Embed Size (px)
Citation preview

EvidenceBasedPractices:WorkingwithYoungChildren
WhoStutter
KristinA.ChmelaM.A.CCC-SLPBCS-FBuffaloGrove,Illinois
Chmela2018/AllRightsReserved1

“Itisnowwidelyacceptedthatstutteringisamultidimensionaldisorder.Itisalsowidelyacceptedthatstutteringisaneurodevelopmentaldisorder,whichmeansthatitarisesduringdevelopmentinchildhood.”
Chmela2018/AllRightsReserved 2
ChildhoodStuttering–WhereareweandWherearewegoing?
AnneSmith,Ph.D.andChristineWeber,Ph.D.,CCC-SLPSeminarsSpeechLang.2016November;
37(4):291–297

Agenda
• ApplyaRiskFactorAnalysis• DevelopDifferentialTreatmentPlans• Demonstrate5EssentialClinicalSkills
Chmela2018/AllRightsReserved 3

RiskFactors
• Knowledgeof3types
• Researchbased
• GuideChmela2018/AllRightsReserved 4

StutteringPersistencevs.Recovery
Preschool-1stgrade
2nd-4thgrade
5th-8thgrade
1yearpostonset: 63%recover2yearspostonset:47%recover3yearspostonset:16%recover4yearspostonset:5%recover
Chmela2018/AllRightsReserved 5

PrimaryRiskFactors(rankordered)
1.Familyhistoryofpersistedstuttering2.MaleGender3.Trendsoffluencypatternflatorincreasedinfrequency4.Persistence6-12monthspostonset5.Ageatonsetafter3½6.Repetitionsof2-3ormoreunits;quickertempo7.Prolongations/Blocks
6
(Yairi&Ambrose,2005,IllinoisPredictionCriteria;Yairi&Seery,2015;Kraft&Yairi,2011)
Chmela2018/AllRightsReserved

SecondaryRiskFactors
Ø Quantityofstutteringremainssevereafter1yearØ Head&neckmovementremainsfrequent&severeafter1
yearØ Phonologicalskillsbelownormalinearlyphaseof
stutteringØ Expressivelanguageskillsremainadvancedovertimeor
presentasweak
7
(Yairi&Ambrose,2005,IllinoisPredictionCriteria;Yairi&Seery,2015;Kraft&Yairi,2011)
Chmela2018/AllRightsReserved

OtherConsiderations
Ø Childshowsfrustration/withdrawal/avoidanceØ Child’stemperamentpresentswithlowersensory
threshold,adaptability,&attention;higherreactivity&distractibility
Ø OtherdevelopmentalissuespresentØ Caregiversdisplaysignificantanxiety/negativemanner
ofreactingØ Familyhistoryofspeech/language,learning,anxiety,
mood,ADHD,ticorcompulsivedisorders;autismspectrumdisorder
8
Jones,Conture,&Walden,2014;Ntourou,Conture,&Walden,2013Choi,Conture,Walden,Lambert,&Tumanova,2013;
Ntourou,Oyler,&Conture,2013;Eggersetal.,2010;Schwenketal.,2007;Karassetal.,2006;Andersonetal.,2003;Embrechtsetal.,2000
Chmela2018/AllRightsReserved
RiskFactorAnalysis
VeryHigh
High
Medium
Low
VeryLow
9Chmela2018/AllRightsReserved

InitialContactKeyQuestionsIsthereafamilyhistoryofpersistedstuttering?Whatgenderisyourchild?Whendidtheproblemstart?Howlonghasitbeengoingon?Canyoudescribethetrend?Whatisyourchilddoingwhenhe/shestutters?Doyouhaveanyotherconcernsforyourchild?Canyoudescribehis/hertemperament?Howareyou-othersfeelingandreactingtothis?
10Chmela2018/AllRightsReserved

Case Example #1• 27monthsoldboy;“extremelyverbal”• Startedtoexhibitsomenormaltypesofdisfluencyaboutonemonthago
• “Thelasttwodayshecan’tgetasentenceoutatall…he’llstartcryingandsayhecan’tremember.”
• Mothercalledverydistressed• Sheandherhusband“constantlytalktohim”andfeelhislanguageskillsareveryadvanced
• Nohistoryofstutteringinthefamily• Nootherconcernswithdevelopment;verysensitive• Itis“sosadandsuddenandwedon’tknowwhattodo.”
Chmela2018/AllRightsReserved 11
’

InitialContactRiskFactorAnalysisCase#1Primaryfactors?Secondaryfactors?Otherconsiderations?LevelofRisk:
Chmela2018/AllRightsReserved 12

Case Example #2• 6years,0monthsold;male• Startedtostutteratabout4yearsofage• Beganwithpartwordrepetitions;prolongationshavenowemergedinlast2months;hekeepsontalking
• Motherfeelsheisawareofit;Peershaveaskedhimwhyhetalksthewayhedoes
• Concernsregardingattention;levelofintensity• Historyofstutteringinthefamily-motherisnotsureifhestillstuttersornot;paternaluncle
• Verybrightchild;1stgradeteachernotesheseemstobelesstalkativeinclassoverthepastmonthorso
• Didhavespeechtherapyforphonologicaldelaywhenhewas3-4yearsofage;nospeechsincehis5thbirthday 13Chmela2018/AllRightsReserved

