Embed Size (px)
Citation preview

Pediatr Blood Cancer 2014;61:1394–1397
Evaluation of Radiation Dose to Cardiac and Pulmonary Tissue Among Patients WithStage IV Wilms Tumor and Pulmonary Metastases
Ahsan Farooqi, PhD,1* Arsalan Siddiqi, PhD,2 Mohammad K. Khan, MD, PhD,2 and Natia Esiashvili, MD2
INTRODUCTION
Lungs are the most common site of hematogenous metastasis in
Wilms tumor (WT), with approximately 10% of all WT cases, and
80% of stage IVWT patients showing some evidence of pulmonary
involvement at initial diagnosis [1,2]. In these patients, whole-lung
irradiation (WLI) is frequently given at diagnosis, usually within
2 weeks from resection of a primary tumor, along with abdominal
radiotherapy (RT) and chemotherapy to control the metastatic and
primary sites of disease. However, the International Society of
Pediatric Oncology (SIOP) demonstrated that 75% of patients with
stage IV WT and pulmonary metastases responded to pre-
nephrectomy chemotherapy consisting of vincristine, dactinomy-
cin, and doxorubicin [3]. Overall survival in this group was
approximately 83% using this treatment strategy [3].
Drawing from SIOP experience, the Children’s OncologyGroup
(COG) initiated a clinical trial (AREN 0533) which limits
pulmonary RT to only those patients with stage IV WT and
pulmonary metastases who fail to respond to 6 weeks of treatment
with chemotherapy. Currently, around 60% of patients enrolled in
AREN 0533 are still requiring pulmonary RT due to persistence of
pulmonary metastases following chemotherapy [4]. Thus, in these
patients, RT is given sequentially leading to overlap of the
abdominal fields with the pulmonary radiation fields. The exact
doses and objective radiation dose limits are not well quantified in
the current AREN 0533 protocol.
Late complications secondary to chemotherapy and radiothera-
py are observed in approximately 25% of patients with Wilms
tumor and are a significant cause of mortality among the
survivors [5–8]. The cumulative frequency of congestive heart
failure (CHF) is 4.4% at 20 years with the relative risk of CHF
increasing with doxorubicin dosage (3.3/100mg/m2), lung irradia-
tion (1.6/10Gy), and left abdominal irradiation (1.8/10Gy) [9].
Pulmonary complications are seen in approximately 4% of patients
at 15 years from diagnosis, with substantially higher risk in patients
that received whole-lung irradiation (WLI) due to pulmonary
metastases (PM) [10]. We suspect that the radiation doses to the
heart and lungs in the sequential approach may be significantly
greater than the historical concurrent radiation approach, and may
increase the incidence of long-term cardiopulmonary toxicities.
METHODS
Patient Selection
For this study, we retrospectively identified 16 patients with
stage IV favorable histology (FH) Wilms tumor and pulmonary
metastases who received radiotherapy at our institution between
2006 and 2012 (Table I). Of the 16 patients, 12 received concurrent
radiotherapy (RT) to their flank/whole abdomen and lungs at the
time of diagnosis, and the remaining 4 received sequential treatment
in that they were first treated for their flank/abdomen for local
disease, and later received WLI to eradicate pulmonary metastases
that were unresponsive to chemotherapy. The CT simulation scans
for each patient were used to simulate either a sequential or
concurrent treatment. This resulted in a total of 32 treatment plans
that were evaluated for heart and lung dosimetric endpoints.
Patient Simulation and Planning
Patients were positioned supine and computerized tomography
(CT) simulation scans were generated. CT slice thickness was 2–
3mm. The lung planning treatment volume (PTV) was determined
by contouring of the three-dimensional clinical target volume
(CTV) representing whole-lung volume (generated from CT
Background. Most patients with stage IV Wilms tumor (WT) andpulmonary metastases are treated with surgery, local radiotherapy(RT), and whole-lung irradiation (WLI). The Children’s OncologyGroup is studying whether WLI should only be given if metastaticlung lesions persist following induction chemotherapy. We hypoth-esized that radiation dose to cardiac and pulmonary organs areincreased when WLI and abdominal RT fields are administeredsequentially. Procedure. We retrospectively identified 16 patientswith stage IV WT and pulmonary metastases to model dosimetryplans for concurrent and sequential flank or whole abdomen andwhole-lung fields. Results. Treatment plans were evaluated fordosimetric endpoints to the heart and the lungs. The mean dose (Gy)was significantly higher to the heart (15.8 vs. 12.1, P<0.0001) and
lungs (14.1 vs. 12.2, P<0.0002) when patients with stage IVWT andpulmonary metastases were treated with sequential RT. The percenttissue organ volumes (V) receiving highRT doses of 15 and 20Gy (V15
and V20) were negligible in concurrent treatment plans. Compara-tively, mean V15 and V20 values for sequential treatment plans were35% and 27%, respectively, for the heart, and 15% and 12%, for thelungs. Conclusions. The dose to the heart and lung tissue issignificantly increased when WLI and abdominal RT fields areadministered sequentially. While omission of WLI may be beneficialfor patients achieving good response to induction chemotherapy, theless favorable response group may be subjected to increased risk ofcardiac and pulmonary toxicities from sequential WLI. Pediatr BloodCancer 2014;61:1394–1397. # 2014 Wiley Periodicals, Inc.
