Embed Size (px)
Citation preview
CASE SERIES
Vol. 27, No. 8 August 2015 229
Abstract: Background. Chronic venous leg ulcers (VLUs) can be chal-lenging to manage and heal. Despite the observed efficacy of surgical debridement, many patients with VLUs refuse the procedure due to the associated pain. Autolytic debridement induces no pain, but is slow or disrupted in chronic VLUs. Elucidation of the wound dressing func-tions that are sufficient to support autolytic debridement is needed. Materials and Methods. The authors report 2 challenging cases with large, nonresponsive VLUs. A 52-year-old female patient, Case 1, pre-sented with a VLU of 91.4cm2 (10.5 cm x 8.7 cm); and a 58-year-old female patient, Case 2, presented with bilateral VLUs, the larger of which was 50 cm2 (10 cm x 5 cm). Both VLU cases were covered with yellow slough, and case 1 had a small area of black necrotic tissue. The patients had received standard care for more than 16 months, but their VLUs were worsening. A self-adaptive wound dressing (SAWD) with a compression wrap was applied 2 to 3 times a week. Results. Within 21 days, the VLUs of both cases had shed the yellow slough, and healthy granulation tissue was visible. Conclusion. In summary, the SAWD removed excess exudate with liquefied components of slough and nonvital tissue; provided sufficient moisture for preventing wound desiccation; sequestered microorganisms, thereby blocking their multi-plication; and supported efficient autolytic debridement, clearing most of the slough and all crusted necrotic tissue within 3 weeks. The effect of SAWD on autolytic debridement is a promising mechanism for pro-moting healing of VLUs and warrants further study.
Key words: venous leg ulcer, self-adaptive wound dressing, autolytic debridement, yellow slough, necrotic tissue, trauma
Wounds 2015;27(8):229-235
From the Department of Medicine, California School of Podiatric Medicine, Samuel Merritt University, San Francisco, CA
Address correspondence to:Alex Reyzelman, DPMCalifornia School of Podiatric MedicineSamuel Merritt University2299 Post St. Ste. 205San Francisco, CA [email protected]
Disclosure: OSNovative Systems Inc, Santa Clara, CA, supported this study by providing the self-adaptive wound dressing and editorial assistance.
Evidence of Intensive Autolytic Debridement With a Self-Adaptive Wound Dressing
Alexander M. Reyzelman, DPM and Mher Vartivarian, DPM
The prevalence of venous leg ulcers (VLUs), the most advanced stage of chronic venous insufficiency, ranges from 0.2% to 1% in Western countries,1 with a higher prevalence in people older than
80 years. A minor injury may initiate a skin break on the leg, and delayed healing can be aggravated by comorbidities such as diabetes, persistently high blood pressure, and chronic venous insufficiency. Chronic (VLUs) in a prospective clinical trial at one clinic ranged in size from 1.1 cm2 to 19.2 cm2, and the duration ranged from 6 weeks to 104 weeks.2 The pro-portion of wounds healed within 2 years ranged from 68% for leg wounds

Reyzelman and Vartivarian
230 WOUNDS® www.woundsresearch.com
to 51% for ankle wounds.2 Patients with chronic bacte-rial infections with Pseudomonas aeruginosa, Staphy-lococcus aureus, Proteus mirabilis, or Enterococcus faecalis in their chronic VLU delayed healing of the wound,3 although S. aureus and Proteus spp. did not appear to inhibit healing in a different clinic.2 Guide-lines for the management of VLUs encompass diagno-sis, necessity of debridement and compression therapy, antibiotics, and adjunctive therapies such as isotonic exercise and leg elevation.4 Despite these guidelines,4-6 healing of chronic VLUs can be challenging, and novel approaches for restarting the healing of chronic VLUs are warranted.
Wound bed preparation for renewed healing re-quires attention to the healthy tissue and removal of necrotic tissue and slough; control of infection and inflammation; maintenance of correct moisture; and preservation of the growing healthy tissue at the edge of the wound during wound dressing changes, as in-dicated by the TIME framework for wound healing.7,8 Wound dressings typically were designed to address 1 or more, but not all, of these critical conditions.
