Embed Size (px)
Citation preview

Translational Science
Evaluation of Explant Responses to STINGLigands: Personalized Immunosurgical Therapyfor Head and Neck Squamous Cell CarcinomaJason R. Baird1, R. Bryan Bell1,2, Victoria Troesch1, David Friedman1, Shelly Bambina1,Gwen Kramer1,Tiffany C. Blair1,Terry Medler1,YapingWu3, Zhaoyu Sun1,Tanja D. de Gruijl4,Rieneke van de Ven4, Rom S. Leidner1, Marka R. Crittenden1,5, and Michael J. Gough1
Abstract
Surgeons have unique in situ access to tumors enablingthem to apply immunotherapies to resection margins as ameans to prevent local recurrence. Here, we developed asurgical approach to deliver stimulator of interferon genes(STING) ligands to the site of a purposeful partial tumorresection using a gel-based biomaterial. In a range of headand neck squamous cell carcinoma (HNSCC) murine tumormodels, we demonstrate that although control-treatedtumors recur locally, tumors treated with STING-loadedbiomaterials are cured. The mechanism of tumor controlrequired activation of STING and induction of type I IFN inhost cells, not cancer cells, and resulted in CD8 T-cell–mediated cure of residual cancer cells. In addition, we used
a novel tumor explant assay to screen individual murine andhumanHNSCC tumor responses to therapies ex vivo. We thenutilized this information to personalize the biomaterial andimmunotherapy applied to previously unresponsive tumorsin mice. These data demonstrate that explant assays identifythe diversity of tumor-specific responses to STING ligandsand establish the utility of the explant assay to personalizeimmunotherapies according to the local response.
Significance: Delivery of immunotherapy directly to resec-tion sites via a gel-based biomaterial prevents locoregionalrecurrence of head and neck squamous cell carcinoma.Cancer Res; 78(21); 6308–19. �2018 AACR.
IntroductionSurgery is a primary mode of treatment for many patients
with head and neck squamous cell carcinoma (HNSCC), butadverse histopathologic features, such as close or positivemargins, extranodal spread of tumor in metastatic lymphnodes, multiple lymph node metastases, and perineural andperivascular spread, are negative prognostic indicators forwhich adjuvant radiotherapy or chemoradiation therapy isrecommended (1). However, despite risk-adapted adjuvanttherapy, almost half of patients with locoregionally advancedHPV-negative (HPV�) HNSCC who undergo surgical resectionrecur locally or distantly. Local recurrence can be particularlyresistant to subsequent therapy, and many patients experiencedevastating complications from uncontrolled tumor progres-sion and/or the salvage treatment.
Despite a concerted effort on the part of surgeons to extirpate allviable tumor cells, local recurrence develops in approximately25% of patients who have histologically negative margins (2).Furthermore, approximately 25% of patients with positive mar-gins do not recur. This observation suggests that residual tumorcells can be present following surgery and that some patients cancontrol residual disease following the operation.Ourprior studieshave demonstrated that immune mechanisms can control min-imal residual disease following surgical resection in preclinicalmodels, and that the addition of systemic immunotherapy canenhance local control (3). Moreover, in melanoma we demon-strated clinical immune control of distant metastasis by localinjections of CpG after surgical removal of the primary tumor and1 week prior to the sentinel lymph node procedure (4). Thus, theability to enhance tumor-specific adaptive immune responsesat the time of the initial procedure may be valuable for controlof residual microscopic disease, as well as distant tumor deposits(3, 5, 6).
Recently, we and others have demonstrated that intratumoralcyclic dinucleotide (CDN) ligand activation of the stimulator ofinterferon genes (STING)pathway strongly induces type I IFN andTNFa responses, resulting in rapid regression of a range of tumors(7–9). We found that STING is strongly expressed in HPVþ
HNSCC cancer cells, but is poorly expressed in HPV� HNSCCcancer cells (10). We and others have shown that local admin-istration of STING ligands to the tumor results in the nonauton-omous activation of STING in noncancer cells within the tumorenvironment, indicating that this therapy can be effective in bothSTINGþ and STING� cancers (7, 8, 10). These data also imply thatin HPV� HNSCC any response to STING ligand will be entirely
1Earle A. Chiles Research Institute, Robert W. Franz Cancer Center, ProvidencePortland Medical Center, Portland, Oregon. 2Head and Neck Institute, Portland,Oregon. 3Pathology, Providence Portland Medical Center, Portland, Oregon.4Department of Medical Oncology, VU Medical Center, Cancer Center Amster-dam, Amsterdam, the Netherlands. 5The Oregon Clinic, Portland, Oregon.
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
Corresponding Author: Michael J. Gough, Providence Portland Medical Center,4805NEGlisan St, Portland, OR 97213. Phone: 503-215-3928; Fax: 503-215-6841;E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-18-1652
�2018 American Association for Cancer Research.
CancerResearch
Cancer Res; 78(21) November 1, 20186308
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

dependent on the response of host cells in the tumor immuneenvironment, and therefore has the potential to vary significantlybetween individuals with widely varying tumor composition.
Recently, novel approaches have been developed that takeadvantage of the wound-healing response to target systemicimmunotherapy to the site of resection (11). STING ligandsrequire local action, and because surgeons are in the uniqueposition of being in direct contact with the tumor during resec-tion, this provides an opportunity to apply therapies directly tothe resection margins to target residual cancer cells. Using thisclose proximity to our advantage, we developed an approach thatapplied immunotherapies directly in the resection cavity at thetime of surgery. Following closure of the resection site, theimmunotherapy will remain in place to activate local immunemechanisms to control residual disease. To apply this therapy, wedeveloped a hydrogel-like formulation of STING ligands that is aliquid when refrigerated but forms a gel following in vivo appli-cation. We call this STING-targeted surgical immunotherapySTINGblade. Herein, we demonstrate using murine models ofpurposeful partial tumor resection that STINGblade results indramatic immune-mediated control of residual disease. We fur-ther develop a postresection explant model to identify the vari-ability of responses to STINGblade inmurine and patient tumors,and demonstrate that based on these responses, STINGblade canbe personalized to improve tumor control.
Materials and MethodsAnimals and cell lines
Six- to 8-week-old female C3H, C57BL/6, or BALB/c mice wereobtained from Charles River Laboratories for use in these experi-ments. STING�/� (Goldenticket Stock# 017537) and IFNAR1�/�
(Stock# 028288) mice were obtained from The Jackson Labora-tory. Survival experiments were performed with 6 to 8 mice perexperimental group, and mechanistic experiments with 4 to 6mice per group. Animal protocols were approved by the Earle A.Chiles Research Institute (EACRI) Institutional Animal Care andUse Committee (Animal Welfare Assurance No. A3913-01).
The SCCVII squamous cell carcinoma cell line was kindlyprovided in 2014 by Dr. Lee (Duke University Medical Center,Durham, NC). The TC1 squamous cell carcinoma cell line is aRas and HPV-transformed mouse cell line, commonly used as aC57BL/6 mouse model of HNSCC (12), and was kindly pro-vided by Dr. Hong Ming Hu (EACRI, Portland, OR). The 4T1mammary carcinoma cell line (BALB/c; ref. 13) was obtainedin 2009 from the ATCC. MOC1 and MOC2 were kindly pro-vided in 2017 by Dr. Ravindra Uppaluri (Dana Farber CancerInstitute, Boston MA; ref. 14). Authentication was performedusing murine haplotype-specific MHC antibodies, and theywere tested for contamination within the past 6 months usinga Mycoplasma Detection Kit (SouthernBiotech).
Antibodies and reagentsThe STING ligands cyclic-di-AMP and rr-cyclic-di-AMP were
obtained from Invivogen. Blocking anti-IL10R antibody (BE0050– BioXCell) was given at a 100 mg dose in the biomaterial.Depleting anti-CD8 (YTS 169.4) antibodies were obtained fromBioXCell and were given i.p. 50 mg one day before treatment andagain 1 week later. Flow cytometry antibodies included CD45-BV786, CD4-PE, TNFa-BV421 (BD Biosciences), CD90.2-AF700,CD11b-BV605, Ly6C-BV711, Ly6G-PE-594, F4/80-PerCPCy5.5
(Biolegend), CD8-AF647, MHCII-FITC (eBioscience), andCD24-APCe780 (Thermo-Fisher).
