Embed Size (px)
Citation preview

© Queen's Printer and Controller of HMSO 2007 1
Evaluation of the National Infarct Angioplasty Project
Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R&D (NCCSDO)
August 2008
prepared by
Professor Steve Goodacre
Health Services Research, University of Sheffield
Ms Fiona Sampson
Health Services Research, University of Sheffield
Dr Angela Carter
Institute of Work Psychology, University of Sheffield
Dr Allan Wailoo
Health Economics & Decision Science, University of Sheffield
Dr Alicia O’Cathain
Medical Care Research Unit, University of Sheffield
Professor Stephen Wood
Institute of Work Psychology, University of Sheffield
Professor Simon Capewell
Clinical Epidemiology, University of Liverpool
Dr Stephen Campbell
Cardiology, Sheffield Teaching Hospitals NHS Foundation Trust

© Queen's Printer and Controller of HMSO 2007 2
Professor Steve Goodacre
Health Services Research, ScHARR, 30 Regent Street, Sheffield S1 4DA
E-mail: [email protected]
© Queen's Printer and Controller of HMSO 2007 3
Contents Report for the National Co-ordinating Centre for NHS Service
Delivery and Organisation R&D (NCCSDO) ............................... 1 August 2008 ............................................................................. 1
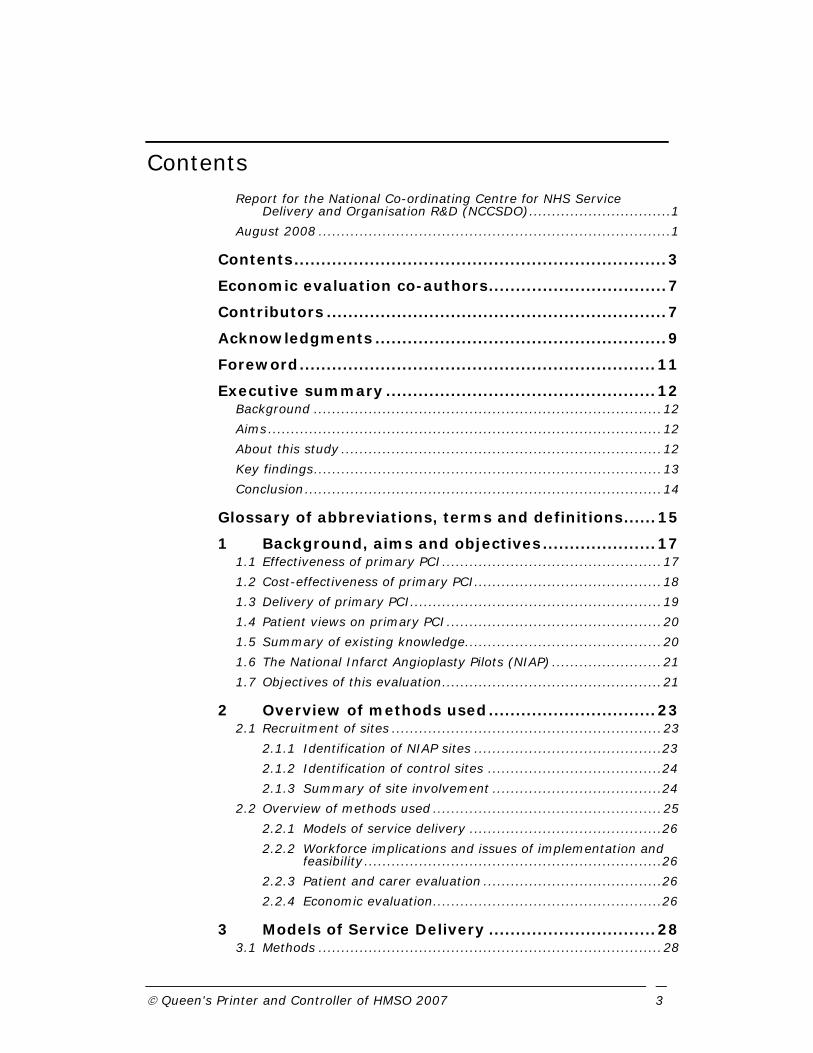
Contents ..................................................................... 3
Economic evaluation co-authors ................................. 7
Contributors ............................................................... 7
Acknowledgments ...................................................... 9
Foreword .................................................................. 11
Executive summary .................................................. 12 Background ............................................................................ 12 Aims ...................................................................................... 12 About this study ...................................................................... 12 Key findings ............................................................................ 13 Conclusion .............................................................................. 14
Glossary of abbreviations, terms and definitions ...... 15
1 Background, aims and objectives ..................... 17 1.1 Effectiveness of primary PCI ................................................ 17 1.2 Cost-effectiveness of primary PCI ......................................... 18 1.3 Delivery of primary PCI ....................................................... 19 1.4 Patient views on primary PCI ............................................... 20 1.5 Summary of existing knowledge........................................... 20 1.6 The National Infarct Angioplasty Pilots (NIAP) ........................ 21 1.7 Objectives of this evaluation ................................................ 21
2 Overview of methods used ............................... 23 2.1 Recruitment of sites ........................................................... 23
2.1.1 Identification of NIAP sites ......................................... 23 2.1.2 Identification of control sites ...................................... 24 2.1.3 Summary of site involvement ..................................... 24
2.2 Overview of methods used .................................................. 25 2.2.1 Models of service delivery .......................................... 26 2.2.2 Workforce implications and issues of implementation and
feasibility ................................................................. 26 2.2.3 Patient and carer evaluation ....................................... 26 2.2.4 Economic evaluation .................................................. 26
3 Models of Service Delivery ............................... 28 3.1 Methods ........................................................................... 28

© Queen's Printer and Controller of HMSO 2007 4
3.2 Description of different models of service delivery .................. 28 3.2.1 Service setting and overview ...................................... 28 3.2.2 Service infrastructure ................................................ 31 3.2.3 Service activity levels ................................................ 32
3.3 Results from the NIAP dataset ............................................. 32 3.3.1 Patient characteristics ................................................ 32 3.3.2 Route into hospital .................................................... 33 3.3.3 Patient treatment pathways ........................................ 34 3.3.4 Place of assessment .................................................. 36 3.3.5 Outcomes ................................................................ 38
3.4 Discussion ........................................................................ 38
4 Workforce Implications and Issues of Implementation and Feasibility ................................ 40
4.1 Background ....................................................................... 40 4.2 Hospitals involved in data collection...................................... 40 4.3 Methods of data collection ................................................... 41
4.3.1 Design and Procedure of Quantitative Data Collection ..... 41 4.3.2 Design and Procedure of Qualitative Data Collection ....... 42 4.3.3 Pilot Hospital Research .............................................. 44 4.3.4 Main Hospital Research .............................................. 44 4.3.4.2 Interviews ............................................................. 45
4.4 Results ............................................................................. 47 4.4.1 Reporting of data ...................................................... 47 4.4.2 Introduction to findings .............................................. 47 4.4.3 Staffing ................................................................... 48 4.4.4 Resources ................................................................ 55 4.4.5 Pathway .................................................................. 57 4.4.6 Change Management ................................................. 60 4.4.7 Solutions offered by primary PCI teams enabling service
development ............................................................ 64 4.5 Discussion ........................................................................ 67 4.6 Recommendations ............................................................. 72
5 Patient and Carer satisfaction .......................... 75 5.1 Background ....................................................................... 75 5.2 Methods ........................................................................... 75
5.2.1 Phase 1: Key aspects of the patient and carer experience75 5.2.2 Phase 2: Quantitative survey ...................................... 76 5.2.3 Phase 3: Further qualitative interviews ........................ 77
5.3 Results ............................................................................. 77 5.3.1 Description of respondents ......................................... 78 5.3.2 Overall satisfaction .................................................... 80 5.3.3 Speed and efficiency of service ................................... 82 5.3.4 Communication ........................................................ 83

© Queen's Printer and Controller of HMSO 2007 5
5.3.5 Consent and decision making...................................... 84 5.3.6 Management of pain and comfort ................................ 85 5.3.7 Hospital location and facilities ..................................... 86 5.3.8 Confidence in the care received ................................... 88 5.3.9 Discharge and follow up ............................................. 90 5.3.10 Different places of care .......................................... 92 5.3.11 Patient views of treatment: thrombolysis or primary
PCI? ........................................................................ 95 5.3.12 Different models of service delivery .......................... 96
5.4 Discussion ........................................................................ 96 5.4.1 Summary of findings ................................................. 96 5.4.2 Strengths of this evaluation ........................................ 98 5.4.3 Limitations of this evaluation ...................................... 98 5.4.4 Other literature ......................................................... 99
5.5 Conclusions ....................................................................... 99
6 Economic Evaluation ...................................... 101 6.1 Background. .................................................................... 101 6.2 Methods ......................................................................... 103
6.2.1 Characteristics of the cost effectiveness model ............ 103 6.2.2 Source of data ........................................................ 103 6.2.3 Patient characteristics .............................................. 104 6.2.4 Treatments provided within the initial episode ............. 104 6.2.5 Ambulance journeys ................................................ 104 6.2.6 Time to treatment ................................................... 105 6.2.7 Subsequent tests and coronary interventions .............. 105 6.2.8 Unit costs .............................................................. 105 6.2.9 Statistical analysis .................................................. 107
6.3 Results ........................................................................... 107 6.3.1 Patient characteristics .............................................. 107 6.3.2 Method of admission ............................................... 108 6.3.3 Time to treatment ................................................... 108 6.3.4 Resource cost ......................................................... 111 6.3.5 Cost analysis adjusting for covariates ........................ 114 6.3.6 Additional coronary interventions .............................. 118 6.3.7 Analysis of cost effectiveness .................................... 119
6.4 Discussion ...................................................................... 122
7 Overview of the evaluation ............................ 125 7.1 Key findings .................................................................... 125
7.1.1 Models of service delivery ........................................ 125 7.1.2 Workforce implications and issues of implementation and
feasibility ............................................................... 125 7.1.3 Patient and carer perspectives .................................. 126 7.1.4 Economic evaluation ................................................ 126
7.2 Integration of findings ...................................................... 127

© Queen's Printer and Controller of HMSO 2007 6
7.3 Limitations of the evaluation ............................................. 129 7.3.1 Generalisability of the findings .................................. 129 7.3.2 Sustainability of primary PCI .................................... 130
7.4 Overview of recommendations for policy and practice ........... 130 7.5 Suggestions for future research ......................................... 131
References ............................................................. 132
Appendix 1. ............................................................ 137
Appendix 2 ............................................................. 143
Appendix 3 ............................................................. 162

© Queen's Printer and Controller of HMSO 2007 7
Economic evaluation co-authors
Mark Sculpher, Professor of Health Economics, University of York
Stephen Palmer, Senior Research Fellow, University of York
Keith Abrams, Professor of Medical Statistics, University of Leicester
Christian Asseburg, Bayesian Statistician, Swedish Institute of Health Economics, Lund
Monica Hernandez, Lecturer, Department of Economics, University of Sheffield
Contributors
List of contributors to Evaluation of the National Infarct Angioplasty Project Steering group members
Roger Boyle, National Director for Heart Disease and Stroke (Co-chair National Infarct Angioplasty Project steering group and pilot project group)
Stephen Campbell, Consultant Cardiologist, Northern General Hospital, Sheffield. (Co-applicant)
Angela Carter, Research Fellow, Institute of Work Psychology, University of Sheffield (Occupational psychologist and co-applicant)
Mark de Belder, Interventional cardiologist, James Cook University Hospital, Middlesbrough (Chair NIAP data monitoring group)
Sue Dodd, Department of Health (NIAP Project Co-ordinator)
Steve Goodacre, Professor of Emergency Medicine, ScHARR and Consultant in Emergency Medicine, Northern General Hospital (Principal Investigator)
Huon Gray, Interventional cardiologist, Southampton (Co-chair National Infarct Angioplasty Project steering group and pilot project group)
Enid Hirst (Independent lay member)
Jason Kendall, Consultant in Emergency Medicine, Frenchay Hospital, Bristol. (Independent member)
Fiona Sampson, Research Fellow, ScHARR, University of Sheffield (Evaluation Project Manager)
Nigel Unwin, Professor of Epidemiology, Newcastle University (Independent Chair)
Allan Wailoo, Senior Lecturer, ScHARR, University of Sheffield (Health Economist)
Project group members

© Queen's Printer and Controller of HMSO 2007 8
Stephen Campbell, Consultant Cardiologist, Northern General Hospital, Sheffield. (Co-applicant)
Simon Capewell, Professor of Clinical Epidemiology, University of Liverpool (Co-applicant)
Angela Carter, Research Fellow, Institute of Work Psychology, University of Sheffield (Occupational psychologist and co-applicant)
Steve Goodacre, Professor of Emergency Medicine, ScHARR and Consultant in Emergency Medicine, Northern General Hospital (Principal Investigator)
Enid Hirst (Independent lay member)
Mark Jackson, Associate Director of Clinical Quality, Cardiothoracic Centre, Liverpool (Co-applicant)
Alicia O’Cathain, Senior Research Fellow, ScHARR, University of Sheffield (Patient carer component)
Fiona Sampson, Research Fellow, ScHARR, University of Sheffield (Evaluation Project Manager)
Rod Stables, Consultant Cardiologist, Cardiothoracic Centre, Liverpool (Co-applicant)
Allan Wailoo, Senior Lecturer, ScHARR, University of Sheffield (Health Economist)
Jim Wardrope, Consultant in Emergency Medicine, Northern General Hospital, Sheffield. (Co-applicant)
Stephen Wood, Professor, Institute of Work Psychology, University of Sheffield (Co-applicant)
Institute of Work Psychology
Leah Butler, Kate Fairhall, Sarah Blore, Suzanne Sondergaard, Holly Kent, Clare Sullivan and Harriet Booth, MSc Occupational Psychology (data collection for workforce implications).
Jacqueline Cameron, Ruth O’Neil and Emma Parry (data collection and analysis of qualitative data for workforce implications).
Principal contacts at NIAP and control sites
London Chest Hospital: Martin Rothman (Interventional cardiologistI) Rodney de Palma (Cardiology SpR), Rachel Parke (Cardiac research co-ordinator)
Doncaster Royal Infirmary: Gillian Payne (Consultant cardiologist), Michelle Barratt (Cardiac rehabilitation sister)
Dryburn Hospital, Durham: Michael Cave (Consultant cardiologist), Julie Close (audit nurse)
Hammersmith Hospital: Chris Baker (Interventional cardiologist), Irene Arenillas (NIAP audit co-ordinator)

© Queen's Printer and Controller of HMSO 2007 9
Harefield Hospital: Miles Dalby (Interventional cardiologist), Kylie Rowles (PPCI nurse), Emma Neves (PPCI nurse)
Hull Royal Infirmary: John Caplin (Consultant cardiologist), Lorraine Rowell (cardiology nurse), Marilyn Brown (cardiology nurse)
James Cook University Hospital, Middlesbrough: Jim Hall (Interventional cardiologist), Andrea Moffitt (audit sister), Bob Morley (audit)
Kings College Hospital: Martyn Thomas (Interventional cardiologist), Jayne Damm (PPCI nurse)
Leeds General Infirmary: Jim McLenachan (Interventional cardiologist), Claire Priestley (PPCI nurse), Kathryn Somers (PPCI nurse)
Manchester Royal Infirmary: Farzin Fath-Ordoubadi (Interventional cardiologist), Roger Gamon (Primary PCI project manager), Sam Chapman (PPCI nurse)
Northern General hospital, Sheffield. Stephen Campbell (Consultant cardiologist)
Oxford Radcliffe hospitals: Adrian Banning (Interventional cardiologist)
Royal Devon and Exeter hospitals: David Smith (Interventional cardiologist), Sam Tampkins (Research nurse), Cathy Allman (reperfusion nurse)
Royal Liverpool University hospital: Mike Fisher (Consultant cardiologist), Rory Cavanagh (cardiology nurse)
Royal Victoria Infirmary, Newcastle: Phil Adams (Consultant cardiologist), Joan Easton (CCU sister)
St Mary’s NHS Trust: Iqbal Malik (Interventional cardiologist), Tina Chan (PPCI nurse), Priscilla Ryder (PPCI nurse)
Wythenshawe hospital: Bernard Prendergast (Interventional cardiologist), Mike Cullen (PPCI nurse), Luke Coleman (audit facilitator)
Acknowledgments
Kathryn Paulucy for clerical assistance
Patients and staff from all the participating hospitals who participated in the research or helped with data collection
The following staff for help with providing cost data for the economic evaluation: Rebecca Stevens, Katrina O’Halloran (Doncaster Royal Infirmary), Stephen Stewart (Northern General, Sheffield), Kiki Anne Doran, Caroline Kitchen (Royal Liverpool), Mark Jackson (CTC, Liverpool), Sheila Jamieson (Freeman hospital, Newcastle), Aidan MacDermott, Louise Matthews (Royal Victoria, Newcastle), Colin Evans, Jan Keenan, Alyn Still

© Queen's Printer and Controller of HMSO 2007 10
(John Radcliffe, Oxford), Sarah Bolton (James Cook, Middlesbrough), Claire Priestley (Leeds General Infirmary), Tina Chan, Lee Lewis (St Mary’s, London), Rachel Parke (London chest hospital).
User group led by Enid Hurst who helped with study design, piloting the patient and carer questionnaire and interpreting the findings.

© Queen's Printer and Controller of HMSO 2007 11
Foreword
The national feasibility study to advise on the extent to which primary angioplasty can be rolled out as the main treatment for heart attack in England was established by the Department of Health and British Cardiovascular Society following a review of national policy by the Prime Minister’s Delivery Unit in summer 2003.
Evidence for the longer term benefits of primary angioplasty are increasingly encouraging but the delivery of this service on a national basis presents a number of challenges when compared to treatment with thrombolysis (clot busting drugs). For example, the need for 24 hour availability of the team to carry out an angioplasty in an emergency, patient and relatives’ concerns about travelling to a hospital which may not be their local hospital and how best to organise services to meet peoples needs in the most clinically and cost effective way.
In February 2008, the Department of Health and British Cardiovascular Society issued an Interim Report on the National Infarct Angioplasty Project based on data and observations from the project’s pilot sites. This showed that primary angioplasty could be delivered in a clinically effective timely fashion using different service models. However, we were aware that certain important aspects of the study were still to come, namely what do patients think about primary angioplasty, what do staff think, how are services best organised and what does it cost?
We welcome this independent evaluation of these key components of the feasibility study undertaken by the School of Health and Related Research and Institute of Work Psychology at the University of Sheffield, which will inform our thinking on future national policy for the treatment of heart attack.
Prof. Roger Boyle National Director for Heart Disease and Stroke Co-chair, National Infarct Angioplasty project
Dr Huon Gray Past President of British Cardiovascular Society Consultant Cardiologist Southampton University Hospital Co-chair, National Infarct Angioplasty project

© Queen's Printer and Controller of HMSO 2007 12
Executive summary
Background
Primary percutaneous coronary intervention (PCI) and thrombolysis (clot-busting drugs) are two alternative treatments for ST-elevation myocardial infarction (heart attack). Primary PCI appears to be more effective than thrombolysis, but costs more to deliver and requires reorganisation of acute services. The National Infarct Angioplasty Project (NIAP) involved establishing primary PCI at ten hospitals to test the feasibility of delivering this service in the NHS.
Aims
• To describe the models of service delivery established at the NIAP sites.
• To assess the workforce implications of a primary PCI service and explore the effect upon staff.
• To explore the feasibility of implementing primary PCI.
• To explore the experience and measure patient and carer satisfaction with primary PCI and thrombolysis-based care.
• To compare costs of primary PCI and thrombolysis, and estimate the cost-effectiveness of PCI-based care.
About this study
We evaluated implementation of primary PCI at NIAP hospitals and compared it to thrombolysis-based care at control hospitals.
• We described the systems used to deliver primary PCI using site visits, data collected by the NIAP hospitals and routinely available health and population data.
• Staff at seven NIAP hospitals contributed to the workforce and organisational study by completing a survey and participating in focus groups and interviews. Ethnographic observations were undertaken in catheter laboratories and objective data were collected on primary PCIs conducted in the month of study. In total 460 observations were collected.
• Patient and carer perspectives were explored using (a) face-to-face semi-structured interviews with ten patients and six carers, (b) postal questionnaires to 679 patients and 486 carers across four NIAP and four control sites, and (c) further interviews with eleven patients at NIAP sites and six at controls.

© Queen's Printer and Controller of HMSO 2007 13
• Cost-effectiveness was assessed using a decision-analysis model populated with cost and time delay data from the NIAP hospitals and four control hospitals.
Key findings
All ten NIAP hospitals implemented primary PCI, although not all provided a 24/7 service. Evaluation showed the following:
• The NIAP hospitals varied in size, configuration, infrastructure, referral routes and activity levels.
• The NIAP hospitals treated 2072 patients (71% male, age range 24 to 104) over the evaluation year, 70% admitted directly to a primary PCI hospital and 30% transferred from a non-PCI hospital.
• Median call-to-balloon times were 87 minutes for direct to catheter laboratory, 132 minutes via coronary care, 140 minutes via the emergency department, and 161 minutes for transfers from a non-PCI hospital.
• Establishing the full 24-hour primary PCI service from the start appeared to work better than incremental expansion.
• Staff needed to work in a flexible, multi-skilled manner across traditional task boundaries.
• On-going training was required to retain experienced team members.
• Failure to harmonise staff pay and conditions before commencing the service meant inequity of reward and rest after out-of-hours working.
• Primary PCI required simple direct access for patients and good teamworking across professional boundaries.
• Building and maintaining relationships with key stakeholders was critical to service development and sustainability.
• Regular audit of the heart attack pathway identified blockages limiting the capacity of the system.
• Development of primary PCI may have been associated with knock-on effects upon elective services and particularly upon rehabilitation.
• Patients and carers reported high overall levels of satisfaction with NIAP and control care (patients 78% v 71% excellent (p=0.074), carers 63% v 55% (p=0.049)).
• Patients at NIAP sites reported higher levels of satisfaction than control sites with the time waited and the efficiency of treatment (80% v 67% excellent (p<0.001) and 83% v 74% (p=0.009)).

© Queen's Printer and Controller of HMSO 2007 14
• Satisfaction with information given on how to manage the condition in future was lower in NIAP than control sites (38% v 46% excellent (p=0.049)).
• The mean cost of the treatment episode was £3,509 for thrombolysis at control sites, £4,361 for thrombolysis at NIAP sites, and £5,176 for PPCI at NIAP sites.
• Primary PCI-based care was more expensive than thrombolysis-based care but at £4520 per quality-adjusted life year gained would be considered cost-effective
• Direct access to the primary PCI hospital catheter laboratory was most likely to be cost-effective, whereas thrombolysis-based care was dominant when analysis was limited to those transferred from a non-PCI centre.
This evaluation was not randomised and was designed to measure the feasibility of establishing a national service rather than clinical benefits of primary PCI. NIAP hospitals were chosen to participate in this pilot study on the basis of willingness and ability to establish a primary PCI service, so they may not be representative of typical NHS hospitals. They also served a more urban, younger and more ethnically diverse population than the United Kingdom average. We did not evaluate the long-term sustainability of primary PCI services.
Conclusion
Primary PCI is feasible in a variety of settings, acceptable to patients and carers, generally supported by staff, and is likely to be a cost-effective use of NHS resources for patients directly accessing a PCI centre. However, primary PCI is unlikely to be cost-effective if significant time delays are incurred, such as those observed in this study when patients arrived via a non-PCI hospital. We have highlighted several organisational features that influence successful implementation.

© Queen's Printer and Controller of HMSO 2007 15
Glossary of abbreviations, terms and definitions
Definitions
Angiogram Diagnostic X-ray movie imaging of the coronary arteries (+/- left ventricle) following injection of contrast (dye) selectively into these structures via a catheter.
Angioplasty See PCI
Catheter Laboratory
The area of the hospital where angioplasty is performed.
CCU Coronary Care Unit. The area of the hospital where patients with a heart attack are initially treated.
CHD Coronary Heart Disease. Hardening of the blood vessels supplying the heart, which can lead to a heart attack.
CTB Call to balloon (time). The time delay between the patient calling for medical assistance and successful inflation of the angioplasty balloon to restore blood flow.
CTN Call to needle (time). The time delay between the patient calling for medical assistance and administration of intravenous thrombolysis.
Emergency department
The area of the hospital where emergency patients are initially assessed and treated. Also known as Accident & Emergency (A&E) or Casualty.
Heart attack A blockage of the blood vessel supplying the heart leading to heart damage and the risk of death or complications. In this report we use the term “heart attack” to refer to ST-elevation myocardial infarction.
In-hospital thrombolysis
Use of clot busting drugs by hospital doctors or nurses after the patient arrives at hospital.
PCI Percutaneous coronary intervention. Use of a catheter passed into the blood vessels supplying the heart to open a blood vessel. Often followed by placement of a stent to keep the blood vessel open. Also referred to as angioplasty.
Pre-hospital thrombolysis
Use of clot busting drugs by ambulance paramedics or general practitioners before the patient arrives at hospital.
Primary PCI PCI performed as an emergency to treat a heart attack.

© Queen's Printer and Controller of HMSO 2007 16
Rescue PCI PCI performed as an emergency after initial unsuccessful treatment of a heart attack with thrombolysis.
Thrombolysis Use of a clot-busting drug to break down the blood clot causing a heart attack.
Abbreviations
AMI Acute myocardial infarction BCIS British Cardiovascular Intervention Society BCS British Cardiovascular Society CABG Coronary artery bypass graft CCAD Central Cardiac Audit Database CCU Coronary Care Unit CHD Coronary heart disease CI Confidence interval CL Catheter laboratory CTB Call to balloon CTN Call to needle DES Drug eluting stents DGH District general hospital DTB Door to balloon DTN Door to needle ECG Electrocardiogram ED Emergency department IABP intra-aortic balloon pump ICER Incremental cost-effectiveness ratio IH In-hours LOS Length of stay MI Myocardial infarction (see ‘heart attack’) MINAP Myocardial Infarction National Audit Project NIAP National Infarct Angioplasty Pilots NHS National Health Service OOH Out of hours PCI Percutaneous coronary intervention PPCI Primary PCI QALY Quality-adjusted life year RCT Randomised controlled trial STEMI ST-elevated myocardial infarction (see ‘heart attack’) UK United Kingdom US United States WTP Willingness to pay

© Queen's Printer and Controller of HMSO 2007 17
1 Background, aims and objectives
Acute ST-elevation myocardial infarction (STEMI) occurs when a coronary artery is occluded by a blood clot. Treatment of STEMI involves removing the coronary artery occlusion to allow restoration of blood flow to the heart. Use of an intravenous thrombolytic agent to break down the clot is cheap, simple and effective, and can be provided in all acute hospitals and by most ambulance services in the National Health Service (NHS). Primary percutaneous coronary intervention (PCI) or angioplasty, where a balloon catheter, with or without subsequent stent implantation, is used to restore blood flow, is more effective for many patients, probably more costly and delivery requires specialist staff and facilities.
Primary PCI has been compared to thrombolysis in clinical trials, but evaluation is required to determine the feasibility and acceptability of routine provision of primary PCI, evaluate the different ways in which services can be organised to deliver primary PCI, investigate the organisational barriers to implementing primary PCI and the associated workforce issues, and estimate the cost-effectiveness of primary PCI in routine practice.
1.1 Effectiveness of primary PCI
Meta-analysis of randomised trials comparing primary PCI to intravenous thrombolysis has established that primary PCI is associated with reduced mortality, reinfarction, stroke and need for coronary artery bypass grafting, compared to thrombolysis (Keeley et al., 2003, Cucherat et al., 2004, Hartwell et al.,2005, Asseburg et al., 2007). However, meta-analysis has also shown that the effectiveness of primary PCI is dependent upon two key time delays (Boersma et al., 2006):
1. Presentation delay: the delay between symptom onset and patient entry into the emergency care system (or randomisation in the case of trial participants)
2. PCI-related delay: the delay between the time at which thrombolysis would have been given and the time at which primary PCI was provided.
The effectiveness of thrombolysis compared to placebo decreases in a non-linear manner as the presentation delay increases (Boersma et al., 1996). Hence thrombolysis is highly effective in the initial hours after symptom onset. Effectiveness decreases over the following hours so that thrombolysis may be no more effective than placebo if presentation delay exceeds 12 hours.

© Queen's Printer and Controller of HMSO 2007 18
The effectiveness of primary PCI has only been evaluated in comparison to thrombolysis. A pooled analysis of randomised trials (Boersma et al., 2006) suggested that primary PCI was associated with a 37% relative reduction in 30-day mortality compared to thrombolysis that did not appear to vary with presentation delay. However, since mortality in the thrombolysis treated group increased with presentation delay the absolute reduction in mortality associated with primary PCI increased with presentation delay.
PCI-related delay can be estimated by subtracting the estimated door to needle time (the time delay between arrival at hospital and administration of thrombolysis) from the estimated door to balloon time (the time delay between arrival at hospital and inflation of the PCI catheter balloon). If thrombolysis is administered prior to arrival at hospital then either a negative door to needle time or call to needle/balloon times should be used (i.e. the times from the patient call to the emergency services). The median door to needle time and door to balloon time in the pooled analysis of randomised trials were 19 and 76 minutes respectively, and the overall PCI-related delay was 54 minutes. The effectiveness of primary PCI compared to thrombolysis depends upon the PCI-related delay. It has been estimated that if the PCI-related delay exceeds 90 minutes then the mortality benefit at 6 months of PCI may be lost (Asseburg et al., 2007).
Time delays are a particularly salient issue when comparing primary PCI to pre-hospital thrombolysis. Most trials have compared primary PCI to in-hospital thombolysis given upon patient arrival at hospital. However, paramedics or doctors may administer thrombolysis prior to arrival at hospital. Meta-analysis of trials comparing pre-hospital to in-hospital thrombolysis has shown mortality benefit associated with pre-hospital thrombolysis (Morrison et al., 2000) The mortality benefit is likely to depend upon the time saving achieved by providing pre-hospital thrombolysis and is thus likely to provide more benefit in settings with long pre-hospital transport times (i.e. rural or highly-congested urban areas).
Few trials have compared primary PCI to pre-hospital thrombolysis. The CAPTIM (Comparison of Angioplasty and Pre-hospital Thrombolysis in Acute Myocardial Infarction) Trial showed no benefit from primary PCI compared to pre-hospital thrombolysis in patients presenting with early myocardial infarction (Bonnefoy et al., 2002). As with comparisons between pre-hospital and in-hospital thrombolysis, the relative effectiveness, and therefore cost-effectiveness, of pre-hospital thrombolysis and primary PCI depends upon pre-hospital transport times.
1.2 Cost-effectiveness of primary PCI
Although the costs of agents vary, thrombolysis is simple to administer and thus a relatively cheap intervention. Primary PCI, by contrast, requires a specialist team of health professionals with access to a catheter laboratory and is thus more expensive. This additional expense may be offset to some

© Queen's Printer and Controller of HMSO 2007 19
extent by subsequent health care costs incurred by patients. For example, shorter hospital stays and less frequent complications will all reduce the overall additional cost associated with primary PCI. Even if these elements do not offset the higher initial treatment cost, the net effect on costs may be justifiable if primary PCI can be provided with an acceptable PCI-related delay and thereby achieves a worthwhile improvement in health outcomes. However, any additional expenditure would need to be justified in comparison to other claims upon health care resources.
Patients receiving primary PCI may require a shorter hospital stay than those receiving thrombolysis, they are less likely to require subsequent coronary angiography or elective PCI, and they are less likely to suffer subsequent bleeding, stoke or reinfarction, all of which will incur health care costs.
Health economists at the University of York have investigated the potential cost-effectiveness of primary PCI to the NHS using decision-analytic modelling techniques (Bravo Vergel et al., 2007) Their analysis suggests that primary PCI is cost-effective, despite incurring increased costs, because of superior mortality benefit and the prevention of non fatal outcomes. The base case analysis suggested an incremental cost-effectiveness ratio of £9,241 per quality adjusted life year (QALY) with a 90% probability of being cost-effective given a threshold for willingness to pay of £20,000 per QALY.
This analysis was based upon data from meta-analysis of randomised trials comparing primary PCI to thrombolysis and thus assumed a PCI-related delay of 54 minutes. If the PCI-related delay exceeded 54 minutes in practice then cost-effectiveness would worsen. A sensitivity analysis suggested that if PCI-related delay were 90 minutes then the base case incremental cost-effectiveness ratio would be £64,750 per QALY and PCI would be unlikely to be considered cost-effective. The analysis also assumed that length of hospital stay following primary PCI would be the same as that following thrombolysis. Analysis suggested that cost effectiveness could be sensitive to this assumption.
It is therefore apparent that there is considerable uncertainty regarding the cost-effectiveness of primary PCI, much of which is due to a lack of empirical data reflecting the routine use of primary PCI in the NHS.
1.3 Delivery of primary PCI
Primary PCI is a complex intervention that needs to be delivered in an emergency by specialist staff using specialist facilities. As outlined above, failure to deliver primary PCI in a timely manner may impair effectiveness and thereby cost-effectiveness. Primary PCI delivered as part of a randomised trial may differ markedly from routine NHS service.
Several models have been suggested for providing widespread access to primary PCI (Waters et al., 2004, Keeley et al., 2004), but little data exist to compare these models. Meta-analysis suggests that primary PCI is superior to thrombolysis even when it requires inter-hospital transfer (Dalby et al., 2003). Data from the United States (US) suggest that centres with a

© Queen's Printer and Controller of HMSO 2007 20
higher volume of PCI procedures have a lower mortality rate (Canto et al., 2000), and that the advantages of primary PCI over thrombolysis are limited to hospitals with a high or intermediate volume of cases (Magid et al., 2000). Meanwhile, regionalisation of PCI services does not appear to increase travel distances for most patients (Kansagra et al., 2004). This has prompted researchers to suggest a network model similar to US trauma networks (Keeley et al., 2004), in which patients bypass or are transferred from local hospitals to specialist centres, although this approach may not be transferable to the NHS (Nicholl and Turner, 1997).
A number of barriers to the delivery of primary PCI have been identified (Keeley et al., 2004), mainly related to the difficulty of providing timely access to appropriate staff and facilities, and strategies have been suggested to overcome these barriers. However, both the barriers and solutions identified have been based on a paucity of empirical data and those identified in other health care systems may not be transferable to the NHS. For example, there are important international differences in the professional groups delivering services and in the way health services are funded and organised.
One of the principal barriers to delivery of a primary PCI service is the 24-hour requirement for specialist medical and nursing staff to be available to respond in an emergency (Fye, 2004). Outcomes from myocardial infarction are related to staffing levels and staff specialisation (Person et al., 2004, Ayanian et al., 2002), appropriate staffing is essential to achieve anticipated outcomes. However, successful implementation may take trained staff away from other important roles, such as on-call commitments and emergency cover, and have some negative consequences for the NHS.
1.4 Patient views on primary PCI
The views of service users should help determine the development of NHS services. It is self-evident that patients and carers want effective services, but other factors may have an important influence upon their experience. For example, implementation of primary PCI may require centralisation of services, which may run counter to patient and carer preferences. Patient views have been sought in developing cardiac care (Niles et al., 1996), in the attempt to weigh the risks and benefits of reperfusion strategies for myocardial infarction (Heyland et al., 2000, Tsui et al., 2005, Stanek et al., 1997], and in comparing diagnostic strategies for chest pain (Goodacre et al., 2004, Rydman et al., 1997). The patient experience of PCI has been explored (Gulanick et al., 1997), but comparison of primary PCI to thrombolysis has focussed upon mortality, morbidity and cost-effectiveness rather than acceptability.
1.5 Summary of existing knowledge
Trial data suggest that primary PCI for STEMI is more effective than thrombolysis and modelling suggests that it represents a cost-effective use of NHS resources despite being more expensive. However, the effectiveness

© Queen's Printer and Controller of HMSO 2007 21
and cost-effectiveness of primary PCI depend upon a number of factors, most notably the timeliness with which it is delivered. These in turn will depend upon organisation of the specialist staff and facilities required to deliver primary PCI. Finally, little is known about patient views of treatment alternatives. Primary PCI is therefore a promising treatment for STEMI but requires evaluation in routine NHS practice before widespread implementation can be recommended.
1.6 The National Infarct Angioplasty Pilots (NIAP)
In 2003 the Prime Minister’s Delivery Unit asked the Department of Health “Heart Team” to develop a clear policy for expanding primary PCI and to draw conclusions on the advisability and feasibility of a national rollout of the service. Up to £1m was allocated in England to support data collection and analysis. The British Cardiovascular Society (BCS) and the British Cardiovascular Intervention Society (BCIS) were invited to collaborate.
Expressions of interest were invited from centres in England wishing to participate. Pilot sites were selected on the basis of their commitment and perceived ability to collect the necessary data, and to reflect a variety of geographical settings and models of service delivery. The seven primary PCI services selected as pilot sites (and their hospital bases) were: Royal Devon & Exeter (Exeter), South Tees (Middlesbrough), West Yorkshire (Leeds), Greater Manchester (MRI and Wythenshawe), North East London (Barts & the London), South East London (King’s) and North West London (St Mary’s, Hammersmith, Harefield).
Each site had a Clinical Lead (an experienced and practising Interventional Cardiologist), and was provided with funding to employ a full-time Project Manager. Pilot sites were not asked to adhere to a centrally determined protocol, since one of the purposes of the project was to compare different models of service delivery. However, all pilot sites were expected to practise in line with published clinical trial evidence and to satisfy local clinical governance scrutiny.
It was planned that data would be collected from all patients with STEMI treated at these centres between 1st April 2005 and 31st March 2006. Data would be collected during the initial hospital episode and would continue up to one year after initial presentation with STEMI. These data were made available for use within this evaluation.
1.7 Objectives of this evaluation
We aimed to evaluate the implementation of primary PCI in the NIAP project. Our specific objectives were:
• To describe the models of service delivery established at the pilot sites in terms of their setting (geography, population, transport and

© Queen's Printer and Controller of HMSO 2007 22
communications), structure (hospitals, referral networks, transfer and access points) and components (staff, facilities, and equipment).
• To explore implementation and feasibility issues by describing the processes involved in establishing primary PCI, identifying facilitating factors and barriers to implementation, and assessing the implications of establishing primary PCI for cardiology and other services.
• To assess the workforce implications of setting up a PCI service at the pilot sites, and measure the effect of providing the service upon the PCI team, support staff, and related staff groups.
• To gain an in depth understanding of patient and carer experience of receiving care at the pilot sites, and measure differences in satisfaction between the pilot sites and sites providing standard, thrombolysis-based care.
• To compare the costs and outcomes of providing PCI and thrombolysis and estimate the incremental cost-effectiveness of a comprehensive primary PCI service, compared to standard, thrombolysis-based care, for the different organisational service models adopted in the pilot sites.

© Queen's Printer and Controller of HMSO 2007 23
2 Overview of methods used
The design was a mixed methods study with four components, each addressing at least one of the research objectives: a description of models of service delivery, an assessment of workforce implications and issues of feasibility and implementation using both qualitative and quantitative methods, an exploration of patient and carer satisfaction using both qualitative and quantitative methods, and an economic evaluation. All components were undertaken concurrently, led by different researchers within the team (Creswell & Plano-Clark, 2007). Integration of findings from different components occurred through discussions of emerging findings during team meetings (O’Cathain et al., 2007). The Project Manager and Principal Investigator were involved in all components and facilitated integration across the study.
The second and third objectives of the evaluation, relating to workforce implications and issues of feasibility and implementation, were addressed together by the same researchers. This was because we anticipated that these issues would be strongly inter-related and would be best addressed by sharing methods for data collection and analysis. Emerging findings confirmed this expectation with themes cutting across both issues. We have therefore reported findings related to both these objectives together.
The methods and findings of each component are reported separately in Chapters 3 to 6. Convergence and discrepancy between findings from different components are discussed within these chapters, where relevant. Finally, all findings are considered together in the overview in Chapter 7.
Ethical approval for the evaluation was obtained from Nottingham MREC in December 2005. Honorary contracts for the Project Manager were obtained for all sites to enable patient interviews and validation of patient data to be undertaken at all sites. Honorary contracts were also obtained for all researchers involved in site visits for the organisational and workforce evaluation.
2.1 Recruitment of sites
2.1.1 Identification of NIAP sites
The NIAP pilot sites had already been selected by the Department of Health working group prior to our evaluation being planned. Expressions of interest to become a pilot site were invited from 14 hospitals in England. Pilot sites were selected based upon their ability to collect data and to provide a range of geographical settings and models of service delivery. One site that did not undertake primary PCI was also selected to collect data for all of their heart attack patients within the same period to provide control data.
© Queen's Printer and Controller of HMSO 2007 24
Ten hospitals in seven pilot sites were provided with funding to employ a full-time audit nurse to collect data on all patients with STEMI for the year April 2005-March 2006 and to collect data on subsequent admissions for the year following their index admission. Pilot sites were expected to provide a primary PCI service as an alternative to thrombolysis, preferably for all patients, with a single route of admission to hospital and with the aim of providing primary PCI 24/7 during the period. Some hospitals also had arrangements with non-primary PCI hospitals for their patients to be transferred in for PPCI. One site offering thrombolysis only was also funded to collect data for the same period.
Two of the pilot sites comprised more than one hospital undertaking primary PCI and were grouped together as ‘sites’. However, we found no evidence of a coherent system for the ‘sites’ as each hospital worked on an individual basis, dealing with their own set of patients and with their own staff. We therefore refer to the ten individual hospitals throughout this study, rather than the seven pilot sites. We refer to these hospitals as the ‘intervention’ or NIAP sites throughout this report.
Data was collected in a project-specific NIAP dataset. This included fields already collected for the Myocardial Infarction National Audit Project (MINAP) and British Cardiovascular Intervention Society (BCIS) audit, with a small number of additional fields (CCAD, 2005). Data collection for the index event was completed by May 2006 and a sample of 4% of all patients at each site was validated by the Project Manager.
2.1.2 Identification of control sites
NIAP was initially established as a feasibility study without control sites. In order to provide comparative data for the patient and carer evaluation and the economic evaluation, we sought data on patients being treated for a heart attack in non-NIAP sites. We identified and recruited six control sites that offered mainly thrombolysis-based reperfusion strategies for use as controls. Control sites were selected to represent a variety of geographical settings, teaching and non-teaching hospitals. We also took practical considerations into account, particularly whether the sites were known to be participating fully in MINAP and collecting reliable data. These sites are referred to as ‘control’ sites throughout this report.
Both NIAP and control sites were selected purposively to provide observational data based upon the service they were providing. Sites were not randomised to intervention or control.
2.1.3 Summary of site involvement
The sites used for the different components of the evaluation are detailed in Table 1.
Table 1: Sites involved in the different components of the evaluation
NIAP sites Control sites

© Queen's Printer and Controller of HMSO 2007 25
Site
ID
St M
ary's
Hamm
ersm
ith
Hare
field
Barts
King
s
Midd
lesbr
ough
Ma
nche
ster R
oyal
Infirm
ary
Wyth
ensh
awe
Leed
s
Exete
r
Dryb
urn
Sheff
ield
Oxfor
d
Hull
Newc
astle
Liver
pool
Donc
aste r
Models of service delivery ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● Organisational component
● ● ● ● ● ● ●
Patient and carer component
● ● ● ● ● ● ● ● ●
Economic component
● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
Each component used data from different time periods. The models of service delivery and the economic evaluation both used data from the pilot year of April 2005-March 2006 whilst the organisational and workforce and patient and carer components collected new data during the evaluation (see chapter 4).
Figure 1: Data collection periods for different study components
For phase 1 of the patient and carer component, we used the first London and first non-London site that completed the ethics and honorary contract process. For phase 2, we selected two London and two non-London sites that were willing to participate in recruitment of patients and ensured that we had included the one District General Hospital in the study. The four control sites selected were those that carried out mainly thrombolysis. By the time of the survey, Sheffield and Oxford had extended the proportion of patients who were receiving primary PCI so were not selected.
2.2 Overview of methods used
The methods used within each component of the evaluation are described in detail within each chapter. A brief overview is provided below.
Models of service delivery
Survey period
Pilot
Interviews & focus groupsStaff surveys
Development interviewsSurveys to sites
Follow-up interviews
Economic evaluation
Data collection
2005 2006 2007Q1 Q2 Q3 Q4Q1 Q2 Q3 Q4
Organisation and workforce component
Patient and carer component
Q2 Q3 Q4

© Queen's Printer and Controller of HMSO 2007 26
2.2.1 Models of service delivery
We collected information about the service setting and infrastructure for each of the intervention and control sites involved in the evaluation from site visits and various sources of routine data. We also analysed a dataset created specifically for the NIAP pilot sites in order to summarise activity levels, routes into hospital and patient characteristics for the intervention sites.
2.2.2 Workforce implications and issues of implementation and feasibility
We undertook pilot interviews and focus groups with members of staff involved in primary PCI and with staff working on the boundaries of the service (i.e. ambulance staff, bed managers) at one site. In addition, we conducted a questionnaire survey with staff. We then undertook similar surveys, stakeholder interviews, teamworking interviews and focus groups with staff at five further intervention sites. Ethnographic observation was also undertaken during site visits. A questionnaire was administered to all staff with a role within the catheter lab team at all of the six hospitals involved in the interviews plus one further intervention site.
2.2.3 Patient and carer evaluation
We undertook the patient and carer evaluation in three phases. The first phase involved face-to-face interviews with patients and carers from intervention sites to understand the key aspects of the patient and carer experience and enable us to develop a survey instrument. The second phase involved a postal survey of patients and carers at four intervention and four control sites. Finally, we undertook further interviews with patients and carers who had responded to the phase 2 survey to examine issues raised in phases 1 and 2 further.
2.2.4 Economic evaluation
We used data collected by the NIAP sites along with additional data from five control sites to estimate the costs and time to treatment of providing primary PCI and thrombolysis in routine NHS practice. Multilevel models were used to estimate the mean cost of thrombolysis and primary PCI, adjusting for patient characteristics and treatment location. These data were then used to populate and develop an existing cost-effectiveness model of primary PCI. This model uses synthesised evidence from 22 randomised trials to estimate the short-term rate of stroke, death, revascularisations and myocardial infarction and then extrapolates over the longer term using registry data. Mortality estimates are adjusted to take into account presentation delay and treatment delay, using data from NIAP and control sites. The model was thus used to estimate the cost effectiveness of operating a comprehensive primary PCI service compared to a thrombolysis-based service in terms of the incremental cost per QALY gained.