Key words: late effects; radiation oncology; Wilms tumor
1Texas Tech University Health Sciences Center, School of Medicine
Cancer Center, Lubbock, Texas; 2Department of Radiation Oncology,
Winship Cancer Institute, Emory University School of Medicine,
Atlanta, Georgia
Conflict of interest: Nothing to declare.
�Correspondence to: Ahsan Farooqi, Texas Tech University Health
Sciences Center School of Medicine Cancer Center, 3601 4th Street
Mail Stop 9445 Lubbock, TX 79415-6450.
E-mail: [email protected]
Received 18 December 2013; Accepted 3 February 2014
�C 2014 Wiley Periodicals, Inc.DOI 10.1002/pbc.25007Published online 28 February 2014 in Wiley Online Library(wileyonlinelibrary.com).

images) with an additional margin of 1 cm for setup and respiratory
motion. For whole abdomen irradiation, the entire peritoneal cavity
was defined as the CTV that included the dome of the diaphragm as
the superior border with 1 cm PTV margin. Flank irradiation fields
encompassed target volume covering pre-operative gross tumor
volume based and involved kidney with at least 1 cm setup margin
and also with the medial border extended to cover the entire
vertebral body. In cases of lymph node involvement, the entire para-
aortic nodal chain was covered in clinical target volume. The CT
simulations were used to create 3D-CRT plans with standard
anterior/posterior (AP)-posterior/anterior (PA) field techniques
(Aria1 Oncology Planning System) using 6-MV photons (Varian
Trilogy Dual-Energy Linear Accelerator, Palo Alto, CA). Patients
who were treated concurrently at the time of diagnosis were
prescribed a total dose of 10.5Gy in 7 fractions to the flank or whole
abdomen (based on indication from pathological findings, i.e.,
presence or absence of peritoneal seeding with tumor cells). Lung
PTV received a total of 12Gy (10.5Gy as part of combined lung/
abdominal field plus additional 1.5Gy to lung PTV). Patients who
were treated sequentially were prescribed 10.8Gy to their flank
fields in 6 fractions or 10.5Gy to whole abdominal fields initially,
and then followed by 12Gy in 8 fractions to the whole-lung fields
(Fig. 1). In all cases, RTwas prescribed to the midplane of the AP/
PA fields and received 100% of the total dose.
Data Analysis
Normal tissue organ volumes (V) receiving high RT doses were
compared between patient treatment plans receiving either
sequential or concurrent RT. The percent tissue organ volumes
(V) receiving high RT doses of 15Gy (V15) and 20Gy (V20) were
calculated for each treatment plan and used for comparison. For the
purposes of this study, dose-volume comparisons were made for the
heart and lungs. The mean dose received by organs at risk (whole
heart and lungs) using either the concurrent or sequential treatment
plans were compared using the two-tailed paired samples t test.
Statistical significance was defined as a P-value of less than 0.05.
RESULTS
A total of 16 patients presenting with stage IV WT and
pulmonary metastases (PM) underwent radiation at our institution
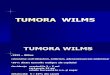
Fig. 1. This image illustrates traditional radiotherapeutic fields used for whole-lung irradiation (WLI) and local radiotherapy (RT) to the primary
tumor site in the setting of a patient with stage IVWTand pulmonarymetastases. ImageA displays a single treatment field that encompasses disease
in both the left flank and the lungs, representing concurrent treatment. ImageB shows the significant overlap that occurs between the flank andWLI
treatment fields, were this patient to be treated sequentially. Note that the overlap occurs over areas which contain significant amounts of cardiac and
pulmonary tissue, resulting in increased radiation dosage to these organs.