Subtotal tumor resection modelTumors were inoculated subcutaneously into immune-
competent female mice at a dose of 5 � 105 SCCVII (C3Hmice),5� 105 TC1, 2� 105 MOC1, 2� 105 MOC2 (all C57BL/6mice),or 2� 104 4T1 (BALB/cmice). Tumorswere allowed to develop to7 to 9 mm in diameter, at which point the mice underwentsubtotal resection. Briefly, mice were anesthetized by Isofluraneinhalation, and following surgical skin prep, an incision wasmade over the tumor and the encapsulated tumor mechanicallydetached from the skin. The tumor capsule attached to theunderlying fascia was left in place and the upper portion of thetumor resected, leaving 1 to 3mmdepth of tumor, approximately20% of the original material, in the resection cavity. Mice wererandomized to treatment with local immunotherapy in a bioma-terial. To develop a simple biomaterial for delivery of immuno-therapy to the resection cavity, we employed the phase transitionproperty of Matrigel (Corning Inc.), a thermoresponsive hydrogelprimarily composed of laminin and collagen IV. Matrigel wasmixed 1:4with PBS or PBS containing 25mg cyclic-di-AMP (CDN)and kept on ice at 4�C. A 0.01mL volume of this liquid agent wasmanually placed dropwise into the surgical cavity and allowed toundergo phase transition over 1 to 5 minutes. On application tothe surgical cavity, the hydrogel formed an amorphous solid thatheld position through wound closure. Following application,the wound was closed and mice were allowed to recover.Tumor-bearing mice were monitored a minimum of 3 days perweek and euthanized when tumors exceeded 12 mm in anydimension, or when body condition score declined one level.Euthanasia was performed with CO2 inhalation followed by asecond method.
Wound-healing modelsTo determine whether normal tissue healing was affected by
treatment, we used a classic excisional injury model. Shaved,anesthetized mice were given full-thickness dermal excisionalwounds using a 3-mm dermal biopsy punch (Acu Punch,Acuderm). Each 3 mm wound was treated with Matrigel con-taining PBS or CDN at a dose of 25 mg as above. Wound healingwas documented, and at day 7 after wounding, mice wereeuthanized and the wounds with surrounding tissue wereexcised and paraffin-embedded for histology. To analyze thedegree of re-epithelialization, 10 mm sections were hematoxylinand eosin–stained and scanned for digital microscopy using aLeica SCN400 whole slide scanner. The distance between epithe-lial tongues was measured at the widest opening.
To determine whether the biomaterials affect the strength ofincisional repair, we use a standard approach to measure themechanical strength of healing incisional wounds. Shaved, anes-thetized mice were given a 2 cm incisional wound extendingthrough the dermis and the panniculus carnosus in the paraspinalregion. The wound site was treated with Matrigel containing PBSorCDNat a dose of 25mg as above and closed using sterile surgicalclips. Surgical clips were removed after 5 days, and the woundswere harvested 2 days later. From each wound, strips perpendic-ular to the incision were excised and subjected to tensiometry. Inthis procedure, sequentially increased tension was applied to theexcisedwound strips using aM7-10 digital force gauge on an ES20test stand, andMESUR gauge software, all acquired fromMark-10
Personalized Surgical Immunotherapy
www.aacrjournals.org Cancer Res; 78(21) November 1, 2018 6309
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

Corporation. Wound disruption strength was defined as the loadvalue of wound disruption.
HNSCC tissue samplesDeidentified human tissue sections and freshly excised surgical
material were obtained with written-informed consent from thepatients and conducted in accordance with recognized ethicalguidelines under IRB# 12-075 approved by the Providence Port-landMedical Center Institutional Review Board. The tumors wereclassified as HPVþ if they scored as positive for p16 by immu-nohistochemistry and originated in the oropharynx. Samples thatwere negative for p16 and/or originated outside the oropharynxwere scored as HPV�. Representative tissue blocks for analysiswere identified by the reviewing pathologist. Patient details areprovided in Supplementary Fig. S1.
Explant assayExcised murine tumors or surgical samples from human sub-
jects undergoing resection forHNSCCwere delivered to the labonice following excision. The fresh tumor samples were dissectedinto 2mmfragments and each fragment placed into 96-well platespreloaded with PBS or 25 mg rr-CDA, which has a broad spectrumactivity to both murine and human STING (8). Explants wereoverlaidwith 100mLmedia containing human serum for 24hoursthen analyzed for cytokine secretion into the media by multiplexbead assay (Life Technologies) as previously described (15) andread on a Luminex 100 array reader. Cytokine concentrations forreplicates of each tumor sample were calculated according to astandard curve.
ImmunohistologyFor immunohistology, murine tumor-draining lymph nodes
were fixed in Z7 zinc-based fixative overnight (16). Tissue wasthenprocessed for paraffin tissue sections.Note that 5mmsectionswere cut andmounted for analysis. Tissue sections were boiled inEDTA buffer for antigen retrieval. Immunohistology antibody tocytokeratin-19 (CK19) was purchased from Santa Cruz Biotech-nology. Primary antibody bindingwas visualizedwith AlexaFluor488–conjugated secondary antibodies (Molecular Probes) andmounted with 40,6-diamidino-2-phenylindole (DAPI; Invitro-gen) to stain nuclear material.
Routinely processed paraffin-embedded tumor tissues fromsurgical specimens of patients tested in the explant assay wereused to prepare 5 mm sections for staining. Sections were depar-affinized, rehydrated, and then deprotected before sequentialstaining with primary antibodies to PDL1 (Cell Signaling Tech-nology), CD163 (Roche), CD8 (Spring Bioscience), Cytokeratin(Dako), CD3 (GeneTex), and FoxP3 (Abcam). Antibody bindingwas visualized using a horseradish peroxidase–conjugated anti-species antibody (Biocare Medical) and an Opal 7-color manualIHC kit (Perkin Elmer). Slides were counterstainedwithDAPI andmounted for analysis. Serial sections were stained for expressionof STING as previously described (10).
Images were acquired using a Zeiss Axio observer Z1with attached Nuance Multispectral Image camera and software(Perkin Elmer). All images displayed in the article are represen-tative of the entire tumor and their respective experimental cohort.
Flow cytometryMOC1 and MOC2 tumors grown in C57BL/6 mice were
harvested, and single-cell suspensions were prepared by dissec-
tion into 2mm fragments followed by agitation in digest solution(1mg/mL collagenase, 100 mg/mL hyaluronidase, and 20mg/mLDNase in PBS) for 1 hour at room temperature as previouslydescribed (17). The digest was filtered through 100 mm nylonmesh to remove macroscopic debris. Cells were left untreated orstimulated with 25 mg/mL CDA in the presence of brefeldin A for4 hours at 37�C. Cells were surface stained for amajor phenotypicmarkers including viability dye and CD45, CD90, CD19, CD4,CD8, CD11b, MHCII, Ly6C, Ly6G, CD11c, CD24, and F4/80to distinguish CD11bþMHCIIþLy6C�Ly6G�F4/80þ macro-phages, CD11bþMHCII�Ly6CþLy6Gþ neutrophils, CD11bþF4/80�Ly6G�Ly6Cþ monocytic cells, and CD24þMHCIIþCD11bhi
DC1, CD24þMHCIIþCD11blow DC2 (21). Cells were addition-ally permeabilized and intracellularly stained with anti-TNFa toidentify the responsive cell subsets. Samples were run on an LSRIIflow cytometer (BD Biosciences) and analyzed using FloJo.
Statistical analysisData were analyzed and graphed using Prism (GraphPad
Software). Individual data sets were compared using the Studentt test, and analysis across multiple groups was performed usingANOVAwith individual groups assessedusing Tukey comparison.Overall survival of groups was compared using the log-rank testfor differences in Kaplan–Meier survival curves.
