Embed Size (px)
Citation preview

Sarah Lawrence College Sarah Lawrence College
DigitalCommons@SarahLawrence DigitalCommons@SarahLawrence
Human Genetics Theses The Joan H. Marks Graduate Program in Human Genetics
5-2017
Evaluating FRAME (Faces Redefining the Art of Medical Evaluating FRAME (Faces Redefining the Art of Medical
Education) videos: The impact of digital storytelling on medical Education) videos: The impact of digital storytelling on medical
students’ attitudes to disability and their learning preferences students’ attitudes to disability and their learning preferences
Shreya Malhotra Sarah Lawrence College
Follow this and additional works at: https://digitalcommons.slc.edu/genetics_etd
Part of the Genetics Commons
Recommended Citation Recommended Citation Malhotra, Shreya, "Evaluating FRAME (Faces Redefining the Art of Medical Education) videos: The impact of digital storytelling on medical students’ attitudes to disability and their learning preferences" (2017). Human Genetics Theses. 38. https://digitalcommons.slc.edu/genetics_etd/38
This Thesis - Open Access is brought to you for free and open access by the The Joan H. Marks Graduate Program in Human Genetics at DigitalCommons@SarahLawrence. It has been accepted for inclusion in Human Genetics Theses by an authorized administrator of DigitalCommons@SarahLawrence. For more information, please contact [email protected].

EvaluatingFRAME(FacesRedefiningtheArtofMedicalEducation)videos:The
impactofdigitalstorytellingonmedicalstudents’attitudestodisabilityand
theirlearningpreferences
May8th,2017
ShreyaMalhotra
JoanH.MarksGraduatePrograminHumanGenetics
SarahLawrenceCollege
SubmittedinpartialcompletionoftheMasterofScienceDegreeatSarahLawrenceCollege,May2017

ABSTRACT
FRAME(FacesRedefiningtheArtofMedicalEducation)isaweb-basedplatformcreatedby
PositiveExposure,anon-profitorganization.FRAMEusesdigitalstorytelling(DST)by
presentingshorteducationalfilmsandimagegalleriesaimedtohelphealthcare
professionalsandstudentsgainanunderstandingofgeneticconditionsanddisability.
Familiesdemonstratehallmarkcharacteristicsinthecontextofastorytomakethevideo
educationalandtruetolife.Thepurposeofthisstudywastoevaluatetheeffectivenessof
FRAMEvideosfor22q11.2deletionsyndrome(22q11.2DS)andfamilialdysautonomia(FD)
inimprovingstudents’attitudesaboutdisability.Fourthyearmedicalstudentswere
recruitedbyemailfromthreeaccreditedU.S.medicalschools.Participantswererandomly
promptedtoreadaboutoneoftwoconditionsonMedscapeandthencompletethe
AttitudestoDisabilityScale(ADS),avalidated16-itemsurvey.TheywatchedtheFRAME
videoonthesameconditionandcompletedtheADSagain.Participantscompletedasurvey
toexplorelearningpreferencesandgatherfeedbackonthevideos.48outof549medical
studentsparticipatedinthestudy(FDn=27,22q11.2DSn=21).Significantattitude
improvementswerefoundintheInclusion,Discrimination,PositiveGainsandCurrent/Future
HopessubscalesoftheADSforthe22q11.2DSvideoandinthePositiveGainssubscalefor
theFDvideo.ThemajorityofparticipantspreferredtheFRAMEvideoforlong-termretention
(FD88%,22q11.2DS86%).Mostparticipants(FD85.7%,22q11.2DS86.4%)agreedor
stronglyagreedtheFRAMEvideogavetheminsightintolivingwithadisability.Forty-two
students(87.5%)agreedorstronglyagreedtheylearnbestwithaudio,visualandtext
resources.TheresultssuggesttheFRAMEvideosimprovedmedicalstudents’attitudes
relatedtomultipleaspectsofdisabilityassociatedwith22q11.2DSandaspecificaspectof
disabilityassociatedwithFD.OurstudyshowsDSTisaneffectivewaytoimprovemedical
students’attitudestowardsindividualswithgeneticconditionsanddisabilities.
KEYWORDS:digitalstorytelling,medicaleducation,AttitudestoDisabilityscale,genetic
conditions

INTRODUCTION
Patient-centeredapproachestohealthcarehavebeenincreasinglyemphasizedwith
theadventofthemedicalhumanities,afielddevelopedinthe1970sfollowingthe
realizationthatmedicaleducationmaynotbeadequateenoughtoteachunderstandingof
humans(Macnaughton,Mbchb,&Drcog,2015).Patientnarrativesarestories,literature,
moviesandothermediaformsthatexploretheexperienceofillness(Kumagai,Murphy,&
Ross,2009).Theadditionalmeritsofpatientnarrativesarestimulationofcriticalthinking
(Cox,2001),linkagebetweentheoryandpractice(Koenig&Zorn,2002)anddevelopment
ofempathy,culturalsensitivityandtolerance(Kirketal.,2013)
PositiveExposure,foundedin1997,isanon-profitorganizationwhichutilizes
photographyandvideototransformpublicperceptionsofpeoplelivingwithgenetic,
physical,cognitiveandbehavioraldifferences.OnecomponentofPositiveExposureisthe
FRAMEproject(FacesRedefiningtheArtofMedicalEducation).FRAMEisaweb-based
platformthatpresentsaseriesofshorteducationalfilmsandphotographicgalleries
designedtohelphealthcareprofessionalsandstudentsgainanunderstandingofgenetic
conditionsanddisabilitieswhilemodelinganattitudeofrespectforthehumanityofthe
patients(Guidotti,n.d.).Eachcondition’swebpagealsoincludesaseparateslideshowof
theinformationaltextandalinktoanationwidesupportgroup.Thepatientsandtheir
familiesintroducethemselvestoviewersanddemonstratehallmarkcharacteristicsinthe
contextofastorymakingthevideoeducationalandtruetolife.Anotherintentionofthis
formatisforindividualswithgeneticconditionstoformpartnershipswiththehealthcare
communityandconnectwithaudiencesworldwide.TheFRAMEfilmsrepresentashiftin
medicinefromatraditionalcurriculumtooneinwhichthereisanapplicationofnarrative
medicineandautilizationoftechnologyinthetrainingofmedicalprofessionals.
TheAssociationofAmericanMedicalColleges(AAMC)createdaGroupofDiversity
andInclusion(GDI)toinformandguidetheadvancementofdiversityandinclusionthrough
academicmedicineandthecommunity(Poladian,2013).Thereisa“CultureofDisability”