© Queen's Printer and Controller of HMSO 2007 27
© Queen's Printer and Controller of HMSO 2007 28
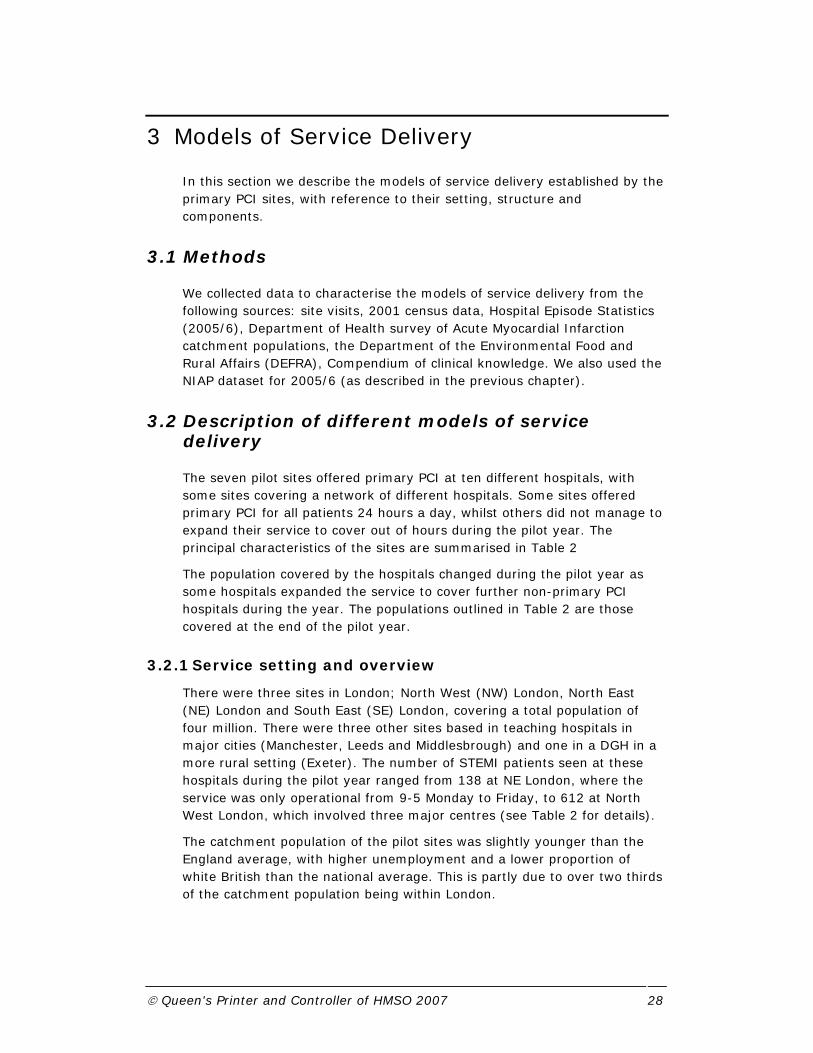
3 Models of Service Delivery
In this section we describe the models of service delivery established by the primary PCI sites, with reference to their setting, structure and components.
3.1 Methods
We collected data to characterise the models of service delivery from the following sources: site visits, 2001 census data, Hospital Episode Statistics (2005/6), Department of Health survey of Acute Myocardial Infarction catchment populations, the Department of the Environmental Food and Rural Affairs (DEFRA), Compendium of clinical knowledge. We also used the NIAP dataset for 2005/6 (as described in the previous chapter).
3.2 Description of different models of service delivery
The seven pilot sites offered primary PCI at ten different hospitals, with some sites covering a network of different hospitals. Some sites offered primary PCI for all patients 24 hours a day, whilst others did not manage to expand their service to cover out of hours during the pilot year. The principal characteristics of the sites are summarised in Table 2
The population covered by the hospitals changed during the pilot year as some hospitals expanded the service to cover further non-primary PCI hospitals during the year. The populations outlined in Table 2 are those covered at the end of the pilot year.
3.2.1 Service setting and overview
There were three sites in London; North West (NW) London, North East (NE) London and South East (SE) London, covering a total population of four million. There were three other sites based in teaching hospitals in major cities (Manchester, Leeds and Middlesbrough) and one in a DGH in a more rural setting (Exeter). The number of STEMI patients seen at these hospitals during the pilot year ranged from 138 at NE London, where the service was only operational from 9-5 Monday to Friday, to 612 at North West London, which involved three major centres (see Table 2 for details).
The catchment population of the pilot sites was slightly younger than the England average, with higher unemployment and a lower proportion of white British than the national average. This is partly due to over two thirds of the catchment population being within London.

© Queen's Printer and Controller of HMSO 2007 29
Table 2: NIAP pilot sites configuration and catchment areas Site name and hospitals
Catchment area a Model Primary PCI location and availability
Size b
NW London (St Mary’s, Harefield & Hammersmith)
Major urban 50.4% white British 5.7% over 75 4.0% unemployed CHD SMR 76
Multiple centre. 3 primary PCI sites plus 7 feeder hospitals
3 teaching hospitals, 2 with EDs and 1 tertiary referral centre with no ED. All offer primary PCI 24/7
1.7m
NE London London Chest Hospital (Barts)
Major urban 53.0% white British 5.7% over 75 5.1% unemployed CHD SMR 168
Single centre plus 6 feeder hospitals
Tertiary referral centre with no ED. primary PCI available 8-4 Mon-Fri.
1.6m
SE London (King’s College Hospital)
Major urban 62.6% white British 5.8% over 75 4.8% unemployed CHD SMR 82
Single centre plus 2 feeder hospitals
Teaching hospital with ED. primary PCI available 24/7
680k
Greater Manchester (Wythenshawe, Manchester Royal Infirmary)
Major urban 86.3% white British 7.1% over 75 3.6% unemployed CHD SMR 148
Multiple centre. 2 primary PCI sites plus feeder hospitals
2 teaching hospitals with EDs. primary PCI available 8-4 Mon-Fri
430k
Exeter (Royal Devon & Exeter)
Rural 96.6% white British 10.6% over 75 2.3% unemployed CHD SMR 66
Single centre District general hospital with ED. primary PCI available 24 hours during weekdays, no service weekends
340k
Leeds (Leeds General Infirmary).
Major urban 89.2% white British 7.2% over 75 3.3% unemployed CHD SMR 140
Single centre. 1 site with 1 feeder hospital
Teaching hospital with ED. primary PCI available 24/7
670k
Middlesbrough (James Cook)
Large urban 95.7% white British 6.8% over 75 5.3% unemployed CHD SMR 164
Single centre Teaching hospital with ED. primary PCI available 24/7
390k
NIAP average 69% white British, 6.4% over 75, 4.2% unemployed England 87% white British, 7.5% over 75, 3.3% unemployed
a Rural urban classification: DEFRA website http://www.defra.gov.uk/rural/ruralstats/rural-defn/LAClassification_datasetregions.xls 2001 census data. EV09 (% white British), UV04 (% over 75), UV28 (% unemployed). CHD morbidity: Mortality from acute myocardial infarction (ICD10 I21:I22), 2002-2004. Source: Compendium of Clinical and Health Indicators / Clinical and Health Outcomes Knowledge Base (www.nchod.nhs.uk or nww.nchod.nhs.uk)

© Queen's Printer and Controller of HMSO 2007 30
A wide range of referral routes were covered by the pilot sites, as outlined in Table 3.
• Eight hospitals received patients via their own emergency department (ED) while two were tertiary referral centres with no ED.
• Eight hospitals (including both tertiary centres) received patients from between one and six nearby EDs (“feeder sites”). However, two of these hospitals only started receiving these patients towards the end of the evaluation year and did not record data from these patients for the study.
The London Ambulance Service established a bypass service whereby they would take patients from anywhere within their catchment area directly to the nearest primary PCI site, bypassing the feeder ED. However, some patients were still taken to the feeder ED site first, either as a ‘brush-by’ whereby the patient did not leave the ambulance but was seen by a medical team in the ambulance and referred straight on, or occasionally the patient would be taken to the feeder ED department, assessed there and then transported to the primary PCI site. There was no bypass service available outside London and patients were transferred from the feeder ED departments following assessment.
During the pilot year many hospitals increased the proportion of ambulance patients with suspected STEMI who were bypassing the ED and being brought directly to the catheter lab area for assessment. The decision to take the patient to the catheter lab was made by the ambulance crew although two sites were able to seek confirmation of diagnosis by faxing (telemetering) ECGs taken in the ambulance to the coronary care unit at the hospital.
Table 3: NIAP pilot site overview and referral routes
Site
ID
1 2 3 4 5 6 7 8 9 10
Site overview: Primary PCI available 24/7 ● ● ● ● ● ● Teaching hospital ● ● ● ● ● ● ● ● ● Cardiothoracic facilities available ● ● ● ● ● ● ● ● ● Referral routes: Own ED ● ● ● ● ● ● ● ● Other referring ED ● ● ● ● ● ● ● ● Ambulance bypass for feeder sites ● ● ● ● ● ED bypass (patients direct to cath lab/CCU) ● ● ● ● ● ECGs telemetered to site ● ●

© Queen's Printer and Controller of HMSO 2007 31
3.2.2 Service infrastructure
The core primary PCI team called out of hours was generally made up of an interventional cardiologist, a cardiology middle grade doctor, a nurse, a radiographer and an ECG technician. Some sites also made use of resident nursing staff or had two nurses involved in some cases. Two hospitals did not include a radiographer within the team.
The core on-call team, size of team available and on-call rotas undertaken during the pilot year are detailed in Table 4. Interventional cardiologists were doing an on-call rota of between 1 in 4 and 1 in 10 with nursing staff doing a rota of between 1 in 5 (at a site who worked a 2 nurse on call system) and 1 in 10). Further discussion of the impact of team size and rotas can be found in chapter 4.
Table 4: Staff numbers and out of hours teams
1 2 3 4 5 6 7 8 9 10
CAPACITY– STAFF NUMBERS IN DEPARTMENT FOR PILOT YEAR (2005/6) Interventional cardiologist 10 9 5 19 5 5 6 7 Cardiology SpR 8 8 8 10 7 8 10 6 Junior medical staff 6 4 5 6 7 8 0 NA Cardiac nurses 12 6 12 35 9 16 11 15 Cardiac physiologists 8 6 20 10 6 9 N/A 12 Radiographer 5 0 18 8 21 9 10 9 Other 0 0 0 16 2 6 2 0
STANDARD OUT OF HOURS TEAM AND ON-CALL ARRANGEMENTS FOR PILOT YEAR (2005/6) Interventional cardiologist ● ● ●
No ou
t of h
ours
servi
ce av
ailab
le du
ring p
ilot y
ear
● ●
No ou
t of h
ours
servi
ce av
ailab
le du
ring p
ilot y
ear
No ou
t of h
ours
servi
ce av
ailab
le du
ring p
ilot y
ear
● ● Cardiology SpR ● ● ● ● ● ● Junior medical staff (resident) ● ● Nursing staff ● ● ● ● ● ● ●* ● ● Cardiac technicians ● ● ● ● ● ● ● Radiographer ● ● ● ● ● Other Cardiologist on-call rota Weekday 1 in 11 1 in 10 1 in 5 1 in 5 1 in 5 1 in 4 1 in 5 Weekend 1 in 6 1 in 6 1 in 5 1 in 5 1 in 5 1 in 7 - SpR on-call rota Weekday 1 in 8 1 in 8 1 in 10 1 in 7 1 in 8 1 in 6 Weekend 1 in 8 1 in 8 1 in 10 1 in 7 1 in 8 1 in 6 Nursing on-call rota Weekday 1 in 8 1 in 6 1 in 10 1 in 10 1 in 8 1 in 5* Weekend 1 in 8 1 in 6 1 in 10 1 in 10 1 in 8 1 in 4* Cardiac technician on-call rota Weekday 1 in 8 1 in 6 1 in 10 1 in 6 1 in 6/7 1 in 7 Weekend 1 in 8 1 in 6 1 in 10 1 in 6 1 in 6/7 1 in 7 Radiographer on-call rota Weekday 1 in 6 N/A 1 in 18 1 in 14 1 in 6/7 1 in 5 Weekend 1 in 6 N/A 1 in 18 1 in 14 1 in 6/7 1 in 5

© Queen's Printer and Controller of HMSO 2007 32
3.2.3 Service activity levels
Table 5 shows the size of the facilities available and the service activity levels for emergency PCI and CABG for each hospital. Service activity levels are those reported within the hospital episode statistics for 2005/6. Emergency PCI admissions includes both primary and rescue PCI.
Table 5: Site infrastructure and service activity levels
Site
ID
1 2 3 4 5 6 7 8 9 10
Service infrastructure: CLs available for primary PCI 3 2 3 3 3 3 4 3 5 2 CCU beds 5 5 12 12 6 14 18 10 7 Cardiology beds 22 19 42 32 18 41 32 56 37 Cardiothoracic beds 22 19 44 25 18 38 18 20 0 Other cardiology/c~thoracic HDU beds 5 10 0 16 15 10 8 0 0
Service activity levels (HES): CABG admissions 2005/6 297 262 880 817 284 434 375 506 512 0 Emergency PCI admissions 2005/6 269 273 716 47 234 249 176 118 385 194 All PCI admissions 2005/6 614 1516 2452 3253 1100 1145 1640 1186 2563 512
3.3 Results from the NIAP dataset
It is important to note that results below differ slightly from those reported within the NIAP interim report [DH Vascular Programme Team 2008] as we have not included the control site (Dryburn) or patients who did not go to one of the ten intervention hospitals within our figures.
3.3.1 Patient characteristics
A total of 2,072 patients with STEMI were identified for the ten hospitals below during the year of evaluation: 71% of the patients were male and the mean age was 64 (range 24-104) (see Table 6). The mean age ranged from 61 to 65 years at all but one site that had a significantly older population (mean 70). The ethnic mix of the population differed considerably between sites, ranging from 57% to 99% white British. This reflects the ethnic mix for the populations covered (see Table 2)

© Queen's Printer and Controller of HMSO 2007 33
Table 6: Characteristics of patients from NIAP database
Site
ID
1 2 3 4 5 6 7 8 9 10
TOTA
L/ AV
ERAG
E
Age (mean, range) 63
25-92 61
26-92 62
29-90 62
26-86 62
30-94 63
32-97 64
28-89 63
37-95 65
32-97 70
29-104 64
24-104 Sex (% male) 73 74 74 75 77 70 71 68 65 68 71 Ethnic origin (% Caucasian) 57 58 63 N/A 84 97 61 95 94 99 81 Previous myocardial infarction (%) 23 18 12 9 16 15 18 15 14 19 16
3.3.2 Route into hospital
Most patients (94%) were out of hospital at the time of onset of their heart attack, and 80% of these activated the emergency services (either via their GP or calling 999 direct) and were brought to hospital by ambulance. Most of the remainder made their own way to hospital and were admitted via the ED. A greater proportion of patients who went direct to the primary PCI site travelled by ambulance, as some of these patients would have been direct ambulance bypass patients. Almost 6% of patients were already inpatients in hospital when their symptoms began.
Figure 2: Method of admission to hospital
Method of admission for transfer or direct patients
65%
28%
11%
5% 6%
82%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Patients transferred to PPCI centre Patients direct to PPCI centre
% o
f all
patie
nts
adm
itted
OtherAlready inpatientSelf-present to A&EAmbulance
© Queen's Printer and Controller of HMSO 2007 34
3.3.3 Patient treatment pathways
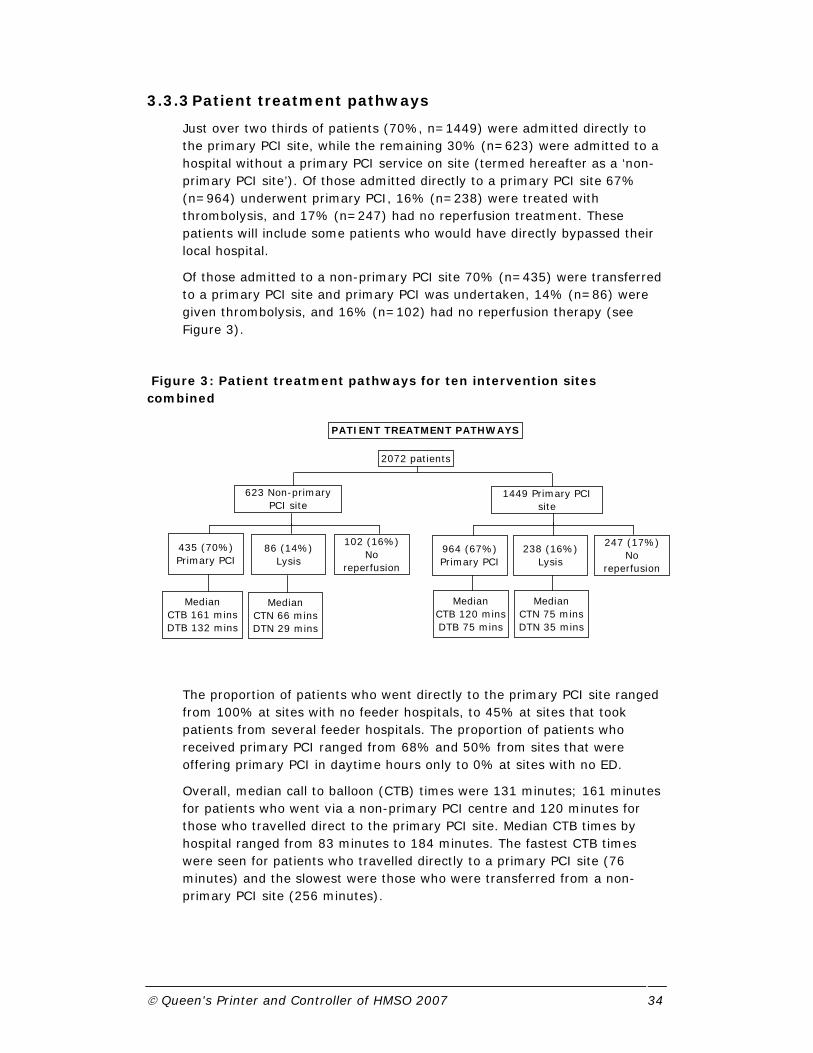
Just over two thirds of patients (70%, n=1449) were admitted directly to the primary PCI site, while the remaining 30% (n=623) were admitted to a hospital without a primary PCI service on site (termed hereafter as a ‘non- primary PCI site’). Of those admitted directly to a primary PCI site 67% (n=964) underwent primary PCI, 16% (n=238) were treated with thrombolysis, and 17% (n=247) had no reperfusion treatment. These patients will include some patients who would have directly bypassed their local hospital.
Of those admitted to a non-primary PCI site 70% (n=435) were transferred to a primary PCI site and primary PCI was undertaken, 14% (n=86) were given thrombolysis, and 16% (n=102) had no reperfusion therapy (see Figure 3).
Figure 3: Patient treatment pathways for ten intervention sites combined
The proportion of patients who went directly to the primary PCI site ranged from 100% at sites with no feeder hospitals, to 45% at sites that took patients from several feeder hospitals. The proportion of patients who received primary PCI ranged from 68% and 50% from sites that were offering primary PCI in daytime hours only to 0% at sites with no ED.
Overall, median call to balloon (CTB) times were 131 minutes; 161 minutes for patients who went via a non-primary PCI centre and 120 minutes for those who travelled direct to the primary PCI site. Median CTB times by hospital ranged from 83 minutes to 184 minutes. The fastest CTB times were seen for patients who travelled directly to a primary PCI site (76 minutes) and the slowest were those who were transferred from a non-primary PCI site (256 minutes).
2072 patients
623 Non-primary PCI site
1449 Primary PCI site
435 (70%) Primary PCI
86 (14%) Lysis
102 (16%) No
reperfusion
238 (16%) Lysis
964 (67%) Primary PCI
247 (17%) No
reperfusion
Median CTB 161 minsDTB 132 mins
Median CTN 66 minsDTN 29 mins
Median CTB 120 minsDTB 75 mins
Median CTN 75 minsDTN 35 mins
PATIENT TREATMENT PATHWAYS
© Queen's Printer and Controller of HMSO 2007 35
Table 7: Patient pathways and call times by hospital
Site
ID
1 2 3 4 5 6 7 8 9 10
TOTA
L
Direct admissions and transfers Direct to primary PCI centre 72 128 123 62 143 188 116 104 173 266 1375 Inter-hospital transfer 53 159 67 76 113 42 1 1 106 1 619 Inpatient 6 2 0 0 0 17 0 2 16 29 72 Other/missing 1 0 1 0 0 0 0 0 3 1 6 % patients from feeder hospitals 40% 55% 35% 55% 45% 17% 0% 0% 36% 0% 30
Treatment received primary PCI 95 214 180 115 178 168 46 29 241 133 1399 Thrombolysis 11 14 0 5 13 42 57 73 33 76 324 No reperfusion 26 61 11 18 65 37 14 5 24 88 349 Total STEMI 132 289 191 138 256 247 117 107 298 297 2072
Call times Overall CTB times (median)** 184 140 83 126 143 137 131 117 138 134 131 Direct to primary PCI centre 156 119 76 100 117 133 131 117 132 134 120 Inter-hospital transfer 256 191 159 142 190 ** - - 147 - 161 Overall DTB times (median)** 150 101 26 45 102 96 116 78 99 79 93 Direct to primary PCI centre 119 58 20 - 68 94 116 78 96 79 Inter-hospital transfer 225 147 104 116 160 ** - - 107 - CTN times (median)** - - - - - 68 57 57 91 95 DTN times (median)** - - - - - 32 32 28 49 43
**Figures only given where>20 cases
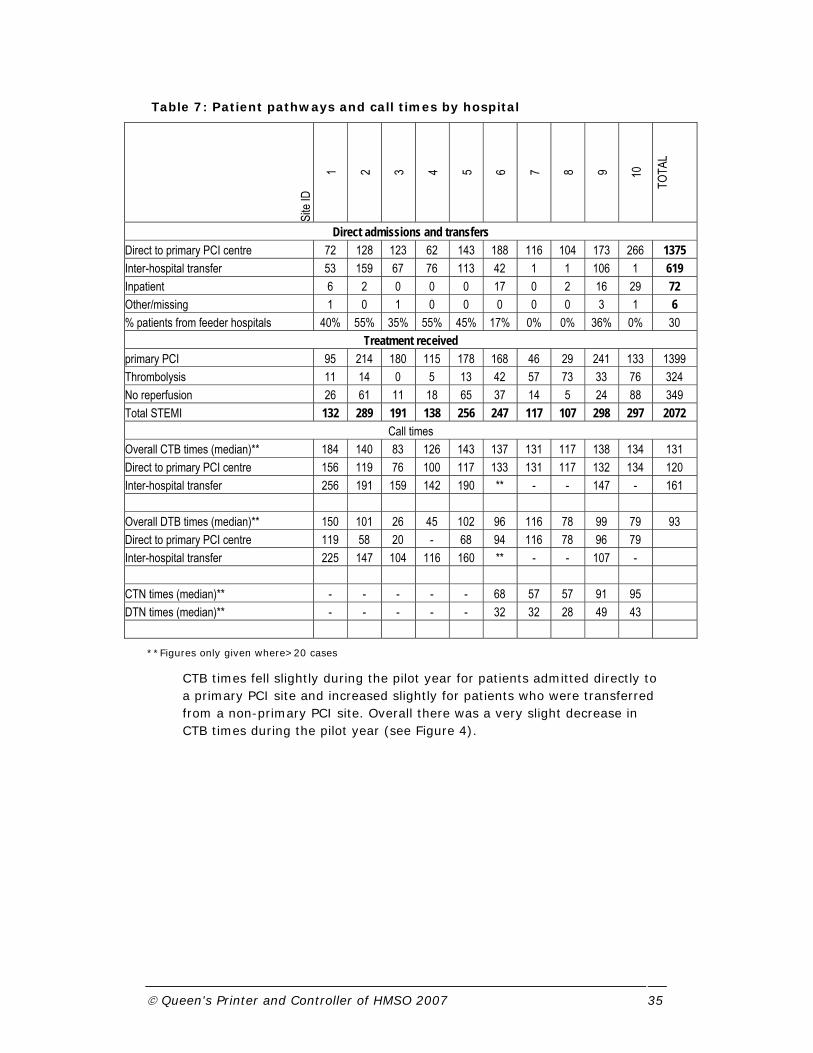
CTB times fell slightly during the pilot year for patients admitted directly to a primary PCI site and increased slightly for patients who were transferred from a non-primary PCI site. Overall there was a very slight decrease in CTB times during the pilot year (see Figure 4).

© Queen's Printer and Controller of HMSO 2007 36
Figure 4: Call to balloon times by month
3.3.4 Place of assessment
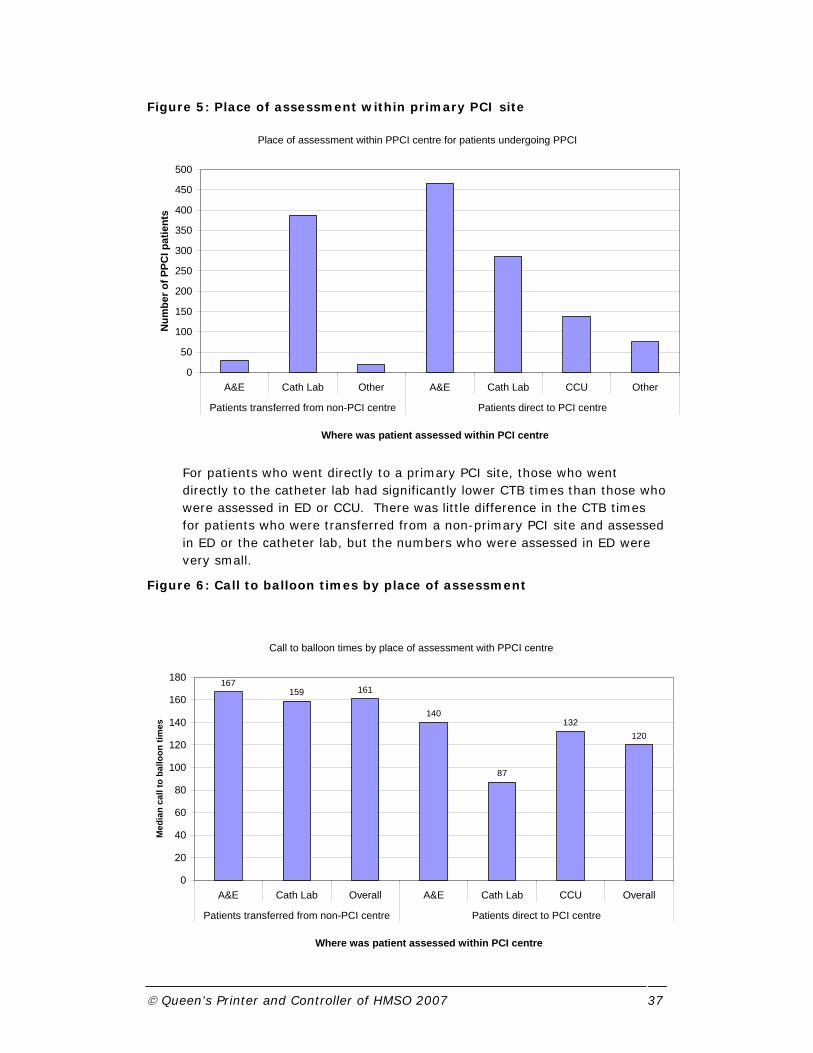
The location of patient assessment has been suggested as a key variable in improving CTB times. The majority of patients who were transferred from a non-PCI site were assessed within the catheter lab once they reached the primary PCI site (see Figure 5). Almost 50% of patients who went directly to the primary PCI site were seen in ED, although 30% were taken direct to the catheter lab.
Call to balloon times for NIAP patients - direct admissions or transfer
0
20
40
60
80
100
120
140
160
180
200
04/2005 05/2005 06/2005 07/2005 08/2005 09/2005 10/2005 11/2005 12/2005 01/2006 02/2006 03/2006
Month
CTB
tim
e (m
inut
es)
Transfer Direct Overall
© Queen's Printer and Controller of HMSO 2007 37
Figure 5: Place of assessment within primary PCI site
For patients who went directly to a primary PCI site, those who went directly to the catheter lab had significantly lower CTB times than those who were assessed in ED or CCU. There was little difference in the CTB times for patients who were transferred from a non-primary PCI site and assessed in ED or the catheter lab, but the numbers who were assessed in ED were very small.
Figure 6: Call to balloon times by place of assessment
Call to balloon times by place of assessment with PPCI centre
167159 161
140
87
132120
0
20
40
60
80
100
120
140
160
180
A&E Cath Lab Overall A&E Cath Lab CCU Overall
Patients transferred from non-PCI centre Patients direct to PCI centre
Where was patient assessed within PCI centre
Med
ian
call
to b
allo
on ti
mes
Place of assessment within PPCI centre for patients undergoing PPCI
0
50
100
150
200
250
300
350
400
450
500
A&E Cath Lab Other A&E Cath Lab CCU Other
Patients transferred from non-PCI centre Patients direct to PCI centre
Where was patient assessed within PCI centre
Num
ber o
f PPC
I pat
ient
s

© Queen's Printer and Controller of HMSO 2007 38
The proportion of patients who were assessed in the catheter lab ranged from zero to almost 100% in hospitals with no ED.
Table 8: Place of assessment by hospital
Site
ID
1 2 3 4 5 6 7 8 9 10
TOTA
L
Where patient was first assessed Catheter lab (%) 14 63 98 94 70 8 0 1 30 8 40 ED (%) 61 31 0 1 28 27 98 98 55 48 40 CCU (%) 2 5 1 4 1 51 0 0 5 22 11 Other 23 1 1 1 1 14 2 1 10 22 9
3.3.5 Outcomes
Overall in-hospital mortality for this population was 6.8%. The mean length of stay was just under six days, five of which was spent at the primary PCI site with a mean of one day at the hospital that the patients were repatriated to (non-primary PCI hospital).
Site
ID
1 2 3 4 5 6 7 8 9 10
TOTA
L
Outcomes In-hospital mortality (%) 10.6 6.2 3.7 2.2 6.3 6.5 8.5 2.8 5.7 12.5 6.8 LOS (mean, capped at 30 days) 5.0 5.4 5.4 4.0 4.5 6.6 7.1 5.8 5.1 7.7 5.7 LOS at primary PCI hospital (mean) 4.3 2.9 2.9 4 3.3 6.1 7.1 5.8 4.3 7.7 4.8 LOS at non-primary PCI hospital (mean) 0.7 2.5 2.5 0 1.2 0.5 0 0 0.8 0 0.9
3.4 Discussion
There was considerable variation in the different models of service delivery offered by the ten intervention sites. Although most hospitals were running a 24/7 service and had expanded the service to outside their own catchment area by the end of the pilot year, there were hospitals that were still running the service in-hours only and dealt with patients only within their catchment area. As a result, the proportion of patients receiving primary PCI differed along with the volumes of primary PCI undertaken.
The majority of patients came into the primary PCI site directly; this included patients who lived within the hospital catchment area and those who were brought in by ambulance and bypassed feeder sites. These

© Queen's Printer and Controller of HMSO 2007 39
patients had considerably lower CTB times than those who were first admitted to a non-primary PCI hospital before being transferred. A similar proportion of patients were given primary PCI (68%) and thrombolysis (16%) whether they went to the PCI site directly or were transferred. This suggests that patients were being referred on for primary PCI once they had been seen in the feeder hospitals.
Lower CTB times were strongly associated with the place of assessment within the primary PCI site. Patients who went directly to the catheter lab and bypassed the ED had CTN times of almost an hour less than those who were assessed in the ED. Le May et al. (2008) recently found similar delays of around one hour when patients were referred from emergency physicians rather than being transferred directly to the catheter lab by paramedics.
All of the London sites were able to take advantage of paramedic assessment of patients, enabling patients to bypass local hospitals or to bring the patients directly to the catheter lab. However, there was still considerable variation between sites as to whether patients were assessed within the catheter lab or brought into the ED for assessment. Similarly, some feeder hospitals would allow direct bypass of their patients whilst others were still assessing patients locally before transferring patients on. These issues are discussed further in chapter 4.
The analysis of the NIAP data suggests that primary PCI is feasible in England, can be provided to a wide variety of patients with STEMI in a range of different settings, and produces similar outcomes to those reported in randomised trials. However, not all the sites were able to establish a 24/7 service or extend the service beyond their immediate catchment area. Analysis of CTB times indicates there to be a clear need for sites to consider bypassing the ED and CCU in favour of transporting patients directly to the catheter lab in order to significantly reduce treatment delays. Further data from the NIAP database will be reported within the economic evaluation chapter of this report (chapter 6).

© Queen's Printer and Controller of HMSO 2007 40
4 Workforce Implications and Issues of Implementation and Feasibility
4.1 Background
While research projects exploring primary PCI have focused on the clinical benefits of primary PCI and the availability of cardiologists and cardiac nurses (Keeley & Grimes, 2004; Fye, 2004; Pearson et al., 2004), there has been little work examining the workforce and organisational implications of providing this type of service. Further, most of this work was undertaken in the US where health care organisations operate differently to the UK. The lack of research into the broader implications of offering emergency intervention for STEMI is surprising as such a service in a major investment for the hospitals concerned and many medical and non-medical staff are involved in its development. The service itself crosses departmental and organisational boundaries between primary and secondary care and involves a number of diverse agencies (such as Ambulance Trusts and community rehabilitation services). This study was designed address this imbalance and focused on four research areas:
• To describe the implementation and feasibility issues of establishing the service – these will be described as start-up issues;
• To examine the facilitators and barriers to setting-up and developing the service;
• To measure the effect of providing the service on the team and boundary relationships – these will be described as knock-on effects to the local cardiology community;
• To appreciate the consequences to other services – these will be described as knock-on effects to the wider health community.
4.2 Hospitals involved in data collection
Seven hospitals contributed to the data collection for the organisational analysis. The characteristics of these hospitals and their workload in terms of primary PCI at the time of study was described in Chapter 3 (see Table 2).
It was difficult to arrange interviews and focus groups in one hospital around their day-to-day working. Here, staff members contributed to the questionnaire survey alone.
One hospital agreed to be the pilot enabling development of methods of data collection. Each hospital will be treated as an individual case study and will not be named in this report.
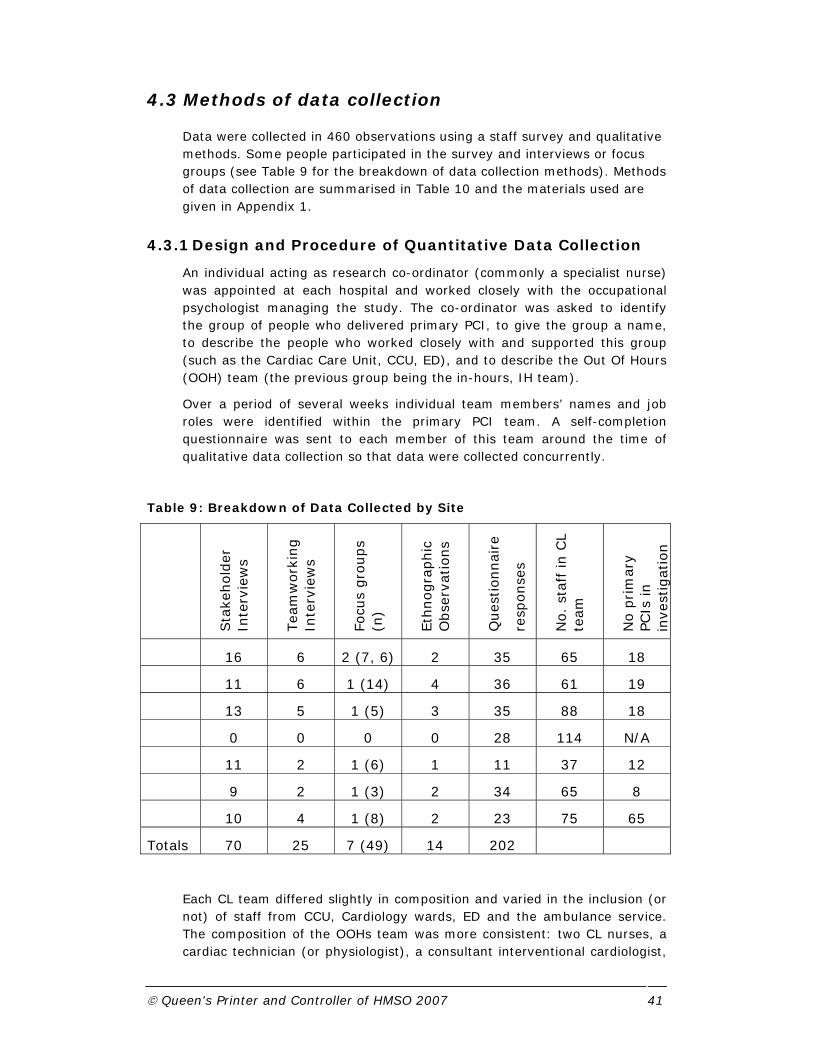
© Queen's Printer and Controller of HMSO 2007 41
4.3 Methods of data collection
Data were collected in 460 observations using a staff survey and qualitative methods. Some people participated in the survey and interviews or focus groups (see Table 9 for the breakdown of data collection methods). Methods of data collection are summarised in Table 10 and the materials used are given in Appendix 1.
4.3.1 Design and Procedure of Quantitative Data Collection
An individual acting as research co-ordinator (commonly a specialist nurse) was appointed at each hospital and worked closely with the occupational psychologist managing the study. The co-ordinator was asked to identify the group of people who delivered primary PCI, to give the group a name, to describe the people who worked closely with and supported this group (such as the Cardiac Care Unit, CCU, ED), and to describe the Out Of Hours (OOH) team (the previous group being the in-hours, IH team).
Over a period of several weeks individual team members’ names and job roles were identified within the primary PCI team. A self-completion questionnaire was sent to each member of this team around the time of qualitative data collection so that data were collected concurrently.
Table 9: Breakdown of Data Collected by Site
Sta
kehold
er
Inte
rvie
ws
Tea
mw
ork
ing
Inte
rvie
ws
Focu
s gro
ups
(n)
Eth
nogra
phic
O
bse
rvat
ions
Ques
tionnai
re
resp
onse
s
No.
staf
f in
CL
team
No p
rim
ary
PCIs
in
inve
stig
atio
n
16 6 2 (7, 6) 2 35 65 18
11 6 1 (14) 4 36 61 19
13 5 1 (5) 3 35 88 18
0 0 0 0 28 114 N/A
11 2 1 (6) 1 11 37 12
9 2 1 (3) 2 34 65 8
10 4 1 (8) 2 23 75 65
Totals 70 25 7 (49) 14 202
Each CL team differed slightly in composition and varied in the inclusion (or not) of staff from CCU, Cardiology wards, ED and the ambulance service. The composition of the OOHs team was more consistent: two CL nurses, a cardiac technician (or physiologist), a consultant interventional cardiologist,

© Queen's Printer and Controller of HMSO 2007 42
a Specialist Registrar (SpR) and an angio-radiographer (one site hospital did not employ radiographers).
Our starting point for this inquiry was the supposition that undertaking emergency primary PCI procedures may constitute a different type of work to traditional cardiology work. We therefore designed a survey to examine differences between people’s experiences when performing emergency primary PCI work and traditional cardiology work (see Table 10).
4.3.2 Design and Procedure of Qualitative Data Collection
We selected qualitative methods to complement quantitative data collection that were relevant and acceptable to participants. These included face-to-face interviews with stakeholders within and outside the cardiology department, focus groups, teamworking interviews and ethnographic observation of CLs. As individuals were identified within the primary PCI team or as stakeholders outside the team, appointments were made over a convenient period for data collection within the department.
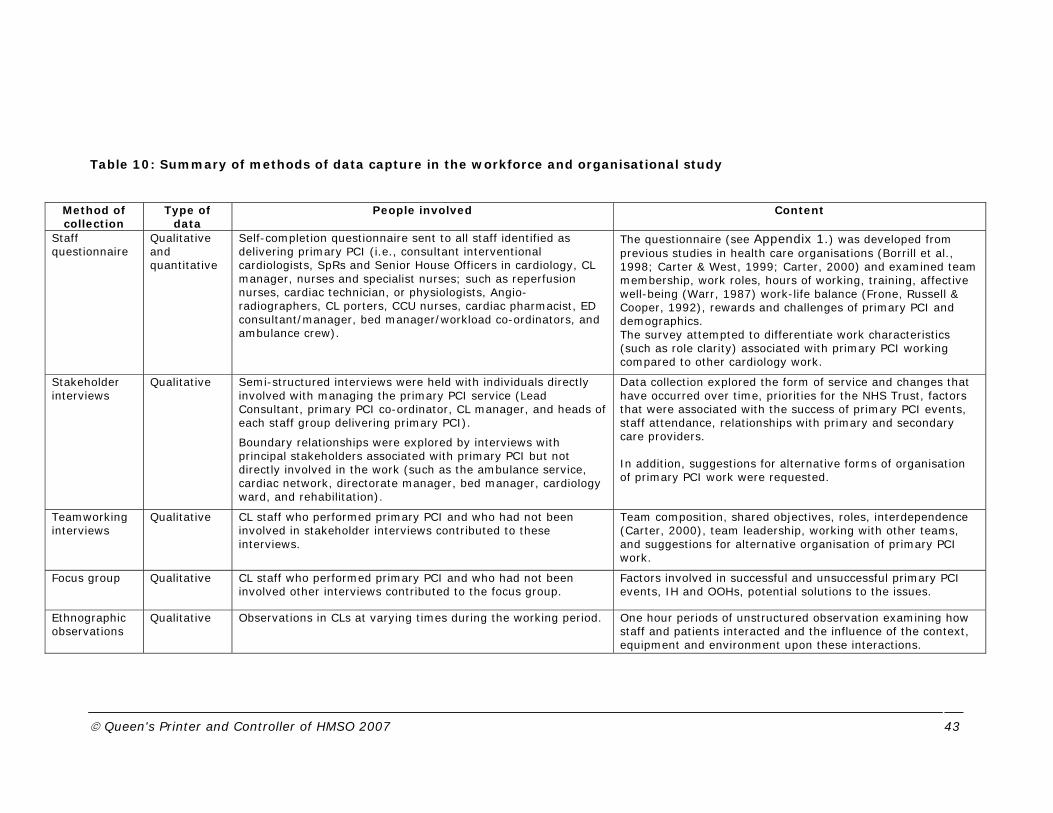
© Queen's Printer and Controller of HMSO 2007 43
Table 10: Summary of methods of data capture in the workforce and organisational study
Method of collection
Type of data
People involved Content
Staff questionnaire
Qualitative and quantitative
Self-completion questionnaire sent to all staff identified as delivering primary PCI (i.e., consultant interventional cardiologists, SpRs and Senior House Officers in cardiology, CL manager, nurses and specialist nurses; such as reperfusion nurses, cardiac technician, or physiologists, Angio-radiographers, CL porters, CCU nurses, cardiac pharmacist, ED consultant/manager, bed manager/workload co-ordinators, and ambulance crew).
The questionnaire (see Appendix 1.) was developed from previous studies in health care organisations (Borrill et al., 1998; Carter & West, 1999; Carter, 2000) and examined team membership, work roles, hours of working, training, affective well-being (Warr, 1987) work-life balance (Frone, Russell & Cooper, 1992), rewards and challenges of primary PCI and demographics. The survey attempted to differentiate work characteristics (such as role clarity) associated with primary PCI working compared to other cardiology work.
Stakeholder interviews
Qualitative Semi-structured interviews were held with individuals directly involved with managing the primary PCI service (Lead Consultant, primary PCI co-ordinator, CL manager, and heads of each staff group delivering primary PCI).
Boundary relationships were explored by interviews with principal stakeholders associated with primary PCI but not directly involved in the work (such as the ambulance service, cardiac network, directorate manager, bed manager, cardiology ward, and rehabilitation).
Data collection explored the form of service and changes that have occurred over time, priorities for the NHS Trust, factors that were associated with the success of primary PCI events, staff attendance, relationships with primary and secondary care providers. In addition, suggestions for alternative forms of organisation of primary PCI work were requested.
Teamworking interviews
Qualitative CL staff who performed primary PCI and who had not been involved in stakeholder interviews contributed to these interviews.
Team composition, shared objectives, roles, interdependence (Carter, 2000), team leadership, working with other teams, and suggestions for alternative organisation of primary PCI work.
Focus group
Qualitative CL staff who performed primary PCI and who had not been involved other interviews contributed to the focus group.
Factors involved in successful and unsuccessful primary PCI events, IH and OOHs, potential solutions to the issues.
Ethnographic observations
Qualitative Observations in CLs at varying times during the working period. One hour periods of unstructured observation examining how staff and patients interacted and the influence of the context, equipment and environment upon these interactions.

