Embed Size (px)
Citation preview
1
Evaluation & Management of
Pediatric Obstructive Sleep Apnea
Stacey Ishman, MD, MPH, FAAP Surgical Director, Upper Airway Center
Director, Otolaryngology Outcomes Research
Divisions Otolaryngology & Pulmonary Medicine
Acknowledge: Scott Brietzke, MD, MPH
None
Objective
1. To compare guidelines from the AASM, AAO-HNS and AAP for diagnosis/management of OSA
2. To formulate a plan for evaluation and management of children with persistent obstructive sleep apnea (OSA) following adenotonsillectomy (T&A)
3. To understand the options and evidence for sleep surgical procedures currently utilized for treatment of OSA after T&A
Pediatric OSA
• 2 to 4% of pediatric population
• Two patterns seen in children
• Complete obstructive apneas
• Partial upper airway obstruction with
hypoventilation
Pediatric OSA
• Higher prevalance in pts with
• Craniofacial anomalies
• Pierre-Robin sequence, Apert syndrome…
• Neuromuscular diseases
• Cerebral palsy
• Muscular dystrophy
• Obesity
• Achondroplasia
• Mucopolysaccharidoses (Hurlers>Hunters)
#1 Cause of OSA in Children

Pediatric Sleep Disordered Breathing
Clinical Practice Guidelines
“Oto” 2011 “Sleep”2011 “Peds” 2012
Committee Composition
Oto Peds Sleep Otolaryngologist – 5
Sleep Medicine – 3
Peds Pulm – 1
Anesthesia – 1
Research - 1
Peds Pulm - 6
Pediatrician – 3
Otolaryngologist – 1
Neonatologist – 1
Neuropsychologist -1
Sleep Med - 11
Target Audience
Oto Peds Sleep Otolaryngologist in any
practice setting where a
child would be
evaluated
uncomplicated
childhood OSAS in an
otherwise healthy child
...who is being evaluated
in the primary care
setting
pediatric physicians
gailforcemarketing.com
Purpose
Oto Peds Sleep to define actions that
could be taken by
otolaryngologists to
deliver quality care
1) increase recognition
of OSAS by primary care
clinicians to minimize
delay in diagnosis 2)
evaluate diagnostic
techniques 3) describe
treatment options
4) provide guidelines for
follow-up 5) discuss
areas requiring further
research
to evaluate the
validity and reliability of
PSG and to determine
its clinical utility for
assessment and
management of various
respiratory disorders
howtoblogabook.com
Methodology “OTO”
• Strong Recommendation
– Benefits> Harm – strong evidence
• Recommendation
– Benefits>Harm – evidence not as strong
• Option
– Quality of evidence suspect OR little advantage
• No Recommendation
blog.plista.com
PSG: “Obvious” High Risk Cases
Oto Peds Sleep Obesity
Down Syndrome
Craniofacial abnormalities
Neuromuscular disorders
Sickle cell disease
Mucopolysaccharidoses
RECOMMENDATION,
GRADE C
Not within the
scope
Obesity
Down Syndrome
Craniofacial abnormalities
Neuromuscular disorders
Prader-Willi
Chiari malformations
Pierre Robin Sequence
ALTE
STANDARD
high-riskmerchant-account.com

PSG: Oto - High Risk Cases PSG: “Healthy” Child
Oto Peds Sleep advocate for PSG prior
to tonsillectomy for SDB
in children…for whom
the need for surgery is
uncertain or when there
is discordance between
tonsillar size on physical
exam and the reported
severity of SDB
RECOMMENDATION,
GRADE C
If a child snores on a
regular basis and has
complaints shown in
Table 2 clinicians should
either 1) obtain PSG or
2) refer to a sleep
specialist or
otolaryngologist
RECOMMENDATION,
GRADE B
PSG is indicated when
the clinical assessment
suggests the diagnosis
of OSAS in children
STANDARD
PSG: “Healthy” Child
Oto Peds Sleep advocate for PSG prior
to tonsillectomy for SDB
in children…for whom
the need for surgery is
uncertain or when there
is discordance between
tonsillar size on physical
exam and the reported
severity of SDB
RECOMMENDATION,
GRADE C
If a child snores on a
regular basis and has
complaints shown in
Table 2 clinicians should
either 1) obtain PSG or
2) refer to a sleep
specialist or
otolaryngologist
RECOMMENDATION,
GRADE B
PSG is indicated when
the clinical assessment
suggests the diagnosis
of OSAS in children
STANDARD
History
• 12 article identified
• 11/12 concluded clinical evaluation is
inaccurate in diagnosing OSA
• Level of evidence was B/B+
Brietzke et al. Otolaryngol Head Neck Surg 2004;131:827-32.
History
• None had an adequate balance sensitivity & specificity
• High sensitivity (positive = actually positive)
• Low specificity (negative = actually negative)
Brietzke et al. Otolaryngol Head Neck Surg 2004;131:827-32.