InitialContactRiskFactorAnalysisCase#2Primaryfactors?Secondaryfactors?Otherconsiderations?LevelofRisk:
Chmela2018/AllRightsReserved 14

Case Example #3• Age3years,9months;female• Startedtostutteraround2½• Trendhasbeenconsistent(abouta“4”acrossa1-10scaleforfrequency);Asofonemonthago,tensionaroundsomepartwordrepetitionshasemerged
• Fatherstutters;persisted(mothersayssherarelyseesit)• Veryeasygoing,happychild;nodifficultywithtransitions• Seemstohavetroubleexplainingthings;usesmultiplewordandpartwordrepetitions;“uhmandlike”are“everywhere”
• Fatherhighlyconcerned-feelsitishisfault• Historyofearinfections,allergies;nomedications 15Chmela2018/AllRightsReserved

InitialContactRiskFactorAnalysisCase#3Primaryfactors?Secondaryfactors?Otherconsiderations?LevelofRisk:
Chmela2018/AllRightsReserved 16

Environment&Family
Ø Essentialtoinvolveothers(Boeyetal.,2009;Langevinetal.,2010;Bothe&Richardson,2011;Mewherter,M.,&CincinnatiChildren'sHospitalMedicalCenter.(2012).Cincinnati(OH):CincinnatiChildren'sHospitalMedicalCenter,(BESt137),1-7.)
Ø Environmentalimpactsmayimpactexacerbateproblem((Anderson,Pellowski,Conture,&Kelly,2003)
Ø Siblingimpacts(Beilbyetal.,2012) Chmela2018/AllRightsReserved 17

Ø Communicativecompetenceandlimitedverbalparticipation;increasegestureuse,abortattemptstoconveyamessage,maywithdrawfromplay
(Langevinetal.,2009)Ø Morethanhalfofpreschoolchildrenareawareoftheirstutteringanddevelopnegativeperceptionsabouttheirabilitytocommunicate,whichbecomesincreasinglyapparentasageincreases
(Boeyetal.,2009;Vanryckeghem,Brutten,&Hernandez,2005)
Chmela2018/AllRightsReserved 18

ClinicalActions
VeryHigh
High
Medium
Low
VeryLow
19Chmela2018/AllRightsReserved

ClinicalActionsVeryLowtoLowRiskatinitialcontact
-Childusuallyveryyoung(underorearly3’s)-Decisionoftenmadebycarefulexplorationofriskfactorsbyphonecontactoraconsultationsession(screening);videosamplessentinbyparent-RTIoption
Chmela2018/AllRightsReserved 20
RTIRedFlag
• DrivenbyRiskFactors(LowtoVeryLow)
• Allottedforashortperiodoftime
• Accompaniedbydocumentation
RTI
Chmela2018/AllRightsReserved 21

ClinicalActionsVeryLowtoLowRiskFactors
1. Provide educational resources & create follow-up plan
ü Resources:stutteringhelp.orgwestutter.orgü Follow-upwithcaregivershouldoccurnolongerthan3monthspostinitiationofplan,unlesssomethingshiftsdramaticallyandanewplaniscreatedsooner
Chmela2018/AllRightsReserved 22

ClinicalActionsVeryLowtoLowRiskFactors
2. Completion by Caregiver-Other: Perceptions of quantity of stuttering & potential contributing factors
ü UsingaRatingScaleof(0-9;0=nostuttering,2=verylittle,9=constantstuttering),anumberisassignedeachdaybaseduponthequantityofstutteringobserved
ü NoteanyChild-Environmentalfactorsthatmayhaveimpactedtheday
ü RatingsareprovidedtoSLPatendofeachweek
23Chmela2018/AllRightsReserved

ClinicalActionsVeryLowtoLowRiskFactors
3. Daily Modification of select fluency enhancing behaviors
ü deSonneville-KoedootC,StolkE,RietveldT,FrankenM-C(2015)
ü Millard,Edwards,&Cook(2009)ü Franken&Putker-deBrujin(2007)ü Chmela(2005)ü Hill(2003)ü Starkweather&Gotwald(1990)Chmela2018/AllRightsReserved 24

ClinicalActions
VeryHigh
High
Medium
Low
VeryLow
25Chmela2018/AllRightsReserved

ClinicalActionsMedium,High,toVeryHighRisk
atinitialcontactProceedtoacompleteevaluationDetermineneed-developtreatmentandplan
26Chmela2018/AllRightsReserved

MultifactorialDynamicPathwaysTheorySmith,A.,&Weber,C.(2017)
Duringthepreschoolyears,rapid“changesinneurobehavioralsystemsareongoing,andcriticalinteractionsamongthesesystemslikelyplayamajorroleindeterminingpersistenceoforrecoveryfromstuttering.”
Chmela2018/AllRightsReserved 27

