Embed Size (px)
Citation preview

manifestations are rare in patients with bone sarcoidosis. Toour knowledge, intermittent arthritis similar to that in ourpatient has not been reported previously. Intermittent arthri-tis manifests as recurrent bouts of oligo- or monoarticularinflammation that subside spontaneously within a few days,leaving no residual clinical radiological abnormalities. Thecombination in our patient of multiorgan sarcoidosis withbone lesions and intermittent arthritis of the hand joints ishighly unusual.
References
[1] Pettersson T. Rheumatic features of sarcoidosis. Curr Opin Rheumatol1997;9:62–7.
[2] Naveau B. Manifestations articulaires de la sarcoïdose. Ann MedInterne (Paris) 1984;135:105–8.
[3] Pettersson T. Sarcoid and erythema nodosum arthropathies. BaillieresBest Pract Res Clin Rheumatol 2000;14:461–76.
[4] Eschard JP, Etienne JC. Les manifestations ostéoarticulaires de lasarcoïdose. Rev Med Interne 1994;15:305S–307s.
[5] James G, Neville E, Carstairs LS. Bone and joint sarcoidosis. SeminArthritis Rheum 1976;6:53–81.
[6] Rohatgi PK. Osseous sarcoidosis. Semin Respir Med 1992;13:468–88.
Fatiha BzamiRachid Bahiri *
Karima BenbouazzaHanan Rkain
Najia Hajjaj-HassouniRhumatology B Department, El Ayachi Hospital,
Rabat-Salé Teaching Hospital, Rabat-Salé, MoroccoE-mail address: [email protected] (R. Bahiri).
Received 27 July 2004; accepted 12 December 2004
Availaible online 03 May 2005
* Corresponding author. Tel.: +212 6 107 6535;fax: +212 3 778 5861.
1297-319X/$ - see front matter © 2005 Published by Elsevier SAS.doi:10.1016/j.jbspin.2004.12.008
Evaluation of the fracture threshold by quantitativeultrasound densitometry in everyday practice
Keywords: Densitometry; Ultrasound; Osteoporosis; Fracture threshold
1. Introduction
Bone density measurement is a noninvasive method formeasuring bone mineral content in patients with conditionsthat affect bone tissue, such as osteoporosis. The results canbe used to evaluate the fracture risk in the individual patient.The gold-standard method is dual-energy X-ray densito-metry (DEXA) [1]. Overall, the fracture risk doubles for eachdecrease by 1 standard deviation in bone mineral density(BMD). The role for ultrasound measurements in evaluatingthe fracture risk remains unclear [1]. Several ultrasoundmachines are available, they test different sites, and themethods used to express results vary across machines. As aresult, comparisons and extrapolations are of limited value.The objective of the present study was to define a fracturethreshold determined by ultrasound densitometry in a cohortof postmenopausal patients.
2. Patients and methods
We studied consecutive postmenopausal women referredto us for BMD evaluation. We excluded patients who used
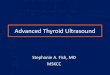
Fig. 2. Computed tomography scan of the chest: images consistent with residual densities, bilateral lung fibrosis, and paracicatricial emphysema.
339Letters to the editor / Joint Bone Spine 72 (2005) 338–344

medications known to affect bone metabolism and those whohad a history of bone disease. For each patient, we recordedage, body mass index, and previous osteoporotic fractures.DEXA was performed (DPX-IQ, Lunar) at the lumbar spineand proximal femur. Ultrasonography (Achilles+, Lunar) ofthe calcaneus was used to determine bone ultrasound attenua-tion (BUA), speed of sound (SOS), and stiffness. Means werecompared using Student’s t-test.A multivariate logistic regres-sion model was built to look for independent associations,and a correlation test was used to investigate correlations. Pvalues smaller than 0.05 were considered statistically signi-ficant. The fracture threshold was determined based on thepresence of prevalent radiographic fractures, and sensitivityand specificity were computed for various ultrasound T-scorevalues.
3. Results
We included 300 women with a mean age of60.5 ± 7 years and a mean age at menopause of49.6 ± 4.9 years. Osteoporotic fractures were noted in 50(16.7%) women, each of whom had one fracture; the sitesinvolved were the wrist (32/50), spine (12/50), and femoralneck (6/50). The patients with fractures were significantlyolder than the other patients (63.8 years vs. 59.9 years;P = 0.0002). The coefficients of variation of the machineswere determined by having the same operator perform fivemeasurements on the same day in 14 healthy individuals; withthe DEXA phantom, the coefficient of variation was 1.8%and with the Achilles+ machine the coefficients of variationwere 3.64% for BUA, 0.59% for SOS, and 1.9% for stiffness.