History
Positive predictive value below 1 èè Overdiagnosis of OSA
when compared to PSG
Brietzke et al. Otolaryngol Head Neck Surg 2004;131:827-32.
History
• A “positive” history is very reliable
– BUT cannot tell you the severity
• A negative history is NOT very reliable
– Poor quality – How much are the parents
observing?
– If the risk/consequences are high – will need
to use objective testing
– This includes post-operative patients
Limitations of the History
Oto Peds Sleep Caregiver reports of
snoring, witnessed
apnea or other nocturnal
symptoms may be
unreliable if the
caregiver does not
directly observe the
child while sleeping or
only observes the child
early in the evening
the sensitivity and
specificity of the history
and physical exam are
poor
Snoring and other
nocturnal
symptoms…showed
inconsistent
correlations with
respiratory parameters
of PSG
marquelrussell.com
Does it Matter?
Does it Matter?
Limitations of the Physical Exam
Oto Peds Sleep “tonsil size does not
predict the severity of
OSAS”
“the size of the tonsils
cannot be used to
predict the presence of
OSAS in an individual
child”
“The task force found
that clinical evaluation
alone does not have
sufficient sensitivity or
specificity to establish a
diagnosis of OSAS”
• Association between subjective pediatric
tonsil size (0 to 4+) and PSG OSA Severity
– Weak at best
• Conclude subjective tonsil size has
limitations for clinical decision making
01
02
03
04
0
1 2 3 4Tonsil_Size
Spearman's rho = 0.0282
Test of Ho: preop_rdi and
tonsil are Independent
Prob > |t| = 0.8847
28
• Based on physical examination
• Preliminary Data
Tonsillar Staging
Tonsil
Grade
Description
Grade 0 No Tonsils
Grade I 0-24% Filling oropharynx
Grade II 25-49%
Grade III 50-74%
Grade IV 75-100%
29
Modified Mallampati Staging
30

31
Results- Pre and Post Surgical RDI
32
0
5
10
15
20
25
30
1 2 3 4
Avera
ge R
DI
Friedman Staging System
Post-Surgical Improvement in RDI
Pre-Op RDI
Post-Op RDI
Percent Surgical Success
33
0
20
40
60
80
100
1 2 3 4
Perc
en
t S
uccess
Friedman Staging System
Percent Surgical Success
Alternatives to PSG
Oto Peds Sleep “Laboratory-based PSG
remains the gold
standard for the
diagnosis of OSA in
children….the panel
recommends against the
routine use of PM over
in laboratory PSG”
RECOMMENDATION
“If PSG is not available,
then clinicians may order
alternative diagnostic
test such as nocturnal
video recording,
nocturnal oximetry,
daytime nap PSG, or
ambulatory PSG ”
OPTION, GRADE C
“Nap (abbreviated) PSG
is not recommended
for the evaluation of
OSAS”
OPTION
*Separate statement
paper on portable
monitors recommends
against use in children
glimpseofpeace.blogspot.com
Adenotonsillectomy
Oto Peds Sleep “Clinicians should
counsel caregivers about
tonsillectomy as a means
to improve health in
children with abnormal
PSG who also have tonsil
hypertrophy and sleep
disordered breathing”
RECOMMENDATION,
GRADE C
“If a child has a clinical
examination consistent
with adenotonsilar
hypertrophy, and does
not have a
contraindication to
surgery, the clinician
should recommend AT as
the first line of
treatment”
RECOMMENDATION,
GRADE B
“Adenotonsillectomy
(AT) is commonly
performed as a first-
line treatment of OSAS
in children”
Adenotonsillectomy – healthy kids

Postoperative Followup
Oto Peds Sleep “Clinicians should
counsel caregivers and
explain that SDB may
persist or recur after
tonsillectomy and may
require further
management”
RECOMMENDATION,
GRADE C
“Clinicians should
clinically reassess all
patients with OSAS for
persisting signs and
symptoms after therapy
to determine whether
further treatment is
required.”
RECOMMENDATION,
GRADE B
“Children with mild
obstructive sleep apnea
syndrome pre-
operatively should have
clinical evaluation
following adeno-
tonsillectomy to assess
for residual symptoms.
If there are residual
symptoms of OSAS, PSG
should be performed. ”
STANDARD
nhstrategicmarketing.com
Persistent OSA after T&A
Oto Peds Sleep
No comments
“Clinicians should refer patients for CPAP
management if symptoms/signs (Table 2)
or objective evidence of OSAS persists
after adenotonsillectomy” RECOMMENDATION, GRADE C
“Clinicians may prescribe topical
intranasal corticosteroids for children
with mild OSAS in whom T&A is
contraindicated or for children with mild
postoperative OSAS”
OPTION, GRADE B
“PSG is
indicated for
positive airway
pressure (PAP)
titration in
children with
obstructive
sleep apnea
syndrome ”
STANDARD
Postoperative Monitoring
Oto Peds Sleep “Clinicians should admit
children with OSA
documented in results of
PSG for inpatient,
overnight monitoring
after tonsillectomy, if
they are under age 3
years or have severe
oxygen saturation nadir
less than 80%, or both”
RECOMMENDATION,
GRADE C
“Clinicians should
monitor high-risk
patients (Table 5)
undergoing
adenotonsillectomy as
inpatients post-
operatively”
RECOMMENDATION,
GRADE B
“PSG is indicated for
positive airway
pressure (PAP) titration
in children with
obstructive sleep apnea
syndrome ”
STANDARD
Should They Stay or Should They Go?
Obvious cases
• 3 or under, prematurity
• Obese
• Craniofacial Syndromes
• “Severe” disease
• Failure to thrive
www.rorycoplin.com
Oto Recommendations
• PSG for SDB in children in whom the need
for surgery is uncertain or discordance
between tonsillar size and severity of SDB
• Communicate PSG results to anesthesia
Non-CPAP therapies in obstructive sleep apnoea. Eur Respir J. 2011 May; 37(5):1000-1028.
Oto Recommendations
• Admit children with OSA if:
– < 3 years
– AHI>10 events/hour
– Oxygen saturation nadir <80%
Non-CPAP therapies in obstructive sleep apnoea. Eur Respir J. 2011 May; 37(5):1000-1028.