ResultsWe developed a model of subtotal tumor resection using
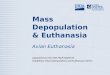
subcutaneous tumors in immunocompetent mice followed bythe application of the hydrogel Matrigel into the resection cavity(Fig. 1A). Matrigel was selected based on useful properties,including its solubility in water, ability to absorb water-solubleagents, capacity to form a gel-like solid when elevated to bodytemperature, and rapid degradation in vivo. In mice bearingestablished SCCVII squamous cell carcinoma that were treatedwith subtotal tumor resection and local application of Matrigel,tumors rapidly recurred at the resection site (Fig. 1A). Our locallyadministered immunotherapy consisted of STING ligands, whichstrongly induce type I IFN and TNFa, resulting in rapid regressionof a range of advanced tumors following direct intratumoralinjection (7–9). When STING ligands are incorporated intoMatrigel, this resulted in cure of the residual tumor (Fig. 1B)without any signs of toxicity. To evaluate long-term tumor con-trol, mice bearing SCCVII tumors received subtotal resection andwere randomized to receive Matrigel containing PBS or CDN tothe resection site. All mice receiving PBS recurred locally, whereasthose mice receiving STING ligands were cured (P < 0.0001; Fig.1C). These data demonstrate that STING ligands act as a potentlocal immunotherapy that controls residual tumors followingsurgical resection in HNSCC preclinical models and suggests arole for implantable immune-modulating interventions toimprove locoregional control in human patients.
To confirm these findings in a differentmodel, we used the TC1tumor model, which is a Ras and HPV-transformed mouse cellline and is commonly used as aC57BL/6mousemodel ofHNSCC(12). As with SCCVII, subtotally resected TC1 tumors regrewlocally, but local recurrencewaspreventedby local administrationof CDN in Matrigel (P < 0.01; Fig. 2A). We then used syngeneicC57BL/6 STING�/� and IFNAR1�/�mice to investigate themech-anism of tumor cure by STING ligands. Subtotal resection pluslocal administration of CDN inMatrigel was no longer effective in
Baird et al.
Cancer Res; 78(21) November 1, 2018 Cancer Research6310
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

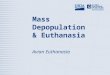
IFNAR1�/� mice, which lack the ability to respond to type I IFN,and as expected was no longer effective in STING�/� mice, wherethe cancer cells are unchanged, but the host cells lack the ability torecognize CDN (wt CDN vs. IFNAR1�/� CDN P < 0.001; wt CDNvs. STING�/� CDN P < 0.0001; Fig. 2A). These data agree withobservations in C3H mice bearing SCCVII tumors (Fig. 1B);because SCCVII lack expression of STING (10), the effectivenessof therapy with STING ligands in this model will be entirelydependent on host cell expression of STING. Prior therapies usingintratumoral injection of STING ligands demonstrated a similardependence on host STING and IFNAR1 responsiveness, but werealso dependent on CD8þ T cells for efficacy (8). The rapidposttreatment tumor regression following STINGblade meant wewere not able to evaluate T-cell influx into the residual tumor.Instead, to determine whether subtotal resection plus localadministration of CDN resulted in adaptive immune control ofresidual disease,mice were depleted of CD8þ T cells starting 1 dayprior to resection. Depletion of CD8þ T cells reduced the efficacyof STINGblade (P < 0.05; Fig. 2B), indicating that adaptiveimmune responses are required for control of residual disease.
However, there remained some efficacy in the absence of T cells,which would be consistent with inflammatory action, such as theT-cell–independent TNFa-mediated hemorrhagic necrosisreported following administration of STING ligands to tumors(7, 19). These data demonstrate that application of STING ligandsto the resection cavity results in local control of tumor recurrencevia activation of STING in host cells, type I IFN signaling in hostcells, and results in CD8þ T-cell–mediated cure of tumors.
Because STINGblade generates CD8-mediated control of resid-ual disease, it is possible that these CD8 T cells can also controldistant tumor. The SCCVII model is spontaneously metastatic,resulting in micrometastases in the tumor-draining lymph node(Fig. 3A; ref. 20), and in untreated mice, lung metastases candevelop (not shown). Mice cured of the primary tumor by STINGligands had no evidence of metastatic disease and remainedtumor-free long term, suggesting control of metastatic diseasewith the local therapy. To determine whether CD8 T-cell immu-nity affected gross distant disease,micewere given tumors onbothflanks and only one treated with subtotal resection plus localadministration of CDN. We found that growth of the distant
TumorSkin
Woundclip
Residualdisease
Immunotherapy
Destroyedtumor
CureRecurrence
Subtotalresection
Subtotalresection
Subtotal resection immunotherapy model
Local recurrence
Tumor cure
Cure - depilated skin
0
5
10
15
+- CDN
Tum
or d
iam
eter
(mm
)
(ii) SCCVII post resection
0
50
100
0 50
PBSCDN
Per
cent
sur
viva
l
(iii) SCCVII survival
100Time (days)
Subtotal resection modelA
C
B
****
PBS
SCCVII Surgery+PBS
Surgery+CDN
(i) Experimental design
C3H
Subtotal resection
****
Hydrogel
Figure 1.
Cure of subtotal resection by STINGblade. C3H mice challenged with SCCVII tumors underwent subtotal resection of the primary tumor, leaving approximately20% of the tumor in place. Matrigel containing PBS (A) or 25 mg CDN (B) was applied into the resection cavity, and the wound was closed. Images show arepresentative example of subtotal resection and local recurrence in PBS group versus cure in CDN group. Hair was removed from the site of cured tumor toreveal the healed skin. C, i, C3H mice challenged with SCCVII tumors were randomized to receive surgery, followed by implantation of Matrigel containing PBS orCDN into the resection cavity and followed for recurrence. Summary of tumor size d12 following resection (ii) and overall survival (iii). ���� , P < 0.0001.
Personalized Surgical Immunotherapy
www.aacrjournals.org Cancer Res; 78(21) November 1, 2018 6311
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

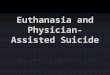
tumor was modestly suppressed by CDN treatment within thesubtotal resection site, but not by surgery alone, indicating somelimited impact of systemic immunity on gross disease (Fig. 3B).To evaluate this in a more aggressive model of metastases, weestablished subcutaneous 4T1 mammary carcinomas in BALB/cmice, which results in early spontaneous development of lungmetastases (Fig. 3C, i; ref. 15). Subtotal resection plus localadministration of CDN resulted in improved local control com-pared with control treatment (Fig. 3C, ii). However, this did notresult in long-term survival due to unchanged progression of lungmetastases (Fig. 3C, iii). Thus, even mice that had their primarytumor cured by STINGblade did not experience improved overallsurvival, suggesting that our local therapy was unable to effec-tively treat this distant disease in the 4T1model. Development oflungmetastases was also unaffected following complete resectionof the primary tumor (Fig. 3D, i), indicating that cancer cells hadalready metastasized prior to the operation and removal of theprimary tumor at this time point had no impact on metastaticprogression. To address this, we performed an early resection of4T1 tumors within 5 days of tumor implantation (Fig. 3D, ii). Inthis setting, STINGblade significantly extended survival oversurgery alone (P < 0.01) and resulted in cure of some mice,with no development of metastatic disease in these animals(Fig. 3D, iii). These data indicate that although application ofSTING ligands to the resection cavity is an effective locoregional
therapy leading to control of metastases if performed beforesystemic spread, our therapy has limited ability to control distantdisease despite its CD8þ T-cell–dependent mechanism of action.
