Embed Size (px)
Citation preview

Gynecologic Oncology 126 (2012) 217–219
Contents lists available at SciVerse ScienceDirect
Gynecologic Oncology
j ourna l homepage: www.e lsev ie r .com/ locate /ygyno
Evaluation of Society of Gynecologic Oncologists (SGO) ovarian cancer qualitysurgical measures
Radhika P. Gogoi a,⁎, Renata Urban b, Haiyan Sun c, Barbara Goff b
a Division of Gynecologic Oncology, Geisinger Medical Center, 100 North Academy Ave. Danville, PA 17822, USAb Division of Gynecologic Oncology, University of Washington Medical Center, 1959 NE Pacific St. Seattle, WA 98195-6460, USAc Center for Health Research. Geisinger Health System, 100 North Academy Ave. Danville, PA 17822, USA
⁎ Corresponding author at: 100 N. Academy Avenue,E-mail addresses: [email protected] (R.P. Gogoi
(R. Urban), [email protected] (H. Sun), [email protected]
0090-8258/$ – see front matter © 2012 Elsevier Inc. Alldoi:10.1016/j.ygyno.2012.04.049
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 28 February 2012Accepted 30 April 2012Available online 3 May 2012Keywords:Ovarian cancerQuality
Objectives. The Society of Gynecologic Oncologists has developed two measures to assess and improve thesurgical care of patients with ovarian cancer (1) description of residual disease following cytoreduction and(2) adequacy of surgical staging. Our aim was to establish baseline surgeon compliance with these twomeasures.
Methods. A retrospective review of patients with ovarian, fallopian tube or peritoneal cancer undergoingsurgery between 7/1/2006 and 7/1/2011 for the purposes of staging and/or cytoreduction was performed atthe University of Washington and Geisinger Medical Center. Operative and pathology reports were reviewed
to obtain information pertaining to stage, histology, residual disease after surgery and the extent of surgicalstaging.Results. 537 cases were identified; 91% with ovarian cancer. 61% of patients had at least stage IIIC disease;15% had recurrent disease and 16% had neoadjuvant therapy. For patients with stages I–IIIB disease, 74% hadfull surgical staging, 10% did not have full surgical staging but documented the reason for this in the operativereport; 15% did not have full surgical staging, no reason was noted. 25% of all operative reports lackeddocumentation of residual disease with 40% documenting no gross residual disease, 18% with residual diseaseb1 cm and 18% had suboptimal debulking with >1 cm disease remaining. There was a statistically significantincrease in appropriate documentation of amount of residual disease over time (pb0.001).
Conclusions. Our study sets benchmarks for evaluation of documentation in gynecologic oncology centers.Improved documentation and staging will allow for equivalent standards of care across institutions.
© 2012 Elsevier Inc. All rights reserved.
Introduction
All aspects of medical practice are increasingly being held toquality standards, not only to insure a high quality of the care beingdelivered, but also to establish a standard for all health care providers.In the surgical field, national standards have been created to promotequality care both prior to and following surgery. The AmericanCollege of Surgeons National Quality Improvement program (NSQIP)is one such initiative within the American College of Surgeons. Hallet al. evaluated hospital risk-adjusted mortality and risk adjustedcomplication rates of 14 academic institutions enrolled in the NSQIPprogram. The data suggests that “NSQIP hospitals appear to beavoiding substantial numbers of complications—improving care andreducing costs.” [1]
Increasing attention has also been paid to quality indicators of theactual surgical procedure within various specialties. In ovarian cancer,the standard of surgery followed by adjuvant chemotherapy as the
Danville, PA 17822, USA.), [email protected] (B. Goff).
rights reserved.
mainstay of treatment has become more complex with the morefrequent incorporation of neoadjuvant chemotherapy, minimallyinvasive surgery and biologic agents. However surgery continues toplay a prominent role in the therapeutic strategy of treating ovariancancer, as either primary cytoreduction or an interval surgicaldebulking [2]. Various factors have been found to be associated withoutcome in surgery for ovarian cancer, such as surgery by agynecologic oncologist and incidence of advanced cancer cases at atertiary surgical center [3,4].
