Embed Size (px)
Citation preview
Evaluation and Optimization ofTherapeutic Footwear for NeuropathicDiabetic Foot Patients Using In-ShoePlantar Pressure AnalysisSICCO A. BUS, PHD
1,2
ROB HASPELS2
TESSA E. BUSCH-WESTBROEK, MD1
OBJECTIVE—Therapeutic footwear for diabetic foot patients aims to reduce the risk of ul-ceration by relievingmechanical pressure on the foot. However, footwear efficacy is generally notassessed in clinical practice. The purpose of this study was to assess the value of in-shoe plantarpressure analysis to evaluate and optimize the pressure-reducing effects of diabetic therapeuticfootwear.
RESEARCHDESIGNANDMETHODS—Dynamic in-shoe plantar pressure distributionwas measured in 23 neuropathic diabetic foot patients wearing fully customized footwear.Regions of interest (with peak pressure .200 kPa) were selected and targeted for pressureoptimization by modifying the shoe or insole. After each of a maximum of three rounds ofmodifications, the effect on in-shoe plantar pressure was measured. Successful optimizationwas achieved with a peak pressure reduction of .25% (criterion A) or below an absolute levelof 200 kPa (criterion B).
RESULTS—In 35 defined regions, mean peak pressure was significantly reduced from 303 (SD77) to 208 (46) kPa after an average 1.6 rounds of footwearmodifications (P, 0.001). This resultconstitutes a 30.2% pressure relief (range 18–50% across regions). All regions were successfullyoptimized: 16 according to criterion A, 7 to criterion B, and 12 to criterion A and B. Footwearoptimization lasted on average 53 min.
CONCLUSIONS—These findings suggest that in-shoe plantar pressure analysis is an effectiveand efficient tool to evaluate and guide footwear modifications that significantly reduce pressurein the neuropathic diabetic foot. This result provides an objective approach to instantly improvefootwear quality, which should reduce the risk for pressure-related plantar foot ulcers.
Diabetes Care 34:1595–1600, 2011
A s a long-term complication of thedisease, foot ulceration poses a sig-nificant burden on patients with
diabetes. Foot ulcers are an importantprecursor to infection and amputation(1,2). Approximately half of diabetic footulcers occur on the plantar surface of thefoot (3). Peripheral neuropathy and in-creased levels of mechanical foot pressureare important factors in the cause ofplantar foot ulceration (4,5). Therapeuticfootwear is often prescribed to prevent
ulceration, particularly for patients whohave suffered prior ulceration. The foot-wear’s primary goal is to redistribute pres-sure on the plantar foot surface to relievepressure at locations that are at risk for(re)ulceration.
When evaluating the efficacy of ther-apeutic footwear in patients with neuro-pathic foot problems, patient feedback isinadequate because of the presence ofneuropathy. Mostly, a trial-and-error ap-proach with subsequent inspection of the
feet is used. Eventually, feedback consistsof the information on whether the patientremains free of ulceration. Objectivemethods to evaluate the footwear, suchas in-shoe plantar pressure analysis, arenot regularly used in clinical practice,despite the fact that the footwear’s pri-mary goal is to relieve pressure. Addi-tionally, the pressure-relieving effect offootwear interventions is difficult to pre-dict at the individual patient level becauseof the variability in outcomes (6–9). Thisresult prevents establishing guidelines foreffective footwear prescriptions and mod-ification and argues for the use of in-shoeplantar pressure assessment for evaluat-ing individual patients (6,10–13).
Within this context, in-shoe plantarpressure assessment may have the addi-tional potential to guide modifications inthe footwear to achieve a more optimalsolution (in terms of pressure reduction)(10,14). If successful, such optimizationwill reduce the variability in outcome offootwear prescriptions and further sup-port the use of in-shoe pressure analysisin clinical practice. Therefore, the pur-pose of this study was to assess the valueof using in-shoe plantar pressure analy-sis to evaluate and optimize the pressure-reducing effects of therapeutic footwearin neuropathic diabetic foot patients.
