,
2009
(166
)
Age
d 12
to 7
5 yr
s, d
iagn
osis
of S
LE, L
N (a
ctiv
e or
ac
tive/
chro
nic)
con
form
ed b
y ki
dney
bio
psy
with
in
6 m
o be
fore
rand
omiz
atio
n as
ISN
/RP
S 2
003
Trea
tmen
t with
MM
F or
IVC
with
in th
e pr
evio
us
year
, con
tinuo
us d
ialy
sis
for ?
2 w
k be
fore
ra
ndom
izat
ion
or a
ntic
ipat
ed d
urin
g lo
nger
than
8
3

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Myc
ophe
nola
te M
ofet
il (M
MF)
vs
Cyc
loph
osph
amid
e (C
YC) I
VA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
eC
lass
III,
IV-S
or I
V-G
, V, I
II+V
, or I
V+V
. Pa
tient
s w
ith c
lass
III o
r V L
N m
ust h
ave
had
prot
einu
ria (a
t le
ast 2
g/d)
whi
ch w
as c
onsi
dere
d cl
inic
ally
si
gnifi
cant
leve
l of p
rote
inur
ia, a
nd m
ight
indi
cate
a
rece
nt d
eter
iora
tion
in re
nal f
unct
ion.
wk,
pan
crea
titis
, gas
troni
ntes
tinal
hem
orrh
age
with
in 6
mo
or a
ctiv
e pe
ptic
ulc
er w
ithin
3 m
o,
seve
re v
iral i
nfec
tion,
sev
ere
card
iova
scul
ar
dise
ase,
bon
e m
arro
w in
suffi
cien
cy w
ith c
ytop
enia
s no
t attr
ibut
able
to S
LE, o
r cur
rent
infe
ctio
n re
quiri
ng in
trave
nous
ant
ibio
tics.
Pul
se
intra
veno
us c
ortic
oste
roid
s w
ere
proh
ibite
d w
ithin
2
wk
befo
re fi
rst r
ando
miz
atio
n an
d th
roug
hout
the
stud
y.
Isen
berg
et a
l, S
ub A
naly
sis
of A
LMS
trial
,20
10(1
67)
Age
d 12
to 7
5 yr
s, d
iagn
osis
of S
LE, L
N (a
ctiv
e or
ac
tive/
chro
nic)
con
form
ed b
y ki
dney
bio
psy
with
in
6 m
o be
fore
rand
omiz
atio
n as
ISN
/RP
S 2
003
Cla
ss II
I, IV
-S o
r IV
-G, V
, III+
V, o
r IV
+V.
Patie
nts
with
cla
ss II
I or V
LN
mus
t hav
e ha
d pr
otei
nuria
(at
leas
t 2g/
d) w
hich
was
con
side
red
clin
ical
ly
sign
ifica
nt le
vel o
f pro
tein
uria
, and
mig
ht in
dica
te a
re
cent
det
erio
ratio
n in
rena
l fun
ctio
n.
Trea
tmen
t with
MM
F or
IVC
with
in th
e pr
evio
us
year
, con
tinuo
us d
ialy
sis
for ?
2 w
k be
fore
ra
ndom
izat
ion
or a
ntic
ipat
ed d
urin
g lo
nger
than
8
wk,
pan
crea
titis
, gas
troni
ntes
tinal
hem
orrh
age
with
in6
mo
or a
ctiv
e pe
ptic
ulc
er w
ithin
3 m
o,
seve
re v
iral i
nfec
tion,
sev
ere
card
iova
scul
ar
dise
ase,
bon
e m
arro
w in
suffi
cien
cy w
ith c
ytop
enia
s no
t attr
ibut
able
to S
LE, o
r cur
rent
infe
ctio
n re
quiri
ng in
trave
nous
ant
ibio
tics.
Pul
se
intra
veno
us c
ortic
oste
roid
s w
ere
proh
ibite
d w
ithin
2
wk
befo
re fi
rst r
ando
miz
atio
n an
d th
roug
hout
the
stud
y.
Rad
hakr
ishn
an
et a
l, A
LMS
+
Gin
zler
et a
l, 20
10
(NO
TE
CO
MB
INE
D 2
st
udie
s)(4
3)
Pur
e C
lass
V L
N in
clud
ed in
this
ana
lysi
s on
ly.
ALM
S-A
ged
12 to
75
yrs,
dia
gnos
is o
f SLE
, LN
(a
ctiv
e or
act
ive/
chro
nic)
con
form
ed b
y ki
dney
bi
opsy
with
in 6
mo
befo
re ra
ndom
izat
ion
as
ISN
/RP
S 2
003
Cla
ss II
I, IV
-S o
r IV
-G, V
, III+
V, o
r IV
+V.
Patie
nts
with
cla
ss II
I or V
LN
mus
t hav
e ha
d pr
otei
nuria
(at l
east
2g/
d) w
hich
was
co
nsid
ered
clin
ical
ly s
igni
fican
t lev
el o
f pro
tein
uria
, an
d m
ight
indi
cate
a re
cent
det
erio
ratio
n in
rena
l fu
nctio
n.G
INZL
ER
-S
LE m
eetin
g 4
clas
sific
atio
n cr
iteria
of
the
AC
R; r
enal
bio
psy
docu
men
ting
lupu
s ne
phrit
is
ALM
S -
Trea
tmen
t with
MM
F or
IVC
with
in th
e pr
evio
us y
ear,
cont
inuo
us d
ialy
sis
for ?
2 w
k be
fore
ra
ndom
izat
ion
or a
ntic
ipat
ed d
urin
g lo
nger
than
8
wk,
pan
crea
titis
, gas
troni
ntes
tinal
hem
orrh
age
with
in 6
mo
or a
ctiv
e pe
ptic
ulc
er w
ithin
3 m
o,
seve
re v
iral i
nfec
tion,
sev
ere
card
iova
scul
ar
dise
ase,
bon
e m
arro
w in
suffi
cien
cy w
ith c
ytop
enia
s no
t attr
ibut
able
to S
LE, o
r cur
rent
infe
ctio
n re
quiri
ng in
trave
nous
ant
ibio
tics.
Pul
se
intra
veno
us c
ortic
oste
roid
s w
ere
proh
ibite
d w
ithin
2
wk
befo
re fi
rst r
ando
miz
atio
n an
d th
roug
hout
the
stud
y.G
INZL
ER
-C
reat
inin
e cl
eara
nce
of le
ss th
an 3
0ml
2

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Myc
ophe
nola
te M
ofet
il (M
MF)
vs
Cyc
loph
osph
amid
e (C
YC) I
VA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
eac
cord
ing
to th
e cl
assi
ficat
ion
of W
HO
III,
IV, o
r V;
clin
ical
act
ivity
as
defin
ed b
y on
e or
mor
e of
the
follo
win
g: in
cide
nce
decr
ease
in re
nal f
unct
ion
(ser
um c
reat
inin
e, >
1mg/
dL (8
8.4
mic
rom
ol/L
), pr
otei
nuria
(def
ined
as
mor
e th
an 5
00m
g of
pro
tein
in
a 2
4-h
urin
e sp
ecim
en),
mic
rosc
opic
hem
atur
ia
(def
ined
as
>5 re
d ce
lls p
er h
igh
pow
er-fi
eld)
or t
he
pres
ence
of c
ellu
lar c
asts
, inc
reas
ing
prot
einu
ria
with
risi
ng le
vels
of s
erum
cre
atin
ine,
act
ive
urin
e se
dim
ent (
hem
atur
ia o
r cel
luar
cas
ts),
or s
erol
ogic
ab
norm
ality
(ant
i-DN
A a
ntib
odie
s or
hy
poco
mpl
emen
tem
ia).
Tho
se w
ith C
lass
III o
r V
lupu
s ne
phrit
is w
ere
requ
ired
to h
ave
a se
rum
cr
eatin
ine
leve
l gre
ater
than
1m
g/dL
or p
rote
inur
ia
grea
ter t
han
2g in
a 2
4-h
urin
e sp
ecim
en.
/min
, ser
um c
reat
inin
e on
repe
ated
test
ing
grea
ter
than
3m
g/dL
(265
.2 m
icro
lmol
/L),
seve
re
coex
istin
g co
nditi
ons
prec
ludi
ng
imm
unos
uppr
essi
ve th
erap
y or
con
ditio
ns re
quiri
ng
intra
veno
us a
ntib
iotic
ther
apy,
prio
r tre
atm
ent w
ith
myc
ophe
nola
te m
ofet
il, tr
eatm
ent w
ith in
trave
nous
cy
clop
hosp
ham
ide
with
in th
e pa
st 1
2 m
onth
s,
mon
oclo
nal a
ntib
ody
ther
apy
with
in th
e pa
st 3
0 da
ys, o
r pre
gnan
cy o
r lac
tatio
n.
El
Sha
fey
et
al, E
gypt
,20
10(1
68)
SLE
mee
ting
4 cl
assi
ficat
ion
crite
ria o
f the
AC
R
with
new
ly d
iagn
osed
act
ive
prol
ifera
tive
clas
s III
or
IV lu
pus
neph
ritis
and
age
d 15
yea
rs o
r old
er w
ere
enro
lled
in th
e st
udy.
Est
imat
ed g
lom
erul
ar fi
ltrat
ion
rate
(eG
FR) o
f les
s th
an 3
0ml p
er m
inut
e, s
erum
cer
eatin
ine
on
repe
ated
test
ing
mor
e th
an 2
00 m
icro
mol
/L, w
hite
bl
ood
cell
(WBC
) cou
nt o
f les
s th
an 3
.5 x
19
9/l,
evid
ence
of m
ajor
infe
ctio
n, h
isto
ry o
f can
cer,
alco
hol o
r sub
stan
ce a
buse
, act
ive
pept
ic u
lcer
di
seas
e, p
regn
ant o
r lac
tatin
g w
omen
, kno
wn
alle
rgy
to M
MF
or c
yclo
phos
pham
ide,
and
the
use
of s
tudy
dru
gs in
the
prec
edin
g 6
mon
ths.
2
MM
F +
AZA
vs
CYC
PO
+ A
ZAA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
e
Cha
n et
al,
Hon
g K
ong,
20
00(1
69)
SLE
acc
ordi
ng to
AR
A in
clud
ing
rena
l-bio
psy
evid
ence
of d
iffus
e pr
olife
rativ
e lu
pus
neph
ritis
(W
HO
IV),
urin
ary
prot
ein
excr
etio
n of
1g
or m
ore
per 2
4 ho
urs,
ser
um a
lbum
in c
once
ntra
tion
of
Ser
um c
reat
inin
e co
ncen
tratio
n hi
gher
than
3.
4mg/
dL (3
00 m
icro
mol
per
lite
r); li
fe-th
reat
enin
g co
mpl
icat
ions
suc
h as
cer
ebra
l lup
us o
r sev
ere
infe
ctio
n, h
isto
ry o
f poo
r com
plia
nce
with
dru
g
2

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
MM
F +
AZA
vs
CYC
PO
+ A
ZAA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
e3.
5g/d
L or
less
. re
gim
ens,
wom
en w
ho w
ere
preg
nant
or u
nwill
ing
to u
se c
ontra
cept
ion.
Pat
ient
s w
ho h
ad re
ceiv
ed
cycl
opho
spha
mid
e w
ithin
the
prev
ious
6 m
onth
s or
w
ho h
ad ta
ken
oral
pre
dnis
olon
e at
ado
se o
f 0.
8mg/
kg o
f bod
y w
eigh
t per
day
or m
ore
for m
ore
than
2 w
eeks
.
Cha
n et
al,
Hon
g K
ong,
20
05(1
70)
SLE
def
ined
by
1982
AR
A c
riter
ia, r
enal
bio
psy
show
ing
diffu
se p
rolif
erat
ive
lupu
s ne
phrit
is (W
HO
C
lass
IV) w
hich
cor
resp
onde
d to
200
3 IS
N/R
PS
cl
ass
IV-S
or I
V-G
, urin
ary
prot
ein
exre
tion
of 1
g/24
ho
urs
or a
bove
, and
ser
um a
lbum
in c
once
ntra
tion
<35g
/L.
Ser
um c
reat
inin
e co
ncen
tratio
n >4
.52
mg/
dL
(400
mic
rom
ol/L
), lif
e-th
reat
enin
g co
mpl
icat
ions
su
ch a
s ce
rebr
al lu
pus
or s
ever
e in
fect
ion,
poo
r dr
ug c
ompl
ianc
e, tr
eatm
ent w
ith C
TX o
r MM
F w
ithin
6 m
o be
fore
bas
elin
e, o
r tre
atm
ent w
ith
pred
niso
lone
at d
ose
>0.4
mg/
kg p
er d
ora
lly fo
r >2
wk
befo
re b
asel
ine.
3
MM
F vs
AZA
vs
CYC
IVA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
e
Con
trera
s et
al
,U
SA
,20
04(1
71)
SLE
acc
ordi
ng to
AR
A w
ho h
ad u
nder
gone
a
kidn
ey b
iops
y. 1
8 ye
ars
of a
ge o
r old
er.
His
tolo
gic
diag
nosi
s of
pro
lifer
ativ
e lu
pus
neph
ritis
(WH
O
Cla
ss II
I, IV
, or V
b)
Cre
atin
ine
clea
ranc
e th
at w
as c
onsi
sten
tly le
ss
than
20m
l/min
, any
clin
ical
ly s
igni
fican
t inf
ectio
n,
preg
nanc
y, re
ceip
t ofm
ore
than
7 d
oses
of
intra
veno
us c
yclo
phos
pham
ide,
or t
he re
ceip
t of
azat
hiop
rine
for l
onge
r tha
n 8
wee
ks.
2
MM
F vs
AZA
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
Jada
dSc
ore
Hou
ssia
u et
al
, M
AIN
TAIN
N
ephr
itis
Tria
l, 20
10(d
iffer
ent
coho
rt fro
m
ELN
T)(1
72)
Age
>=1
4 ye
ars,
SLE
acc
ordi
ng to
AC
R
clas
sific
atio
n cr
iteria
, 24h
pro
tein
uria
>=
500m
g,
biop
sy –
prov
en W
HO
Cla
ss II
I, IV
, Vc
or V
d lu
pus
glom
erul
onep
hriti
s (b
iops
y pe
rform
ed le
ss th
an 1
m
onth
bef
ore
entry
to p
roto
col),
con
trace
ptio
n (o
r se
xual
abs
tinen
ce)
Non
-lupu
s re
late
d re
nal d
isea
se (s
uch
as
mic
roth
rom
botic
dis
ease
ass
ocia
ted
with
an
tipho
spho
lipid
syn
drom
e),tr
eatm
ent w
ith
gluc
ocor
ticoi
ds (G
Cs)
(>15
mg
equi
vale
nt
pred
niso
lone
/day
) in
the
last
mon
th b
efor
e en
try
into
t he
stud
y (e
xcep
t a v
ery
shor
t-cou
rse
high
-do
se o
ral G
C tr
eatm
ent b
efor
e re
ferra
l), tr
eatm
ent
with
CY,
AZA
, MM
F, o
r cyc
losp
orin
e A
in th
e
3

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
MM
F vs
AZA
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
Jada
dSc
ore
prev
ious
yea
r, pr
e-ex
istin
g ch
roni
c re
nal f
ailu
re
(def
ined
as
a se
rum
cre
atin
ine
valu
e ab
ove
the
uppe
r nor
mal
val
ue fo
r the
loca
l lab
orat
ory)
due
to
a pr
evio
us e
piso
de o
f LN
or o
ther
cau
se,
preg
nanc
y, b
reas
t fee
ding
, pre
viou
s m
alig
nanc
y (e
xcep
t for
ski
n an
d ce
rvic
al in
traep
ithel
ial
neop
lasi
as),
diab
etes
mel
litus
, pre
viou
sly
docu
men
ted
seve
re to
xici
ty o
f im
mun
osup
pres
sant
s, a
ntic
ipat
ed n
on-c
ompl
ianc
e w
ith th
e pr
otoc
ol.
Abs
tract
A
LMS
M
aint
enan
ce
(Wof
sy e
t al,
2010
)
0
Leflu
nom
ide
vs C
YC IV
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
Jada
dSc
ore
Wan
g et
al,
Leflu
nom
id
Lupu
s N
ephr
itis
Stu
dy G
roup
,C
hina
,20
08(1
73)
SLE
acc
ordi
ng to
199
7 A
CR
crit
eria
; SLE
DA
I >=
8;
clin
ical
ly e
vide
nt re
nal d
isea
se a
nd b
iops
y-do
cum
ente
d di
ffuse
pro
lifer
ativ
e or
foca
l pr
olife
rativ
e lu
pus
neph
ritis
(IS
N/R
PS
200
3 Ty
pe IV
A
or A
/C a
nd T
ype
III A
or A
/C) w
ith o
r with
out
coin
cide
nt m
embr
anou
s ne
phro
path
y an
d pa
thol
ogic
al a
ctiv
ity in
dex
(AI)
>=4.
Rec
eive
d cy
clop
hosp
ham
ide
with
in th
e pr
evio
us 3
m
onth
s. C
ereb
ral l
upus
, sev
ere
infe
ctio
n, li
ver
dise
ase,
pre
gnan
cy, a
nd a
ntic
ipat
ed p
oor
com
plia
nce
with
the
prot
ocol
.
0
Ritu
xim
abA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
eA
BST
RA
CT
-Fur
ie e
t al,
LUN
AR
,20
09
Pts
with
Cla
ss II
I/IV
LN
and
urin
e pr
otei
n to
cr
eatin
ine
ratio
>1