The EORTC-GCG recently published the results of a literaturesearch to identify quality indicators for ovarian cancer surgery [5].For grossly early stage disease, this included the performance of asystemic pelvic and para aortic lymphadenectomy in the presenceof medium or high-risk features; for patients with advanced cancer,this included the documentation of the size and location of residualdisease and the performance of a staging surgery. In a separateforum [6], that included a literature review in addition to amultidisciplinary panel utilizing the Delphi method, additional factorsincluded the proportion of patients with advanced disease under-going debulking to residual disease of 1 cm and the proportion ofpatients with early stage disease who underwent complete surgical
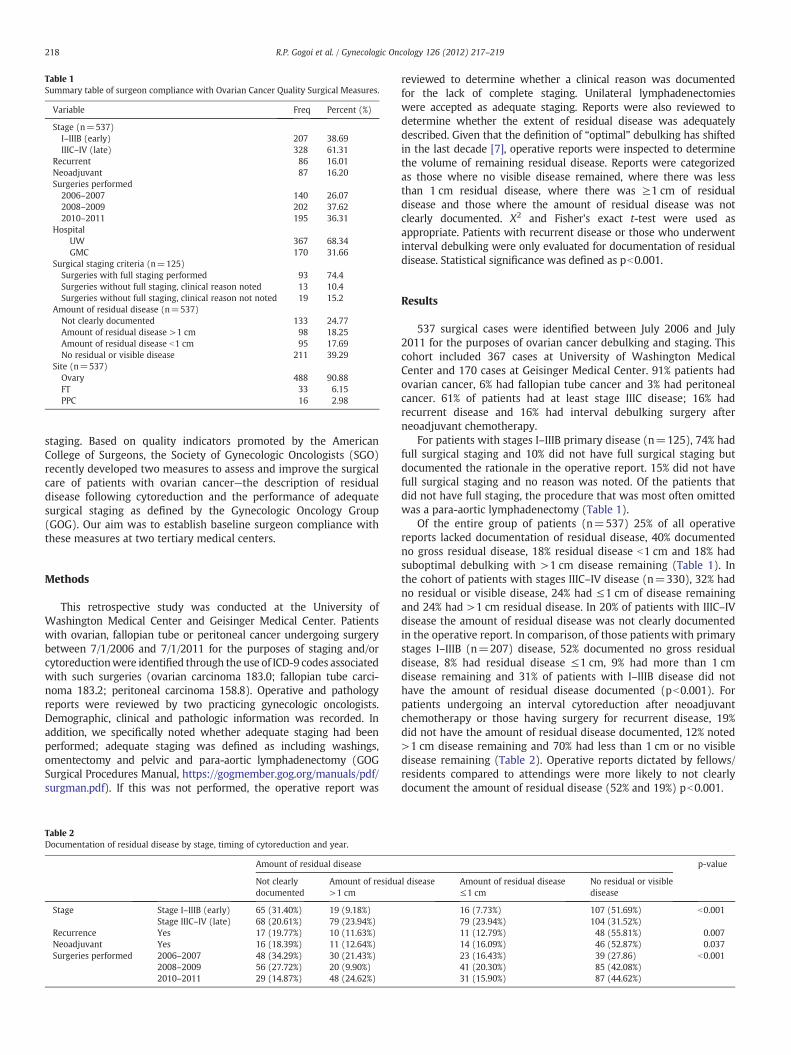
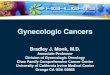
Table 1Summary table of surgeon compliance with Ovarian Cancer Quality Surgical Measures.
Variable Freq Percent (%)
Stage (n=537)I–IIIB (early) 207 38.69IIIC–IV (late) 328 61.31
Recurrent 86 16.01Neoadjuvant 87 16.20Surgeries performed
2006–2007 140 26.072008–2009 202 37.622010–2011 195 36.31
HospitalUW 367 68.34GMC 170 31.66
Surgical staging criteria (n=125)Surgeries with full staging performed 93 74.4Surgeries without full staging, clinical reason noted 13 10.4Surgeries without full staging, clinical reason not noted 19 15.2
Amount of residual disease (n=537)Not clearly documented 133 24.77Amount of residual disease >1 cm 98 18.25Amount of residual disease b1 cm 95 17.69No residual or visible disease 211 39.29
Site (n=537)Ovary 488 90.88FT 33 6.15PPC 16 2.98
218 R.P. Gogoi et al. / Gynecologic Oncology 126 (2012) 217–219
staging. Based on quality indicators promoted by the AmericanCollege of Surgeons, the Society of Gynecologic Oncologists (SGO)recently developed two measures to assess and improve the surgicalcare of patients with ovarian cancer—the description of residualdisease following cytoreduction and the performance of adequatesurgical staging as defined by the Gynecologic Oncology Group(GOG). Our aim was to establish baseline surgeon compliance withthese measures at two tertiary medical centers.
