Embed Size (px)
Citation preview

CBPRA-00500; No of Pages 13: 4C
Available online at www.sciencedirect.com
ScienceDirectCognitive and Behavioral Practice xx (2014) xxx-xxx
www.elsevier.com/locate/cabp
Evidence-Based Assessment Meets Evidence-Based Treatment: An Approachto Science-Informed Case Conceptualization
Lillian M. Christon, University of North Carolina–Chapel HillBryce D. McLeod, Virginia Commonwealth University
Amanda Jensen-Doss, University of Miami
Keywobased
1077© 20Publ
PleCas
Though case conceptualization is considered to be a component of evidence-based practice, the case conceptualization process is notalways guided by scientific findings. Case conceptualization is a collaborative process of generating hypotheses about causes,antecedents, and maintaining influences for an individual client’s problems within a biopsychosocial context. We argue that adoptinga scientific approach to case conceptualization informed by research findings and evidence-based assessment tools can help informclinical decision-making from intake to treatment termination. Our approach to case conceptualization involves 5 stages. In the firststages, a clinician synthesizes and integrates research evidence from various literatures to identify presenting problems and casual andmaintaining factors (Stage 1), to classify diagnoses (Stage 2), to inform the development of hypotheses about variables contributing to aclient’s problems (Stage 3), and to select a treatment approach and plan (Stage 4). In the final stage, the clinician takes a scientificapproach to developing individualized assessment methods that can be used to test and revise hypotheses through the treatment processand to measure outcomes (Stage 5). A case example illustrating practical use of these steps is presented.
W Eare currently in an era of evidence-based practice(EBP) that places an emphasis on using scientific
findings to inform clinical practice. To increase thequality of mental health care, federal agencies fundingtreatment research (e.g., National Institute of MentalHealth [NIMH], 2008), state mental health agencies(e.g., Jensen-Doss, Hawley, Lopez, & Osterberg, 2009), andprofessional organizations (e.g., American PsychologicalAssociation [APA] Presidential Task Force on Evidence--Based Practice, 2006) have all endorsed the use of EBP incommunity settings. Generally, EBP encompasses bothevidence-based assessment (EBA; Hunsley & Mash, 2007)and evidence-based treatment (EBT) practices (APA,2006).
Despite the push to incorporate EBP into clinicalpractice, these efforts have faced practical barriers. Theliterature is voluminous and it can be challenging to applyresearch findings to specific clients. Further, there is ahistory of controversy over the extent to which researchstudies apply to clients seen in practice settings, as these
rds: case conceptualization; evidence-based assessment; evidence--practice; clinical decision-making; evidence-based treatment
-7229/13/xxx-xxx$1.00/013 Association for Behavioral and Cognitive Therapies.ished by Elsevier Ltd. All rights reserved.
ase cite this article as: Christon et al., Evidence-Based Assessment Mee Conceptualization, Cognitive and Behavioral Practice (2014), http://d
clients may not match the characteristics of participants inresearch studies (Gonzales, Ringeisen, & Chambers, 2002;Persons & Silberschatz, 1998). Given these challenges, it isnot surprising that clinicians have mixed attitudes towardsusing EBP to inform clinical practice (Nelson, Steele, &Mize, 2006). Another factor that may contribute toclinician ambivalence is that they may regard EBP assimply using manual-guided EBTs (e.g., Addis & Krasnow,2000). However, EBP involves a great deal more thanapplying treatment manuals. At its core, EBP integratesthe best available research, clinician expertise, and clientcharacteristics and preferences (APA, 2006; www.ebbp.org) to inform clinical decision-making. However, themove toward EBP raises an important question: How canclinicians reasonably integrate research into their clinicalpractice?
In this paper, we present an approach to caseconceptualization that uses scientific findings to guideclinical decision-making. Case conceptualization is de-fined as developing a complete picture of a client bycollecting data that are used to generate hypotheses aboutthe causes, antecedents, and maintaining influences foran individual client’s problems within a biopsychosocialcontext (e.g., McLeod, Jensen-Doss, & Ollendick, 2013a;Nezu, Nezu, Peacock, & Girdwood, 2004). The ability todevelop a case conceptualization informed by scientificfindings is a critical therapeutic skill required for EBP(APA, 2006).
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

2 Christon et al.
Case conceptualization originated with the medicaldiagnostic approach of Hippocrates and Galen, whereindiagnoses were based on theory and guided by assessment(McLeod et al., 2013a; McLeod, Jensen-Doss, & Ollendick,2013b). Approaches to case conceptualization in psychol-ogy have traditionally relied on etiological theories (e.g.,psychoanalytic, behavioral) to guide conceptualization andtreatment (McLeod et al., 2013a). Our case conceptualiza-tion approach differs in an important way. Instead ofadhering to a particular therapy model, we emphasize theimportance of (a) incorporating EBA strategies to thor-oughly assess factors contributing to and maintaining eachpresenting problem and to measure outcomes over time;(b) using the theoretical and empirical literature to informassessment; and (c) accessing the empirical literature toguide treatment selection.
The case conceptualization model presented herein isintended to help guide the treatment process from intaketo termination using a hypothesis-testing approachinformed by EBA (Hunsley & Mash, 2007). In thispaper, the core tenets of EBA are reviewed andadvantages of science-informed case conceptualizationare discussed. We present clinical guidelines for thisapproach and, to illustrate its practical use at each stage, aclinical case example.
EBA: The Foundation of Science-InformedCase Conceptualization
Case conceptualization is the backbone of therapy,providing structure at every point of the treatmentprocess; EBA fortifies and supports this backbone.Hunsley and Mash (2007, p. 30) define EBA as “anapproach to clinical evaluation that uses research andtheory to guide the selection of constructs to be assessedfor a specific assessment purpose, the methods andmeasures to be used in the assessment, and the mannerin which the assessment process unfolds.” EBA methodsand measures are used to collect, organize, and integratedata on presenting problems and factors that cause ormaintain symptoms (McLeod et al., 2013b) and to testhypotheses about these relationships.
In an EBA framework, various assessment measuresand methods are needed to inform a case conceptualiza-tion. Assessment focuses on (a) symptoms and function-ing, (b) mediators— factors accounting for change in thepresenting problem (e.g., cognitions), (c) moderators —factors that might influence the course of treatment(e.g., developmental delays), and (d) therapy processfactors — client and/or clinician factors that mightinfluence treatment delivery (McLeod et al., 2013b).Within each category, research evidence and theoryshould be used to identify what to target and how toassess those targets. A core tenet of EBA is that measuresand methods should be selected based on their
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
reliability, validity, and clinical utility for a given clientand assessment purpose (Hunsley & Mash, 2007). Toinform the treatment process, this often requires the useof measures pulled from nomothetic and idiographicassessment traditions.
Nomothetic strategies are associated with diagnostic assess-ment and involve comparing an individual client to otherindividuals by using data from assessment instrumentsadministered in a standardized fashion (Haynes, Mumma,& Pinson, 2009; McLeod et al., 2013b). Nomothetic tools(e.g., rating scales, interviews, structured observations)provide global information about how a client’s symptomsand behavior compare to the larger population, or thedegree of fit of a client’s problems with diagnostic criteria(Haynes & O’Brien, 2000). Data from nomotheticmeasures are often used for screening, assessing symptoms,and determining prognosis.