© Queen's Printer and Controller of HMSO 2007 44
4.3.3 Pilot Hospital Research
Research at the initial hospital (undertaken in November 2006) provided the opportunity to pilot interview schedules and focus group discussions. A wide range of participants were chosen to participate (16 stakeholder interviews, six teamworking interviews, two focus groups with primary PCI staff and staff on the boundary of primary PCI work such as general radiography) over four days. Questionnaires were distributed just before the site visit so that the researchers would act as a prompt to staff to complete the questionnaire.
We found some repetition of data collected at the initial site so fewer participants were chosen at follow-on research sites and only the focus group with primary PCI staff was held reducing the time in each department to two days. Staff working on the boundaries of the primary PCI service (such as rehabilitation and bed managers) were interviewed.
In the pilot study, staff were extremely supportive of running a primary PCI service and few if any negative voices were heard. Effort was made at follow-on sites to identify individuals or groups who described alternative viewpoints allowing negative voices to be heard.
4.3.4 Main Hospital Research
Data collection across the remaining five hospitals was carried out between June 2007 and August 2007, this relatively short time period ensuring the overall climate of operation would be similar enabling comparisons across sites to be made.
4.3.4.1 Sampling
Participants were asked to volunteer to take part in the research by the co-ordinator or the occupational psychologist. Individuals were selected for interview or focus group depending on their job role and proximity to the group providing primary PCI.
Prior to taking part in interviews or focus groups, participants were provided with an information sheet outlining the research project (see Appendix 1.). Where practical a two-day site visit was conducted and where key individuals were absent telephone interviews were undertaken at a later date.
Participation was voluntary and at the beginning of each interview and focus group the overall aims of the study were outlined and participants informed of their rights to anonymity, confidentiality and opportunity to withdraw from the study at any stage (see interview schedule, Appendix 1.). Participants were asked to read and sign a consent form indicating their agreement to be involved in the research (see Appendix 1.).

© Queen's Printer and Controller of HMSO 2007 45
4.3.4.2 Interviews
The interviews lasted approximately one hour and were conducted by trained researchers using identical interview schedules. All the interviews, except for the telephone interviews, took place on-site in rooms away from CLs to provide privacy. Audio taping was not used in order to increase participants’ confidence in the confidentiality of data collected.
Member checking was used to record and validate participants’ responses, in line with recommended good practice (Bryman & Bell, 2003). During the interview the researcher repeated, summarised, or paraphrased information obtained from the interviewee to ensure correct understanding of the material before recording themes on the interview sheet. Member checking is used to increase credibility within qualitative research, ensuring that the participant agrees with the recorded response. In keeping with the ethos of reflexivity within qualitative research, researchers recorded field notes immediately at the end of each interview. Information such as the interviewer’s perception of the rapport between interviewer and interviewee and any learning points about the overall interview process were noted and referred to during the analyses.
4.3.4.3 Focus Groups
Focus groups were used as they allow respondents to react to and build upon responses made by others in the group, thus facilitating in-depth discussion of a topic to complement data gathered by other more structured methods. The group dynamics involved in a focus group have been found to be particularly useful for allowing participants to develop solutions to problems (Bryman & Bell, 2003) and this reinforced the choice of this method of data collection as we were interested in identifying problems and possible means to overcome them.
Focus group facilitators introduced the overall aims of the project and emphasised confidentiality and anonymity of the data collected prior to each session commencing. The introduction was standardised to aid comparisons across sites (see Appendix 1.).
Focus groups were undertaken as early in a site visit as possible to enable people to engage with the research team and feel more relaxed about the data gathering process.
4.3.4.4 Ethnographic Observation
Researchers undertook some direct observation of CL work at each site. We watched a variety of non-emergency PCI procedures and observed the CL area. This enabled the researchers to familiarise themselves with CL work in general and to build a picture of what it was like to work in CL at that specific site. On two occasions a primary PCI occurred whilst researchers were in the CL offering an ideal opportunity to observe this work at close hand.

© Queen's Printer and Controller of HMSO 2007 46
Observation provides another form of data collection that can validate participant self-report (see Appendix 1. for details). Where self-report themes are supported by ethnographic observation “this was also observed” will be noted.
4.3.4.5 Qualitative data analysis
We used a Thematic Analysis approach (Braun & Clarke, 2006) to analyse the qualitative data whereby analysis was driven by the research questions of interest. In addition, sub-ordinate themes were derived using an inductive approach, building themes directly from the data.
Having read all the data a broad coding template was developed from data provided at the pilot hospital. Initial ideas or themes relevant to the research questions were recorded against sections of the ‘transcripts’ and then grouped together under broader headings, clustering similar issues together. Researcher judgement was employed in determining themes, considering the research questions at all times.
A second researcher read through all the data and began a comparison coding exercise (inter-rater agreement), finding agreement on coding in approximately 90% of cases. As a result of this, a coding template was developed (see Appendix 1.) which consisted of super-ordinate and sub-ordinate themes. These themes were mapped against the original research questions.
In order to gain multiple perspectives on the data, analyses were undertaken by three researchers, using the initial coding template as a broad guide. All researchers involved in the analysis phase were involved in the data collection phase.
Researchers developed individualised templates for each site (see Appendix 1.), reflecting the themes and issues that were identified during interviews and focus groups. Once each case study template was produced comparisons were made across sites of similarities and disparities in themes.
Templates from each hospital were examined for similarity and difference of recorded theme. Four themes were identified through the analysis: Staffing (all aspects human resource management including training, management style and teamworking); Resourcing (all aspects of non-human resources such as equipment, drugs and stents); Pathway (process that begins with public and primary care education and ends in effective rehabilitation); and Change management (all process aimed at managing a change of service delivery along with the maintenance of staff motivation). These headings are used to organise the rich picture of data that was collected.

© Queen's Printer and Controller of HMSO 2007 47
4.4 Results
4.4.1 Reporting of data
Findings taken from the quantitative element of the staff survey will be reported when they are statistically significant. Occasionally a non-significant finding will be noted if it contributes to overall understanding of the data. Seven hospitals contributed the survey.
Qualitative data was obtained from interviews, focus groups and free text contributions to the questionnaire survey. These data cannot be interpreted by statistical analyses or rating scales; however, they can be seen as a series of common themes. If a particular theme is reported by staff at a number of hospitals it implies this may be a common experience. Alternatively, a theme described by staff at one hospital is no less important as it may be describing a unique experience that may have important implications. Six hospitals contributed to the interviews and focus groups.
In the findings the number of hospitals reporting a particular theme will be reported (e.g., 3/6 meaning staff at three of the six hospitals reported this theme). Any quotes that are “surrounded by double quotation marks” are not our wording but the words of the participant.
4.4.2 Introduction to findings
Data were collected in 446 observations from seven hospitals. In addition, 14 ethnographic observations of CL working were undertaken.
Two hundred and two staff from seven hospitals working in all occupational groups contributed to the staff survey (66% were female, 47% had children living at home, 80% were born in Britain, with 82% being white).
One hundred and forty-four staff working in all occupational groups from six hospitals contributed to interviews and focus groups conducted on-site. All staff participating in the study were identified by a local research co-ordinator as being actively involved in primary PCI or working on the boundary of the CL service in the heart attack pathway (from ambulance to rehabilitation).
The workload of primary PCI cases varied across the hospitals (between 8-65 cases in the month of study, see Table 7 in chapter 3). However, with the exception of one hospital that saw 65 cases in the month of study most hospitals saw less than 20 cases per month.
We will describe the findings of this study by integrating the quantitative and qualitative outputs. Four specific themes arose from our analyses: Staffing; Resources; Pathway; and Change Management. We shall use these themes to structure our findings and discussion.

© Queen's Printer and Controller of HMSO 2007 48
4.4.3 Staffing
Examination of quantitative and qualitative data shows several areas of concern about staffing.
The qualitative inquiry asked participants about various stages of development of primary PCI working and the heart attack pathway (start-up, facilitators and barriers to working, knock-on effects to cardiology and other services). These are shown in Table 11. The main areas of concern are having sufficient, experienced staff to undertake the work at start-up, providing the team with on-going training and effective management. The heavy nature of primary PCI work was described. However, staff at all hospitals described the intrinsic satisfaction they gained doing this type of work and how this motivated them to want to develop the service further.
The main areas of potential concern for staff relate to role clarity, training, work-family relationships and attitudes towards change.
4.4.3.1 Work Role
We asked staff what percentage of time they spent doing primary PCI work. The average time spent of primary PCI work as 22%, with the majority of the sample (85%) spending less than half their time on primary PCI work. Therefore, primary PCI is not the major part of most peoples’ work.
Generally role perceptions did not vary greatly for the two types of work; staff contributed to both emergency and elective work (this was also observed). The following quotation describes this point:
“There is no real team doing primary PCI; everyone in the department participates in all cases: elective and acute PCIs, paediatrics, EPS and pacing”.
Differences were seen in role clarity and feedback in primary PCI compared to other cardiology work; but only amongst those for whom PCI is at least 50% of their role. The people who see primary PCI as a main part of their work role experience greater role clarity, more feedback and less role conflict when doing this work compared to other cardiology work. Ethnographic observation saw a group of staff working closely together and communicating effectively to undertake the task, communicate with the patient and clear the CL for the next patient.
Further, the extent of training on primary PCI affected the level of role clarity; those who had some specialist training were more likely to perceive their roles to be well defined. For example, they are more likely to know what they were expected to do and their responsibilities; whereas those without specialist training were typically likely to see their roles as less clearly defined.
The following quotations illustrate the importance of role clarity:
“The team roles involved in this work need to be very clearly defined as it can be a free for all when patient arrives”.
© Queen's Printer and Controller of HMSO 2007 49
“There is a disorganised approach to this work – there is no clearly defined PCI team, patients are allocated to whichever lab is free at time, there are no defined roles, lots of additional paperwork and it is all very frustrating!!”
Further inspection of qualitative analyses revealed behaviours indicative of a lack of role clarity and strategies to improve role clarity. Staff described behaviours indicative of poor role clarity such as duplication of work (e.g. the search for beds for emergency patients being done by more than one member of CL staff) or too many nurses trying to do the same thing in CL. Ethnographic observation saw staff waiting for equipment, searching for information and equipment and some miscommunication.
Staff at two hospitals specifically mentioned the development of written protocols for primary PCI procedures to strengthen and develop role clarity. In addition, conversations were described about clarification of job roles with boundary personnel (such as who should monitor a patient’s vital signs once outside the ambulance and how a patient is handed over post-primary PCI to CCU staff).
Qualitative analyses revealed difficulties maintaining adequate staffing. Many of these problems relate to managing a group of staff in a fair and equitable manner. While several hospitals noted that they had a manager in charge of CL (or a co-ordinator) this individual was usually a nurse with either CL or other specialist responsibilities. Co-ordinating staff frequently stated that they did not have time in the working day for “managerial activities”. Only one hospital had a dedicated manager whose role was to manage and co-ordinate medical and non-medical staff balancing elective and emergency scheduling in the CL. Given the complexity of these tasks and the need to develop fair and equitable rotas a dedicated managerial role, without clinical responsibilities, would seem the best solution.
A further staffing issue was the heavy nature of CL working requiring wearing of lead aprons and maintaining a high degree of concentration. For many people this is the challenge of primary PCI working, but when there are more patients, frequent OOHs working and inadequate rest this becomes more difficult. At these times that the differences in pay and conditions between staff becomes highlighted. Staff in the OOH team get paid differently for on-call work and often have different periods of rest after OOHs working. Staff seem prepared to tolerate this during the set-up of the service but once the frequency of primary PCI patients increases the lack of harmonisation, particularly across the OOHs team, becomes more of an issue. Add to this extra hours of working to compensate for the delays emergency patients make in elective lists staff begin to feel aggrieved. It was frequently stated by staff that the service was running on their good will and that is was not sustainable.

© Queen's Printer and Controller of HMSO 2007 50
Table 11. Summary of qualitative comments from staff interviews and focus groups about Staffing - note 4.3.1 for data interpretation
START – UP FACILITATORS BARRIERS KNOCK – ON CARDIOLOGY
KNOCK – ON OTHER SERVICES
Ensure sufficient experienced staff to run the service - 6/6 Commence with 24/7 service - 5/6 or run a regional service - 2/6 Ensure there is an adequate budget for on-call working - 6/6 Extend hours of working (IH) from 8-8 - 2/6 CL staff have pride and ownership of the service that will drive its development but this requires nurture (e.g., flexible but fair rotas balancing resources and enthusiasm) 5/6
Strengthen the team - 6/6 by having: adequate staffing (not too many) multi-skilled, flexible, confident, experienced staff, staff who are aware of the impact on team if they are off sick, non-hierarchical working.
Provide training for the team.
Be aware of the big picture of what is happening in cardiology.
Effective management - 6/6 by having: coordinating processes; rotas that are fair and effort is balanced across team; opportunities to develop sufficient experience; staff contracts explicit of hours of working; a well managed, adequate budget; effective decision-making processes; systems that prioritise patients effectively; awareness of staff needs focus on their welfare; trust and support within and between teams; everyone is in the right place at the right time to treat patient OOHs.
Intrinsic motivation – 6/6: Staff are strongly motivated to provide PCI – they enjoy the work and developing new skills, they find PCI challenging and exciting.
Difficulties in maintaining adequate staffing - 6/6 such as having: inexperienced staff in CL, staff who are unable to multitask and slow the process down; too few or too many staff in CL; absences making it difficult to rota an experienced team; no time available in working day for management duties; an appreciation that supervising inexperienced staff takes time and effort; difficulties due to budgetary limitations.
All sites described difficulties recruiting experienced staff who will do on-call, and senior staff who will manage the service.
Poor working conditions for staff -5/6 such as: heavy work in CL requiring concentration for long periods of time and wearing heavy lead aprons; frequent undesirable shifts, inadequate rest and not getting planned breaks from work resulting in fatigue; increased workload in CL; lack of financial compensation for long hours of work and on-call; difficulty in gaining access to CL OOHs; different pay and rest after OOH working.
Staff feel service runs on good will.
Loss of staff development opportunities due to workload in CL
Increased contact with patient relatives
Limited rehabilitation resource resulting in few patients being seen post procedure - 2/6
Lack of financial investment in aftercare – posts frozen in acute care and few posts in community - 2/6
Limited training opportunities for DGH cardiologists unless working in partnership with the tertiary centre and sharing rotas
Cardiology Day clinics are understaffed and stretched to complete work after OOH working - 3/6 Backlogs and cancellations of elective cases following emergency patients being taken in CL – 3/6.
Issues for ambulance services - 3/6 including: difficulties providing additional staff training on new primary PCI procedures while covering existing work effectively;
concern that primary PCI will result in deskilling of ambulance staff in thrombolysis use;
Concern that long journeys to regional centres will occupy rural ambulance for long periods of time placing them out of service use for other emergency patients.

© Queen's Printer and Controller of HMSO 2007 51
Table 11. (continued). Summary of qualitative comments from staff interviews and focus groups about Staffing
RESEARCH AREA / THEME
START – UP FACILITATORS BARRIERS KNOCK – ON CARDIOLOGY KNOCK – ON OTHER SERVICES
STAFFING
Staff contribution to service is valued 2/6 Staff receive feedback on PCI procedures that are successful 2/6 Clear work protocols are developed 4/6 Encouragement for staff to adapt to service changes
Lack of support from HR to develop adequate terms and conditions of service
Everyone assuming something is being done in CL but no one has done it 2/6
Few people with decision-making capability so issues remain unresolved for long periods building resentment 2/6
Ambulance arrives before staff can open CL OOH either due to on-call staff living far away, busy traffic, transport difficulties or lack of staff parking 3/6
Some peoples’ negative reactions to stressful situations makes teamworking difficult
Lack of feedback available as to the success of individual primary PCI cases
Lack of recognition of the effort put in by staff to get the work done by senior department managers
Work-home spill-over such as: not getting time off after OOH working 3/6; work extending into breaks and off duty periods 3/6; inadequate rest after primary PCI 3/6; difficulty switching off after a CL shift; fatigue after OOH working. Home-work spill-over: difficulty finding child minder if called in OOHs.
CCU issues such as 3/6: workload increases if nurses are training DGH staff, PCI patients take a lot of staff time.
As patients spend little time in acute cardiac care CCU nurses fear job cuts and acute care work is becoming less interesting with fewer acute cases requiring care on the ward 3/6
Cardiology wards describe difficulties when they send a nurse to assist CL in an emergency. These include the following workload difficulties: loss of a member of staff required for specific duties, difficulty maintaining continuity of care, having to share the workload being a nurse down, further increased workload if the ward is required to “sit out” patients awaiting discharge 3/6
Managers at DGHs are concerned about retaining staff (especially cardiologists) who will want to work at tertiary centre

© Queen's Printer and Controller of HMSO 2007 52
The vast majority of the staff who responded to the survey (96%) identify themselves as working in a team. Moreover they perceive their teams to have clear objectives that can not be achieved without their working closely with others. A series of interviews with team members examined these concepts more closely (see Appendix 1. for template).
Participants had some confusion describing team roles; staff at some hospitals felt CL roles were clear (3/6) while others felt there was some role confusion IH (“when there can be up to five nurses in CL”) or that roles varied “depending on who was in the team” (1/6). These findings support those found from the survey and detailed above.
There was a strong sense of working together in the team (5/6) with people describing “sharing roles”, “blurring roles” and multi-tasking to “help each other out”. Staff at one hospital described the focus for medical staff was on the artery while others monitored and cared for the patient (1/6).
Participants were unclear about team objectives; some described team objectives (2/6) while others described individual objectives (4/6). Some people described “providing the best treatment for the patient and their relatives” (1/6); others focused on caring for the patient (2/6) or developing the service (1/6). Only one hospital was clear about the distinction between individual and team objectives illustrating the team development work that had had been undertaken at this hospital. CL teams would benefit from further teamworking development focusing on team roles and shared objectives.
Participants were asked about the boundary relationships of the team. The most commonly described were with: the rest of Cardiology (4/6), Out Patients’ Department (2/6) and CCU (2/6). Rehabilitation was mentioned less frequently (1/6) as were ED (1/6), DGHs (1/6) and the cardiac network (1/6). These descriptions suggest the close-to boundary relations are well developed and boundary relationships with the distal part of the pathway are less developed.
4.4.3.2 Training
From our survey we found that 60% (N=115) of staff have had specialist training to work as part of the primary PCI team, but of these only 55% had completed it. Yet even those who had not completed tended to consider the training thus far was adequate to support their primary PCI work; however 12% of those who had completed the training did not feel it was adequate.
The extent of training or perceived adequacy of training was not associated with any particular occupation, or to the extent to which primary PCI was the person’s major role. In fact over half of those for whom it was not their primary role had had some training. This point was reinforced by responses in the free text portion of the survey which showed most staff were content with training.

© Queen's Printer and Controller of HMSO 2007 53
Participants outlined many forms of training undertaken such as: Intermediate and Advanced Life Support, introduction to specialist equipment, reading ECGs, interventional cardiology, use of balloon pumps and stents, the role of the scrubbed nurse role and drug usage. Much training was on-the-job shadowing of more experienced members of staff (this was also observed) or acting as runners for the team while observing practice. Ethnographic observation saw a complex case being used as a learning opportunity for staff. One hospital had specifically trained CL nurses to undertake technician roles when there was a shortage of technical staff in CL.
However, not all staff working in primary PCI have received training. Twenty-five percent of staff surveyed for whom primary PCI was their main role reported having had no training, with 35% of those for whom it was around 50% of their role also having no training. This was supported by number of staff in the free text portion of the survey commenting that they had received no training in primary PCI (56 people). However, it should be noted that many sites identified a large group of people as working in the primary PCI team whose main role may not be in CL (such as in CCU and on cardiology wards). This may explain why a large number of people did not feel that they had had specific training.
The importance of training for primary PCI was highlighted in the qualitative study by staff at all hospitals. A key theme of service development was training an experienced team who were able to multi-task. It was noted that inexperienced staff lacked confidence and slowed down procedures and placed an extra work load on those with experience who were required to supervise, or caused problems in the diagnosis of the condition for treatment. In addition, staff commonly described difficulties recruiting and retaining trained and experienced staff, particularly cardiac technicians and CL nurses. Staff emphasised the need for on-going training to retain staff. Ethnographic observation saw training in CL with all staff groups.
Training was seen as extending beyond the technical. For example, one attendee at a focus group said:
“CL staff need to develop skills to care for patients’ relatives, usually the domain of ward staff”.
Further, CCU staff at some hospitals described having to train cardiac nurses from the DGHs in acute cardiac care. This is a new role for DGH staff as primary PCI patients are being moved away from of the tertiary centre CCU a few hours after their primary PCI procedure.
There was concern that insufficient resources were being put into training. Staff particularly stressed the need for continuous training and not a “one off” experience. Staff talked of feeling “out of date” regarding new procedures in acute cardiac care and needed more time to be allocated to learn and maintain skills. Several staff felt training had been incomplete and that they would like further information on drugs and administrative procedures. Others commented that they wanted further training to be

© Queen's Printer and Controller of HMSO 2007 54
provided in the future to keep them up to date and to develop their knowledge further.
It was noted that some staff (in varying roles) were reluctant to multi-task and did not want to take on the roles of others within the team because they felt this was not the job they had trained for, or that it constituted extra work. Such issues are barriers to the development of primary PCI and are best acknowledged rather than assumptions made that all staff wish to work in a multi-skilled and multi-tasked way.
Staff at several hospitals described the need to be able to reflect on performance and identify staff development and training needs. In particular, debriefing was requested after unsuccessful events that staff had found distressing. The focus groups offered an opportunity for all staff groups involved in primary PCI to get together and talk about their work experience. Many found this an opportunity rarely possible in their working day and therefore beneficial. Indeed it was noted where staff were not prepared to reflect on the performance of primary PCI this was a barrier to service development and described as “a lack of learning culture”.
Training needs extend to the ambulance crews involved in the entry to the heart attack pathway. Most hospitals encourage crews to stay in CL during the procedure to familiarise themselves with the process (this was also observed). However, ambulance staff are trained to give thrombolysis and primary PCI is a departure from that process. Ambulance staff felt crews required retraining in the appropriate procedures with primary PCI patients. However, ambulance staff explained that training can cause logistic difficulties to the service as it takes staff away from their regular day-to-day work or can occupy an ambulance longer on a transfer than anticipated.
4.4.3.3 Work-Family conflict
We examined through the survey whether work interfered with home life or vice versa to a greater or lesser extent when working on primary PCI than when not. The average work-to-home interference was significantly greater when working on primary PCI than when doing other work but only for those who do a substantial amount of primary PCI work. This was supported by teamworking interviews in which staff said:
“Doing on-call (work) affects our lives”
“There are delays finishing lists now – we have to work after 5pm.”
The difference in work-to-home conflict was unaffected by gender, but was affected by having a dependent at home. For those with dependents, primary PCI is likely to have increased the interference of work on their home life.
The qualitative analysis unearthed some of the reasons for work-to-home spill-over as staff at several hospitals described not getting time back after

© Queen's Printer and Controller of HMSO 2007 55
OOH working (3/61); work eating into break or off-duty time (3/6) and getting inadequate rest after primary PCI work (3/6). Variation was seen in adherence to the European Working Time Directive (EWTD) with some staff groups taking 11 hours rest after OOH working and others not. Staff at some hospitals (3/6) noted difficulties getting used to the shift patterns of work to comply with EWTD. Other problems included difficulty “switching off from work” after a CL shift; and fatigue following OOH working leaving individuals unable to participate in family and social life (e.g., spending time-off from work catching up on sleep).
Having children or other dependents affects home-to-work balance regardless of whether working in primary PCI or doing other cardiology work. Nonetheless, staff noted difficulties in maintaining work-life balance as one of the challenges of providing a primary PCI service.
4.4.4 Resources
Examination of qualitative data revealed a number of areas of concern to staff that related to the sufficiency of resources in both start-up and steady state phases of primary PCI development (see Table 12). Most of the concerns are about having sufficient equipment (such as stents) available for the procedure and difficulties finding a hospital bed for the unplanned admission.
This type of equipment is expensive and staff at several hospitals described hitting budget limits preventing ordering of replacement items. Further, staff described incidents of equipment failure and lack of mobile ECG transmission equipment that had been stolen from ambulances. Ethnographic observation saw equipment failure and delays caused by looking for, and sometimes not finding equipment. Specific stent sizes were unavailable and compromises were made to work with what was available. A variety of stents were observed along with the use of other specialist equipment.
As primary PCI cases arrive as emergencies they can disrupt the planned CL working day delaying elective cases. Ethnographic observation saw an emergency patient arriving while all the CLs were in use. Several sites were considering / were allocating time slots for emergencies or designating one CL to receive emergency patients to reduce the delays to elective cases.
Several difficulties were noted in planning the day to day running of a service providing primary PCI. Most notably the unpredictability of when emergency cases may arrive (several in one shift followed by none over the next two or three working days) and the lack of good financial information about the department budget hampering resource planning.
1 See note 4.3.1 for data interpretation.

© Queen's Printer and Controller of HMSO 2007 56
Table 12. Summary of qualitative comments from staff interviews and focus groups about Resources - note 4.3.1 for data interpretation
RESEARCH AREA / THEME
START – UP FACILITATORS BARRIERS KNOCK – ON CARDIOLOGY
KNOCK – ON OTHER
SERVICES
RESOURCES
Having sufficient equipment available in all CLs (such as a full range of stents) 6/6
Consider either a dedicated CL for primary PCI patients Study the efficiency of CL use and when peaks and troughs of demand appear to enable the planning of resources.
Having ring fenced beds available for patient after the procedure Effective bed management in Trust 2/6
Have all the patient information available in CL at the start of the procedure Having sufficient stock of equipment available in every CL Consider designated primary PCI “slots” in CL timetable to accommodate emergency arrivals 2/6 Have enough CLs to cope with the workload.
Difficulties in maintaining adequate resources 6/6 due to: Variable number of primary PCI cases; Variation in when CLs are available to take cases due to the elective cases that are pre-planned; ECG transmission equipment stolen or not working; CLs set up differently so staff spend time searching for equipment; Difficulties in finding a bed for emergency admission; Expense of equipment hitting budget limits; Poor stock-taking systems not showing when items are unavailable so particular items are unavailable when an emergency case arrives; Budgetary limits preventing ordering of new stock; CL may be busy when patient arrives and they have to wait; Equipment may fail to work. Lack of good financial information to enable future planning.
Cardiology day clinics disrupted and patients’ elective treatment delayed because of emergency patients’ arrival.

© Queen's Printer and Controller of HMSO 2007 57
4.4.5 Pathway
Analyses of qualitative data reveals that staff have concerns about the heart attack pathway in all stages of start-up, steady state and knock-on to cardiology and other services (see Table 13).
Staff at a majority of hospitals agree that the best entry to the system is a simple pathway going straight from the ambulance entrance to the CL (this was also observed). To reduce false alarms staff felt that this pathway should have a gatekeeper who will activate the process. Staff noted it was important to have a gate-keeper both IH and OOHs. The barriers to steady state working were delays in getting patients into the pathway and communicating this need to others.
Once in the pathway staff were concerned that patients and carers may feel overwhelmed by the speed of the process and the lack of facilities for pain control and support for relatives whilst in CL. Ethnographic observation saw only one incidence of a patient complaining about pain in the CL, and this was controlled.
Post-procedure there were blockages of the patient’s exit from the pathway either to DGHs or primary care. Bed occupancy continued for longer than planned waiting for drugs or future appointments to take home. These factors limited the capacity of the system to take further emergencies. On occasions these waits resulted in patients being moved from one location to another while awaiting transfer. The knock-on was principally felt by the DGHs who need to care for an acutely ill patient in the short-term and primary care agencies such as GPs and rehabilitation services who require good information about the primary PCI procedure to prescribe adequate follow-up care and treatment. Staff at two hospitals involved in rehabilitation noted adequate post-procedure information was not made available to GPs.
Another interesting knock-on effect of having primary PCI was described by staff in interviews and focus groups. Patients may not realise the serious nature of their illness believing that they have been “fixed” by a swift intervention resulting in a short hospital stay. Therefore, thinking their condition is not serious they don’t make the required life style changes that may result in longer-term complications.

© Queen's Printer and Controller of HMSO 2007 58
Table 13: Summary of qualitative comments from staff interviews and focus groups about Pathway - note 4.3.1 for data interpretation
RESEARCH AREA / THEME
START – UP FACILITATORS BARRIERS KNOCK – ON CARDIOLOGY KNOCK-ON OTHER SERVICES
PATHWAY
Have a gatekeeper controlling the entry to the service both IH and OOH 5/6 Have a simple, direct pathway to CL avoiding ED 4/6 Take steps to increase public education about the treatment of HA in the area served by centre 5/6
Maintain relationships with key stakeholders and plan how best to provide to aftercare and rehabilitation for patients who spend such a short time in CCU 3/6
Develop a learning culture across care providers to reflect on audit findings and take action to change the service to make it more effective 4/6
Increase public awareness of symptoms of HA and what actions to take if they think they are having a HA 2/6
By-pass ED and go straight to CL 2/6
Simplify the process of working in CL and develop a clear protocol that explains exactly what each person should be doing 2/6
Delays in getting patients to CL 6/6 are associated with: GPs; ED; the geographical position of CL being a long way from the ambulance entrance; no ECG being done before arriving at CL; information and the patient not being available (such as history and allergies); staff being delayed getting to the CL the start the procedure OOHs; and differences of medical opinion on diagnosis delaying the decision to call in the CL team. Difficulties communicating the needs of primary PCI patients 6/6 to: cardiology; other secondary care providers (such as anaesthetists who do not understand the urgency of their attendance in CL if called; and the ambulance service to transfer the patient to a DGH swiftly.
Difficulty providing rehabilitation care 6/6 such as: no time to see patients in CCU, limited rehabilitation resources and patients leave the unit quickly.
Cardiology day clinics disrupted and delayed by arrival of emergency patients
Difficulties in working effectively with DGHs who do not want to take patients back from the tertiary centre 2/6
Extra workload causing difficulties providing cardiac critical care as there are more patients requiring additional nursing time 3/6
Patients don’t realise the serious nature of their illness thinking they are “fixed” and don’t make required life style changes resulting in longer-term complications. Lack of support / interest in rehabilitation in the tertiary centre.
Staff were concerned that DGHs receive unstable patients that they may not be trained to deal with
Varying transfer times (some at eight hours, others at 12 hours) from CCU can cause aftercare confusion at DGHs Difficulties in accessing rehabilitation services 3/6 resulting in poor follow-up as patient leaves the system so quickly, or services in community have been cut back.
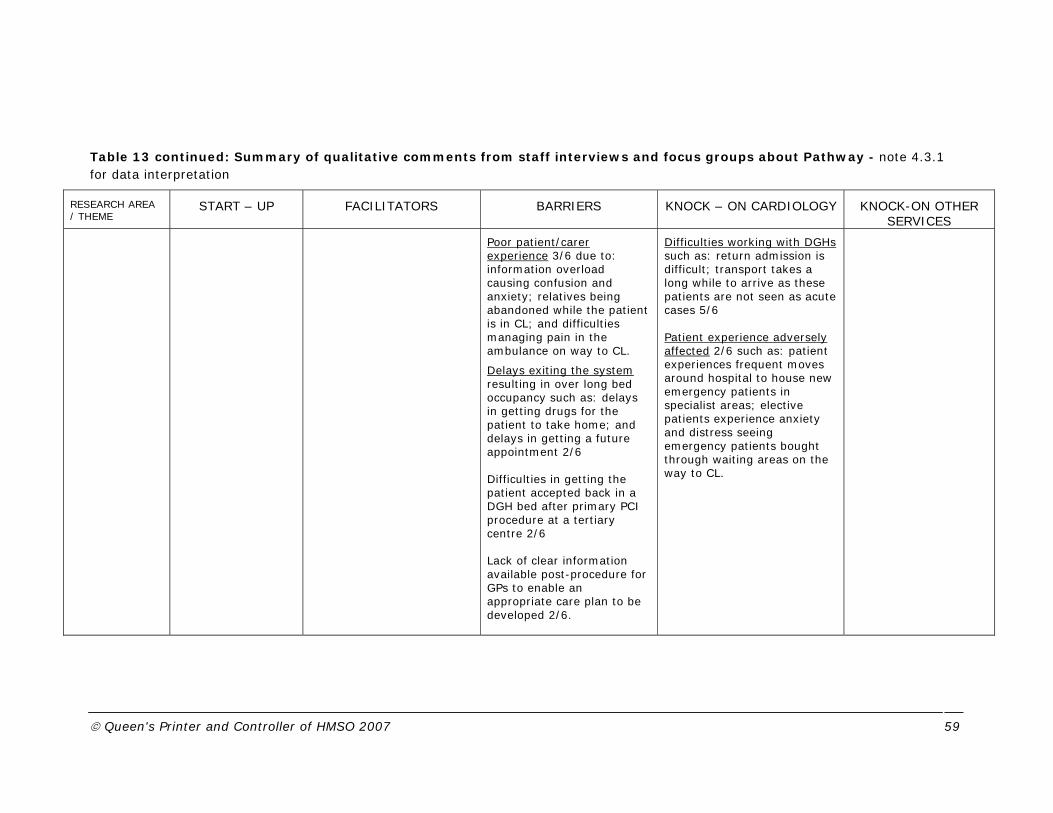
© Queen's Printer and Controller of HMSO 2007 59
Table 13 continued: Summary of qualitative comments from staff interviews and focus groups about Pathway - note 4.3.1 for data interpretation
RESEARCH AREA / THEME
START – UP FACILITATORS BARRIERS KNOCK – ON CARDIOLOGY KNOCK-ON OTHER SERVICES
Poor patient/carer experience 3/6 due to: information overload causing confusion and anxiety; relatives being abandoned while the patient is in CL; and difficulties managing pain in the ambulance on way to CL.
Delays exiting the system resulting in over long bed occupancy such as: delays in getting drugs for the patient to take home; and delays in getting a future appointment 2/6 Difficulties in getting the patient accepted back in a DGH bed after primary PCI procedure at a tertiary centre 2/6 Lack of clear information available post-procedure for GPs to enable an appropriate care plan to be developed 2/6.
Difficulties working with DGHs such as: return admission is difficult; transport takes a long while to arrive as these patients are not seen as acute cases 5/6 Patient experience adversely affected 2/6 such as: patient experiences frequent moves around hospital to house new emergency patients in specialist areas; elective patients experience anxiety and distress seeing emergency patients bought through waiting areas on the way to CL.

© Queen's Printer and Controller of HMSO 2007 60
4.4.6 Change Management
Staff working in CL described strong pride and ownership of the service driving their willingness to develop and expand the service. The survey asked staff what they enjoyed about working in primary PCI. There was considerable agreement across hospitals that the intrinsic job satisfaction (6/7) of doing work that makes people better and saving lives were the most important rewards from their work.
Next, staff at all hospitals rated the enjoyment of working as part of a strong, competent team as a reward. Further enjoyable aspects of primary PCI work were the challenge, excitement and unpredictability of the work (4/7) along with the opportunity to develop new skills (4/7).
There was less agreement across the hospitals as to what was seen as the challenges of primary PCI work. The main challenge noted was the difficulty of working with unstable patients (6/7) such as the need to use multiple drugs and treatments with acutely ill patients, the stress of working with very ill patients and people dying despite the best efforts of staff. Ethnographic observation noted complex cases that sometimes could not be treated by intervention.
Other challenges were: trying to maintain achievements while consistently achieving high standards of care with minimal disruption to other services (2/7); difficulties in coordinating resources after OOH working and elective patients being delayed by emergencies (1/7); difficulties maintaining work-life balance after long hours of work and inadequate rest after on-call while still being able to maintain their concentration at work the next day (1/7). Staff at one hospital felt particularly strongly about inequalities of pay and conditions of service across the OOH teams.
The results of a comparison of job–related well-being experienced by staff when working on primary PCI compared with other cardiology work reflect both their general reaction to primary PCI and their concerns. We used measures of two main dimensions of well-being: depression to enthusiasm and anxiety to contentment developed by Warr (1987, 1990) in our survey.
We found that the average level of depression-enthusiasm is higher when staff are working on primary PCI (mean= 3.93) than when performing other cardiology work (mean = 3.83; p<0.02). This implies slightly greater levels of enthusiasm (or less depression) when working on primary PCI (normative data for a group of 5,000 professional workers offers a mean of 3.59; Stride et al., 2008, Wall & Catley, 2008). Qualitative findings would concur with levels of enthusiasm expressed by staff at various hospitals when talking about the primary PCI service. However, a doctor at a busy hospital commented in a teamworking interview that “Keeping up enthusiasm gets difficult after a while”.
In contrast, respondents’ levels of anxiety-contentment did not differ on average between the types of work (means = 3.52 for primary PCI work and 3.58 for other work). A comparable sample of 5,000 professional workers the mean was 3.10 (Stride et al., 2008). However, we found that

© Queen's Printer and Controller of HMSO 2007 61
for those whom primary PCI was their main work role that the level of anxiety-contentment was lower (i.e., anxiety was higher) when doing primary PCI rather than other cardiology work (mean = 3.63 for primary PCI work and 3.89 for other work). This suggests as the frequency of primary PCI increases staff may become more anxious about the work.
Training is an important factor in the perception of individual well-being. If people doing primary PCI work perceive that their training was inadequate scores on both scales (depression-enthusiasm and anxiety- contentment) are lower on average. There was no significant difference in anxiety-contentment for those who had had training that was considered adequate or had not had training. However, for those who had had training that they felt was inadequate the level of anxiety-contentment was significantly different between the two types of work (mean for non-PCI of 3.36 and for PCI work of 2.90). Therefore, if staff feel inadequately trained they are more likely to feel anxious when undertaking primary PCI work.
In the case of depression—enthusiasm there was no difference for the two types of work for those who felt they were not adequately trained, however their level of enthusiasm was significant lower (mean of 3.65) for both types of work than for those who gauged they were adequately trained (mean of 3.87).
There are some occupational differences with doctors reporting being more contented and less anxious when doing primary PCI work than elsewhere. Nurses’ contentment is slightly lower when working in primary PCI than outside it, but their levels of contentment in both work situations is still higher than that of doctors.
Qualitative analyses revealed some issues that may lie behind the anxieties surrounding primary PCI work (see Table 14): staff at all hospitals felt inexperienced staff doing emergency work slowed the procedure and increased work demands for experienced staff. These concerns were exacerbated if there were delays getting patients into the CL (6/6).
Other issues that could increase anxiety were: various CLs being set-up in different ways making it difficult for OOH staff to find things quickly and the time required and difficulties caused looking for and finding a bed for emergency patients (6/6). Staff at certain hospitals talked about difficulties travelling to the centre OOH (involving heavy traffic, or over long distances) and accessing the CL OOH (e.g., OOH passes do not activate car park barriers or having no car parking available OOH). Further, increased contact with patients’ relatives also caused some initial anxiety as some CL staff felt that they had not been trained to deal with relatives and they wanted to be able to assist them in a sensitive and appropriate manner.
Analyses of qualitative data demonstrated key areas of change management that will be helpful in service development (see Table 14 over leaf). There was wide agreement that change management strategies such as having an internal champion (seen in most centres) and developing and managing relationships with the various stakeholders in the heart attack pathway was advantageous in the start-up process. Staff at two hospitals

© Queen's Printer and Controller of HMSO 2007 62
were critical of the lack of support offered by their local Trust to develop the service. A strong learning culture was seen with a majority of sites instigating reflective processes to review and develop the service whilst acknowledging threats to the service.
Maintaining relationships and reflective practices were key facilitators of steady state working. However, staff noted the challenge was to encourage those involved to consider change not be unusual but a normal part of service development. Several organisational barriers to change were noted such as long decision-making processes and competition for resources.
Resistance to change was noted with secondary care providers (such as ED) and the ambulance service. Some staff involved in primary PCI work were resistant to changes of working hours as many had taken work in cardiology as it offered work from 9am to 5pm, unusual in nursing. Changing these hours and extending the working day was not seen positively by some staff members. It was noted by some staff in teamworking interviews that they were “concerned about how we will manage in the planned extension to 24/7 working”.
An interesting knock-on effect noted was that the learning culture associated with the development of primary PCI was seen to offer opportunities to change and develop other services in cardiology.

