Embed Size (px)
Citation preview
Guideline
European Society of Hypertension Position Paper onAmbulatory Blood PressureMonitoring
Eoin OrsquoBrien Gianfranco Parati George Stergiou Roland Asmar Laurie Beilin Grzegorz BiloDenis Clement Alejandro de la Sierra Peter de Leeuw Eamon Dolan Robert Fagard John GravesGeoffrey A Head Yutaka Imai Kazuomi Kario Empar Lurbe Jean-Michel Mallion GiuseppeMancia Thomas Mengden Martin Myers Gbenga Ogedegbe Takayoshi Ohkubo Stefano OmboniPaolo Palatini Josep Redon Luis M Ruilope Andrew Shennan Jan A StaessenGert vanMontfrans Paolo Verdecchia Bernard Waeber Jiguang Wang Alberto ZanchettiYuqing Zhang on behalf of the European Society of Hypertension Working Group on BloodPressure Monitoring
C
Journal of Hypertension 2013 311731ndash1768
Correspondence to Eoin OrsquoBrien MD FRCP Conway Institute University CollegeDublin Dublin 4 Ireland E-mail eobrieniolieEoin OrsquoBrien Gianfranco Parati and George Stergiou contributed equally to the
writing of this article
The affiliations of the co-authors are listed at the end of the paper preceding thereference list
Received 3 June 2013 Accepted 4 June 2013
J Hypertens 311731ndash1768 2013 Wolters Kluwer Health | Lippincott Williams amp
Jo
Ambulatory blood pressure monitoring (ABPM) is beingused increasingly in both clinical practice and hypertensionresearch Although there are many guidelines thatemphasize the indications for ABPM there is nocomprehensive guideline dealing with all aspects of thetechnique It was agreed at a consensus meeting on ABPMin Milan in 2011 that the 34 attendees should prepare acomprehensive position paper on the scientific evidence forABPMThis position paper considers the historical backgroundthe advantages and limitations of ABPM the thresholdlevels for practice and the costndasheffectiveness of thetechnique It examines the need for selecting anappropriate device the accuracy of devices the additionalinformation and indices that ABPM devices may provideand the software requirementsAt a practical level the paper details the requirements forusing ABPM in clinical practice editing considerations thenumber of measurements required and the circumstancessuch as obesity and arrhythmias when particular careneeds to be taken when using ABPMThe clinical indications for ABPM among which white-coatphenomena masked hypertension and nocturnalhypertension appear to be prominent are outlined indetail along with special considerations that apply incertain clinical circumstances such as childhood theelderly and pregnancy and in cardiovascular illnessexamples being stroke and chronic renal disease and theplace of home measurement of blood pressure in relationto ABPM is appraisedThe role of ABPM in research circumstances such aspharmacological trials and in the prediction of outcome inepidemiological studies is examined and finally theimplementation of ABPM in practice is considered inrelation to the issue of reimbursement in differentcountries the provision of the technique by primary carepractices hospital clinics and pharmacies and the growingrole of registries of ABPM in many countries
opyright copy Lippincott Williams amp Wilkins Unauthurnal of Hypertension
Keywords ambulatory blood pressure monitoring clinicblood pressure measurement clinical indicationsguidelines home blood pressure measurementrecommendations research application
or
Wil
DO
1
ize
kins
I10
INTRODUCTION
2
HISTORICAL PERSPECTIVE
3
GENERAL CONSIDERATIONS
31 Why is ABPM superior to conventional BPmeasurement
32 ABPM thresholds for clinical practice33 Cost-effectiveness of ABPM34 Limitations of ABPM
d re
1097H
DEVICES AND SOFTWARE
4
41 Choosing an ABPM device
411 Selecting an accurate device412 Validation requirements for ABPM
devices in special populations413 Additional features for ABPM monitors
42 Software for ABPM data analysis421 Software requirements422 Indices derived from ABPM recordings
prod
JH0b013
PROCEDURE
5
51 Training requirements52 Fitting an ABP monitor53 Explanation to patient
uction of this article is prohibited
e328363e964
wwwjhypertensioncom 1731
Cop
OrsquoBrien et al
1732
54 Identification of daytime and night-time periodsand editing ABPM data
55 The arm for measurement56 Selecting the appropriate cuff and bladder57 Conditions in which ABPM may be difficult to
perform
yrigw
ICAL INDICATIONS FOR ABPM
CLIN
6
61 Role of ABPM in the diagnosis of hypertension62 White-coat phenomena
621 White-coat hypertension622 White-coat effect
63 Masked phenomena631 Masked hypertension632 Masked uncontrolled hypertension
64 Abnormal 24-h blood pressure patterns641 Daytime hypertension642 Siesta dippingpostprandial hypoten-
sion643 Nocturnal hypertension644 Dipping nondipping extreme dipping
and rising645 Morning hypertension and morning
BP surge646 Obstructive sleep apnea
65 Assessment of treatment651 BP variability and treatment652 Assessing efficacy of blood pressure
control653 Resistant hypertension
66 Hypertension in the elderly67 Hypertension in children and adolescents68 Hypertension in pregnancy69 Hypertension in high-risk patients
691 Diabetes692 Stroke693 Coronary heart disease694 Chronic kidney disease
610 Ambulatory hypotension611 Hypertension in Parkinsonrsquos disease612 Endocrine hypertension613 Follow-up
6131 When to repeat ABPM6132 ABPM versus Home BP
h
t copy Lwwjhy
ip
ABPM IN RESEARCH
7
71 ABPM in pharmacological research72 Regulatory recommendations for pharmacologi-
cal studies73 ABPM in outcome studies
IMPLEMENTATION OF ABPM IN CLINICAL
8
PRACTICE81 General principles82 Financial considerations83 Specialist clinics84 Primary care85 Pharmacies86 Healthcare providers87 ABPM registries and databases
871 Spanish registry872 Italian registry873 Irish registry874 Japanese registry
ppincott Williams amp Wilkins Unauthorizertensioncom
875 Australian registry876 IDACO database877 ARTEMIS registry878 Ambulatory blood pressure international
database
ed r
eprod
S
REFERENCE
1 INTRODUCTIONThe Working Group on Blood Pressure Monitoring ofthe European Society of Hypertension (ESH) publishedrecommendations for blood pressure (BP) measurementin 2003 [1] and a guideline for home BP measurement(HBPM) in 2008 [2] Ambulatory blood pressure monitoring(ABPM) is a subject of considerable scientific interest withover 10 000 papers listed on PubMed in 2012 In 2001 theUnited States Center for Medicare and Medicaid Servicesapproved ABPM for reimbursement for the identification ofindividuals with white-coat hypertension [3] Since thenhealthcare providers in many other countries providereimbursement for ABPM and in 2011 the National Institutefor Health and Clinical Excellence (NICE) in the UnitedKingdom recommended that ABPM should be offered as acost-effective technique to all people suspected of havinghypertension [4]
One of the first meetings to examine the potential ofABPM was held in Ghent in 1978 [5] The ESH WorkingGroup on Blood Pressure Monitoring has held severalconsensus conferences on ABPM since the first one inBerlin over 20 years ago [6] The most recent one was heldin Milan in 2011 at which the technique was comprehen-sively reviewed It was agreed that a writing committeeconsisting of Eoin OrsquoBrien Gianfranco Parati and GeorgeStergiou should draft two documents ndash a comprehensivereview of the scientific evidence for ABPM that was pre-sented at the Milan conference taking into considerationalso relevant publications up to the end of January 2013 (thepresent paper) and a second short paper with conciseinstructions as tohow thebest information couldbeobtainedfrom 24-h ABPM in clinical practice A number of drafts werecirculated to all the participants in theConsensus Conferencefor their comments and suggestions and the final version ofthe present paper is based on the agreed comments from 34international experts Data from randomized controlled trialsof sufficient power with ABPM are still small and this limitsformal grading of recommendations based on the availableevidence As the number of references cited in this paper islarge and in the interest of saving journal space somereferences have been listed in the supplementary filehttplinkslwwcomHJHA283 that accompanies thispaper In the text citations these references are identifiedby the letter w after the reference number
2 HISTORICAL PERSPECTIVETraditionally BP in the office or clinic has been assessedwith the auscultatory technique which was introduced intoclinical medicine at the beginning of the twentieth centuryand which has survived to this day in clinical practiceAlthough the technique is inherently accurate it is
uction of this article is prohibitedVolume 31 Number 9 September 2013
Box 1 Advantages of ambulatory blood pressure monitoring over clinicblood pressure
Gives a larger number of readings than office blood pressuremeasurement
Provides a profile of blood pressure behavior in the patientrsquosusual daily environment
Allows identification of white-coat and masked hypertensionphenomena
Demonstrates nocturnal hypertension Assesses blood pressure variability over the 24-h period Assesses the 24-h efficacy of antihypertensive medication Is a stronger predictor of cardiovascular morbidity and mortality
than office measurement
Guideline
dependent on observer attention to detail which is oftenlacking and it provides only a momentary measurement ofBP usually under circumstances that can influence the levelof BP being measured To overcome these serious meth-odological problems techniques for obtaining automatedprofiles of BP over 24 h and measures of BP in the homesetting have been developed
ABPM has been available in one form or another forsome 50 years having been developed initially to study thecircadian changes in BP and to determine the influence ofBP-lowering drugs on the 24-h profile The first major breakwith traditional BP measurement was the introduction of adirect intraarterial technique for the measurement of BPover the 24-h period The data on antihypertensive drugefficacy provided by studies using this system were particu-larly valuable because they provided continuous BPmeasurement throughout the day and night but use ofthe technique was limited by safety and ethical consider-ations Efforts were focused therefore on developing adevice that would record ambulatory BP noninvasively andin the 1960s the Remler device which was capable ofmeasuring BP intermittently during the daytime periodprovided clinicians with a new technique for assessingBP This device was limited by having to be operated bythe patient which made measurement of BP impossibleduring sleep The next technological advance was theintroduction of fully automated devices that could measureBP intermittently at predetermined intervals over the 24-hperiod This class of devices provided a methodology thatwas applicable not only for research but also for use inroutine clinical practice [7ndash101w]
3 GENERAL CONSIDERATIONS
31 Why is ambulatory blood pressuremonitoring superior to conventional bloodpressure measurementTraditionally office BP measurement has been performedusing a sphygmomanometer and stethoscope Recentlyautomated office BP measurement has been proposed asan alternative to traditional measurement Automated officeBP is the mean of multiple BP readings recorded with a fullyautomated device with the patient resting quietly alone inthe officeclinic [11] It has several advantages over manualBP especially in routine clinical practice by virtually elim-inating office-induced increases in BP improving accuracyminimizing observer error and providing a more stand-ardized measurement technique using an automated oscil-lometric sphygmomanometer [2w] The mean automatedoffice BP for diagnosing hypertension is similar to the meanawake ambulatory BP and home BP (13585 mmHg)Preliminary data suggest that automated office BP is a betterpredictor of target organ damage [3w4w] especially com-pared with routine manual office BP which correlatespoorly with intermediate end-points such as left ventricularmass [5w] Longitudinal clinical outcome studies with auto-mated office BP have not yet been reported
BP recorded in the patientrsquos home is a significantly betterpredictor of future cardiovascular risk than is office BPStandard protocols have been developed for recordinghome BP [2] and include the mean of duplicate readings
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
taken twice daily for 7 consecutive days with readings fromthe first day excluded The cut-point for hypertension usinghome BP is the same as for the awake ambulatory BP(13585 mmHg) In order to avoid reporting bias [12] ahome BP recorder with a memory for storing readingsshould be used and the patient should take the device tothe physicianrsquos office to have the mean home BP verifieddirectly from the devicersquos display More recently remotetransmissions of home BP readings [13] is becoming avail-able allowing BP readings recorded in the home to beautomatically sent to a data collection center via a tele-phone modem or internet link and from there forwarded tothe physicianrsquos office
The advantages of ABPM which have been stated incomprehensive reviews [11014] have influenced recom-mendations for the technique to be used much more widelyin clinical practice [15ndash186w7w] These advantages maybe briefly summarized as follows (Box 1) first and fore-most ABPM simply gives many more measurements thanconventional BP measurement and usual BP is reflectedmore accurately by repeated measurements ABPM pro-vides a profile of BP away from the medical environmentthereby allowing identification of individuals with a white-coat response or masked hypertension ABPM can demon-strate a number of patterns of BP behavior over 24 h thatmay be relevant to clinical practice such as nocturnalhypertension or increased BP variability by showing BPbehavior in different windows of a 24-h period such as thewhite-coat and nocturnal periods as well as the BP fluctu-ations triggered by environmental stimuli it is possible toassess the efficacy of antihypertensive medication through-out the day and night rather than relying on a casual BPABPM is a stronger predictor of cardiovascular morbidityand mortality than conventional measurement and evi-dence is growing that nocturnal BP measured by ABPMis an important predictor of cardiovascular outcome fromwhich it follows that the measurement of night-time BPshould be an important part of clinical practice and ABPMprovides a means for not only improving the diagnosis andmanagement of hypertension but also for ensuring thateffective control of hypertension is achieved throughoutthe entire 24-h period (Box 1)
32 Ambulatory blood pressure monitoringthresholds for clinical practiceAs with conventional BP measurement the levels of BP thatconstitute normality for ABPM have been a subject of much
orized reproduction of this article is prohibitedwwwjhypertensioncom 1733
OrsquoBrien et al
debate over the years [19ndash241w8wndash19w] The issue ismore complex than for conventional measurement becausenormality needs to be defined for both daytime and night-time pressures and outcome data are scarce
In defining normality for ABPM it is necessary to move onfrom diagnostic thresholds determined in a statistical way innormotensive andor hypertensive reference populations tooutcome-driven thresholds The International Database ofAmbulatory blood pressure in relation to CardiovascularOutcome (IDACO) based on 5682 participants followedfor 97 years determined ABPM thresholds which yielded10-year cardiovascular risk (for cardiovascular cardiac andstroke outcomes) corresponding to high BP on officemeasurement (gt14090mmHg) Corresponding thresholdsfor hypertension with ABPM were 1310794 for 24h 1382864 for daytime and 1195708mmHg for night-time [25]
Whereas outcome-driven thresholds are currently avail-able for adults the question remains to be resolved whetherthey are applicable across the whole age range and in allconditions or whether separate recommendations arenecessary for older and very old individuals and for preg-nant women In the case of children and adolescents adifferent approach is needed and therefore thresholdsbased on population distribution have been proposed(See Section 67)
Head et al [26] examined a different approach to deriveage-related and sex-related ABPM equivalents to clinic BPthresholds for diagnosis and treatment of hypertension byaccounting for age and sex They also compared clinicmeasurements taken by nonmedically qualified health pro-fessionals with those taken by doctors to assess whether alsquowhite-coatrsquo effect might have influenced the findings ofprevious studies that were based solely on doctorrsquosmeasurements This analysis provided a range of daytimeABPM measurements equivalent to recognized clinic BPthresholds which when predicted from clinic BP valueswere close to those derived from other outcome analyses
The threshold values in the recent NICE guidelines [4]the JNC 7 guideline [27] and the ESHESC guidelines for2003 2007 and 2013 [12829] and the results of outcomestudies such as IDACO [25] and Ohasama [30] have con-tributed to the definition of consensus values summarizedin Box 2 It is recognized that the levels in Box 2 might beregarded as conservative by some and it is acknowledgedthat further studies are needed to define thresholds moreprecisely particularly in high-risk patients
33 Cost-effectiveness of ambulatory bloodpressure monitoringThe cost-effectiveness of ABPM has been considered from anumber of perspectives First ABPM may enable financialsavings in drug prescribing ABPM is superior to othermeasurement techniques in demonstrating the efficacy of
Box 2 Thresholds for hypertension diagnosis based on ambulatory bloodpressure monitoring
24-h average 13080 mmHg
Awake (daytime) average 13585 mmHg
Asleep (night-time) average 12070 mmHg
Copyright copy Lippincott Williams amp Wilkins Unaut1734 wwwjhypertensioncom
antihypertensive drugs in pharmacological trials [3132]Adjustment of antihypertensive therapy according to ABPMrather than office BP has been shown to result in lessantihypertensive medication being prescribed withoutcompromising target organ involvement [33] It has alsobeen shown that in patients on treatment with BP-loweringdrugs ABPM was a better predictor of cardiovascular out-come than office BP [34] Reduction in office BP due toamelioration of the white-coat effect especially in elderlypatients who have greater BP variability may be attributedwrongly to a BP-lowering effect of antihypertensive medi-cation if ABPM is not used to assess treatment efficacy[35]
Second by identifying patients with white-coat hyper-tension ABPM may improve drug prescribing in a cost-effective manner [36] The cost of care for hypertension isdominated by the long-term occurrence of cardiovascularcomplications and the costs for drug treatment rather thanby the short-term cost for visits and investigations [3720w]
Third ABPM can identify individuals with normal BP inthe office but elevated BP levels in daily life (rsquomaskedhypertensionrsquo) a condition that has been shown to carrythe same adverse prognosis as sustained arterial hyperten-sion both in the clinic and in daily life (see Section 63)
Until recently ABPM is generally cited as being moreexpensive than other measurement techniques though ithas been shown to be cost-effective both in specialistservices and in primary care [3621w] This has been attrib-uted to the fact that only tangible benefits have beenconsidered such as identifying patients with white-coathypertension and the savings that might be made from themore efficient prescribing of BP-lowering drugs Howevercost-effectiveness considerations must be extended toinclude the financial potential of the technique not onlyto improve the diagnosis and management of hypertensionbut also as a means of ensuring that effective control ofhypertension is implemented at community level [9] ABPMis the most effective technique for identifying white-coathypertension which may be present in as many as 20 ofpeople who appear to have hypertension with office BPand these patients may be spared years of unnecessary andexpensive drug treatment which is often not free from side-effects They may also avoid being penalized unnecessarilyfor insurance or employment by having the diagnosis oflsquohypertensionrsquo misapplied [9]
A number of studies have analyzed the costndashbenefitaspects of ABPM Krakoff [36] has shown that potentialsavings of 3ndash14 for cost of care for hypertension and 10ndash23 reduction in treatment days when ABPM was incorp-orated into the diagnostic process On an annual basis thecost of ABPM would be less than 10 of treatment costsOther costndashbenefit analyses have shown that ABPM is mostcost-effective for the diagnosis and management of newlydiagnosed hypertension [921w]
Recently NICE undertook detailed costndashbenefit analysisfor ABPM and showed that the use of ABPM is the most cost-effective method of confirming a diagnosis of hypertensionin a population suspected of having high BP based on aconventional BP screening measurement of more than 14090mmHg and that the technique would result in substantialsavings to the UK National Health Service [438] However
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
the validity of the underlying assumptions by NICE has notbeen universally accepted [39]
Other potential benefits of ABPM that have not beenconsidered by NICE are the savings to be made in havingdrug treatment targeted to achieve 24-h BP control and thesubstantial savings to be made by the prevention of strokeand other cardiovascular consequences of hypertensionwith improved BP control Nor has NICE considered thepotential benefits of identifying the white-coat and maskedhypertension phenomena in treated individuals or of treat-ing nocturnal hypertension which is a major predictorof outcome
In a further extensive study of the cost of ABPM aMarkov model-based probabilistic cost-effectivenessanalysis concluded that ABPM is the most cost-effectivestrategy for the diagnosis of hypertension for men andwomen of all ages mainly by virtue of its potential toreduce misdiagnosis and to direct better targeted treatment[38]
As the cost of ABPM and hypertension managementdiffer greatly from country to country and is dependenton the method of healthcare delivery the cost-effectivenessof ABPM may need to be evaluated at a national level Forexample in Japan it has been estimated that the introduc-tion of ABPM for the management of hypertension hasreduced medical costs by about 948 trillion yen over 10years [40] (see Section 82)
34 Limitations of ambulatory blood pressuremonitoringThe technique of ABPM has many advantages over otheravailable techniques but it has its limitations whichinclude availability the provision of intermittent measure-ments during which the patient is sedentary rather thanlsquoambulatoryrsquo the possibility of inaccurate readings duringactivity and the inability to detect artefactual measure-ments the technique makes demands on the patient timeis needed to fit the device and it may cause discomfortparticularly during the night resulting in resistance fromsome patients to having repeat ABPM [11014] limitedreproducibility when the procedure is not standardized[41] and cost implications although the cost of devicesis reducing and costndashbenefit analyses have shown thatshort-term costs are justified by long-term savings (seeSection 33 Box 3)
Copyright copy Lippincott Williams amp Wilkins Unauth
Box 3 Limitations of ambulatory blood pressure monitoring
Application Limited availability May cause discomfort particularly at night Reluctance to use by some patients especially for repeat
measurement Cost implications (although the cost of devices is reducing
and possibly more cost-effective than office measurements)Function Imperfect reproducibility Provision of intermittent measurements in sedentary rather than
ambulatory conditions Possibility of inaccurate readings during activity Inability to detect genuine artefactual measurements
Journal of Hypertension
4 DEVICES AND SOFTWARE
41 Choosing an ambulatory blood pressuremonitoring device
411 Selecting an accurate deviceAn accurate device is fundamental to all BP measurementsif the device used to measure BP is inaccurate attention tomethodological detail is of little relevance It is acknow-ledged that the accuracy of BP-measuring devices shouldnot be based solely on claims from manufacturers whichcan at times be somewhat misleading Instead independ-ent validation using an established protocol with the resultspublished in peer-reviewed journals should be demanded[4222w] However manufacturers often ignore this recom-mendation and potential purchasers are generally unawareof this requirement assuming ndash not unreasonably ndash that ifa product reaches the market place it will measure BPaccurately The most popular validation protocol is theEuropean Society of Hypertension International Protocol(ESH-IP) and a recent review showed that from thepublication of the first version of the ESH-IP in 2002until June 2010 48 studies of device accuracy have beenreported using the British Hypertension Society (BHS)protocol 38 using the AAMI standard and 104 using theESH-IP 2010 [23w] Thus it seems that the ESH-IPsucceeded in expanding by three-fold to four-fold theuse of validation procedures worldwide compared withthe period before its publication [23w] A criticism bymembers of the AAMI Committee that the reduction inthe number of patients might compromise the validity ofthe protocol [24w] has been shown to be statisticallyunfounded [25w] The availability of the ESH-IP in anon-line version will further facilitate the validation of ABPMdevices [26w]
Since the ESH-IP was first published there has been animprovement in the performance of the oscillometric devi-ces for BP measurement [23w] but protocol violations andmisreporting have been particularly common suggestingthat there is a need for stricter standardization for conduct-ing and reporting a validation study [27w] The revisedversion of the ESH-IP protocol applied tighter validationcriteria for the pass level [42] and the application of thesemore stringent criteria is expected to double the validationfailure rate allowing more accurate devices to enter themarket [23w]
The AAMI protocol requires additional testing for ABPMdevices in 85 patients in the supine seated and standingpositions and stipulates that three devices should beassessed in ambulatory conditions all of which would bevery difficult and costly to perform [4328w] The BHSprotocol which is rarely used now also requires an in-use (field) assessment of ambulatory monitors [44] TheInternational Organization for Standardization (ISO) pro-tocol also requires additional clinical validation in 35patients in standardized conditions of physical activity(after exercise on a bicycle ergometer or treadmill toincrease heart rate by 10ndash20) [45]
It has recently been suggested that the validation ofautomated BP-measuring devices should be complementedby an overall quality check The PANET International
orized reproduction of this article is prohibitedwwwjhypertensioncom 1735
OrsquoBrien et al
Quality Certification Protocol denotes additional criteria ofquality for BP-measuring devices that fulfilled basic vali-dation criteria published in full in peer-reviewed medicaljournals On the basis of this evaluation a quality certifi-cation is released to the manufacturer and published onwwwpressionearteriosanet and wwwdableducationalorg[46]
The majority of devices for ABPM use oscillometry tomeasure BP but some devices also measure BP by micro-phonic detection of the Korotkoff sounds and such devicesneed to have both measurement methods validated accord-ing to accepted validation protocols [29w]
412 Validation requirements for ambulatoryblood pressure monitoring devices in specialpopulationsSeparate validation is required in specific populations suchas children and adolescents pregnant women and theelderly and in certain diseases such as obesity and arrhyth-mias [30w] Patients with arrhythmias children the elderlyand pregnant women present special challenges for vali-dation of oscillometric ABPM devices However althoughABPM devices are used frequently in these patient popu-lations specific validation studies have often not beenperformed this limitation applies also to other methodsof BP measurement such as home and office measure-ments The validation status of ABPM devices in differentpopulations can be checked on dedicated websites (egwwwpressionearteriosanet or wwwdableducationalorg)Although specific validation studies of ABPM devices inthese special populations are desirable in the future devi-ces that have been validated in the general hypertensivepopulation can be used so that high-risk patients are notdenied the benefit of ABPM
ChildrenFour ABPM devices have been validated in children andadolescents [31wndash34w] A number of factors that includeconsent adherence to the validation protocol whichphase to choose for defining DBP size of cuff and leveland range of BP make validation studies in children muchmore difficult than in adults [4735w]
PregnancyA number of ABPM devices have been validated innormotensive and hypertensive women in pregnancyand preeclampsia and although more devices are beingrecommended for use in clinical practice there are severaldevices that are not accurate in pregnancy [484936wndash41w] In pregnancy auscultation of DBP has been contro-versial leading to differences of opinion between mufflingand disappearance of sounds as the criterion for DBP [49]There is now general agreement that disappearance ofsounds is the best measure of DBP [50]
The elderlyValidation data in elderly patients are available only for theSpaceLabs 90207 [42w] It is important to define clearly theage group in which the device is being assessed Individualsover the age of 65 years will also have a higher prevalenceof diseases and conditions that can affect arterial stiffness
Copyright copy Lippincott Williams amp Wilkins Unaut1736 wwwjhypertensioncom
and therefore influence the outcome of validation studiesThe elderly have an increased prevalence of arrhythmiasincluding atrial fibrillation bradycardia and ventriculartachyarrhythmias and are more likely to have inter-armdifferences in pressures due to upper arm arterial diseasewhich would make them unsuitable for validation studies[51]
Patients with arrhythmiasThere are no formal validation studies using establishedprotocols for ABPM devices in this special population Inpatients with arrhythmias it is difficult to standardize theheart rates during validation Good recordings can beobtained with ABPM in most patients although there is atendency for electronic devices to overestimate DBP inpatients with atrial fibrillation [52]
Obese patientsNo validation studies of ABPM monitors have been per-formed in the obese population Obesity has an adverseimpact on vascular stiffness influencing thereby theaccuracy of the oscillometric technique and these patientshave large arms which may complicate recruitment forvalidation studies particularly when a specified range ofcuffs has to be assessed [53]
Patients with renal diseaseOnly one ABPM device has been validated for patients withrenal disease [43w] Validating devices in patients with end-stage renal disease (ESRD) and chronic kidney disease(CKD) presents a number of problems [43w44w] thatinclude finding an available upper extremity the effectof arterial stiffness on the oscillometric methodologyespecially for DBP [54] and the demanding schedule ofdialysis that makes recruitment of patients difficult
413 Additional features for ambulatory bloodpressure monitorsAll ABPM monitors measure BP and pulse rate and mostprovide measurements not only for SBP and DBP but alsofor mean BP and pulse pressure Over the past decadeABPM devices have been developed to measure or calcu-late intermittently or continuously other parameters suchas the ECG pulse wave velocity and central BP Further-more accessories such as position sensors and accelerom-eters for physical activity analysis have been incorporatedto provide a more precise pathophysiological profileMajor limitations of these innovative devices are theirrelatively high price and the need to validate the associatedfunctions according to adequate protocols and to provideevidence for their clinical usefulness Until these require-ments are fulfilled the use of such ABPM devices shouldbe restricted to research laboratories and specializedcenters
Ambulatory blood pressure monitoring and homeblood pressureDevices which can be used either for 24-h ABPM or in a7-day mode to collect multiday BP data are being devel-oped and one has been validated [45w46w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Ambulatory blood pressure monitoring and ECGDevices have been developed allowing 24-h ABPM withcontinuous 24-h ECG in a single procedure Besides theusual well established indications for each of these pro-cedures the interaction between these two signals providescomplementary interrelated information in one procedureThe use of the real heart rate to determine the deflation ratecan provide more precise BP measurement and additionalextra BP measurements can be triggered by abnormal ECGactivities such as arrhythmias and ST segment abnormal-ities Limitations are the relatively high cost of monitors andsoftware the complexity compared to the simple ABPMprocedure and the difficulties in performing validationstudies for the combined functions [47w48w] Thesedisadvantages are offset to some extent by being ableto perform the two procedures simultaneously in olderpatients in whom arterial hypertension and paroxysmalatrial fibrillation often coexist Another development hasbeen the use of spectral analysis of heart rate to provide ameans for improving screening for obstructive sleep apnea(OSA) [49w50w]
Ambulatory blood pressure monitoring and arterialfunctionDevices are being developed that measure arterial stiffnessso as to provide interesting information on 24-h ABPM andon arterial function [51wndash55w]
Ambulatory blood pressure monitoring and positionsensingPosition sensors have been developed to determinewhether the patient is standing or lying during ABPMrecording and this facility allows an estimation of the sleepperiod [5556w]
Ambulatory blood pressure monitoring and activitysensingActivity sensors and accelerometers have been developedfor monitoring patient activity during ABPM so as to providean indirect measure of activity and rest with the formerbeing an estimate of the awake period and the latter ofsleep Some of these sensors are incorporated in the devicewhereas others are complementary accessories placedeither at wrist thigh or chest level [57w]
Ambulatory blood pressure monitoring and centralblood pressureSeveral 24-h oscillometric ABPM monitors use specificalgorithms and software for pulse wave analysis by record-ing 24-h ABPM data as well as calculating central BP [5651wndash53w58wndash61w] Further studies are needed howeverto demonstrate the validity and clinical usefulness of thesedevices which at present should not be used for makingclinical decisions
42 Software for ambulatory blood pressuremonitoring data analysisRecommendations on procedures for ABPM use tend toconcentrate on the accuracy of the devicersquos hardware withlittle attention being paid to software presentation and
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
analysis of ABPM data As a consequence the practisingphysician who has to interpret the considerable amount ofdata provided by ABPM is often faced with a bewilderingreport with reams of paper containing plots histogramsand data analysis that have little relevance for clinicalpractice It is important for ABPM software programs tobe suitable for the intended use of the device For examplein a busy general practice perhaps only basic data givingaverage 24-h daytime and night-time values and a visualplot are all that will be required whereas for researchpurposes statistical detail on the windows of the 24-hprofile and other indices may be required [10] A recentstudy has stressed that whereas monitors for ABPM aresubject to extensive validation protocols there is no inter-national guideline on the software processing of the col-lected raw data to prevent error being introduced by thesoftware permutations An example of software-inducederror was demonstrated for the SpaceLabs Report Manage-ment System 92506 which showed errors in 92 of reportsamounting to a numerical difference between printout andon-screen hourly averages ranging from 37 to 18mmHgfor SBP and from 16 to 10mmHg for DBP [62w] Anadditional problem can arise from the calculation of 24-haverage BP values that are not weighted for the differentnumber of hourly measurements during daytime and night-time weighted hourly BP values have been shown to bemore reliable than calculations based on the average of allindividual readings [57]
The use of ABPM in clinical practice can be facilitated bystandardizing the graphic presentation of ABPM datamuch as is the case for ECG recordings so that the pres-entation of data is independent of the type of ABPMmonitor used and the user is not required to becomefamiliar with a variety of programs Standardization alsofacilitates the interchange of ABPM recordings betweendatabases such as a hospital and primary care practiceMoreover if ABPM software programs provide a printedreport of the standardized ABPM data with a validatedinterpretative report [58] (signed by the physician in chargeof the service whenever legally required) doctors andnurses unfamiliar with the technique are assisted inlearning the variety of patterns generated by ABPM andbecause an individualized physician report is not a require-ment in most cases the cost of ABPM is reduced [110](Box 4)
421 Software requirementsThe following facilities are recommended for ABPM soft-ware in clinical practice [1910]
Clinical reportThe following information should be available in a one-page report
or
1
ize
Standardized plot format with each BP measurementon the vertical axis and time of day on horizontal axiswith different windows of the 24-h period identifiedand normal bands clearly demarcated The sleep timeinterval used to calculate asleep BP should be indi-cated (shaded) and preferably based on the indivi-dualsrsquo sleep time report (diary cards) In the plot the
d reproduction of this article is prohibitedwwwjhypertensioncom 1737
Cop
Box 4 Software requirements
Clinical report Ambulatory blood pressure measurement analysis and report should be standardized independent of the monitor type Standardized plot of all the blood pressure measurements with daytime and night-time windows and normal blood pressure bands demarcated Average SBP DBP and heart rate to be displayed Nocturnal blood pressure decline () for SBP and DBP Summary statistics for time-weighted average SBP and DBP and heart rate for the 24-h period daytime and night-time with standard deviations and number
of valid blood pressure readings Facility for showing error readings if requiredOptional requirements Automated software generated interpretative report indicating the normal or abnormal patterns and whether the requirements for a valid recording are
fulfilled Facility to plot heart rate and mean blood pressure Trend report for comparing repeated ambulatory blood pressure measurement recordings Ability to centrally host dataResearch report Data storage and raw data export capability for research analysis and audit Parameters include variability measures (such as 24-h SD 24-h weighted SD average real variability coefficient of variation) area under the curve
calculations blood pressure load parameters ratendashpressure product trough and peak levels smoothness index (the last two parameters requiring ABPMdata before and during treatment to be available) cusum-derived statistics and ambulatory arterial stiffness index
OrsquoBrien et al
1738
upper value of the Y-axis should not be fixed butadjustable to the highest BP value recorded in orderto maximize the graphic presentation of BP variationsover the 24-h period A plot of SBP and DBP through-out the 24-h period with a facility for plotting heartrate and mean BP so as to provide evidence ofcircadian behavior should be provided
2
Summary statistics for time-weighted SBP and DBPand heart rate in the windows of the 24-h period andseparately for the awake and asleep subperiods withthe respective standard deviations and the number ofvalid BP readings included in the analysis and afacility for indicating the time of going to bed andawakening
3
Medication details
4
Facility for showing error readings if required
Interpretative reportTo remove the variance associated with the ABPMinterpretation by human observers and to simplify theevaluation of results in routine clinical practice for thoseunfamiliar with the technique there should be an auto-mated software-generated interpretative report indicatingnormal or abnormal BP patterns and whether there aresufficient measurements for the recording to be valid [10]The interpretative report should be validated by testing thecomputer-generated report against reports from experts[5859]
Trend reportThe provision of a trend report allows ABPMs to be com-pared over time to demonstrate the response to changes inmanagement If ABPM is to be used to achieve better BPcontrol it is important for prescribing doctors (and patients)to be able to see whether medication is achieving controlthroughout the entire 24-h period
Research reportThe system should be capable of storing data for detailedanalysis for research and audit according to evidence-based
yright copy Lippincott Williams amp Wilkins Unautwwwjhypertensioncom
definitions for time-weighted arithmetic and mean valuesfor measures of BP level In view of evidence that short-term BP variability may give information over and abovemean BP levels and that reduction in 24-h BP variabilitymay be beneficial [63w] time-weighted and other measuresof short-term BP variability are helpful for on-goingresearch in this area Informative indices associated withoutcome such as area under the curve calculations BP loadparameters trough and peak levels the smoothness index(the last two parameters requiring ABPM data before andduring treatment to be available) cusum-derived statisticsand most recently the ambulatory arterial stiffness index(AASI) should also be provided [6061] The system shouldbe capable of storing and exporting raw data for researchpurposes and additional analyses [606163w]
422 Indices derived from ambulatory bloodpressure monitoring recordingsAverage BP values (over 24 h daytime and night-time) areundoubtedly the most important parameters obtained fromABPM recordings based on outcome data However alarge number of additional indices with promising clinicalevidence may be derived from ABPM recordings and someof them are occasionally included in the reports generatedby ABPM systems
Blood pressure loadThis index is defined as the percentage of readings in agiven period (24-h day or night) which exceed a prede-fined threshold value typically set at the proposed nor-malcy level for average BP values of that period The aim ofBP load is to quantify the number of readings with elevatedBP and mathematically it depends on both average BPlevels and distribution of BP readings [62] Although intheory clinically appealing and thus commonly incorpor-ated in the ABPM software this index has a number oflimitations Firstly there is no evidence that the thresholdsdefined for average BP values have any prognostic meaningwhen applied to single BP measurements Secondly whencomparing recordings with similar average BP levels differ-ences in BP load can be largely explained by differences in
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
BP variability making this index largely redundant ThirdlyBP load does not contain the prognostically importantinformation on how much the threshold level has beenexceeded To overcome the latter limitation it has beenproposed to modify the classic BP load definition bycalculating the total area under the timendashpressure curvewhen BP exceeds the threshold [63] Finally although somestudies support the usefulness of BP load in predictingorgan damage [6464w] it has never been convincinglydemonstrated that it provides any additional and clinicallyrelevant information independently of what is obtained byfocusing on average BP values The use of BP load inchildren has also been examined but it has not been foundhelpful in diagnosis [65w]
Ratendashpressure productThis index which is defined as heart rate multiplied by SBPis used as an index of myocardial work during exercise andit has prognostic relevance [66w] The availability of bothheart rate and BP data in ABPM makes it possible to obtainthe index readily especially if ABPM is accompanied byactigraphy [65] Although potentially promising the clinicalapplication of this index requires further research
rsquoVascularrsquo indicesSeveral ABPM-based indices have been proposed to pro-vide information on vascular wall properties Their ration-ale is based on the observation that the stiffness of thearterial wall increases when it is being stretched in patientswith impaired arterial wall elasticity SBP increases moresteeply than DBP whereas in a patient with elastic arteriesSBP and DBP increase in parallel The AASI which iscalculated as 1 ndash slope of regression of DBP on SBP isreadily obtainable from ABPM [6066]
AASI appears to have a direct relationship to carotidndashfemoral pulse wave velocity (a validated index of largearteriesrsquo stiffness) and an independent relationship withcardiovascular outcomes [606167wndash70w] Howeverthe ability of AASI to reflect arterial stiffness has beenchallenged because of its dependence on nocturnal BP falland the fact that it implies the use of asymmetric regressionpossibly affecting the precision of slope estimation[67ndash6971w72w] Modifications to AASI have been pro-posed but further data are awaited as to their ability tosurpass AASI in predicting outcome [73w74w]
The QndashKd interval which measures the time intervalbetween the onset of the QRS on the electrocardiogram (Q)and the last Korotkoff sound (K) corresponding to thediastolic pressure (d) has also been shown to have prog-nostic value [70]
Indices for indicating the pattern of treatment-induced changes in 24-h blood pressure loweringTwo principal indices are available for assessing thesmoothness and consistency of antihypertensive treatmenteffect over 24 h with ABPM The trough-to-peak ratio is theratio between BP reduction achieved by treatment at theend of dosing interval (trough which for drugs adminis-tered once daily means 24 h after the last dose intake) andpeak BP reduction usually achieved a few hours after dose
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
intake [7172] The trough-to-peak ratio is characterized by ahigh degree of variability in individual patients and istherefore not suitable for application to clinical practice[73] The smoothness index is calculated as the ratiobetween the average of hourly BP reductions over 24 hand the standard deviation (SD) of such an average valuethus integrating information on the size of BP reduction bytreatment and on its homogeneity throughout the 24-hperiod [7173] The smoothness index is highest for potentdrugs or drug combinations which also provide the mosthomogeneous BP reduction It is more reproducible thanthe troughpeak ratio [7173] and predicts treatment-induced changes in indices of organ damage includingleft ventricular mass and carotid arterial wall thickness[75w] A recent meta-analysis has provided informationon clinical determinants of the smoothness index suchas age ethnicity sex and smoking [74] The relevance ofthese indices in predicting the impact of treatment onoutcome and the reference values remain to be assessed
5 PROCEDURE
51 Training requirementsThe technique of ABPM is a specialized one and should beapproached with the care reserved for any such procedureAn understanding of the principles of traditional BPmeasurement cuff fitting monitor function and analysisand interpretation of ABPM data is required In practice anurse with an interest and experience in hypertension canmaster the use of ABPM devices after a relatively brieftraining However the interpretation of ABPM profilesrequires experience in the technique which is best pro-vided by the doctor in charge of an ABPM service [19]
52 Fitting an ambulatory blood pressuremonitorTime needs to be given to fitting the monitor and preparingthe patient for the monitoring period if good results are tobe obtained [19] The key to successful ABPM is educatingthe patient on the process of monitoring and the instruc-tions should be explained and printed on a diary card Inclinical practice measurements are preferably performedon a routine working day Although ABPM is best notperformed while patients are admitted to hospital becausehospitalization leads to underestimation of BP and over-diagnosis of nondippers [10] there are occasions such asthe evaluation of severely resistant hypertension andassessment of patients following a stroke when ABPM inhospital may be indicated
The frequency of measurement during the 24-h period isgenerally not more than every 15 min (which could inter-fere with normal activity) nor less than every 30min (whichcould give an inadequate number of measurements) Morefrequent measurements at night may disturb sleep andsleep disturbance has been shown to reduce the prognosticvalue of ABPM [75] To improve reproducibility repetitionof ABPM should be performed on like days for example onroutine working or recreational days A diary card can beused to record symptoms and events that may influenceABPM measurements
orized reproduction of this article is prohibitedwwwjhypertensioncom 1739
OrsquoBrien et al
53 Explanation to patientThe first step is adequate explanation of the procedure in anattempt to allay anxiety especially in nervous patientsPatients having ABPM for the first time should be told thatthere is minor discomfort caused by inflation of the cuff It isimportant to emphasize to the patient to follow hisherusual daily activities but as much as possible to remain stillwith the arm relaxed and not extended or contracted atheart level during each BP measurement [19] It can behelpful to have patients record periods of stress the time ofmeals the time of a siesta the time of going to bed andrising the quality of sleep and the time and type ofdrug ingestion
Box 5 Evaluation of ambulatory blood pressure monitoring data
Definition of daytime and night-time Daytime and night-time intervals are best defined using sleeping times
reported by individual usersrsquo diary cards (awake and asleep periods) Fixed narrow time intervals can be applied by discarding transition
periods between daytime and night-time (eg daytime defined as0900ndash2100 h and night-time 0100ndash0600 h)
Editing requirements Editing is not necessary for calculating average 24-h daytime and
night-time values The ambulatory blood pressure monitoring should be repeated if thefollowing criteria are not met
24-h recording with at least 70 of expected measurements20 valid awake (0900 to 2100 h)7 valid asleep (0100 to 0600 h)Blood pressure measurements at 30-min intervalsFor research purposes at least two valid daytime and one valid
night-time measurement per hour
54 Identification of daytime and night-timeperiods and editing ambulatory blood pressuremonitoring dataOne simple and popular method for identifying daytimeand night-time subperiods is to assess the time of awaken-ing and sleeping from diary card entries Another method isto use a fixed-narrow time interval approach in which forexample the retiring (2101 to 0059 h) and rising (0601 to0859 h) periods (which are subject to considerable vari-ation) are eliminated with the daytime period being from0900 to 2100 h and night-time from 0100 to 0600 h in thisway the variations in the time spent in bed that may existbetween the young and the old and in different culturesare to some extent eliminated from the analysis [176w]This method has the disadvantage of eliminating infor-mation on the white-coat window on the early phase ofnight sleep when dipping can be most evident and onthe early morning surge of BP which may be associatedwith cardiovascular events However these windows canbe analyzed separately for research or if considered import-ant in practice In countries where a daytime siesta ispopular a record of sleeping times both during day andnight is important and ABPM software should be able toadjust for this otherwise there may be underestimation ofthe nocturnal BP dip and overdiagnosis of nondippers[77w]
Many statistical techniques exist for editing ABPMrecords and no one method is ideal [176w] The detec-tion of artefactual readings and the handling of outliervalues (which may or may not be erroneous) have indeedbeen the subject of debate [76w] There are a number ofways of separately analyzing BPs recorded during the dayand night [7678w] Several automatic procedures havebeen proposed to reject outlying measurements based ona univariate multivariate or temporal approach Morecomplex procedures requiring the intervention of theobserver have been proposed but they are time consum-ing and not suitable for clinical practice [77] It has beenshown that rejection of outliers may alter the results ofABPM in individual patients sometimes significantlyaffecting average SBP levels [777879w] Editing pro-cedures can reduce mean systolic ABPM by 4 mmHg incomparison with unedited recordings thereby decreasingthe likelihood of diagnosing sustained hypertension Inone study the prevalence of sustained hypertension wasdecreased by 6ndash10 when several editing methods were
Copyright copy Lippincott Williams amp Wilkins Unaut1740 wwwjhypertensioncom
applied to raw 24-h data [79w] To make the results ofdifferent laboratories comparable common editingcriteria for ABPM should be used The problem is toestablish which of the methods proposed in the literatureprovides the most reliable data While awaiting moreobjective criteria to identify a universally acceptable edit-ing procedure we recommend that editing is not necess-ary for calculating average 24-h daytime and night-timevalues and that only physiologically impossible readingsshould be deleted from recordings However when thereare excessive artefacts in a tracing a repeat recordingrather than editing should be performed Some editingmight be required when focusing on analysis of BPvariability for the quantification of which the presenceof artefacts may introduce appreciable errors If editing isconsidered necessary a method proposed by Casadeiet al [80w] and modified by Winnicki et al [78] providescomparable performance to other proposed editing pro-cedures
There are no firm data on which to base recommen-dations for a satisfactory ABPM recording but the recom-mendation for having at least 70 of expectedmeasurements provides a basic working recommendationfor clinical practice This figure will be influenced by theperiod demarcated as daytime (awake) or night-time(asleep) periods and by the number of measurementsselected (usually 30-min but often 15 or 20-min intervals)In the previous ESH guideline on measurement it wasrecommended that there should be a minimum of 14measurements during the day and seven measurementsat night [1] Having considered what evidence is availableand the practical issues of performing repeat ABPM inpractice it seems reasonable to increase the minimum ofdaytime measurements to 20 while retaining a minimumseven measurements at night based on measurementsbeing performed every 30min and with fixed time periodsbeing used to define day (0900 to 2100 h) and night (0100 to0600 h) [1] (Box 5)
55 The arm for measurementABPM is best measured in the nondominant arm so as tointerfere as little as possible with daily activity unless there
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
has been documented evidence of a difference in BPbetween arms in which case the arm known to have thehigher BP values should be chosen [1] It is commonpractice for BP to be measured by a conventional techniqueat the same time as an ABPM monitor is being fitted and todetermine whether there is a discrepancy between thetechniques However BP variability is such that any suchcomparison has little validity and to determine a significantdifference it is necessary to perform simultaneousmeasurement according to a definitive protocol and thisis not feasible in practice [42] Because of these limitationsthe practice of performing a comparative measurement isnot recommended
56 Selecting the appropriate cuff and bladderThere is unequivocal evidence that either too narrow ortoo short a bladder (undercuffing) will cause overesti-mation of BP so-called lsquocuff hypertensionrsquo and there isgrowing evidence that too wide or too long a bladder(overcuffing) may cause underestimation of BP Under-cuffing has the effect in clinical practice of overdiagnos-ing hypertension and overcuffing leads to hypertensivepatients being diagnosed as normotensive Either even-tuality has serious implications for the epidemiology ofhypertension and for clinical practice [79] It is importanttherefore to select a cuff containing an inflatable bladderof correct length and width for the arm in which ABPM isto be measured All ABPM devices should provide cuffscontaining bladders for small medium and large-sizedarms as recommended in international guidelines[18081] However in many obese individuals the largebladder sizes cannot be used because the arm length istoo short to accommodate the bladder [81w] Anotherproblem is that the cylindrical shape of the commonlyused cuffs does not always wrap snugly around conical-shaped arms in obese and very muscular arms[8282w83w] Recently novel oscillometric homemonitors with cuff technology that allows a singlefixed-size cuff to be used on a wide range of arm circum-ferences have been developed [84wndash87w]
Another issue that needs consideration is the possibilitythat the discomfort caused by inflation of a large cuff inobese patients might cause elevation of BP This issuebecomes more important during ABPM because ofrepeated measurement especially during night-time sleepOscillometric devices for home use that measure BP duringcuff inflation may induce less discomfort because themeasurement is completed before maximal inflation[84w88w] However to date no study has specificallyaddressed this issue
Forearm BP measurement may have to be consideredwhen extreme obesity makes upper arm BP measurementimpossible BP measurements tend to be higher with fore-arm compared with upper arm measurement but meth-odological differences in these studies make it difficult toprovide recommendations for all populations [8389wndash94w] Despite the questionable accuracy of forearm BPmeasurement it may be the only acceptable option forABPM in individuals with very large upper arms providedthe patient is instructed to keep the forearm at heart levelduring measurement [94w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
No wrist devices have been validated for ABPM whereastechnology for continuous beat-to-beat monitoring ofambulatory BP in the finger has been developed usingthe volume-clamp method first described by Penaz [95w]A number of studies that compared this technology withintraarterial or noninvasive BP measurement showedunderestimation of BP particularly diastolic yet it remainsa practical alternative to intraarterial measurement for theevaluation of beat-to-beat BP changes and variability inresearch studies [8496wndash98w]
57 Conditions in which ambulatory bloodpressure monitoring may be difficult toperform
Obese patientsObesity is a well established major risk factor for hyperten-sion with higher prevalence in specific population groupssuch as patients with diabetes mellitus [99w] or OSA [100w]Despite the increasing prevalence of obesity worldwide[101w] and the close link between obesity and hyperten-sion scarce data are available on the application of ABPM inobese and extremely obese individuals ABPM is oftenrequired in these individuals and technical difficultiesshould not exclude them from such a valuable technology[79] The problem of miscuffing in obese pregnant womenmay result in diagnostic discrepancies [85]
Patients with atrial fibrillationBP measurement in patients with atrial fibrillation is lessprecise as this type of arrhythmia is accompanied byincreased beat-to-beat BP variability due to variations inventricular filling time stroke volume and contractilityInternational guidelines [181] recognize the relatively poorprecision of a single BP measurement and recommendrepeated readings in order to improve the accuracy ofestimates Theoretically ABPM should fulfill this stipulationas it provides a relatively high number of readings in a shortperiod of time Unfortunately published evidence regard-ing the role of ABPM in patients with arrhythmias andspecifically in patients with atrial fibrillation is scarce
Patients with atrial fibrillation have been usuallyexcluded from trials using ABPM as well as from validationprotocols of ABPM devices Four studies have addressedthe possible value of ABPM in patients with atrial fibrillation[48w102wndash104w] The evidence from these studiessuggests that ABPM may be useful in these patients pro-vided its limitations are taken into account The proportionof readings with errors the variability of BP and therepeatability coefficients do not appear to be different fromthose in patients in sinus rhythm DBP measured using anABPM monitor in patients with atrial fibrillation appears tobe relatively higher than that obtained with the traditionaloffice measurement or by the same ABPM procedure whenthe patient achieves sinus rhythm This finding is supportedby a review and meta-analysis of studies that validatedelectronic devices in patients with sustained atrial fibrilla-tion which showed consistent overestimation of DBP [52]In spite of this and although larger trials in patients on atrialfibrillation are recommended there is no reason to exclude
orized reproduction of this article is prohibitedwwwjhypertensioncom 1741
OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
Cop
OrsquoBrien et al
1732
54 Identification of daytime and night-time periodsand editing ABPM data
55 The arm for measurement56 Selecting the appropriate cuff and bladder57 Conditions in which ABPM may be difficult to
perform
yrigw
ICAL INDICATIONS FOR ABPM
CLIN
6
61 Role of ABPM in the diagnosis of hypertension62 White-coat phenomena
621 White-coat hypertension622 White-coat effect
63 Masked phenomena631 Masked hypertension632 Masked uncontrolled hypertension
64 Abnormal 24-h blood pressure patterns641 Daytime hypertension642 Siesta dippingpostprandial hypoten-