AAP Recommendations
• Admit children with OSA if:
– < 3 years
– AHI≥24 events/hour
– Oxygen saturation nadir <80%
– Peak end tidal CO2 >60mmHg
Marcus C et al. Pediatrics. 2012; 130:576.
Putting the Puzzle Together….
• Clinical Evaluation
– Verify the quality of the history
– Remember that the specificity is low
– Get a 3D impression of the tonsils (gag)
allthingsd.com
Putting the Puzzle Together….
• Use of PSG
– Diagnostic uncertainty
– Higher operative risk
• Bleeding dyscrasia
• Malignant hyperthermia
allthingsd.com
Putting the Puzzle Together….
• Pros of PSG
– Recognize nonobstructive disease to avoid surgery
– Negative study allow high risk children to defer or
delay surgery
– Baseline to compare with future results
– Assist with perioperative planning – admission,
cardiac evaluation, preoperative CPAP, opioids
procondebaters.wordpress.com
Putting the Puzzle Together…. Cons of PSG
• High cost
• Limited availability
• Delay in treatment
• Does not change admission for high-risk children
copyfight.corante.com
• Post-op Monitoring
– Outpatient with observation period
• 2 vs 4 hours as a minimum
– Inpatient
• 3 or under (10 kg), history of prematurity
• Obese, craniofacial syndrome, neuromuscular
Putting the Puzzle Together….
allthingsd.com

• Post-op PSG
– When there is any doubt
• Persistent symptoms of SDB/OSA
– High risk for persistent OSA
• Obesity
• Down’s Syndrome …
Putting the Puzzle Together….
dchawks.com 50
Management of
Persistent Pediatric OSA
Options
• Non-surgical treatment
– Weight loss/Sleep Hygiene
– Pharmacotherapy
– Palate expansion/Dental appliances
– CPAP
• Surgical treatments
– Adenoidectomy
– Tonsillectomy vs. tonsillotomy
– Nasal treatments
– Tongue/tongue base procedures
Non-surgical modalities
– Weight loss
– Sleep hygiene
– Pharmacotherapy
– Oral appliances/Rapid Maxillary Expansion
– Nasal continuous positive airway pressure
Medical Weight Loss
• 10yr Counseled behavior & dietary approach • 34% had 20% weight loss • 30% were no longer obese
• Meta-analysis: 342 adults after surgery • BMI decreased 57.6 to 37.7 kg/m2
• AHI decreased 54.7 to 15.8 events/hour • Many still with moderate to severe OSA
• 34 adolescents • Mean weight loss 58kg • OSA in 19/34
– 10 underwent repeat PSG (9.1 to 0.7/hr) – resolved
Karla M et al. Obes Res 2005;13(7):1175-9.
Weight Loss
• Medical Weight loss (10-18yo; N=132) – 49 with SDB, 42 with RDI>2/hour (14>5/hr) – Overall Mean preop RDI=1.9 events/hr – 71% resolved with weight loss – 32% decrease in BMI
Hoorenbeeck K,et al. Obesity 2012;20(1):172.
Pretreatment SDB
ODI<2�
ODI�2-5�
ODI>5�

Weight Loss
• 5 Guidelines/Recommendations – 2007 Health Care organization 4 stage model
• Convened by AMA and CDC
– 2007 Canadian clinical practice guidelines
– 2008 Endocrine Society recommendations
– 2009 Obesity Management 7 step model
– 2010 U.S. Preventive Task Force recs
Kirschenbaum DS et al. J Consult Clin Psychol 2013, 81(2):347-60
Bariatric Surgery
• ASMBS best practice guidelines
– “mounting body of evidence supports the use of
modern surgical weight loss procedures for carefully
selected, extremely obese adolescents”
• BMI of 40 kg/m2 with other co-morbidities
– HTN, INS resistance, glucose intolerance, OSA with
AHI≥5, dyslipidemia, substantially impaired QOL/ADL
• BMI > 35 kg/m2 with major co-morbidities
– Type 2 DM, mod-svr OSA (AHI≥15),pseudotumor
cerebri, or severe NASH
Michalsky M, et al. Surgery for Obesity & Related Diseases 2012;8(1):1-7.
Bariatric Surgery
• Prospective trial (N=50)
– 14-18yo, BMI >35
– Medically supervised lifestyle vs gastric banding
– 2 years postoperatively
lifestyle surgery
Mean %EWL 13% 79%
Metabolic synd (B) 40% 36%
Metabolic syndr(2yr) 44% 0%
– Surgery group: 33% reop rate in 2 years
• Band slippage, pouch dilation, injury to port side tubing
Ibele AR, Mattar SG. Surgery Clin NA, (2011) 91(6) 1339.
Bariatric Surgery
• Prospective cohort study (N=226)
– 5-21 yo, BMI >35 kg/m
– Pre and post gastric sleeve
baseline 3yr
BMI (mean) 48 30
OSA present 43% 7% (15/16 improved)
Alqahtani AR. Surgery Obesity Related Dz. 2014;10:842.
Pharmacotherapy
• Steroids
–Oral Steroids – 5D trial (1mg/kg) – no reduction
–Nasal Steroids – 6 wk course in 25 pts – decreased RDI from 11 to 6/hr
Al-Ghamdi AS et al. Laryngoscope (1997) 107:1382-7.
Brouillette RT et al. J Pediatr (2001) 138:838-44.
Pharmacotherapy
• Leukotriene Modifiers
– Increased # leukotriene receptors in tonsils of
sleep apnea patient
– Demonstrated a specific topographic pattern of
expression
Goldbart AD et al. Chest (2004) 126:13-18.
Goldbart AD et al. AM J Resp Crit Care Med (2005) 172:364-70.

Leukotriene Modifiers
Montelukast daily use x 16 wks in 24 mild osa pts
• Improvement in hypercarbia and AHI
• Decrease in adenoid size
Goldbart AD. Pediatrics. 2012 Sep;130(3):e575-80.
Combo Montelukast/Nasal Steroid
Montelukast daily use x 12 wks in 752 mild osa pts
• Normalization PSG in 62%
• Less likely to work in children > 7 years or obesity
Kheirandish-Gozal L. Chest. 2014;146(1):88-95.
0
1
2
3
4
5
pretreatment
posttreatment
Oral Appliances
• Most effective in nonobese patients with retro or micrognathia
• Better for mild to moderate cases
• 20 healthy kids versus 20 with mild to moderate OSA – Reduced mandibular length – Overbite – Superior hyoid bone position – Smaller dental arch
Cozza et al. Eur J Orthod (2004) 26:523-30.
Evaluation for Surgery
• Physical examination • Cine MRI • Sleep endoscopy
Villa MP et al. Sleep Med. 2007;8(2):128.
Villa MP et al. Sleep Breath. 2011;15:179.
Cine MRI
• 2003 – 32 children with and without OSA
– Airway measurement/collapsibility differ
• 2004 – 15 children with Down Synd
– Relative macroglossia 74%
– Glossoptosis 63%
– Recurrent/enlarged adenoids 63%
– Enlarged lingual tonsils 30%
– Hypopharyngeal collapse 22%
• 2008/2010 – reproduced results
Lane F et al. Radiology. 2003;227:239.
Shott S et al. Laryngoscope. 2004;114(10):1724.
Guimaraes C et al. Ped Radiology. 2008;38:1062.
Schaaf WE et al. Am J on Roentgenology. 2010;194(5):120.
Cine MRI - Axial
Hypopharyngeal
collapse
Glossoptosis

Cine MRI
Indications for DISE
• Indications currently under debate
• Original papers focused on syndromic children
• Evolution to:
– Persistent pediatric OSA
– Children without obvious area of obstruction
– Children with significant comorbidities
– State-dependent laryngomalacia
• Anesthesia to approximate natural sleep
• Look at the dynamic movement of the
airway
• Use flexible laryngoscopy or bronchoscopy
Drug induced sleep endoscopy
• 1986 - Sher - syndromic children with PRS
– Reported Glossoptosis & pharyngeal collapse
• 1991 - Sleep endoscopy was described by Croft
and Pringle
Croft CB. Sleep nasendoscopy: a technique of assessment in snoring and obstructive sleep apnoea. Clin
Otolaryngol Allied Sci. 1991;16(5):504.
Sher A et al. IJPO. 1986;11(2):135.
Drug induced sleep endoscopy
Drug induced sleep endoscopy
• Then mentioned recently in pediatric
literature as a valuable tool in management
of persistent pediatric OSA by identifying
site of obstruction
Lin AC, Koltai PJ. Sleep Endoscopy in the Evaluation of Pediatric OSA. IJPO 2012; 2012:576719
DISE
• 2000 -2013
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
tongue base
supraglottic collapse
*
* *
*
* = persistent
OSA