© Queen's Printer and Controller of HMSO 2007 63
Table 14: Qualitative comments from staff interviews and focus groups about Change Management - note 4.3.1 for data interpretation
RESEARCH AREA / THEME
START – UP FACILITATORS BARRIERS KNOCK – ON CARDIOLOGY
KNOCK-ON OTHER
SERVICES
CHANGE MANAGEMENT
Have an internal champion of primary PCI 3/6
Build key relationships with: the senior Trust management team 2/6; key stakeholders in process (such as the Ambulance Service, DGHs, GPs, service development forum, Commissioners) 5/6
Champions should build up a picture of service information to track the progress and efficiency of the service 5/6 such as: PCI numbers, staff numbers and hours of work; efficiency of CL usage and utilisation of services 5/6
Evaluate and reflect on information 5/6 such as: build learning points into protocols; build on cross-boundary working; develop joint rotas with other centres; review in-house transfer system; and develop a forum to discuss development
Acknowledge threats to the service 3/6 such as: professional jealousy, Trust targets, anxiety, resistance to change. Advice - be persistent.
Maintain relationship with key PCI stakeholders 6/6; build a strong network; encourage interest from outside the Trust; and maintain strong relationships with senior management of the Trust
Take time to appreciate others perspectives to help everyone to pull together
Examine audit and reflect on: quality and speed of service 2/6; patient and carer experience 4/6; within the big picture of cardiac care 2/6,; efficiency of DGH transfer Accept change as a normal part of service development 6/6 Bonus of this sort of working is that the mapping and auditing processes can lead to improvements in other areas of work.
Organisational barriers to strategic development 2/6 such as: lack of support within the Trust for service; processes requiring formal papers to be written that requires time and resources followed by long periods of inaction; lack of forward planning; competition for resources; organisational politics influencing decision-making; lack of volume of primary PCIs making it difficult to justify services; competition with other hospitals
Staff are concerned about the lack of availability of primary PCI in some areas and a postcode lottery for treatment
Resistance to change 5/6 such as: blame culture between secondary care providers about delays; difficulties with ambulance services and ED; some staff resist working different hours and undertaking different roles.
Primary PCI provides opportunities to learn positive lessons that can be transferred to other services increasing efficiency.

© Queen's Printer and Controller of HMSO 2007 64
4.4.7 Solutions offered by primary PCI teams enabling service development
In this section we will examine the solutions people providing primary PCI offered in focus groups to some of the issues raised.
Overview: Providing a primary PCI service requires speed, access to CL and accurate diagnosis by trained staff supported by good communication and technology. Consideration needs to be given to better conditions of working for staff and the impact of primary PCI on non-emergency patients. The costing of solutions should be considered in terms of the wider health economy.
The solutions offered mirrored the themes in the research2:
Staffing issues - 5/6;
Resource issues 4/6;
Pathway issues - 5/6;
Change Management - 3/6.
4.4.7.1 Staffing Solutions
The most frequently discussed topic was staffing issues and many of these were common across the hospitals. Key issues were training, size of the OOH team and harmonisation of pay and conditions of service.
An effective team has experienced staff who are able to multi-task. Therefore it is important to identify the training needs of staff (5/6) and continue their education while recognising training staff in the work situation requires time and effort (this was also observed) and is often reliant on a few senior people (4/6). A key aspect to training is to expose staff to critical situations in primary PCI early in their training so they can develop a confident response in future working.
Staff at two hospitals described developing clear protocols so that everyone’s roles were clear in the event of an emergency.
Participants from three hospitals talked about reducing the number of staff in the OOH team (commonly to two doctors and two others, rather than the existing group of six staff). Staff at other hospitals commented that it is important to have optimum levels of staff (neither too high nor too low) in the team (3/6). Whilst a smaller team would cost less the main driver for this change was to have a smaller team of people who could assemble more quickly and therefore deal more effectively with the primary PCI case. Managers at one hospital were planning specialist activities for technicians and radiographers taking them away from emergency working. However,
2 note 4.4.1 for data interpretation

© Queen's Printer and Controller of HMSO 2007 65
elsewhere there were few active steps were being taken to move this change beyond discussion.
Staff at five hospitals described the need to align pay and working conditions across the various staff groups providing primary PCI. Principally the issues were of different pay and statutory rest patterns for the various staff groups undertaking OOH working. Staff at several hospitals were having such discussions but were finding difficulty gaining consensus across the staff groups to align shift patterns with EWTD (3/6). There appeared to be little assistance from HR or other Trust resources to develop solutions to these problems. Some staff suggested that financial incentives should be provided for those who provide OOH working (3/6) and that the service should not to rely on staff good-will to continually work longer or unsocial hours.
Staff at one busy hospital described providing primary PCI as hard work and that more recognition and feedback from top management would help to maintain staff motivation.
4.4.7.2 Resource Solutions
The next most frequently discussed topic was service provision with many issues being common across the hospitals. Important issues were commencing with a 24/7 service, tariff and targets for primary PCI, designated CLs for emergencies, and bed availability.
Staff at several hospitals felt it would have been easier to start the primary PCI service over a 24/7 period rather than incrementally growing their service by slowly expanding the geographic area covered (3/6). Only three hospitals out of the seven involved in this study had commenced with 24/7 working. Hospitals that were running an expanded regional service were able to develop joint rotas with cardiologists employed within the region to reduce the on-call burden (3/6).
Varying situations with the tariff for primary PCI were described making it difficult to recover the costs of service provision. One hospital had developed a system where they shared their tariff with the DGH so that there was a fair division of income for both parties. At another hospital, staff described issues they were having with the NHS targets for thrombolysis; by providing a primary PCI service their thrombolysis numbers were low and they were being penalised in the national recording system.
Staff at several hospitals described resourcing issues associated with emergencies arriving at CL and posed a number of solutions. There should be a designated CL available for emergencies (3/6) or designated “time slots” in CL schedules (3/6) to reduce delays when a patient arrives and allow time for this work to be scheduled. Staff at one busy site suggested that thrombolysis be used if several patients are waiting to go into CL.
Some staff described the strategy (OOHs) of switching on more than one CL at a time in case of equipment failure (2/6) and developing a problem-solving guide as a result of audit.

© Queen's Printer and Controller of HMSO 2007 66
Many staff felt strongly that there should be more ring-fenced cardiology beds to reduce the difficulty of finding a bed for primary PCI patients, especially at night.
4.4.7.3 Pathway Solutions
The pathway was a frequent topic by staff in focus groups examining the development of a simple pathway, rehabilitation services, geographical position of CL, access to the hospital OOHs, availability of primary PCI, and preparation and practice in CLs.
Staff at a majority of hospitals described the establishment of a simple pathway to CL where patients by-passed ED and reduced delays (4/6). Two hospitals described the need to simplify their care pathway and to ensure that they had a pathway co-ordinator over a 24 hour period (they currently have only a day-time co-ordinator). Staff at another hospital wanted effective criteria to be established to assist diagnosis (OOHs) and reduce false alarms and call outs. In another hospital CCU staff were being asked to prepare the CL while staff were travelling in order to save time as equipment was already up and running when the OOH team arrived. Further, there should be a designated area for primary PCI patients to wait or enter CL to offer privacy and reduce the impact on non-emergency patients.
Staff at three hospitals described activities to make their rehabilitation service and discharge planning more efficient so patients left the tertiary centre more swiftly there by making beds available for new emergency patients.
Difficulties moving patients across the hospital were acknowledged by staff at one hospital; the suggested solution was to move the CL nearer CCU. Cardiology staff were proactively trying to encourage a bed review process to take place that would highlight the need for this move.
Staff at two hospitals described difficulties in gaining access to the hospital and parking difficulties OOHs. These problems were proving difficult to solve, particularly for non-medical staff. Two hospitals were considering resident on-call for staff who lived a long way from the centre, or to reduce multiple journeys to the hospital OOHs.
Staff at a majority of hospitals (5/6) felt strongly that primary PCI should be offered to every patient suffering a heart attack twenty-four hours a day, seven days a week, even if they did not offer this service at the moment.
Staff at three hospitals felt that information leaflets explaining the procedure to patients should be available in multiple languages enabling patients to make informed consent. Further, patients should be given adequate time to adjust to what is happening to them before being rushed into the CL.
Staff at several hospitals felt that more public education was required to teach people about what to do if they are having a heart attack and to

© Queen's Printer and Controller of HMSO 2007 67
encourage them to call an ambulance immediately (3/6) there by gaining swift entry to the pathway.
Staff at two hospitals felt is was important that everyone involved in primary PCI should to be aware of “the bigger picture of cardiac care” and the knock-on effects that occur when treating emergency patients delaying the elective lists. Staff at two further hospitals were concerned that poor discharge information was given to GPs as a result of speeding up the discharge of patients. They worried that this could result in compromised longer-term care.
4.4.7.4 Change Management Solutions
Change management was frequently discussed by staff in the focus groups describing systems that had been put in place to reflect on practice and how to improve on working relationships was DGHs.
Staff from several hospitals described systems that they had put in place for auditing and learning from mistakes (3/6). Staff at one hospital described weekly meetings with key stakeholders that discussed problems that had been experienced and working out changes that needed to be made to minimise future occurrences.
Issues around change management were frequently labelled as communication problems with groups such as DGHs. Staff felt that communication between DGHs and tertiary centres needed to be improved particularly about the preparation of the patient for primary PCI and operating smooth transfers between the centre and the DGH where it was often difficult to get a bed for the returning patient (3/6).
The next section will look at the overall findings of the workforce and organisational implications and put them in context with previous research.
4.5 Discussion
This chapter has presented information about primary PCI from the perspectives of medical and non-medical staff that provide the service at seven hospitals. There was a high level of agreement across the sites as to the issues surrounding the provision of a primary PCI service. Suggestions have been made about the achievement of a sustainable service and barriers and problems identified.
It is important to note that all the hospitals we examined were running some type of primary PCI service. However, most of the people contributing to this study spent less than half their time doing primary PCI work. This suggests that running an emergency intervention service is feasible to some extent but we must remember that these hospitals were self-selecting and there was a great deal of enthusiasm to establish a service. However, the goal to deliver a 24/7 service at all hospitals was achieved only by three hospitals during the period of investigation. Further, only one of these

© Queen's Printer and Controller of HMSO 2007 68
hospitals was seeing over 50 patients in a monthly period. Reading the comments made by staff at the remaining five hospitals it was clear they were having difficulties expanding their service to this level.
Looking at the service provided by the various hospitals, with the exception of three hospitals running a 24/7 service, others had developed their service by delivering first to a small local population and then incrementally expanding the catchment area to encompass more potential cases. In this way the new service was overlaid on existing ways of working. While primary PCI is in an experimental phase with only a few cases per month, few difficulties were seen with this slow expansion strategy. However, as the numbers of emergency patients increase issues of staff capacity, pay and reward become more critical. Staff suggest 24/7 was the best way to start the service particularly as people become aware of their commitments and shift patterns at the onset and will not be required to work additional duties or hours as the service expands. Participants advised that it was important staff realised the changes that were required to make in their working day (such as working extended shifts and more frequent on-call working) and that contracts of employment reflected these changes. It was suggested that staff should be issued with new contracts of employment making conditions of working clear in the start-up phase. These comments describe a shift from the notion of a 9-5 working day that attracted many non-medical staff to work in cardiology to 24/7 working that may be unattractive to some staff members.
Critical to the successful development of a primary PCI service are staff who are experienced, flexible and prepared to multi-task. This study has shown that not all staff were happy to work across role boundaries and this represents a shift in the way people work together in the heart attack pathway. Key to the development of skills to work across normal role demarcations are selection, training and clear protocols of working that state the roles to be undertaken.
In addition, service development requires experienced management operating as a dedicated role (not as part of a clinical role) to co-ordinate and develop activities in a fair and equitable manner. Feedback to staff about individual and group performance and recognition of their contribution to the service are critical to maintaining motivation to continue to develop the local service. In addition, provision of on-going training rather than “one off” training when the CL is set up is important to the maintenance of the service as retention of experienced staff appears to be difficult.
Managing a primary PCI multi-disciplinary team of medical, nursing and Allied Health Professionals is in itself a challenge with conditions of working and reward varying among the staff groups. Nurses, technicians and radiographers all get different rates of pay for on-call working. Some harmonisation of pay and conditions is required, particularly for non-medical staff undertaking on-call working, for effective teamworking to be sustained in the longer-term. Medical staff become used to on-call or OOHs working during their training but this is less usual for non-medical staff. Different
© Queen's Printer and Controller of HMSO 2007 69
pay and conditions of working, and even access to the hospital may have little impact on staff motivation when people are called in to work OOHs occasionally. However, when OOHs working becomes more frequent staff are more likely to notice inequity of reward, access or rest after on-call events. This is a real threat to service development as staff, most of whom are currently only treating a small number of primary PCI cases, are already noticing changes in their work-life balance providing this level of service. Clear contracts of employment and fair and equitable reward and conditions of service IH and OOHs are required to maintain this development.
Good team and boundary working is required along the heart attack pathway. People are required to work across role boundaries, as well as being able to work across departmental and organisational boundaries to maintain a quality service. Team activities focusing on exploring and clarifying team roles and objectives would be helpful to support these teams in their development and growth.
A simple, direct pathway to CL controlled by an entry gatekeeper is the preferred model delivering the patient to CL with the minimum of delay. Post-procedure swift transfer to acute cardiac care and then onto to the referring DGH or to primary care and community rehabilitation is required. The knock-on effects of emergency patient arrivals displacing elective treatments is a reality of offering this type of service; either at the time of arrival or as a consequence of OOHs working reducing staff resources the following day. The knock-on effects require sensitive handling to maintain good quality patient experience while not diminishing staff motivation. Managing and co-ordinating CL resources requires proactive and flexible management able to cope with variable resource usage dependent on demand. Primary PCI is an expensive service to maintain as many high priced consumables are required to be kept in stock in the CLs. However, some economies of scale will be possible when higher patient throughput is achieved. As resource aspects are critical to this service, dedicated management is critical to the success of this service rather than someone undertaking a managerial role in addition to their CL duties.
Further, when setting up the pathway it is important to consider the efficiency of exits from the pathway to stop blocks occurring and enable new emergency patients to enter the system. One of those blockages is the prompt receipt of drugs from pharmacy on patient discharge. An innovative response from two hospitals was to develop a cardiac pharmacy post to dispense drugs from the cardiac ward. In addition, working with primary care rehabilitation resources enabling follow-up to occur after a short in-patient episode and enabling GPs to receive adequate follow-up information is important for the patient’s longer term recovery. This distal end of the heart attack pathway would appear to be the most neglected part of this service.
Building and maintaining relationships with key stakeholders along the heart attack pathway is critical to service development and sustainability. Such activities were found at most hospitals and need to be continued in a regular and frequent manner when greater patient numbers are being seen.

© Queen's Printer and Controller of HMSO 2007 70
Reflection encourages an understanding of the “bigger picture” of cardiac care that extends across primary and secondary care boundaries. This study has shown that it is important to engage senior management stakeholders in the Trust as well as clinical and service contacts along the pathway. A visible champion of Primary PCI can be valuable in this role. Taking time to audit and reflect on the effectiveness of service provision and make appropriate changes were described as critical activities to managing this change. These factors echo effective change management strategies.
The vulnerable staff group within this service in the UK would appear to be cardiac technicians. Staff at several sites described difficulty in maintaining an adequate technical workforce to staff CLs particularly in urban areas where there is competition for trained technicians and jobs without an on-call component are popular. Previous comments regarding harmonisation are salient for this group with sufficient rewards being required for OOHs working. When equivalent jobs are available locally without OOH working these will be seen as preferable. The impact of having few cardiac technicians is felt not only in the CL but in other areas of cardiology were technicians play various important roles. Knock-on effects in cardiology were frequent when a technician was unavailable after on-call working. A salient comment was that one on-call case could disrupt an entire elective clinic the following day. This problem is particularly real when there are few staff members to cover rest periods.
Cardiac nurses working in CCU have noticed changes in the quality of their work and workload when associated with a district “treat and return” service. In the set-up of the service they are busy training DGH staff in acute cardiac care but as these transfers become more frequent nursing activities focus on elective patient care and transfers of “treat and return” patients. At the same time CL staff are being put under pressure to support and assist patient’s relatives at their entry to the heart attack pathway. More flexible cross boundary working between the CL and CCU would seem useful. This was demonstrated at some hospitals when CCU staff would ready the CL while staff were travelling in OOHs. Some more formalisation of these activities into work roles would be helpful so people knew this was a required part of their job and not that they were “helping others out”.
There are several limitations to this study, most notably that of a small sample who volunteered to be involved in the study. However, active steps were taken to hear less enthusiastic voices and a number of limitations have been identified. At the time of study there were less than 10 hospitals providing a comprehensive primary PCI service in England, and of those a majority of these took part in this study. A rich picture of working in a cardiology department providing primary PCI was gained by using both quantitative and qualitative methods.
Having discussed the main findings of this study it is useful to reflect on the literature to see where others have found issues in the establishment of primary PCI services. Concerns were raised by Fye (2004) about the growing shortage of cardiologists in the US and how this may affect the number of primary PCIs that could be performed. However, in this study

© Queen's Printer and Controller of HMSO 2007 71
several hospitals setting up this service had five or less interventional cardiologists doing this work. However, cardiologists agreed that undertaking primary PCI was an increase in their workload but most felt that this was acceptable while numbers of patients were low. When prompted, cardiologists suggested there should be a minimum of six interventionalists before setting-up this type of service, otherwise the on-call obligation would become too onerous with more than one day a week disrupted with OOHs emergency patients. The site with the largest number of primary PCI cases at the time of study had incorporated interventionalists from DGHs into their rota and had just commenced an extended rota with a split weekend shift. This rota had the advantages of a reduced frequency of on-call and the ability to recover from a busy weekend shift before commencing the next week’s work. Further, it offered interventionalists working in regional DGHs a stronger link to their tertiary centre and the opportunity to maintain their interventional skills.
Pearson et al., (2004) reported a study of patients with Acute Myocardial Infarction examining the ratio of registered nurses per patient. They found that higher registered nursing staffing levels were associated with lower patient mortality and cautioned against strategies decreasing the number of registered nurses for cost savings. This study found that experienced staff of all disciplines were important to the development and sustainability of the primary PCI service and that on-going training was required to retain experienced staff, in particular nurses and cardiac technicians. Training was commonly provided in the CL placing additional work demands on experienced members of staff. Consideration should be given to the work role and work load of experienced staff so this does not exceed their capacity and appropriate reward strategies put in place to motivate retention.
In their review of 23 randomised trails Keeley and Grimes (2004) anticipated there would be a lack of timely available CL facilities. However, apart from the consideration of operator expertise no other workforce or organisational factors were considered in the review. This investigation has shown a variety of models of service delivery such as regional centres, “treat and return” to DGHs, and a DGH hospital can provide a primary PCI service. However, with only (at the time of this study) one regional site with a network of DGHs treating in excess of 50 patients a month it is contentious to consider how much further expansion the other hospitals can achieve unless they alter their daily working patterns. Furthermore, evidence from this study suggests there are issues of readmission in terms of both bed availability and ambulance transport that need to be resolved between regional and tertiary centres. Hospital staff described strategies to accommodate emergency patients into their working pattern such as designating slots in the CL timetable. Further difficulties were encountered finding emergency beds for patients and maintaining a full range of equipment such as stents as the cost of these items was causing budgetary limits to be reached. In addition, knock-on effects causing planned work to be delayed were reported in the daily work pattern or after OOHs working. Staff at many hospitals believed that these issues would be reduced when

© Queen's Printer and Controller of HMSO 2007 72
more patients were being treated, but only a few sites were undertaking proactive actions with key stakeholders to plan for this increase. These are issues of real concern that may threaten the viability of the service, particularly as numbers of emergency patients increase and staff and equipment resources are stretched.
In summary this study has demonstrated that primary PCI services can be established at NHS hospitals. However, with the exception of one regional site the workload of primary PCIs at the time of study was not high and a majority of staff spent less than half their time doing primary PCI work. Even considering these low numbers of primary PCIs, one busy urban centre was struggling to maintain adequate numbers of experienced staff suggesting they may have difficulties expanding the service under the present model. Participants at two other hospitals reported difficulties in the process of changing terms and conditions of service to expand the hours of working of the CL. Several participants felt the service relied on staff good-will that was becoming stretched. Further, participants noted difficulties managing and co-ordinating the service where there was not a dedicated CL manager. Finally, the multi-disciplinary, multi-tasked nature of the service is a challenge that needs to be fully embraced if the service is to be sustainable over time.
This study has highlighted a number of important decisions that need to be taken while a service is being set-up in order for it to develop in a sustainable manner. The next section will examine these recommendations in more detail.
4.6 Recommendations
Our recommendations are summarised in Table 15 along with suggestions as to the threats to the service if these recommendations are not considered.
Key to the start-up of the service is a clear decision of its future size and shape. Once the scope of the service is defined adequate resources can be planned and allocated. This study suggests a regional service operating 24/7 would be the best model. Staff at three hospitals have described a step-wise growth in catchment area covered by the service. While this has allowed the early development of the service within the confines of a small budget it is unlikely it can be sustained over time unless a new model of staff working (incorporating extended hours and equitable pay and conditions of on-call) has been instigated. Further, it is critical that the knock-on effects of on-call working on clinics held the next day is covered to reduce delays and cancellations.

© Queen's Printer and Controller of HMSO 2007 73
Table 15: Summary of suggestions for ensuring a successful primary PCI service and threats to establishing and sustaining the service
Suggestions for a successful primary PCI service Threats to establishing and sustaining service • Decide on catchment size of service at the onset and plan resources
accordingly in the context of workload of the cardiology department. A regional model working 24/7 would seem to be the best model.
• If the service gradual grows from a 9-5 model without new ways of working and resources it will eventually become over stretched and unsustainable. The knock-on effect on on-call working to the next day’s elective workload must be considered or frequent delays and cancellations will occur.
• Issue new contracts for hours of work and on-call conditions
harmonising terms and conditions across the staff groups involved in OOH working.
• If there are different conditions and rewards for on-call working for the various staff groups’ tensions will develop if these are not equitable. If rest periods after OOH working are inadequate staff health will suffer and sickness absence will rise making it difficult to cover subsequent work and sustain the service.
• Select and develop an experienced, flexible, multi-skilled team who
are prepared to work across traditional task boundaries to conduct Primary PCIs. It is preferable that the OOHs team is no larger than four people. There should be no fewer than six interventional cardiologists on the rota. Training should be provided in an on-going manner at both the individual and team level.
• The costs of maintaining all the various staff roles in the OOH team is probably unsustainable. Experienced staff will withdraw if training and development is not on-going leaving inexperienced team members unable to cope with the challenges of acute cardiac care.
• Appoint a manager and co-ordinator of service who is independent of the CL team.
• If management work is fitted in with other clinical duties individuals will not have the capacity to manage the service in a fair and equitable manner. This is an expensive resource that requires careful and flexible management to balance the varying demands of elective and emergency working. Staff motivation is key to developing and sustaining the service and this requires nurture.
• Devise a simple pathway straight to CL with an entry gatekeeper and
clear protocol of working. Audit the efficiency of the heart attack pathway frequently to find solutions to blockages that will limit the capacity of the system.
• Delays that will influence the outcome of PCI will occur if the pathway involves other agencies or the patient has to travel long distances from the ambulance entrance of the hospital to CL. If the public and primary care agencies are not educated as to what to do in the event of a heart attack further delays will be experienced. If there is no gatekeeper the team may be called in unnecessarily and this will tire individuals.
• Identify a senior champion of primary PCI and build and maintain
relationships with stakeholders across the whole heart attack pathway. Building strong relationships with the Trust’s senior management team is an important part of this activity.
• If the service is not represented by senior champion barriers and delays will be experienced that will frustrate individuals keen to develop the service reducing their motivation to deliver the service. If relationships with primary and secondary care agencies are poor rehabilitation after PCI is the first thing to suffer reducing longer-term health benefits.
• Audit, evaluate and reflect on the service developing a learning culture across the pathway that is prepared to make changes.
• If stakeholders are not prepared to reflect and learn how to adapt the service centrally or at the primary and secondary care boundaries the service will not be sustainable.
© Queen's Printer and Controller of HMSO 2007 74
Staff should be selected to work in the CL and along the heart attack pathway who are prepared to work in a multi-skilled boundary-spanning manner. On-going staff training at both individual and team level is required to develop and sustain this group of workers. It is unlikely OOH teams of six people will be sustainable over time due to financial constraints of the sufficient availability of experienced staff. It is advisable that hospitals should look to rationalise to four-person teams. Larger regional rotas of interventional cardiologists involving DGH staff would seem to be the best way to spread the workload to limit fatigue and reduce knock-on delays in elective working.
An experienced, dedicated CL manager is required to manage this resource and to maintain fair and equitable rotas for emergency and elective working. Careful selection of staff, training, and balancing work shifts with adequate rest is required to maintain both elective and emergency working. Staff motivation is the key to the successful running of this service leadership and managerial duties should not be considered as an additional duty to a clinical role.
A simple pathway should be devised taking an ambulance patient straight to CL with minimal delay. An entry gatekeeper is required guarding admission and activating OOHs teams reducing unnecessary call-outs. There should be a clear protocol of working for the CL team that is understood by primary and secondary care agencies. The public and primary care services should be familiar with this pathway to reduce delays. Hospitals should develop strong relationships with primary care and rehabilitation agencies so there is good rehabilitation and follow-up after a heart attack. The efficiency of the heat attack pathway should be audited frequently to explore and resolve blockages in the system that reduce its capacity to receive further emergency and elective cases.
Identify a senior champion of primary PCI and build and maintain relationships with stakeholders across the whole heart attack pathway. Time and energy is required to develop an appropriate heart attack pathway and the issues and needs of various organisations and agencies need to be balanced for this to work effectively. Taking time to audit, evaluate and reflect on the service developing is critical to managing the change and it is important to develop a learning culture across the pathway in order to make the necessary changes.

© Queen's Printer and Controller of HMSO 2007 75
5 Patient and Carer satisfaction
5.1 Background
Despite considerable research into the clinical and potential economic benefits of primary PCI, little research has been undertaken into the patient experience of this procedure. Some qualitative research into the patient experience of PCI has been undertaken in the US, but concentrates largely on patients undergoing PCI as an elective procedure (Gulanick et al., 1994, Gulanick et al., 1997). Gulanick found patients were generally very satisfied with the procedure and level of care received, although there was a significant minority of patients who reported negative experiences of the management of comfort and a lack of control in decision-making.
It is important to gain an understanding of key aspects of the patient experience in order to develop primary PCI services that are acceptable to patients. Although primary PCI offers improved patient outcomes, there are other factors that may affect the acceptability of the procedure for patients and carers. In particular, the implementation of primary PCI in the UK is likely to require some degree of centralisation, which may run counter to patient and carer preferences. We aimed to evaluate the patient and carer experience of primary PCI in terms of convenience, comfort and pain, levels of confidence in the procedure, staff and institutional facilities supporting PCI. We also compared it to the experience of people being treated for a heart attack at sites offering traditional thrombolysis-based treatment.
5.2 Methods
There were three phases of the patient and carer component of the evaluation: interviews to understand the key aspects of the patient and carer experience and develop a survey instrument; a survey of NIAP and control sites; further interviews to examine issues raised in phases 1 and 2.
5.2.1 Phase 1: Key aspects of the patient and carer experience
We undertook semi-structured interviews with NIAP patients and carers to identify key aspects of the experience and develop NIAP-specific instruments for measuring patient and carer satisfaction.
Patients who were admitted to hospital at two of the intervention sites with a heart attack were asked if they would like to participate in the study. We also asked them if we could speak to their carer. We used purposive sampling to indicate the range of referral routes (i.e. via ED, direct to catheter lab, bypass) and then undertook maximum diversity sampling of differing ages, sex and time of admission. We also undertook further interviews with two patients and their carers at one of the control sites to

© Queen's Printer and Controller of HMSO 2007 76
identify further aspects of the patient and carer experience at non-NIAP sites. We continued to recruit patients until no new themes emerged from the interviews.
Patients were invited for interview and written informed consent was obtained from all participants prior to interview. All participants agreed to the interview being recorded. All face to face semi-structured interviews were carried out within participants’ homes by the same researcher (FS). We used the critical incident technique (Flanagan, 1954) to identify key aspects of the patient and carer experience. Participants talked through their experiences from onset of symptoms to discharge home and were asked to comment on positive and negative aspects of each step of the journey (see Appendix 2 for details of interview schedule). Participants were interviewed at between one and four weeks following their treatment.
Analysis The interviews were transcribed verbatim and checked by FS. We used the first stages of Framework (Ritchie & Spencer, 1994) to analyse interview transcripts. Transcripts were read by FS to identify themes, with a subset of transcripts also read by AoC. The subset of transcripts were then discussed in detail to identify a thematic framework. All transcripts were then coded systematically according to the thematic framework.
5.2.2 Phase 2: Quantitative survey
We developed a questionnaire to send to both intervention and control groups based upon the themes identified within the interviews. This included communication and confidence in staff, time waiting for treatment, confidence in treatment, facilities for visitors, care at hospital discharged to and support and follow up post discharge (see Appendix 2 for details of questionnaire). We piloted the draft questionnaire by sending it to our user group and to patients and their carers who had expressed an interest in taking part in phase one above but had not been selected for interview.
Patients were recruited from four intervention and four control sites (see section 2.1.3 for site recruitment). All patients with a STEMI at these hospitals were logged by a research nurse at each site. In order to comply with ethics committee requirements, patients were asked to consent to being sent a questionnaire. A questionnaire and up to two reminders were then sent from the University of Sheffield at around one week after admission. Recruitment took place between 1st February and 30th November 2007.
Data was analysed using SPSS version 12.0 and STATA version 8. We dichotomised satisfaction variables into ‘excellent’ and ‘very good to poor’. We undertook logistic regression, adjusting for age and sex, and testing whether the proportion of patients reporting ‘excellent’ differed in intervention and control sites. It was important to adjust for age as it is known to affect satisfaction levels (Crow et al., 2002). We also undertook the analysis taking the clustering by site into consideration. This had minimal impact on the findings.

© Queen's Printer and Controller of HMSO 2007 77
We also analysed the free text comments at the end of the questionnaire (O’Cathain & Thomas, 2004). These indicated the strength of feeling that respondents had about certain aspects of their care and elucidated answers within the structured part of the questionnaire. Comments were read by FS and key themes were identified. All comments were coded to these themes.
Definition of main and transfer hospital
Within the survey we asked patients about their experiences in the hospital that we named on the form (i.e. the four intervention and four control hospitals that we selected). Throughout the results we refer to this as the main hospital. We also asked them about their experiences if they were transferred back to another hospital for an overnight stay of at least one night. This is referred to as the transfer hospital. For intervention sites, the transfer hospital was likely to be a local, non-primary PCI hospital where the patient is repatriated after their initial emergency treatment. For control sites, the transfer hospital was likely to be a hospital with improved cardiac facilities where the patient was transferred in the emergency situation for care (primary PCI, angiogram etc).
5.2.3 Phase 3: Further qualitative interviews
In July 2007 we selected our sample of patients to take part in further interviews from the database of 322 patients who had responded to phase 2. Based on interviews in phase 1 and an initial analysis of the questionnaire data, we identified discharge and rehabilitation as areas in need of further exploration. We selected questionnaire respondents who said that they would be happy to be contacted again who had selected ‘good’, ‘fair’ or ‘poor’ for three questions concerning information given about management of their condition and support post-discharge and who had selected ‘fair’ or ‘poor’ for at least one in order to identify patients who had expressed dissatisfaction with discharge and rehabilitation. This yielded 23 patients across seven of the eight sites. We then contacted the research leads at each site to ensure that it was appropriate to contact these patients again. We then wrote to 21 of the 23 patients in August 2007 to invite them to take part in further interviews.
When analysing the phase 1 interviews we identified a theme of patients feeling ‘fixed’ that we wished to explore further. We therefore wrote to a further 34 patients in October 2007 who had selected ‘fully’ or ‘not at all’ to the question in the survey about whether they felt their health problem had been sorted out. We undertook telephone interviews and asked about support provided following discharge from hospital, lifestyle changes made and whether they felt as though their health problem had been sorted out (see Appendix 2 for details of interview schedule).
5.3 Results
We have combined the results of the qualitative and quantitative aspects of the patient and carer evaluation within a set of themes. Themes relate to topics highlighted within the research brief and to other themes that arose

© Queen's Printer and Controller of HMSO 2007 78
during the course of the research. We report the patient and carer results together, as the carer often reported upon the experience of the patient, or how they felt the patient’s needs were met. We also report some aspects of the carer experiences separately, where they refer to their own needs. Full tables of results from the survey are provided in Appendix 2.
5.3.1 Description of respondents
Phase 1
We interviewed ten patients and six carers from intervention sites, as well as two patients and carers at one control site. These included the range of admission times and routes intended (see Table 16)
Table 16: Characteristics of participants for phase 1 interviews
Characteristic Numbers
Site 6 patients and 4 carers from site 1, 4 patients and 2 carers from site 2. 2 patients and 2 carers from control site
Age (patients) Mean age: 70.8 years. Range: 57-83 years. Sex (patients) 7 male, 5 female Time of admission 6 in hours weekday, 3 out of hours weekday, 3 out of
hours weekend Route 4 ambulance direct to catheter lab, 3 direct transfer
(bypass DGH), 1 ambulance transfer via DGH ED, 1 self-presented to DGH ED, 1 via GP. 2 control ambulance to ED
Phase 2
For the survey, 1165 patient eligible patients were identified across 4 intervention and 4 control sites, of whom 682 (59%) were recruited into the study. Recruitment rates were similar for intervention and control sites (57% (432/756) v 60% (336/395), p=0.395). These figures do not include recruitment rates for one site where we did not have the patient log. Reasons for non-recruitment included patients being discharged or transferred to a feeder site before they could be approached for consent, and being too ill to approach (see Table 17).
Table 17: Reasons for non-recruitment for questionnaire
Intervention Control All n % n % Total %
Discharged/transferred 102 32% 25 16% 127 27%
No reason given 81 25% 19 12% 100 20%
Missed 18 6% 62 38% 80 16%
Too ill 46 14% 20 12% 66 14
English language problems 27 8% 3 2% 30 6%
Confused/unable to consent 13 4% 11 7% 24 5%
Died 11 4% 13 9% 24 5%
Refused 22 7% 0 0% 22 5%
Other 4 1% 6 4% 10 2%
TOTAL 324 100% 159 100% 483 100%
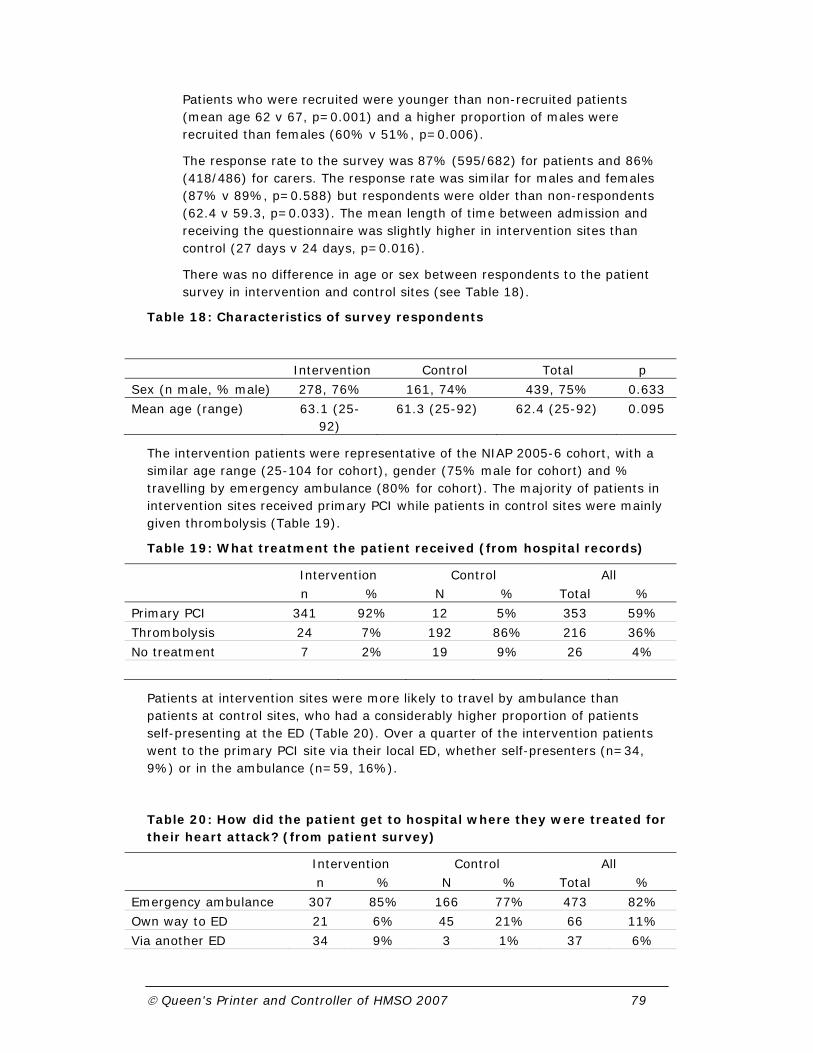
© Queen's Printer and Controller of HMSO 2007 79
Patients who were recruited were younger than non-recruited patients (mean age 62 v 67, p=0.001) and a higher proportion of males were recruited than females (60% v 51%, p=0.006).
The response rate to the survey was 87% (595/682) for patients and 86% (418/486) for carers. The response rate was similar for males and females (87% v 89%, p=0.588) but respondents were older than non-respondents (62.4 v 59.3, p=0.033). The mean length of time between admission and receiving the questionnaire was slightly higher in intervention sites than control (27 days v 24 days, p=0.016).
There was no difference in age or sex between respondents to the patient survey in intervention and control sites (see Table 18).
Table 18: Characteristics of survey respondents
Intervention Control Total p
Sex (n male, % male) 278, 76% 161, 74% 439, 75% 0.633
Mean age (range) 63.1 (25-92)
61.3 (25-92) 62.4 (25-92) 0.095
The intervention patients were representative of the NIAP 2005-6 cohort, with a similar age range (25-104 for cohort), gender (75% male for cohort) and % travelling by emergency ambulance (80% for cohort). The majority of patients in intervention sites received primary PCI while patients in control sites were mainly given thrombolysis (Table 19).
Table 19: What treatment the patient received (from hospital records)
Intervention Control All n % N % Total %
Primary PCI 341 92% 12 5% 353 59%
Thrombolysis 24 7% 192 86% 216 36%
No treatment 7 2% 19 9% 26 4%
Patients at intervention sites were more likely to travel by ambulance than patients at control sites, who had a considerably higher proportion of patients self-presenting at the ED (Table 20). Over a quarter of the intervention patients went to the primary PCI site via their local ED, whether self-presenters (n=34, 9%) or in the ambulance (n=59, 16%).
Table 20: How did the patient get to hospital where they were treated for their heart attack? (from patient survey)
Intervention Control All n % N % Total %
Emergency ambulance 307 85% 166 77% 473 82%
Own way to ED 21 6% 45 21% 66 11%
Via another ED 34 9% 3 1% 37 6%

© Queen's Printer and Controller of HMSO 2007 80
Inpatient 0 0% 1 1% 1 0%
Other 1 0% 1 1% 2 0%
Table 21: For patients travelling by emergency ambulance, where did the ambulance go? (from patient survey)
Intervention Control All n % n % Total %
Direct to hospital where treated 238 79% 154 94% 392 85%
‘Brush by’ other ED (didn’t leave amb.) 6 2% 0 0% 6 1%
Other ED (left ambulance) 53 18% 10 6% 63 14%
Not sure 3 1% 0 0% 3 1%
(See 3.2.1 for details of terminology in table above)
Phase 3
We undertook telephone interviews with 11 patients at intervention and 6 patients at control sites between September 2007 and December 2007. The characteristics of participants are shown in Table 22.
Table 22: Characteristics of participants for phase 3 interviews.
Characteristic Numbers
Sample 10 patient from sample 1 (concerns re rehab), 7 patients from sample 2 (fixed/not fixed)
Site 11 intervention, 6 control Age Mean age: 58 Range: 34-86 years. Sex 13 male, 4 female Weeks since admission Mean: 22, range: 8-44 Treatment given 10 primary PCI, 5 thrombolysis, 1 thrombolysis +
rescue, 1 none
5.3.2 Overall satisfaction
Patient and carer overall satisfaction with their treatment for a heart attack was very high in both intervention and control sites (see Table 23 and
Table 24).
Table 23: Patient satisfaction with treatment for a heart attack
Intervention Control All n % N % Total % p
How would you rate your overall experience of
Excellent 287 78% 155 71% 442 76% 0.074
Very good 63 17% 52 24% 115 20%
Good 13 4% 11 5% 24 4%
Fair 1 0% 0 0% 1 0%
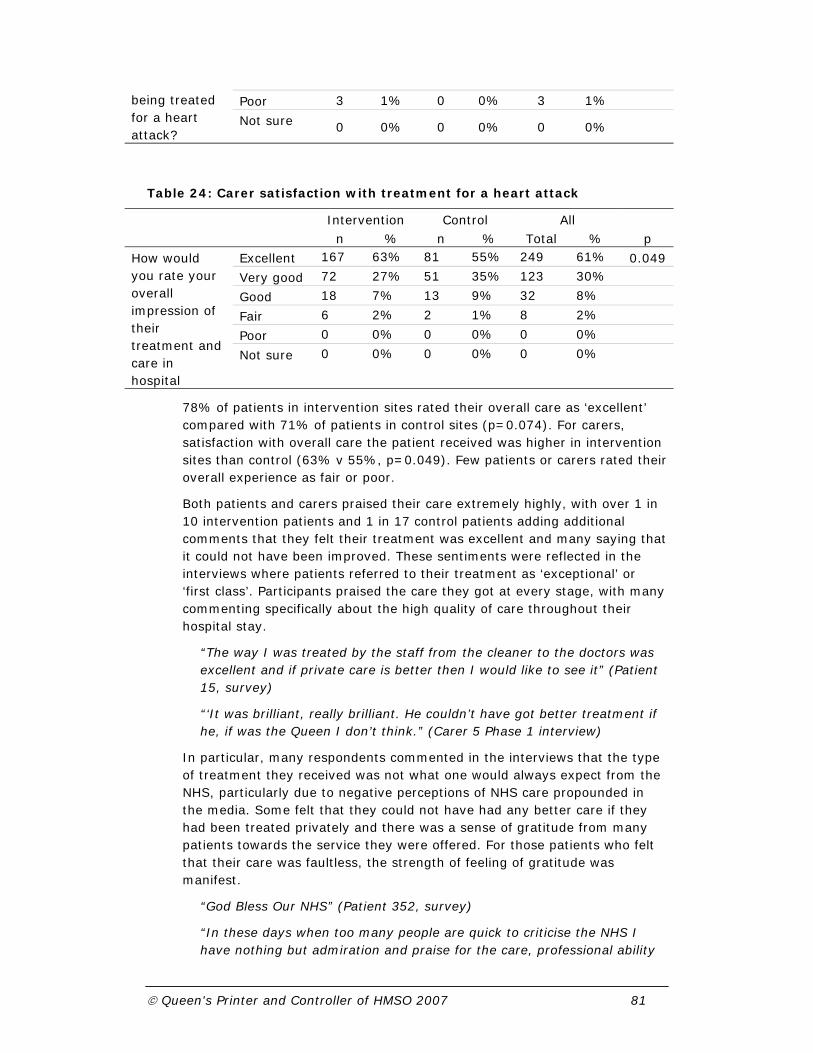
© Queen's Printer and Controller of HMSO 2007 81
being treated for a heart attack?
Poor 3 1% 0 0% 3 1%
Not sure 0 0% 0 0% 0 0%
Table 24: Carer satisfaction with treatment for a heart attack
Intervention Control All n % n % Total % p
How would you rate your overall impression of their treatment and care in hospital
Excellent 167 63% 81 55% 249 61% 0.049
Very good 72 27% 51 35% 123 30%
Good 18 7% 13 9% 32 8%
Fair 6 2% 2 1% 8 2%
Poor 0 0% 0 0% 0 0%
Not sure 0 0% 0 0% 0 0%
78% of patients in intervention sites rated their overall care as ‘excellent’ compared with 71% of patients in control sites (p=0.074). For carers, satisfaction with overall care the patient received was higher in intervention sites than control (63% v 55%, p=0.049). Few patients or carers rated their overall experience as fair or poor.
Both patients and carers praised their care extremely highly, with over 1 in 10 intervention patients and 1 in 17 control patients adding additional comments that they felt their treatment was excellent and many saying that it could not have been improved. These sentiments were reflected in the interviews where patients referred to their treatment as ‘exceptional’ or ‘first class’. Participants praised the care they got at every stage, with many commenting specifically about the high quality of care throughout their hospital stay.
“The way I was treated by the staff from the cleaner to the doctors was excellent and if private care is better then I would like to see it” (Patient 15, survey)
“‘It was brilliant, really brilliant. He couldn’t have got better treatment if he, if was the Queen I don’t think.” (Carer 5 Phase 1 interview)
In particular, many respondents commented in the interviews that the type of treatment they received was not what one would always expect from the NHS, particularly due to negative perceptions of NHS care propounded in the media. Some felt that they could not have had any better care if they had been treated privately and there was a sense of gratitude from many patients towards the service they were offered. For those patients who felt that their care was faultless, the strength of feeling of gratitude was manifest.
“God Bless Our NHS” (Patient 352, survey)
“In these days when too many people are quick to criticise the NHS I have nothing but admiration and praise for the care, professional ability

© Queen's Printer and Controller of HMSO 2007 82
and humanity shown to me and my family by all staff involved” (Patient 496, survey)
5.3.3 Speed and efficiency of service
Patients were highly satisfied with the time waited before having treatment and the efficiency with which they were treated, with significantly higher satisfaction at intervention than control sites (80% v 67%, p<0.001 and 83% v 74%, p=0.009 respectively). These high levels of satisfaction were strongly reflected within the free text comments and the interviews. 12% of intervention patients and 6% of control patients added comments within the survey praising the speed with which they were dealt with by the emergency services (often perceived as immediate) and the speed and efficiency of the procedure/treatment. Patients and carers alike reported that they were amazed at the short time period between when they contacted the emergency services to the treatment being completed. Patients who were transferred swiftly from non-primary PCI sites, or who bypassed their local hospital praised the speed of the decision made by ambulance staff and felt it was a life-saving decision. There was a perception that patients had had their lives saved by the speed and efficiency of their treatment.
“This for me was the NHS working at its very best. From the 999 call to coming out of surgery took 3.5 hours” (Patient 307, survey)
In addition to the speed of the treatment, intervention patients perceived an efficiency and a ‘smoothness’ in the care provided. In both interviews and free text comments, patients described how the team were waiting for them when they arrived in hospital, ready to work on them as soon as they arrived, with everyone seamlessly performing their own roles but working well together as a team.
“I mean the whole beauty about this situation was how it was done. The efficiency was unbelievable. The speed and efficiency was unbelievable” (Patient 2, phase 1 interviews)
“There was a very acute awareness that I had that they knew exactly what they were doing. A dedicated department, dedicated people to this procedure. Totally ready for it. You know the thing that I, the thing that amazed me having read certain negative things in newspapers that one shouldn’t read, was the speed and efficiency at which this came together without any panicking or any unplanned hurriedness. There was just a gentle speed, if those two words could be used together” (Patient 8, phase 1 interviews)
Although the majority of patients seemed impressed at the speed and immediacy of their treatment, there were some notable exceptions where the system had not worked as efficiently. In particular, some patients complained of either misdiagnosis or being made to wait around to be seen and subsequently transferred at feeder hospital or non-primary PCI emergency departments.