sion643 Nocturnal hypertension644 Dipping nondipping extreme dipping
and rising645 Morning hypertension and morning
BP surge646 Obstructive sleep apnea
65 Assessment of treatment651 BP variability and treatment652 Assessing efficacy of blood pressure
control653 Resistant hypertension
66 Hypertension in the elderly67 Hypertension in children and adolescents68 Hypertension in pregnancy69 Hypertension in high-risk patients
691 Diabetes692 Stroke693 Coronary heart disease694 Chronic kidney disease
610 Ambulatory hypotension611 Hypertension in Parkinsonrsquos disease612 Endocrine hypertension613 Follow-up
6131 When to repeat ABPM6132 ABPM versus Home BP
h
t copy Lwwjhy
ip
ABPM IN RESEARCH
7
71 ABPM in pharmacological research72 Regulatory recommendations for pharmacologi-
cal studies73 ABPM in outcome studies
IMPLEMENTATION OF ABPM IN CLINICAL
8
PRACTICE81 General principles82 Financial considerations83 Specialist clinics84 Primary care85 Pharmacies86 Healthcare providers87 ABPM registries and databases
871 Spanish registry872 Italian registry873 Irish registry874 Japanese registry
ppincott Williams amp Wilkins Unauthorizertensioncom
875 Australian registry876 IDACO database877 ARTEMIS registry878 Ambulatory blood pressure international
database
ed r
eprod
S
REFERENCE
1 INTRODUCTIONThe Working Group on Blood Pressure Monitoring ofthe European Society of Hypertension (ESH) publishedrecommendations for blood pressure (BP) measurementin 2003 [1] and a guideline for home BP measurement(HBPM) in 2008 [2] Ambulatory blood pressure monitoring(ABPM) is a subject of considerable scientific interest withover 10 000 papers listed on PubMed in 2012 In 2001 theUnited States Center for Medicare and Medicaid Servicesapproved ABPM for reimbursement for the identification ofindividuals with white-coat hypertension [3] Since thenhealthcare providers in many other countries providereimbursement for ABPM and in 2011 the National Institutefor Health and Clinical Excellence (NICE) in the UnitedKingdom recommended that ABPM should be offered as acost-effective technique to all people suspected of havinghypertension [4]
One of the first meetings to examine the potential ofABPM was held in Ghent in 1978 [5] The ESH WorkingGroup on Blood Pressure Monitoring has held severalconsensus conferences on ABPM since the first one inBerlin over 20 years ago [6] The most recent one was heldin Milan in 2011 at which the technique was comprehen-sively reviewed It was agreed that a writing committeeconsisting of Eoin OrsquoBrien Gianfranco Parati and GeorgeStergiou should draft two documents ndash a comprehensivereview of the scientific evidence for ABPM that was pre-sented at the Milan conference taking into considerationalso relevant publications up to the end of January 2013 (thepresent paper) and a second short paper with conciseinstructions as tohow thebest information couldbeobtainedfrom 24-h ABPM in clinical practice A number of drafts werecirculated to all the participants in theConsensus Conferencefor their comments and suggestions and the final version ofthe present paper is based on the agreed comments from 34international experts Data from randomized controlled trialsof sufficient power with ABPM are still small and this limitsformal grading of recommendations based on the availableevidence As the number of references cited in this paper islarge and in the interest of saving journal space somereferences have been listed in the supplementary filehttplinkslwwcomHJHA283 that accompanies thispaper In the text citations these references are identifiedby the letter w after the reference number
2 HISTORICAL PERSPECTIVETraditionally BP in the office or clinic has been assessedwith the auscultatory technique which was introduced intoclinical medicine at the beginning of the twentieth centuryand which has survived to this day in clinical practiceAlthough the technique is inherently accurate it is
uction of this article is prohibitedVolume 31 Number 9 September 2013
Box 1 Advantages of ambulatory blood pressure monitoring over clinicblood pressure
Gives a larger number of readings than office blood pressuremeasurement
Provides a profile of blood pressure behavior in the patientrsquosusual daily environment
Allows identification of white-coat and masked hypertensionphenomena
Demonstrates nocturnal hypertension Assesses blood pressure variability over the 24-h period Assesses the 24-h efficacy of antihypertensive medication Is a stronger predictor of cardiovascular morbidity and mortality
than office measurement
Guideline
dependent on observer attention to detail which is oftenlacking and it provides only a momentary measurement ofBP usually under circumstances that can influence the levelof BP being measured To overcome these serious meth-odological problems techniques for obtaining automatedprofiles of BP over 24 h and measures of BP in the homesetting have been developed
ABPM has been available in one form or another forsome 50 years having been developed initially to study thecircadian changes in BP and to determine the influence ofBP-lowering drugs on the 24-h profile The first major breakwith traditional BP measurement was the introduction of adirect intraarterial technique for the measurement of BPover the 24-h period The data on antihypertensive drugefficacy provided by studies using this system were particu-larly valuable because they provided continuous BPmeasurement throughout the day and night but use ofthe technique was limited by safety and ethical consider-ations Efforts were focused therefore on developing adevice that would record ambulatory BP noninvasively andin the 1960s the Remler device which was capable ofmeasuring BP intermittently during the daytime periodprovided clinicians with a new technique for assessingBP This device was limited by having to be operated bythe patient which made measurement of BP impossibleduring sleep The next technological advance was theintroduction of fully automated devices that could measureBP intermittently at predetermined intervals over the 24-hperiod This class of devices provided a methodology thatwas applicable not only for research but also for use inroutine clinical practice [7ndash101w]
3 GENERAL CONSIDERATIONS
31 Why is ambulatory blood pressuremonitoring superior to conventional bloodpressure measurementTraditionally office BP measurement has been performedusing a sphygmomanometer and stethoscope Recentlyautomated office BP measurement has been proposed asan alternative to traditional measurement Automated officeBP is the mean of multiple BP readings recorded with a fullyautomated device with the patient resting quietly alone inthe officeclinic [11] It has several advantages over manualBP especially in routine clinical practice by virtually elim-inating office-induced increases in BP improving accuracyminimizing observer error and providing a more stand-ardized measurement technique using an automated oscil-lometric sphygmomanometer [2w] The mean automatedoffice BP for diagnosing hypertension is similar to the meanawake ambulatory BP and home BP (13585 mmHg)Preliminary data suggest that automated office BP is a betterpredictor of target organ damage [3w4w] especially com-pared with routine manual office BP which correlatespoorly with intermediate end-points such as left ventricularmass [5w] Longitudinal clinical outcome studies with auto-mated office BP have not yet been reported
BP recorded in the patientrsquos home is a significantly betterpredictor of future cardiovascular risk than is office BPStandard protocols have been developed for recordinghome BP [2] and include the mean of duplicate readings
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
taken twice daily for 7 consecutive days with readings fromthe first day excluded The cut-point for hypertension usinghome BP is the same as for the awake ambulatory BP(13585 mmHg) In order to avoid reporting bias [12] ahome BP recorder with a memory for storing readingsshould be used and the patient should take the device tothe physicianrsquos office to have the mean home BP verifieddirectly from the devicersquos display More recently remotetransmissions of home BP readings [13] is becoming avail-able allowing BP readings recorded in the home to beautomatically sent to a data collection center via a tele-phone modem or internet link and from there forwarded tothe physicianrsquos office
The advantages of ABPM which have been stated incomprehensive reviews [11014] have influenced recom-mendations for the technique to be used much more widelyin clinical practice [15ndash186w7w] These advantages maybe briefly summarized as follows (Box 1) first and fore-most ABPM simply gives many more measurements thanconventional BP measurement and usual BP is reflectedmore accurately by repeated measurements ABPM pro-vides a profile of BP away from the medical environmentthereby allowing identification of individuals with a white-coat response or masked hypertension ABPM can demon-strate a number of patterns of BP behavior over 24 h thatmay be relevant to clinical practice such as nocturnalhypertension or increased BP variability by showing BPbehavior in different windows of a 24-h period such as thewhite-coat and nocturnal periods as well as the BP fluctu-ations triggered by environmental stimuli it is possible toassess the efficacy of antihypertensive medication through-out the day and night rather than relying on a casual BPABPM is a stronger predictor of cardiovascular morbidityand mortality than conventional measurement and evi-dence is growing that nocturnal BP measured by ABPMis an important predictor of cardiovascular outcome fromwhich it follows that the measurement of night-time BPshould be an important part of clinical practice and ABPMprovides a means for not only improving the diagnosis andmanagement of hypertension but also for ensuring thateffective control of hypertension is achieved throughoutthe entire 24-h period (Box 1)
32 Ambulatory blood pressure monitoringthresholds for clinical practiceAs with conventional BP measurement the levels of BP thatconstitute normality for ABPM have been a subject of much
orized reproduction of this article is prohibitedwwwjhypertensioncom 1733
OrsquoBrien et al
debate over the years [19ndash241w8wndash19w] The issue ismore complex than for conventional measurement becausenormality needs to be defined for both daytime and night-time pressures and outcome data are scarce
In defining normality for ABPM it is necessary to move onfrom diagnostic thresholds determined in a statistical way innormotensive andor hypertensive reference populations tooutcome-driven thresholds The International Database ofAmbulatory blood pressure in relation to CardiovascularOutcome (IDACO) based on 5682 participants followedfor 97 years determined ABPM thresholds which yielded10-year cardiovascular risk (for cardiovascular cardiac andstroke outcomes) corresponding to high BP on officemeasurement (gt14090mmHg) Corresponding thresholdsfor hypertension with ABPM were 1310794 for 24h 1382864 for daytime and 1195708mmHg for night-time [25]
Whereas outcome-driven thresholds are currently avail-able for adults the question remains to be resolved whetherthey are applicable across the whole age range and in allconditions or whether separate recommendations arenecessary for older and very old individuals and for preg-nant women In the case of children and adolescents adifferent approach is needed and therefore thresholdsbased on population distribution have been proposed(See Section 67)
Head et al [26] examined a different approach to deriveage-related and sex-related ABPM equivalents to clinic BPthresholds for diagnosis and treatment of hypertension byaccounting for age and sex They also compared clinicmeasurements taken by nonmedically qualified health pro-fessionals with those taken by doctors to assess whether alsquowhite-coatrsquo effect might have influenced the findings ofprevious studies that were based solely on doctorrsquosmeasurements This analysis provided a range of daytimeABPM measurements equivalent to recognized clinic BPthresholds which when predicted from clinic BP valueswere close to those derived from other outcome analyses
The threshold values in the recent NICE guidelines [4]the JNC 7 guideline [27] and the ESHESC guidelines for2003 2007 and 2013 [12829] and the results of outcomestudies such as IDACO [25] and Ohasama [30] have con-tributed to the definition of consensus values summarizedin Box 2 It is recognized that the levels in Box 2 might beregarded as conservative by some and it is acknowledgedthat further studies are needed to define thresholds moreprecisely particularly in high-risk patients
33 Cost-effectiveness of ambulatory bloodpressure monitoringThe cost-effectiveness of ABPM has been considered from anumber of perspectives First ABPM may enable financialsavings in drug prescribing ABPM is superior to othermeasurement techniques in demonstrating the efficacy of
Box 2 Thresholds for hypertension diagnosis based on ambulatory bloodpressure monitoring
24-h average 13080 mmHg
Awake (daytime) average 13585 mmHg
Asleep (night-time) average 12070 mmHg
Copyright copy Lippincott Williams amp Wilkins Unaut1734 wwwjhypertensioncom
antihypertensive drugs in pharmacological trials [3132]Adjustment of antihypertensive therapy according to ABPMrather than office BP has been shown to result in lessantihypertensive medication being prescribed withoutcompromising target organ involvement [33] It has alsobeen shown that in patients on treatment with BP-loweringdrugs ABPM was a better predictor of cardiovascular out-come than office BP [34] Reduction in office BP due toamelioration of the white-coat effect especially in elderlypatients who have greater BP variability may be attributedwrongly to a BP-lowering effect of antihypertensive medi-cation if ABPM is not used to assess treatment efficacy[35]
Second by identifying patients with white-coat hyper-tension ABPM may improve drug prescribing in a cost-effective manner [36] The cost of care for hypertension isdominated by the long-term occurrence of cardiovascularcomplications and the costs for drug treatment rather thanby the short-term cost for visits and investigations [3720w]
Third ABPM can identify individuals with normal BP inthe office but elevated BP levels in daily life (rsquomaskedhypertensionrsquo) a condition that has been shown to carrythe same adverse prognosis as sustained arterial hyperten-sion both in the clinic and in daily life (see Section 63)
Until recently ABPM is generally cited as being moreexpensive than other measurement techniques though ithas been shown to be cost-effective both in specialistservices and in primary care [3621w] This has been attrib-uted to the fact that only tangible benefits have beenconsidered such as identifying patients with white-coathypertension and the savings that might be made from themore efficient prescribing of BP-lowering drugs Howevercost-effectiveness considerations must be extended toinclude the financial potential of the technique not onlyto improve the diagnosis and management of hypertensionbut also as a means of ensuring that effective control ofhypertension is implemented at community level [9] ABPMis the most effective technique for identifying white-coathypertension which may be present in as many as 20 ofpeople who appear to have hypertension with office BPand these patients may be spared years of unnecessary andexpensive drug treatment which is often not free from side-effects They may also avoid being penalized unnecessarilyfor insurance or employment by having the diagnosis oflsquohypertensionrsquo misapplied [9]
A number of studies have analyzed the costndashbenefitaspects of ABPM Krakoff [36] has shown that potentialsavings of 3ndash14 for cost of care for hypertension and 10ndash23 reduction in treatment days when ABPM was incorp-orated into the diagnostic process On an annual basis thecost of ABPM would be less than 10 of treatment costsOther costndashbenefit analyses have shown that ABPM is mostcost-effective for the diagnosis and management of newlydiagnosed hypertension [921w]
Recently NICE undertook detailed costndashbenefit analysisfor ABPM and showed that the use of ABPM is the most cost-effective method of confirming a diagnosis of hypertensionin a population suspected of having high BP based on aconventional BP screening measurement of more than 14090mmHg and that the technique would result in substantialsavings to the UK National Health Service [438] However
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
the validity of the underlying assumptions by NICE has notbeen universally accepted [39]
Other potential benefits of ABPM that have not beenconsidered by NICE are the savings to be made in havingdrug treatment targeted to achieve 24-h BP control and thesubstantial savings to be made by the prevention of strokeand other cardiovascular consequences of hypertensionwith improved BP control Nor has NICE considered thepotential benefits of identifying the white-coat and maskedhypertension phenomena in treated individuals or of treat-ing nocturnal hypertension which is a major predictorof outcome
In a further extensive study of the cost of ABPM aMarkov model-based probabilistic cost-effectivenessanalysis concluded that ABPM is the most cost-effectivestrategy for the diagnosis of hypertension for men andwomen of all ages mainly by virtue of its potential toreduce misdiagnosis and to direct better targeted treatment[38]
As the cost of ABPM and hypertension managementdiffer greatly from country to country and is dependenton the method of healthcare delivery the cost-effectivenessof ABPM may need to be evaluated at a national level Forexample in Japan it has been estimated that the introduc-tion of ABPM for the management of hypertension hasreduced medical costs by about 948 trillion yen over 10years [40] (see Section 82)
34 Limitations of ambulatory blood pressuremonitoringThe technique of ABPM has many advantages over otheravailable techniques but it has its limitations whichinclude availability the provision of intermittent measure-ments during which the patient is sedentary rather thanlsquoambulatoryrsquo the possibility of inaccurate readings duringactivity and the inability to detect artefactual measure-ments the technique makes demands on the patient timeis needed to fit the device and it may cause discomfortparticularly during the night resulting in resistance fromsome patients to having repeat ABPM [11014] limitedreproducibility when the procedure is not standardized[41] and cost implications although the cost of devicesis reducing and costndashbenefit analyses have shown thatshort-term costs are justified by long-term savings (seeSection 33 Box 3)
Copyright copy Lippincott Williams amp Wilkins Unauth
Box 3 Limitations of ambulatory blood pressure monitoring
Application Limited availability May cause discomfort particularly at night Reluctance to use by some patients especially for repeat
measurement Cost implications (although the cost of devices is reducing
and possibly more cost-effective than office measurements)Function Imperfect reproducibility Provision of intermittent measurements in sedentary rather than
ambulatory conditions Possibility of inaccurate readings during activity Inability to detect genuine artefactual measurements
Journal of Hypertension
4 DEVICES AND SOFTWARE
41 Choosing an ambulatory blood pressuremonitoring device
411 Selecting an accurate deviceAn accurate device is fundamental to all BP measurementsif the device used to measure BP is inaccurate attention tomethodological detail is of little relevance It is acknow-ledged that the accuracy of BP-measuring devices shouldnot be based solely on claims from manufacturers whichcan at times be somewhat misleading Instead independ-ent validation using an established protocol with the resultspublished in peer-reviewed journals should be demanded[4222w] However manufacturers often ignore this recom-mendation and potential purchasers are generally unawareof this requirement assuming ndash not unreasonably ndash that ifa product reaches the market place it will measure BPaccurately The most popular validation protocol is theEuropean Society of Hypertension International Protocol(ESH-IP) and a recent review showed that from thepublication of the first version of the ESH-IP in 2002until June 2010 48 studies of device accuracy have beenreported using the British Hypertension Society (BHS)protocol 38 using the AAMI standard and 104 using theESH-IP 2010 [23w] Thus it seems that the ESH-IPsucceeded in expanding by three-fold to four-fold theuse of validation procedures worldwide compared withthe period before its publication [23w] A criticism bymembers of the AAMI Committee that the reduction inthe number of patients might compromise the validity ofthe protocol [24w] has been shown to be statisticallyunfounded [25w] The availability of the ESH-IP in anon-line version will further facilitate the validation of ABPMdevices [26w]
Since the ESH-IP was first published there has been animprovement in the performance of the oscillometric devi-ces for BP measurement [23w] but protocol violations andmisreporting have been particularly common suggestingthat there is a need for stricter standardization for conduct-ing and reporting a validation study [27w] The revisedversion of the ESH-IP protocol applied tighter validationcriteria for the pass level [42] and the application of thesemore stringent criteria is expected to double the validationfailure rate allowing more accurate devices to enter themarket [23w]
The AAMI protocol requires additional testing for ABPMdevices in 85 patients in the supine seated and standingpositions and stipulates that three devices should beassessed in ambulatory conditions all of which would bevery difficult and costly to perform [4328w] The BHSprotocol which is rarely used now also requires an in-use (field) assessment of ambulatory monitors [44] TheInternational Organization for Standardization (ISO) pro-tocol also requires additional clinical validation in 35patients in standardized conditions of physical activity(after exercise on a bicycle ergometer or treadmill toincrease heart rate by 10ndash20) [45]
It has recently been suggested that the validation ofautomated BP-measuring devices should be complementedby an overall quality check The PANET International
orized reproduction of this article is prohibitedwwwjhypertensioncom 1735
OrsquoBrien et al
Quality Certification Protocol denotes additional criteria ofquality for BP-measuring devices that fulfilled basic vali-dation criteria published in full in peer-reviewed medicaljournals On the basis of this evaluation a quality certifi-cation is released to the manufacturer and published onwwwpressionearteriosanet and wwwdableducationalorg[46]
The majority of devices for ABPM use oscillometry tomeasure BP but some devices also measure BP by micro-phonic detection of the Korotkoff sounds and such devicesneed to have both measurement methods validated accord-ing to accepted validation protocols [29w]
412 Validation requirements for ambulatoryblood pressure monitoring devices in specialpopulationsSeparate validation is required in specific populations suchas children and adolescents pregnant women and theelderly and in certain diseases such as obesity and arrhyth-mias [30w] Patients with arrhythmias children the elderlyand pregnant women present special challenges for vali-dation of oscillometric ABPM devices However althoughABPM devices are used frequently in these patient popu-lations specific validation studies have often not beenperformed this limitation applies also to other methodsof BP measurement such as home and office measure-ments The validation status of ABPM devices in differentpopulations can be checked on dedicated websites (egwwwpressionearteriosanet or wwwdableducationalorg)Although specific validation studies of ABPM devices inthese special populations are desirable in the future devi-ces that have been validated in the general hypertensivepopulation can be used so that high-risk patients are notdenied the benefit of ABPM
ChildrenFour ABPM devices have been validated in children andadolescents [31wndash34w] A number of factors that includeconsent adherence to the validation protocol whichphase to choose for defining DBP size of cuff and leveland range of BP make validation studies in children muchmore difficult than in adults [4735w]
PregnancyA number of ABPM devices have been validated innormotensive and hypertensive women in pregnancyand preeclampsia and although more devices are beingrecommended for use in clinical practice there are severaldevices that are not accurate in pregnancy [484936wndash41w] In pregnancy auscultation of DBP has been contro-versial leading to differences of opinion between mufflingand disappearance of sounds as the criterion for DBP [49]There is now general agreement that disappearance ofsounds is the best measure of DBP [50]
The elderlyValidation data in elderly patients are available only for theSpaceLabs 90207 [42w] It is important to define clearly theage group in which the device is being assessed Individualsover the age of 65 years will also have a higher prevalenceof diseases and conditions that can affect arterial stiffness
Copyright copy Lippincott Williams amp Wilkins Unaut1736 wwwjhypertensioncom
and therefore influence the outcome of validation studiesThe elderly have an increased prevalence of arrhythmiasincluding atrial fibrillation bradycardia and ventriculartachyarrhythmias and are more likely to have inter-armdifferences in pressures due to upper arm arterial diseasewhich would make them unsuitable for validation studies[51]
Patients with arrhythmiasThere are no formal validation studies using establishedprotocols for ABPM devices in this special population Inpatients with arrhythmias it is difficult to standardize theheart rates during validation Good recordings can beobtained with ABPM in most patients although there is atendency for electronic devices to overestimate DBP inpatients with atrial fibrillation [52]
Obese patientsNo validation studies of ABPM monitors have been per-formed in the obese population Obesity has an adverseimpact on vascular stiffness influencing thereby theaccuracy of the oscillometric technique and these patientshave large arms which may complicate recruitment forvalidation studies particularly when a specified range ofcuffs has to be assessed [53]
Patients with renal diseaseOnly one ABPM device has been validated for patients withrenal disease [43w] Validating devices in patients with end-stage renal disease (ESRD) and chronic kidney disease(CKD) presents a number of problems [43w44w] thatinclude finding an available upper extremity the effectof arterial stiffness on the oscillometric methodologyespecially for DBP [54] and the demanding schedule ofdialysis that makes recruitment of patients difficult
413 Additional features for ambulatory bloodpressure monitorsAll ABPM monitors measure BP and pulse rate and mostprovide measurements not only for SBP and DBP but alsofor mean BP and pulse pressure Over the past decadeABPM devices have been developed to measure or calcu-late intermittently or continuously other parameters suchas the ECG pulse wave velocity and central BP Further-more accessories such as position sensors and accelerom-eters for physical activity analysis have been incorporatedto provide a more precise pathophysiological profileMajor limitations of these innovative devices are theirrelatively high price and the need to validate the associatedfunctions according to adequate protocols and to provideevidence for their clinical usefulness Until these require-ments are fulfilled the use of such ABPM devices shouldbe restricted to research laboratories and specializedcenters
Ambulatory blood pressure monitoring and homeblood pressureDevices which can be used either for 24-h ABPM or in a7-day mode to collect multiday BP data are being devel-oped and one has been validated [45w46w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Ambulatory blood pressure monitoring and ECGDevices have been developed allowing 24-h ABPM withcontinuous 24-h ECG in a single procedure Besides theusual well established indications for each of these pro-cedures the interaction between these two signals providescomplementary interrelated information in one procedureThe use of the real heart rate to determine the deflation ratecan provide more precise BP measurement and additionalextra BP measurements can be triggered by abnormal ECGactivities such as arrhythmias and ST segment abnormal-ities Limitations are the relatively high cost of monitors andsoftware the complexity compared to the simple ABPMprocedure and the difficulties in performing validationstudies for the combined functions [47w48w] Thesedisadvantages are offset to some extent by being ableto perform the two procedures simultaneously in olderpatients in whom arterial hypertension and paroxysmalatrial fibrillation often coexist Another development hasbeen the use of spectral analysis of heart rate to provide ameans for improving screening for obstructive sleep apnea(OSA) [49w50w]
Ambulatory blood pressure monitoring and arterialfunctionDevices are being developed that measure arterial stiffnessso as to provide interesting information on 24-h ABPM andon arterial function [51wndash55w]
Ambulatory blood pressure monitoring and positionsensingPosition sensors have been developed to determinewhether the patient is standing or lying during ABPMrecording and this facility allows an estimation of the sleepperiod [5556w]
Ambulatory blood pressure monitoring and activitysensingActivity sensors and accelerometers have been developedfor monitoring patient activity during ABPM so as to providean indirect measure of activity and rest with the formerbeing an estimate of the awake period and the latter ofsleep Some of these sensors are incorporated in the devicewhereas others are complementary accessories placedeither at wrist thigh or chest level [57w]
Ambulatory blood pressure monitoring and centralblood pressureSeveral 24-h oscillometric ABPM monitors use specificalgorithms and software for pulse wave analysis by record-ing 24-h ABPM data as well as calculating central BP [5651wndash53w58wndash61w] Further studies are needed howeverto demonstrate the validity and clinical usefulness of thesedevices which at present should not be used for makingclinical decisions
42 Software for ambulatory blood pressuremonitoring data analysisRecommendations on procedures for ABPM use tend toconcentrate on the accuracy of the devicersquos hardware withlittle attention being paid to software presentation and
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
analysis of ABPM data As a consequence the practisingphysician who has to interpret the considerable amount ofdata provided by ABPM is often faced with a bewilderingreport with reams of paper containing plots histogramsand data analysis that have little relevance for clinicalpractice It is important for ABPM software programs tobe suitable for the intended use of the device For examplein a busy general practice perhaps only basic data givingaverage 24-h daytime and night-time values and a visualplot are all that will be required whereas for researchpurposes statistical detail on the windows of the 24-hprofile and other indices may be required [10] A recentstudy has stressed that whereas monitors for ABPM aresubject to extensive validation protocols there is no inter-national guideline on the software processing of the col-lected raw data to prevent error being introduced by thesoftware permutations An example of software-inducederror was demonstrated for the SpaceLabs Report Manage-ment System 92506 which showed errors in 92 of reportsamounting to a numerical difference between printout andon-screen hourly averages ranging from 37 to 18mmHgfor SBP and from 16 to 10mmHg for DBP [62w] Anadditional problem can arise from the calculation of 24-haverage BP values that are not weighted for the differentnumber of hourly measurements during daytime and night-time weighted hourly BP values have been shown to bemore reliable than calculations based on the average of allindividual readings [57]
The use of ABPM in clinical practice can be facilitated bystandardizing the graphic presentation of ABPM datamuch as is the case for ECG recordings so that the pres-entation of data is independent of the type of ABPMmonitor used and the user is not required to becomefamiliar with a variety of programs Standardization alsofacilitates the interchange of ABPM recordings betweendatabases such as a hospital and primary care practiceMoreover if ABPM software programs provide a printedreport of the standardized ABPM data with a validatedinterpretative report [58] (signed by the physician in chargeof the service whenever legally required) doctors andnurses unfamiliar with the technique are assisted inlearning the variety of patterns generated by ABPM andbecause an individualized physician report is not a require-ment in most cases the cost of ABPM is reduced [110](Box 4)
421 Software requirementsThe following facilities are recommended for ABPM soft-ware in clinical practice [1910]
Clinical reportThe following information should be available in a one-page report
or
1
ize
Standardized plot format with each BP measurementon the vertical axis and time of day on horizontal axiswith different windows of the 24-h period identifiedand normal bands clearly demarcated The sleep timeinterval used to calculate asleep BP should be indi-cated (shaded) and preferably based on the indivi-dualsrsquo sleep time report (diary cards) In the plot the
d reproduction of this article is prohibitedwwwjhypertensioncom 1737
Cop
Box 4 Software requirements
Clinical report Ambulatory blood pressure measurement analysis and report should be standardized independent of the monitor type Standardized plot of all the blood pressure measurements with daytime and night-time windows and normal blood pressure bands demarcated Average SBP DBP and heart rate to be displayed Nocturnal blood pressure decline () for SBP and DBP Summary statistics for time-weighted average SBP and DBP and heart rate for the 24-h period daytime and night-time with standard deviations and number
of valid blood pressure readings Facility for showing error readings if requiredOptional requirements Automated software generated interpretative report indicating the normal or abnormal patterns and whether the requirements for a valid recording are
fulfilled Facility to plot heart rate and mean blood pressure Trend report for comparing repeated ambulatory blood pressure measurement recordings Ability to centrally host dataResearch report Data storage and raw data export capability for research analysis and audit Parameters include variability measures (such as 24-h SD 24-h weighted SD average real variability coefficient of variation) area under the curve
calculations blood pressure load parameters ratendashpressure product trough and peak levels smoothness index (the last two parameters requiring ABPMdata before and during treatment to be available) cusum-derived statistics and ambulatory arterial stiffness index
OrsquoBrien et al
1738
upper value of the Y-axis should not be fixed butadjustable to the highest BP value recorded in orderto maximize the graphic presentation of BP variationsover the 24-h period A plot of SBP and DBP through-out the 24-h period with a facility for plotting heartrate and mean BP so as to provide evidence ofcircadian behavior should be provided
2
Summary statistics for time-weighted SBP and DBPand heart rate in the windows of the 24-h period andseparately for the awake and asleep subperiods withthe respective standard deviations and the number ofvalid BP readings included in the analysis and afacility for indicating the time of going to bed andawakening
3
Medication details
4
Facility for showing error readings if required
Interpretative reportTo remove the variance associated with the ABPMinterpretation by human observers and to simplify theevaluation of results in routine clinical practice for thoseunfamiliar with the technique there should be an auto-mated software-generated interpretative report indicatingnormal or abnormal BP patterns and whether there aresufficient measurements for the recording to be valid [10]The interpretative report should be validated by testing thecomputer-generated report against reports from experts[5859]
Trend reportThe provision of a trend report allows ABPMs to be com-pared over time to demonstrate the response to changes inmanagement If ABPM is to be used to achieve better BPcontrol it is important for prescribing doctors (and patients)to be able to see whether medication is achieving controlthroughout the entire 24-h period
Research reportThe system should be capable of storing data for detailedanalysis for research and audit according to evidence-based
yright copy Lippincott Williams amp Wilkins Unautwwwjhypertensioncom
definitions for time-weighted arithmetic and mean valuesfor measures of BP level In view of evidence that short-term BP variability may give information over and abovemean BP levels and that reduction in 24-h BP variabilitymay be beneficial [63w] time-weighted and other measuresof short-term BP variability are helpful for on-goingresearch in this area Informative indices associated withoutcome such as area under the curve calculations BP loadparameters trough and peak levels the smoothness index(the last two parameters requiring ABPM data before andduring treatment to be available) cusum-derived statisticsand most recently the ambulatory arterial stiffness index(AASI) should also be provided [6061] The system shouldbe capable of storing and exporting raw data for researchpurposes and additional analyses [606163w]
422 Indices derived from ambulatory bloodpressure monitoring recordingsAverage BP values (over 24 h daytime and night-time) areundoubtedly the most important parameters obtained fromABPM recordings based on outcome data However alarge number of additional indices with promising clinicalevidence may be derived from ABPM recordings and someof them are occasionally included in the reports generatedby ABPM systems
Blood pressure loadThis index is defined as the percentage of readings in agiven period (24-h day or night) which exceed a prede-fined threshold value typically set at the proposed nor-malcy level for average BP values of that period The aim ofBP load is to quantify the number of readings with elevatedBP and mathematically it depends on both average BPlevels and distribution of BP readings [62] Although intheory clinically appealing and thus commonly incorpor-ated in the ABPM software this index has a number oflimitations Firstly there is no evidence that the thresholdsdefined for average BP values have any prognostic meaningwhen applied to single BP measurements Secondly whencomparing recordings with similar average BP levels differ-ences in BP load can be largely explained by differences in
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
BP variability making this index largely redundant ThirdlyBP load does not contain the prognostically importantinformation on how much the threshold level has beenexceeded To overcome the latter limitation it has beenproposed to modify the classic BP load definition bycalculating the total area under the timendashpressure curvewhen BP exceeds the threshold [63] Finally although somestudies support the usefulness of BP load in predictingorgan damage [6464w] it has never been convincinglydemonstrated that it provides any additional and clinicallyrelevant information independently of what is obtained byfocusing on average BP values The use of BP load inchildren has also been examined but it has not been foundhelpful in diagnosis [65w]
Ratendashpressure productThis index which is defined as heart rate multiplied by SBPis used as an index of myocardial work during exercise andit has prognostic relevance [66w] The availability of bothheart rate and BP data in ABPM makes it possible to obtainthe index readily especially if ABPM is accompanied byactigraphy [65] Although potentially promising the clinicalapplication of this index requires further research
rsquoVascularrsquo indicesSeveral ABPM-based indices have been proposed to pro-vide information on vascular wall properties Their ration-ale is based on the observation that the stiffness of thearterial wall increases when it is being stretched in patientswith impaired arterial wall elasticity SBP increases moresteeply than DBP whereas in a patient with elastic arteriesSBP and DBP increase in parallel The AASI which iscalculated as 1 ndash slope of regression of DBP on SBP isreadily obtainable from ABPM [6066]
AASI appears to have a direct relationship to carotidndashfemoral pulse wave velocity (a validated index of largearteriesrsquo stiffness) and an independent relationship withcardiovascular outcomes [606167wndash70w] Howeverthe ability of AASI to reflect arterial stiffness has beenchallenged because of its dependence on nocturnal BP falland the fact that it implies the use of asymmetric regressionpossibly affecting the precision of slope estimation[67ndash6971w72w] Modifications to AASI have been pro-posed but further data are awaited as to their ability tosurpass AASI in predicting outcome [73w74w]
The QndashKd interval which measures the time intervalbetween the onset of the QRS on the electrocardiogram (Q)and the last Korotkoff sound (K) corresponding to thediastolic pressure (d) has also been shown to have prog-nostic value [70]
Indices for indicating the pattern of treatment-induced changes in 24-h blood pressure loweringTwo principal indices are available for assessing thesmoothness and consistency of antihypertensive treatmenteffect over 24 h with ABPM The trough-to-peak ratio is theratio between BP reduction achieved by treatment at theend of dosing interval (trough which for drugs adminis-tered once daily means 24 h after the last dose intake) andpeak BP reduction usually achieved a few hours after dose
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
intake [7172] The trough-to-peak ratio is characterized by ahigh degree of variability in individual patients and istherefore not suitable for application to clinical practice[73] The smoothness index is calculated as the ratiobetween the average of hourly BP reductions over 24 hand the standard deviation (SD) of such an average valuethus integrating information on the size of BP reduction bytreatment and on its homogeneity throughout the 24-hperiod [7173] The smoothness index is highest for potentdrugs or drug combinations which also provide the mosthomogeneous BP reduction It is more reproducible thanthe troughpeak ratio [7173] and predicts treatment-induced changes in indices of organ damage includingleft ventricular mass and carotid arterial wall thickness[75w] A recent meta-analysis has provided informationon clinical determinants of the smoothness index suchas age ethnicity sex and smoking [74] The relevance ofthese indices in predicting the impact of treatment onoutcome and the reference values remain to be assessed
5 PROCEDURE
51 Training requirementsThe technique of ABPM is a specialized one and should beapproached with the care reserved for any such procedureAn understanding of the principles of traditional BPmeasurement cuff fitting monitor function and analysisand interpretation of ABPM data is required In practice anurse with an interest and experience in hypertension canmaster the use of ABPM devices after a relatively brieftraining However the interpretation of ABPM profilesrequires experience in the technique which is best pro-vided by the doctor in charge of an ABPM service [19]
52 Fitting an ambulatory blood pressuremonitorTime needs to be given to fitting the monitor and preparingthe patient for the monitoring period if good results are tobe obtained [19] The key to successful ABPM is educatingthe patient on the process of monitoring and the instruc-tions should be explained and printed on a diary card Inclinical practice measurements are preferably performedon a routine working day Although ABPM is best notperformed while patients are admitted to hospital becausehospitalization leads to underestimation of BP and over-diagnosis of nondippers [10] there are occasions such asthe evaluation of severely resistant hypertension andassessment of patients following a stroke when ABPM inhospital may be indicated
The frequency of measurement during the 24-h period isgenerally not more than every 15 min (which could inter-fere with normal activity) nor less than every 30min (whichcould give an inadequate number of measurements) Morefrequent measurements at night may disturb sleep andsleep disturbance has been shown to reduce the prognosticvalue of ABPM [75] To improve reproducibility repetitionof ABPM should be performed on like days for example onroutine working or recreational days A diary card can beused to record symptoms and events that may influenceABPM measurements
orized reproduction of this article is prohibitedwwwjhypertensioncom 1739
OrsquoBrien et al
53 Explanation to patientThe first step is adequate explanation of the procedure in anattempt to allay anxiety especially in nervous patientsPatients having ABPM for the first time should be told thatthere is minor discomfort caused by inflation of the cuff It isimportant to emphasize to the patient to follow hisherusual daily activities but as much as possible to remain stillwith the arm relaxed and not extended or contracted atheart level during each BP measurement [19] It can behelpful to have patients record periods of stress the time ofmeals the time of a siesta the time of going to bed andrising the quality of sleep and the time and type ofdrug ingestion
Box 5 Evaluation of ambulatory blood pressure monitoring data
Definition of daytime and night-time Daytime and night-time intervals are best defined using sleeping times
reported by individual usersrsquo diary cards (awake and asleep periods) Fixed narrow time intervals can be applied by discarding transition
periods between daytime and night-time (eg daytime defined as0900ndash2100 h and night-time 0100ndash0600 h)
Editing requirements Editing is not necessary for calculating average 24-h daytime and
night-time values The ambulatory blood pressure monitoring should be repeated if thefollowing criteria are not met
24-h recording with at least 70 of expected measurements20 valid awake (0900 to 2100 h)7 valid asleep (0100 to 0600 h)Blood pressure measurements at 30-min intervalsFor research purposes at least two valid daytime and one valid
night-time measurement per hour
54 Identification of daytime and night-timeperiods and editing ambulatory blood pressuremonitoring dataOne simple and popular method for identifying daytimeand night-time subperiods is to assess the time of awaken-ing and sleeping from diary card entries Another method isto use a fixed-narrow time interval approach in which forexample the retiring (2101 to 0059 h) and rising (0601 to0859 h) periods (which are subject to considerable vari-ation) are eliminated with the daytime period being from0900 to 2100 h and night-time from 0100 to 0600 h in thisway the variations in the time spent in bed that may existbetween the young and the old and in different culturesare to some extent eliminated from the analysis [176w]This method has the disadvantage of eliminating infor-mation on the white-coat window on the early phase ofnight sleep when dipping can be most evident and onthe early morning surge of BP which may be associatedwith cardiovascular events However these windows canbe analyzed separately for research or if considered import-ant in practice In countries where a daytime siesta ispopular a record of sleeping times both during day andnight is important and ABPM software should be able toadjust for this otherwise there may be underestimation ofthe nocturnal BP dip and overdiagnosis of nondippers[77w]
Many statistical techniques exist for editing ABPMrecords and no one method is ideal [176w] The detec-tion of artefactual readings and the handling of outliervalues (which may or may not be erroneous) have indeedbeen the subject of debate [76w] There are a number ofways of separately analyzing BPs recorded during the dayand night [7678w] Several automatic procedures havebeen proposed to reject outlying measurements based ona univariate multivariate or temporal approach Morecomplex procedures requiring the intervention of theobserver have been proposed but they are time consum-ing and not suitable for clinical practice [77] It has beenshown that rejection of outliers may alter the results ofABPM in individual patients sometimes significantlyaffecting average SBP levels [777879w] Editing pro-cedures can reduce mean systolic ABPM by 4 mmHg incomparison with unedited recordings thereby decreasingthe likelihood of diagnosing sustained hypertension Inone study the prevalence of sustained hypertension wasdecreased by 6ndash10 when several editing methods were
Copyright copy Lippincott Williams amp Wilkins Unaut1740 wwwjhypertensioncom
applied to raw 24-h data [79w] To make the results ofdifferent laboratories comparable common editingcriteria for ABPM should be used The problem is toestablish which of the methods proposed in the literatureprovides the most reliable data While awaiting moreobjective criteria to identify a universally acceptable edit-ing procedure we recommend that editing is not necess-ary for calculating average 24-h daytime and night-timevalues and that only physiologically impossible readingsshould be deleted from recordings However when thereare excessive artefacts in a tracing a repeat recordingrather than editing should be performed Some editingmight be required when focusing on analysis of BPvariability for the quantification of which the presenceof artefacts may introduce appreciable errors If editing isconsidered necessary a method proposed by Casadeiet al [80w] and modified by Winnicki et al [78] providescomparable performance to other proposed editing pro-cedures
There are no firm data on which to base recommen-dations for a satisfactory ABPM recording but the recom-mendation for having at least 70 of expectedmeasurements provides a basic working recommendationfor clinical practice This figure will be influenced by theperiod demarcated as daytime (awake) or night-time(asleep) periods and by the number of measurementsselected (usually 30-min but often 15 or 20-min intervals)In the previous ESH guideline on measurement it wasrecommended that there should be a minimum of 14measurements during the day and seven measurementsat night [1] Having considered what evidence is availableand the practical issues of performing repeat ABPM inpractice it seems reasonable to increase the minimum ofdaytime measurements to 20 while retaining a minimumseven measurements at night based on measurementsbeing performed every 30min and with fixed time periodsbeing used to define day (0900 to 2100 h) and night (0100 to0600 h) [1] (Box 5)
55 The arm for measurementABPM is best measured in the nondominant arm so as tointerfere as little as possible with daily activity unless there
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
has been documented evidence of a difference in BPbetween arms in which case the arm known to have thehigher BP values should be chosen [1] It is commonpractice for BP to be measured by a conventional techniqueat the same time as an ABPM monitor is being fitted and todetermine whether there is a discrepancy between thetechniques However BP variability is such that any suchcomparison has little validity and to determine a significantdifference it is necessary to perform simultaneousmeasurement according to a definitive protocol and thisis not feasible in practice [42] Because of these limitationsthe practice of performing a comparative measurement isnot recommended
56 Selecting the appropriate cuff and bladderThere is unequivocal evidence that either too narrow ortoo short a bladder (undercuffing) will cause overesti-mation of BP so-called lsquocuff hypertensionrsquo and there isgrowing evidence that too wide or too long a bladder(overcuffing) may cause underestimation of BP Under-cuffing has the effect in clinical practice of overdiagnos-ing hypertension and overcuffing leads to hypertensivepatients being diagnosed as normotensive Either even-tuality has serious implications for the epidemiology ofhypertension and for clinical practice [79] It is importanttherefore to select a cuff containing an inflatable bladderof correct length and width for the arm in which ABPM isto be measured All ABPM devices should provide cuffscontaining bladders for small medium and large-sizedarms as recommended in international guidelines[18081] However in many obese individuals the largebladder sizes cannot be used because the arm length istoo short to accommodate the bladder [81w] Anotherproblem is that the cylindrical shape of the commonlyused cuffs does not always wrap snugly around conical-shaped arms in obese and very muscular arms[8282w83w] Recently novel oscillometric homemonitors with cuff technology that allows a singlefixed-size cuff to be used on a wide range of arm circum-ferences have been developed [84wndash87w]
Another issue that needs consideration is the possibilitythat the discomfort caused by inflation of a large cuff inobese patients might cause elevation of BP This issuebecomes more important during ABPM because ofrepeated measurement especially during night-time sleepOscillometric devices for home use that measure BP duringcuff inflation may induce less discomfort because themeasurement is completed before maximal inflation[84w88w] However to date no study has specificallyaddressed this issue
Forearm BP measurement may have to be consideredwhen extreme obesity makes upper arm BP measurementimpossible BP measurements tend to be higher with fore-arm compared with upper arm measurement but meth-odological differences in these studies make it difficult toprovide recommendations for all populations [8389wndash94w] Despite the questionable accuracy of forearm BPmeasurement it may be the only acceptable option forABPM in individuals with very large upper arms providedthe patient is instructed to keep the forearm at heart levelduring measurement [94w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
No wrist devices have been validated for ABPM whereastechnology for continuous beat-to-beat monitoring ofambulatory BP in the finger has been developed usingthe volume-clamp method first described by Penaz [95w]A number of studies that compared this technology withintraarterial or noninvasive BP measurement showedunderestimation of BP particularly diastolic yet it remainsa practical alternative to intraarterial measurement for theevaluation of beat-to-beat BP changes and variability inresearch studies [8496wndash98w]
57 Conditions in which ambulatory bloodpressure monitoring may be difficult toperform
Obese patientsObesity is a well established major risk factor for hyperten-sion with higher prevalence in specific population groupssuch as patients with diabetes mellitus [99w] or OSA [100w]Despite the increasing prevalence of obesity worldwide[101w] and the close link between obesity and hyperten-sion scarce data are available on the application of ABPM inobese and extremely obese individuals ABPM is oftenrequired in these individuals and technical difficultiesshould not exclude them from such a valuable technology[79] The problem of miscuffing in obese pregnant womenmay result in diagnostic discrepancies [85]
Patients with atrial fibrillationBP measurement in patients with atrial fibrillation is lessprecise as this type of arrhythmia is accompanied byincreased beat-to-beat BP variability due to variations inventricular filling time stroke volume and contractilityInternational guidelines [181] recognize the relatively poorprecision of a single BP measurement and recommendrepeated readings in order to improve the accuracy ofestimates Theoretically ABPM should fulfill this stipulationas it provides a relatively high number of readings in a shortperiod of time Unfortunately published evidence regard-ing the role of ABPM in patients with arrhythmias andspecifically in patients with atrial fibrillation is scarce
Patients with atrial fibrillation have been usuallyexcluded from trials using ABPM as well as from validationprotocols of ABPM devices Four studies have addressedthe possible value of ABPM in patients with atrial fibrillation[48w102wndash104w] The evidence from these studiessuggests that ABPM may be useful in these patients pro-vided its limitations are taken into account The proportionof readings with errors the variability of BP and therepeatability coefficients do not appear to be different fromthose in patients in sinus rhythm DBP measured using anABPM monitor in patients with atrial fibrillation appears tobe relatively higher than that obtained with the traditionaloffice measurement or by the same ABPM procedure whenthe patient achieves sinus rhythm This finding is supportedby a review and meta-analysis of studies that validatedelectronic devices in patients with sustained atrial fibrilla-tion which showed consistent overestimation of DBP [52]In spite of this and although larger trials in patients on atrialfibrillation are recommended there is no reason to exclude
orized reproduction of this article is prohibitedwwwjhypertensioncom 1741
OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Box 1 Advantages of ambulatory blood pressure monitoring over clinicblood pressure
Gives a larger number of readings than office blood pressuremeasurement
Provides a profile of blood pressure behavior in the patientrsquosusual daily environment
Allows identification of white-coat and masked hypertensionphenomena
Demonstrates nocturnal hypertension Assesses blood pressure variability over the 24-h period Assesses the 24-h efficacy of antihypertensive medication Is a stronger predictor of cardiovascular morbidity and mortality
than office measurement
Guideline
dependent on observer attention to detail which is oftenlacking and it provides only a momentary measurement ofBP usually under circumstances that can influence the levelof BP being measured To overcome these serious meth-odological problems techniques for obtaining automatedprofiles of BP over 24 h and measures of BP in the homesetting have been developed
ABPM has been available in one form or another forsome 50 years having been developed initially to study thecircadian changes in BP and to determine the influence ofBP-lowering drugs on the 24-h profile The first major breakwith traditional BP measurement was the introduction of adirect intraarterial technique for the measurement of BPover the 24-h period The data on antihypertensive drugefficacy provided by studies using this system were particu-larly valuable because they provided continuous BPmeasurement throughout the day and night but use ofthe technique was limited by safety and ethical consider-ations Efforts were focused therefore on developing adevice that would record ambulatory BP noninvasively andin the 1960s the Remler device which was capable ofmeasuring BP intermittently during the daytime periodprovided clinicians with a new technique for assessingBP This device was limited by having to be operated bythe patient which made measurement of BP impossibleduring sleep The next technological advance was theintroduction of fully automated devices that could measureBP intermittently at predetermined intervals over the 24-hperiod This class of devices provided a methodology thatwas applicable not only for research but also for use inroutine clinical practice [7ndash101w]
3 GENERAL CONSIDERATIONS
31 Why is ambulatory blood pressuremonitoring superior to conventional bloodpressure measurementTraditionally office BP measurement has been performedusing a sphygmomanometer and stethoscope Recentlyautomated office BP measurement has been proposed asan alternative to traditional measurement Automated officeBP is the mean of multiple BP readings recorded with a fullyautomated device with the patient resting quietly alone inthe officeclinic [11] It has several advantages over manualBP especially in routine clinical practice by virtually elim-inating office-induced increases in BP improving accuracyminimizing observer error and providing a more stand-ardized measurement technique using an automated oscil-lometric sphygmomanometer [2w] The mean automatedoffice BP for diagnosing hypertension is similar to the meanawake ambulatory BP and home BP (13585 mmHg)Preliminary data suggest that automated office BP is a betterpredictor of target organ damage [3w4w] especially com-pared with routine manual office BP which correlatespoorly with intermediate end-points such as left ventricularmass [5w] Longitudinal clinical outcome studies with auto-mated office BP have not yet been reported
BP recorded in the patientrsquos home is a significantly betterpredictor of future cardiovascular risk than is office BPStandard protocols have been developed for recordinghome BP [2] and include the mean of duplicate readings
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
taken twice daily for 7 consecutive days with readings fromthe first day excluded The cut-point for hypertension usinghome BP is the same as for the awake ambulatory BP(13585 mmHg) In order to avoid reporting bias [12] ahome BP recorder with a memory for storing readingsshould be used and the patient should take the device tothe physicianrsquos office to have the mean home BP verifieddirectly from the devicersquos display More recently remotetransmissions of home BP readings [13] is becoming avail-able allowing BP readings recorded in the home to beautomatically sent to a data collection center via a tele-phone modem or internet link and from there forwarded tothe physicianrsquos office