thatissubjecttostereotypes,prejudicedattitudesandinstitutionalbarriers(Eddy&Robey,
2005).Patientswithchronicdisabilitiesoftenperceivealackofsensitivityamongphysicians
duringclinicalencounters(Sabharwal,2001).Moreover,theOfficeofSurgeonGeneral
reportspeoplewithdisabilitiesciteashortageofprovidertrainingaboutthedailyrealities
oflivingwithadisability(Brown,Graham,Richeson,Wu,&McDermott,2010).Inadequate
preparationofdoctorsmayleadtonegativeperceptionsofthesepatientssuchastheyare
timeconsuming,difficulttorelateto,poorlyinsuredandaremedicallyandsociallycomplex
(Woodward,L.,S.M.,Zwygart,&Perkins,2012).
Thesefindingshighlighttheimportanceofdisabilityrelatedtrainingatalllevelsof
healthcareeducationandpractice(Minihan,Robey,&Long-Bellil,2011).Thereisaneedto
explorealternativestrategiesforprovidingstudentswithinsightintothelivesofpeople
withdisabilitiessotheycanbemorecomfortableprovidingmedicalcare.
TheAAMChasrecognizedgeneticsasoneofthecontemporaryissuesinmedicine
(Medical,Society,Genetics,&Genetics,2008).TheAmericanSocietyofHumanGenetics
(ASHG)andtheAssociationofProfessorsofHumanandMedicalGenetics(APHMG)
developedamedicalschoolcompetencybasedcorecurriculumtoprovideguidance
regardingmedicalgeneticsknowledge,skillsandbehaviorsallcurrentmedicalstudentswill
needduringtheircareers.(Medicaletal.,2008)
Medicalstudentsareexpectedtoaccomplishaseriesofknowledgeandattitudes
basedskillsthatassistinthediagnosis,preventionandtreatmentofgeneticdiseases.An
underlyingthemeofthecompetenciesincludestheneedforpsychosocialskillsbecause
geneticconditionsrequirefamilycenteredcareandsupportivecounseling.Therefore,
studentsmustbecomfortablemaneuveringsensitiverelationshipsinacollaborative
manner(Medicaletal.,2008).Additionally,geneticspresentsuniqueethicalissuesin
genetictesting,releaseofinformationanduniquepsychologicalissues.Theabilityto
empathizewithpatientsandunderstandtheneedforprivacyiscrucialtoasuccessful
doctor-patientrelationship.
Manynon-geneticistphysicianshaveminimaldirectprofessionalexposureto
geneticconditionsandthusalimitedunderstandingofitsimpactonthelivesofpatients

andtheircaregivers(Kirklin,2003).OnesolutionhasbeenawebsitecalledTellingStories,
UnderstandingRealLifeGenetics(www.tellingstories.nhs.uk)whichfeaturesover100
storiesintextandvideoformats.Thesestoriesaresortedby11themes,whichinclude
professionalcompetenciesandlearningoutcomes,geneticconditions,inheritancepattern
andgeneticintervention.Thiswebsiteisuniquebecauseitlinksthestorytoaprofessional
practicethroughaUKgenetic-genomicseducationframework(Kirketal.,2013).
TheresourcewasevaluatedbythenetworkofnurseeducatorsattheNHSNational
GeneticsEducationandDevelopmentCentreandtwoe-learningspecialists(thedelegates).
Thequalitativefeedbackwasencouraging.Positiveaspectsofthisresourceincludedtheuse
ofstoriestolinktheoryandpracticeandthatthestoriesareavailableinmultipleformats.
Thisstudydemonstratesthevalueincreatingaweb-basedresourceforhealthcare
professionalstouseattheirleisure.Additionally,thestudyhighlightsthemeritsinusing
patientstotransmitknowledge(Kirketal.,2013).Theliteraturesuggeststheuseofpatient
narrativemaybeawaytoincreaseexposuretoconditionsforarangeofhealthcare
professionalsandstudents.
Inthisstudy,weaddressedthefollowingquestions:1)DoestheFRAMEapproachto
medicaleducationimprovestudents’attitudessotheycancultivateasenseofrespectand
compassionforindividualswithdisabilitiesand/orgeneticconditions?2)Domedical
student’slearningpreferencesfavortraditionaltext-basedmethodsortheFRAMEapproach
ofdigitalstorytelling?Inaddition,weaskedparticipantstoprovidefeedbackfortheFRAME
videotodeterminestrengthsandareasofimprovementforfuturedevelopmentofthe
platform.
MATERIALSANDMETHODS
EthicalConsiderations
TheSarahLawrenceCollegeInstitutionalReviewBoardapprovedthestudyforexpedited
review(#00009775)onDecember5th,2016.
Sample
FourthyearmedicalstudentsatselectmedicalschoolsaccreditedbytheLiaison

CommitteeonMedicalEducation(LCME)wereeligibletoparticipate.Theparticipantpool
consistsofstudentsfromthreedifferentmedicalschoolsacrosstwostates,IowaandTexas.
TheseschoolswereselectedbecausetheyareestablishedcontactsofPositiveExposure.
Fourthyearstudentswerechosensincetheyhaveestablishedlearningpreferencesand
havecompletedamajorityoftheirclerkshipsintheprimaryspecialties.
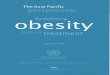
Methods(figure1)
RecruitmentbeganinDecember2016by
contactingrepresentativesatsevengeographically
diversemedicalschoolstorequestthedistributionof
emailinvitationstofourthyearmedicalstudents.The
recruitmentemailincludedalinktotheconsentanda
descriptionofthestudy.Threemedicalschoolsagreed
toforwardtherecruitmentemailtothefourthyear
class(N=549).Thefirstrecruitmentemailwas
forwardedinJanuary2017andtheparticipating
medicalschoolsdidnotsendmorethantworeminders
totheclassaftertheinitialrecruitmentemailwas
forwarded.Thesurveyswereactiveuntiltheendof
February2017.
MedscapeEducation
Afterconsenting,participantsbeganthestudy
activitybyclickingonalinktoaMedscapewebpage
about22q11.2DeletionSyndrome(22q11.2DS)or
familialdysautonomia(FD).Participantswere
randomlyassignedoneoftwoconditions.Thestudents
didnothavepreviousknowledgeaboutwhich
conditionswereincludedinthestudy.Theywere
promptedtotake5-10minutestoreadaboutthe
syndromeinMedscapeasiftheywerepreparingto
EmailtocontactsatselectLCMEaccreditedUSmedical
schools
Contactsdistributeemailstudyinvitationto4thyearmedial
students
Medicalstudentsreviewconsentand,ifagree,clicklink
tobeginstudy
Randomizedto22q11.2deletionsyndromeorfamilial
dysautonomia
ReviewinformationaboutconditiononMedscape
Pre-ADS
WatchFRAMEvideoaboutcondition
Post-ADS
EvaluationofLearningActivity
Linktoe-giftcard
Figure1:Summaryofstudyactivities

