Embed Size (px)
Citation preview
Evaluation of a pilot Pressure Ulcer Prevention Initiative (PUPI) for patients with traumatic spinal cord injury
admitted to an acute care setting
John Cobb, Occupational Therapist IIAcute Spine Unit, Vancouver General Hospital
2015 Quality Forum, Creating Connections
Context• Vancouver General Hospital Acute Spine Unit
• Full compliment of medical and allied health professionals
• Approximately 120 newly spinal cord injured admissions per year
• Length of stay varies from weeks to months
• 15% of traumatic spinal cord injured patients develop at least one pressure ulcer during their acute care admission (Street, J., Thorogood, N.P., Cheung, A. et al. 2013)
Problem/Issue
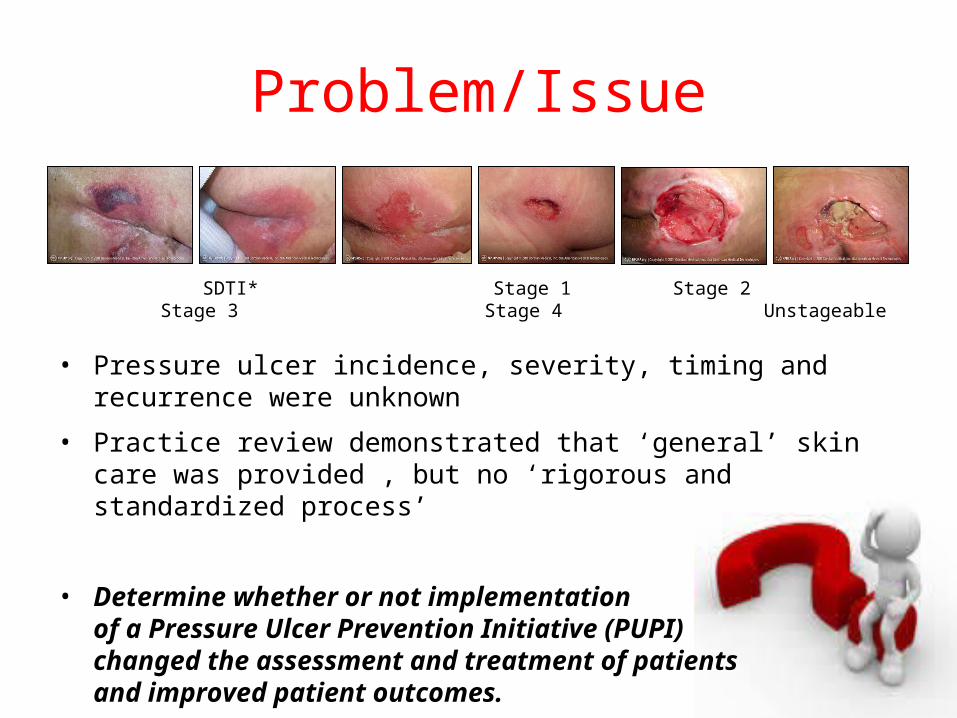
• Pressure ulcer incidence, severity, timing and recurrence were unknown
• Practice review demonstrated that ‘general’ skin care was provided , but no ‘rigorous and standardized process’
• Determine whether or not implementationof a Pressure Ulcer Prevention Initiative (PUPI)changed the assessment and treatment of patientsand improved patient outcomes.