Debridement usually is performed before applica-tion of the dressing.8 Debridement of chronic VLUs removes necrotic tissue, any debris, and bacteria from the wound; and it exposes the viable tissue to facili-tate healing.8 Types of wound debridement techniques include autolytic debridement, in which the body re-moves the necrotic tissue; enzymatic debridement, such as with collagenase-based products; biodebride-ment using sterilized maggots;9 mechanical debride-ment; and surgical debridement.10 Autolytic debride-ment usually causes no pain and leaves the wound bed at the correct moisture balance to promote granula-
tion and growth of epithelial cells, but it can be a slow process.10 A chronic VLU has difficulty employing ad-equate autolytic debridement because the wound envi-ronment is not conducive to the process, in that there is too much exudate with an increased number of ma-trix metalloproteinaises. Enzymatic debridement re-quires frequent dressing changes, and the specificity of the protein cleavage is determined by the collagenase or the collagenase/papain preparation. Mechanical de-bridement may involve wound cleansing at 4-14 psi, hydrosurgery at 15,000 psi, whirlpool, atomized saline, polyester fiber pad, or ultrasonic techniques. These techniques are nonspecific, can provide fast results, but can be painful and harm viable tissue.7,10 Chemi-cal debridement often includes the use of antimicrobi-als, and its short-term use can be effective; but it may be painful and may harm healthy tissues.7 From a pain standpoint, autolytic debridement is the clear choice for patient comfort, but inadequate autolytic debride-ment, insufficiently controlled inflammation, and infec-tion contribute to nonhealing VLUs. Autolytic debride-ment may be supported by dressings with hypertonic saline and/or honey via osmosis, and by semiocclusive dressings containing hydrocolloids or hydrogels.7 Re-moval of excess exudate and cellular debris appears to assist in maintaining the process of autolytic de-bridement.11 Hydration response technology, negative pressure wound therapy,11 and a self-adaptive wound dressing (SAWD),12 among other dressings, can remove excess exudate. The optimal moisture levels vary for the different stages of wound healing: a moist milieu is needed to promote granulation and growth of epithe-lial cells, whereas a drier milieu is needed on the new skin at the wound edge.
Wound bed preparation and healing involves the recurrent removal of excess exudate, microorganisms, semisolid slough debris, degraded necrotic tissue, hy-pertonic fluids containing toxic and/or corrosive com-ponents, and maintenance of moisture balance at the wound edge and low-exuding or nonexuding wound areas.5,7,8,13 Minimal or no tissue damage during dress-ing removal maintains the progress of the healing pro-cess. The SAWD can continuously remove the exudate; sequester wound bed microorganisms from debris that may act as food sources; confine absorbed exudate and hypertonic fluids containing toxic and/or corro-sive components, regardless of compression and grav-ity; maintain moisture balance in distinct microzones of the wound bed; adjust moisture in microzones as
Keypoints
• Autolytic debridement usually causes no pain andleaves the wound bed at the correct moisture bal-ance but can be a slow process.10
• A chronic venous leg ulcer (VLU) has difficulty em-ploying adequate autolytic debridement becausethe wound environment is not conducive to theprocess (ie, too much exudate with an increasednumber of matrix metalloproteinaises).
• These case studies examined the ability of a self-adaptive wound dressing and compression wrapsto support relatively rapid autolytic debridement of2 large VLUs that had been unresponsive to vari-ous treatments.

Reyzelman and Vartivarian
Vol. 27, No. 8 August 2015 231
needed; and be removed without damage to newly formed epidermis.14 The authors hypothesized these 6 conditions provided by the novel SAWD are not only necessary but also sufficient to support efficient au-tolytic debridement. These case studies examined the ability of SAWD and compression wraps to support relatively rapid autolytic debridement of 2 large VLUs that had been unresponsive to various treatments for 16.8 months and 19.2 months.
Methods and MaterialsDemographics. The personal medical history for each
patient—demographic (ie, age, race/ethnic origin, and gender), health status (ie, weight, height, and comorbidi-ties), and previous history of VLUs including initiating event, size, prior treatments, and trend of wound—was recorded. Patients were queried on their pain level using a scale of 1 to 10, where 1 indicated no pain and 10 in-dicated the worst pain. The presence or absence of odor and quantity of exudate were recorded.