T-scores in the overall population were −1.24 ± 1.41(DEXA, lumbar spine), −1 ± 1.03 (DEXA, femur), and−1.47 ± 1.49 (stiffness). Significant correlations were foundamong measurement sites and between DEXA and ultra-sound (P < 0.001). Significant differences were found for allcomparisons of patients with and without fractures (Table 1),even after adjustment for age. Sensitivity and specificity ofstiffness for discriminating patients with and without fractu-res were plotted (Fig. 1); the best compromise for the frac-ture threshold value, identified as the intersection between
the two curves, was a T-score of −2.07, which was 68% sen-sitive and 68% specific. According to ISCD recommenda-tions (detection of 90% of patients with osteoporosis, sensi-tivity 90%) [2], the stiffness T-score was –0.75.
4. Discussion
Our results obtained during everyday practice are compa-rable to findings from prospective and cohort studies that useda variety of ultrasound machines. Taken together, these datashow that ultrasound can discriminate between patients withand without fractures and that thresholds are comparableacross studies [3–14].
5. Conclusions
The results of this observational study confirm the useful-ness of ultrasound calcaneus density measurement in post-menopausal women managed in everyday clinical practice.
References
[1] Kanis JA, Gluer CC, for the Committee of scientific advisors, IOF. Anupdate on the diagnosis and assessment of osteoporosis with densito-metry. Osteoporos Int 2000;11:192–202.
[2] Miller PD, Njeh CF, Jankowski LG, Lenchik L. What are the stan-dards by which bone mass measurement at peripheral skeletal sitesshould be used in the diagnosis of osteoporosis? J Clin Densitom2002;5:S39–45.
Table 1Dual-energy X-ray densitometry and ultrasound results in 50 postmenopausal women with fractures and 250 postmenopausal controls. For all these values, thecomparison of the two groups yielded P values smaller than 0.0001 (Student’s t-test)
Patients with fractures (n = 50) Controls without fractures (n = 250)Age 63.8 59.9BMD, spine (standard deviation) 0.935 (0.162) 1.037 (0.168)T-score (standard deviation) −2.02 (1.34) −1.09 (1.38)BMD, femoral neck (standard deviation) 0.794 (0.1) 0.869 (0.134)T-score (standard deviation) –1.59 (0.767) –0.89 (1.04)BUA (standard deviation) 101.9 (10.7) 111.1 (12.9)SOS (standard deviation) 1502.8 (25.3) 1525.6 (32.8)Stiffness (standard deviation) 68.7 (13.2) 81.3 (16.2)T-score for stiffness (standard deviation) −2.42 (1.20) −1.28 (1.48)
BMD, bone mineral density; BUA, broadband ultrasound attenuation; SOS, speed of sound.
Fig. 1. Sensitivity and specificity of the stiffness T-score in discriminatingbetween patients with and without fractures.
340 Letters to the editor / Joint Bone Spine 72 (2005) 338–344

[3] Hans D, Dargent-Molina P, Schott AM, Sebert JL, Cormier C,Kotzki PO, et al. Ultrasonographic heel measurements to predict hipfracture in elderly women: the EPIDOS prospective study. Lancet1996;348:511–4.
[4] Bauer DC, Gluer CC, Cauley JA, Vogt TM, Ensrud KE, Genant HK,et al. Broadband ultrasound attenuation predicts fractures stronglyand independently of densitometry in older women. A prospectivestudy. Arch Intern Med 1997;157:629–34.
[5] Huang C, Ross PD, Yates AJ, Walker RE, Imose K, Emi K, et al.Prediction of fracture risk by radiographic absorptiometry and quan-titative ultrasound: a prospective study. Calcif Tissue Int 1998;63:380–4.
[6] Pluijm SM, Graafmans WC, Bouter LM, Lips P. Ultrasound measure-ments for the prediction of osteoporotic fractures in elderly people.Osteoporos Int 1999;9:550–6.
[7] Khaw KT, Reeve J, Luben R, Bingham S, Welch A, Wareham N, et al.Prediction of total and hip fracture risk in men and women by quanti-tative ultrasound of the calcaneus: EPIC-Norfolk prospective popula-tion study. Lancet 2004;363:197–202.
[8] Huopio J, Kröger H, Honkanen R, Jurvelin J, Saarikoski S, Alhava E.Calcaneal ultrasound predicts early postmenopausal fractures as wellas axial BMD. A prospective study of 422 women. Osteoporos Int2004;15:190–5.