Occult Laryngomalacia Severe OSA
Surgical Treatment Beyond T&A
– Adenoidectomy – revision
– Completion Tonsillectomy
– Palatal surgery (UPPP)
– Nasal surgery
– Maxillary expansion
– Tongue/tongue base procedures
– Supraglottoplasty
Adenoidectomy
– Long-term follow-up (3-5 years)
• Snoring 88%, Obstructed breathing 44%
– 32 no improvement /worsening • Adenoid hypertrophy seen in 50% (16/32)
– 174 with improved symptoms • 11% (20/174)
Joshua B. Otolaryngology–Head and Neck Surgery (2006) 135, 576.
Adenoidectomy
• Retrospective (n=48 sdb, 52 no sdb)
– Likelihood of future tonsillectomy or revision
adenoidectomy
– 38% with sdb underwent subsequent surgery versus
19% of those with nonobstructive
Brietzke S. Otolaryngology–Head and Neck Surgery (2006) 134, 979.
Tonsillotomy • Retrospective study
– 1,731 partial tonsillectomy group vs
– 1,212 patients traditional tonsillectomy
– Tonsillotomy
• Decreased posttonsillectomy hemorrhage (1.1% vs. 3.4%, p
< 0.001)
• Decreased severe pain or dehydration requiring medical
attention (3.0% vs. 5.4%, p = 0.002)
• 0.64% required revision completion tonsillectomy for
tonsillar hypertrophy
Schmidt R. Arch OtoHNS. 2007;133(9):925