Methods
This retrospective study was conducted at the University ofWashington Medical Center and Geisinger Medical Center. Patientswith ovarian, fallopian tube or peritoneal cancer undergoing surgerybetween 7/1/2006 and 7/1/2011 for the purposes of staging and/orcytoreductionwere identified through the use of ICD-9 codes associatedwith such surgeries (ovarian carcinoma 183.0; fallopian tube carci-noma 183.2; peritoneal carcinoma 158.8). Operative and pathologyreports were reviewed by two practicing gynecologic oncologists.Demographic, clinical and pathologic information was recorded. Inaddition, we specifically noted whether adequate staging had beenperformed; adequate staging was defined as including washings,omentectomy and pelvic and para-aortic lymphadenectomy (GOGSurgical Procedures Manual, https://gogmember.gog.org/manuals/pdf/surgman.pdf). If this was not performed, the operative report was
Table 2Documentation of residual disease by stage, timing of cytoreduction and year.
Amount of residual disease
Not clearlydocumented
Amount of residua>1 cm
Stage Stage I–IIIB (early) 65 (31.40%) 19 (9.18%)Stage IIIC–IV (late) 68 (20.61%) 79 (23.94%)
Recurrence Yes 17 (19.77%) 10 (11.63%)Neoadjuvant Yes 16 (18.39%) 11 (12.64%)Surgeries performed 2006–2007 48 (34.29%) 30 (21.43%)
2008–2009 56 (27.72%) 20 (9.90%)2010–2011 29 (14.87%) 48 (24.62%)
reviewed to determine whether a clinical reason was documentedfor the lack of complete staging. Unilateral lymphadenectomieswere accepted as adequate staging. Reports were also reviewed todetermine whether the extent of residual disease was adequatelydescribed. Given that the definition of “optimal” debulking has shiftedin the last decade [7], operative reports were inspected to determinethe volume of remaining residual disease. Reports were categorizedas those where no visible disease remained, where there was lessthan 1 cm residual disease, where there was ≥1 cm of residualdisease and those where the amount of residual disease was notclearly documented. Χ2 and Fisher's exact t-test were used asappropriate. Patients with recurrent disease or those who underwentinterval debulking were only evaluated for documentation of residualdisease. Statistical significance was defined as pb0.001.
Results
537 surgical cases were identified between July 2006 and July2011 for the purposes of ovarian cancer debulking and staging. Thiscohort included 367 cases at University of Washington MedicalCenter and 170 cases at Geisinger Medical Center. 91% patients hadovarian cancer, 6% had fallopian tube cancer and 3% had peritonealcancer. 61% of patients had at least stage IIIC disease; 16% hadrecurrent disease and 16% had interval debulking surgery afterneoadjuvant chemotherapy.
For patients with stages I–IIIB primary disease (n=125), 74% hadfull surgical staging and 10% did not have full surgical staging butdocumented the rationale in the operative report. 15% did not havefull surgical staging and no reason was noted. Of the patients thatdid not have full staging, the procedure that was most often omittedwas a para-aortic lymphadenectomy (Table 1).
Of the entire group of patients (n=537) 25% of all operativereports lacked documentation of residual disease, 40% documentedno gross residual disease, 18% residual disease b1 cm and 18% hadsuboptimal debulking with >1 cm disease remaining (Table 1). Inthe cohort of patients with stages IIIC–IV disease (n=330), 32% hadno residual or visible disease, 24% had ≤1 cm of disease remainingand 24% had >1 cm residual disease. In 20% of patients with IIIC–IVdisease the amount of residual disease was not clearly documentedin the operative report. In comparison, of those patients with primarystages I–IIIB (n=207) disease, 52% documented no gross residualdisease, 8% had residual disease ≤1 cm, 9% had more than 1 cmdisease remaining and 31% of patients with I–IIIB disease did nothave the amount of residual disease documented (pb0.001). Forpatients undergoing an interval cytoreduction after neoadjuvantchemotherapy or those having surgery for recurrent disease, 19%did not have the amount of residual disease documented, 12% noted>1 cm disease remaining and 70% had less than 1 cm or no visibledisease remaining (Table 2). Operative reports dictated by fellows/residents compared to attendings were more likely to not clearlydocument the amount of residual disease (52% and 19%) pb0.001.