In contrast, idiographic strategies involve tailoringassessment tools to the individual client and comparingthe client to him-/herself (Haynes & O’Brien, 2000).These strategies allow the clinician to identify howvariables are uniquely patterned within an individual(Ollendick, McLeod, & Jensen-Doss, 2013). Idiographictools (e.g., functional analysis, direct observation, self--monitoring) are particularly useful for assessing theinfluence of context on behavior, judging change intarget behaviors, and providing specific informationneeded to form and test hypotheses. Data generatedfrom idiographic tools can help clinicians translateinformation from the empirical literature for use withindividual clients (Haynes et al., 2009).
In sum, developing hypotheses and then testing themare critical components of a scientific approach to caseconceptualization, and it is important to use EBAmethods to achieve these goals. For further informationabout using EBA to inform case conceptualization, seeMcLeod et al. (2013a, 2013b) and Jensen-Doss, Ollendick,and McLeod (2013).
Why Should Scientific Findings InformCase Conceptualizations?
A case conceptualization informed by scientific findingscan help clinicians achieve the goals of EBP by helping totranslate research findings into clinical practice for individ-ual clients. Early in treatment, diagnostic informationprovides access to the psychopathology literature that canhelp guide assessment (e.g., identify potential risk factors fora given disorder) and treatment planning (e.g., identifypotential EBTs). However, a clinician must then determinehow to apply information from the empirical literature foruse with a particular client. Two clients with the samediagnosis can have distinct symptom profiles that are causedand maintained by different factors. Using EBA, a cliniciancan build a case conceptualization that takes information
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

3Science-Informed Case Conceptualization
from the literature (e.g., about the different potential causalfactors for a particular disorder) to ultimately identify theunique factors at play for a particular client. In this way,information from the literature can be translated for aparticular case via a case conceptualization.
A science-informed case conceptualization also promotesbetter decision-making (Jensen-Doss, McLeod, &Ollendick,2013). Clinical judgment and expertise are importantcomponents of clinical practice (APA, 2006). However,clinical judgment and decision-making can be impactedby individual biases, attitudes, experiences, and training(Croskerry, 2009; Dawes, Faust, & Meehl, 1989). To helpguard against these potential biases, it is important forclinicians to receive feedback about the impact of theirclinical decisions (Lambert,Whipple, Hawkins, Vermeersch,Nielsen, & Smart, 2003). A scientific approach to caseconceptualization involves collecting and analyzing datathroughout treatment in order to test hypotheses abouta given client. This creates a feedback loop that can helpguard against errors in clinical judgment.
Table 1Guidelines to Science-Informed Case Conceptualization
Stage Potential E
Stage 1: Identify and quantify presenting problems,causal/maintaining factors, and historical factors.
• Adm• Adm• Adm• Use
Attamea
Stage 2: Assign diagnoses. • Rev• Con
sis
Stage 3: Develop initial case conceptualization. • Deviden
• Com(e.g
Stage 4: Proceed with treatment plan and selection. • Conof tr
• Conet a
Stage 5: Monitor and evaluate treatment outcomes andrevise case conceptualization as necessary.
• Admmea
• Con• Ask• Eng• Use• Inte• At
stanstat
Note: This aims to be a comprehensive list; not every method listed will be
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
Practical Guidelines to Science-InformedCase Conceptualization
In this section, we present a model for science-informed case conceptualization. Our approach is appli-cable to most ages, settings, and diagnostic profiles.Though informed by empirical findings, the approach isatheoretical and does not focus on specific applications ofa particular theoretical approach to treatment. Theprocess itself has not been empirically validated. Rather,the term “science-informed” places emphasis on integrat-ing scientific findings. That being said, a solid under-standing of behavioral theory and single-case seriesdesigns provides the foundation for competently imple-menting these steps (McLeod et al., 2013a).
Our case conceptualization approach progressesthrough five stages designed to unfold over the courseof treatment (Table 1). Throughout this process, thepsychopathology, assessment, and treatment literaturesare consulted, and ongoing use of EBA informs the case
BA methods
inister broad symptom rating scalesinister specific symptom rating scalesinister standardized clinical interviewsidiographic tools to identify presenting problems (e.g., Goalinment Scaling, Kiresuk & Sherman, 1968; Top Problemssure, Weisz et al., 2011)
iew results of rating scales and standardized clinical interviewssider following the evidence-based medicine approach to diagno-(Youngstrom et al., this issue)
elop specific hypotheses about connections between variablestified in Stage 1plete figural drawings of relationships between variables., Figures 2 and 3)
sult treatment outcome studies and online searchable databaseseatmentssider using Probability of Treatment Benefit charting (Lindheiml., 2012)
inister specific symptom rating scales designed for repeatedsurementduct mood check-ups in sessionclient to engage in self-monitoringage in behavioral observationsTop Problems measure for tracking outcomesgrate data using clinical dashboards or graphingtermination, re-administer broad symptom rating scales anddardized clinical interviews to confirm progress and diagnosticus
used within a single case.
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

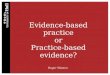
Note. Case conceptualization is a data-driven cyclical process that forms a feedback loop over
the course of treatment. EBA plays a role in generating the initial case conceptualization, which
then informs selection of EBTs. After treatment begins, EBA helps to assess the accuracy of the
case conceptualization as well as evaluate outcomes.
Figure 1. Science-Informed Case Conceptualization.
4 Christon et al.
conceptualization, which then informs selection of EBTs(Figure 1). After treatment begins, EBA is used to test theaccuracy of the case conceptualization and monitortreatment outcomes. This process involves identifyingpresenting problems and their causal/maintaining fac-tors as well as setting treatment goals (Stage 1), generatingdiagnoses (Stage 2), producing initial hypotheses aboutinfluences on a client’s problems (Stage 3), and selecting atreatment (Stage 4). Data are then collected to test andrevise the hypotheses (Stage 5). We describe each stage inmore detail below and illustrate it with a case example. Ourfocus is on using assessment data, so we do not describethe assessment process. Rather, we reference scores onmeasures collected as part of a sample battery designed tobe feasible in an outpatient clinical setting.
Case Example
Erika Phillips was a 13-year-old female who presentedfor an initial outpatient intake evaluation in an urbancommunity mental health clinic. Erika and her parentssought services for treatment of Erika’s panic attacksand agoraphobia, which began 3 months prior to theNovember intake session. Erika lived with her biologicalparents and a 7-year-old brother, in a single-family homeadjacent to a low-income housing development in a largecity. Mr. Phillips worked as an electrician and Mrs. Phillipswas a stay-at-homemother. Amonth before the intake, Erikahad switched from a public school to home schoolingdue to Erika’s panic attacks and refusal to attend school.Mrs. Phillips felt home schooling was necessary to ensurethat Erika did not get further behind in her academics.