One concern in developing a postresection immunotherapy iswhether it interferes with wound healing. To address effects ofSTINGblade on wound healing, we tested the effect of MatrigelplusCDNdissolved in PBSorMatrigel plus PBS control in both anincisional wound strength model and an excisional wound-heal-ing model. For the incisional wound strength model, shaved,anesthetized mice were given an incisional wound extendingthrough the dermis and the panniculus carnosus. The woundsite was then treated with Matrigel containing PBS or CDN andclosed using sterile surgical clips. Surgical clipswere removed after5 days, and the skin surrounding the wound was harvested at day7. For each wound, strips perpendicular to the incision wereexcised and subjected to tensiometry (Fig. 4A, i). We found nosignificant difference in wound strength between PBS and CDN-treated wounds (Fig. 4A, ii). For the excisional model, shaved,anesthetized mice were given full-thickness dermal excisionalwounds using a dermal biopsy punch and then treated withMatrigel containing PBS or CDN. There was no difference inwound closure between PBS and CDA-treated animals (Fig. 4B, i).Pathologic assessment did not identify any significant differencesin immune infiltrate of wounds between PBS and CDA-treatedanimals, and histologic examination of the closed wounds
0
5
10
15
+ + + +- + - +- - + +
MatrigelCDNAnti-CD8
Tum
or d
iam
eter
(mm
)
****
(ii) SCCVII post resection
0
5
10
15
+ + + +- + - +- - + +
MatrigelCDNIFNAR1-/-
Tum
or d
iam
eter
(mm
)
(ii) TC1 post resection
- - - - STING-/-
++-+
0
50
100
0 20
wt PBSwt CDN
Per
cent
sur
viva
l
(iii) TC1 survival
40Time (days)
IFNAR1-/- PBSIFNAR1-/- CDNSTING-/- CDN
80
0
50
100
0 20
PBSCDN
Per
cent
sur
viva
l
(iii) SCCVII survival
40Time (days)
Anti-CD8 PBSAnti-CD8 CDN
8060
TC1 Surgery + PBS
Surgery + CDN
(i) Experimental design
C57BL/6STING-/-
IFNAR1-/-
A
B
SCCVII Surgery + PBS
Surgery + CDN
(i) Experimental design
C3H+/- anti-CD8
**N
SN
SN
SNS
******
60
******
**** ****
Figure 2.
Tumor cure by STINGblade depends on STING expression and IFNAR1 expression by the host and is mediated by CD8 T cells. A, i, C57BL/6 mice, STING�/�,or IFNAR1�/� mice on the C57BL/6 background were implanted with TC1 tumors and randomized to receive surgery, followed by implantation ofMatrigel containing PBS or CDN into the resection cavity and followed for recurrence. Summary of tumor size d12 following resection (ii) and overallsurvival (iii). B, i, C3H mice bearing SCCVII tumors were randomized to receive anti–CD8-depleting antibody or no treatment, and 1 day later, mice were furtherrandomized to receive surgery, followed by implantation of Matrigel containing PBS or CDN into the resection cavity and followed for recurrence. Summaryof tumor size d12 following resection (ii) and overall survival (iii). NS, not significant; � , P < 0.05; �� , P < 0.01; ��� , P < 0.001; ���� , P < 0.0001.
Baird et al.
Cancer Res; 78(21) November 1, 2018 Cancer Research6312
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

demonstrated that in both groups thewounds actively closedwitha defined epithelial tongue, resulting in no significant differencein re-epithelialization of the excisional wound between groups(Fig. 4B, ii and iii). These data demonstrate that STINGblade curestumors without affectingwound healing, suggesting that this is animmunotherapy that can be safely applied without adverselyaffecting surgical outcomes.
Intratumoral injection of STING ligands has demonstratedefficacy in a range of tumor models and mouse backgrounds(7–9); however, not all mouse tumor models respond to thistherapy (9). To evaluate this diversity of responses in tumors, wedeveloped an explant model, where the resected portion of thetumor was tested for its ex vivo response to STING ligands(Fig. 5A). To determine whether this explant approach could be
(ii) Late TDLN(i) Early TDLN
0
5
10
15
+ + -- + -
SurgeryCDN
Tum
or d
iam
eter
(mm
)
(ii) Opposite flank tumor
RL
RL
No surgery
Surgery + PBS
Surgery + CDNRL
(i) Experimental design
* *
A B
0
50
100
0 10
PBSCDN
Per
cent
sur
viva
l
(iii) 4T1 survival
20Time (days)
40300
5
10
15Tu
mor
dia
met
er (m
m)
0 10 20Time (days)
4030
(ii) Local recurrence
Surgery + PBS
Surgery + CDN
(i) Experimental designC
(i) Lung metastases
CDN - +0
20
80
Num
ber o
f met
s/lu
ng
60
40
- +Complete + + - -
Partial - - + +
TC1TC1
Green - cytokeratinBlue - DAPI
Lung metastases
4T1
(iii) Early resection
0
50
100
Per
cent
sur
viva
l
Surgery + PBS
Surgery + CDN
4T1
d12
d4
(ii) Experimental designD
0 20 40Time (days)
8060
PBSCDN
*
NS
**
Figure 3.
STINGblade cures locoregional metastases but not distant disease. A, C3H mice bearing SCCVII tumors were euthanized at d14 (early; i) or d21 (late; ii)time points, and the tumor-draining lymph nodes were harvested and assessed for metastases by immunofluorescence histology for CK19 (green) and DAPI (blue).Representative images show infiltration of cancer cells in the subcellular capsule at d14 and trabeculae at d21. Scale bar, 100 mm. B, i, C57BL/6 mice wereimplanted with a primary TC1 tumor on the right flank at d0 and a secondary tumor on the left flank at d9. Mice were randomized to no treatment or to receivesurgery to the primary tumor, followed by implantation of Matrigel containing PBS or CDN into the resection cavity. ii, Summary of secondarytumor size d10 following the operation. C, i, BALB/c mice bearing day 12 4T1 tumors were randomized to receive surgery, followed by implantation ofMatrigel containingPBSor CDN into the resection cavity and followed for recurrence. Recurrence of theprimary tumor (ii) andoverall survival (iii).D, i,Assessment ofthe number of metastases per lung at euthanasia in mice treated as in C with subtotal or complete resection, followed by implantation of Matrigel containingPBS or CDN into the resection cavity. ii, Metastases per lung at euthanasia. BALB/c mice bearing day 5 4T1 tumors were randomized to receive surgery,followed by implantation of Matrigel containing PBS or CDN into the resection cavity and followed for recurrence. iii, Overall survival following early resection.NS, not significant; �, P < 0.05; �� , P < 0.01.
Personalized Surgical Immunotherapy
www.aacrjournals.org Cancer Res; 78(21) November 1, 2018 6313
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

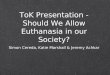
applied to evaluate the response of patient tumors to STINGligands, we acquired surgical samples from patients undergoingresection for HNSCC and treated them ex vivowith STING ligandsor PBS. Treatment with STING ligands consistently resulted instatistically significant increases in IFNa secretion from theexplant (Fig. 5A, ii; Supplementary Fig. S2). However, IFNb,TNFa, and IL10 secretion tended to be more patient-specific. Toevaluate the effect of treatment with STING ligands on immunecell recruitment to the tumor, we also evaluated chemokinesecretion from the explants. Although the tumor samples from4 of 5 patients significantly increased secretion of CCL3 followingtreatment with STING ligands, none of the patients significantlyincreased CXCL10 secretion (Fig. 5A, ii; Supplementary Fig. S2).We have previously demonstrated that increased expression ofCCL3 in tumors results in improved T-cell recruitment andimproved tumor control (21, 22), potentially linking the inflam-matory effects of STING ligands to T-cell–dependent tumorcontrol (Figs. 2 and 3). Because the patient samples includedboth HPVþ and HPV� HNSCC, and because our previous datademonstrate that HPV� HNSCC does not express STING (10),wewere also able to identify sampleswhere the response to STINGligands is dependent on the tumor stroma. To confirm this, westained matched tissue blocks from these tumors for expressionof STING (Fig. 5B). HPV� HNSCC patient CRI-2799 did notexpress STING in the cancer cells (Fig. 5B, i and ii). Therefore,in this tumor, the stromal expressing STINGmust be critical to theresponse to STING ligands. In contrast, the HPVþ HNSCC
expresses STING in both cancer cells and in the stroma(Fig. 5B, iv and v). To assess the mix of immune cells infiltratingthese tumors, we performed multiplex immunohistology forimmune markers. The multiplex images demonstrate a diverseimmune environment in these tumors, consistent with previousresults (Fig. 5B, iii and vi; ref. 23). The tumors exhibit not onlyextensive infiltrates of CD8 T cells, but also abundant FoxP3þ Tregulatory cells, CD163þ macrophages, and high levels of PDL1on cancer cells and stromal cells (Supplementary Fig. S3). TheHPV� HNSCC CRI-2799 had a decreased immune infiltratecompared with the HPVþ HNSCC CRI-2751, but further studiesare necessary todetermine the critical stromal elements that definethe cytokine response to STING ligands. These data demonstratethat patient tumor explants treated ex vivo with STING ligandsgenerate a rapid cytokine response that is dependent on thepatient-specific immune stroma. We propose that this novelapproach can be used to understand the variability of patientresponses to STING ligands, investigate the critical cells that drivethese responses, and identify therapies to improve local control.
