Embed Size (px)
Citation preview
10/22/2014
1
Michelle Von Arx, MS, OT/L
Director of Rehabilitation, PSHR
Participants will define community re-entry
Participants will be able to identify barriers to successful community re-entry for Brain Injured patients
Participants will understand relevant research & best practices to support the role of community re-entry in rehabilitation programs
Community Re-Entry Community Integration Community Reintegration
Community reintegration is achieved in the form of functional independence in environments outside of institutions. (Yasui & Bervin, 2009)
10/22/2014
2
Community integration refers to re-establishing, to the degree possible, previously existing roles and relationships, creating substitute new ones, and assisting people in making these changes. (Egbert, Koch, Coeling and Ayers, 2006)
The concept of community integration extends beyond self-care and physical function to include engagement in expected vocational, social, and community roles. (Salter, Foley, Jutai, Bayley & Teasell, 2008)
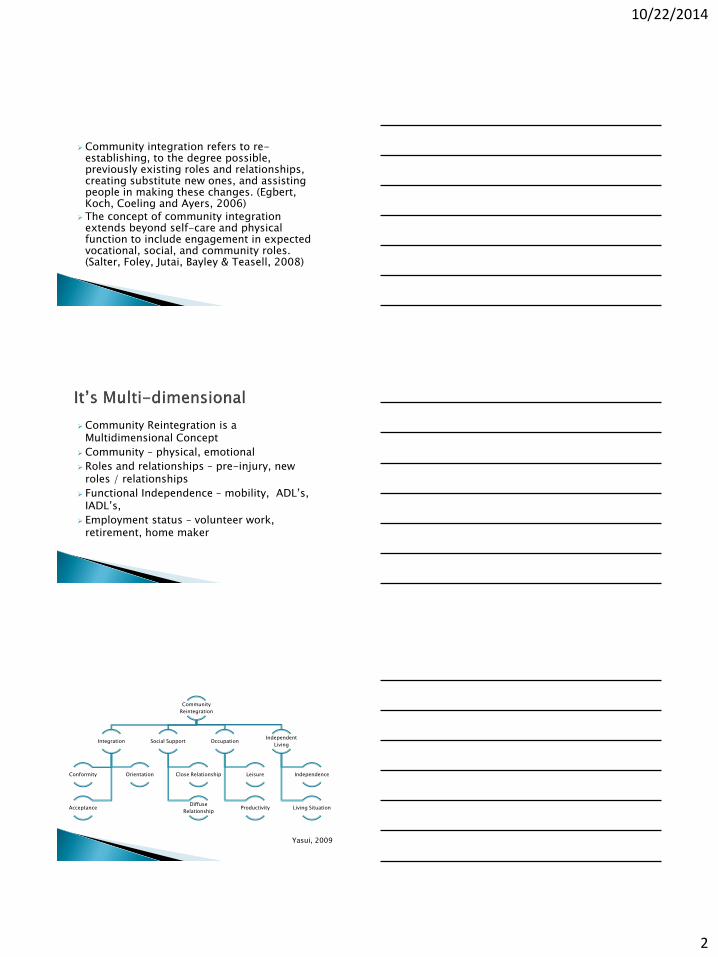
Community Reintegration is a Multidimensional Concept
Community – physical, emotional
Roles and relationships – pre-injury, new roles / relationships
Functional Independence – mobility, ADL’s, IADL’s,
Employment status – volunteer work, retirement, home maker
Community
Reintegration
Integration
Conformity Orientation
Acceptance
Social Support
Close Relationship
Diffuse
Relationship
Occupation
Leisure
Productivity
Independent
Living
Independence
Living Situation
Yasui, 2009
10/22/2014
3
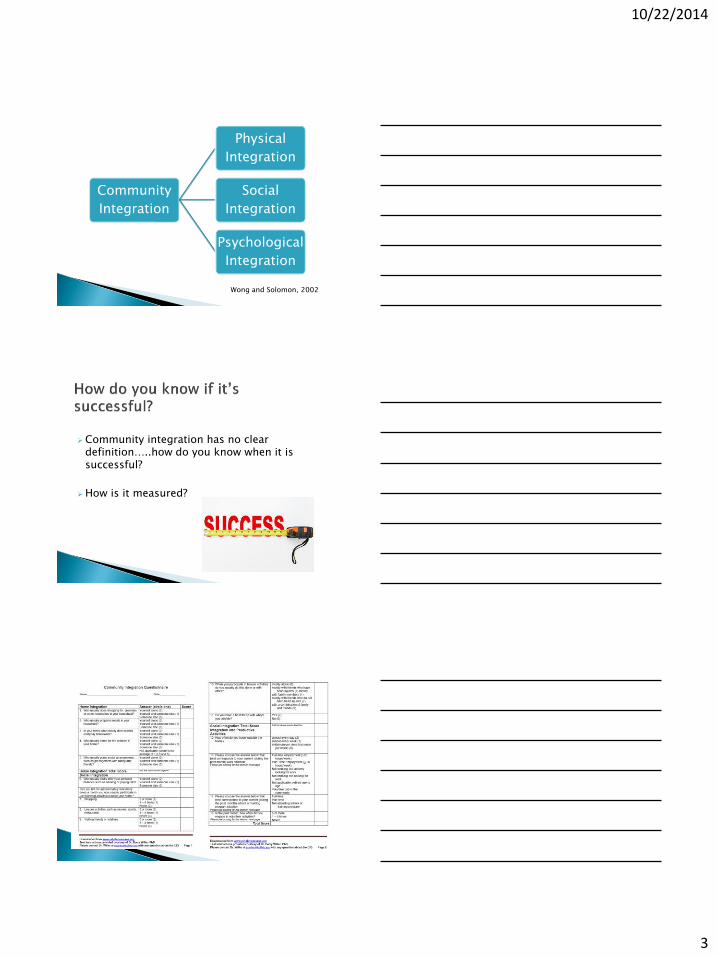
Community
Integration
Physical
Integration
Social
Integration
Psychological
Integration
Wong and Solomon, 2002
Community integration has no clear definition…..how do you know when it is successful?
How is it measured?

10/22/2014
4
Pros: • Strong psychometric properties
• Easy administration (Yasui, 2009)
Cons: • Skewed results for sex, age, level of education
• Favors those who engage in many different activities (Ritchie, 2014)
Community Integration Measure (CIM)
Craig Handicap Assessment and Reporting Technique (CHART)
Reintegration to Normal Living Index (RNLI)
Sidney Psychosocial Reintegration Scale (SPRS)
Salter, 2008
Community Re-Entry
• Commonly used terminology without a clear definition
• Multidimensional
• Client-specific
• Measurable
10/22/2014
5
• Executive dysfunction
• Memory deficits
• Self regulation difficulty
• Impaired self awareness
• Impaired attention & concentration
• Aggression & irritability
• Impulsivity
• Disinhibition
• Depression & anxiety
• Personality changes
• Lack of motivation
• Alcohol & drug misuse
• Fatigue
Mahar and Fraser, 2012
208 patients 2-5 years post discharge from inpatient rehab
Used CIQ to divide patients into 3 groups (working, balanced, poorly integrated)
Poorly integrated group had a more severe injury characterized by longer periods of acute care, post-traumatic amnesia, and greater functional disability on discharge
Balanced group had higher participation in home and social activities compared to working group
Hypothesized that working part-time may allow more time for home and social activities and therefore higher level of community integration
Doig, Fleming, and Tooth, 2001
10/22/2014
6
40 patients with severe TBI at average of 9 years post injury
Used CIQ, CIM, and SPRS
Same findings as Doig for predicting poor community re-entry