Tonsillotomy
• Risk of tonsillar regrowth (0.5-17%):
– 17% (7/42) – Krespi – 1-10 year results (laser)
– 2-4% cited for symptomatic evaluation only
– Most studies with low numbers are 1 year follow-up
or less
– Risk factors for tonsil tissue recurrence ?
• Young age at the time of surgery
• Acute tonsillitis during the recovery period
Krespi YP. J Otolaryngol1994;23:325.
Celenk F. Int J Pediatr Otorhinolaryngol. 2008 Jan;72(1):19
UPPP
• UPPP proposed in neurologically impaired, obese
and Downs kids – All retrospective studies
– Nasopharyngeal stenosis at increased risk when
performed along with adenoidectomy
Kerschner JE. IJPO. 2002;62(3):229.
Kostko J. IJPO. 1995;32:241.
Nasal / Nasopharyngeal
• Nasal/Nasopharyngeal
– Adenoidectomy
– Nasal turbinate reduction
– Septoplasty – concern about nasal growth
Nasal Surgery
• Nasal obstruction = potential OSA contributor
• Several studies have shown that
– Nasal obstruction alone may cause or exacerbate
apnea in some children
– Children with turbinate hypertrophy are more likely
to have persistent OSA after T&A
• No data on treatment of nasal obstruction alone
for treatment of SDB in children
Morita T et al. Am J Otolaryngol. 2004;25(5):334-338.
Sullivan S, et al. Ann Acad Med Singapore. 2008;37:645-648.
Nasal Surgery
• Meta-analysis: Effect of nasal surgery on OSA
– Reduction 11 events/hour
Ishii L, et al. OtoHNS. 2015; Epub ahead of print.
Nasal Surgery
• Randomized, controlled trial on effect of RF turbinate
ablation on NAO in adults
– Improves NAO and nasal CPAP compliance
• ? Consider nasal turbinate reduction routinely in
children with inferior turbinate hypertrophy
• ? Wait as turbinate hypertrophy noted to be commonly
improved after adenoidectomy & suggests that many
will benefit from adenoidectomy alone
Powell NB, et al. Laryngoscope. 2001;111(10):1783-1790.
Nasal Turbinate Reduction
• Nasal turbinate reduction
– Retrospective case review
– 28 T&A, 23 with T&A/Turb
With Turbinate Reduction Without Turbinate Reduction
Preop Postop Preop Postop p
AHI 15.6 (5.2-28) 0.8 (0.2-1.6) 15.0 (5.4-26) 3.5 (0.5-4.6) <0.01
Min Sat 84 (76-94) 94 (92-97) 83 (75-92) 93 (91-96) <0.05
Min xsec area 0.16 (0.08-0.24) 0.31 (0.25-0.37) 0.15 (0.05-0.26) 0.16 (0.07-0.27) <0.01
Cheng PW. Laryngoscope. 2012 Oct 15
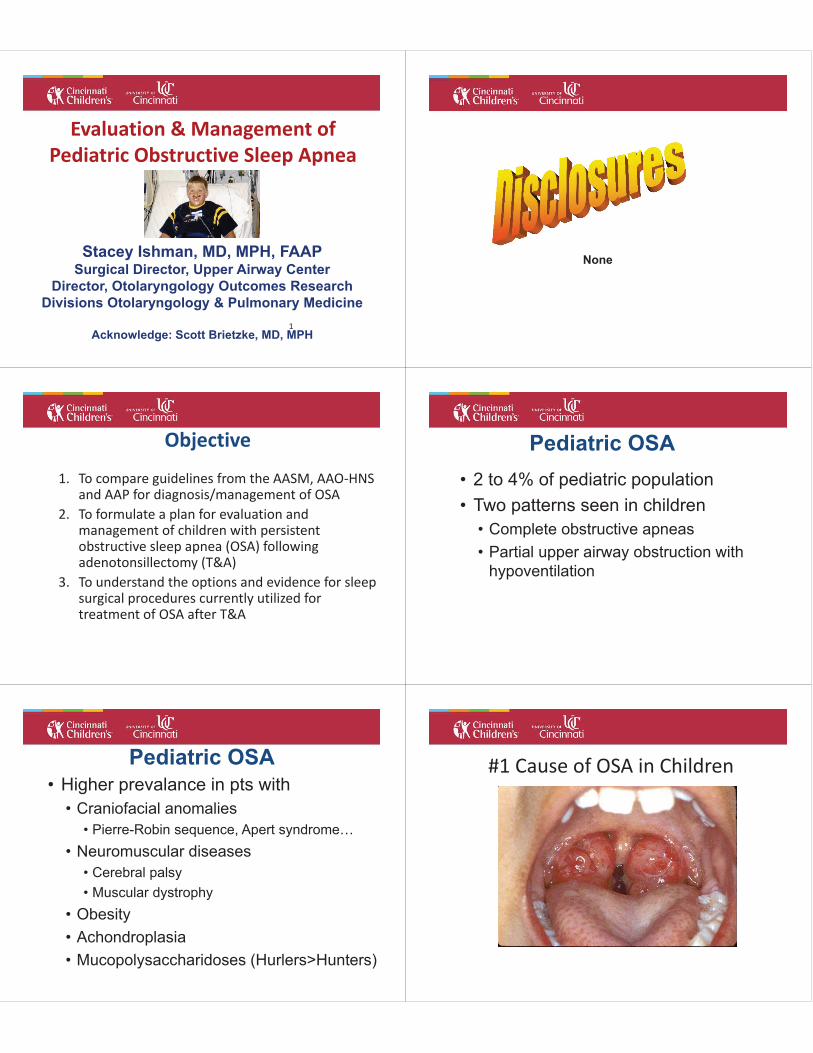
Rapid Maxillary Expansion
• Device fitted to the molars with expansion of the maxilla
• Carried out over 12 months or less
http://www.orthopraxis.gr/?p=29&lang=en
Rapid Maxillary Expansion
• 2006 – Study of 14 children – Snoring & AHI reduced ( 5.8 to 1.5 events/hr) – Daytime symptoms (sleepiness, tiredness, and oral
breathing) significantly improved – Mean expansion
• 3.7 0.7 mm for the intercanine • 5.0 2.2 mm for the inter pre-molar
• 2011 – Follow-up of 10/14 – Repeat PSG in 12 and 24 months – 24 months later, improvement in AHI and clinical
symptoms persisted
Villa MP et al. Sleep Med. 2007;8(2):128.
Villa MP et al. Sleep Breath. 2011;15:179.
Rapid Maxillary Expansion
• 2004 –31 children (4 month followup ) – 10-20 day expansion; 6-12 months of consolidation – AHI reduced ( 12.2 to <1 events/hr) – Mean expansion
• 3.9 0.3 mm for the intermolar • 3.0 0.2 mm for the interincisive
Pirelli P et al. Sleep. 2004;27(4):761.
Procedures
• Tongue/Tongue Base
– Macroglossia
– Lingual tonsillectomy
– Glossoptosis, tongue base obstruction treatment
including surgery
• Tongue suspension suture
• Radiofrequency ablation
• Hyoid suspension
• Partial Midline Glossectomy
• Genioglossal advancement
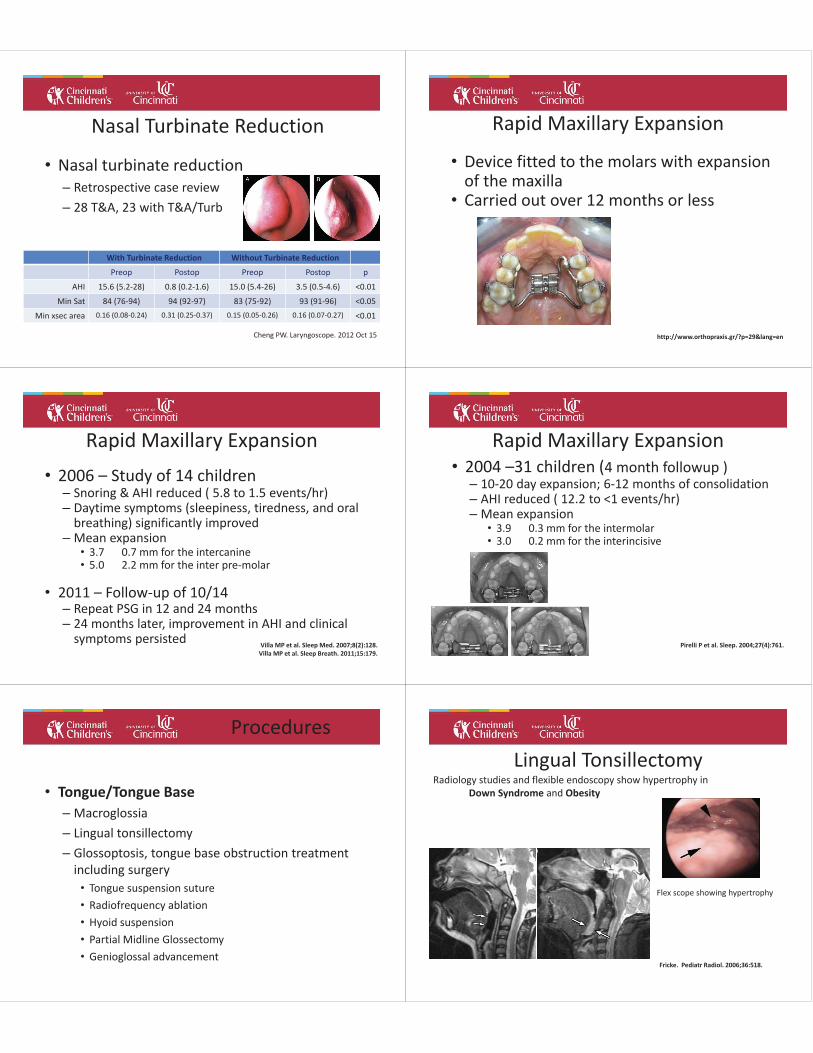
Lingual Tonsillectomy
Fricke. Pediatr Radiol. 2006;36:518.
Radiology studies and flexible endoscopy show hypertrophy in
Down Syndrome and Obesity
Flex scope showing hypertrophy