RESEARCH DESIGN ANDMETHODS
SubjectsA total of 23 neuropathic diabetic footpatients participated (17 men, 6 women).Mean age was 59.1 (SD 12.6) years, andmean BMI was 33.0 (8.7) kg/m2. Eightpatients had type 1 diabetes, and 15 hadtype 2 diabetes.Mean duration of diabeteswas 13.8 (10.1) years, and mean HbA1c
level was 7.3 (1.1) percent. A total of18 patients had a history of plantar footulceration, which included nontraumaticneuropathic foot ulcers located at thehallux (n = 3), toes (n = 1), metatarsalheads (n = 11), or midfoot (n = 3). Allpatients had at least one foot deformity
c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c
From the 1Department of Rehabilitation, AcademicMedical Center, University of Amsterdam, Amsterdam, theNetherlands; and the 2Diabetic Foot Unit, Department of Surgery, Ziekenhuisgroep Twente, Almelo, theNetherlands.
Corresponding author: Sicco A. Bus, [email protected] 24 November 2010 and accepted 20 April 2011.DOI: 10.2337/dc10-2206© 2011 by the American Diabetes Association. Readers may use this article as long as the work is properly
cited, the use is educational and not for profit, and thework is not altered. See http://creativecommons.org/licenses/by-nc-nd/3.0/ for details.
care.diabetesjournals.org DIABETES CARE, VOLUME 34, JULY 2011 1595
E m e r g i n g T r e a t m e n t s a n d T e c h n o l o g i e sO R I G I N A L A R T I C L E

(claw/hammer toes, hallux valgus, mid-foot Charcot deformity, limited jointmobility, pes planus, or pes cavus). Pe-ripheral neuropathy was confirmed bythe inability to feel the pressure of a10-g Semmes-Weinstein monofilamentat one or more of six plantar foot sites.
Patients from four different outpa-tient clinics were included. Two clinicsprovided four participating patients, oneclinic six patients, and one clinic ninepatients. All participants were consec-utive referrals for footwear evaluationbecause of previous ulcer healing, thepresence of severe deformity, or presignsof ulceration and a measured in-shoeplantar pressure .200 kPa. The studywas conducted as a noninterventionalstudy in a patient care setting. For thisreason, the local ethics committee waivedthe requirement for ethical approval ofthe study.
Footwear and instrumentationThe prescribed therapeutic footwear con-sisted of fully customized footwear (n = 22)or custom molded insoles in an extra-depth shoe (n = 1). Nine patients worenew footwear, and 14 patients wore pre-viously delivered footwear. The overallmean age of the tested footwear was 2.3months. The footwear was generally man-ufactured on a last that was created from anegative or positive cast or foam impres-sion of the patient’s foot. Blueprints and/orglass-plate images of the feet were used toidentify foot shape and specific at-risklocations to target footwear design andmanufacturing. Shoes were mostly anklehigh and made from leather with a stiff-ened rubber outsole and roller configura-tion. Custom molded insoles were madefrom multidensity-layered materials,with a moldable base and an open orclosed-cell material top cover. Patientswore their own socks, which were mostlythin seamless socks. The footwear in eachclinic was prescribed and manufacturedby a rehabilitation specialist and an ortho-pedic shoe technician (qualification simi-lar to a certified pedorthist) who had aminimum of 4 years’ experience withtreating the diabetic foot.
In-shoe plantar pressures were mea-sured using the Pedar-X system (Novel,Munich, Germany). This system comprises2-mm-thick flexible pressure-sensing in-soles including 99 sensors each measuringthe vertical (normal) pressure at the shoe-sock interface at a sample frequency of50Hz. Pedar-wide insoles were available infive different length sizes to accommodate
different foot sizes. Before the pressuremeasurements, each of the 99 individualsensors per insole was calibrated accord-ing to the manufacturer’s guidelines.
Protocol and footwear optimizationPatients repeatedly walked at a self-selected speed along a 12-m walkwaywhile in-shoe plantar pressures were mea-sured.With each pressuremeasurement, aminimum of 15 midgait steps were col-lected in four walking trials. Walkingspeed was measured between two fixedpoints using a stopwatch and kept con-stant between trials (maximum 5% de-viation).