To determine whether this explant assay could be used topersonalize therapy according to the tumor-specific response toSTING ligands, we tested the tumor explant assay on a panel ofmurine HNSCC. We included the aggressive MOC2 HNSCCtumor model that has been shown to be unresponsive to STINGligands, aswell as the immunogenicMOC1HNSCC tumormodelthat can be cured with the same treatment (9). MOC2 has adistinct profile of infiltrating immune cells compared withMOC1
CDNPBS
d0
d1
d2
d3
d4
d5
d7
1.02
mm
0
0.5
1.0
1.5
2.0
Wou
nd w
idth
(mm
)
(iii) Epithelial width(ii) Wound histology(i) Excisional wound repair
0
0.5
1.0
1.5
Forc
e (N
)
(ii) Incisional strength
NS
NS
- + CDN
- + CDN
C3H
Surgery + PBS
Surgery + CDN
(i) Incisional strength modelA
B
Tensitometry
3 mm
Figure 4.
STINGblade does not affect wound healing. A, i, C3Hmice received full thickness incisional wounds thatwere treatedwith Matrigel containing PBS or 25 mg CDNand closed. Following removal of wound clips, the micewere euthanized and the skin removed for tensitometry.ii, The force required to break thewoundwas calculated.Each symbol represents one animal. B, C3H micereceived full thickness excisional wounds using a 3-mmsterile dermal biopsy punch. The site was treated withMatrigel containing PBS or 25 mg CDN and allowed toclose without further treatment. i, Representativeimages of healing wounds. ii, Seven days followingexcision, the wound sites were harvested and analyzedby histology to identify the widest opening. iii, Thedistance between epithelia in CDN and control-treatedwounds. NS, not significant.
Baird et al.
Cancer Res; 78(21) November 1, 2018 Cancer Research6314
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

(9, 24), and because our therapy is dependent on the action ofSTING ligands on host cells, we proposed that the outcome oftumor therapy with STING ligands could be predicted by theresponse of the immune cells within the tumor. Treatment withSTING ligands resulted in rapid induction of TNFa and type I IFNin all HNSCC-related tumor explants (Fig. 6A; Supplementary Fig.S4). These results closely match the cytokine responses observedin tumors following direct injection in vivo (7). Notably, MOC1tumors exhibited responses thatmatched SCCVII andTC1,where-as MOC2 tumors uniquely resulted in IL10 secretion followingstimulation with STING ligands (Fig. 6A). Using the explantmodel in mice also allows us to evaluate the role of the cancercells versus the stroma in the response to STING ligands, by testingexplants grown inwild-typemice versus STING�/�mice. Explantsgrown in wild-type mice made a strong cytokine response CDA,but this was lost in STING�/� mice, indicating STING expressionin the stroma is key (Fig. 6B). ERAdP has been described as analternative target for CDA, which can generate responses inSTING�/� mice (25). We see no evidence of a response to CDAin STING�/�, indicating that ERAdP cannot substitute for STINGin this setting. To confirm this, we also treated explants withcGAMP, which does not activate ERAdP (25). We found thatcGAMP generated a similar response to CDA and was also
dependent on STING expression in the tumor stroma (Fig. 6B),suggesting that STING in noncancer cells is the sole sensorresponsible for the activity of cyclic dinucleotides in this model.To identify the principle-responsive cell population, we per-formed an unbiased assessment of the cytokine-producing cellsin the tumor. Tumor-infiltrating cells were stimulatedwith STINGligands in the presence of secretion inhibitors and surface stainedwith an immune cell panel and intracellularly stained for TNFa.We found that TNFa was being produced by a subpopulation oftumor-associated macrophages (CD45þCD11bþLy6C�Ly6G�F4/80þMHCIIþ cells) as well as tumor-infiltrating monocytic cells(CD45þCD11bþLy6CþLy6G�; Fig. 6C). T cells and Neutrophils(CD45þCD11bþLy6CþLy6Gþ) did not generate significantresponses, and the MOC1 and MOC2 models lacked significantpopulations of dendritic cells (DC1: CD45þLy6C�Ly6G�F4/80�
MHCIIþCD24þCD103�CD11bþ and DC2: CD45þLy6C�Ly6G�
F4/80�MHCIIþCD24þCD103þCD11b� cells), using the paneldescribed by Broz and colleagues (Supplementary Fig. S5; ref.18). In view of the divergent cytokine response of MOC2 and itsknown unresponsiveness to STING ligands, we evaluated whetherthe response to STINGblade was similarly divergent in MOC2tumors. As previously reported, with a similar tumor challenge,MOC2 grows much more aggressively than MOC1 (Fig. 6D).
(i) Explant assay design
Excisedtumor
CDNVehicle
Cytokine analysis
Tumor explants
(ii) Human HNSCC explant response
Comparative histology
IFNα IFNβ
CDA- +
TNFα IL10
20
15
10
5
0
2,000
1,500
1,000
500
400
300
200
100
300
200
100
0
CDA- + CDA- +
0
CDA- +
(i) CRI-2799 H&E
(iv) CRI-2751 H&E
CRI-2843
CRI-2799
CRI-2806
CRI-2805
CRI-2751
(ii) CRI-2799 STING
(v) CRI-2751 STING
(iii) CRI-2799 Immune
(vi) CRI-2751 Immune
Brown - STINGGreen - Nuclei
Blue - DAPICyan - CK
Red - PDL1Orange - CD163
Yellow - CD8Green - FoxP3
Purple - CD3
CXCL1010,000
8,000
6,000
0
CDA- +
CCL3
CDA- +
Cyt
okin
e (p
g/m
L)
4,000
2,000
2,000
1,500
1,000
500
0
A
B
Figure 5.
Using patient HNSCC tumor explant responses to STING ligands to identify the diversity of responses. A, i, Tumor material was obtained from HNSCCpatients scheduled for surgical resection. One- to 2-mm explants were placed in culture with media containing PBS vehicle or 25 mg/mL CDN. Twenty-fourhours later, the supernatants were analyzed for cytokines by multiplex bead assay. ii, Each box represents the mean of replicate measures and was given a coloraccording to the scale at right. Raw values and statistics are shown in Supplementary Fig. S1. B, Immunohistology for infiltrating immune cells in tumors frompatient CRI-2799 (i-iii) and patient CRI-2751 (iv–vi). Representative images of serial sections showing hematoxylin and eosin (H&E; i and iv) andimmunohistology for STING (brown; ii and v) with green nuclear counterstain and multiplex immunohistology for cytokeratin (CK, cyan), PDL1 (red), CD163(orange), CD3 (purple), CD8 (yellow), FoxP3 (green), and DAPI stain of nuclei (blue; iii and vi). Individual stains are shown in Supplementary Fig. S2.