Self-adaptive wound dressing. The SAWD (Enluxtra, OSNovative Systems, Inc, Santa Clara, CA) consisted of multiple complex layers.14 Each layer of the dress-ing was manufactured to gather secretions from the wound bed in microzones and promote optimal condi-tions for healing. A vapor-permeable layer exhibited a rapid moisture vapor transmission rate (2500 g/m2/24 hours). Other advantageous properties included an absorbent pad that remained flexible even when near capacity, and the vapor-permeable layer that blocked migration of any microbes to the surface. Microzones of the liquid and vapor-permeable layer changed from a high rate of vapor removal for wound beds releasing exudate to a low rate of vapor removal for the peri-wound skin and wound edge, as needed to maintain the optimal moisture conditions for each area. The authors used 4-in gauze wrap (Kerlix, Covidien, Man-sfield, MA) and 4-in self-adherent wrap (Coban, 3M, St. Paul, MN) for compression.
The authors’ private practice wound clinic treats approximately 20-30 patients with VLUs each month. In approximately 50% of the patients, the treating cli-nicians perform surgical debridement, but 45% of pa-tients with VLUs refuse it due to pain. Thus, the authors sought alternative methods that might support pain-less autolytic debridement. The clinic’s current treat-ment procedure shifted to SAWD since July 2014. Since the shift toward SAWD began, the authors have treated 100 patients with VLUs. Here, the authors report 2 of
the more challenging recent cases at the clinic to illus-trate the effect of the SAWD on autolytic debridement.
Case ReportsCase 1. An African-American female of 52 years
presented at the author’s clinic with hypertension, varicose veins, gastroesophageal reflux disease, pred-nisone use, depression, and renal transplantation (5 years prior) in May 2013. Her medications included Loestrin, (Allergan, Parsippany, NJ), Prograf (Astellas Pharma US Inc, Northbrook, IL), furosemide, Protonix (Pfizer Inc, New York, NY), and Cellcept (Genentech, San Francisco, CA). She presented with 2 VLUs measur-ing 10.5 cm x 8.7 cm (91.4cm2) and 8 cm x 5.4 cm (43.2 cm2), which were located on her anterior mid-leg and had arisen from bumping her leg against a sharp corner. The patient’s major complaints included the nonhealing open wound, pain at 10 on the previously described scale of 1 to 10, odor, reduced quality of life (QoL), edema, and an exuberant amount of drainage. Prior treatment for the wound included compression, multiple courses of oral antibiotics, a gel containing platelet-derived growth factor (Regranex, Smith & Nephew, St. Petersburg, FL) for 3 months, and surgical debridement 5 times. The patient refused additional surgical debridement due to pain.
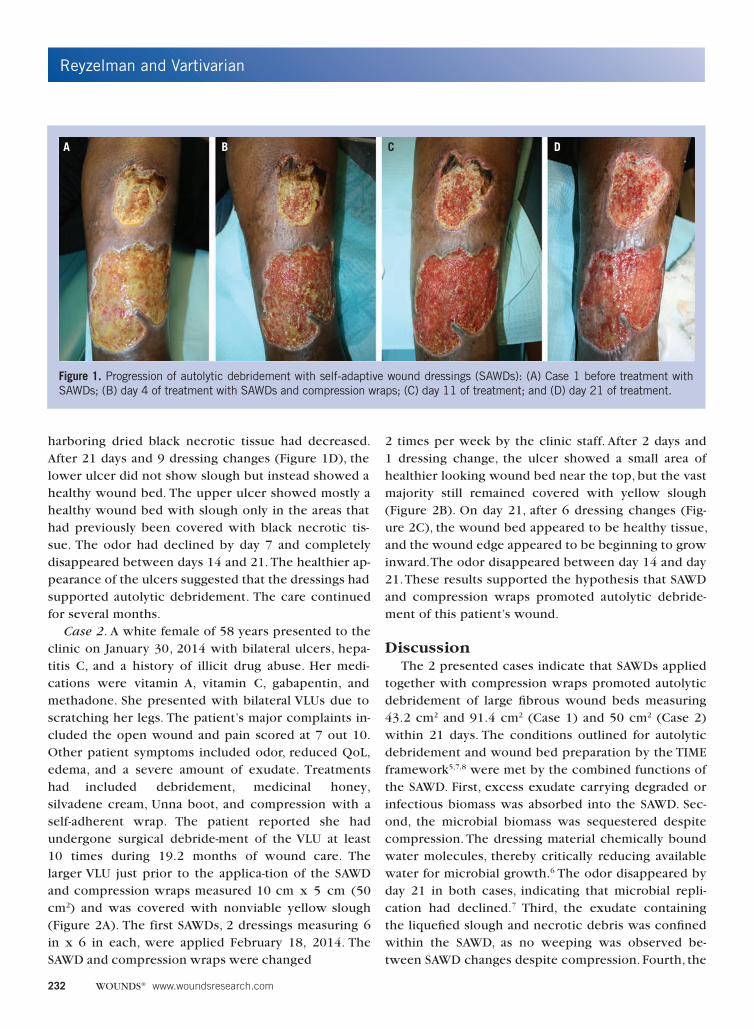