Thistheorymotivatestheclinicalpractitionerto“determinethespecificfactorsthatcontributetoeachchild’spathwaytothediagnosisofstutteringandthosemostlikelytopromoterecovery.”
Chmela2018/AllRightsReserved 28

FamilyEnvironment
Executive Functioning
MotorSocial Emotional
SensoryLanguageCognitive
Child
TheBigPicture
Chmela2018/AllRightsReserved 29
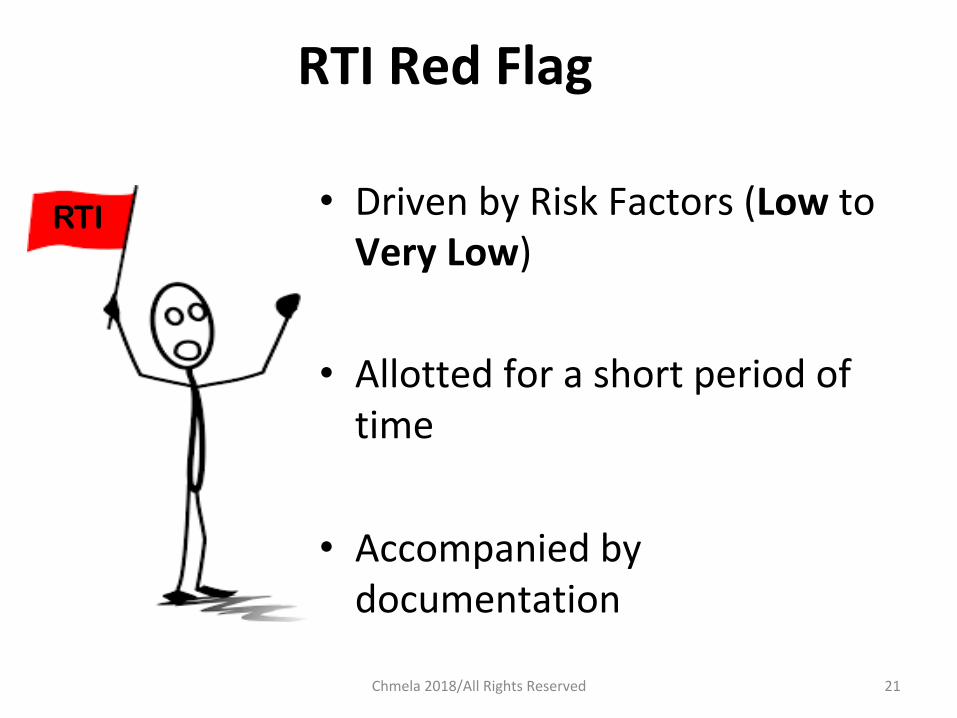
StandardizedFluencyMeasure
InformalSLPFluencyRatings
InformalParent-OtherFluency
Ratings
DetailedHistory Attitudes&Feelings
LanguageMeasures
OtherMeasures ClinicalObservations
TheCritical8EvaluationComponents
Chmela2018/AllRightsReserved30

TreatmentGoal• Establishpatternofnormalfluency(presenceofOtherDisfluencywithinnormalrange;Ratingsofstutter-likedisfluencywithinthe1-2rangeforconsecutiveperiodof8weeks)
• Treatmentinvolvescaregiver• Itispositive,andnaturallyreinforcingtothedevelopmentofpositiveattitudesandfeelingsaboutcommunication;carefulattentionispaidtothechild’sresponseandproblemsaresolvedastheyarise
31Chmela2018/AllRightsReserved

FollowUp
• Treatmentgraduallyfadesaway
• Follow-upoccursforapproximately1year
Chmela2018/AllRightsReserved 32

BriefOverviewofClinicalActionsChildEnrolledinStutteringTreatment
SLP provides education about therapy & resources to caregiver-other
ü Onesessionperweek(unlessotherwarrantedspeech-languagegoals)
ü Overviewofwhattherapyentails
ü Resourcesaboutearlystuttering
33Chmela2018/AllRightsReserved

BriefOverviewofClinicalActionsChildEnrolledinStutteringTreatment
SLP teaches CORE Therapy Element #1: 1) Daily Ratings of stuttering-observations of contributing factors
ü UsingaRatingScaleof(1-10;1=nostuttering,2=verylittle,10=constantstuttering),anumberisassignedeachdaybaseduponthequantityofstutteringobserved;noteanyChild-Environmentalfactorsthatmayhaveimpactedtheday
ü RatingsprovidedtoSLPatendofeachweek;SLPmakesownratingforeachsession;DataChartkept
34Chmela2018/AllRightsReserved

BriefOverviewofClinicalActionsChildEnrolledinStutteringTreatment
SLP teaches caregiver-other CORE Therapy Element #2 Providing 3 kinds of Daily Feedback
ü FeedbackA:VerbalPraiseorRecognitionofSmoothtalking
ü FeedbackB:RequestforSelf-Evaluation
ü FeedbackC:RequestforSelf-Correction
35Chmela2018/AllRightsReserved