© Queen's Printer and Controller of HMSO 2007 83
“Went to [name of feeder hospital] by ambulance and left in A+E 30 minutes before being seen to and transferred by ambulance to [name of primary PCI hospital] very quickly” (Patient 56, survey)
“First visit (am) to A+E did not diagnose problem. Given a chronic indigestion at 12.30 and discharged. Re-admitted by 999 ambulance by approx 15.00” (Patient 558, survey)
5.3.4 Communication
Communication was identified as being important to patients and their carers in the phase 1 interviews. We therefore asked a range of questions about communication in the phase 2 survey. There were no significant differences between intervention and control sites for patient satisfaction with communication (see Figure 7). Interestingly, female patients were less likely than male patients to be satisfied with the explanations given about what was wrong with them (p=0.04) and of the risks and benefits of treatment (p=0.006). Despite lower levels of satisfaction reported for communication than other aspects of care patients praised the amount of information they received and the ability to ask staff questions within the interviews and the free text comments.
Figure 7: Patient and carer satisfaction with aspects of communication
A small number of patients referred to communication in the free text comments, largely related to a desire for further information about what had happened to them and about the risks and benefits of their treatment. In particular, there was a desire for further information about their condition at discharge (see section 5.3.9).

© Queen's Printer and Controller of HMSO 2007 84
Communication was raised as an important issue for carers in interviews and free text responses alike, both whilst the emergency treatment was underway and during the hospital stay. In the emergency situation, communication appeared more valuable to the carer as there were times when they could not tell what was happening with the patient and relied entirely upon staff for information and reassurance. Carer satisfaction levels with reassurance and support were high at both intervention and control sites (60% v 55% excellent, p=0.276), with some exceptions. Carers clearly valued being kept informed of what was happening to the patient and welcomed kindness and reassurance at a time when they felt extremely vulnerable. They praised situations where staff made them feel reassured that the patient was being well looked after and being given clear and simple explanations.
During the interviews, some carers expressed concerns that they were unable to speak to the consultant responsible for treating the patient as they were unable to visit during ward rounds and felt that they were reliant on second-hand information from the patient. However, satisfaction with the opportunity to ask doctors and nurses all the questions that they wanted was higher for carers at intervention sites than control (p=0.004). There was no difference between intervention and control for patients (p=0.780). One in six carers commented in the free text comments about reassurance and communication offered, with positive and negative comments in equal measure. This implies some variability in this aspect of the service.
“Information and reassurance from both doctors and nurses of what was happening, every step of the way” (Carer 571, survey)
“When my wife was admitted I was left in a room by myself for 1½ hours. Nobody came to tell me what was happening. I had to go find a nurse and ask. There is vast scope for improvement here” (Carer 302, survey)
A few patients commented that they were unable to find out where the patient was when they were first taken into hospital, which caused considerable anxiety. This may be due to the patient being taken direct to CCU or the catheter lab, rather than ED where the receptionist or switchboard operator might expect to find them.
5.3.5 Consent and decision making
Consent and decision-making arose as a negative concern in Gulanick’s study of patients undergoing elective PCI (Gulanick 1997). We therefore asked about consent and participation in decision-making within interviews and the survey. There appeared to be a contradiction between the survey and interviews or free text comments regarding consent for treatment and decision-making. In the survey, patients reported relatively low satisfaction with their involvement in decisions about treatment at both intervention and control sites (37% v 32% excellent), with around 1 in 12 patients rating it as fair or poor and a further 8% stating they were unsure. However, the free text comments did not provide any indication of negative issues around

© Queen's Printer and Controller of HMSO 2007 85
decision-making or consent to explain these figures. Only four people made any comment, saying that they were given the information about the decision too quickly to comprehend it and that they were not in a fit state to understand.
Despite low reported levels of satisfaction within the survey, patients and carers spoke of consent issues within the interviews but did not express concerns. Patients appeared more reluctant to be involved in decisions about their treatment, with a perception that the ‘doctor knows best’. There was evidence that they did not feel that consent was an important issue in the emergency situation due to necessity for speed in helping to resolve the patient’s condition.
“The 'not sure' answers in Q1 reflect the fact that I was in a lot of pain and distress. At that time I was unfit to share in decision making, but very grateful for speedy action” (Patient 318, survey)
“As a patient having a heart attack I don’t feel that I was in any condition as a, you know, sort of mentally, physically, or had the knowledge to make a decision like that. And so I mean I said ‘well, you know, that’s what I would expect you to tell me. You’re the doctor effectively.” (Patient 485, phase 3 interview)
Patients often could not recall the consent process fully as they were feeling too ill and anxious at the time. They understood the gravity of having a heart attack sufficiently to want to be treated immediately. Some felt so ill that they did not care what procedure was instigated, as long as it would ameliorate their symptoms. Carers similarly felt that the treatment was the patients ‘only hope’ and feared they would lose the patient if the procedure did not go ahead. Where they did recall, there was a perception that they had little choice because they were being offered a treatment without which they would die.
“Well I mean at this point when you’re in agony with pain etc, you’re happy to do whatever they say aren’t you? If a man said “you’ve got to have this done or you’ll die”, you do it, don’t you?” (Patient 5, phase 1 interview)
“I wasn’t bothered as long as they did something to help. I wasn’t bothered as long as it made me better.” (Patient 1, phase 1 interview)
Thus although from the structured questions in the survey it appeared that patients and carers were not satisfied with this aspect of care, the free text comments and interviews revealed that this was not an important aspect of care in this emergency situation. This demonstrates how important it is to consider context and not simply assume that finding from other contexts (e.g. Gulanick 2004) will be applicable.
5.3.6 Management of pain and comfort
Management of pain and comfort was included in the survey because it was identified as an important issue for elective PCI (Gulanick et al., 1997) and highlighted within the research brief. However, we had very little negative
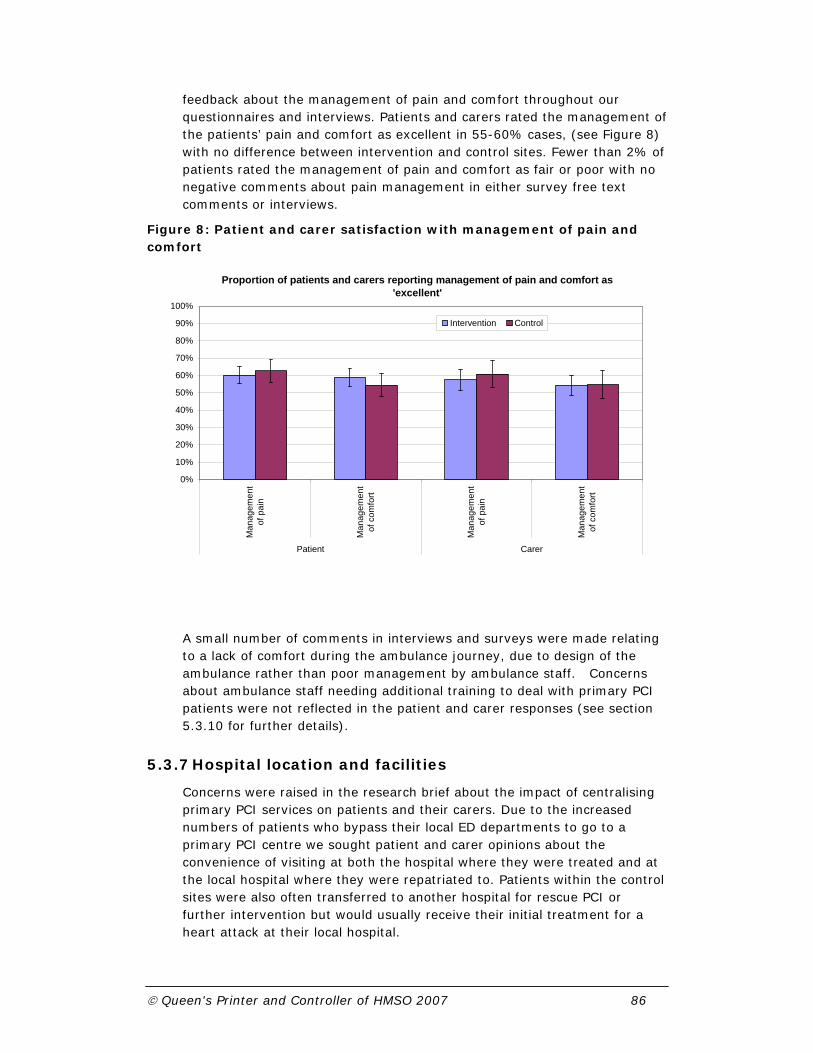
© Queen's Printer and Controller of HMSO 2007 86
feedback about the management of pain and comfort throughout our questionnaires and interviews. Patients and carers rated the management of the patients’ pain and comfort as excellent in 55-60% cases, (see Figure 8) with no difference between intervention and control sites. Fewer than 2% of patients rated the management of pain and comfort as fair or poor with no negative comments about pain management in either survey free text comments or interviews.
Figure 8: Patient and carer satisfaction with management of pain and comfort
A small number of comments in interviews and surveys were made relating to a lack of comfort during the ambulance journey, due to design of the ambulance rather than poor management by ambulance staff. Concerns about ambulance staff needing additional training to deal with primary PCI patients were not reflected in the patient and carer responses (see section 5.3.10 for further details).
5.3.7 Hospital location and facilities
Concerns were raised in the research brief about the impact of centralising primary PCI services on patients and their carers. Due to the increased numbers of patients who bypass their local ED departments to go to a primary PCI centre we sought patient and carer opinions about the convenience of visiting at both the hospital where they were treated and at the local hospital where they were repatriated to. Patients within the control sites were also often transferred to another hospital for rescue PCI or further intervention but would usually receive their initial treatment for a heart attack at their local hospital.
Proportion of patients and carers reporting management of pain and comfort as 'excellent'
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Man
agem
ent
of p
ain
Man
agem
ent
of c
omfo
rt
Man
agem
ent
of p
ain
Man
agem
ent
of c
omfo
rt
Patient Carer
Intervention Control

© Queen's Printer and Controller of HMSO 2007 87
Carers rated the convenience of visiting considerably lower than the patients at intervention sites (p<0.001) (see Figure 9) and slightly lower than at control sites (p=0.055). Although there was only a small difference between intervention and control sites in the proportion of carers rating satisfaction with convenience as excellent, the proportion of carers who rated convenience as fair or poor was 28% at intervention sites, compared with 8% at control sites.
Figure 9: Patient and carer satisfaction with hospital location and facilities for visitors
In the free text comments on the survey, concerns were raised about the convenience of visiting hours when carers were travelling a long way, and found the split visiting hours (afternoon/ evening) difficult to fit in. Carers travelling by public transport sometimes found that the journey was so long that they could only come for one of the visiting slots. Some carers were unhappy that they were unable to be present during consultant ward rounds as they felt that they were unable to speak to the medical staff about the patients’ care.
“The visiting hours would be better if they were morning too, as when you have to travel into London by train, being alone in London in the dark at night is quite scary when you are a female alone” (Carer 81, survey)
Although we did not specifically ask about availability of overnight accommodation, a number of patients in both interviews and free text comments mentioned the problems of having to get home late at night and appeared not to have been offered overnight accommodation. The prohibitive cost of parking facilities was raised both within the interviews and within the free text comments. Carers often found it difficult to park
Proportion of patients reporting aspects of the hospital location and facilities for visitors as 'excellent'
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Con
veni
ence
of v
isiti
ng -
mai
nho
spita
l
Con
veni
ence
of v
isiti
ng -
loca
l hos
pita
l
Con
veni
ence
of v
isiti
ng
Vis
iting
times
Faci
litie
sav
aila
ble
tovi
sito
rs
Patient Carer
Intervention Control

© Queen's Printer and Controller of HMSO 2007 88
and the cost was a concern to both patients and carers and caused some distress.
“My wife went by, err you can get a bus from here or a couple of buses from here, which there again can take anything up to 2 hours.” (Patient 5, phase 1 interview)
“I used to worry about my wife. They used to go up there in a morning and then come back at night. Paying that money for the car park was a worry.” (Patient 6, phase 1 interview)
However, despite some concerns about inconvenience of visiting, interview participants and survey respondents felt happy to travel further to access the specialist PCI facilities. Some intervention patients and carers who had bypassed their local hospital felt that their lives had been saved by being transferred to the primary PCI centre and felt that this far outweighed the inconvenience of travelling. Others would have liked the facility to be available at their local hospital.
“I think it’s a good thing he was brought there you know, I think if he had gone to his local hospital then he mightn’t, you know, I wouldn’t rate his chances to be honest” (Carer 5, phase 1 interview)
“I would like to say it is a shame you have to go so far to have this procedure done.” (Carer 192, survey)
Other issues arising from the free text comments were around ward facilities, food and cleanliness. While some participants praised the food, others criticised in particular the lack of healthy options available. They were unhappy at being offered food for their meals that they were specifically being advised to avoid, such as butter and cheese, and at the lack of fresh fruit available.
Carers were less satisfied with facilities available for visitors than other aspects of care, with less than 30% of carers rating their satisfaction as excellent. Satisfaction was slightly higher at intervention sites (28% v 19%) but this was not significant (p=0.067). In addition to request for overnight accommodation or late-night transport home, carers requested better facilities for visitors, particularly somewhere to obtain refreshments on or near the wards once the patient had been moved onto the CCU or coronary ward.
5.3.8 Confidence in the care received
The research brief explicitly asked for information about the levels of confidence that patients and carers had in the procedure, staff and institutional facilities. Intervention patients and their carers in the first phase interviews expressed extremely high levels of confidence in the primary PCI procedure and the care they received. This appeared to be engendered partly by the speed of the patient’s recovery and the transition from feeling ‘dreadfully ill’, or ‘looking like death’ to feeling fully recovered, pain-free and back to ‘their old self’ within a few hours. In particular, carers
© Queen's Printer and Controller of HMSO 2007 89
who had been with the patient prior to and following the PCI, spoke of the ‘total transformation’ of the patient when they came out of the catheter lab.
“Everything did to me, everything worked well because I was a new man when they took the drip off me, you'd think that there was nothing ever wrong with me.” (Patient 6, phase 1 interview)
Having gone from feeling extremely ill, to being back to their 'old self', many appeared to believe that they had been 'fixed' and spoke as if the procedure had brought closure to their heart condition. They talked of the 'problem' being 'sorted'
“I mean, within three hours of the heart attack, I was back in a ward, back in a bed, basically fixed.” (Patient 2, phase 1 interview)
The phase 1 interviews suggested that the procedure itself may have contributed to the feeling of being fixed. In addition to being impressed at the high-technology surroundings of the catheter lab and what one patient referred to as the ‘Star Trek’ equipment, the technology enabled them to witness the artery being opened. This allowed patients to witness the ‘fixing’ taking place and instill a sense of confidence in the procedure.
“I can only comment on the fact that I saw with my own eyes that there was quite a serious problem in a major artery in my heart that was fixed within a couple of hours of it being discovered and I don't think I could ask for better than that, so I'm sure, I'm sure it was just what was needed just at the right time” (Patient 8, phase 1 interview)
“Well the problem was my closed artery and that stent has opened it up […]And like I say, without that and the technology of it erm I wouldn’t be here, it’s that simple” (Patient 87, phase 3 interview)
The high level of confidence in the treatment, and subsequent feeling of being ‘fixed’ appeared to leave some patients questioning whether they had actually had a heart attack. This is surprising given how serious the problem seemed to patients and their carers prior to the PCI and the perception appeared to be due to the speed of the resolution of symptoms. Their experience of having a heart attack was different to their expectations, and patients talked in particular of not having symptoms they would expect when having a heart attack. One patient felt that she was ‘having them [the doctors] on’ as her pain resolved so quickly. Similarly, most patients felt little pain or discomfort during the procedure, which went counter to their expectations of being treated for a heart attack.
“Whether I had a heart attack or whether it was a near thing I’m not even sure now. I’ve been told I had a heart attack but it is not what I thought I would have had”’ (Patient 7, phase 1 interview)
“In fact he looked his old self you know, as I say I think this is why it's been hard in some ways for both of us to really grasp that he'd had a heart attack because it was almost as if, like I say it was almost as if he'd just cut his finger you know because once he'd had the procedure he looked and felt so much better.” (Carer 2, phase 1 interview)

© Queen's Printer and Controller of HMSO 2007 90
The survey also showed that both patients and carers had a very high degree of confidence in the treatment they received, with patients at intervention sites having higher satisfaction than those at control sites (71% v 61% ‘excellent’, p=0.022). Despite this, there was no difference in the proportions of patients who felt their condition had been fully sorted out between intervention and control within the survey (50% v 45%, p=0.308). Phase 3 interviews, selected to elucidate on what made patients feel fixed or not, suggested that patients’ degree of feeling fixed may be related to whether they had been informed that they may need further treatment, or how much damage their heart had suffered rather than the type of treatment they received.
5.3.9 Discharge and follow up
Within the first phase interviews, discharge was highlighted as the one aspect of care that was deficient in the entire process. In the survey, patient and carer satisfaction with discharge and follow-up procedures was notably lower than for other aspects of care (see Figure 10) and interestingly was slightly lower for most measures in the intervention sites than the control. Nearly one in five patients rated the time spent waiting to be discharged as ‘fair’ or ‘poor’, and only 28% of patients rated it as excellent. Although we did not ask carers about the discharge process within the questionnaire, several carers made free text comments relating to the unacceptably long wait for discharge, largely due to waiting around to obtain drugs from pharmacy. Patients reported waiting between 4 and 6 hours from being told they could go home until their drugs were ready in pharmacy, and found this wait frustrating.
“The issuing of my drugs from the hospital pharmacy was disgraceful – a wait of more than five hours before I could leave, even though I was given discharge.” (Patient 110, survey)
Figure 10: Patient satisfaction with discharge from hospital
Proportion of patients reporting aspects of the discharge and follow-up process as 'excellent'
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Tim
e w
aitin
gfo
r dis
char
ge
Info
rmat
ion
abou
tm
anag
ing
cond
ition
infu
ture
Info
rmat
ion
abou
tm
edic
atio
n &
side
-effe
cts
Sup
port
and
follo
w-u
p af
ter
disc
harg
e
Intervention Control

© Queen's Printer and Controller of HMSO 2007 91
There were mixed reports about communication prior to discharge. While many patients and carers were happy with the information they were given about medication and potential side effects and about how to manage their condition in future, there was a significant minority of patients who wrote free text comments expressing their discontentment about this. Some patients felt that the explanations about what each drug was for and any potential side effects were lacking, and they were not given enough time to take in the information. They reported feeling anxious when having side effects of medication as they did not know what was ‘normal’ and what might be a warning sign of something more serious.
“And it is a bit unfortunate that nobody said, you know, you must make sure you take this medication with food or, you know, with milk, because he has been waking up with terrible heartburn. And of course when you’ve had a heart attack and you’ve got this pain you’re sort of panicking and thinking, you know.” (Carer 2, phase 1 interview)
“Drugs are daunting - and staff have quite a job explaining to 'laymen'.” (Patient 471, survey)
Patients reported finding it difficult to absorb information about the drugs they were taking and future management of their condition whilst in hospital as they described being ‘still in shock’ during the period immediately following their heart attack. Satisfaction with information given on how to manage the condition in future was lower in intervention than control sites (38% excellent v 46% excellent, p=0.049). This may be due to speedier discharge following primary PCI, or due to patients being repatriated back to a non-primary PCI hospital before being given the discharge information they felt they needed.
“There was not enough time to inform me about medication etc as the ambulance was waiting to take me back to (transfer hospital)” (Patient 321, survey)
There was some evidence that discharge procedures between hospitals needed improvement and that lines of responsibility for rehabilitation were not clearly identified when patients were transferred between hospitals.
There were mixed reports around rehabilitation and follow-up after discharge at both intervention and control hospitals. Patients were very positive about rehabilitation if they received it and found it useful in helping them to deal with their condition. However, some problems in accessing rehabilitation were identified. Some patients felt that they were waiting too long to speak to a rehabilitation nurse or for their consultant follow-up and were anxious about their condition in the interim period. A number of patients also appeared to have been missed from the system in terms of follow-up and had not been offered any rehabilitation at all.
“When I was in the CCU the care was excellent, when moved, care went downhill. Aftercare was non-existing. I was told by the staff that the cardiac nurse would contact me. Never happened. No visit. No advice apart from see your GP.” (Patient 230, survey)

© Queen's Printer and Controller of HMSO 2007 92
“Once home an elderly person living alone should be visited by a medical person sooner than 7 to 10 days after getting home from suffering a heart attack and needing heart by-pass surgery.” (Patient 608, survey)
Patients who perceived that they had not received adequate rehabilitation following discharge sought help elsewhere, from their GP or from charities such as the British Heart Foundation. Although they found reassurance in the written information they had been given upon leaving hospital or received elsewhere, they felt that they missed individual advice and reassurance relating to their circumstances, particularly in the period immediately following discharge from hospital. In particular, patients were aware of needing to improve their fitness but were unaware of the level of exercise they could take without individual advice.
“Loss of self-confidence may have been reduced by having contact with someone for reassurance.” (Patient 436, survey)
“I mean, you know if you’re waiting for someone to tell you what you should be doing and what you shouldn’t be doing it’s a hard thing really.” (Patient 50, phase 3 interview)
The satisfaction with discharge procedures and follow-up contrasted in many accounts with the high level of satisfaction with previous hospital treatment. Patients and carers often referred to the discharge procedure as the only negative aspect of their care. It is possible that the high level of satisfaction with the emergency aspect of their treatment accentuated the dissatisfaction with the discharge and aftercare.
“As far as, you know, the treatment I’ve got when I first had the angioplasty at (hospital name) and even in the hospital at (repatriated hospital) I can’t fault to be honest. I’m grateful or I wouldn’t be here, but I can’t fault it, but as to the aftercare, I’m, I was a bit concerned.” (Patient 56, phase 3 interview)
5.3.10 Different places of care
Many patients and carers praised the high levels of care received throughout their journey, from initial contact with the ambulance crew to being on the hospital ward. Levels of praise and gratitude to staff were extremely high within interviews and free text comments from both patients and carers. Over a quarter of patients added free text comments praising staff in some way, demonstrating the strength of feeling.
“From my initial heart attack to my discharge 4 days later, I cannot express my gratitude enough. The response vehicle, ambulance crew, doctors and all the nurses were wonderful to me.” (Patient 164, survey)
“Every aspect of care from the ambulance staff, A+E staff, through doctors + nursing staff to cleaning and catering staff is a credit to the organisation. They are friendly, approachable and thoroughly professional. They are your most important asset” (Patient 571, survey)
Satisfaction with the professional skill and ability of staff was high overall for both patients and carers but higher at intervention sites (81% v 73%

© Queen's Printer and Controller of HMSO 2007 93
‘excellent’ for patients, p=0.043, 75% v 66% ‘excellent’ for carers, p= 0.051) (see Figure 11). Patient satisfaction with the professional skill and ability of staff at the transfer hospital was considerably lower than at the main hospital for both intervention and control sites. The difference was greater for intervention sites (81% excellent for main hospital v 54% excellent at transfer hospital, p<0.001) than control sites (73% excellent for main hospital v 61% excellent at transfer hospital, p=0.035).
Figure 11: Patient and carer satisfaction with staff
A similar difference in the satisfaction with the main hospital and transfer hospital is shown in the measure of satisfaction with the overall stay in the main and transfer hospitals for intervention sites (68% excellent for main hospital v 47% excellent at transfer hospital, p<0.001) (see Figure 12). There was no significant different in satisfaction with the overall stay in the main and transfer hospitals for control sites (62% excellent for main hospital v 56% excellent at transfer hospital, p=0.345). This could reflect the different role of the transfer hospital at intervention and control sites (see section 5.2.2. for explanation of the difference in transfer hospital at intervention and control sites).
Although few patients elaborated upon their care at the hospital where they were transferred, some mentioned that they felt the standard of care was poorer at their transfer hospital. They did not feel that the staff at the transfer hospitals had the same level of expertise as at the hospital where they were initially treated. Some patients also spoke of problems in obtaining beds in the local hospitals and were aware of communication problems in the transfer process.
“I do feel that […]they need to be a little more geared up because the level of support, care, attention that I’d just come from was not replicated at (repatriated) hospital” (Patient 8, phase 1 interview).

© Queen's Printer and Controller of HMSO 2007 94
Figure 12: Patient satisfaction with care received from different services
The level of satisfaction with care within different parts of the system was generally high, but highest overall for CCU. The level of care on CCU was praised highly in questionnaires and interviews for both intervention and control sites alike (80% v 84% ‘excellent’, p=0.220) and there were some negative comments about the lower standard of care once the patient returned to a general ward. Patients and carers strongly valued the one-to-one care and high level of support that they received on CCU. There were also many positive comments about subsequent ward care, in addition to the small number of concerns about wards being short staffed and delivering a lower standard of care.
“The staff in the CCU were excellent especially the nurses, nothing was too much trouble for them. Their care and professionalism was above reproach” (Patient 186, survey)
Patients were significantly more satisfied with their experience of the ambulance journey at intervention than control sites (73% v 59% ‘excellent’, p=0.037) and possibly more satisfied with the ED at intervention than control sites (68% v 58% excellent, p=0.056). Within the free text comments, respondents expressed gratitude towards staff and praised the speed and professional attitude of ambulance staff in particular, but gave no indication as to why satisfaction was higher in intervention than control sites.

© Queen's Printer and Controller of HMSO 2007 95
5.3.11 Patient views of treatment: thrombolysis or primary PCI?
Throughout the interviews, a number of comments were raised regarding the use of thrombolysis or primary PCI as a treatment for heart attack. During our initial interviews, we felt that the level of patient satisfaction was so high that we wondered whether this was attributable to being treated successfully for a potentially fatal heart attack, or whether it was due to something specific about the PCI.
In the free text comments and interviews, some patients and carers who had primary PCI were very keen to see the service provided throughout the country, particularly if they were aware that is was only offered in certain locations. There was a sense of gratitude at being able to have the procedure and a desire for everyone to be offered it.
“I would like to see more urgent angioplasty units available. They MUST be responsible for saving many lives.” (Carer 318, survey)
There was a sense of relief amongst some primary PCI patients that they had had ‘the opportunity’ to have PCI immediately, rather than be treated by thrombolysis. Some felt that having the stent inserted gave them a sense of reassurance that they did not feel they would have if they had been thrombolysed. In particular, they were relieved that they did not have to wait around for elective PCI down the line.
“If they use a drug instead of the operation then they have to wait and that must be terrible for people. I mean, it must be awful having had a heart attack and wondering if you are going to have another one.” (Patient 2, phase 1 interview)
“They have assessed you, you know what's wrong with you and I think it is pretty good that they do it there and then and that's the end of it. You haven't got to think about it, it is done isn't it. End of story really” (Patient 5, phase 1 interview)
Patients who had actually been thrombolysed did not wholly reflect this concern, as many felt that the drugs had dispersed the clot and therefore helped to resolve their health problem in the same way as a stent. However, during the phase 3 interviews, some thrombolysis patients did suggest that they would have preferred primary PCI if it were an option. Patients who were booked in for elective PCI or further testing experienced some anxiety whilst waiting for their procedure, feeling as though they were having to wait and put their lives on hold until they could actually see the state of their arteries. One patient who had had to undergo elective PCI following thrombolysis spoke of their disappointment that they had not had the treatment ‘in one go’:
“It’s done then isn’t it, you know, you haven’t got to wait maybe, what, three months or more I’ve been waiting. […] I’ll be glad when it’s done and out of the way with.” (Patient 447, phase 3 interview)
“I do have an appointment for what they call an echo test but that isn’t until January which is, what, almost three months after the heart attack

© Queen's Printer and Controller of HMSO 2007 96
so that’s an awful long time for me not to know what condition, you know, my other arteries are in.” (Patient 502, phase 3 interview)
Interestingly, when we looked at overall patient satisfaction with care based upon whether they actually underwent primary PCI or thrombolysis (rather than by intervention or control site), we found no difference (77% v 75% ‘excellent’, p=0.542). Similarly, there was no difference in the proportion of patients who considered their health problem to have been sorted out (54% v 52% ‘fully sorted out’, p=0.724)
5.3.12 Different models of service delivery
The numbers of respondents within each intervention site were not sufficient to look for differences between different models of service delivery. However, we did compare the site with the considerably higher workload with the other intervention sites because this has been identified as a significant aspect of service delivery in the workforce component (section 4). We found that although this site had a considerably higher throughput than other intervention sites, there was no evidence of a reduction in patient satisfaction.
5.4 Discussion
5.4.1 Summary of findings
Patients and carers in our evaluation were highly satisfied with their experience of being treated for a heart attack at both intervention and control sites. They were particularly impressed at the speed and the efficiency with which they were treated and the speed at which their pain was resolved.
Although both intervention and control sites were rated highly, patients at intervention sites were more satisfied with the speed and efficiency of their treatment and had a higher level of confidence in the treatment they received and in the professional skill and ability of the doctors and nurses who treated them. They were also more satisfied with their experience of the ambulance journey, which suggests that the patient pathway for patients going to an intervention site is smoother and appears more efficient than for control patients. Patients who bypassed their local hospital appeared to be pleased with the arrangement as they felt that it was more important for them to be able to have the appropriate treatment than be seen locally. The main sources of anxiety for patients were when there were delays, either in ED prior to being transferred, or in awaiting transfer to hospital for primary PCI.
Within the workforce component of this evaluation, staff expressed concern that patients should be given adequate time to adjust before being rushed into the catheter lab. However, the patients and carers within our evaluation valued speed and did not attribute much importance to the consent process in the emergency situation.

© Queen's Printer and Controller of HMSO 2007 97
Some patients did express frustration that the service was not available locally. The issue of bypass appeared more important to carers who found the parking fees restrictive and visiting hours inflexible when trying to accommodate long journey times. In particular, sites should ensure that they have facilities for visitors at night (accommodation or travel home). However, the convenience of the hospital and problems with visiting were considered a low priority in a potentially life-saving emergency situation by patients and carers alike.
It is unclear to what degree the higher levels of satisfaction at intervention sites was due to the improved patient pathway and speed of procedure and to what extent it was due to the procedure itself. Patients who are treated with thrombolysis may be administered the drug sooner than those who have PCI, but patients who have PCI perceive that they have undergone surgery and therefore are extremely impressed at the speed in which they are in and out of the ‘theatre’. Although after our phase one interviews, we postulated that patients who had undergone primary PCI had a high level of confidence due to the high-technology equipment used and the ability to see the unblocked artery, we did not find any significant difference in the degree to which patients felt as though their health problem had been sorted out between intervention and control sites. Patients who we interviewed some time after their procedure appeared aware of the state of their arteries, either due to having subsequent angiography or echocardiography and based their perception of being ‘fixed’ upon this, whether or not they had had primary PCI.
The role of communication differed for patients and carers. Whilst carers were not the subject of the treatment and therefore frequently not the recipient of information, they have specific information needs and valued being given timely information about the patients care, particularly during the anxious time when the patient is undergoing their emergency treatment. In the workforce interviews (see Table 13), staff raised concerns about feeling that they abandoned relatives whilst the patient was in the catheter lab and carer experiences certainly supported the need to ensure relatives are informed and given a place to stay during the procedure.
Patients valued communication particularly relating to their longer-term care, particularly around the use of medication and potential side effects. As in the workforce component of this study, the issues of discharge and aftercare arose throughout as being the ‘weak link’ in the patient and carer experience. Patients from all sites complained of long waits for pharmacy once they had been discharged, reflecting staff views (see Table 13). The seemingly unnecessary wait for medication could be resolved if more wards were able to dispense the relevant drugs directly by employing a cardiac pharmacist.
A significant minority of patients were extremely unhappy with their aftercare and felt unsupported and anxious about their future, which contrasted with the high level of confidence in their inpatient care. Patients valued the rehabilitation highly when they were able to access the service but access appeared to be inconsistent. Delays in accessing rehabilitation

© Queen's Printer and Controller of HMSO 2007 98
left patients unsure as to how much they could exercise to improve their health and anxious about side-effects of medication. Changes in the patient pathway such as transfer to another hospital for rehabilitation or shorter length of stay that are associated with primary PCI may mean that patients are less likely to have their rehabilitation arranged whilst in hospital, and increases the likelihood of their missing out on their rehabilitation altogether.
5.4.2 Strengths of this evaluation
This patient and carer evaluation is based upon a sample of 595 consecutive patients from four intervention and four control sites who were surveyed within 2 weeks of their initial hospital admission and interviews with 29 patients and 6 carers. For the survey there was a reasonable recruitment rate of eligible patients (59%) although with some evidence of patient bias. Recruited patients were younger than non-recruited as some patients were considered too ill to approach. The survey response rate was very high (86%) for both patients and their carers, suggesting little effect of any non-response bias.
Whilst the survey allowed us to compare the levels of satisfaction at different sites, it did not provide any indication of the weight of each aspect of satisfaction. The qualitative interviews and the analysis of free text comments allowed us to explore the issues that were salient to patients and their carers and to understand the importance of different issues. This mixture of qualitative and quantitative methods within the patient and carer evaluation allowed us to achieve a better understanding of the patient and carer experience than would have been possible by either method alone. Also, by speaking to both patients and their carers, we were able to build a better picture of the overall impact of this service development.
Any potential clustering by site was taken into account within the analysis.
5.4.3 Limitations of this evaluation
The control sites were selected to be comparable to the intervention sites in terms of size and population served. However, there was no randomisation involved. Differences in satisfaction between the intervention and control sites might have occurred because the intervention sites historically offered different quality of care rather than because primary PCI based care offered higher satisfaction than thrombolysis based care. Also, the intervention sites were self-selected and were extremely keen to provide an innovative, efficient service, constantly working to improve and ‘prove’ their service. The patient experience at these ‘early implementers’ may therefore be more positive than for patients who undergo primary PCI at sites that are less dedicated to demonstrating the benefits of primary PCI. Although recruitment rates for the survey were reasonable, almost 20% of patients who were not recruited were transferred or discharged very early. We may have under-represented the views of people who were repatriated back to feeder hospitals in the intervention group or who were transferred for further treatment in the control group. The repatriation rates were different

© Queen's Printer and Controller of HMSO 2007 99
between sites so any differences between intervention sites will have differential non-response bias due to the non-recruitment of repatriated patients. This is particularly an issue for the site with the highest throughput that discharged patients very early back to their local hospital.
While conducting the survey soon after the patients’ admission provided us with a picture of the patient satisfaction with the hospital experience, this does not allow us to examine the long-term impact of care upon the patient. Patients are likely to feel extremely positive immediately after their discharge from hospital for treatment for a potentially fatal heart attack, due to relief at being home and having ‘survived’. It is possible that the picture will be less positive once the patient has had a chance to digest what has happened and to consider the future.
5.4.4 Other literature
Although there is little literature available around patient experiences of PCI, similar positive patient experiences, particularly in relation to the speed of the process have been reported elsewhere. (Gulanick et al., 1997, Astin et al., 2007). Astin et al have recently looked at the patient information needs of patients undergoing primary PCI at one UK Teaching Hospital and reported a high level of patient satisfaction with the procedure and particularly with the speed of the procedure. Gulanick et al. found a significant minority of extreme negative reactions, referring to unmet needs around comfort in having the procedure and around decision-making. However, the majority of the patients involved in their study had undergone PCI as an elective procedure. Our patients expressed little displeasure with comfort or pain, possibly due to an understanding that there will be some ‘acceptable discomfort’ in a life-saving procedure. In contrast to Gulanick, few of the patients in our study expressed concern around decision-making processes, probably due to the emergency nature of this procedure in our study. They reported little dissatisfaction with the emergency consent process and were content to take a passive role in decision-making. This highlights the importance of context when interpreting the findings from previous studies and considering their relevance to another situation
5.5 Conclusions
Overall, patients and carers had high levels of satisfaction with primary PCI and thrombolysis-based care. Patients reported particularly high levels of satisfaction with the speed and efficiency of primary PCI services, and a high level of confidence in the treatment provided.
Carers were concerned about travelling longer distances to visit patients but accepted this in the context of the provision of optimal patient care.
Satisfaction with both primary PCI and thrombolysis-based care was lower in relation to issues around discharge home, aftercare and rehabilitation than for other aspects of care. Satisfaction was lower in sites offering primary PCI, indicating that services need to ensure patients are given

© Queen's Printer and Controller of HMSO 2007 100
adequate access to rehabilitation and follow-up when discharging patients quickly, or transferring patients back to feeder hospitals.
© Queen's Printer and Controller of HMSO 2007 101
6 Economic Evaluation
6.1 Background.
Whilst there is evidence that primary PCI may offer clinical benefits over thrombolysis in terms of mortality, reinfarction and stroke (Keeley et al., 2003), it is not yet clear whether the NHS should strive to offer primary PCI as standard first line treatment. Thrombolysis offers advantages in terms of relatively low costs and simplicity: all acute hospitals and many ambulance services are capable of providing thrombolysis. Primary PCI may be more effective, although the effectiveness may be time dependent, and is likely to be more costly to provide and require specialist staff and facilities.
In terms of cost effectiveness, a recent UK study by Bravo Vergel et al. (Bravo Vergel et al 2007 – hereafter referred to as the York model) compared primary PCI to thrombolysis, based on synthesis of clinical trials to estimate short term event rates which were then extrapolated over the longer term to estimate costs and benefits. The principal conclusion of this study was that primary PCI is likely to be cost effective provided the additional time delay to treatment compared to thrombolysis does not exceed one hour.
The York model provided a model of the potential cost-effectiveness of PCI based upon data from randomised trials. The NIAP evaluation provided an opportunity to populate this model with real-life data from a representative sample of UK NHS acute hospitals. In doing this we needed to develop specific aspects of the model so that it more accurately reflected routine practice.
Firstly, the model estimated outcomes by extrapolating from time delay and clinical outcome data (mortality and cardiovascular events) acquired in randomised trials. Although trials provide the most reliable estimates of the relationship between time delay and events, the time delays may not reflect routine practice. We therefore planned to use data from NIAP and MINAP sources to estimate time delays seen in the UK NHS and use these in the cost effectiveness model.
Secondly, randomised trials have only compared primary PCI to thrombolysis at the individual patient level, whereas economic analysis is more appropriately addressed at system level. The key economic question is whether we should provide a primary PCI-based system or a thrombolysis-based system. Not all patients within a particular system will receive the same treatment. For example, patients may be contraindicated for a particular treatment, there may not be capacity to perform primary PCI at a specific time or the service may not provide 24 hour primary PCI. Conversely, a thrombolysis-based system may opportunistically provide primary PCI if patients attend when facilities are available and accessible.

© Queen's Printer and Controller of HMSO 2007 102
This is reflected in the NIAP and MINAP data. Although the NIAP sites provided a primary PCI-based, system a proportion of patients received thrombolysis. Similarly, MINAP data revealed that control sites offering a thrombolysis-based system provided primary PCI to a small proportion of patients. Both the costs of treatment and the time to treatment (which influences patient outcomes) may differ not only according to whether thrombolysis or primary PCI is given, but the location in which that treatment is provided.
This observation provides another important rationale for undertaking the analysis at the system level. Observational time delay data from systems in which both primary PCI and thrombolysis may be used is likely to be biased if it is used selectively. Patients receiving primary PCI in a primary PCI-based system are likely to be systematically different to patients receiving thrombolysis in a thrombolysis-based system. The best way to overcome this bias is to analyse at system level and include all treated patients. On the basis of the reasons outlined above we decided to take a system-level approach.
Thirdly, the NIAP evaluation provides the opportunity to replace estimates in the York model with real life data. On the cost side, some estimates in the model were based on national, published average costs or were not available for the precise category of resource use in question. For example, the base case analysis (the set of parameter estimates considered most plausible) assumed that the mean length of stay would not differ between primary PCI and thrombolysis treated patients and was equivalent to the mean length of stay for patients with myocardial infarction.
Fourthly, the York model assumed that the benefit of primary PCI over thrombolysis was only dependent upon the primary PCI-associated treatment delay and was independent of the presentation delay. A recent analysis by Boersma (2006) suggests that the relative effect of PCI compared to thrombolysis is independent of presentation delay, but since the treatment effect of thrombolysis decreases with presentation delay (Boersma 1994) the absolute effect of PCI is likely to vary with presentation delay. We therefore planned to incorporate this assumption into an updated version of the model.
Using NIAP data to populate the York model we aimed to answer the following specific questions.
• What is the cost of primary PCI compared to thrombolysis in terms of: (a) The initial procedure; (b) The initial episode, including length and location of hospital stay, investigative tests performed and additional coronary procedures performed; (c) Additional coronary procedures performed up to one year from the initial event?
• What is the time delay associated with patients receiving primary PCI in a primary PCI-based service?
• How do these costs and time delays differ according to organisational factors?