Personalized Surgical Immunotherapy
www.aacrjournals.org Cancer Res; 78(21) November 1, 2018 6315
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

Following purposeful partial tumor resection and application ofSTING ligands inMatrigel, thehighly immunogenicMOC1tumorswere cured by STINGblade like SCCVII and TC1, though a signif-
icant proportionwere curedbypartial resection alone (Fig. 6Ei). Bycontrast, no MOC2-bearing mice were cured by STINGblade(Fig. 6Eii). Using the explant response to inform therapy, we
IFNγ
8,000
6,000
4,000
2,000 Cyt
okin
e (p
g/m
L)
IFNα IFNβ
0CDA - + - + - +
TNFα IL10
2,000
1,500
1,000
500
0CDA - + - +
Mouse HNSCC models explant cytokine response
Moc1
Moc2
TC1
SCCVII
0
50
100
0
PBSCDN
Per
cent
sur
viva
l
(ii) Moc2 survival
50Time (days)
100
aIL10RCDN+aIL10R
0
50
100
0
PBSCDN
Per
cent
sur
viva
l
(i) Moc1 survival
50Time (days)
100
Moc tumor differences
Moc1Moc2
0
10
15
0
Tum
or d
iam
eter
(mm
)
20Time (days)
6040
5
**** ****
NS
Stromal STING response
*
5,000
3,0002,0001,000
4,000
1,500
500
1,000
Cyt
okin
e (p
g/m
L)
CDAcGAMP
- + -- - +
IFNβ
TNFα
C57BL/6
STING-/-
C57BL/6
STING-/-
CDAcGAMP
- + -- - +
TNFα TNFα
Monocytic TAM
MH
CII
MH
CII
PB
SC
DA
CD
4+
CD
8+
Mon
ocyt
ic
TAM
Neu
troph
ils
0
5
10
15
20P
erce
nt T
NFα
+(ii) MOC1 tumors
PBSCDA
CD
4+
CD
8+
Mon
ocyt
ic
TAM
Neu
troph
ils
0
5
10
15
20
Per
cent
TN
Fα+
(iii) MOC2 tumors
PBSCDA
C
D E
A B
(i)
** **** NS *
Figure 6.
Using murine HNSCC tumor explant responses to STING ligands to personalize therapy. A, Tumors were harvested from mice and 1- to 2-mm explantsplaced in culture with media containing PBS vehicle or 25 mg/mL CDN. Twenty-four hours later, the supernatants were analyzed for cytokines by multiplexbead assay. Summary of cytokine responses from explants of MOC1, MOC2, and TC1 tumors grown in C57BL/6mice, and SCCVII tumors grown in C3Hmice. Each boxrepresents the mean of replicate measures and was given a color according to the scale at right. Raw values and statistics are shown in Supplementary Fig. S3.B, Tumor explants were prepared from MOC2 tumors grown in wild-type C57BL/6 mice or STING�/� mice and treated as per A with CDA or cGAMP, andanalyzed for TNFa and IFNb responses. Each box represents the mean of replicate measures and was given a color according to the scale at right. C, Single-cellsuspensions from established MOC1 and MOC2 tumors were stimulated in vitro with 25 mg CDA or PBS control in the presence of brefeldin A and intracellularlystained for TNFa in a major cell populations (i). Graphs show a summary of cell types expressing TNFa in MOC1 (ii) and MOC2 (iii) tumors following treatment withPBS orCDA.D,C57BL/6micewere challengedwithMOC1 orMOC2 tumors and followed for tumor growth.E, i,C57BL/6mice bearingMOC1 tumorswere randomizedto receive surgery, followedby implantation ofMatrigel containingPBS or CDN into the resection cavity. Graph shows overall survival. ii,C57BL/6mice bearingMOC2tumors were randomized to receive surgery, followed by implantation of Matrigel containing PBS, PBS þ anti-IL10R, CDN, or CDN þ anti-IL10R into the resectioncavity. Graph shows overall survival. NS, not significant; �, P < 0.05; �� , P < 0.01; ��� , P < 0.001; ���� , P < 0.0001.
Baird et al.
Cancer Res; 78(21) November 1, 2018 Cancer Research6316
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

evaluated whether IL10 production was responsible for the poorresponse of MOC2 tumors to STING ligands. MOC2 tumors inC57BL/6mice with subtotal resection plus local administration ofCDN alone or in combinationwith anti–IL10R-blocking antibodyincorporated into thebiomaterial. Additionof anti-IL10Rresults ina significant extension in survival andcureof tumors in aportionofthe mice (Fig. 6Eii). These data demonstrate that analysis of thecytokine response to tumor explants treated ex vivo identifiestumors with variable immune responses to STING ligands, andenables personalization of the immunotherapy-containing bio-material to induce tumor cure.
DiscussionIn this study, we demonstrated that in preclinical models of
HNSCC, the incorporation of STING ligands into a hydrogel thatis delivered into a subtotal resection cavity results in tumor cure.We show that this mechanism occurs through activation of hostSTING-expressing cells, not cancer cells, and requires induction oftype I IFN, resulting in CD8 T-cell–mediated control of residualdisease. Although the therapy is effective locally, it can alsoeliminate locoregional recurrence and impact, but not cure distantdisease. Furthermore, we developed a tumor explant model torapidly screen responses to STING ligands in tumors with diver-gent immune environments in both mice and in patients, andshow that the implanted biomaterial can be personalized accord-ing to the explant response to improve outcomes followingtherapy.
This approach has specific relevance to HNSCC because closeor positive resection margins are strongly associated with localtumor recurrence (26), and local recurrence occurs in approx-imately 30% of HNSCC patients receiving resection with cura-tive intent. In addition, tumor encroachment on or proximal tocritical structures, such as the carotid artery, limits the feasi-bility of a complete and curative resection in some patients.This is a clear area in which immunotherapy can be incorpo-rated to build upon surgical procedures to minimize localrecurrence, while potentially generating immune-mediatedcontrol of distant metastasis. In our model, therapy had arestricted locoregional action and did not affect distant metas-tases that were present before treatment started. However,because the final control of local tumors occurs via CD8 Tcells, it would be reasonable to combine this therapy withT-cell–targeted therapies such as checkpoint inhibitors toimprove distant control, as has proven effective in distantcontrol of immunogenic tumors treated with direct injectionof STING ligands (9). In addition, we have previously shownthat STING ligands synergize with radiotherapy to control localand distant tumors (7), which is commonly prescribed forHNSCC patients following surgery. Therefore, it is likely thatthe addition of STING ligands to the surgical site will synergizewell with current adjuvant therapies to improve control of bothlocal and distant tumor recurrence.
The biomaterial used in this study was Matrigel, which is notoptimized for sustained release, but instead undergoes the defaultrapid diffusion-based "burst" release of incorporated drug, fol-lowed by further low-level release on gradual degradation of thepolymer scaffold. In this setting, the primary purpose of theMatrigel is to localize the STING ligands to the resection cavityand prevent leakage before wound closure. An array of alternativebiomaterials can be considered for use in patients. Recent studies
demonstrated that an alginate scaffold incorporating anti-CD3,anti-CD28, and anti-CD137 microparticles along with NKG2DCAR-engineered T cells placed alongside pancreatic tumorsresulted in optimal tumor control when loaded with a mesopor-ous silica microparticle containing STING agonists (27). Thesedata indicate howbiomaterials can be furthermodified to includeadditional agents, and potentially personalized. There are awide variety of suitable biomaterial options, and further refine-ment could be used to develop formulations with controlledrelease properties. For example, a sustained release formulation ofSTING ligands significantly improved treatment of mice wheninjected into the same area where cancer cells had been injected 3days previously (28). Since completing these studies, a recentpublication has reported on a very similar model, using STINGligands incorporated into an extended release hydrogel in aperioperative setting (29). Distinct from our model, local admin-istration of innate adjuvants was able to control the progressionof lung metastases of 4T1-luciferase expressing luciferase (29),suggesting that either there are differences in the complete resec-tionmodel used in this study or the extended release formulationcontaining a 4 fold higher dose of STING ligands is critical forefficacy. Despite these data, cyclic dinucleotides may not beappropriate for longer-term release strategies, as they are subjectto rapid in vivo degradation by ubiquitous enzymes. Incorpo-ration of small-molecule STING agonists (30, 31) or alternativeinnate adjuvants (32) could further alter the properties of suchbiomaterials for improved tumor control.