BriefOverviewofClinicalActionsChildEnrolledinStutteringTreatment
SLP teaches caregiver-other CORE Therapy Element #3 Problem Solving & Parent Modeling deSonneville-KoedootC,StolkE,RietveldT,FrankenM-C(2015)
ü Eachsessionplottingofratingsfromallparties,discussionofchild’sresponsetofeedback;contributingfactorsfortheweek
ü GradualintroductionofInteractiveCommunicativeBehaviorsasnatural,warranted,andappropriatelytimed
ü Ongoingsupportofoveralldevelopment 36Chmela2018/AllRightsReserved

EvaluationandCaseReview#1
Chmela2018/AllRightsReserved 37
• FemaleM,age5-1;biological2parentfamily,onebrotherage7-6;fatherstuttersandhaspersisted-butonlyoccasionallyaccordingtomother’sreports;onemalecousinonmaternalsidehasADHD;familialenvironmentreportedsomewhathectic,fastpacedcommunicators,frequentrelativesvisitingovernight;frequentsiblingcompetitionfortalking;
• Pediatriciantoldparentsitwouldresolveoverpastyears;parentschosetogethelpatthispoint;moretroublenoticedwhenstorytelling-morecomplexideas
• Medicalhistorynegative;seasonalallergieswithnomedication;cognitiveanddevelopmentalmilestone’swithinnormallimits;easy,gentletemperament

• Stutteringonset2years,11months;cyclicalbutnevercompletelyabated;frequencyandseverityhavemarkedlyincreasedoverpast6months;prolongationsof6-10secondswithpitchandloudnessrise;multiplepartword,rapidrepetitions;Mhasverbalizedabout“notbeingabletotalk;”sometimeswhenMis“caughtupshejustwalksaway”
• Pre-Kteacherconcerned-reducedverbaloutputcomparedtoherpeers;nootherconcerns
• TOCS:ModeratetoSevereRangeofStuttering;PPVT-4:125StandardScore;EVT-2:103StandardScore;CELF-Pscoreswithinaveragetohighaverage,nosignificantdiscrepancies;TNL:86NarrativeLanguageIndex
38Chmela2018/AllRightsReserved

EvaluationandCaseReview#2
39
• Male,age4-2;biological2parentfamily;3malesiblings,ages6,8,10);nohistoryofstutteringinfamily;maternalnephew(age20)dxAutismSpectrumDisorder;structuredandconsistentroutines;highcompetitionfortalking;parentsveryfacepacedcommunicators
• Medicalhistoryrevealedlatetalker;motormilestonesWNL;frequentearinfectionsreporteduntilabout3½yearsofage
• Stutteringonset3-10;severeblockswithincreasesinloudness;facialtensionandarmmovementsusedtogetwordsout;
Chmela2018/AllRightsReserved
• frequentOtherDisfluencies(“uhmuhmuhmuhm”)upto20repetitionsatstartofsomephrases;patternconsistentsinceonset,withratingsof4-7infrequencyoverpastfewweeks)
• Parentsfeltnoawarenessorconcernfromchild;hekeepsontalking;increaseswhenroutinechanges;lackofsleep
• Difficultyfallingasleep;motherreportsheoftenhas“trickydayswithbigmeltdowns”
• Schoolscreeningindicatednostutteringandrecommendedfollowupin3months;followupatschool-nostutteringobserved;pediatrician(4yearoldcheck-up)recommendedspeechevaluation;
40Chmela2018/AllRightsReserved
• Preschoolteachernotestroubletransitioningbetweenactivities&highverbaloutputwithintheclasssetting
• PPVT-4:105StandardScore;EVT-2:100StandardScore;CELF-P:CoreLanguage98;nodiscrepanciesacrosssubtests;developarticerrors
• Temperamentnotedaslessrhythmic,lowerthresholdwithintensereactivity;slightlymorenegativeinmood,distractible;approachesquickly(“seemsfearless”)
41Chmela2018/AllRightsReserved

EvaluationandCaseReview#3
42
• Femaleage2-9;biological2parentfamily;sisterage2months;onsetofstutteringat2-5;Unremarkablebirth,medical,developmentalhistory;Daycareprogram3fulldaysperweek;napsatprogram
• Nohistoryofstuttering;mother(anxietyanddepression;fatherdepression&ADHD);familyrecentlyrelocatedpriortobirthofsecondchild;routinestructuredandconsistent;transitionshurriedandstressful;dadreports“givingintoher”whensheisupset;momsays“painfultowatchandhearthestuttering,butItryandhidemyemotionsfromher”
• SLDatonsetmultiplerepetitions(partwordandwholeword);sinceonsetincreasedtomoreeffort
Chmela2018/AllRightsReserved