TABLE I. Characteristics of Patients With Stage IVWilms Tumor
Patient Gender
Age of
diagnosis
(year)
Concurrent (C)
or sequential (S)
Local site
of radiation
1 Female 5 C Left
2 Female 9 C Right
3 Female 2 C Whole
abdomen
4 Female 7 C Left
5 Female 5 C Left
6 Male 2 C Right
7 Male 9 C Left
8 Female 4 C Left
9 Female 6 C Whole
abdomen
10 Male 5 C Left
11 Male 8 C Left
12 Female 7 C Left
13 Female 5 S Left
14 Male 6 S Left
15 Male 3 S Left
16 Female 5 S Left
Pediatr Blood Cancer DOI 10.1002/pbc
Evaluation of Radiation Dose in Wilms Tumor 1395

as part of this study (Table I). To produce a robust data set for dose-
volume comparison, we generated simulation plans for each of the
16 patients for both concurrent and sequential treatment. We
observed that due to overlap of treatment fields for abdominal/flank
irradiation and WLI (Fig. 1), patients who undergo sequential
treatment received a higher dose of radiation to critical organs such
as the heart and lungs. The mean dose received by the heart was
significantly (15.8 vs. 12.1, P< 0.0001) higher when patients were
treated sequentially (Fig. 2A, Table II). Similarly, the mean dose
received to the lungs was significantly increased (14.1 vs. 12.2,
P< 0.0002) when patients underwent sequential RT (Fig. 2B,
Table II). Patients 3 and 9, who required whole abdominal
irradiationþWLI, received the highest combined dose to the heart
and lungs when treated sequentially (Table II), due to a larger area
of overlap relative to patients receiving flank irradiation and WLI.
Note that there was no difference in combined dose to the heart and
lungs for concurrent treatment plans between the patients receiving
whole abdominal irradiation versus flank irradiation.
We also quantified the normal tissue organ volumes (V)
receiving high RT dosages of 15 and 20Gy (V15 and V20), in these
simulated treatment plans for both the heart and lungs. Because the
maximum dose to the heart and lungs in concurrent treatment plans
was less than 15Gy in all cases, the V15 and V20 values were
negligible. However, mean V15 and V20 values for sequential
treatment plans were 35% and 27%, respectively, for the heart, and
15% and 12%, for the lungs (Table II). These data support our
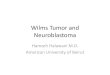
Fig. 2. Comparison of mean cardiac and lung doses between concurrent and sequential radiotherapy in the management of patients with stage IV
WTand pulmonary metastatic disease. A: The mean cardiac dose was found to be significantly (P< 0.0001) higher when patients were planned to
receive sequential irradiation to the flank/abdomen first, followed by whole-lung irradiation. B: Similarly, the mean lung dose was significantly
(P< 0.0002) increased among the sequential RT treatment plans as well.
TABLE II. Dosimetric Comparison of Mean Dose to Heart and Lungs, Among 16 Patients With Stage IVWTand Pulmonary Metastases
Patient
Heart Lungs
Mean dose
concurrent (Gray)
Mean dose
sequential (Gray)
Sequential
V15|V20 values
Mean dose
concurrent (Gray)
Mean dose
sequential (Gray)
Sequential
V15|V20 values
1 12.3 18.5 69%|55% 12.5 14.0 16%|11%
2 12.6 16.7 50%|30% 12.7 15.4 28%|20%
3 12.4 20.3 79%|68% 12.6 17.6 49%|40%
4 12.2 17.0 50%|42% 12.5 14.1 13%|9%
5 12.2 12.8 0%|0% 12.6 13.3 2%|1%
6 12.1 16.4 43%|35% 12.2 15.5 30%|25%
7 12.3 15.4 28%|21% 12.4 13.6 9%|6%
8 12.3 18.3 61%|50% 12.4 14.1 13%|9%
9 12.4 20.6 64%|58% 12.3 17.3 44%|38%
10 12.6 16.9 47%|34% 13.0 14.3 16%|11%
11 12.5 15.9 30%|21% 12.5 12.7 3%|2%
12 12.4 12.4 0%|0% 12.3 12.3 0%|0%
13 10.9 13.5 11%|4% 11.1 12.4 5%|3%
14 12.3 12.3 0%|0% 12.3 12.3 0%|0%
15 10.8 14.2 21%|10% 11.1 12.9 6%|1%
16 11.2 12.9 0%|0% 11.3 13.7 8%|6%
Mean 12.1 15.8 35%|27% 12.2 14.1 15%|12%
P< 0.0001 P< 0.0002
Pediatr Blood Cancer DOI 10.1002/pbc
1396 Farooqi et al.

hypothesis that dosage to the heart and lung tissue is increasedwhen
RT is administered sequentially, as opposed to concurrently at the
time of diagnosis in patients with stage IV disease and pulmonary
metastases.
