Embed Size (px)
Citation preview

Evaluation of ABO blood group as a prognosticmarker in renal cell carcinoma (RCC)Michela de Martino, Matthias Waldert, Andrea Haitel*, Georg Schatzl,Shahrokh F. Shariat and Tobias KlatteDepartments of Urology and *Clinical Pathology, Medical University of Vienna, Vienna, Austria
Objective• To evaluate ABO blood group as a prognostic marker in
patients with renal cell carcinoma (RCC).
Patients and Methods• This retrospective study included 556 consecutive patients
who underwent surgery for RCC at a single institution.• The associations of ABO blood group with clinical and
pathological variables were assessed using Kruskal–Wallisand chi-squared tests.
• The impact on overall survival (OS) and RCC-specificsurvival (RCC-SS) was analysed using univariable andmultivariable Cox proportional hazards regression models.
Results• Blood group O was associated with the absence of lymph
node metastases (P = 0.034) and the presence of bilateralRCC (P = 0.017).
• No associations with age, gender, body mass index, Charlsoncomorbidity index, T stage, M stage, grade and histologicalsubtype were observed.
• In univariable and multivariable survival analysis,ABO blood group was not associated with OS andRCC-SS.
Conclusions• In the present study, ABO blood group was not linked with
RCC prognosis.• Blood group O may be associated with the absence of
lymph node metastases and the presence of bilateralRCC.
• External validation in larger cohorts is necessary.
KeywordsABO, blood group, blood type, prognosis
IntroductionRenal cell carcinoma is the third leading tumour type of thegenitourinary tract with >60 000 new cases being diagnosed inthe USA annually [1]. Tobacco use, obesity, and arterialhypertension are modifiable risk factors for the disease [2],and a familial history in a first-degree relative increases thelifetime risk 1.6-fold [3]. RCC is also associated with severalgenetic syndromes such as von Hippel–Lindau disease,hereditary papillary RCC, and Birt–Hogg–Dubé’s syndrome[4]. Surgery is the mainstay of therapy for RCC, and TNMstage and grade are its most established prognostic factors[5–8].
ABO blood group is a potential inherited marker of cancersusceptibility and progression. Studies show that blood groupis associated with the risk of various solid malignancies[9–11], and may also serve as a prognostic marker [12,13]. InRCC, a study conducted several decades ago suggested arelationship between blood group antigens and the risk ofdeveloping the disease [14], whereas other studies havereported no association [15–17]. Kaffenberger et al. [18]
recently showed, in a cohort of 900 patients with RCC withoutdistant metastases, that blood group O was associated withbetter overall survival (OS). Thus, data suggest a possible roleof ABO blood group in the progression of RCC. The aim ofthe present study was to verify this blood group status as aprognostic marker.
Materials and MethodsStudy Design
The cohort of the present retrospective study consisted of556 consecutive white patients, who underwent radical orpartial nephrectomy for RCC of all subtypes and all stages atour institution between January 2002 and December 2012.Patients with familial RCC and hereditary RCC wereexcluded.
Patient data were collected prospectively in the institutionalkidney cancer database. The database was analysedretrospectively after obtaining institutional review boardapproval (protocol registration number 1958/2012). Clinical,
BJU Int 2014; 113: E62–E66© 2013 The Authors
BJU International © 2013 BJU International | doi:10.1111/bju.12436wileyonlinelibrary.com Published by John Wiley & Sons Ltd. www.bjui.org

pathological, laboratory and follow-up information wasgathered. Clinical data included ABO blood group, age,gender, self-reported history of smoking and body mass index(BMI). Comorbidity status was graded using the Charlsoncomorbidity index (CCI). Pathological data comprisedhistological subtype, according to the WHO classification [19],TNM stage, according to the 2010 criteria [20], and Fuhrmangrade [21]. All surgical specimens were examined by an experturological pathologist (A.H.). N stage was assigned fromradiological and pathological data. Patients with clinicallypositive nodes, defined as the presence of at least one node>10 mm in size in the retroperitoneal lymphatic area atpreoperative imaging, underwent a node dissection. In patientswith negative nodes on imaging, the node dissection wasperformed at the surgeon’s discretion. The positive nodesreported in the present study were all confirmedpathologically. No adjuvant therapy was administered.Postoperative surveillance was performed according toestablished guidelines [5].