assistinthecareofapatientwiththatconditionthenextday.Theyweregivennoguidance
onwhichtopicstospecificallyfocusonduringthisstudyactivity.Thepromptwas
intentionallyvaguetoreplicatetheindividualprocessthatmedicalstudentsusetolookupa
diseaseinpreparationforapatientencounter.Medscapeisthemostaccessiblepoint-of-
carereferenceavailabletohealthcareprofessionalsontheinternet.Itisprimarilytext
basedwithafewimagesofthehallmarkclinicalfeatures.
BaselinescoresAttitudestoDisabilitiesscale(ADS)
AfterreviewingtheMedscapewebpageoneitherFDor22q11.2DS,participants
completedtheAttitudestoDisabilityScale(ADS).Theywerepromptedtothinkabout
disabilityandpeoplewitheitherFDor22q11.2DSwhilecompletingthequestions.Formost
ofthequestionsinthescale,thephrase“peoplewithdisabilities”wasreplacedwith
“peoplewithfamilialdysautonomia”or“peoplewith22q11.2deletionsyndrome”
dependingonwhichdiseasetheyreadaboutinMedscape.Thegoalwastoassessthe
medicalstudents’attitudestowardsdisabilityonlyasitrelatestothegeneticconditionthey
learnedaboutonMedscape.
FRAMEVideoandpostvideoADSscores
AftercompletingabaselineADS,participantswatchedaFRAMEvideoonthesame
diseasetheyresearchedonMedscape.ThecontentforFRAMEvideosaredecidedbya
teamofgeneticcounselorsandmedicalprofessionals.ThereweretwoFRAMEvideos
chosenforthisstudy,onefor22q11.2deletionsyndromeandoneforfamilialdysautonomia
(FD).Thesegeneticdisorderswereselectedbecauseaffectedindividualsexhibitphysical
andintellectualdisabilities.Additionally,tominimizepriorknowledgeofoneofthe
conditions,theresearchteamchosefamilialdysautonomiawhichisararergeneticdisease.
Eachvideowasbetween9-10minuteslongtomatchthetimeparticipantswereinstructed
tospendonMEDSCAPE.Atminimum,thevideosincludepatientsandfamilymemberswho
presentinformationaboutgeneticetiology,clinicalfindings,pathophysiologyandgeneral
managementofthecondition.Afterwatchingthevideo,participantscompletedasecond
ADSsurvey.

VideoEvaluationSurvey
Thefinalportionofthestudyincludedcompletingthevideoevaluationquestions.
Eachparticipantwasoffereda$10e-giftcardfortheirparticipation.
Measures
Informationwascollectedthroughaself-administered,voluntaryandanonymous
46-questionsurveyonSurveyMonkey.Itemsinthesurveywerebasedareviewofthe
literature,whichidentifiedmethodstomeasureattitudestowardsdisabilitiesandto
evaluatemultimedialearningtools.Participantshadthefreedomtoskipanyquestions.
1.TheAttitudestoDisabilityScale(ADS)generalversion(seeAppendixA):Thisisa16-item
scaleusedfortheassessmentofattitudestodisabilityandqualityoflifeacrosstheadult
lifespan.TheADScanbeusedtoassessattitudesinphysicallyandintellectuallydisabled
groups.Comparedwithexistingscales,theADSincludesmoreaspects,suchasprospects
andhopes.Additionally,thisisthefirstscaletohavecross-culturalvalidityalongwith
directlydrawingonattitudesandexperiencesofindividualslivingwithdisabilities(Power&
Green,2010).ADSuseda5pointLikertScaleforeachitem(1=stronglydisagreeand5=
stronglyagree)andfocusesonfourdifferentaspectsofdisabilities(Power&Green,2010)
I. Subscale1:Issuesofinclusionandexclusionandburdenonfamiliesandsociety.
II. Subscale2:Issuesrelatedtodiscrimination
III. Subscale3:Reflectspositivegainstoselfandtoothers
IV. Subscale4:Currentandfuturehopesandprospectsandwhetherornotdisability
hasanimpactonthem
2.VideoEvaluationSurvey(seeappendixB):Thisisa9-itemquestionnairedevelopedbythe
researchteam.ThepurposeofthissurveyistoevaluatetheFRAMEvideoandto
understandwhetherlearningpreferencesfavorMedscapeortheFRAMEapproachofdigital
storytelling.
Subscale1:Retentionofinformationandlearningstyles
RetentionoftheFRAMEvideowasmeasuredthroughtwoquestions.Thefirstused
aLikertscaletoassesslikelihoodofparticipantsrememberingtheFRAMEvideo.Thesecond

questionaskedparticipantstopickwhichlearningapproach(FRAMEorMedscape)allows
forlongtermretentionaboutthegeneticconditionandtoexplainwhy.Finally,tomeasure
students’preferencesformultimodallearningstyles,participantsfilledoutaLikertscale
questionforthestatement:“IlearnbestwhenIamexposedtoaudio,visualandtext
resources”.
Subscale2:Perspectivesaboutdisabilityandcomfortlevels
ThefirstquestionusedaLikertscaletoassesswhethertheFRAMEvideogave
insightintoapatient’sperspectiveoflivingwithadisability.Animportantgoalofthe
FRAMEvideoishelphealthcareprofessionalsimprovetheircomfortlevelwhentreating
patientswithdisabilities.Therefore,aLikertscalequestionpromptsparticipantstoselect
theirlevelofagreementforthestatement“Iwouldfeelcomfortablebeinginvolvedinthe
careofsomeonewith(familialdysautonomiaor22q11.2deletionsyndrome)”.
Subscale3:FeedbackfortheFRAMEvideos
Participantscompletedtwofreeresponsequestionsthatpromptedthemtoexplain
whattheylikedthemostabouttheFRAMEvideoandhowtheythinkthevideocanbe
improved.Ayes/noquestionasksaboutwhetherparticipantswouldbeinterestedinhaving
accesstoadditionalFRAMEvideosaboutotherdisorders.
DataAnalysis
StatisticalAnalyses
Bothsampleswereanalyzedusingthepairedsamplet-testtoassesschangeinthe
ADSscorespreandpostFRAMEvideo.Forthevideoevaluationsurvey,dataanalysisfor
eachsampleincludeddescriptivestatisticssuchasunivariateanalysisandfrequency
distribution.AllanalyseswereconductedusingSPSSV.24andthesignificancelevelwasset
atp<0.05.