HNSCCs are known to be immunosuppressive. In this study,we identified IL10 production to be a prominent component ofthe response to STING ligands in the MOC2 tumor. Althoughwe do not believe that IL10 is the sole immunosuppressivefactor operational in this tumor, IL10 production can beindicative of a distinct differentiation profile of tumor-infiltrat-ing macrophages (33–35). STING ligands cause IL10 produc-tion in MOC2 tumors, and this likely has a direct impact on theimmune cells present in that tumor's microenvironment. IL10can suppress inflammation in a number of cell types, includingantigen-presenting cells, which respond to IL10 by downregu-lating antigen processing and presentation (36, 37), macro-phages, which increase alternative macrophage differentiation(38), and T cells, where costimulation is suppressed (reviewedin ref. 16). Because IL10 shortens the duration of inflammatoryresponses (39) and suppresses antitumor adaptive immuneresponses during tumor progression (40), it is plausible thatIL10 diminishes many of the positive benefits of STINGblade.Our findings are consistent with previous studies demonstrat-ing that blocking IL10 responses results in more effectiveimmune-mediated control of tumors (41–44). Thus, althoughIL10 may not be the only suppressive factor expressed in MOC2tumors, it is a strong target to redirect the inflammatoryresponse to STINGblade.
In summary, local failure is a critical problem in HPV�
HNSCC and other immunosuppressive solid tumors. The localdelivery of STING agonists, with or without systemic immu-notherapy, may enhance the efficacy of surgical resection byminimizing local recurrence, and further serving as a platformto generate systemic immunity to treat or control metastaticdisease. We believe that the tumor explant assay is a rapidmethod that can be used ex vivo to predict the response totreatment with STING ligands in vivo based on the uniqueenvironment of patient tumors.
Personalized Surgical Immunotherapy
www.aacrjournals.org Cancer Res; 78(21) November 1, 2018 6317
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

Disclosure of Potential Conflicts of InterestM.J. Gough reports receiving commercial research grant from Bristol Myers
Squibb. No potential conflicts of interest were disclosed by the other authors.
Authors' ContributionsConception and design: J.R. Baird, T.C. Blair, M.R. Crittenden, M.J. GoughDevelopment of methodology: J.R. Baird, D. Friedman, Z. Sun, T.D. de Gruijl,R. van de Ven, R.S. Leidner, M.R. CrittendenAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): J.R. Baird, V. Troesch, D. Friedman, S. Bambina,G. Kramer, T. Medler, Y. Wu, R.S. LeidnerAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): J.R. Baird, V. Troesch, D. Friedman, G. Kramer, Y.Wu,M.R. Crittenden, M.J. GoughWriting, review, and/or revision of the manuscript: J.R. Baird, R.B. Bell,T.C. Blair, Y. Wu, T.D. de Gruijl, R.S. Leidner, M.R. Crittenden, M.J. Gough
Administrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): J.R. Baird, Y. Wu, M.J. GoughStudy supervision: Y. Wu, M.R. Crittenden, M.J. Gough
AcknowledgmentsThis work was supported by a postdoctoral fellowship from the American
Cancer Society (J.R. Baird) and a research grant from the Oral MaxillofacialSurgery Foundation (M.J. Gough, R.B. Bell, and J.R. Baird).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
ReceivedMay 30, 2018; revised August 10, 2018; accepted September 4, 2018;published first September 17, 2018.
References1. Bernier J, Cooper JS, Pajak TF, vanGlabbekeM, Bourhis J, Forastiere A, et al.
Defining risk levels in locally advanced head and neck cancers: a compar-ative analysis of concurrent postoperative radiation plus chemotherapytrials of the EORTC (#22931) and RTOG (#9501). Head Neck2005;27:843–50.
2. Jones AS, Bin Hanafi Z, Nadapalan V, Roland NJ, Kinsella A, Helliwell TR.Do positive resection margins after ablative surgery for head and neckcancer adversely affect prognosis? A study of 352 patients with recurrentcarcinoma following radiotherapy treated by salvage surgery. Br J Cancer1996;74:128–32.
3. Gough MJ, Crittenden MR, Sarff M, Pang P, Seung SK, Vetto JT, et al.Adjuvant therapy with agonistic antibodies to CD134 (OX40) increaseslocal control after surgical or radiation therapy of cancer in mice.J Immunother 2010;33:798–809.
4. Koster BD, van den Hout MFCM, Sluijter BJR, Molenkamp BG, VuylstekeRJCLM, Baars A, et al. Local adjuvant treatmentwith low-dose CpG-B offersdurable protection against disease recurrence in clinical stage I-II melano-ma: data from two randomized phase II trials. Clin Cancer Res 2017;23:5679–86.
5. Hsueh EC, Gupta RK, Yee R, Leopoldo ZC, Qi K, Morton DL. Doesendogenous immune response determine the outcome of surgical therapyfor metastatic melanoma? Ann Surg Oncol 2000;7:232–8.
6. Liu J, Blake SJ, YongMC,Harjunp€a€aH,Ngiow SF, Takeda K, et al. Improvedefficacy of neoadjuvant compared to adjuvant immunotherapy to eradicatemetastatic disease. Cancer Discov 2016;6:1382–99.
7. Baird JR, Friedman D, Cottam B, Dubensky TW Jr, Kanne DB, BambinaS, et al. Radiotherapy combined with novel STING-targeting oligonu-cleotides results in regression of established tumors. Cancer Res2016;76:50–61.
8. Corrales L, Glickman LH,McWhirter SM, KanneDB, Sivick KE, KatibahGE,et al. Direct activation of STING in the tumor microenvironment leads topotent and systemic tumor regression and immunity. Cell Rep 2015;11:1018–30.
9. Moore E, Clavijo PE, Davis R, CashH, VanWaes C, Kim Y, et al. EstablishedT cell-inflamed tumors rejected after adaptive resistance was reversed bycombination STING activation and PD-1 pathway blockade. CancerImmunol Res 2016;4:1061–71.
10. Baird JR, Feng Z, Xiao HD, Friedman D, Cottam B, Fox BA, et al. STINGexpression and response to treatment with STING ligands in premalignantand malignant disease. PLoS One 2017;12:e0187532.
11. WangC, SunW, Ye Y,HuQ, BombaHN,GuZ. In situ activation of plateletswith checkpoint inhibitors for post-surgical cancer immunotherapy.Nat Biomed Eng 2017;1:0011.
12. Lin K-Y, Guarnieri FG, Staveley-O'Carroll KF, Levitsky HI, August JT,Pardoll DM, et al. Treatment of established tumors with a novel vaccinethat enhances major histocompatibility class II presentation of tumorantigen. Cancer Res 1996;56:21–6.
13. Aslakson CJ,Miller FR. Selective events in themetastatic process defined byanalysis of the sequential dissemination of subpopulations of a mousemammary tumor. Cancer Res 1992;52:1399–405.
14. JuddNP,Winkler AE,Murillo-SaucaO, Brotman JJ, Law JH, Lewis JS Jr, et al.ERK1/2 regulation of CD44 modulates oral cancer aggressiveness. CancerRes 2012;72:365–74.
15. Crittenden MR, Savage T, Cottam B, Bahjat KS, Redmond WL, Bambina S,et al. The peripheral myeloid expansion driven by murine cancer progres-sion is reversed by radiation therapy of the tumor. PLoS One 2013;8:e69527.
16. Taylor A, Verhagen J, Blaser K, Akdis M, Akdis CA. Mechanisms of immunesuppression by interleukin-10 and transforming growth factor-beta: therole of T regulatory cells. Immunology 2006;117:433–42.
17. Gough MJ, Ruby CE, Redmond WL, Dhungel B, Brown A, Weinberg AD.OX40 agonist therapy enhances CD8 infiltration and decreases immunesuppression in the tumor. Cancer Res 2008;68:5206–15.