© Queen's Printer and Controller of HMSO 2007 103
• Using the York cost effectiveness model to estimate short-term and longer-term event rates based on observed time-to-treatment, what is the cost effectiveness of PCI-based services versus thrombolysis-based services?
6.2 Methods
6.2.1 Characteristics of the cost effectiveness model
The York model comprises two main elements to compare thrombolysis with primary PCI in terms of cost effectiveness. Up to six months, the model estimates the probability of death, non-fatal MI, non-fatal stroke and revascularisations according to treatment based on a statistical synthesis of 22 randomised controlled trials. The costs up to six months (including the initial treatment costs) are calculated. Long term costs and benefits are then estimated in the second part of the model by extrapolating using the Nottingham Heart Attack Register (NHAR). The model expresses benefits in terms of Quality Adjusted Life Years (QALYs) by adjusting the weight allocated to the time period the average patient is alive by the probability of being in each of the health states. Weights were applied to stroke and MI based on published literature.
The model adopted an NHS perspective with 2003-4 prices used. We updated all relevant costs to 2006-7 when adapting the model for use in this analysis.
6.2.2 Source of data
In order to gain reliable estimates of resource use for patients attending sites specialising in primary PCI versus those specialising in thrombolysis, we analysed data collected as part of the NIAP project and collected similar information on patients attending sites not part of the project. The NIAP study covers ten sites that were funded by the Department of Health to collect data on all patients treated for STEMI. Details of these sites are provided in previous sections of this report. Four sites that routinely provide thrombolysis were contacted to supply information on all patients treated for STEMI during the study period. These were Doncaster Royal Infirmary (n=188), Royal Liverpool Hospital (n=161), Newcastle Royal Victoria Infirmary (n=133) and John Radcliffe Hospital, Oxford (n=276). In addition, data were collected from one “control” site as part of the NIAP pilot project. This site (University Hospital of North Durham) contributed data on 161 patients. Thus a total of 919 control patients were included.
Data from these same patients were used to estimate the median presentation time (the time from first call for help to arrival at the hospital) and the median time from presentation to treatment (either injection of thrombolytic drug or inflation of the first balloon for primary PCI). The cost effectiveness model includes these timings to adjust the probability of subsequent complications (reinfarction, stroke, mortality) based on meta analysis of trial data.

© Queen's Printer and Controller of HMSO 2007 104
The study period was taken as 1st April 2005 to 31st March 2006 and covers all patients admitted with a diagnosis of STEMI.
6.2.3 Patient characteristics
Data were collected on a number of patient characteristics in order to allow comparisons between sites and to adjust for case mix. These covered simple demographic variables (age, sex, ethnicity), clinically relevant comorbidities (hypertension, hypercholesterolaemia, diabetes, peripheral vascular disease, cerebrovascular disease, asthma, chronic renal failure), previous coronary heart disease (previous MI, angina, PCI or CABG) and variables that indicated patients condition at presentation (peak troponin and left ventricular ejection fraction).
6.2.4 Treatments provided within the initial episode
Data were provided on where, when and which treatments were provided, including the overall duration of stay in hospital and tests performed whilst still in hospital. This included data on drugs received, all consumables and devices used for primary PCI (such as stents, balloons, guiding catheters, guidewires, drug eluting stents), coronary angiograms, and other tests performed. We assumed that a coronary angiogram would be performed for all patients treated by primary PCI. Tests were only included if they were performed, not if they were planned to take place after discharge.
The NIAP database does not record the duration of primary PCI or the staff involved in procedures. Therefore, a survey of 50 events at five primary PCI sites was used to estimate the mean duration of each procedure, the typical staffing of the catheter lab and how this differs according to whether a procedure occurs in or out of usual operating hours. The analysis only calculates staff cost directly for those patients receiving primary PCI treatment. Other staff costs, for example associated with assessment, treatment with thrombolysis and subsequent care, are assumed to be equal irrespective of the treatment received and/or are included in the unit costs for duration of stay.
Patients that had non-primary PCI or CABG during the initial episode were identified but these were not included as costs associated with initial therapy.
6.2.5 Ambulance journeys
Patients treated at primary PCI centres may be transferred from feeder sites, resulting in additional ambulance journeys. These were defined as transfers of patients between non-PCI centres and primary PCI centres for any reason, and transfers of patients from primary PCI centres back to other hospitals. Where clinical staff accompanied the ambulance crew, this was recorded. In the absence of data on the duration of ambulance journeys, we did not include any cost for ambulance journeys made by patients to the first site, irrespective of the treatment they received. This may result in an underestimation of the cost of primary PCI, since some

© Queen's Printer and Controller of HMSO 2007 105
centres operate a “bypass” system, whereby patients are not taken to the nearest ED centre but instead undertake a longer journey to the primary PCI centre.
6.2.6 Time to treatment
For those that received thrombolysis the time from call to the emergency services to the arrival at the hospital (“door”) and the subsequent time to needle were recorded. For patients already in hospital the door time was either the time of the first call for help or, if that was not reported, the time of symptom onset.
6.2.7 Subsequent tests and coronary interventions
All sites provided information on subsequent coronary interventions (PCI and CABG) performed up to one year after the initial episode. For the control sites, these interventions were likely to be performed at a different local trust and these were contacted for this follow up information. The costs of these events were not included as part of the treatment episode cost but were included in other analyses.
6.2.8 Unit costs
Costs are expressed using 2006/2007 figures and where available were taken from national sources. Full details are provided in Table 35 (Appendix 3).
All drugs were costed according to the British National Formulary (BNF 2007). Where doses were weight based we applied the cost for a patient with the mean weight of the patient sample (75kgs). Drugs included were thrombolytics (by type), clopidogrel, glycoprotein 2b/3a inhibitors, heparin and low molecular weight heparin, bivalirudin, and angiotensin inhibitors. Although NIAP data reported the exact type of glycoprotein inhibitor used, the control sites only report whether or not a glycoprotein inhibitor was used, not the type. We therefore assume abciximab is used in all cases. However, less than 2% of cases used other glycoprotein inhibitors. All drugs were included whether they were administered prior to arrival at hospital, at the first hospital for transferred patients, or at the subsequent PCI/treatment centre. We assumed that drugs used for prophylaxis were given for one month. Differences beyond this point would not be expected to be related to the treatment given.
In the NIAP dataset, patient stay is classified according to location in CCU, ITU, HDU, other wards and dialysis. It was not possible to obtain this degree of information from control sites. Therefore, the average cost per day based on the weighted average of stays for NIAP patients was calculated. The cost per hospital day by location was estimated from NHS reference costs (NHS reference costs 2006/7).
Angiograms performed within the initial episode and radionuclide study costs were derived from 2005/6 reference costs and inflated by 3% based on the NHS price index (Curtis, 2007). This source is used in order to

© Queen's Printer and Controller of HMSO 2007 106
estimate the procedure cost of angiography. Exercise tests and echocardiography unit costs were from 2006/7 reference costs. Coronary interventions (PCI and CABG) occurring up to a year from the initial episode were costed based on the mean reported elective and non elective reference costs, weighted according to Finished Consultant Episodes (FCEs).
No data were available on the duration of ambulance journeys. We therefore applied the mean cost for an emergency transfer from NHS reference costs (2006/7). Where journeys were accompanied by members of staff other than the paramedics or ambulance technicians, these were assumed to be costs that were incurred for twice the mean duration of an ambulance journey (44.4 minutes), as calculated by Curtis (2007).
Staff costs were estimated from Curtis (2007). For consultants, we used the cost per minute of patient contact time. The cost includes payments made for being on call. For specialist registrars, the calculations by Curtis (2007) specifically include an element to account for out of hours work. For all other staff we used the cost per minute. This difference reflects differences in contractual arrangements for out of hours work and the fact that no out of hours payments are factored in to the calculations by Curtis (2007) for these staff. Nurses, technicians and radiographers are covered by the NHS Agenda for Change.
Whilst local arrangements vary in terms of payments made for out of hours work, we reflect the terms outlined in Agenda for Change (2004) in the costs for this study. For staff on call, a pay enhancement is made which is determined by the frequency of the on call arrangements. We assume a 4.5% pay enhancement is made based on on-call arrangements of between 1 in 6 and 1 in 3 of the defined out of hours sessions. For staff called into work whilst on-call, staff are entitled to either time off in lieu or additional payments for the period they are required to work, including travel time (assumed to be one hour per event). Additional payments are made at time and a half.
Each trust was asked to provide unit cost information on consumables and the operating costs of the catheter labs per minute of patient time. Due to the commercial sensitivity of this information, we do not report the cost of each individual item in this report but instead provide the mean cost for items within each category. The analysis used the exact items used for each patient and their corresponding mean unit cost from the trusts that reported a value for that item.
For drug eluting stents (DES), unit costs were only provided for four types from the responding trusts. Three other types of drug eluting stent are used by sites participating in the NIAP pilot although their use is not widespread (just 15 out of 481 cases). These were assigned the mean cost of the four other types. Where patient records only reported the types of drug-eluting stent and not the number of stents opened, we assumed one DES was used.
No unit cost was supplied for TEC arthero thrombus removal devices so the mean cost of other resources in this category was applied although this was

© Queen's Printer and Controller of HMSO 2007 107
relevant to only four patients. No unit cost was supplied for intra coronary drug delivery in the procedural devices field. This was relevant to 5.8% of primary PCI cases (81/1399) but almost all were treated at the same site. We therefore applied a zero cost to this item on the basis that this was not typically used. In the circulatory support field, we applied the cost of intra-aortic balloon pumps to the 11 patients where inotropes were used.
The mean cost per minute of operating the catheter labs excluding the staffing, drugs and consumables accounted for as individual items were provided by NIAP sites.
6.2.9 Statistical analysis
We used a range of patient covariates to control for case mix, treatment covariates and other explanatory variables relating either to the individual patient, the type of treatment given or the site in which treatment was given in order to explain differences in total cost.
The focus was on estimating mean costs and their variance and since cost data are typically skewed we used appropriate methods to deal with this issue. These are described in the sections below.
6.3 Results
6.3.1 Patient characteristics
The characteristics of the patients included in the analysis, by treatment and by location type are given in Table 36 (Appendix 3). The analysis is split between NIAP sites and five control sites.
A total of 3002 patients were included in the analysis, 2083 treated at NIAP sites and 919 controls. More patients at NIAP sites received primary PCI compared to thrombolysis (67.1% vs. 15.8%) which was significantly different from the control sites (4.3% vs. 72.6%).
Overall patients at the NIAP sites were younger, more ethnically diverse, had a higher prevalence of previous MI and angina, a higher prevalence of hypertension, peripheral vascular disease and diabetes, and a higher troponin rise.
Slightly more patients received no treatment at the control sites. These patients tended to be older, have more evidence of previous CHD and a lower troponin rise than the treated patients at both NIAP and control sites. The untreated patients at NIAP sites tended to have a lower troponin rise than those at control sites. In other respects differences between untreated patients in NIAP and control sites reflected overall population differences (i.e. NIAP patients were younger, more ethnically diverse and higher prevalence of previous angina).
At both NIAP and control sites patients receiving PCI tended to be younger, have a lower prevalence of previous MI and a higher troponin rise than those receiving thrombolysis.

© Queen's Printer and Controller of HMSO 2007 108
These findings suggest that there were significant differences between the patient populations at NIAP and control sites that need to be adjusted for in analysis. However, some caveats regarding data collection should be borne in mind:
• Methods of data recording differed between sites with more resources available to support data collection at NIAP sites. It is therefore possible that differences in previous CHD and co-morbidities represent differences in the rigor of data recording rather than true differences. It is paradoxical, although potential explicable by socio-economic or ethnic differences, that patients attending NIAP sites were younger but had more evidence of previous CHD and co-morbidities.
• The peak troponin rise is influenced by timing of blood sampling. It is noticeable that primary PCI-treated patients had double the troponin rise of thrombolysis-treated patients at both NIAP and control sites, whereas the mean troponin rise at NIAP sites was higher than controls. This may be explained by troponin sampling being systematically different in PCI-treated patients.
6.3.2 Method of admission
48% (672/1397) of patients treated in NIAP sites by primary PCI were assessed in the catheter lab. For those treated with thrombolysis, most were assessed in the ED (71%).
Many NIAP sites operate a hub and spoke type arrangement whereby patients may be taken to a feeder site and then transferred to the NIAP PCI centre. Alternatively, some sites had arrangements with ambulance trusts to take patients with suspected STEMI direct to the primary PCI centre. 31% of patients treated by primary PCI in the NIAP centres were transferred from a different hospital and 17% of those treated by thrombolysis.
There was no statistically significant difference in the proportion of thrombolysis-treated patients who received prehospital treatment, 9% (58/662) in the control sites compared to 8% (25/319) in the NIAPP sites.
6.3.3 Time to treatment
Several measures of time to treatment are reported in Table 25: time from first call for help to treatment and time from arrival at hospital to treatment. The first of these cannot be negative whereas door to treatment can be negative for patients treated prior to arrival (pre hospital thrombolysis).
Table 25: Time to treatment in minutes
Median 95% CI
low high

© Queen's Printer and Controller of HMSO 2007 109
Call to needle – control (n=522) 67 64 69
Call to needle – NIAP (n=202) 75 68 87
Call to balloon – control (n=27) 119 109 144
Call to balloon – NIAP (n=1172) 131 129 135
Door to needle – control (n=646) 22 20 24
Door to needle – NIAP (n=304) 32 28 36
Door to balloon – control (n=33) 70 60 87
Door to balloon – NIAP (n=1333) 91 87 94
NIAP only
Call to needle – transfers (n=26) 74 58 104
Call to needle - non transfers (n=169) 75 69 87
Call to balloon – transfers (n=368) 167 159 174
Call to balloon - non transfers (n=838) 120 115 124
Call to balloon - direct to catheter lab (n=588) 123 116 130
Call to balloon - not direct to catheter lab (n=618) 140 136 145
Call to balloon - not transferred and not direct to
catheter lab (n=560) 137 132 142
Call to balloon - not transferred and direct to
catheter lab (n=272) 87 83 90
Call to balloon - transferred and not direct to
catheter lab (n=40) 165.5 153 255
Call to balloon - transferred and direct to catheter
lab (n=300) 161.5 154 169
The data are skewed and therefore medians and binomial exact confidence intervals are reported. Median time to needle was shorter than time to balloon in all analyses. Call to treatment was shortest in patients receiving thrombolysis in the control sites (67mins, 95% CI 64 to 69). For patients treated with thrombolysis in the NIAP sites this was longer (75mins, 95% CI 68 to 87) but this was not statistically significant.
CTB times were lower in patients receiving treatment in control sites (119mins, 95% CI 109 to 144) compared to NIAP sites (131 mins, 95% CI 129 to 135) although there were only 27 observations in the former category. Again, this was not statistically significant. This is because the NIAP sites included transfers from other hospitals whereas control sites did

© Queen's Printer and Controller of HMSO 2007 110
not. The CTB time among non-transfers at the NIAP sites was the same as the controls (120 mins, 95% CI 115 to 124). The difference in the median time from call to treatment for those treated by thrombolysis in the control sites and those treated with primary PCI in the NIAP sites was 64 minutes.
A similar pattern is shown when comparing door to treatment times. The shortest time was for patients treated by thrombolysis in control sites (22mins, 95% CI 20 to 24), followed by those treated by thrombolysis in NIAP sites (32mins, 95% CI 28 to 38). DTB times were longer and highest in NIAP sites (91 mins, 95% CI 87 to 94). The difference in the median time from door to treatment was 69 minutes when comparing those treated with thrombolysis in the control sites with those treated by primary PCI in the NIAP sites.
There was no difference in the median CTN time for patients treated by thrombolysis who were transferred to a NIAP centre from a different hospital. However, CTB time was significantly higher for patients transferred from another hospital (median 167mins, 95% CI 159 to 174) compared to non transferred patients (median 120mins, 95% CI 115 to 124).
Patients who were taken directly to the catheter lab had a significantly lower median CTB time (123mins, 95% CI 116 to 130) compared to those who were not taken directly to the catheter lab (140mins, 95% CI, 136 vs. 145). The subgroup of NIAP patients that were taken direct to a primary PCI centre and direct to the catheter lab (n=272) had a median CTB time of 87mins (95% CI 83 to 90), a difference of 20 minutes compared to thrombolysis patients treated in control sites.
We also calculated the distribution of “presentation delays” for patients treated in control sites with thrombolysis for use in the cost effectiveness analysis. This distribution (presented in Table 26) allows the cost effectiveness model to be modified to take into account both the baseline time delay as well as the additional time taken to administer primary PCI compared to thrombolysis, using data reported in Boersma et al. (2006). We defined presentation delay to be consistent with Boersma et al. as the difference between the onset of symptoms and the arrival at hospital for patients. Patients that were already in hospital were excluded from the analysis whilst for patients that received pre-hospital thrombolysis, time of thrombolytic injection was used in place of arrival at hospital.
The table shows that approximately half of these patients presented within 2 hours of symptom onset and 68% within 3 hours. 15% had a presentation delay in excess of six hours.
Table 26: Presentation delay in thrombolysis patients treated at control sites
n %
cumulative
%
0-1h 111 18.9% 18.9%
>1-2h 196 33.3% 52.2%

© Queen's Printer and Controller of HMSO 2007 111
>2-3h 97 16.5% 68.7%
>3-6h 95 16.2% 84.9%
>6h 89 15.1% 100.0%
Total 588
6.3.4 Resource cost
The mean total cost of the treatment episode for patients by treatment and location is presented in Table 27. Patients treated by thrombolysis in the control sites (£2,983) were less costly than either those treated by thrombolysis in the NIAP sites (£3,945) (p<0.01) or those treated by primary PCI in the NIAP sites (£4,900)(p<0.01). Primary PCI patients in the control sites did not have sufficient information to permit costing of their treatment. These patients were included in the analysis of cost effectiveness where it was assumed that the treatment cost was the same as for other primary PCI patients. There was no significant difference in the costs of those that received neither treatment.
Table 27: Total cost of treatment episode (£ 2007/8)
95% CI
Mean se Low High
Control sites lysis 2983 95 2808 3167
NIAP sites lysis 3945 157 3676 4293
Control sites primary PCI NA
NIAP sites primary PCI 4900 54 4796 5009
Control sites no
treatment 3353 219 2929 3812
NIAP sites no treatment 3394 180 3045 3762
Figure 13 and Figure 14 show the categories of cost that make up these totals in percentage and absolute terms. Hospital stay is the largest cost category for any patient group. Even for patients treated by primary PCI, where length of stay is lowest, this accounts for 41% of total cost.
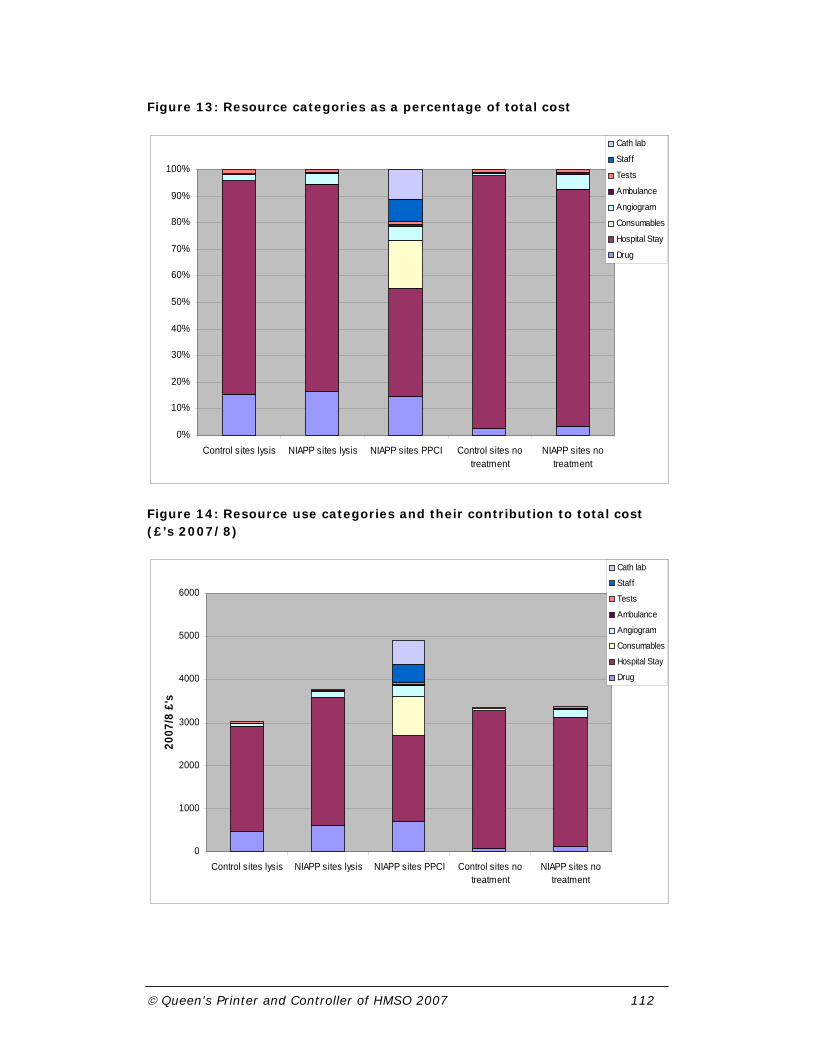
© Queen's Printer and Controller of HMSO 2007 112
Figure 13: Resource categories as a percentage of total cost
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Control sites lysis NIAPP sites lysis NIAPP sites PPCI Control sites notreatment
NIAPP sites notreatment
Cath lab
Staff
Tests
Ambulance
Angiogram
Consumables
Hospital Stay
Drug
Figure 14: Resource use categories and their contribution to total cost (£’s 2007/8)
0
1000
2000
3000
4000
5000
6000
Control sites lysis NIAPP sites lysis NIAPP sites PPCI Control sites notreatment
NIAPP sites notreatment
2007
/8 £
's
Cath lab
Staff
Tests
Ambulance
Angiogram
Consumables
Hospital Stay
Drug

© Queen's Printer and Controller of HMSO 2007 113
The length of stay for the entire episode was calculated and results are presented in Table 28. Due to skewness in the distribution of length of stay, we report bootstrap, bias corrected confidence intervals around the mean based on 1,000 replications.
Table 28: Length of hospital stay in days
95% CI
Median Mean se Low High
Control sites all 5 7.32 0.21 6.92 7.73
NIAP sites all
4 6.58 0.14 6.34 6.89
*
*
*
Control sites lysis 5 6.92 0.22 6.53 7.34
NIAP sites lysis
6 8.40 0.38 7.73 9.17
*
*
*
Control sites primary PCI 4 4.44 0.62 3.41 5.92
NIAP sites primary PCI 4 5.66 0.15 5.38 5.96
*
*
Control sites no
treatment 7 9.10 0.51 8.18 10.12
NIAP sites no treatment 4 8.54 0.50 7.54 9.53
*** p<0.01
** p<0.05
* p<0.1
Considering all patients, NIAP sites had a mean duration of stay that was 0.74 days less than control sites (p<0.01). Interestingly, the mean duration of stay was longer in the NIAP sites for patients that were treated by thrombolysis (8.4 vs.6.9 days, p<0.01) or by primary PCI (5.66 vs. 4.44 days, p=0.047).
For treated patients, drug costs accounted for approximately 16% of total cost, even in patients treated by primary PCI. Differences in this category were largely driven by the use of Glycoprotein 2b/3a inhibitors in 84% of NIAP primary PCI patients compared to 14% of thrombolysis patients in

© Queen's Printer and Controller of HMSO 2007 114
NIAP sites and 7.5% of thrombolysis patients in the control sites. For patients receiving thrombolysis, there were substantial cost differences between the thrombolytic drugs available. Streptokinase is £81 per dose compared to a minimum of £612 for the other thrombolytics. In the control sites, 38% of thrombolysed patients received streptokinase whereas in the NIAP sites 25% received streptokinase.
Consumables accounted for 18% of the total cost of treatment for patients treated in NIAP sites by primary PCI. Within this category of cost, stents and drug eluting stents accounted for 70% of mean total cost. DES were used by 35% of patients (450/1283) who were treated by primary PCI in the NIAP sites and this accounted for 35% (£314, standard error (SE) £15.9) of total consumable cost. Of those that received DES, 37% received more than one. Considering the types of stents used, 60% of patients received the same type of DES which has a unit cost of approximately the average of all stents used. 26% of patients received the most expensive types of DES whilst none received the DES with the lowest unit cost. There is a difference of £200 between the average unit cost of the cheapest DES and the average unit cost of the most expensive DES.
88% of primary PCI patients received bare metal stents and, of these, 42% (499/1182) received more than one.
Coronary angiography was used more frequently in the NIAP cohort, so the mean cost was higher for patients treated in NIAP sites compared to controls (p<0.01).
Other cost categories contributed little to overall cost differences. There were just 289 additional ambulance journeys for NIAP patients, either to transfer them from a non primary PCI centre to a primary PCI centre, or to transport them back again. Of those that were treated by primary PCI, 13% (179/1399) had an additional ambulance journey and 7% of those treated by thrombolysis (24/330).
6.3.5 Cost analysis adjusting for covariates
One of the typical problems in analysing cost data is that the distribution of the data tends to be skewed. In this situation, typical regression methods which rely on the assumption of conditional normality are inappropriate. Figure 15 shows a plot of the distribution of total cost and a superimposed normal distribution plot. It is clear that the distribution of costs is skewed and has a much longer tail than a normal distribution. Although the plot does not condition on other variables, this departure from normality remains in evidence even after conditioning.
Figure 15: Distribution of total cost versus normal distribution

© Queen's Printer and Controller of HMSO 2007 115
01.
0e-0
42.
0e-0
43.
0e-0
4D
ensi
ty
0 5000 10000 15000Total cost
Distribution of total cost
To overcome this problem we first used a Generalised Linear Model (GLM) approach. Using the deviance as a measure of fit, a gamma distribution with an identity link was chosen to transform the expected costs. However, the data also have a clustered structure. Figure 16 illustrates how the mean total cost varies for patients treated by primary PCI across the NIAP sites. Patients are grouped within hospitals which differ in terms of the mean length of stay, the types of thrombolytic drugs used, the use of drug eluting stents and several other factors which have a substantial bearing on overall cost. Costs within a hospital tended to vary less than costs for patients chosen at random from different hospitals. Ignoring this structure in the data runs the risk of making inappropriate inferences. Therefore, a Generalised Linear Multilevel Model was used which respects the clustered structure of the data. A gamma distribution with an identity link was employed together with correlated random coefficients for the variables “no treatment”, “thrombolysis” and “primary PCI”. These random coefficients take into account the remaining unexplained variability across hospitals. Variables were only deleted from the model where they were grossly insignificant with t-values well below one. A quadratic effect of age on total cost was found to perform better either than using age on its own or the logarithm of age. Data on previous AMI, angina, PCI and CABG had a large number of missing values. Two different specifications were tried, one with all four dummy variables and another where they were combined in one dummy variable with the value of one if patients had had any previous AMI, angina, PCI and CABG. The latter model had a better fit and was therefore retained for subsequent analyses.

© Queen's Printer and Controller of HMSO 2007 116
Figure 16: Total mean treatment cost by site, primary PCI patients
NIAPP 10NIAPP 9NIAPP 8NIAPP 7NIAPP 6NIAPP 5NIAPP 4NIAPP 3NIAPP 2NIAPP 1
Hospital
6500.00
6000.00
5500.00
5000.00
4500.00
4000.00
3500.00
Mea
n (9
5% C
I) to
tal c
ost (
£'s)

© Queen's Printer and Controller of HMSO 2007 117
The results of the full regression analysis of total costs are shown in Table 29.
Table 29: Generalised linear multilevel model of total cost
Independent variable Coefficient se p 95% CI
No treatment 3343 643 0.000 2083 4604
Thrombolysis 3509 667 0.000 2202 4817
Primary PCI 5176 599 0.000 4002 6350
NIAP thrombolysis 852 396 0.032 75 1628
Age in years/ 10 -592 199 0.003 -982 -203
(Age in years / 10)2 75 17 0.000 42 107
Previous CHD 203 107 0.057 -6 412
Hypertension 111 91 0.220 -67 289
Hypercholesterolaemia 202 95 0.033 16 387
Peripheral vascular disease 925 288 0.001 361 1489
Cerebrovascular disease 777 230 0.001 326 1228
Diabetes 245 129 0.057 -7 497
Dead at discharge -702 190 0.000 -1073 -330
Primary PCI out of hours 245 146 0.093 -41 531
Non-primary PCI in this admission 251 178 0.158 -98 601
CABG at this admission 4630 965 0.000 2738 6523
The coefficients for no treatment, thrombolysis and primary PCI provide the mean estimated episode cost across all hospitals according to treatment given. For patients treated with neither thrombolysis or primary PCI, there was no significant difference between NIAP hospitals and control hospitals and this final version of the model therefore does not include any variable to distinguish location for these patients. For patients treated by thrombolysis, the conditional mean cost was £3,509 but was higher in NIAP sites by £852. For patients treated by primary PCI the conditional mean cost was £5,176 for those treated within working hours and was higher for patients treated out of hours by £245.
A number of other patient covariates were included in the analysis. This model includes both age and age-squared variables which allows for a U-shaped effect on cost. The minimum cost occurs at approximately 40 years old as illustrated in Figure 17. Previous CHD (any of previous MI, angina, PCI or CABG) is positively correlated with treatment cost as are all other

© Queen's Printer and Controller of HMSO 2007 118
comorbidities. Variables with particularly large coefficients are peripheral vascular disease and cerebrovascular disease. Unsurprisingly, the mean cost is lower where patients die before discharge. Finally, although the procedure costs of non primary PCI and CABG are not components of the costs calculated here, these do contribute to overall costs principally through their impact on length of stay. CABG at this admission has a large effect (£4,630) on treatment cost.
Figure 17: The effect of age on cost
-1500
-1000
-500
0
500
1000
1500
2000
20 30 40 50 60 70 80 90 100
Age (yrs)
Diff
eren
ce in
cos
t of t
reat
men
t
6.3.6 Additional coronary interventions
Table 30 shows the unadjusted numbers of patients who underwent PCI or CABG within one year of admission. The probability of subsequent PCI was significantly higher for thrombolysis patients compared to primary PCI patients, irrespective of whether the thrombolysis was given in a control site or a NIAP site. The probability of a subsequent CABG was significantly higher only in thrombolysis patients in the NIAP sites. There was no statistically significant difference between primary PCI patients and thrombolysis patients in the control sites.
Table 30: Additional cardiac interventions up to one year
NIAP Control York model
PPCI (n=1398) Lysis (n=330) Lysis (n=667) PPCI Lysis
PCI 244 17.4% 79 23.9%* 149 22.3%* 5.4% 28.1%
CABG 33 2.4% 21 6.4%* 20 3.0% 5.4% 7.1%
* p<0.01 compared to NIAP PPCI group
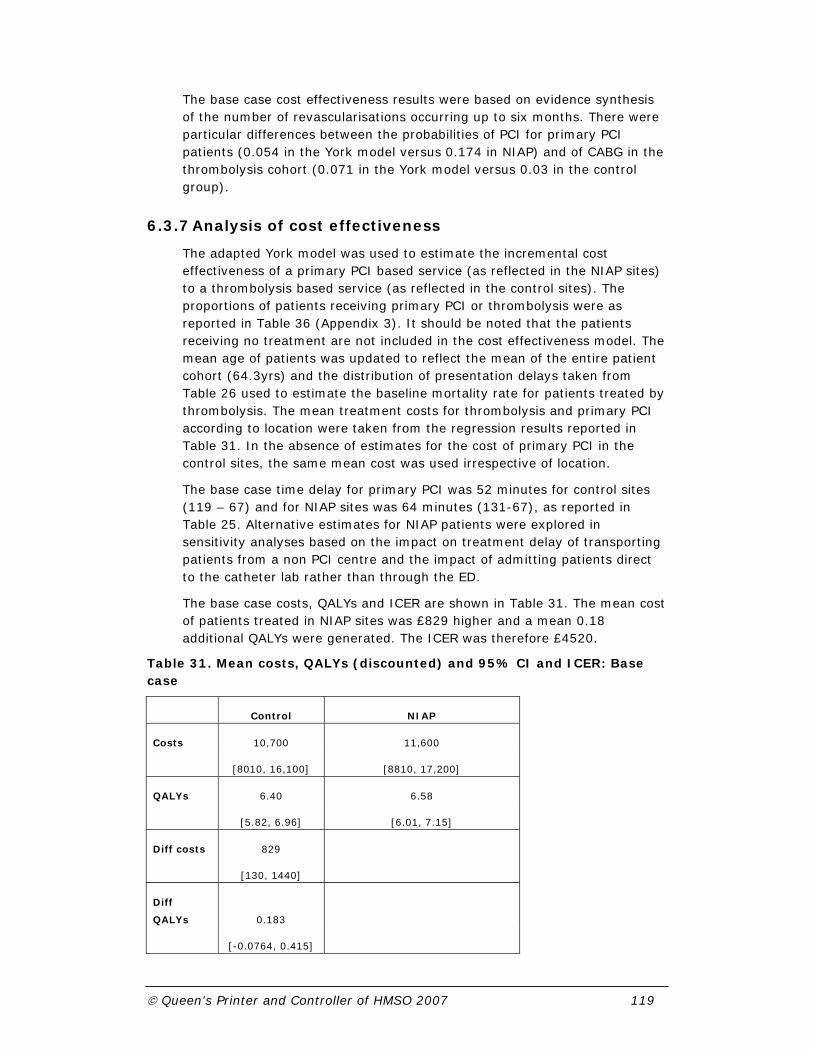
© Queen's Printer and Controller of HMSO 2007 119
The base case cost effectiveness results were based on evidence synthesis of the number of revascularisations occurring up to six months. There were particular differences between the probabilities of PCI for primary PCI patients (0.054 in the York model versus 0.174 in NIAP) and of CABG in the thrombolysis cohort (0.071 in the York model versus 0.03 in the control group).
6.3.7 Analysis of cost effectiveness
The adapted York model was used to estimate the incremental cost effectiveness of a primary PCI based service (as reflected in the NIAP sites) to a thrombolysis based service (as reflected in the control sites). The proportions of patients receiving primary PCI or thrombolysis were as reported in Table 36 (Appendix 3). It should be noted that the patients receiving no treatment are not included in the cost effectiveness model. The mean age of patients was updated to reflect the mean of the entire patient cohort (64.3yrs) and the distribution of presentation delays taken from Table 26 used to estimate the baseline mortality rate for patients treated by thrombolysis. The mean treatment costs for thrombolysis and primary PCI according to location were taken from the regression results reported in Table 31. In the absence of estimates for the cost of primary PCI in the control sites, the same mean cost was used irrespective of location.
The base case time delay for primary PCI was 52 minutes for control sites (119 – 67) and for NIAP sites was 64 minutes (131-67), as reported in Table 25. Alternative estimates for NIAP patients were explored in sensitivity analyses based on the impact on treatment delay of transporting patients from a non PCI centre and the impact of admitting patients direct to the catheter lab rather than through the ED.
The base case costs, QALYs and ICER are shown in Table 31. The mean cost of patients treated in NIAP sites was £829 higher and a mean 0.18 additional QALYs were generated. The ICER was therefore £4520.
Table 31. Mean costs, QALYs (discounted) and 95% CI and ICER: Base case
Control NIAP
Costs 10,700 11,600
[8010, 16,100] [8810, 17,200]
QALYs 6.40 6.58
[5.82, 6.96] [6.01, 7.15]
Diff costs 829
[130, 1440]
Diff
QALYs 0.183
[-0.0764, 0.415]

© Queen's Printer and Controller of HMSO 2007 120
ICER 4520
The cost effectiveness acceptability curve Figure 18 shows the probability that treatment with PCI based care, as used in the NIAP hospitals, would be cost effective across a range of values that a decision maker might be willing to pay for an additional QALY. At a willingness to pay (WTP) of £20k per QALY, the probability that NIAP would be cost effective is approximately 0.9.
Figure 18: Cost effectiveness acceptability curve – Base case
0 20000 40000 60000 80000 100000 120000 140000
0.0
0.2
0.4
0.6
0.8
1.0
Cost-effectiveness acceptability
WTP (£)
prob
abili
ty
ICER
Table 37 (Appendix 3) shows the differences in short term event rates, Table 38 (Appendix 3) the differences between strategies and treatments in terms of costs, while Table 39 (Appendix 3) shows the mean QALYs and life years gained.
Two issues were explored in sensitivity analysis: the additional treatment delay associated with primary PCI and the rate of revascularisations. For treatment delay we considered the impact of inter-hospital transfer and of ED or CCU bypass for primary PCI patients.
Overall, transferred patients had a median additional treatment delay of 100 minutes (167 – 67 mins, see Table 25). The impact of this additional delay could eliminate or even reverse the mortality benefit of primary PCI. The point estimate in this evaluation was that treatment in a control site dominated PCI based care in this situation, that is, it was less costly and more effective (see Table 32). However, the confidence intervals for costs and effects both cross zero, so there is considerable uncertainty. The probability that PCI-based care was cost effective for these patients was approximately 0.4 at the £20,000 threshold and never exceeded 0.45, irrespective of the willingness to pay threshold.

© Queen's Printer and Controller of HMSO 2007 121
Table 32: Differences in Costs and Utilities (NIAP – Control), ICER of the means: transferred patients
Mean SE 95%-CI Diff. Costs 664 585 [-324, 1390] Diff. Utilities -0.0848 0.300 [-0.831, 0.343]
ICER Control
dominates
The shortest median time delay, of 20 minutes (87-67, see Table 25), was recorded among patients who bypassed the ED or CCU and were taken directly to the catheter lab. Table 33 shows the costs and QALYs associated with this approach. The ICER for this system was £2730 and the probability it would be considered cost-effective at the £20,000 threshold was over 0.95. This compares to an ICER of £6112 for patients arriving via the ED or CCU and a probability of 0.75 that this would be considered cost-effective at the £20,000 threshold.
Table 33: Differences in Costs and Utilities (NIAP – Control), ICER of the means: direct to catheter lab at PCI site.
Mean SE 95%-CI Diff. Costs 969 518 [227, 1710] Diff. Utilities 0.355 0.121 [0.135, 0.597]
ICER 2730
Substituting the revascularisation rates reported in the evidence synthesis of clinical trials for the observational data identified in Table 30 increased the ICER to £7070, as shown in Table 34, since the benefit of primary PCI was less, particularly in terms of the rate of repeat PCI. The probability NIAP would be cost effective in this scenario is approximately 0.9 at a willingness to pay of £20k per QALY.
Table 34: Differences in Costs and Utilities (NIAP – Control), ICER of the means: observational data on revascularisations
Mean SE 95%-CI Diff. Costs 1300 504 [595, 1900] Diff. Utilities 0.183 0.128 [-0.0764, 0.415]
ICER 7070

© Queen's Printer and Controller of HMSO 2007 122
6.4 Discussion
This analysis used patient level data to estimate the mean cost of the initial treatment episode and the time to treatment for primary PCI and thrombolysis patients in the UK NHS. These estimates were used to update an existing model of cost effectiveness. The new parameter values reflected actual duration of stay, the specific types of drugs, including thrombolytics used, the actual consumables used including stents and drug eluting stents by type whereas the previous version of the model relied on assumed typical patterns of usage by procedure. The methods used to estimate mean treatment cost used a framework that respects both the skewed and clustered nature of the data.
The estimates of the mean cost of the initial treatment episode used in the York model were not substantially different to those estimated here. For thrombolysis the mean cost was £2,850 compared to £3,509 in the control sites and £4,361 in the NIAP sites. For primary PCI the mean cost was £5,329 compared to £5,176 in this analysis. There were substantial differences between the two sets of estimates in terms of the component costs and it should also be recognised that the base cost years were not the same.
The estimates of mean treatment cost presented in this report demonstrate that the cost of the initial treatment episode differed significantly between NIAP and control sites and between primary PCI and thrombolytic treated patients.
The additional treatment delay associated with primary PCI was slightly in excess of one hour but this varied substantially between patients that were transferred from another hospital and patients that were taken directly to the catheter lab.
Overall the NIAP primary PCI based service was very likely (90% probable) to be considered cost effective but the impact of additional treatment delays was important. The average additional delay for patients transferred from other hospitals was such that the primary PCI based service was unlikely to be considered cost effective in this situation. At the other extreme, the benefits were greatest, and consequently cost effectiveness was most favourable, in patients with the shortest additional treatment delay. These were patients not transferred from another hospital who bypassed the ED and CCU.
There are limitations to this study. The provision of primary PCI is rapidly evolving and the data used in this study may already be out of date. The analysis reflects practice as it was between 2005 and 2006. This creates an inconsistency between the time the data were collected and the unit cost data. Practice may have changed in order to reflect changed unit costs. For example, it may be case that the types of drug eluting stents used in practice now reflect the substantial differences in the prices paid by trusts. Furthermore, as systems develop we might anticipate that time delays associated with primary PCI would decrease. Analysis in section 3.3.3

© Queen's Printer and Controller of HMSO 2007 123
suggested a small improvement in time delays for patients attending a PCI centre directly but no improvement in time delays for transferred patients.
It is not possible to consider patients that receive no treatment in the cost effectiveness analysis. Our analysis identified that there were significant differences between the untreated populations, though not in terms of their cost. It seems unlikely that this limitation would significantly influence the results.
National agreements on staffing for out of hours work have been used in this analysis but this is likely to vary in practice across sites. Current arrangements may not be considered sustainable in the long term (see chapter 4 on workforce implications) which could increase costs beyond those attributed here.
We do not have detailed information on the cost of primary PCI in the control sites and therefore assume an equal cost to the NIAP sites. Given that there are substantial differences in the cost of thrombolytic treatment between the two systems there may also be differences between primary PCI patients.
Whilst we have incorporated both the impact of presentation delay to estimate baseline mortality and additional primary PCI treatment delay, this is hampered by the limited available evidence.
Finally, the rate of prehospital thrombolysis in the control cohort was relatively low. It could therefore be argued that we did not compare the NIAP hospitals to the best alternative, although we did compare then to the real-life alternative. The effectiveness and cost-effectiveness of PCI depends upon the delay between when thrombolysis could have been given and when PCI was given. If more widespread use of prehospital thrombolysis reduced call to needle times in thrombolysis-based practice then the potential effectiveness and cost-effectiveness of PCI would be reduced.
Implications for practice
Primary PCI based services appear to represent a cost-effective use of resources. However, it is important that treatment delays are minimised as the service will not be cost-effective if patients sustain significant treatment delays. In this analysis, transfer of patients from a non-primary PCI site to a primary PCI site was unlikely to be considered cost-effective and may have been less effective than thrombolysis based care. If time delays associated with transfer cannot be reduced, it may be better to give thrombolysis to patients presenting to a non-primary PCI site than transfer for primary PCI. The most obvious solution would be for ambulance services to ensure that suspected STEMI patients bypass the non-primary PCI centre, even if it is the nearest hospital, and transport the patient directly to the primary PCI hospital. There are two caveats to note here. The first is that misdiagnoses will incur additional costs to the system and steps should be taken to minimise their occurrence. Second, local geographical circumstances must be considered. There may be situations where inter hospital transfers can be achieved within acceptable time limits and other situations where delays are excessive even with bypass.

© Queen's Printer and Controller of HMSO 2007 124
Primary PCI systems which bypassed the ED or CCU were more likely to be effective and cost effective than those that did not. If we are willing to pay £20,000 per QALY gained then the probability that direct to catheter lab primary PCI would be considered cost-effective exceeded 95%. This probability was only 75% if patients arrived via the ED or CCU. Rapid and direct access to the catheter lab is therefore important for ensuring an effective and cost-effective service.