QualitativeAnalyses
Thematicanalysiswasconductedonthefree-responseanswersinthevideoevaluation
survey.Ourdata-drivenapproachusedopencodingandaxialcodingtofurtherevolve
themes.Aninitialcodebookwasdevelopedtocapturekeythoughtsandconceptsfromthe
data.Thecategorydefinitionswerereviewedandrevisedmultipletimes.Theresultsofthe
descriptivecodingwereorganizedintofinalthemestobetterunderstandparticipants’
perspectivesontheFRAMEvideoasamedicaleducationtool.
Results
A.AttitudechangesPreandPostVideo
1.22q11.2DeletionSyndromeGroup
InclusionSubscale:Significantandfavorablechangesinattitudewerefoundinthreeoutof
fouritemsmeasuringinclusion/exclusionandburden(Table1).Adecreaseinthe“Mean
PostVideo”foreachstatementindicatedmoredisagreementandthus,improvedattitudes.
Nosignificantchangewasfoundforthestatement“peoplewith22q11.1areaburdenon
society”.
Table1:AttitudeChangetowardPeoplewith22q11.2DeletionSyndrome(Inclusion)PreandPostVideo(1=stronglydisagree,5=stronglyagree) InclusionSubscale
Mean PreVideo (N=21)
Mean Post Video (N=21)
Mean Difference
tvalue
plevel*
Peoplewith22q11.2findithardertomakenewfriends
3.85 (SD=.91)
3.05(SD=1.16)
.80 3.30 p<.01
Peoplewith22q11.2haveproblemsgettingengagedinsociety
4.09 (SD=.76)
2.62(SD=1.24)
1.48 5.41 p<.001.
Peoplewith22q11.2areaburdenonsociety
2.42 (SD=1.21)
2.28 (SD=1.10)
.14 .90 n.s.
Peoplewith22q11.2areaburdenontheirfamily
3.10 (SD=1.17)
2.43 (SD=1.08)
.67 3.16 p<.01
*forone-tailedtest DiscriminationSubscale:Significantandfavorablechangesinattitudewerealsofoundin
threeoutoffouritemsmeasuringdiscrimination(table2).Adecreaseinthe“MeanPost
Video”foreachstatementindicatedmoredisagreementandthus,improvedattitudes.No

significantchangewasfoundforpeoplewith22q11.1beingaburdenonsociety.
Table2:AttitudeChangetowardPeoplewith22q11.1DeletionSyndrome(Discrimination)PreandPostVideo(1=stronglydisagree,5=stronglyagree) Discrimination
Mean PreVideo (N=21)
Mean Post Video (N=21)
Mean Difference
tvalue
plevel*
Peopleoftenmakefunofdisabilities
3.57 (SD=1.03)
3.33(SD=1.15)
.24 1.42 n.s.
Peoplewith22q11.2areeasiertotakeadvantageofcomparedtootherpeople
3.47 (SD=1.08)
3.09(SD=1.18)
.38 1.79 p<.05.
Peopletendtobecomeimpatientwiththosewith22q11.1
3.43 (SD=.92)
2.62 (SD=.86)
.81 4.95 p<.001
Peopletendtotreatthosewith22q11.1asiftheyhavenofeelings
2.95 (SD=1.20)
2.48 (SD=1.12)
.47 2.68 p<.01
*forone-tailedtest
PositiveGainsSubscale:Favorablechangesinpositivegainsofpeoplewith22q11.1deletion
syndromewerefoundinthreeoutoffourareas(table3).Anincreaseinthe“MeanPost
Video”foreachstatementindicatedmoreagreementandthus,improvedattitudes.No
significantchangewasfoundinsomepeopleachievingmorebecauseoftheirdisabilities.
Table3:AttitudeChangetowardsPeoplewith22q11.1DeletionSyndrome(PositiveGains)PreandPostVideo(1=stronglydisagree,5=stronglyagree) PositiveGains Mean
PreVideo (N=21)
Mean Post Video (N=21)
Mean Difference
tvalue
plevel*
Having22q11.1canmakesomeoneastrongerperson
3.57 (SD=1.08)
3.95(SD=.86)
-.38 -2.35 p<.01.
Having22q11.1canmakesomeoneawiserperson
3.09 (SD=1.13)
3.47(SD=1.03)
-.38 -2.35 p<.01.
Somepeopleachievemorebecauseoftheirdisabilities
3.24 (SD=1.13)
3.52 (SD=1.03)
-.28 -1.55 n.s.
Peoplewith22q11.1aremoredeterminedthanotherstoreachtheirgoals
2.90 (SD=1.09)
3.38 (SD=.92)
-.48 -2.50 p<.01

Current/FutureHopes:Significantchangesinattitudewerefoundintwooutoffouritems
measuringcurrentandfuturehopes(table4).Adecreaseinthe“MeanPostVideo”for
eachstatementindicatedmoredisagreementandthus,improvedattitudes.Nosignificant
changewasfoundforthetwootherstatementsaboutsexdiscussionsandlookingforward
tothefuture.
Table4:Attitudechangetowardspeoplewith22q11.2DeletionSyndrome(current/futurehopes)PreandPostVideo Current/FutureHopes
Mean PreVideo (N=21)
Mean Post Video (N=21)
Mean Difference
tvalue
plevel*
Sexshouldnotbediscussedwithpeoplewith22q11.1
2.14 (SD=1.12)
1.90(SD=1.15)
.24 1.31 n.s.
Peopleshouldnotexpecttoomuchfrompeoplewith22q11.1
2.24 (SD=1.09)
1.90(SD=89)
.33 2.09 p<.05.
Peoplewith22q11.1shouldnotbetoooptimisticabouttheirfuture
2.19 (SD=1.08)
1.86 (SD=.86)
.33 1.92 p<.05
Peoplewith22q11.1havelesstolookforwardtothanothers
2.33 (SD=1.20)
2.00 (SD=.95)
.33 1.67 n.s.
*Forone-tailedtest
Overallscores:ThegreatestmeandifferenceforADSscorespreandpostvideowasinthe
“inclusion”subscale(3.09)andtheleastmeandifferencewasinthe“currentandfuture
hopes”subscale(1.24).Table5showsthemeandifferenceoverallandbysubscaleforthe
22q11.2DSgroup.Themeandifferencefortotalscorespreandpostvideowas7.76.Forall
subscales,theplevelwassignificant.
Table5:SummaryofAttitudeChangestowardspeoplewith22q11.2DeletionSyndromePreandPostVideo Prevideomean Postvideomean Meandifference plevelTotalscore 47.00(SD=8.42) 39.23(SD=9.14) 7.76 p<.001Inclusion 13.47(SD=3.37) 10.38(SD=4.16) 3.09 p<.001Discrimination 13.47(SD=3.22) 11.52(SD=3.81) 1.9 p<.001PositiveGains 12.81(SD=4.06) 14.33(SD=-1.52) -1.52 p<0.05Hopes 8.9(SD=4.17) 7.67(SD=3.55) 1.24 p<0.05Note:Thepositivegainscorewasrecordedinthesamedirectionastheother3subscalestocomputeatotalattitudescore(plevelsareforaone-tailedtest)