The 2 VLUs showed widespread slough and some dried necrotic tissue in the proximal ulcer before the first SAWDs (2 dressings, each measuring 6 in x 6 in) were applied on January 30, 2014 (Figure 1A), at 16.8 months post-VLU injury. The self-adaptive wound dress-ings and compression wrap were changed every 2 days by the patient at home. On day 4, after 2 SAWD changes (Figure 1B), less slough was observed in the lower ulcer and the lower region of the upper ulcer. Black necrotic tissue was evident on the top ulcer. On day 11, after 5 dressing changes (Figure 1C), the slough disappeared from the lower ulcer but remained present next to the areas with necrotic tissue in the upper ulcer. The area
Keypoints
• The authors’ private practice wound clinic treatsapproximately 20-30 patients with venous leg ul-cers each month.
• 45% of these patients refuse surgical debridementdue to pain.
• The clinic’s current treatment procedure shifted toself-adaptive wound dressings to support painlessautolytoic debridement.
Reyzelman and Vartivarian
232 WOUNDS® www.woundsresearch.com
harboring dried black necrotic tissue had decreased. After 21 days and 9 dressing changes (Figure 1D), the lower ulcer did not show slough but instead showed a healthy wound bed. The upper ulcer showed mostly a healthy wound bed with slough only in the areas that had previously been covered with black necrotic tis-sue. The odor had declined by day 7 and completely disappeared between days 14 and 21. The healthier ap-pearance of the ulcers suggested that the dressings had supported autolytic debridement. The care continued for several months.
Case 2. A white female of 58 years presented to the clinic on January 30, 2014 with bilateral ulcers, hepa-titis C, and a history of illicit drug abuse. Her medi-cations were vitamin A, vitamin C, gabapentin, and methadone. She presented with bilateral VLUs due to scratching her legs. The patient’s major complaints in-cluded the open wound and pain scored at 7 out 10. Other patient symptoms included odor, reduced QoL, edema, and a severe amount of exudate. Treatments had included debridement, medicinal honey, silvadene cream, Unna boot, and compression with a self-adherent wrap. The patient reported she had undergone surgical debride-ment of the VLU at least 10 times during 19.2 months of wound care. The larger VLU just prior to the applica-tion of the SAWD and compression wraps measured 10 cm x 5 cm (50 cm2) and was covered with nonviable yellow slough (Figure 2A). The first SAWDs, 2 dressings measuring 6 in x 6 in each, were applied February 18, 2014. The SAWD and compression wraps were changed
2 times per week by the clinic staff. After 2 days and 1 dressing change, the ulcer showed a small area of healthier looking wound bed near the top, but the vast majority still remained covered with yellow slough (Figure 2B). On day 21, after 6 dressing changes (Fig-ure 2C), the wound bed appeared to be healthy tissue, and the wound edge appeared to be beginning to grow inward. The odor disappeared between day 14 and day 21.These results supported the hypothesis that SAWDand compression wraps promoted autolytic debride-ment of this patient’s wound.