The footwear optimization algorithmis shown in Fig. 1. In-shoe plantar pres-sures were first measured in the non-modified footwear (baseline assessment).From the peak pressure distribution dia-grams shown on-screen in the Novel stepanalysis program, regions of interest(ROIs) were defined as target regions forpressure optimization. These ROIs cor-responded with locations of previous ul-ceration, severe foot deformity (Charcotosteoarthropathy), or preulcerative signs,all in which the measured peak pressurewas .200 kPa. Other regions showingpeak pressures .300 kPa were alsotargeted. A maximum of three ROIs perfoot were selected.
The shoe technician modified thefootwear with the goal to reduce peakpressure at the ROI. Necessary machineryand materials were available at the testingsite. The choice of modification was madeby the shoe technician and/or physicianand consisted of the local removal orsoftening ofmaterial in the insole; replace-ment of the insole top cover; the additionof a metatarsal pad, hallux pad, or meta-tarsal bar in the insole; or the adjustmentof the rocker or roller in the shoe outsoleor insole (i.e., earlier or more significant).More than one footwear modification wasallowed at the same time. Modificationsthat would require significant extra timeor special machinery such as the applica-tion of a new rocker outsole or the re-placement of midsole materials were notapplied.
Footwear modification was directlyfollowed by an in-shoe pressure measure-ment. Walking speed was kept consistentwith the speed measured during baselineassessment (maximum 5% deviation).Change in peak pressure at the ROI com-pared with baseline was calculated fromthe on-screen display of the peak pres-sure diagrams.
The footwear was classified as suc-cessfully optimized when, compared withthe baseline assessment, a minimum 25%reduction in mean peak pressure at theROI was achieved (criterion A) or meanpeak pressure was reduced below anabsolute level of 200 kPa (criterion B).Both criteria were chosen to represent asignificant, probably clinically relevant,reduction in plantar pressure. Criterion Bwas based on previous results showing anaverage in-shoe peak pressure of;200 kPausing similar equipment in patients whohad remained healed in their prescribedfootwear after an episode of ulceration (15).
If the optimization criteria were notmet after the first round of one or moremodifications, additional in-shoe pres-sure evaluations and modifications wereallowed, up to a maximum of three rounds.This number of modification rounds wasmaximized for feasibility reasons consid-ering the (potential) use of this approachin clinical practice. If the optimization cri-teria were not met within three rounds,optimization was considered a failure. Thetime required to complete the session, in-cluding all pressure measurements andfootwear modifications, was recorded.
Data analysisUsing Novel multimask software, maskswere drawn for each ROI and, in the samefoot, for each of 10 anatomical foot regions:medial and lateral heel, medial andlateral midfoot, metatarsal 1, metatarsals2/3, metatarsals 4/5, hallux, toes 2/3, andtoes 4/5. For each mask, mean peak pres-sure and pressure-time integral over allcollected steps per foot were calculated.
Figure 1—Schematic diagram of the footwearoptimization algorithm used in the study. PP,peak pressure.
1596 DIABETES CARE, VOLUME 34, JULY 2011 care.diabetesjournals.org
Pressure optimization in therapeutic footwear

Specific analyses were performed for eachROI, for each major foot location wherethe ROI were present (hallux, metatarsals,andmidfoot), for each shoe technician, fornew and already worn footwear, and foreach type of modification applied. Whenmore than one modification was made inthe same round of footwear modifications,the effect of these modifications on peakpressure was considered evenly distrib-uted. Peak pressure effects in neighboring(anatomical) regions of each ROI aftermodifying the footwear were calculatedand considered excessive if increased.25kPa and .25% compared with baseline.Where data were compared statistically,paired t tests or ANOVA were conductedin SPSS (version 16.0).
RESULTS—A total 35 ROIs were se-lected for footwear optimization. A totalof 17 were located at the metatarsal heads(first, n = 6; second or third, n = 9; fifth,n = 2), 13 at the hallux, and 5 at the mid-foot. In 9 of the 18 patients who had aprevious foot ulcer, the ROI correspondedwith the previous ulcer location.