2.FamilialDysautonomiaGroup
InclusionSubscale:Nosignificantchangesinattitudewerefoundinallfouritemsmeasuring
inclusion,exclusionandburdenforpeoplewithfamilialdysautonomia.
DiscriminationSubscale:Nosignificantchangesinattitudewerefoundinallfouritems
measuringdiscriminationtowardspeoplewithfamilialdysautonomia.
PositiveGains:Favorableattitudechangesinthepositivegainscategorywerefoundin3out
of4areas(table6).Thestatement“havingFDcanmakesomeoneastrongerperson”went
fromameanof3.50orbetween“agreement”and“uncertain”to4.00or“agreement”.The
statement“Havingfamilialdysautonomiacanmakeapersonwiser”wentfromameanof
3.44orbetween“uncertain”and“agree”to3.67oragreaterlevelof“agreement”.The
statement“PeoplewithFDaremoredeterminedthanotherstoreachtheirgoals”went
fromameanof2.96or“uncertain”to3.33between“uncertain”and“agreement”.No
significantchangewasfoundinthestatement“somepeopleachievingmorebecauseof
theirdisabilities”.
Table6:Attitudechangetowardspeoplewithfamilialdysautonomia(PositiveGains)PreandPostVideoPositiveGains
MeanPreVideo(N=27)
MeanPostVideo(N=27)
MeanDifference
tvalue
plevel*
HavingFDcanmakesomeoneastrongerperson
3.50(SD=.90)
4.00(SD=.56)
-.50 -2.82 p<.01.
HavingFDcanmakesomeoneawiserperson
3.44(SD=.85)
3.67(SD=.68)
-.23 -2.00 p<.05.
Somepeopleachievemorebecauseoftheirdisabilities
3.37(SD=.97)
3.52(SD=.88)
-.15 -1.44 n.s.
PeoplewithFDaremoredeterminedthanotherstoreachtheirgoals
2.96(SD=.44)
3.33(SD=.88)
-.37 -2.43 p<.05
*forone-tailedtest
Currentandfuturehopes:Nosignificantchangesinattitudewerefoundinthefouritems

measuringcurrentandfuturehopesforpeoplewithfamilialdysautonomia.
Overallscores:TheonlystatisticallysignificantmeandifferenceforADSscoreswasforthe
“positivegains”subscale(-1.27).Table7showsthemeandifferenceoverallandbysubscale
fortheFDgroup.ThemeandifferencefortotalADSscorespreandpostvideowas2.0.
Table7:SummaryofAttitudeChangestowardspeoplewithfamilialdysautonomiaPreandPostVideo Prevideomean Postvideomean Meandifference plevelTotalscore 41.15(SD=6.22) 39.15(SD=8.07) 2.00 p<.05Inclusion 11.00(SD=2.66) 10.67(SD=3.35) 0.33 n.s.Discrimination 12.22(SD=2.64) 11.67(SD=2.88) 0.55 n.s.PositiveGains 13.27(SD=2.32) 14.54(SD=2.39) -1.27 p<.001Hopes 7.3(SD=2.45) 7.48(SD=2.71) -0.18 n.sNote:Thepositivegainscorewasrecordedinthesamedirectionastheother3subscalestocomputeatotalattitudescore(plevelsareforaone-tailedtest)
B.VideoEvaluationSurveyResults
Retentionofthevideoandlearningstyles
Forthegroupthat
reviewedthe22q11.2
deletionsyndromevideo
(N=21),allbutthree
peoplethoughtthe
FRAMEvideo,not
Medscape,wouldbebest
fortheretentionof
informationaboutthis
disease.Allthreeofthesepeoplewereuncertainordisagreedtheywouldrememberthings
fromtheFRAMEvideo,while100%ofthosewhopreferredtheFRAMEvideoagreedthe
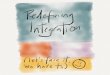
FRAMEvideowouldberememberedinthefuture.86%ofparticipants(n=18)fromthe
22q11.2DSgroupagreedorstronglyagreedtheywouldremembertheFRAMEvideointhe
future(figure2).Finally,18participants(82.8%)agreedtheylearnedbestwhenmultiple
0 03
22
21 2
13
5
05
10152025
StronglyDisagree
Disagree Uncertain Agree StronglyAgree
numbe
rofp
articipants
Figure2:Summaryofresponsestostatement“IwillrememberthisFRAMEvideointhefuture”22q11.2DSn=
21;FDn=27
FD 22q11.2DS

learningmodes(audio,video,text)wereutilized.
Forthegroupthatwasassignedthefamilialdysautonomia(FD)video(N=27),allbutthree
peoplethoughttheFRAMEvideo,notMedscape,wouldbebestforinformationretention
aboutthisdisease(Figure3).Twoofthesethreeparticipants(66.7%)wereuncertainabout
rememberingthingsfrom
theFRAMEvideo,while
93.8%ofthosewho
preferredtheFRAMEvideo
agreedtheFRAMEvideo
wouldberememberedin
thefuture.93%of
participants(n=24)intheFD
group“agreed”or“strongly
agreed”theywouldremembertheFRAMEvideointhefuture(Figure3).Atotalof24
people(89%)agreedtheylearnedbestwhenmultiplelearningmodes(audio,text,video)
wereutilized.
Perspectivesaboutdisabilityandcomfortlevels
Forthegroupreviewingthe22q11.2deletionsyndromevideo(N=21),14participants
(63.6%)agreedorstronglyagreedtheywouldfeelcomfortablebeinginvolvedincaringfor
someonewiththiscondition.Nineteenparticipants(86.4%)agreedorstronglyagreedthe
22q11.2deletionsyndromevideogavetheminsightintolivingwithadisability.Onlyoneof
thethreeparticipantswhopreferredtheMedscapeinformationagreedtheywouldbe
comfortablecaringforsomeonewith22q11.2deletionsyndrome.Similarly,onlyoneofthe
threeagreeditgavetheminsightintolivingwiththedisability(figure4).
3 3
18
24
051015202530
22q11.2DS FDnumbe
rofp
articipants
Figure3:Summaryofresponsestostatement"Whichlearningapproachdoyoufeelwillbestallowyoutoretaininformationinthelongterm?"FDn=27,22q11.2DSn=21
Medscape FRAMEvideo

ForthetheFDgroup(N=27),24participants(85.7%)agreedorstronglyagreedtheywould
feelcomfortablebeinginvolvedincaringforsomeonewithFD.Eventhoughthreepeople
preferredtheMedscapeinformation,allagreedtheywouldbecomfortablecaringfor
someonewithFD.
100%ofparticipants
agreedorstrongly
agreedtheFDvideo
gavetheminsightinto
livingwithadisability
(figure4).
FeedbackfortheFRAMEvideos
Forthe22q11.2DSsample(N=21),onlytwopeople(9.1%)wouldnotbeinterestedin
additionalFRAMEvideosaboutotherdisorders.FortheFDsample,onlyfourpeopleoutof
27(14.8%)wouldnotbeinterestedinadditionalFRAMEvideosaboutotherdisorders.
C.ThematicAnalysisoflongtermretentionofgeneticcondition
Atotalof43participantsansweredtheopenendedquestiontoexplainwhetherFRAME
videoorMedscapeisabetterlearningapproachtoretaininformationinthelongterm.
ThreethemesemergedfromparticipantsthatpickedtheFRAMEvideo.Participants
mentionedthatseeingavisual(n=24)andhearingstoriesandexperiences(n=16)allowed
themtobetterretaintheinformation.Thethirdthemewasorganizationofthevideoand
howtheinformationwaspresented(n=3).Oneparticipantsaid:
“Seeingfamiliestalkabouthowtheillnessaffectstheirlivesandwatchingtheminteractwiththeirchildwith22q11.2deletionsyndromeprovidedinvaluableinformationabouttheday-to-daylifeoflivingwiththisdisorder.Ittakestextandtransformsittorealpeoplewhowantthesamethingwealldo-tobehappyandhealthy.Ifeltmoreinspiredtocareforsomeonewiththissyndromeafterthevideo
0 0
16
11
1 1
118
0
5
10
15
20
StronglyDisagree Uncertain Agree StronglyAgreenumbe
rofp
articipants
Figure4:Summaryofresponsestostatement"TheFRAMEvideoonFDor22q11.2DSgavemeinsightintoapatient'sperspectives
oflivingwithadisability"FDN=27,22q11.2DSN=21
FD 22q11.2DS