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Bel
imum
abA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
eA
BST
RA
CT
-Man
zi e
t al,
BLI
SS
2010
Ser
opos
itive
(AN
A >
=1:3
0 an
d/or
ant
i-dsD
NA
>=3
0 IU
/mL)
SLE
with
SEL
ENA
SLE
DAI
>=6
on
stab
le
stan
dard
-of –
care
ther
apy
ofr >
=30d
wer
e en
rolle
d
No
activ
e LN
Toci
lizum
abA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
e
Illei
, et a
l,U
SA
,20
10(1
74)
Age
>18
yea
rs w
ho fu
lfille
d A
CR
cla
ssifi
catio
n cr
iteria
for S
LE, m
oder
atel
y ac
tive
lupu
s de
fined
by
1 of
the
2 se
ts o
f crit
eria
. C
riter
ia s
et 1
–pr
esen
ce
of c
hron
ic g
lom
erul
onep
hriti
s w
ith a
n in
adeq
uate
re
spon
se to
at l
east
6 m
onth
s of
ade
quat
e im
mun
osup
pres
sive
ther
apy
(with
eith
er
met
hylp
redn
isol
one
puls
e do
ses,
cy
lcop
hosp
ham
ide,
aza
thio
prin
e, c
yclo
spor
ine,
m
ycop
heno
late
mof
etil,
hig
h-do
se d
ialy
co
rtico
ster
oids
, met
hotre
xate
, or i
ntra
veno
us
imm
unog
lobu
lin, p
lus
the
follo
win
g 4
feat
ures
: les
s th
an a
30%
inc
reas
e in
ser
um c
reat
inin
e le
vels
as
com
pare
d w
ith th
e lo
wes
t lev
el a
chiv
ed d
urin
g tre
atm
ent;
prot
einu
ria a
t lev
els
<=1.
5 tim
es th
e va
lue
at b
asel
ine
(bef
ore
treat
men
t); <
= 2+
cel
lula
r ca
sts
in th
e ur
inar
y se
dim
ents
; and
ext
rare
nal
dise
ase
activ
ity n
ot e
xcee
ding
a s
core
of 1
0 on
the
nonr
enal
com
pone
nts
of th
e SE
LEN
A ve
rsio
n of
S
LED
AI.
Cre
iteria
set
2 c
onsi
sted
of m
oder
atel
y ac
tive
extra
rena
l lup
us, d
efin
ed a
s ex
trare
nal
SE
LEN
A-S
LED
AI s
core
in th
e ra
nge
of 3
-10.
S
ELE
NA
-SLE
DA
I sco
re m
ust h
ave
been
sta
ble
for
Pre
gnan
cy, a
ny th
erap
y w
ith h
uman
, mur
ine
antib
odie
s, o
r any
exp
erim
enta
l the
rapy
with
in 3
m
onth
s, th
erap
y w
ith c
yclo
phos
pham
ide,
pul
se
met
hylp
redn
isol
one
or IV
IG w
ithin
4 w
eeks
, or
azat
hiop
rine,
myc
ophe
nola
te m
ofet
il, c
yclo
spor
ine,
or
met
hotre
xate
with
in 2
wee
ks o
f the
firs
t dos
e of
st
udy
med
icat
ion.
Ser
um c
reat
inin
e le
vel >
3.0
mg/
dl, w
hite
blo
od c
ell c
ount
<35
00/m
icro
L,
abso
lute
neu
troph
il co
unt <
300
0 m
icro
lL, a
bsol
ute
lym
phoc
yte
coun
t <=
500/
mic
rolL
, hem
oglo
bin
valu
e <8
.0 g
m/d
l, pl
atel
et c
ount
<50
000/
mic
rolL
, A
ST o
r ALT
leve
ls >
1.5
times
the
uppe
r lim
its o
f no
rmal
, or >
1000
Eps
tein
-Bar
r viru
s ge
nom
e eq
uiva
lent
s/10
6 p
reip
hera
l blo
od m
onon
ucle
ar
cells
.
0
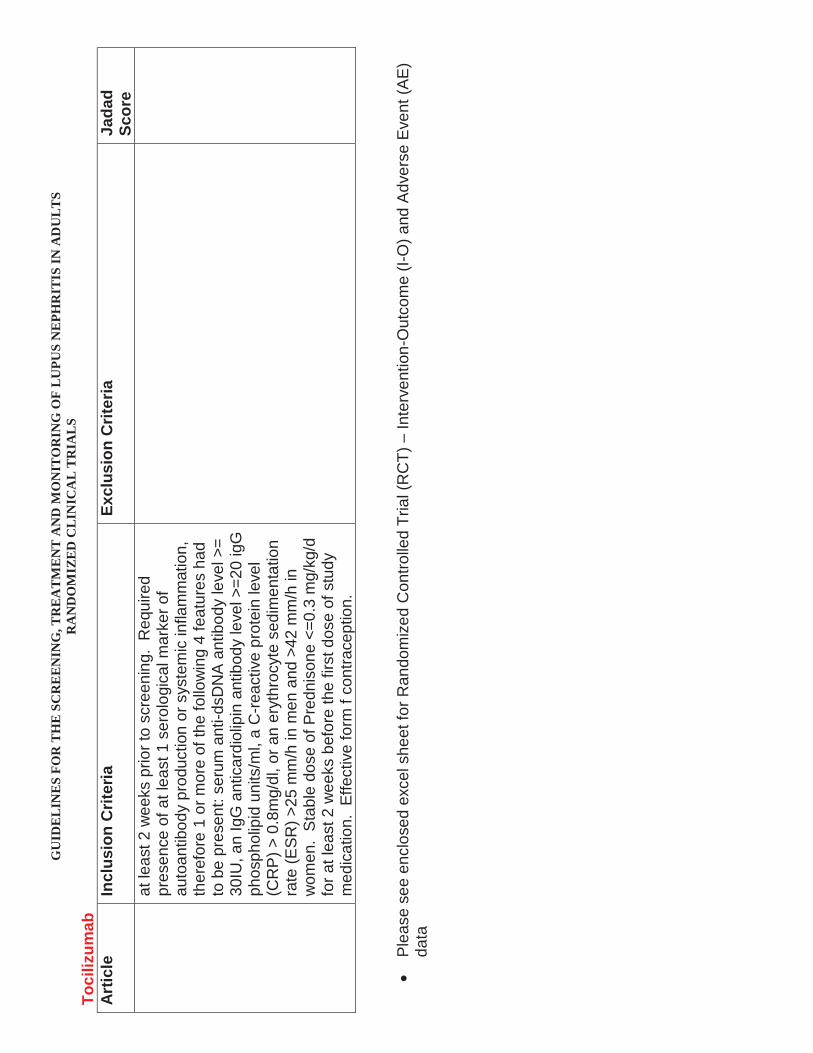
GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
LS
Toci
lizum
abA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaJa
dad
Scor
eat
leas
t 2 w
eeks
prio
r to
scre
enin
g. R
equi
red
pres
ence
of a
t lea
st 1
ser
olog
ical
mar
ker o
f au
toan
tibod
y pr
oduc
tion
or s
yste
mic
infla
mm
atio
n,
ther
efor
e 1
or m
ore
of th
e fo
llow
ing
4 fe
atur
es h
ad
to b
e pr
esen
t: se
rum
ant
i-dsD
NA
ant
ibod
y le
vel >
= 30
IU, a
n Ig
G a
ntic
ardi
olip
in a
ntib
ody
leve
l >=2
0 ig
G
phos
phol
ipid
uni
ts/m
l, a
C-re
activ
e pr
otei
n le
vel
(CR
P) >
0.8
mg/
dl, o
r an
eryt
hroc
yte
sedi
men
tatio
n ra
te (E
SR
) >25
mm
/h in
men
and
>42
mm
/h in
w
omen
. S
tabl
e do
se o
f Pre
dnis
one
<=0.
3 m
g/kg
/d
for a
t lea
st 2
wee
ks b
efor
e th
e fir
st d
ose
of s
tudy
m
edic
atio
n. E
ffect
ive
form
f co
ntra
cept
ion.
Ple
ase
see
encl
osed
exc
el s
heet
for R
ando
miz
ed C
ontro
lled
Tria
l (R
CT)
–In
terv
entio
n-O
utco
me
(I-O
) and
Adv
erse
Eve
nt (A
E)
data
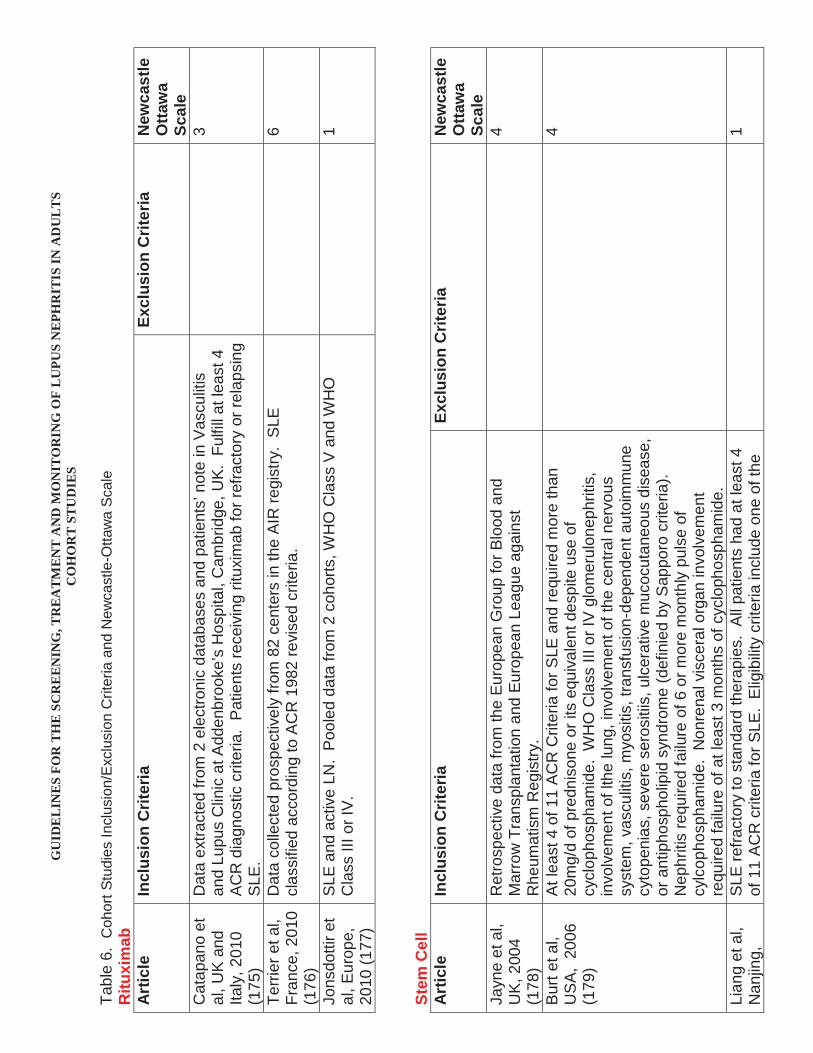
GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
CO
HO
RT
ST
UD
IES
Tabl
e 6.
Coh
ort S
tudi
es In
clus
ion/
Excl
usio
n C
riter
ia a
nd N
ewca
stle
-Otta
wa
Scal
eR
ituxi
mab
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
New
cast
le
Otta
wa
Scal
eC
atap
ano
et
al, U
K a
nd
Italy
, 201
0(1
75)
Dat
a ex
tract
ed fr
om 2
ele
ctro
nic
data
base
s an
d pa
tient
s’ n
ote
in V
ascu
litis
an
d Lu
pus
Clin
ic a
t Add
enbr
ooke
’s H
ospi
tal,
Cam
brid
ge, U
K. F
ulfil
l at l
east
4A
CR
dia
gnos
tic c
riter
ia.
Pat
ient
s re
ceiv
ing
ritux
imab
for r
efra
ctor
y or
rela
psin
g S
LE.
3
Terri
er e
t al,
Fran
ce, 2
010
(176
)
Dat
a co
llect
ed p
rosp
ectiv
ely
from
82
cent
ers
in th
e A
IR re
gist
ry.
SLE
cl
assi
fied
acco
rdin
g to
AC
R 1
982
revi
sed
crite
ria.
6
Jons
dotti
r et
al, E
urop
e,
2010
(177
)
SLE
and
act
ive
LN.
Pool
ed d
ata
from
2 c
ohor
ts, W
HO
Cla
ss V
and
WH
O
Cla
ss II
I or I
V.
1
Stem
Cel
lA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaN
ewca
stle
O
ttaw
a Sc
ale
Jayn
e et
al,
UK
, 200
4(1
78)
Ret
rosp
ectiv
e da
ta fr
om th
e Eu
rope
an G
roup
for B
lood
and
M
arro
w T
rans
plan
tatio
n an
d Eu
rope
an L
eagu
e ag
ains
t R
heum
atis
m R
egis
try.
4
Bur
t et a
l, U
SA
, 20
06(1
79)
At l
east
4 o
f 11
AC
R C
riter
ia fo
r SLE
and
requ
ired
mor
e th
an
20m
g/d
of p
redn
ison
e or
its
equi
vale
nt d
espi
te u
se o
f cy
clop
hosp
ham
ide.
WH
O C
lass
III o
r IV
glo
mer
ulon
ephr
itis,
in
volv
emen
t of l
the
lung
, inv
olve
men
t of t
he c
entra
l ner
vous
sy
stem
, vas
culit
is, m
yosi
tis, t
rans
fusi
on-d
epen
dent
aut
oim
mun
e cy
tope
nias
, sev
ere
sero
sitii
s, u
lcer
ativ
e m
ucoc
utan
eous
dis
ease
, or
ant
ipho
spho
lipid
syn
drom
e (d
efin
ied
by S
appo
ro c
riter
ia).
N
ephr
itis
requ
ired
failu
re o
f 6 o
r mor
e m
onth
ly p
ulse
of
cylc
opho
spha
mid
e. N
onre
nal v
isce
ral o
rgan
invo
lvem
ent
requ
ired
failu
re o
f at l
east
3 m
onth
s of
cyc
loph
osph
amid
e.
4
Lian
g et
al,
Nan
jing,
S
LE re
fract
ory
to s
tand
ard
ther
apie
s. A
ll pa
tient
s ha
d at
leas
t 4
of 1
1 A
CR
crit
eria
for S
LE.
Elig
ibili
ty c
riter
ia in
clud
e on
e of
the
1
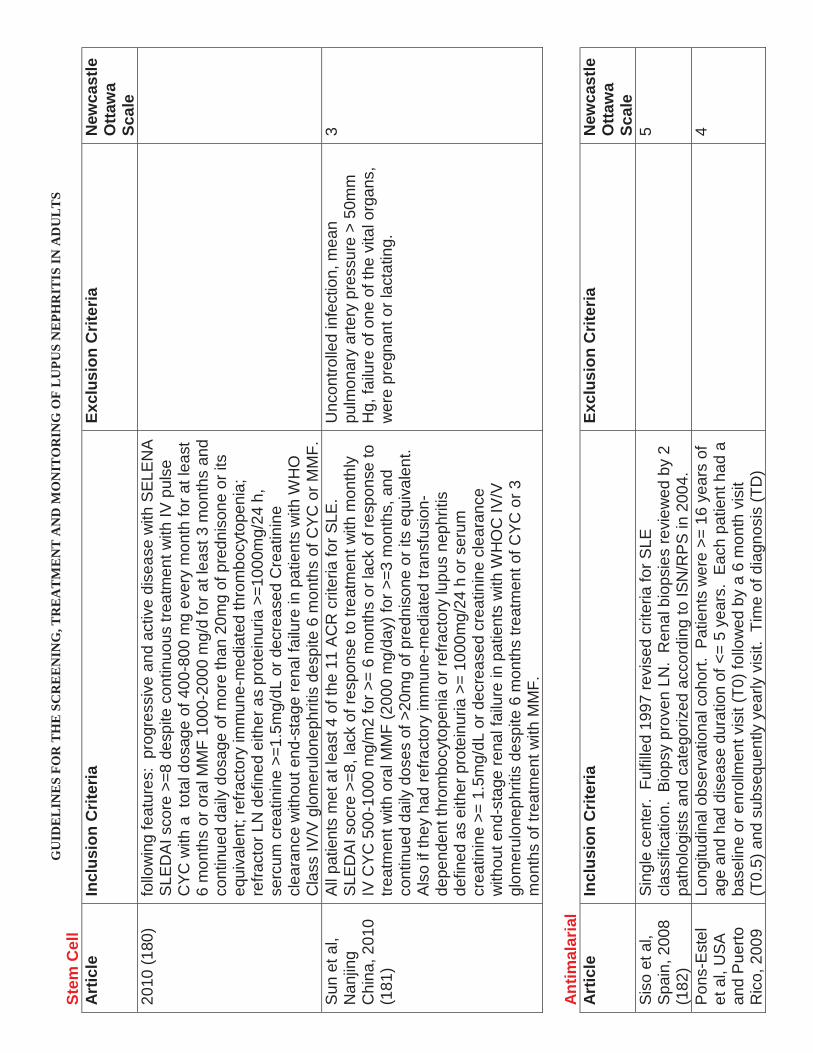
GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
Stem
Cel
lA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaN
ewca
stle
O
ttaw
a Sc
ale
2010
(180
)fo
llow
ing
feat
ures
: pr
ogre
ssiv
e an
d ac
tive
dise
ase
with
SEL
EN
A
SLE
DA
I sco
re >
=8 d
espi
te c
ontin
uous
trea
tmen
t with
IV p
ulse
C
YC w
ith a
tot
al d
osag
e of
400
-800
mg
ever
y m
onth
for a
t lea
st
6 m
onth
s or
ora
l MM
F 10
00-2
000
mg/
d fo
r at l
east
3 m
onth
s an
d co
ntin
ued
daily
dos
age
of m
ore
than
20m
g of
pre
dnis
one
or it
s eq
uiva
lent
; ref
ract
ory
imm
une-
med
iate
d th
rom
bocy
tope
nia;
re
fract
or L
N d
efin
ed e
ither
as
prot
einu
ria >
=100
0mg/
24 h
, se
rcum
cre
atin
ine
>=1.
5mg/
dL o
r dec
reas
ed C
reat
inin
e cl
eara
nce
with
out e
nd-s
tage
rena
l fai
lure
in p
atie
nts
with
WH
O
Cla
ss IV
/V g
lom
erul
onep
hriti
s de
spite
6 m
onth
s of
CYC
or M
MF.
Sun
et a
l, N
anjin
g C
hina
, 201
0(1
81)
All
patie
nts
met
at l
east
4 o
f the
11
AC
R c
riter
ia fo
r SLE
. S
LED
AI s
ocre
>=8
, lac
k of
resp
onse
to tr
eatm
ent w
ith m
onth
ly
IV C
YC 5
00-1
000
mg/
m2
for >
= 6
mon
ths
or la
ck o
f res
pons
e to
tre
atm
ent w
ith o
ral M
MF
(200
0 m
g/da
y) fo
r >=3
mon
ths,
and
co
ntin
ued
daily
dos
es o
f >20
mg
of p
redn
ison
e or
its
equi
vale
nt.
Als
o if
they
had
refra
ctor
y im
mun
e-m
edia
ted
trans
fusi
on-
depe
nden
t thr
ombo
cyto
peni
a or
refra
ctor
y lu
pus
neph
ritis
de
fined
as
eith
er p
rote
inur
ia >
= 10
00m
g/24
h o
r ser
um
crea
tinin
e >=
1.5
mg/
dL o
r dec
reas
ed c
reat
inin
e cl
eara
nce
with
out e
nd-s
tage
rena
l fai
lure
in p
atie
nts
with
WH
OC
IV/V
gl
omer
ulon
ephr
itis
desp
ite 6
mon
ths
treat
men
t of C
YC o
r 3
mon
ths
of tr
eatm
ent w
ith M
MF.
Unc
ontro
lled
infe
ctio
n, m
ean
pulm
onar
y ar
tery
pre
ssur
e >
50m
m
Hg,
failu
re o
f one
of t
he v
ital o
rgan
s,
wer
e pr
egna
nt o
r lac
tatin
g.
3
Ant
imal
aria
lA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaN
ewca
stle
O
ttaw
a Sc
ale
Sis
o et
al,
Spa
in, 2
008
(182
)
Sin
gle
cent
er.
Fulfi
lled
1997
revi
sed
crite
ria fo
r SLE
cl
assi
ficat
ion.
Bio
psy
prov
en L
N.
Ren
al b
iops
ies
revi
ewed
by
2 pa
thol
ogis
ts a
nd c
ateg
oriz
ed a
ccor
ding
to IS
N/R
PS
in 2
004.
5
Pon
s-E
stel
et
al,
USA
an
d P
uerto
R
ico,
200
9
Long
itudi
nal o
bser
vatio
nal c
ohor
t. P
atie
nts
wer
e >=
16
year
s of
ag
e an
d ha
d di
seas
e du
ratio
n of
<=
5 ye
ars.
Eac
h pa
tient
had
a
base
line
or e
nrol
lmen
t vis
it (T
0) fo
llow
ed b
y a
6 m
onth
vis
it (T
0.5)
and
sub
sequ
ently
yea
rly v
isit.
Tim
e of
dia
gnos
is (T
D)
4

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
Ant
imal
aria
lA
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaN
ewca
stle
O
ttaw
a Sc
ale
LUM
INA
st
udy
(183
)w
as d
efin
ed a
s th
e tim
e w
hen
each
pat
ient
met
4 A
CR
crit
eria
.
Cyc
losp
orin
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
New
cast
le
Otta
wa
Scal
eR
ihov
a et
al,
Cze
ch
Rep
ublic
, 20
07(1
84)
Ret
rosp
ectiv
e ch
arge
revi
ew.
Pat
ient
mee
t the
198
2 A
CR
cr
iteria
for t
he d
iagn
osis
of S
LE a
nd h
ave
an a
ctiv
e LN
ver
ified
an
d cl
assi
fied
by a
rena
l bio
psy,
trea
ted
with
CsA
.
2
Cyc
loph
osph
amid
e (C
YC)
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
New
cast
le
Otta
wa
Scal
e
Doo
ley
et a
l, U
SA
, 199
6(1
85)
Ren
al b
iops
y di
agno
sis
of S
LE-D
PG
N fr
om w
ithin
the
Glo
mer
ular
Dis
ease
Col
labo
rativ
e N
etw
ork
(GD
CN
) wer
e el
igib
le
for i
nclu
sion
in th
is s
tudy
. P
atie
nt fu
lfille
d 4
or m
ore
crite
ria fr
om
the
1982
AC
R re
vise
d cr
iteria
for c
lass
ifica
tion
of S
LE.
Doc
umen
tatio
n of
trea
tmen
t or i
nten
tion
to tr
eat w
ith C
YC IV
was
re
quire
d fo
r stu
dy e
ntry
.
0
Ioan
nidi
s et
al
, US
A a
nd
Gre
ece,
20
00(1
86)
All
patie
nts
with
bio
psy-
docu
men
ted
diag
nosi
s of
pro
lifer
ativ
e lu
pus
neph
ritis
(WH
O ty
pe II
I or I
V) t
reat
ed w
ith IV
C.
1
Mok
et a
l, H
ong
Kon
g,
Chi
na, 2
004
(187
)
SLE
pat
ient
s w
ith b
iops
y pr
oven
DP
GN
initi
ally
trea
ted
with
re
gim
ens
that
incl
uded
CYC
and
cor
ticos
tero
ids
betw
een
year
s 19
88 a
nd 2
001.
All
fulfi
lled
at le
ast 4
of t
he A
CR
crit
eria
for S
LE
clas
sific
atio
n.
3
de C
astro
et
al, B
razi
l, 20
07(1
88)
SLE
cla
ssifi
catio
n by
AC
R c
lass
ifica
tion
crite
ria, t
reat
ed a
nd
follo
wed
from
Jul
y 19
88 to
Dec
embe
r 200
3.H
isto
logi
cal c
lass
II o
r V a
ccor
ding
to
1995
WH
O c
lass
ifica
tion.
6

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
Cyc
loph
osph
amid
e (C
YC)
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
New
cast
le
Otta
wa
Scal
e
Mok
et a
l, H
ong
Kon
g C
hina
, 200
6(1
89)
Ren
al b
iops
y pr
oven
diff
use
prol
ifera
tive
lupu
s gl
omer
ulon
ephr
itis
(199
5 W
HO
Cla
ss IV
) tre
ated
in H
ong
Kon
g id
entif
ied
by c
linic
al re
gist
ries
or re
nal b
iops
y da
taba
ses.
All
patie
nts
fulfi
lled
at le
ast 4
AC
R c
riter
ia fo
r SLE
cla
ssifi
catio
ns
and
wer
e in
itial
ly tr
eate
d w
ith c
ortic
oste
roid
s an
d C
YC.
3
Pet
ri et
al,
US
A, 2
010
(190
)
Pro
spec
tive
rand
omiz
ed tr
ial w
ith 1
:1 ra
ndom
izat
ion.
SLE
pa
tient
s m
et >
= 4
of re
vise
d A
CR
crit
eria
for S
LE w
ith m
oder
ate
to s
ever
e ac
tivity
in a
n or
gan
as d
efin
ed a
s B
ILA
G A
or a
hig
h sc
ore
for t
hat o
rgan
on
the
SLA
M o
r hos
pita
lizat
ion
for
invo
lvem
ent o
f tha
t org
an.
Lack
of r
espo
nse
or e
xpec
ted
lack
of
resp
onse
to m
oder
ate-
to h
igh-
dose
cor
ticos
tero
ids,
to th
e eq
uiva
lent
deg
ree
of im
mun
osup
pres
sion
, or t
o ap
prop
riate
ot
her t
reat
men
t. C
ombi
natio
n th
erap
y of
bot
h hy
drox
ycho
rolo
guin
e an
d qu
inac
rine
as w
ell a
s im
mun
osup
pres
sion
had
to h
ave
faile
d fo
r SLE
pat
ient
s w
ith
cuta
neou
s lu
pus.
Mus
culo
skel
etal
lupu
s fro
m th
e ca
tego
ry o
f elig
ible
org
an in
volv
emen
t.4
Imm
unos
uppr
essi
ves
vs C
yclo
phos
pham
ide
(CYC
)A
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaN
ewca
stle
O
ttaw
a Sc
ale
Uro
witz
et a
l, To
ront
o,
Can
ada,
20
07(1
91)
SLE
>=
4 A
CR
crit
eria
or 3
AC
R c
riter
ia p
lus
a ty
pica
l hi
stol
ogic
al le
sion
of S
LE o
n re
nal o
r ski
n bi
opsy
. P
atie
nts
with
ac
tive
rena
l dis
ease
trea
ted
with
imm
unos
uppr
essi
ve/c
ytot
oxic
m
edic
atio
ns in
the
year
afte
r dia
gnos
is o
f act
ive
rena
l dis
ease
w
ere
sele
cted
from
clin
ic d
atab
ase.
Act
ive
rena
l dis
ease
de
fined
as
pres
ence
of 2
con
secu
tive
visi
ts o
f one
of:
red
bloo
d ce
ll ca
sts
or h
emeg
ranu
lar c
asts
, hem
atur
ia o
r pyr
uia
in th
e ab
senc
e of
oth
er c
ause
s, o
r pro
tein
uria
(>50
0mg/
24h
or >
= 3+
on
dip
stic
k) o
r an
abno
rmal
kid
ney
biop
sy s
how
ing
activ
e lu
pus
neph
ritis
.
3
Cyc
loph
osph
amid
e (C
YC) v
s A
zath
iopr
ine
(AZA
)

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
New
cast
le
Otta
wa
Scal
e
Dec
ker e
t al,
NIH
, 197
5(1
92)
Dia
gnos
is o
f SLE
by
ARA
crit
eria
incl
udin
g a
posi
tive
eryt
hem
atos
us c
ell t
est;
kidn
ey d
isea
se w
ith e
ither
ery
thro
cyte
ca
sts,
cel
luar
cas
ts, a
nd e
ither
hem
atur
ia (2
0 er
ythr
ocyt
es/h
pf)
or h
igh
anti-
DN
A a
ntib
odie
s, lo
w c
ompl
emen
t, an
d a
posi
tive
rena
l bio
psy,
and
diff
use
glom
erul
onep
hriti
s w
ith a
t lea
st a
po
rtion
of a
ll gl
omer
uli i
nvol
ved.
Ser
um c
reat
inin
e of
gre
ater
than
4m
g/10
0ml o
r cre
atin
ine
clea
ranc
e of
le
ss th
an 2
0ml/m
in
3
Cyc
loph
osph
amid
e (C
YC) +
Aza
thio
prin
e (A
ZA)
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
New
cast
le
Otta
wa
Scal
e
Cha
n et
al,
Hon
g K
ong,
C
hina
, 200
5(1
70)
Pro
spec
tive
coho
rt. D
iagn
osis
of W
HO
Cla
ss IV
lupu
s ne
phrit
is
conf
irmed
by
rena
l bio
psy,
bas
elin
e ur
inar
y pr
otei
n ex
cret
ion
exce
edin
g 1g
/24h
, bas
elin
e se
rum
alb
umin
bel
ow 3
5g/L
, tre
atm
ent w
ith s
eque
ntia
l im
mun
osup
pres
sion
. P
atie
nts
with
su
perim
pose
d m
embr
anou
s ch
ange
s w
ere
incl
uded
pro
vide
d th
at th
ere
wer
e co
ncom
itant
diff
use
prol
ifera
tive
feat
ures
.
Ser
um c
reat
inin
e ex
ceed
ing
400m
icro
mol
/L, t
reat
men
t with
cy
clop
hosp
ham
ide
or m
ycop
heno
late
m
ofet
il w
ithin
6 m
onth
s, o
r pr
edni
solo
ne d
ose
exce
edin
g 0.
4mg/
kg/d
for m
ore
than
2 w
eeks
prio
r to
bas
elin
e/
3
Hig
h do
se c
yclo
phos
pham
ide
(CYC
) vs
Low
dos
e cy
clop
hosp
ham
ide
follo
wed
by
Aza
thio
prin
e (A
ZA)
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
New
cast
le
Otta
wa
Scal
e
Hou
ssia
u et
al
, Eur
ope,
E
LNT,
200
4S
uban
alys
is(1
93)
SLE
pat
ient
s ac
cord
ing
to A
CR
crit
eria
, age
14
year
s or
old
er
with
bio
psy
prov
en p
rolif
erat
ive
lupu
s gl
omer
ulon
ephr
itis
(WH
O
Cla
ss II
I, IV
, Vc,
or V
d) a
nd p
rote
inur
ia >
= 50
0mg/
24 h
.
Pat
ient
s w
ho h
ad ta
ken
CYC
or A
ZA
durin
g th
e pr
evio
us y
ear o
r had
take
n >=
15m
g/da
y pr
edni
sone
(or e
quiv
alen
t) du
ring
the
prev
ious
mon
th w
ere
excl
uded
(exc
ept f
or a
cou
rse
of
gluc
ocor
ticoi
ds fo
r a m
axim
um o
f 10
days
bef
ore
the
refe
rral).
Oth
er
excl
usio
n cr
iteria
wer
e re
nal t
hrom
botic
m
icro
angi
opat
hy, p
reex
istin
g ch
roni
c re
nal f
ailu
re, p
regn
ancy
, pre
viou
s m
alig
nanc
y (e
xcep
t ski
n an
d ce
rvic
al
3
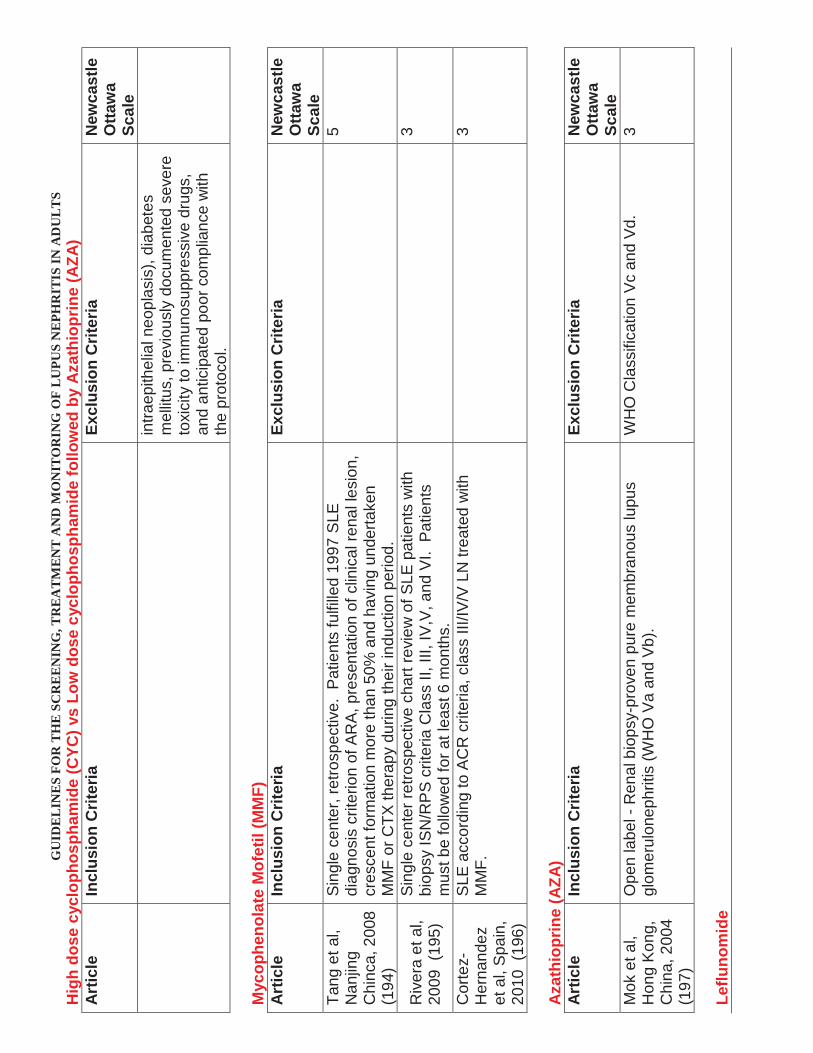
GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
Hig
h do
se c
yclo
phos
pham
ide
(CYC
) vs
Low
dos
e cy
clop
hosp
ham
ide
follo
wed
by
Aza
thio
prin
e (A
ZA)
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
New
cast
le
Otta
wa
Scal
ein
traep
ithel
ial n
eopl
asis
), di
abet
es
mel
litus
, pre
viou
sly
docu
men
ted
seve
re
toxi
city
to im
mun
osup
pres
sive
dru
gs,
and
antic
ipat
ed p
oor c
ompl
ianc
e w
ith
the
prot
ocol
.
Myc
ophe
nola
te M
ofet
il (M
MF)
A
rtic
leIn
clus
ion
Crit
eria
Excl
usio
n C
riter
iaN
ewca
stle
O
ttaw
a Sc
ale
Tang
et a
l, N
anjin
g C
hinc
a, 2
008
(194
)
Sin
gle
cent
er, r
etro
spec
tive.
Pat
ient
s fu
lfille
d 19
97 S
LE
diag
nosi
s cr
iterio
n of
AR
A, p
rese
ntat
ion
of c
linic
al re
nal l
esio
n,
cres
cent
form
atio
n m
ore
than
50%
and
hav
ing
unde
rtake
n M
MF
or C
TX th
erap
y du
ring
thei
r ind
uctio
n pe
riod.
5
Riv
era
et a
l, 20
09(1
95)
Sin
gle
cent
er re
trosp
ectiv
e ch
art r
evie
w o
f SLE
pat
ient
s w
ith
biop
sy IS
N/R
PS
crit
eria
Cla
ss II
, III,
IV,V
, and
VI.
Pat
ient
s m
ust b
e fo
llow
ed fo
r at l
east
6 m
onth
s.
3
Cor
tez-
Her
nand
ez
et a
l, S
pain
, 20
10(1
96)
SLE
acc
ordi
ng to
AC
R c
riter
ia, c
lass
III/I
V/V
LN
trea
ted
with
M
MF.
3
Aza
thio
prin
e (A
ZA)
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
New
cast
le
Otta
wa
Scal
eM
ok e
t al,
Hon
g K
ong,
C
hina
, 200
4(1
97)
Ope
n la
bel -
Ren
al b
iops
y-pr
oven
pur
e m
embr
anou
s lu
pus
glom
erul
onep
hriti
s (W
HO
Va
and
Vb)
.W
HO
Cla
ssifi
catio
n V
c an
d V
d.3
Leflu
nom
ide

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
Art
icle
Incl
usio
n C
riter
iaEx
clus
ion
Crit
eria
New
cast
le
Otta
wa
Scal
e
Zhan
g et
al,
Har
bin
Chi
na, 2
009
(198
)
Fulfi
lled
1997
AC
R c
lass
ifica
tion
crite
ria fo
r SLE
adm
itted
as
inpa
tient
s un
derg
oing
kid
ney
biop
sy.
Sev
ere
insu
ffici
ency
of o
rgan
s be
side
s ki
dney
, inc
ludi
ng h
eart
failu
re, l
iver
fa
ilure
, sev
ere
psyc
hosi
s, le
ukoc
yte
and
plat
elet
cou
nt le
ss th
an 3
x 1
0 9/
L an
d 50
x 1
0 9
resp
ectiv
ely,
pre
gnan
t w
omen
, lac
tatin
g w
omen
, chi
ldre
n of
le
ss th
an 1
6 ag
e.
3
Ple
ase
see
encl
osed
exc
el s
heet
for C
ohor
t Tria
l –In
terv
entio
n-O
utco
me
(I-O
) and
Adv
erse
Eve
nt (A
E) d
ata