DiscussionThe 2 presented cases indicate that SAWDs applied
together with compression wraps promoted autolytic debridement of large fibrous wound beds measuring 43.2 cm2 and 91.4 cm2 (Case 1) and 50 cm2 (Case 2) within 21 days. The conditions outlined for autolytic debridement and wound bed preparation by the TIME framework5,7,8 were met by the combined functions of the SAWD. First, excess exudate carrying degraded or infectious biomass was absorbed into the SAWD. Sec-ond, the microbial biomass was sequestered despite compression. The dressing material chemically bound water molecules, thereby critically reducing available water for microbial growth.6 The odor disappeared by day 21 in both cases, indicating that microbial repli-cation had declined.7 Third, the exudate containing the liquefied slough and necrotic debris was confined within the SAWD, as no weeping was observed be-tween SAWD changes despite compression. Fourth, the
Figure 1. Progression of autolytic debridement with self-adaptive wound dressings (SAWDs): (A) Case 1 before treatment with SAWDs; (B) day 4 of treatment with SAWDs and compression wraps; (C) day 11 of treatment; and (D) day 21 of treatment.
A B C D

Reyzelman and Vartivarian
Vol. 27, No. 8 August 2015 233
appropriate moisture balance was maintained at the wound edge and low-exuding or nonexuding wound areas. Fifth, the change from slough and crusted necrot-ic tissue to healthy granulation bed involved microzone management of moisture balance, and likely required the dynamic and reversible switching from absorption and hydration properties of SAWD. Moisture levels on the wound bed were adjusted by the SAWD’s absorbent pad, the 2 permeable layers for both liquids and vapors are engineered to adjust moisture build-up in wound microzones, and feature a vapor-breathable layer of hy-groscopic nonwoven fabrics and membranes.14 Sixth, the SAWD removal did not induce noticeable damage to the wound bed or wound edge, so autolytic debride-ment was able to proceed efficiently. Since the VLUs had changed from slough covered (Cases 1 and 2) and bordered with necrotic tissue (Case 1) to a healthy wound bed that could support granulation and reepi-thelialization (Figures 1, 2), these 6 conditions were not only necessary, but were also sufficient, for enabling ef-ficient autolytic debridement in these 2 large chronic VLUs. Self-absorbent wound dressing applications had efficiently supported autolytic debridement during the initial 3 weeks of their use, which was a shorter time period than previously documented.10,15,16
Despite hydration-controlling dressings and antimi-crobial-impregnated dressings, wound care for VLUs,
especially large ulcers (> 20.0cm2), is extremely chal-lenging due to patient variability, the complexity of the wound healing process, and myriad range of available dressings.17 However, Wolcott and Fischenich12 recent-ly reported SAWDs perform satisfactorily for numerous types of wounds, such as diabetic ulcers, venous ulcers, chronic wounds, pressure ulcers, and surgical wounds. Since debridement is a critical step in healing all types of wounds, these results suggest that the wide appli-
Figure 2. Progression of autolytic debridement with self-adaptive wound dressings (SAWDs): (A) Case 2 before treatment with SAWD; (B) day 2 of treatment with SAWDs and compression wraps; and (C) day 21 of treatment.
Keypoints
• The 2 presented cases indicate that self-adaptivewound dressings (SAWD) applied with compres-sion wraps promoted autolytic debridement oflarge fibrous wound beds measuring 43.2 cm2 and91.4 cm2 (Case 1) and 50 cm2 (Case 2) within 21days.
• These 2 cases were challenging because the ve-nous leg ulcers (VLUs) were large, chronic, had notresponded to many types of dressings and treat-ments, and both patients had refused surgical de-bridement due to the pain of the procedure.
• An SAWD in conjunction with compression wrapssupported efficient autolytic debridement alongwith significant pain reduction by the dressing’sremoval of excess exudate, slough, necrotic tissue,and microbial bioburden, as well as its facilitationof the formation of healthy granulation tissue.
A B C
Reyzelman and Vartivarian
234 WOUNDS® www.woundsresearch.com
cability of the SAWD12 may arise at least in part from this dressing’s support of autolytic debridement and its ability to evacuate and sequester microorganisms within the layers, thereby preventing microbial growth and reinfection10 even under compression.
LimitationsOne limitation of this study was the small number
of cases. These 2 cases were challenging because the VLUs were large (91.4 cm2 and 50 cm2); chronic (16.8 months and 19.2 months); had not responded to many types of dressings and treatments; and both patients had refused surgical debridement due to the pain of the procedure. Wound healing of the first patient’s ul-cers was further complicated by her medications, in-
cluding prednisone and immunosuppressive medica-tion for her renal transplant.