SDTI* Stage 1 Stage 2 Stage 3 Stage 4 Unstageable
Intervention1 - Identify• All new traumatic spinal cord
injured patients
2 - Assess• OT Skin Care Chart Template • Braden Risk for Pressure Ulcer
Assessment
3 - Intervene• Prescribe and provide a
therapeutic support surface• Alert other team members
4 - Follow-Up• Monitor patients until discharge• Direct therapeutic support
surface upgrades and downgrades
5 - Document• OT Skin Care Chart Template• Photos if/as necessary
Measurement• Success of PUPI implementation was evaluated by:
– Examining the percentage of patients with completed:
i) occupational therapist skin care assessments
ii) prescriptions for therapeutic support surfaces (ie. mattress)
• Effect on patient outcomes was evaluated by:
– Examining changes in:
i) pressure ulcer incidence, severity, timing and recurrence in acute care
ii) pressure ulcer prevalence and life satisfaction in the community
Tests used: Wilcoxon-T-test, Fisher’s exact test, Chi-square test, Mann-Whitney test, p-value <0.05
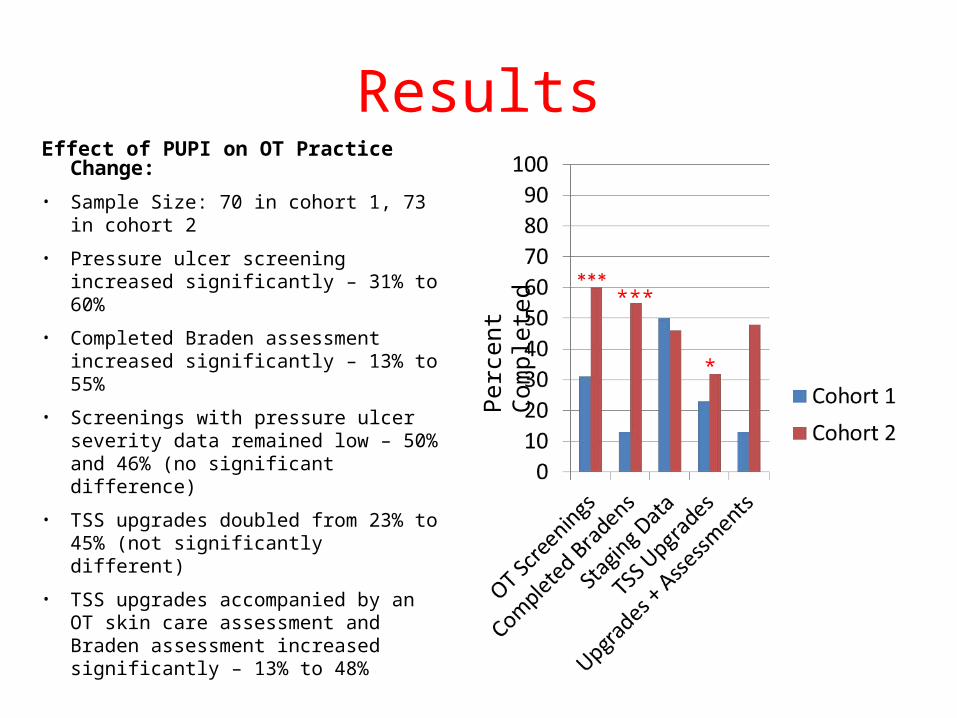
ResultsEffect of PUPI on OT Practice Change:• Sample Size: 70 in cohort 1, 73 in
cohort 2
• Pressure ulcer screening increased significantly – 31% to 60%
• Completed Braden assessment increased significantly – 13% to 55%
• Screenings with pressure ulcer severity data remained low – 50% and 46% (no significant difference)
• TSS upgrades doubled from 23% to 45% (not significantly different)
• TSS upgrades accompanied by an OT skin care assessment and Braden assessment increased significantly – 13% to 48%
***
*
Per
cent
Com
plet
ed
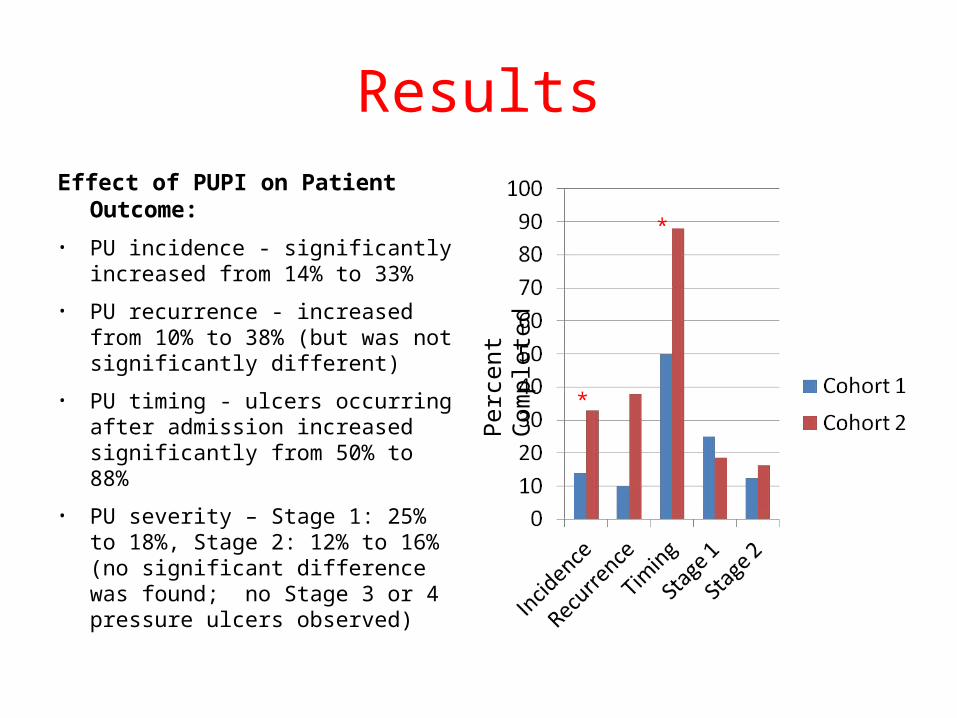
ResultsEffect of PUPI on Patient Outcome: • PU incidence - significantly increased
from 14% to 33%
• PU recurrence - increased from 10% to 38% (but was not significantly different)
• PU timing - ulcers occurring after admission increased significantly from 50% to 88%