The advantages of ABPM which have been stated incomprehensive reviews [11014] have influenced recom-mendations for the technique to be used much more widelyin clinical practice [15ndash186w7w] These advantages maybe briefly summarized as follows (Box 1) first and fore-most ABPM simply gives many more measurements thanconventional BP measurement and usual BP is reflectedmore accurately by repeated measurements ABPM pro-vides a profile of BP away from the medical environmentthereby allowing identification of individuals with a white-coat response or masked hypertension ABPM can demon-strate a number of patterns of BP behavior over 24 h thatmay be relevant to clinical practice such as nocturnalhypertension or increased BP variability by showing BPbehavior in different windows of a 24-h period such as thewhite-coat and nocturnal periods as well as the BP fluctu-ations triggered by environmental stimuli it is possible toassess the efficacy of antihypertensive medication through-out the day and night rather than relying on a casual BPABPM is a stronger predictor of cardiovascular morbidityand mortality than conventional measurement and evi-dence is growing that nocturnal BP measured by ABPMis an important predictor of cardiovascular outcome fromwhich it follows that the measurement of night-time BPshould be an important part of clinical practice and ABPMprovides a means for not only improving the diagnosis andmanagement of hypertension but also for ensuring thateffective control of hypertension is achieved throughoutthe entire 24-h period (Box 1)
32 Ambulatory blood pressure monitoringthresholds for clinical practiceAs with conventional BP measurement the levels of BP thatconstitute normality for ABPM have been a subject of much
orized reproduction of this article is prohibitedwwwjhypertensioncom 1733
OrsquoBrien et al
debate over the years [19ndash241w8wndash19w] The issue ismore complex than for conventional measurement becausenormality needs to be defined for both daytime and night-time pressures and outcome data are scarce
In defining normality for ABPM it is necessary to move onfrom diagnostic thresholds determined in a statistical way innormotensive andor hypertensive reference populations tooutcome-driven thresholds The International Database ofAmbulatory blood pressure in relation to CardiovascularOutcome (IDACO) based on 5682 participants followedfor 97 years determined ABPM thresholds which yielded10-year cardiovascular risk (for cardiovascular cardiac andstroke outcomes) corresponding to high BP on officemeasurement (gt14090mmHg) Corresponding thresholdsfor hypertension with ABPM were 1310794 for 24h 1382864 for daytime and 1195708mmHg for night-time [25]
Whereas outcome-driven thresholds are currently avail-able for adults the question remains to be resolved whetherthey are applicable across the whole age range and in allconditions or whether separate recommendations arenecessary for older and very old individuals and for preg-nant women In the case of children and adolescents adifferent approach is needed and therefore thresholdsbased on population distribution have been proposed(See Section 67)
Head et al [26] examined a different approach to deriveage-related and sex-related ABPM equivalents to clinic BPthresholds for diagnosis and treatment of hypertension byaccounting for age and sex They also compared clinicmeasurements taken by nonmedically qualified health pro-fessionals with those taken by doctors to assess whether alsquowhite-coatrsquo effect might have influenced the findings ofprevious studies that were based solely on doctorrsquosmeasurements This analysis provided a range of daytimeABPM measurements equivalent to recognized clinic BPthresholds which when predicted from clinic BP valueswere close to those derived from other outcome analyses
The threshold values in the recent NICE guidelines [4]the JNC 7 guideline [27] and the ESHESC guidelines for2003 2007 and 2013 [12829] and the results of outcomestudies such as IDACO [25] and Ohasama [30] have con-tributed to the definition of consensus values summarizedin Box 2 It is recognized that the levels in Box 2 might beregarded as conservative by some and it is acknowledgedthat further studies are needed to define thresholds moreprecisely particularly in high-risk patients
33 Cost-effectiveness of ambulatory bloodpressure monitoringThe cost-effectiveness of ABPM has been considered from anumber of perspectives First ABPM may enable financialsavings in drug prescribing ABPM is superior to othermeasurement techniques in demonstrating the efficacy of
Box 2 Thresholds for hypertension diagnosis based on ambulatory bloodpressure monitoring
24-h average 13080 mmHg
Awake (daytime) average 13585 mmHg
Asleep (night-time) average 12070 mmHg
Copyright copy Lippincott Williams amp Wilkins Unaut1734 wwwjhypertensioncom
antihypertensive drugs in pharmacological trials [3132]Adjustment of antihypertensive therapy according to ABPMrather than office BP has been shown to result in lessantihypertensive medication being prescribed withoutcompromising target organ involvement [33] It has alsobeen shown that in patients on treatment with BP-loweringdrugs ABPM was a better predictor of cardiovascular out-come than office BP [34] Reduction in office BP due toamelioration of the white-coat effect especially in elderlypatients who have greater BP variability may be attributedwrongly to a BP-lowering effect of antihypertensive medi-cation if ABPM is not used to assess treatment efficacy[35]
Second by identifying patients with white-coat hyper-tension ABPM may improve drug prescribing in a cost-effective manner [36] The cost of care for hypertension isdominated by the long-term occurrence of cardiovascularcomplications and the costs for drug treatment rather thanby the short-term cost for visits and investigations [3720w]
Third ABPM can identify individuals with normal BP inthe office but elevated BP levels in daily life (rsquomaskedhypertensionrsquo) a condition that has been shown to carrythe same adverse prognosis as sustained arterial hyperten-sion both in the clinic and in daily life (see Section 63)
Until recently ABPM is generally cited as being moreexpensive than other measurement techniques though ithas been shown to be cost-effective both in specialistservices and in primary care [3621w] This has been attrib-uted to the fact that only tangible benefits have beenconsidered such as identifying patients with white-coathypertension and the savings that might be made from themore efficient prescribing of BP-lowering drugs Howevercost-effectiveness considerations must be extended toinclude the financial potential of the technique not onlyto improve the diagnosis and management of hypertensionbut also as a means of ensuring that effective control ofhypertension is implemented at community level [9] ABPMis the most effective technique for identifying white-coathypertension which may be present in as many as 20 ofpeople who appear to have hypertension with office BPand these patients may be spared years of unnecessary andexpensive drug treatment which is often not free from side-effects They may also avoid being penalized unnecessarilyfor insurance or employment by having the diagnosis oflsquohypertensionrsquo misapplied [9]
A number of studies have analyzed the costndashbenefitaspects of ABPM Krakoff [36] has shown that potentialsavings of 3ndash14 for cost of care for hypertension and 10ndash23 reduction in treatment days when ABPM was incorp-orated into the diagnostic process On an annual basis thecost of ABPM would be less than 10 of treatment costsOther costndashbenefit analyses have shown that ABPM is mostcost-effective for the diagnosis and management of newlydiagnosed hypertension [921w]
Recently NICE undertook detailed costndashbenefit analysisfor ABPM and showed that the use of ABPM is the most cost-effective method of confirming a diagnosis of hypertensionin a population suspected of having high BP based on aconventional BP screening measurement of more than 14090mmHg and that the technique would result in substantialsavings to the UK National Health Service [438] However
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
the validity of the underlying assumptions by NICE has notbeen universally accepted [39]
Other potential benefits of ABPM that have not beenconsidered by NICE are the savings to be made in havingdrug treatment targeted to achieve 24-h BP control and thesubstantial savings to be made by the prevention of strokeand other cardiovascular consequences of hypertensionwith improved BP control Nor has NICE considered thepotential benefits of identifying the white-coat and maskedhypertension phenomena in treated individuals or of treat-ing nocturnal hypertension which is a major predictorof outcome
In a further extensive study of the cost of ABPM aMarkov model-based probabilistic cost-effectivenessanalysis concluded that ABPM is the most cost-effectivestrategy for the diagnosis of hypertension for men andwomen of all ages mainly by virtue of its potential toreduce misdiagnosis and to direct better targeted treatment[38]
As the cost of ABPM and hypertension managementdiffer greatly from country to country and is dependenton the method of healthcare delivery the cost-effectivenessof ABPM may need to be evaluated at a national level Forexample in Japan it has been estimated that the introduc-tion of ABPM for the management of hypertension hasreduced medical costs by about 948 trillion yen over 10years [40] (see Section 82)
34 Limitations of ambulatory blood pressuremonitoringThe technique of ABPM has many advantages over otheravailable techniques but it has its limitations whichinclude availability the provision of intermittent measure-ments during which the patient is sedentary rather thanlsquoambulatoryrsquo the possibility of inaccurate readings duringactivity and the inability to detect artefactual measure-ments the technique makes demands on the patient timeis needed to fit the device and it may cause discomfortparticularly during the night resulting in resistance fromsome patients to having repeat ABPM [11014] limitedreproducibility when the procedure is not standardized[41] and cost implications although the cost of devicesis reducing and costndashbenefit analyses have shown thatshort-term costs are justified by long-term savings (seeSection 33 Box 3)
Copyright copy Lippincott Williams amp Wilkins Unauth
Box 3 Limitations of ambulatory blood pressure monitoring
Application Limited availability May cause discomfort particularly at night Reluctance to use by some patients especially for repeat
measurement Cost implications (although the cost of devices is reducing
and possibly more cost-effective than office measurements)Function Imperfect reproducibility Provision of intermittent measurements in sedentary rather than
ambulatory conditions Possibility of inaccurate readings during activity Inability to detect genuine artefactual measurements
Journal of Hypertension
4 DEVICES AND SOFTWARE
41 Choosing an ambulatory blood pressuremonitoring device
411 Selecting an accurate deviceAn accurate device is fundamental to all BP measurementsif the device used to measure BP is inaccurate attention tomethodological detail is of little relevance It is acknow-ledged that the accuracy of BP-measuring devices shouldnot be based solely on claims from manufacturers whichcan at times be somewhat misleading Instead independ-ent validation using an established protocol with the resultspublished in peer-reviewed journals should be demanded[4222w] However manufacturers often ignore this recom-mendation and potential purchasers are generally unawareof this requirement assuming ndash not unreasonably ndash that ifa product reaches the market place it will measure BPaccurately The most popular validation protocol is theEuropean Society of Hypertension International Protocol(ESH-IP) and a recent review showed that from thepublication of the first version of the ESH-IP in 2002until June 2010 48 studies of device accuracy have beenreported using the British Hypertension Society (BHS)protocol 38 using the AAMI standard and 104 using theESH-IP 2010 [23w] Thus it seems that the ESH-IPsucceeded in expanding by three-fold to four-fold theuse of validation procedures worldwide compared withthe period before its publication [23w] A criticism bymembers of the AAMI Committee that the reduction inthe number of patients might compromise the validity ofthe protocol [24w] has been shown to be statisticallyunfounded [25w] The availability of the ESH-IP in anon-line version will further facilitate the validation of ABPMdevices [26w]
Since the ESH-IP was first published there has been animprovement in the performance of the oscillometric devi-ces for BP measurement [23w] but protocol violations andmisreporting have been particularly common suggestingthat there is a need for stricter standardization for conduct-ing and reporting a validation study [27w] The revisedversion of the ESH-IP protocol applied tighter validationcriteria for the pass level [42] and the application of thesemore stringent criteria is expected to double the validationfailure rate allowing more accurate devices to enter themarket [23w]
The AAMI protocol requires additional testing for ABPMdevices in 85 patients in the supine seated and standingpositions and stipulates that three devices should beassessed in ambulatory conditions all of which would bevery difficult and costly to perform [4328w] The BHSprotocol which is rarely used now also requires an in-use (field) assessment of ambulatory monitors [44] TheInternational Organization for Standardization (ISO) pro-tocol also requires additional clinical validation in 35patients in standardized conditions of physical activity(after exercise on a bicycle ergometer or treadmill toincrease heart rate by 10ndash20) [45]
It has recently been suggested that the validation ofautomated BP-measuring devices should be complementedby an overall quality check The PANET International
orized reproduction of this article is prohibitedwwwjhypertensioncom 1735
OrsquoBrien et al
Quality Certification Protocol denotes additional criteria ofquality for BP-measuring devices that fulfilled basic vali-dation criteria published in full in peer-reviewed medicaljournals On the basis of this evaluation a quality certifi-cation is released to the manufacturer and published onwwwpressionearteriosanet and wwwdableducationalorg[46]
The majority of devices for ABPM use oscillometry tomeasure BP but some devices also measure BP by micro-phonic detection of the Korotkoff sounds and such devicesneed to have both measurement methods validated accord-ing to accepted validation protocols [29w]
412 Validation requirements for ambulatoryblood pressure monitoring devices in specialpopulationsSeparate validation is required in specific populations suchas children and adolescents pregnant women and theelderly and in certain diseases such as obesity and arrhyth-mias [30w] Patients with arrhythmias children the elderlyand pregnant women present special challenges for vali-dation of oscillometric ABPM devices However althoughABPM devices are used frequently in these patient popu-lations specific validation studies have often not beenperformed this limitation applies also to other methodsof BP measurement such as home and office measure-ments The validation status of ABPM devices in differentpopulations can be checked on dedicated websites (egwwwpressionearteriosanet or wwwdableducationalorg)Although specific validation studies of ABPM devices inthese special populations are desirable in the future devi-ces that have been validated in the general hypertensivepopulation can be used so that high-risk patients are notdenied the benefit of ABPM
ChildrenFour ABPM devices have been validated in children andadolescents [31wndash34w] A number of factors that includeconsent adherence to the validation protocol whichphase to choose for defining DBP size of cuff and leveland range of BP make validation studies in children muchmore difficult than in adults [4735w]
PregnancyA number of ABPM devices have been validated innormotensive and hypertensive women in pregnancyand preeclampsia and although more devices are beingrecommended for use in clinical practice there are severaldevices that are not accurate in pregnancy [484936wndash41w] In pregnancy auscultation of DBP has been contro-versial leading to differences of opinion between mufflingand disappearance of sounds as the criterion for DBP [49]There is now general agreement that disappearance ofsounds is the best measure of DBP [50]
The elderlyValidation data in elderly patients are available only for theSpaceLabs 90207 [42w] It is important to define clearly theage group in which the device is being assessed Individualsover the age of 65 years will also have a higher prevalenceof diseases and conditions that can affect arterial stiffness
Copyright copy Lippincott Williams amp Wilkins Unaut1736 wwwjhypertensioncom
and therefore influence the outcome of validation studiesThe elderly have an increased prevalence of arrhythmiasincluding atrial fibrillation bradycardia and ventriculartachyarrhythmias and are more likely to have inter-armdifferences in pressures due to upper arm arterial diseasewhich would make them unsuitable for validation studies[51]
Patients with arrhythmiasThere are no formal validation studies using establishedprotocols for ABPM devices in this special population Inpatients with arrhythmias it is difficult to standardize theheart rates during validation Good recordings can beobtained with ABPM in most patients although there is atendency for electronic devices to overestimate DBP inpatients with atrial fibrillation [52]
Obese patientsNo validation studies of ABPM monitors have been per-formed in the obese population Obesity has an adverseimpact on vascular stiffness influencing thereby theaccuracy of the oscillometric technique and these patientshave large arms which may complicate recruitment forvalidation studies particularly when a specified range ofcuffs has to be assessed [53]
Patients with renal diseaseOnly one ABPM device has been validated for patients withrenal disease [43w] Validating devices in patients with end-stage renal disease (ESRD) and chronic kidney disease(CKD) presents a number of problems [43w44w] thatinclude finding an available upper extremity the effectof arterial stiffness on the oscillometric methodologyespecially for DBP [54] and the demanding schedule ofdialysis that makes recruitment of patients difficult
413 Additional features for ambulatory bloodpressure monitorsAll ABPM monitors measure BP and pulse rate and mostprovide measurements not only for SBP and DBP but alsofor mean BP and pulse pressure Over the past decadeABPM devices have been developed to measure or calcu-late intermittently or continuously other parameters suchas the ECG pulse wave velocity and central BP Further-more accessories such as position sensors and accelerom-eters for physical activity analysis have been incorporatedto provide a more precise pathophysiological profileMajor limitations of these innovative devices are theirrelatively high price and the need to validate the associatedfunctions according to adequate protocols and to provideevidence for their clinical usefulness Until these require-ments are fulfilled the use of such ABPM devices shouldbe restricted to research laboratories and specializedcenters
Ambulatory blood pressure monitoring and homeblood pressureDevices which can be used either for 24-h ABPM or in a7-day mode to collect multiday BP data are being devel-oped and one has been validated [45w46w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Ambulatory blood pressure monitoring and ECGDevices have been developed allowing 24-h ABPM withcontinuous 24-h ECG in a single procedure Besides theusual well established indications for each of these pro-cedures the interaction between these two signals providescomplementary interrelated information in one procedureThe use of the real heart rate to determine the deflation ratecan provide more precise BP measurement and additionalextra BP measurements can be triggered by abnormal ECGactivities such as arrhythmias and ST segment abnormal-ities Limitations are the relatively high cost of monitors andsoftware the complexity compared to the simple ABPMprocedure and the difficulties in performing validationstudies for the combined functions [47w48w] Thesedisadvantages are offset to some extent by being ableto perform the two procedures simultaneously in olderpatients in whom arterial hypertension and paroxysmalatrial fibrillation often coexist Another development hasbeen the use of spectral analysis of heart rate to provide ameans for improving screening for obstructive sleep apnea(OSA) [49w50w]
Ambulatory blood pressure monitoring and arterialfunctionDevices are being developed that measure arterial stiffnessso as to provide interesting information on 24-h ABPM andon arterial function [51wndash55w]
Ambulatory blood pressure monitoring and positionsensingPosition sensors have been developed to determinewhether the patient is standing or lying during ABPMrecording and this facility allows an estimation of the sleepperiod [5556w]
Ambulatory blood pressure monitoring and activitysensingActivity sensors and accelerometers have been developedfor monitoring patient activity during ABPM so as to providean indirect measure of activity and rest with the formerbeing an estimate of the awake period and the latter ofsleep Some of these sensors are incorporated in the devicewhereas others are complementary accessories placedeither at wrist thigh or chest level [57w]
Ambulatory blood pressure monitoring and centralblood pressureSeveral 24-h oscillometric ABPM monitors use specificalgorithms and software for pulse wave analysis by record-ing 24-h ABPM data as well as calculating central BP [5651wndash53w58wndash61w] Further studies are needed howeverto demonstrate the validity and clinical usefulness of thesedevices which at present should not be used for makingclinical decisions
42 Software for ambulatory blood pressuremonitoring data analysisRecommendations on procedures for ABPM use tend toconcentrate on the accuracy of the devicersquos hardware withlittle attention being paid to software presentation and
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
analysis of ABPM data As a consequence the practisingphysician who has to interpret the considerable amount ofdata provided by ABPM is often faced with a bewilderingreport with reams of paper containing plots histogramsand data analysis that have little relevance for clinicalpractice It is important for ABPM software programs tobe suitable for the intended use of the device For examplein a busy general practice perhaps only basic data givingaverage 24-h daytime and night-time values and a visualplot are all that will be required whereas for researchpurposes statistical detail on the windows of the 24-hprofile and other indices may be required [10] A recentstudy has stressed that whereas monitors for ABPM aresubject to extensive validation protocols there is no inter-national guideline on the software processing of the col-lected raw data to prevent error being introduced by thesoftware permutations An example of software-inducederror was demonstrated for the SpaceLabs Report Manage-ment System 92506 which showed errors in 92 of reportsamounting to a numerical difference between printout andon-screen hourly averages ranging from 37 to 18mmHgfor SBP and from 16 to 10mmHg for DBP [62w] Anadditional problem can arise from the calculation of 24-haverage BP values that are not weighted for the differentnumber of hourly measurements during daytime and night-time weighted hourly BP values have been shown to bemore reliable than calculations based on the average of allindividual readings [57]
The use of ABPM in clinical practice can be facilitated bystandardizing the graphic presentation of ABPM datamuch as is the case for ECG recordings so that the pres-entation of data is independent of the type of ABPMmonitor used and the user is not required to becomefamiliar with a variety of programs Standardization alsofacilitates the interchange of ABPM recordings betweendatabases such as a hospital and primary care practiceMoreover if ABPM software programs provide a printedreport of the standardized ABPM data with a validatedinterpretative report [58] (signed by the physician in chargeof the service whenever legally required) doctors andnurses unfamiliar with the technique are assisted inlearning the variety of patterns generated by ABPM andbecause an individualized physician report is not a require-ment in most cases the cost of ABPM is reduced [110](Box 4)
421 Software requirementsThe following facilities are recommended for ABPM soft-ware in clinical practice [1910]
Clinical reportThe following information should be available in a one-page report
or
1
ize
Standardized plot format with each BP measurementon the vertical axis and time of day on horizontal axiswith different windows of the 24-h period identifiedand normal bands clearly demarcated The sleep timeinterval used to calculate asleep BP should be indi-cated (shaded) and preferably based on the indivi-dualsrsquo sleep time report (diary cards) In the plot the
d reproduction of this article is prohibitedwwwjhypertensioncom 1737
Cop
Box 4 Software requirements
Clinical report Ambulatory blood pressure measurement analysis and report should be standardized independent of the monitor type Standardized plot of all the blood pressure measurements with daytime and night-time windows and normal blood pressure bands demarcated Average SBP DBP and heart rate to be displayed Nocturnal blood pressure decline () for SBP and DBP Summary statistics for time-weighted average SBP and DBP and heart rate for the 24-h period daytime and night-time with standard deviations and number
of valid blood pressure readings Facility for showing error readings if requiredOptional requirements Automated software generated interpretative report indicating the normal or abnormal patterns and whether the requirements for a valid recording are
fulfilled Facility to plot heart rate and mean blood pressure Trend report for comparing repeated ambulatory blood pressure measurement recordings Ability to centrally host dataResearch report Data storage and raw data export capability for research analysis and audit Parameters include variability measures (such as 24-h SD 24-h weighted SD average real variability coefficient of variation) area under the curve
calculations blood pressure load parameters ratendashpressure product trough and peak levels smoothness index (the last two parameters requiring ABPMdata before and during treatment to be available) cusum-derived statistics and ambulatory arterial stiffness index
OrsquoBrien et al
1738
upper value of the Y-axis should not be fixed butadjustable to the highest BP value recorded in orderto maximize the graphic presentation of BP variationsover the 24-h period A plot of SBP and DBP through-out the 24-h period with a facility for plotting heartrate and mean BP so as to provide evidence ofcircadian behavior should be provided
2
Summary statistics for time-weighted SBP and DBPand heart rate in the windows of the 24-h period andseparately for the awake and asleep subperiods withthe respective standard deviations and the number ofvalid BP readings included in the analysis and afacility for indicating the time of going to bed andawakening
3
Medication details
4
Facility for showing error readings if required
Interpretative reportTo remove the variance associated with the ABPMinterpretation by human observers and to simplify theevaluation of results in routine clinical practice for thoseunfamiliar with the technique there should be an auto-mated software-generated interpretative report indicatingnormal or abnormal BP patterns and whether there aresufficient measurements for the recording to be valid [10]The interpretative report should be validated by testing thecomputer-generated report against reports from experts[5859]
Trend reportThe provision of a trend report allows ABPMs to be com-pared over time to demonstrate the response to changes inmanagement If ABPM is to be used to achieve better BPcontrol it is important for prescribing doctors (and patients)to be able to see whether medication is achieving controlthroughout the entire 24-h period
Research reportThe system should be capable of storing data for detailedanalysis for research and audit according to evidence-based
yright copy Lippincott Williams amp Wilkins Unautwwwjhypertensioncom
definitions for time-weighted arithmetic and mean valuesfor measures of BP level In view of evidence that short-term BP variability may give information over and abovemean BP levels and that reduction in 24-h BP variabilitymay be beneficial [63w] time-weighted and other measuresof short-term BP variability are helpful for on-goingresearch in this area Informative indices associated withoutcome such as area under the curve calculations BP loadparameters trough and peak levels the smoothness index(the last two parameters requiring ABPM data before andduring treatment to be available) cusum-derived statisticsand most recently the ambulatory arterial stiffness index(AASI) should also be provided [6061] The system shouldbe capable of storing and exporting raw data for researchpurposes and additional analyses [606163w]
422 Indices derived from ambulatory bloodpressure monitoring recordingsAverage BP values (over 24 h daytime and night-time) areundoubtedly the most important parameters obtained fromABPM recordings based on outcome data However alarge number of additional indices with promising clinicalevidence may be derived from ABPM recordings and someof them are occasionally included in the reports generatedby ABPM systems
Blood pressure loadThis index is defined as the percentage of readings in agiven period (24-h day or night) which exceed a prede-fined threshold value typically set at the proposed nor-malcy level for average BP values of that period The aim ofBP load is to quantify the number of readings with elevatedBP and mathematically it depends on both average BPlevels and distribution of BP readings [62] Although intheory clinically appealing and thus commonly incorpor-ated in the ABPM software this index has a number oflimitations Firstly there is no evidence that the thresholdsdefined for average BP values have any prognostic meaningwhen applied to single BP measurements Secondly whencomparing recordings with similar average BP levels differ-ences in BP load can be largely explained by differences in
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
BP variability making this index largely redundant ThirdlyBP load does not contain the prognostically importantinformation on how much the threshold level has beenexceeded To overcome the latter limitation it has beenproposed to modify the classic BP load definition bycalculating the total area under the timendashpressure curvewhen BP exceeds the threshold [63] Finally although somestudies support the usefulness of BP load in predictingorgan damage [6464w] it has never been convincinglydemonstrated that it provides any additional and clinicallyrelevant information independently of what is obtained byfocusing on average BP values The use of BP load inchildren has also been examined but it has not been foundhelpful in diagnosis [65w]
Ratendashpressure productThis index which is defined as heart rate multiplied by SBPis used as an index of myocardial work during exercise andit has prognostic relevance [66w] The availability of bothheart rate and BP data in ABPM makes it possible to obtainthe index readily especially if ABPM is accompanied byactigraphy [65] Although potentially promising the clinicalapplication of this index requires further research
rsquoVascularrsquo indicesSeveral ABPM-based indices have been proposed to pro-vide information on vascular wall properties Their ration-ale is based on the observation that the stiffness of thearterial wall increases when it is being stretched in patientswith impaired arterial wall elasticity SBP increases moresteeply than DBP whereas in a patient with elastic arteriesSBP and DBP increase in parallel The AASI which iscalculated as 1 ndash slope of regression of DBP on SBP isreadily obtainable from ABPM [6066]
AASI appears to have a direct relationship to carotidndashfemoral pulse wave velocity (a validated index of largearteriesrsquo stiffness) and an independent relationship withcardiovascular outcomes [606167wndash70w] Howeverthe ability of AASI to reflect arterial stiffness has beenchallenged because of its dependence on nocturnal BP falland the fact that it implies the use of asymmetric regressionpossibly affecting the precision of slope estimation[67ndash6971w72w] Modifications to AASI have been pro-posed but further data are awaited as to their ability tosurpass AASI in predicting outcome [73w74w]
The QndashKd interval which measures the time intervalbetween the onset of the QRS on the electrocardiogram (Q)and the last Korotkoff sound (K) corresponding to thediastolic pressure (d) has also been shown to have prog-nostic value [70]
Indices for indicating the pattern of treatment-induced changes in 24-h blood pressure loweringTwo principal indices are available for assessing thesmoothness and consistency of antihypertensive treatmenteffect over 24 h with ABPM The trough-to-peak ratio is theratio between BP reduction achieved by treatment at theend of dosing interval (trough which for drugs adminis-tered once daily means 24 h after the last dose intake) andpeak BP reduction usually achieved a few hours after dose
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
intake [7172] The trough-to-peak ratio is characterized by ahigh degree of variability in individual patients and istherefore not suitable for application to clinical practice[73] The smoothness index is calculated as the ratiobetween the average of hourly BP reductions over 24 hand the standard deviation (SD) of such an average valuethus integrating information on the size of BP reduction bytreatment and on its homogeneity throughout the 24-hperiod [7173] The smoothness index is highest for potentdrugs or drug combinations which also provide the mosthomogeneous BP reduction It is more reproducible thanthe troughpeak ratio [7173] and predicts treatment-induced changes in indices of organ damage includingleft ventricular mass and carotid arterial wall thickness[75w] A recent meta-analysis has provided informationon clinical determinants of the smoothness index suchas age ethnicity sex and smoking [74] The relevance ofthese indices in predicting the impact of treatment onoutcome and the reference values remain to be assessed
5 PROCEDURE
51 Training requirementsThe technique of ABPM is a specialized one and should beapproached with the care reserved for any such procedureAn understanding of the principles of traditional BPmeasurement cuff fitting monitor function and analysisand interpretation of ABPM data is required In practice anurse with an interest and experience in hypertension canmaster the use of ABPM devices after a relatively brieftraining However the interpretation of ABPM profilesrequires experience in the technique which is best pro-vided by the doctor in charge of an ABPM service [19]
52 Fitting an ambulatory blood pressuremonitorTime needs to be given to fitting the monitor and preparingthe patient for the monitoring period if good results are tobe obtained [19] The key to successful ABPM is educatingthe patient on the process of monitoring and the instruc-tions should be explained and printed on a diary card Inclinical practice measurements are preferably performedon a routine working day Although ABPM is best notperformed while patients are admitted to hospital becausehospitalization leads to underestimation of BP and over-diagnosis of nondippers [10] there are occasions such asthe evaluation of severely resistant hypertension andassessment of patients following a stroke when ABPM inhospital may be indicated
The frequency of measurement during the 24-h period isgenerally not more than every 15 min (which could inter-fere with normal activity) nor less than every 30min (whichcould give an inadequate number of measurements) Morefrequent measurements at night may disturb sleep andsleep disturbance has been shown to reduce the prognosticvalue of ABPM [75] To improve reproducibility repetitionof ABPM should be performed on like days for example onroutine working or recreational days A diary card can beused to record symptoms and events that may influenceABPM measurements
orized reproduction of this article is prohibitedwwwjhypertensioncom 1739
OrsquoBrien et al
53 Explanation to patientThe first step is adequate explanation of the procedure in anattempt to allay anxiety especially in nervous patientsPatients having ABPM for the first time should be told thatthere is minor discomfort caused by inflation of the cuff It isimportant to emphasize to the patient to follow hisherusual daily activities but as much as possible to remain stillwith the arm relaxed and not extended or contracted atheart level during each BP measurement [19] It can behelpful to have patients record periods of stress the time ofmeals the time of a siesta the time of going to bed andrising the quality of sleep and the time and type ofdrug ingestion
Box 5 Evaluation of ambulatory blood pressure monitoring data
Definition of daytime and night-time Daytime and night-time intervals are best defined using sleeping times
reported by individual usersrsquo diary cards (awake and asleep periods) Fixed narrow time intervals can be applied by discarding transition
periods between daytime and night-time (eg daytime defined as0900ndash2100 h and night-time 0100ndash0600 h)
Editing requirements Editing is not necessary for calculating average 24-h daytime and
night-time values The ambulatory blood pressure monitoring should be repeated if thefollowing criteria are not met
24-h recording with at least 70 of expected measurements20 valid awake (0900 to 2100 h)7 valid asleep (0100 to 0600 h)Blood pressure measurements at 30-min intervalsFor research purposes at least two valid daytime and one valid
night-time measurement per hour
54 Identification of daytime and night-timeperiods and editing ambulatory blood pressuremonitoring dataOne simple and popular method for identifying daytimeand night-time subperiods is to assess the time of awaken-ing and sleeping from diary card entries Another method isto use a fixed-narrow time interval approach in which forexample the retiring (2101 to 0059 h) and rising (0601 to0859 h) periods (which are subject to considerable vari-ation) are eliminated with the daytime period being from0900 to 2100 h and night-time from 0100 to 0600 h in thisway the variations in the time spent in bed that may existbetween the young and the old and in different culturesare to some extent eliminated from the analysis [176w]This method has the disadvantage of eliminating infor-mation on the white-coat window on the early phase ofnight sleep when dipping can be most evident and onthe early morning surge of BP which may be associatedwith cardiovascular events However these windows canbe analyzed separately for research or if considered import-ant in practice In countries where a daytime siesta ispopular a record of sleeping times both during day andnight is important and ABPM software should be able toadjust for this otherwise there may be underestimation ofthe nocturnal BP dip and overdiagnosis of nondippers[77w]
Many statistical techniques exist for editing ABPMrecords and no one method is ideal [176w] The detec-tion of artefactual readings and the handling of outliervalues (which may or may not be erroneous) have indeedbeen the subject of debate [76w] There are a number ofways of separately analyzing BPs recorded during the dayand night [7678w] Several automatic procedures havebeen proposed to reject outlying measurements based ona univariate multivariate or temporal approach Morecomplex procedures requiring the intervention of theobserver have been proposed but they are time consum-ing and not suitable for clinical practice [77] It has beenshown that rejection of outliers may alter the results ofABPM in individual patients sometimes significantlyaffecting average SBP levels [777879w] Editing pro-cedures can reduce mean systolic ABPM by 4 mmHg incomparison with unedited recordings thereby decreasingthe likelihood of diagnosing sustained hypertension Inone study the prevalence of sustained hypertension wasdecreased by 6ndash10 when several editing methods were
Copyright copy Lippincott Williams amp Wilkins Unaut1740 wwwjhypertensioncom
applied to raw 24-h data [79w] To make the results ofdifferent laboratories comparable common editingcriteria for ABPM should be used The problem is toestablish which of the methods proposed in the literatureprovides the most reliable data While awaiting moreobjective criteria to identify a universally acceptable edit-ing procedure we recommend that editing is not necess-ary for calculating average 24-h daytime and night-timevalues and that only physiologically impossible readingsshould be deleted from recordings However when thereare excessive artefacts in a tracing a repeat recordingrather than editing should be performed Some editingmight be required when focusing on analysis of BPvariability for the quantification of which the presenceof artefacts may introduce appreciable errors If editing isconsidered necessary a method proposed by Casadeiet al [80w] and modified by Winnicki et al [78] providescomparable performance to other proposed editing pro-cedures
There are no firm data on which to base recommen-dations for a satisfactory ABPM recording but the recom-mendation for having at least 70 of expectedmeasurements provides a basic working recommendationfor clinical practice This figure will be influenced by theperiod demarcated as daytime (awake) or night-time(asleep) periods and by the number of measurementsselected (usually 30-min but often 15 or 20-min intervals)In the previous ESH guideline on measurement it wasrecommended that there should be a minimum of 14measurements during the day and seven measurementsat night [1] Having considered what evidence is availableand the practical issues of performing repeat ABPM inpractice it seems reasonable to increase the minimum ofdaytime measurements to 20 while retaining a minimumseven measurements at night based on measurementsbeing performed every 30min and with fixed time periodsbeing used to define day (0900 to 2100 h) and night (0100 to0600 h) [1] (Box 5)
55 The arm for measurementABPM is best measured in the nondominant arm so as tointerfere as little as possible with daily activity unless there
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
has been documented evidence of a difference in BPbetween arms in which case the arm known to have thehigher BP values should be chosen [1] It is commonpractice for BP to be measured by a conventional techniqueat the same time as an ABPM monitor is being fitted and todetermine whether there is a discrepancy between thetechniques However BP variability is such that any suchcomparison has little validity and to determine a significantdifference it is necessary to perform simultaneousmeasurement according to a definitive protocol and thisis not feasible in practice [42] Because of these limitationsthe practice of performing a comparative measurement isnot recommended
56 Selecting the appropriate cuff and bladderThere is unequivocal evidence that either too narrow ortoo short a bladder (undercuffing) will cause overesti-mation of BP so-called lsquocuff hypertensionrsquo and there isgrowing evidence that too wide or too long a bladder(overcuffing) may cause underestimation of BP Under-cuffing has the effect in clinical practice of overdiagnos-ing hypertension and overcuffing leads to hypertensivepatients being diagnosed as normotensive Either even-tuality has serious implications for the epidemiology ofhypertension and for clinical practice [79] It is importanttherefore to select a cuff containing an inflatable bladderof correct length and width for the arm in which ABPM isto be measured All ABPM devices should provide cuffscontaining bladders for small medium and large-sizedarms as recommended in international guidelines[18081] However in many obese individuals the largebladder sizes cannot be used because the arm length istoo short to accommodate the bladder [81w] Anotherproblem is that the cylindrical shape of the commonlyused cuffs does not always wrap snugly around conical-shaped arms in obese and very muscular arms[8282w83w] Recently novel oscillometric homemonitors with cuff technology that allows a singlefixed-size cuff to be used on a wide range of arm circum-ferences have been developed [84wndash87w]
Another issue that needs consideration is the possibilitythat the discomfort caused by inflation of a large cuff inobese patients might cause elevation of BP This issuebecomes more important during ABPM because ofrepeated measurement especially during night-time sleepOscillometric devices for home use that measure BP duringcuff inflation may induce less discomfort because themeasurement is completed before maximal inflation[84w88w] However to date no study has specificallyaddressed this issue
Forearm BP measurement may have to be consideredwhen extreme obesity makes upper arm BP measurementimpossible BP measurements tend to be higher with fore-arm compared with upper arm measurement but meth-odological differences in these studies make it difficult toprovide recommendations for all populations [8389wndash94w] Despite the questionable accuracy of forearm BPmeasurement it may be the only acceptable option forABPM in individuals with very large upper arms providedthe patient is instructed to keep the forearm at heart levelduring measurement [94w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
No wrist devices have been validated for ABPM whereastechnology for continuous beat-to-beat monitoring ofambulatory BP in the finger has been developed usingthe volume-clamp method first described by Penaz [95w]A number of studies that compared this technology withintraarterial or noninvasive BP measurement showedunderestimation of BP particularly diastolic yet it remainsa practical alternative to intraarterial measurement for theevaluation of beat-to-beat BP changes and variability inresearch studies [8496wndash98w]
57 Conditions in which ambulatory bloodpressure monitoring may be difficult toperform
Obese patientsObesity is a well established major risk factor for hyperten-sion with higher prevalence in specific population groupssuch as patients with diabetes mellitus [99w] or OSA [100w]Despite the increasing prevalence of obesity worldwide[101w] and the close link between obesity and hyperten-sion scarce data are available on the application of ABPM inobese and extremely obese individuals ABPM is oftenrequired in these individuals and technical difficultiesshould not exclude them from such a valuable technology[79] The problem of miscuffing in obese pregnant womenmay result in diagnostic discrepancies [85]
Patients with atrial fibrillationBP measurement in patients with atrial fibrillation is lessprecise as this type of arrhythmia is accompanied byincreased beat-to-beat BP variability due to variations inventricular filling time stroke volume and contractilityInternational guidelines [181] recognize the relatively poorprecision of a single BP measurement and recommendrepeated readings in order to improve the accuracy ofestimates Theoretically ABPM should fulfill this stipulationas it provides a relatively high number of readings in a shortperiod of time Unfortunately published evidence regard-ing the role of ABPM in patients with arrhythmias andspecifically in patients with atrial fibrillation is scarce
Patients with atrial fibrillation have been usuallyexcluded from trials using ABPM as well as from validationprotocols of ABPM devices Four studies have addressedthe possible value of ABPM in patients with atrial fibrillation[48w102wndash104w] The evidence from these studiessuggests that ABPM may be useful in these patients pro-vided its limitations are taken into account The proportionof readings with errors the variability of BP and therepeatability coefficients do not appear to be different fromthose in patients in sinus rhythm DBP measured using anABPM monitor in patients with atrial fibrillation appears tobe relatively higher than that obtained with the traditionaloffice measurement or by the same ABPM procedure whenthe patient achieves sinus rhythm This finding is supportedby a review and meta-analysis of studies that validatedelectronic devices in patients with sustained atrial fibrilla-tion which showed consistent overestimation of DBP [52]In spite of this and although larger trials in patients on atrialfibrillation are recommended there is no reason to exclude
orized reproduction of this article is prohibitedwwwjhypertensioncom 1741
OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

OrsquoBrien et al
debate over the years [19ndash241w8wndash19w] The issue ismore complex than for conventional measurement becausenormality needs to be defined for both daytime and night-time pressures and outcome data are scarce
In defining normality for ABPM it is necessary to move onfrom diagnostic thresholds determined in a statistical way innormotensive andor hypertensive reference populations tooutcome-driven thresholds The International Database ofAmbulatory blood pressure in relation to CardiovascularOutcome (IDACO) based on 5682 participants followedfor 97 years determined ABPM thresholds which yielded10-year cardiovascular risk (for cardiovascular cardiac andstroke outcomes) corresponding to high BP on officemeasurement (gt14090mmHg) Corresponding thresholdsfor hypertension with ABPM were 1310794 for 24h 1382864 for daytime and 1195708mmHg for night-time [25]
Whereas outcome-driven thresholds are currently avail-able for adults the question remains to be resolved whetherthey are applicable across the whole age range and in allconditions or whether separate recommendations arenecessary for older and very old individuals and for preg-nant women In the case of children and adolescents adifferent approach is needed and therefore thresholdsbased on population distribution have been proposed(See Section 67)
Head et al [26] examined a different approach to deriveage-related and sex-related ABPM equivalents to clinic BPthresholds for diagnosis and treatment of hypertension byaccounting for age and sex They also compared clinicmeasurements taken by nonmedically qualified health pro-fessionals with those taken by doctors to assess whether alsquowhite-coatrsquo effect might have influenced the findings ofprevious studies that were based solely on doctorrsquosmeasurements This analysis provided a range of daytimeABPM measurements equivalent to recognized clinic BPthresholds which when predicted from clinic BP valueswere close to those derived from other outcome analyses
The threshold values in the recent NICE guidelines [4]the JNC 7 guideline [27] and the ESHESC guidelines for2003 2007 and 2013 [12829] and the results of outcomestudies such as IDACO [25] and Ohasama [30] have con-tributed to the definition of consensus values summarizedin Box 2 It is recognized that the levels in Box 2 might beregarded as conservative by some and it is acknowledgedthat further studies are needed to define thresholds moreprecisely particularly in high-risk patients
33 Cost-effectiveness of ambulatory bloodpressure monitoringThe cost-effectiveness of ABPM has been considered from anumber of perspectives First ABPM may enable financialsavings in drug prescribing ABPM is superior to othermeasurement techniques in demonstrating the efficacy of
Box 2 Thresholds for hypertension diagnosis based on ambulatory bloodpressure monitoring
24-h average 13080 mmHg
Awake (daytime) average 13585 mmHg
Asleep (night-time) average 12070 mmHg
Copyright copy Lippincott Williams amp Wilkins Unaut1734 wwwjhypertensioncom
antihypertensive drugs in pharmacological trials [3132]Adjustment of antihypertensive therapy according to ABPMrather than office BP has been shown to result in lessantihypertensive medication being prescribed withoutcompromising target organ involvement [33] It has alsobeen shown that in patients on treatment with BP-loweringdrugs ABPM was a better predictor of cardiovascular out-come than office BP [34] Reduction in office BP due toamelioration of the white-coat effect especially in elderlypatients who have greater BP variability may be attributedwrongly to a BP-lowering effect of antihypertensive medi-cation if ABPM is not used to assess treatment efficacy[35]
Second by identifying patients with white-coat hyper-tension ABPM may improve drug prescribing in a cost-effective manner [36] The cost of care for hypertension isdominated by the long-term occurrence of cardiovascularcomplications and the costs for drug treatment rather thanby the short-term cost for visits and investigations [3720w]
Third ABPM can identify individuals with normal BP inthe office but elevated BP levels in daily life (rsquomaskedhypertensionrsquo) a condition that has been shown to carrythe same adverse prognosis as sustained arterial hyperten-sion both in the clinic and in daily life (see Section 63)
Until recently ABPM is generally cited as being moreexpensive than other measurement techniques though ithas been shown to be cost-effective both in specialistservices and in primary care [3621w] This has been attrib-uted to the fact that only tangible benefits have beenconsidered such as identifying patients with white-coathypertension and the savings that might be made from themore efficient prescribing of BP-lowering drugs Howevercost-effectiveness considerations must be extended toinclude the financial potential of the technique not onlyto improve the diagnosis and management of hypertensionbut also as a means of ensuring that effective control ofhypertension is implemented at community level [9] ABPMis the most effective technique for identifying white-coathypertension which may be present in as many as 20 ofpeople who appear to have hypertension with office BPand these patients may be spared years of unnecessary andexpensive drug treatment which is often not free from side-effects They may also avoid being penalized unnecessarilyfor insurance or employment by having the diagnosis oflsquohypertensionrsquo misapplied [9]
A number of studies have analyzed the costndashbenefitaspects of ABPM Krakoff [36] has shown that potentialsavings of 3ndash14 for cost of care for hypertension and 10ndash23 reduction in treatment days when ABPM was incorp-orated into the diagnostic process On an annual basis thecost of ABPM would be less than 10 of treatment costsOther costndashbenefit analyses have shown that ABPM is mostcost-effective for the diagnosis and management of newlydiagnosed hypertension [921w]
Recently NICE undertook detailed costndashbenefit analysisfor ABPM and showed that the use of ABPM is the most cost-effective method of confirming a diagnosis of hypertensionin a population suspected of having high BP based on aconventional BP screening measurement of more than 14090mmHg and that the technique would result in substantialsavings to the UK National Health Service [438] However
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
the validity of the underlying assumptions by NICE has notbeen universally accepted [39]
Other potential benefits of ABPM that have not beenconsidered by NICE are the savings to be made in havingdrug treatment targeted to achieve 24-h BP control and thesubstantial savings to be made by the prevention of strokeand other cardiovascular consequences of hypertensionwith improved BP control Nor has NICE considered thepotential benefits of identifying the white-coat and maskedhypertension phenomena in treated individuals or of treat-ing nocturnal hypertension which is a major predictorof outcome
In a further extensive study of the cost of ABPM aMarkov model-based probabilistic cost-effectivenessanalysis concluded that ABPM is the most cost-effectivestrategy for the diagnosis of hypertension for men andwomen of all ages mainly by virtue of its potential toreduce misdiagnosis and to direct better targeted treatment[38]
As the cost of ABPM and hypertension managementdiffer greatly from country to country and is dependenton the method of healthcare delivery the cost-effectivenessof ABPM may need to be evaluated at a national level Forexample in Japan it has been estimated that the introduc-tion of ABPM for the management of hypertension hasreduced medical costs by about 948 trillion yen over 10years [40] (see Section 82)
34 Limitations of ambulatory blood pressuremonitoringThe technique of ABPM has many advantages over otheravailable techniques but it has its limitations whichinclude availability the provision of intermittent measure-ments during which the patient is sedentary rather thanlsquoambulatoryrsquo the possibility of inaccurate readings duringactivity and the inability to detect artefactual measure-ments the technique makes demands on the patient timeis needed to fit the device and it may cause discomfortparticularly during the night resulting in resistance fromsome patients to having repeat ABPM [11014] limitedreproducibility when the procedure is not standardized[41] and cost implications although the cost of devicesis reducing and costndashbenefit analyses have shown thatshort-term costs are justified by long-term savings (seeSection 33 Box 3)
Copyright copy Lippincott Williams amp Wilkins Unauth
Box 3 Limitations of ambulatory blood pressure monitoring
Application Limited availability May cause discomfort particularly at night Reluctance to use by some patients especially for repeat
measurement Cost implications (although the cost of devices is reducing
and possibly more cost-effective than office measurements)Function Imperfect reproducibility Provision of intermittent measurements in sedentary rather than
ambulatory conditions Possibility of inaccurate readings during activity Inability to detect genuine artefactual measurements
Journal of Hypertension
4 DEVICES AND SOFTWARE
41 Choosing an ambulatory blood pressuremonitoring device
411 Selecting an accurate deviceAn accurate device is fundamental to all BP measurementsif the device used to measure BP is inaccurate attention tomethodological detail is of little relevance It is acknow-ledged that the accuracy of BP-measuring devices shouldnot be based solely on claims from manufacturers whichcan at times be somewhat misleading Instead independ-ent validation using an established protocol with the resultspublished in peer-reviewed journals should be demanded[4222w] However manufacturers often ignore this recom-mendation and potential purchasers are generally unawareof this requirement assuming ndash not unreasonably ndash that ifa product reaches the market place it will measure BPaccurately The most popular validation protocol is theEuropean Society of Hypertension International Protocol(ESH-IP) and a recent review showed that from thepublication of the first version of the ESH-IP in 2002until June 2010 48 studies of device accuracy have beenreported using the British Hypertension Society (BHS)protocol 38 using the AAMI standard and 104 using theESH-IP 2010 [23w] Thus it seems that the ESH-IPsucceeded in expanding by three-fold to four-fold theuse of validation procedures worldwide compared withthe period before its publication [23w] A criticism bymembers of the AAMI Committee that the reduction inthe number of patients might compromise the validity ofthe protocol [24w] has been shown to be statisticallyunfounded [25w] The availability of the ESH-IP in anon-line version will further facilitate the validation of ABPMdevices [26w]
Since the ESH-IP was first published there has been animprovement in the performance of the oscillometric devi-ces for BP measurement [23w] but protocol violations andmisreporting have been particularly common suggestingthat there is a need for stricter standardization for conduct-ing and reporting a validation study [27w] The revisedversion of the ESH-IP protocol applied tighter validationcriteria for the pass level [42] and the application of thesemore stringent criteria is expected to double the validationfailure rate allowing more accurate devices to enter themarket [23w]
The AAMI protocol requires additional testing for ABPMdevices in 85 patients in the supine seated and standingpositions and stipulates that three devices should beassessed in ambulatory conditions all of which would bevery difficult and costly to perform [4328w] The BHSprotocol which is rarely used now also requires an in-use (field) assessment of ambulatory monitors [44] TheInternational Organization for Standardization (ISO) pro-tocol also requires additional clinical validation in 35patients in standardized conditions of physical activity(after exercise on a bicycle ergometer or treadmill toincrease heart rate by 10ndash20) [45]
It has recently been suggested that the validation ofautomated BP-measuring devices should be complementedby an overall quality check The PANET International
orized reproduction of this article is prohibitedwwwjhypertensioncom 1735
OrsquoBrien et al
Quality Certification Protocol denotes additional criteria ofquality for BP-measuring devices that fulfilled basic vali-dation criteria published in full in peer-reviewed medicaljournals On the basis of this evaluation a quality certifi-cation is released to the manufacturer and published onwwwpressionearteriosanet and wwwdableducationalorg[46]
The majority of devices for ABPM use oscillometry tomeasure BP but some devices also measure BP by micro-phonic detection of the Korotkoff sounds and such devicesneed to have both measurement methods validated accord-ing to accepted validation protocols [29w]
412 Validation requirements for ambulatoryblood pressure monitoring devices in specialpopulationsSeparate validation is required in specific populations suchas children and adolescents pregnant women and theelderly and in certain diseases such as obesity and arrhyth-mias [30w] Patients with arrhythmias children the elderlyand pregnant women present special challenges for vali-dation of oscillometric ABPM devices However althoughABPM devices are used frequently in these patient popu-lations specific validation studies have often not beenperformed this limitation applies also to other methodsof BP measurement such as home and office measure-ments The validation status of ABPM devices in differentpopulations can be checked on dedicated websites (egwwwpressionearteriosanet or wwwdableducationalorg)Although specific validation studies of ABPM devices inthese special populations are desirable in the future devi-ces that have been validated in the general hypertensivepopulation can be used so that high-risk patients are notdenied the benefit of ABPM
ChildrenFour ABPM devices have been validated in children andadolescents [31wndash34w] A number of factors that includeconsent adherence to the validation protocol whichphase to choose for defining DBP size of cuff and leveland range of BP make validation studies in children muchmore difficult than in adults [4735w]