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
Stage 1: Identify and Quantify Presenting Problems,Causal/Maintaining Factors, and Historical Factors
The goals of this stage are to identify the presentingproblem(s), list the presenting problems in terms oftreatment priority, and to begin the process of collectinginformation on the factors that serve to cause or maintainthose presenting problems. A main focus is to operatio-nalize presenting problems. To the extent possible, thepresenting problems should be described in concrete,observable, and measurable terms (Persons, Davidson,Tompkins, 2001). It is helpful to define the topography ofpresenting problems (frequency, intensity, and duration)across various responsemodes (cognitions, affect, behavior).Doing so produces a detailed description of the presentingproblems that makes it easier to assess the problemsthroughout treatment and determine whether treatment isworking. Once the presenting problems are identified anddefined, they should be ranked in order of treatmentpriority. Adopting a collaborative approach with the client tocomplete the ranking can help strengthen the alliance andensure client preferences are accounted for in treatmentplanning. Severity and/or level of impairment caused bypresenting problems and client preference should be takeninto account when ranking them.
EBA strategies that can be used to help identifypresenting problems include rating scales and standardizedinterviews. Broad assessmentmeasures that cover a range ofsymptoms may be used initially, followed by rating scalesthat include more in-depth assessment of symptomsendorsed on the broad measures. Relevant modules ofstandardized interviews can then be administered to
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

5Science-Informed Case Conceptualization
further flesh out presenting problems (Youngstrom, 2012)and provide important diagnostic information for Stage 2.Idiographic tools can help structure the process of identify-ing and ranking presenting problems. For instance, GoalAttainment Scaling (Kiresuk & Sherman, 1968), in whichclient goals for therapy are listed and progress towards thesegoals is assessed, or the Top Problems measure (Weisz et al.,2011), which identifies the problems that brought the clientinto treatment and assigns a severity rating to each problem,can facilitate this process. An added benefit of idiographicmeasures is that they produce information that can be usedto monitor treatment outcomes (see Stage 5).
After the presenting problems are defined, data to helpbuild the case conceptualization are gathered, including:(a) contextual information about when andwhere a presentingproblem occurs; (b) historical factors that predispose a clientto exhibit a presenting problem via specific causal factors;(c) causal factors that immediately precede and influencethe presenting problem (antecedents); and (d) maintainingfactors that maintain the occurrence of the presentingproblem via conditioning or operant mechanisms (conse-quences). Causal factors are proximal influences thatimmediately precede the presenting problems and canbe addressed in treatment. Historical factors are distalinfluences that contribute to the development of causalinfluences, but cannot be targeted in treatment. Thehistorical factors provide a lens throughwhich to understandcausal factors. For instance, knowing that a client presentingwith anxiety also has a history of early behavioral inhibition(historical factor) can help a clinician to assess for causalfactors linked to behavioral inhibition, such as physiologicaloverarousal or avoidance of social interactions (Fox,Henderson, Marshall, Nichols, & Ghera, 2005). Also, asdiscussed later, each category is not discrete, and it ispossible for a factor to be both a presenting problem anda causal or maintaining factor (see Stage 3). Lastly, acomprehensive case conceptualization also includes assess-ment of a client’s strengths (Persons et al., 2001) andquality of life (Youngstrom, 2012).
Information about historical, causal, and maintainingvariables can be gathered by asking clients about areassuch as developmental history, medical history, history oftrauma or abuse, family psychiatric history, physical orsomatic symptoms, coping skills, cognitive processessurrounding presenting problems, and family factors,such as marital satisfaction or parenting strategies.Nomothetic and ideographic assessment tools such assemistructured or structured clinical interviews, behav-ioral or symptom rating scales (e.g., the Anxiety SensitivityIndex-3, a measure of physical, cognitive, and socialconcerns associated with anxiety; Taylor et al., 2007),behavioral observation, or structured measures forobtaining clinical history (e.g., the Structured Develop-mental History form of the Behavior Assessment System
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
for Children, Second Edition, BASC-2; Reynolds &Kamphaus, 2004) can help to define these variables.
Stage 1: Erika’s CaseUsing an idiographic approach, Erika and her parents
were asked to identify the Top Problems (Weisz et al.,2011) that brought her into treatment and to provideseverity ratings for each problem. They were in agree-ment that the problems were, in order of importance/severity: (1) panic attacks; (2) fear of leaving her house;and (3) feelings of sadness.
For Erika, the Self-Report of Personality and the ParentRatingScales of theBASC-2 (Reynolds&Kamphaus, 2004), abroad nomothetic behavior rating scale, yielded clinicallysignificant scores on the Internalizing Problems Scale andthe Anxiety and Depression Subscale. Further, Erikaendorsed a number of critical items on the BASC-2 (e.g.,“Sometimes I want to hurt myself”). Given these findings, itwas determined that data from a specific symptom ratingscale would be useful. Erika’s scores on the Revised Anxietyand Depression Scale (RCADS; Chorpita, Yim, Moffitt,Umemoto, & Francis, 2000), a nomothetic symptom ratingscale, were in the clinical range on the Panic Disorder andDepression subscales and on the Total Anxiety and TotalAnxiety and Depression scales. Mrs. Phillips’ scores on theRCADS-P were in the clinical range on the Panic Disorderand Depression subscales and the Total Anxiety scale.
Data on the presenting problems and history wasgatheredwith relevantmodules of theK-SADS-PL (Kaufman,Birmaher, Brent, Rao, & Ryan, 1996), a semistructuredclinical interview, and supplemented by an unstructuredclinical interview. Erika experienced her first panic attackwhen she was 10 years old. Between ages 10 and 13, shehad roughly one to two panic attacks per year (presentingproblem). Her parents also reported that as a young child,Erika had a withdrawn temperament and she exhibitedbehavioral inhibition, or a reticence to approach novelstimuli and situations (historical factor); they noted thatshe became more open to new experiences as she gotolder. However, the summer prior to 9th grade, thefrequency of Erika’s panic attacks increased to at leastone per day on days she had to leave the house (contextualinformation), and on an almost nightly basis. Erikareported a pervasive concern about having a panic attackin situations where she could not easily escape andendorsed being fearful that something awful mighthappen to her, that nobody would help her, that shemight be going crazy, and that she was going to die (causalfactors). Erika was very sensitive to physiological sensa-tions and often noticed her heart beating faster, whichmade her worry about having a panic attack (causalfactor). At intake, returning to school was not a priorityfor Erika or her parents. However, her parents did wantErika to go other places, as she rarely left the house, had
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

6 Christon et al.
stopped hanging out with friends, and was hesitant to goanywhere. Erika said she did not want to leave the housebecause she was worried that she would have a panic attack(maintaining factor), and believed that she was “safe” fromthese symptoms while at home (maintaining factor).
Erika also endorsed depressive symptoms that hadbeen present to some degree for the past three months(presenting problem). In the two weeks prior to the intake,she reportedly experienced depressed mood for at least afew hours each day, decreased interest in her usualactivities most of each day, and difficulty sleeping andconcentrating, feeling restless, decreased appetite, andfeelings of guilt. She reported intentionally hurtingherself (i.e., cutting her upper arm with a razorblade)without any intent to die (presenting problem and maintain-ing factor) a few times over the past three months. Theseself-injurious behaviors reportedly waxed and waned andher urges to harm herself did not last for longer than aday at a time. A thorough risk assessment was conducted,and Erika said she engaged in nonsuicidal self-injury(NSSI) to relieve distress and reduce anxiety. She deniedhaving thoughts about wanting to die or about killingherself currently or in the past.