Lingual Tonsillectomy
Manickam et al. Laryngoscope. 2015; Epub ahead of print.
Author N Mean age Resolution O2 Sat
pre/post
AHI
pre/post
Abdul-Aziz 16 NR 68% 84/91 10.5/3.2
Chen 68 11 57% 89/91 11.8/5.7
Truong 31 7 NR NR 18.3/9.7
Lin 26 11 61% 89/90 14.7/8.1
Wootten 9 9 66% 83/84 8.5/4.1
Tongue Suspension Suture • Case reports showing variable success
• Wooten/Shott -2010 - 31 patients – with RFA BOT
•Mean age = 11 years; 9/31 Downs
•Success = 61% (66% no DS)
Radiofrequency Ablation
•Safety with tongue lymphatic malformation
•Study combined with tongue suspension
•Meta-analysis in adults •Mean treatments = 4.3 (2.4-5.5 range)
•Long-term changes
• ESS 32% reduction at 24m (OR 0.68, .43-.73)
• RDI 45% reduction at 24m (OR .55, .45-.72)
Farrar. Laryngoscope. 2008;118:1878.
Partial Midline Glossectomy
•Submucosal lingual excision (SMILE) •Pediatric cadaver studies only
•Endoscopic guidance with coblation
•Equivalent to RF BOT – 55% change in AHI (2008)
•RCT: UPPP with 1)RF vs 2)SMILE-RF vs 3)SMILE-harmonic
Babademez et al. OtoHNS. 2011;145(5):858.
Friedman M. Oto HNS. 2008;139:378.
Maturo SC. Ann Otol Rhinol Laryngol. 2006 ;115(8):624.
Partial Midline Glossectomy •PMG – Clark/Shott – 2011 ASPO
•22 Patients
•Success in 59%
•Current treatment protocol includes PMG with
tongue suspension if needed
Shott S. Curr Opin Otolaryngol Head Neck Surg. 2011 Dec;19(6):449.
Supraglottoplasty after T&A
Manickam et al. Laryngoscope. 2015; Epub ahead of print.
Author N Mean age Resolution O2 Sat
pre/post
AHI
pre/post
Chen 24 7 56% 88/89 14.9/4.9
Chen & Truong 9 NR NR NR 10.4/2.9
Truong 8 NR NR NR 9.7/5.7
Digoy 36 5 72% 83/87 13.3/4.1
Additional Procedures
•Genioglossal advancement •Pediatric case reports
•Adults - 70% reduction in RDI • With multiple adjunctive procedures
•Consider older kids with well-developed mandible
•Mandibular & craniofacial procedures •Tongue-lip adhesion
•Mandibular distraction osteogenesis
•Tracheostomy Miller FR. Oto HNS. 2004;130:73.
Procedures
••
•
Other Procedures
• Tracheostomy
– Highly effective
– Useful in kids with multiple
levels of obstruction or
neurologic impairment
– Increased risk of
perioperative complications COMPLICATIONS
Respiratory
1992 – 69 pts – 16 (23%) with complications
• Retrospective chart review
• Complications associated with:
– Younger than 3
– Severe OSA
– Weight <5%ile
– Craniofacial abnormalities
• Recommended hospitalization postop for all
McColley SA et al. Arch OtoHNS. (1992) 118(9):940.
Complications
Respiratory
1994 – 37 pts – 10 with complications
• Retrospective chart review
Rosen G et al. Pediatrics. (1994) 93(5):784.
Complications