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
Has
hem
i V, N
adja
fi I,
Azz
orde
gan
F,
Gha
hram
ani N
, Br
oum
and
B. S
haria
ti H
ospi
tal,
Tehr
an
Uni
vers
ity o
f Med
ical
Sc
ienc
es, I
ran.
Tr
ansp
lant
Pro
c.
1999
D
ec;3
1(8)
:314
2-3.
Ren
al
trans
plan
tatio
n in
sy
stem
ic lu
pus
eryt
hem
atos
us: a
m
ultic
ente
r stu
dy
with
37
patie
nts
in
Iran.
Look
ed a
t 37
pts
with
LN
and
ESR
D w
ho
had
unde
rgon
ere
nal t
rans
plan
tatio
n. P
ost-
trans
plan
t med
s =
CsA
, aza
, and
pre
d,
exce
pt in
1 c
ase
aza+
pred
.
Gra
ft su
rviv
al a
t 1 y
r = 8
5.6%
, 3 y
r = 7
3%. N
o co
rrela
tion
w/
gend
er, a
ge a
t tra
nspl
ant,
and
dono
r sou
rce.
Cau
ses
of g
raft
loss
: chr
onic
gra
ft re
ject
ion
11/3
7, a
cute
reje
ctio
n 2/
37,
recu
rren
ce o
f LN
1/3
7. P
atie
nt s
urvi
val a
t 1 y
r 94.
4%, a
t 3 y
rs
91.7
%. 2
/37
died
of M
I, 1/
37 d
ied
of p
neum
ococ
cal
infe
ctio
n/se
psis
, 1/3
7 di
ed o
f opi
um to
xici
ty.
War
d M
M.
Pal
o A
lto
Hea
lth C
are
Sys
tem
, Pa
lo A
lto, C
A K
idne
y In
t. 20
00
May
;57(
5):2
136-
43.
Out
com
es o
f ren
al
trans
plan
tatio
n am
ong
patie
nts
with
en
d-st
age
rena
l di
seas
e ca
used
by
lupu
s ne
phrit
is.
Gra
ft fa
ilure
and
pat
ient
mor
talit
y af
ter t
he
first
cad
aver
ic re
nal t
rans
plan
tatio
n w
ere
com
pare
d be
twee
n 77
2 ad
ults
with
ES
RD
ca
used
by lu
pus
neph
ritis
and
32,
644
adul
ts
with
ESR
D c
ause
d by
oth
er c
ause
s w
ho
rece
ived
a tr
ansp
lant
bet
wee
n 19
87 a
nd
1994
and
wer
e in
clud
ed in
the
Uni
ted
Sta
tes
Ren
al D
ata
Sys
tem
. The
med
ian
follo
w-u
p tim
es w
ere
4.9
and
5.0
year
s in
the
two
grou
ps, r
espe
ctiv
ely.
Mul
tivar
iate
Cox
re
gres
sion
mod
els
wer
e us
ed to
adj
ust t
he
risks
of g
raft
failu
re a
nd m
orta
lity
for g
roup
di
ffere
nces
in re
cipi
ent a
nd d
onor
ch
arac
teris
tics.
Sim
ilar c
ompa
rison
s w
ere
perfo
rmed
bet
wee
n 39
0 ad
ults
with
ES
RD
ca
used
by
lupu
s ne
phrit
is a
nd 1
0,51
2 ad
ults
w
ith E
SRD
cau
sed
by o
ther
cau
ses
afte
r fir
st li
ving
-rel
ated
rena
l tra
nspl
anta
tion.
RES
ULT
S: In
an
unad
just
ed a
naly
sis,
the
risk
of g
raft
failu
re a
fter
first
cad
aver
ic tr
ansp
lant
was
slig
htly
but
sig
nific
antly
gre
ater
am
ong
patie
nts
with
ESR
D c
ause
d by
lupu
s ne
phrit
is th
an
amon
g th
ose
with
ESR
D c
ause
d by
oth
er c
ause
s [h
azar
d ra
tio
(HR
), 1.
13; 9
5% C
I, 1.
01 to
1. 2
6, P
= 0
.04]
. How
ever
, afte
r ad
just
men
t for
pot
entia
l con
foun
ding
fact
ors,
the
risk
of g
raft
failu
re w
as n
ot in
crea
sed
in p
atie
nts
with
ESR
D c
ause
d by
lupu
s ne
phrit
is (H
R, 1
.08;
95%
CI,
0.94
to 1
.23,
P =
0.2
8). M
orta
lity
afte
r the
firs
t cad
aver
ic tr
ansp
lant
atio
n di
d no
t diff
er b
etw
een
grou
ps. T
he a
djus
ted
risks
of g
raft
failu
re (H
R, 1
.06;
95%
CI,
0.84
to 1
.32,
P =
0.6
2) a
nd p
atie
nt m
orta
lity
(HR
= 0
. 69;
95%
CI,
0.45
to 1
.05,
P =
0.0
9) a
fter t
he fi
rst l
ivin
g-re
late
d re
nal t
rans
plan
t w
ere
also
not
sig
nific
antly
hig
her a
mon
g pa
tient
s w
ith E
SRD
ca
used
by
lupu
s ne
phrit
is. C
ON
CLU
SIO
NS:
Gra
ft an
d pa
tient
su
rviv
al a
fter f
irst c
adav
eric
and
firs
tliv
ing-
rela
ted
rena
l tra
nspl
ants
are
sim
ilar i
n pa
tient
s w
ith E
SRD
cau
sed
by lu
pus
neph
ritis
and
pat
ient
s w
ith E
SRD
from
oth
er c
ause
s.
Gor
al S
, Yna
res
C,
Shap
pell
SB,
Sny
der
S, F
eure
r ID
, Ka
zanc
iogl
u R
, Fog
o AB
, Hel
derm
an J
H.
Uni
vers
ity o
f Pe
nnsy
lvan
ia S
choo
l of
Med
icin
e
Tran
spla
ntat
ion.
200
3 M
ar 1
5;75
(5):6
51-6
.
Rec
urre
nt lu
pus
neph
ritis
in re
nal
trans
plan
t rec
ipie
nts
revi
site
d: it
is n
ot
rare
.
The
reco
rds
of 5
4 re
nal t
rans
plan
t rec
ipie
nts
with
SLE
wer
e re
view
ed. T
hirty
-one
pat
ient
s un
derw
ent b
iops
y be
caus
e of
wor
seni
ng
rena
l fun
ctio
n an
d pr
otei
nuria
. All
biop
sy
spec
imen
s w
ere
eval
uate
d by
ligh
t m
icro
scop
y, im
mun
oflu
ores
cenc
e (IF
), an
d el
ectro
n m
icro
scop
y (E
M).
RES
ULT
S: A
mon
g th
e 50
pat
ient
s w
ith a
t lea
st 3
mon
ths
of
follo
w-u
p, R
LN w
as p
rese
nt in
15
(52%
of p
atie
nts
who
un
derw
ent b
iops
y, 3
0% o
f tot
al p
atie
nts)
: mes
angi
al lu
pus
neph
ritis
(LN
) (cl
ass
II) in
eig
ht, f
ocal
pro
lifer
ativ
e LN
(cla
ss II
I) in
fo
ur, a
nd m
embr
anou
s LN
(cla
ss V
b) in
thre
e pa
tient
s. O
ne
patie
nt h
ad g
raft
loss
bec
ause
of R
LN (c
lass
II) a
t 10.
5 ye
ars.
Th
e du
ratio
n of
dia
lysi
s be
fore
tran
spla
ntat
ion
was
not
diff
eren
t be
twee
n pa
tient
s w
ith R
LN c
ompa
red
to p
atie
nts
with
out R
LN
(P=0
.40)
. Ove
rall
patie
nt s
urvi
val (
n=50
) was
96%
at 1
yea
r and
82
% a
t 5 y
ears
, and
gra
ft su
rviv
al w
as 8
7% a
t1 y
ear a
nd 6
0% a
t 5
year
s. G
raft
surv
ival
was
wor
se in
pat
ient
s w
ho u
nder
wen
t bi
opsy
com
pare
d w
ith p
atie
nts
who
nev
er u
nder
wen
t bio
psy
(P<0
.01)
. CO
NC
LUSI
ON
S: R
LN is
mor
e co
mm
on th
an

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
prev
ious
ly re
porte
d, b
ut in
our
ser
ies,
gra
ft lo
ss b
ecau
se o
f RLN
w
as ra
re. A
ggre
ssiv
e us
e of
allo
graf
t bio
psie
s an
d m
orph
olog
ic
eval
uatio
n w
ith IF
and
EM
are
impo
rtant
fact
ors
in th
e di
agno
sis
of R
LN. T
he im
pact
of n
ew im
mun
osup
pres
sive
age
nts
on th
e in
cide
nce
of R
LN re
mai
ns to
be
seen
.
Dee
gens
JK,
Artz
M
A, H
oits
ma
AJ,
Wet
zels
JF.
U
nive
rsity
Med
ical
C
ente
r of N
ijmeg
en,
The
Net
herla
nds.
Tr
ansp
l Int
. 200
3 Ju
n;16
(6):4
11-8
. Ep
ub 2
003
Mar
19.
Out
com
e of
rena
l tra
nspl
anta
tion
in
patie
nts
with
sy
stem
ic lu
pus
eryt
hem
atos
us.
We
stud
ied
the
outc
ome
of re
nal
trans
plan
tatio
n in
pat
ient
s w
ith S
LE w
ho
unde
rwen
t tra
nspl
anta
tions
in o
ur c
ente
r be
twee
n 19
68 a
nd 2
001.
Pat
ient
and
gra
ft su
rviv
al w
ere
com
pare
d w
ith a
mat
ched
co
ntro
l gro
up. W
e sp
ecifi
cally
look
ed fo
r any
ev
iden
ce o
f rec
urre
nt d
isea
se. T
here
wer
e 23
pat
ient
s (tw
o m
ale,
21
fem
ale)
with
a
mea
n +/
-SD
age
of 3
4+/-1
2 ye
ars
at
trans
plan
tatio
n.
One
pat
ient
dev
elop
ed re
nal f
ailu
re w
ith s
erol
ogic
al e
vide
nce
of
SLE
activ
ity a
t 61
mon
ths
afte
r tra
nspl
anta
tion.
In th
e ab
senc
e of
ur
ine
abno
rmal
ities
we
favo
red
the
diag
nosi
s of
reje
ctio
n,
alth
ough
recu
rren
ce o
f lup
us n
ephr
itis
coul
d no
t for
mal
ly b
e ex
clud
ed. T
his
was
the
only
cas
e of
a p
ossi
ble
recu
rren
ce o
f lu
pus
neph
ritis
. Tw
o ot
her p
atie
nts
deve
lope
d ex
tra-r
enal
m
anife
stat
ions
of S
LE a
t 6 a
nd 1
7 m
onth
s af
ter t
rans
plan
tatio
n.
Patie
nt a
nd g
raft
surv
ival
rate
s at
5 y
ears
afte
r tra
nspl
anta
tion
wer
e 86
% a
nd 6
8%, r
espe
ctiv
ely.
Sur
viva
l rat
es w
ere
not
sign
ifica
ntly
diff
eren
t fro
m th
ose
of a
mat
ched
con
trol g
roup
, 95%
an
d 78
%, r
espe
ctiv
ely.
Rec
urre
nce
of S
LE a
fter t
rans
plan
tatio
n is
ra
re. T
he re
sults
of r
enal
tran
spla
ntat
ion
in p
atie
nts
with
SLE
do
not d
iffer
sig
nific
antly
from
a m
atch
ed c
ontro
l gro
up. R
enal
tra
nspl
anta
tion
is a
goo
d al
tern
ativ
e fo
r ren
al re
plac
emen
t th
erap
y in
pat
ient
s w
ith lu
pus
neph
ritis
.M
oron
i G, T
anta
rdin
i F,
Gal
lelli
B, Q
uagl
ini
S, B
anfi
G, P
oli F
, M
onta
gnin
o G
, M
eron
i P, M
essa
P,
Pont
icel
li C
. C
entro
Tr
asfu
sion
ale
e di
Im
mun
olog
ia d
ei
Trap
iant
i IR
CC
S,
Osp
edal
e M
aggi
ore
Mila
no, I
taly
Am
J
Kidn
ey D
is. 2
005
May
;45(
5):9
03-1
1.
The
long
-term
pr
ogno
sis
of re
nal
trans
plan
tatio
n in
pa
tient
s w
ith lu
pus
neph
ritis
.
Betw
een
June
198
2 an
d 20
04, a
tota
l of 3
3 ad
ults
with
lupu
s ne
phrit
is re
ceiv
ed 3
5 ki
dney
allo
graf
ts. O
utco
mes
of t
hese
gra
fts
and
thos
e of
70
cont
rols
mat
ched
for a
ge,
sex,
and
don
or s
ourc
e w
ho u
nder
wen
t tra
nspl
anta
tion
durin
gth
e sa
me
perio
d w
ere
com
pare
d.
RES
ULT
S: M
ean
follo
w-u
p af
ter r
enal
tran
spla
ntat
ion
was
91
+/-
59 m
onth
s fo
r pat
ient
s w
ith lu
pus
and
90 +
/-64
mon
ths
for
cont
rols
. Act
uaria
l 15-
year
pat
ient
(80%
ver
sus
83%
) and
dea
th-
cens
ored
gra
ft su
rviv
al ra
tes
(69%
ver
sus
67%
) wer
e no
t si
gnifi
cant
ly d
iffer
ent b
etw
een
patie
nts
with
lupu
s an
d co
ntro
ls.
Ris
ks fo
r acu
te a
nd c
hron
ic re
ject
ion,
arte
rial h
yper
tens
ion,
and
in
fect
ion
wer
e no
t diff
eren
t bet
wee
n th
e 2
grou
ps. M
ean
seru
m
crea
tinin
e le
vels
als
o w
ere
sim
ilar i
n th
e 2
grou
ps a
t the
last
fo
llow
-up
visi
t. In
trava
scul
ar th
rom
botic
eve
nts
occu
rred
in 9
pa
tient
s w
ith S
LE (2
6%) a
nd 6
con
trols
(8.6
%; P
= 0
.038
). In
the
SLE
grou
p, 6
of 7
ant
ipho
spho
lipid
(aPL
) ant
ibod
y-po
sitiv
e ve
rsus
3 o
f 17
aPL
antib
ody-
nega
tive
patie
nts
expe
rienc
ed
thro
mbo
tic e
vent
s ( P
= 0
.015
). R
ecur
renc
e of
lupu
s ne
phrit
is
was
doc
umen
ted
in 3
rena
l gra
fts (8
.6%
), bu
t no
graf
t was
lost
be
caus
e of
recu
rren
t lup
us n
ephr
itis.
CO
NC
LUSI
ON
: Lon
g-te
rm
patie
nt a
nd g
raft
surv
ival
pro
babi
litie
s w
ere
sim
ilar i
n pa
tient
s
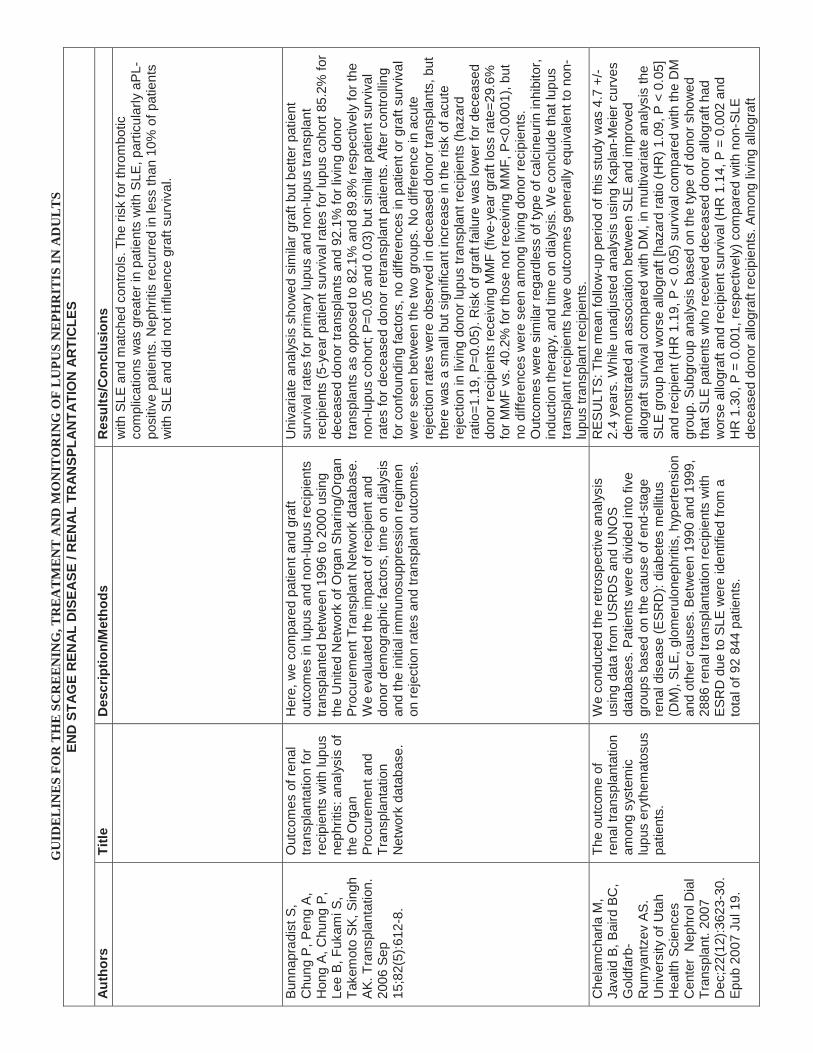
GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
with
SLE
and
mat
ched
con
trols
. The
risk
for t
hrom
botic
co
mpl
icat
ions
was
gre
ater
in p
atie
nts
with
SLE
, par
ticul
arly
aPL
-po
sitiv
e pa
tient
s. N
ephr
itis
recu
rred
in le
ss th
an 1
0% o
f pat
ient
s w
ith S
LE a
nd d
id n
ot in
fluen
ce g
raft
surv
ival
.
Bunn
apra
dist
S,
Chu
ng P
, Pen
g A,
H
ong
A, C
hung
P,
Lee
B, F
ukam
i S,
Take
mot
o SK
, Sin
gh
AK. T
rans
plan
tatio
n.
2006
Sep
15
;82(
5):6
12-8
.
Out
com
es o
f ren
al
trans
plan
tatio
n fo
r re
cipi
ents
with
lupu
s ne
phrit
is: a
naly
sis
of
the
Org
an
Proc
urem
ent a
nd
Tran
spla
ntat
ion
Net
wor
k da
taba
se.
Her
e, w
e co
mpa
red
patie
nt a
nd g
raft
outc
omes
in lu
pus
and
non-
lupu
s re
cipi
ents
tra
nspl
ante
d be
twee
n 19
96 to
200
0 us
ing
the
Uni
ted
Net
wor
k of
Org
an S
harin
g/O
rgan
Pr
ocur
emen
t Tra
nspl
ant N
etw
ork
data
base
. W
e ev
alua
ted
the
impa
ct o
f rec
ipie
nt a
nd
dono
r dem
ogra
phic
fact
ors,
tim
e on
dia
lysi
s an
d th
e in
itial
imm
unos
uppr
essi
on re
gim
en
on re
ject
ion
rate
s an
d tra
nspl
ant o
utco
mes
.
Uni
varia
te a
naly
sis
show
ed s
imila
r gra
ft bu
t bet
ter p
atie
nt
surv
ival
rate
s fo
r prim
ary
lupu
s an
d no
n-lu
pus
trans
plan
t re
cipi
ents
(5-y
ear p
atie
nt s
urvi
val r
ates
for l
upus
coh
ort 8
5.2%
for
dece
ased
don
or tr
ansp
lant
s an
d 92
.1%
for l
ivin
g do
nor
trans
plan
ts a
s op
pose
d to
82.
1% a
nd 8
9.8%
resp
ectiv
ely
for t
he
non-
lupu
s co
hort;
P=0
.05
and
0.03
) but
sim
ilar p
atie
nt s
urvi
val
rate
s fo
r dec
ease
d do
nor r
etra
nspl
ant p
atie
nts.
Afte
r con
trolli
ng
for c
onfo
undi
ng fa
ctor
s, n
o di
ffere
nces
in p
atie
nt o
r gra
ft su
rviv
al
wer
e se
en b
etw
een
the
two
grou
ps. N
o di
ffere
nce
in a
cute
re
ject
ion
rate
s w
ere
obse
rved
in d
ecea
sed
dono
r tra
nspl
ants
, but
th
ere
was
a s
mal
l but
sig
nific
ant i
ncre
ase
in th
e ris
k of
acu
te
reje
ctio
n in
livi
ng d
onor
lupu
s tra
nspl
ant r
ecip
ient
s (h
azar
d ra
tio=1
.19,
P=0
.05)
. Ris
k of
gra
ft fa
ilure
was
low
er fo
r dec
ease
d do
nor r
ecip
ient
s re
ceiv
ing
MM
F (fi
ve-y
ear g
raft
loss
rate
=29.
6%
for M
MF
vs. 4
0.2%
for t
hose
not
rece
ivin
g M
MF,
P<0
.000
1), b
ut
no d
iffer
ence
s w
ere
seen
am
ong
livin
g do
nor r
ecip
ient
s.
Out
com
es w
ere
sim
ilar r
egar
dles
s of
type
of c
alci
neur
in in
hibi
tor,
indu
ctio
n th
erap
y, a
nd ti
me
on d
ialy
sis.
We
conc
lude
that
lupu
s tra
nspl
ant r
ecip
ient
s ha
ve o
utco
mes
gen
eral
ly e
quiv
alen
t to
non-
lupu
s tra
nspl
ant r
ecip
ient
s.C
hela
mch
arla
M,
Java
id B
, Bai
rd B
C,
Gol
dfar
b-R
umya
ntze
v AS
. U
nive
rsity
of U
tah
Hea
lth S
cien
ces
Cen
ter
Nep
hrol
Dia
l Tr
ansp
lant
. 200
7 D
ec;2
2(12
):362
3-30
. Ep
ub 2
007
Jul 1
9.
The
outc
ome
of
rena
ltra
nspl
anta
tion
amon
g sy
stem
ic
lupu
s er
ythe
mat
osus
pa
tient
s.
We
cond
ucte
d th
e re
trosp
ectiv
e an
alys
is
usin
g da
ta fr
om U
SR
DS
and
UN
OS
da
taba
ses.
Pat
ient
s w
ere
divi
ded
into
five
gr
oups
bas
ed o
n th
e ca
use
of e
nd-s
tage
re
nal d
isea
se (E
SRD
): di
abet
es m
ellit
us
(DM
), SL
E, g
lom
erul
onep
hriti
s, h
yper
tens
ion
and
othe
r cau
ses.
Bet
wee
n 19
90 a
nd 1
999,
28
86 re
nal t
rans
plan
tatio
n re
cipi
ents
with
ES
RD
due
to S
LE w
ere
iden
tifie
d fro
m a
to
tal o
f 92
844
patie
nts.
RES
ULT
S: T
he m
ean
follo
w-u
p pe
riod
of th
is s
tudy
was
4.7
+/-
2.4
year
s. W
hile
una
djus
ted
anal
ysis
usi
ng K
apla
n-M
eier
cur
ves
dem
onst
rate
d an
ass
ocia
tion
betw
een
SLE
and
impr
oved
al
logr
aft s
urvi
val c
ompa
red
with
DM
, in
mul
tivar
iate
ana
lysi
s th
e SL
E gr
oup
had
wor
se a
llogr
aft [
haza
rd ra
tio (H
R) 1
.09,
P <
0.0
5]
and
reci
pien
t (H
R 1
.19,
P <
0.0
5) s
urvi
val c
ompa
red
with
the
DM
gr
oup.
Sub
grou
p an
alys
is b
ased
on
the
type
of d
onor
sho
wed
th
at S
LE p
atie
nts
who
rece
ived
dec
ease
d do
nor a
llogr
aft h
ad
wor
se a
llogr
aft a
nd re
cipi
ent s
urvi
val (
HR
1.1
4, P
= 0
.002
and
H
R 1
.30,
P =
0.0
01, r
espe
ctiv
ely)
com
pare
d w
ith n
on-S
LE
dece
ased
don
or a
llogr
aft r
ecip
ient
s. A
mon
g liv
ing
allo
graf
t