All 35 ROIs could be optimized ac-cording to the defined criteria: 16 on thebasis of a minimum 25% peak pressurerelief compared with baseline, 7 on thebasis of a peak pressure reduction below alevel of 200 kPa, and 12 on the basis ofboth criteria. The mean peak pressuremeasured at baseline in all ROIs was 303(SD 77) kPa. Peak pressure significantlyreduced with 95 kPa (30.2%, P, 0.001)to a mean 208 (SD 46) kPa after all nec-essary rounds of footwear modification.The range in peak pressure relief acrossindividual ROI was 17.1–51.8%. Meanrelief in pressure-time integral across allROIs after modifying the footwear was24.3% (P , 0.001). The mean time re-quired to complete the testing sessionwas 53 min (SD 13, range 34–78).
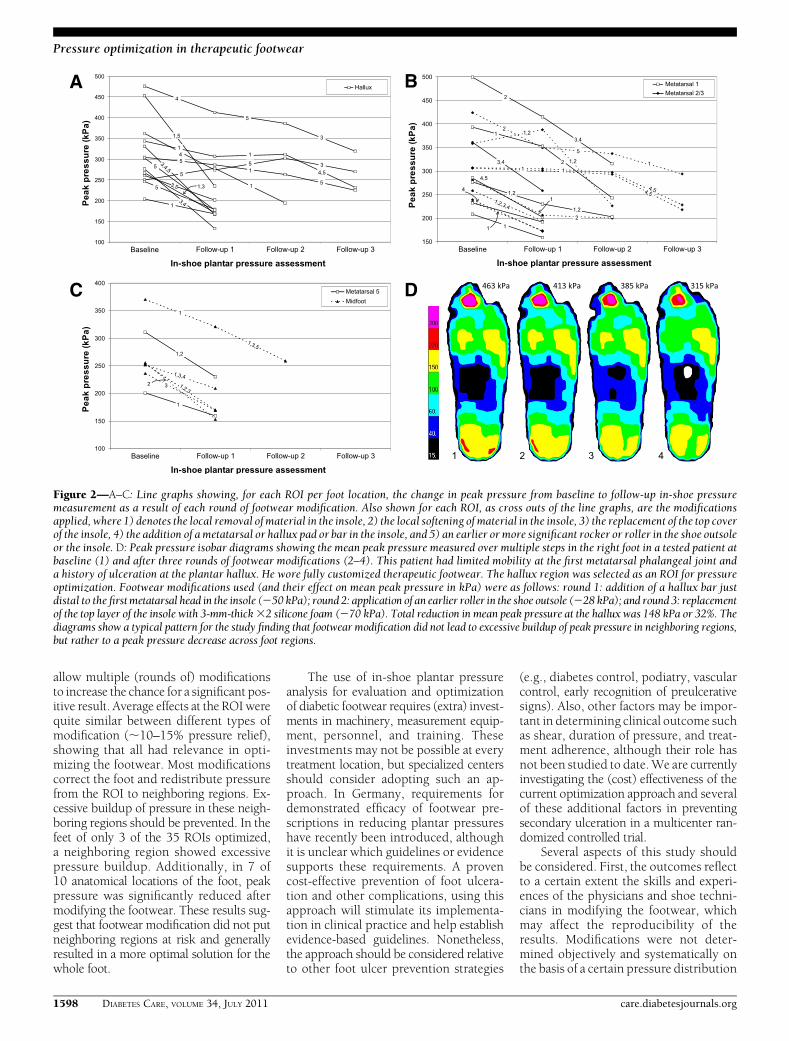
An average 1.6 rounds of footwearmodifications were needed to satisfy theoptimization criteria. In the 21 ROIs re-quiring one round, mean peak pressurerelief compared with baseline was 30.3%.In the seven ROIs requiring two rounds,mean peak pressure relief was 9.2% afterthe first round and 23.0% after the secondround. In the seven ROIs requiring threerounds, mean peak pressure relief was10.6% after the first, 1.7% after thesecond, and 18.5% after the third round.Figure 2 shows the peak pressure changesper follow-up in-shoe pressure measure-ment together with the applied modi-fications in each round of footwear
modification for all 35 individual ROIs.Peak pressure diagrams for a patient whohad his footwear successfully optimizedare also shown in Fig. 2.