thanIdidafterreadingthemedscapearticle.”
ThreethemesemergedfromthesixparticipantswhochoseMedscapeoverFRAME.These
participantsemphasizedtheFRAMEvideosdidnothaveenoughinformation(n=2)and
werelessefficientthanMedscape(n=1).Twoparticipantsalsomentionedtheylearnbetter
byreadingandthereforeMedscapewouldallowthemtoretaininformationinthelongrun.
Oneparticipantsaid:
“TheFRAMEvideoismorememorablebutdidnotprovideadequateinformationregardingtheclinicalpresentation,diagnosis,andmanagementofthedisease.Iftheparticipantsinthevideohadagreaterdiscussionregardingthosetopics,itwouldhavebeenanexcellentmeansoflearningthematerial…”
D.ThematicAnalysisofthestrengthsoftheFRAMEvideo
Atotalof45participantsansweredtheopenendedquestionaboutwhattheymostliked
abouttheFRAMEvideo.Themajorityofparticipantsmentionedfamilyinvolvement(n=14)
andpatientstoriesandperspectives(n=16)astheirtopreasons.Someparticipantswrote
aboutthewidephenotypicspectrumrepresentedinthevideos(n=5)andotherssaidthe
videoswereinformative(n=3).Oneparticipantwroteabouthoweffectivethestorieswere
increatingamemory.
“ThefeelingsbroughtaboutbyhearingthosewhoactuallyhaveFDandthechallengesfacedbythemfromtheirperspectiveandtheirfamiliescreatesamorevividmemory.”
Anotherparticipantdescribedhowtwochildrenwith22q11.2deletionsyndromecould
havedifferentclinicalfeatures,ageneticsconceptknownasvariableexpressivity.
“Ilikedthatitportrayedchildrenonallareasofthespectrumintermsofseverityofthecondition.Icouldseethatforsomeparentsittookupasignificantamountofattentionandtimetocareforthe22q11.2deletionsyndromechild,whileinotherfamiliesitwasminor.“
E.ThematicAnalysisofimprovementstotheFRAMEvideo
Atotalof44participantsansweredtheopenendedquestionabouthowtheFRAMEvideo
canbeimproved.Tenparticipantsrespondedwitheither“notsure”or“nochanges
needed”.AnothermajorthemewastheFRAMEvideoneededmoreinformation(n=13),

suchasdetailsaboutprognosis,treatment,diagnosticstrategies,pathophysiologyanddaily
challenges.OneparticipanthighlightedthedifferencebetweenthegoalsofFRAMEand
Medscape.
“Italldependsontheintendedaudience.Forpreparingmeasahealthcareprovider,itiscertainlyinadequate,incontrasttoknowledgecontainedwithintheMedscapepages.However,ifitisintendedasanoverviewforthepublictounderstandthisconditionexists,itssufferersareotherwise"normal"people,andthestrugglesaresignificant.”
ThisquotehighlightsthatwhiletheFRAMEvideoisunabletocontainasmuchinformation
asMedscape,itservesasavehicleforpatientstosharetheirexperienceslivingwiththe
condition.Anotherparticipantdescribedhowthevideosdidnotcontainenoughstories
aboutfamilychallengesandnegativeexperiencesinsociety.
“Iwouldhavelikedtoseethefullpictureofhowthesyndromeaffectsfamiliesandhowthesekidsaretreatedinschoolandsociety.Iunderstandthatthevideoisintendedtobeoptimistic,butIwouldhavelikedtohearmoreofhowmuchsomefamiliesstruggledtocareforthechildwiththissyndrome,especiallywhenthereareotherchildreninthefamilytopayattentiontoaswell.Ialsowonderhowoftenthesechildrenaremistreatedinschoolandinsociety.”
AsmallnumberofparticipantsmentionedthattheFRAMEvideosshouldhaveincluded
moretextslides(n=2),morevisualaidsforhallmarkcharacteristics(n=3)andthe
involvementofahealthprofessional(n=5).
DISCUSSION
Thereisalackofresearchcomparingtheeffectivenessofdigitalstorytellingwith
traditionalmedicaleducationmethods.Ourstudyisoneofthefirsttoexploretheimpact
thatanonlinemedicaleducationdigitalstorytellingtoolhasonmedicalstudents’attitudes
towardsindividualswithdisability.TheFRAMElibraryofvideosandphotographicgalleries
isuniquebecauseitisanonline,multimediaresourcethatdesignatespeoplewithgenetic
conditionsandtheircaregiversastheeducatorsforhealthcarestudentsandprofessionals.
Eachfilmisdesignedtoincreaseunderstandingofthefeaturedgenetic,physical,
intellectualand/orbehavioralaspectsofdifferentconditions.Inthisstudy,weusedthe
AttitudestoDisabilitiesScale(ADS)tomeasuremedicalstudents’attitudesbeforeandafter
watchingoneoftwoFRAMEvideosabouteither22q11.2deletionsyndromeorfamilial