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
reci
pien
ts, t
here
wer
e no
sig
nific
ant d
iffer
ence
s in
eith
er a
llogr
aft
or re
cipi
ent s
urvi
val c
ompa
red
with
non
-SLE
reci
pien
ts.
CO
NC
LUSI
ON
S: S
LE a
s a
caus
e of
ES
RD
in re
nal t
rans
plan
t re
cipi
ents
is a
ssoc
iate
d w
ith w
orse
allo
graf
t and
reci
pien
t sur
viva
l co
mpa
red
with
DM
; thi
s as
soci
atio
n is
true
for t
he e
ntire
po
pula
tion
and
for t
he re
cipi
ents
of d
ecea
sed
dono
r (bu
t not
liv
ing
dono
r) tr
ansp
lant
. Dec
ease
d do
nor a
llogr
aft r
ecip
ient
s ha
ve
wor
se o
utco
mes
com
pare
d w
ith li
ving
allo
graf
t rec
ipie
nts.
Tang
H,
Che
lam
char
la M
, Ba
ird B
C, S
hiha
b FS
, Ko
ford
JK,
Gol
dfar
b-R
umya
ntze
v AS
. U
nive
rsity
of U
tah
Scho
ol o
f Med
icin
e
Clin
Tra
nspl
ant.
2008
M
ay-J
un;2
2(3)
:263
-72
.
Fact
ors
affe
ctin
g ki
dney
-tran
spla
nt
outc
ome
in
reci
pien
ts w
ith lu
pus
neph
ritis
.
Usi
ng th
e da
ta fr
om th
e U
nite
d St
ates
Ren
al
Dat
a S
yste
m o
f pat
ient
s tra
nspl
ante
d be
twee
n Ja
nuar
y 1,
199
5 th
roug
h D
ecem
ber 3
1, 2
002
(and
follo
wed
thro
ugh
Dec
embe
r 31,
200
3) (n
= 2
882)
, we
perfo
rmed
a re
trosp
ectiv
e an
alys
is o
f fac
tors
as
soci
ated
with
long
-term
dea
th-c
enso
red
graf
t sur
viva
l and
reci
pien
t sur
viva
l.
RES
ULT
S: T
he n
umbe
r of p
retra
nspl
ant p
regn
anci
es
incr
emen
tally
incr
ease
d th
e ris
k of
gra
ft fa
ilure
[haz
ard
ratio
(HR
) 1.
54, p
< 0
.05]
in th
e en
tire
subg
roup
of f
emal
es a
nd in
the
subg
roup
of r
ecip
ient
s ag
ed 2
5-35
yr.
Rec
ipie
nt a
nd d
onor
age
ha
d an
ass
ocia
tion
with
bot
h th
e ris
k of
gra
ft fa
ilure
(HR
0.9
6, p
<
0.00
1; H
R 1
.01,
p <
0.0
05) a
nd re
cipi
ent d
eath
(HR
1.0
4, p
<
0.00
1; H
R 1
.01,
p<
0.05
). G
reat
er g
raft-
failu
re ri
sk a
ccom
pani
ed
incr
ease
d re
cipi
ent w
eigh
t (H
R 1
.01,
p <
0.0
01);
Afric
an
Amer
ican
s co
mpa
red
with
whi
tes
(HR
1.5
5, p
< 0
.001
); gr
eate
r C
harls
on c
omor
bidi
ty in
dex
(HR
1.1
7, p
< 0
.05)
; and
gre
ater
pa
nel r
eact
ive
antib
ody
(PR
A)le
vels
(HR
1.0
6, p
< 0
.001
). Pr
etra
nspl
ant p
erito
neal
dia
lysi
s as
the
pred
omin
ant m
odal
ity
had
an a
ssoc
iatio
n w
ith d
ecre
ased
risk
of g
raft
failu
re (H
R 0
.49,
p
< 0.
001)
, whi
le p
rior t
rans
plan
tatio
n w
as a
ssoc
iate
d w
ith
grea
ter r
isk
of g
raft
failu
re a
nd re
cipi
ent d
eath
(HR
2.2
9, p
<
0.00
1; H
R 3
.59,
p <
0.0
01, r
espe
ctiv
ely)
com
pare
d w
ith
hem
odia
lysi
s (H
D).
The
num
ber o
f mat
ched
hum
an le
ukoc
yte
antig
ens
(HLA
) ant
igen
s an
d liv
ing
dono
rs (H
R 0
.92,
p <
0.0
5;
HR
0.6
4, p
< 0
.001
, res
pect
ivel
y) w
as a
ssoc
iate
d w
ith d
ecre
ased
ris
k of
gra
ft fa
ilure
. Inc
reas
ed ri
sk o
f gra
ft fa
ilure
and
reci
pien
t de
ath
was
ass
ocia
ted
with
non
use
of c
alci
neur
in in
hibi
tors
(HR
1.
89, p
< 0
.005
; HR
1.8
0, p
< 0
.005
) and
myc
ophe
nolic
aci
d (M
PA) (
incl
udin
g m
ycop
heno
late
mof
etil
and
MP
A) o
r az
athi
oprin
e (H
R 1
.41,
p <
0.0
5; H
R 1
.66,
p <
0.0
1). U
sing
bot
h cy
clos
porin
e an
d ta
crol
imus
was
ass
ocia
ted
with
incr
ease
d ris
k of
gra
ft fa
ilure
(HR
2.0
9, p
< 0
.05)
. Usi
ng M
PA
is a
ssoc
iate
d w
ith
grea
ter r
isk
of re
cipi
ent d
eath
com
pare
d w
ith a
zath
iopr
ine
(HR
1.
47,p
< 0
.05)
. CO
NC
LUS
ION
: In
rena
l tra
nspl
ant r
ecip
ient
s w
ith
lupu
s ne
phrit
is, m
ultip
le p
regn
anci
es, m
ultip
le b
lood
tran
sfus
ions
, gr
eate
r com
orbi
dity
inde
x, h
ighe
r bod
y w
eigh
t, ag
e an
d Af
rican
Am
eric
an ra
ce o
f the
don
or o
r rec
ipie
nt, p
rior h
isto
ry o
f

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
trans
plan
tatio
n, g
reat
er P
RA
leve
ls, l
ower
leve
l of H
LA m
atch
ing,
de
ceas
ed d
onor
s, a
nd H
D in
pre
trans
plan
t per
iod
have
an
asso
ciat
ion
with
incr
ease
d ris
k of
gra
ft fa
ilure
. Sim
ilarly
, hig
her
reci
pien
t and
don
or a
ge, p
rior t
rans
plan
tatio
ns, a
nd h
ighe
r rat
e of
pr
etra
nspl
ant t
rans
fusi
ons
are
asso
ciat
ed w
ith g
reat
er ri
sk o
f re
cipi
ent m
orta
lity.
Usi
ng n
eith
er c
yclo
spor
ine
nor t
acro
limus
or
usin
g bo
th (c
ompa
red
with
tacr
olim
us) a
nd n
eith
er M
PA
nor
azat
hiop
rine
(com
pare
d w
ith a
zath
iopr
ine)
was
ass
ocia
ted
with
in
crea
sed
risk
of g
raft
failu
re a
nd re
cipi
ent d
eath
. Usi
ng M
PA is
as
soci
ated
with
gre
ater
risk
of r
ecip
ient
dea
th c
ompa
red
with
az
athi
oprin
e. T
estin
g th
ese
resu
lts in
a p
rosp
ectiv
e st
udy
mig
ht
prov
ide
impo
rtant
info
rmat
ion
for c
linic
al p
ract
ice.
War
d M
M.
NIH
/NIA
MS
/IRP
J
Rhe
umat
ol. 2
009
Jan;
36(1
):63-
7.
Cha
nges
in th
e in
cide
nce
of
ends
tage
rena
l di
seas
e du
e to
lupu
s ne
phrit
is in
the
Uni
ted
Stat
es, 1
996-
2004
.
Patie
nts
age
15 y
ears
or o
lder
with
inci
dent
ES
RD
due
to lu
pus
neph
ritis
in 1
996-
2004
an
d liv
ing
in o
ne o
f the
50 U
nite
d St
ates
or
the
Dis
trict
of C
olum
bia
wer
e id
entif
ied
usin
g th
e U
S R
enal
Dat
a S
yste
m, a
nat
iona
l po
pula
tion-
base
d re
gist
ry o
f all
patie
nts
rece
ivin
g re
nal r
epla
cem
ent t
hera
py fo
r ES
RD
. Inc
iden
ce ra
tes
wer
e co
mpu
ted
for
each
cal
enda
r yea
r, us
ing
popu
latio
n es
timat
es o
f the
US
cens
us a
s de
nom
inat
ors.
RES
ULT
S: O
ver t
he 9
-yea
r stu
dy p
erio
d, 9
199
new
cas
es o
f ES
RD
due
to lu
pus
neph
ritis
wer
e ob
serv
ed. I
ncid
ence
rate
s,
adju
sted
to th
e ag
e, s
ex, a
nd ra
ce c
ompo
sitio
n of
the
US
popu
latio
n in
200
0, w
ere
4.4
per m
illio
n in
199
6 an
d 4.
9 pe
r m
illion
in 2
004.
Com
pare
d to
the
pool
ed in
cide
nce
rate
in 1
996-
1998
, the
rela
tive
risk
of E
SRD
due
to lu
pus
neph
ritis
in 1
999-
2000
was
0.9
9 (9
5% C
I 0.9
3-1.
06),
in 2
001-
2002
was
0.9
9 (9
5%
CI 0
.92-
1.06
), an
d in
200
3-20
04 w
as 0
.96
(95%
CI 0
.89-
1.02
). Fi
ndin
gs w
ere
sim
ilar i
n an
alys
es s
tratif
ied
by s
ex, a
ge g
roup
, ra
ce, a
nd s
ocio
econ
omic
sta
tus.
CO
NC
LUS
ION
: The
re w
as n
o de
crea
se in
the
inci
denc
e of
ESR
D d
ue to
lupu
s ne
phrit
is
betw
een
1996
and
200
4. T
his
may
refle
ct th
e lim
its o
f ef
fect
iven
ess
of c
urre
nt tr
eatm
ents
, or l
imita
tions
in a
cces
s, u
se,
or a
dher
ence
to tr
eatm
ent.
Burg
os P
I, Pe
rkin
s EL
, Pon
s-Es
tel G
J,
Kend
rick
SA, L
iu J
M,
Kend
rick
WT,
Coo
k W
J, J
ulia
n B
A,
Alar
cón
GS,
Kew
CE
2n
d. U
nive
rsity
of
Alab
ama
at
Birm
ingh
am A
rthrit
is
Rhe
um. 2
009
Sep;
60(9
):275
7-66
.
Ris
k fa
ctor
s an
d im
pact
of r
ecur
rent
lu
pus
neph
ritis
in
patie
nts
with
sy
stem
ic lu
pus
eryt
hem
atos
us
unde
rgoi
ng re
nal
trans
plan
tatio
n: d
ata
from
a s
ingl
e U
S in
stitu
tion.
The
arch
ival
reco
rds
of a
ll ki
dney
tran
spla
nt
reci
pien
ts w
ith a
prio
r dia
gnos
is o
f SLE
(a
ccor
ding
to th
e Am
eric
an C
olle
ge o
f R
heum
atol
ogy
crite
ria) f
rom
Jun
e 19
77 to
Ju
ne 2
007
wer
e re
view
ed. P
atie
nts
who
had
di
ed o
r los
t the
allo
graf
t with
in 9
0 da
ys o
f en
graf
tmen
t wer
e ex
clud
ed. T
ime-
to-e
vent
da
ta w
ere
exam
ined
by
univ
aria
ble
and
mul
tivar
iabl
e C
ox p
ropo
rtion
al h
azar
ds
regr
essi
on a
naly
ses.
RES
ULT
S: T
wo
hund
red
twen
ty o
f nea
rly 7
,000
rena
l tra
nspl
anta
tions
wer
e pe
rform
ed in
202
SLE
pat
ient
s du
ring
the
30-y
ear i
nter
val.
Of t
he 1
77 p
atie
nts
who
met
the
crite
ria fo
r st
udy
entry
, the
maj
ority
wer
e w
omen
(80%
) and
Afri
can
Amer
ican
(65%
), th
e m
ean
age
was
35.
6 ye
ars,
and
the
mea
n di
seas
e du
ratio
n w
as 1
1.2
year
s. R
ecur
rent
lupu
s ne
phrit
is w
as
note
d in
20
patie
nts
(11%
), al
logr
aft l
oss
in 6
9 pa
tient
s (3
9%),
and
deat
h in
36 p
atie
nts
(20%
). Af
rican
Am
eric
an e
thni
city
was
fo
und
to b
e as
soci
ated
with
a s
horte
r tim
e-to
-eve
nt fo
r rec
urre
nt
lupu
s ne
phrit
is (h
azar
d ra
tio [H
R] 4
.63,
95%
con
fiden
ce in
terv
al
[95%
CI]
1.29
-16.
65) a
nd d
eath
(HR
2.4
7, 9
5% C
I 0.9
1-6.
71),
alth
ough
, with
the
latte
r, th
e as
soci
atio
n w
as n
ot s
tatis
tical
ly
sign
ifica
nt. R
ecur
rent
lupu
s ne
phrit
is a
nd c
hron
ic re
ject
ion
of th
e ki
dney
tran
spla
nt w
ere
foun
d to
be
risk
fact
ors
for a
llogr
aft l
oss
(HR
2.4
8, 9
5% C
I 1.0
9-5.
60 a
nd H
R 2
.72,
95%
CI 1
.55-
4.78
, re
spec
tivel
y). I
n pa
tient
s w
ith re
curr
ent l
upus
nep
hriti
s, th
e le
sion

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
in th
e en
graf
ted
kidn
ey w
as p
redo
min
antly
mes
angi
al, c
ompa
red
with
a p
redo
min
ance
of p
rolif
erat
ive
or m
embr
anou
s le
sion
s in
th
e na
tive
kidn
eys.
CO
NC
LUSI
ON
: Afri
can
Amer
ican
eth
nici
ty
was
inde
pend
ently
ass
ocia
ted
with
recu
rren
t lup
us n
ephr
itis.
Al
logr
aft l
oss
was
ass
ocia
ted
with
chr
onic
tran
spla
nt re
ject
ion
and
recu
rren
ce o
f lup
us n
ephr
itis.
Rec
urre
nt lu
pus
neph
ritis
is
infre
quen
t and
rela
tivel
y be
nign
, with
out i
nflu
ence
on
a pa
tient
's
surv
ival
.
Lian
g C
C, H
uang
CC
, W
ang
IK, C
hang
CT,
C
hen
KH
, Wen
g C
H,
Lin
JL, H
ung
CC
, Ya
ng C
W, Y
en T
H.
Chi
na M
edic
al
Uni
vers
ity H
ospi
tal,
Taic
hung
, Tai
wan
Th
er A
pher
Dia
l. 20
10 F
eb;1
4(1)
:35-
42.
Impa
ct o
f ren
al
surv
ival
on
the
cour
se a
nd o
utco
me
of s
yste
mic
lupu
s er
ythe
mat
osus
pa
tient
s tre
ated
with
ch
roni
c pe
riton
eal
dial
ysis
.
This
long
itudi
nal s
tudy
inve
stig
ated
whe
ther
re
nal s
urvi
val c
an a
ffect
the
cour
se a
nd
outc
ome
of s
yste
mic
lupu
s er
ythe
mat
osus
(S
LE) p
atie
nts
treat
ed w
ith c
hron
ic
perit
onea
l dia
lysi
s (P
D).
Thirt
y-fiv
e SL
E pa
tient
s, o
ut o
f 111
5 en
d-st
age
rena
l di
seas
e (E
SR
D) p
atie
nts
treat
ed w
ith
chro
nic
PD
, wer
e se
en b
etw
een
1990
and
20
07 a
t the
Cha
ng G
ung
Mem
oria
l Hos
pita
l. Pa
tient
s w
ere
follo
wed
up
for a
mea
n of
38
.8 +
/-22
.9 m
onth
s.
Ther
e w
ere
no s
igni
fican
t diff
eren
ces
betw
een
patie
nts
with
sho
rt re
nal s
urvi
val (
<3 y
ears
) and
long
rena
l sur
viva
l (>3
yea
rs) f
or th
e va
rious
dem
ogra
phic
var
iabl
es s
uch
as a
ge, s
ex, P
D d
urat
ion,
im
mun
osup
pres
sive
dru
g ad
min
istra
tion,
or e
xcha
nge
syst
em (P
>
0.05
). In
tere
stin
gly,
bef
ore
PD, p
atie
nts
with
sho
rt re
nal
surv
ival
had
low
er s
erum
com
plem
ent l
evel
s th
an p
atie
nts
with
lo
ng re
nal s
urvi
val (
C3,
40.
2 +/
-14.
4 vs
76.
3 +/
-18.
5 m
g/dL
, P <
0.
001;
and
C4,
14.
8 +/
-4.7
vs
22.4
+/-
8.1
mg/
dL, P
< 0
.05)
. H
owev
er, t
he d
iffer
ence
s in
com
plem
ent l
evel
s be
twee
n th
e gr
oups
dis
appe
ared
afte
r PD
(C3,
76.
5 +/
-27.
3 vs
84.
2 +/
-27.
8 m
g/dL
; and
C4,
26.
7 +/
-11.
3 vs
22.
6 +/
-10.
8 m
g/dL
, bot
h P
> 0.
05).
Patie
nts
with
sho
rt re
nal s
urvi
val w
ere
mor
e lik
ely
to h
ave
a hi
gh p
erito
neal
sol
ute
trans
porte
r rat
e (P
STR
) tha
n th
eir l
ong
rena
l sur
viva
l cou
nter
parts
(chi
(2)-
test
, P =
0.0
2, a
nd A
UR
OC
=
0.74
4 an
d P
= 0
.040
); ho
wev
er, t
here
wer
e no
sig
nific
ant
diffe
renc
es fo
r oth
er v
aria
bles
suc
h as
car
diot
hora
cic
ratio
(CTR
), Kt
/V, r
esid
ual r
enal
func
tion,
exi
t site
infe
ctio
n, a
nd p
erito
nitis
(P
> 0.
05).
Fina
lly, K
apla
n-M
eier
ana
lysi
s re
veal
ed th
at th
e tw
o gr
oups
did
not
diff
er in
pat
ient
and
tech
nica
l sur
viva
l (P
> 0.
05).
Ther
efor
e it
was
con
clud
ed th
at re
nal s
urvi
val m
ight
be
asso
ciat
ed w
ith P
STR
, but
not
with
pat
ient
and
tech
nica
l sur
viva
l in
SLE
pat
ient
s tre
ated
with
PD
.

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
Nor
by G
E, S
trøm
EH
, M
idtv
edt K
, Har
tman
n A,
Gilb
oe IM
, Le
ives
tad
T,
Ste
nstrø
m J
, Hol
daas
H
. O
slo
Uni
vers
ity
Hos
pita
l, N
orw
ay.
A
nn R
heum
Dis
. 20
10
Aug;
69(8
):148
4-7.
Ep
ub 2
010
May
24.
Rec
urre
nt lu
pus
neph
ritis
afte
r kid
ney
trans
plan
tatio
n: a
su
rvei
llanc
e bi
opsy
st
udy.
All p
atie
nts
with
SLE
that
had
und
ergo
ne
trans
plan
t with
a fu
nctio
ning
gra
ft w
ere
aske
d in
200
8 to
par
ticip
ate
in a
cro
ss-
sect
iona
l stu
dy. T
he s
tudy
incl
uded
a
stan
dard
ised
clin
ical
exam
inat
ion,
labo
rato
ry
test
s an
d a
biop
sy o
f the
tran
spla
nted
ki
dney
.
RES
ULT
S: A
tota
l of 4
1 (9
3%) o
f a c
ohor
t of 4
4 pa
tient
s w
ith
SLE
with
rena
l tra
nspl
ants
par
ticip
ated
. Of t
he b
iops
ies,
3 w
ere
indi
catio
n bi
opsi
es a
nd 3
8 w
ere
surv
eilla
nce
biop
sies
. In
all,
22
patie
nts
(54%
) had
bio
psy-
prov
en re
curr
ence
of L
N. T
he m
ajor
ity
of th
e ca
ses
wer
e su
bclin
ical
and
cha
ract
eris
ed a
s cl
ass
I/cla
ss II
LN
. Pro
tein
uria
(mg
prot
ein/
mm
ol c
reat
inin
e) w
as s
igni
fican
tly
incr
ease
d in
pat
ient
s w
ith re
curr
ence
, 70.
6 (1
04.9
) mg/
mm
ol
vers
us 1
1.9
(6.7
) mg/
mm
ol in
pat
ient
s w
ithou
t rec
urre
nce
(p=0
.038
). Lu
pus
antic
oagu
lant
was
foun
d m
ore
frequ
ently
in th
e pa
tient
s w
ith re
curr
ence
, nin
e ve
rsus
two
patie
nts
(p=0
.033
). R
ecur
renc
e of
LN
was
ass
ocia
ted
with
rece
ivin
g a
kidn
ey fr
om a
liv
ing
dono
r (p=
0.04
9). I
n al
l, 83
% (3
4 of
41)
had
chr
onic
allo
graf
t ne
phro
path
y in
the
trans
plan
ted
kidn
eys
with
no
diffe
renc
e be
twee
n pa
tient
s w
ith re
curr
ence
or w
ithou
t. C
ON
CLU
SIO
NS:
Su
bclin
ical
recu
rren
ce o
f LN
is c
omm
on in
pat
ient
s w
ith re
nal
trans
plan
tsw
ith S
LE. T
he m
ajor
ity o
f the
pat
ient
s ha
ve c
hron
ic
allo
graf
t nep
hrop
athy
.Bu
mga
rdne
r GL,
M
auer
SM
, Pay
ne W
, D
unn
DL,
Sut
herla
nd
DE
, Fry
d D
S, A
sche
r N
L, S
imm
ons
RL,
N
ajar
ian
JS.
Uni
vers
ity o
f M
inne
sota
, M
inne
apol
is
Tran
spla
ntat
ion.
198
8 N
ov;4
6(5)
:703
-9.
Sing
le-c
ente
r 1-1
5-ye
ar re
sults
of r
enal
tra
nspl
anta
tion
in
patie
nts
with
sy
stem
ic lu
pus
eryt
hem
atos
us.
How
ever
, sin
ce th
e lo
ng-te
rm o
utco
me
afte
r tra
nspl
anta
tion
in th
is g
roup
of p
atie
nts
is
not w
ell e
stab
lishe
d, w
e ha
ve e
xam
ined
the
long
-term
out
com
e in
SLE
pat
ient
s w
ho
unde
rwen
t ren
al tr
ansp
lant
atio
n at
the
Uni
vers
ity o
f Min
neso
ta. T
hirty
-two
SLE
pa
tient
s re
ceiv
ing
33 tr
ansp
lant
s be
twee
n D
ecem
ber 1
969
and
Dec
embe
r 198
7 w
ere
stud
ied
retro
spec
tivel
y an
d co
mpa
red
with
co
ntro
ls m
atch
ed fo
r age
, sex
, don
orso
urce
, HLA
mat
ch, d
ate
of tr
ansp
lant
, and
di
abet
ic s
tatu
s.
A to
tal o
f 69%
(22/
32) o
f pat
ient
s un
derw
ent l
ess
than
1 y
ear o
f di
alys
is p
rior t
o tra
nspl
anta
tion,
and
50%
(16/
32) e
xper
ienc
ed
biop
sy-p
rove
d ac
ute
reje
ctio
n, w
hich
was
reve
rsib
le in
67%
(1
1/16
).Ac
tuar
ial g
raft
func
tion
and
patie
nt s
urvi
val r
ate
in S
LE
patie
nts
wer
e no
t sig
nific
antly
diff
eren
t fro
m th
ose
in th
e m
atch
ed
cont
rol g
roup
. Dur
atio
n of
prio
r dia
lysi
s di
d no
t affe
ct o
utco
me.
Su
rviv
ing
graf
ts h
ave
exce
llent
func
tion
as m
easu
red
by s
erum
cr
eatin
ine
(1.3
+/-
0.4
mg/
dl, m
eans
+/-
SD).
Cau
ses
of d
eath
w
ere
seps
is (5
) and
myo
card
ial i
nfar
ctio
n (1
). O
ne p
atie
nt lo
st th
e gr
aft f
rom
reje
ctio
n af
ter w
ithdr
awal
of i
mm
unos
uppr
essi
on
beca
use
of a
mal
igna
ncy
one
mon
th p
osttr
ansp
lant
. Thr
ee
patie
nts
lost
gra
ft fu
nctio
n du
e to
chr
onic
reje
ctio
n. T
o da
te n
o pa
tient
s ha
ve h
ad e
vide
nce
of re
curr
ent S
LE n
ephr
itis.
Pollo
ck C
A, Ib
els
LS.
Roy
al N
orth
Sho
re
Hos
pita
l, N
SW.
Aus
t N
Z J
Med
. 198
7 Ju
n;17
(3):3
21-5
.
Dia
lysi
s an
d tra
nspl
anta
tion
in
patie
nts
with
rena
lfa
ilure
due
to
syst
emic
lupu
s er
ythe
mat
osus
. The
A
ustra
lian
and
New
Ze
alan
d ex
perie
nce.
Betw
een
1977
and
198
5, 5
726
patie
nts
in
Aust
ralia
and
New
Zea
land
ent
ered
end
st
age
rena
l fai
lure
pro
gram
mes
. Of t
hese
, 63
pat
ient
s ha
d re
nal f
ailu
re d
ue to
sys
tem
ic
lupu
s er
ythe
mat
osus
(a p
reva
lenc
e of
1.1
%
of p
atie
nts
ente
ring
rena
l rep
lace
men
t pr
ogra
mm
es).
Whe
n co
mpa
red
with
pat
ient
s w
ith o
ther
form
s of
gl
omer
ulon
ephr
itis,
ther
e w
as a
fem
ale
prep
onde
ranc
e an
d a
youn
ger a
ge d
istri
butio
n in
pat
ient
s w
ith re
nal f
ailu
redu
e to
lupu
s ne
phrit
is. I
nteg
rate
d pa
tient
, dia
lysi
s, a
nd tr
ansp
lant
sur
viva
l dat
a sh
owed
that
resu
lts in
pat
ient
s w
ith re
nal f
ailu
re d
ue to
lupu
s ne
phrit
is w
ere
com
para
ble
with
thos
e in
pat
ient
s w
ith o
ther
form
s of
glo
mer
ulon
ephr
itis
or in
pat
ient
s w
ith re
nal f
ailu
re d
ue to
any
ca
use.
Age
at e
ntry
sig
nific
antly
affe
cted
sur
viva
l, w
ith s
igni
fican
t di
ffere
nces
bei
ng fo
und
in th
ose
patie
nts
unde
r as
oppo
sed
to
over
50
year
s of
age
. Cau
ses
of d
eath
in p
atie
nts
with
lupu
s ne
phrit
is w
ere
sim
ilar t
o th
ose
in p
atie
nts
with
rena
l fai
lure
due
to
othe
r cau
ses.
It is
con
clud
ed th
at d
ialy
sis
and
trans
plan
tatio
n ar
e