p-value
l disease Amount of residual disease≤1 cm
No residual or visibledisease
16 (7.73%) 107 (51.69%) b0.00179 (23.94%) 104 (31.52%)11 (12.79%) 48 (55.81%) 0.00714 (16.09%) 46 (52.87%) 0.03723 (16.43%) 39 (27.86) b0.00141 (20.30%) 85 (42.08%)31 (15.90%) 87 (44.62%)

219R.P. Gogoi et al. / Gynecologic Oncology 126 (2012) 217–219
Given that the definition of “optimal” has recently changed, weanalyzed the percentage of operative reports that adequately describedthe amount of residual disease according to year of surgery. Therewas astatistically significant increase in appropriate documentation ofamount of residual disease over time (pb0.001) (Table 2). There wasno statistically significant difference in residual disease documentationand surgical staging between the two institutions.
Discussion
Within the surgical community various measurements of qualityoutcome such as NSQIP have been developed. Given that the Societyof Gynecologic Oncologists has developed its own standards forsufficiency in the area of surgery for ovarian cancer, we sought toassess compliance and establish a baseline measure of complianceto these standards at two tertiary medical centers. The creation andimportance of such surgical indicators has been recently describedby Dr. Karl Podratz [8] in his division's experience with ovarian cancercytoreduction at the Mayo Clinic [9].
It is interesting to note that over time in our cohort, there was astatistically significant increase in the documentation of the volumeof residual disease. This may have been due in part to the adjustmentof the definition of “optimal” debulking from less than 1 cm ofresidual disease to no visible disease remaining after surgery. As theresources for research in cancer dwindle [10], the availability ofresearch assistants who are qualified to review operative reports inorder to include patients in clinical trials may also decrease. Surgeonswill thereby have an obligation to provide operative documentationwith increased clarity. The data also suggest that we surgeons aremore likely document residual disease appropriately in moreadvanced stage disease.
In 10% of patients with I–IIIB disease complete surgical staging wasnot performed—a clinical reason for the absence of staging wasdocumented in the operative report. However in 15% of these patients,complete staging was not performed and no reason was given. Themajority of such patients did not have a para-aortic lymphadenectomyperformed during their surgery. It may be that the lymph nodes werepalpated and not found to be enlarged; however this has been found tobe an inaccurate modality of assessing for disease in the retroperitonealspace [11]. In addition, the absence of a lymphadenectomymay translateinto patients being inadequately treated for advanced disease; a priorBritish model of intraoperative assessment of apparent early-stageovarian cancer demonstrated thatwithout the performance of a systemiclymphadenectomy, 6% of patients may not receive further treatment[12]. Furthermore, given that surgeon documentation has a significantimpact in the retrospective assessment of patient care [13], surgeonsmust be alert in their documentation of intraoperative decision making.
The strengths of our study include our analysis of data from twoseparate institutions, composed of 10 active gynecologic oncologists.All operative and pathology reports were assessed by two staffgynecologic oncologists. Furthermore, the rate of patients with lessthan 1 cm or no residual disease remaining is comparable to thatseen in other centers that specialize in surgery for ovarian cancer[14]. Our study was limited by the retrospective nature of its data.The shifting definition of “optimal” debulking may have also led toan overestimation of the numbers of patients who did not have anadequate description of the volume of residual disease, as “optimal”has previously referred to a set measurement of less than 1 cm ofresidual disease. Although there is no literature attesting to theaccuracy of dictations by fellows or residents in gynecologic oncology,a prior prospective study in general surgery noted an error rate ofgreater than 25% when comparing reports dictated by residents to
those dictated by the attending surgeon [15]. Our study similarlyidentified that operative reports dictated by residents or fellowswere less likely to adequately document residual disease.