Statistical Analysis
The continuous variables age and BMI were found to benon-normally distributed (Kolmogorov–Smirnov P > 0.3).These variables are therefore presented as median values withinterquartile ranges (IQRs).
Because of the low numbers of patients in several stratums,ABO blood group was evaluated as O and non-O, aspreviously suggested [18]. Univariable associations withclinical and pathological factors (age, gender, BMI, smokinghistory, CCI, TNM stage, grade, bilaterality and subtype) wereanalysed using Kruskal–Wallis and chi-squared tests, asappropriate. Significant univariable predictor variables weretested in multivariable logistic regression models.
The Kaplan–Meier product limit method was used to estimatefunctions for OS and RCC-specific survival (RCC-SS).Follow-up information was available for 442 of the 556 RCCpatients (79.5%). The survival times were calculated from thedate of surgery to the date of last follow-up, death or deathfrom RCC, respectively. Differences in Kaplan–Meier curveswere assessed using log-rank tests. Univariable andmultivariable Cox proportional hazards regression modelswere used to evaluate the relationship of OS and RCC-SS withABO blood group and clinical and pathological variables. Toreduce the risk of over-fitting in multivariable Cox models,only factors that were significantly (P < 0.05) associated withsurvival in univariable analysis were included for multivariablemodelling with ABO blood group. Multivariable Cox modelswere bootstrap-corrected to account for dichotomization bias(200 resamples). All statistical testing was two-sided and a Pvalue <0.05 was considered to indicate statistical significance.The statistical package STATA 11.2 (Stata Corp., College Station,TX, USA) was used for all analyses.
ResultsAssociation with Clinical and Pathological Factors
Results are shown in Table 1. Blood group O was associatedwith a significantly lower risk of lymph node metastases (1.0%vs 4.0%, P = 0.034). Of the 16 patients with positive nodes, 14(87.5%) had a non-O blood group. In multivariable logisticregression analysis, non-O blood group (odds ratio [OR] 5.79,95% CI 1.22–27.51, P = 0.027), M stage (OR 5.29, 95% CI1.64–17.12, P = 0.005), and grade (hazard ratio [HR] 22.32,95% CI 2.69–185.42, P = 0.004) were independent predictorsof lymph node metastases.
Furthermore, blood group O increased the risk of bilateralRCC (OR 2.45, 95% CI 1.15–5.24, P = 0.017). Of 29 (58.6%)patients with bilateral RCC, 17 had blood group O, comparedwith 193 of 527 (36.6%) patients with unilateral disease. Inmultivariable analysis, blood group O was an independentpredictor of bilateral disease (OR 0.42, 95% CI 0.19–0.87, P =0.023), while age, gender, T stage, N stage, M stage and gradewere not.
No associations of ABO blood group with age, gender, BMI,smoking history, CCI, T stage, M stage, grade or subtype wereobserved (Table 1).
Association with Survival
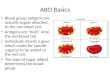
The median (IQR) follow-up was 39 (45) months. There were93 overall deaths, of which 61 (66%) were attributable toRCC. The 5-year OS and RCC-SS rates (±SE) were 75 (±3) %and 83 (±2) %, respectively, with no difference betweenpatients with blood group O and non-O (P = 0.33 andP = 0.99, respectively). Similarly, if blood groups wereanalysed unstratified as O, A, B, and AB, no differences in theKaplan–Meier functions were seen (every P value >0.4; Fig. 1).Similar results were obtained when the cohort was stratifiedinto non-metastatic (P = 0.14 and P = 0.75) and metastaticdisease (P = 0.91 and P = 0.91). In non-metastatic disease,there was also no association with recurrence-free survival(P = 0.81). In univariable and multivariable Cox modelspredicting OS and RCC-SS, ABO blood group was not asignificant prognostic factor (Table 2).