PregnancyA number of ABPM devices have been validated innormotensive and hypertensive women in pregnancyand preeclampsia and although more devices are beingrecommended for use in clinical practice there are severaldevices that are not accurate in pregnancy [484936wndash41w] In pregnancy auscultation of DBP has been contro-versial leading to differences of opinion between mufflingand disappearance of sounds as the criterion for DBP [49]There is now general agreement that disappearance ofsounds is the best measure of DBP [50]
The elderlyValidation data in elderly patients are available only for theSpaceLabs 90207 [42w] It is important to define clearly theage group in which the device is being assessed Individualsover the age of 65 years will also have a higher prevalenceof diseases and conditions that can affect arterial stiffness
Copyright copy Lippincott Williams amp Wilkins Unaut1736 wwwjhypertensioncom
and therefore influence the outcome of validation studiesThe elderly have an increased prevalence of arrhythmiasincluding atrial fibrillation bradycardia and ventriculartachyarrhythmias and are more likely to have inter-armdifferences in pressures due to upper arm arterial diseasewhich would make them unsuitable for validation studies[51]
Patients with arrhythmiasThere are no formal validation studies using establishedprotocols for ABPM devices in this special population Inpatients with arrhythmias it is difficult to standardize theheart rates during validation Good recordings can beobtained with ABPM in most patients although there is atendency for electronic devices to overestimate DBP inpatients with atrial fibrillation [52]
Obese patientsNo validation studies of ABPM monitors have been per-formed in the obese population Obesity has an adverseimpact on vascular stiffness influencing thereby theaccuracy of the oscillometric technique and these patientshave large arms which may complicate recruitment forvalidation studies particularly when a specified range ofcuffs has to be assessed [53]
Patients with renal diseaseOnly one ABPM device has been validated for patients withrenal disease [43w] Validating devices in patients with end-stage renal disease (ESRD) and chronic kidney disease(CKD) presents a number of problems [43w44w] thatinclude finding an available upper extremity the effectof arterial stiffness on the oscillometric methodologyespecially for DBP [54] and the demanding schedule ofdialysis that makes recruitment of patients difficult
413 Additional features for ambulatory bloodpressure monitorsAll ABPM monitors measure BP and pulse rate and mostprovide measurements not only for SBP and DBP but alsofor mean BP and pulse pressure Over the past decadeABPM devices have been developed to measure or calcu-late intermittently or continuously other parameters suchas the ECG pulse wave velocity and central BP Further-more accessories such as position sensors and accelerom-eters for physical activity analysis have been incorporatedto provide a more precise pathophysiological profileMajor limitations of these innovative devices are theirrelatively high price and the need to validate the associatedfunctions according to adequate protocols and to provideevidence for their clinical usefulness Until these require-ments are fulfilled the use of such ABPM devices shouldbe restricted to research laboratories and specializedcenters
Ambulatory blood pressure monitoring and homeblood pressureDevices which can be used either for 24-h ABPM or in a7-day mode to collect multiday BP data are being devel-oped and one has been validated [45w46w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Ambulatory blood pressure monitoring and ECGDevices have been developed allowing 24-h ABPM withcontinuous 24-h ECG in a single procedure Besides theusual well established indications for each of these pro-cedures the interaction between these two signals providescomplementary interrelated information in one procedureThe use of the real heart rate to determine the deflation ratecan provide more precise BP measurement and additionalextra BP measurements can be triggered by abnormal ECGactivities such as arrhythmias and ST segment abnormal-ities Limitations are the relatively high cost of monitors andsoftware the complexity compared to the simple ABPMprocedure and the difficulties in performing validationstudies for the combined functions [47w48w] Thesedisadvantages are offset to some extent by being ableto perform the two procedures simultaneously in olderpatients in whom arterial hypertension and paroxysmalatrial fibrillation often coexist Another development hasbeen the use of spectral analysis of heart rate to provide ameans for improving screening for obstructive sleep apnea(OSA) [49w50w]
Ambulatory blood pressure monitoring and arterialfunctionDevices are being developed that measure arterial stiffnessso as to provide interesting information on 24-h ABPM andon arterial function [51wndash55w]
Ambulatory blood pressure monitoring and positionsensingPosition sensors have been developed to determinewhether the patient is standing or lying during ABPMrecording and this facility allows an estimation of the sleepperiod [5556w]
Ambulatory blood pressure monitoring and activitysensingActivity sensors and accelerometers have been developedfor monitoring patient activity during ABPM so as to providean indirect measure of activity and rest with the formerbeing an estimate of the awake period and the latter ofsleep Some of these sensors are incorporated in the devicewhereas others are complementary accessories placedeither at wrist thigh or chest level [57w]
Ambulatory blood pressure monitoring and centralblood pressureSeveral 24-h oscillometric ABPM monitors use specificalgorithms and software for pulse wave analysis by record-ing 24-h ABPM data as well as calculating central BP [5651wndash53w58wndash61w] Further studies are needed howeverto demonstrate the validity and clinical usefulness of thesedevices which at present should not be used for makingclinical decisions
42 Software for ambulatory blood pressuremonitoring data analysisRecommendations on procedures for ABPM use tend toconcentrate on the accuracy of the devicersquos hardware withlittle attention being paid to software presentation and
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
analysis of ABPM data As a consequence the practisingphysician who has to interpret the considerable amount ofdata provided by ABPM is often faced with a bewilderingreport with reams of paper containing plots histogramsand data analysis that have little relevance for clinicalpractice It is important for ABPM software programs tobe suitable for the intended use of the device For examplein a busy general practice perhaps only basic data givingaverage 24-h daytime and night-time values and a visualplot are all that will be required whereas for researchpurposes statistical detail on the windows of the 24-hprofile and other indices may be required [10] A recentstudy has stressed that whereas monitors for ABPM aresubject to extensive validation protocols there is no inter-national guideline on the software processing of the col-lected raw data to prevent error being introduced by thesoftware permutations An example of software-inducederror was demonstrated for the SpaceLabs Report Manage-ment System 92506 which showed errors in 92 of reportsamounting to a numerical difference between printout andon-screen hourly averages ranging from 37 to 18mmHgfor SBP and from 16 to 10mmHg for DBP [62w] Anadditional problem can arise from the calculation of 24-haverage BP values that are not weighted for the differentnumber of hourly measurements during daytime and night-time weighted hourly BP values have been shown to bemore reliable than calculations based on the average of allindividual readings [57]
The use of ABPM in clinical practice can be facilitated bystandardizing the graphic presentation of ABPM datamuch as is the case for ECG recordings so that the pres-entation of data is independent of the type of ABPMmonitor used and the user is not required to becomefamiliar with a variety of programs Standardization alsofacilitates the interchange of ABPM recordings betweendatabases such as a hospital and primary care practiceMoreover if ABPM software programs provide a printedreport of the standardized ABPM data with a validatedinterpretative report [58] (signed by the physician in chargeof the service whenever legally required) doctors andnurses unfamiliar with the technique are assisted inlearning the variety of patterns generated by ABPM andbecause an individualized physician report is not a require-ment in most cases the cost of ABPM is reduced [110](Box 4)
421 Software requirementsThe following facilities are recommended for ABPM soft-ware in clinical practice [1910]
Clinical reportThe following information should be available in a one-page report
or
1
ize
Standardized plot format with each BP measurementon the vertical axis and time of day on horizontal axiswith different windows of the 24-h period identifiedand normal bands clearly demarcated The sleep timeinterval used to calculate asleep BP should be indi-cated (shaded) and preferably based on the indivi-dualsrsquo sleep time report (diary cards) In the plot the
d reproduction of this article is prohibitedwwwjhypertensioncom 1737
Cop
Box 4 Software requirements
Clinical report Ambulatory blood pressure measurement analysis and report should be standardized independent of the monitor type Standardized plot of all the blood pressure measurements with daytime and night-time windows and normal blood pressure bands demarcated Average SBP DBP and heart rate to be displayed Nocturnal blood pressure decline () for SBP and DBP Summary statistics for time-weighted average SBP and DBP and heart rate for the 24-h period daytime and night-time with standard deviations and number
of valid blood pressure readings Facility for showing error readings if requiredOptional requirements Automated software generated interpretative report indicating the normal or abnormal patterns and whether the requirements for a valid recording are
fulfilled Facility to plot heart rate and mean blood pressure Trend report for comparing repeated ambulatory blood pressure measurement recordings Ability to centrally host dataResearch report Data storage and raw data export capability for research analysis and audit Parameters include variability measures (such as 24-h SD 24-h weighted SD average real variability coefficient of variation) area under the curve
calculations blood pressure load parameters ratendashpressure product trough and peak levels smoothness index (the last two parameters requiring ABPMdata before and during treatment to be available) cusum-derived statistics and ambulatory arterial stiffness index
OrsquoBrien et al
1738
upper value of the Y-axis should not be fixed butadjustable to the highest BP value recorded in orderto maximize the graphic presentation of BP variationsover the 24-h period A plot of SBP and DBP through-out the 24-h period with a facility for plotting heartrate and mean BP so as to provide evidence ofcircadian behavior should be provided
2
Summary statistics for time-weighted SBP and DBPand heart rate in the windows of the 24-h period andseparately for the awake and asleep subperiods withthe respective standard deviations and the number ofvalid BP readings included in the analysis and afacility for indicating the time of going to bed andawakening
3
Medication details
4
Facility for showing error readings if required
Interpretative reportTo remove the variance associated with the ABPMinterpretation by human observers and to simplify theevaluation of results in routine clinical practice for thoseunfamiliar with the technique there should be an auto-mated software-generated interpretative report indicatingnormal or abnormal BP patterns and whether there aresufficient measurements for the recording to be valid [10]The interpretative report should be validated by testing thecomputer-generated report against reports from experts[5859]
Trend reportThe provision of a trend report allows ABPMs to be com-pared over time to demonstrate the response to changes inmanagement If ABPM is to be used to achieve better BPcontrol it is important for prescribing doctors (and patients)to be able to see whether medication is achieving controlthroughout the entire 24-h period
Research reportThe system should be capable of storing data for detailedanalysis for research and audit according to evidence-based
yright copy Lippincott Williams amp Wilkins Unautwwwjhypertensioncom
definitions for time-weighted arithmetic and mean valuesfor measures of BP level In view of evidence that short-term BP variability may give information over and abovemean BP levels and that reduction in 24-h BP variabilitymay be beneficial [63w] time-weighted and other measuresof short-term BP variability are helpful for on-goingresearch in this area Informative indices associated withoutcome such as area under the curve calculations BP loadparameters trough and peak levels the smoothness index(the last two parameters requiring ABPM data before andduring treatment to be available) cusum-derived statisticsand most recently the ambulatory arterial stiffness index(AASI) should also be provided [6061] The system shouldbe capable of storing and exporting raw data for researchpurposes and additional analyses [606163w]
422 Indices derived from ambulatory bloodpressure monitoring recordingsAverage BP values (over 24 h daytime and night-time) areundoubtedly the most important parameters obtained fromABPM recordings based on outcome data However alarge number of additional indices with promising clinicalevidence may be derived from ABPM recordings and someof them are occasionally included in the reports generatedby ABPM systems
Blood pressure loadThis index is defined as the percentage of readings in agiven period (24-h day or night) which exceed a prede-fined threshold value typically set at the proposed nor-malcy level for average BP values of that period The aim ofBP load is to quantify the number of readings with elevatedBP and mathematically it depends on both average BPlevels and distribution of BP readings [62] Although intheory clinically appealing and thus commonly incorpor-ated in the ABPM software this index has a number oflimitations Firstly there is no evidence that the thresholdsdefined for average BP values have any prognostic meaningwhen applied to single BP measurements Secondly whencomparing recordings with similar average BP levels differ-ences in BP load can be largely explained by differences in
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
BP variability making this index largely redundant ThirdlyBP load does not contain the prognostically importantinformation on how much the threshold level has beenexceeded To overcome the latter limitation it has beenproposed to modify the classic BP load definition bycalculating the total area under the timendashpressure curvewhen BP exceeds the threshold [63] Finally although somestudies support the usefulness of BP load in predictingorgan damage [6464w] it has never been convincinglydemonstrated that it provides any additional and clinicallyrelevant information independently of what is obtained byfocusing on average BP values The use of BP load inchildren has also been examined but it has not been foundhelpful in diagnosis [65w]
Ratendashpressure productThis index which is defined as heart rate multiplied by SBPis used as an index of myocardial work during exercise andit has prognostic relevance [66w] The availability of bothheart rate and BP data in ABPM makes it possible to obtainthe index readily especially if ABPM is accompanied byactigraphy [65] Although potentially promising the clinicalapplication of this index requires further research
rsquoVascularrsquo indicesSeveral ABPM-based indices have been proposed to pro-vide information on vascular wall properties Their ration-ale is based on the observation that the stiffness of thearterial wall increases when it is being stretched in patientswith impaired arterial wall elasticity SBP increases moresteeply than DBP whereas in a patient with elastic arteriesSBP and DBP increase in parallel The AASI which iscalculated as 1 ndash slope of regression of DBP on SBP isreadily obtainable from ABPM [6066]
AASI appears to have a direct relationship to carotidndashfemoral pulse wave velocity (a validated index of largearteriesrsquo stiffness) and an independent relationship withcardiovascular outcomes [606167wndash70w] Howeverthe ability of AASI to reflect arterial stiffness has beenchallenged because of its dependence on nocturnal BP falland the fact that it implies the use of asymmetric regressionpossibly affecting the precision of slope estimation[67ndash6971w72w] Modifications to AASI have been pro-posed but further data are awaited as to their ability tosurpass AASI in predicting outcome [73w74w]
The QndashKd interval which measures the time intervalbetween the onset of the QRS on the electrocardiogram (Q)and the last Korotkoff sound (K) corresponding to thediastolic pressure (d) has also been shown to have prog-nostic value [70]
Indices for indicating the pattern of treatment-induced changes in 24-h blood pressure loweringTwo principal indices are available for assessing thesmoothness and consistency of antihypertensive treatmenteffect over 24 h with ABPM The trough-to-peak ratio is theratio between BP reduction achieved by treatment at theend of dosing interval (trough which for drugs adminis-tered once daily means 24 h after the last dose intake) andpeak BP reduction usually achieved a few hours after dose
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
intake [7172] The trough-to-peak ratio is characterized by ahigh degree of variability in individual patients and istherefore not suitable for application to clinical practice[73] The smoothness index is calculated as the ratiobetween the average of hourly BP reductions over 24 hand the standard deviation (SD) of such an average valuethus integrating information on the size of BP reduction bytreatment and on its homogeneity throughout the 24-hperiod [7173] The smoothness index is highest for potentdrugs or drug combinations which also provide the mosthomogeneous BP reduction It is more reproducible thanthe troughpeak ratio [7173] and predicts treatment-induced changes in indices of organ damage includingleft ventricular mass and carotid arterial wall thickness[75w] A recent meta-analysis has provided informationon clinical determinants of the smoothness index suchas age ethnicity sex and smoking [74] The relevance ofthese indices in predicting the impact of treatment onoutcome and the reference values remain to be assessed
5 PROCEDURE
51 Training requirementsThe technique of ABPM is a specialized one and should beapproached with the care reserved for any such procedureAn understanding of the principles of traditional BPmeasurement cuff fitting monitor function and analysisand interpretation of ABPM data is required In practice anurse with an interest and experience in hypertension canmaster the use of ABPM devices after a relatively brieftraining However the interpretation of ABPM profilesrequires experience in the technique which is best pro-vided by the doctor in charge of an ABPM service [19]
52 Fitting an ambulatory blood pressuremonitorTime needs to be given to fitting the monitor and preparingthe patient for the monitoring period if good results are tobe obtained [19] The key to successful ABPM is educatingthe patient on the process of monitoring and the instruc-tions should be explained and printed on a diary card Inclinical practice measurements are preferably performedon a routine working day Although ABPM is best notperformed while patients are admitted to hospital becausehospitalization leads to underestimation of BP and over-diagnosis of nondippers [10] there are occasions such asthe evaluation of severely resistant hypertension andassessment of patients following a stroke when ABPM inhospital may be indicated
The frequency of measurement during the 24-h period isgenerally not more than every 15 min (which could inter-fere with normal activity) nor less than every 30min (whichcould give an inadequate number of measurements) Morefrequent measurements at night may disturb sleep andsleep disturbance has been shown to reduce the prognosticvalue of ABPM [75] To improve reproducibility repetitionof ABPM should be performed on like days for example onroutine working or recreational days A diary card can beused to record symptoms and events that may influenceABPM measurements
orized reproduction of this article is prohibitedwwwjhypertensioncom 1739
OrsquoBrien et al
53 Explanation to patientThe first step is adequate explanation of the procedure in anattempt to allay anxiety especially in nervous patientsPatients having ABPM for the first time should be told thatthere is minor discomfort caused by inflation of the cuff It isimportant to emphasize to the patient to follow hisherusual daily activities but as much as possible to remain stillwith the arm relaxed and not extended or contracted atheart level during each BP measurement [19] It can behelpful to have patients record periods of stress the time ofmeals the time of a siesta the time of going to bed andrising the quality of sleep and the time and type ofdrug ingestion
Box 5 Evaluation of ambulatory blood pressure monitoring data
Definition of daytime and night-time Daytime and night-time intervals are best defined using sleeping times
reported by individual usersrsquo diary cards (awake and asleep periods) Fixed narrow time intervals can be applied by discarding transition
periods between daytime and night-time (eg daytime defined as0900ndash2100 h and night-time 0100ndash0600 h)
Editing requirements Editing is not necessary for calculating average 24-h daytime and
night-time values The ambulatory blood pressure monitoring should be repeated if thefollowing criteria are not met
24-h recording with at least 70 of expected measurements20 valid awake (0900 to 2100 h)7 valid asleep (0100 to 0600 h)Blood pressure measurements at 30-min intervalsFor research purposes at least two valid daytime and one valid
night-time measurement per hour
54 Identification of daytime and night-timeperiods and editing ambulatory blood pressuremonitoring dataOne simple and popular method for identifying daytimeand night-time subperiods is to assess the time of awaken-ing and sleeping from diary card entries Another method isto use a fixed-narrow time interval approach in which forexample the retiring (2101 to 0059 h) and rising (0601 to0859 h) periods (which are subject to considerable vari-ation) are eliminated with the daytime period being from0900 to 2100 h and night-time from 0100 to 0600 h in thisway the variations in the time spent in bed that may existbetween the young and the old and in different culturesare to some extent eliminated from the analysis [176w]This method has the disadvantage of eliminating infor-mation on the white-coat window on the early phase ofnight sleep when dipping can be most evident and onthe early morning surge of BP which may be associatedwith cardiovascular events However these windows canbe analyzed separately for research or if considered import-ant in practice In countries where a daytime siesta ispopular a record of sleeping times both during day andnight is important and ABPM software should be able toadjust for this otherwise there may be underestimation ofthe nocturnal BP dip and overdiagnosis of nondippers[77w]
Many statistical techniques exist for editing ABPMrecords and no one method is ideal [176w] The detec-tion of artefactual readings and the handling of outliervalues (which may or may not be erroneous) have indeedbeen the subject of debate [76w] There are a number ofways of separately analyzing BPs recorded during the dayand night [7678w] Several automatic procedures havebeen proposed to reject outlying measurements based ona univariate multivariate or temporal approach Morecomplex procedures requiring the intervention of theobserver have been proposed but they are time consum-ing and not suitable for clinical practice [77] It has beenshown that rejection of outliers may alter the results ofABPM in individual patients sometimes significantlyaffecting average SBP levels [777879w] Editing pro-cedures can reduce mean systolic ABPM by 4 mmHg incomparison with unedited recordings thereby decreasingthe likelihood of diagnosing sustained hypertension Inone study the prevalence of sustained hypertension wasdecreased by 6ndash10 when several editing methods were
Copyright copy Lippincott Williams amp Wilkins Unaut1740 wwwjhypertensioncom
applied to raw 24-h data [79w] To make the results ofdifferent laboratories comparable common editingcriteria for ABPM should be used The problem is toestablish which of the methods proposed in the literatureprovides the most reliable data While awaiting moreobjective criteria to identify a universally acceptable edit-ing procedure we recommend that editing is not necess-ary for calculating average 24-h daytime and night-timevalues and that only physiologically impossible readingsshould be deleted from recordings However when thereare excessive artefacts in a tracing a repeat recordingrather than editing should be performed Some editingmight be required when focusing on analysis of BPvariability for the quantification of which the presenceof artefacts may introduce appreciable errors If editing isconsidered necessary a method proposed by Casadeiet al [80w] and modified by Winnicki et al [78] providescomparable performance to other proposed editing pro-cedures
There are no firm data on which to base recommen-dations for a satisfactory ABPM recording but the recom-mendation for having at least 70 of expectedmeasurements provides a basic working recommendationfor clinical practice This figure will be influenced by theperiod demarcated as daytime (awake) or night-time(asleep) periods and by the number of measurementsselected (usually 30-min but often 15 or 20-min intervals)In the previous ESH guideline on measurement it wasrecommended that there should be a minimum of 14measurements during the day and seven measurementsat night [1] Having considered what evidence is availableand the practical issues of performing repeat ABPM inpractice it seems reasonable to increase the minimum ofdaytime measurements to 20 while retaining a minimumseven measurements at night based on measurementsbeing performed every 30min and with fixed time periodsbeing used to define day (0900 to 2100 h) and night (0100 to0600 h) [1] (Box 5)
55 The arm for measurementABPM is best measured in the nondominant arm so as tointerfere as little as possible with daily activity unless there
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
has been documented evidence of a difference in BPbetween arms in which case the arm known to have thehigher BP values should be chosen [1] It is commonpractice for BP to be measured by a conventional techniqueat the same time as an ABPM monitor is being fitted and todetermine whether there is a discrepancy between thetechniques However BP variability is such that any suchcomparison has little validity and to determine a significantdifference it is necessary to perform simultaneousmeasurement according to a definitive protocol and thisis not feasible in practice [42] Because of these limitationsthe practice of performing a comparative measurement isnot recommended
56 Selecting the appropriate cuff and bladderThere is unequivocal evidence that either too narrow ortoo short a bladder (undercuffing) will cause overesti-mation of BP so-called lsquocuff hypertensionrsquo and there isgrowing evidence that too wide or too long a bladder(overcuffing) may cause underestimation of BP Under-cuffing has the effect in clinical practice of overdiagnos-ing hypertension and overcuffing leads to hypertensivepatients being diagnosed as normotensive Either even-tuality has serious implications for the epidemiology ofhypertension and for clinical practice [79] It is importanttherefore to select a cuff containing an inflatable bladderof correct length and width for the arm in which ABPM isto be measured All ABPM devices should provide cuffscontaining bladders for small medium and large-sizedarms as recommended in international guidelines[18081] However in many obese individuals the largebladder sizes cannot be used because the arm length istoo short to accommodate the bladder [81w] Anotherproblem is that the cylindrical shape of the commonlyused cuffs does not always wrap snugly around conical-shaped arms in obese and very muscular arms[8282w83w] Recently novel oscillometric homemonitors with cuff technology that allows a singlefixed-size cuff to be used on a wide range of arm circum-ferences have been developed [84wndash87w]
Another issue that needs consideration is the possibilitythat the discomfort caused by inflation of a large cuff inobese patients might cause elevation of BP This issuebecomes more important during ABPM because ofrepeated measurement especially during night-time sleepOscillometric devices for home use that measure BP duringcuff inflation may induce less discomfort because themeasurement is completed before maximal inflation[84w88w] However to date no study has specificallyaddressed this issue
Forearm BP measurement may have to be consideredwhen extreme obesity makes upper arm BP measurementimpossible BP measurements tend to be higher with fore-arm compared with upper arm measurement but meth-odological differences in these studies make it difficult toprovide recommendations for all populations [8389wndash94w] Despite the questionable accuracy of forearm BPmeasurement it may be the only acceptable option forABPM in individuals with very large upper arms providedthe patient is instructed to keep the forearm at heart levelduring measurement [94w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
No wrist devices have been validated for ABPM whereastechnology for continuous beat-to-beat monitoring ofambulatory BP in the finger has been developed usingthe volume-clamp method first described by Penaz [95w]A number of studies that compared this technology withintraarterial or noninvasive BP measurement showedunderestimation of BP particularly diastolic yet it remainsa practical alternative to intraarterial measurement for theevaluation of beat-to-beat BP changes and variability inresearch studies [8496wndash98w]
57 Conditions in which ambulatory bloodpressure monitoring may be difficult toperform
Obese patientsObesity is a well established major risk factor for hyperten-sion with higher prevalence in specific population groupssuch as patients with diabetes mellitus [99w] or OSA [100w]Despite the increasing prevalence of obesity worldwide[101w] and the close link between obesity and hyperten-sion scarce data are available on the application of ABPM inobese and extremely obese individuals ABPM is oftenrequired in these individuals and technical difficultiesshould not exclude them from such a valuable technology[79] The problem of miscuffing in obese pregnant womenmay result in diagnostic discrepancies [85]
Patients with atrial fibrillationBP measurement in patients with atrial fibrillation is lessprecise as this type of arrhythmia is accompanied byincreased beat-to-beat BP variability due to variations inventricular filling time stroke volume and contractilityInternational guidelines [181] recognize the relatively poorprecision of a single BP measurement and recommendrepeated readings in order to improve the accuracy ofestimates Theoretically ABPM should fulfill this stipulationas it provides a relatively high number of readings in a shortperiod of time Unfortunately published evidence regard-ing the role of ABPM in patients with arrhythmias andspecifically in patients with atrial fibrillation is scarce
Patients with atrial fibrillation have been usuallyexcluded from trials using ABPM as well as from validationprotocols of ABPM devices Four studies have addressedthe possible value of ABPM in patients with atrial fibrillation[48w102wndash104w] The evidence from these studiessuggests that ABPM may be useful in these patients pro-vided its limitations are taken into account The proportionof readings with errors the variability of BP and therepeatability coefficients do not appear to be different fromthose in patients in sinus rhythm DBP measured using anABPM monitor in patients with atrial fibrillation appears tobe relatively higher than that obtained with the traditionaloffice measurement or by the same ABPM procedure whenthe patient achieves sinus rhythm This finding is supportedby a review and meta-analysis of studies that validatedelectronic devices in patients with sustained atrial fibrilla-tion which showed consistent overestimation of DBP [52]In spite of this and although larger trials in patients on atrialfibrillation are recommended there is no reason to exclude
orized reproduction of this article is prohibitedwwwjhypertensioncom 1741
OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Guideline
the validity of the underlying assumptions by NICE has notbeen universally accepted [39]
Other potential benefits of ABPM that have not beenconsidered by NICE are the savings to be made in havingdrug treatment targeted to achieve 24-h BP control and thesubstantial savings to be made by the prevention of strokeand other cardiovascular consequences of hypertensionwith improved BP control Nor has NICE considered thepotential benefits of identifying the white-coat and maskedhypertension phenomena in treated individuals or of treat-ing nocturnal hypertension which is a major predictorof outcome
In a further extensive study of the cost of ABPM aMarkov model-based probabilistic cost-effectivenessanalysis concluded that ABPM is the most cost-effectivestrategy for the diagnosis of hypertension for men andwomen of all ages mainly by virtue of its potential toreduce misdiagnosis and to direct better targeted treatment[38]
As the cost of ABPM and hypertension managementdiffer greatly from country to country and is dependenton the method of healthcare delivery the cost-effectivenessof ABPM may need to be evaluated at a national level Forexample in Japan it has been estimated that the introduc-tion of ABPM for the management of hypertension hasreduced medical costs by about 948 trillion yen over 10years [40] (see Section 82)
34 Limitations of ambulatory blood pressuremonitoringThe technique of ABPM has many advantages over otheravailable techniques but it has its limitations whichinclude availability the provision of intermittent measure-ments during which the patient is sedentary rather thanlsquoambulatoryrsquo the possibility of inaccurate readings duringactivity and the inability to detect artefactual measure-ments the technique makes demands on the patient timeis needed to fit the device and it may cause discomfortparticularly during the night resulting in resistance fromsome patients to having repeat ABPM [11014] limitedreproducibility when the procedure is not standardized[41] and cost implications although the cost of devicesis reducing and costndashbenefit analyses have shown thatshort-term costs are justified by long-term savings (seeSection 33 Box 3)
Copyright copy Lippincott Williams amp Wilkins Unauth
Box 3 Limitations of ambulatory blood pressure monitoring
Application Limited availability May cause discomfort particularly at night Reluctance to use by some patients especially for repeat
measurement Cost implications (although the cost of devices is reducing
and possibly more cost-effective than office measurements)Function Imperfect reproducibility Provision of intermittent measurements in sedentary rather than
ambulatory conditions Possibility of inaccurate readings during activity Inability to detect genuine artefactual measurements
Journal of Hypertension
4 DEVICES AND SOFTWARE
41 Choosing an ambulatory blood pressuremonitoring device
411 Selecting an accurate deviceAn accurate device is fundamental to all BP measurementsif the device used to measure BP is inaccurate attention tomethodological detail is of little relevance It is acknow-ledged that the accuracy of BP-measuring devices shouldnot be based solely on claims from manufacturers whichcan at times be somewhat misleading Instead independ-ent validation using an established protocol with the resultspublished in peer-reviewed journals should be demanded[4222w] However manufacturers often ignore this recom-mendation and potential purchasers are generally unawareof this requirement assuming ndash not unreasonably ndash that ifa product reaches the market place it will measure BPaccurately The most popular validation protocol is theEuropean Society of Hypertension International Protocol(ESH-IP) and a recent review showed that from thepublication of the first version of the ESH-IP in 2002until June 2010 48 studies of device accuracy have beenreported using the British Hypertension Society (BHS)protocol 38 using the AAMI standard and 104 using theESH-IP 2010 [23w] Thus it seems that the ESH-IPsucceeded in expanding by three-fold to four-fold theuse of validation procedures worldwide compared withthe period before its publication [23w] A criticism bymembers of the AAMI Committee that the reduction inthe number of patients might compromise the validity ofthe protocol [24w] has been shown to be statisticallyunfounded [25w] The availability of the ESH-IP in anon-line version will further facilitate the validation of ABPMdevices [26w]
Since the ESH-IP was first published there has been animprovement in the performance of the oscillometric devi-ces for BP measurement [23w] but protocol violations andmisreporting have been particularly common suggestingthat there is a need for stricter standardization for conduct-ing and reporting a validation study [27w] The revisedversion of the ESH-IP protocol applied tighter validationcriteria for the pass level [42] and the application of thesemore stringent criteria is expected to double the validationfailure rate allowing more accurate devices to enter themarket [23w]
The AAMI protocol requires additional testing for ABPMdevices in 85 patients in the supine seated and standingpositions and stipulates that three devices should beassessed in ambulatory conditions all of which would bevery difficult and costly to perform [4328w] The BHSprotocol which is rarely used now also requires an in-use (field) assessment of ambulatory monitors [44] TheInternational Organization for Standardization (ISO) pro-tocol also requires additional clinical validation in 35patients in standardized conditions of physical activity(after exercise on a bicycle ergometer or treadmill toincrease heart rate by 10ndash20) [45]
It has recently been suggested that the validation ofautomated BP-measuring devices should be complementedby an overall quality check The PANET International
orized reproduction of this article is prohibitedwwwjhypertensioncom 1735
OrsquoBrien et al
Quality Certification Protocol denotes additional criteria ofquality for BP-measuring devices that fulfilled basic vali-dation criteria published in full in peer-reviewed medicaljournals On the basis of this evaluation a quality certifi-cation is released to the manufacturer and published onwwwpressionearteriosanet and wwwdableducationalorg[46]
The majority of devices for ABPM use oscillometry tomeasure BP but some devices also measure BP by micro-phonic detection of the Korotkoff sounds and such devicesneed to have both measurement methods validated accord-ing to accepted validation protocols [29w]
412 Validation requirements for ambulatoryblood pressure monitoring devices in specialpopulationsSeparate validation is required in specific populations suchas children and adolescents pregnant women and theelderly and in certain diseases such as obesity and arrhyth-mias [30w] Patients with arrhythmias children the elderlyand pregnant women present special challenges for vali-dation of oscillometric ABPM devices However althoughABPM devices are used frequently in these patient popu-lations specific validation studies have often not beenperformed this limitation applies also to other methodsof BP measurement such as home and office measure-ments The validation status of ABPM devices in differentpopulations can be checked on dedicated websites (egwwwpressionearteriosanet or wwwdableducationalorg)Although specific validation studies of ABPM devices inthese special populations are desirable in the future devi-ces that have been validated in the general hypertensivepopulation can be used so that high-risk patients are notdenied the benefit of ABPM
ChildrenFour ABPM devices have been validated in children andadolescents [31wndash34w] A number of factors that includeconsent adherence to the validation protocol whichphase to choose for defining DBP size of cuff and leveland range of BP make validation studies in children muchmore difficult than in adults [4735w]
PregnancyA number of ABPM devices have been validated innormotensive and hypertensive women in pregnancyand preeclampsia and although more devices are beingrecommended for use in clinical practice there are severaldevices that are not accurate in pregnancy [484936wndash41w] In pregnancy auscultation of DBP has been contro-versial leading to differences of opinion between mufflingand disappearance of sounds as the criterion for DBP [49]There is now general agreement that disappearance ofsounds is the best measure of DBP [50]
The elderlyValidation data in elderly patients are available only for theSpaceLabs 90207 [42w] It is important to define clearly theage group in which the device is being assessed Individualsover the age of 65 years will also have a higher prevalenceof diseases and conditions that can affect arterial stiffness
Copyright copy Lippincott Williams amp Wilkins Unaut1736 wwwjhypertensioncom
and therefore influence the outcome of validation studiesThe elderly have an increased prevalence of arrhythmiasincluding atrial fibrillation bradycardia and ventriculartachyarrhythmias and are more likely to have inter-armdifferences in pressures due to upper arm arterial diseasewhich would make them unsuitable for validation studies[51]
Patients with arrhythmiasThere are no formal validation studies using establishedprotocols for ABPM devices in this special population Inpatients with arrhythmias it is difficult to standardize theheart rates during validation Good recordings can beobtained with ABPM in most patients although there is atendency for electronic devices to overestimate DBP inpatients with atrial fibrillation [52]
Obese patientsNo validation studies of ABPM monitors have been per-formed in the obese population Obesity has an adverseimpact on vascular stiffness influencing thereby theaccuracy of the oscillometric technique and these patientshave large arms which may complicate recruitment forvalidation studies particularly when a specified range ofcuffs has to be assessed [53]
Patients with renal diseaseOnly one ABPM device has been validated for patients withrenal disease [43w] Validating devices in patients with end-stage renal disease (ESRD) and chronic kidney disease(CKD) presents a number of problems [43w44w] thatinclude finding an available upper extremity the effectof arterial stiffness on the oscillometric methodologyespecially for DBP [54] and the demanding schedule ofdialysis that makes recruitment of patients difficult
413 Additional features for ambulatory bloodpressure monitorsAll ABPM monitors measure BP and pulse rate and mostprovide measurements not only for SBP and DBP but alsofor mean BP and pulse pressure Over the past decadeABPM devices have been developed to measure or calcu-late intermittently or continuously other parameters suchas the ECG pulse wave velocity and central BP Further-more accessories such as position sensors and accelerom-eters for physical activity analysis have been incorporatedto provide a more precise pathophysiological profileMajor limitations of these innovative devices are theirrelatively high price and the need to validate the associatedfunctions according to adequate protocols and to provideevidence for their clinical usefulness Until these require-ments are fulfilled the use of such ABPM devices shouldbe restricted to research laboratories and specializedcenters
Ambulatory blood pressure monitoring and homeblood pressureDevices which can be used either for 24-h ABPM or in a7-day mode to collect multiday BP data are being devel-oped and one has been validated [45w46w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Ambulatory blood pressure monitoring and ECGDevices have been developed allowing 24-h ABPM withcontinuous 24-h ECG in a single procedure Besides theusual well established indications for each of these pro-cedures the interaction between these two signals providescomplementary interrelated information in one procedureThe use of the real heart rate to determine the deflation ratecan provide more precise BP measurement and additionalextra BP measurements can be triggered by abnormal ECGactivities such as arrhythmias and ST segment abnormal-ities Limitations are the relatively high cost of monitors andsoftware the complexity compared to the simple ABPMprocedure and the difficulties in performing validationstudies for the combined functions [47w48w] Thesedisadvantages are offset to some extent by being ableto perform the two procedures simultaneously in olderpatients in whom arterial hypertension and paroxysmalatrial fibrillation often coexist Another development hasbeen the use of spectral analysis of heart rate to provide ameans for improving screening for obstructive sleep apnea(OSA) [49w50w]
Ambulatory blood pressure monitoring and arterialfunctionDevices are being developed that measure arterial stiffnessso as to provide interesting information on 24-h ABPM andon arterial function [51wndash55w]
Ambulatory blood pressure monitoring and positionsensingPosition sensors have been developed to determinewhether the patient is standing or lying during ABPMrecording and this facility allows an estimation of the sleepperiod [5556w]
Ambulatory blood pressure monitoring and activitysensingActivity sensors and accelerometers have been developedfor monitoring patient activity during ABPM so as to providean indirect measure of activity and rest with the formerbeing an estimate of the awake period and the latter ofsleep Some of these sensors are incorporated in the devicewhereas others are complementary accessories placedeither at wrist thigh or chest level [57w]
Ambulatory blood pressure monitoring and centralblood pressureSeveral 24-h oscillometric ABPM monitors use specificalgorithms and software for pulse wave analysis by record-ing 24-h ABPM data as well as calculating central BP [5651wndash53w58wndash61w] Further studies are needed howeverto demonstrate the validity and clinical usefulness of thesedevices which at present should not be used for makingclinical decisions
42 Software for ambulatory blood pressuremonitoring data analysisRecommendations on procedures for ABPM use tend toconcentrate on the accuracy of the devicersquos hardware withlittle attention being paid to software presentation and
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
analysis of ABPM data As a consequence the practisingphysician who has to interpret the considerable amount ofdata provided by ABPM is often faced with a bewilderingreport with reams of paper containing plots histogramsand data analysis that have little relevance for clinicalpractice It is important for ABPM software programs tobe suitable for the intended use of the device For examplein a busy general practice perhaps only basic data givingaverage 24-h daytime and night-time values and a visualplot are all that will be required whereas for researchpurposes statistical detail on the windows of the 24-hprofile and other indices may be required [10] A recentstudy has stressed that whereas monitors for ABPM aresubject to extensive validation protocols there is no inter-national guideline on the software processing of the col-lected raw data to prevent error being introduced by thesoftware permutations An example of software-inducederror was demonstrated for the SpaceLabs Report Manage-ment System 92506 which showed errors in 92 of reportsamounting to a numerical difference between printout andon-screen hourly averages ranging from 37 to 18mmHgfor SBP and from 16 to 10mmHg for DBP [62w] Anadditional problem can arise from the calculation of 24-haverage BP values that are not weighted for the differentnumber of hourly measurements during daytime and night-time weighted hourly BP values have been shown to bemore reliable than calculations based on the average of allindividual readings [57]
The use of ABPM in clinical practice can be facilitated bystandardizing the graphic presentation of ABPM datamuch as is the case for ECG recordings so that the pres-entation of data is independent of the type of ABPMmonitor used and the user is not required to becomefamiliar with a variety of programs Standardization alsofacilitates the interchange of ABPM recordings betweendatabases such as a hospital and primary care practiceMoreover if ABPM software programs provide a printedreport of the standardized ABPM data with a validatedinterpretative report [58] (signed by the physician in chargeof the service whenever legally required) doctors andnurses unfamiliar with the technique are assisted inlearning the variety of patterns generated by ABPM andbecause an individualized physician report is not a require-ment in most cases the cost of ABPM is reduced [110](Box 4)
421 Software requirementsThe following facilities are recommended for ABPM soft-ware in clinical practice [1910]
Clinical reportThe following information should be available in a one-page report
or
1
ize
Standardized plot format with each BP measurementon the vertical axis and time of day on horizontal axiswith different windows of the 24-h period identifiedand normal bands clearly demarcated The sleep timeinterval used to calculate asleep BP should be indi-cated (shaded) and preferably based on the indivi-dualsrsquo sleep time report (diary cards) In the plot the
d reproduction of this article is prohibitedwwwjhypertensioncom 1737
Cop
Box 4 Software requirements
Clinical report Ambulatory blood pressure measurement analysis and report should be standardized independent of the monitor type Standardized plot of all the blood pressure measurements with daytime and night-time windows and normal blood pressure bands demarcated Average SBP DBP and heart rate to be displayed Nocturnal blood pressure decline () for SBP and DBP Summary statistics for time-weighted average SBP and DBP and heart rate for the 24-h period daytime and night-time with standard deviations and number
of valid blood pressure readings Facility for showing error readings if requiredOptional requirements Automated software generated interpretative report indicating the normal or abnormal patterns and whether the requirements for a valid recording are
fulfilled Facility to plot heart rate and mean blood pressure Trend report for comparing repeated ambulatory blood pressure measurement recordings Ability to centrally host dataResearch report Data storage and raw data export capability for research analysis and audit Parameters include variability measures (such as 24-h SD 24-h weighted SD average real variability coefficient of variation) area under the curve
calculations blood pressure load parameters ratendashpressure product trough and peak levels smoothness index (the last two parameters requiring ABPMdata before and during treatment to be available) cusum-derived statistics and ambulatory arterial stiffness index
OrsquoBrien et al
1738
upper value of the Y-axis should not be fixed butadjustable to the highest BP value recorded in orderto maximize the graphic presentation of BP variationsover the 24-h period A plot of SBP and DBP through-out the 24-h period with a facility for plotting heartrate and mean BP so as to provide evidence ofcircadian behavior should be provided
2
Summary statistics for time-weighted SBP and DBPand heart rate in the windows of the 24-h period andseparately for the awake and asleep subperiods withthe respective standard deviations and the number ofvalid BP readings included in the analysis and afacility for indicating the time of going to bed andawakening
3
Medication details
4
Facility for showing error readings if required
Interpretative reportTo remove the variance associated with the ABPMinterpretation by human observers and to simplify theevaluation of results in routine clinical practice for thoseunfamiliar with the technique there should be an auto-mated software-generated interpretative report indicatingnormal or abnormal BP patterns and whether there aresufficient measurements for the recording to be valid [10]The interpretative report should be validated by testing thecomputer-generated report against reports from experts[5859]
Trend reportThe provision of a trend report allows ABPMs to be com-pared over time to demonstrate the response to changes inmanagement If ABPM is to be used to achieve better BPcontrol it is important for prescribing doctors (and patients)to be able to see whether medication is achieving controlthroughout the entire 24-h period
Research reportThe system should be capable of storing data for detailedanalysis for research and audit according to evidence-based
yright copy Lippincott Williams amp Wilkins Unautwwwjhypertensioncom
definitions for time-weighted arithmetic and mean valuesfor measures of BP level In view of evidence that short-term BP variability may give information over and abovemean BP levels and that reduction in 24-h BP variabilitymay be beneficial [63w] time-weighted and other measuresof short-term BP variability are helpful for on-goingresearch in this area Informative indices associated withoutcome such as area under the curve calculations BP loadparameters trough and peak levels the smoothness index(the last two parameters requiring ABPM data before andduring treatment to be available) cusum-derived statisticsand most recently the ambulatory arterial stiffness index(AASI) should also be provided [6061] The system shouldbe capable of storing and exporting raw data for researchpurposes and additional analyses [606163w]
422 Indices derived from ambulatory bloodpressure monitoring recordingsAverage BP values (over 24 h daytime and night-time) areundoubtedly the most important parameters obtained fromABPM recordings based on outcome data However alarge number of additional indices with promising clinicalevidence may be derived from ABPM recordings and someof them are occasionally included in the reports generatedby ABPM systems
Blood pressure loadThis index is defined as the percentage of readings in agiven period (24-h day or night) which exceed a prede-fined threshold value typically set at the proposed nor-malcy level for average BP values of that period The aim ofBP load is to quantify the number of readings with elevatedBP and mathematically it depends on both average BPlevels and distribution of BP readings [62] Although intheory clinically appealing and thus commonly incorpor-ated in the ABPM software this index has a number oflimitations Firstly there is no evidence that the thresholdsdefined for average BP values have any prognostic meaningwhen applied to single BP measurements Secondly whencomparing recordings with similar average BP levels differ-ences in BP load can be largely explained by differences in
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
BP variability making this index largely redundant ThirdlyBP load does not contain the prognostically importantinformation on how much the threshold level has beenexceeded To overcome the latter limitation it has beenproposed to modify the classic BP load definition bycalculating the total area under the timendashpressure curvewhen BP exceeds the threshold [63] Finally although somestudies support the usefulness of BP load in predictingorgan damage [6464w] it has never been convincinglydemonstrated that it provides any additional and clinicallyrelevant information independently of what is obtained byfocusing on average BP values The use of BP load inchildren has also been examined but it has not been foundhelpful in diagnosis [65w]
Ratendashpressure productThis index which is defined as heart rate multiplied by SBPis used as an index of myocardial work during exercise andit has prognostic relevance [66w] The availability of bothheart rate and BP data in ABPM makes it possible to obtainthe index readily especially if ABPM is accompanied byactigraphy [65] Although potentially promising the clinicalapplication of this index requires further research
rsquoVascularrsquo indicesSeveral ABPM-based indices have been proposed to pro-vide information on vascular wall properties Their ration-ale is based on the observation that the stiffness of thearterial wall increases when it is being stretched in patientswith impaired arterial wall elasticity SBP increases moresteeply than DBP whereas in a patient with elastic arteriesSBP and DBP increase in parallel The AASI which iscalculated as 1 ndash slope of regression of DBP on SBP isreadily obtainable from ABPM [6066]
AASI appears to have a direct relationship to carotidndashfemoral pulse wave velocity (a validated index of largearteriesrsquo stiffness) and an independent relationship withcardiovascular outcomes [606167wndash70w] Howeverthe ability of AASI to reflect arterial stiffness has beenchallenged because of its dependence on nocturnal BP falland the fact that it implies the use of asymmetric regressionpossibly affecting the precision of slope estimation[67ndash6971w72w] Modifications to AASI have been pro-posed but further data are awaited as to their ability tosurpass AASI in predicting outcome [73w74w]
The QndashKd interval which measures the time intervalbetween the onset of the QRS on the electrocardiogram (Q)and the last Korotkoff sound (K) corresponding to thediastolic pressure (d) has also been shown to have prog-nostic value [70]
Indices for indicating the pattern of treatment-induced changes in 24-h blood pressure loweringTwo principal indices are available for assessing thesmoothness and consistency of antihypertensive treatmenteffect over 24 h with ABPM The trough-to-peak ratio is theratio between BP reduction achieved by treatment at theend of dosing interval (trough which for drugs adminis-tered once daily means 24 h after the last dose intake) andpeak BP reduction usually achieved a few hours after dose
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
intake [7172] The trough-to-peak ratio is characterized by ahigh degree of variability in individual patients and istherefore not suitable for application to clinical practice[73] The smoothness index is calculated as the ratiobetween the average of hourly BP reductions over 24 hand the standard deviation (SD) of such an average valuethus integrating information on the size of BP reduction bytreatment and on its homogeneity throughout the 24-hperiod [7173] The smoothness index is highest for potentdrugs or drug combinations which also provide the mosthomogeneous BP reduction It is more reproducible thanthe troughpeak ratio [7173] and predicts treatment-induced changes in indices of organ damage includingleft ventricular mass and carotid arterial wall thickness[75w] A recent meta-analysis has provided informationon clinical determinants of the smoothness index suchas age ethnicity sex and smoking [74] The relevance ofthese indices in predicting the impact of treatment onoutcome and the reference values remain to be assessed
5 PROCEDURE
51 Training requirementsThe technique of ABPM is a specialized one and should beapproached with the care reserved for any such procedureAn understanding of the principles of traditional BPmeasurement cuff fitting monitor function and analysisand interpretation of ABPM data is required In practice anurse with an interest and experience in hypertension canmaster the use of ABPM devices after a relatively brieftraining However the interpretation of ABPM profilesrequires experience in the technique which is best pro-vided by the doctor in charge of an ABPM service [19]
52 Fitting an ambulatory blood pressuremonitorTime needs to be given to fitting the monitor and preparingthe patient for the monitoring period if good results are tobe obtained [19] The key to successful ABPM is educatingthe patient on the process of monitoring and the instruc-tions should be explained and printed on a diary card Inclinical practice measurements are preferably performedon a routine working day Although ABPM is best notperformed while patients are admitted to hospital becausehospitalization leads to underestimation of BP and over-diagnosis of nondippers [10] there are occasions such asthe evaluation of severely resistant hypertension andassessment of patients following a stroke when ABPM inhospital may be indicated
The frequency of measurement during the 24-h period isgenerally not more than every 15 min (which could inter-fere with normal activity) nor less than every 30min (whichcould give an inadequate number of measurements) Morefrequent measurements at night may disturb sleep andsleep disturbance has been shown to reduce the prognosticvalue of ABPM [75] To improve reproducibility repetitionof ABPM should be performed on like days for example onroutine working or recreational days A diary card can beused to record symptoms and events that may influenceABPM measurements
orized reproduction of this article is prohibitedwwwjhypertensioncom 1739
OrsquoBrien et al
53 Explanation to patientThe first step is adequate explanation of the procedure in anattempt to allay anxiety especially in nervous patientsPatients having ABPM for the first time should be told thatthere is minor discomfort caused by inflation of the cuff It isimportant to emphasize to the patient to follow hisherusual daily activities but as much as possible to remain stillwith the arm relaxed and not extended or contracted atheart level during each BP measurement [19] It can behelpful to have patients record periods of stress the time ofmeals the time of a siesta the time of going to bed andrising the quality of sleep and the time and type ofdrug ingestion
Box 5 Evaluation of ambulatory blood pressure monitoring data
Definition of daytime and night-time Daytime and night-time intervals are best defined using sleeping times
reported by individual usersrsquo diary cards (awake and asleep periods) Fixed narrow time intervals can be applied by discarding transition