Authors noted that interventions that minimize challenging behavior and disability can make a significant difference in level of community integration
Winkler et al, 2006
605 subjects
Mean years since injury = 28.8
Respondents with longer time since injury were less likely to report any TBI-related problems
Authors noted importance of counseling patients and families in the acute phase that recovery can continue over the lifespan with progressive improvement
Brown et al, 2011
119 clients with severe TBI Cognitive and motor ability at discharge can
predict return to “work” FIM (Functional Independence Measure)+FAM
(Functional Assessment Measure) scores “Work” includes volunteer work and
full/part-time vocationally related education
Foy, 2014

10/22/2014
7
http://www.tbims.org/combi/FAM/famform.pdf
141 patients admitted to inpatient rehab and followed up at 1-2 yrs post injury
CIQ, CHART
For patients with mild/moderate injury, better family functioning = greater home integration; and less caregiver distress = better social integration
For patients with severe injury, greater caregiver perceived support = better outcomes in productivity and social integration
Authors concluded early interventions targeted towards decreasing caregiver distress, increasing support, and improving family functioning can positively impact later outcomes
Sady et al, 2010
136 persons with TBI with follow up at 1 month post discharge from acute rehab
CIQ, CHART
Better emotional functioning in caregivers = greater occupation and social integration outcomes within 6 months post injury
Authors suggest screening caregivers early during post acute rehabilitation to target those who need assistance to improve their support of the person with TBI
Sander et al, 2012
10/22/2014
8
8 tiered approach to deliver caregiver support Early engagement Meeting cultural needs Keeping families together Actively listening Active involvement Education Skills training Support for community re-integration
Practical Examples: Family meetings scheduled within 5 days of admission Caregivers are included in community outings
Foster et al, 2012
2 different studies: Peer Mentoring programs improve community
reintegration and increased satisfaction with social life respectively
Hanks et al showed peer mentoring significantly improved • Behavioral control • Lower alcohol use • Less emotion-focused and avoidance coping • Physical quality of life
Hanks et al, 2012 and Strutchen et al, 2011
RCT (Randomized Control Trial) with 52 TBI patients
Group treatment program for social communication skills training (90 min sessions, 1x per week, for 12 weeks)
Subjects demonstrated improved communication skills that were maintained at 6 month follow up and overall life satisfaction scores significantly improved
Dahlberg et al, 2007
10/22/2014
9
46 subjects with moderate to severe TBI 1 year or greater post injury
High level of happiness and QOL associated with high satisfaction with activities and high proportion of those activities performed with others
Increasing variety and frequency of social and leisure activities may not influence QOL
Instead, increasing opportunities to participate with others and enhancing subjective experience of activities positively influences QOL (individualized approach is essential)
McLean et al, 2014
Good psychological adjustment to TBI was related to low levels of emotional distress and small discrepancy between current and aspired functional status
Poor functional status did not significantly impact psychological adjustment in individuals with poor self-awareness