DiscussionIn the present study, we analysed the association of ABOblood group with clinicopathological factors and prognosis ofpatients with RCC. Blood group O was associated with theabsence of lymph node metastases and the presence ofbilateral RCC, but was not linked to survival.
The primary goal of our study was to validate ABO bloodgroup as a prognostic factor. Recently, Kaffenberger et al. [18]found in a cohort of 900 patients without distant metastasesthat blood group O was associated with improved OS. The
ABO blood group as prognostic marker in RCC
© 2013 The AuthorsBJU International © 2013 BJU International E63

3-year OS rates were 75% for patients with blood group O and68% for those with blood group non-O. In the multivariableanalysis, patients with blood group non-O had a 1.68-foldgreater risk of death from all causes. In addition, a
nonsignificant trend (P = 0.065) was observed for RCC-SS. Inthe present study, we could not demonstrate a survivaldifference between patients with blood group O and non-O.There are several possible explanations for the discrepancy
Table 1 Associations of ABO blood group with clinical and pathological variables in 556 patientswith RCC.
Variable All patients,N = 556
Blood group P
O, n = 210 Non-O, n = 346
Median (IQR) age, years 64 (55–72) 63 (56–70) 65 (54–73) 0.47Male, n (%) 367 (49.2) 140 (66.7) 227 (65.6) 0.80Median (IQR) BMI 27.0 (24.1–30.1) 27.1 (24.2–30.4) 26.9 (23.9–29.8) 0.32Pack years, n (%) 0.77
0 358 (64.4) 139 (66.2) 219 (63.3)1–40 108 (19.4) 38 (18.1) 70 (20.2)>40 90 (16.2) 33 (15.7) 57 (16.5)
CCI >1, n (%) 239 (43.0) 85 (40.5) 154 (44.5) 0.35pT stage, n (%) 0.69
T1–2 309 (55.6) 119 (56.7) 190 (54.9)T3–4 247 (44.4) 91 (43.3) 156 (45.1)
pN stage, n (%) 0.034pNx/N0 540 (97.1) 208 (99.0) 332 (96.0)pN+ 16 (2.9) 2 (1.0) 14 (4.0)
M stage, n (%) 0.65M0 484 (87.1) 181 (86.2) 303 (87.6)M1 72 (12.9) 29 (13.8) 43 (12.4)
Fuhrman grade, n (%) 0.741–2 399 (71.8) 149 (71.0) 250 (72.3)3–4 157 (28.2) 61 (29.0) 96 (27.7)
Laterality, n (%) 0.017Unilateral 527 (94.8) 193 (91.9) 334 (96.5)Bilateral 29 (5.2) 17 (8.1) 12 (3.5)
Subtype, n (%) 0.48Clear-cell 394 (70.9) 154 (73.3) 240 (69.4)Papillary 107 (19.2) 35 (16.7) 72 (20.8)Chromophobe 55 (9.9) 21 (10.0) 34 (9.8)
Blood group O was associated with the absence of lymph node metastases and the presence of bilateral RCC.
0.0
0.2
0.4
0.6
0.8
1.0
0 12
OABABNon-O
Numbers at risk
A B
134148
6025
233
106112
4722
181
66642915
108
5340141367
77913820
149
24Months from surgery
p = n.s.
Prob
abili
ty o
f ove
rall
surv
ival
36 48 600.0
0.2
0.4
0.6
0.8
1.0
0 12 24Months from surgery
p = n.s.Prob
abili
ty o
f RCC
-spe
cific
surv
ival
36 48 60
OABABNon-O
Numbers at risk134148
6025
233
106112
4722
181
66642915
108
5340141367
77913820
149
Fig. 1 Kaplan–Meier curves for (A), OS and
(B), RCC-SS according to ABO blood group.
There was no significant difference for any
comparison. Non-O blood groups are also
summarized (dashed curve). The numbers of
patients at risk are indicated.
de Martino et al.