• Someprolongations2-5secondswithpitchrise;frequencycontinuestobevariable;atpresentSLDmoderatetosevere;increasedstutteringwithexcitementor“fightingforthefloor;”shekeepsontalkingnomatterwhat
• Atonset,childverbalizedfrustrationatnotbeingableto“getwordsout”buthasnotsaidanythingsince;veryverbal;daycareteacherseesstutteringduringtransitions(dropoff)andwhenfrustrated(ex:notwantingtosharewithapeer)
• DevelopmentalIndicatorsfortheAssessmentofLearning(DIAL-4):WNL;otherS/LareasWNL
• Moderatelevelofwithdrawal;lowerthreshold;mildintensityofreactions;moreadaptable
43Chmela2018/AllRightsReserved

5EssentialClinicalSkillsfor
earlystutteringtreatment
Chmela2018/AllRightsReserved 44

5EssentialClinicalSkills
Chmela2018/AllRightsReserved 45
1.MakingDailyRatings2.TeachingVerbalFeedbackA:Praiseor NoticeSmoothTalking
3.TeachingVerbalFeedbackB:Request forSelf-EvaluationofSmooth Talking
4.TeachingVerbalFeedbackC:Request forRetryofStuttering
5.ProblemSolving&ParentModeling

ClinicalSkill1:MakingDailyRatings
Chmela2018/AllRightsReserved 46
q DiscussOtherDisfluencies(OD)vs.Stutter-LikeDisfluencies(SLD)
q DiscussRatingScale(1-10)usedforvariousaspectsofcommunicativebehavior:1=noobservation,2=verylittleobservation,and10=constantobservation
q ClinicianandcaregivereachmakeratingofSLDatendofsessionandcompareresults

q Caregiverisassignedtomakearatingattheendofeachdayusingthe(1-10)scale.“Attheendoftheday,howmuchSLDdidyouhear?”
q Ratingsarecollectedeveryweek&plottedondatachart
MakingDailyRatings
Chmela2018/AllRightsReserved 47

Troubleshootingv Feeling bad rating higher
v Not doing it
v Not bringing it
v Differentiating between OD and SLD
v Rating severity of “moment” verses daily quantity Chmela2018/AllRightsReserved 48

ClinicalSkill#2:TeachingVerbalFeedbackAPRAISEorNOTICESmoothTalking
q ExplainVerbalFeedbackAtocaregiverq DemonstratehowtoadministerFeedbackAduringshortactivitywithnaturalinteraction;reducelanguagedemandifneededinordertofacilitatesmoothspeechtoprovidethiscontingency
q AllowthecaregivertoaskquestionsaboutFeedbackA
Chmela2018/AllRightsReserved 49
q Havecaregivertryandadminister5-10ofFeedbackAonhisorherowninsession
q AssignDailySpecialTimefor10minuteswithadministrationofabout(ahandful,5-6orso)ofFeedbackA(Praise/Notice)onlyduringthespecialtime.
Chmela2018/AllRightsReserved 50

Troubleshootingv What to say
v How to say it
v When to have special time
v What to do during special time
v Dealing with the child’s response Chmela2018/AllRightsReserved 51

q ExplainVerbalFeedbackBtocaregiverq DemonstratehowtoadministerfeedbackA+Btogether,orA(fourtimes),followedbyB(onetime) A+A+A+A+B=OnesetofFeedback
q AllowthecaregivertoaskquestionsaboutprovidingAandBFeedbacktogether
Chmela2018/AllRightsReserved 52
ClinicalSkill#3:TeachingVerbalFeedbackBREQUESTaSELF-EVALUATIONofSmooth
Talking
q Havecaregivertryandadminister1stand2ndtypesonhisorherowninsession
q Observechild’sresponseandproblemsolveifwarranted
q AssigncombinationofbothtypesduringDailySpecialTime
Chmela2018/AllRightsReserved 53

Troubleshootingv What to say
v How to get child’s attention
v What to do when you get no response
v What to do if the response is not correct
Chmela2018/AllRightsReserved 54

q ExplainVerbalFeedbackCtocaregiverq DemonstratehowtoadministerFeedbackC
q ReviewhowFeedbackCiscombinedwithA+B:4(Praise-Notice)+1(RequestforSelf-Evaluation)+1(RequestforRetry)=1SETofFeedbackorContingencies
Chmela2018/AllRightsReserved 55
ClinicalSkill#4:TeachingVerbalFeedbackCREQUESTaReTry

q Allowthecaregivertoaskquestionsabout3rdtype
q Havecaregivertryandadminister1-2fullsets
duringsessionq ContinueDailySpecialTime;havecaregiver
administer2FullSetsduringthattime,andanothersetanyothertimeofday.
Chmela2018/AllRightsReserved 56
VerbalFeedbackC:REQUESTaRETRY

Troubleshootingv What to say
v How to get child’s attention
v When to administer it v Dealing with the child’s response
Chmela2018/AllRightsReserved 57

RESTART-DCMApplicationsØ Reducingdemands&enhancingcapacitiesØ ParentModelingoftypicalfluencyenhancingbehaviorsØ ReinforcementforchildØ ClinicalModeling
Chmela2018/AllRightsReserved 58
ParentProblemSolving&Modeling
deSonneville-KoedootC,StolkE,RietveldT,FrankenM-C(2015)DirectversusIndirectTreatmentforPreschoolChildrenwhoStutter:TheRESTARTRandomizedTrial.PLoSONE10(7):e0133758.doi:10.1371/journal.pone.0133758