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
acce
ptab
le fo
rms
of tr
eatm
ent f
or p
atie
nts
with
end
sta
ge re
nal
failu
re d
ue to
sys
tem
ic lu
pus
eryt
hem
atos
us.
Loch
head
KM
, Pirs
ch
JD, D
'Ale
ssan
dro
AM, K
nech
tle S
J,
Kala
yogl
u M
, So
lling
er H
W, B
elze
r FO
. U
nive
rsity
of
Wis
cons
in H
ospi
tal
and
Clin
ics
Kid
ney
Int.
1996
Fe
b;49
(2):5
12-7
.
Ris
k fa
ctor
s fo
r ren
al
allo
graf
t los
s in
pa
tient
s w
ith
syst
emic
lupu
s er
ythe
mat
osus
.
This
stu
dy is
a re
trosp
ectiv
e ev
alua
tion
ofea
ch o
f the
se in
depe
nden
t ris
k fa
ctor
s in
80
rena
l tra
nspl
ants
for E
SRD
sec
onda
ry to
SL
E do
ne a
t our
inst
itutio
n be
twee
n 19
71
and
1994
. Our
ent
ire n
on-d
iabe
tic c
ohor
t of
1,96
6 re
nal t
rans
plan
ts is
use
d as
a
com
paris
on g
roup
.
Our
resu
lts s
how
ed e
quiv
alen
t gra
ft su
rviv
al ra
tes
betw
een
lupu
s pa
tient
s an
d th
e co
hort
at 1
, 5 a
nd 1
0 ye
ars
(P =
0.5
6). H
owev
er,
an a
naly
sis
of c
yclo
spor
ine-
era
cada
ver g
rafts
reve
aled
that
the
lupu
s gr
oup
had
poor
er 5
-yea
r gra
ft su
rviv
al th
an th
e co
hort
(41%
vs.
71%
, P =
0.0
2). E
valu
atio
n of
cyc
losp
orin
e-er
a lu
pus
graf
t sur
viva
l sho
wed
sig
nific
antly
impr
oved
out
com
e in
livi
ng-
rela
ted
lupu
s re
cipi
ents
ove
r cad
aver
gra
fts a
t fiv
e ye
ars
(89%
vs
. 41%
, P =
0.0
03).
The
maj
ority
of g
rafts
lost
in th
e lu
pus
cada
ver r
ecip
ient
s w
ere
due
to c
hron
ic re
ject
ion.
Rej
ectio
n w
as
incr
ease
d in
lupu
s re
cipi
ents
: 69%
of l
upus
pat
ient
s ex
perie
nced
re
ject
ion
in th
e fir
st y
ear c
ompa
red
to 5
8% o
f con
trols
(P =
0.0
1).
Stra
tifie
d fo
r age
, sex
, rac
e an
d cy
clos
porin
e us
e, th
is d
iffer
ence
re
mai
ned
sign
ifica
nt (P
=0.
003,
rela
tive
risk
1.7)
. Nep
hrec
tom
y,
sple
nect
omy
and
3 to
6 m
onth
s of
pre
trans
plan
t dia
lysi
s di
d no
t im
prov
e gr
aft s
urvi
val.
A di
alys
is d
urat
ion
of g
reat
er th
an 2
5 m
onth
s pr
edic
ted
wor
se g
raft
surv
ival
(P =
0.0
1). A
mon
g lu
pus
patie
nts,
PR
A di
d no
t cor
rela
te w
ith g
raft
outc
ome
(P =
0.5
), an
d H
LA-id
entic
al c
adav
er g
rafts
had
impr
oved
out
com
es c
ompa
red
to c
adav
er g
rafts
. We
conc
lude
that
acu
te a
nd c
hron
ic re
ject
ion
are
the
maj
or ri
sk fa
ctor
s fo
r gra
ft lo
ss in
lupu
s pa
tient
s. T
he
supe
rior o
utco
me
of li
ving
-rel
ated
ove
r cad
aver
gra
fts in
lupu
s pa
tient
s su
gges
ts a
n in
crea
sed
role
for l
ivin
g-re
late
d gr
afts
. Pr
etra
nspl
ant d
ialy
sis,
nep
hrec
tom
y an
d sp
lene
ctom
y ar
e no
t in
dica
ted.
Hau
bitz
M, K
liem
V,
Koch
KM
, Nas
han
B,
Schl
itt H
J, P
ichl
may
r R
, Bru
nkho
rst R
. M
edic
al S
choo
l H
anno
ver,
Ger
man
y.
Tran
spla
ntat
ion.
199
7 M
ay 1
5;63
(9):1
251-
7.
Ren
al
trans
plan
tatio
n fo
r pa
tient
s w
ith
auto
imm
une
dise
ases
: sin
gle-
cent
er e
xper
ienc
e w
ith 4
2 pa
tient
s.
Long
-term
gra
ft su
rviv
al a
nd g
raft
func
tion
of
rena
l tra
nspl
ant r
ecip
ient
s w
ith S
LE,
Weg
ener
's g
ranu
lom
atos
is, m
icro
scop
ic
poly
angi
itis,
Goo
dpas
ture
's s
yndr
ome,
and
H
enoc
h-Sc
honl
ein
purp
ura
wer
e ev
alua
ted
in a
sin
gle
cent
er. I
n ad
ditio
n, th
e in
cide
nce
of re
nal a
nd e
xtra
rena
l rel
apse
s an
d th
e im
pact
of t
he im
mun
osup
pres
sive
ther
apy
on th
e co
urse
of t
he a
utoi
mm
une
dise
ase
RES
ULT
S: R
enal
tran
spla
nt re
cipi
ents
with
aut
oim
mun
e di
seas
es s
uch
as v
ascu
litis
and
SLE
had
a p
atie
nt s
urvi
val r
ate
(94%
afte
r 5 y
ears
) and
a g
raft
surv
ival
rate
(65%
afte
r 5 y
ears
) co
mpa
rabl
e to
thos
e of
pat
ient
s w
ith o
ther
cau
ses
of e
nd-s
tage
re
nal d
isea
se (p
atie
nt s
urvi
val 8
8% a
nd g
raft
surv
ival
71%
afte
r 5
year
s). G
raft
loss
es d
ue to
the
unde
rlyin
g di
seas
e w
ere
rare
. Ex
trare
nal r
elap
ses
occu
rred
in th
ree
patie
nts
with
Weg
ener
's
gran
ulom
atos
is, o
ne p
atie
nt w
ith m
icro
scop
ic p
olya
ngiit
is, a
nd
thre
e pa
tient
s w
ith S
LE, b
ut w
ere
less
freq
uent
com
pare
d w
ith
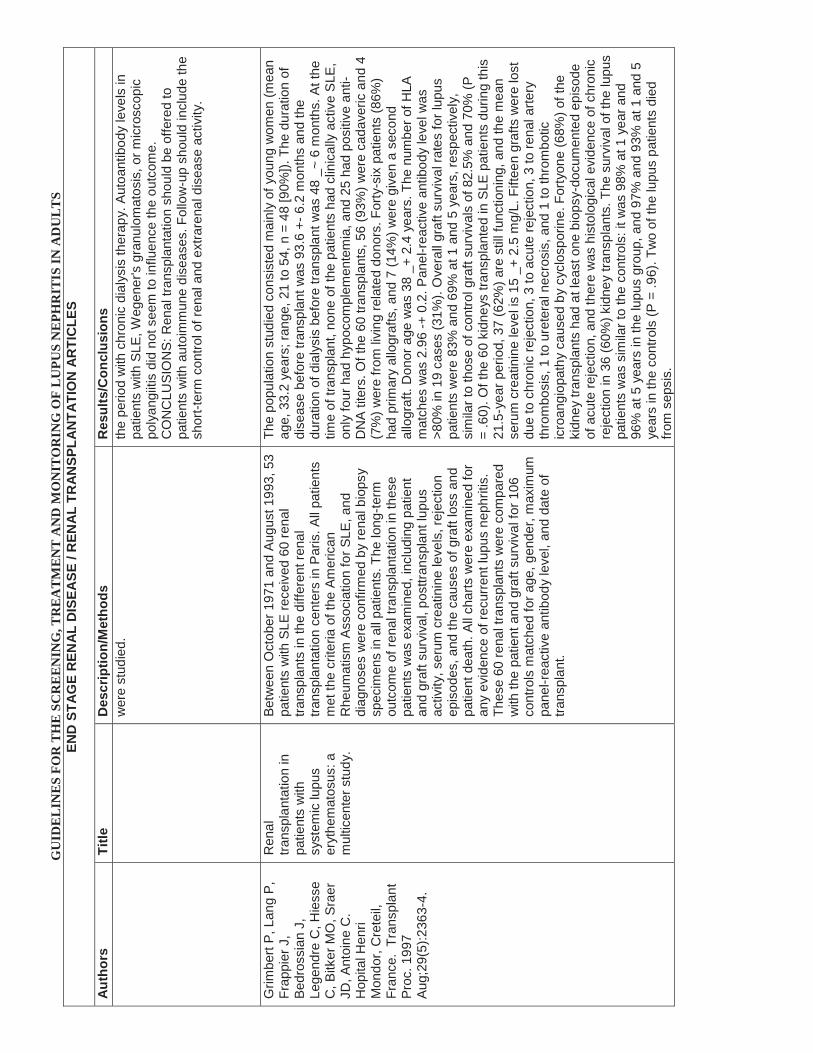
GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
wer
e st
udie
d.th
e pe
riod
with
chr
onic
dia
lysi
s th
erap
y. A
utoa
ntib
ody
leve
ls in
pa
tient
s w
ith S
LE, W
egen
er's
gra
nulo
mat
osis
, or m
icro
scop
ic
poly
angi
itis
did
not s
eem
toin
fluen
ce th
e ou
tcom
e.
CO
NC
LUSI
ON
S: R
enal
tran
spla
ntat
ion
shou
ld b
e of
fere
d to
pa
tient
s w
ith a
utoi
mm
une
dise
ases
. Fol
low
-up
shou
ld in
clud
e th
e sh
ort-t
erm
con
trol o
f ren
al a
nd e
xtra
rena
l dis
ease
act
ivity
.
Grim
bert
P, L
ang
P,
Frap
pier
J,
Bedr
ossi
an J
, Le
gend
re C
, Hie
sse
C, B
itker
MO
, Sra
er
JD, A
ntoi
ne C
. H
opita
l Hen
ri M
ondo
r, C
rete
il,
Fran
ce.
Tran
spla
nt
Proc
. 199
7 Au
g;29
(5):2
363-
4.
Ren
al
trans
plan
tatio
n in
pa
tient
s w
ith
syst
emic
lupu
s er
ythe
mat
osus
: a
mul
ticen
ter s
tudy
.
Betw
een
Oct
ober
197
1 an
d Au
gust
199
3, 5
3 pa
tient
s w
ith S
LE re
ceiv
ed 6
0 re
nal
trans
plan
ts in
the
diffe
rent
rena
l tra
nspl
anta
tion
cent
ers
in P
aris
. All
patie
nts
met
the
crite
ria o
f the
Am
eric
an
Rhe
umat
ism
Ass
ocia
tion
for S
LE, a
nd
diag
nose
s w
ere
conf
irmed
by
rena
l bio
psy
spec
imen
s in
all
patie
nts.
The
long
-term
ou
tcom
e of
rena
l tra
nspl
anta
tion
in th
ese
patie
nts
was
exa
min
ed, i
nclu
ding
pat
ient
an
d gr
aft s
urvi
val,
post
trans
plan
t lup
us
activ
ity, s
erum
cre
atin
ine
leve
ls, r
ejec
tion
epis
odes
, and
the
caus
es o
f gra
ft lo
ss a
nd
patie
nt d
eath
. All
char
ts w
ere
exam
ined
for
any
evid
ence
of r
ecur
rent
lupu
s ne
phrit
is.
Thes
e 60
rena
l tra
nspl
ants
wer
e co
mpa
red
with
the
patie
nt a
nd g
raft
surv
ival
for 1
06
cont
rols
mat
ched
for a
ge, g
ende
r, m
axim
um
pane
l-rea
ctiv
e an
tibod
y le
vel,
and
date
of
trans
plan
t.
The
popu
latio
n st
udie
d co
nsis
ted
mai
nly
of y
oung
wom
en (m
ean
age,
33.
2 ye
ars;
rang
e, 2
1 to
54,
n =
48
[90%
]). T
he d
urat
ion
of
dise
ase
befo
re tr
ansp
lant
was
93.
6 +-
6.2
mon
ths
and
the
dura
tion
of d
ialy
sis
befo
re tr
ansp
lant
was
48
_~ 6
mon
ths.
At t
he
time
of tr
ansp
lant
, non
e of
the
patie
nts
had
clin
ical
ly a
ctiv
e S
LE,
only
four
had
hyp
ocom
plem
ente
mia
, and
25
had
posi
tive
anti-
DN
A tit
ers.
Of t
he 6
0 tra
nspl
ants
, 56
(93%
) wer
e ca
dave
ric a
nd 4
(7
%) w
ere
from
livi
ng re
late
d do
nors
. For
ty-s
ix p
atie
nts
(86%
) ha
d pr
imar
y al
logr
afts
, and
7 (1
4%) w
ere
give
n a
seco
nd
allo
graf
t. D
onor
age
was
38
_+ 2
.4 y
ears
. The
num
ber o
f HLA
m
atch
es w
as 2
.96
-+ 0
.2. P
anel
-rea
ctiv
e an
tibod
y le
vel w
as
>80%
in 1
9 ca
ses
(31%
). O
vera
ll gr
aft s
urvi
val r
ates
for l
upus
pa
tient
s w
ere
83%
and
69%
at 1
and
5 y
ears
, res
pect
ivel
y,
sim
ilar t
o th
ose
of c
ontro
l gra
ft su
rviv
als
of 8
2.5%
and
70%
(P
= .6
0). O
f the
60
kidn
eys
trans
plan
ted
in S
LE p
atie
nts
durin
g th
is
21.5
-yea
r per
iod,
37
(62%
) are
stil
l fun
ctio
ning
, and
the
mea
n se
rum
cre
atin
ine
leve
l is
15 _
+ 2.
5 m
g/L.
Fifte
en g
rafts
wer
e lo
st
due
to c
hron
ic re
ject
ion,
3 to
acu
te re
ject
ion,
3 to
rena
l arte
ry
thro
mbo
sis,
1 to
ure
tera
l nec
rosi
s, a
nd 1
to th
rom
botic
ic
roan
giop
athy
cau
sed
by c
yclo
spor
ine.
For
tyon
e (6
8%) o
f the
ki
dney
tran
spla
nts
had
at le
ast o
ne b
iops
y-do
cum
ente
d ep
isod
e of
acu
te re
ject
ion,
and
ther
e w
as h
isto
logi
cal e
vide
nce
of c
hron
ic
reje
ctio
n in
36
(60%
) kid
ney
trans
plan
ts. T
he s
urvi
val o
f the
lupu
s pa
tient
s w
as s
imila
r to
the
cont
rols
: it w
as 9
8% a
t 1 y
ear a
nd
96%
at 5
yea
rs in
the
lupu
s gr
oup,
and
97%
and
93%
at 1
and
5
year
s in
the
cont
rols
(P =
.96)
. Tw
o of
the
lupu
s pa
tient
s di
ed
from
sep
sis.

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
Ston
e JH
, Mill
war
d C
L, O
lson
JL,
Am
end
WJ,
Cris
wel
l LA
.
Uni
vers
ity o
f C
alifo
rnia
, San
Fr
anci
sco
Arth
ritis
R
heum
. 199
8 Ap
r;41(
4):6
78-8
6.
Freq
uenc
y of
re
curr
ent l
upus
ne
phrit
is a
mon
g ni
nety
-sev
en re
nal
trans
plan
t pat
ient
s du
ring
the
cycl
ospo
rine
era.
We
revi
ewed
the
post
trans
plan
t clin
ical
co
urse
and
rena
l bio
psy
resu
lts in
97
cons
ecut
ive
SLE
patie
nts
who
und
erw
ent a
to
tal o
f 106
rena
l tra
nspl
anta
tion
proc
edur
es
at o
ur c
ente
r fro
m J
anua
ry 1
984
to
Sept
embe
r 199
6.
RES
ULT
S: T
here
wer
e 81
fem
ale
and
16 m
ale
patie
nts,
with
a
mea
n ag
e of
35
year
s. M
ean
dura
tion
of d
ialy
sis
prio
r to
trans
plan
tatio
n w
as 3
3.5
mon
ths;
9 p
atie
nts
wer
e ne
ver d
ialy
zed.
In
all
patie
nts,
the
dise
ase
was
clin
ical
ly a
nd s
erol
ogic
ally
qu
iesc
ent a
t the
tim
e of
tran
spla
ntat
ion.
The
mea
n po
sttra
nspl
anta
tion
follo
wup
per
iod
was
62.
6 m
onth
s. P
atie
nts
unde
rwen
t a to
tal o
f 143
pos
ttran
spla
nt b
iops
ies.
Nin
e pa
tient
s ha
d pa
thol
ogic
evi
denc
e of
recu
rren
t LN
. Six
of t
he p
atie
nts
with
re
curr
ence
had
cad
aver
ic g
rafts
, 2 h
ad li
ving
-rel
ated
gra
fts, a
nd 1
ha
d a
livin
g-un
rela
ted
graf
t. R
ecur
renc
e oc
curr
ed a
n av
erag
e of
3.
1 ye
ars
afte
r tra
nspl
anta
tion;
the
long
est i
nter
val w
as 9
.3 y
ears
an
d th
e sh
orte
st, 5
day
s. H
isto
path
olog
ic d
iagn
oses
on
recu
rren
ce in
clud
ed d
iffus
e pr
olife
rativ
e gl
omer
ulon
ephr
itis,
foca
l pr
olife
rativ
e gl
omer
ulon
ephr
itis,
mem
bran
ous
glom
erul
onep
hriti
s,
and
mes
angi
al g
lom
erul
onep
hriti
s. In
4 p
atie
nts,
recu
rren
t LN
co
ntrib
uted
to g
raft
loss
. Thr
ee o
f the
pat
ient
s w
ith re
curr
ence
ha
d se
rolo
gic
evid
ence
of a
ctiv
e lu
pus,
but
onl
y 1
had
sym
ptom
s of
act
ive
lupu
s (a
rthrit
is).
Thre
e pa
tient
s w
ho lo
st th
eir g
rafts
se
cond
ary
to re
curr
ent L
N u
nder
wen
t sec
ond
rena
l tra
nspl
anta
tion
proc
edur
es a
nd h
ad fu
nctio
ning
graf
ts a
t 7, 3
0,
and
35 m
onth
s, re
spec
tivel
y. C
ON
CLU
SIO
N: I
n th
e la
rges
t sin
gle
med
ical
cen
ter s
erie
s of
rena
l tra
nspl
ant p
atie
nts
with
SLE
, re
curr
ent L
N w
as m
ore
com
mon
than
repo
rted
in th
e lit
erat
ure,
bu
t was
not
alw
ays
asso
ciat
ed w
ith a
llogr
aft l
oss.
Rec
urre
nt L
N
was
ofte
n pr
esen
t in
the
abse
nce
of c
linic
al a
nd s
erol
ogic
ev
iden
ce o
f act
ive
SLE.
Ston
e JH
, Am
end
WJ,
Cris
wel
l LA
. Jo
hns
Hop
kins
U
nive
rsity
Arth
ritis
R
heum
. 199
8 Au
g;41
(8):1
438-
45.
Out
com
e of
rena
l tra
nspl
anta
tion
in
nine
ty-s
even
cy
clos
porin
e-er
a pa
tient
s w
ith
syst
emic
lupu
s er
ythe
mat
osus
and
m
atch
ed c
ontro
ls.
A to
tal o
f 97
SLE
pat
ient
s w
ho u
nder
wen
t re
nal t
rans
plan
tatio
n be
twee
n Ja
nuar
y 19
84
and
Sept
embe
r 199
6 w
ere
sele
cted
for
stud
y an
d w
ere
mat
ched
with
a g
roup
of
non-
SLE
con
trols
(1 c
ontro
l for
eac
h SL
E pa
tient
) who
als
o re
ceiv
ed tr
ansp
lant
s du
ring
that
per
iod.
SLE
pat
ient
s an
d co
ntro
ls
wer
e m
atch
ed o
n 6
cova
riate
s: a
ge, s
ex,
race
, typ
e of
allo
graf
t (ca
dave
ric v
ersu
s liv
ing-
rela
ted)
, num
ber o
f pre
viou
s tra
nspl
ants
, and
yea
r of t
rans
plan
tatio
n. A
ll st
udy
subj
ects
rece
ived
eith
er c
yclo
spor
ine
or F
K-50
6/ta
crol
imus
as
part
of th
eir
imm
unos
uppr
essi
ve re
gim
en. I
n a
rigor
ous
med
ical
reco
rds
revi
ew, t
he s
tatu
s of
eac
h al
logr
aft a
nd th
e ca
use
of e
ach
graf
t los
s
RES
ULT
S: T
he c
ontro
lgro
up in
clud
ed p
atie
nts
with
20
diffe
rent
ca
uses
of e
nd-s
tage
rena
l dis
ease
(ES
RD
). Th
e m
ean
follo
wup
tim
es fo
r the
SLE
pat
ient
s an
d co
ntro
ls w
ere
323
wee
ks a
nd 3
20
wee
ks, r
espe
ctiv
ely.
Dur
ing
the
follo
wup
per
iod,
52
SLE
patie
nts
and
37 c
ontro
ls lo
st th
eir a
llogr
afts
. The
1-,
2-, 5
-, an
d 10
-yea
r al
logr
aft s
urvi
val p
roba
bilit
ies
for t
he 2
gro
ups
(SLE
ver
sus
cont
rols
) wer
e as
follo
ws:
81.
7% v
ersu
s 88
.2%
(1-y
ear)
; 74.
7%
vers
us 8
4.4%
(2-y
ear)
; 45.
9% v
ersu
s 75
.0%
(5-y
ear)
; and
18.
5%
vers
us 3
4.8%
(10-
year
). In
the
mul
tivar
iate
mod
el, t
he re
lativ
e ha
zard
of a
llogr
aft l
oss
asso
ciat
ed w
ith S
LE a
s th
e ca
use
of
ESR
D w
as 2
.1 (9
5% c
onfid
ence
inte
rval
1.0
6-4.
06, P
= 0
.032
8).
The
tota
l num
ber o
f HLA
mis
mat
ches
, sm
okin
g st
atus
, and
de
laye
d al
logr
aft f
unct
ion
wer
e al
so a
ssoc
iate
d w
ith a
llogr
aft l
oss
in th
e m
ultiv
aria
te m
odel
. CO
NC
LUSI
ON
: Com
pare
d w
ith
mat
ched
con
trols
, ren
al tr
ansp
lant
pat
ient
s w
ith S
LE h
ad in
ferio
r tra
nspl
anta
tion
outc
omes
, with
mor
e th
an tw
ice
the
risk
of