18. Broz ML, Binnewies M, Boldajipour B, Nelson AE, Pollack JL, Erle DJ,et al. Dissecting the tumor myeloid compartment reveals rare activatingantigen-presenting cells critical for T cell immunity. Cancer Cell2014;26:638–52.
19. Downey CM, Aghaei M, Schwendener RA, Jirik FR. DMXAA causes tumorsite-specific vascular disruption in murine non-small cell lung cancer, andlike the endogenous non-canonical cyclic dinucleotide STING agonist,2030-cGAMP, induces M2 macrophage repolarization. PLoS One 2014;9:e99988.
20. Egenolf DD, Rafferty P, Brosnan K, Walker M, Jordan J, Makropoulos D,et al. Development of a murine model of lymph node metastases suitablefor immunotoxicity studies. J Pharmacol Toxicol Methods 2011;63:236–49.
21. GoughM, CrittendenM, ThanarajasingamU, Sanchez-Perez L, ThompsonJ, Jevremovic D, et al. Gene therapy tomanipulate effector T cell traffickingto tumors for immunotherapy. J Immunol 2005;174:5766–73.
22. Crittenden M, Gough M, Harrington K, Olivier K, Thompson J, Vile RG.Expression of inflammatory chemokines combined with local tumordestruction enhances tumor regression and long-term immunity. CancerRes 2003;63:5505–12.
23. Feng Z, Bethmann D, Kappler M, Ballesteros-Merino C, Eckert A, Bell RB,et al.Multiparametric immuneprofiling inHPV-oral squamous cell cancer.JCI Insight 2017;2.
24. Cash H, Shah S, Moore E, Caruso A, Uppaluri R, Van Waes C, et al. mTORand MEK1/2 inhibition differentially modulate tumor growth and theimmune microenvironment in syngeneic models of oral cavity cancer.Oncotarget 2015;6:36400–17.
25. Xia P, Wang S, Xiong Z, Zhu X, Ye B, Du Y, et al. The ERmembrane adaptorERAdP senses the bacterial second messenger c-di-AMP and initiates anti-bacterial immunity. Nat Immunol 2018;19:141–50.
26. Alicandri-Ciufelli M, Bonali M, Piccinini A, Marra L, Ghidini A, CunsoloEM, et al. Surgical margins in head and neck squamous cell carcinoma:what is `close'? Eur Arch Otorhinolaryngol 2013;270:2603–9.
27. Smith TT, Moffett HF, Stephan SB, Opel CF, Dumigan AG, Jiang X,et al. Biopolymers codelivering engineered T cells and STING agonistscan eliminate heterogeneous tumors. J Clin Invest 2017;127:2176–91.
Baird et al.
Cancer Res; 78(21) November 1, 2018 Cancer Research6318
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

28. Leach DG, Dharmaraj N, Piotrowski SL, Lopez-Silva TL, Lei YL, Sikora AG,et al. STINGel: controlled release of a cyclic dinucleotide for enhancedcancer immunotherapy. Biomaterials 2018;163:67–75.
29. Park CG, Hartl CA, Schmid D, Carmona EM, Kim HJ, Goldberg MS.Extended release of perioperative immunotherapy prevents tumor recur-rence and eliminates metastases. Sci Translat Med 2018;10.
30. Sali TM, Pryke KM, Abraham J, Liu A, Archer I, Broeckel R, et al. Charac-terization of a novel human-specific STING agonist that elicits antiviralactivity against emerging alphaviruses. PLoS Pathog 2015;11:e1005324.
31. Cavlar T, Deimling T, Ablasser A, Hopfner KP, Hornung V. Species-specificdetection of the antiviral small-molecule compound CMA by STING.EMBO J 2013;32:1440–50.
32. Baird JR, Monjazeb AM, Shah O, McGee H, Murphy WJ, Crittenden MR,et al. Stimulating innate immunity to enhance radiation therapy-inducedtumor control. Int J Radiat Oncol Biol Phys 2017;99:362–73.
33. Saccani A, Schioppa T, Porta C, Biswas SK, Nebuloni M, Vago L, et al. p50nuclear factor-kappaB overexpression in tumor-associated macrophagesinhibits M1 inflammatory responses and antitumor resistance. Cancer Res2006;66:11432–40.
34. Fraser DA, Arora M, Bohlson SS, Lozano E, Tenner AJ. Generation ofinhibitory NFkappaB complexes and phosphorylated cAMP responseelement-binding protein correlates with the anti-inflammatory activity ofcomplement protein C1q in human monocytes. J Biol Chem 2007;282:7360–7.
35. Crittenden MR, Cottam B, Savage T, Nguyen C, Newell P, Gough MJ.Expression of NF-kappaB p50 in tumor stroma limits the control of tumorsby radiation therapy. PLoS One 2012;7:e39295.
36. de Waal Malefyt R, Abrams J, Bennett B, Figdor CG, de Vries JE. Interleukin10(IL-10) inhibits cytokine synthesis by human monocytes: an autoregu-latory role of IL-10 produced bymonocytes. J ExpMed1991;174:1209–20.
37. de Waal Malefyt R, Haanen J, Spits H, Roncarolo MG, te Velde A,Figdor C, et al. Interleukin 10 (IL-10) and viral IL-10 strongly reduceantigen-specific human T cell proliferation by diminishing the antigen-presenting capacity of monocytes via downregulation of class II majorhistocompatibility complex expression. J Exp Med 1991;174:915–24.
38. KuwataH,Watanabe Y,MiyoshiH, YamamotoM,Kaisho T, TakedaK, et al.IL-10-inducible Bcl-3 negatively regulates LPS-induced TNF-alpha produc-tion in macrophages. Blood 2003;102:4123–9.
39. Kuhn R, L€ohler J, Rennick D, Rajewsky K, M€uller W. Interleukin-10-deficient mice develop chronic enterocolitis. Cell 1993;75:263–74.
40. Halak BK HC, Maguire Jr., Lattime EC. Tumor-induced interleukin-10inhibits type 1 immune responses directed at a tumor antigen as well asa non-tumor antigen present at the tumor site. Cancer Res 1999;59:911–7.
41. Ruffell B, Chang-StrachanD, Chan V, Rosenbusch A, Ho CM, Pryer N, et al.Macrophage IL-10 blocks CD8þ T cell-dependent responses to chemo-therapy by suppressing IL-12 expression in intratumoral dendritic cells.Cancer Cell 2014;26:623–37.
42. Vicari AP, Chiodoni C, Vaure C, A€�t-Yahia S, Dercamp C, Matsos F, et al.Reversal of tumor-induced dendritic cell paralysis by CpG immunostimu-latory oligonucleotide and anti-interleukin 10 receptor antibody. J ExpMed 2002;196:541–9.
43. Guiducci C, Vicari AP, Sangaletti S, Trinchieri G, ColomboMP. Redirectingin vivo elicited tumor infiltrating macrophages and dendritic cells towardstumor rejection. Cancer Res 2005;65:3437–46.
44. Lu H, Wagner WM, Gad E, Yang Y, Duan H, Amon LM, et al. Treatmentfailure of a TLR-7 agonist occurs due to self-regulation of acute inflam-mation and can be overcome by IL-10 blockade. J Immunol2010;184:5360–7.
www.aacrjournals.org Cancer Res; 78(21) November 1, 2018 6319
Personalized Surgical Immunotherapy
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652

2018;78:6308-6319. Published OnlineFirst September 17, 2018.Cancer Res Jason R. Baird, R. Bryan Bell, Victoria Troesch, et al. CarcinomaImmunosurgical Therapy for Head and Neck Squamous Cell Evaluation of Explant Responses to STING Ligands: Personalized
Updated version
10.1158/0008-5472.CAN-18-1652doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2018/09/15/0008-5472.CAN-18-1652.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/78/21/6308.full#ref-list-1
This article cites 42 articles, 20 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/78/21/6308To request permission to re-use all or part of this article, use this link
on March 28, 2020. © 2018 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 17, 2018; DOI: 10.1158/0008-5472.CAN-18-1652