periods between daytime and night-time (eg daytime defined as0900ndash2100 h and night-time 0100ndash0600 h)
Editing requirements Editing is not necessary for calculating average 24-h daytime and
night-time values The ambulatory blood pressure monitoring should be repeated if thefollowing criteria are not met
24-h recording with at least 70 of expected measurements20 valid awake (0900 to 2100 h)7 valid asleep (0100 to 0600 h)Blood pressure measurements at 30-min intervalsFor research purposes at least two valid daytime and one valid
night-time measurement per hour
54 Identification of daytime and night-timeperiods and editing ambulatory blood pressuremonitoring dataOne simple and popular method for identifying daytimeand night-time subperiods is to assess the time of awaken-ing and sleeping from diary card entries Another method isto use a fixed-narrow time interval approach in which forexample the retiring (2101 to 0059 h) and rising (0601 to0859 h) periods (which are subject to considerable vari-ation) are eliminated with the daytime period being from0900 to 2100 h and night-time from 0100 to 0600 h in thisway the variations in the time spent in bed that may existbetween the young and the old and in different culturesare to some extent eliminated from the analysis [176w]This method has the disadvantage of eliminating infor-mation on the white-coat window on the early phase ofnight sleep when dipping can be most evident and onthe early morning surge of BP which may be associatedwith cardiovascular events However these windows canbe analyzed separately for research or if considered import-ant in practice In countries where a daytime siesta ispopular a record of sleeping times both during day andnight is important and ABPM software should be able toadjust for this otherwise there may be underestimation ofthe nocturnal BP dip and overdiagnosis of nondippers[77w]
Many statistical techniques exist for editing ABPMrecords and no one method is ideal [176w] The detec-tion of artefactual readings and the handling of outliervalues (which may or may not be erroneous) have indeedbeen the subject of debate [76w] There are a number ofways of separately analyzing BPs recorded during the dayand night [7678w] Several automatic procedures havebeen proposed to reject outlying measurements based ona univariate multivariate or temporal approach Morecomplex procedures requiring the intervention of theobserver have been proposed but they are time consum-ing and not suitable for clinical practice [77] It has beenshown that rejection of outliers may alter the results ofABPM in individual patients sometimes significantlyaffecting average SBP levels [777879w] Editing pro-cedures can reduce mean systolic ABPM by 4 mmHg incomparison with unedited recordings thereby decreasingthe likelihood of diagnosing sustained hypertension Inone study the prevalence of sustained hypertension wasdecreased by 6ndash10 when several editing methods were
Copyright copy Lippincott Williams amp Wilkins Unaut1740 wwwjhypertensioncom
applied to raw 24-h data [79w] To make the results ofdifferent laboratories comparable common editingcriteria for ABPM should be used The problem is toestablish which of the methods proposed in the literatureprovides the most reliable data While awaiting moreobjective criteria to identify a universally acceptable edit-ing procedure we recommend that editing is not necess-ary for calculating average 24-h daytime and night-timevalues and that only physiologically impossible readingsshould be deleted from recordings However when thereare excessive artefacts in a tracing a repeat recordingrather than editing should be performed Some editingmight be required when focusing on analysis of BPvariability for the quantification of which the presenceof artefacts may introduce appreciable errors If editing isconsidered necessary a method proposed by Casadeiet al [80w] and modified by Winnicki et al [78] providescomparable performance to other proposed editing pro-cedures
There are no firm data on which to base recommen-dations for a satisfactory ABPM recording but the recom-mendation for having at least 70 of expectedmeasurements provides a basic working recommendationfor clinical practice This figure will be influenced by theperiod demarcated as daytime (awake) or night-time(asleep) periods and by the number of measurementsselected (usually 30-min but often 15 or 20-min intervals)In the previous ESH guideline on measurement it wasrecommended that there should be a minimum of 14measurements during the day and seven measurementsat night [1] Having considered what evidence is availableand the practical issues of performing repeat ABPM inpractice it seems reasonable to increase the minimum ofdaytime measurements to 20 while retaining a minimumseven measurements at night based on measurementsbeing performed every 30min and with fixed time periodsbeing used to define day (0900 to 2100 h) and night (0100 to0600 h) [1] (Box 5)
55 The arm for measurementABPM is best measured in the nondominant arm so as tointerfere as little as possible with daily activity unless there
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
has been documented evidence of a difference in BPbetween arms in which case the arm known to have thehigher BP values should be chosen [1] It is commonpractice for BP to be measured by a conventional techniqueat the same time as an ABPM monitor is being fitted and todetermine whether there is a discrepancy between thetechniques However BP variability is such that any suchcomparison has little validity and to determine a significantdifference it is necessary to perform simultaneousmeasurement according to a definitive protocol and thisis not feasible in practice [42] Because of these limitationsthe practice of performing a comparative measurement isnot recommended
56 Selecting the appropriate cuff and bladderThere is unequivocal evidence that either too narrow ortoo short a bladder (undercuffing) will cause overesti-mation of BP so-called lsquocuff hypertensionrsquo and there isgrowing evidence that too wide or too long a bladder(overcuffing) may cause underestimation of BP Under-cuffing has the effect in clinical practice of overdiagnos-ing hypertension and overcuffing leads to hypertensivepatients being diagnosed as normotensive Either even-tuality has serious implications for the epidemiology ofhypertension and for clinical practice [79] It is importanttherefore to select a cuff containing an inflatable bladderof correct length and width for the arm in which ABPM isto be measured All ABPM devices should provide cuffscontaining bladders for small medium and large-sizedarms as recommended in international guidelines[18081] However in many obese individuals the largebladder sizes cannot be used because the arm length istoo short to accommodate the bladder [81w] Anotherproblem is that the cylindrical shape of the commonlyused cuffs does not always wrap snugly around conical-shaped arms in obese and very muscular arms[8282w83w] Recently novel oscillometric homemonitors with cuff technology that allows a singlefixed-size cuff to be used on a wide range of arm circum-ferences have been developed [84wndash87w]
Another issue that needs consideration is the possibilitythat the discomfort caused by inflation of a large cuff inobese patients might cause elevation of BP This issuebecomes more important during ABPM because ofrepeated measurement especially during night-time sleepOscillometric devices for home use that measure BP duringcuff inflation may induce less discomfort because themeasurement is completed before maximal inflation[84w88w] However to date no study has specificallyaddressed this issue
Forearm BP measurement may have to be consideredwhen extreme obesity makes upper arm BP measurementimpossible BP measurements tend to be higher with fore-arm compared with upper arm measurement but meth-odological differences in these studies make it difficult toprovide recommendations for all populations [8389wndash94w] Despite the questionable accuracy of forearm BPmeasurement it may be the only acceptable option forABPM in individuals with very large upper arms providedthe patient is instructed to keep the forearm at heart levelduring measurement [94w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
No wrist devices have been validated for ABPM whereastechnology for continuous beat-to-beat monitoring ofambulatory BP in the finger has been developed usingthe volume-clamp method first described by Penaz [95w]A number of studies that compared this technology withintraarterial or noninvasive BP measurement showedunderestimation of BP particularly diastolic yet it remainsa practical alternative to intraarterial measurement for theevaluation of beat-to-beat BP changes and variability inresearch studies [8496wndash98w]
57 Conditions in which ambulatory bloodpressure monitoring may be difficult toperform
Obese patientsObesity is a well established major risk factor for hyperten-sion with higher prevalence in specific population groupssuch as patients with diabetes mellitus [99w] or OSA [100w]Despite the increasing prevalence of obesity worldwide[101w] and the close link between obesity and hyperten-sion scarce data are available on the application of ABPM inobese and extremely obese individuals ABPM is oftenrequired in these individuals and technical difficultiesshould not exclude them from such a valuable technology[79] The problem of miscuffing in obese pregnant womenmay result in diagnostic discrepancies [85]
Patients with atrial fibrillationBP measurement in patients with atrial fibrillation is lessprecise as this type of arrhythmia is accompanied byincreased beat-to-beat BP variability due to variations inventricular filling time stroke volume and contractilityInternational guidelines [181] recognize the relatively poorprecision of a single BP measurement and recommendrepeated readings in order to improve the accuracy ofestimates Theoretically ABPM should fulfill this stipulationas it provides a relatively high number of readings in a shortperiod of time Unfortunately published evidence regard-ing the role of ABPM in patients with arrhythmias andspecifically in patients with atrial fibrillation is scarce
Patients with atrial fibrillation have been usuallyexcluded from trials using ABPM as well as from validationprotocols of ABPM devices Four studies have addressedthe possible value of ABPM in patients with atrial fibrillation[48w102wndash104w] The evidence from these studiessuggests that ABPM may be useful in these patients pro-vided its limitations are taken into account The proportionof readings with errors the variability of BP and therepeatability coefficients do not appear to be different fromthose in patients in sinus rhythm DBP measured using anABPM monitor in patients with atrial fibrillation appears tobe relatively higher than that obtained with the traditionaloffice measurement or by the same ABPM procedure whenthe patient achieves sinus rhythm This finding is supportedby a review and meta-analysis of studies that validatedelectronic devices in patients with sustained atrial fibrilla-tion which showed consistent overestimation of DBP [52]In spite of this and although larger trials in patients on atrialfibrillation are recommended there is no reason to exclude
orized reproduction of this article is prohibitedwwwjhypertensioncom 1741
OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
OrsquoBrien et al
Quality Certification Protocol denotes additional criteria ofquality for BP-measuring devices that fulfilled basic vali-dation criteria published in full in peer-reviewed medicaljournals On the basis of this evaluation a quality certifi-cation is released to the manufacturer and published onwwwpressionearteriosanet and wwwdableducationalorg[46]
The majority of devices for ABPM use oscillometry tomeasure BP but some devices also measure BP by micro-phonic detection of the Korotkoff sounds and such devicesneed to have both measurement methods validated accord-ing to accepted validation protocols [29w]
412 Validation requirements for ambulatoryblood pressure monitoring devices in specialpopulationsSeparate validation is required in specific populations suchas children and adolescents pregnant women and theelderly and in certain diseases such as obesity and arrhyth-mias [30w] Patients with arrhythmias children the elderlyand pregnant women present special challenges for vali-dation of oscillometric ABPM devices However althoughABPM devices are used frequently in these patient popu-lations specific validation studies have often not beenperformed this limitation applies also to other methodsof BP measurement such as home and office measure-ments The validation status of ABPM devices in differentpopulations can be checked on dedicated websites (egwwwpressionearteriosanet or wwwdableducationalorg)Although specific validation studies of ABPM devices inthese special populations are desirable in the future devi-ces that have been validated in the general hypertensivepopulation can be used so that high-risk patients are notdenied the benefit of ABPM
ChildrenFour ABPM devices have been validated in children andadolescents [31wndash34w] A number of factors that includeconsent adherence to the validation protocol whichphase to choose for defining DBP size of cuff and leveland range of BP make validation studies in children muchmore difficult than in adults [4735w]
PregnancyA number of ABPM devices have been validated innormotensive and hypertensive women in pregnancyand preeclampsia and although more devices are beingrecommended for use in clinical practice there are severaldevices that are not accurate in pregnancy [484936wndash41w] In pregnancy auscultation of DBP has been contro-versial leading to differences of opinion between mufflingand disappearance of sounds as the criterion for DBP [49]There is now general agreement that disappearance ofsounds is the best measure of DBP [50]
The elderlyValidation data in elderly patients are available only for theSpaceLabs 90207 [42w] It is important to define clearly theage group in which the device is being assessed Individualsover the age of 65 years will also have a higher prevalenceof diseases and conditions that can affect arterial stiffness
Copyright copy Lippincott Williams amp Wilkins Unaut1736 wwwjhypertensioncom
and therefore influence the outcome of validation studiesThe elderly have an increased prevalence of arrhythmiasincluding atrial fibrillation bradycardia and ventriculartachyarrhythmias and are more likely to have inter-armdifferences in pressures due to upper arm arterial diseasewhich would make them unsuitable for validation studies[51]
Patients with arrhythmiasThere are no formal validation studies using establishedprotocols for ABPM devices in this special population Inpatients with arrhythmias it is difficult to standardize theheart rates during validation Good recordings can beobtained with ABPM in most patients although there is atendency for electronic devices to overestimate DBP inpatients with atrial fibrillation [52]
Obese patientsNo validation studies of ABPM monitors have been per-formed in the obese population Obesity has an adverseimpact on vascular stiffness influencing thereby theaccuracy of the oscillometric technique and these patientshave large arms which may complicate recruitment forvalidation studies particularly when a specified range ofcuffs has to be assessed [53]
Patients with renal diseaseOnly one ABPM device has been validated for patients withrenal disease [43w] Validating devices in patients with end-stage renal disease (ESRD) and chronic kidney disease(CKD) presents a number of problems [43w44w] thatinclude finding an available upper extremity the effectof arterial stiffness on the oscillometric methodologyespecially for DBP [54] and the demanding schedule ofdialysis that makes recruitment of patients difficult
413 Additional features for ambulatory bloodpressure monitorsAll ABPM monitors measure BP and pulse rate and mostprovide measurements not only for SBP and DBP but alsofor mean BP and pulse pressure Over the past decadeABPM devices have been developed to measure or calcu-late intermittently or continuously other parameters suchas the ECG pulse wave velocity and central BP Further-more accessories such as position sensors and accelerom-eters for physical activity analysis have been incorporatedto provide a more precise pathophysiological profileMajor limitations of these innovative devices are theirrelatively high price and the need to validate the associatedfunctions according to adequate protocols and to provideevidence for their clinical usefulness Until these require-ments are fulfilled the use of such ABPM devices shouldbe restricted to research laboratories and specializedcenters
Ambulatory blood pressure monitoring and homeblood pressureDevices which can be used either for 24-h ABPM or in a7-day mode to collect multiday BP data are being devel-oped and one has been validated [45w46w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Ambulatory blood pressure monitoring and ECGDevices have been developed allowing 24-h ABPM withcontinuous 24-h ECG in a single procedure Besides theusual well established indications for each of these pro-cedures the interaction between these two signals providescomplementary interrelated information in one procedureThe use of the real heart rate to determine the deflation ratecan provide more precise BP measurement and additionalextra BP measurements can be triggered by abnormal ECGactivities such as arrhythmias and ST segment abnormal-ities Limitations are the relatively high cost of monitors andsoftware the complexity compared to the simple ABPMprocedure and the difficulties in performing validationstudies for the combined functions [47w48w] Thesedisadvantages are offset to some extent by being ableto perform the two procedures simultaneously in olderpatients in whom arterial hypertension and paroxysmalatrial fibrillation often coexist Another development hasbeen the use of spectral analysis of heart rate to provide ameans for improving screening for obstructive sleep apnea(OSA) [49w50w]
Ambulatory blood pressure monitoring and arterialfunctionDevices are being developed that measure arterial stiffnessso as to provide interesting information on 24-h ABPM andon arterial function [51wndash55w]
Ambulatory blood pressure monitoring and positionsensingPosition sensors have been developed to determinewhether the patient is standing or lying during ABPMrecording and this facility allows an estimation of the sleepperiod [5556w]
Ambulatory blood pressure monitoring and activitysensingActivity sensors and accelerometers have been developedfor monitoring patient activity during ABPM so as to providean indirect measure of activity and rest with the formerbeing an estimate of the awake period and the latter ofsleep Some of these sensors are incorporated in the devicewhereas others are complementary accessories placedeither at wrist thigh or chest level [57w]
Ambulatory blood pressure monitoring and centralblood pressureSeveral 24-h oscillometric ABPM monitors use specificalgorithms and software for pulse wave analysis by record-ing 24-h ABPM data as well as calculating central BP [5651wndash53w58wndash61w] Further studies are needed howeverto demonstrate the validity and clinical usefulness of thesedevices which at present should not be used for makingclinical decisions
42 Software for ambulatory blood pressuremonitoring data analysisRecommendations on procedures for ABPM use tend toconcentrate on the accuracy of the devicersquos hardware withlittle attention being paid to software presentation and
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
analysis of ABPM data As a consequence the practisingphysician who has to interpret the considerable amount ofdata provided by ABPM is often faced with a bewilderingreport with reams of paper containing plots histogramsand data analysis that have little relevance for clinicalpractice It is important for ABPM software programs tobe suitable for the intended use of the device For examplein a busy general practice perhaps only basic data givingaverage 24-h daytime and night-time values and a visualplot are all that will be required whereas for researchpurposes statistical detail on the windows of the 24-hprofile and other indices may be required [10] A recentstudy has stressed that whereas monitors for ABPM aresubject to extensive validation protocols there is no inter-national guideline on the software processing of the col-lected raw data to prevent error being introduced by thesoftware permutations An example of software-inducederror was demonstrated for the SpaceLabs Report Manage-ment System 92506 which showed errors in 92 of reportsamounting to a numerical difference between printout andon-screen hourly averages ranging from 37 to 18mmHgfor SBP and from 16 to 10mmHg for DBP [62w] Anadditional problem can arise from the calculation of 24-haverage BP values that are not weighted for the differentnumber of hourly measurements during daytime and night-time weighted hourly BP values have been shown to bemore reliable than calculations based on the average of allindividual readings [57]
The use of ABPM in clinical practice can be facilitated bystandardizing the graphic presentation of ABPM datamuch as is the case for ECG recordings so that the pres-entation of data is independent of the type of ABPMmonitor used and the user is not required to becomefamiliar with a variety of programs Standardization alsofacilitates the interchange of ABPM recordings betweendatabases such as a hospital and primary care practiceMoreover if ABPM software programs provide a printedreport of the standardized ABPM data with a validatedinterpretative report [58] (signed by the physician in chargeof the service whenever legally required) doctors andnurses unfamiliar with the technique are assisted inlearning the variety of patterns generated by ABPM andbecause an individualized physician report is not a require-ment in most cases the cost of ABPM is reduced [110](Box 4)
421 Software requirementsThe following facilities are recommended for ABPM soft-ware in clinical practice [1910]
Clinical reportThe following information should be available in a one-page report
or
1
ize
Standardized plot format with each BP measurementon the vertical axis and time of day on horizontal axiswith different windows of the 24-h period identifiedand normal bands clearly demarcated The sleep timeinterval used to calculate asleep BP should be indi-cated (shaded) and preferably based on the indivi-dualsrsquo sleep time report (diary cards) In the plot the
d reproduction of this article is prohibitedwwwjhypertensioncom 1737
Cop
Box 4 Software requirements
Clinical report Ambulatory blood pressure measurement analysis and report should be standardized independent of the monitor type Standardized plot of all the blood pressure measurements with daytime and night-time windows and normal blood pressure bands demarcated Average SBP DBP and heart rate to be displayed Nocturnal blood pressure decline () for SBP and DBP Summary statistics for time-weighted average SBP and DBP and heart rate for the 24-h period daytime and night-time with standard deviations and number
of valid blood pressure readings Facility for showing error readings if requiredOptional requirements Automated software generated interpretative report indicating the normal or abnormal patterns and whether the requirements for a valid recording are
fulfilled Facility to plot heart rate and mean blood pressure Trend report for comparing repeated ambulatory blood pressure measurement recordings Ability to centrally host dataResearch report Data storage and raw data export capability for research analysis and audit Parameters include variability measures (such as 24-h SD 24-h weighted SD average real variability coefficient of variation) area under the curve
calculations blood pressure load parameters ratendashpressure product trough and peak levels smoothness index (the last two parameters requiring ABPMdata before and during treatment to be available) cusum-derived statistics and ambulatory arterial stiffness index
OrsquoBrien et al
1738
upper value of the Y-axis should not be fixed butadjustable to the highest BP value recorded in orderto maximize the graphic presentation of BP variationsover the 24-h period A plot of SBP and DBP through-out the 24-h period with a facility for plotting heartrate and mean BP so as to provide evidence ofcircadian behavior should be provided
2
Summary statistics for time-weighted SBP and DBPand heart rate in the windows of the 24-h period andseparately for the awake and asleep subperiods withthe respective standard deviations and the number ofvalid BP readings included in the analysis and afacility for indicating the time of going to bed andawakening
3
Medication details
4
Facility for showing error readings if required
Interpretative reportTo remove the variance associated with the ABPMinterpretation by human observers and to simplify theevaluation of results in routine clinical practice for thoseunfamiliar with the technique there should be an auto-mated software-generated interpretative report indicatingnormal or abnormal BP patterns and whether there aresufficient measurements for the recording to be valid [10]The interpretative report should be validated by testing thecomputer-generated report against reports from experts[5859]
Trend reportThe provision of a trend report allows ABPMs to be com-pared over time to demonstrate the response to changes inmanagement If ABPM is to be used to achieve better BPcontrol it is important for prescribing doctors (and patients)to be able to see whether medication is achieving controlthroughout the entire 24-h period
Research reportThe system should be capable of storing data for detailedanalysis for research and audit according to evidence-based
yright copy Lippincott Williams amp Wilkins Unautwwwjhypertensioncom
definitions for time-weighted arithmetic and mean valuesfor measures of BP level In view of evidence that short-term BP variability may give information over and abovemean BP levels and that reduction in 24-h BP variabilitymay be beneficial [63w] time-weighted and other measuresof short-term BP variability are helpful for on-goingresearch in this area Informative indices associated withoutcome such as area under the curve calculations BP loadparameters trough and peak levels the smoothness index(the last two parameters requiring ABPM data before andduring treatment to be available) cusum-derived statisticsand most recently the ambulatory arterial stiffness index(AASI) should also be provided [6061] The system shouldbe capable of storing and exporting raw data for researchpurposes and additional analyses [606163w]
422 Indices derived from ambulatory bloodpressure monitoring recordingsAverage BP values (over 24 h daytime and night-time) areundoubtedly the most important parameters obtained fromABPM recordings based on outcome data However alarge number of additional indices with promising clinicalevidence may be derived from ABPM recordings and someof them are occasionally included in the reports generatedby ABPM systems
Blood pressure loadThis index is defined as the percentage of readings in agiven period (24-h day or night) which exceed a prede-fined threshold value typically set at the proposed nor-malcy level for average BP values of that period The aim ofBP load is to quantify the number of readings with elevatedBP and mathematically it depends on both average BPlevels and distribution of BP readings [62] Although intheory clinically appealing and thus commonly incorpor-ated in the ABPM software this index has a number oflimitations Firstly there is no evidence that the thresholdsdefined for average BP values have any prognostic meaningwhen applied to single BP measurements Secondly whencomparing recordings with similar average BP levels differ-ences in BP load can be largely explained by differences in
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
BP variability making this index largely redundant ThirdlyBP load does not contain the prognostically importantinformation on how much the threshold level has beenexceeded To overcome the latter limitation it has beenproposed to modify the classic BP load definition bycalculating the total area under the timendashpressure curvewhen BP exceeds the threshold [63] Finally although somestudies support the usefulness of BP load in predictingorgan damage [6464w] it has never been convincinglydemonstrated that it provides any additional and clinicallyrelevant information independently of what is obtained byfocusing on average BP values The use of BP load inchildren has also been examined but it has not been foundhelpful in diagnosis [65w]
Ratendashpressure productThis index which is defined as heart rate multiplied by SBPis used as an index of myocardial work during exercise andit has prognostic relevance [66w] The availability of bothheart rate and BP data in ABPM makes it possible to obtainthe index readily especially if ABPM is accompanied byactigraphy [65] Although potentially promising the clinicalapplication of this index requires further research
rsquoVascularrsquo indicesSeveral ABPM-based indices have been proposed to pro-vide information on vascular wall properties Their ration-ale is based on the observation that the stiffness of thearterial wall increases when it is being stretched in patientswith impaired arterial wall elasticity SBP increases moresteeply than DBP whereas in a patient with elastic arteriesSBP and DBP increase in parallel The AASI which iscalculated as 1 ndash slope of regression of DBP on SBP isreadily obtainable from ABPM [6066]
AASI appears to have a direct relationship to carotidndashfemoral pulse wave velocity (a validated index of largearteriesrsquo stiffness) and an independent relationship withcardiovascular outcomes [606167wndash70w] Howeverthe ability of AASI to reflect arterial stiffness has beenchallenged because of its dependence on nocturnal BP falland the fact that it implies the use of asymmetric regressionpossibly affecting the precision of slope estimation[67ndash6971w72w] Modifications to AASI have been pro-posed but further data are awaited as to their ability tosurpass AASI in predicting outcome [73w74w]
The QndashKd interval which measures the time intervalbetween the onset of the QRS on the electrocardiogram (Q)and the last Korotkoff sound (K) corresponding to thediastolic pressure (d) has also been shown to have prog-nostic value [70]
Indices for indicating the pattern of treatment-induced changes in 24-h blood pressure loweringTwo principal indices are available for assessing thesmoothness and consistency of antihypertensive treatmenteffect over 24 h with ABPM The trough-to-peak ratio is theratio between BP reduction achieved by treatment at theend of dosing interval (trough which for drugs adminis-tered once daily means 24 h after the last dose intake) andpeak BP reduction usually achieved a few hours after dose
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
intake [7172] The trough-to-peak ratio is characterized by ahigh degree of variability in individual patients and istherefore not suitable for application to clinical practice[73] The smoothness index is calculated as the ratiobetween the average of hourly BP reductions over 24 hand the standard deviation (SD) of such an average valuethus integrating information on the size of BP reduction bytreatment and on its homogeneity throughout the 24-hperiod [7173] The smoothness index is highest for potentdrugs or drug combinations which also provide the mosthomogeneous BP reduction It is more reproducible thanthe troughpeak ratio [7173] and predicts treatment-induced changes in indices of organ damage includingleft ventricular mass and carotid arterial wall thickness[75w] A recent meta-analysis has provided informationon clinical determinants of the smoothness index suchas age ethnicity sex and smoking [74] The relevance ofthese indices in predicting the impact of treatment onoutcome and the reference values remain to be assessed
5 PROCEDURE
51 Training requirementsThe technique of ABPM is a specialized one and should beapproached with the care reserved for any such procedureAn understanding of the principles of traditional BPmeasurement cuff fitting monitor function and analysisand interpretation of ABPM data is required In practice anurse with an interest and experience in hypertension canmaster the use of ABPM devices after a relatively brieftraining However the interpretation of ABPM profilesrequires experience in the technique which is best pro-vided by the doctor in charge of an ABPM service [19]
52 Fitting an ambulatory blood pressuremonitorTime needs to be given to fitting the monitor and preparingthe patient for the monitoring period if good results are tobe obtained [19] The key to successful ABPM is educatingthe patient on the process of monitoring and the instruc-tions should be explained and printed on a diary card Inclinical practice measurements are preferably performedon a routine working day Although ABPM is best notperformed while patients are admitted to hospital becausehospitalization leads to underestimation of BP and over-diagnosis of nondippers [10] there are occasions such asthe evaluation of severely resistant hypertension andassessment of patients following a stroke when ABPM inhospital may be indicated
The frequency of measurement during the 24-h period isgenerally not more than every 15 min (which could inter-fere with normal activity) nor less than every 30min (whichcould give an inadequate number of measurements) Morefrequent measurements at night may disturb sleep andsleep disturbance has been shown to reduce the prognosticvalue of ABPM [75] To improve reproducibility repetitionof ABPM should be performed on like days for example onroutine working or recreational days A diary card can beused to record symptoms and events that may influenceABPM measurements
orized reproduction of this article is prohibitedwwwjhypertensioncom 1739
OrsquoBrien et al
53 Explanation to patientThe first step is adequate explanation of the procedure in anattempt to allay anxiety especially in nervous patientsPatients having ABPM for the first time should be told thatthere is minor discomfort caused by inflation of the cuff It isimportant to emphasize to the patient to follow hisherusual daily activities but as much as possible to remain stillwith the arm relaxed and not extended or contracted atheart level during each BP measurement [19] It can behelpful to have patients record periods of stress the time ofmeals the time of a siesta the time of going to bed andrising the quality of sleep and the time and type ofdrug ingestion
Box 5 Evaluation of ambulatory blood pressure monitoring data
Definition of daytime and night-time Daytime and night-time intervals are best defined using sleeping times
reported by individual usersrsquo diary cards (awake and asleep periods) Fixed narrow time intervals can be applied by discarding transition
periods between daytime and night-time (eg daytime defined as0900ndash2100 h and night-time 0100ndash0600 h)
Editing requirements Editing is not necessary for calculating average 24-h daytime and
night-time values The ambulatory blood pressure monitoring should be repeated if thefollowing criteria are not met
24-h recording with at least 70 of expected measurements20 valid awake (0900 to 2100 h)7 valid asleep (0100 to 0600 h)Blood pressure measurements at 30-min intervalsFor research purposes at least two valid daytime and one valid
night-time measurement per hour
54 Identification of daytime and night-timeperiods and editing ambulatory blood pressuremonitoring dataOne simple and popular method for identifying daytimeand night-time subperiods is to assess the time of awaken-ing and sleeping from diary card entries Another method isto use a fixed-narrow time interval approach in which forexample the retiring (2101 to 0059 h) and rising (0601 to0859 h) periods (which are subject to considerable vari-ation) are eliminated with the daytime period being from0900 to 2100 h and night-time from 0100 to 0600 h in thisway the variations in the time spent in bed that may existbetween the young and the old and in different culturesare to some extent eliminated from the analysis [176w]This method has the disadvantage of eliminating infor-mation on the white-coat window on the early phase ofnight sleep when dipping can be most evident and onthe early morning surge of BP which may be associatedwith cardiovascular events However these windows canbe analyzed separately for research or if considered import-ant in practice In countries where a daytime siesta ispopular a record of sleeping times both during day andnight is important and ABPM software should be able toadjust for this otherwise there may be underestimation ofthe nocturnal BP dip and overdiagnosis of nondippers[77w]
Many statistical techniques exist for editing ABPMrecords and no one method is ideal [176w] The detec-tion of artefactual readings and the handling of outliervalues (which may or may not be erroneous) have indeedbeen the subject of debate [76w] There are a number ofways of separately analyzing BPs recorded during the dayand night [7678w] Several automatic procedures havebeen proposed to reject outlying measurements based ona univariate multivariate or temporal approach Morecomplex procedures requiring the intervention of theobserver have been proposed but they are time consum-ing and not suitable for clinical practice [77] It has beenshown that rejection of outliers may alter the results ofABPM in individual patients sometimes significantlyaffecting average SBP levels [777879w] Editing pro-cedures can reduce mean systolic ABPM by 4 mmHg incomparison with unedited recordings thereby decreasingthe likelihood of diagnosing sustained hypertension Inone study the prevalence of sustained hypertension wasdecreased by 6ndash10 when several editing methods were
Copyright copy Lippincott Williams amp Wilkins Unaut1740 wwwjhypertensioncom
applied to raw 24-h data [79w] To make the results ofdifferent laboratories comparable common editingcriteria for ABPM should be used The problem is toestablish which of the methods proposed in the literatureprovides the most reliable data While awaiting moreobjective criteria to identify a universally acceptable edit-ing procedure we recommend that editing is not necess-ary for calculating average 24-h daytime and night-timevalues and that only physiologically impossible readingsshould be deleted from recordings However when thereare excessive artefacts in a tracing a repeat recordingrather than editing should be performed Some editingmight be required when focusing on analysis of BPvariability for the quantification of which the presenceof artefacts may introduce appreciable errors If editing isconsidered necessary a method proposed by Casadeiet al [80w] and modified by Winnicki et al [78] providescomparable performance to other proposed editing pro-cedures
There are no firm data on which to base recommen-dations for a satisfactory ABPM recording but the recom-mendation for having at least 70 of expectedmeasurements provides a basic working recommendationfor clinical practice This figure will be influenced by theperiod demarcated as daytime (awake) or night-time(asleep) periods and by the number of measurementsselected (usually 30-min but often 15 or 20-min intervals)In the previous ESH guideline on measurement it wasrecommended that there should be a minimum of 14measurements during the day and seven measurementsat night [1] Having considered what evidence is availableand the practical issues of performing repeat ABPM inpractice it seems reasonable to increase the minimum ofdaytime measurements to 20 while retaining a minimumseven measurements at night based on measurementsbeing performed every 30min and with fixed time periodsbeing used to define day (0900 to 2100 h) and night (0100 to0600 h) [1] (Box 5)
55 The arm for measurementABPM is best measured in the nondominant arm so as tointerfere as little as possible with daily activity unless there
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
has been documented evidence of a difference in BPbetween arms in which case the arm known to have thehigher BP values should be chosen [1] It is commonpractice for BP to be measured by a conventional techniqueat the same time as an ABPM monitor is being fitted and todetermine whether there is a discrepancy between thetechniques However BP variability is such that any suchcomparison has little validity and to determine a significantdifference it is necessary to perform simultaneousmeasurement according to a definitive protocol and thisis not feasible in practice [42] Because of these limitationsthe practice of performing a comparative measurement isnot recommended
56 Selecting the appropriate cuff and bladderThere is unequivocal evidence that either too narrow ortoo short a bladder (undercuffing) will cause overesti-mation of BP so-called lsquocuff hypertensionrsquo and there isgrowing evidence that too wide or too long a bladder(overcuffing) may cause underestimation of BP Under-cuffing has the effect in clinical practice of overdiagnos-ing hypertension and overcuffing leads to hypertensivepatients being diagnosed as normotensive Either even-tuality has serious implications for the epidemiology ofhypertension and for clinical practice [79] It is importanttherefore to select a cuff containing an inflatable bladderof correct length and width for the arm in which ABPM isto be measured All ABPM devices should provide cuffscontaining bladders for small medium and large-sizedarms as recommended in international guidelines[18081] However in many obese individuals the largebladder sizes cannot be used because the arm length istoo short to accommodate the bladder [81w] Anotherproblem is that the cylindrical shape of the commonlyused cuffs does not always wrap snugly around conical-shaped arms in obese and very muscular arms[8282w83w] Recently novel oscillometric homemonitors with cuff technology that allows a singlefixed-size cuff to be used on a wide range of arm circum-ferences have been developed [84wndash87w]
Another issue that needs consideration is the possibilitythat the discomfort caused by inflation of a large cuff inobese patients might cause elevation of BP This issuebecomes more important during ABPM because ofrepeated measurement especially during night-time sleepOscillometric devices for home use that measure BP duringcuff inflation may induce less discomfort because themeasurement is completed before maximal inflation[84w88w] However to date no study has specificallyaddressed this issue
Forearm BP measurement may have to be consideredwhen extreme obesity makes upper arm BP measurementimpossible BP measurements tend to be higher with fore-arm compared with upper arm measurement but meth-odological differences in these studies make it difficult toprovide recommendations for all populations [8389wndash94w] Despite the questionable accuracy of forearm BPmeasurement it may be the only acceptable option forABPM in individuals with very large upper arms providedthe patient is instructed to keep the forearm at heart levelduring measurement [94w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
No wrist devices have been validated for ABPM whereastechnology for continuous beat-to-beat monitoring ofambulatory BP in the finger has been developed usingthe volume-clamp method first described by Penaz [95w]A number of studies that compared this technology withintraarterial or noninvasive BP measurement showedunderestimation of BP particularly diastolic yet it remainsa practical alternative to intraarterial measurement for theevaluation of beat-to-beat BP changes and variability inresearch studies [8496wndash98w]
57 Conditions in which ambulatory bloodpressure monitoring may be difficult toperform
Obese patientsObesity is a well established major risk factor for hyperten-sion with higher prevalence in specific population groupssuch as patients with diabetes mellitus [99w] or OSA [100w]Despite the increasing prevalence of obesity worldwide[101w] and the close link between obesity and hyperten-sion scarce data are available on the application of ABPM inobese and extremely obese individuals ABPM is oftenrequired in these individuals and technical difficultiesshould not exclude them from such a valuable technology[79] The problem of miscuffing in obese pregnant womenmay result in diagnostic discrepancies [85]
Patients with atrial fibrillationBP measurement in patients with atrial fibrillation is lessprecise as this type of arrhythmia is accompanied byincreased beat-to-beat BP variability due to variations inventricular filling time stroke volume and contractilityInternational guidelines [181] recognize the relatively poorprecision of a single BP measurement and recommendrepeated readings in order to improve the accuracy ofestimates Theoretically ABPM should fulfill this stipulationas it provides a relatively high number of readings in a shortperiod of time Unfortunately published evidence regard-ing the role of ABPM in patients with arrhythmias andspecifically in patients with atrial fibrillation is scarce
Patients with atrial fibrillation have been usuallyexcluded from trials using ABPM as well as from validationprotocols of ABPM devices Four studies have addressedthe possible value of ABPM in patients with atrial fibrillation[48w102wndash104w] The evidence from these studiessuggests that ABPM may be useful in these patients pro-vided its limitations are taken into account The proportionof readings with errors the variability of BP and therepeatability coefficients do not appear to be different fromthose in patients in sinus rhythm DBP measured using anABPM monitor in patients with atrial fibrillation appears tobe relatively higher than that obtained with the traditionaloffice measurement or by the same ABPM procedure whenthe patient achieves sinus rhythm This finding is supportedby a review and meta-analysis of studies that validatedelectronic devices in patients with sustained atrial fibrilla-tion which showed consistent overestimation of DBP [52]In spite of this and although larger trials in patients on atrialfibrillation are recommended there is no reason to exclude
orized reproduction of this article is prohibitedwwwjhypertensioncom 1741
OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Guideline
Ambulatory blood pressure monitoring and ECGDevices have been developed allowing 24-h ABPM withcontinuous 24-h ECG in a single procedure Besides theusual well established indications for each of these pro-cedures the interaction between these two signals providescomplementary interrelated information in one procedureThe use of the real heart rate to determine the deflation ratecan provide more precise BP measurement and additionalextra BP measurements can be triggered by abnormal ECGactivities such as arrhythmias and ST segment abnormal-ities Limitations are the relatively high cost of monitors andsoftware the complexity compared to the simple ABPMprocedure and the difficulties in performing validationstudies for the combined functions [47w48w] Thesedisadvantages are offset to some extent by being ableto perform the two procedures simultaneously in olderpatients in whom arterial hypertension and paroxysmalatrial fibrillation often coexist Another development hasbeen the use of spectral analysis of heart rate to provide ameans for improving screening for obstructive sleep apnea(OSA) [49w50w]
Ambulatory blood pressure monitoring and arterialfunctionDevices are being developed that measure arterial stiffnessso as to provide interesting information on 24-h ABPM andon arterial function [51wndash55w]
Ambulatory blood pressure monitoring and positionsensingPosition sensors have been developed to determinewhether the patient is standing or lying during ABPMrecording and this facility allows an estimation of the sleepperiod [5556w]
Ambulatory blood pressure monitoring and activitysensingActivity sensors and accelerometers have been developedfor monitoring patient activity during ABPM so as to providean indirect measure of activity and rest with the formerbeing an estimate of the awake period and the latter ofsleep Some of these sensors are incorporated in the devicewhereas others are complementary accessories placedeither at wrist thigh or chest level [57w]
Ambulatory blood pressure monitoring and centralblood pressureSeveral 24-h oscillometric ABPM monitors use specificalgorithms and software for pulse wave analysis by record-ing 24-h ABPM data as well as calculating central BP [5651wndash53w58wndash61w] Further studies are needed howeverto demonstrate the validity and clinical usefulness of thesedevices which at present should not be used for makingclinical decisions
42 Software for ambulatory blood pressuremonitoring data analysisRecommendations on procedures for ABPM use tend toconcentrate on the accuracy of the devicersquos hardware withlittle attention being paid to software presentation and
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
analysis of ABPM data As a consequence the practisingphysician who has to interpret the considerable amount ofdata provided by ABPM is often faced with a bewilderingreport with reams of paper containing plots histogramsand data analysis that have little relevance for clinicalpractice It is important for ABPM software programs tobe suitable for the intended use of the device For examplein a busy general practice perhaps only basic data givingaverage 24-h daytime and night-time values and a visualplot are all that will be required whereas for researchpurposes statistical detail on the windows of the 24-hprofile and other indices may be required [10] A recentstudy has stressed that whereas monitors for ABPM aresubject to extensive validation protocols there is no inter-national guideline on the software processing of the col-lected raw data to prevent error being introduced by thesoftware permutations An example of software-inducederror was demonstrated for the SpaceLabs Report Manage-ment System 92506 which showed errors in 92 of reportsamounting to a numerical difference between printout andon-screen hourly averages ranging from 37 to 18mmHgfor SBP and from 16 to 10mmHg for DBP [62w] Anadditional problem can arise from the calculation of 24-haverage BP values that are not weighted for the differentnumber of hourly measurements during daytime and night-time weighted hourly BP values have been shown to bemore reliable than calculations based on the average of allindividual readings [57]
The use of ABPM in clinical practice can be facilitated bystandardizing the graphic presentation of ABPM datamuch as is the case for ECG recordings so that the pres-entation of data is independent of the type of ABPMmonitor used and the user is not required to becomefamiliar with a variety of programs Standardization alsofacilitates the interchange of ABPM recordings betweendatabases such as a hospital and primary care practiceMoreover if ABPM software programs provide a printedreport of the standardized ABPM data with a validatedinterpretative report [58] (signed by the physician in chargeof the service whenever legally required) doctors andnurses unfamiliar with the technique are assisted inlearning the variety of patterns generated by ABPM andbecause an individualized physician report is not a require-ment in most cases the cost of ABPM is reduced [110](Box 4)
421 Software requirementsThe following facilities are recommended for ABPM soft-ware in clinical practice [1910]
Clinical reportThe following information should be available in a one-page report
or
1
ize
Standardized plot format with each BP measurementon the vertical axis and time of day on horizontal axiswith different windows of the 24-h period identifiedand normal bands clearly demarcated The sleep timeinterval used to calculate asleep BP should be indi-cated (shaded) and preferably based on the indivi-dualsrsquo sleep time report (diary cards) In the plot the
d reproduction of this article is prohibitedwwwjhypertensioncom 1737
Cop
Box 4 Software requirements
Clinical report Ambulatory blood pressure measurement analysis and report should be standardized independent of the monitor type Standardized plot of all the blood pressure measurements with daytime and night-time windows and normal blood pressure bands demarcated Average SBP DBP and heart rate to be displayed Nocturnal blood pressure decline () for SBP and DBP Summary statistics for time-weighted average SBP and DBP and heart rate for the 24-h period daytime and night-time with standard deviations and number
of valid blood pressure readings Facility for showing error readings if requiredOptional requirements Automated software generated interpretative report indicating the normal or abnormal patterns and whether the requirements for a valid recording are
fulfilled Facility to plot heart rate and mean blood pressure Trend report for comparing repeated ambulatory blood pressure measurement recordings Ability to centrally host dataResearch report Data storage and raw data export capability for research analysis and audit Parameters include variability measures (such as 24-h SD 24-h weighted SD average real variability coefficient of variation) area under the curve
calculations blood pressure load parameters ratendashpressure product trough and peak levels smoothness index (the last two parameters requiring ABPMdata before and during treatment to be available) cusum-derived statistics and ambulatory arterial stiffness index
OrsquoBrien et al
1738
upper value of the Y-axis should not be fixed butadjustable to the highest BP value recorded in orderto maximize the graphic presentation of BP variationsover the 24-h period A plot of SBP and DBP through-out the 24-h period with a facility for plotting heartrate and mean BP so as to provide evidence ofcircadian behavior should be provided
2
Summary statistics for time-weighted SBP and DBPand heart rate in the windows of the 24-h period andseparately for the awake and asleep subperiods withthe respective standard deviations and the number ofvalid BP readings included in the analysis and afacility for indicating the time of going to bed andawakening
3
Medication details
4
Facility for showing error readings if required
Interpretative reportTo remove the variance associated with the ABPMinterpretation by human observers and to simplify theevaluation of results in routine clinical practice for thoseunfamiliar with the technique there should be an auto-mated software-generated interpretative report indicatingnormal or abnormal BP patterns and whether there aresufficient measurements for the recording to be valid [10]The interpretative report should be validated by testing thecomputer-generated report against reports from experts[5859]
Trend reportThe provision of a trend report allows ABPMs to be com-pared over time to demonstrate the response to changes inmanagement If ABPM is to be used to achieve better BPcontrol it is important for prescribing doctors (and patients)to be able to see whether medication is achieving controlthroughout the entire 24-h period
Research reportThe system should be capable of storing data for detailedanalysis for research and audit according to evidence-based
yright copy Lippincott Williams amp Wilkins Unautwwwjhypertensioncom
definitions for time-weighted arithmetic and mean valuesfor measures of BP level In view of evidence that short-term BP variability may give information over and abovemean BP levels and that reduction in 24-h BP variabilitymay be beneficial [63w] time-weighted and other measuresof short-term BP variability are helpful for on-goingresearch in this area Informative indices associated withoutcome such as area under the curve calculations BP loadparameters trough and peak levels the smoothness index(the last two parameters requiring ABPM data before andduring treatment to be available) cusum-derived statisticsand most recently the ambulatory arterial stiffness index(AASI) should also be provided [6061] The system shouldbe capable of storing and exporting raw data for researchpurposes and additional analyses [606163w]
422 Indices derived from ambulatory bloodpressure monitoring recordingsAverage BP values (over 24 h daytime and night-time) areundoubtedly the most important parameters obtained fromABPM recordings based on outcome data However alarge number of additional indices with promising clinicalevidence may be derived from ABPM recordings and someof them are occasionally included in the reports generatedby ABPM systems
Blood pressure loadThis index is defined as the percentage of readings in agiven period (24-h day or night) which exceed a prede-fined threshold value typically set at the proposed nor-malcy level for average BP values of that period The aim ofBP load is to quantify the number of readings with elevatedBP and mathematically it depends on both average BPlevels and distribution of BP readings [62] Although intheory clinically appealing and thus commonly incorpor-ated in the ABPM software this index has a number oflimitations Firstly there is no evidence that the thresholdsdefined for average BP values have any prognostic meaningwhen applied to single BP measurements Secondly whencomparing recordings with similar average BP levels differ-ences in BP load can be largely explained by differences in
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
BP variability making this index largely redundant ThirdlyBP load does not contain the prognostically importantinformation on how much the threshold level has beenexceeded To overcome the latter limitation it has beenproposed to modify the classic BP load definition bycalculating the total area under the timendashpressure curvewhen BP exceeds the threshold [63] Finally although somestudies support the usefulness of BP load in predictingorgan damage [6464w] it has never been convincinglydemonstrated that it provides any additional and clinicallyrelevant information independently of what is obtained byfocusing on average BP values The use of BP load inchildren has also been examined but it has not been foundhelpful in diagnosis [65w]
Ratendashpressure productThis index which is defined as heart rate multiplied by SBPis used as an index of myocardial work during exercise andit has prognostic relevance [66w] The availability of bothheart rate and BP data in ABPM makes it possible to obtainthe index readily especially if ABPM is accompanied byactigraphy [65] Although potentially promising the clinicalapplication of this index requires further research
rsquoVascularrsquo indicesSeveral ABPM-based indices have been proposed to pro-vide information on vascular wall properties Their ration-ale is based on the observation that the stiffness of thearterial wall increases when it is being stretched in patientswith impaired arterial wall elasticity SBP increases moresteeply than DBP whereas in a patient with elastic arteriesSBP and DBP increase in parallel The AASI which iscalculated as 1 ndash slope of regression of DBP on SBP isreadily obtainable from ABPM [6066]
AASI appears to have a direct relationship to carotidndashfemoral pulse wave velocity (a validated index of largearteriesrsquo stiffness) and an independent relationship withcardiovascular outcomes [606167wndash70w] Howeverthe ability of AASI to reflect arterial stiffness has beenchallenged because of its dependence on nocturnal BP falland the fact that it implies the use of asymmetric regressionpossibly affecting the precision of slope estimation[67ndash6971w72w] Modifications to AASI have been pro-posed but further data are awaited as to their ability tosurpass AASI in predicting outcome [73w74w]
The QndashKd interval which measures the time intervalbetween the onset of the QRS on the electrocardiogram (Q)and the last Korotkoff sound (K) corresponding to thediastolic pressure (d) has also been shown to have prog-nostic value [70]
Indices for indicating the pattern of treatment-induced changes in 24-h blood pressure loweringTwo principal indices are available for assessing thesmoothness and consistency of antihypertensive treatmenteffect over 24 h with ABPM The trough-to-peak ratio is theratio between BP reduction achieved by treatment at theend of dosing interval (trough which for drugs adminis-tered once daily means 24 h after the last dose intake) andpeak BP reduction usually achieved a few hours after dose
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
intake [7172] The trough-to-peak ratio is characterized by ahigh degree of variability in individual patients and istherefore not suitable for application to clinical practice[73] The smoothness index is calculated as the ratiobetween the average of hourly BP reductions over 24 hand the standard deviation (SD) of such an average valuethus integrating information on the size of BP reduction bytreatment and on its homogeneity throughout the 24-hperiod [7173] The smoothness index is highest for potentdrugs or drug combinations which also provide the mosthomogeneous BP reduction It is more reproducible thanthe troughpeak ratio [7173] and predicts treatment-induced changes in indices of organ damage includingleft ventricular mass and carotid arterial wall thickness[75w] A recent meta-analysis has provided informationon clinical determinants of the smoothness index suchas age ethnicity sex and smoking [74] The relevance ofthese indices in predicting the impact of treatment onoutcome and the reference values remain to be assessed
5 PROCEDURE
51 Training requirementsThe technique of ABPM is a specialized one and should beapproached with the care reserved for any such procedureAn understanding of the principles of traditional BPmeasurement cuff fitting monitor function and analysisand interpretation of ABPM data is required In practice anurse with an interest and experience in hypertension canmaster the use of ABPM devices after a relatively brieftraining However the interpretation of ABPM profilesrequires experience in the technique which is best pro-vided by the doctor in charge of an ABPM service [19]
52 Fitting an ambulatory blood pressuremonitorTime needs to be given to fitting the monitor and preparingthe patient for the monitoring period if good results are tobe obtained [19] The key to successful ABPM is educatingthe patient on the process of monitoring and the instruc-tions should be explained and printed on a diary card Inclinical practice measurements are preferably performedon a routine working day Although ABPM is best notperformed while patients are admitted to hospital becausehospitalization leads to underestimation of BP and over-diagnosis of nondippers [10] there are occasions such asthe evaluation of severely resistant hypertension andassessment of patients following a stroke when ABPM inhospital may be indicated