A second limitation of this study was the short du-ration of 3 weeks. However, within 3 weeks of initi-ating SAWD, the wound bed of both cases appeared to undergo significant improvement. The rapid transi-tion from slough to granulation tissue bed suggests the SAWD provides the appropriate wound environment for rapid autolytic debridement.
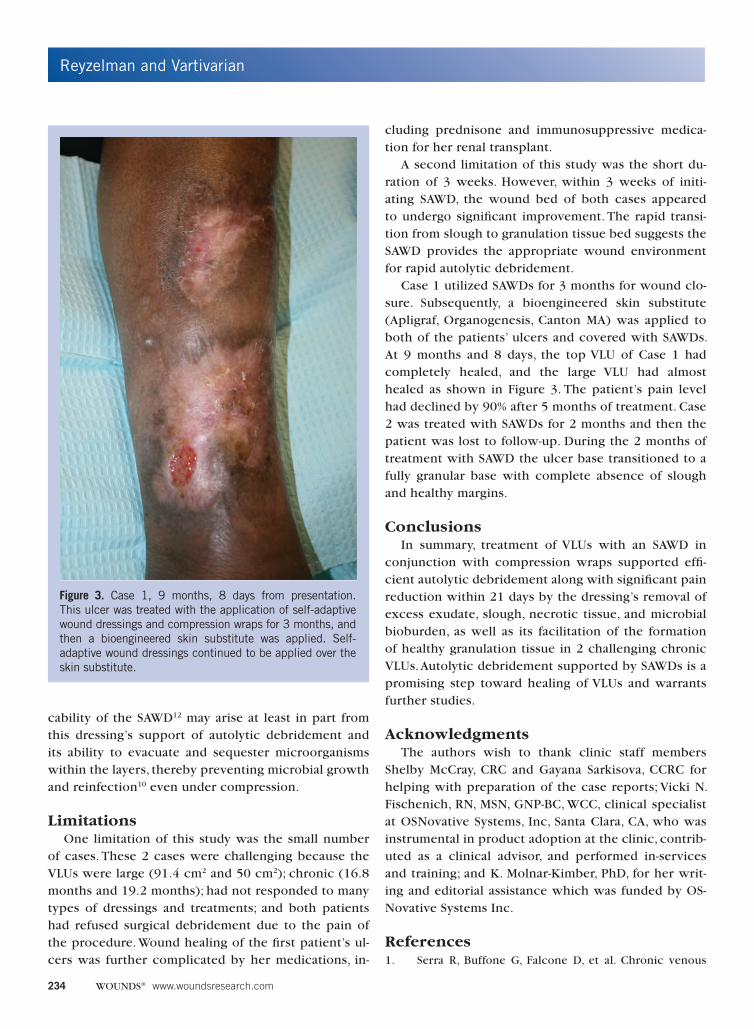
Case 1 utilized SAWDs for 3 months for wound clo-sure. Subsequently, a bioengineered skin substitute (Apligraf, Organogenesis, Canton MA) was applied to both of the patients’ ulcers and covered with SAWDs. At 9 months and 8 days, the top VLU of Case 1 had completely healed, and the large VLU had almost healed as shown in Figure 3. The patient’s pain level had declined by 90% after 5 months of treatment. Case 2 was treated with SAWDs for 2 months and then the patient was lost to follow-up. During the 2 months of treatment with SAWD the ulcer base transitioned to a fully granular base with complete absence of slough and healthy margins.
ConclusionsIn summary, treatment of VLUs with an SAWD in
conjunction with compression wraps supported effi-cient autolytic debridement along with significant pain reduction within 21 days by the dressing’s removal of excess exudate, slough, necrotic tissue, and microbial bioburden, as well as its facilitation of the formation of healthy granulation tissue in 2 challenging chronic VLUs. Autolytic debridement supported by SAWDs is a promising step toward healing of VLUs and warrants further studies.