© 2013 The AuthorsE64 BJU International © 2013 BJU International

between the two studies. First, the inclusion criteria differed.We included patients of all stages, whereas Kaffenberger et al.[18] excluded patients with distant metastases. This differencein inclusion criteria, however, should have been balanced withmultivariable modelling. Second, the distribution of bloodgroups differs among countries and races and thus among theinstitutions, which subsequently affects statistical power.Finally, a significant association may have been blurred by thelower number of patients (n = 556) and the relatively lownumber of events (n = 93), so that the present study may havebeen underpowered to detect a significant difference. The βerror may have been a limitation of the present study, i.e. thatthe null hypothesis (no survival difference) is false, but is notrejected; however, it is also possible that a significantdifference would not have been detected with more patientsand events. To the best of our knowledge, no other dataregarding the prognostic impact of ABO blood group in RCCare available. Further studies are necessary.
Our data suggest that blood group O is associated with alower risk of lymph node metastases. As the number ofpatients with positive nodes was small (n = 16) and themajority of these patients presented with concomitantdistant metastases, this did not translate into a survivaldifference in either univariable or multivariable analyses.Data suggest that different routes of metastatic spread(lymphatic vs haematogenous spread) are the result ofunique biological propensities [22]. One could thushypothesize that blood group O may be protective withregard to lymphatic, but not haematogenous spread. Ourfinding is in contrast to the study by Kaffenberger et al. [18],who reported no association with lymph node involvement.This may, in part, be attributed to selection bias, as theseauthors excluded patients with distant metastasis. We didnot exclude patients with distant metastases; these patientsaccounted for the majority of those with metastatic lymph
nodes. The results of the present study further suggest thatblood group O is associated with bilateral RCC. To thebest of our knowledge, this is the first study showing thisrelationship. Reflecting the overall low incidence of positivenodes and bilateral disease, our data are derived from a smallnumber of patients. The present study generates hypotheses,and external validation in larger datasets is necessary.
The mechanisms through which blood group may influencecancer risk and progression are largely unknown. The ABOgene is located on chromosome 9q34 and is encoding forglycosyl-transferases, which catalyse the transfer of sugars tothe H antigen to form the blood group antigen [23]. The Oallele encodes a non-functional glycosyl-transferase and the Hantigen, which leaves the H antigen unaltered. ABO bloodgroup antigens are expressed on red blood cells and severalother normal and tumour tissues, including the kidney andseveral RCC cell lines [24,25]. Blood group antigens maycontribute by modifying cell adhesion, membrane signalling,and immune surveillance, which may in turn affect cancerdevelopment and progression [26]. These processes may inpart be influenced by TNF-α, as polymorphisms at the ABOgene locus are linked with TNF-α serum levels [27].
The best data on the impact of ABO blood group on cancerrisk and survival come from studies on pancreatic cancer. Twolarge, independent, prospective cohort studies showed that therisk of pancreatic cancer is increased 1.32–1.72-fold if anon-O blood group is present [11]. Moreover, it has beenshown that a non-O blood group decreases the risk of skincancer [28] and that the B antigen increases the incidence ofovarian cancer [29], while other studies have not shown anassociation of blood group with cancer risk [16,30]. A fewstudies have investigated the role of blood group as aprognostic marker in malignancies other than RCC, withvarying results [12,13,18,30].
Table 2 Univariable and bootstrap-corrected multivariable Cox models predicting OS and RCC-SS.