There were no significant differencesin mean peak pressure relief achievedbetween the ROI optimized by the fourshoe technicians (range 26.7–32.8%, P =0.37). There were also no significantdifferences in mean peak pressure reliefachieved between the ROI located at dif-ferent major foot locations: 33.4% (range17.6–51.8) for the hallux (n = 13 ROI),27.9% (17.2–38.2) for the metatarsal re-gions (n = 17), and 29.7% (17.1–40.0) forthe midfoot (n = 5) (P = 0.23). Analysis ofthe 10 anatomical foot locations showedsignificant mean peak pressure reduc-tions after modifying the footwear in allbut three locations (lateral midfoot, toes2/3, and toes 2/5) (P , 0.05). Excessivebuildup of pressure in a neighboring re-gion was present with three of the 35ROIs.
Five different types of footwear mod-ifications were used in the study. Theirfrequency distribution and mean effectson peak pressure are shown in Table 1.Differences in effects between the types ofmodification were small and nonsignifi-cant (P = 0.64). Additionally, there wasno clear difference in the type of modifi-cations used and the optimization successbetween newly delivered and alreadyworn shoes (mean peak pressure relief28.5 and 31.3%, respectively).
CONCLUSIONS—The results of thisstudy showed a substantial relief inpeak pressure of ;30% at selected high-pressure ROIs after modifying the custom-made footwear of neuropathic diabeticfoot patients using in-shoe plantar pres-sure analysis as a guidance tool to themodifications made. All selected ROIswere optimized according to the definedoptimization criteria, within an average of53 min. This result demonstrates in ourview the success and feasibility of the ap-proach. Because an increase in plantarfoot pressure increases the risk for dia-betic foot ulceration, such optimizationresults should reduce the risk of foot ulcer-ation. However, this effect remains to beinvestigated in a prospective clinical trial.
The study results substantiate earliercase reports showing that significant pres-sure relief is achievable when using in-shoe pressure analysis as a guidance toolfor footwear modification (14). Further-more, the results support earlier suggestionsthat in-shoe plantar pressure analysis
should be an integral part of footwearevaluation in high-risk neuropathic dia-betic patients (6,10,11,13,16). The ap-proach offers an individual-based solutionto instantly achieve more optimal footwearon the assumption that different footweardesign principles or modifications maywork for different patients. This result issupported by the finding that not all ROIswere optimized within one round or withone type of footwear modification, but re-quired subsequent rounds and/or differentmodifications to achieve the desired out-come (Fig. 2). The result is less variabilityin outcome on pressure relief across indi-vidual patients. This provides the clinicalteam with a valuable approach to achievebetter quality footwear for the individualpatient.
At baseline, the patients’ footwear wasnot yet optimal in relieving pressure,although half of the previous ulcer loca-tions were not selected as an ROI, appar-ently showing already good pressurerelief at these locations. The suboptimalfootwear is probably due to the lack ofavailable (evidence-based) guidelines forfootwear prescription and lack of predict-able effects of footwear design principles.This scenario currently makes the provi-sion and evaluation of footwear largely atrial-and-error process, where the skillsand experience of the clinical team deter-mine the outcome. However, the lack ofdifferences found in outcome betweenthe four teams of physicians/shoe techni-cians suggest that positive results can beachieved by any experienced team. Onlyrecently, quantitative approaches such asthe use of dynamic barefoot pressure re-cordings and three-dimensional footshape measurements have been intro-duced in the provision of footwear for di-abetic patients. The application of suchmethods can result in footwear providingalso an ;30% pressure relief comparedwith footwear made using conventionalmethods (17). Combining these methodswith the current optimization approachmaypotentially further optimize the pressure-relieving capacity of prescribed therapeuticfootwear. This scenario should be tested infuture studies.