GradualDismissalTransitionØ 13-16sessionsapproximately(somechildrentakemuchlonger;somecontinuetopersist)
Ø Criteria:-Caregiverdailyratingsfor6-8weeksof1sand2s,(severalperiodsof1sinarow)-Similarclinicalobservations;nootherspeech- languagegoalsorconcerns
Ø Graduallyreducetherapysessions(overthecourseof1year)
DuringtheTransitionPeriod,caregiverscontinueengaginginbehaviorsconducivetohealthycommunicationdevelopment,providingverbalcontingencies,andmakingdailyratings.Administrationofcontingenciesgraduallyfadesawayasthecaregiveriscomfortable.
59Chmela2018/AllRightsReserved

Troubleshootingv When to introduce
v How to highlight it
v How to integrate it into work with feedback
Chmela2018/AllRightsReserved 60

Manner Space Position Routine Support
Chmela2018/AllRightsReserved 61
KeyElements:workingwithyoungchildrenwhostutter

62
RecommendedBooks:HowtoTalkSoLittleKidsWillListen:ASurvivalGuidetoLifewithChildrenAges2-7(Faber&King,2017)
TheWholeBrainChild(DanielSiegel)
Chmela2018/AllRightsReserved

63
• HowdoIknowthat?• Whatdoesthatlooklike?• AmI/arewemakinganassumption?• Isthatanobservationorajudgment?Chmela2018/AllRightsReserved

Alm,P.A.(2014).Stutteringinrelationtoanxiety,temperament,andpersonality:Reviewandanalysiswithfocusoncausality.JournalofFluencyDisorders,40,5-21.Ambrose,N.G.,Yairi,E.,&Cox,N.(1993).GeneticAspectsofearlychildhoodstuttering.JournalofSpeechandHearingResearch,1,289-300.Ambrose,N.G.,Yairi,E.,&Cox,N.(1997).Thegeneticbasisofpersistenceandrecoveryinstuttering.JournalofSpeechandHearingResearch,36,701-707.Anderson,J.D.,Pellowski,M.W.,&Conture,E.G.(2005).Childhoodstutteringanddissociationsacrosslinguisticdomains.JournalofFluencyDisorders,30(3),219-253.Anderson,J.D.,Pellowski,M.W.,Conture,E.G.,&Kelly,E.M.(2003).Temperamentalcharacteristicsofyoungchildrenwhostutter.JournalofSpeech,Language,andHearingResearch,46(5),1221-1233.Beilby,J.M.,Byrnes,M.L.,&Young,K.N.(2012).Theexperiencesoflivingwithasiblingwhostutters:Apreliminarystudy.JournalofFluencyDisorders,37,135–148.BernsteinRatner,N.(2005).Evidenced-basedpracticeinstuttering:Somequestionstoconsider.JournalofFluencyDisorders,Vol30,3,pp.163-188.Bloodstein,O.&BernsteinRatner,N.(2008).Ahandbookonstuttering,6thedition.Clifton,NY:DelmarBoey,R.A.,VandeHeyning,P.H.,Wuyts,F.L.,Heylen,L.,Stoop,R.,&DeBodt,M.S.(2009).AwarenessandreactionsofyoungStutteringchildrenaged2–7yearsoldtowardstheirspeechdisfluency.JournalofCommunicationDisorders,42,334–346.Bothe,A.K.,&Richardson,J.D.(2011).Statistical,practical,clinical,andpersonalsignificance:Definitionsandapplicationsinspeech-languagepathology.AmericanJournalofSpeech-LanguagePathology,20,233–242.Bothe,A.K.(2004).Evidenced-based,Outcomes-focuseddecisionsaboutstutteringtreatment:Clinicalrecommendationsincontext.InA.K.Bothe’s(Ed.),Evidenced-basedtreatmentofstuttering:Empericalbasesandclinicalapplications(pp.261-270).Mahwah,NewJersey:LawrenceErlbaumAssociates.Chang,S.E.(2014).Researchupdatesinneuroimagingstudiesofchildrenwhostutter.SeminarsinSpeechandLanguage,35,67-79.Chang,S.E.,Erickson,K.I.,Ambrose,N.G.,Hasegawa-Johnson,M.A.,&Ludlow,C.L.(2008).BrainanatomydifferencesinChildhoodstuttering.Neuroimage,39(3),1333-1344.Chang,S.E.,&Zhu,D.C.(2013).Neuralnetworkconnectivitydifferencesinchildrenwhostutter.Brain,136(Pt.12),3709-3726.Choi,D.,Conture,E.G.,Walden,T.A.,Lambert,W.E.,&Tumanova,V.(2013).Behavioralinhibitionandchildhoodstuttering.JournalofFluencyDisorders,38(2),171-183.Chmela,K.A.(2015*).Workingwithpreschoolerswhostutter:Successfulinterventionstrategies.Memphis,TN:StutteringFoundationof
America.*(originallyfilmedin2004)
64
SelectedReferencesandResources
Chmela2018/AllRightsReserved