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
was
det
erm
ined
.al
logr
aft l
oss.
Grim
bert
P, F
rapp
ier
J, B
edro
ssia
nJ,
Le
gend
re C
, Ant
oine
C
, Hie
sse
C, B
itker
M
O, S
raer
JD
, Lan
g P
. H
ôpita
l Hen
ri M
ondo
r, C
réte
il,
Fran
ce.
Tran
spla
ntat
ion.
199
8 O
ct 2
7;66
(8):1
000-
3.
Long
-term
out
com
e of
kid
ney
trans
plan
tatio
n in
pa
tient
s w
ith
syst
emic
lupu
s er
ythe
mat
osus
: a
mul
ticen
ter s
tudy
. G
roup
e C
oope
ratif
de
Tra
nspl
anta
tion
d'île
de
Fran
ce.
The
patie
nts
rece
ived
thei
r tra
nspl
ants
ove
r a
260-
mon
th p
erio
d (2
1.5
year
s) b
etw
een
Oct
ober
197
1 an
d Au
gust
199
3. T
he
popu
latio
n w
as p
redo
min
antly
wom
en
(90%
), an
d th
e m
ean
age
at th
e tim
e of
the
trans
plan
tatio
n w
as 3
3.2
year
s (r
ange
: 21-
54 y
ears
). Fi
fty-s
ix tr
ansp
lant
s (9
3%) w
ere
from
cad
aver
ic d
onor
s, a
nd 4
(7%
) wer
e fro
m li
ving
-rel
ated
don
ors;
46
patie
nts
(86%
) ha
d pr
imar
y al
logr
afts
, and
7 (1
4%) r
ecei
ved
a se
cond
allo
graf
t. Th
e du
ratio
n of
dis
ease
be
fore
tran
spla
ntat
ion
was
93.
6+/-6
.2
mon
ths,
and
the
dura
tion
of d
ialy
sis
befo
re
trans
plan
tatio
n w
as 4
8+/-6
mon
ths.
RES
ULT
S: N
o pa
tient
had
clin
ical
ly a
ctiv
e sy
stem
ic lu
pus
eryt
hem
atos
us (S
LE) a
t the
tim
e of
tran
spla
ntat
ion.
The
1-y
ear
graf
t and
pat
ient
sur
viva
l rat
es w
ere
83%
and
98%
, and
the
5-ye
ar g
raft
and
patie
nt s
urvi
val r
ates
wer
e 69
% a
nd 9
6%.
Actu
aria
l gra
ft an
d pa
tient
sur
viva
l rat
es in
SLE
pat
ient
s w
ere
not
sign
ifica
ntly
diff
eren
t fro
m th
ose
of th
e m
atch
ed c
ontro
l gro
up.
Chr
onic
reje
ctio
n w
as th
e m
ajor
risk
fact
or fo
r gra
ft lo
ss. L
upus
ne
phrit
is re
curr
ed in
the
graf
t of o
ne p
atie
nt 3
mon
ths
afte
r tra
nspl
anta
tion,
and
ther
e w
ere
extra
rena
l man
ifest
atio
ns o
f SLE
in
four
oth
ers.
CO
NC
LUSI
ON
S: T
he p
rese
nt s
tudy
con
firm
s th
at
patie
nts
with
SLE
can
rece
ive
trans
plan
ts w
ith e
xcel
lent
gra
ft an
d pa
tient
sur
viva
l rat
es a
nd a
low
rate
of c
linic
al re
curr
ent l
upus
ne
phrit
is.
Aze
vedo
LS
, Rom
ão
JE J
r, M
alhe
iros
D,
Sald
anha
LB,
Ianh
ez
LE, S
abba
ga E
.
Uni
vers
ity o
f São
Pa
ulo
Med
ical
Sc
hool
, SP,
Bra
zil.
N
ephr
ol D
ial
Tran
spla
nt. 1
998
Nov
;13(
11):2
894-
8.
Ren
al
trans
plan
tatio
n in
sy
stem
ic lu
pus
eryt
hem
atos
us. A
ca
se c
ontro
l stu
dy o
f 45
pat
ient
s.
Forty
-five
pat
ient
s w
ith s
yste
mic
lupu
s er
ythe
mat
osus
sub
ject
ed to
48
kidn
ey
trans
plan
ts w
ere
stud
ied.
For
com
para
tive
purp
oses
, a c
ase-
cont
rol p
opul
atio
n w
as
sele
cted
, mat
ched
for g
ende
r, ra
ce, t
ype
of
dono
r, ag
e, a
nd ti
me
of tr
ansp
lant
atio
n.
Patie
nts
with
non
-glo
mer
ulon
ephr
itis
dise
ases
wer
e ex
clud
ed.
RES
ULT
S: N
o di
ffere
nces
in a
cute
epi
sode
s of
reje
ctio
n, c
ause
s of
kid
ney
loss
or p
atie
nt d
eath
wer
e ob
serv
ed. G
ener
al a
s w
ell a
s in
fect
ious
com
plic
atio
ns w
ere
sim
ilar.
Preg
nanc
y ra
tes
and
outc
omes
wer
e si
mila
r with
no
dele
terio
us e
ffect
on
patie
nts
or
graf
ts. A
ctua
rial 1
-and
5-y
ear p
atie
nt s
urvi
vals
(97.
7 an
d 91
.1%
fo
r SLE
and
95.
4 an
d 87
% fo
r con
trols
, res
pect
ivel
y) a
nd g
raft
surv
ival
s (9
3.1
and
80.7
% fo
r SLE
and
88.
8 an
d 70
.2%
for
cont
rols
, res
pect
ivel
y) w
ere
sim
ilar.
Long
-term
rena
l fun
ctio
n ex
pres
sed
by s
erum
cre
atin
ine
was
the
sam
e. N
o di
ffere
nces
in
imm
unos
uppr
essi
vedr
ug (a
zath
iopr
ine,
pre
dnis
one,
and
cy
clos
porin
) req
uire
men
ts w
ere
foun
d. C
linic
al S
LE re
curr
ence
w
as s
uspe
cted
onl
y on
ce (a
pat
ient
with
thro
mbo
cyto
peni
a,
hypo
com
plem
enta
emia
with
low
com
plem
ent l
evel
s an
d po
sitiv
e an
tipla
tele
t ant
ibod
ies)
. Tw
o SL
E pa
tient
s sh
owed
mes
angi
al
prol
ifera
tive
glom
erul
onep
hriti
s co
mpa
tible
with
recu
rren
ce. B
oth
graf
ts w
ere
lost
. Tw
o fu
rther
pat
ient
s sh
owed
mem
bran
ous
glom
erul
onep
hriti
s w
ith a
n im
mun
oflu
ores
cenc
e pa
ttern
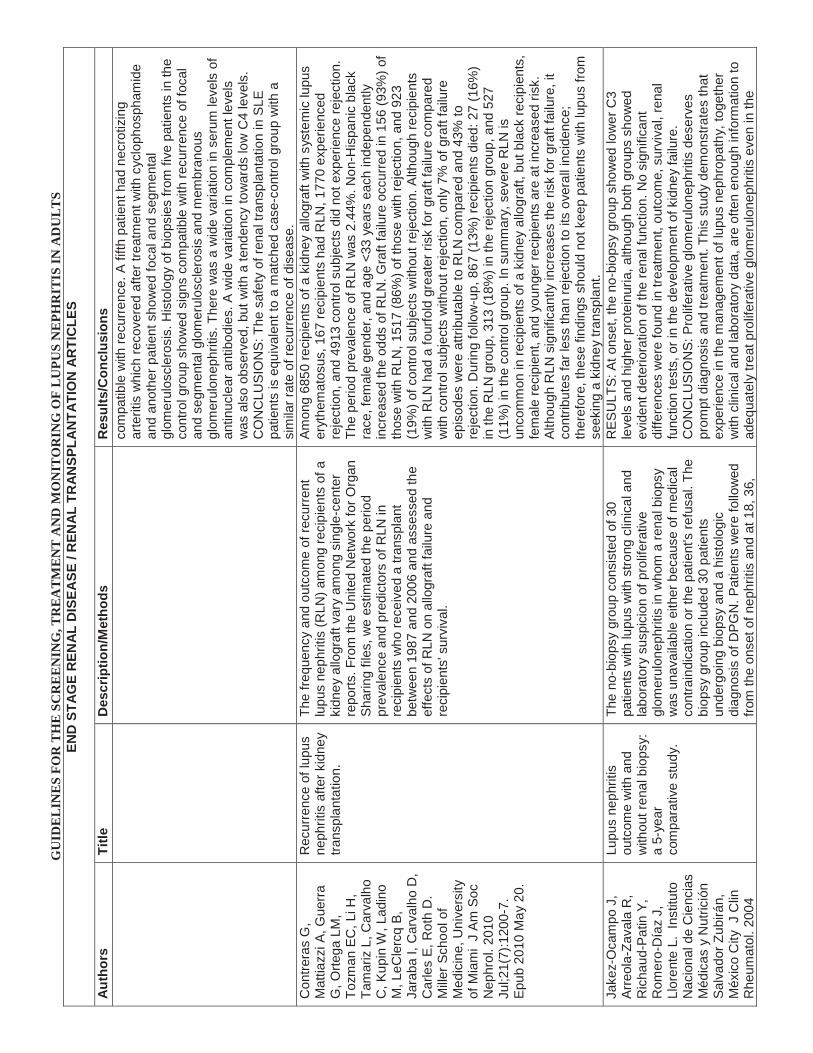
GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
com
patib
le w
ith re
curr
ence
. A fi
fth p
atie
nt h
ad n
ecro
tizin
gar
terit
is w
hich
reco
vere
d af
ter t
reat
men
t with
cyc
loph
osph
amid
e an
d an
othe
r pat
ient
sho
wed
foca
l and
seg
men
tal
glom
erul
oscl
eros
is. H
isto
logy
of b
iops
ies
from
five
pat
ient
s in
the
cont
rol g
roup
sho
wed
sig
ns c
ompa
tible
with
recu
rren
ce o
f foc
al
and
segm
enta
l glo
mer
ulos
cler
osis
and
mem
bran
ous
glom
erul
onep
hriti
s. T
here
was
a w
ide
varia
tion
in s
erum
leve
ls o
f an
tinuc
lear
ant
ibod
ies.
A w
ide
varia
tion
in c
ompl
emen
t lev
els
was
als
o ob
serv
ed, b
ut w
ith a
tend
ency
tow
ards
low
C4
leve
ls.
CO
NC
LUSI
ON
S: T
he s
afet
y of
rena
l tra
nspl
anta
tion
in S
LE
patie
nts
is e
quiv
alen
t to
a m
atch
ed c
ase-
cont
rol g
roup
with
a
sim
ilar r
ate
of re
curr
ence
of d
isea
se.
Con
trera
s G
, M
attia
zzi A
, Gue
rra
G, O
rtega
LM
, To
zman
EC
, Li H
, Ta
mar
iz L
, Car
valh
o C
, Kup
in W
, Lad
ino
M, L
eCle
rcq
B,
Jara
ba I,
Car
valh
o D
, C
arle
s E
, Rot
h D
. M
iller S
choo
l of
Med
icin
e, U
nive
rsity
of
Mia
mi
J Am
Soc
N
ephr
ol. 2
010
Jul;2
1(7)
:120
0-7.
Ep
ub 2
010
May
20.
Rec
urre
nce
of lu
pus
neph
ritis
afte
r kid
ney
trans
plan
tatio
n.
The
frequ
ency
and
out
com
e of
recu
rren
t lu
pus
neph
ritis
(RLN
) am
ong
reci
pien
ts o
f a
kidn
ey a
llogr
aft v
ary
amon
g si
ngle
-cen
ter
repo
rts. F
rom
the
Uni
ted
Net
wor
k fo
r Org
an
Shar
ing
files
, we
estim
ated
the
perio
d pr
eval
ence
and
pre
dict
ors
of R
LN in
re
cipi
ents
who
rece
ived
a tr
ansp
lant
be
twee
n 19
87 a
nd 2
006
and
asse
ssed
the
effe
cts
of R
LN o
n al
logr
aft f
ailu
re a
nd
reci
pien
ts' s
urvi
val.
Amon
g 68
50 re
cipi
ents
of a
kid
ney
allo
graf
t with
sys
tem
ic lu
pus
eryt
hem
atos
us, 1
67 re
cipi
ents
had
RLN
, 177
0 ex
perie
nced
re
ject
ion,
and
491
3 co
ntro
l sub
ject
s di
d no
t exp
erie
nce
reje
ctio
n.
The
perio
d pr
eval
ence
of R
LN w
as 2
.44%
. Non
-His
pani
c bl
ack
race
, fem
ale
gend
er, a
nd a
ge <
33 y
ears
eac
h in
depe
nden
tly
incr
ease
d th
e od
ds o
f RLN
. Gra
ft fa
ilure
occ
urre
d in
156
(93%
) of
thos
e w
ith R
LN, 1
517
(86%
) of t
hose
with
reje
ctio
n, a
nd 9
23
(19%
) of c
ontro
l sub
ject
s w
ithou
t rej
ectio
n. A
lthou
gh re
cipi
ents
w
ith R
LN h
ad a
four
fold
gre
ater
risk
for g
raft
failu
re c
ompa
red
with
con
trol s
ubje
cts
with
out r
ejec
tion,
onl
y 7%
of g
raft
failu
re
epis
odes
wer
e at
tribu
tabl
e to
RLN
com
pare
d an
d 43
% to
re
ject
ion.
Dur
ing
follo
w-u
p, 8
67 (1
3%) r
ecip
ient
s di
ed: 2
7 (1
6%)
in th
e R
LN g
roup
, 313
(18%
) in
the
reje
ctio
n gr
oup,
and
527
(1
1%) i
n th
e co
ntro
l gro
up. I
n su
mm
ary,
sev
ere
RLN
is
unco
mm
on in
reci
pien
ts o
f a k
idne
y al
logr
aft,
but b
lack
reci
pien
ts,
fem
ale
reci
pien
t, an
d yo
unge
r rec
ipie
nts
are
at in
crea
sed
risk.
Al
thou
gh R
LN s
igni
fican
tly in
crea
ses
the
risk
for g
raft
failu
re, i
t co
ntrib
utes
far l
ess
than
reje
ctio
n to
its
over
all i
ncid
ence
; th
eref
ore,
thes
e fin
ding
s sh
ould
not
kee
p pa
tient
s w
ith lu
pus
from
se
ekin
g a
kidn
ey tr
ansp
lant
.Ja
kez-
Oca
mpo
J,
Arre
ola-
Zava
la R
, R
icha
ud-P
atin
Y,
Rom
ero-
Día
z J,
Ll
oren
te L
. In
stitu
to
Nac
iona
l de
Cie
ncia
s M
édic
as y
Nut
rició
n Sa
lvad
or Z
ubirá
n,
Méx
ico
City
J C
lin
Rhe
umat
ol. 2
004
Lupu
s ne
phrit
is
outc
ome
with
and
w
ithou
t ren
al b
iops
y:
a 5-
year
co
mpa
rativ
e st
udy.
The
no-b
iops
y gr
oup
cons
iste
d of
30
patie
nts
with
lupu
s w
ith s
trong
clin
ical
and
la
bora
tory
sus
pici
on o
f pro
lifer
ativ
e gl
omer
ulon
ephr
itis
in w
hom
a re
nal b
iops
y w
as u
nava
ilabl
e ei
ther
bec
ause
of m
edic
al
cont
rain
dica
tion
or th
e pa
tient
's re
fusa
l. Th
e bi
opsy
gro
up in
clud
ed 3
0 pa
tient
s un
derg
oing
bio
psy
and
a hi
stol
ogic
di
agno
sis
of D
PGN
. Pat
ient
s w
ere
follo
wed
fro
m th
e on
set o
f nep
hriti
s an
d at
18,
36,
RES
ULT
S: A
t ons
et, t
he n
o-bi
opsy
gro
up s
how
ed lo
wer
C3
leve
ls a
nd h
ighe
r pro
tein
uria
, alth
ough
bot
h gr
oups
sho
wed
ev
iden
t det
erio
ratio
n of
the
rena
l fun
ctio
n. N
o si
gnifi
cant
di
ffere
nces
wer
e fo
und
in tr
eatm
ent,
outc
ome,
sur
viva
l, re
nal
func
tion
test
s, o
r in
the
deve
lopm
ent o
f kid
ney
failu
re.
CO
NC
LUSI
ON
S: P
rolif
erat
ive
glom
erul
onep
hriti
s de
serv
es
prom
pt d
iagn
osis
and
trea
tmen
t. Th
is s
tudy
dem
onst
rate
s th
at
expe
rienc
e in
the
man
agem
ent o
f lup
us n
ephr
opat
hy, t
oget
her
with
clin
ical
and
labo
rato
ry d
ata,
are
ofte
n en
ough
info
rmat
ion
to
adeq
uate
ly tr
eat p
rolif
erat
ive
glom
erul
onep
hriti
s ev
en in
the

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
Dec
;10(
6):2
89-9
4.an
d 60
mon
ths.
abse
nce
of a
rena
l bio
psy.
Nyb
erg
G, K
arlb
erg
I, Sv
alan
der C
, H
edm
an L
, Blo
hmé
I. Sa
hlgr
ensk
a H
ospi
tal,
Göt
ebor
g,
Sw
eden
. Sc
and
J U
rol N
ephr
ol.
1990
;24(
4):3
07-1
3.
Ren
al
trans
plan
tatio
n in
pa
tient
s w
ith
syst
emic
lupu
s er
ythe
mat
osus
: in
crea
sed
risk
of
early
gra
ft lo
ss.
The
outc
ome
of p
rimar
y re
nal
trans
plan
tatio
n in
31
SLE
pat
ient
s w
as
eval
uate
d in
rela
tion
to tw
o co
ntem
pora
ry
cont
rols
per
pat
ient
, mat
ched
for a
ge, s
ex
and
imm
unos
uppr
essi
ve th
erap
y. T
he
prop
ortio
n of
livi
ng d
onor
s w
as o
ne th
ird in
bo
th g
roup
s.
Patie
nt s
urvi
val d
id n
ot d
iffer
, but
gra
ft su
rviv
al a
t 6 a
nd 1
2 m
onth
s po
st tr
ansp
lant
atio
n w
as s
igni
fican
tly re
duce
d in
SLE
pa
tient
s (p
less
than
0.0
01).
Whe
n di
vide
d in
to g
roup
s us
ing
eith
er a
zath
iopr
ine
and
ster
oids
or c
ombi
natio
ns in
clud
ing
cycl
ospo
rin A
(14
and
17 S
LE p
atie
nts
in e
ach
grou
p), g
raft
surv
ival
was
sig
nific
antly
redu
ced
for t
he a
zath
iopr
ine-
treat
ed
SLE
patie
nts,
36%
vs.
82%
for t
heir
cont
rols
at o
ne y
ear.
For
cycl
ospo
rin-tr
eate
d SL
E pa
tient
s, o
ne-y
ear g
raft
surv
ival
was
59
% v
s. 8
5% fo
r the
ir co
ntro
ls, a
nd 6
out
of 1
7 gr
afts
in th
e cy
clos
porin
-trea
ted
grou
p w
ere
lost
with
in th
e fir
st m
onth
vs.
onl
y 4
out o
f 34
cont
rols
. The
se d
iffer
ence
s w
ere,
how
ever
, not
st
atis
tical
ly d
iffer
ent.
Mos
t fai
led
graf
ts w
ere
lost
from
reje
ctio
n,
with
a h
igh
prop
ortio
n of
acu
te v
ascu
lar r
ejec
tion,
isol
ated
or i
n co
mbi
natio
n w
ith c
ellu
lar r
ejec
tion.
The
re w
as n
o ap
pare
nt
asso
ciat
ion
betw
een
reje
ctio
n an
d H
LA-m
atch
ed o
r pre
senc
e of
H
LA a
ntib
odie
s. R
etra
nspl
anta
tion
was
suc
cess
ful i
n6
out o
f 7
case
s. W
e co
nclu
de th
at S
LE p
atie
nts
have
an
incr
ease
d ris
k of
ea
rly g
raft
reje
ctio
n, b
ut th
at th
is m
ay b
e ov
erco
me
by m
ore
pow
erfu
l im
mun
osup
pres
sive
ther
apy.
el-S
haha
wy
MA,
As
wad
S, M
ende
z R
G, B
angs
il R
, M
ende
z R
, Mas
sry
SG. U
nive
rsity
of
Sout
hern
Cal
iforn
ia
Scho
ol o
f M
edic
ineA
m J
N
ephr
ol.
1995
;15(
2):1
23-8
.
Ren
al
trans
plan
tatio
n in
sy
stem
ic lu
pus
eryt
hem
atos
us: a
si
ngle
-cen
ter
expe
rienc
e w
ith
sixt
y-fo
ur c
ases
.
The
outc
ome
of re
nal t
rans
plan
tatio
n in
64
patie
nts
with
end
-sta
ge re
nal d
isea
se(E
SRD
) sec
onda
ry to
lupu
s ne
phrit
is is
the
subj
ect o
f thi
s re
port.
The
pat
ient
s w
ere
trans
plan
ted
over
a 1
50-m
onth
(12.
5-ye
ar)
perio
d (b
etw
een
July
5, 1
979,
and
Jan
uary
30
, 199
2). T
he s
tudy
pop
ulat
ion
is
pred
omin
antly
mad
e up
of y
oung
fem
ales
(m
ean
age,
34.
7 +/
-9 y
ears
, n =
54,
81.
3%).
Fifty
-one
tran
spla
nts
(79.
7%) a
re c
adav
eric
, an
d 13
(20.
3%) a
re fr
om li
ving
-rel
ated
do
nors
. Fift
y-ei
ght p
atie
nts
(90.
6%) h
ad
prim
ary
(firs
t) al
logr
afts
, and
6 (9
.4%
) re
ceiv
ed a
sec
ond
allo
graf
t.
For a
ll 64
pat
ient
s co
mbi
ned,
the
1-ye
ar g
raft
and
patie
nt s
urvi
val
rate
s ar
e 68
.8 a
nd 8
6.5%
, res
pect
ivel
y, w
here
as 5
-yea
r gra
ft an
d pa
tient
sur
viva
l rat
es a
re 6
0.9
and
85.9
%, r
espe
ctiv
ely.
Pat
ient
s w
hose
imm
unos
uppr
essi
ve re
gim
en w
as C
sA-b
ased
had
a 1
-ye
ar g
raft
surv
ival
of 7
1.5
vers
us 6
3.6%
in th
e AZ
A gr
oup.
H
owev
er, t
his
7.9%
diff
eren
ce d
id n
ot re
ach
stat
istic
al
sign
ifica
nce
(p =
0.9
5). T
he 5
-yea
r gra
ft su
rviv
al o
f the
CsA
-ba
sed
grou
p w
as 6
9.1
vers
us 4
5.5%
for t
he A
ZA g
roup
, p <
0.0
5.
One
-yea
r pat
ient
sur
viva
l was
77.
3% fo
r the
AZA
gro
up a
nd
92.9
% fo
r the
CsA
gro
up, p
< 0
.05)
. The
dat
a sh
ow th
at p
atie
nts
with
ESR
D s
econ
dary
to lu
pus
neph
ritis
can
und
ergo
rena
l tra
nspl
anta
tion
with
sat
isfa
ctor
y ou
tcom
e. Im
mun
osup
pres
sion
ba
sed
upon
CsA
impr
oves
firs
t-yea
r pat
ient
and
allo
graf
t sur
viva
l by
15.
6 an
d 7.
9%. r
espe
ctiv
ely.

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, T
RE
AT
ME
NT
AN
D M
ON
ITO
RIN
G O
F L
UPU
S N
EPH
RIT
IS IN
AD
UL
TS
END
STA
GE
REN
AL
DIS
EASE
/ R
ENA
L TR
AN
SPLA
NTA
TIO
N A
RTI
CLE
S
Aut
hors
Title
Des
crip
tion/
Met
hods
Res
ults
/Con
clus
ions
Post
trans
plan
tatio
n im
mun
osup
pres
sion
co
nsis
ted
of a
zath
iopr
ine
and
pred
niso
ne
(AZA
gro
up, n
= 2
2, 3
4.3%
) or A
ZA,
pred
niso
ne a
nd c
yclo
spor
ine
(CsA
gro
up, n
=
42, 6
5.6%
).

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, D
IAG
NO
SIS,
TR
EA
TM
EN
T A
ND
MO
NIT
OR
ING
OF
LU
PUS
NE
PHR
ITIS
IN A
DU
LT
S
Tabl
e 8.
Sum
mar
y of
Com
mon
ly U
sed
Med
icat
ions
’Ter
atog
enic
Effe
cts
PREG
NA
NC
Y A
ND
LU
PUS
NEP
HR
ITIS
Trea
tmen
tPr
egna
ncy
C
ateg
ory
Cro
sses
Pl
acen
ta?
Anim
al
Stud
ies
Hum
an S
tudi
es
Cyc
loph
osph
ami
deD
yes
Tera
toge
nic
Tera
toge
nic
effe
cts
have
bee
n re
porte
d in
ass
ocia
tion
with
the
use
of
cycl
opho
spha
mid
e. In
gen
eral
, alk
ylat
ing
agen
ts w
hen
give
n du
ring
the
first
tri
mes
ter a
re b
elie
ved
to c
ause
slig
ht in
crea
ses
in th
e ris
k of
con
geni
tal
mal
form
atio
ns, b
ut w
hen
give
n du
ring
the
seco
nd o
r thi
rd tr
imes
ters
are
bel
ieve
d to
onl
y in
crea
se th
e ris
k of
gro
wth
retri
ctio
n (G
lant
z, 1
994)
. In
one
cas
e se
ries
of
4 pa
tient
s tre
ated
with
cyc
loph
osph
amid
e fo
r lup
us d
urin
g pr
egna
ncy
(2 d
urin
g fir
st tr
imes
ter,
2 du
ring
2ndtri
mes
ter),
all
4 re
sulte
d in
pre
gnan
cy lo
ss (C
low
se
Lupu
s 20
05)
Azat
hiop
rine
D
Yes
(but
feta
l liv
er la
cks
enzy
me
whi
ch
conv
erts
dr
ug to
ac
tive
met
abol
ites)
Tera
toge
nic
Azat
hiop
rine
has
been
use
d du
ring
preg
nanc
y in
org
an tr
ansp
lant
reci
pien
ts.
Dur
ing
over
40
year
s of
exp
erie
nce
with
aza
thio
prin
e as
an
imm
unos
uppr
essa
nt
in o
rgan
tran
spla
nt p
atie
nts,
no
pred
omin
ant o
r spe
cific
mal
form
atio
n pa
ttern
has
be
en id
entif
ied
whi
ch is
attr
ibut
able
to th
is d
rug.
Ret
rosp
ectiv
e re
view
of
preg
nanc
y ou
tcom
es re
veal
ed th
at in
fant
s ex
pose
d to
aza
thio
prin
e m
ay d
evel
op
the
follo
win
g ad
vers
e ef
fect
s: th
ymic
atro
phy,
leuk
open
ia, a
nem
ia,
thro
mbo
cyto
peni
a, c
hrom
osom
e ab
erra
tions
, red
uced
imm
unog
lobu
lin le
vels
, an
d in
fect
ions
. Adj
ustm
ent o
f aza
thio
prin
e do
sage
to m
aint
ain
norm
al m
ater
nal
leuk
ocyt
e co
unts
may
dec
reas
e or
pre
vent
neo
nata
l leu
kope
nia
and
thro
mbo
cyto
peni
a (A
rmen
ti et
al,
1998
). C
urre
nt g
uide
lines
rega
rdin
g pr
egna
nt
rena
l tra
nspl
ant p
atie
nts
stat
e th
at im
mun
osup
pres
sive
ther
apy
with
or w
ithou
t st
eroi
ds a
nd a
zath
iopr
ine
may
be
cont
inue
d du
ring
preg
nanc
y (E
BPG
Exp
ert
Gro
up o
n R
enal
Tra
nspl
anta
tion,
200
2).
MM
FD
Unk
now
nTe
rato
geni
c
The
Nat
iona
l Tra
nspl
anta
tion
Preg
nanc
y R
egis
try (N
TPR
) rep
orts
24
fem
ale
kidn
ey re
cipi
ents
with
33
preg
nanc
ies
expo
sed
to m
ycop
heno
late
mof
etil.
The
re
wer
e 15
spo
ntan
eous
abo
rtion
s (4
5%) a
nd 1
8 liv
e bi
rths,
with
stru
ctur
al
abno
rmal
ities
wer
e pr
esen
t in
4 of
thes
e 18
infa
nts
(22%
). Ba
sed
on
post
mar
ketin
g da
ta c
olle
cted
by
the
NTP
R fr
om 1
995
to 2
007
amon
g w
omen
(n
=77)
with
sys
tem
ic e
xpos
ure
to m
ycop
heno
late
mof
etil
durin
g pr
egna
ncy,
sp
onta
neou
s ab
ortio
ns o
ccur
red
in 2
5 w
omen
and
feta
l/inf
ant m
alfo
rmat
ions
oc
curr
ed in
14
offs
prin
g. E
ar a
bnor
mal
ities
wer
e pr
esen
t in
6 of
the
14
mal
form
ed in
fant
s. W
ith d
oses
bel
ow e
quiv
alen
t hum
an c
linic
al d
oses
, fet
al
reso
rptio
ns a
nd/o
r mal
form
atio
ns in
the
abse
nce
of m
ater
nal t
oxic
ity h
ave
occu
rred
in ra
ts a
nd ra
bbits
(Pro
d In
fo C
ellC
ept(R
) ora
l cap
sule
s, ta
blet
s,

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, D
IAG
NO
SIS,
TR
EA
TM
EN
T A
ND
MO
NIT
OR
ING
OF
LU
PUS
NE
PHR
ITIS
IN A
DU
LT
SPR
EGN
AN
CY
AN
D L
UPU
S N
EPH
RIT
IS
Trea
tmen
tPr
egna
ncy
C
ateg
ory
Cro
sses
Pl
acen
ta?
Anim
al
Stud
ies
Hum
an S
tudi
es
susp
ensi
on, I
V in
ject
ion,
200
9).
Not
e th
at in
200
7, th
e pr
egna
ncy
cate
gory
was
ch
ange
d fro
m C
to D
bec
ause
of t
he n
oted
pat
tern
of a
bnor
mal
ities
Leflu
nom
ide
XU
nkno
wn
Tera
toge
nic
Leflu
nom
ide
use
is c
ontra
indi
cate
d in
wom
en w
ho a
re o
r may
bec
ome
preg
nant
. Ba
sed
on a
nim
al d
ata,
leflu
nom
ide
may
incr
ease
the
risk
of fe
tal d
eath
or
tera
toge
nic
effe
cts
in p
regn
ant w
omen
. Prio
r to
initi
atio
n of
leflu
nom
ide,
pr
egna
ncy
mus
t be
excl
uded
and
the
use
of re
liabl
e co
ntra
cept
ion
mus
t be
conf
irmed
. P O
f 168
pre
gnan
t wom
en e
valu
ated
as
of J
anua
ry 2
004
in a
co
ntro
lled,
coh
ort s
tudy
(OTI
S R
heum
atoi
d Ar
thrit
is in
Pre
gnan
cy),
wom
en w
ith
rheu
mat
oid
arth
ritis
(RA)
exp
osed
to le
fluno
mid
e ea
rly in
pre
gnan
cy (n
=43)
and
th
ose
with
RA
not e
xpos
ed to
leflu
nom
ide
durin
g pr
egna
ncy
(n=7
8) w
ere
a si
gnifi
cant
12
times
(95%
con
fiden
ce in
terv
al (C
I) 2.
5, 5
9.2)
and
a s
igni
fican
t 10
.1 ti
mes
(95%
CI 2
.2, 4
7.3)
, res
pect
ivel
y, m
ore
likel
y to
del
iver
pre
term
infa
nts
com
pare
d w
ith th
ose
in th
e no
n-di
seas
ed c
ontro
l gro
up (n
=47)
. The
adj
uste
d m
ean
birth
wei
ght o
f ful
l ter
m in
fant
s w
as a
lso
sign
ifica
ntly
low
er in
the
RA
leflu
nom
ide
grou
p (3
158
g, 9
5% C
I 297
9, 3
336)
and
the
RA
cont
rol g
roup
(325
0 g,
95%
CI 3
124,
337
5) c
ompa
red
with
the
non-
dise
ased
con
trol g
roup
(361
8 g,
95
% C
I 348
7, 3
748;
p le
ss th
an 0
.001
). O
vera
ll, a
ll gr
oups
had
the
sam
e pr
opor
tion
of in
fant
s bo
rn w
ith m
ajor
and
/or m
inor
mal
form
atio
ns (C
ham
bers
et
al, 2
004)
. H
owev
er, i
n a
follo
w-u
p st
udy
publ
ishe
d in
201
0, a
mon
g 64
wom
en
who
wer
e ex
pose
dto
leflu
nom
ide
early
in p
regn
ancy
, but
sto
pped
the
drug
and
w
ere
treat
ed w
ith c
hole
styr
amin
e, th
ere
was
no
subs
tant
ial i
ncre
ase
in a
dver
se
preg
nanc
y ou
tcom
es (C
ham
bers
Arth
ritis
Rhe
um 2
010)
.
Chl
oram
buci
lD
Yes
Tera
toge
nic
Tera
toge
nic
effe
cts
have
bee
n re
porte
d in
ass
ocia
tion
with
the
use
of
chlo
ram
buci
l. Th
e te
rato
geni
c ef
fect
s of
chl
oram
buci
l may
be
pote
ntia
ted
by
caffe
ine
(Ber
mas
& H
ill, 1
995)
. In
gene
ral,
alky
latin
g ag
ents
, whe
n gi
ven
durin
g th
e fir
st tr
imes
ter,
are
belie
ved
to c
ause
slig
ht in
crea
ses
in th
e ris
k of
con
geni
tal
mal
form
atio
ns, b
ut w
hen
give
n du
ring
the
seco
nd o
r thi
rd tr
imes
ters
are
bel
ieve
d to
onl
y in
crea
se th
e ris
k of
gro
wth
rest
rictio
n (G
lant
z, 1
994a
)..
Tacr
olim
usC
Yes
Ret
rosp
ectiv
e ca
se a
naly
sis:
100
pre
gnan
cies
(84
wom
en) 7
1 pr
egna
ncie
s pr
ogre
ssed
to d
eliv
ery,
resu
lting
in 6
8 liv
e bi
rths
and
24 p
regn
anci
es th
at w
ere
spon
tane
ousl
y or
ele
ctiv
ely
abor
ted.
Fou
r of t
he 6
8 su
rviv
ing
neon
ates
had
co
ngen
ital m
alfo
rmat
ions
, whe
reas
non
e of
the
24 a
borte
d fe
tuse
s ex
hibi
ted
dete
ctab
le m
alfo
rmat
ions
. Pre
mat
urity
rate
of 5
9% ;o
nly
10%
of t
he in
fant
s w
ere
outs
ide
of th
e 10
th to
90t
h pe
rcen
tile
rang
e fo
r birt
h w
eigh
t whe
n co
nsid
erin
g th
e ge
stat
iona
l age
of t
he n
eona
te (K
ainz
et a
l, 20
00).