dysautonomia.Additionally,weaskedparticipantstocompleteavideoevaluationsurveyto
investigatetheirpreferencesforMedscapeversusFRAME.Anotherpurposeofthevideo
evaluationwastoassesshoweffectiveFRAMEvideosareforhelpingviewersunderstand
theexperiencesoflivingwithdisability.
OurfindingssuggestthatbywatchingFRAMEvideos,medicalstudentsattitudes
towardsindividualswithdisabilityaresignificantlyimproved.InboththeFDand22q11.2DS
groups,therewerefavorableattitudechangesinthreeoutofthefourstatementsinthe
“positivegains”categoryoftheADSpreandpostvideo.Thesethreestatementsinvestigate
participants’attitudesaboutwhetherhaving22q11.2DSorFDmakessomeoneastronger,
wiserandmoredeterminedperson.Thissubscaleisuniquebecauseitexplicitlyreflects
positivegainsinrelationtoselfandtoothersthatmaybeasurpriseaboutdisability(Power
&Green,2010).Literaturedemonstratesthatthedisabilitiescommunityfacesstigma,
stereotypes,prejudicedattitudesandinstitutionalbarriersinhealthcare(Brownetal.,
2010;Eddy&Robey,2005;Woodward,L.etal.,2012).
Thereweremoresignificantandfavorableattitudesubscalechangesforthe22q11.2
DSgroupthanfortheFDgroup.Inthe22q11.2DSgroup,therewerepositiveattitude
changesforthreeoutofthefourstatementsintheinclusion,discriminationandpositive
gainssubscales.Notably,intheinclusionsubscale,participantswentfromagreetobetween
disagreeanduncertainforthestatement“peoplewith22q11.2deletionsyndromehave
problemsgettingengagedinsociety”.Thissignificantimprovementmaybeexplainedby
thevideo’semphasisonhighlightingthestoryofpatientsthatwentontobecome
successfulcollegestudents.Therewerepositivechangesforthe22q11.2DSgroupintwo
outofthefourstatementsinthesubscalewhichhighlightsattitudesaboutcurrentand
futurehopes.ThisFRAMEvideodidnotdiscusstopicsrelatedtosexwhichmayexplainthe
lackofsignificantimprovementinattitudeforthestatement“Sexshouldnotbediscussed
withpeoplewith22q11.2deletionsyndrome”.
FortheFDgroup,therewerefavorableattitudechangesinthreeoutoffour
statementsinonlyonesubscaleoftheADS.ThechangeintotalADSscorewassignificant
indicatingoverallattitudestowardsFDwereimproved.Theremaybeseveralexplanations

forthedifferenceinsubscalescoresbetweentheFDand21q11.2DSgroups.The
participantsintheFDvideospresentedwithmorenoticeablephysicaldifferencesand
speechimpediments.ItispossibletheFRAMEvideoinisolationmaynotbeenoughto
improveADSscoresinallthesubscalesformoreseveredisabilities.Apreviousstudy
suggeststhatusingdigitalstorytellingisakey,butnotsolecomponentwithinaclinical
trainingmoduledesignedtoimproveknowledge,attitudesandcomfortlevelswhencaring
forpatientswithdisabilities(Woodward,L.etal.,2012).Additionalconfoundingfactors
whencomparingresultsbetweenthetwoconditionsincludedifferencesinvideo
productionandpriorstudentexposurestodisabilitytraining.Itisimportanttonotethat
eventhoughtherewerelesssignificantchangesintheADSscoresfortheFDgroup,100%of
participantsagreedthisFRAMEvideoprovidedinsightintothelivesofindividualswith
disabilitiesand24participants(85.7%)agreedorstronglyagreedthattheywouldfeel
comfortablebeinginvolvedincaringforsomeonewithFD.Tobetterunderstandthe
differentresultsbetweenthetwoconditions,afuturestudycouldbedoneinwhichone
individualwatchestwoFRAMEvideosandthechangesinADSscoresforeachvideoare
compared.Thisapproachwouldlikelyreducetheconfoundingfactorsrelatedtodifferent
individualswatchingdifferentvideos.
Anothersignificantfindingis89%ofstudentsidentifiedtheneedforexposureto
multiplelearningmodes(audio,textandvisual)formaximumabsorptionofknowledge.
Thisfindingisconsistentwithliteraturethatsuggestsdigitalstorytellingandtechnology
promptdeeperlearningandknowledgeretention(Alessie&Trollip,2001;Nowaczyk,2012;
Sandars,Murray,&Pellow,2008;Smeda,Dakich,&Sharda,2014).Similarly,whenaskedto
explainwhyparticipantspickedFRAMEastheirpreferredlearningapproach,theanswers
werefocusedaroundthemesofvisualimagery,auditoryexperienceofhearingstoriesand
videoorganization.ThemajorityofparticipantsagreedthattheFRAMEvideowouldbe
rememberedinthefuture(86%for22q11.2DS,89%forFD)andthereisamajority
preferenceforFRAMEoverMedscape.
StrengthsandLimitationsoftheStudy
Weusedanestablishedandvalidatedself-reportscaleforattitudechangesand

qualitativesurveys.Ourmixedmethodapproachcanbeconsideredastrengthofthisstudy.
Additionally,oursampleincluded4thyearmedicalstudentsfromthreedifferentschoolsto
createamorerepresentativesample.
OnelimitationofthisstudyisweonlyevaluatedtwoFRAMEvideosontwogenetic
conditions.FuturestudiescanbedonetoanalyzeattitudechangesformoreFRAMEvideos
ondifferentconditions.Additionally,baselineexposuretothegeneticconditionandprior
disabilitiestraininginmedicalschoolwerenotassessedtoavoidexcessparticipantburden.
Lastly,ourstudyusesself-reporteddatatoexploretheeffectivenessofdigitalstorytellingas
asupplementarylearningtool.AfuturestudycouldcompareFRAMEvideosandtraditional
learningmethodsinmedicalschool.
Conclusion
TheresultsofthisstudysuggesttheFRAMEvideosareuniqueandeffectivelearning
toolsinmedicaleducation.Overall,theFRAMEvideosimprovedattitudestowards
individualswithdisabilitiesinboththegroups.Additionally,medicalstudentsinthisstudy
expressedpreferencesfortheFRAMEvideooveratraditionaltext-basedlearningmethod
suchasMedscape.Thesevideosarearesponsetotheneedforhealthcareprofessionals
andstudentstohaveexposuretogeneticconditionsanddisabilitiesinthehopestheywill
bemorecomfortableprovidingthesepatientswithmedicalcare.Understandingthe
benefitsandlimitationsofsupplementarymedicaleducationtoolswillfacilitatefurther
developmentandresearchindigitalstorytellingasanimportantadditiontohealthcare
educationandtrainingprograms.
ACKNOWLEDGMENTS
IwouldliketheacknowledgeAnneGreb,ElizabethGrossmanandRickGuidottifortheir
guidanceandDr.MichaelSmithforhisstatisticalconsultation.