Variable OS RCC-SS
Univariable Multivariable Univariable Multivariable
HR 95% CI P HR 95% CI P HR 95% CI P HR 95% CI P
Age >65 years 1.88 1.24–2.85 0.003 2.33 1.50–3.60 <0.001 1.64 0.98–2.73 0.06Male vs female 1.25 0.80–1.95 0.33 1.25 0.72–2.17 0.43BMI 0.99 0.95–1.03 0.71 1.02 0.98–1.07 0.33CCI >1 1.58 1.05–2.38 0.028 1.16 0.76–1.78 0.49 1.57 0.95–2.61 0.08T3–4 vs T1- 2.86 1.86–4.39 <0.001 1.63 0.99–2.66 0.052 7.42 3.76–14.63 <0.001 3.08 1.44–6.60 0.004N+ vs Nx/0 9.23 4.88–17.46 <0.001 4.04 1.97–8.29 <0.001 14.95 7.69–29.07 <0.001 3.63 1.76–7.46 <0.001M1 vs M0 8.11 5.30–12.39 <0.001 5.99 3.70–9.70 <0.001 18.83 10.96–32.37 <0.001 10.20 5.53–18.82 <0.001Grade 3/4 vs 1/2 3.05 2.02–4.60 <0.001 1.85 1.16–2.96 0.010 5.25 3.09–8.95 <0.001 2.23 1.21–4.10 0.010Non-clear-cell vs clear-cell 0.96 0.61–1.50 0.84 0.75 0.41–1.36 0.34Bilateral vs unilateral 0.88 0.41–1.91 0.75 0.81 0.29–2.24 0.69Blood group non-O vs O 0.82 0.54–1.23 0.33 0.72 0.48–1.10 0.13 1.00 0.60–1.67 0.99 0.86 0.51–1.45 0.56
In all analyses, ABO blood group was not an independent prognostic factor.
ABO blood group as prognostic marker in RCC
© 2013 The AuthorsBJU International © 2013 BJU International E65

The present study has several limitations. Its design wasretrospective and we analysed a relatively small cohort ofpatients with a short follow-up. Some hypotheses, e.g. thatblood group O is associated with the absence of lymph nodemetastases and the presence of bilateral RCC, are generatedfrom sub-analyses of small cohorts and should be confirmedwith larger datasets. The study did not confirm the previouslyreported association of ABO blood group with OS [18], butour analysis may have been underpowered to detect asignificant difference. Since the study population and inclusioncriteria differed considerably, the two studies should beinterpreted as complementary, not oppositional. We suggestthat there is a different impact of ABO blood group onsurvival, although our conclusions are limited.
In conclusion, the present study showed ABO blood groupwas not associated with RCC prognosis. Blood group O was,however, associated with the absence of lymph nodemetastasis and the presence of bilateral RCC. Externalvalidation of these findings on larger well-defined cohorts isnecessary.
Conflict of InterestNone declared.
References1 Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J
Clin 2012; 62: 10–292 Navai N, Wood CG. Environmental and modifiable risk factors in renal
cell carcinoma. Urol Oncol 2012; 30: 220–43 Schlehofer B, Pommer W, Mellemgaard A et al. International
renal-cell-cancer study. VI. the role of medical and family history. Int JCancer 1996; 66: 723–6
4 Klatte T, Pantuck AJ. Molecular biology of renal cortical tumors. UrolClin North Am 2008; 35: 573–80
5 Ljungberg B, Cowan NC, Hanbury DC et al. EAU guidelines on renalcell carcinoma: the 2010 update. Eur Urol 2010; 58: 398–406
6 Bianchi M, Becker A, Hansen J et al. Conditional survival afternephrectomy for renal cell carcinoma (RCC): changes in future survivalprobability over time. BJU Int 2013; 111: E283–9
7 Bolton DM. Trends in the surgical management of localized renal masses.BJU Int 2013; 111: 1182–3
8 de Martino M, Klatte T, Seemann C et al. Validation of serum C-reactiveprotein (CRP) as an independent prognostic factor for disease-freesurvival in patients with localised renal cell carcinoma (RCC). BJU Int2013; 111: E348–53
9 Poole EM, Gates MA, High BA et al. ABO blood group and risk ofepithelial ovarian cancer within the Ovarian Cancer AssociationConsortium. Cancer Causes Control 2012; 23: 1805–10