DISCUSSION
Radiation therapy (RT) is one of the major contributors to side
effects seen among patients treated for Wilms tumor [5]. Prior
studies conducted by the National Wilms Tumor Study Group
(NWTS) attempted to limit the use of RT, and established that RT
can be omitted for patients with stages I and II disease and favorable
histology (FH), and lowered the treatment dose to 1,080 cGy (from
2,000 cGy) for patients with stages III and IV FH tumors [11–13].
However, controversy remains in regards to the use of RT to treat
lung metastases of patients with stage IV disease. The International
Society of Pediatric Oncology (SIOP) found that the majority of
patients with stage IV disease can achieve a long-term complete
response (CR) using only dose-intensive chemotherapy, and
reported a good event-free survival (EFS) and overall survival
(OS) with this strategy [14]. However, the number of patients who
ultimately received lung RT due to relapse was not reported in this
study. In another study conducted by the United Kingdom
Children’s Cancer Study Group (UKCCSG), EFS was severely
compromised in patients with stage IV disease when pulmonary RT
was withheld (79.2% vs. 53.3%, P¼ 0.009) [15]. Based on these
reports, it has been proposed that there exist two groups of patients
with stage IV WT and pulmonary metastases (PM): those that
respond to initial chemotherapy and show resolution of PM, and
those that require further therapy including whole-lung irradiation
(WLI) to eradicate chemorefractory disease.
The Children’s Oncology Group (COG) is studying whether it is
effective to limit pulmonary RT to only those patients who fail to
respond to 6 weeks of treatment with doxorubicin, dactinomycin,
and vincristine. Based on initial report, approximately 40% of
patients are showing complete response (CR) to pulmonary disease
following treatment with chemotherapy, whereas the remaining
60% are progressing to receiveWLI [4]. Unfortunately, there are no
good biomarkers to assess which patients are likely to respond to
chemotherapy, andwhichwill require chemotherapyþWLI to treat
pulmonary metastatic disease.
Our study introduces another variable that needs to be addressed
with regards to the role of RT in the management of patients with
stage IV WT and pulmonary metastases. Our data indicate that
patients not achieving complete response to initial chemotherapy
and undergoing sequential RT will inadvertently receive a
significantly higher dose of radiation to the heart and lungs. This
is largely due to the overlap that occurs in traditional treatment
fields for the flank/abdomen and the lungs. In these patients, the
increased dose received to the heart and lungs places them at an
increased risk of developing serious late-stage complications
frequently seen among WT survivors, such as pulmonary fibrosis,
and congestive heart failure [9,10].
Our data also highlight the importance of identifying novel
strategies based on more sophisticated methods for evaluating
tumor burden in the lungs or the use of tumor biomarkers that may
aid in discriminating between those patients whose metastases are
likely to respond to chemotherapy and those who will need more
intensive treatment such as WLI. Molecular studies have indicated
that elevated mRNA levels of telomerase components, hTERT,
encoding the telomerase catalytic component, and hTR, encoding
the telomerase RNA component, correlate with a negative
prognosis in Wilms tumor and an increased chance of recur-
rence [16,17]. Furthermore, loss of heterozygosity for chromo-
somes 16q and 1p in Wilms tumor predicts an adverse outcome
[18]. It is possible that these genetic changes, or other unknown
molecular events, confer resistance to chemoradiotherapy in the
setting of stage IV Wilms tumor. A recent report suggests that
survival of patients with stage IV WT and pulmonary metastases is
highly dependent upon primary tumor histology [19]. In this study,
patients were treated with pre-nephrectomy chemotherapy using
the SIOP strategy and then histologically graded following surgery
using the revised SIOP classification of renal tumors [20]. Overall
survival was found to be significantly poorer in children with high-
risk primary tumor histology (OS 44.4%) compared to intermediate
risk (OS 89.2%, P< 0.001) and low risk histology (OS 100.0%,
P< 0.001). These data indicate that high-risk histology may be
used as a marker to identify patients that require more aggressive
therapy at diagnosis.
In conclusion, our data show that patients with stage IVWTand
pulmonary metastases are exposed to increased radiation dose to
cardiac and pulmonary tissue if they undergo sequential RT as
opposed to concurrent RT. Additional studies are needed to identify
those patients with stage IV disease whowill require intensification
of therapy, and those in whom omission of WLI will be a safe
strategy for achieving good disease outcome and lower long-term
toxicities.