Five different types of modificationswere applied, and all five were commonlyused. The effect of these modifications onpeak pressure was quite variable fromROI to ROI (Table 1, Fig. 2), confirmingthe lack of predictability of these modifica-tions in individual cases. This result sup-ports the use of the optimization approach,in particular, because of its flexibility to
care.diabetesjournals.org DIABETES CARE, VOLUME 34, JULY 2011 1597
Bus, Haspels, and Busch-Westbroek
allow multiple (rounds of) modificationsto increase the chance for a significant pos-itive result. Average effects at the ROI werequite similar between different types ofmodification (;10–15% pressure relief),showing that all had relevance in opti-mizing the footwear. Most modificationscorrect the foot and redistribute pressurefrom the ROI to neighboring regions. Ex-cessive buildup of pressure in these neigh-boring regions should be prevented. In thefeet of only 3 of the 35 ROIs optimized,a neighboring region showed excessivepressure buildup. Additionally, in 7 of10 anatomical locations of the foot, peakpressure was significantly reduced aftermodifying the footwear. These results sug-gest that footwear modification did not putneighboring regions at risk and generallyresulted in a more optimal solution for thewhole foot.
The use of in-shoe plantar pressureanalysis for evaluation and optimizationof diabetic footwear requires (extra) invest-ments in machinery, measurement equip-ment, personnel, and training. Theseinvestments may not be possible at everytreatment location, but specialized centersshould consider adopting such an ap-proach. In Germany, requirements fordemonstrated efficacy of footwear pre-scriptions in reducing plantar pressureshave recently been introduced, althoughit is unclear which guidelines or evidencesupports these requirements. A provencost-effective prevention of foot ulcera-tion and other complications, using thisapproach will stimulate its implementa-tion in clinical practice and help establishevidence-based guidelines. Nonetheless,the approach should be considered relativeto other foot ulcer prevention strategies
(e.g., diabetes control, podiatry, vascularcontrol, early recognition of preulcerativesigns). Also, other factors may be impor-tant in determining clinical outcome suchas shear, duration of pressure, and treat-ment adherence, although their role hasnot been studied to date.We are currentlyinvestigating the (cost) effectiveness of thecurrent optimization approach and severalof these additional factors in preventingsecondary ulceration in a multicenter ran-domized controlled trial.
Several aspects of this study shouldbe considered. First, the outcomes reflectto a certain extent the skills and experi-ences of the physicians and shoe techni-cians in modifying the footwear, whichmay affect the reproducibility of theresults. Modifications were not deter-mined objectively and systematically onthe basis of a certain pressure distribution
Figure 2—A–C: Line graphs showing, for each ROI per foot location, the change in peak pressure from baseline to follow-up in-shoe pressuremeasurement as a result of each round of footwear modification. Also shown for each ROI, as cross outs of the line graphs, are the modificationsapplied, where 1) denotes the local removal of material in the insole, 2) the local softening of material in the insole, 3) the replacement of the top coverof the insole, 4) the addition of a metatarsal or hallux pad or bar in the insole, and 5) an earlier or more significant rocker or roller in the shoe outsoleor the insole. D: Peak pressure isobar diagrams showing the mean peak pressure measured over multiple steps in the right foot in a tested patient atbaseline (1) and after three rounds of footwear modifications (2–4). This patient had limited mobility at the first metatarsal phalangeal joint anda history of ulceration at the plantar hallux. He wore fully customized therapeutic footwear. The hallux region was selected as an ROI for pressureoptimization. Footwear modifications used (and their effect on mean peak pressure in kPa) were as follows: round 1: addition of a hallux bar justdistal to the firstmetatarsal head in the insole (250 kPa); round 2: application of an earlier roller in the shoe outsole (228 kPa); and round 3: replacementof the top layer of the insole with 3-mm-thick32 silicone foam (270 kPa). Total reduction in mean peak pressure at the hallux was 148 kPa or 32%. Thediagrams show a typical pattern for the study finding that footwear modification did not lead to excessive buildup of peak pressure in neighboring regions,but rather to a peak pressure decrease across foot regions.