© Queen's Printer and Controller of HMSO 2007 125
7 Overview of the evaluation
In this section we provide an overview of the key findings of each component of the evaluation and integrate findings from the separate components by identifying common themes.
7.1 Key findings
7.1.1 Models of service delivery The NIAP study has shown that primary PCI was feasible in a wide
variety of settings and achieved acceptable call to balloon times
for most patients, although not all the hospitals were able to
provide a 24/7 service during the pilot year.
Call to balloon times depended upon the route taken to the
catheter laboratory and were markedly shorter if the patient
was transferred directly rather than via the ED or CCU.
Call to balloon times were longer when patients were transferred
from a non-PCI centre. The time delays incurred were such that
promptly administered thrombolysis at the non-PCI centre may
have been as effective in these circumstances.
7.1.2 Workforce implications and issues of implementation and feasibility
Planned implementation of a 24-hour primary PCI service from
the outset appeared to work better than incremental
development by gradual expansion.
Failure to plan (and possibly harmonise) staff pay and conditions
at the outset, particularly for out of hours work, may lead to
difficulties with sustaining the service if staff are paid in
different ways for similar commitments.
Staff needed to be prepared to multi-task and work across
traditional task and department boundaries.
On-going training was required to develop staff experience,
maintain confidence and skills and retain staff.
© Queen's Printer and Controller of HMSO 2007 126
A dedicated manager could help to control resources and balance
elective and emergency use of the catheter lab. This individual
should not have clinical responsibilities and should be proactive
to motivate and sustain service development.
A direct, simple pathway into the system, facilitated by a specified
gatekeeper, could reduce time delays.
Regular audit of the efficiency of the pathway was needed to find
solutions to blockages that reduce the capacity of the system.
Stakeholders, especially ambulance services and emergency
departments, needed to be engaged in the change
management process. This could be helped by the active
involvement of senior management and the presence of a
specific individual to act as a primary PCI champion.
Excessive focus upon emergency care with primary PCI may have
resulted in the neglect of other services, such as rehabilitation.
7.1.3 Patient and carer perspectives Overall, patients and carers had high levels of satisfaction with
primary PCI and thrombolysis-based care.
Patients reported particularly high levels of satisfaction with the
speed and efficiency of primary PCI services, and a high level
of confidence in the treatment provided.
Carers were concerned about travelling longer distances to visit
patients but this was accepted in the context of the provision of
optimal patient care.
Satisfaction with both PCI and thrombolysis-based care was lower
in relation to issues around discharge home, aftercare and
rehabilitation than for other aspects of care.
7.1.4 Economic evaluation Primary PCI was a more expensive treatment than thrombolysis,
but was associated with reduced length of hospital stay
Overall, the initial treatment episode in the NIAP PCI-based
service was more expensive than in the thrombolysis-based
control service
Although the NIAP service was more expensive than
thrombolysis-based care it was very likely (around 90%) to be

© Queen's Printer and Controller of HMSO 2007 127
considered a cost-effective use of NHS resources according to
NICE criteria for willingness to pay for health gain
Direct access to the catheter lab, was almost certain (over 95%)
to be considered a cost-effective system, whereas access via
the emergency department or coronary care unit was less
certain, although still likely to be cost-effective (around 75%)
The delays associated with transfer from a non-PCI to a PCI
hospital meant that providing treatment in this way may be
less effective than thrombolysis and was on balance unlikely
(40% probability) to be considered cost-effective
7.2 Integration of findings
The economic evaluation showed that a primary PCI-based service was more expensive than a thrombolysis-based service but was likely to be considered a cost-effective use of NHS resources provided time delays were controlled. Findings from other components of the evaluation provide useful insights into this general conclusion. In the economic model the effect of primary PCI, and therefore cost-effectiveness, was dependent upon PCI-related delay. The descriptions of models of service delivery showed that the direct to catheter lab pathway was associated with shortest delays and was therefore the most cost-effective model. In contrast, transfer from a non-PCI centre was associated with longer delays and was unlikely to be cost-effective.
The organisational evaluation found that direct to catheter lab transfer could be facilitated by having a specified gatekeeper and was assisted by the engagement of stakeholders in the process. Given that cost-effectiveness is related to time delay, investment in developing a gatekeeper role may be worthwhile.
It is possible that time delays associated with transfer from a non-PCI centre may reduce as systems develop. However, analysis of time delays over the year of the NIAP evaluation showed no evidence of improvement in transferred patients. We must also be careful about drawing over-generalised conclusions from our data. Data presented in section 3.3.3 suggest that different NIAP sites (and their feeder hospitals) have different time delays for transferred patients. Since the participating hospitals were self-selected we might anticipate that other hospitals would struggle to match the performance reported here.
The obvious alternative solution for patients brought by ambulance to a non-PCI centre is to bypass the local hospital and transfer directly to the PCI-centre. This will involve travelling a longer distance and in some settings may still not avoid excessive delays, especially in comparison to prehospital thrombolysis. It also does not solve the problem of how to manage patients who self-present to a non-PCI centre.

© Queen's Printer and Controller of HMSO 2007 128
The key issue to note here is that there is no universal “right” answer that can be applied throughout the NHS. The best system will depend upon local geography, facilities and transport options. The suggestion that primary PCI may be cost-effective in some settings but not others is controversial, and may be considered to imply a “postcode lottery”, but this would be a major misinterpretation. A postcode lottery implies provision of services on a haphazard basis. The decision to provide primary PCI or thrombolysis can be rationally made on the same explicit criteria and yet result in different services being recommended in different settings.
The crucial factor is the PCI-related delay, i.e. the difference between the time when thrombolysis would have been administered and when balloon inflation occurs. If the PCI-related delay exceeds 90 minutes then the benefits of PCI are uncertain and may even be negative in comparison to thrombolysis. The probability that PCI will be considered cost-effective falls as PCI-related delay approaches 90 minutes and if this threshold is exceeded then thrombolysis should be preferred.
Primary PCI as a procedure costs more to provide than thrombolysis. Some of these additional costs may be offset by reducing hospital length of stay, but additional costs will need to be found to support the service. Furthermore, it is not clear how costs saved by reducing length of stay will be released unless the number of acute beds is actually reduced. Providing primary PCI is therefore likely to require additional funding.
Other elements of the evaluation provide insights into the practicalities of supporting a primary PCI service and the potential knock-on effects. Shortcomings in discharge processes, aftercare and rehabilitation were identified as potential problems by the organisational evaluation and as a source of patient and carer dissatisfaction. If cardiac care resources are redirected towards acute management then discharge, aftercare and rehabilitation could be further neglected. This may be counterproductive. Difficulties associated with arranging take-home medication were identified as a potentially important cause of delayed discharge. If discharge arrangements are neglected then reductions in length of stay associated with PCI may be lost.
The costing of primary PCI was based upon data collected from the NIAP sites and national unit costs. However, the workforce evaluation suggested that at least some of the NIAP sites were using staffing arrangements that were unlikely to be sustainable in the long-term and recommended planning and harmonisation of pay and conditions when the service is first provided. Although this may provide a more sustainable arrangement it is also likely to increase the cost of providing primary PCI. The economic analysis suggested that the incremental cost-effectiveness ratio of primary PCI was well within the NICE threshold, so it is unlikely that increased costs will render primary PCI uneconomic, but potential additional costs need to be taken into account when setting a tariff for primary PCI.
Our evaluation gave us the opportunity to explore some issues from both staff and patient perspectives and address specific concerns about primary PCI:
© Queen's Printer and Controller of HMSO 2007 129
• Focus groups showed that some catheter lab staff were concerned that they were not trained or able to reassure patients’ relatives while they were waiting during the intervention. In contrast, the patient and carer research showed that, on the whole, carers valued being kept informed and generally had a high level of satisfaction with the support and reassurances that they received. Carers in NIAP sites were significantly more satisfied with the opportunity to ask questions to staff. It therefore appears that, despite their concerns, staff were providing appropriate support and reassurance.
• Ambulance staff expressed concern about the management of pain while bringing patients into hospital. However, few patients (<2%) rated the management of pain as “fair” or “poor” in the patient and carer research and patients within the NIAP sites had higher satisfaction with the ambulance journey. Again this suggests that, despite their concerns, staff were providing an adequate service. Alternatively, it may reflect limitations in the use of current methods to elicit negative aspects of the patient experience.
• Staff described that patients felt they had “been fixed” by the intervention procedure and therefore did not feel they had to change their lifestyle to reduce the chance of further cardiac problems. This same point was found in the patient and carer research and highlights the importance of addressing appropriate aftercare and cardiac rehabilitation.
7.3 Limitations of the evaluation
We have discussed limitations of each specific methodology in the sections relating to each component of the evaluation. Here we will consider two general limitations of the evaluation that applied across the individual components.
7.3.1 Generalisability of the findings
The NIAP sites were not randomly sampled from NHS hospitals and may therefore not be representative of NHS practice. This was recognised in the individual elements of our evaluation. In the description of models of service delivery we highlighted that the NIAP sites tended to serve a more urban population, with younger mean age and higher prevalence of ethnic minority population and unemployment than the general UK population. However, the NIAP sites did represent a wide variety of different settings, including rural locations, and implementation did not appear to differ markedly between settings.
The workforce and organisation of NIAP sites may also not be representative of the NHS in general. The selection process for the NIAP project involved sites putting themselves forward and demonstrating that they would be capable of pioneering the service. It is therefore likely that

© Queen's Printer and Controller of HMSO 2007 130
the participating centres were at least led, if not staffed, by enthusiasts and those who were keen to embrace change. This observation is unlikely to cast doubt upon the various barriers we identified in the workforce evaluation, but it would be reasonable to speculate that less enthusiastic sites might identify other or more severe barriers to implementation.
7.3.2 Sustainability of primary PCI
Our evaluation took place over the initial establishment of primary PCI at most sites, although some had been providing this service for up to several years before the evaluation. It is therefore difficult to determine whether primary PCI as established in the NIAP evaluation is sustainable in the longer term, although the workforce evaluation identified areas of concern. Different staff groups were being asked to develop new ways of working, particularly with regard to out of hours work. This tended to cause difficulties if different staff groups were paid in different ways for out of hours work or if staff, having chosen a particular career path expecting most work to be office hours, were increasingly being asked to work out of hours. These problems may be manageable in the short term but may produce a substantial threat to the service in the long term.
Cardiology technicians in particular are in short supply and vulnerable to “poaching” by other centres offering work without out of hours commitments. Lack of cardiac technicians may threaten the sustainability of a primary PCI service and may also have knock-on effects on elective services in the same centre, especially if out of hours working is complemented by time off the next working day (which may be unpredictable). This can lead to reduced staff availability for elective clinics.
7.4 Overview of recommendations for policy and practice
The NIAP evaluation has shown that primary PCI was feasible in a variety of settings (although not always delivered 24/7), was acceptable to patients and carers, was generally supported by staff, and although more expensive than thrombolysis was likely to be a cost-effective use of NHS resources. However, time delays varied significantly between different models of service delivery. Effectiveness, and therefore cost-effectiveness, of primary PCI depends upon time delay, so it is not appropriate to make a general recommendation about whether primary PCI or thrombolysis should be the treatment of choice across the whole NHS. Instead, this decision should be made on a regional basis, using the data presented in this report and elsewhere. In particular, rural areas are more likely to have longer prehospital time delays and were under-represented in the NIAP sample. Our recommendations may not be applicable to rural areas.
In this evaluation primary PCI was unlikely to be cost-effective for patients transferred after first attending a non-PCI hospital. Thrombolysis should therefore continue to be provided for patients attending a non-PCI hospital unless systems can be established and demonstrated to achieve acceptable
© Queen's Printer and Controller of HMSO 2007 131
times delays. Bypassing the nearest hospital provides an obvious solution for reducing transfer-related delays in ambulance-borne patients. Local geography and health service configuration will determine whether this process results in time delays that might impair cost-effectiveness.
If primary PCI can be delivered within an acceptable timeframe then it is likely to be cost effective. We make the following recommendations to guide policymakers and practitioners who decide to implement a primary PCI service:
• Patients should access the catheter lab by the most direct route possible, bypassing the ED or CCU. A specified gatekeeper at the PCI centre who is available 24 hours a day to accept primary PCI referrals may assist this process.
• Primary PCI should be implemented by planning the full service from the beginning rather than incrementally building up. Staff pay and conditions should be planned to support the full service from the start, rather than gradually changing working patterns in response to an increasing workload.
• Attempts should be made to harmonise staff pay and conditions for out of hours work so that different staff groups are not being paid in different ways for the same pattern of work.
• Stakeholders, such as ambulance services and emergency departments, should be engaged in the service. This can be assisted by the involvement of senior management and an appropriate champion for the primary PCI service.
• Dedicated catheter lab managers should be used to manage resources effectively.
• Cardiac service managers should ensure that development of primary PCI does not come at the expense of discharge, aftercare and rehabilitation services.
• The source of additional resources required to support primary PCI should be identified. These resources should be sustainable and adequate to support the changes in staff pay and conditions required to implement the service.
• Overnight accommodation should be provided or travel costs reimbursed for carers who have to travel a significant distance from their home to the PCI centre.
7.5 Suggestions for future research
As discussed previously, the effectiveness (and therefore cost-effectiveness) of primary PCI compared to thrombolysis inevitably depends upon local factors, such as the availability of services, distances travelled to access services and transport options. Hence the decision to provide primary PCI should be made on a regional basis, particularly in rural areas where NIAP data is least applicable and where prehospital thrombolysis is most likely to

© Queen's Printer and Controller of HMSO 2007 132
be beneficial. However this does not mean that it should be made on the basis of guesswork. We have reasonable data to estimate the relationship between anticipated time delays and the effectiveness of primary PCI. Economic modelling can use these data to estimate the likely cost-effectiveness of primary PCI.
Our economic model provides an overall estimate of the cost-effectiveness of primary PCI across the NIAP sites. This approach could be adapted to generate specific estimates of cost-effectiveness of primary PCI in different settings. This would also probably require modelling of STEMI epidemiology and anticipated time delays with different potential systems of care. Further research is therefore required to develop a model of STEMI care that could be applied to different regions to generate specific estimates of cost-effectiveness.
Patient, carer and workforce evaluations revealed concerns about the quality of discharge arrangements, aftercare and rehabilitation. Future research should not just focus upon emergency management but should identify ways of improving care at the end of, and after, acute hospital admission.
References
Asseburg C, Bravo Vergel Y, Palmer S, Fenwick E, de Belder M, Abrams K and Sculpher M. Assessing the effectiveness of primary angioplasty compared to thrombolysis and its relationship to time delay: a Bayesian evidence synthesis. Heart 2007;93:1244-50.
Asseburg C, Bravo Vergel Y, Palmer S, Fenwick E, Abrams K, de Belder M, Sculpher M et al. A cost-effectiveness analysis comparing primary percutaneous coronary interventions to thrombolytic therapy for acute myocardial infaction. Centre for Health Economics Technical Report, 2005.
Astin F, Hunter S, Priestley C, McLenachan J, Jose Closs S. Eur J Cardiovasc Nursing 6[S1], S21. 2007
Ayanian JZ, Landrum MB, Guadagnoli E, Gaccione P. Specialty of ambulatory care physicians and mortality among elderly patients after myocardial infarction. N Engl J Med 2002; 347:1678-86.
Boersma E, Maas ACP, Deckers JW, Simoons ML. Early thrombolytic treatment in acute myocardial infarction: reappraisal of the golden hour. Lancet 1996; 348: 771-75
Boersma E and the PCAT-2 Trialists’ Collaborative Group. Does time matter? A pooled analysis of randomized clinical trials comparing primary pertcutaneous coronary intervention and in-hospital fibrinolysis in acute myocardial infarction patients. Eur Heart J, 2006, 27:779-788.
Bonnefoy E, Lapostolle F, Leizorovicz A et al for the CAPTIM study group. Primary angioplasty versus prehospital fibrinolysis in acute myocardial infarction: a randomised study. Lancet 2002; 360:825-829

© Queen's Printer and Controller of HMSO 2007 133
Borrill, C.S., West, M.A., Wall, T.D., Shapiro, D.A., Haynes, C.E., Stride, C. Woods, D., & Carter, A.J. (1998) Stress among staff in NHS Trusts. Published by the Institute of Work Psychology, University of Sheffield, England.
Boyle R. Mending hearts and brains - clinical case for change. 2006. London, Department of Health.
Braun, V. & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3, 77-101.
Bravo Vergel Y. Palmer S. Asseburg C. Fenwick E. de Belder M. Abrams K. Sculpher M. Is primary angioplasty cost effective in the UK? Results of a comprehensive decision analysis. Heart 2007;93:1238-43
British Cardiovascular Society. National Infarct Angioplasty Project (NIAP). http://www.bcs.com/pages/full_news.asp?NewsID=2154 . 2005.
British National Formulary, September 2007, Vol.54.
Bryman, A. & Bell, E. (2003). Business Research Methods. Oxford University Press.
Canto JG, Every NR, Magid DJ et al. The volume of primary angioplasty procedures and survival after acute myocardial infarction. National Registry of Myocardial Infarction 2 Investigators. N Engl J Med 2000;342:1573-80.
Carter, A. J., & West, M. A. (1999). Sharing the burden - teamwork in health care settings. In R. Payne & J. Firth-Cozens (Eds.). (pp. 191- 202). Stress in Health Professionals: Psychological and organisational causes and Interventions. Chichester: Wiley.
Carter, A.J. (2000). Sharing the burden: A study of teamwork and well-being in secondary health care teams. Unpublished doctoral dissertation, Institute of Work Psychology, University of Sheffield, Sheffield.
CCAD NIAP dataset http://www.ic.nhs.uk/our-services/improving-patient-care/heart-disease/infarct-angioplasty
Cook S, Walker A, Hugli O, Togni M, Meier B. Percutaneous coronary interventions in Europe: prevalence, numerical estimates, and projections based on data up to 2004. Clin Res Cardiol 2007; 96(6):375-382.
Creswell, J. W., & Plano-Clark, V. (2007). Designing and conducting mixed methods research. Thousand Oaks, CA: Sage Publications.
Crow R, Gage H, Hampson S, Hart J, Kimber A, Storey L et al. The measurement of satisfaction with healthcare: implications for practice from a systematic review of the literature. Health Technol Assess 2002; 6 (32)
Cucherat, M., E. Bonnefoy, and G. Tremeau, Primary angioplasty versus intravenous thrombolysis for acute myocardial infarction.[update of Cochrane Database Syst Rev. 2000;(2):CD001560; PMID: 10796812]. Cochrane Database of Systematic Reviews, 2004. 3.
Curtis L. Costs of health and social care 2007. Kent: Personal Social Services Research Unit, 2007.

© Queen's Printer and Controller of HMSO 2007 134
Dalby M, Bouzamondo A, Lechat P, Montalescot G. Transfer for primary angioplasty versus immediate thrombolysis in acute myocardial infarction - A meta-analysis. Circulation 2003;108:1809-1814.
Department of Health. National Infarct Angioplasty Project (NIAP) Interim report. 2008
Flanagan JC. The critical incident technique. Psychol Bull 1954; 51:327-358.
Frone, M.R., Russel, M., & Cooper, M.L. (1992). Antecedents and outcomes of work-family conflict: Testing a model of the work-family interface. Journal of Applied Psychology, 77, (1), 65-78.
Fye WB. Introduction: The origins and implications of a growing shortage of cardiologists. J Am Coll Cardiol 2004;44:221-32.
Goodacre S, Sampson F. Evaluating the National Infarct Angioplasty Project Pilots. http://www.library.nhs.uk/cardiovascular/Page.aspx?pagename=ED21 . 2006.
Goodacre SW, Quinney D, Revill S, Morris F, Capewell S & Nicholl J. Patient and Primary Care Physician Satisfaction with Chest Pain Unit and Routine Care. Acad Emerg Med 2004;11:827-833.
Grimes DA. The uncritical acceptance of medical intervention. JAMA 1993; 269:3030-3033.
Grines CL Marsalese DL, Brodie B et al. Safety and cost-effectiveness of early discharge after primary angioplasty in low risk patients with acute myocardial, infarction. PAMI-II Investigators. Primary Angioplasty in Myocardial Infarction. J Am Coll Cardiol 1998; 31(5):967-972.
Gulanick M, Bliley A, Perino B, Keough V. Patients’ responses to the angioplasty experience: a qualitative study. Am J Crit Care 1997; 6:25-32.
Gulanick M, Naito A. Patients' reactions to angioplasty: realistic or not? Am J Crit Care 1994; 3(5):368-373.
Hartwell D, Colquitt J, Loveman E, et al. Clinical effectiveness and cost-effectiveness of immediate angioplasty for acute myocardial infarction: systematic review and economic evaluation. Health Technol Assess 2005;9.
Haynes, C.E., Wall, T.D., Bolden, R.I, Stride, C.B & Rick, J.E. (1999). Measures of perceived work characteristics for health service research: Test of a measurement model and normative data. British Journal of Health Psychology, 4, 257-275.
Heyland DK, Gafni A, Levine MA. Do potential patients prefer tissue plasminogen activator (TPA) over streptokinase (SK)? An evaluation of the risks and benefits of TPA from the patient's perspective. J Clin Epidemiol 2000;53:888-94.
Kansagra SM, Curtis LH, Schulman KA. Regionalization of percutaneous transluminal coronary angioplasty and implications for patient travel distance. JAMA 2004;292:1717-23.

© Queen's Printer and Controller of HMSO 2007 135
Kaptchuk TJ, Goldman P, Stone DA, Statson WB. Do medical devices have enhanced placebo effects? J Clin Epidemiol 2000; 53:786-792.
Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003; 361: 13–20.
Keeley EC, Grines CL. Primary percutaneous coronary intervention for every patient with ST-segment elevation myocardial infarction: what stands in the way? Ann Intern Med 2004;141:298-304.
King, N. (2004). Using interviews in qualitative research. In C. Cassell & G. Symon (Eds.) Essential Guide to Qualitative Methods in Organisational Research. (pp. 11-22). Sage. London.
LeMay MR, So DY, Dionne R, Glover CA et al. A citywide protocol for Primary PCI in ST-segment elevation Myocardial Infarction. NEJM 2008; 357:231-40
Magid DJ, Calonge BN, Rumsfeld JS et al. Relation between hospital primary angioplasty volume and mortality for patients with acute MI treated with primary angioplasty vs thrombolytic therapy. JAMA 2000;284:3131-8.
Manning W G. Mullahy J. Estimating log models: to transform or not to transform? Journal of Health Economics 2001; 20:461-494.
MINAP steering group. How the NHS manages heart attacks. Sixth public report on the Myocardial Infarction National Audit Project (MINAP). 2007. London, Royal College of Physicians.
Morrison LJ, Verbeek PR, McDonald AC, Sawadsky BV, Cook DJ. Mortality and prehospital thrombolysis for acute myocardial infarction: a meta-analysis. JAMA 2000; 238:2686-2692.
NHS National Schedule of Reference Costs 2006-07 for NHS trusts.
Nicholl J and Turner J. Effectiveness of a regional trauma system in reducing mortality from major trauma. BMJ 1997;315:1349-54.
Niles N et al. Using qualitative and quantitative patient satisfaction data to improve the quality of cardiac care. Joint Commission Journal on Quality Improvement 1996; 22: 323-35.
O'Cathain, A., Murphy, E., & Nicholl, J. (2007). Integration and publications as indicators of 'yield' from mixed methods studies Journal of Mixed Methods Research 1(2), 147-163.
O’Cathain A, Thomas KJ. “Any other comments?” Open questions on questionnaires – a bane or a bonus to research? BMC Medical Research Methodology 2004,4:25
Person SD, Allison JJ, Kiefe CI et al. Nurse staffing and mortality for Medicare patients with acute myocardial infarction. Med Care 2004;42:4-12.
Poses RM, Krueger JI, Sloman S, Elstein AS. Physicians' judgements of survival after medical management and mortality risk reduction due to revascularisation procedures for patients with coronary heart disease. Chest 2002; 122:122-133.

© Queen's Printer and Controller of HMSO 2007 136
Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Bryman, Burgess, editors. Analysing qualitative data. London: Routledge, 1994: 173-194.
Rydman RJ, Zalenski RJ, Roberts RR, Albrecht GA, Misieswicz VM, Kampe L et al. Patient satisfaction with an emergency department chest pain observation unit. Ann Emerg Med 1997; 29:109-15.
Stanek EJ, Cheng JW, Peeple PJ, Simko RJ, Spinler SJ. Patient preferences for thrombolytic therapy in acute myocardial infarction. Med Decis Making 1997;17:464-71.
Stone GW, Grines CL, Rothbaum D et al. Analysis of the relative costs and effectiveness of primary angioplasty versus tissue-type plasminogen activator: the Primary Angioplasty in Myocardial Infarction (PAMI) trial. The PAMI Trial Investigators. J Am Coll Cardiol 1997;29:901-7.
Stride, C.B., Wall, T.D., & Catley, N. (2008). Measures of job satisfaction, organisational commitmemnt, mental health and job-related well-being: A benchmarking manual. 2nd Ed. Chichester: John Wiley & Sons, Ltd.
Tsui W, Pierre K, Massel D. Patient reperfusion preferences in acute myocardial infarction: mortality versus stroke, benefits versus costs, high technology versus drugs. Can J Cardiol 2005;21:423-31.
Warr, P.B. (1987). Work, unemployment, and mental health. Oxford: Clarendon Press.
Warr, P.B. (1990). The measurement of well-being and other aspects of mental health. Journal of Occupational Psychology, 63, 193-210.
Waters RE, Singh KP, Roe MT et al. Rationale and strategies for implementing community-based transfer protocols for primary percutaneous coronary intervention for acute ST-segment elevation myocardial infarction. J Am Coll Cardiol 2004;43:2153-9.
Wiles R. Patients' perceptions of their heart attack and recovery: the influence of epidemiological "evidence" and personal experience. Soc Sci Med 1998; 46(11):1477-1486.

© Queen's Printer and Controller of HMSO 2007 137
Appendix 1.
Workforce and organisational implications appendices
Site number: Participant:
Primary PCI Stakeholder interview Good morning/afternoon, my name is X and I would like to thank you for giving me someof your valuable time for this interview. This is one of a series of interviews we are conducting with staff in this Trust to examine how people work together when there is aPCI event. Particularly I am interested in the way the people work together to make this asuccessful procedure and how this fits in with the other work undertaken in this Trust.
This work is part of a larger study evaluating the National Infarct Angioplasty Project Pilots(NIAPP). I hope you will have seen the information sheet about the study. If not here is another copy. We are looking at all the pilot sites and some other Trusts that undertakethis type of work. These interviews are an important part of this study so many thanks foryour co-operation in this work.
This is a supportive study, no one is here to criticise what you do. We are not judging howwell this work is done; we want to know what it is like to do this work. There are no rightor wrong answers to these questions. The aim of the project is to explore how toimplement a successful angioplasty service and explore methods of working acrossdepartments. The interview will take about 55 minutes to complete and I hope that won’tcause you any problems?
Anything that you say to me/us today will be treated in confidence and NO individual will be identified. I only have your name to note that I have completed my interviews asplanned. You will be considered by the name of your role (e.g., doctor, nurse, manager) sothe data will not be traceable to you. We will examine issues today and ask for your suggestions that will be put in our final report. Further, no feedback will be given to anyone in the Trust or other organizations about the content of this interview. The studywill conclude next year and the findings will be made available to all participants.
The interview will take a little less than one hour and I have a copy of the questions foryou to have a look at to help you. Is there anything you would like to ask before we begin?Are you happy to continue? Would you mind signing the consent form? Here are the questions so you can see what we are going to talk about:
What is your role in relation to the Primary Angioplasty Team? How long have you been working with the team?
How long have the service been in operation?
Is this service a high priority for the Trust?
Have the form of this service changed over time?
What makes a successful PCI event?
What factors cause difficulties in operating this service?
Is staff attendance an issue with this team? (Sickness absence)
Describe the relationships between the Primary PCI Team and other secondary care providers?
Describe the relationships between the Primary PCI Team and other primary care providers?
How does Primary Angioplasty fit in with the other work that you do?
Can you suggest any other way of organising Primary Angioplasty work, in this Trust, that may be more effective than the way it is working now?

© Queen's Printer and Controller of HMSO 2007 138
Site number:
The Primary PCI team: teamworking interview
Good morning/afternoon, my name is X and I would like to thank you for giving me some of your valuable time for this interview. This is one of a series of interviews we are conducting with staff in this Trust to examine how people work together when there is anemergency PCI event. Particularly I am interested in the way the people work together to make this a successful procedure and how this fits in with the other work that you do.
This work is part of a larger study evaluating the National Infarct Angioplasty Project Pilots(NIAPP). I hope you will have seen the information sheet about the study. If not here is another copy. We are looking at all the pilot sites and some other Trusts that undertakethis type of work. These interviews are an important part of this study so many thanks foryour co-operation in this work.
This is a supportive study, no one is here to criticise what you do. We are not judging howwell this work is done; we want to know what it is like to do this work. There are no rightor wrong answers to these questions. The aim of the project is to explore how toimplement a successful angioplasty service and explore methods of working acrossdepartments. The interview will take about 55 minutes to complete and I hope that won’tcause you any problems?
Anything that you say to me/us today will be treated in confidence and NO individual will be identified. I only have your name to note that I have completed my interviews asplanned. You will be considered as a “nurse”, “doctor”, “radiographer” or “technician” sothe data will not be traceable to you. We will examine issues today and ask for your suggestions that will be put in our final report. Further, no feedback will be given to anyone in the department about the content of this interview. The study will conclude nextyear and the findings will be made available to all participants.
The interview will take a little less than one hour and I have a copy of the questions foryou to have a look at to help you. Is there anything you would like to ask before we begin?Are you happy to continue? Would you mind signing the consent form? Here are the questions so you can see what we are going to talk about:
How many people work in the Emergency Primary Angioplasty Team (the Cath Lab team)? Does this list match the team you know? What hours does this team operate? What is your role in this team? How does this fit in with others’ roles? Do people need to work together to achieve their tasks? What are the objectives of the team/s? (Or individuals) Who is the leader of the Primary Angioplasty Team and what do they do in their leadership role? What other teams (and individuals) do you work with? How does emergency Primary Angioplasty fit in with the other work that you do? What are the things you enjoy about Primary Angioplasty work? What things do you find a challenge about Primary Angioplasty work? Can you suggest any other way of organising emergency Primary Angioplasty work, in this Trust, that may be more effective than the way you are working now?

© Queen's Printer and Controller of HMSO 2007 139
Primary PCI focus group As people come in ask them to complete the consent form Introduction 5 minutes Good morning/afternoon, my name is X and I am a researcher working on the National Infarct Angioplasty Project Pilots (NIAPP) study. I hope you will have seen the information sheet about the study. If not here is another copy. If you are happy to take part in this discussion I would be grateful if you could sign the consent form.
This is one of a planned series of focus groups and interviews to discuss with staff involved in the angioplasty service what it is like to do this work and what makes a successful PCI event. The aim of the project is to appreciate the things that contribute to an effective service and how this may be implemented elsewhere. We are interested in your ideas of how this work can be done in the best way. So many thanks for your co-operation in this work.
This is a supportive study no one is here to criticise what you do. We will examine issues today and ask for your suggestions that will be put in our final report. Anything that you say to us today will be treated in confidence and NO individual will be identified. Identities will be protected and individuals will not be named. Further, no feedback will be given to anyone in the Trust or other organizations about the content of this interview. The study will conclude next year and the findings will be made available. It is intended that we work together for 75 minutes. Are you happy to continue? Let anyone leave who is not happy to contribute to the study. Start of group First establish that the group are people who undertake PCI themselves and exactly what hours the service operates. Note what roles are represented. 1) For the first part of the session I am going to ask you to think of a successful PCI event. Can you write down (for a few minutes keeping this to yourself) the things that made this a successful event (after this discussion we will examine events that were less than successful). Individual working for three to four minutes 3 mins Go round the group recording material on a flip chart exploring comments for specific detail 15 mins RECORD ANY MATERIAL ON A FLIP CHART FOR ANALYSIS 1a) Are there any differences in and out of hours working?
5 minutes
1b) Is this the way the service has always been run in this Trust or have there been different methods of working?
5 minutes
Site no. Group: Date:

© Queen's Printer and Controller of HMSO 2007 140
1c) Do all teams work in the same way? 3 minutes
1d) do you have many false alarms and what impact does this haveon the team? 3 minutes 2. Now I am going to ask you to think of an unsuccessful PCI event. Can you write down (for a few minutes keeping this to yourself) thethings that made this event less than successful? Individual working for three to four minutes 3 mins Go round the group recording material on a flip chart exploring comments for specific detail 10 mins RECORD ANY MATERIAL ON A FLIP CHART THAT CAN BE REMOVED FORANALYSIS. 3. What can be done with these issues? What are your suggestionsabout the way that this service can be organised to be moreeffective? Can I suggest you think about this for a few minutes and then we will goaround the group so that we can record these on the flip chart? NOTE ON CHART THE ISSUE AND A POSSIBLE SOLUTION Individual working for two or three minutes 3mins Go round group to get out ideas (2 minutes each) put these on one page andnote the number of repeats. ENCOURAGE A DEBATE AND WORKABLESOLUTIONS LOOKING FOR THE RESOURCES THAT WILL BE REQUIRED TOCARRY THIS THROUGH 10 MINS DEBATE AND DISCUSS SOLUTIONS SUGGESTING THAT IF JUST ONE GOOD IDEA COMES FROM THIS GROUP THAT WILL BE SUFFICIENT sowork it through in some detail 10 MINS Are there any other issues that you would like to describe thatinfluence the way the Primary PCI team work together? 5 mins Conclusion 1 min We have reached the end of our time now and would like to thank you foryour participation. Many thanks for your time; a copy of our findings will bemade available to all who have participated in this study. End

© Queen's Printer and Controller of HMSO 2007 141
INFORMATION SHEET
We are inviting you to take part in an important study. Before you take part, it isimportant for you to understand why the research is being done and what it will involve. Please take time to read the following information carefully and discuss itwith others, if you wish. Please do not hesitate to ask us if there is anything thatis not clear or if you would like more information (a contact is given at the foot of this document).
This project is being carried out by researchers from the Medical Care Research Unit, and Institute of Work Psychology at the University of Sheffield. This is an independent research unit that has a long history of undertaking research into the National Health Service. The project is funded by the NHS Service Delivery and Organisation Programme of Research.
What is the purpose of the study?
The aim of this study is to compare the care provided at hospitals offering a primary angioplasty service with other hospitals that continue to provide thrombolysis-based care for patients with myocardial infarction. We are assessing whether the primary angioplasty service is feasible, acceptable to patients and carers, its workforce implications and whether it gives value for money for the health service. We need to interview staff and key stakeholders in the primary angioplasty sites to find out how the teams providing the service work and explore the implications for the workforce and working methods of providing it.
Why have I been chosen?
You have been chosen to take part in this study because you are a member of staff in one of the NIAPP sites and understanding your views and experiences of working in this site are central to the project.
Do I have to take part?
It is up to you to decide whether or not to take part. When take part you will be asked to sign a consent form. You are still free to withdraw at any time.
What will happen to me if I take part?
We, the research team, Prof. Stephen Wood and Dr Angela Carter of the Institute of Work Psychology at the University of Sheffield will contact you to arrange your participation in an interview or a focus group. This will only involve you for a short period of time and you will find it interesting to discuss your work with others undertaking associated tasks. Data from the interviews and focus groups will be recorded in an anonymous form and in no way will you be identified in any way. We are the only people who will access to your data and it will be treated anonymously in any analysis or reports written.

© Queen's Printer and Controller of HMSO 2007 142
What are the possible benefits of taking part?
The information we get from this study will add greatly to our understanding of how primary angioplasty services and the impact they may have on other services. The aim is that they study will be used by policy makers and NHS managers when making decisions about angioplasty services in future.
Will my taking part in this study be kept confidential?
If you consent to take part in the research your name will not be disclosedoutside of the research team at the University of Sheffield. All of the informationyou give us will be kept strictly confidential. All data will be handled in accordancewith the Data Protection Act 1998. What will happen to the results of the research study?
You will be sent a summary of the results of the study. The results of theresearch will then be used in a report, which will be shared with the professionalsresponsible for the organisation and provision of angioplasty and othertreatments for heart attacks, and a report may be published in a medical journal.You will not be identified in any report of the study. If you would like any further information about the overall project please contact: Fiona Sampson, Medical Care Research Unit, University of Sheffield Telephone: 0114 222 0842 Or Dr Angela Carter and Prof. Stephen Wood Institute of Work Psychology University of Sheffield S10 2TN 0114 2223250 [email protected]

© Queen's Printer and Controller of HMSO 2007 143
Appendix 2
NIAPP Phase 1 - Interview schedule for angioplasty patients Introduction. Explanation about recording with digital recording. Free to withdraw whenever etc. You were admitted to (___) hospital on (day) where you had an emergency angioplasty. I’d like to hear the story about this and what you thought worked well and did not work well. 1. Thinking back to before you went into hospital, can you tell me about when you felt that something was wrong? (Prompt – symptoms, time, place) 2. Can you tell me about getting to the hospital? (Prompt for info on transfers and timings. Where the patient was transferred prompt for info on transfer – information given etc). What worked well? What could be improved? 3. Can you tell me about the decision to have an angliopasty? What worked well? What could be improved? 4. Can you tell me about having the procedure done? What worked well? What could be improved? 5. Can you tell me a bit about your hospital stay following the procedure? What worked well? What could be improved? 6. Can you tell me about being discharged from hospital? (Prompt: adequate stay in hospital, discharge information) What worked well? What could be improved? 7. Just thinking back over the whole experience, is there anything you would like to say about
How easy it was for friends and family to visit?
Asking all the questions you wanted?
Doctors and nurses telling you what you wanted to be told?
Written information given to you
Knowing what was going on
Pain relief
Waiting around for things to happen
Being comfortable
How good the doctors and nurses were at their jobs
Having the right procedure for your condition
How confident did you feel about going home? Thank you for talking to me today. The information you have given me will be looked at together with a lot of other data and the interviews will be written up in a report at the end of the project. We will produce a short summary of the results. Would you like us to send you a copy of this summary?

© Queen's Printer and Controller of HMSO 2007 144
NIAPP phase 1 interview schedule for carers Introduction. Explanation about recording with digital recording. Free to withdraw whenever etc. (___) was admitted to (___) hospital on (day) where they had an emergency angioplasty. I’d like to hear your story on this and what you thought worked well and did not work well. 1. Thinking back to before they went into hospital, can you tell me about when they felt that something was wrong? (Prompt – symptoms, time, place) 2. Can you tell me about how they got to the hospital? (Prompt for info on transfers and timings. Where the patient was transferred prompt for info on transfer – information given etc Did they accompany patient?). What worked well? What could be improved? 3. Can you tell me about when they made the decision for (___) to have an angioplasty? (Prompt forinfo on consent process) What worked well? What could be improved? 4. Can you tell me about what happened when the procedure was done? What worked well? What could be improved? 5. Can you tell me a bit about when they stayed in hospital following the procedure? What worked well? What could be improved? 6. Can you tell me about when (___) was discharged from hospital? (Prompt: adequate stay in hospital, discharge information) What worked well? What could be improved? 7. Just thinking back over the whole experience, is there anything you would like to say about
Visiting times and facilities
Asking all the questions you wanted?
Doctors and nurses telling you and (___) what you wanted to be told?
Written information provided
Knowing what was going on
Pain relief and comfort
Waiting around for things to happen
How good the doctors and nurses were at their jobs
Having the right procedure for their condition
How able you felt to care for (___) after the procedure Thank you for talking to me today. The information you have given me will be looked at together with a lot of other data and the interviews will be written up in a report at the end of the project. We will produce a short summary of the results. Would you like us to send you a copy of this summary?

© Queen's Printer and Controller of HMSO 2007 145
Patient questionnaire
NHS Study number:
On / / 200 you were admitted to (Name) Hospital where you were treated for a heart attack. Below are some questions that relate to this admission. We would be very grateful if you could answer them by ticking the boxes.
Please tick one only Q1. Thinking about your treatment and care in (Name) Hospital, how would you rate the following? Excellent Very
Good Good Fair Poor Not sure
Explanations given about what was wrong with you
Explanations given to you of the risks and benefits of your treatment
Your involvement in decisions about your treatment
Time waited before having the treatment
The efficiency with which you were treated
Your confidence in the treatment you received
The management of your pain
The management of your comfort
The ease and convenience for friends and family to visit
Please tick one only Q2. Thinking about the staff who treated you in this hospital, how would you rate the following? Excellent Very
Good Good Fair Poor Not
sure
Professional skill and ability of the doctors and nurses
Your confidence in the doctors and nurses treating you
The reassurance and support offered by the doctors and nurses
Opportunity to ask doctors and nurses all the questions you wanted to
SECTION A: Your stay in (Name) Hospital.
About this questionnaire
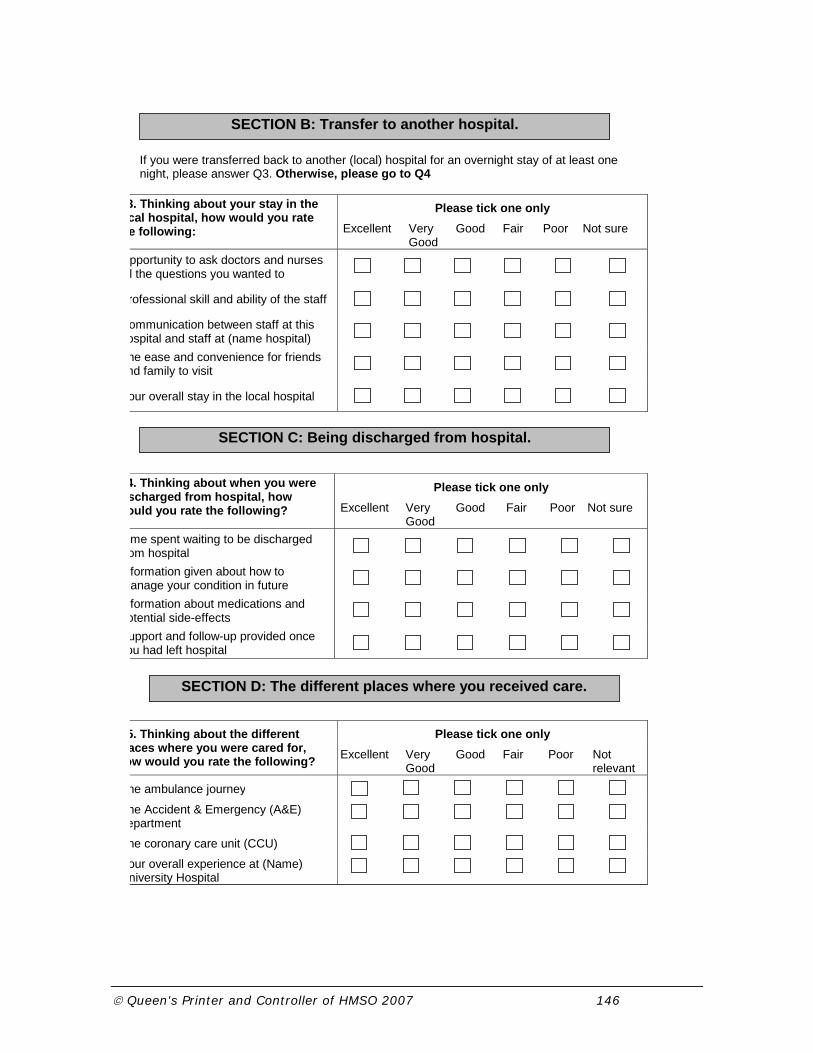
© Queen's Printer and Controller of HMSO 2007 146
If you were transferred back to another (local) hospital for an overnight stay of at least one night, please answer Q3. Otherwise, please go to Q4
Please tick one only 3. Thinking about your stay in the cal hospital, how would you rate e following: Excellent Very
Good Good Fair Poor Not sure
pportunity to ask doctors and nurses l the questions you wanted to
rofessional skill and ability of the staff
ommunication between staff at this ospital and staff at (name hospital)
he ease and convenience for friends nd family to visit
our overall stay in the local hospital
Please tick one only 4. Thinking about when you were scharged from hospital, how ould you rate the following? Excellent Very
Good Good Fair Poor Not sure
me spent waiting to be discharged om hospital
formation given about how to anage your condition in future
formation about medications and otential side-effects
upport and follow-up provided once ou had left hospital
Please tick one only 5. Thinking about the different aces where you were cared for,
ow would you rate the following? Excellent Very Good
Good Fair Poor Not relevant
he ambulance journey
he Accident & Emergency (A&E) epartment
he coronary care unit (CCU)
our overall experience at (Name) niversity Hospital
SECTION B: Transfer to another hospital.
SECTION C: Being discharged from hospital.
SECTION D: The different places where you received care.
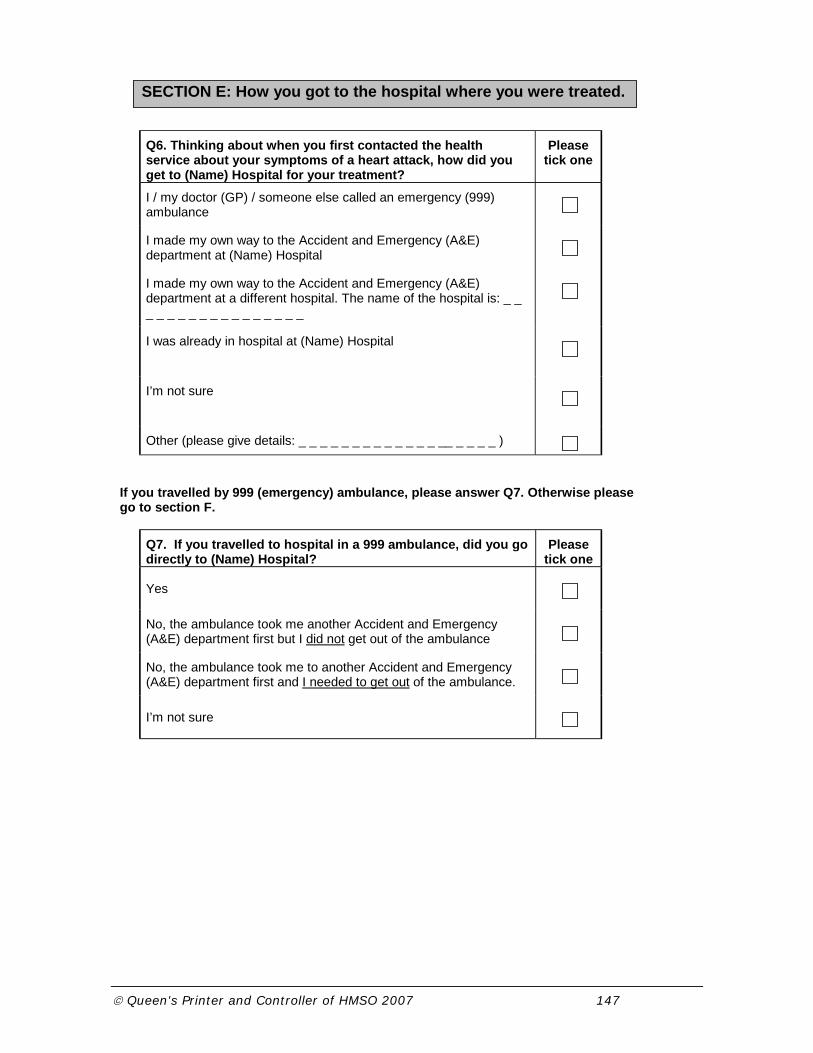
© Queen's Printer and Controller of HMSO 2007 147
Q6. Thinking about when you first contacted the health service about your symptoms of a heart attack, how did you get to (Name) Hospital for your treatment?
Please tick one
I / my doctor (GP) / someone else called an emergency (999) ambulance
I made my own way to the Accident and Emergency (A&E) department at (Name) Hospital
I made my own way to the Accident and Emergency (A&E) department at a different hospital. The name of the hospital is: _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
I was already in hospital at (Name) Hospital
I’m not sure
Other (please give details: _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ )
If you travelled by 999 (emergency) ambulance, please answer Q7. Otherwise please go to section F.
Q7. If you travelled to hospital in a 999 ambulance, did you go directly to (Name) Hospital?
Please tick one
Yes
No, the ambulance took me another Accident and Emergency (A&E) department first but I did not get out of the ambulance
No, the ambulance took me to another Accident and Emergency (A&E) department first and I needed to get out of the ambulance.
I’m not sure
SECTION E: How you got to the hospital where you were treated.