The frequency of measurement during the 24-h period isgenerally not more than every 15 min (which could inter-fere with normal activity) nor less than every 30min (whichcould give an inadequate number of measurements) Morefrequent measurements at night may disturb sleep andsleep disturbance has been shown to reduce the prognosticvalue of ABPM [75] To improve reproducibility repetitionof ABPM should be performed on like days for example onroutine working or recreational days A diary card can beused to record symptoms and events that may influenceABPM measurements
orized reproduction of this article is prohibitedwwwjhypertensioncom 1739
OrsquoBrien et al
53 Explanation to patientThe first step is adequate explanation of the procedure in anattempt to allay anxiety especially in nervous patientsPatients having ABPM for the first time should be told thatthere is minor discomfort caused by inflation of the cuff It isimportant to emphasize to the patient to follow hisherusual daily activities but as much as possible to remain stillwith the arm relaxed and not extended or contracted atheart level during each BP measurement [19] It can behelpful to have patients record periods of stress the time ofmeals the time of a siesta the time of going to bed andrising the quality of sleep and the time and type ofdrug ingestion
Box 5 Evaluation of ambulatory blood pressure monitoring data
Definition of daytime and night-time Daytime and night-time intervals are best defined using sleeping times
reported by individual usersrsquo diary cards (awake and asleep periods) Fixed narrow time intervals can be applied by discarding transition
periods between daytime and night-time (eg daytime defined as0900ndash2100 h and night-time 0100ndash0600 h)
Editing requirements Editing is not necessary for calculating average 24-h daytime and
night-time values The ambulatory blood pressure monitoring should be repeated if thefollowing criteria are not met
24-h recording with at least 70 of expected measurements20 valid awake (0900 to 2100 h)7 valid asleep (0100 to 0600 h)Blood pressure measurements at 30-min intervalsFor research purposes at least two valid daytime and one valid
night-time measurement per hour
54 Identification of daytime and night-timeperiods and editing ambulatory blood pressuremonitoring dataOne simple and popular method for identifying daytimeand night-time subperiods is to assess the time of awaken-ing and sleeping from diary card entries Another method isto use a fixed-narrow time interval approach in which forexample the retiring (2101 to 0059 h) and rising (0601 to0859 h) periods (which are subject to considerable vari-ation) are eliminated with the daytime period being from0900 to 2100 h and night-time from 0100 to 0600 h in thisway the variations in the time spent in bed that may existbetween the young and the old and in different culturesare to some extent eliminated from the analysis [176w]This method has the disadvantage of eliminating infor-mation on the white-coat window on the early phase ofnight sleep when dipping can be most evident and onthe early morning surge of BP which may be associatedwith cardiovascular events However these windows canbe analyzed separately for research or if considered import-ant in practice In countries where a daytime siesta ispopular a record of sleeping times both during day andnight is important and ABPM software should be able toadjust for this otherwise there may be underestimation ofthe nocturnal BP dip and overdiagnosis of nondippers[77w]
Many statistical techniques exist for editing ABPMrecords and no one method is ideal [176w] The detec-tion of artefactual readings and the handling of outliervalues (which may or may not be erroneous) have indeedbeen the subject of debate [76w] There are a number ofways of separately analyzing BPs recorded during the dayand night [7678w] Several automatic procedures havebeen proposed to reject outlying measurements based ona univariate multivariate or temporal approach Morecomplex procedures requiring the intervention of theobserver have been proposed but they are time consum-ing and not suitable for clinical practice [77] It has beenshown that rejection of outliers may alter the results ofABPM in individual patients sometimes significantlyaffecting average SBP levels [777879w] Editing pro-cedures can reduce mean systolic ABPM by 4 mmHg incomparison with unedited recordings thereby decreasingthe likelihood of diagnosing sustained hypertension Inone study the prevalence of sustained hypertension wasdecreased by 6ndash10 when several editing methods were
Copyright copy Lippincott Williams amp Wilkins Unaut1740 wwwjhypertensioncom
applied to raw 24-h data [79w] To make the results ofdifferent laboratories comparable common editingcriteria for ABPM should be used The problem is toestablish which of the methods proposed in the literatureprovides the most reliable data While awaiting moreobjective criteria to identify a universally acceptable edit-ing procedure we recommend that editing is not necess-ary for calculating average 24-h daytime and night-timevalues and that only physiologically impossible readingsshould be deleted from recordings However when thereare excessive artefacts in a tracing a repeat recordingrather than editing should be performed Some editingmight be required when focusing on analysis of BPvariability for the quantification of which the presenceof artefacts may introduce appreciable errors If editing isconsidered necessary a method proposed by Casadeiet al [80w] and modified by Winnicki et al [78] providescomparable performance to other proposed editing pro-cedures
There are no firm data on which to base recommen-dations for a satisfactory ABPM recording but the recom-mendation for having at least 70 of expectedmeasurements provides a basic working recommendationfor clinical practice This figure will be influenced by theperiod demarcated as daytime (awake) or night-time(asleep) periods and by the number of measurementsselected (usually 30-min but often 15 or 20-min intervals)In the previous ESH guideline on measurement it wasrecommended that there should be a minimum of 14measurements during the day and seven measurementsat night [1] Having considered what evidence is availableand the practical issues of performing repeat ABPM inpractice it seems reasonable to increase the minimum ofdaytime measurements to 20 while retaining a minimumseven measurements at night based on measurementsbeing performed every 30min and with fixed time periodsbeing used to define day (0900 to 2100 h) and night (0100 to0600 h) [1] (Box 5)
55 The arm for measurementABPM is best measured in the nondominant arm so as tointerfere as little as possible with daily activity unless there
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
has been documented evidence of a difference in BPbetween arms in which case the arm known to have thehigher BP values should be chosen [1] It is commonpractice for BP to be measured by a conventional techniqueat the same time as an ABPM monitor is being fitted and todetermine whether there is a discrepancy between thetechniques However BP variability is such that any suchcomparison has little validity and to determine a significantdifference it is necessary to perform simultaneousmeasurement according to a definitive protocol and thisis not feasible in practice [42] Because of these limitationsthe practice of performing a comparative measurement isnot recommended
56 Selecting the appropriate cuff and bladderThere is unequivocal evidence that either too narrow ortoo short a bladder (undercuffing) will cause overesti-mation of BP so-called lsquocuff hypertensionrsquo and there isgrowing evidence that too wide or too long a bladder(overcuffing) may cause underestimation of BP Under-cuffing has the effect in clinical practice of overdiagnos-ing hypertension and overcuffing leads to hypertensivepatients being diagnosed as normotensive Either even-tuality has serious implications for the epidemiology ofhypertension and for clinical practice [79] It is importanttherefore to select a cuff containing an inflatable bladderof correct length and width for the arm in which ABPM isto be measured All ABPM devices should provide cuffscontaining bladders for small medium and large-sizedarms as recommended in international guidelines[18081] However in many obese individuals the largebladder sizes cannot be used because the arm length istoo short to accommodate the bladder [81w] Anotherproblem is that the cylindrical shape of the commonlyused cuffs does not always wrap snugly around conical-shaped arms in obese and very muscular arms[8282w83w] Recently novel oscillometric homemonitors with cuff technology that allows a singlefixed-size cuff to be used on a wide range of arm circum-ferences have been developed [84wndash87w]
Another issue that needs consideration is the possibilitythat the discomfort caused by inflation of a large cuff inobese patients might cause elevation of BP This issuebecomes more important during ABPM because ofrepeated measurement especially during night-time sleepOscillometric devices for home use that measure BP duringcuff inflation may induce less discomfort because themeasurement is completed before maximal inflation[84w88w] However to date no study has specificallyaddressed this issue
Forearm BP measurement may have to be consideredwhen extreme obesity makes upper arm BP measurementimpossible BP measurements tend to be higher with fore-arm compared with upper arm measurement but meth-odological differences in these studies make it difficult toprovide recommendations for all populations [8389wndash94w] Despite the questionable accuracy of forearm BPmeasurement it may be the only acceptable option forABPM in individuals with very large upper arms providedthe patient is instructed to keep the forearm at heart levelduring measurement [94w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
No wrist devices have been validated for ABPM whereastechnology for continuous beat-to-beat monitoring ofambulatory BP in the finger has been developed usingthe volume-clamp method first described by Penaz [95w]A number of studies that compared this technology withintraarterial or noninvasive BP measurement showedunderestimation of BP particularly diastolic yet it remainsa practical alternative to intraarterial measurement for theevaluation of beat-to-beat BP changes and variability inresearch studies [8496wndash98w]
57 Conditions in which ambulatory bloodpressure monitoring may be difficult toperform
Obese patientsObesity is a well established major risk factor for hyperten-sion with higher prevalence in specific population groupssuch as patients with diabetes mellitus [99w] or OSA [100w]Despite the increasing prevalence of obesity worldwide[101w] and the close link between obesity and hyperten-sion scarce data are available on the application of ABPM inobese and extremely obese individuals ABPM is oftenrequired in these individuals and technical difficultiesshould not exclude them from such a valuable technology[79] The problem of miscuffing in obese pregnant womenmay result in diagnostic discrepancies [85]
Patients with atrial fibrillationBP measurement in patients with atrial fibrillation is lessprecise as this type of arrhythmia is accompanied byincreased beat-to-beat BP variability due to variations inventricular filling time stroke volume and contractilityInternational guidelines [181] recognize the relatively poorprecision of a single BP measurement and recommendrepeated readings in order to improve the accuracy ofestimates Theoretically ABPM should fulfill this stipulationas it provides a relatively high number of readings in a shortperiod of time Unfortunately published evidence regard-ing the role of ABPM in patients with arrhythmias andspecifically in patients with atrial fibrillation is scarce
Patients with atrial fibrillation have been usuallyexcluded from trials using ABPM as well as from validationprotocols of ABPM devices Four studies have addressedthe possible value of ABPM in patients with atrial fibrillation[48w102wndash104w] The evidence from these studiessuggests that ABPM may be useful in these patients pro-vided its limitations are taken into account The proportionof readings with errors the variability of BP and therepeatability coefficients do not appear to be different fromthose in patients in sinus rhythm DBP measured using anABPM monitor in patients with atrial fibrillation appears tobe relatively higher than that obtained with the traditionaloffice measurement or by the same ABPM procedure whenthe patient achieves sinus rhythm This finding is supportedby a review and meta-analysis of studies that validatedelectronic devices in patients with sustained atrial fibrilla-tion which showed consistent overestimation of DBP [52]In spite of this and although larger trials in patients on atrialfibrillation are recommended there is no reason to exclude
orized reproduction of this article is prohibitedwwwjhypertensioncom 1741
OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Cop
Box 4 Software requirements
Clinical report Ambulatory blood pressure measurement analysis and report should be standardized independent of the monitor type Standardized plot of all the blood pressure measurements with daytime and night-time windows and normal blood pressure bands demarcated Average SBP DBP and heart rate to be displayed Nocturnal blood pressure decline () for SBP and DBP Summary statistics for time-weighted average SBP and DBP and heart rate for the 24-h period daytime and night-time with standard deviations and number
of valid blood pressure readings Facility for showing error readings if requiredOptional requirements Automated software generated interpretative report indicating the normal or abnormal patterns and whether the requirements for a valid recording are
fulfilled Facility to plot heart rate and mean blood pressure Trend report for comparing repeated ambulatory blood pressure measurement recordings Ability to centrally host dataResearch report Data storage and raw data export capability for research analysis and audit Parameters include variability measures (such as 24-h SD 24-h weighted SD average real variability coefficient of variation) area under the curve
calculations blood pressure load parameters ratendashpressure product trough and peak levels smoothness index (the last two parameters requiring ABPMdata before and during treatment to be available) cusum-derived statistics and ambulatory arterial stiffness index
OrsquoBrien et al
1738
upper value of the Y-axis should not be fixed butadjustable to the highest BP value recorded in orderto maximize the graphic presentation of BP variationsover the 24-h period A plot of SBP and DBP through-out the 24-h period with a facility for plotting heartrate and mean BP so as to provide evidence ofcircadian behavior should be provided
2
Summary statistics for time-weighted SBP and DBPand heart rate in the windows of the 24-h period andseparately for the awake and asleep subperiods withthe respective standard deviations and the number ofvalid BP readings included in the analysis and afacility for indicating the time of going to bed andawakening
3
Medication details
4
Facility for showing error readings if required
Interpretative reportTo remove the variance associated with the ABPMinterpretation by human observers and to simplify theevaluation of results in routine clinical practice for thoseunfamiliar with the technique there should be an auto-mated software-generated interpretative report indicatingnormal or abnormal BP patterns and whether there aresufficient measurements for the recording to be valid [10]The interpretative report should be validated by testing thecomputer-generated report against reports from experts[5859]
Trend reportThe provision of a trend report allows ABPMs to be com-pared over time to demonstrate the response to changes inmanagement If ABPM is to be used to achieve better BPcontrol it is important for prescribing doctors (and patients)to be able to see whether medication is achieving controlthroughout the entire 24-h period
Research reportThe system should be capable of storing data for detailedanalysis for research and audit according to evidence-based
yright copy Lippincott Williams amp Wilkins Unautwwwjhypertensioncom
definitions for time-weighted arithmetic and mean valuesfor measures of BP level In view of evidence that short-term BP variability may give information over and abovemean BP levels and that reduction in 24-h BP variabilitymay be beneficial [63w] time-weighted and other measuresof short-term BP variability are helpful for on-goingresearch in this area Informative indices associated withoutcome such as area under the curve calculations BP loadparameters trough and peak levels the smoothness index(the last two parameters requiring ABPM data before andduring treatment to be available) cusum-derived statisticsand most recently the ambulatory arterial stiffness index(AASI) should also be provided [6061] The system shouldbe capable of storing and exporting raw data for researchpurposes and additional analyses [606163w]
422 Indices derived from ambulatory bloodpressure monitoring recordingsAverage BP values (over 24 h daytime and night-time) areundoubtedly the most important parameters obtained fromABPM recordings based on outcome data However alarge number of additional indices with promising clinicalevidence may be derived from ABPM recordings and someof them are occasionally included in the reports generatedby ABPM systems
Blood pressure loadThis index is defined as the percentage of readings in agiven period (24-h day or night) which exceed a prede-fined threshold value typically set at the proposed nor-malcy level for average BP values of that period The aim ofBP load is to quantify the number of readings with elevatedBP and mathematically it depends on both average BPlevels and distribution of BP readings [62] Although intheory clinically appealing and thus commonly incorpor-ated in the ABPM software this index has a number oflimitations Firstly there is no evidence that the thresholdsdefined for average BP values have any prognostic meaningwhen applied to single BP measurements Secondly whencomparing recordings with similar average BP levels differ-ences in BP load can be largely explained by differences in
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
BP variability making this index largely redundant ThirdlyBP load does not contain the prognostically importantinformation on how much the threshold level has beenexceeded To overcome the latter limitation it has beenproposed to modify the classic BP load definition bycalculating the total area under the timendashpressure curvewhen BP exceeds the threshold [63] Finally although somestudies support the usefulness of BP load in predictingorgan damage [6464w] it has never been convincinglydemonstrated that it provides any additional and clinicallyrelevant information independently of what is obtained byfocusing on average BP values The use of BP load inchildren has also been examined but it has not been foundhelpful in diagnosis [65w]
Ratendashpressure productThis index which is defined as heart rate multiplied by SBPis used as an index of myocardial work during exercise andit has prognostic relevance [66w] The availability of bothheart rate and BP data in ABPM makes it possible to obtainthe index readily especially if ABPM is accompanied byactigraphy [65] Although potentially promising the clinicalapplication of this index requires further research
rsquoVascularrsquo indicesSeveral ABPM-based indices have been proposed to pro-vide information on vascular wall properties Their ration-ale is based on the observation that the stiffness of thearterial wall increases when it is being stretched in patientswith impaired arterial wall elasticity SBP increases moresteeply than DBP whereas in a patient with elastic arteriesSBP and DBP increase in parallel The AASI which iscalculated as 1 ndash slope of regression of DBP on SBP isreadily obtainable from ABPM [6066]
AASI appears to have a direct relationship to carotidndashfemoral pulse wave velocity (a validated index of largearteriesrsquo stiffness) and an independent relationship withcardiovascular outcomes [606167wndash70w] Howeverthe ability of AASI to reflect arterial stiffness has beenchallenged because of its dependence on nocturnal BP falland the fact that it implies the use of asymmetric regressionpossibly affecting the precision of slope estimation[67ndash6971w72w] Modifications to AASI have been pro-posed but further data are awaited as to their ability tosurpass AASI in predicting outcome [73w74w]
The QndashKd interval which measures the time intervalbetween the onset of the QRS on the electrocardiogram (Q)and the last Korotkoff sound (K) corresponding to thediastolic pressure (d) has also been shown to have prog-nostic value [70]
Indices for indicating the pattern of treatment-induced changes in 24-h blood pressure loweringTwo principal indices are available for assessing thesmoothness and consistency of antihypertensive treatmenteffect over 24 h with ABPM The trough-to-peak ratio is theratio between BP reduction achieved by treatment at theend of dosing interval (trough which for drugs adminis-tered once daily means 24 h after the last dose intake) andpeak BP reduction usually achieved a few hours after dose
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
intake [7172] The trough-to-peak ratio is characterized by ahigh degree of variability in individual patients and istherefore not suitable for application to clinical practice[73] The smoothness index is calculated as the ratiobetween the average of hourly BP reductions over 24 hand the standard deviation (SD) of such an average valuethus integrating information on the size of BP reduction bytreatment and on its homogeneity throughout the 24-hperiod [7173] The smoothness index is highest for potentdrugs or drug combinations which also provide the mosthomogeneous BP reduction It is more reproducible thanthe troughpeak ratio [7173] and predicts treatment-induced changes in indices of organ damage includingleft ventricular mass and carotid arterial wall thickness[75w] A recent meta-analysis has provided informationon clinical determinants of the smoothness index suchas age ethnicity sex and smoking [74] The relevance ofthese indices in predicting the impact of treatment onoutcome and the reference values remain to be assessed
5 PROCEDURE
51 Training requirementsThe technique of ABPM is a specialized one and should beapproached with the care reserved for any such procedureAn understanding of the principles of traditional BPmeasurement cuff fitting monitor function and analysisand interpretation of ABPM data is required In practice anurse with an interest and experience in hypertension canmaster the use of ABPM devices after a relatively brieftraining However the interpretation of ABPM profilesrequires experience in the technique which is best pro-vided by the doctor in charge of an ABPM service [19]
52 Fitting an ambulatory blood pressuremonitorTime needs to be given to fitting the monitor and preparingthe patient for the monitoring period if good results are tobe obtained [19] The key to successful ABPM is educatingthe patient on the process of monitoring and the instruc-tions should be explained and printed on a diary card Inclinical practice measurements are preferably performedon a routine working day Although ABPM is best notperformed while patients are admitted to hospital becausehospitalization leads to underestimation of BP and over-diagnosis of nondippers [10] there are occasions such asthe evaluation of severely resistant hypertension andassessment of patients following a stroke when ABPM inhospital may be indicated
The frequency of measurement during the 24-h period isgenerally not more than every 15 min (which could inter-fere with normal activity) nor less than every 30min (whichcould give an inadequate number of measurements) Morefrequent measurements at night may disturb sleep andsleep disturbance has been shown to reduce the prognosticvalue of ABPM [75] To improve reproducibility repetitionof ABPM should be performed on like days for example onroutine working or recreational days A diary card can beused to record symptoms and events that may influenceABPM measurements
orized reproduction of this article is prohibitedwwwjhypertensioncom 1739
OrsquoBrien et al
53 Explanation to patientThe first step is adequate explanation of the procedure in anattempt to allay anxiety especially in nervous patientsPatients having ABPM for the first time should be told thatthere is minor discomfort caused by inflation of the cuff It isimportant to emphasize to the patient to follow hisherusual daily activities but as much as possible to remain stillwith the arm relaxed and not extended or contracted atheart level during each BP measurement [19] It can behelpful to have patients record periods of stress the time ofmeals the time of a siesta the time of going to bed andrising the quality of sleep and the time and type ofdrug ingestion
Box 5 Evaluation of ambulatory blood pressure monitoring data
Definition of daytime and night-time Daytime and night-time intervals are best defined using sleeping times
reported by individual usersrsquo diary cards (awake and asleep periods) Fixed narrow time intervals can be applied by discarding transition
periods between daytime and night-time (eg daytime defined as0900ndash2100 h and night-time 0100ndash0600 h)
Editing requirements Editing is not necessary for calculating average 24-h daytime and
night-time values The ambulatory blood pressure monitoring should be repeated if thefollowing criteria are not met
24-h recording with at least 70 of expected measurements20 valid awake (0900 to 2100 h)7 valid asleep (0100 to 0600 h)Blood pressure measurements at 30-min intervalsFor research purposes at least two valid daytime and one valid
night-time measurement per hour
54 Identification of daytime and night-timeperiods and editing ambulatory blood pressuremonitoring dataOne simple and popular method for identifying daytimeand night-time subperiods is to assess the time of awaken-ing and sleeping from diary card entries Another method isto use a fixed-narrow time interval approach in which forexample the retiring (2101 to 0059 h) and rising (0601 to0859 h) periods (which are subject to considerable vari-ation) are eliminated with the daytime period being from0900 to 2100 h and night-time from 0100 to 0600 h in thisway the variations in the time spent in bed that may existbetween the young and the old and in different culturesare to some extent eliminated from the analysis [176w]This method has the disadvantage of eliminating infor-mation on the white-coat window on the early phase ofnight sleep when dipping can be most evident and onthe early morning surge of BP which may be associatedwith cardiovascular events However these windows canbe analyzed separately for research or if considered import-ant in practice In countries where a daytime siesta ispopular a record of sleeping times both during day andnight is important and ABPM software should be able toadjust for this otherwise there may be underestimation ofthe nocturnal BP dip and overdiagnosis of nondippers[77w]
Many statistical techniques exist for editing ABPMrecords and no one method is ideal [176w] The detec-tion of artefactual readings and the handling of outliervalues (which may or may not be erroneous) have indeedbeen the subject of debate [76w] There are a number ofways of separately analyzing BPs recorded during the dayand night [7678w] Several automatic procedures havebeen proposed to reject outlying measurements based ona univariate multivariate or temporal approach Morecomplex procedures requiring the intervention of theobserver have been proposed but they are time consum-ing and not suitable for clinical practice [77] It has beenshown that rejection of outliers may alter the results ofABPM in individual patients sometimes significantlyaffecting average SBP levels [777879w] Editing pro-cedures can reduce mean systolic ABPM by 4 mmHg incomparison with unedited recordings thereby decreasingthe likelihood of diagnosing sustained hypertension Inone study the prevalence of sustained hypertension wasdecreased by 6ndash10 when several editing methods were
Copyright copy Lippincott Williams amp Wilkins Unaut1740 wwwjhypertensioncom
applied to raw 24-h data [79w] To make the results ofdifferent laboratories comparable common editingcriteria for ABPM should be used The problem is toestablish which of the methods proposed in the literatureprovides the most reliable data While awaiting moreobjective criteria to identify a universally acceptable edit-ing procedure we recommend that editing is not necess-ary for calculating average 24-h daytime and night-timevalues and that only physiologically impossible readingsshould be deleted from recordings However when thereare excessive artefacts in a tracing a repeat recordingrather than editing should be performed Some editingmight be required when focusing on analysis of BPvariability for the quantification of which the presenceof artefacts may introduce appreciable errors If editing isconsidered necessary a method proposed by Casadeiet al [80w] and modified by Winnicki et al [78] providescomparable performance to other proposed editing pro-cedures
There are no firm data on which to base recommen-dations for a satisfactory ABPM recording but the recom-mendation for having at least 70 of expectedmeasurements provides a basic working recommendationfor clinical practice This figure will be influenced by theperiod demarcated as daytime (awake) or night-time(asleep) periods and by the number of measurementsselected (usually 30-min but often 15 or 20-min intervals)In the previous ESH guideline on measurement it wasrecommended that there should be a minimum of 14measurements during the day and seven measurementsat night [1] Having considered what evidence is availableand the practical issues of performing repeat ABPM inpractice it seems reasonable to increase the minimum ofdaytime measurements to 20 while retaining a minimumseven measurements at night based on measurementsbeing performed every 30min and with fixed time periodsbeing used to define day (0900 to 2100 h) and night (0100 to0600 h) [1] (Box 5)
55 The arm for measurementABPM is best measured in the nondominant arm so as tointerfere as little as possible with daily activity unless there
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
has been documented evidence of a difference in BPbetween arms in which case the arm known to have thehigher BP values should be chosen [1] It is commonpractice for BP to be measured by a conventional techniqueat the same time as an ABPM monitor is being fitted and todetermine whether there is a discrepancy between thetechniques However BP variability is such that any suchcomparison has little validity and to determine a significantdifference it is necessary to perform simultaneousmeasurement according to a definitive protocol and thisis not feasible in practice [42] Because of these limitationsthe practice of performing a comparative measurement isnot recommended
56 Selecting the appropriate cuff and bladderThere is unequivocal evidence that either too narrow ortoo short a bladder (undercuffing) will cause overesti-mation of BP so-called lsquocuff hypertensionrsquo and there isgrowing evidence that too wide or too long a bladder(overcuffing) may cause underestimation of BP Under-cuffing has the effect in clinical practice of overdiagnos-ing hypertension and overcuffing leads to hypertensivepatients being diagnosed as normotensive Either even-tuality has serious implications for the epidemiology ofhypertension and for clinical practice [79] It is importanttherefore to select a cuff containing an inflatable bladderof correct length and width for the arm in which ABPM isto be measured All ABPM devices should provide cuffscontaining bladders for small medium and large-sizedarms as recommended in international guidelines[18081] However in many obese individuals the largebladder sizes cannot be used because the arm length istoo short to accommodate the bladder [81w] Anotherproblem is that the cylindrical shape of the commonlyused cuffs does not always wrap snugly around conical-shaped arms in obese and very muscular arms[8282w83w] Recently novel oscillometric homemonitors with cuff technology that allows a singlefixed-size cuff to be used on a wide range of arm circum-ferences have been developed [84wndash87w]
Another issue that needs consideration is the possibilitythat the discomfort caused by inflation of a large cuff inobese patients might cause elevation of BP This issuebecomes more important during ABPM because ofrepeated measurement especially during night-time sleepOscillometric devices for home use that measure BP duringcuff inflation may induce less discomfort because themeasurement is completed before maximal inflation[84w88w] However to date no study has specificallyaddressed this issue
Forearm BP measurement may have to be consideredwhen extreme obesity makes upper arm BP measurementimpossible BP measurements tend to be higher with fore-arm compared with upper arm measurement but meth-odological differences in these studies make it difficult toprovide recommendations for all populations [8389wndash94w] Despite the questionable accuracy of forearm BPmeasurement it may be the only acceptable option forABPM in individuals with very large upper arms providedthe patient is instructed to keep the forearm at heart levelduring measurement [94w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
No wrist devices have been validated for ABPM whereastechnology for continuous beat-to-beat monitoring ofambulatory BP in the finger has been developed usingthe volume-clamp method first described by Penaz [95w]A number of studies that compared this technology withintraarterial or noninvasive BP measurement showedunderestimation of BP particularly diastolic yet it remainsa practical alternative to intraarterial measurement for theevaluation of beat-to-beat BP changes and variability inresearch studies [8496wndash98w]
57 Conditions in which ambulatory bloodpressure monitoring may be difficult toperform
Obese patientsObesity is a well established major risk factor for hyperten-sion with higher prevalence in specific population groupssuch as patients with diabetes mellitus [99w] or OSA [100w]Despite the increasing prevalence of obesity worldwide[101w] and the close link between obesity and hyperten-sion scarce data are available on the application of ABPM inobese and extremely obese individuals ABPM is oftenrequired in these individuals and technical difficultiesshould not exclude them from such a valuable technology[79] The problem of miscuffing in obese pregnant womenmay result in diagnostic discrepancies [85]
Patients with atrial fibrillationBP measurement in patients with atrial fibrillation is lessprecise as this type of arrhythmia is accompanied byincreased beat-to-beat BP variability due to variations inventricular filling time stroke volume and contractilityInternational guidelines [181] recognize the relatively poorprecision of a single BP measurement and recommendrepeated readings in order to improve the accuracy ofestimates Theoretically ABPM should fulfill this stipulationas it provides a relatively high number of readings in a shortperiod of time Unfortunately published evidence regard-ing the role of ABPM in patients with arrhythmias andspecifically in patients with atrial fibrillation is scarce
Patients with atrial fibrillation have been usuallyexcluded from trials using ABPM as well as from validationprotocols of ABPM devices Four studies have addressedthe possible value of ABPM in patients with atrial fibrillation[48w102wndash104w] The evidence from these studiessuggests that ABPM may be useful in these patients pro-vided its limitations are taken into account The proportionof readings with errors the variability of BP and therepeatability coefficients do not appear to be different fromthose in patients in sinus rhythm DBP measured using anABPM monitor in patients with atrial fibrillation appears tobe relatively higher than that obtained with the traditionaloffice measurement or by the same ABPM procedure whenthe patient achieves sinus rhythm This finding is supportedby a review and meta-analysis of studies that validatedelectronic devices in patients with sustained atrial fibrilla-tion which showed consistent overestimation of DBP [52]In spite of this and although larger trials in patients on atrialfibrillation are recommended there is no reason to exclude
orized reproduction of this article is prohibitedwwwjhypertensioncom 1741
OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Guideline
BP variability making this index largely redundant ThirdlyBP load does not contain the prognostically importantinformation on how much the threshold level has beenexceeded To overcome the latter limitation it has beenproposed to modify the classic BP load definition bycalculating the total area under the timendashpressure curvewhen BP exceeds the threshold [63] Finally although somestudies support the usefulness of BP load in predictingorgan damage [6464w] it has never been convincinglydemonstrated that it provides any additional and clinicallyrelevant information independently of what is obtained byfocusing on average BP values The use of BP load inchildren has also been examined but it has not been foundhelpful in diagnosis [65w]
Ratendashpressure productThis index which is defined as heart rate multiplied by SBPis used as an index of myocardial work during exercise andit has prognostic relevance [66w] The availability of bothheart rate and BP data in ABPM makes it possible to obtainthe index readily especially if ABPM is accompanied byactigraphy [65] Although potentially promising the clinicalapplication of this index requires further research
rsquoVascularrsquo indicesSeveral ABPM-based indices have been proposed to pro-vide information on vascular wall properties Their ration-ale is based on the observation that the stiffness of thearterial wall increases when it is being stretched in patientswith impaired arterial wall elasticity SBP increases moresteeply than DBP whereas in a patient with elastic arteriesSBP and DBP increase in parallel The AASI which iscalculated as 1 ndash slope of regression of DBP on SBP isreadily obtainable from ABPM [6066]
AASI appears to have a direct relationship to carotidndashfemoral pulse wave velocity (a validated index of largearteriesrsquo stiffness) and an independent relationship withcardiovascular outcomes [606167wndash70w] Howeverthe ability of AASI to reflect arterial stiffness has beenchallenged because of its dependence on nocturnal BP falland the fact that it implies the use of asymmetric regressionpossibly affecting the precision of slope estimation[67ndash6971w72w] Modifications to AASI have been pro-posed but further data are awaited as to their ability tosurpass AASI in predicting outcome [73w74w]
The QndashKd interval which measures the time intervalbetween the onset of the QRS on the electrocardiogram (Q)and the last Korotkoff sound (K) corresponding to thediastolic pressure (d) has also been shown to have prog-nostic value [70]
Indices for indicating the pattern of treatment-induced changes in 24-h blood pressure loweringTwo principal indices are available for assessing thesmoothness and consistency of antihypertensive treatmenteffect over 24 h with ABPM The trough-to-peak ratio is theratio between BP reduction achieved by treatment at theend of dosing interval (trough which for drugs adminis-tered once daily means 24 h after the last dose intake) andpeak BP reduction usually achieved a few hours after dose
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
intake [7172] The trough-to-peak ratio is characterized by ahigh degree of variability in individual patients and istherefore not suitable for application to clinical practice[73] The smoothness index is calculated as the ratiobetween the average of hourly BP reductions over 24 hand the standard deviation (SD) of such an average valuethus integrating information on the size of BP reduction bytreatment and on its homogeneity throughout the 24-hperiod [7173] The smoothness index is highest for potentdrugs or drug combinations which also provide the mosthomogeneous BP reduction It is more reproducible thanthe troughpeak ratio [7173] and predicts treatment-induced changes in indices of organ damage includingleft ventricular mass and carotid arterial wall thickness[75w] A recent meta-analysis has provided informationon clinical determinants of the smoothness index suchas age ethnicity sex and smoking [74] The relevance ofthese indices in predicting the impact of treatment onoutcome and the reference values remain to be assessed
5 PROCEDURE
51 Training requirementsThe technique of ABPM is a specialized one and should beapproached with the care reserved for any such procedureAn understanding of the principles of traditional BPmeasurement cuff fitting monitor function and analysisand interpretation of ABPM data is required In practice anurse with an interest and experience in hypertension canmaster the use of ABPM devices after a relatively brieftraining However the interpretation of ABPM profilesrequires experience in the technique which is best pro-vided by the doctor in charge of an ABPM service [19]
52 Fitting an ambulatory blood pressuremonitorTime needs to be given to fitting the monitor and preparingthe patient for the monitoring period if good results are tobe obtained [19] The key to successful ABPM is educatingthe patient on the process of monitoring and the instruc-tions should be explained and printed on a diary card Inclinical practice measurements are preferably performedon a routine working day Although ABPM is best notperformed while patients are admitted to hospital becausehospitalization leads to underestimation of BP and over-diagnosis of nondippers [10] there are occasions such asthe evaluation of severely resistant hypertension andassessment of patients following a stroke when ABPM inhospital may be indicated
The frequency of measurement during the 24-h period isgenerally not more than every 15 min (which could inter-fere with normal activity) nor less than every 30min (whichcould give an inadequate number of measurements) Morefrequent measurements at night may disturb sleep andsleep disturbance has been shown to reduce the prognosticvalue of ABPM [75] To improve reproducibility repetitionof ABPM should be performed on like days for example onroutine working or recreational days A diary card can beused to record symptoms and events that may influenceABPM measurements
orized reproduction of this article is prohibitedwwwjhypertensioncom 1739
OrsquoBrien et al
53 Explanation to patientThe first step is adequate explanation of the procedure in anattempt to allay anxiety especially in nervous patientsPatients having ABPM for the first time should be told thatthere is minor discomfort caused by inflation of the cuff It isimportant to emphasize to the patient to follow hisherusual daily activities but as much as possible to remain stillwith the arm relaxed and not extended or contracted atheart level during each BP measurement [19] It can behelpful to have patients record periods of stress the time ofmeals the time of a siesta the time of going to bed andrising the quality of sleep and the time and type ofdrug ingestion
Box 5 Evaluation of ambulatory blood pressure monitoring data
Definition of daytime and night-time Daytime and night-time intervals are best defined using sleeping times
reported by individual usersrsquo diary cards (awake and asleep periods) Fixed narrow time intervals can be applied by discarding transition
periods between daytime and night-time (eg daytime defined as0900ndash2100 h and night-time 0100ndash0600 h)
Editing requirements Editing is not necessary for calculating average 24-h daytime and
night-time values The ambulatory blood pressure monitoring should be repeated if thefollowing criteria are not met
24-h recording with at least 70 of expected measurements20 valid awake (0900 to 2100 h)7 valid asleep (0100 to 0600 h)Blood pressure measurements at 30-min intervalsFor research purposes at least two valid daytime and one valid
night-time measurement per hour
54 Identification of daytime and night-timeperiods and editing ambulatory blood pressuremonitoring dataOne simple and popular method for identifying daytimeand night-time subperiods is to assess the time of awaken-ing and sleeping from diary card entries Another method isto use a fixed-narrow time interval approach in which forexample the retiring (2101 to 0059 h) and rising (0601 to0859 h) periods (which are subject to considerable vari-ation) are eliminated with the daytime period being from0900 to 2100 h and night-time from 0100 to 0600 h in thisway the variations in the time spent in bed that may existbetween the young and the old and in different culturesare to some extent eliminated from the analysis [176w]This method has the disadvantage of eliminating infor-mation on the white-coat window on the early phase ofnight sleep when dipping can be most evident and onthe early morning surge of BP which may be associatedwith cardiovascular events However these windows canbe analyzed separately for research or if considered import-ant in practice In countries where a daytime siesta ispopular a record of sleeping times both during day andnight is important and ABPM software should be able toadjust for this otherwise there may be underestimation ofthe nocturnal BP dip and overdiagnosis of nondippers[77w]
Many statistical techniques exist for editing ABPMrecords and no one method is ideal [176w] The detec-tion of artefactual readings and the handling of outliervalues (which may or may not be erroneous) have indeedbeen the subject of debate [76w] There are a number ofways of separately analyzing BPs recorded during the dayand night [7678w] Several automatic procedures havebeen proposed to reject outlying measurements based ona univariate multivariate or temporal approach Morecomplex procedures requiring the intervention of theobserver have been proposed but they are time consum-ing and not suitable for clinical practice [77] It has beenshown that rejection of outliers may alter the results ofABPM in individual patients sometimes significantlyaffecting average SBP levels [777879w] Editing pro-cedures can reduce mean systolic ABPM by 4 mmHg incomparison with unedited recordings thereby decreasingthe likelihood of diagnosing sustained hypertension Inone study the prevalence of sustained hypertension wasdecreased by 6ndash10 when several editing methods were
Copyright copy Lippincott Williams amp Wilkins Unaut1740 wwwjhypertensioncom
applied to raw 24-h data [79w] To make the results ofdifferent laboratories comparable common editingcriteria for ABPM should be used The problem is toestablish which of the methods proposed in the literatureprovides the most reliable data While awaiting moreobjective criteria to identify a universally acceptable edit-ing procedure we recommend that editing is not necess-ary for calculating average 24-h daytime and night-timevalues and that only physiologically impossible readingsshould be deleted from recordings However when thereare excessive artefacts in a tracing a repeat recordingrather than editing should be performed Some editingmight be required when focusing on analysis of BPvariability for the quantification of which the presenceof artefacts may introduce appreciable errors If editing isconsidered necessary a method proposed by Casadeiet al [80w] and modified by Winnicki et al [78] providescomparable performance to other proposed editing pro-cedures
There are no firm data on which to base recommen-dations for a satisfactory ABPM recording but the recom-mendation for having at least 70 of expectedmeasurements provides a basic working recommendationfor clinical practice This figure will be influenced by theperiod demarcated as daytime (awake) or night-time(asleep) periods and by the number of measurementsselected (usually 30-min but often 15 or 20-min intervals)In the previous ESH guideline on measurement it wasrecommended that there should be a minimum of 14measurements during the day and seven measurementsat night [1] Having considered what evidence is availableand the practical issues of performing repeat ABPM inpractice it seems reasonable to increase the minimum ofdaytime measurements to 20 while retaining a minimumseven measurements at night based on measurementsbeing performed every 30min and with fixed time periodsbeing used to define day (0900 to 2100 h) and night (0100 to0600 h) [1] (Box 5)
55 The arm for measurementABPM is best measured in the nondominant arm so as tointerfere as little as possible with daily activity unless there
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
has been documented evidence of a difference in BPbetween arms in which case the arm known to have thehigher BP values should be chosen [1] It is commonpractice for BP to be measured by a conventional techniqueat the same time as an ABPM monitor is being fitted and todetermine whether there is a discrepancy between thetechniques However BP variability is such that any suchcomparison has little validity and to determine a significantdifference it is necessary to perform simultaneousmeasurement according to a definitive protocol and thisis not feasible in practice [42] Because of these limitationsthe practice of performing a comparative measurement isnot recommended
56 Selecting the appropriate cuff and bladderThere is unequivocal evidence that either too narrow ortoo short a bladder (undercuffing) will cause overesti-mation of BP so-called lsquocuff hypertensionrsquo and there isgrowing evidence that too wide or too long a bladder(overcuffing) may cause underestimation of BP Under-cuffing has the effect in clinical practice of overdiagnos-ing hypertension and overcuffing leads to hypertensivepatients being diagnosed as normotensive Either even-tuality has serious implications for the epidemiology ofhypertension and for clinical practice [79] It is importanttherefore to select a cuff containing an inflatable bladderof correct length and width for the arm in which ABPM isto be measured All ABPM devices should provide cuffscontaining bladders for small medium and large-sizedarms as recommended in international guidelines[18081] However in many obese individuals the largebladder sizes cannot be used because the arm length istoo short to accommodate the bladder [81w] Anotherproblem is that the cylindrical shape of the commonlyused cuffs does not always wrap snugly around conical-shaped arms in obese and very muscular arms[8282w83w] Recently novel oscillometric homemonitors with cuff technology that allows a singlefixed-size cuff to be used on a wide range of arm circum-ferences have been developed [84wndash87w]
Another issue that needs consideration is the possibilitythat the discomfort caused by inflation of a large cuff inobese patients might cause elevation of BP This issuebecomes more important during ABPM because ofrepeated measurement especially during night-time sleepOscillometric devices for home use that measure BP duringcuff inflation may induce less discomfort because themeasurement is completed before maximal inflation[84w88w] However to date no study has specificallyaddressed this issue
Forearm BP measurement may have to be consideredwhen extreme obesity makes upper arm BP measurementimpossible BP measurements tend to be higher with fore-arm compared with upper arm measurement but meth-odological differences in these studies make it difficult toprovide recommendations for all populations [8389wndash94w] Despite the questionable accuracy of forearm BPmeasurement it may be the only acceptable option forABPM in individuals with very large upper arms providedthe patient is instructed to keep the forearm at heart levelduring measurement [94w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
No wrist devices have been validated for ABPM whereastechnology for continuous beat-to-beat monitoring ofambulatory BP in the finger has been developed usingthe volume-clamp method first described by Penaz [95w]A number of studies that compared this technology withintraarterial or noninvasive BP measurement showedunderestimation of BP particularly diastolic yet it remainsa practical alternative to intraarterial measurement for theevaluation of beat-to-beat BP changes and variability inresearch studies [8496wndash98w]
57 Conditions in which ambulatory bloodpressure monitoring may be difficult toperform
Obese patientsObesity is a well established major risk factor for hyperten-sion with higher prevalence in specific population groupssuch as patients with diabetes mellitus [99w] or OSA [100w]Despite the increasing prevalence of obesity worldwide[101w] and the close link between obesity and hyperten-sion scarce data are available on the application of ABPM inobese and extremely obese individuals ABPM is oftenrequired in these individuals and technical difficultiesshould not exclude them from such a valuable technology[79] The problem of miscuffing in obese pregnant womenmay result in diagnostic discrepancies [85]
Patients with atrial fibrillationBP measurement in patients with atrial fibrillation is lessprecise as this type of arrhythmia is accompanied byincreased beat-to-beat BP variability due to variations inventricular filling time stroke volume and contractilityInternational guidelines [181] recognize the relatively poorprecision of a single BP measurement and recommendrepeated readings in order to improve the accuracy ofestimates Theoretically ABPM should fulfill this stipulationas it provides a relatively high number of readings in a shortperiod of time Unfortunately published evidence regard-ing the role of ABPM in patients with arrhythmias andspecifically in patients with atrial fibrillation is scarce
Patients with atrial fibrillation have been usuallyexcluded from trials using ABPM as well as from validationprotocols of ABPM devices Four studies have addressedthe possible value of ABPM in patients with atrial fibrillation[48w102wndash104w] The evidence from these studiessuggests that ABPM may be useful in these patients pro-vided its limitations are taken into account The proportionof readings with errors the variability of BP and therepeatability coefficients do not appear to be different fromthose in patients in sinus rhythm DBP measured using anABPM monitor in patients with atrial fibrillation appears tobe relatively higher than that obtained with the traditionaloffice measurement or by the same ABPM procedure whenthe patient achieves sinus rhythm This finding is supportedby a review and meta-analysis of studies that validatedelectronic devices in patients with sustained atrial fibrilla-tion which showed consistent overestimation of DBP [52]In spite of this and although larger trials in patients on atrialfibrillation are recommended there is no reason to exclude
orized reproduction of this article is prohibitedwwwjhypertensioncom 1741
OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

OrsquoBrien et al
53 Explanation to patientThe first step is adequate explanation of the procedure in anattempt to allay anxiety especially in nervous patientsPatients having ABPM for the first time should be told thatthere is minor discomfort caused by inflation of the cuff It isimportant to emphasize to the patient to follow hisherusual daily activities but as much as possible to remain stillwith the arm relaxed and not extended or contracted atheart level during each BP measurement [19] It can behelpful to have patients record periods of stress the time ofmeals the time of a siesta the time of going to bed andrising the quality of sleep and the time and type ofdrug ingestion
Box 5 Evaluation of ambulatory blood pressure monitoring data
Definition of daytime and night-time Daytime and night-time intervals are best defined using sleeping times
reported by individual usersrsquo diary cards (awake and asleep periods) Fixed narrow time intervals can be applied by discarding transition
periods between daytime and night-time (eg daytime defined as0900ndash2100 h and night-time 0100ndash0600 h)
Editing requirements Editing is not necessary for calculating average 24-h daytime and
night-time values The ambulatory blood pressure monitoring should be repeated if thefollowing criteria are not met
24-h recording with at least 70 of expected measurements20 valid awake (0900 to 2100 h)7 valid asleep (0100 to 0600 h)Blood pressure measurements at 30-min intervalsFor research purposes at least two valid daytime and one valid
night-time measurement per hour
54 Identification of daytime and night-timeperiods and editing ambulatory blood pressuremonitoring dataOne simple and popular method for identifying daytimeand night-time subperiods is to assess the time of awaken-ing and sleeping from diary card entries Another method isto use a fixed-narrow time interval approach in which forexample the retiring (2101 to 0059 h) and rising (0601 to0859 h) periods (which are subject to considerable vari-ation) are eliminated with the daytime period being from0900 to 2100 h and night-time from 0100 to 0600 h in thisway the variations in the time spent in bed that may existbetween the young and the old and in different culturesare to some extent eliminated from the analysis [176w]This method has the disadvantage of eliminating infor-mation on the white-coat window on the early phase ofnight sleep when dipping can be most evident and onthe early morning surge of BP which may be associatedwith cardiovascular events However these windows canbe analyzed separately for research or if considered import-ant in practice In countries where a daytime siesta ispopular a record of sleeping times both during day andnight is important and ABPM software should be able toadjust for this otherwise there may be underestimation ofthe nocturnal BP dip and overdiagnosis of nondippers[77w]
Many statistical techniques exist for editing ABPMrecords and no one method is ideal [176w] The detec-tion of artefactual readings and the handling of outliervalues (which may or may not be erroneous) have indeedbeen the subject of debate [76w] There are a number ofways of separately analyzing BPs recorded during the dayand night [7678w] Several automatic procedures havebeen proposed to reject outlying measurements based ona univariate multivariate or temporal approach Morecomplex procedures requiring the intervention of theobserver have been proposed but they are time consum-ing and not suitable for clinical practice [77] It has beenshown that rejection of outliers may alter the results ofABPM in individual patients sometimes significantlyaffecting average SBP levels [777879w] Editing pro-cedures can reduce mean systolic ABPM by 4 mmHg incomparison with unedited recordings thereby decreasingthe likelihood of diagnosing sustained hypertension Inone study the prevalence of sustained hypertension wasdecreased by 6ndash10 when several editing methods were
Copyright copy Lippincott Williams amp Wilkins Unaut1740 wwwjhypertensioncom
applied to raw 24-h data [79w] To make the results ofdifferent laboratories comparable common editingcriteria for ABPM should be used The problem is toestablish which of the methods proposed in the literatureprovides the most reliable data While awaiting moreobjective criteria to identify a universally acceptable edit-ing procedure we recommend that editing is not necess-ary for calculating average 24-h daytime and night-timevalues and that only physiologically impossible readingsshould be deleted from recordings However when thereare excessive artefacts in a tracing a repeat recordingrather than editing should be performed Some editingmight be required when focusing on analysis of BPvariability for the quantification of which the presenceof artefacts may introduce appreciable errors If editing isconsidered necessary a method proposed by Casadeiet al [80w] and modified by Winnicki et al [78] providescomparable performance to other proposed editing pro-cedures
There are no firm data on which to base recommen-dations for a satisfactory ABPM recording but the recom-mendation for having at least 70 of expectedmeasurements provides a basic working recommendationfor clinical practice This figure will be influenced by theperiod demarcated as daytime (awake) or night-time(asleep) periods and by the number of measurementsselected (usually 30-min but often 15 or 20-min intervals)In the previous ESH guideline on measurement it wasrecommended that there should be a minimum of 14measurements during the day and seven measurementsat night [1] Having considered what evidence is availableand the practical issues of performing repeat ABPM inpractice it seems reasonable to increase the minimum ofdaytime measurements to 20 while retaining a minimumseven measurements at night based on measurementsbeing performed every 30min and with fixed time periodsbeing used to define day (0900 to 2100 h) and night (0100 to0600 h) [1] (Box 5)
55 The arm for measurementABPM is best measured in the nondominant arm so as tointerfere as little as possible with daily activity unless there
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
has been documented evidence of a difference in BPbetween arms in which case the arm known to have thehigher BP values should be chosen [1] It is commonpractice for BP to be measured by a conventional techniqueat the same time as an ABPM monitor is being fitted and todetermine whether there is a discrepancy between thetechniques However BP variability is such that any suchcomparison has little validity and to determine a significantdifference it is necessary to perform simultaneousmeasurement according to a definitive protocol and thisis not feasible in practice [42] Because of these limitationsthe practice of performing a comparative measurement isnot recommended