1598 DIABETES CARE, VOLUME 34, JULY 2011 care.diabetesjournals.org
Pressure optimization in therapeutic footwear

profile because guidelines on how toreduce these pressures do not exist. Wefollowed the dominant current practicein footwear evaluation in which a trial-and-error approach is used. Nevertheless,logical choices were made in modifyingthe footwear using a limited set of gen-erally effective modifications, which re-sulted, after one or more rounds, inoptimized footwear. Differences in opti-mization results were not found betweenshoe technicians. For these reasons, re-producibility of the results may still bequite high. Second, the optimizationcriteria were chosen somewhat arbi-trarily. They were based on what weconsidered a clinically relevant pressurereduction, partly on the basis of previousrecommendations (15), which could beachieved in a reasonable time. Neverthe-less, future research will have to showwhether these chosen criteria are clini-cally meaningful. Third, the number oftested patients could be considered quitesmall given the variability in pressure dis-tribution profiles and footwear modifica-tions applied. However, all 35 selectedROI were optimized, and percentagepeak pressure reductions in the ROIswere significantly skewed toward thepositive side (17–52%). On the basis ofthese consistent results, we believe thatrelevant conclusions can be drawn fromthis small study sample. Finally, themajority of footwear tested (14 of 23) waspreviously worn for some period. Thisconcerned mostly footwear in which pa-tients had developed an ulcer and whichwas modified after the healing of the ulcerin another device. Wear and tear of thisfootwear may have increased the chancefor successful optimization, although theresults show no clear differences in typesof modifications used and pressure reliefachieved between the new and already-worn footwear. The results show that eval-uation and optimization is worthwhile infootwear of any age, but the most appropri-ate moment is probably close to delivery.Future studies will have to demonstrate theoptimization success in a larger sample ofnewly prescribed footwear and the optimalfrequency for in-shoe pressure evaluation.
In conclusion, the results of this studyshow that custom-made therapeutic foot-wear of at-risk neuropathic diabetic footpatients can be effectively and efficientlyoptimized for its pressure-relieving capacitywhen using in-shoe plantar pressure anal-ysis as a tool to guide modifications to thefootwear. This provides the clinical teamwith a valuable, objective, and efficient
method to assess and improve therapeuticfootwearquality for individualpatients. Suchoptimization should reduce the risk ofplantar foot ulceration in this patient group,although this result will have to be con-firmed in future prospective clinical trials.
Acknowledgments—No potential conflicts ofinterest relevant to this article were reported.S.A.B. researched data, contributed to dis-
cussion, and wrote the manuscript. R.H. andT.E.B.-W. researched data, contributed to dis-cussion, and reviewed and edited themanuscript.Preliminary results of this study were pre-
sented in abstract form at the Diabetic FootStudyGroup (DFSG)meeting,Elsinore,Denmark,10–13 September 2006.The authors acknowledge the contribution
of Paul Mooren, shoe technician, AcademicMedical Center, Amsterdam.
References1. Boulton AJ, Kirsner RS, Vileikyte L. Clin-
ical practice: neuropathic diabetic footulcers. N Engl J Med 2004;351:48–55
2. Pecoraro RE, Reiber GE, Burgess EM.Pathways to diabetic limb amputation:basis for prevention. Diabetes Care 1990;13:513–521
3. Prompers L, HuijbertsM, Apelqvist J, et al.High prevalence of ischaemia, infectionand serious comorbidity in patients withdiabetic foot disease in Europe: baselineresults from the Eurodiale study. Dia-betologia 2007;50:18–25