Authors offer the opinion: Rehabilitation outcomes may be improved “if brain-injured individuals are supported in their process of coming to grips with the consequences of their brain injury, not only at a functional level, but also in terms of revision of one’s self-concept and person growth.”
Schonberger et al, 2014
Unable to return
to premorbid
lifestyle
Low perceived
level of
functioning
Depressive
symptoms
Poor community
integration
Ownsworth et al, 2011
10/22/2014
10
“Occupation Enabler” according to AOTA
Allows greater participation in IADL’s, work, education and other activities
Classen et al conducted a literature review of assessment tools predicting driving performance in individuals with TBI • Strong evidence for combination of self report,
significant others’ report, and functional status
• Good evidence for Comprehensive Driving Evaluation
Liddle et al collected information from clients with TBI, family members, and health care practitioners • Rehab approaches need to provide clear,
consistent information about safe return to driving and the process for doing so Patients and family members do not know the
process and healthcare workers either don’t talk about it or explain it well enough
• Alternative transportation should be encouraged to support continued involvement in the community to reduce frustration experienced by people “on hold” from driving
A systematic review by Brasure et al on participation after multidisciplinary rehabilitation for moderate to severe traumatic brain injury showed no difference in one approach versus another.
Examples: • Increased inpatient rehab intensity (adding Sat therapy
versus therapy only on weekdays) • Intense cog rehab plus standard neuro-rehab versus
standard neuro-rehab alone
Participation as measured by productivity (return to work) and scales measuring community integration
10/22/2014
11
Comprehensive, holistic, multidisciplinary, individualized approach
Includes family/caregivers and addresses their functional and emotional needs
Addresses driving
Peer mentoring for patients and families
Communication skills practice
Opportunities to practice and/or develop interests/activities that are enjoyable and involve interaction with others
Psychological adjustment
Use of predictive tools to guide interventions
Yasui NY, Berven NL. Community Integration: Conceptualisation and Measurement. Diabil Rehabil. 2009; 31(9): 761-771.
Egbert N, Koch L, Coeling H, Ayers D. The Role of Social Support in the Family and Community Integration of Right-hemispheric Stroke Survivors. Heath Communication. 2006; 20(1): 45-55.
Salter K, Foley N, Jutai J, Bayley M, Teasell R. Assessment of Community Integration Following Traumatic Brain Injury. Brain Injury. 2008; 22(11): 820-835.
Mahar C, Fraser K. Barriers to Successful Community Reintegration Following Acquired Brain Injury (ABI). International Journal of Disability Management. 2012; 6; 49-67.
Wong Y-LI, Solomon PL. Community Integration of Persons with Psychiatric Disabilities in Supportive Independent Housing: A Conceptual Model and Methodological Considerations. Ment Health Serv Res. 2002; 4:13-28.
Willer B. Community Integration Questionnaire Form. Retrieved from http://www.rehabmeasures.org
Ritchie L, Wright-St Clair VA, Keogh J, Gray M. Community Integration After Traumatic Brain Injury: A Systematic Review of the Clinical Implications of Measurement and Service Provision for Older Adults. Arch of Phys Med Rehabil. 2014; 95(1): 163-175.