56 Selecting the appropriate cuff and bladderThere is unequivocal evidence that either too narrow ortoo short a bladder (undercuffing) will cause overesti-mation of BP so-called lsquocuff hypertensionrsquo and there isgrowing evidence that too wide or too long a bladder(overcuffing) may cause underestimation of BP Under-cuffing has the effect in clinical practice of overdiagnos-ing hypertension and overcuffing leads to hypertensivepatients being diagnosed as normotensive Either even-tuality has serious implications for the epidemiology ofhypertension and for clinical practice [79] It is importanttherefore to select a cuff containing an inflatable bladderof correct length and width for the arm in which ABPM isto be measured All ABPM devices should provide cuffscontaining bladders for small medium and large-sizedarms as recommended in international guidelines[18081] However in many obese individuals the largebladder sizes cannot be used because the arm length istoo short to accommodate the bladder [81w] Anotherproblem is that the cylindrical shape of the commonlyused cuffs does not always wrap snugly around conical-shaped arms in obese and very muscular arms[8282w83w] Recently novel oscillometric homemonitors with cuff technology that allows a singlefixed-size cuff to be used on a wide range of arm circum-ferences have been developed [84wndash87w]
Another issue that needs consideration is the possibilitythat the discomfort caused by inflation of a large cuff inobese patients might cause elevation of BP This issuebecomes more important during ABPM because ofrepeated measurement especially during night-time sleepOscillometric devices for home use that measure BP duringcuff inflation may induce less discomfort because themeasurement is completed before maximal inflation[84w88w] However to date no study has specificallyaddressed this issue
Forearm BP measurement may have to be consideredwhen extreme obesity makes upper arm BP measurementimpossible BP measurements tend to be higher with fore-arm compared with upper arm measurement but meth-odological differences in these studies make it difficult toprovide recommendations for all populations [8389wndash94w] Despite the questionable accuracy of forearm BPmeasurement it may be the only acceptable option forABPM in individuals with very large upper arms providedthe patient is instructed to keep the forearm at heart levelduring measurement [94w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
No wrist devices have been validated for ABPM whereastechnology for continuous beat-to-beat monitoring ofambulatory BP in the finger has been developed usingthe volume-clamp method first described by Penaz [95w]A number of studies that compared this technology withintraarterial or noninvasive BP measurement showedunderestimation of BP particularly diastolic yet it remainsa practical alternative to intraarterial measurement for theevaluation of beat-to-beat BP changes and variability inresearch studies [8496wndash98w]
57 Conditions in which ambulatory bloodpressure monitoring may be difficult toperform
Obese patientsObesity is a well established major risk factor for hyperten-sion with higher prevalence in specific population groupssuch as patients with diabetes mellitus [99w] or OSA [100w]Despite the increasing prevalence of obesity worldwide[101w] and the close link between obesity and hyperten-sion scarce data are available on the application of ABPM inobese and extremely obese individuals ABPM is oftenrequired in these individuals and technical difficultiesshould not exclude them from such a valuable technology[79] The problem of miscuffing in obese pregnant womenmay result in diagnostic discrepancies [85]
Patients with atrial fibrillationBP measurement in patients with atrial fibrillation is lessprecise as this type of arrhythmia is accompanied byincreased beat-to-beat BP variability due to variations inventricular filling time stroke volume and contractilityInternational guidelines [181] recognize the relatively poorprecision of a single BP measurement and recommendrepeated readings in order to improve the accuracy ofestimates Theoretically ABPM should fulfill this stipulationas it provides a relatively high number of readings in a shortperiod of time Unfortunately published evidence regard-ing the role of ABPM in patients with arrhythmias andspecifically in patients with atrial fibrillation is scarce
Patients with atrial fibrillation have been usuallyexcluded from trials using ABPM as well as from validationprotocols of ABPM devices Four studies have addressedthe possible value of ABPM in patients with atrial fibrillation[48w102wndash104w] The evidence from these studiessuggests that ABPM may be useful in these patients pro-vided its limitations are taken into account The proportionof readings with errors the variability of BP and therepeatability coefficients do not appear to be different fromthose in patients in sinus rhythm DBP measured using anABPM monitor in patients with atrial fibrillation appears tobe relatively higher than that obtained with the traditionaloffice measurement or by the same ABPM procedure whenthe patient achieves sinus rhythm This finding is supportedby a review and meta-analysis of studies that validatedelectronic devices in patients with sustained atrial fibrilla-tion which showed consistent overestimation of DBP [52]In spite of this and although larger trials in patients on atrialfibrillation are recommended there is no reason to exclude
orized reproduction of this article is prohibitedwwwjhypertensioncom 1741
OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Guideline
has been documented evidence of a difference in BPbetween arms in which case the arm known to have thehigher BP values should be chosen [1] It is commonpractice for BP to be measured by a conventional techniqueat the same time as an ABPM monitor is being fitted and todetermine whether there is a discrepancy between thetechniques However BP variability is such that any suchcomparison has little validity and to determine a significantdifference it is necessary to perform simultaneousmeasurement according to a definitive protocol and thisis not feasible in practice [42] Because of these limitationsthe practice of performing a comparative measurement isnot recommended
56 Selecting the appropriate cuff and bladderThere is unequivocal evidence that either too narrow ortoo short a bladder (undercuffing) will cause overesti-mation of BP so-called lsquocuff hypertensionrsquo and there isgrowing evidence that too wide or too long a bladder(overcuffing) may cause underestimation of BP Under-cuffing has the effect in clinical practice of overdiagnos-ing hypertension and overcuffing leads to hypertensivepatients being diagnosed as normotensive Either even-tuality has serious implications for the epidemiology ofhypertension and for clinical practice [79] It is importanttherefore to select a cuff containing an inflatable bladderof correct length and width for the arm in which ABPM isto be measured All ABPM devices should provide cuffscontaining bladders for small medium and large-sizedarms as recommended in international guidelines[18081] However in many obese individuals the largebladder sizes cannot be used because the arm length istoo short to accommodate the bladder [81w] Anotherproblem is that the cylindrical shape of the commonlyused cuffs does not always wrap snugly around conical-shaped arms in obese and very muscular arms[8282w83w] Recently novel oscillometric homemonitors with cuff technology that allows a singlefixed-size cuff to be used on a wide range of arm circum-ferences have been developed [84wndash87w]
Another issue that needs consideration is the possibilitythat the discomfort caused by inflation of a large cuff inobese patients might cause elevation of BP This issuebecomes more important during ABPM because ofrepeated measurement especially during night-time sleepOscillometric devices for home use that measure BP duringcuff inflation may induce less discomfort because themeasurement is completed before maximal inflation[84w88w] However to date no study has specificallyaddressed this issue
Forearm BP measurement may have to be consideredwhen extreme obesity makes upper arm BP measurementimpossible BP measurements tend to be higher with fore-arm compared with upper arm measurement but meth-odological differences in these studies make it difficult toprovide recommendations for all populations [8389wndash94w] Despite the questionable accuracy of forearm BPmeasurement it may be the only acceptable option forABPM in individuals with very large upper arms providedthe patient is instructed to keep the forearm at heart levelduring measurement [94w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
No wrist devices have been validated for ABPM whereastechnology for continuous beat-to-beat monitoring ofambulatory BP in the finger has been developed usingthe volume-clamp method first described by Penaz [95w]A number of studies that compared this technology withintraarterial or noninvasive BP measurement showedunderestimation of BP particularly diastolic yet it remainsa practical alternative to intraarterial measurement for theevaluation of beat-to-beat BP changes and variability inresearch studies [8496wndash98w]
57 Conditions in which ambulatory bloodpressure monitoring may be difficult toperform
Obese patientsObesity is a well established major risk factor for hyperten-sion with higher prevalence in specific population groupssuch as patients with diabetes mellitus [99w] or OSA [100w]Despite the increasing prevalence of obesity worldwide[101w] and the close link between obesity and hyperten-sion scarce data are available on the application of ABPM inobese and extremely obese individuals ABPM is oftenrequired in these individuals and technical difficultiesshould not exclude them from such a valuable technology[79] The problem of miscuffing in obese pregnant womenmay result in diagnostic discrepancies [85]
Patients with atrial fibrillationBP measurement in patients with atrial fibrillation is lessprecise as this type of arrhythmia is accompanied byincreased beat-to-beat BP variability due to variations inventricular filling time stroke volume and contractilityInternational guidelines [181] recognize the relatively poorprecision of a single BP measurement and recommendrepeated readings in order to improve the accuracy ofestimates Theoretically ABPM should fulfill this stipulationas it provides a relatively high number of readings in a shortperiod of time Unfortunately published evidence regard-ing the role of ABPM in patients with arrhythmias andspecifically in patients with atrial fibrillation is scarce
Patients with atrial fibrillation have been usuallyexcluded from trials using ABPM as well as from validationprotocols of ABPM devices Four studies have addressedthe possible value of ABPM in patients with atrial fibrillation[48w102wndash104w] The evidence from these studiessuggests that ABPM may be useful in these patients pro-vided its limitations are taken into account The proportionof readings with errors the variability of BP and therepeatability coefficients do not appear to be different fromthose in patients in sinus rhythm DBP measured using anABPM monitor in patients with atrial fibrillation appears tobe relatively higher than that obtained with the traditionaloffice measurement or by the same ABPM procedure whenthe patient achieves sinus rhythm This finding is supportedby a review and meta-analysis of studies that validatedelectronic devices in patients with sustained atrial fibrilla-tion which showed consistent overestimation of DBP [52]In spite of this and although larger trials in patients on atrialfibrillation are recommended there is no reason to exclude
orized reproduction of this article is prohibitedwwwjhypertensioncom 1741
OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

OrsquoBrien et al
such patients from ABPM procedures Some novel oscillo-metric devices have an embedded algorithm for automateddetection of atrial fibrillation during routine BP measure-ment which appears to have high diagnostic accuracy[105wndash107w] However to date this function has not beentested in ABPM devices (Box 6)
6 CLINICAL INDICATIONS FORAMBULATORY BLOOD PRESSUREMONITORING
61 Role of ambulatory blood pressuremonitoring in the diagnosis of hypertensionIn reaching a consensus on the clinical indicationsfor ABPM we have relied on the recommendations ofinternational guidelines published from 2000 to 2013
Copyright copy Lippincott Williams amp Wilkins Un
Box 6 Requirements for obtaining a satisfactory ambulatory blood pressuremeasurement
Basic requirements Patients must be capable of understanding and coping with the device Ambulatory blood pressure measurement should be performed
preferably on a routine working day Repeat ambulatory blood pressure measurements should be on
like days for example on routine working or recreational days 10ndash15 min needed to program and fit the device depending on
first or follow-up recording Patient should be relaxed in quiet roomFitting the monitor Ensure that there is sufficient battery power Enter patient details into monitor Initialize monitor Select frequency of measurement ndash usually 15ndash30 min for day and
night Inactivate measurement LCD display Apply cuff to nondominant arm Choose appropriate cuff with bladder length to encircle 80ndash100
of arm circumference Center of bladder should be over the brachial artery Place cuff on bare arm with tubing passing upward around patientrsquos
neck to be connected to the monitor on the waist Perform trial measurement to check working and to familiarize
patient with the monitor and bleeping soundsAdvice to the patient Procedure should be explained and instructions printed on a
diary card Patients should be told to follow their usual daily activities but to
remain still during measurement with the arm relaxed at heart level Instruct patient to place monitor on the bed or beneath the
pillow at night Warn patient not to take a shower or bath Advise patient not to drive but if this is necessary to stop driving
if possible during measurement Mark the brachial artery so that if the cuff becomes loose the patient
can refit it Give patient oral and written instructions and a diary card to record
the time of drug intake the time of rising and going to bedand any symptoms
Instruct patient how to switch off the monitor in case ofmalfunctioning such as repeated inflation
If appropriate instruct patient on how to remove and inactivatemonitor after 25 h
Removing the monitor Usually removed by operator but patients can be instructed to
remove monitor and send it to the operatorrsquos center Download the data from the monitor 24-h minimum 70 of expected number of readings and at least 20
valid daytime and seven night-time blood pressure measurements If minimum requirement not met measurement should be repeated
though suboptimal data can be helpful
Box 7 Clinical indications for ambulatory blood pressure monitoring
Identifying white-coat hypertension phenomenaWhite-coat hypertension in untreated patientsWhite-coat effect in treated or untreated patientsFalse-resistant hypertension in treated patients
Identifying masked hypertension phenomenaMasked hypertension in untreated patientsMasked uncontrolled hypertension in treated patients
Identifying abnormal 24-h blood pressure patternsDaytime hypertension
Siesta dippingpostprandial hypotensionNocturnal hypertension
Dipping statusMorning hypertension and morning blood pressure surgeObstructive sleep apneaIncreased blood pressure variability
Assessment of treatmentIncreased on-treatment blood pressure variabilityAssessing 24-h blood pressure controlIdentifying true-resistant hypertension
Assessing hypertension in the elderlyAssessing hypertension in children and adolescentsAssessing hypertension in pregnancyAssessing hypertension in high-risk patientsIdentifying ambulatory hypotensionIdentifying blood pressure patterns in Parkinsonrsquos diseaseEndocrine hypertension
1742 wwwjhypertensioncom
aut
[12127286286ndash94] All these guidelines were in agree-ment that ABPM is indicated for the exclusion or confir-mation of suspected white-coat hypertension all but onewere in agreement that ABPM is indicated for the confir-mation of a diagnosis of hypotension and to identifypatients with resistant hypertension 80 recommendedABPM to assess drug efficacy over the 24-h period andfor the assessment of the nocturnal dipping status and morethan half recommended ABPM to identify masked hyper-tension The most recent NICE guideline published in 2011stated unequivocally that ABPM should be offered to any-one suspected of having hypertension by virtue of havinghad an elevated conventional BP measurement [4] Giventhe strong recommendations supporting the greater use ofABPM in clinical practice it is now incumbent on eachcountry to provide ABPM services to patients who willbenefit from improved management of hypertension asoutlined below (Box 7)
62 White-coat phenomena
621 White-coat hypertension (isolated clinichypertension)In clinical practice the main indication for performingABPM is to determine accurately an individualrsquos BP statusThe main advantages of ABPM over other forms of BPmeasurement are to identify untreated patients who havehigh BP readings in the office but normal readings duringusual daily activities outside of this setting and to identifyvarying 24-h BP profiles Pickering et al [95108w] intro-duced the term lsquowhite-coat hypertensionrsquo to describe thiscondition which is now commonly defined as a BP readingat least 140 mmHg systolic andor at least 90mmHg diastolicin the clinicoffice and a mean awake ambulatory SBPDBPless than 135 and less than 85mmHg [28] A comparison
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Guideline
between the ambulatory BP and office BP obtained inroutine clinical practice by the physician ordering theABPM gives the best measure of the degree of white-coathypertension which is present [11] The first few ambulatoryBP readings taken in the ABPM unit are often higher thansubsequent readings because of transient anxiety experi-enced by some patients in this setting [109w] This increasein BP is usually not as great as that seen in the office of thereferring physician [96] Readings obtained during the firsthour of the ABPM recording have sometimes beenexcluded from the calculation of the mean awake ambu-latory BP as they may reflect the patientrsquos white-coat effectand not their BP during usual daily activities
In recent years there has been increased interest in BPreadings obtained using ABPM during sleep Nocturnal BPis now recognized to be superior to daytime BP in predict-ing cardiovascular risk [1697] The traditional definition ofwhite-coat hypertension is based on an elevated office BPwith a normal BP during the awake period on ABPM inuntreated patients [1110w] but because of the contributionof asleep BP as a predictor of outcome it seems illogical toexclude this period from consideration and it is proposedthat an alternative definition of white-coat hypertensionmight encompass patients with office readings at least 14090mmHg and a mean 24-h BP less than 13080 mmHg
White-coat hypertension is virtually eliminated if officereadings are obtained through use of automated BPmeasurement in the office waiting room [96] In circum-stances in which ABPM is not available home BP readingsperformed according to standardized protocols have alsobeen used to diagnose white-coat hypertension [28]
Findings in a number of clinical outcome studies indifferent populations have clarified the clinical significanceof white-coat hypertension Almost invariably individualswith elevated office BP who have normal average readingson ABPM were at much lower risk of experiencing cardio-vascular events than patients whose clinic and ambulatoryBP were both elevated [97ndash102111w] Nonetheless insome clinical outcome studies [98ndash102111w112w]patients with this condition may have a slightly increasednonsignificant cardiovascular risk compared with normo-tensive controls In almost every instance in which thisincrease has been noted the ambulatory BP of the white-coat hypertensive patients was higher than in the normo-tensive individuals even though mean ambulatory BPvalues for both groups were in the normotensive rangeThis difference in ambulatory BP could account for theslightly higher cardiovascular risk in the white-coathypertension group
There are other reasons why white-coat hypertensionmay not be a completely benign condition The risk ofdeveloping sustained hypertension in subsequent yearsmay be increased in patients with white-coat hypertension[100102112w] Furthermore some studies have associatedwhite-coat hypertension with an increased prevalence oftarget organ damage [113wndash115w] Once again the meanambulatory BP in the control groups in these studies hasgenerally been lower compared with the white-coat hyper-tensive patients Although a meta-analysis performed by theIDACO group did not find any increase in cardiovascularevents in patients with white-coat hypertension there was a
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
significant increase in risk in specific subgroups includingmen and patients with diabetes [111w] This meta-analysisalso clearly showed that any increased risk of experiencinga future cardiovascular event because of white-coat hyper-tension was quite small and substantially lower than the riskseen with either persistent hypertension or masked hyper-tension
Nonetheless some patients initially identified as havingwhite-coat hypertension will go on to develop sustainedhypertension in future years Whether the percentage doingso exceeds the expected number of normotensive individ-uals with comparable 24-h ambulatory BP values but nor-mal office BP remains uncertain The potential risks ofwhite-coat hypertension may also be confounded by anti-hypertensive drug therapy prescribed because of the highoffice BP readings So far it has not been possible toaccount for this factor in the analysis of cardiovascular riskin patients with white-coat hypertension who are receivingmedical care over many years in the community
Several hypertension guidelines [2728] recommendABPM when white-coat hypertension is suspected Thebasis for selecting patients with possible white-coat hyper-tension is somewhat imprecise as there are no character-istics that have a high specificity for diagnosing thiscondition Findings in several studies [95116wndash118w] havesuggested that the prevalence of white-coat hypertensionin untreated patients with uncomplicated hypertensionincreases in the presence of the following office SBP140ndash159mmHg or DBP 90ndash99mmHg female sex increas-ing age nonsmokers hypertension of recent onset limitednumber of BP measurements in the office and normal leftventricular mass Nonetheless the clinical characteristicsassociated with white-coat hypertension are not sufficientlystrong to estimate accurately the probability of an individualpatient having this condition Perhaps the best reason tosuspect white-coat hypertension is when patients with highoffice BP report normal BP readings taken at home or in thecommunity Indeed a high out-of-office reading is theprimary indication for reimbursement of ABPM by govern-ment insurance plans in some countries such as the UnitedStates
Although the above-mentioned characteristics increasethe probability that a patient has white-coat hypertension ithas to be emphasized that no one group seems to beexempt from white-coat hypertension it may affect theyoung the elderly normotensive individuals and pregnantwomen The consequences of failing to identify thecondition are considerable Young (and indeed the notso young) people may be penalized for insurance andpension policies and for employment Life-long treatmentmay be prescribed unnecessarily and if antihypertensivemedication is given to people whose 24-h pressures arenormal they may be made unwell by the adverse effects ofmedication In the elderly in whom white-coat hyper-tension is common the inappropriate use of drugs mayhave serious debilitating consequences It is recommendedthat people with white-coat hypertension should havethe diagnosis confirmed in 3ndash6 months and be followedat yearly intervals with ABPM or home BP monitoringso as to detect whether and when sustained hypertensionoccurs [121]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1743
OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

OrsquoBrien et al
Children with white-coat hypertension tend to have ahigher left ventricular mass index than confirmed normo-tensive individuals [117w119w] but there are no long-termfollow-up studies of children with white-coat hypertension
Due to the limited association of white-coat hyperten-sion with the alerting reaction to the presence of a phys-ician it has been suggested that the alternative termlsquoisolated office hypertensionrsquo is more appropriate becausethe combination of elevated BP in the office and normalambulatory BP levels may depend also on factors other thanthe alerting reaction to the doctorrsquos visit [103120w] Thesame considerations apply to white-coat hypertensionidentified through home BP monitoring [121w]
With the prevalence of white-coat hypertension in thecommunity being as high as 20ndash25 [88] it is extremelyimportant to make an accurate diagnosis of this conditionThis goal can best be achieved by performing 24-h ABPMandor home BP monitoring in all patients with uncompli-cated stage 1 and 2 essential hypertension before prescrib-ing antihypertensive drug therapy ABPM is cost-effective[38] in that it reduces healthcare expenditures by decreasingdrug costs physician visits and adverse effects due toinappropriate treatment Finally after the initial diagnosisof white-coat hypertension has been made patients shouldhave their BP status monitored more carefully preferablywith home BP or automated office BP If a trend towardhigher BP readings is noted then ABPM should be repeatedin order to detect the development of sustained hyper-tension [21]
622 White-coat effectlsquoWhite-coat effectrsquo is defined as the rise in BP that occurs inthe medical environment regardless of the daytime ABPMlevel or the use of antihypertensive drugs In generallsquowhite-coat effectrsquo is present when the office BP is higherthan the awake ambulatory BP White-coat hypertensionexists if the office BP is high and the awake ambulatory BPis normal in a patient not yet receiving antihypertensivemedication Thus white-coat hypertension could be seenas a subset of white-coat effect although it has beendemonstrated that office BP values higher than ambulatoryBP may occur independently of a white-coat effect [103]
Patients with an office BP at least 20mmHg systolicandor 10 mmHg diastolic higher than the awake ambulat-ory BP have been designated as having a lsquoclinically import-ant rsquo white-coat effect [4122w] This term was introduced todistinguish these patients from those who have only a smalldifference between office and ambulatory BP a differencetoo small to warrant changes in drug therapy Treatedpatients with office BP at least 14090 mmHg and awakeambulatory BP less than 13585 mmHg could be designatedas having lsquopseudo-resistant hypertension due to white-coateffectrsquo [104] as they have apparent hypertension basedupon office readings but are actually normotensiveWhite-coat effect is a recognized cause of lsquofalse-resistantrsquohypertension [105] and may be present in anyone treatedfor hypertension regardless of the number of drugs beingtaken [104] Other patients may have only mild hyper-tension based on ABPM and yet appear to have severehypertension due to a white-coat effect on office BP[103121w123w]
Copyright copy Lippincott Williams amp Wilkins Unaut1744 wwwjhypertensioncom
It is important to detect those patients with white-coateffect in order to avoid prescribing unnecessary antihyper-tensive drug therapy which could lead to serious adverseeffects White-coat effect is more likely to occur in indivi-duals with the same characteristics as those associatedwith white-coat hypertension (see above) White-coateffect may be somewhat diminished if office BP is recordedwith strict adherence to guidelines for proper BP measure-ment [11]
The white-coat effect may not be necessarily the same asthe increase in BP which has been reported when a physi-cian enters the room to see the patient sometimes called anlsquoalerting reactionrsquo [106] The presence of a physician (or anyother health professional) does increase BP but it is only onecomponent of the white-coat effect Even if the patient isalone and records BP by activating an automated sphyg-momanometer there may still be some alerting effectpresent [124w] although this has not been found whensystematically checking the effect of self-BP measurementson intraarterial BP simultaneously recorded [125w] Thusfactors related to the patient such as anxiety the presence ofa doctor or nurse and the medical environment may eachcontribute to higher office BP readings with nurses usuallyhaving a smaller BP effect than doctors [126w]
In some patients the pressor response to the clinicenvironment can be directly observed in the ABPM tracingwith BP values characteristically higher in the initial (andpossibly also final) portion of the recording (when thepatient attends the clinic for device placement and removal)and may be influenced by the alerting circumstances of theofficeclinic environment compared with the remainingperiod [109w]
Patients who have exhibited a white-coat effect mayneed to be followed with other types of BP readings suchas automated office BP home BP and repeat ABPMespecially if a trend to higher BP readings is noted
63 Masked phenomena
631 Masked hypertensionThe usual definition of masked hypertension is that it ispresent in patients who have a normal office BP 14090mmHg or less with elevated daytime BP on ABPM orhome BP at least 13585 mmHg [107108] However as withthe definition of white-coat hypertension it is inappropriateto exclude nocturnal BP and the definition should beextended to include also 24-h BP values at least 13080mmHg Concerning the question as to whether or notthe definition of masked hypertension should be appliedalso to individuals on BP-lowering medication and not onlyto untreated individuals it is clearly inappropriate to applythe term to individuals on treatment because by definitionhypertension has been diagnosed and cannot be lsquomaskedrsquoTherefore when treated individuals have a normal officeBP but persistently elevated ambulatory or home BP theterm lsquomasked uncontrolled hypertensionrsquo is more appro-priate (see next paragraph)
The problem for clinical practice is how to identify andmanage these patients which may affect 10 of the generalpopulation [108] The phenomenon might be suspected inindividuals who have had an elevated clinic BP at some
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Box 8 Definition of white-coat and masked hypertension phenomena
White-coat hypertensionUntreated patients with elevated office blood pressure14090 mmHg and
24-h ambulatory blood pressure measurement lt13080 mmHg andAwake ambulatory blood pressure measurement lt13585 mmHg
andSleep measurement lt12070 mmHg orHome blood pressure lt13585 mmHg
Masked hypertensionUntreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Masked uncontrolled hypertensionTreated patients with office blood pressure lt14090 mmHg and24-h ambulatory blood pressure measurement 13080 mmHg
andorAwake ambulatory blood pressure measurement 13585 mmHg
andorSleep measurement 12070 mmHg orHome blood pressure 13585 mmHg
Diagnoses require confirmation by repeating ambulatory blood pressuremonitoring or home blood pressure monitoring within 3ndash6 months dependingon the individualrsquos total cardiovascular riskAmbulatory blood pressure values obtained in the clinic during the first or lasthour of a 24-h recording may also partly reflect the white-coat effect
Guideline
time in young individuals with normal or high-normaloffice BP and left ventricular hypertrophy in individualswith a family history of hypertension in both parentspatients with multiple risk factors for cardiovascular dis-ease and perhaps diabetic patients It appears to be moreprevalent in patients of male sex in younger age groups(including children and adolescents) in those with higherawake heart rate or high cholesterol levels and in obesepatients and those who smoke and ingest alcohol [127w]Exercise-induced hypertension also increases the likeli-hood of masked hypertension [128w129w] The BPincrease at night triggered by OSA has been noted tocontribute to masked hypertension in particular whenthe latter condition is defined by considering 24-h ornight-time ABPM values
Adults with masked hypertension have increased riskof target organ damage and cardiovascular morbidity[199101108] In adolescents masked hypertension hasbeen shown to be present in nearly 40 of individualsand these were more than twice as likely to have aparental history of hypertension and to have a higherambulatory pulse rate BMI and greater prevalence of leftventricular hypertrophy than normotensive individuals[109134w]
Although no definitive data are available masked hy-pertension has been estimated to occur in approximately10ndash30 of individuals with the variability in these figuresdepending on the diagnostic criteria used to identify thiscondition and on the characteristics of the populationexamined [108109]
A study of the agreement between ABPM and home BPin the diagnosis of masked hypertension has shown thatmore patients with masked hypertension are detected byABPM (14) than by home BP (11) [110] The maskedhypertension pattern has been shown to persist in approxi-mately 50 of children with 10 of them progressing frommasked hypertension to sustained hypertension during amedian follow-up period of 37 months [109134w] In asmall group of adults with masked hypertension 71 ofindividuals continued to manifest the phenomenon atrepeat ABPM whereas 80 of those with masked hyper-tension on repeat ABPM had masked hypertension orsustained hypertension on the first ABPM [135w] A studyevaluating masked hypertension over three ABPMs within6 months showed a declining prevalence of the pheno-menon with repeated ABPMs [136w]
632 Masked uncontrolled hypertensionAs mentioned above it is not appropriate to apply the termmasked hypertension to patients receiving antihypertensivetreatment because if a patient is receiving BP-loweringdrugs hypertension can no longer be defined as lsquomaskedrsquoWhat could be lsquomaskedrsquo however is poor control of BPwith medication during the day or night-time periods inspite of normal office BPs This phenomenon which is bestdenoted by the term lsquomasked uncontrolled hypertensionrsquo isdeserving of separate consideration because patients needto be identified so that they can be offered effective thera-peutic BP control throughout the 24-h period to prevent thecardiovascular consequences of uncontrolled hypertension[71111] (Box 8)
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
64 Abnormal 24-h blood pressure patternsAbnormal BP patterns include a number of conditionscharacterized by different behavior of BP during the day-time andor the night-time One such condition is anincrease in short-term BP variability within the 24 h whichcan only be assessed with 24-h ABPM More details on thisBP phenotype and on its clinical relevance are provided inSection 651
641 Daytime hypertensionThedaytimewindow ofABPM is theperiod when the patientis away from the medical environment and engaged in usualactivities [10] For almost all patients with hypertension BPsduring thiswindoware lower thanofficeor clinic BP [26112]HoweverBPsduring thisperiodare subject toeffectsofworkand environmental stress activity body and arm movementand the effect of exercise and other activities such as drivingall of whichmay have an influence on the average level of BPrecorded as well as on BP variability [137w] These effects arelargely absent in BP measured during the nocturnal period[16138w] Systolicanddiastolichypertension is thecommon-est daytime pattern in patients aged less than 60 years [1113]Average daytime BP is superior to clinic BP in predictingoutcome but inferior to nocturnal BP in some populationsand conditions [16] For example white-coat hypertensiontends to be more common inwomen isolated systolic hyper-tension and nocturnal hypertension tend to occur morefrequently in the elderly and isolated diastolic hypertensionis found more frequently in younger individuals [113]
642 Siesta dipping and postprandial hypotensionThe classical siesta is common in some Mediterraneansocieties but many patients particularly the elderly takea rest after lunch and this may be accompanied by sleep thecombination of a postprandial fall in BP together with
orized reproduction of this article is prohibitedwwwjhypertensioncom 1745
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
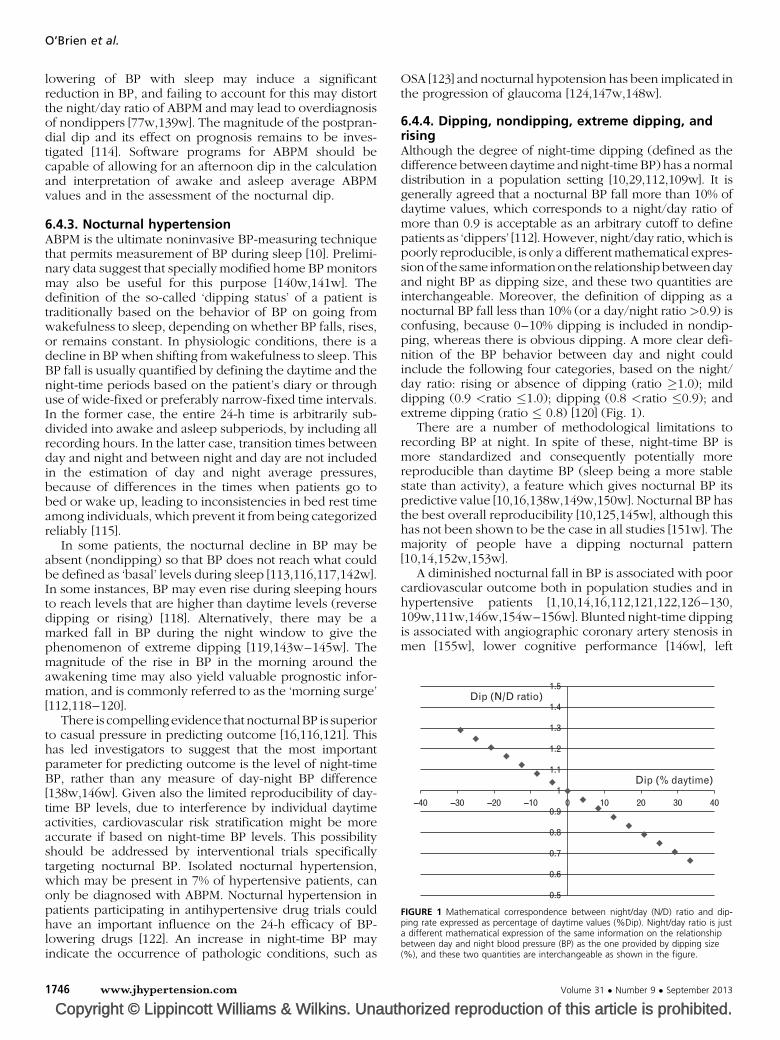
15
14
13
12
11
1
09
08
07
06
05
4030
Dip ( daytime)
Dip (ND ratio)
20100ndash10ndash20ndash30ndash40
FIGURE 1 Mathematical correspondence between nightday (ND) ratio and dip-ping rate expressed as percentage of daytime values (Dip) Nightday ratio is justa different mathematical expression of the same information on the relationshipbetween day and night blood pressure (BP) as the one provided by dipping size() and these two quantities are interchangeable as shown in the figure
OrsquoBrien et al
lowering of BP with sleep may induce a significantreduction in BP and failing to account for this may distortthe nightday ratio of ABPM and may lead to overdiagnosisof nondippers [77w139w] The magnitude of the postpran-dial dip and its effect on prognosis remains to be inves-tigated [114] Software programs for ABPM should becapable of allowing for an afternoon dip in the calculationand interpretation of awake and asleep average ABPMvalues and in the assessment of the nocturnal dip
643 Nocturnal hypertensionABPM is the ultimate noninvasive BP-measuring techniquethat permits measurement of BP during sleep [10] Prelimi-nary data suggest that specially modified home BP monitorsmay also be useful for this purpose [140w141w] Thedefinition of the so-called lsquodipping statusrsquo of a patient istraditionally based on the behavior of BP on going fromwakefulness to sleep depending on whether BP falls risesor remains constant In physiologic conditions there is adecline in BP when shifting from wakefulness to sleep ThisBP fall is usually quantified by defining the daytime and thenight-time periods based on the patientrsquos diary or throughuse of wide-fixed or preferably narrow-fixed time intervalsIn the former case the entire 24-h time is arbitrarily sub-divided into awake and asleep subperiods by including allrecording hours In the latter case transition times betweenday and night and between night and day are not includedin the estimation of day and night average pressuresbecause of differences in the times when patients go tobed or wake up leading to inconsistencies in bed rest timeamong individuals which prevent it from being categorizedreliably [115]
In some patients the nocturnal decline in BP may beabsent (nondipping) so that BP does not reach what couldbe defined as lsquobasalrsquo levels during sleep [113116117142w]In some instances BP may even rise during sleeping hoursto reach levels that are higher than daytime levels (reversedipping or rising) [118] Alternatively there may be amarked fall in BP during the night window to give thephenomenon of extreme dipping [119143wndash145w] Themagnitude of the rise in BP in the morning around theawakening time may also yield valuable prognostic infor-mation and is commonly referred to as the lsquomorning surgersquo[112118ndash120]
There is compelling evidence that nocturnalBP is superiorto casual pressure in predicting outcome [16116121] Thishas led investigators to suggest that the most importantparameter for predicting outcome is the level of night-timeBP rather than any measure of day-night BP difference[138w146w] Given also the limited reproducibility of day-time BP levels due to interference by individual daytimeactivities cardiovascular risk stratification might be moreaccurate if based on night-time BP levels This possibilityshould be addressed by interventional trials specificallytargeting nocturnal BP Isolated nocturnal hypertensionwhich may be present in 7 of hypertensive patients canonly be diagnosed with ABPM Nocturnal hypertension inpatients participating in antihypertensive drug trials couldhave an important influence on the 24-h efficacy of BP-lowering drugs [122] An increase in night-time BP mayindicate the occurrence of pathologic conditions such as
Copyright copy Lippincott Williams amp Wilkins Unaut1746 wwwjhypertensioncom
OSA [123] and nocturnal hypotension has been implicated inthe progression of glaucoma [124147w148w]
644 Dipping nondipping extreme dipping andrisingAlthough the degree of night-time dipping (defined as thedifference between daytime and night-time BP) has a normaldistribution in a population setting [1029112109w] It isgenerally agreed that a nocturnal BP fall more than 10 ofdaytime values which corresponds to a nightday ratio ofmore than 09 is acceptable as an arbitrary cutoff to definepatients as lsquodippersrsquo [112] However nightday ratio which ispoorly reproducible is only a different mathematical expres-sionof the same informationon the relationshipbetweendayand night BP as dipping size and these two quantities areinterchangeable Moreover the definition of dipping as anocturnal BP fall less than 10 (or a daynight ratio gt09) isconfusing because 0ndash10 dipping is included in nondip-ping whereas there is obvious dipping A more clear defi-nition of the BP behavior between day and night couldinclude the following four categories based on the nightday ratio rising or absence of dipping (ratio 10) milddipping (09 ltratio 10) dipping (08 ltratio 09) andextreme dipping (ratio 08) [120] (Fig 1)
There are a number of methodological limitations torecording BP at night In spite of these night-time BP ismore standardized and consequently potentially morereproducible than daytime BP (sleep being a more stablestate than activity) a feature which gives nocturnal BP itspredictive value [1016138w149w150w] Nocturnal BP hasthe best overall reproducibility [10125145w] although thishas not been shown to be the case in all studies [151w] Themajority of people have a dipping nocturnal pattern[1014152w153w]
A diminished nocturnal fall in BP is associated with poorcardiovascular outcome both in population studies and inhypertensive patients [1101416112121122126ndash130109w111w146w154wndash156w] Blunted night-time dippingis associated with angiographic coronary artery stenosis inmen [155w] lower cognitive performance [146w] left
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Box 9 Patterns of disrupted diurnal blood pressure variation identified byambulatory blood pressure monitoring
Dipping Nocturnal blood pressure fall gt10 of daytimevalues or
Nightday blood pressure ratio lt09 andgt08 ndash normal diurnal blood pressurepattern
Reduceddipping
Nocturnal blood pressure fall from 1 to 10of daytime values or
Nightday blood pressure ratio lt1 andgt09 ndash reduced diurnal blood pressurepattern
Nondipping andrising
No reduction or increase in nocturnal bloodpressure or
Nightday ratio 1 ndash associated with poorcardiovascular risk
Extreme dipping Marked nocturnal blood pressure fall gt20of daytime values or
Nightday ratio lt08 ndash debatable cardiovascularrisk
Nocturnalhypertension
Increased absolute level of night-time bloodpressure
Associated with increased cardiovascular risk ndashmay indicate obstructive sleep apnea
Morning surge Excessive blood pressure elevation rising in morning
Definitions thresholds and prognostic impactdebatable
The classic definition of nondipping (nocturnal blood pressure falllt10 or nightday ratio gt09) may be criticized because lsquoreduceddippingrsquo is in effect a form of lsquonondippingrsquo
Guideline
ventricular hypertrophy [128156w] and renal damage[122129] This association parallels the finding that for each10-mmHg increase in mean night-time SBP the mortalityrisk increases by 21 [15122] A recent meta-analysissuggests that both the quantity and quality of sleep mayalso predict cardiovascular outcome thereby raising thequestion as to how sleep may influence nocturnal BP [130]
A nocturnal lsquorisingrsquo pattern occurs when BP rises abovedaytime pressures rather than falling during the night thusresulting in a nightday BP ratio more than 1 These patientshave the worst cardiovascular prognosis both for strokeand cardiac events [117]
Finally a marked nocturnal fall in BP arbitrarily definedas a night-time BP reduction more than 20 of daytimevalues is defined as lsquoextreme dippingrsquo The evidence for anassociation of extreme dipping pattern with a poor out-come is not strong but patients with atherosclerotic diseasemay be at risk of nonfatal ischemic stroke and silentmyocardial ischemia if excessive nocturnal BP reductionis induced by injudicious BP-lowering treatment [31117]Extreme dipping is closely associated with an excessivemorning surge in BP which may make the interpretation ofthe latter phenomenon more complex [118] Reduced dip-ping at night and even more so a rising pattern may beregarded as a marker of the occurrence of pathologicconditions at night such as OSA [123]
With regard to prognosis it has been suggested thatrisers have the worst prognosis whereas the prognosis isnot necessarily different between dippers and mild dippersand between dippers and extreme dippers [120]
Investigation of nocturnal BP behavior using ABPM mayprovide information on the presence of salt sensitivity acondition associated with increased sympathetic activityand an increased cardiovascular risk [131132157wndash159w]
There are thus many patterns of nocturnal BP behaviorand although these may be associated with an adverseprognosis there has been relatively little study into thebenefits of therapeutic modification of nocturnal patternsHowever there is overall agreement that the reduction ofnocturnal hypertension should be an objective so as toachieve BP control over the entire 24-h period
645 Morning hypertension and morning bloodpressure surgeIn the presence of a nocturnal BP reduction a morningincrease in BP at awakening and even more so whenresuming daytime activities has to be regarded as a physio-logic phenomenon However some studies have suggestedthat a more pronounced morning BP surge quantified byABPM may carry negative prognostic implications[119133134160wndash166w] but this has not been confirmedin other investigations [135136] Circadian variations inother biochemical and physiological parameters besidesBP (such as heart rate plasma cortisol plasma catechol-amines platelet aggregability etc) help to explain astriggering factors the increased occurrence of acute cardi-ovascular events in early morning hours [137167w]
Given the methodological problems in determining themorning surge that include its association with the degreeof night-time BP fall different methods for its quantifi-cation poor reproducibility and the variety of definitions
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
used in different studies its relevance to clinical practiceis limited
A measure of the morning surge based on a mathematicalestimate of the rate and amplitudeof the rise which has beenshown to be higher in hypertensive patients and in patientswith white-coat hypertension is modifiable by some BP-lowering drugs suggesting that the measure may be theor-etically useful to highlight those individuals at greatest risk ofcardiovascular events and for determining an importanteffect of antihypertensive therapy [134166w] (Box 9)
646 Obstructive sleep apneaOSA is one of a number of sleep-related breathing disordersthat include habitual snoring central sleep apnea and OSAsyndrome (OSA accompanied by daytime symptoms andsleep hypoventilation syndrome) [138168w] It has beenknown since polysomnographic recordings were firstdescribed that alternating obstructive apnea and hyper-ventilation episodes during sleep are accompanied by acutechanges in nocturnal cardiovascular parameters whichinclude wide oscillations in BP and heart rate [139]
In addition to increasing the risk for car accidentsworsening the quality of life mood and cognitive perform-ance OSA is an additional and independent risk factor forcardiovascular diseases [140] There is increasing evidencethat OSA and hypertension as well as the need of theircombined treatment should be considered in patients withrefractory hypertension and a nondipping BP profile[2728123141ndash143169wndash185w] Although this associationmay be partly mediated by coexisting risk factors such asobesity there is evidence supporting an independent roleof OSA in the pathogenesis of both night-time and daytimehypertension even if this issue is still matter of debate[143174w175w]
orized reproduction of this article is prohibitedwwwjhypertensioncom 1747
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
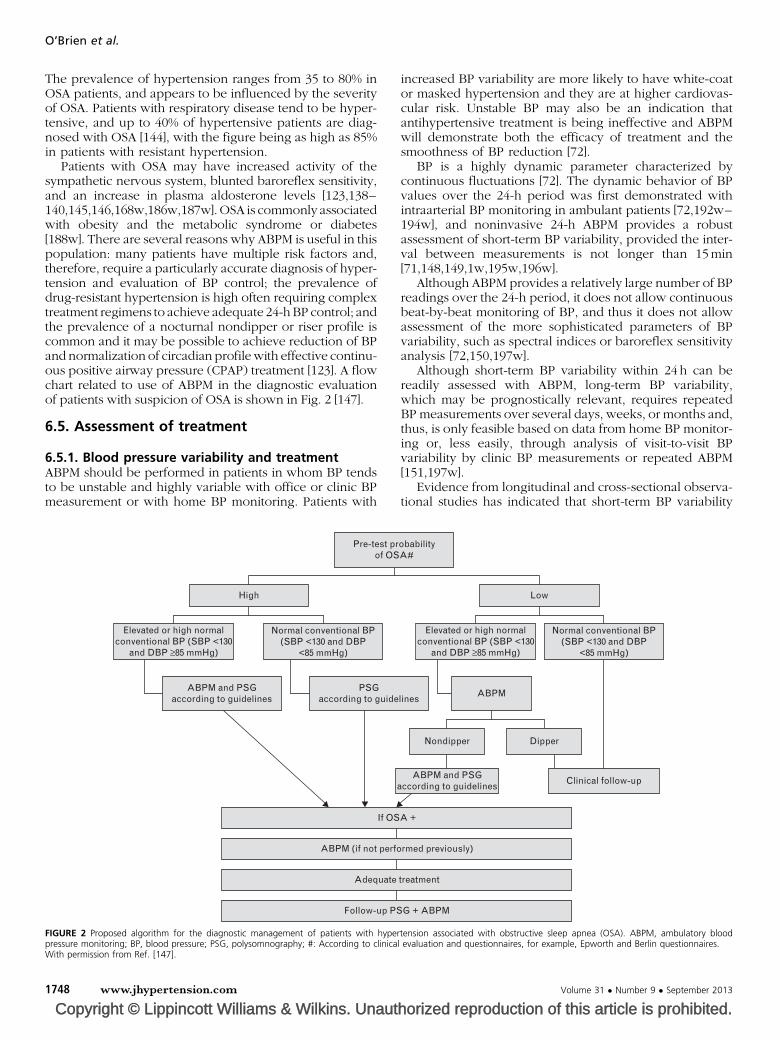
OrsquoBrien et al
The prevalence of hypertension ranges from 35 to 80 inOSA patients and appears to be influenced by the severityof OSA Patients with respiratory disease tend to be hyper-tensive and up to 40 of hypertensive patients are diag-nosed with OSA [144] with the figure being as high as 85in patients with resistant hypertension
Patients with OSA may have increased activity of thesympathetic nervous system blunted baroreflex sensitivityand an increase in plasma aldosterone levels [123138ndash140145146168w186w187w] OSA is commonly associatedwith obesity and the metabolic syndrome or diabetes[188w] There are several reasons why ABPM is useful in thispopulation many patients have multiple risk factors andtherefore require a particularly accurate diagnosis of hyper-tension and evaluation of BP control the prevalence ofdrug-resistant hypertension is high often requiring complextreatment regimens to achieve adequate 24-hBP control andthe prevalence of a nocturnal nondipper or riser profile iscommon and it may be possible to achieve reduction of BPand normalization of circadian profile with effective continu-ous positive airway pressure (CPAP) treatment [123] A flowchart related to use of ABPM in the diagnostic evaluationof patients with suspicion of OSA is shown in Fig 2 [147]
65 Assessment of treatment
651 Blood pressure variability and treatmentABPM should be performed in patients in whom BP tendsto be unstable and highly variable with office or clinic BPmeasurement or with home BP monitoring Patients with
Copyright copy Lippincott Williams amp Wilkins Unaut
Pre-test prof OS
High
ABPM (if not perfo
Adequate
Follow-up PS
If OS
ABPM and PSGaccording to guidelines
a
PSGaccording to guide
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
FIGURE 2 Proposed algorithm for the diagnostic management of patients with hyperpressure monitoring BP blood pressure PSG polysomnography According to clinicalWith permission from Ref [147]
1748 wwwjhypertensioncom
increased BP variability are more likely to have white-coator masked hypertension and they are at higher cardiovas-cular risk Unstable BP may also be an indication thatantihypertensive treatment is being ineffective and ABPMwill demonstrate both the efficacy of treatment and thesmoothness of BP reduction [72]
BP is a highly dynamic parameter characterized bycontinuous fluctuations [72] The dynamic behavior of BPvalues over the 24-h period was first demonstrated withintraarterial BP monitoring in ambulant patients [72192wndash194w] and noninvasive 24-h ABPM provides a robustassessment of short-term BP variability provided the inter-val between measurements is not longer than 15min[711481491w195w196w]
Although ABPM provides a relatively large number of BPreadings over the 24-h period it does not allow continuousbeat-by-beat monitoring of BP and thus it does not allowassessment of the more sophisticated parameters of BPvariability such as spectral indices or baroreflex sensitivityanalysis [72150197w]
Although short-term BP variability within 24 h can bereadily assessed with ABPM long-term BP variabilitywhich may be prognostically relevant requires repeatedBP measurements over several days weeks or months andthus is only feasible based on data from home BP monitor-ing or less easily through analysis of visit-to-visit BPvariability by clinic BP measurements or repeated ABPM[151197w]
Evidence from longitudinal and cross-sectional observa-tional studies has indicated that short-term BP variability
horized reproduction of this article is prohibited
obabilityA
Low
Normal conventional BP(SBP lt130 and DBP
lt85 mmHg)
ABPM
rmed previously)
treatment
G + ABPM
Dipper
Clinical follow-up
A +
Nondipper
ABPM and PSGccording to guidelines
lines
Elevated or high normalconventional BP (SBP lt130
and DBP ge85 mmHg)
tension associated with obstructive sleep apnea (OSA) ABPM ambulatory bloodevaluation and questionnaires for example Epworth and Berlin questionnaires
Volume 31 Number 9 September 2013
Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Guideline
within the 24-h period may contribute to cardiovascular risk[133135149ndash154192w195wndash207w] Evidence that cor-rection of deranged BP variability has a positive impacton prognosis is only present in experimental animals [208w]and there are no consistent data as yet on the benefitsderiving from reduced short-term BP variability in humans
ABPM has been used to assess the effects of therapeuticstrategies on reducing nocturnal BP and there is someevidence suggesting that administration of antihypertensivedrugs in the evening rather than in the morning may restorenormal nocturnal dipping and that cardiovascular risk maybe reduced but these results need to be confirmed byfurther trials [155209wndash211w] Treatment effects on short-term BP variability may also be assessed by calculatingvarious ABPM indices to quantify the persistence andhomogeneity of a BP-lowering effect (see Section4234) [71737475w] Visit-to-visit office BP variabilityand ambulatory BP variability which predict cardiovascularoutcomes may also provide a means to assess drug treat-ment efficacy [151156154w197w206w212w]
In conclusion based on the available evidence short-term BP variability might be considered for risk stratificationin population and cohort studies However it does not yetrepresent a parameter for routine use in clinical practicebecause of the current lack of generally accepted thresholdsseparating normal from pathologic BP variability levels andbecause controlled intervention studies are still needed toestablish whether a treatment-induced reduction in short-term BP variability will be accompanied by a reduction incardiovascular events and mortality
652 Assessing efficacy of blood pressure controlABPM may be useful in the management of hypertensionwith drug therapy [1213w214w] In a well controlled studyadjustment of antihypertensive treatment based on eitherABPM or clinic BP measurement resulted in less intensivedrug treatment in patients managed with ABPM despitecomparable BP control in both groups Furthermore leftventricular mass was not increased in patients managedwith ABPM even though they received less antihyperten-sive medication [33] ABPM also provides a better assess-ment of the response to treatment than does clinic BP theefficacy of treatment without the white-coat effect can beascertained excessive drug effect and the occurrence ofsymptoms can be determined the duration of BP controlover the 24-h period and the consequences of missed doseson BP can be demonstrated [215w]
The inability of clinic BP to assess antihypertensive drugeffect on the nocturnal BP dip or on the morning surge wasillustrated in two prospective observational studies intreated hypertensive patients who appeared to have wellcontrolled BP on routine clinic measurements but haduncontrolled hypertension during the early morning hours[157158]
The antihypertensive effect of drug therapy can also bequantified by applying specific mathematical indices suchas the trough-to-peak ratio and the smoothness index toABPM data [71216w217w] These indices have differentcharacteristics and different indications The smoothnessindex combines information on BP lowering size and onhomogeneity of BP reduction over the 24-h time it is highly
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
reproducible and is associated with rate of organ damageprogression in individual patients Trough-to-peak ratiowhich only quantifies the distribution of antihypertensivedrug effect over 24 h is best when averaged for groups ofpatients and is characterized by a very low reproducibilityin individual patients Therefore its use is mostly confinedto pharmacologic research
ABPM can also demonstrate the excessive effects of BP-lowering treatment in particular at the time of symptomsduring the 24-h period and especially at the time of peakeffect of the drug which can be related to episodes ofhypotension [1014]
653 Resistant hypertensionHypertensive patients whose clinic BP remains persistentlyhigh despite taking three or more antihypertensive drugs atmaximum dose including a diuretic are defined as havingresistant hypertension and may account for 10 of hyper-tensive patients referred to specialized clinics [105218wndash220w] Despite extensive diagnostic work-up in manycases it is not possible to find a potentially correctablecause for the elevated BP even though compliance tomedication seems to be adequate [28221w] Patients whosehypertension is uncontrolled are more likely to have targetorgan damage and a higher long-term cardiovascular riskthan are patients whose BP is controlled For a better riskstratification BP measurement outside the clinical environ-ment is recommended in order to exclude the existence of apersistent white-coat effect which might erroneouslysuggest the occurrence of resistant hypertension when infact BP is controlled in daily life [22728159]
In a large Spanish registry about one-third of 8295patients with resistant hypertension based on office BPmeasurements had normal ABPMs suggesting the presenceof a white-coat effect or lsquofalsersquo resistance [159] which hasalso been termed lsquopseudo-resistant hypertensionrsquo [104105]Rather than create another category it is best to regardpatients with this phenomenon as exhibiting a white-coateffect and that ABPM has simply demonstrated that they donot have resistant hypertension The reverse phenomenonmay also be detected with ABPM whereby patients onmaximal drug therapy have low office but elevated ambu-latory BP [222w]
The recommendation to use out-of-office BP measure-ments in resistant hypertension is based on the evidencethat ABPM gives better prognostic information than officemeasurement [160ndash163] One study showed that in patientswith resistant hypertension with or without a previouscardiovascular event ABPM was an independent markerof risk for new cardiovascular events suggesting that ABPMwas useful in stratifying the risk in patients with resistanthypertension [163] Two studies [161162] have confirmedthese results and reinforced the superiority of ABPM overoffice BP for stratifying risk Also home BP monitoring maybe useful in identifying patients with lsquotrue-resistantrsquo andlsquofalse-resistantrsquo hypertension although this approach atpresent cannot provide information on night-time BP [162]
66 Hypertension in the elderlyThe elderly can show striking variability of BP with periodsof hypotension interspersed with hypertension on ABPM
orized reproduction of this article is prohibitedwwwjhypertensioncom 1749
OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

OrsquoBrien et al
[164] This pattern which is often indicative of autonomicfailure is important to identify so that treatment can betailored to take account of such fluctuations in BP [204w]There are four major age-related changes in the ABPMprofile in the elderly white-coat hypertension is morecommon than in younger adults there is a predominantincrease in 24-h SBP with a mild decrease in 24-h DBP after60ndash70 years of age and as a result an increase in 24-h pulsepressure and the prevalence of 24-h isolated systolic hy-pertension there is exaggerated ambulatory BP variabilityand morning BP surge and disrupted diurnal BP variation(nondipping) and postural and postprandial hypotensionare more common in the elderly [88165166]
Outcome studies in the elderly have shown 24-h SBP tobe more closely associated with both fatal and nonfatalcardiovascular events andor total mortality than office BP[126167168223wndash227w] and 24-h ambulatory pulse pres-sure has also been associated with cardiovascular disease[169228w] with associations being closer for stroke thancoronary artery disease [170]
The physiological nocturnal BP fall gradually diminisheswith increasing age Nondippers and risers with highernocturnal than daytime BP are more frequently found inthe elderly and these BP patterns are more closely associ-ated with target organ damage cardiovascular events andmortality [169ndash171228w] In addition nondipping andnocturnal hypertension in the elderly are associated withcognitive dysfunction and impaired physical activity [172]In elderly diabetic hypertensive patients the absence of theusual decline in nocturnal heart rate is associated with anincrease in total and cardiovascular mortality [229w] and asynergistic effect of BP and heart rate nondipping oncardiovascular events has been reported in elderly hyper-tensive patients [173] The quality of sleep in elderly patientscan be affected by concomitant conditions such as prostatichypertrophy sleep apnea and sleep fragmentation [230w]and in such cases nocturnal BP loses some of its prognosticsignificance [75]
Whether extreme dipping with marked nocturnal BP fallis associated with increased cardiovascular risk is uncertainwith some studies showing increased risk [173174231w]and others failing to show an association [88175] The riskof extreme dipping in the elderly may be partially explainedby its association with a steeper morning surge in BP whichfrequently accompanies an excessive nocturnal fall in BP[134] The disrupted circadian BP variation in the elderly isalso associated with orthostatic BP dysregulation [232w]and reverse dipping is associated with orthostatic hypo-tension [176]
BP variability significantly increases with age predom-inantly due to baroreflex failure and increased arterialstiffness and may advance target organ damage and triggercardiovascular events in the elderly patients [177]
An increase in the physiological morning BP surge isdetermined by advancing age and higher 24-h BP level Theexaggerated morning BP surge can only be identified byABPM and is associated with increased risk of subclinicaltarget organ damage cardiovascular events and cardiovas-cular and total mortality independently of age and average24-h BP [164233w] However a recent study did not showan excess risk of cardiovascular morbidity and mortality in