10 Wang Z, Liu L, Ji J et al. ABO Blood Group System and Gastric Cancer: aCase-Control Study and Meta-Analysis. Int J Mol Sci 2012; 13: 13308–21
11 Wolpin BM, Chan AT, Hartge P et al. ABO blood group and the risk ofpancreatic cancer. J Natl Cancer Inst 2009; 101: 424–31
12 Costantini M, Fassio T, Canobbio L, Landucci M, Resasco M, BoccardoF. Role of blood groups as prognostic factors in primary breast cancer.Oncology 1990; 47: 308–12
13 Engin H, Bilir C, Ustun H, Gokmen A. ABO blood group and risk ofpancreatic cancer in a Turkish population in Western Blacksea region.Asian Pac J Cancer Prev 2012; 13: 131–3
14 Desai M, Brown HE. ABO blood group in relation to hypernephroma.Urology 1976; 8: 596–7
15 Schneider W, Dick W, Brockmüller K. Malignant tumor diseases andblood group substance H. Med Welt 1965; 38: 2144–7
16 Iodice S, Maisonneuve P, Botteri E, Sandri MT, Lowenfels AB. ABOblood group and cancer. Eur J Cancer 2010; 46: 3345–50
17 Joh HK, Cho E, Choueiri TK. ABO blood group and risk of renal cellcancer. Cancer Epidemiol 2012; 36: 528–32
18 Kaffenberger SD, Morgan TM, Stratton KL et al. ABO blood group is apredictor of survival in patients undergoing surgery for renal cellcarcinoma. BJU Int 2012; 110 (11 Pt B): E641–E6
19 Eble JN, Togashi K, Pisani P, Sauter G, Epstein JI, Sesterhenn IA.Tumours of the Kidney. World Health Organization Classification ofTumours: Pathology and Genetics of Tumours of the Urinary System andMale Genital Organs. Lyon: IARC Press, 2004: 9–87
20 Sobin LH, Gospodarowicz MK, Wittekind C. Urological Tumours –Kidney. TNM Classification of Malignant Tumours, 7th edn. Oxford:Wiley-Blackwell, 2009: 255–7
21 Fuhrman SA, Lasky LC, Limas C. Prognostic significance of morphologicparameters in renal cell carcinoma. Am J Surg Pathol 1982; 6: 655–63
22 Kroeger N, Seligson DB, Klatte T et al. Clinical, molecular, and geneticcorrelates of lymphatic spread in clear cell renal cell carcinoma. Eur Urol2012; 61: 888–95
23 Yazer MH. What a difference 2 nucleotides make: a short review of ABOgenetics. Transfus Med Rev 2005; 19: 200–9
24 Ueda R, Ogata S, Morrissey DM et al. Cell surface antigens of humanrenal cancer defined by mouse monoclonal antibodies: identification oftissue-specific kidney glycoproteins. Proc Natl Acad Sci U S A 1981; 78:5122–6
25 Breimer ME, Molne J, Norden G, Rydberg L, Thiel G, Svalander CT.Blood group A and B antigen expression in human kidneys correlated toA1/A2/B, Lewis, and secretor status. Transplantation 2006; 82: 479–85
26 Hakomori S. Antigen structure and genetic basis of histo-blood groups A,B and O: their changes associated with human cancer. Biochim BiophysActa 1999; 1473: 247–66
27 Melzer D, Perry JR, Hernandez D et al. A genome-wide association studyidentifies protein quantitative trait loci (pQTLs). PLoS Genet 2008; 4:e1000072
28 Xie J, Qureshi AA, Li Y, Han J. ABO blood group and incidence of skincancer. PLoS One 2010; 5: e11972
29 Gates MA, Wolpin BM, Cramer DW, Hankinson SE, Tworoger SS. ABOblood group and incidence of epithelial ovarian cancer. Int J Cancer 2011;128: 482–6
30 Gates MA, Xu M, Chen WY, Kraft P, Hankinson SE, Wolpin BM. ABOblood group and breast cancer incidence and survival. Int J Cancer 2012;130: 2129–37
Correspondence: Tobias Klatte, Department of Urology,Medical University of Vienna, Vienna General Hospital,Währinger Gürtel 18-20, A-1090 Vienna, Austria.
e-mail: [email protected]
Abbreviations: BMI, body mass index; CCI, Charlsoncomorbidity index; OS, overall survival; RCC-SS, RCC-specificsurvival; OR, odds ratio; HR, hazard ratio; IQR, interquartilerange.
de Martino et al.
© 2013 The AuthorsE66 BJU International © 2013 BJU International