Mahar C , Fraser K. Strategies to Facilitate Successful Community Reintegration Following Acquired Brain Injury (ABI). International Journal of Disability Management. 2012; 6: 68-78.
Doig E, Fleming J, Tooth L. Patterns of Community Integration 2-5 Years Post-discharge from Brain Injury Rehabilitation. Brain Inj. 2001; 15(9): 747-762.
Winkler D, Unsworth C, Sloan S. Factors that Lead to Successful Community Integration Following Severe Traumatic Brain Injury. J Head Trauma Rehabil. 2006; 21(1): 8-21.
10/22/2014
12
Brown AW, Moessner AM, Mandrekar J, Diehl NN, Leibson CL, Malec JF. A Survey of Very-Long- Term Outcomes after Traumatic Brain Injury among Members of a Population-Based Incident Cohort. Journal of Neurotrauma. 2011; 28:167-176.
Foy, Catherine M. Long Term Efficacy of an Integrated Neurological and Vocational Rehabilitation Programme for Young Adults with Acquired Brain Injury. Journal of Occupational Rehabilitation. 2014; 24(3): 533-542.
Sady MD, Sander AM, Clark AN, Sherer M, Nakase-Richardson R, Malec JF. Relationship of Preinjury Caregiver and Family Functioning to Community Integration in Adults with Traumatic Brain Injury. Arch of Phys Med Rehabil. 2010; 91(10): 1542-1551.
Sander AM, Maestas KL, Sherer M, Malec JF, Nakese-Richardson R. Relationship of Caregiver and Family Functioning to Participation Outcomes After Postacute Rehabilitation for Traumatic Brain Injury: A Multicenter Investigation. Arch of Phys Med Rehabil. 2012; 93(5): 842-849.
Foster AM, Armstrong J, Buckley A, et al. Encouraging Family Engagement in the Rehabilitation Process: A Rehabilitation Provider’s Development of Support Strategies for Family members of People with Traumatic Brain Injury. Disability & Rehabilitation. 2012; 34(22): 1855-1862.
Hanks RA, Rapport LJ, Wertheimer J, Koviak C. Randomized Controlled Trial of Peer Mentoring for Individuals with Traumatic Brain Injury and Their Significant Others. Archives of Phys Med Rehabil. 2012; 93(8): 1297-1304.
Struchen MA, Davis LC, Bogaards JA, et al. Making Connections After Brain Injury: Development and Evaluation of a Social Peer-mentoring Program for Persons with Traumatic Brain Injury. Journal of Head Trauma Rehabilitation. 2011; 26(1): 4-19.
Dahlber CA, Cusick CP, Hawley LA, et al. Treatment Efficacy of Social Communication Skills Training After Traumatic Brain Injury: A Randomized Treatment and Deferred Treatment Controlled Trial. Arch of Phys Med Rehabil. 2007; 88(12): 1561-1573.
McLean AM, Jarus T, Hubley AM, Jongbloed L. Associations Between Social Participation and Subjective Quality of Life for Adults With Moderate to Severe Traumatic Brain Injury. Disabil Rehabil. 2014; 36(17): 1409 -1418.
Schonberger M, Ponsford J, McKay A, et al. Development and Predictors of Psychological Adjustment During the Course of Community-based Rehabilitation of Traumatic Brain Injury: A Preliminary Study. Neuropsychol Rehabil. 2014; 24(2): 202-219.
Ownsworth T, Fleming J, Haines T, et al. Development of Depressive Symptoms During Early Community Reintegration After Traumatic Brain Injury. J Int Neuropsychol Soc. 2011; 17(1): 112-119.
Classen S, Levy C, McCarthy D, Mann WC, Lanford D, Waid-Ebbs JK. Traumatic Brain Injury and Driving Assesment: An Evidence-Based Literature Review. The American Journal of Occupational Therapy. 2009; 63(5): 580-591.
Liddle J, Fleming J, McKenna K, Turpin M, Whitelaw P, Allen S. Driving and Driving Cessation After Traumatic Brain Injury: Processes and Key Times of Need. Disabil Rehabil. 2011; 33(25-26): 2574-2586.
Brasure M, Lamberty GJ, Sayer NA, et al. Participation After Multidisciplinary Rehabilitation for Moderate to Severe Traumatic Brain Injury in Adults: A Systematic Review. Arch of Phys Med Rehabil. 2013; 94(7): 1398-1421.