REFERENCES
1. Davidoff AM. Wilms’ tumor. Curr Opin Pediatr 2009;21:357–364.
2. Green DM, Fernbach DJ, Norkool P, et al. The treatment of Wilms’ tumor patients with pulmonary
metastases detected only with computed tomography: A report from the National Wilms’ Tumor Study. J
Clin Oncol 1991;9:1776–1781.
3. de Kraker J, Lemerle J, Voute PA, et al. Wilm’s tumor with pulmonary metastases at diagnosis: The
significance of primary chemotherapy. International Society of Pediatric Oncology Nephroblastoma Trial
and Study Committee. J Clin Oncol 1990;8:1187–1190.
4. Dome JS, Fernandez CV, Mullen EA, et al. Children’s Oncology Group’s 2013 blueprint for research:
Renal tumors. Pediatr Blood Cancer 2013;60:994–1000.
5. Wright KD, Green DM, Daw NC. Late effects of treatment for wilms tumor. Pediatr Hematol Oncol
2009;26:407–413.
6. Termuhlen AM, Tersak JM, Liu Q, et al. Twenty-five year follow-up of childhood wilms tumor: A report
from the childhood cancer survivor study. Pediatr Blood Cancer 2011;57:1210–1216.
7. Cotton CA, Peterson S, Norkool PA, et al. Early and late mortality after diagnosis of wilms tumor. J Clin
Oncol 2009;27:1304–1309.
8. Paulino AC,Wen BC, Brown CK, et al. Late effects in children treated with radiation therapy for Wilms’
tumor. Int J Radiat Oncol Biol Phys 2000;46:1239–1246.
9. Green DM, Grigoriev YA, Nan B, et al. Congestive heart failure after treatment for Wilms’ tumor: A
report from the National Wilms’ Tumor Study group. J Clin Oncol 2001;19:1926–1934.
10. Green DM, Lange JM, Qu A, et al. Pulmonary disease after treatment for wilms tumor: A report
from the national Wilms tumor long-term follow-up study. Pediatr Blood Cancer 2013;60:
1721–1726.
11. D’Angio GJ, Breslow N, Beckwith JB, et al. Treatment of Wilms’ tumor. Results of the Third National
Wilms’ Tumor study. Cancer 1989;64:349–360.
12. D’Angio GJ, Evans A, Breslow N, et al. The treatment of Wilms’ tumor: Results of the Second National
Wilms’ Tumor study. Cancer 1981;47:2302–2311.
13. Green DM, Beckwith JB, Breslow NE, et al. Treatment of children with stages II to IV anaplastic
Wilms’ tumor: A report from the National Wilms’ Tumor Study Group. J Clin Oncol 1994;12:
2126–2131.
14. Verschuur A, Van Tinteren H, Graf N, et al. Treatment of pulmonary metastases in children with stage IV
nephroblastoma with risk-based use of pulmonary radiotherapy. J Clin Oncol 2012;30:3533–3539.
15. Nicolin G, Taylor R, Baughan C, et al. Outcome after pulmonary radiotherapy in Wilms’ tumor patients
with pulmonarymetastases at diagnosis: AUKChildren’s Cancer Study Group,Wilms’ TumourWorking
Group Study. Int J Radiat Oncol Biol Phys 2008;70:175–180.
16. Dome JS, Chung S, Bergemann T, et al. High telomerase reverse transcriptase (hTERT) messenger RNA
level correlates with tumor recurrence in patients with favorable histology Wilms’ tumor. Cancer Res
1999;59:4301–4307.
17. Dome JS, Bockhold CA, Li SM, et al. High telomerase RNA expression level is an adverse prognostic
factor for favorable-histology Wilms’ tumor. J Clin Oncol 2005;23:9138–9145.
18. Grundy PE, Telzerow PE, Breslow N, et al. Loss of heterozygosity for chromosomes 16q and 1p in
Wilms’ tumors predicts an adverse outcome. Cancer Res 1994;54:2331–2333.
19. Warmann SW, Furtwangler R, Blumenstock G, et al. Tumor biology influences the prognosis of
nephroblastoma patients with primary pulmonary metastases: Results from SIOP 93-01/GPOH and SIOP
2001/GPOH. Ann Surg 2011;254:155–162.
20. Vujanic GM, Sandstedt B, Harms D, et al. Revised International Society of Paediatric Oncology (SIOP)
working classification of renal tumors of childhood. Med Pediatr Oncol 2002;38:79–82.
Pediatr Blood Cancer DOI 10.1002/pbc
Evaluation of Radiation Dose in Wilms Tumor 1397