The initial assessment did not reveal any evidence ofsubstance use, trauma, or any other psychiatric symptoms.Erika did not have any notable medical history and herprenatal, birth, and developmental histories were normal.Her family history was positive for depression in herpaternal grandfather and unspecified anxiety and panicattacks in her maternal aunt. Erika received As and Bsthroughout middle school and appeared to enjoy school.However, her grades declined to Cs andDs in the fall of herfreshman year when her attendance declined.
Stage 2: Assign Diagnoses
In this stage, the clinician uses data collected about thepresenting problems to determine if the client meetsdiagnostic criteria for one or more diagnoses. Diagnosesare useful for a number of reasons. First, diagnosesprovide access to the assessment literature, which canhelp to identify assessment targets and tools. Second,diagnoses provide access to the psychopathology litera-ture, which can help generate the hypotheses in the caseconceptualization (Nezu et al., 2004; Persons et al., 2001).For instance, if a client is diagnosed with panic disorder, aclinician might use Bouton, Mineka, and Barlow’s (2001)modern learning theory to generate hypotheses abouthow conditioned anxiety elicited by interoceptive cues(e.g., racing heart) may precipitate panic reactions,furthering the panic cycle. Third, diagnoses provideaccess the treatment literature, as most EBTs aredeveloped for specific diagnoses. Finally, diagnoses are adimension on which to assess treatment outcomes.
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
Although a number of individuals presenting fortreatment have subclinical problems (e.g., Westen, Novotny,Thompson-Brenner, 2004), data suggest that these individ-uals often have impairments similar to others who exceedclinical cutoffs (e.g., Angold, Costello, Farmer, Burns, &Erkanli, 1999). For individuals who do not meet diagnosticcriteria, a case conceptualization should be developedwithout a diagnosis. Individuals with clinical and subclinicalsymptoms will likely respond to the same kinds of treatment,andmany treatment outcome studies have inclusion criteriaof either specific diagnoses or clinically elevated problemlevels (e.g., see Weisz et al., 2012). As such, it is importantto document subclinical symptoms, both because they canbe the focus of treatment and can be used to access theliterature.
Several EBA strategies can be used to supportdiagnosis, including standardized symptom-rating scalesand/or standardized diagnostic interviews. Youngstrom,Choukas-Bradley, Calhoun, and Jensen-Doss (this issue)provide detailed discussions of an evidence-based medi-cine approach to diagnosis, relying on estimatingprobabilities of diagnoses from risk factors and test resultsusing a Bayesian approach. Other methods for combiningdiagnostic assessment data are discussed in Jensen-Doss,McLeod, et al. (2013).
Stage 2: Erika’s CaseBased on information gathered in Stages 1 and 2, it was
determined that Erika met DSM-5 criteria (AmericanPsychiatric Association, 2013) for panic disorder, agorapho-bia, and major depressive disorder (MDD), single episode.
Stage 3: Develop Initial Case Conceptualization
In Stage 3, the clinician develops working hypothesesabout factors that contribute to and maintain a client’sproblems (Persons et al., 2001); these hypotheses aremodified in later stages as indicated by assessment data.The case conceptualization is a comprehensive picture,roadmap, or story of how the client’s presenting problemsare formed and maintained. Each presenting problemidentified in Stage 1 is viewed as a dependent variable thatthe clinician will attempt to change during treatment.Each of the proximal causal or maintaining factorsidentified in Stage 1 become the variables that will betargeted with specific therapeutic interventions. The coreof the conceptualization is the hypotheses about relation-ships between these variables. Each hypothesis should begrounded in the literature, testable, and based onassessment data. It can be valuable to write out and mapthe variables and their relationships using figural draw-ings. Different ways exist to generate a diagram (e.g., theCognitive Conceptualization Diagram; Beck, 2011). Werecommend mapping out presenting problems first(with the top problem in the top row; e.g., Figure 2).
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

Figure 2. Figural Drawing of Erika’s Initial Case Conceptualization ([1]-[10]).
7Science-Informed Case Conceptualization
Then, identify and place the causal and maintaining factorsin corresponding columns, and finally, place historicalfactors in a column preceding causal factors. This approachrepresents a flexible variation of the case conceptualizationdiagram; firm lines are not drawn between each column,allowing some factors to fall under multiple categories. Forinstance, in Erika’s case (Figure 2), avoidance [6] is both apresenting problem as well as a maintaining factor for herpanic attacks, and is thus placed between these two columns.This initial map is a foundation, and is revised throughouttreatment.
It is important to share the conceptualization with theclient (and in the case of a child client, the child’s family).Sharing the conceptualization and soliciting feedbackserves two purposes. First, it helps ensure that the clientand clinician have a shared understanding of the client’sproblems. Second, it allows the client to give correctivefeedback and share relevant information. Open dialogueallows for the client and clinician to enter the treatment-planning phase with a collaborative mindset. Throughoutthis process, the formation of a genuine, empathic, andcollaborative therapeutic relationship that is respectful tothe client’s individuality, autonomy, and culture is essential,as is remaining attentive to therapeutic engagement.
Stage 3: Erika’s Case ConceptualizationErika had a history of panic attacks and behavioral
inhibition (historical factors; [1] in Figure 2). Behavioral
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
inhibition was described in her early temperament, so is ahistorical factor rather than a causal/maintaining factor.Erika reported significant sensitivity to physiologicalsymptoms (internal stimuli) — when she noticedsensations she believed were abnormal (e.g., racingheart), she became anxious about having a panic attack(causal factors; [2] and [3]). This resulted in greaterawareness of her physiological state and increased hersymptoms of anxiety ([4]), often resulting in a panicattack (presenting problem; [5]). By avoiding situations inwhich Erika believed she was likely to experience thephysiological sensations (both a maintaining factor for herpanic attacks, and a presenting problem nominated by Erikaand her parents; [6]), she reduced opportunities toexperience disconfirming events (e.g., not having apanic attack) and reduced the frequency of her experi-ence of physiological symptoms (maintaining factor; [8]).Erika’s negative cognitions about her anxiety and herinability to cope maintained her anxiety (maintainingfactor; [9]). Erika’s parents unintentionally also main-tained her anxiety by allowing her to avoid or leave fearedplaces while her anxiety was at a heightened level(maintaining factor; [6]; negative reinforcement). Thisavoidance reduced her anxiety in the short term(maintaining factor; [8]), but led Erika to develop thebelief that avoidance reduced the likelihood of anegative outcome (maintaining factor; [9]). Erika alsorelied on her parents as safety objects, a further form of
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

8 Christon et al.
avoidance (maintaining factor, [6]), reinforcing her beliefthat she could not manage her anxiety independently.Erika’s depressive symptoms were secondary to heranxiety. Her depressed mood resulted from her agora-phobia and self-limiting of pleasurable activities (present-ing problem; [7]). Finally, her NSSI reflected poor copingskills and was a means of escape from distress caused byher persistent physiological arousal and depression(presenting problem; [10]). This conceptualization wasshared with Erika and her parents, who were inagreement.
Stage 4: Proceed With Treatment Plan and Selection
In Stage 4, the clinician works to identify treatmentgoals and the treatment approach. First, for eachpresenting problem that the client and therapist agreeshould be a treatment priority, a corresponding treatmentgoal should be identified. These goals are the desiredoutcome for each presenting problem (or dependentvariable) and should be outlined in specific, concrete goalstatements (e.g., “Jake will have fewer depressive symp-toms”; Persons et al., 2001). Second, treatment goalsshould be ordered in terms of priority, yielding atreatment plan. Interventions should then target therelationships between the causal, maintaining, anddependent variables in the case conceptualization, withthe aim of leading to the desired changes clearly outlinedas treatment goals. In general, each variable should betargeted with a specific intervention. For instance,depressive cognitions maintaining a client’s major de-pressive disorder could be targeted with cognitivestrategies.