The unique nature of gynecologic oncology as a specialty requiresthe creation of quality control indicators that focus on measures toimprove care for women with gynecologic malignancies and allowfor transparency in health care we deliver. In the future we hopethe use of an electronic medical record will make the processavailable in “real time”. In addition, the SGO is currently evaluating8 other measures including; pts offered IP chemotherapy afteroptimal cytoreduction, VTE prophylaxis, antibiotic prophylaxis andchemotherapy administered 14 days prior to death as part of theSGO/ASCO QOPI ovarian cancer module. The profession as a specialtyshould not only continue to develop its own quality regulators [16]pertaining to surgical, chemotherapy, radiation, and morbidityoutcomes [17,18], but also to look at our own performance inaccordance with these indicators and find ways to improve ourperformance.
Conflict of interestNo conflict of interest.
References
[1] Hall BL, Hamilton BH, Richards K, Bilimoria KY, Cohen ME, Ko CY. Does surgicalquality improve in the American College of Surgeons National Surgical QualityImprovement Program: an evaluation of all participating hospitals. Ann Surg2009;250:363–76.
[2] Bristow RE, Eisenhauer EL, Santillan A, Chi DS. Delaying the primary surgical effortfor advanced ovarian cancer: a systematic review of neoadjuvant chemotherapyand interval cytoreduction. Gynecol Oncol 2007;104:480–90.
[3] Mercado C, Zingmond D, Karlan BY, et al. Quality of care in advanced ovariancancer: the importance of provider specialty. Gynecol Oncol 2010;117:18–22.
[4] Bristow RE, Palis BE, Chi DS, Cliby WA. The National Cancer Database report onadvanced-stage epithelial ovarian cancer: impact of hospital surgical case volumeon overall survival and surgical treatment paradigm. Gynecol Oncol 2010;118:262–7.
[5] Verleye L, Ottevanger PB, van der Graaf W, Reed NS, Vergote I. EORTC-GCGprocess quality indicators for ovarian cancer surgery. Eur J Cancer 2009;45:517–26.
[6] Gagliardi AR, Fung MF, Langer B, Stern H, Brown AD. Development of ovariancancer surgery quality indicators using a modified Delphi approach. GynecolOncol 2005;97:446–56.
[7] Chi DS, Eisenhauer EL, Lang J, et al. What is the optimal goal of primarycytoreductive surgery for bulky stage IIIC epithelial ovarian carcinoma (EOC)?Gynecol Oncol 2006;103:559–64.
[8] Podratz KC. Quality improvement in gynecologic surgery: the new frontier. Am JObstet Gynecol 2006;195:891–5.
[9] Aletti GD, Dowdy SC, Gostout BS, et al. Aggressive surgical effort and improvedsurvival in advanced-stage ovarian cancer. Obstet Gynecol 2006;107:77–85.
[10] Varmus H. Newsmaker interview: Harold Varmus. Piloting cancer research with ashrinking budget. Interview by Jocelyn Kaiser. Science 2011;333:397.
[11] Eisenkop SM, Spirtos NM. The clinical significance of occult macroscopicallypositive retroperitoneal nodes in patients with epithelial ovarian cancer. GynecolOncol 2001;82:143–9.
[12] Warwick J, Vardaki E, Fattizzi N, et al. Defining the surgical management ofsuspected early-stage ovarian cancer by estimating patient numbers throughalternative management strategies. BJOG 2009;116:1225–41.
[13] Hyman NH, Ko CY, Cataldo PA, Cohen JL, Roberts PL. The New England colorectalcancer quality project: a prospective multi-institutional feasibility study. J Am CollSurg 2006;202:36–44.
[14] Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect ofmaximal cytoreductive surgery for advanced ovarian carcinoma during theplatinum era: a meta-analysis. J Clin Oncol 2002;20:1248–59.
[15] Novitsky YW, Sing RF, Kercher KW, Griffo ML, Matthews BD, Heniford BT.Prospective, blinded evaluation of accuracy of operative reports dictated bysurgical residents. Am Surg 2005;71:627–31 [discussion 31-2].
[16] Hacker NF. Quality control in ovarian cancer surgery. Ann Oncol 2011;22(Suppl.8):viii19–22.
[17] Aletti GD, Santillan A, Eisenhauer EL, et al. A new frontier for quality of care ingynecologic oncology surgery: multi-institutional assessment of short-termoutcomes for ovarian cancer using a risk-adjusted model. Gynecol Oncol2007;107:99–106.
[18] http://www.facs.org/cancer/ncdb/colonmeasures.pdf.