GU
IDE
LIN
ES
FOR
TH
E S
CR
EE
NIN
G, D
IAG
NO
SIS,
TR
EA
TM
EN
T A
ND
MO
NIT
OR
ING
OF
LU
PUS
NE
PHR
ITIS
IN A
DU
LT
SPR
EGN
AN
CY
AN
D L
UPU
S N
EPH
RIT
IS
Trea
tmen
tPr
egna
ncy
C
ateg
ory
Cro
sses
Pl
acen
ta?
Anim
al
Stud
ies
Hum
an S
tudi
es
Cyc
losp
orin
eC
Yes
No
In a
stu
dy o
f 48
preg
nant
wom
en b
eing
trea
ted
with
ther
apeu
tic d
oses
of
cycl
ospo
rine,
no
evid
ence
of d
irect
haz
ard
to th
e fe
tus
was
dem
onst
rate
d.
(Coc
kbur
n et
al,
1989
). N
o sp
ecifi
c bi
rth d
efec
t has
bee
n as
soci
ated
with
CSA
, al
thou
gh m
any
spor
adic
con
geni
tal a
nom
alie
s ha
ve b
een
repo
rted
(Pet
ri Au
toim
mun
ity 2
003)
. In
pos
t-mar
ketin
g su
rvei
llanc
e of
166
pre
gnan
cies
, 45%
w
ere
pre-
term
, and
the
med
ian
birth
wei
ght w
as 2
300
g (A
rella
no M
ed C
lin 1
991)
.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
Miniter, et al. (209) RIA 0.68 0.82 3.76 0.39
Ballou,et al. (210) Crithidia 0.53 0.64 1.46 0.73
Isenberg, et al.
(211)
ELISA 0.76 0.54 1.65 0.44
Abrass, et al. (102) RIA 0.33 0.68 1.03 0.97 0.44 0.57 1.02 0.98
Davis, et al. (212) RIA 0.93 0.78 3.48 0.1
Feldman, et al.
(213)
Farr 0.2 0.88 1.6 0.9 0.25 0.93 3.6 0.8 NA NA NA NA
Weighted means 0.66 0.66 4.14 0.51 0.65 0.41 1.7 0.76 0.86 0.45 1.7 0.3
Table 9 . Use of anti-DNA antibodies for prognosis among SLE patients.
Reference Technique
Overall SLE active vs. inactive
Renal involvement present vs. absent
Renal disease active vs. inactive
Sen Spec +LR -LR Sen Spec +LR -LR Sen Spec +LR -LR
Froelich, et al. (199). ELISA 0.75 0.75 3.0 0.33
Emlen, et al.(200) ELISA 0.69 0.77 3.05 0.4
Farr 0.98 0.97 25.2 0.02
Crithidia 0.56 0.97 24.1 0.45
Isenberg, et al.(201) Crithidia 0.62 0.75 1.8 0.5 0.92 0.55 2.1 0.14
Ter Borg, et al. (90) ELISA 0.32 0.64 0.88 1.06
Crithidia 0.14 0.91 1.55 0.94
Farr 0.41 0.73 1.5 0.81
Chubick et al. (202) ELISA 0.92 0.44 1.6 0.18 0.97 0.44 1.7 0.07
Farr 0.73 0.72 2.6 0.38 0.76 0.72 2.7 0.33
Kalmin, et al. (203) ELISA 0.71 0.33 1.05 0.88 0.91 0.08 0.99 1.12
Crithidia 0.43 0.6 1.07 0.95 0.46 0.6 1.15 0.9
Cameron, et al. (103) Farr 0.89 0.25 1.2 0.44
Bootsma, et al. (204) Crithidia 1.00 0.13 1.15 0.38
Farr 0.89 0.4 1.48 0.28
Pincus, et al. (205) Farr 0.82 0.18 1.0 0.97 0.91 0.33 1.4 0.26
Ballou, et al. (206) Crithidia 0.74 0.95 14.8 0.27 0.88 0.41 1.5 0.29
Garcia, et al. (207) Crithidia 0.85 0.33 2.6 0.45
Weitzman, et al.
(208)
Farr 0.76 0.66 2.28 0.36 0.82 0.32 1.2 0.56