deSonneville-KoedootC,StolkE,RietveldT,FrankenM-C(2015)DirectversusIndirectTreatmentforPreschoolChildrenwhoStutter:TheRESTARTRandomizedTrial.PLoSONE10(7):e0133758.doi:10.1371/journal.pone.0133758
Einarsdόttir,J.,&Ingham,R.(2009).Accuracyofparentidentificationofstutteringoccurrence.InternationalJournalofLanguage&CommunicationDisorders,44,847–863.
Ezrati-Vincour,R.,Platzky,R.,&Yairi,E.(2001).Theyoungchild'sawarenessofstuttering-likedisfluency.JournalofSpeech,Language,andHearingResearch,44,368-380.
Foote,G.(2013,March).Stuttering,bilingualism,andworkingconfidentlyoutsideyourcomfortzone.TheASHALeader.Retrievedfromhttp://leader.pubs.asha.org/Article.aspx?articleid=1784842.
Franken,M.,Kielstra-VanderSchalk,C.,&Boelens,H.(2005).Experimentaltreatmentofearlystuttering:Apreliminarystudy.JournalofFluencyDisorders,30(3),189-199.)
Franken,M.C.&Putker-deBruijn,D.(2007).Restart-DCMMethod.TreatmentprotocoldevelopedwithinthescopeoftheZonMWprojectCost-effectivenessoftheDemandsandCapacitiesModelbasedtreatmentcomparedtotheLidcombeprogrammeofearlystutteringintervention:Randomisedtria.l
Gregory,H.H.(1973b).Stuttering:Differentialevaluationandtherapy.Indianapolis:Bobbs-Merrill.Gregory,H.H.(2003).Stutteringtherapy:rationaleandprocedures,(pp.217-262).Boston:Allyn&Bacon.Hill,D.(2003).Differentialtreatmentofstutteringintheearlystages.InH.H.Gregory(Eds.),StutteringTherapy:rationaleandprocedures(pp.
142-184).Boston,M.A.:Allyn&Bacon.Jones,R.M.,Conture,E.G.,&Walden,T.A.(2014).Emotionalreactivityandregulationassociatedwithfluentandstutteredutterancesof
preschool-agechildrenwhostutter.JournalofCommunicationDisorders,48,38-51.Jones,R.,Choi,D.,Conture,E.,&Walden,T.(2014,May).Temperament,emotion,andchildhoodstuttering.SeminarsinSpeechandLanguage,
35(2),114-131).Thieme.Jones,M.,Onslow,M.,Packman,A.,Williams,S.,Ormond,T.,Schwarz,I.,&Gebski,V.(2005).RandomisedcontrolledtrialoftheLidcombe
programmeofearlystutteringintervention.BritishMedicalJournal,331(7518),659-661.Jones,M.,Hearne,A.,Onslow,M.,Ormond,T.,Williams,S.,Schwarz,I.,&O'Brian,S.(2007)Extendedfollowupofarandomisedcontrolledtrial
oftheLidcombeProgramofEarlyStutteringIntervention.Manuscriptinpreparation.Karrass,J.,Walden,T.A.,Conture,E.G.,Graham,C.G.,Arnold,H.S.,Hartfield,K.N.,&Schwenk,K.A.(2006).Relationofemotionalreactivityand
regulationtochildhoodstuttering.JournalofCommunicationDisorders,39,pp.402-423.Langevin,M.,Packman,A.,&Onslow,M.(2009).Peerresponsestostutteringinthepreschoolsetting.AmericanJournalofSpeech-Language
Pathology,18,264–276.Langevin,M.,Packman,A.,etal.(2010).ParentPerceptionsoftheImpactofStutteringonTheirPreschoolersandThemselves.JournalofCommunicationDisorders,43(5),407-423.
�
65Chmela2018/AllRightsReserved