It is helpful to use a cost-benefit analysis to develop thetreatment plan (Nezu et al., 2004). With this approach,the clinician must consider what the likelihood is thattargeting a particular causal or maintaining factor willactually yield meaningful changes in presenting problems(e.g., some marital partners may not be able to fullyengage in couples work, even if relationship factors seem tobe maintaining the client’s problems) and what potentialcosts there are for particular approaches (e.g., insisting oninvolving parents in treatment when an adolescent does notwant their involvement could lead to a rupture in thealliance; McLeod et al., 2013a). The clinician must alsoreflect on the feasibility of a particular interventionapproach (e.g., time, cost, client skills, and clinicianexpertise; Nezu et al., 2004).
After treatment planning, the clinician must select atreatment approach. There are a number of factors toconsider in this decision. It is beneficial to consultthe treatment literature to guide treatment selection.There may be multiple EBTs for a particular disorder(e.g., interpersonal therapy and cognitive-behavioral
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
therapy for depression; David-Ferdon & Kaslow, 2008) oran EBTmay not exist for a particular disorder (e.g., variouspersonality disorders). In other words, a perfect fit maynot exist. The clinician must therefore use the caseconceptualization to make decisions about how to applythe literature to a particular client (e.g., by picking an EBTthat focuses on the causal mechanisms that seem mostrelevant to that client).
Many clients present with comorbid conditions, andclinicians must make decisions about how to apply theliterature to those cases. We encourage clinicians toengage in collaborative decision-making with theclient around (a) the order in which presenting problems(i.e., those that require a treatment focus) are to beaddressed, and (b) the specific goals for each problem. Itis possible that there are problem areas identified thatmay not have corresponding treatment goals, forinstance, if the problem area is not nominated by thepatient as a priority for treatment. Clinicians may alsodevelop “back-up” treatment goals, for problems that areclinician-identified but are not currently direct clientconcerns. In the case of comorbid conditions, we recom-mend that treatment ensue for the primary presentingproblem first. It is impractical to address all of the potentialproblem areas at once, and the empirical literatureencourages a more focused approach. For instance, Craskeand colleagues (2007) have found that focused CBT forpanic disorder in the presence of comorbid disordersyielded more beneficial outcomes than CBT for panicdisorder with “straying” to CBT for comorbid disorders. If acomorbid presenting problem becomes urgent or interfer-ing during treatment for theprimary problem(e.g., suicidalideation), or does not ameliorate during treatment for theprimary problem, treating these comorbid problems maythen become the treatment focus.
Treatment outcome studies provide information onthe average benefit clients with particular diagnoses andcharacteristics may expect to receive from an interven-tion; however, not all participants have the samelikelihood of that benefit. EBA strategies may providesupplementary information to clinicians about whether aclient may benefit from a treatment. For instance, onepromising approach to generating an individualizedlikelihood that a client will benefit from a particulartherapy approach is Probability of Treatment Benefit(PTB) charting (Lindheim, Kolko, & Cheng, 2012). ThePTB method must first be applied to clinical trial data(efficacy or effectiveness trials) before individual clini-cians can use this tool to make idiographic predictionsabout their patients. This is an interesting direction ofresearch that can presently be applied to a few problems,and in the future, may yield useful tools for clinicians intreatment selection, although it may not be feasible for allproblems.
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

9Science-Informed Case Conceptualization
Online, searchable databases may also help clinicians inthe treatment selection process. Some of these databasesare available for purchase (e.g., PracticeWise Evidence--Based Services Database [PWEBS], PracticeWise, LLC,2004–2013a; www.practicewise.com), while others areavailable free of charge (e.g., Cochrane Database ofSystematic Reviews, 2013; www.effectivechildtherapy.com;www.psychologicaltreatments.org). Of note, the PWEBS(2004–2013) database allows clinicians to tailor results tomatch an individual child client’s characteristics. Publishedhandbooks may also be useful to clinicians for identifyingEBTs for clients with particular disorders (e.g., Barlow,2007; Sturmey & Hersen, 2012).
Clinicians also have to make decisions about how tosequence various treatment components and what theintensity of treatment should be (McLeod et al., 2013a).Efforts have been made to simplify treatment decision--making for clinicians working with child and adults.Distillation of practice elements has helped to identifyelements of EBTs (e.g., Chorpita, Daleiden, & Weisz,2005). Modular treatments based on these elements(which have different modules addressing particularcausal and maintaining factors) may be especially usefulfor clients with comorbid disorders, as different treatmentmodules may be delivered based on the specific caseconceptualization (Weisz et al., 2012). Transdiagnostictreatments, like the Unified Protocol for TransdiagnosticTreatment of Emotional Disorders, a cognitive-behavioraltherapy (CBT) program developed to be applicable to arange of adult emotional disorders (Barlow et al., 2011),can also be used with clients with many different types ofdifficulties.
Stage 4: Erika’s CaseThe primary goals that Erika, her parents, and the
clinician agreed to target in treatment corresponded toher Top Problems: (a) reduce panic attacks; (b) increaseamount of time spent out of the house); and (c) reducedepressive symptoms. Erika and her parents preferred tokeep her home-schooled for the time being; to respecttheir wishes in this area, it was decided that return-to-school would not be an immediate treatment goal.As their main goals were related to panic and agorapho-bia, it was mutually decided that the primary treatmentapproach would address these symptoms; her depressivesymptoms would be addressed if they interfered with, or ifthey remained following, the primary treatment.
Given these treatment goals, the clinician consultedthe treatment literature for panic disorder and depres-sion. In general, CBT has been evaluated to be a “wellestablished” treatment for both anxiety and depression inyouth (Chorpita et al., 2011). A review of the literaturerevealed that Panic Control Treatment for Adolescentswas a good treatment option (PCT-A; Pincus, Ehrenreich,
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
& Mattis, 2008). PCT-A aims to alter misinterpretationalaspects of panic ([2], [3], and [9] in Figure 2), reduce thephysiological (hyperventilatory) response ([4] and [5]),and conditioned reactions to hyperventilation ([8]), anddecreasing avoidance/escape ([6]) through interoceptiveexposures. While PCT was the focused treatment ap-proach, CBT strategies were integrated to address Erika’sdepression ([7]) and NSSI ([10]), when these symptomsinterfered with panic treatment. Had Erika rated herdepression as her primary presenting problem, theclinician would have begun treatment for depressionrather than for panic disorder.
Stage 5: Monitor and Evaluate Treatment Outcomes andRevise Case Conceptualization as Necessary
The last stage of case conceptualization is to develop aplan for outcome evaluation and monitoring. A treatment-monitoring plan focuses on repeated assessments collectedduring treatment designed to test hypotheses andmonitor treatment progress. In contrast, the treatment-evaluation plan includes the measures used to assesswhether the long-term treatment goals have beenaccomplished. EBA methods can be used in both plans.