• PU severity – Stage 1: 25% to 18%, Stage 2: 12% to 16% (no significant difference was found; no Stage 3 or 4 pressure ulcers observed)
Per
cent
Com
plet
ed
*
*
Conclusions
• PUPI was successful in changing clinical practice in pressure ulcer prevention but no statistically significant improvement in pressure ulcer -related patient outcomes was demonstrated.
• No effect of the PUPI was seen on immediate or long-term patient outcomes during the study period.
Challenges
Implementation:
• Implementation alongside day-to-day operations
• OT’s lack of pressure ulcer knowledge and comfort to stage
Data collection:
• Lack of OT follow-up documentation
• Lack of data required for study analysis
Lessons LearnedImplementation:
• Use of an implementation model (National Implementation Research Network)
• Providing formal training and testing of the OT’s pressure ulcer knowledge
Data collection:
• Trialing the skin care charting template to a greater degree
• Performing documentation audits after implementation
Next Steps1. Maintain PUPI and refine
2. Obtain focus group feedback
3. Reintroduce using a formal implementation model
4. Increase OT knowledge and confidence
5. Simplify OT documentation tool
6. Maintain the Braden Scale for Predicting Pressure Ulcer Risk©(Braden, B.J., Makleburst, J.)
7. Introduce the Therapeutic Surface Selection Tool©(Norton, L., Coutts, P., Sibbald, R.G.)
8. Explore regular access to high-specification therapeutic support surfaces
9. Present findings to the VGH Quality Council
10. Determine if the PUPI should become a required organizational practise
Thank you!John Cobb, BScOT, Occupational Therapist IIVGH Acute Spine Program, Centennial PavilionVancouver General Hospital, 855 W. 12th Ave.Vancouver, BC, V5Z 1M9(604) [email protected]
This project has been published:Journal of Wound Care, May 2014Volume 23, Number 5Pages 211-224