Millard,S.K.,Edwards,S.,&Cook,F.M.(2009).Parent-childinteractiontherapy:Addingtotheevidence.InternationalJournalofSpeech-LanguagePathology,Vol.11,No.1.,pp.61-76.Millard,S.K.,&Davis,S.(2016).ThePalinParentRatingScales:Parents’PerspectivesofChildhoodStutteringandItsImpact.JournalofSpeech,Language,andHearingResearch,Vol.59,950-963.Ntourou,K.,Conture,E.G.,&Lipsey,M.W.(2011).Languageabilitiesofchildrenwhostutter:Ameta-analyticalreview.AmericanJournalof
Speech-LanguagePathology,20(3),163-179.Ntourou,K.,Conture,E.G.,&Walden,T.A.(2013).Emotionalreactivityandregulationinpreschool-agechildrenwhostutter.JournalofFluency
Disorders,38(3),260-274.Nye,C.,Vanryckeghem,M.,Schwartz,J.,Herder,C.,Turner,H.,&Howard,C.(2013).Behavioralstutteringinterventionsforchildrenand
adolescents:Asystematicreviewandmeta-analysis.JournalofSpeech,Language,andHearingResearch,56,921-932.Onslow,M.,&O'Brian,S.(2012).Managementofchildhoodstuttering.JournalofPaediatricsandChildHealth,49(2),E112-E115.Onslow,M.,&Packman,A.(1999).TheLidcombeProgramofEarlyStutteringIntervention.InN.B.Ratner&E.C.Healy(Eds.),StutteringResearchandPractice–BridgingtheGap(pp.193-210).N.J:LawrenceErlbaumAssociates,Inc.Onslow,M.,Packman,A.&Harrison,E.(2003).TheLidcombeProgramofearlystutteringintervention:Aclinician’sguide.Austin,TX:Pro-Ed.Packman,A.,Onslow,M.,Webber,M.,Harrison,E.,Arnott,S.,Bridgman,K.,&Lloyd,W.(2016).TheLidcombeProgramtreatmentguide.
Retrievedfromhttp://sydney.edu.au/health-sciences/asrc/docs/lp_treatment_guide_2016.pdfPiaget,J.(1971).Biologyandknowledge.Chicago:UniversityofChicagoPress.Plexico,L.W.,&Burrus,E.(2012).Copingwithachildwhostutters:Aphenomenologicalanalysis.JournalofFluencyDisorders,37,275–288.Riley,G.D.(2009).StutteringSeverityInstrument–FourthEdition.SanAntonio,TX:Pearson.Shenker,R.C.(2013).Bilingualmyth-bustersseries.Whenyoungchildrenwhostutterarealsobilingual:Somethoughtsaboutassessmentandtreatment.PerspectivesonCommunicationDisordersandSciencesinCulturallyandLinguisticallyDiverse(CLD)Populations,20(1),15-23.StarkweatherCW.Theepigenesisofstuttering.JFluencyDisord2002Winter;27(4):269–87.PMID:12506446StarkweatherCW,GottwaldSR.ThedemandsandcapacitiesmodelII:Clinicalapplications.JFluencyDisord1990;15(3):143–157.Vanryckeghem,M.,&Brutten,G.J.(2007).CommunicationAttitudeTestforPreschoolandKindergartenChildrenWhoStutter(KiddyCAT).SanDiego,CA:Plural.Vanryckeghem,M.,Brutten,G.J.,&Hernandez,L.M.(2005).Acomparativeinvestigationofthespeech-associatedattitudeofpreschoolandkindergartenchildrenwhodoanddonotstutter.JournalofFluencyDisorders,30,307–318.Woods,S.,Shearsby,J.,Onslow,M.,&Burnham,D.(2002).ThepsychologicalimpactoftheLidcombeProgramofearlystutteringintervention:Eightcasestudies.InternationalJournalofLanguageandCommunicationDisorders,37,31-40.
66Chmela2018/AllRightsReserved

Yairi,E.,&Ambrose,N.G.(1999).EarlychildhoodstutteringI:Persistencyandrecoveryrates.JournalofSpeech,Language,andHearingResearch,42(5),1097-1112
Yairi,E.,Ambrose,N.,&Cox,N.(1996).Geneticsofstuttering:Acriticalreview.JournalofSpeechandHearingResearch,39,
771-784.
Yairi,E.,&Ambrose,N.G.(2005).Earlychildhoodstuttering:Forcliniciansbyclinicians.Austin,TX:Pro-Ed.Yairi,E.,&Ambrose,N.G.(2013).Epidemiologyofstuttering:21stcenturyadvancements.JournalofFluencyDisorders.38,66-87.
Yairi,E.(1997).Disfluencycharacteristicsofchildhoodstuttering.InR.F.Curlee&G.M.Siegel(Eds.),Stutteringresearchand
practice:Bridgingthegap(pp.45-54).Malwah,NJ:LawrenceErlbaumAssociates.Yairi,E.,&Seery,E.(2015).Stuttering:Foundationsandclinicalapplications.(2nded.)NeedhamHeights,MA:Allyn&Bacon.
Yaruss,J.S.(1998).Real-timeanalysisofspeechfluency:Proceduresandreliabilitytraining.AmericanJournalofSpeechLanguagePathology,7(2),25-37.
Yaruss,J.S.,Coleman,C.,&Hammer,D.(2006).Treatingpreschoolchildrenwhostutter:Descriptionandpreliminaryevaluationofafamily-focusedtreatmentapproach.Language,Speech,andHearingServicesinSchools,37,pp.118-136.
Ø StutteringFoundation:stutteringhelp.org;1-800-992-9392Ø AmericanBoardofFluencyandFluencyDisorders:stutteringspecialists.orgØ TheStutteringHomePage:www.stutteringhomepage.comØ TheNationalStutteringAssociation(nsa.org);FriendsWhoStutter:(friendswhostutter.org);SAY:StutteringAssociationfortheYoung
(say.org)
Chmela2018/AllRightsReserved 67