4. Frykberg RG, Lavery LA, PhamH,HarveyC,Harkless L, Veves A. Role of neuropathy andhigh foot pressures in diabetic foot ulcera-tion. Diabetes Care 1998;21:1714–1719
5. Pham H, Armstrong DG, Harvey C,Harkless LB, Giurini JM, Veves A. Screeningtechniques to identify people at high riskfor diabetic foot ulceration: a prospectivemulticenter trial. Diabetes Care 2000;23:606–611
6. Bus SA, Ulbrecht JS, Cavanagh PR. Pressurerelief and load redistribution by custom-made insoles in diabetic patients withneuropathy and foot deformity. Clin Bio-mech (Bristol, Avon) 2004;19:629–638
7. Raspovic A,Newcombe L, Lloyd J, Dalton E.Effect of customized insoles on verticalplantar pressures in sites of previous neu-ropathic ulceration in the diabetic foot.Foot 2000;10:133–138
8. Kato H, Takada T, Kawamura T, Hotta N,Torii S. The reduction and redistributionof plantar pressures using foot orthoses indiabetic patients. Diabetes Res Clin Pract1996;31:115–118
9. Lord M, Hosein R. Pressure redistributionby molded inserts in diabetic footwear:a pilot study. J Rehabil Res Dev 1994;31:214–221
10. Cavanagh PR. Therapeutic footwear forpeople with diabetes. Diabetes Metab ResRev 2004;20(Suppl. 1):S51–S55
Table
1—Type
andnum
berof
footwear
modifi
cationsand
theirmean
effecton
in-shoepeak
pressurefor
allROIs
andfor
theROIs
perfoot
location
nAlllocation
s(n
=35
ROIs)
nHallux
(n=13
ROIs)
nMetatarsals
(n=17
ROIs)
nMidfoot
(n=5ROIs)
Type
offootwear
modification
Localremovalof
materialin
insole26
11.2%(2
4.2to
30.2)7
13.0%(2
1.3to
30.2)15
10.1%(2
4.2to
26.7)4
9.8%(5.7
–13.2)Localsoftening
ofmaterialin
insole12
14.1%(2
4.2to
40.0)0
—10
11.8%(2
4.2to
31.2)2
25.5%(10.9
–40.0)Addition
ofmetatarsalor
halluxpad
orbar
ininsole
1216.0%
(6.2–28.0)
518.6%
(12.7–25.9)
714.2%
(6.2–28.0)
0—
Replacem
entof
topcover
ofinsole
1414.4%
(6.2–25.9)
616.7%
(10.6–25.9)
411.7%
(6.2–14.6)
413.6%
(6.4–10.9)
Earlier
ormore
significantrocker
orroller
inshoe
outsole
orinsole
1612.3%
(211.2
to41.6)
1111.5%
(211.2
to41.6)
412.9%
(3.4–23.6)
16.4%
Data
arenorm
eaneffect(range),w
iththe
effectonpeak
pressureexpressed
aspercentage
reductioncom
pared
with
theprevious
in-shoe
pressuremeasurem
entinthe
session(negative
valuesdenote
anincrease
inpeak
pressure).
care.diabetesjournals.org DIABETES CARE, VOLUME 34, JULY 2011 1599
Bus, Haspels, and Busch-Westbroek

11. Guldemond NA, Leffers P, Schaper NC,Sanders AP, Nieman FH, WalenkampGH. Comparison of foot orthosesmade bypodiatrists, pedorthists and orthotists re-garding plantar pressure reduction in theNetherlands. BMC Musculoskelet Disord2005;6:61
12. van Schie C, Ulbrecht JS, Becker MB,Cavanagh PR. Design criteria for rigidrocker shoes. Foot Ankle Int 2000;21:833–844
13. Praet SF, Louwerens JW. The influence ofshoe design on plantar pressures in neu-ropathic feet. Diabetes Care 2003;26:441–445
14. Mueller MJ. Application of plantar pres-sure assessment in footwear and insertdesign. J Orthop Sports Phys Ther 1999;29:747–755
15. Owings TM, Apelqvist J, Stenström A,et al. Plantar pressures in diabetic pa-tients with foot ulcers which have
remained healed. Diabet Med 2009;26:1141–1146
16. Cavanagh PR, Bus SA. Off-loading the di-abetic foot for ulcer prevention and healing.J Vasc Surg 2010;52(Suppl.):37S–43S
17. Owings TM, Woerner JL, Frampton JD,Cavanagh PR, Botek G. Custom thera-peutic insoles based on both foot shapeand plantar pressure measurement pro-vide enhanced pressure relief. DiabetesCare 2008;31:839–844
1600 DIABETES CARE, VOLUME 34, JULY 2011 care.diabetesjournals.org
Pressure optimization in therapeutic footwear


![ORIGINAL ARTICLE Perceived role of therapeutic footwear in ... · treatment modalities are not readily available in most developing countries.[4,5] A frequently referenced component](https://img.pdfslide.us/doc/110x75/5eac14d41558734120261c85/original-article-perceived-role-of-therapeutic-footwear-in-treatment-modalities.jpg)


