REFERENCES
Alessie,S.,&Trollip,R.(2001).Multimediaforlearning:Methodsanddevelopment(3eed.).
Allyn&Bacon.
Ali,A.,Strydom,A.,Williams,R.,Williams,R.,&King,M.(2008).Ameasureofperceived
stigmainpeoplewithintellectualdisability.BritishJournalofPsychiatry,193,410–415.
Brown,R.S.,Graham,C.L.,Richeson,N.,Wu,J.,&McDermott,S.(2010).Evaluationof
medicalstudentperformanceonobjectivestructureclinicalexamswithstandardized
patientswithandwithoutdisabilities.AcademicMedicine,85(11),1766–1771.
Cox,K.(2001).Storiesascaseknowledge :caseknowledgeasstories,862–866.
Ditchman,N.,Werner,S.,Kosyluk,K.,Jones,N.,Elg,B.,&Corrigan,P.W.(2013).Stigmaand
intellectualdisability:Potentialapplicationofmentalillnessresearch.Rehabilitation
Psychology,58(2),206–216.http://doi.org/10.1037/a0032466
Eddy,G.E.,&Robey,K.L.(2005).Consideringthecultureofdisabilityincultural
competenceeducation.AcademicMedicine,80(5),706–712.
Greb,A.E.,Brennan,S.,&Mcparlane,L.(2009).Retentionofmedicalgeneticsknowledge
andskillsby,11(5),3–8.http://doi.org/10.1097/GIM.0b013e31819c6b2d
Guidotti,R.(n.d.).FRAME.Retrievedfromhttp://positiveexposure.org/frame/
Kirk,M.,Tonkin,E.,Skirton,H.,Mcdonald,K.,Cope,B.,&Morgan,R.(2013).Nurse
EducationTodayStorytellersaspartnersindevelopingageneticseducationresource
forhealthprofessionals.YNEDT,33(5),518–524.
http://doi.org/10.1016/j.nedt.2011.11.019
Kirklin,D.(2003).Respondingtotheimplicationsofthegeneticsrevolutionforthe
educationandtrainingofdoctors :amedicalhumanitiesapproach,168–173.
Koenig,J.M.,&Zorn,C.R.(2002).UsingStorytellingasanApproachtoTeachingand
LearningWithDiverseStudents,41(9).
Kumagai,A.K.,Murphy,Æ.E.A.,&Ross,Æ.P.T.(2009).toteachpatient-centeredcare,
315–326.http://doi.org/10.1007/s10459-008-9123-5
Macnaughton,J.,Mbchb,M.A.,&Drcog,M.(2015).EuropePMCFundersGroupMedical
humanities’challengetomedicine,17(5),927–932.http://doi.org/10.1111/j.1365-

2753.2011.01728.x.Medical
Medical,P.,Society,T.A.,Genetics,H.,&Genetics,M.(2008).AssociationofProfessorsof
HumanandMedicalGenetics/AmericanSocietyofHumanGeneticsMEDICALSCHOOL
CORECURRICULUMINGENETICS,(1995),1–8.
Minihan,P.M.,Robey,K.L.,&Long-Bellil,L.M.(2011).Desirededucationaloutcomesof
disability-relatedtrainingforthegeneralistphysician:knowledge,attitudes,andskills.
AcademicMedicine,86(9),1171–1178.
Nowaczyk,M.J.M.(2012).Narrativemedicineinclinicalgeneticspractice.AmericanJournal
ofMedicalGenetics,PartA,158A(8),1941–1947.
http://doi.org/10.1002/ajmg.a.35482
Poladian,K.(2013).GDINavigatortoExcellence:SummariesofDisabilityArticles.Retrieved
from
https://www.aamc.org/download/328092/data/disabilityarticlesinacademicmedicine.p
df
Power,M.J.,&Green,A.M.(2010).TheAttitudestoDisabilityScale(ADS):Development
andpsychometricproperties.JournalofIntellectualDisabilityResearch,54(9),860–
874.http://doi.org/10.1111/j.1365-2788.2010.01317.x
Ruffin,A.(2004).ContemporaryIssuesinMedicine :GeneticsEducation,(June).
Sabharwal,S.(2001).Objectiveassessmentandstructuredteachingofdisabilityetiquette.
AcademicMedicine.AcademicMedicine,76(5).
Sandars,J.,Murray,C.,&Pellow,A.(2008).Twelvetipsforusingdigitalstorytellingto
promotereflectivelearningbymedicalstudents,774–777.
http://doi.org/10.1080/01421590801987370
Smeda,N.,Dakich,E.,&Sharda,N.(2014).Theeffectivenessofdigitalstorytellinginthe
classrooms :acomprehensivestudy,1–21.http://doi.org/10.1186/s40561-014-0006-3
Woodward,L.,H.,S.M.,Zwygart,K.K.,&Perkins,E.A.(2012).Aninnovativeclerkship
modulefocusedonpatientswithdisabilities.AcademicMedicine,87(4),537–542.

APPENDIXA:ADSScale(22q11.2DeletionSyndrome)
StronglyDisagree Disagree Uncertain Agree Strongly
Agree1 Peoplewith22q11.2deletion
syndromefindithardertomakenewfriends
2 Peoplewith22q11.2deletionsyndromehaveproblemsgettinginvolvedinsociety
3 Peopleoftenmakefunofdisabilities
4 Peoplewith22q11.2deletionsyndromeareeasiertotakeadvantageof(exploitortreatbadly)comparedwithotherpeople
5 Peoplewith22q11.2deletionsyndromeareaburdenonsociety
6 Peoplewith22q11.2deletionsyndromeareaburdenontheirfamily
7 Having22q11.2deletionsyndromecanmakesomeoneastrongerperson
8 Having22q11.2deletionsyndromecanmakesomeoneawiserperson
9 Somepeopleachievemorebecauseoftheirdisability(e.g.theyaremoresuccessful)
10 Peoplewith22q11.2deletionsyndromearemoredeterminedthanotherstoreachtheirgoals
11 Peopletendtobecomeimpatientwiththosewith22q11.2deletionsyndrome
12 Peopletendtotreatthosewith22q11.2deletionsyndromeasiftheyhavenofeelings
13 Sexshouldnotbediscussedwithpeoplewith22q11.2deletionsyndrome
14 Peopleshouldnotexpecttoomuchfromthosewith22q11.2deletionsyndrome
15 Peoplewith22q11.2deletionsyndromeshouldnotbeoptimistic(hopeful)abouttheirfuture
16 Peoplewith22q11.2deletionsyndromehavelesstolookforwardtothanothers

AppendixB:VideoEvaluationSurvey(22q11.2deletionsyndrome)
StronglyDisagree Disagree Uncertain Agree Strongly
Agree1 IwillrememberthisFRAMEvideoin
thefuture.
2 Iwouldfeelcomfortablebeinginvolvedinthecareofsomeonewith22q11.2deletionsyndrome.
3 TheFRAMEvideoon22q11.2deletionsyndromegavemeinsightintoapatient’sperspectiveoflivingwithadisability.
4 IlearnbestwhenIamexposedtoaudio,visualandtextresources.
5.Whichlearningapproachdoyoufeelwillbestallowyoutoretaininformationabout22q11.2deletionsyndromeinthelongterm?
A.MedscapeB.FRAMEvideoPleaseexplainyourchoice________________
6.WhatdoyoulikemostabouttheFRAMEvideoon22q11.2deletionsyndrome?7.HowdoyouthinktheFRAMEvideoon22q11.2deletionsyndromecanbeimproved?7.Wouldyoubeinterestedinhavingaccesstoadditionalvideosaboutotherdisordersforyourresource? A.Yes B.No8.Whatmedicalspecialtyareyouplanningtopractice?