It is critical to collect assessment data during treatment.By collecting data at regular intervals, a feedback loop iscreated and the clinician can alter or adjust the caseconceptualization and treatment approach if needed,which can help improve client outcomes (Lambert et al.,2003). Indeed, some have recommended that if a clientdoes not show clinical improvements on objectivemeasuresthroughout the first 4 to 8 weeks/sessions, the treatmentapproach should be reevaluated (Youngstrom, 2012). Aspecific assessment strategy should be identified for eachhypothesis. In addition to conventional psychometricconsiderations (e.g., reliability, validity, etc.), assessmentinstruments used for outcome monitoring should besensitive to change and capable of assessing clinicalsignificant changes, so clinically relevant changes can bedetected. Ideally, these assessments should be focusedon specific symptoms/presenting problems that aretargets of treatment and should be able to be scoredquickly (e.g., prior to a session). Someexamples include theOutcome Questionnaire (OQ; Lambert et al., 1996) andthe Revised Child Anxiety and Depression Scale (RCADS;Chorpita et al., 2000). Both have computer-scoring options,facilitating timely scoring and interpretation. In particular,the OQ may be administered on a computer to a clientbefore a session, scored immediately, and the data is thenavailable to the clinician immediately prior to session.
Idiographic strategies are well suited for repeatedmeasurement and they allow the clinician to developindividualized approaches that can be used to test and revisehypotheses. Self-monitoring strategies such as behavior
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

10 Christon et al.
tracking charts, daily report cards or mood check-ups insession can be valuable (Haynes et al., 2009; Youngstrom,2012). Behavioral observations by external observers(e.g., a teacher) about specific behaviors (e.g., number ofprosocial initiations by a child client) may also be used(Haynes et al.). Also, as noted before, the Top Problemsmeasure can be used to identify week-by-week trajectoriesof change and to inform the clinician as to whetherclient-nominated problems respond to intervention (Weiszet al., 2011).
Gathering data is only the first step—the clinician mustbe able to draw meaningful conclusions from the data.Making sense of varied idiographic assessment measuresand different treatment goals can be done in a variety ofways. Data from idiographic assessment instruments can betracked and plotted systematically on a clinical dashboard.Such dashboards are available for purchase from organiza-tions such as PracticeWise, LLC (2004–2013b), or cliniciansmay opt to useMicrosoft Excel or a comparable program tograph or chart the data on their own. It can be useful toshare these graphs with clients to facilitate transparency inthe therapeutic process and aid in discussions aboutongoing treatment planning.
Terminating treatment occurs when the clinician andclient have agreed that adequate treatment gains have beenobtained. This is based both on the client’s subjectiveperspective of “feeling better,” as well as on ongoingassessment data about resolution of significant presentingproblems (e.g., decreased symptomatology). Assessmentdata can be used to determine if a client has experiencedclinically significant change defined as no longer above aclinical threshold (based on standardized norms) on aparticular measure. A clinician can also review diagnosticcriteria at the end of treatment to decide whether a personstill meets criteria for their diagnosis.
Stage 5: Erika’s CaseThe treatment plan called for weekly individual sessions
with Erika that included regular updates with her parents.Ongoing assessment of Erika’s symptoms and treatmentprogress took place using the RCADS on a bimonthly basis(a nomothetic assessment tool used in an idiographic fashion).Erika and her parents also each independently completedthe Top Problems measure in the waiting room prior toeach session (idiographic assessment). Additionally, Erika’sdaily anxiety level, daily number of panic attacks, andnumber of times leaving the house each week were trackedand mood check-ups were conducted at the beginning ofeach session, with the clinician keeping track of Erika’sself-reported ratings (idiographic assessment). The clinicianalso asked Erika at the beginning of each session to reporton the frequency and context of any NSSI that occurredover the prior week (idiographic assessment). Erika did notengage in NSSI after the second session, where a focus was
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
on safety planning and generating alternative copingactivities to replace self-harm behaviors.
Over the first eight sessions of PCT-A, Erika’s panicand agoraphobia symptoms did not decrease. In fact, shereported more panic attacks and she did not showreduction in anxiety ratings in session while completinginteroceptive exposures. These findings were reviewedwith Erika at the eighth session. At this time, Erika becametearful and asked if she could share something that shehad not shared with anyone before. Erika stated that whileshe had denied any past traumas in the intake, this was notthe truth. She reported that in the summer before 9th
grade, she had been walking home from a friend’s houseand witnessed an unrecognizable person in amask shootingand killing one of her classmates. She had run home andbegun crying, but did not tell her parents or friends for fearof worrying them. When school began the following week,she had to pass by where the incident had occurred on herway to and from school. At this point, her panic attacksbegan and she began to avoid going to school. She startedto have nightmares nightly and began experiencingnocturnal panic attacks. Erika was tearful throughout thisdiscussion and said she had not felt comfortable enough inprior meetings to share this information.
After an assessment and administering the KSADSPost-Traumatic Stress Module, Erika’s diagnosis was revisedto posttraumatic stress disorder (PTSD) and the clinicianrevised the case conceptualization (see Figure 3). It wasdetermined that Erika’s panic attacks (presenting problem; [D])resulted from activation of her autonomic nervous system(causal factor; [C]) when exposed to trauma-related cues(causal factor; [I]), both internal (cognitions) and external(walking past traumatic event location). Her agoraphobiaand NSSI were reconceptualized as avoidance/escape oftrauma cues (considered both a maintaining factor forher panic attacks, and a presenting problem nominated byErika and her parents; [E]), which reduced her symptomsshort-term (maintaining factor; [G]), but ultimately main-tained negative cognitions about trauma-related cues(maintaining factor; [H]). Her depressive symptoms werehypothesized to result from the trauma (historical factor;[B]), as well as her avoidance ([E]).
A change in the treatment plan was discussed with Erikaand her parents. A literature review identified thattrauma-focused CBT (TF-CBT) is efficacious for PTSD(Cohen, Mannarino, & Deblinger, 2006) and was thereforeselected and implemented. The UCLA PosttraumaticStress Disorder Reaction Index (UCLA-RI) Adolescentand Parent-Report versions (Steinberg, Brymer, Decker, &Pynoos, 2004) were administered on a bimonthly basis toassess for trauma-symptoms, alternating with the RCADS(nomothetic assessment). Self-monitoring of her anxietyand depressive symptoms on a weekly basis continued(idiographic assessment).
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

Figure 3. Figural Drawing of Erika’s Revised Case Conceptualization ([A]-[I]).
11Science-Informed Case Conceptualization
TF-CBT was implemented and, over time, Erika beganto report a reduction in her anxiety, panic attacks, andagoraphobia (on idiographic self-monitoring measures).These subjective reports were corroborated with self-and parent-reports on the UCLA-RI and the RCADS(nomothetic assessment). After four months, her symptomson these measures had reduced significantly. Theclinician therefore decided to readminister the broadscale administered at intake: the BASC-2, and the PTSDsection of the KSADS-PL (nomothetic assessment). Thefindings affirmed that Erika no longer met criteria forPTSD. The treatment focus then shifted to addressingErika’s remaining depressive symptoms until Erika, herparents, and the clinician mutually agreed on termina-tion.