[9] Krieg MA, Cornuz J, Ruffieux C, Sandini L, Buche D, Dam-bacher MA, et al. Comparison of three bone ultrasounds for thediscrimination of subjects with and without osteoporotic fracturesamong 7562 elderly women. J Bone Miner Res 2003;18:1261–6.
[10] Gluer C, Eastell R, Reid DM, Felsenberg D, Roux C, Barkmann R,et al. Association of five quantitative ultrasound devices and bonedensitometry with osteoporotic vertebral fractures in a population-based sample: the OPUS study. J Bone Miner Res 2004;19:782–93.
[11] Lopez-Rodriguez F, Mezquita-Raya P, Dios Luna J, Escobar-Jime-nez F, Munoz-Torres M. Performance of quantitative ultrasound in thediscrimination of prevalent osteoporotic fractures in a bone metabolicunit. Bone 2003;32:571–8.
[12] Burke PK. Use of heel ultrasound to screen for osteoporosis: compari-son with spine and femur DXA. J Bone Miner Res 2003;18:S207.
[13] Hosszu E, Meszaros S, Ferencz V, Horvath C. Performance evaluationof the Achilles insight: precision, accuracy, and comparison to centralDXA. J Bone Miner Res 2003;18:S208.
[14] Falgarone G, Porcher R, Duché A, Kolta S, Dougados M, Roux C.Discrimination of osteoporotic patients with quantitative ultrasoundusing imaging for non-imaging device. Joint Bone Spine 2004;71:419–23.
Daniel Wendling *Didier Moser
Jean-Pierre CedozEric Toussirot
Anne LohseFabrice Michel
Rheumatology Department, Jean Minjoz TeachingHospital, 25030 Besançon cedex, France
E-mail address: [email protected](D. Wendling).
Received 1 July 2004; accepted 15 December 2004
Available online 31 March 2005
* Auteur correspondant. Service de Rhumatologie, CHU deJean Minjoz, 25030 Besançon cedex, France. Tel.: +33 3 8166 82 41; fax: +33 3 81 66 86 86.
1297-319X/$ - see front matter © 2005 Elsevier SAS. All rights reserved.doi:10.1016/j.jbspin.2004.12.001
Scleroderma complicated with tamponade duringpregnancy
Keywords: Scleroderma; Pericarditis; Tamponade; Pregnancy; Gravidichypertension
1. Introduction
Pericardial involvement in systemic sclerosis is usuallysilent and benign and is clinically manifest in 5–10%. Tam-ponade is exceptional [1–3]. We describe a case with limitedcutaneous systemic sclerosis (LSSc) and chronic pericardialeffusion complicated by tamponade at the 34th week of pre-gnancy.
2. Case report
A 33 year-old-woman developed 5 years ago, Raynaud’sphenomenon, thickened skin affecting hands, telangiectasiaand impaired oesophageal motility. She was diagnosed asLSSc and treated with colchicine. One year later, she presen-ted a moderate pericardial effusion without compression signs.There was no biological sign of inflammation and renal func-tion was normal. Immunology tests were negative. There wasno serological evidence of bacterial or viral infection. Thediagnosis was pericarditis related to LSSc. She was treatedwith captopril for 3.5 years until she desired to become pre-gnant. At the 16th week of pregnancy, she was admitted withthe diagnosis of toxaemia of pregnancy. Her blood pressurewas 220/100 mmHg, renal function was normal. She was trea-ted with Aldomet. At the 34th week of gestation, she com-plained of orthopnea, her blood pressure was 110/60 mmHg.An echocardiogram showed a large pericardial effusion essen-tially posterior (Fig. 1). The renal function was normal.Because of the posterior localisation and the absence of foe-tal maturity, the therapeutic decision was to wait in the inten-sive care unit. At the 36th week of pregnancy, she underwentelective caesarean section, a pericardiocentesis yielded 500 ccaseptic fluid. She was treated with colchicine and captopril.Three months later, her blood pressure and renal function werenormal, an echocardiography showed a moderate pericardialeffusion.
3. Discussion
Tamponade in LSSc is exceptional [1]. In our patient,toxaemia and tamponade occurred without renal failure, which
341Letters to the editor / Joint Bone Spine 72 (2004) 338–344









![Computerized Densitometry and Color Coding of … · Computerized Densitometry and Color Coding of ['"C] Deoxyglucose Autoradiographs Charles Goochee, BS, Wayne Rasband, MS, and Louis](https://img.pdfslide.us/doc/110x75/5b2b5e317f8b9af73e8b745b/computerized-densitometry-and-color-coding-of-computerized-densitometry-and.jpg)
