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
REFERENCES
1. Guidelines for referral and management of systemic lupus erythematosus in adults. American College of Rheumatology Ad Hoc Committee on Systemic Lupus Erythematosus Guidelines. Arthritis Rheum. 1999;42(9):1785-96.
2. Markowitz GS, D'Agati VD. The ISN/RPS 2003 classification of lupus nephritis: an assessment at 3 years. Kidney Int. 2007;71(6):491-5.
3. Bomback AS, Appel GB. Updates on the treatment of lupus nephritis. J Am Soc Nephrol. 2010;21(12):2028-35.
4. Griffiths B, Mosca M, Gordon C. Assessment of patients with systemic lupus erythematosus and the use of lupus disease activity indices. Best Pract Res Clin Rheumatol. 2005;19(5):685-708.
5. Gordon C, Sutcliffe N, Skan J, Stoll T, Isenberg DA. Definition and treatment of lupus flares measured by the BILAG index. Rheumatology (Oxford). 2003;42(11):1372-9.
6. Isenberg DA, Gordon C. From BILAG to BLIPS--disease activity assessment in lupus past, present and future. Lupus. 2000;9(9):651-4.
7. Gladman DD, Goldsmith CH, Urowitz MB, Bacon P, Fortin P, Ginzler E, et al. The Systemic Lupus International Collaborating Clinics/American College of Rheumatology (SLICC/ACR) Damage Index for Systemic Lupus Erythematosus International Comparison. J Rheumatol. 2000;27(2):373-6.
8. Gladman DD, Ibanez D, Urowitz MB. Systemic lupus erythematosus disease activity index 2000. J Rheumatol. 2002;29(2):288-91.
9. Isenberg DA, Rahman A, Allen E, Farewell V, Akil M, Bruce IN, et al. BILAG 2004. Development and initial validation of an updated version of the British Isles Lupus Assessment Group's disease activity index for patients with systemic lupus erythematosus. Rheumatology (Oxford). 2005;44(7):902-6.
10. Furie R, Petri M, Zamani O, Cervera R, Wallace DJ, Tegzova D, et al. A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. 2011;63(12):3918-30.
11. Dooley MA, Jayne D, Ginzler EM, Isenberg D, Olsen NJ, Wofsy D, et al. Mycophenolate versus azathioprine as maintenance therapy for lupus nephritis. N Engl J Med. 2011;365(20):1886-95.
12. Saag KG, Teng GG, Patkar NM, Anuntiyo J, Finney C, Curtis JR, et al. American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease-modifying antirheumatic drugs in rheumatoid arthritis. Arthritis Rheum. 2008;59(6):762-84.
13. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17(1):1-12.
14. Wells G, Shea B, O'Connnell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. 2010 [cited; Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
15. Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, et al. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. Circulation. 2005;112(12):e154-235.
16. Shekelle PG, Woolf SH, Eccles M, Grimshaw J. Clinical guidelines: developing guidelines. BMJ. 1999;318(7183):593-6.
17. Zhang W, Doherty M, Arden N, Bannwarth B, Bijlsma J, Gunther KP, et al. EULAR evidence based recommendations for the management of hip osteoarthritis: report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis. 2005;64(5):669-81.
18. Gordon T. The Delphi Project; 1994.
19. Fitch K, Bernstein S, Aguilar M, Burnand B, Lacalle JR, Lozaro P, et al. The RAND/UCLA Appropriateness Method User's Manual. Santa Monica: RAND Corporation; 2001.
20. Shekelle PG, Chassin MR, Park RE. Assessing the predictive validity of the RAND/UCLA appropriateness method criteria for performing carotid endarterectomy. Int J Technol Assess Health Care. 1998;14(4):707-27.
21. Weening JJ, D'Agati VD, Schwartz MM, Seshan SV, Alpers CE, Appel GB, et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int. 2004;65(2):521-30.
22. Furness PN, Taub N. Interobserver reproducibility and application of the ISN/RPS classification of lupus nephritis-a UK-wide study. Am J Surg Pathol. 2006;30(8):1030-5.
23. Yokoyama H, Wada T, Hara A, Yamahana J, Nakaya I, Kobayashi M, et al. The outcome and a new ISN/RPS 2003 classification of lupus nephritis in Japanese. Kidney Int. 2004;66(6):2382-8.
24. Austin HA, 3rd, Muenz LR, Joyce KM, Antonovych TA, Kullick ME, Klippel JH, et al. Prognostic factors in lupus nephritis. Contribution of renal histologic data. Am J Med. 1983;75(3):382-91.
25. Wernick RM, Smith DL, Houghton DC, Phillips DS, Booth JL, Runckel DN, et al. Reliability of histologic scoring for lupus nephritis: a community-based evaluation. Ann Intern Med. 1993;119(8):805-11.
26. Mosca M, Pasquariello A, Tavoni A, Moriconi L, Moneta I, Innocenti M, et al. Predictors of renal outcome in diffuse proliferative glomerulonephritis in systemic lupus erythematosus. Lupus. 1997;6(4):371-8.
27. Stamenkovic I, Favre H, Donath A, Assimacopoulos A, Chatelanat F. Renal biopsy in SLE irrespective of clinical findings: long-term follow-up. Clin Nephrol. 1986;26(3):109-15.
28. Ayodele OE, Okpechi IG, Swanepoel CR. Predictors of poor renal outcome in patients with biopsy-proven lupus nephritis. Nephrology (Carlton). 2010;15(4):482-90.
29. Whiting-O'Keefe Q, Henke JE, Shearn MA, Hopper J, Jr., Biava CG, Epstein WV. The information content from renal biopsy in systemic lupus erythematosus. Ann Intern Med. 1982;96(6 Pt 1):718-23.
30. Makino H, Hayashi Y, Yamasaki Y, Shikata K, Kashihara N, Kira S, et al. Clinical significance of necrosis in lupus nephritis. Intern Med. 1994;33(8):461-5.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
31. Miranda JM, Garcia-Torres R, Jara LJ, Medina F, Cervera H, Fraga A. Renal biopsy in systemic lupus erythematosus: significance of glomerular thrombosis. Analysis of 108 cases. Lupus. 1994;3(1):25-9.
32. Esdaile JM, Joseph L, MacKenzie T, Kashgarian M, Hayslett JP. The pathogenesis and prognosis of lupus nephritis: information from repeat renal biopsy. Semin Arthritis Rheum. 1993;23(2):135-48.
33. Esdaile JM, Federgreen W, Quintal H, Suissa S, Hayslett JP, Kashgarian M. Predictors of one year outcome in lupus nephritis: the importance of renal biopsy. Q J Med. 1991;81(295):907-18.
34. Tang Z, Wang Z, Zhang HT, Hu WX, Zeng CH, Chen HP, et al. Clinical features and renal outcome in lupus patients with diffuse crescentic glomerulonephritis. Rheumatol Int. 2009;30(1):45-9.
35. Faurschou M, Dreyer L, Kamper AL, Starklint H, Jacobsen S. Long-term mortality and renal outcome in a cohort of 100 patients with lupus nephritis. Arthritis Care Res (Hoboken). 2010;62(6):873-80.
36. Austin HA, 3rd, Muenz LR, Joyce KM, Antonovych TT, Balow JE. Diffuse proliferative lupus nephritis: identification of specific pathologic features affecting renal outcome. Kidney Int. 1984;25(4):689-95.
37. Parichatikanond P, Francis ND, Malasit P, Laohapand T, Nimmannit S, Singchoovong L, et al. Lupus nephritis: clinicopathological study of 162 cases in Thailand. J Clin Pathol. 1986;39(2):160-6.
38. Nossent HC, Henzen-Logmans SC, Vroom TM, Berden JH, Swaak TJ. Contribution of renal biopsy data in predicting outcome in lupus nephritis. Analysis of 116 patients. Arthritis Rheum. 1990;33(7):970-7.
39. Kojo S, Sada KE, Kobayashi M, Maruyama M, Maeshima Y, Sugiyama H, et al. Clinical usefulness of a prognostic score in histological analysis of renal biopsy in patients with lupus nephritis. J Rheumatol. 2009;36(10):2218-23.
40. Yu F, Wu LH, Tan Y, Li LH, Wang CL, Wang WK, et al. Tubulointerstitial lesions of patients with lupus nephritis classified by the 2003 International Society of Nephrology and Renal Pathology Society system. Kidney Int. 2010;77(9):820-9.
41. McLaughlin JR, Bombardier C, Farewell VT, Gladman DD, Urowitz MB. Kidney biopsy in systemic lupus erythematosus. III. Survival analysis controlling for clinical and laboratory variables. Arthritis Rheum. 1994;37(4):559-67.
42. Gladman DD, Urowitz MB, Cole E, Ritchie S, Chang CH, Churg J. Kidney biopsy in SLE. I. A clinical-morphologic evaluation. Q J Med. 1989;73(272):1125-33.
43. Radhakrishnan J, Moutzouris DA, Ginzler EM, Solomons N, Siempos, II, Appel GB. Mycophenolate mofetil and intravenous cyclophosphamide are similar as induction therapy for class V lupus nephritis. Kidney Int. 2010;77(2):152-60.
44. Austin HA, 3rd, Illei GG, Braun MJ, Balow JE. Randomized, controlled trial of prednisone, cyclophosphamide, and cyclosporine in lupus membranous nephropathy. J Am Soc Nephrol. 2009;20(4):901-11.
45. Dujovne I, Pollak VE, Pirani CL, Dillard MG. The distribution and character of glomerular deposits in systemic lupus erythematosus. Kidney Int. 1972;2(1):33-50.
GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
46. Najafi CC, Korbet SM, Lewis EJ, Schwartz MM, Reichlin M, Evans J. Significance of histologic patterns of glomerular injury upon long-term prognosis in severe lupus glomerulonephritis. Kidney Int. 2001;59(6):2156-63.
47. Ferluga D, Jerse M, Vizjak A, Hvala A, Rozman B, Kos-Golja M, et al. Correlation among WHO classes, histomorphologic patterns of glomerulonephritis and glomerular immune deposits in SLE. Wien Klin Wochenschr. 2000;112(15-16):692-701.
48. Blanco FJ, De la Mata J, Lopez-Fernandez JI, Gomez-Reino JJ. Light, immunofluorescence and electron microscopy renal biopsy findings as predictors of mortality in eighty-five Spanish patients with systemic lupus erythematosus. Br J Rheumatol. 1994;33(3):260-6.
49. Yu F, Tan Y, Liu G, Wang SX, Zou WZ, Zhao MH. Clinicopathological characteristics and outcomes of patients with crescentic lupus nephritis. Kidney Int. 2009;76(3):307-17.
50. Tateno S, Kobayashi Y, Shigematsu H, Hiki Y. Study of lupus nephritis: its classification and the significance of subendothelial deposits. Q J Med. 1983;52(207):311-31.
51. Austin HA, 3rd, Boumpas DT, Vaughan EM, Balow JE. High-risk features of lupus nephritis: importance of race and clinical and histological factors in 166 patients. Nephrol Dial Transplant. 1995;10(9):1620-8.
52. Descombes E, Droz D, Drouet L, Grunfeld JP, Lesavre P. Renal vascular lesions in lupus nephritis.Medicine (Baltimore). 1997;76(5):355-68.
53. Banfi G, Bertani T, Boeri V, Faraggiana T, Mazzucco G, Monga G, et al. Renal vascular lesions as a marker of poor prognosis in patients with lupus nephritis. Gruppo Italiano per lo Studio della Nefrite Lupica (GISNEL). Am J Kidney Dis. 1991;18(2):240-8.
54. Magil AB, Tyler M. Tubulo-interstitial disease in lupus nephritis. A morphometric study. Histopathology. 1984;8(1):81-7.
55. Kasiske BL, Cangro CB, Hariharan S, Hricik DE, Kerman RH, Roth D, et al. The evaluation of renal transplantation candidates: clinical practice guidelines. Am J Transplant. 2001;1 Suppl 2:3-95.
56. Tang H, Chelamcharla M, Baird BC, Shihab FS, Koford JK, Goldfarb-Rumyantzev AS. Factors affecting kidney-transplant outcome in recipients with lupus nephritis. Clin Transplant. 2008;22(3):263-72.
57. Lochhead KM, Pirsch JD, D'Alessandro AM, Knechtle SJ, Kalayoglu M, Sollinger HW, et al. Risk factors for renal allograft loss in patients with systemic lupus erythematosus. Kidney Int. 1996;49(2):512-7.
58. Bunnapradist S, Chung P, Peng A, Hong A, Lee B, Fukami S, et al. Outcomes of renal transplantation for recipients with lupus nephritis: analysis of the Organ Procurement and Transplantation Network database. Transplantation. 2006;82(5):612-8.
59. Bumgardner GL, Mauer SM, Payne W, Dunn DL, Sutherland DE, Fryd DS, et al. Single-center 1-15-year results of renal transplantation in patients with systemic lupus erythematosus. Transplantation. 1988;46(5):703-9.
60. Ward MM. Outcomes of renal transplantation among patients with end-stage renal disease caused by lupus nephritis. Kidney Int. 2000;57(5):2136-43.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
61. Moroni G, Tantardini F, Gallelli B, Quaglini S, Banfi G, Poli F, et al. The long-term prognosis of renal transplantation in patients with lupus nephritis. Am J Kidney Dis. 2005;45(5):903-11.
62. Deegens JK, Artz MA, Hoitsma AJ, Wetzels JF. Outcome of renal transplantation in patients with systemic lupus erythematosus. Transpl Int. 2003;16(6):411-8.
63. Haubitz M, Kliem V, Koch KM, Nashan B, Schlitt HJ, Pichlmayr R, et al. Renal transplantation for patients with autoimmune diseases: single-center experience with 42 patients. Transplantation. 1997;63(9):1251-7.
64. Grimbert P, Lang P, Frappier J, Bedrossian J, Legendre C, Hiesse C, et al. Renal transplantation in patients with systemic lupus erythematosus: a multicenter study. Transplant Proc. 1997;29(5):2363-4.
65. Grimbert P, Frappier J, Bedrossian J, Legendre C, Antoine C, Hiesse C, et al. Long-term outcome of kidney transplantation in patients with systemic lupus erythematosus: a multicenter study. Groupe Cooperatif de Transplantation d'ile de France. Transplantation. 1998;66(8):1000-3.
66. Azevedo LS, Romao JE, Jr., Malheiros D, Saldanha LB, Ianhez LE, Sabbaga E. Renal transplantation in systemic lupus erythematosus. A case control study of 45 patients. Nephrol Dial Transplant. 1998;13(11):2894-8.
67. Norby GE, Strom EH, Midtvedt K, Hartmann A, Gilboe IM, Leivestad T, et al. Recurrent lupus nephritis after kidney transplantation: a surveillance biopsy study. Ann Rheum Dis. 2010;69(8):1484-7.
68. Contreras G, Mattiazzi A, Guerra G, Ortega LM, Tozman EC, Li H, et al. Recurrence of lupus nephritis after kidney transplantation. J Am Soc Nephrol. 2010;21(7):1200-7.
69. Smyth A, Oliveira GH, Lahr BD, Bailey KR, Norby SM, Garovic VD. A systematic review and meta-analysis of pregnancy outcomes in patients with systemic lupus erythematosus and lupus nephritis. Clin J Am Soc Nephrol. 2010;5(11):2060-8.
70. Oviasu E, Hicks J, Cameron JS. The outcome of pregnancy in women with lupus nephritis. Lupus. 1991;1(1):19-25.
71. Illei GG, Tackey E, Lapteva L, Lipsky PE. Biomarkers in systemic lupus erythematosus. I. General overview of biomarkers and their applicability. Arthritis Rheum. 2004;50(6):1709-20.
72. Mok CC. Biomarkers for lupus nephritis: a critical appraisal. J Biomed Biotechnol. 2010;2010:638413.
73. Liu CC, Ahearn JM. The search for lupus biomarkers. Best Pract Res Clin Rheumatol. 2009;23(4):507-23.
74. Isenberg DA, Manson JJ, Ehrenstein MR, Rahman A. Fifty years of anti-ds DNA antibodies: are we approaching journey's end? Rheumatology (Oxford). 2007;46(7):1052-6.
75. Tseng CE, Buyon JP, Kim M, Belmont HM, Mackay M, Diamond B, et al. The effect of moderate-dose corticosteroids in preventing severe flares in patients with serologically active, but clinically stable, systemic lupus erythematosus: findings of a prospective, randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2006;54(11):3623-32.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
76. Bootsma H, Spronk P, Derksen R, de Boer G, Wolters-Dicke H, Hermans J, et al. Prevention of relapses in systemic lupus erythematosus. Lancet. 1995;345(8965):1595-9.
77. Kavanaugh AF, Solomon DH. Guidelines for immunologic laboratory testing in the rheumatic diseases: anti-DNA antibody tests. Arthritis Rheum. 2002;47(5):546-55.
78. Bardana EJ, Jr., Harbeck RJ, Hoffman AA, Pirofsky B, Carr RI. The prognostic and therapeutic implications of DNA:anti-DNA immune complexes in systemic lupus erythematosus (SLE). Am J Med. 1975;59(4):515-22.
79. Alarcon GS, Calvo-Alen J, McGwin G, Jr., Uribe AG, Toloza SM, Roseman JM, et al. Systemic lupus erythematosus in a multiethnic cohort: LUMINA XXXV. Predictive factors of high disease activity over time. Ann Rheum Dis. 2006;65(9):1168-74.
80. Cortes-Hernandez J, Ordi-Ros J, Labrador M, Bujan S, Balada E, Segarra A, et al. Antihistone and anti-double-stranded deoxyribonucleic acid antibodies are associated with renal disease in systemic lupus erythematosus. Am J Med. 2004;116(3):165-73.
81. Huong DL, Papo T, Beaufils H, Wechsler B, Bletry O, Baumelou A, et al. Renal involvement in systemic lupus erythematosus. A study of 180 patients from a single center. Medicine (Baltimore). 1999;78(3):148-66.
82. Ignat GP, Rat AC, Sychra JJ, Vo J, Varga J, Teodorescu M. Information on diagnosis and management of systemic lupus erythematosus derived from the routine measurement of 8 nuclear autoantibodies. J Rheumatol. 2003;30(8):1761-9.
83. Mirzayan MJ, Schmidt RE, Witte T. Prognostic parameters for flare in systemic lupus erythematosus. Rheumatology (Oxford). 2000;39(12):1316-9.
84. Urowitz MB, Feletar M, Bruce IN, Ibanez D, Gladman DD. Prolonged remission in systemic lupus erythematosus. J Rheumatol. 2005;32(8):1467-72.
85. Yee CS, Farewell V, Isenberg DA, Rahman A, Teh LS, Griffiths B, et al. British Isles Lupus Assessment Group 2004 index is valid for assessment of disease activity in systemic lupus erythematosus. Arthritis Rheum. 2007;56(12):4113-9.
86. Forger F, Matthias T, Oppermann M, Becker H, Helmke K. Clinical significance of anti-dsDNA antibody isotypes: IgG/IgM ratio of anti-dsDNA antibodies as a prognostic marker for lupus nephritis. Lupus. 2004;13(1):36-44.
87. Gladman DD, Urowitz MB, Keystone EC. Serologically active clinically quiescent systemic lupus erythematosus: a discordance between clinical and serologic features. Am J Med. 1979;66(2):210-5.
88. Gladman DD, Hirani N, Ibanez D, Urowitz MB. Clinically active serologically quiescent systemic lupus erythematosus. J Rheumatol. 2003;30(9):1960-2.
89. Ng KP, Manson JJ, Rahman A, Isenberg DA. Association of antinucleosome antibodies with disease flare in serologically active clinically quiescent patients with systemic lupus erythematosus. Arthritis Rheum. 2006;55(6):900-4.
90. ter Borg EJ, Horst G, Hummel EJ, Limburg PC, Kallenberg CG. Measurement of increases in anti-double-stranded DNA antibody levels as a predictor of disease exacerbation in systemic lupus erythematosus. A long-term, prospective study. Arthritis Rheum. 1990;33(5):634-43.
GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
91. Bootsma H, Spronk PE, Ter Borg EJ, Hummel EJ, de Boer G, Limburg PC, et al. The predictive value of fluctuations in IgM and IgG class anti-dsDNA antibodies for relapses in systemic lupus erythematosus. A prospective long-term observation. Ann Rheum Dis. 1997;56(11):661-6.
92. Ho A, Magder LS, Barr SG, Petri M. Decreases in anti-double-stranded DNA levels are associated with concurrent flares in patients with systemic lupus erythematosus. Arthritis Rheum. 2001;44(10):2342-9.
93. Swaak AJ, Groenwold J, Aarden LA, Statius van Eps LW, Feltkamp EW. Prognostic value of anti-dsDNA in SLE. Ann Rheum Dis. 1982;41(4):388-95.
94. Swaak AJ, Aarden LA, Statius van Eps LW, Feltkamp TE. Anti-dsDNA and complement profiles as prognostic guides in systemic lupus erythematosus. Arthritis Rheum. 1979;22(3):226-35.
95. Swaak AJ, Groenwold J, Bronsveld W. Predictive value of complement profiles and anti-dsDNA in systemic lupus erythematosus. Ann Rheum Dis. 1986;45(5):359-66.
96. Zonana-Nacach A, Salas M, Sanchez ML, Camargo-Coronel A, Bravo-Gatica C, Mintz G. Measurement of clinical activity of systemic lupus erythematosus and laboratory abnormalities: a 12-month prospective study. J Rheumatol. 1995;22(1):45-9.
97. Bastian HM, Alarcon GS, Roseman JM, McGwin G, Jr., Vila LM, Fessler BJ, et al. Systemic lupus erythematosus in a multiethnic US cohort (LUMINA) XL II: factors predictive of new or worsening proteinuria. Rheumatology (Oxford). 2007;46(4):683-9.
98. Bastian HM, Roseman JM, McGwin G, Jr., Alarcon GS, Friedman AW, Fessler BJ, et al. Systemic lupus erythematosus in three ethnic groups. XII. Risk factors for lupus nephritis after diagnosis. Lupus. 2002;11(3):152-60.
99. Cortes-Hernandez J, Ordi-Ros J, Labrador M, Segarra A, Tovar JL, Balada E, et al. Predictors of poor renal outcome in patients with lupus nephritis treated with combined pulses of cyclophosphamide and methylprednisolone. Lupus. 2003;12(4):287-96.
100. Linnik MD, Hu JZ, Heilbrunn KR, Strand V, Hurley FL, Joh T. Relationship between anti-double-stranded DNA antibodies and exacerbation of renal disease in patients with systemic lupus erythematosus. Arthritis Rheum. 2005;52(4):1129-37.
101. Wada Y, Ito S, Ueno M, Nakano M, Arakawa M, Gejyo F. Renal outcome and predictors of clinical renal involvement in patients with silent lupus nephritis. Nephron Clin Pract. 2004;98(4):c105-11.
102. Abrass CK, Nies KM, Louie JS, Border WA, Glassock RJ. Correlation and predictive accuracy of circulating immune complexes with disease activity in patients with systemic lupus erythematosus. Arthritis Rheum. 1980;23(3):273-82.
103. Cameron JS, Lessof MH, Ogg CS, Williams BD, Williams DG. Disease activity in the nephritis of systemic lupus erythematosus in relation to serum complement concentrations. DNA-binding capacity and precipitating anti-DNA antibody. Clin Exp Immunol. 1976;25(3):418-27.
104. El Hachmi M, Jadoul M, Lefebvre C, Depresseux G, Houssiau FA. Relapses of lupus nephritis: incidence, risk factors, serology and impact on outcome. Lupus. 2003;12(9):692-6.
105. van den Berg L, Nossent H, Rekvig O. Prior anti-dsDNA antibody status does not predict later disease manifestations in systemic lupus erythematosus. Clin Rheumatol. 2006;25(3):347-52.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
106. Arbuckle MR, James JA, Kohlhase KF, Rubertone MV, Dennis GJ, Harley JB. Development of anti-dsDNA autoantibodies prior to clinical diagnosis of systemic lupus erythematosus. Scand J Immunol. 2001;54(1-2):211-9.
107. Alba P, Bento L, Cuadrado MJ, Karim Y, Tungekar MF, Abbs I, et al. Anti-dsDNA, anti-Sm antibodies, and the lupus anticoagulant: significant factors associated with lupus nephritis. Ann Rheum Dis. 2003;62(6):556-60.
108. Mosca M, Chimenti D, Pratesi F, Baldini C, Anzilotti C, Bombardieri S, et al. Prevalence and clinico-serological correlations of anti-alpha-enolase, anti-C1q, and anti-dsDNA antibodies in patients with systemic lupus erythematosus. J Rheumatol. 2006;33(4):695-7.
109. Manger K, Manger B, Repp R, Geisselbrecht M, Geiger A, Pfahlberg A, et al. Definition of risk factors for death, end stage renal disease, and thromboembolic events in a monocentric cohort of 338 patients with systemic lupus erythematosus. Ann Rheum Dis. 2002;61(12):1065-70.
110. Esdaile JM, Abrahamowicz M, MacKenzie T, Hayslett JP, Kashgarian M. The time-dependence of long-term prediction in lupus nephritis. Arthritis Rheum. 1994;37(3):359-68.
111. Esdaile JM, Joseph L, Abrahamowicz M, Li Y, Danoff D, Clarke AE. Routine immunologic tests in systemic lupus erythematosus: is there a need for more studies? J Rheumatol. 1996;23(11):1891-6.
112. Sinico RA, Rimoldi L, Radice A, Bianchi L, Gallelli B, Moroni G. Anti-C1q autoantibodies in lupus nephritis. Ann N Y Acad Sci. 2009;1173:47-51.
113. Moroni G, Radice A, Giammarresi G, Quaglini S, Gallelli B, Leoni A, et al. Are laboratory tests useful for monitoring the activity of lupus nephritis? A 6-year prospective study in a cohort of 228 patients with lupus nephritis. Ann Rheum Dis. 2009;68(2):234-7.
114. Tsirogianni A, Pipi E, Soufleros K. Relevance of anti-C1q autoantibodies to lupus nephritis. Ann N Y Acad Sci. 2009;1173:243-51.
115. Porcel JM, Ordi J, Castro-Salomo A, Vilardell M, Rodrigo MJ, Gene T, et al. The value of complement activation products in the assessment of systemic lupus erythematosus flares. Clin Immunol Immunopathol. 1995;74(3):283-8.
116. Nagy G, Brozik M, Varga L, Fust G, Kirschfink M, Kiss E, et al. Usefulness of detection of complement activation products in evaluating SLE activity. Lupus. 2000;9(1):19-25.
117. Ramos-Casals M, Campoamor MT, Chamorro A, Salvador G, Segura S, Botero JC, et al. Hypocomplementemia in systemic lupus erythematosus and primary antiphospholipid syndrome: prevalence and clinical significance in 667 patients. Lupus. 2004;13(10):777-83.
118. Sullivan KE, Wisnieski JJ, Winkelstein JA, Louie J, Sachs E, Choi R, et al. Serum complement determinations in patients with quiescent systemic lupus erythematosus. J Rheumatol. 1996;23(12):2063-7.
119. Ho A, Barr SG, Magder LS, Petri M. A decrease in complement is associated with increased renal and hematologic activity in patients with systemic lupus erythematosus. Arthritis Rheum. 2001;44(10):2350-7.
120. Buyon JP, Tamerius J, Belmont HM, Abramson SB. Assessment of disease activity and impending flare in patients with systemic lupus erythematosus. Comparison of the use of complement split products and conventional measurements of complement. Arthritis Rheum. 1992;35(9):1028-37.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
121. Hopkins P, Belmont HM, Buyon J, Philips M, Weissmann G, Abramson SB. Increased levels of plasma anaphylatoxins in systemic lupus erythematosus predict flares of the disease and may elicit vascular injury in lupus cerebritis. Arthritis Rheum. 1988;31(5):632-41.
122. Laitman RS, Glicklich D, Sablay LB, Grayzel AI, Barland P, Bank N. Effect of long-term normalization of serum complement levels on the course of lupus nephritis. Am J Med. 1989;87(2):132-8.
123. Foundation NK. NKF-KDOQI Guidelines. 1997 [cited; Available from: http://www.kidney.org/professionals/kdoqi/guidelines_commentaries.cfm#guidelines
124. Post TW, Rose BD. Overview of the management of chronic kidney disease in adults. UpToDate 182; 2010.
125. Norby GE, Holme I, Fellstrom B, Jardine A, Cole E, Abedini S, et al. Effect of fluvastatin on cardiac outcomes in kidney transplant patients with systemic lupus erythematosus: a randomized placebo-controlled study. Arthritis Rheum. 2009;60(4):1060-4.
126. Yazdany J, Tonner C, Trupin L, Panopalis P, Gillis JZ, Hersh AO, et al. Provision of preventive health care in systemic lupus erythematosus: data from a large observational cohort study. Arthritis Res Ther. 2010;12(3):R84.
127. McInnes PM, Schuttinga J, Sanslone WR, Stark SP, Klippel JH. The economic impact of treatment of severe lupus nephritis with prednisone and intravenous cyclophosphamide. Arthritis Rheum. 1994;37(7):1000-6.
128. Wilson EC, Jayne DR, Dellow E, Fordham RJ. The cost-effectiveness of mycophenolate mofetil as firstline therapy in active lupus nephritis. Rheumatology (Oxford). 2007;46(7):1096-101.
129. Ward MM. Access to care and the incidence of endstage renal disease due to systemic lupus erythematosus. J Rheumatol. 2010;37(6):1158-63.
130. Hopkinson ND, Jenkinson C, Muir KR, Doherty M, Powell RJ. Racial group, socioeconomic status, and the development of persistent proteinuria in systemic lupus erythematosus. Ann Rheum Dis. 2000;59(2):116-9.
131. Ward MM. Medical insurance, socioeconomic status, and age of onset of endstage renal disease in patients with lupus nephritis. J Rheumatol. 2007;34(10):2024-7.
132. Contreras G, Lenz O, Pardo V, Borja E, Cely C, Iqbal K, et al. Outcomes in African Americans and Hispanics with lupus nephritis. Kidney Int. 2006;69(10):1846-51.
133. Barr RG, Seliger S, Appel GB, Zuniga R, D'Agati V, Salmon J, et al. Prognosis in proliferative lupus nephritis: the role of socio-economic status and race/ethnicity. Nephrol Dial Transplant. 2003;18(10):2039-46.
134. Petri M, Perez-Gutthann S, Longenecker JC, Hochberg M. Morbidity of systemic lupus erythematosus: role of race and socioeconomic status. Am J Med. 1991;91(4):345-53.
135. Fernandez M, Alarcon GS, Calvo-Alen J, Andrade R, McGwin G, Jr., Vila LM, et al. A multiethnic, multicenter cohort of patients with systemic lupus erythematosus (SLE) as a model for the study of ethnic disparities in SLE. Arthritis Rheum. 2007;57(4):576-84.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
136. Ward MM. Access to renal transplantation among patients with end-stage renal disease due to lupus nephritis. Am J Kidney Dis. 2000;35(5):915-22.
137. Carls G, Li T, Panopalis P, Wang S, Mell AG, Gibson TB, et al. Direct and indirect costs to employers of patients with systemic lupus erythematosus with and without nephritis. J Occup Environ Med. 2009;51(1):66-79.
138. Clarke AE, Petri M, Manzi S, Isenberg DA, Gordon C, Senecal JL, et al. The systemic lupus erythematosus Tri-nation Study: absence of a link between health resource use and health outcome. Rheumatology (Oxford). 2004;43(8):1016-24.
139. Li T, Carls GS, Panopalis P, Wang S, Gibson TB, Goetzel RZ. Long-term medical costs and resource utilization in systemic lupus erythematosus and lupus nephritis: a five-year analysis of a large medicaid population. Arthritis Rheum. 2009;61(6):755-63.
140. Pelletier EM, Ogale S, Yu E, Brunetta P, Garg J. Economic outcomes in patients diagnosed with systemic lupus erythematosus with versus without nephritis: results from an analysis of data from a US claims database. Clin Ther. 2009;31(11):2653-64.
141. Contreras G, Pardo V, Cely C, Borja E, Hurtado A, De La Cuesta C, et al. Factors associated with poor outcomes in patients with lupus nephritis. Lupus. 2005;14(11):890-5.
142. Esdaile JM, Levinton C, Federgreen W, Hayslett JP, Kashgarian M. The clinical and renal biopsy predictors of long-term outcome in lupus nephritis: a study of 87 patients and review of the literature. Q J Med. 1989;72(269):779-833.
143. Hill GS, Delahousse M, Nochy D, Remy P, Mignon F, Mery JP, et al. Predictive power of the second renal biopsy in lupus nephritis: significance of macrophages. Kidney Int. 2001;59(1):304-16.
144. Magil AB, Puterman ML, Ballon HS, Chan V, Lirenman DS, Rae A, et al. Prognostic factors in diffuse proliferative lupus glomerulonephritis. Kidney Int. 1988;34(4):511-7.
145. Moroni G, Quaglini S, Gallelli B, Banfi G, Messa P, Ponticelli C. The long-term outcome of 93 patients with proliferative lupus nephritis. Nephrol Dial Transplant. 2007;22(9):2531-9.
146. Zavada J, Pesickova S, Rysava R, Olejarova M, Horak P, Hrncir Z, et al. Cyclosporine A or intravenous cyclophosphamide for lupus nephritis: the Cyclofa-Lune study. Lupus. 2010;19(11):1281-9.
147. Steinberg AD, Decker JL. A double-blind controlled trial comparing cyclophosphamide, azathioprine and placebo in the treatment of lupus glomerulonephritis. Arthritis Rheum. 1974;17(6):923-37.
148. Carette S, Klippel JH, Decker JL, Austin HA, Plotz PH, Steinberg AD, et al. Controlled studies of oral immunosuppressive drugs in lupus nephritis. A long-term follow-up. Ann Intern Med. 1983;99(1):1-8.
149. Austin HA, 3rd, Klippel JH, Balow JE, le Riche NG, Steinberg AD, Plotz PH, et al. Therapy of lupus nephritis. Controlled trial of prednisone and cytotoxic drugs. N Engl J Med. 1986;314(10):614-9.
150. Steinberg AD, Steinberg SC. Long-term preservation of renal function in patients with lupus nephritis receiving treatment that includes cyclophosphamide versus those treated with prednisone only. Arthritis Rheum. 1991;34(8):945-50.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
151. Grootscholten C, Ligtenberg G, Hagen EC, van den Wall Bake AW, de Glas-Vos JW, Bijl M, et al. Azathioprine/methylprednisolone versus cyclophosphamide in proliferative lupus nephritis. A randomized controlled trial. Kidney Int. 2006;70(4):732-42.
152. Boumpas DT, Austin HA, 3rd, Vaughn EM, Klippel JH, Steinberg AD, Yarboro CH, et al. Controlled trial of pulse methylprednisolone versus two regimens of pulse cyclophosphamide in severe lupus nephritis. Lancet. 1992;340(8822):741-5.
153. Gourley MF, Austin HA, 3rd, Scott D, Yarboro CH, Vaughan EM, Muir J, et al. Methylprednisolone and cyclophosphamide, alone or in combination, in patients with lupus nephritis. A randomized, controlled trial. Ann Intern Med. 1996;125(7):549-57.
154. Donadio JV, Jr., Holley KE, Ferguson RH, Ilstrup DM. Progressive lupus glomerulonephritis. Treatment with prednisone and combined prednisone and cyclophosphamide. Mayo Clin Proc. 1976;51(8):484-94.
155. Donadio JV, Jr., Holley KE, Ferguson RH, Ilstrup DM. Treatment of diffuse proliferative lupus nephritis with prednisone and combined prednisone and cyclophosphamide. N Engl J Med. 1978;299(21):1151-5.
156. Clark WF, Cattran DC, Balfe JW, Williams W, Lindsay RM, Linton AL. Chronic plasma exchange in systemic lupus erythematosus nephritis. Proc Eur Dial Transplant Assoc. 1983;20:629-35.
157. Pohl MA, Lan SP, Berl T. Plasmapheresis does not increase the risk for infection in immunosuppressed patients with severe lupus nephritis. The Lupus Nephritis Collaborative Study Group. Ann Intern Med. 1991;114(11):924-9.
158. Lewis EJ, Hunsicker LG, Lan SP, Rohde RD, Lachin JM. A controlled trial of plasmapheresis therapy in severe lupus nephritis. The Lupus Nephritis Collaborative Study Group. N Engl J Med. 1992;326(21):1373-9.
159. Mok CC, Ho CT, Siu YP, Chan KW, Kwan TH, Lau CS, et al. Treatment of diffuse proliferative lupus glomerulonephritis: a comparison of two cyclophosphamide-containing regimens. Am J Kidney Dis.2001;38(2):256-64.
160. Houssiau FA, Vasconcelos C, D'Cruz D, Sebastiani GD, Garrido Ed Ede R, Danieli MG, et al. Immunosuppressive therapy in lupus nephritis: the Euro-Lupus Nephritis Trial, a randomized trial of low-dose versus high-dose intravenous cyclophosphamide. Arthritis Rheum. 2002;46(8):2121-31.
161. Bao H, Liu ZH, Xie HL, Hu WX, Zhang HT, Li LS. Successful treatment of class V+IV lupus nephritis with multitarget therapy. J Am Soc Nephrol. 2008;19(10):2001-10.
162. Hu W, Liu Z, Chen H, Tang Z, Wang Q, Shen K, et al. Mycophenolate mofetil vs cyclophosphamide therapy for patients with diffuse proliferative lupus nephritis. Chin Med J (Engl). 2002;115(5):705-9.
163. Ong LM, Hooi LS, Lim TO, Goh BL, Ahmad G, Ghazalli R, et al. Randomized controlled trial of pulse intravenous cyclophosphamide versus mycophenolate mofetil in the induction therapy of proliferative lupus nephritis. Nephrology (Carlton). 2005;10(5):504-10.
164. Ginzler EM, Dooley MA, Aranow C, Kim MY, Buyon J, Merrill JT, et al. Mycophenolate mofetil or intravenous cyclophosphamide for lupus nephritis. N Engl J Med. 2005;353(21):2219-28.
165. Wang J, Hu W, Xie H, Zhang H, Chen H, Zeng C, et al. Induction therapies for class IV lupus nephritis with non-inflammatory necrotizing vasculopathy: mycophenolate mofetil or intravenous cyclophosphamide. Lupus. 2007;16(9):707-12.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
166. Appel GB, Contreras G, Dooley MA, Ginzler EM, Isenberg D, Jayne D, et al. Mycophenolate mofetil versus cyclophosphamide for induction treatment of lupus nephritis. J Am Soc Nephrol. 2009;20(5):1103-12.
167. Isenberg D, Appel GB, Contreras G, Dooley MA, Ginzler EM, Jayne D, et al. Influence of race/ethnicity on response to lupus nephritis treatment: the ALMS study. Rheumatology (Oxford). 2010;49(1):128-40.
168. El-Shafey EM, Abdou SH, Shareef MM. Is mycophenolate mofetil superior to pulse intravenous cyclophosphamide for induction therapy of proliferative lupus nephritis in Egyptian patients? Clin Exp Nephrol. 2010;14(3):214-21.
169. Chan TM, Li FK, Tang CS, Wong RW, Fang GX, Ji YL, et al. Efficacy of mycophenolate mofetil in patients with diffuse proliferative lupus nephritis. Hong Kong-Guangzhou Nephrology Study Group. N Engl J Med. 2000;343(16):1156-62.
170. Chan TM, Tse KC, Tang CS, Lai KN, Li FK. Long-term outcome of patients with diffuse proliferative lupus nephritis treated with prednisolone and oral cyclophosphamide followed by azathioprine. Lupus. 2005;14(4):265-72.
171. Contreras G, Pardo V, Leclercq B, Lenz O, Tozman E, O'Nan P, et al. Sequential therapies for proliferative lupus nephritis. N Engl J Med. 2004;350(10):971-80.
172. Houssiau FA, D'Cruz D, Sangle S, Remy P, Vasconcelos C, Petrovic R, et al. Azathioprine versus mycophenolate mofetil for long-term immunosuppression in lupus nephritis: results from the MAINTAIN Nephritis Trial. Ann Rheum Dis. 2010;69(12):2083-9.
173. Wang HY, Cui TG, Hou FF, Ni ZH, Chen XM, Lu FM, et al. Induction treatment of proliferative lupus nephritis with leflunomide combined with prednisone: a prospective multi-centre observational study. Lupus. 2008;17(7):638-44.
174. Illei GG, Shirota Y, Yarboro CH, Daruwalla J, Tackey E, Takada K, et al. Tocilizumab in systemic lupus erythematosus: data on safety, preliminary efficacy, and impact on circulating plasma cells from an open-label phase I dosage-escalation study. Arthritis Rheum. 2010;62(2):542-52.
175. Catapano F, Chaudhry AN, Jones RB, Smith KG, Jayne DW. Long-term efficacy and safety of rituximab in refractory and relapsing systemic lupus erythematosus. Nephrol Dial Transplant. 2010;25(11):3586-92.
176. Terrier B, Amoura Z, Ravaud P, Hachulla E, Jouenne R, Combe B, et al. Safety and efficacy of rituximab in systemic lupus erythematosus: results from 136 patients from the French AutoImmunity and Rituximab registry. Arthritis Rheum. 2010;62(8):2458-66.
177. Jonsdottir T, Gunnarsson I, Mourao AF, Lu TY, van Vollenhoven RF, Isenberg D. Clinical improvements in proliferative vs membranous lupus nephritis following B-cell depletion: pooled data from two cohorts. Rheumatology (Oxford). 2010;49(8):1502-4.
178. Jayne D, Passweg J, Marmont A, Farge D, Zhao X, Arnold R, et al. Autologous stem cell transplantation for systemic lupus erythematosus. Lupus. 2004;13(3):168-76.
179. Burt RK, Traynor A, Statkute L, Barr WG, Rosa R, Schroeder J, et al. Nonmyeloablative hematopoietic stem cell transplantation for systemic lupus erythematosus. JAMA. 2006;295(5):527-35.
180. Liang J, Zhang H, Hua B, Wang H, Lu L, Shi S, et al. Allogenic mesenchymal stem cells transplantation in refractory systemic lupus erythematosus: a pilot clinical study. Ann Rheum Dis. 2010;69(8):1423-9.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
181. Sun L, Wang D, Liang J, Zhang H, Feng X, Wang H, et al. Umbilical cord mesenchymal stem cell transplantation in severe and refractory systemic lupus erythematosus. Arthritis Rheum. 2010;62(8):2467-75.
182. Siso A, Ramos-Casals M, Bove A, Brito-Zeron P, Soria N, Munoz S, et al. Previous antimalarial therapy in patients diagnosed with lupus nephritis: influence on outcomes and survival. Lupus. 2008;17(4):281-8.
183. Pons-Estel GJ, Alarcon GS, McGwin G, Jr., Danila MI, Zhang J, Bastian HM, et al. Protective effect of hydroxychloroquine on renal damage in patients with lupus nephritis: LXV, data from a multiethnic US cohort. Arthritis Rheum. 2009;61(6):830-9.
184. Rihova Z, Vankova Z, Maixnerova D, Dostal C, Jancova E, Honsova E, et al. Treatment of lupus nephritis with cyclosporine - an outcome analysis. Kidney Blood Press Res. 2007;30(2):124-8.
185. Dooley MA, Hogan S, Jennette C, Falk R. Cyclophosphamide therapy for lupus nephritis: poor renal survival in black Americans. Glomerular Disease Collaborative Network. Kidney Int. 1997;51(4):1188-95.
186. Ioannidis JP, Boki KA, Katsorida ME, Drosos AA, Skopouli FN, Boletis JN, et al. Remission, relapse, and re-remission of proliferative lupus nephritis treated with cyclophosphamide. Kidney Int. 2000;57(1):258-64.
187. Mok CC, Ying KY, Tang S, Leung CY, Lee KW, Ng WL, et al. Predictors and outcome of renal flares after successful cyclophosphamide treatment for diffuse proliferative lupus glomerulonephritis. Arthritis Rheum. 2004;50(8):2559-68.
188. de Castro WP, Morales JV, Wagner MB, Graudenz M, Edelweiss MI, Goncalves LF. Hypertension and Afro-descendant ethnicity: a bad interaction for lupus nephritis treated with cyclophosphamide? Lupus. 2007;16(9):724-30.
189. Mok CC, Ying KY, Ng WL, Lee KW, To CH, Lau CS, et al. Long-term outcome of diffuse proliferative lupus glomerulonephritis treated with cyclophosphamide. Am J Med. 2006;119(4):355 e25-33.
190. Petri M, Brodsky RA, Jones RJ, Gladstone D, Fillius M, Magder LS. High-dose cyclophosphamide versus monthly intravenous cyclophosphamide for systemic lupus erythematosus: a prospective randomized trial. Arthritis Rheum. 2010;62(5):1487-93.
191. Urowitz MB, Ibanez D, Ali Y, Gladman DD. Outcomes in patients with active lupus nephritis requiring immunosuppressives who never received cyclophosphamide. J Rheumatol. 2007;34(7):1491-6.
192. Decker JL, Klippel JH, Plotz PH, Steinberg AD. Cyclophosphamide or azathioprine in lupus glomerulonephritis. A controlled trial: results at 28 months. Ann Intern Med. 1975;83(5):606-15.
193. Houssiau FA, Vasconcelos C, D'Cruz D, Sebastiani GD, de Ramon Garrido E, Danieli MG, et al. Early response to immunosuppressive therapy predicts good renal outcome in lupus nephritis: lessons from long-term followup of patients in the Euro-Lupus Nephritis Trial. Arthritis Rheum. 2004;50(12):3934-40.
194. Tang Z, Yang G, Yu C, Yu Y, Wang J, Hu W, et al. Effects of mycophenolate mofetil for patients with crescentic lupus nephritis. Nephrology (Carlton). 2008;13(8):702-7.
195. Rivera TL, Belmont HM, Malani S, Latorre M, Benton L, Weisstuch J, et al. Current therapies for lupus nephritis in an ethnically heterogeneous cohort. J Rheumatol. 2009;36(2):298-305.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
196. Cortes-Hernandez J, Torres-Salido MT, Medrano AS, Tarres MV, Ordi-Ros J. Long-term outcomes--mycophenolate mofetil treatment for lupus nephritis with addition of tacrolimus for resistant cases. Nephrol Dial Transplant. 2010;25(12):3939-48.
197. Mok CC, Ying KY, Lau CS, Yim CW, Ng WL, Wong WS, et al. Treatment of pure membranous lupus nephropathy with prednisone and azathioprine: an open-label trial. Am J Kidney Dis. 2004;43(2):269-76.
198. Zhang FS, Nie YK, Jin XM, Yu HM, Li YN, Sun Y. The efficacy and safety of leflunomide therapy in lupus nephritis by repeat kidney biopsy. Rheumatol Int. 2009;29(11):1331-5.
199. Froelich CJ, Wallman J, Skosey JL, Teodorescu M. Clinical value of an integrated ELISA system for the detection of 6 autoantibodies (ssDNA, dsDNA, Sm, RNP/Sm, SSA, and SSB). J Rheumatol. 1990;17(2):192-200.
200. Emlen W, Jarusiripipat P, Burdick G. A new ELISA for the detection of double-stranded DNA antibodies. J Immunol Methods. 1990;132(1):91-101.
201. Isenberg DA, Ehrenstein MR, Longhurst C, Kalsi JK. The origin, sequence, structure, and consequences of developing anti-DNA antibodies. A human perspective. Arthritis Rheum. 1994;37(2):169-80.
202. Chubick A, Sontheimer RD, Gilliam JN, Ziff M. An appraisal of tests for native DNA antibodies in connective tissue diseases. Clinical usefulness of Crithidia luciliae assay. Ann Intern Med. 1978;89(2):186-92.
203. Kalmin ND, Bartholomew WR, Wicher K. Relative values of laboratory assays in systemic lupus erythematosus. Am J Clin Pathol. 1981;75(6):846-51.
204. Bootsma H, Spronk PE, Hummel EJ, de Boer G, ter Borg EJ, Limburg PC, et al. Anti-double stranded DNA antibodies in systemic lupus erythematosus: detection and clinical relevance of IgM-class antibodies. Scand J Rheumatol. 1996;25(6):352-9.
205. Pincus T, Schur PH, Rose JA, Decker JL, Talal N. Measurement of serum DNA-binding activity in systemic lupus erythematosus. N Engl J Med. 1969;281(13):701-5.
206. Ballou SP, Kushner I. Anti-native DNA detection by the Crithidia luciliae method: an improved guide to the diagnosis and clinical management of systemic lupus erythematosus. Arthritis Rheum. 1979;22(4):321-7.
207. Garcia CO, Molina JF, Gutierrez-Urena S, Scopelitis E, Wilson WA, Gharavi AE, et al. Autoantibody profile in African-American patients with lupus nephritis. Lupus. 1996;5(6):602-5.
208. Weitzman RJ, Walker SE. Relation of titred peripheral pattern ANA to anti-DNA and disease activity in systemic lupus erythematosus. Ann Rheum Dis. 1977;36(1):44-9.
209. Miniter MF, Stollar BD, Agnello V. Reassessment of the clinical significance of native DNA antibodies in systemic lupus erythematosus. Arthritis Rheum. 1979;22(9):959-68.
210. Ballou SP, Kushner I. Lupus patients who lack detectable anti-DNA: clinical features and survival. Arthritis Rheum. 1982;25(9):1126-9.
211. Isenberg DA, Shoenfeld Y, Schwartz RS. Multiple serologic reactions and their relationship to clinical activity in systemic lupus erythematosus. Arthritis Rheum. 1984;27(2):132-8.

GUIDELINES FOR THE SCREENING, DIAGNOSIS, TREATMENT AND MONITORING OF LUPUS NEPHRITIS IN ADULTS
212. Davis P, Percy JS, Russell AS. Correlation between levels of DNA antibodies and clinical disease activity in SLE. Ann Rheum Dis. 1977;36(2):157-9.
213. Feldman MD, Huston DP, Karsh J, Balow JE, Klima E, Steinberg AD. Correlation of serum IgG, IgM, and anti-native-DNA antibodies with renal and clinical indexes of activity in systemic lupus erythematosus. J Rheumatol. 1982;9(1):52-8.


![Burden of Lupus Nephritis among Patients Managed in ... · Keywords: Lupus Nephritis, Burden, Flares, Hospitalizations, Europe . 1. ... compared with Caucasians (14%) [5].Approximately](https://img.pdfslide.us/doc/110x75/5f08e9627e708231d42452c4/burden-of-lupus-nephritis-among-patients-managed-in-keywords-lupus-nephritis.jpg)