Challenges to Applying Science-Informed CaseConceptualization
With any approach, there may be challenges orbarriers to implementation. One potential barrier to ourapproach is accessing the psychopathology and EBTliterature. However, information about treatmentoptions is becomingmore widely accessible via the internet(e.g., www.psychologicaltreatments.org). Further, a num-ber of psychopathology books provide informationneeded to inform case conceptualization and assessment(e.g., Barlow, 2007). Another potential barrier to using EBAmay include a lack of time, money, or organizationalsupport (Jensen-Doss & Hawley, 2010). Certain measuresare costly or only available in journal articles, whichmay make them difficult to access. However, free measuresare increasingly becoming available for youth and adult
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
psychopathology (see Beidas et al., this issue). There mayalso be concerns about the availability of measures indifferent languages, but a growing number of freelyavailable assessment measures have now been translatedinto different languages (e.g., the RCADS, the PediatricSymptom Checklist [http://www.massgeneral.org/psychiatry/services/psc_forms.aspx], the Patient HealthQuestionnaire [http://www.phqscreeners.com/]). Thus,the field is taking steps to address some of these barriers.
Conclusion
In sum, case conceptualization is a critical componentof EBP, bridging the gap between the empirical literatureand practice with individual clients. We have presented ascience-informed case conceptualization model designedto help translate research to clinical practice and reducebiases in clinical decision-making. Core features of thisapproach involve the clinician developing testable hy-potheses about the client’s presenting problems, selectinga treatment approach to test these hypotheses, and usingEBA methods to assess outcomes and accuracy ofhypotheses. Throughout, clinicians should rely on empir-ically validated theories and scientific literature to tailortreatment to the individual client. This process sets up afeedback loop wherein clinicians’ hypotheses and prac-tices are evaluated, opening the door to revise practicesbased on the data, ultimately maximizing the likelihood ofpositive clinical outcomes.
References
Addis, M. E., & Krasnow, A. D. (2000). A national survey of practicingpsychologists’ attitudes toward psychotherapy treatment manuals.Journal of Consulting and Clinical Psychology, 68(2), 331–339.
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

12 Christon et al.
American Psychiatric Association. (2013). Diagnostic and statisticalmanual of mental disorders (5th ed.). Washington, DC: Author.
American Psychological Association [APA] Presidential Task Force onEvidence-Based Practice. (2006). Evidence-based practice inpsychology. American Psychologist, 61(4), 271–85.
Angold, A., Costello, E. J., Farmer, E. M. Z., Burns, B. J., & Erkanli, A.(1999). Impaired but undiagnosed. Journal of the American Academyof Child & Adolescent Psychiatry, 38, 129–137.
Barlow, D. H. (2007). Clinical handbook of psychological disorders, fourthedition: A step-by-step treatment manual. New York: The GuilfordPress.
Barlow, D. H., Farchione, T. J., Fairholme, C. P., Ellard, K. K., Boisseau,C. L., Allen, L. B., & Ehrenreich-May, J. (2011). The unified protocolfor transdiagnostic treatment of emotional disorders: Therapist guide.New York: Oxford University Press.
Beck, J. S. (2011). Cognitive behavior therapy: Basics and beyond (2nd ed.).New York: The Guilford Press.
Beidas, R.S., Stewart, R.E., Walsh, L., Lucas, S., Downey, M.M., Jackson,K., & Mandell, D.S. (this issue). Free, brief, and validated;Standardized instruments for low-resource mental health settings.Cognitive and Behavioral Practice.
Bouton, M. E., Mineka, S., & Barlow, D. H. (2001). A modern learningtheory perspective on the etiology of panic disorder. PsychologicalReview, 108(1), 4–32.
Chorpita, B. F., Daleiden, E. L., Ebesutani, C., Young, J., Becker, K. D.,Nakamura, B. J., … Starace, N. (2011). Evidence-based treatmentsfor children and adolescents: An updated review of indicators ofefficacy and effectiveness. Clinical Psychology: Science and Practice,18, 154–172.
Chorpita, B. F., Daleiden, E. L., & Weisz, J. R. (2005). Identifying andselecting the common elements of evidence based interventions:A distillation and matching model. Mental Health Services Research,7(1), 5–20.
Chorpita, B. F., Yim, L.M., Moffitt, C. E., Umemoto, L. A., & Francis, S. E.(2000). Assessment of symptoms of DSM-IV anxiety and depressionin children: A Revised Child Anxiety and Depression Scale.Behaviour Research and Therapy, 38, 835–855.
Cochrane Database of Systematic Reviews. (2013). The CochraneLibrary. Retrieved on July 12, 2013 from: http://www.thecochranelibrary.com/view/0/index.html.
Cohen, J. A., Mannarino, A. P., & Deblinger, E. (2006). Treating traumaand traumatic grief in children and adolescents. New York: TheGuilford Press.
Craske, M. G., Farchione, T. J., Allen, L. B., Barrios, V., Stoyanova, M.,& Rose, R. (2007). Cognitive behavioral therapy for panic disorderand comorbidity: More of the same or less of more? BehaviourResearch and Therapy, 45(6), 1095–1109.
Croskerry, P. (2009). A universal model of diagnostic reasoning.Academic Medicine: Journal of the Association of American MedicalColleges, 84(8), 1022–8.
David-Ferdon, C., & Kaslow, N. J. (2008). Evidence-based psychosocialtreatments for child and adolescent depression. Journal of ClinicalChild and Adolescent Psychology, 37(1), 62–104.
Dawes, R. M., Faust, D., & Meehl, P. E. (1989). Clinical versus actuarialjudgment. Science, 243(4899), 1668–1674.
Fox, N. A., Henderson, H. A., Marshall, P. J., Nichols, K. E., & Ghera,M.M.(2005). Behavioral inhibition: Linking biology and behavior within adevelopmental framework. Annual Review of Psychology, 56, 235–62.
Haynes, S.N.,Mumma,G.H.,&Pinson, C. (2009). Idiographic assessment:Conceptual and psychometric foundations of individualized behav-ioral assessment. Clinical Psychology Review, 29(2), 179–91.
Haynes, S. N., & O’Brien, W. O. (2000). Principles of behavioral assessment:A functional approach to psychological assessment. New York:Plenum/Kluwer Press.
Hunsley, J., & Mash, E. J. (2007). Evidence-based assessment. AnnualReview of Clinical Psychology, 3, 29–51.
Gonzales, J. J., Ringeisen, H. L., & Chambers, D. A. (2002). The tangledand thorny path of science to practice: Tensions in interpretingand applying “evidence.” Clinical Psychology Science and Practice,9(2), 204–209.
Jensen-Doss, A., Hawley, K. M., Lopez, M., & Osterberg, L. D. (2009).Using evidence-based treatments: The experiences of youth
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
providers working under a mandate. Professional Psychology:Research and Practice, 40, 417–424.
Jensen-Doss, A., & Hawley, K. M. (2010). Understanding barriers toevidence-based assessment: Clinician attitudes toward standardizedassessment tools. Journal of Clinical Child & Adolescent Psychology,39(6), 885–896.
Jensen-Doss, A., McLeod, B. D., & Ollendick, T. H. (2013). Diagnosticassessment. In B. D. McLeod, A. Jensen-Doss, & T. H. Ollendick(Eds.), Diagnostic and behavioral assessment in children and adolescents:A clinical guide (pp. 34–55). New York, NY: Guilford Press.