© Queen's Printer and Controller of HMSO 2007 148
Q8. What treatment did you receive for your heart attack? Please tick one
I had an angioplasty (balloon / stent)
I was treated by drugs alone
I’m not sure / don’t know
Other (please give details _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ )
Please tick one only Q9. How would you rate:
Excellent Very Good
Good Fair Poor Not sure
Your overall experience of being treated for a heart attack
Please tick one only Q10: Fully Partly Not at all Not sure
To what extent do you feel your health problem has been sorted out?
SECTION G: Your overall experience
SECTION F: About your treatment

© Queen's Printer and Controller of HMSO 2007 149
Q11. Please answer the following questions about yourself
What is your age? ________________ years
Are you male or female? (please tick one)
Male Female
At the end of the research project (early 2008) we will produce a short summary of the findings of our research. Would you like to be sent a copy of this?
I WOULD like to be sent a summary of results
I WOULD NOT like to be sent a summary of results
The answers to this questionnaire are all anonymous. However, we may be interested in finding out more about the experiences you talk about in this questionnaire. If you would be willing for us to contact you to talk about your experiences further, please tick the box below.
I AM happy to be contacted again
I AM NOT happy to be contacted again
If you would like to be contacted again we would be grateful if you could also fill out your contact details on the attached form. This will be stored separately from this survey.
SECTION H: About you.
SECTION I: Further involvement in this research.

© Queen's Printer and Controller of HMSO 2007 150
Other comments: If there is anything else you would like to tell us about your experiences of being treated for a heart attack, please do so here. If you need any more space for any of your comments, please use the space below the boxes.
a) If you would like to explain any of your answers further, please do so here.
b) Was there anything particularly good about your care?
c) Was there anything that could have been improved?
d) Is there anything else you’d like to add?
THANK YOU VERY MUCH FOR YOUR HELP
SECTION I: Comments.

© Queen's Printer and Controller of HMSO 2007 151
Carer questionnaire
NHSStudy number:
Q1. What treatment did the patient receive for their heart attack? Please tick one
They had an angioplasty (balloon / stent)
They were treated with drugs only
I’m not sure
Other (please give details _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ )
Please tick one only Q2. Thinking about the patient’s treatment and care in (Name) Hospital, how would you rate the following?
Excellent Very Good
Good Fair Poor Not sure
The management of the patient’s pain
The management of the patient’s comfort
Information you were given about what was happening to the patient
Your confidence in the treatment they received
The convenience of the hospital for you to visit the patient
Visiting times
Facilities available to visitors (i.e. accommodation, refreshments)
Your overall impression of their treatment and care in hospital
Please tick one only Q3. Thinking about the staff who treated the patient in this hospital, how would you rate the following? Excellent Very
Good Good Fair Poor Not
sure Professional skill and ability of the doctors and nurses
Your confidence in the doctors and nurses treating the patient
The reassurance and support offered by the doctors and nurses
Opportunity to ask doctors and nurses all the questions you wanted to
SECTION A: About the treatment in (Name) Hospital

© Queen's Printer and Controller of HMSO 2007 152
NIAPP carer questionnaire version 001, date 07/11/20061
Please answer the following questions about yourself: Q4. What is your age? ________________ years Q5. Are you male or female? (please tick one)
Male Female
Q6. Are you the patient’s: (please tick one only) Husband/Wife Neighbour
Daughter/Son Care worker
Other relative Other
Friend If other, please give details:
Q7. Do you live with the patient Yes No
Other comments: If there is anything else you would like to tell us about your experiences when the patient was treated for a heart attack, we would welcome any comments below. Please feel free to continue on another piece of paper if you need more space.
Was there anything particularly good that you would like to comment on?
Was there anything that could have been improved?
Is there anything else you’d like to add?
The answers to this questionnaire are all anonymous. However, we may be interested in finding out more about the experiences you talk about in this questionnaire. If you would be willing for us to contact you to talk about your experiences further, please tick the box below. I AM happy to be contacted again I AM NOT happy to be contacted
again
At the end of the research project (early 2008) we will produce a short summary of the findings of our research. Would you like to be sent a copy of this?
I WOULD like to be sent a copy of the research findings
I WOULD NOT like to be sent a copy of the research findings
THANK YOU VERY MUCH FOR YOUR HELP
SECTION B: About you.
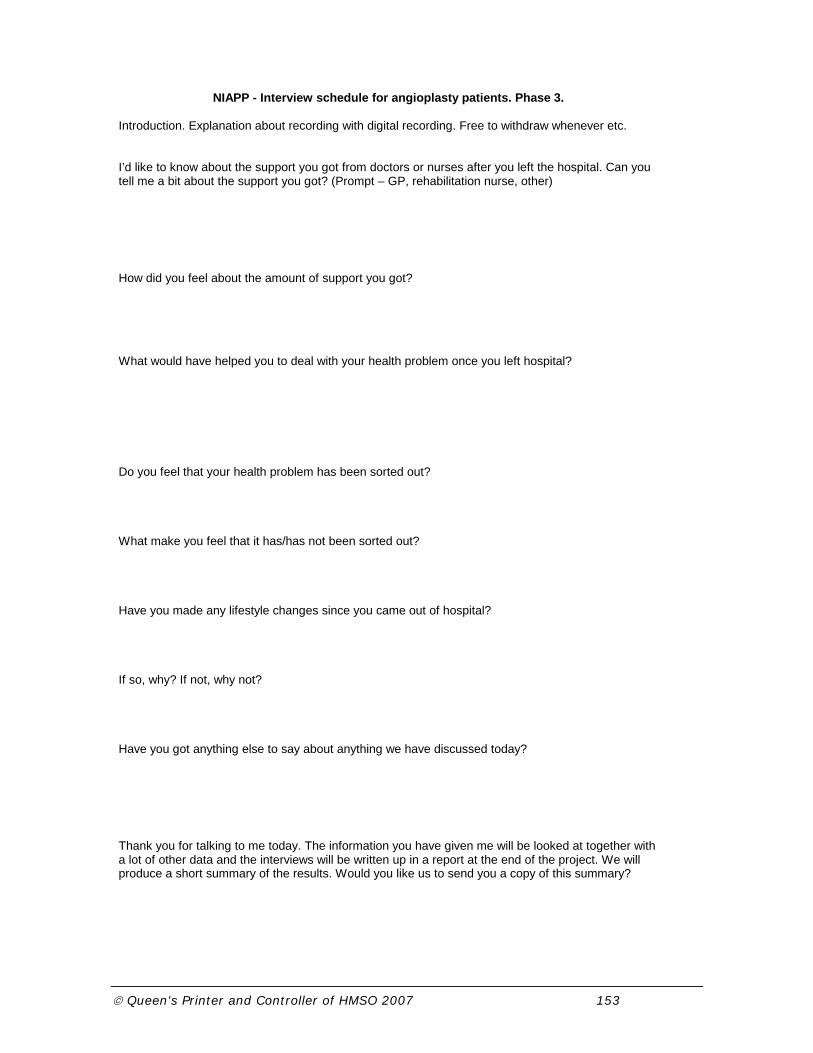
© Queen's Printer and Controller of HMSO 2007 153
NIAPP - Interview schedule for angioplasty patients. Phase 3. Introduction. Explanation about recording with digital recording. Free to withdraw whenever etc. I’d like to know about the support you got from doctors or nurses after you left the hospital. Can you tell me a bit about the support you got? (Prompt – GP, rehabilitation nurse, other) How did you feel about the amount of support you got? What would have helped you to deal with your health problem once you left hospital? Do you feel that your health problem has been sorted out? What make you feel that it has/has not been sorted out? Have you made any lifestyle changes since you came out of hospital? If so, why? If not, why not? Have you got anything else to say about anything we have discussed today? Thank you for talking to me today. The information you have given me will be looked at together with a lot of other data and the interviews will be written up in a report at the end of the project. We will produce a short summary of the results. Would you like us to send you a copy of this summary?

© Queen's Printer and Controller of HMSO 2007 154
Results of patient and carer questionnaire Intervention Control All n % n % Total % p
How would you rate explanations given about what was wrong with you
Excellent 206 56% 109 50% 315 54% 0.105
Very good 108 30% 81 37% 189 32%
Good 32 9% 21 10% 53 9%
Fair 3 12% 8 4% 11 2%
Poor 2 1% 0 0% 2 0%
Not sure 5 1% 1 0% 6 1%
365 220 585
Intervention Control All n % n % Total % p
How would you rate explanations given about the risks and benefits
Excellent 170 47% 96 44% 266 46% 0.604
Very good 119 33% 79 37% 198 34%
Good 40 11% 27 13% 67 12%
Fair 13 4% 7 3% 20 3%
Poor 4 1% 0 0% 4 1%
Not sure 15 4% 7 3% 22 4%
361 216 577
Intervention Control All n % n % Total % p
How would you rate your involvement in decisions
Excellent 133 37% 70 32% 203 35% 0.182
Very good 112 31% 71 33% 183 32%
Good 53 15% 45 21% 98 17%
Fair 18 5% 16 7% 34 6%
Poor 9 3% 2 1% 11 2%
Not sure 32 9% 12 6% 44 8%
357 216 573
Intervention Control All n % n % Total % p
How would you rate time waited before having treatment
Excellent 292 80% 148 67% 440 75% 0.000
Very good 50 14% 49 22% 99 17%
Good 11 3% 15 7% 26 4%
Fair 3 1% 2 1% 5 1%
Poor 1 0% 3 1% 4 1%
Not sure 7 2% 2 1% 9 2%
364 219 583
Intervention Control All n % n % Total % p
How would you rate the efficiency with which you were treated
Excellent 306 83% 162 74% 468 80% 0.009
Very good 47 13% 44 20% 91 15%
Good 15 4% 13 6% 28 5%
Fair 0 0% 0 0% 0 0%
Poor 1 0% 0 0% 1 0%
Not sure 0 0% 0 0% 0 0%
369 219 588
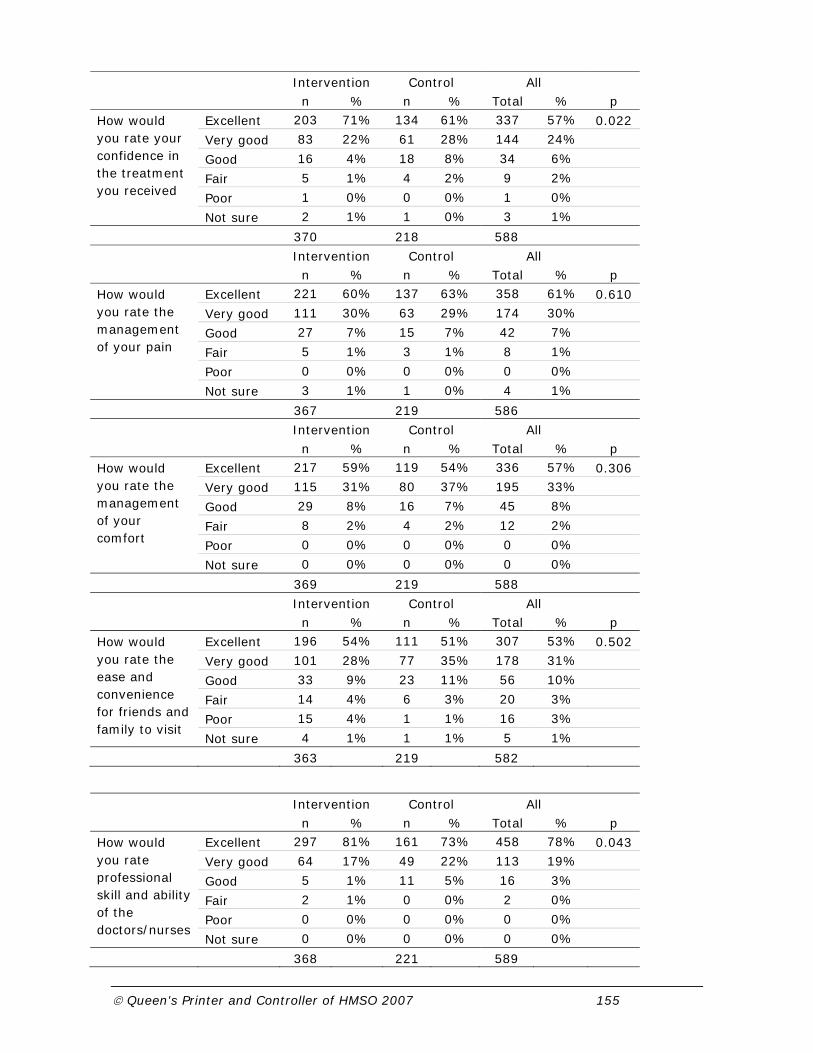
© Queen's Printer and Controller of HMSO 2007 155
Intervention Control All n % n % Total % p
How would you rate your confidence in the treatment you received
Excellent 203 71% 134 61% 337 57% 0.022
Very good 83 22% 61 28% 144 24%
Good 16 4% 18 8% 34 6%
Fair 5 1% 4 2% 9 2%
Poor 1 0% 0 0% 1 0%
Not sure 2 1% 1 0% 3 1%
370 218 588
Intervention Control All n % n % Total % p
How would you rate the management of your pain
Excellent 221 60% 137 63% 358 61% 0.610
Very good 111 30% 63 29% 174 30%
Good 27 7% 15 7% 42 7%
Fair 5 1% 3 1% 8 1%
Poor 0 0% 0 0% 0 0%
Not sure 3 1% 1 0% 4 1%
367 219 586
Intervention Control All n % n % Total % p
How would you rate the management of your comfort
Excellent 217 59% 119 54% 336 57% 0.306
Very good 115 31% 80 37% 195 33%
Good 29 8% 16 7% 45 8%
Fair 8 2% 4 2% 12 2%
Poor 0 0% 0 0% 0 0%
Not sure 0 0% 0 0% 0 0%
369 219 588
Intervention Control All n % n % Total % p
How would you rate the ease and convenience for friends and family to visit
Excellent 196 54% 111 51% 307 53% 0.502
Very good 101 28% 77 35% 178 31%
Good 33 9% 23 11% 56 10%
Fair 14 4% 6 3% 20 3%
Poor 15 4% 1 1% 16 3%
Not sure 4 1% 1 1% 5 1%
363 219 582
Intervention Control All n % n % Total % p
How would you rate professional skill and ability of the doctors/nurses
Excellent 297 81% 161 73% 458 78% 0.043
Very good 64 17% 49 22% 113 19%
Good 5 1% 11 5% 16 3%
Fair 2 1% 0 0% 2 0%
Poor 0 0% 0 0% 0 0%
Not sure 0 0% 0 0% 0 0%
368 221 589

© Queen's Printer and Controller of HMSO 2007 156
Intervention Control All n % n % Total % p
How would you rate your confidence in the doctors and nurses treating you
Excellent 278 75% 151 69% 429 73% 0.108
Very good 77 21% 56 26% 133 23%
Good 13 4% 11 5% 24 4%
Fair 1 0% 1 1% 2 0%
Poor 0 0% 0 0% 0 0%
Not sure 0 0% 0 0% 0 0%
369 219 588
Intervention Control All n % n % Total % p
How would you rate the reassurance and support offered
Excellent 242 66% 148 67% 390 66% 0.572
Very good 98 27% 55 25% 153 26%
Good 23 6% 16 7% 39 7%
Fair 5 1% 1 0% 6 1%
Poor 0 0% 0 0% 0 0%
Not sure 0 0% 0 0% 0 0%
368 220 588
Intervention Control All n % n % Total % p
How would you rate the opportunity to ask doctors and nurses questions
Excellent 203 55% 122 56% 325 55% 0.780
Very good 108 29% 61 28% 169 29%
Good 45 12% 24 11% 69 12%
Fair 8 2% 8 4% 16 3%
Poor 3 1% 2 1% 5 1%
Not sure 2 1% 2 1% 4 1%
369 219 588
Section B: Transfer to another hospital
Intervention Control All n % n % Total % p
How would you rate the opportunity to ask doctors and nurses questions
Excellent 72 42% 47 44% 119 43% 0.796
Very good 53 31% 44 44% 97 35%
Good 32 19% 14 13% 46 16%
Fair 8 5% 2 2% 10 4%
Poor 6 3% 1 1% 7 3%
Not sure 1 1% 0 0% 1 0%
172 108 280
Intervention Control All n % n % Total % p
How would you rate the professional skill and ability of the staff
Excellent 90 54% 65 61% 155 57% 0.179
Very good 53 31% 35 33% 88 32%
Good 19 11% 6 6% 25 9%
Fair 4 2% 0 0% 4 1%
Poor 2 1% 0 0% 2 1%
Not sure 0 0% 0 0% 0 0%
168 106 274

© Queen's Printer and Controller of HMSO 2007 157
Intervention Control All n % n % Total % p
How would you rate communication between staff at diff hospitals
Excellent 61 41% 44 51% 105 44% 0.198
Very good 40 27% 22 25% 62 26%
Good 23 15% 11 13% 34 14%
Fair 6 4% 2 2% 8 3%
Poor 3 2% 1 1% 4 2%
Not sure 17 11% 7 8% 24 10%
150 87 237
Intervention Control All n % n % Total % p
How would you rate the ease and convenience for friends and family to visit
Excellent 76 47% 50 55% 126 50% 0.170
Very good 47 29% 23 25% 70 28%
Good 23 14% 14 15% 37 15%
Fair 8 5% 2 2% 10 4%
Poor 7 4% 1 1% 8 3%
Not sure 1 1% 1 1% 2 1%
162 91 253
Intervention Control All n % n % Total % p
How would you rate your overall stay in the local hospital
Excellent 75 47% 49 56% 124 50% 0.149
Very good 51 32% 25 28% 76 31%
Good 21 13% 12 14% 33 13%
Fair 9 6% 1 1% 10 4%
Poor 4 3% 1 1% 5 2%
Not sure 0 0% 0 0% 0 0%
160 88 248
Section C: Being discharged from hospital
Intervention Control All n % n % Total % p
How would you rate time spent waiting to be discharged
Excellent 115 38% 84 46% 199 41% 0.205
Very good 100 33% 60 33% 160 33%
Good 48 16% 23 13% 71 15%
Fair 25 8% 8 4% 33 7%
Poor 15 5% 3 2% 18 4%
Not sure 3 1% 4 2% 7 1%
306 182 488
Intervention Control All n % n % Total % p
How would you rate information given about how to manage your condition
Excellent 78 25% 55 30% 133 27% 0.049
Very good 98 32% 66 36% 164 33%
Good 69 22% 30 16% 99 20%
Fair 35 11% 16 9% 51 10%
Poor 30 10% 14 8% 44 9%
Not sure 1 0% 1 1% 2 0%
311 182 493

© Queen's Printer and Controller of HMSO 2007 158
Intervention Control All n % n % Total % p
How would you rate info about medications and potential side-effects
Excellent 104 34% 69 38% 173 35% 0.281
Very good 102 33% 59 32% 161 33%
Good 42 14% 24 13% 66 13%
Fair 32 10% 17 9% 49 10%
Poor 24 8% 7 4% 31 6%
Not sure 4 1% 7 4% 11 2%
308 183 491
Intervention Control All n % n % Total % p
How would you rate support and follow up provided once you left hospital
Excellent 108 36% 56 32% 164 35% 0.676
Very good 64 21% 47 27% 111 23%
Good 65 22% 31 18% 96 20%
Fair 25 8% 15 9% 40 8%
Poor 26 9% 10 6% 36 8%
Not sure 12 4% 16 9% 28 6%
300 175 475
Section D: The different places you received care
Intervention Control All n % n % Total % p
How would you rate the ambulance journey
Excellent 216 73% 93 59% 309 68% 0.037
Very good 48 16% 29 18% 77 17%
Good 12 4% 14 9% 26 6%
Fair 8 3% 2 1% 10 2%
Poor 3 1% 3 2% 6 1%
Not sure 8 3% 17 11% 25 6%
295 158 453
Intervention Control All n % n % Total % p
How would you rate the A+E department
Excellent 179 68% 81 58% 260 64% 0.056
Very good 37 14% 25 18% 62 15%
Good 10 4% 7 5% 17 4%
Fair 2 1% 5 4% 7 2%
Poor 4 2% 2 1% 6 1%
Not sure 33 13% 21 15% 54 13%
265 141 406
Intervention Control All n % n % Total % p
How would you rate the coronary care unit
Excellent 238 80% 142 84% 380 81% 0.220
Very good 49 16% 17 10% 66 14%
Good 11 4% 8 5% 19 4%
Fair 0 0% 1 1% 1 0%
Poor 0 0% 0 0% 0 0%
Not sure 0 0% 2 1% 2 0%
298 170 468

© Queen's Printer and Controller of HMSO 2007 159
Intervention Control All n % n % Total % p
How would you rate you overall experience
Excellent 207 68% 105 62% 312 66% 0.207
Very good 76 25% 46 27% 122 26%
Good 18 6% 15 9% 33 7%
Fair 1 0% 2 1% 3 1%
Poor 1 0% 0 0% 1 0%
Not sure 0 0% 2 1% 2 0%
303 170 473
Section G: Your overall experience
Intervention Control All n % n % Total % p
How would you rate your overall experience of being treated for a heart attack?
Excellent 287 78% 155 71% 442 76% 0.074
Very good 63 17% 52 24% 115 20%
Good 13 4% 11 5% 24 4%
Fair 1 0% 0 0% 1 0%
Poor 3 1% 0 0% 3 1%
Not sure 0 0% 0 0% 0 0%
367 218 585
Intervention Control All n % n % Total % p
To what extent do you feel your health sorted
Fully 181 50% 98 45% 279 48% 0.308
Partly 154 42% 101 47% 255 44%
Not at all 9 3% 2 1% 11 2%
Not sure 21 6% 16 7% 37 6%
365 217 582
Results of the carer questionnaire Intervention Control All n % n % Total % p
How would you rate the management of the patients pain
Excellent 151 57% 90 61% 241 59% 0.870
Very good 83 32% 47 32% 130 32%
Good 24 9% 11 7% 35 9%
Fair 1 0% 0 0% 1 0%
Poor 0 0% 0 0% 0 0%
Not sure 4 2% 0 0% 4 1%
263 148 411
Intervention Control All n % n % Total % p
How would you rate the management of the patients comfort
Excellent 142 54% 81 55% 223 54% 0.880
Very good 89 34% 51 34% 140 34%
Good 22 8% 16 11% 38 9%
Fair 6 2% 0 0% 6 1%
Poor 1 0% 0 0% 1 0%
Not sure 2 1% 0 0% 2 0%
262 148 410

© Queen's Printer and Controller of HMSO 2007 160
Intervention Control All n % n % Total % p
How would you rate information you were given about what was happening to patient
Excellent 130 49% 64 43% 194 47% 0.742
Very good 79 30% 45 30% 124 30%
Good 32 12% 18 12% 50 12%
Fair 12 5% 12 8% 24 6%
Poor 9 3% 10 7% 19 5%
Not sure 1 0% 0 0% 1 0%
263 149 412
Intervention Control All n % n % Total % p
How would you rate your confidence in the treatment they received
Excellent 157 59% 79 53% 236 57% 0.171
Very good 84 32% 50 34% 134 33%
Good 22 8% 15 10% 37 9%
Fair 2 1% 2 2% 4 1%
Poor 0 0% 0 0% 0 0%
Not sure 0 0% 1 1% 1 0%
265 147 412
Intervention Control All n % n % Total % p
How would you rate the convenience of the hospital for you to visit the patient
Excellent 72 28% 50 34% 122 30% 0.158
Very good 54 21% 58 40% 112 28%
Good 57 22% 25 17% 82 20%
Fair 44 17% 10 7% 54 13%
Poor 30 11% 2 1% 32 8%
Not sure 4 2% 0 0% 4 1%
261 145 406
Intervention Control All n % n % Total % p
How would you rate visiting times
Excellent 77 30% 46 31% 123 30% 0.881
Very good 85 33% 59 40% 144 35%
Good 64 25% 34 23% 98 24%
Fair 22 8% 7 5% 29 7%
Poor 8 3% 2 1% 10 2%
Not sure 2 2% 0 0% 2 0%
258 148 406
Intervention Control All n % n % Total % p
How would you rate facilities available to visitors
Excellent 71 28% 28 19% 99 25% 0.067
Very good 73 29% 45 31% 118 30%
Good 57 22% 38 26% 95 24%
Fair 29 11% 12 8% 41 10%
Poor 11 4% 8 6% 19 5%
Not sure 13 5% 13 9% 26 7%
254 144 398

© Queen's Printer and Controller of HMSO 2007 161
Intervention Control All n % n % Total % p
How would you rate your overall impression of their treatment
Excellent 167 63% 81 55% 248 60% 0.049
Very good 72 27% 51 35% 123 30%
Good 18 7% 13 9% 31 8%
Fair 6 2% 2 1% 8 2%
Poor 0 0% 0 0% 0 0%
Not sure 0 0% 0 0% 0 0%
263 147 410
Intervention Control All n % n % Total % p
How would you rate professional skill and ability of doctors/nurses
Excellent 198 75% 98 66% 296 71% 0.051
Very good 53 20% 44 30% 97 23%
Good 11 4% 6 4% 17 4%
Fair 1 0% 1 1% 2 0%
Poor 0 0% 0 0% 0 0%
Not sure 2 1% 0 0% 2 0%
265 149 414
Intervention Control All n % n % Total % p
How would you rate your confidence in the doctors / nurses treating the patient
Excellent 181 68% 97 65% 278 67% 0.438
Very good 68 26% 42 28% 110 27%
Good 13 5% 9 6% 22 5%
Fair 1 0% 1 1% 2 0%
Poor 0 0% 0 0% 0 0%
Not sure 2 1% 0 0% 2 0%
265 149 414
Intervention Control All n % n % Total % p
How would you rate the reassurance and support offered
Excellent 158 60% 82 55% 240 59% 0.276
Very good 69 26% 46 31% 115 28%
Good 24 9% 9 9% 33 8%
Fair 8 3% 5 3% 13 3%
Poor 3 1% 1 1% 4 1%
Not sure 3 1% 1 1% 4 1%
265 144 409
Intervention Control All n % n % Total % p
How would you rate opportunity to ask doctors/nurses all the questions
Excellent 135 51% 55 37% 190 46% 0.004
Very good 76 29% 46 31% 122 29%
Good 27 10% 27 18% 54 13%
Fair 16 6% 12 8% 28 7%
Poor 11 4% 6 24% 17 4%
Not sure 1 0% 3 2% 4 1%
266 149 415
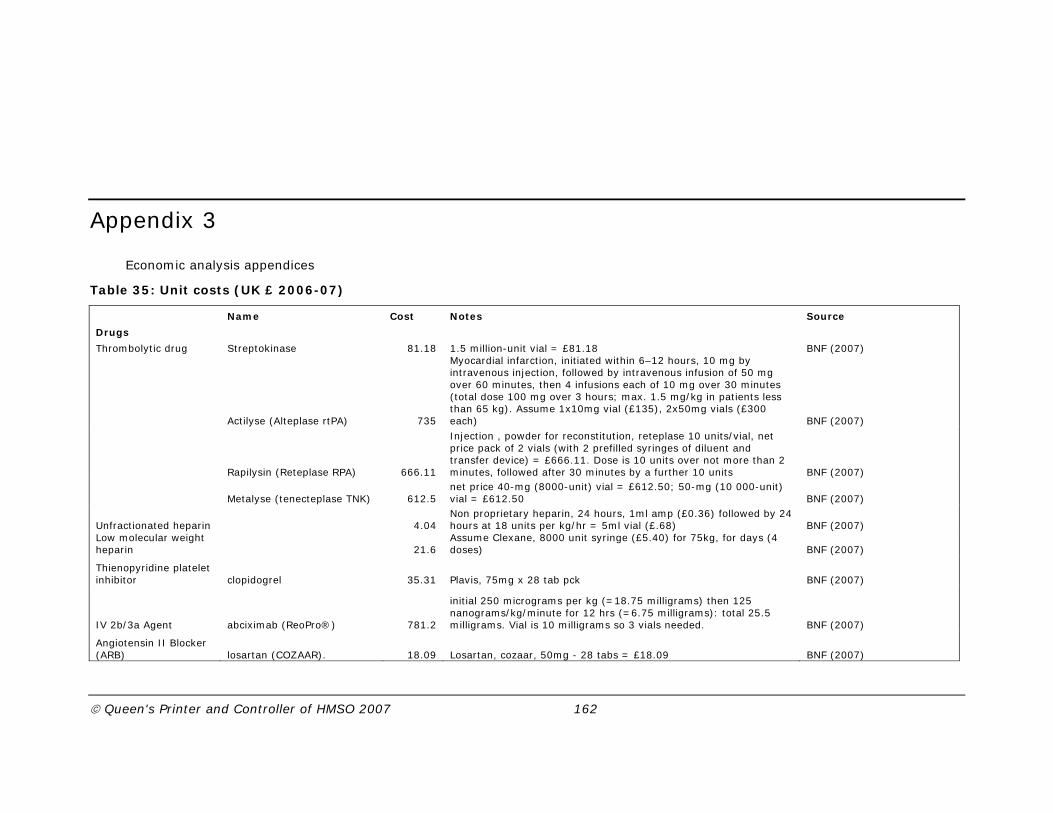
© Queen's Printer and Controller of HMSO 2007 162
Appendix 3
Economic analysis appendices
Table 35: Unit costs (UK £ 2006-07)
Name Cost Notes Source
Drugs
Thrombolytic drug Streptokinase 81.18 1.5 million-unit vial = £81.18 BNF (2007)
Actilyse (Alteplase rtPA) 735
Myocardial infarction, initiated within 6–12 hours, 10 mg by intravenous injection, followed by intravenous infusion of 50 mg over 60 minutes, then 4 infusions each of 10 mg over 30 minutes (total dose 100 mg over 3 hours; max. 1.5 mg/kg in patients less than 65 kg). Assume 1x10mg vial (£135), 2x50mg vials (£300 each) BNF (2007)
Rapilysin (Reteplase RPA) 666.11
Injection , powder for reconstitution, reteplase 10 units/vial, net price pack of 2 vials (with 2 prefilled syringes of diluent and transfer device) = £666.11. Dose is 10 units over not more than 2 minutes, followed after 30 minutes by a further 10 units BNF (2007)
Metalyse (tenecteplase TNK) 612.5 net price 40-mg (8000-unit) vial = £612.50; 50-mg (10 000-unit) vial = £612.50 BNF (2007)
Unfractionated heparin 4.04 Non proprietary heparin, 24 hours, 1ml amp (£0.36) followed by 24 hours at 18 units per kg/hr = 5ml vial (£.68) BNF (2007)
Low molecular weight heparin 21.6
Assume Clexane, 8000 unit syringe (£5.40) for 75kg, for days (4 doses) BNF (2007)
Thienopyridine platelet inhibitor clopidogrel 35.31 Plavis, 75mg x 28 tab pck BNF (2007)
IV 2b/3a Agent abciximab (ReoPro®) 781.2
initial 250 micrograms per kg (=18.75 milligrams) then 125 nanograms/kg/minute for 12 hrs (=6.75 milligrams): total 25.5 milligrams. Vial is 10 milligrams so 3 vials needed. BNF (2007)
Angiotensin II Blocker (ARB) losartan (COZAAR). 18.09 Losartan, cozaar, 50mg - 28 tabs = £18.09 BNF (2007)

© Queen's Printer and Controller of HMSO 2007 163
Bivalirudin Angiox 620
net price 250mg vial =£310, initially by intravenous injection, 750 micrograms/kg then by intravenous infusion 1.75 mg/kg/hour for up to 4 hours after procedure. We assume 2 hours infusion, 75kg weight and vials split between initial injection and subsequent infusion BNF (2007)
Tests
Exercise Test 59 NHS reference costs 2006/7 TDADS DA15
Echocardiography 58 NHS reference costs 2006/7 TDADS DA02
Radionuclide Study 312.09 NHS reference costs 2005/6 TRADIO RBJ1 (£303) inflated by 3% based on price index (Curtis 2007)
Angiography 258.53 NHS reference costs 2005/6 TRADIO RBF2 (£251) inflated by 3% based on price index (Curtis 2007)
CABG 7976 NHS reference costs 2006/7 TEI, EA14Z, Coronary Artery Bypass Graft (First Time)
PCI 2534 NHS reference costs 2006/7 TEI, EA32Z, Percutaneous Coronary Intervention (0-2 stents) and Catheterisation
Hospital stay
Day on ITU 990 NHS reference costs 2006/7,'XC06ZTHE, 'Intensive Therapy Unit / Intensive Care Unit:1 Organs Supported, TCCSAL
Day on CCU 450 NHS reference costs 2006/7, CC7, Coronary Care Unit, TCORCU
Day on HDU 657 NHS reference costs 2006/7, 'XC06ZHDU, 'High Dependancy Unit:1 Organs Supported, TCCSAL
Day on Acute Ward 223 NHS reference costs 2006/7 in Curtis (2007)
Day on dialysis 381
NHS reference costs 2006/7, 'LC02A, 'Haemodialysis/Filtration 19 years and over, TRENAL (NOTE: we assume this cost is added to a stay on a general ward)
Ambulance journeys
Paramedic emergency transfer 247 NHS reference costs 2006/7 TUPAR(EM), Emergency Transfers/Urgents, PSETU
Staff costs per minute

© Queen's Printer and Controller of HMSO 2007 164
Cardiologist in hours 2.53 Curtis 2007, per minute, patient related excluding qualifications, medical consultant
out of hours 2.53
Nurse in hours 0.35
Curtis 2007, assumes nurse, 24 hour ward, mid point grade 5 agenda for change, excluding qualifications, per minute, upgraded by 4.5%
out of hours 0.52
Technician in hours 0.42 Assume the same as radiographer
out of hours 0.63
Radiographer in hours 0.42 Curtis 2007, assumes mid point grade 5 agenda for change, excluding qualifications, per minute 2006/7, upgraded by 4.5%
out of hours 0.63
Cath lab operating costs per minute 9.08 average from NIAPP sites
PPCI consumables
Drug eluting stents 634.74 average from NIAPP sites Non drug eluting stents 216.00 average from NIAPP sites
Diagnostic devices 659.58 average from NIAPP sites
Procedural devices 628.59 average from NIAPP sites
Athero-thrombus removal devices 401.09 average from NIAPP sites
Emboli protection device(s) used (PCI) 523.11 average from NIAPP sites Circulatory support (PCI) 585.21 average from NIAPP sites
Pacing wire used (PCI) 92.74 average from NIAPP sites
Arterial management (PCI) 55.61 average from NIAPP sites
Sheath 10.65 average from NIAPP sites
Guide catheter 21.88 average from NIAPP sites
J wire 2.25 average from NIAPP sites
Guide wires 49.50 average from NIAPP sites
Over the wire balloon 73.75 average from NIAPP sites

© Queen's Printer and Controller of HMSO 2007 165
Table 36: Patient characteristics
NIAPP Sites Control Sites PPCI Lysis None All PPCI Lysis None All n % n % n % n % n % n % n % n % Total 1398 67.1 330 15.8 355 17.0 2083 100.0 39 4.3 667 72.6 213 23.2 919 100 Mean age in years (se) 62.3 0.4 65 0.8 66.9*** 0.87 63.5*** 0.31 59.7 1.65 64.5 0.5 72.2*** 0.92 66.1*** 0.44 Ethnic group caucasian 911 78.7 267 87.5 229 80.1 1407 80.5*** 4 100.0 497 98.4 123 96.1 624 98.0*** black 29 2.5 4 1.3 17 5.9 50 2.9 0 0.0 0 0.0 2 1.6 2 0.3 asian 151 13.1 18 5.9 23 8 192 11.0 0 0.0 8 1.6 2 1.6 10 1.6 oriental 5 0.4 1 0.3 3 1.1 9 0.5 0 0.0 0 0.0 1 0.8 1 0.2 Previous CHD AMI 194 14.1 60 18.2* 72 21 326 15.9 3 7.9 92 13.9* 41 19.8 136 15 Angina 264 19.4 78 24.5*** 99 29 441 21.8*** 1 0.8 59 14.8*** 16 21.1 76 15.9*** Previous PCI 119 8.6 24 7.4*** 33 9.5*** 176 8.6*** 1 2.6 15 2.3*** 7 3.7*** 23 2.6*** Previous CABG 45 3.2 13 4.0** 20 5.8 78 3.8*** 0 0.0 7 1.3** 3 1.7 10 1.3*** Comorbidities Hypertension 618 45.1 148 46.8*** 165 48.4 931 45.9*** 13 41.9 234 37.4*** 80 45.5 327 39.3*** Hypercholesterolaemia 569 42.7 107 35.2** 113 35.1 789 40.3 15 50.0 260 43.1** 68 42.8 343 43.3 peripheral vascular disease 54 4.0 10 3.3* 23 6.7 87 4.3*** 0 0.0 6 1.2* 6 5.6 12 2.0*** Cerebrovascular disease 74 5.4 18 5.8 37 10.9 129 6.4 3 8.6 24 3.73 17 8.9 44 5.1 Asthma or COPD 154 11.2 42 13.5 42 12.3 238 11.8 1 3.2 71 11.2 25 13.5 97 11.4 Chronic renal failure 29 2.1 7 2.2 14 4.1 50 2.5 0 0.0 10 1.52 9 4.4 19 2.1 Diabetes 230 16.7 50 15.7** 59 17.0 339 16.6*** 3 7.7 67 10.2** 31 15.0 101 11.17*** MI severity Mean peak troponin (se) 42.9 5.8 17.4 2.0 7.1*** 1.1 32.3*** 3.8 43.4 2.1 20.6 0.9 13.7*** 1.2 19.9*** 0.71 LVEF Good 367 54.4 91 58.0 89 58.9 547 55.7 3 75.0 123 60.59 25 48.1 151 58.3 Moderate 241 35.7 46 29.3 40 26.5 327 33.3 1 25.0 66 32.51 22 42.3 89 34.36 Poor 67 9.9 20 12.7 22 14.6 109 11.1 0 0.0 14 6.9 5 9.6 19 7.34 Note: P values only reported where there are more than 5 observations in a cell ***p<0.01, **p<0.05, * p<0.1.We tested NIAPP PPCI vs control PPCI, NIAPP lysis vs Control lysis, NIAPP none vs Control none and NIAPP all vs. Control all.

© Queen's Printer and Controller of HMSO 2007 166
Table 37: Probabilities of short-term endpoints, means and 95%-CI – Base case
Dead (1 month) Dead (6 months) MI (6 months) Stroke (6 months) Thrombolysis 0.0759
[0.0743, 0.0776] 0.0895
[0.0757, 0.131] 0.0762
[0.0662, 0.107] 0.0267
[0.0112, 0.0672] Control PPCI 0.0510
[0.0338, 0.0725] 0.0619
[0.0385, 0.101] 0.0276
[0.0156, 0.0495] 0.0069
[0.0022, 0.0178] NIAPP PCI 0.0592
[0.0381, 0.0870] 0.0719
[0.0432, 0.121] 0.0294
[0.0155, 0.0555] 0.00727
[0.0023, 0.0187]
Table 38: Costs breakdown for the combinations centre/intervention, £ disc – Base case
Mean SE 95%-CI
Control Thrombolysis 10,700 2120 [7960, 16,000] - Initial Intervention 2980 95 [2800, 3170] - Revascularisations 1300 180 [978, 1690] - Long-Term Model 6410 2110 [3740, 11,700]
Control PPCI 11,600 2260 [8790, 17,400] - Initial Intervention 4900 54 [4790, 5010] - Revascularisations 581 111 [394, 825] - Long-Term Model 6130 2250 [3310, 11,900]
NIAPP Thrombolysis 11,700 2120 [8910, 16,900] - Initial Intervention 3940 157 [3640, 4260] - Revascularisations 1300 180 [978, 1690] - Long-Term Model 6410 2110 [3740, 11,700]
NIAPP PPCI 11,600 2230 [8760, 17,300] - Initial Intervention 4900 54 [4760, 5010] - Revascularisations 581 111 [394, 825] - Long-Term Model 6080 2230 [3290, 11,800]

© Queen's Printer and Controller of HMSO 2007 167
Table 39: QALY and LY by centre/intervention (discounted) – Base case
Mean SE 95%-CI
QALYs Control Thrombolysis 6.38 0.294 [5.80, 6.94] Control PPCI 6.71 0.288 [6.14, 7.27] NIAPP Thrombolysis 6.38 0.294 [5.80, 6.94] NIAPP PPCI 6.63 0.298 [6.05, 7.21]
Life-Years Control Thrombolysis 12.5 0.646 [11.3, 13.8] Control PPCI 13.2 0.628 [11.9, 14.4] NIAPP Thrombolysis 12.5 0.646 [11.3, 13.8] NIAPP PPCI 13.0 0.645 [11.7, 14.3]