AcknowledgmentsThe authors wish to thank clinic staff members
Shelby McCray, CRC and Gayana Sarkisova, CCRC for helping with preparation of the case reports; Vicki N. Fischenich, RN, MSN, GNP-BC, WCC, clinical specialist at OSNovative Systems, Inc, Santa Clara, CA, who was instrumental in product adoption at the clinic, contrib-uted as a clinical advisor, and performed in-services and training; and K. Molnar-Kimber, PhD, for her writ-ing and editorial assistance which was funded by OS-Novative Systems Inc.
References1. Serra R, Buffone G, Falcone D, et al. Chronic venous
Figure 3. Case 1, 9 months, 8 days from presentation. This ulcer was treated with the application of self-adaptive wound dressings and compression wraps for 3 months, and then a bioengineered skin substitute was applied. Self-adaptive wound dressings continued to be applied over the skin substitute.
Reyzelman and Vartivarian
Vol. 27, No. 8 August 2015 235
leg ulcers are associated with high levels of metallo-
proteinases-9 and neutrophil gelatinase-associated lipo-
calin.Wound Repair Regen. 2013;21(3):395-401.
2. Lantis JC, 2nd, Marston WA, Farber A, et al. The influence
of patient and wound variables on healing of venous
leg ulcers in a randomized controlled trial of growth-
arrested allogeneic keratinocytes and fibroblasts. J Vasc
Surg. 2013;58(2):433-439.
3. Renner R, Sticherling M, Rüger R, Simon J. Persistence
of bacteria like Pseudomonas aeruginosa in non-heal-
ing venous ulcers. Eur J Dermatol. 2012;22(6):751-
757.
4. Kelechi TJ, Johnson JJ; and WOCN Society.Guideline
for the management of wounds in patients with low-
er-extremity venous disease: an executive summary. J
Wound Ostomy Continence Nurs. 2012;39(6):598-606.
5. Sibbald RG, Goodman L, Woo KY, et al. Special consider-
ations in wound bed preparation 2011: an update. Adv
Skin Wound Care. 2011;24(9):415-436..
6. Robson MC, Cooper DM, Aslam R, et al. Guidelines for
the treatment of venous ulcers.Wound Repair Regen.
2006;14(6):649-662.
7. Leaper DJ, Schultz G, Carville K, Fletcher J, Swanson
T, Drake R. Extending the TIME concept: what have
we learned in the past 10 years?(*). Int Wound J.
2012;9(Suppl 2):1-19.
8. Mosti G. Wound care in venous ulcers. Phlebology.
2013;28(Suppl 1):79-85.
9. Mudge E, Price P, Walkley N, Harding KG. A random-
ized controlled trial of larval therapy for the debride-
ment of leg ulcers: results of a multicenter, randomized,
controlled, open, observer blind, parallel group study.
Wound Repair Regen. 2014;22(1):43-51.
10. Madhok BM, Vowden K, Vowden P. New techniques for
wound debridement. Int Wound J. 2013;10(3):247-251.
11. Hermans MH, Cutting K. NPWT or HRT-dressing? Re-
sults of an expert panel and a Delphi panel analysis. J
Wound Care. 2013;22(11):573-574,576-581.
12. Wolcott R, Fischenich V. Ultimate standardization of
first-line wound dressings to a single type. Todays
Wound Clinic. 2014;8(3):1-3.
13. Sibbald RG, Orsted HL, Coutts PM, Keast DH. Best prac-
tice recommendations for preparing the wound bed:
update 2006.Adv Skin Wound Care. 2007;20(7):390-
405.
14. Siniaguine O, Kachiguina E, inventors. Self-adaptive and
optionally also otherwise adaptable wound dressing.
US patent 9,050,211 B2. June 9, 2015.
15. Alvarez OM, Phillips TJ, Menzoian JO, Patel M, Andries-
sen A. An RCT to compare a bio-cellulose wound dress-
ing with a non-adherent dressing in VLUs. J Wound
Care. 2012;21(9):448-453.
16. Meaume S, Dissemond J, Addala A, et al. Evaluation of
two fibrous wound dressings for the management of
leg ulcers: results of a European randomised controlled
trial (EARTH RCT). J Wound Care. 2014;23(3):105-
106,108-111,114-116.
17. Dargaville TR, Farrugia BL, Broadbent JA, Pace S, Upton
Z,Voelcker NH. Sensors and imaging forwound healing:
a review. Biosens Bioelectron. 2013;41:30-42.