Jensen-Doss, A., Ollendick, T. H., & McLeod, B. D. (2013). Diagnosticand behavioral assessment in action. In B. D. McLeod, A.Jensen-Doss, & T. H. Ollendick (Eds.), Diagnostic and behavioralassessment in children and adolescents: A clinical guide (pp. 417–448).New York: Guilford Press.
Kaufman, J., Birmaher, B., Brent, D., Rao, U., & Ryan, N. (1996). Theschedule for affective disorders and schizophrenia for school-age childrenand lifetime version. Pittsburgh, PA: Department of Psychiatry,University of Pittsburgh School of Medicine.
Kiresuk, T. J., & Sherman, R. E. (1968). Goal attainment scaling:A general method for evaluating comprehensive communitymental health programs. Community Mental Health Journal, 4(6),443–453.
Lambert, M. J., Burlingame, G. M., Umphress, V., Hansen, N. B.,Vermeersch, D. A., Clouse, G. C., & Yanchar, S. C. (1996). Thereliability and validity of the Outcome Questionnaire. ClinicalPsychology & Psychotherapy, 3(4), 249–258.
Lambert, M. J., Whipple, J. L., Hawkins, E. J., Vermeersch, D. A.,Nielsen, S. L., & Smart, D. W. (2003). Is it time for clinicians toroutinely track patient outcome? A meta-analysis. Clinical Psychology:Science & Practice, 10, 288–301.
Lindhiem,O., Kolko, D. J., & Cheng, Y. (2012). Predicting psychotherapybenefit: a probabilistic and individualized approach. BehaviorTherapy, 43(2), 381–392.
McLeod, B. D., Jensen-Doss, A., & Ollendick, T. H. (2013a). Caseconceptualization, treatment planning and outcome monitoring.In B. D. McLeod, A. Jensen-Doss, & T. H. Ollendick (Eds.),Diagnostic and behavioral assessment in children and adolescents: Aclinical guide (pp. 77–100). New York: Guilford Press.
McLeod, B. D., Jensen-Doss, A., & Ollendick, T. H. (2013b). Overviewof diagnostic and behavioral assessment. In B. D. McLeod, A.Jensen-Doss, & T. H. Ollendick (Eds.), Diagnostic and behavioralassessment in children and adolescents: A clinical guide (pp. 3–33).New York: Guilford Press.
National Institute of Mental Health. (2008). The National Institute ofMental Health strategic plan. Retrieved from www.nimh.nih.gov/about/strategic-planning-reports/index.shtml.
Nelson, T. D., Steele, R. G., & Mize, J. A. (2006). Practitioner attitudestoward evidence-based practice: Themes and challenges. Admin-istration and Policy in Mental Health and Mental Health ServicesResearch, 33(3), 398–409.
Nezu, A. M., Nezu, C. M., Peacock, M. A., & Girdwood, C. P. (2004).Case formulation in cognitive-behavior therapy. In M. Hersen(Series Ed.) & S. N. Haynes & E. M. Heiby (Vol. Eds.), Comprehensivehandbook of psychological assessment: Vol. 3. Behavioral assessment(pp. 402–426). Hoboken, NJ: Wiley.
Ollendick, T. H., McLeod, B. D., & Jensen-Doss, A. (2013). Behavioralassessment. In B. D. McLeod, A. Jensen-Doss, & T. H. Ollendick(Eds.), Diagnostic and behavioral assessment in children and adolescents:A clinical guide (pp. 56–76). New York: Guilford Press.
Persons, J. B., & Silberschatz, G. (1998). Are results of randomizedcontrolled trials useful to psychotherapists? Journal of Consultingand Clinical Psychology, 66(1), 126–35.
Persons, J. B., Davidson, J., & Tompkins, M. A. (2001). Essentialcomponents of cognitive-behavioral therapy for depression. WashingtonDC: American Psychological Association.
Pincus, D. B., Ehrenreich, J. T., & Mattis, S. G. (2008).Mastery of anxietyand panic for adolescents, therapist guide. New York: OxfordUniversity Press.
PracticeWise, LLC. (2004–2013a). Services: PracticeWise Evidence-BasedServices Database [PWEBS]. Retrieved July 12, 2013, from http://www.practicewise.com/#services.
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004

13Science-Informed Case Conceptualization
PracticeWise, LLC. (2004–2013b). Services: Clinical dashboard. RetrievedJuly 12, 2013, from http://www.practicewise.com/#services.
Reynolds, C. R., & Kamphaus, R. W. (2004). Manual for the behaviorassessment system for children, (2nd ed.). Circle Pines, MN: AmericanGuidance Service.
Steinberg, A. M., Brymer, M. J., Decker, K. B., & Pynoos, R. S. (2004).The University of California at Los Angeles Post-traumatic StressDisorder Reaction Index. Current Psychiatry Reports, 6(2), 96–100.
Sturmey, P., & Hersen, M. (2012). Handbook of evidence-based practice inclinical psychology (Volumes I and II). Hoboken, NJ: JohnWiley & Sons.
Taylor, S., Zvolensky, M. J., Cox, B. J., Deacon, B., Heimberg, R. G.,Ledley, D. R., … Cardenas, S. J. (2007). Robust dimensions ofanxiety sensitivity: development and initial validation of theAnxiety Sensitivity Index-3. Psychological assessment, 19(2), 176–88.
Weisz, J. R., Chorpita, B. F., Frye, A., Ng, M. Y., Lau, N., Bearman, S. K.,…Hoagwood, K. E. (2011). Youth Top Problems: Using idiographic,consumer-guided assessment to identify treatment needs and totrack change during psychotherapy. Journal of Consulting and ClinicalPsychology, 79(3), 369–80.
Weisz, J. R., Chorpita, B. F., Palinkas, L. A., Schoenwald, S. K., Miranda,J., Bearman, S. K., … Gibbons, R. D. (2012). Testing standard andmodular designs for psychotherapy treating depression, anxiety,and conduct problems in youth: a randomized effectiveness trial.Archives of General Psychiatry, 69(3), 274–282.
Please cite this article as: Christon et al., Evidence-Based Assessment MeCase Conceptualization, Cognitive and Behavioral Practice (2014), http://d
Westen, D., Novotny, C. M., & Thompson-Brenner, H. (2004).The empirical status of empirically supported psychotherapies:assumptions, findings, and reporting in controlled clinical trials.Psychological Bulletin, 130(4), 631.
Youngstrom, E. A. (2012). Future directions in psychological assess-ment: Combining evidence-based medicine innovations withpsychology’s historical strengths to enhance utility. Journal ofClinical Child and Adolescent Psychology, 42(1), 139–59.
Youngstrom, E.A., Choukas-Bradley, S., Calhoun, C., & Jensen-Doss, A.(this issue). Clinical guide to the evidence-based medicineapproach to diagnosis. Cognitive and Behavioral Practice.
The authors thank Cassidy Arnold for his consultation regarding thecase example in this manuscript.
Address correspondence to Lillian M. Christon, Ph.D., Depart-ment of Psychology, University of North Carolina–Chapel Hill, DavieHall Campus Box 3270, Chapel Hill, NC 27599-3270; e-mail:[email protected].
Received: July 30, 2013Accepted: December 1, 2013Available online xxxx
ets Evidence-Based Treatment: An Approach to Science-Informedx.doi.org/10.1016/j.cbpra.2013.12.004