Respiratory
1994 – Recommended selected admission after T&A
Rosen G et al. Pediatrics. (1994) 93(5):784.
Complications
Effect of Anesthesia on Sleep
1988– 8 healthy volunteers (20s)-isoflurane (3hr)
• Reduction in slow-wave sleep first night
• Sleep after surgery is low in REM and slow-wave sleep
• Poor sleep in the immediate postoperative period
– Analgesic drugs
– Pain
– Environmental noise
– Disturbance by nursing interventions
– Anxiety in unfamiliar environment
Moote CA, Knill RL. Anesthesiology. (1988) 69:327.
Complications
Sleep after T&A
2005– PSG 1st postop night after T&A for OSA (N=10)
– 5 mild OSA (1-10 events/hr)
– 5 severe OSA (>10 events/hr)
Nixon G et al. Ped Pulm. (2005) 39:332.
Complications
All 3 to 5 years old
Sleep after T&A 2005– PSG 1st postop night after T&A for OSA (N=10)
Nixon G et al. Ped Pulm. (2005) 39:332.
Complications
preop
1st night postop
6 weeks postop
Analgesic Sensitivity in OSA
2004– Age and preoperative sat nadir correlated with total opioid dose (N=46)
Brown K et al. Anesthesiology. (2004) 100:806.
Complications
Mean age = 43±19 months
Analgesic Sensitivity in OSA
2006– Children with preoperative sat nadir <85% required ½ opioid after surgery than those ≥85% (N=22)
Concluded: Recurrent hypoxemia in OSA associated with increased opioid sensitivity
Brown K et al. Anesthesiology. (2006) 105:665.
Complications
Mean age = 43±19 months

Postoperative Pain Management
2006– Children with preoperative sat nadir <85% required ½ opioid after surgery than those ≥85% (N=22)
Concluded: Recurrent hypoxemia in OSA associated with increased opioid sensitivity
Brown K et al. Anesthesiology. (2006) 105:665.
Complications
Mean age = 43±19 months • Morbidly obese 13yo with sleep apnea
• T&A, UPPP and SMR turbinate resection 12/9/13
• Planned admission to the PICU
• Severe bleeding, transfusions
• Cardiac arrest & anoxic brain death
• Declared dead POD3 - eval that included 2 EEG
• Goldman et al. 2013 M&M after T&A
– AAO newsletter, 552 respondents
– 51 mortalities reported
• 4 with anoxic brain injury
Sales
Pediatric
Adult
Unknown
• Goldman et al. 2013 M&M after T&A
–Mechanism
• Medication 22%
• Pulmonary/CV factors 20%
• Hemorrhage 16%
• Perioperative events 7%
• Progression of underlying disease 5%
• Unexplained (All but 1 outside) 31%
• Goldman et al. 2013 M&M after T&A
– Preop OSA dx NOT associated with increased risk of
death or anoxic brain injury
– Timing
• 55% in the first 2 days after surgery
– Events unrelated to bleeding accounted for the
preponderance of deaths & anoxic brain injury
• Hill, Hartnick et al. 2011 Risk factors for airway
complications in T&A for severe osa
– N=83 with AHI>10 – all admitted
– Major complications – 4.8%
• Increased level of care
• CPAP/BIPAP use
• Pulmonary edema
• Reintubation
– Minor Complications – 19.3%
• Oxygen sat < 90%
Hill et al. IJPO. 2011;75(11):1385.

• Hill, Hartnick et al. 2011 Risk factors for airway
complications in T&A for severe osa
– Independent predictors of complications
• Age < 2 years
• AHI >= 24 events/hour
• Intraop laryngospasm requiring treatment
• Oxygen sats <90% on RA in PACU
• PACU stay > 100 mins
– Any of these factors – 38% complications (vs 2%)
Hill et al. IJPO. 2011;75(11):1385.
• Dalesio, Smith, Ishman et al.
– CO2 driver of complications
– Unadjusted Modeling
• Sat nadir 0.0096
• Peak CO2 < 0.001
– Adjusted model
• Age significant and correlated with sat nadir/peak CO2
• ? Confounder of the relationship between CO2 and
complications
• Dalesio, Smith, Ishman et al.
– CO2 driver of complications
– Unadjusted Modeling
• Sat nadir 0.0096
• Peak CO2 < 0.001
– Adjusted model
• Age significant and correlated with sat nadir/peak CO2
• ? Confounder of the relationship between CO2 and
complications
• Gaps:
– Who needs to be admitted?
– What level of admission is necessary?
• Floor, ICU, stepdown
– What is appropriate and safe pain control in these
children?
#8
Thank You Stacey Ishman, MD, MPH
Surgical Director, Upper Airway Center
Multidisciplinary Treatment of Children with
Persistent Sleep Apnea