Copyright copy Lippincott Williams amp Wilkins Unaut1750 wwwjhypertensioncom
hypertensive patients with exaggerated morning BP surgeemphasizing on the contrary the increased risk associatedwith nondipping or rising BP pattern at night [136]
Daytime sleep (siesta) may modify the diurnal variation ofBP as well as of the cardiovascular risk in the elderly [233w]Two-peak diurnal BP variation (morning and evening) instroke onset was observed in elderly patients who had asiesta which occurred in parallel with a two-peak diurnalvariation in BP heart rate and physical activity suggestingthat an abrupt change in physical activity is not only a majordeterminant of the diurnal variation of BP but might also bean important triggering factor for a stroke event [178]
Postural and postprandial hypotension which are morecommon in the elderly [153233w] and which can beexaggerated by antihypertensive drugs such as diureticsor alpha-blockers and also by noncardiovascular drugssuch as neuroleptics and antidepressants are best diag-nosed with ABPM
67 Hypertension in children and adolescentsThere is increasing interest in pediatric hypertensionbecause of evidence for increased prevalence of hyperten-sion among children and adolescents [109179] In 2009 theESH published guidelines for hypertension management inchildren and adolescents [109] which are consistent withthe 2004 US Task Force Guidelines on pediatric hyperten-sion [179] Moreover a scientific statement on ABPM inchildren and adolescents has been published by the Amer-ican Heart Association [180]
According to both European and American recommen-dations ABPM is now increasingly recognized as beingindispensable for the diagnosis and management of hyper-tension in children and adolescents [109179180] In chil-dren ABPM is particularly useful for the detection of white-coat and also masked hypertension [109179180] whichmay be more common than white-coat hypertensionMasked hypertension appears to be a forerunner of sus-tained hypertension and has been associated with leftventricular hypertrophy [109180134w] Moreover in chil-dren and adolescents with type-1 diabetes ABPM is avaluable tool for the evaluation of nocturnal hypertensionwhich appears to be associated with the development ofmicroalbuminuria [181]
The clinical use of ABPM depends on the use of normalBP ranges as reference values In adults the most mean-ingful reference values for both office BP and ABPM havebeen based on long-term prospective studies relating BP tocardiovascular morbidity and mortality rates In children itis very difficult if not impossible to validate diagnosticreference values based on morbidity and mortality becauseof the very low incidence of clinical events in this agegroup Therefore reference values for normal and highoffice and ambulatory BP have been developed from thedistribution of BP readings in thousands of childrengrouped by age sex and height [182183234w] In futureit may be possible to refine these values by relating signs oftarget organ involvement such as left ventricular mass tothe ambulatory BP
BP measurement in children presents a number of diffi-culties and variability of BP is greater than in adults with theresult that any single reading is less likely to represent the
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
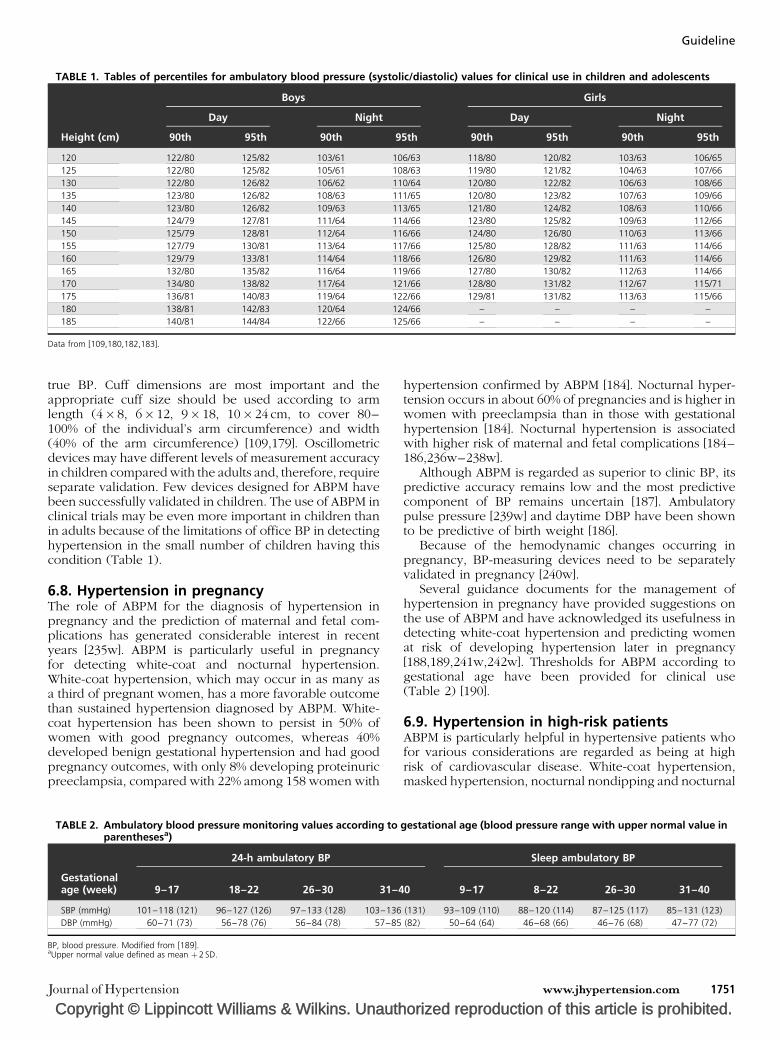
TABLE 1 Tables of percentiles for ambulatory blood pressure (systolicdiastolic) values for clinical use in children and adolescents
Boys Girls
Day Night Day Night
Height (cm) 90th 95th 90th 95th 90th 95th 90th 95th
120 12280 12582 10361 10663 11880 12082 10363 10665
125 12280 12582 10561 10863 11980 12182 10463 10766
130 12280 12682 10662 11064 12080 12282 10663 10866
135 12380 12682 10863 11165 12080 12382 10763 10966
140 12380 12682 10963 11365 12180 12482 10863 11066
145 12479 12781 11164 11466 12380 12582 10963 11266
150 12579 12881 11264 11666 12480 12680 11063 11366
155 12779 13081 11364 11766 12580 12882 11163 11466
160 12979 13381 11464 11866 12680 12982 11163 11466
165 13280 13582 11664 11966 12780 13082 11263 11466
170 13480 13882 11764 12166 12880 13182 11267 11571
175 13681 14083 11964 12266 12981 13182 11363 11566
180 13881 14283 12064 12466 ndash ndash ndash ndash
185 14081 14484 12266 12566 ndash ndash ndash ndash
Data from [109180182183]
Guideline
true BP Cuff dimensions are most important and theappropriate cuff size should be used according to armlength (4 8 6 12 9 18 10 24 cm to cover 80ndash100 of the individualrsquos arm circumference) and width(40 of the arm circumference) [109179] Oscillometricdevices may have different levels of measurement accuracyin children compared with the adults and therefore requireseparate validation Few devices designed for ABPM havebeen successfully validated in children The use of ABPM inclinical trials may be even more important in children thanin adults because of the limitations of office BP in detectinghypertension in the small number of children having thiscondition (Table 1)
68 Hypertension in pregnancyThe role of ABPM for the diagnosis of hypertension inpregnancy and the prediction of maternal and fetal com-plications has generated considerable interest in recentyears [235w] ABPM is particularly useful in pregnancyfor detecting white-coat and nocturnal hypertensionWhite-coat hypertension which may occur in as many asa third of pregnant women has a more favorable outcomethan sustained hypertension diagnosed by ABPM White-coat hypertension has been shown to persist in 50 ofwomen with good pregnancy outcomes whereas 40developed benign gestational hypertension and had goodpregnancy outcomes with only 8 developing proteinuricpreeclampsia compared with 22 among 158 women with
Copyright copy Lippincott Williams amp Wilkins Unauth
TABLE 2 Ambulatory blood pressure monitoring values according toparenthesesa)
24-h ambulatory BP
Gestationalage (week) 9ndash17 18ndash22 26ndash30 31ndash4
SBP (mmHg) 101ndash118 (121) 96ndash127 (126) 97ndash133 (128) 103ndash136
DBP (mmHg) 60ndash71 (73) 56ndash78 (76) 56ndash84 (78) 57ndash85
BP blood pressure Modified from [189]aUpper normal value defined as mean thorn2 SD
Journal of Hypertension
hypertension confirmed by ABPM [184] Nocturnal hyper-tension occurs in about 60 of pregnancies and is higher inwomen with preeclampsia than in those with gestationalhypertension [184] Nocturnal hypertension is associatedwith higher risk of maternal and fetal complications [184ndash186236wndash238w]
Although ABPM is regarded as superior to clinic BP itspredictive accuracy remains low and the most predictivecomponent of BP remains uncertain [187] Ambulatorypulse pressure [239w] and daytime DBP have been shownto be predictive of birth weight [186]
Because of the hemodynamic changes occurring inpregnancy BP-measuring devices need to be separatelyvalidated in pregnancy [240w]
Several guidance documents for the management ofhypertension in pregnancy have provided suggestions onthe use of ABPM and have acknowledged its usefulness indetecting white-coat hypertension and predicting womenat risk of developing hypertension later in pregnancy[188189241w242w] Thresholds for ABPM according togestational age have been provided for clinical use(Table 2) [190]
69 Hypertension in high-risk patientsABPM is particularly helpful in hypertensive patients whofor various considerations are regarded as being at highrisk of cardiovascular disease White-coat hypertensionmasked hypertension nocturnal nondipping and nocturnal
orized reproduction of this article is prohibited
gestational age (blood pressure range with upper normal value in
Sleep ambulatory BP
0 9ndash17 8ndash22 26ndash30 31ndash40
(131) 93ndash109 (110) 88ndash120 (114) 87ndash125 (117) 85ndash131 (123)
(82) 50ndash64 (64) 46ndash68 (66) 46ndash76 (68) 47ndash77 (72)
wwwjhypertensioncom 1751
OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

OrsquoBrien et al
hypertension and increased BP variability are more fre-quent and pronounced in these patients than in low-riskpatients with high BP These phenomena are best detectedwith ABPM which is merited on the grounds that identi-fication of these BP characteristics may improve the man-agement of patients already exposed at a high risk ofcardiovascular events
691 DiabetesABPM is particularly useful in diabetic patients for charac-terizing the nocturnal profile because a nondipping orhypertensive nocturnal BP pattern is more common indiabetic patients and is a strong predictor of future cardi-ovascular events Nondipping may reflect autonomic dys-function but other pathophysiological mechanisms suchas OSA are commonly encountered in obese patients withtype 2 diabetes [15171191] The nondipping pattern foundin diabetic patients may be associated with short duration ofsleep [243w]
Some studies have shown that the reproducibility of BPvalues in diabetic patients is better with ABPM than withoffice BP in particular the reproducibility of nondipping ishigher in diabetic patients than in the general population[244w] The prevalence of white-coat hypertension mayalso be lower in this population especially in patients withdiabetic nephropathy [245w] On the other hand maskedhypertension may be present in one out of two patientswith type 2 diabetes [246w] further increasing the risk ofbrain and kidney [247w] and possibly also cardiac damage[248w249w]
An increase in SBP during the night may antedate thedevelopment of microalbuminuria in young patients withtype 1 diabetes and themagnitude of the nocturnal dip in BPpredicts the development of microalbuminuria [181250w]Although carefully taken clinic BP can identify many patientswith diabetes in need of treatment ABPM can identify asignificant number of patients with lsquomasked hypertensionrsquoeither during the day or the night-time [15191]
Apart from dayndashnight BP changes ABPM is able toprovide information on other features of BP variability thatmay be of interest in diabetic patients and have clinicalrelevance An increase in overall BP variability commonlyexpressed as a standard deviation of average 24-h day ornight BP values may be a marker of deranged autonomiccontrol in patients with diabetic autonomic neuropathy[251w] and may be an independent predictor of cardio-vascular complications Postprandial hypotension which isoften associated with autonomic neuropathy may bepresent in diabetic patients [252w] Morning hypertensionwhich is an adverse marker in nondiabetic patients iscommon in diabetic patients and in one study it was shownto predict the rate of progression of diabetic nephropathy[159w]
ABPM provides a number of other relevant parametersover and above average SBP and DBP values which can beuseful in diabetic patients These include a rough estimateof heart rate variability which when decreased mayindicate diabetic neuropathy pulse pressure which whenincreased may be a surrogate marker of arterial wallstiffening and the AASI which predicts cardiovascularevents and organ damage [253w]
Copyright copy Lippincott Williams amp Wilkins Unaut1752 wwwjhypertensioncom
An important application of ABPM in hypertension isrelated to its ability to evaluate the changes in BP inducedby antihypertensive therapy with greater accuracy and in amuch more detailed fashion than is the case for office BP[31] Because adequate BP control is especially important indiabetic patients it becomes essential to verify the appro-priateness of antihypertensive treatment with ABPM ABPMidentifies patients with masked uncontrolled hypertension(see Section 632) or patients with true-resistant hyperten-sion ABPM also allows for assessment of the efficacy oftreatment on particularly important periods of the circadiancycle such as the night-time and morning Studies usingABPM in diabetic patients treated for hypertension haveshown that restoring nocturnal BP fall in diabetic non-dippers may be a difficult task with conventional antihy-pertensive therapy [254w] and that oral drugs used in type 2diabetes in particular thiazolidinediones may have abeneficial effect on 24-h BP level and may also improvethe dayndashnight profile in diabetic [255wndash258w] or predia-betic patients [259w260w] By the same token hypogly-cemic drugs may have adverse off-target effects on BP thatcan be identified with ABPM [192193]
The use of ABPM in diabetic patients to determine theassociation between BP variability and the prevalence ofmicrovascular and macrovascular complications merits fur-ther study [261wndash263w] ABPM devices use oscillometryalmost exclusively to measure BP but altered vessel wallproperties in diabetic patients may differ from those innondiabetic patients Therefore validation of devices forABPM should be performed separately in diabetic patients[264w] An important and still unresolved issue is thedefinition of ABPM cut-off points for hypertension diag-nosis and therapeutic targets in diabetic patients Suchthresholds are fairly well defined for patients at low-to-intermediate risk based on the results of outcome studieswhereas no similar definitions are available in diabetes[194]
692 StrokeABPM can be useful both in monitoring the acute effects ofischemic and hemorrhagic stroke and in predicting out-come in stroke survivors A frequent finding in strokepatients is the loss of nocturnal BP dipping which maylead to worse target organ damage and facilitate recurrentstroke Moreover BP recorded during sleep or in the earlymorning is more predictive of first or recurring strokeevents than daytime SBP especially in the elderly [195]Conventional BP recordings may therefore be inadequateto precisely identify these changes in BP over 24 h Thereare limited data on circadian rhythm in acute stroke patients[265w266w] Both hypertensive and normotensive patientshave been shown to have similar percentages of abnormalcircadian rhythm of SBP and more nondipping and reversedipping patterns when assessed with repeat ABPM [195]However there seem to be differences in the ABPM profilein acute stroke subtypes of different etiology which mighthave implications in the optimal management of poststrokehypertension [266w] In the West Birmingham Stroke Proj-ect patients with ischemic stroke showed a loss of thediurnal BP rhythm whereas a trend toward reverse dippingwas seen in patients with intracerebral hemorrhage [267w]
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Guideline
Alterations in the 24-h profile on ABPM were associatedwith a worse prognosis including a higher rate of strokein the Spanish Cardiorisk Study [268w] Moreover a closeassociation has been reported between stroke andincreased 24-h BP variability An increase in short-termBP variability and in morning BP surge may increase therisk for stroke and cardiovascular events [153203w] Insummary both hypertensive and normotensive survivorsof stroke develop a chronic disruption of circadianrhythm of BP which can vary with the stroke typeModest preservation of nocturnal BP dipping and thephysiological circadian pattern of BP may induce aprotective effect on cerebral circulation in patientswith ischemic stroke Also modulation of short-termBP variability may be beneficial in stroke patients butthe value of tentative lowering of BP to maintain thephysiological dipping phenomena after acute stroke hasyet to be addressed in large randomized controlled trials[269w]
693 Coronary heart diseaseOnly a few studies have addressed the usefulness of ABPMin patients with coronary heart disease In most cases asignificant relationship was found between coronary heartdisease prevalence and either nondipping or increasedambulatory pulse pressure [155w270w] ABPM can alsobe useful in predicting prognosis in patients with coronaryheart disease [196]
694 Chronic kidney diseaseHypertension is highly prevalent in CKD further increasingthe already high cardiovascular risk associated with thiscondition Early identification of hypertension and achieve-ment of tight BP control is essential for prevention ofcardiovascular disease in patients with CKD
BP control in CKD presents some unique challengesPatients often show marked alterations disappearance oreven inversion of the circadian BP pattern Loss of thenormal nocturnal decline in BP is present in about 50of patients with CKD and in up to 80 in ESRD [271w]Office BP is misleading even when standardized and this isreflected by the high prevalence of white-coat hypertension(28ndash30) and masked hypertension (26ndash34) [27] InESRD the marked reductions in intravascular volumeimmediately after hemodialysis and its progressive increasethroughout the period between dialysis can cause markedfluctuations in BP [272w] which may be further influencedby the presence of cardiac dysfunction increased largeartery stiffness endothelial dysfunction inadequate vol-ume control dialysate composition and administrationof erythropoiesis-stimulating agents BP control in ESRDmay be further complicated because of altered pharmaco-kinetics of antihypertensive drugs such as impaired elim-ination of drug
The few prospective studies in CKD comparing theprognostic role of ABPM versus clinic BP have shownsuperiority of ABPM in predicting left ventricular hyper-trophy [197] cardiovascular events [198199273w] all-cause mortality and progression to ESRD [200274w] Arecent analysis of a prospective CKD cohort found asuperior and independent prognostic value of ABPM
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
(especially night-time SBP) for the primary end-points ofmortality from renal disease and fatal and nonfatal cardio-vascular events when compared with office BP [199] Ofnote neither office BP readings nor office BP targetspredicted any of the cardiovascular outcomes raising con-cerns about the adequacy of office BP targets for CKDrecommended by current guidelines
In ESRD predialysis and postdialysis office BP is poorlycorrelated with ABPM while ABPM between dialysis isprognostically superior to predialysis or postdialysis officeBP in predicting development of organ damage andmortality [201] In a recent prospective cohort of hemo-dialysis patients predialysis or postdialysis office BPperformed over 2 weeks failed to predict the main out-come of the study whereas ABPM between dialysis was asignificant predictor of mortality [202] Aside from causinghypertension volume excess induces alterations in day-to-night BP profiles which are of prognostic relevanceElevated nocturnal SBP is an independent predictor ofcardiovascular mortality [274w] and a nondipping patternof BP has shown to be a potent predictor of cardiovascularevents and cardiovascular mortality in ESRD [203] Vol-ume excess may also manifest with certain patterns onABPM which might also be prognostically relevant inESRD [275w]
Longitudinal studies in CKD have demonstratedelevated night-time BP to be a better predictor of fataland nonfatal cardiovascular events ESRD and mortalitythan daytime or 24-h BP [199200204273w] The presenceof a nondipping pattern of BP has been associatedwith development of microalbuminuria [181] increase inproteinuria [211w276w] diminished renal function[205271w277w278w] faster progression of CKD poorrenal prognosis [206279wndash281w] and developmentand progression of left ventricular hypertrophy [204156w282w]
In conclusion it is clear that without the use of ABPM alarge proportion of patients with CKD will have unmeas-ured BP-related risk Future studies are still needed how-ever including data from current on-going registries onABPM in CKD to ascertain important questions such aswhat are optimal ambulatory targets to provide maximumcardiovascular protection in CKD and to determine theamount of BP lowering that will reduce cardiovascularmorbidity and mortality
610 Ambulatory hypotensionABPM can be particularly useful in identifying hypoten-sion in patients with symptoms suggestive of low BPHypotension is particularly likely to occur in the elderlyin whom postprandial and postural hypotension arecommon often because of autonomic or baroreceptorfailure ABPM may also identify hypotension especiallyin young slim women and in hypertensive patients withsymptoms of dizziness or light-headedness The diagno-sis of symptomatic drug-induced hypotension is import-ant especially in patients who may have a compromisedarterial circulation such as those with coronary andcerebrovascular disease and fragile elderly patients[114130w283w] It should be acknowledged howeverthat the accuracy in identifying sudden and short
orized reproduction of this article is prohibitedwwwjhypertensioncom 1753
OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

OrsquoBrien et al
hypotensive episodes is limited with ABPM due to theintermittency of BP measurements
611 Hypertension in Parkinsonrsquos diseaseParkinsonrsquos disease is characterized by important changesin BP regulation with an increase in 24-h BP variabilityoften leading to symptomatic orthostatic hypotensionwhich may affect about 20 of patients [207284w] Thisis attributed to primary autonomic failure with involvementof the peripheral nervous system and to dopamine-mimeticdrugs which are often prescribed [284w] The characteristicpattern on 24-h ABPM is the reversal of circadian rhythmwith daytime and postprandial hypotension and nocturnalhypertension [285w286w] Supine hypertension coupledwith orthostatic hypotension is observed in up to 50 ofpatients with Parkinsonrsquos disease and autonomic failureand appears to be driven by residual sympathetic activityand changes in sensitivity of vascular adrenergic receptorsit might be induced or worsened by antihypertensive drugs[208287w] Twenty-four-hour ABPM is thus a valuabletool for the evaluation of hypotensive episodes duringdaytime as well as of nocturnal hypertension in thesepatients
612 Endocrine hypertensionSome 70 of patients with endocrine forms of secondaryhypertension present with alterations in 24-h ABPM inparticular a blunted nocturnal BP dipping pattern or evena rise in nocturnal BP with the average reduction in night-time BP in these patients being only a third to a half of thatseen in normal individuals [288w] This is not surprisingconsidering that the production of several hormonesdirectly or indirectly influencing BP are themselves subjectto circadian rhythms Circadian BP variation is influencedby the hypothalamo-pituitary-adrenal axis [209] In patientswith Cushingrsquos syndrome a higher prevalence of nondip-ping or reverse dipping has been reported compared withpatients with essential hypertension or primary aldosteron-ism [209] The same is true for patients receiving exogenousglucocorticoid administration for certain autoimmune dis-orders in whom BP tends to be lower in the afternoon andthen begins to rise throughout the night attaining a peaklevel in the morning [289w] Alterations in circadian BPvariation in patients with Cushingrsquos syndrome are primarilydue to glucocorticoid excess itself rather than to otherfactors such as concomitant mineralocorticoid excessStudies in primary hyperaldosteronism have failed to showa significant association between an altered circadian BPprofile and aldosterone levels or aldosterone-to-renin ratio[290w] Interestingly a deficiency of cortisol in Addisonrsquosdisease has also been associated with a loss of circadian BPrhythmicity [210] suggesting the existence of an importantrelationship between circadian rhythms of cortisol and ofBP Furthermore normalization of day-to-night BP changeshas been observed in these patients following replacementtherapy [210]
A higher prevalence of a nondipping profile has beenreported in patients with either hypothyroidism [211] orhyperthyroidism [291w292w] with the risk of nondippingbeing directly correlated with the severity of thyroid dys-function [211291w292w]
Copyright copy Lippincott Williams amp Wilkins Unaut1754 wwwjhypertensioncom
Adrenomedullary hyperactivity and the associated sym-pathetic activation may not only induce elevations in BPlevels but also significantly interfere with circadian rhythmof BP and short-term BP variability In a study on type 1diabetic patients increasing levels of plasma epinephrineand norepinephrine were directly correlated with meannocturnal BP levels and inversely correlated with night-timeBP dipping [293w] Consistent with these findings inpatients with pheochromocytoma arterial hypertension isvery often accompanied by a blunted or inverted dippingpattern [294w] the degree of impairment being directlyrelated to catecholamine excretion [295w] Moreover theexcess of catecholamines in patients with pheochromocy-toma has been associated with increased BP variability anda lsquoriserrsquo nocturnal BP profile [296w] Surgical treatment ofpheochromocytoma has been shown to be accompaniedby significant reductions in both daytime and especiallynight-time BP [297w] with restoration of BP dipping [212]and significant reductions in BP variability [296w]
Overall it has to be said that no ABPM pattern has beenshown to be specific for any of endocrine forms of secon-dary hypertension However the presence of a nondippingpattern especially in patients with resistant hypertensionshould raise a clinical suspicion of secondary hypertension[213298w] and prompt investigation for secondary hyper-tension including endocrine causes
613 Follow-up
6131 When to repeat ambulatory blood pressuremonitoringThe decision as to when to repeat ABPM is largely one ofclinical judgment which may be influenced by factors suchas excessive BP variability an office BP that appears to beunrepresentative an inappropriate response to treatmentan adverse risk factor profile and the need for tight controlof BP throughout 24 h including the night such as inhypertensive patients with diabetes mellitus renal diseaseor severe cardiovascular disease [1]
The most common reasons for repeating ABPM are toclarify borderline results with the initial ABPM to confirmthe diagnosis of masked or white-coat hypertension toassess an apparent poor response to antihypertensivetherapy or to assess the response to modified treatment
Whenever feasible home BP monitoring should berecommended for treated hypertensive patients in orderto obtain out of office BP data over a long-term follow-upHowever ABPM remains the only method that assessesasleep BP Repeat ABPM may be indicated if there ispersistent discrepancy between office and home BP valuesThe provision of a trend report showing the degree of BPcontrol achieved between successive ABPM recordings ishelpful in deciding when to repeat ABPM [10]
ABPM should be offered to patients suspected of havinghypertension whenever possible to obtain a quantificationof day and night BP aimed at confirming the diagnosis andthe need for long-term intervention [2410]
It is advisable to confirm the diagnosis of white-coathypertension by repeating out-of-office BP monitoring (ifpossible ABPM within 3ndash6 months depending on the totalcardiovascular risk of the individual) because a substantial
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Guideline
number of patients with white-coat hypertension maydevelop sustained hypertension [1102299wndash302w] Inpatients with confirmed white-coat hypertension and anormal risk factor profile it is as a general rule usuallyunnecessary to repeat ABPM more frequently than annu-ally or every 2 years if the pattern appears to be estab-lished and consistent as indeed is often the case [1] If onthe contrary a patient with confirmed white-coat hyper-tension has a high-risk profile ABPM every 6 monthsmay be indicated so as to detect the transition from thewhite-coat hypertension state to sustained hypertensionand the need for antihypertensive medication Alterna-tively HBPM may be combined with ABPM to reduce thefrequency of ABPM The diagnosis of masked hyper-tension also requires confirmation within a few weeksor months dependent on the total cardiovascular riskand the assessment of BP control in these patients alsorequires ABPM which can be combined with homeBP monitoring
The frequency of repeat ABPM to evaluate the efficacy ofantihypertensive medication will be dependent on theseverity of hypertension and the response to treatmentIn patients with severe hypertension and evidence of targetorgan damage BP reduction is urgent and in the initialstages of treatment ABPM may be required frequently asdifferent drug combinations are introduced and dosagelevels are altered In patients with mild hypertension andno evidence of target organ involvement ABPM has to berepeated less frequently according to the device availabilitythe individual patientrsquos needs and preference and thephysicianrsquos discretion [1]
In an evaluation of the most appropriate time interval torepeat ABPM to ensure sustained BP control in patientswith white-coat-resistant hypertension it was considerednecessary to perform a confirmatory ABPM after 3 monthsof the first white-coat-resistant hypertension diagnosis andto repeat the procedure at 6-month intervals except inpatients with daytime SBP of 115 mmHg or less in whomABPM should be repeated annually [214] HBPMs should beencouraged in all patients with treated hypertension as anapproach complementary to ABPM [2]
6132 Ambulatory blood pressure monitoringversus home blood pressureABPM and home BP are both useful in the management ofpatients with hypertension However ABPM is capable ofproviding unique information on an individualrsquos BP statusbeyond what can be obtained using home BP Examplesinclude an assessment of BP during sleep (mean night-timeambulatory BP is the best predictor of future cardiovascularevents in relation to BP status) readings that are not subjectto reporting bias and BP data obtained during usualdaily activities
HBPM has been recommended as an initial screeningprocedure to evaluate the out-of-office BP with ABPMbeing performed when the diagnosis of hypertension isstill uncertain [303w] However ABPM and home BP pro-vide different and complementary clinical information onan individualrsquos BP status [211219w304w305w] There issome evidence that HBPM and ABPM may provide differentpredictive target organ information [304w]
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
ABPM should be performed whenever possible in allpatients with suspected hypertension in whom it isnecessary to confirm the diagnosis of sustained hyper-tension (ie to exclude white-coat hypertension) toassess the severity of hypertension throughout the 24-hperiod to detect nocturnal hypertension to detect pat-terns of BP behavior such as isolated systolic hyperten-sion nondipping and autonomic failure and to be able toanalyze the 24-h data for indices of BP fluctuations suchas AASI and measures of BP variability [410165214]ABPM is particularly appropriate for the initial evaluationbecause it provides information within 24 h and withoutneed of training skills and commitment as required forhome BP
In parallel with ABPM and particularly when ABPM isnot readily available out-of-office assessment of BP maycomplement office visits by obtaining a HBPM sessionwith duplicate morning and evening measurements for7 days and calculating the average after discarding thefirst day this provides a measurement that approximatesto average daytime ABPM [238215] HBPM also has arole in monitoring BP control in treated patients overextended periods of time between office visits especiallyin patients with good BP control on ABPM and there isthe added advantage that HBPM can improve long-termadherence to medication and thereby hypertension con-trol rates [216217] Finally whereas ABPM remains theleading technique in the pharmacological assessment ofantihypertensive drugs HBPM has a potentially valuablerole in outcome trials carried out in large populations inwhich the effects of BP lowering are being assessed overmany months or years [112168218219306wndash313w] Acomparison of the different BP measurement methods isshown in Table 3
7 AMBULATORY BLOOD PRESSUREMONITORING IN RESEARCH
71 Ambulatory blood pressure monitoring inpharmacological researchABPM was first used over 30 years ago in pharmaco-logical studies on the efficacy of BP-lowering drugs[731220314w] From the results of early studies usingdaytime and 24-h ABPM to assess the efficacy ofBP- lowering drugs [31] a number of patterns emergedFirst ABPM could be in agreement with clinic BPmeasurements Second clinic BP measurement couldfail to detect the BP-lowering effect demonstrated byABPM Finally reductions in clinic BP could be signi-ficant but ABPM might be either nonconfirmatory orshow that the clinic BP reduction coincided only witha brief period of BP reduction on ABPM [31] These earlystudies showed that many drugs would have beendeclared as quite efficacious (including 24-h durationof action) with conventional BP measurement whereasABPM showed a pattern of activity that was far lessimpressive
Later studies have shown that treatment-induced BPlowering is greater with office BP measurement than withABPM ABPM does not provoke a white-coat reactionexhibits negligible placebo effects and less regression to
orized reproduction of this article is prohibitedwwwjhypertensioncom 1755
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
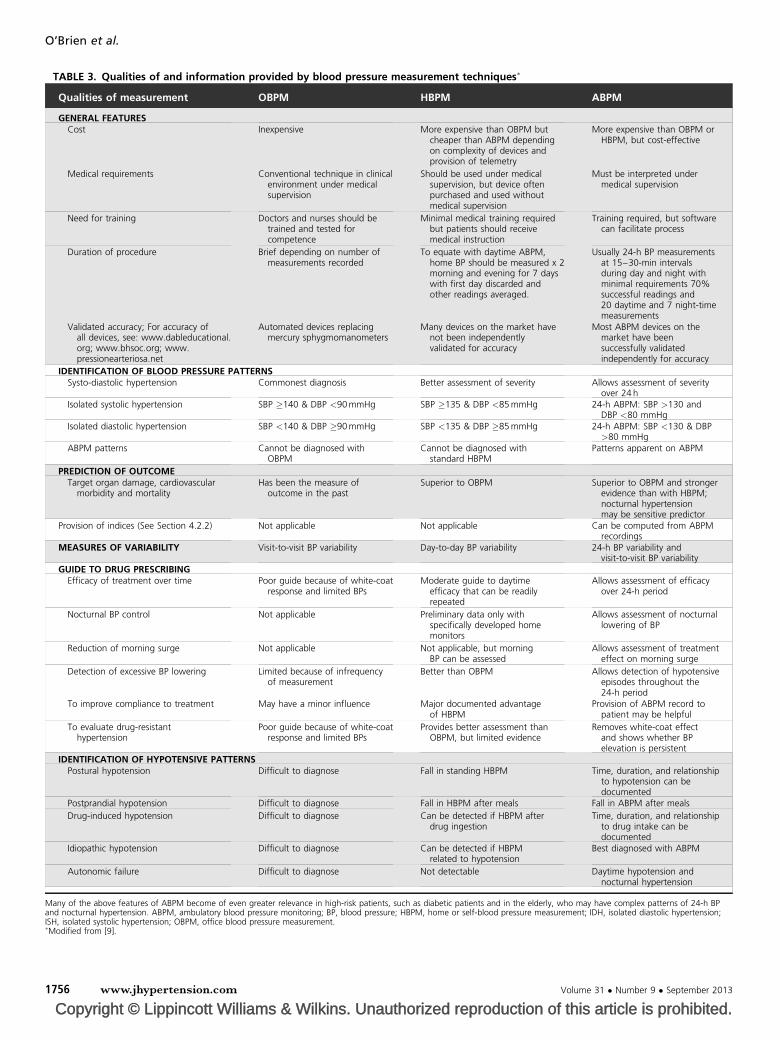
Copyright copy Lippincott Williams amp Wilkins Unauthorized reproduction of this article is prohibited
TABLE 3 Qualities of and information provided by blood pressure measurement techniques
Qualities of measurement OBPM HBPM ABPM
GENERAL FEATURESCost Inexpensive More expensive than OBPM but
cheaper than ABPM dependingon complexity of devices andprovision of telemetry
More expensive than OBPM orHBPM but cost-effective
Medical requirements Conventional technique in clinicalenvironment under medicalsupervision
Should be used under medicalsupervision but device oftenpurchased and used withoutmedical supervision
Must be interpreted undermedical supervision
Need for training Doctors and nurses should betrained and tested forcompetence
Minimal medical training requiredbut patients should receivemedical instruction
Training required but softwarecan facilitate process
Duration of procedure Brief depending on number ofmeasurements recorded
To equate with daytime ABPMhome BP should be measured x 2morning and evening for 7 dayswith first day discarded andother readings averaged
Usually 24-h BP measurementsat 15ndash30-min intervalsduring day and night withminimal requirements 70successful readings and20 daytime and 7 night-timemeasurements
Validated accuracy For accuracy ofall devices see wwwdableducationalorg wwwbhsocorg wwwpressionearteriosanet
Automated devices replacingmercury sphygmomanometers
Many devices on the market havenot been independentlyvalidated for accuracy
Most ABPM devices on themarket have beensuccessfully validatedindependently for accuracy
IDENTIFICATION OF BLOOD PRESSURE PATTERNSSysto-diastolic hypertension Commonest diagnosis Better assessment of severity Allows assessment of severity
over 24 hIsolated systolic hypertension SBP 140 amp DBP lt90 mmHg SBP 135 amp DBP lt85 mmHg 24-h ABPM SBP gt130 and
DBP lt80 mmHgIsolated diastolic hypertension SBP lt140 amp DBP 90 mmHg SBP lt135 amp DBP 85 mmHg 24-h ABPM SBP lt130 amp DBP
gt80 mmHgABPM patterns Cannot be diagnosed with
OBPMCannot be diagnosed with
standard HBPMPatterns apparent on ABPM
PREDICTION OF OUTCOMETarget organ damage cardiovascular
morbidity and mortalityHas been the measure of
outcome in the pastSuperior to OBPM Superior to OBPM and stronger
evidence than with HBPMnocturnal hypertensionmay be sensitive predictor
Provision of indices (See Section 422) Not applicable Not applicable Can be computed from ABPMrecordings
MEASURES OF VARIABILITY Visit-to-visit BP variability Day-to-day BP variability 24-h BP variability andvisit-to-visit BP variability
GUIDE TO DRUG PRESCRIBINGEfficacy of treatment over time Poor guide because of white-coat
response and limited BPsModerate guide to daytime
efficacy that can be readilyrepeated
Allows assessment of efficacyover 24-h period
Nocturnal BP control Not applicable Preliminary data only withspecifically developed homemonitors
Allows assessment of nocturnallowering of BP
Reduction of morning surge Not applicable Not applicable but morningBP can be assessed
Allows assessment of treatmenteffect on morning surge
Detection of excessive BP lowering Limited because of infrequencyof measurement
Better than OBPM Allows detection of hypotensiveepisodes throughout the24-h period
To improve compliance to treatment May have a minor influence Major documented advantageof HBPM
Provision of ABPM record topatient may be helpful
To evaluate drug-resistanthypertension
Poor guide because of white-coatresponse and limited BPs
Provides better assessment thanOBPM but limited evidence
Removes white-coat effectand shows whether BPelevation is persistent
IDENTIFICATION OF HYPOTENSIVE PATTERNSPostural hypotension Difficult to diagnose Fall in standing HBPM Time duration and relationship
to hypotension can bedocumented
Postprandial hypotension Difficult to diagnose Fall in HBPM after meals Fall in ABPM after meals
Drug-induced hypotension Difficult to diagnose Can be detected if HBPM afterdrug ingestion
Time duration and relationshipto drug intake can bedocumented
Idiopathic hypotension Difficult to diagnose Can be detected if HBPMrelated to hypotension
Best diagnosed with ABPM
Autonomic failure Difficult to diagnose Not detectable Daytime hypotension andnocturnal hypertension
Many of the above features of ABPM become of even greater relevance in high-risk patients such as diabetic patients and in the elderly who may have complex patterns of 24-h BPand nocturnal hypertension ABPM ambulatory blood pressure monitoring BP blood pressure HBPM home or self-blood pressure measurement IDH isolated diastolic hypertensionISH isolated systolic hypertension OBPM office blood pressure measurementModified from [9]
OrsquoBrien et al
1756 wwwjhypertensioncom Volume 31 Number 9 September 2013
Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Box 10 Ambulatory blood pressure monitoring in pharmacological trials
Ambulatory blood pressure monitoring is clearly superior to any otherblood pressure measurement method and indispensable for theinvestigation of the efficacy duration of action and homogeneityof the effect of antihypertensive drugs
Ambulatory blood pressure measurement is valuable in clinical trialsbecause it identifies patients with white-coat hypertension is notaffected by placebo and is more reproducible than officemeasurements thereby increasing the study power and reducing therequired study sample
The implementation of ambulatory blood pressure monitoring inoutcome trials has been largely limited to nonrandomized subgroupsand with incomplete baseline and repeat evaluation
Future outcome trials should apply ambulatory blood pressuremonitoring in all participants before randomization and at varioustimes during treatment
Guideline
the mean of averaged BP values and the reduction in night-time BP is smaller on ABPM than for daytime BP [221] Theadvantages of ABPM for assessing treatment effects inclinical trials include the exclusion of patients withwhite-coat hypertension who show little response to anti-hypertensive drugs the ability to evaluate the duration ofaction of a drug and to analyze its effects on night-time BPas well as on BP variability the almost complete absence ofa placebo response the increase in the power of studieswith fewer patients to assess antihypertensive drug efficacyand the reduction of the sample size required and bettercorrelation of the results with clinical outcomes [31221]
Studies using both ABPM and conventional BP measure-ment clearly show the added value of ABPM in detectingpharmacological effects that would not have been evidentfrom conventional BP measurement alone [222315wndash335w] It is also of interest to note that the use of ABPMin pharmacological trials is not always successful Forexample ABPM recordings can fail to meet the a prioricriteria for a successful recording in as many as a quarterof patients enrolled for studies [222332w] This unaccept-able level of rejected measurements can be prevented byhaving real-time on-line transmission of ABPM recordingsso that failed ABPM measurements are notified to theinvestigators allowing for unsatisfactory ABPM recordingsto be repeated
We do not yet know whether treatment strategies basedon BP assessment by ABPM are significantly better thanoffice BP in reducing the rate of cardiovascular eventsNotwithstanding this limitation the above-mentionedadvantages of ABPM strongly support the inclusion ofABPM in all future pharmacological trials of antihyperten-sive drug therapy [31]
72 Regulatory recommendations forpharmacological studiesThe US Food and Drug Administration (FDA) guidelinesacknowledge that ABPM adds valuable information on theduration of antihypertensive drug dosing interval and ondosendashresponse elements [223] The current European Medi-cines Agency (EMA) guidelines lsquostrongly recommendrsquoABPM for the evaluation of new antihypertensive agentsbut adds that lsquothere are insufficient data to accept ABPM asthe sole basis for efficacy in an approval processrsquo [224] Theguideline then goes on to stipulate the requirements forABPM but unfortunately these fail to give attention to thepractical realities that are necessary if the technique is to besuccessfully implemented in pharmacological studies [31]
ABPM in clinical research has been facilitated by com-mercially available systems which can provide real-timeanalysis of ABPM in multicenter clinical trials based onABPM providing features that include separate viewingand editing facilities for investigators monitors and super-visors full multicenter support allowing investigators toaccess data relating to their specific center with monitorsand supervisors having access to data from all centersprovision of audit and progress reports to assist monitorsto check data validation of all ABPMs and comprehensiveexport of ABPM raw data and statistics [31]
A recent interesting aspect of the pharmacologicalassessment of drugs has been a growing demand for
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
information by the regulatory authorities especially theFDA on the effect of noncardiovascular drugs on 24-hBP Previously the cardiovascular effects of such drugshas tended to focus on ECG changes such as prolongationof the QT interval but in the future noncardiovasculardrugs will also be scrutinized for their potential to lower orraise BP [32192193336w] (Box 10)
73 Ambulatory blood pressure monitoring inoutcome studiesObservational studies have shown that ABPM monitoringpredicts the incidence of cardiovascular morbid or fatalevents [16126218225226] Evidence also exists that therelationship with cardiovascular risk is steeper for 24-hmean BP than for clinic BP [16126218] and that use ofthe two methods together may increase the ability of BP topredict outcome [112]
ABPM has also been performed in subsets of patients inmorbiditymortality trials of antihypertensive drug therapyIn most instances the number of patients having ABPM hasbeen relatively small [151337wndash342w] Furthermore insome studies ABPM comparisons have considered non-randomized subgroups with often clinical and demo-graphic characteristics different from those of the mainstudy Finally ABPM has usually been performed only onceor twice during treatment sometimes without any baselinerecording These limitations do not provide the answer toan important question does inclusion of patients intoclinical outcome studies of antihypertensive drug therapyon the basis of ABPM and their subsequent managementusing ABPM provide a better method for assessing hyper-tension treatment strategies than conventional BP measure-ment Use of ABPM in trials has nevertheless provideduseful data for the following reasons [227] One the 24-hmean BP reductions induced by treatment are usually lessthan the concomitant clinic BP reduction the ratio betweenthe former and the latter change ranging between 06 and07 [221] and even less in the very elderly [228] Two there isa significant but by no means close relationship betweenclinic and 24-h mean BP changes induced by treatment ndashcorrelation coefficients of the order of 02ndash04 ndash whichmeans that in a given individual daily life BP reductionswith treatment can hardly be predicted by the clinic BPreductions [229230337w339w] However in a single-center study a substantially higher correlation was
orized reproduction of this article is prohibitedwwwjhypertensioncom 1757
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
OrsquoBrien et al
observed between changes in clinic and 24-h BP [231]Three in some trials average clinic BP changes with treat-ment were reflected by the concomitant 24-h BP changesbut this was not the case in other trials For example in theEuropean Lacidipine Study on Atherosclerosis (ELSA)study treatment with atenolol or lacidipine was associatedwith similar changes in clinic BP but atenolol-based treat-ment induced a greater 24-h BP reduction than lacidipine[229] Furthermore in the Heart Outcomes PreventionEvaluation (HOPE) study ramipril caused a small reductionin clinic BP and a greater one (especially during the night)in ABPM [338w] Finally in the Ongoing Telmisartan Aloneand in Combination with Ramipril Global Endpoint Trial(ONTARGET) ramipril and telmisartan showed a similareffect on clinic but not on ABPM which was more effec-tively lowered by the latter drug with a particularly pro-nounced reduction when the combination of the two drugswas used [341w] Likewise in the Simplicity trials to deter-mine the efficacy of renal denervation the failure to utilizethe data from ABPM has left the results of the techniqueopen to serious question [343w]
In conclusion in order to minimize the above-men-tioned limitations future trials should make use of ABPMin all patients and the design should provide ABPM databoth before randomization and at various times duringtreatment This will allow more reliable information to beobtained on the debated question whether and to whatextent the cardiovascular protection associated with anti-hypertensive treatment depends on specific BP-independ-ent properties of the drug employed The presence orabsence of cardiovascular protection is presently attributedto a drug if the incidence of cardiovascular events is greateror less in the presence or absence of a reduction in clinicBP In such a context it should be acknowledged thatestablishing the BP changes by clinic BP only is notsufficient
8 IMPLEMENTATIONOFAMBULATORYBLOOD PRESSUREMONITORING INCLINICAL PRACTICE
81 General principlesDespite the large diversity in the structure of healthcaresystems across different countries the vast majority ofhypertensive patients are being managed in primary careThus in practice primary care doctors may establish theirown ABPM service or alternatively they may refer theirpatients to an external ABPM service as they routinely dofor multiple other medical tests Models to develop suchservices might include specialist clinics healthcare pro-viders in the private sector pharmacy-based servicesand other solutions
82 Financial considerationsThe ready provision of ABPM in primary care will bedependent on reimbursement to physicians or other health-care providers by the national healthcare systems or byprivate insurance ABPM is currently reimbursed in severalcountries including Switzerland (s90 per ABPM) Italy(s50ndash70) The Netherlands (s60 for general practitioners
Copyright copy Lippincott Williams amp Wilkins Unaut1758 wwwjhypertensioncom
only) Germany (s7ndash8) Greece (s40) United States($60ndash120 by Medicare only for white-coat hypertensionand $75ndash225 by private insurances for several indications)Canada by some private insurers (CDN $50ndash75) in Ontariothe provincial government is currently giving considerationto fund ABPM probably in the $50ndash75 range) and China[RBM 150ndash200 (s20ndash28) 80ndash90 reimbursed] Howeverin other countries [eg Ireland Belgium Spain (regionaldifferences exist) Australia] ABPM is not currently reim-bursed [344w345w]
83 Specialist clinicsThe ESH has accredited lsquoCentres of Excellencersquo in hyper-tension across Europe (httpwwweshonlineorg) [232]and promotes a structure connecting these centers withaffiliated Blood Pressure and Vascular Protection Clinics[233] The availability of ABPM is regarded as an essentialrequirement for both the ESH Centers and Clinics [232233]More recently the American Society of Hypertensionlaunched a similar initiative that involves formal recognitionof lsquoHypertension Centersrsquo that have demonstrated expertisein the management of complex hypertension (httpwwwash-usorg) [234] These initiatives can ensure theapplication of ABPM in many patients with complex hy-pertension and might also accommodate referrals for ABPMthrough models of continuing care such as lsquoshared carersquowith primary care physicians or lsquointermediate carersquo withspecialist nurse teams or other models [233]
84 Primary carePrimary care doctors and practices may establish their ownABPM services which may be supported by specialistnurses or medical assistants The progressive decline inthe cost of ambulatory monitors in recent years togetherwith reimbursement schemes as mentioned above isexpected to facilitate the spread of the technique in primarycare which will be necessary to meet the increasingdemand for routine application of ABPM in practice
Several studies have investigated the usefulness of ABPMimplementation in primary care [9168235] One of thesestudies showed that BP measurements made by doctorswere much higher than those using ABPM [235] Anotherstudy showed that office BP incorrectly labeled nearly athird of patients with a white-coat effect as having poor BPcontrol and that these patients were likely to be recalled forunnecessary follow-up and intervention [346w] An Irishstudy in primary care showed that only 12 of patientsachieved target BP with office BP compared with more thanone-third of patients with ABPM Furthermore 38 ofpatients had a change in their medication as a resultof ABPM 32 had a new medication started and 14 ofuntreated patients with elevated office BP who were can-didates for drug treatment were not started on medicationbecause ABPM was normal [236]
The largest study to date on ABPM in primary care comesfrom Spain where a nationwide project to promote the useof ABPM in primary care settings has been established[195237] In this large cohort of some 20 000 patients clinicBPs were higher than ABPM in patients categorized asbeing at low-to-moderate added risk with a greater
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

Guideline
difference (2323mmHg) in those categorized as being athigh risk despite receiving much more antihypertensivetreatment Moreover a nondipping nocturnal BP patternwas common in high-risk hypertensive patients These datasupport the wider use of ABPM to gain more accurate riskstratification of patients in the community and to be able toobtain a more accurate estimate of the control of BP in thecommunity [347w] As in the Irish study BP control wasbetter when assessed by ABPM than by office BP indicatingthat the white-coat effect with office BP is leading toan underestimation of BP control in the community[195236237] BP control was underestimated in more thanone-third of patients and overestimated in some 5 byoffice BP as compared with ABPM Notably BP was uncon-trolled by both methods of measurement in 43 of patientsHigh-risk patients showed worse ambulatory BP controlthan low-to-moderate risk patients in spite of receivingmuch more antihypertensive treatment [195237] Finallyin the Italian MARTE study assessment of BP control byoffice measurement was poor and showed that apparentcontrol of BP with office measurement did not reflect 24-hBP control in daily life [18]
85 PharmaciesWhereas primary care practices and hypertension centerswill be the main providers of ABPM (provided adequatereimbursement is made available) the valuable role ofpharmacies in achieving improved control of hypertensionhas been recognized for many years [238239348wndash354w]Indeed it has been shown that when pharmacists becomeengaged in the management of hypertension BP controlimproves [239350wndash353w]
When considering pharmacies as providers of ABPM itis essential that ABPM assessment and reporting isprovided in collaboration with primary care physiciansandor specialists Recently ABPM has been introducedto pharmacists in a few European countries and thepharmacy-based service is proving popular with patientsand is being increasingly adopted as shown in a recentIrish report [355w]
For the implementation of ABPM within the pharmacyautomated interpretation of the results by the monitorsoftware according to current guidelines is essential forthe initial evaluation of the recording in order to adviseimmediate medical consultation whenever required Thusif ABPM in a pharmacy is normal the patient is instructed tobring the report to hisher general practitioner at their nextattendance but if the ABPM is reported as abnormalinstruction is given to make an appointment as soon aspossible [355w] The advantages of ABPM in pharmaciesinclude greater availability of ABPM to the public rapidaccess to a conveniently located pharmacy short or absentwaiting lists provision of an interpretative report to thepatient who is informed as to the degree of BP control closecollaboration between the pharmacist and the patientrsquosgeneral practitioner provision of a trend report to patientshaving a repeat ABPM so as to indicate the response to BP-lowering medication availability of data in a central data-base to provide demographic information on national BPtrends and patient awareness as to their BP control andencouragement to adhere to medication and management
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
[355w] Moreover the pharmacy ABPM service is less costlythan that provided by doctors
86 Healthcare providersHealthcare providers in the private sector that havecontracts with the healthcare system or with insurancecompanies are increasingly providing ABPM services as isthe case with multiple other medical tests such as ultra-sound tests computer tomography 24-h ECG and bloodtests
87 Ambulatory blood pressure monitoringregistries and databasesIn recent years several countries have established registriesto assess the impact of ABPM on hypertension managementand related outcomes Disease or condition registries aredefined as databases with details of patients having thesame diagnosis such as hypertension [240] It is importantto recognize that a disease registry is not a database con-taining information on patient cohorts with a particulardisease though such databases may ultimately form thebasis for establishing a disease registry Rather the purposeof a disease registry is to organize a system that usesobservational study methods to collect uniform data inorder to define the prevalence and to study outcome relatedto specific strategies that may include scientific researchand epidemiological and health economic methods ofanalysis Patients are observed and followed as they presentfor care and the data collected generally reflect currentpractice Such registries by classifying patients according todisease allow patients the opportunity to participate in aresearch study appropriate to their illness [240] Govern-ments are beginning to recognize that disease registries maylead to improvements in health outcomes and to lowercosts Through the use of such registries healthcare pro-viders can compare identify and adopt best practices forpatients [241] For example the Swedish Government iscommitted to increasing its annual financial support fordisease registries from $10 to $45 million by 2013 [362w]
ABPM registries are more commonly based on patientswith documented hypertension or on patients referred todoctors for possible hypertension who would benefit fromABPM Some of the current registries represent a mix ofhypertensive and normotensive individuals and are moreproperly labeled as population studies Many of the existingABPM registries serve as valuable databases and could bestructured to fulfill the requirements to become diseaseregistries The following ABPM registries are in existence
871 Spanish registryThis registry was established in 2004 with the initial aim ofmaking ABPM readily available in primary care and tocreate an ABPM education program The registry involves1700 doctors and obtained about 150 000 ABPM recordingsData are transmitted via the Internet from a specialist centerto primary care physicians alerting them to the degree of BPcontrol The results which have been published in severalpapers [195237268w] have influenced the use of ABPM inprimary care and improved the management of hyper-tension in Spain
orized reproduction of this article is prohibitedwwwjhypertensioncom 1759
OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

OrsquoBrien et al
872 Italian registryThe Telemapanet Project started in 2008 is aimed atencouraging the use of ABPM in primary care The mainpurpose is to assess the degree of 24-h BP and cardiovas-cular risk factor control of treated or untreated hypertensivepatients and to encourage adherence to national guidelinesData from patients with uncontrolled treated or untreatedarterial hypertension or with indications for ABPM are sentthrough a GPRS wireless interface to a web-based tele-medicine platform where after automatic analysis a reportis sent via E-mail to the primary care physician Preliminarydata from 7000 patients show that BP control differsbetween office BP and ABPM and ABPM provides a meansfor doctors to improve the management of hypertension byidentifying uncontrolled patients
873 Irish registryA national on-line system with central hosting of ABPM dataand the provision of standardized ABPM has been inoperation in Ireland for some years The provision of atrend report has facilitated the identification of poorlycontrolled hypertensive patients The registry has beenextended to pharmacists so as to make ABPM more acces-sible to the public and the data from pharmacies are storedcentrally Preliminary analysis shows a high prevalence ofwhite-coat hypertension and nondipping hypertension[236]
874 Japanese registryFour population-based studies have been conducted inJapan among which the most important is the prospectivecohort study of some 2000 residents in Ohasama who havebeen followed with ABPM and assessment of other cardio-vascular risk factors [242132w] In addition several ABPMdatabases have been established in Japan which includethe Jichi Medical School ABPM Study in older Japanesehypertensive patients the cross-sectional study in Yamana-shi University and the cross-sectional study in NagoyaUniversity
875 Australian registryIn 2008 the Australian Database for ABPM was initiated toaddress the need for ABPM equivalents for target BP formanagement of hypertension in low-risk and high-riskpatients The database is the result of the cooperative effortof individuals and the financial and logistic support fromthe High Blood Pressure Research Council of Australia andthe National Heart Foundation of Australia which hasenabled this contribution to the appropriate use and inter-pretation of ABPM and effective management of hyperten-sion [26] Data are available from over 8000 patients [363w]
876 International Database of Ambulatory bloodpressure in relation to Cardiovascular OutcomedatabaseIn 2005 an international consortium of investigators startedconstructing the IDACO [154243364w365w] based onprospective population-based studies reporting fatal as wellas nonfatal outcomes The database currently includes12 854 participants recruited in 12 countries from threecontinents Articles published so far have demonstrated
Copyright copy Lippincott Williams amp Wilkins Unaut1760 wwwjhypertensioncom
that although the absolute cardiovascular risk is lower inwomen than it is in men the relationship between the riskof a cardiovascular event and the ambulatory BP is strongerin women than men These observations highlight missedopportunities for cardiovascular prevention in women Inpopulation-based cohorts both diabetes mellitus and theambulatory BP contributed equally to the risk of cardio-vascular complications without evidence for a synergisticeffect
877 ARTEMIS registryThe ARTEMIS (international Ambulatory blood pressureRegistry TEleMonitoring of hypertension and cardiovascu-lar rISk project) is endorsed by the ESH and is the firstinternational registry of ABPM aimed at assessing the actualdegree of BP and cardiovascular risk control of hyper-tensive patients followed by doctors in many countries(wwwartemisnetorg) [244] Objectives are the creationof a worldwide network of centers performing ABPMrecordings the collection of a large registry of patientsfrom different countries of various continents in whombasic clinical information is available as well as at least oneABPM fulfilling predefined criteria the design and initiationof a series of research studies focusing on ABPM and basedon this collected dataset the promotion of the applicationof ABPM in clinical practice and the dissemination ofknowledge on its correct use and interpretation and finallythe active collaboration with international scientificsocieties in their activities related to ABPM in particularin the preparation of recommendations for ABPM use inclinical and research settings
The registry was launched in 2010 with a two-stepapproach A first phase has collected data from approxi-mately 10 000 patients from 38 countries in five continents(Europe America Asia Oceania and Africa) Preliminaryresults provide interesting comparative information onhypertension phenotypes in treated and untreated patientsattending hypertension clinics worldwide In particularwhite-coat hypertension was more common in untreatedpatients whereas masked uncontrolled hypertension wasmore common in treated patients In addition significantlyhigher prevalence of sustained hypertension was observedin clinics in Europe and South America than in Asia andOceania A second phase using a dedicated web-basedmultilingual telemedicine system will allow collection ofdata from patients having consecutive ABPMs
878 Ambulatory blood pressure internationaldatabaseInitiated by Thomas Pickering the ABP-International data-base was constructed by systematically merging eight pro-spective studies from three European three Japanese oneNorth American and one Australian centers Currentlystudies are eligible for inclusion if they involve a randompopulation sample or patients referred to hospital forhypertension if baseline information on ABPM and cardio-vascular risk factors are available and if the follow-upincludes fatal and nonfatal cardiovascular events ABP-International includes data from 11 235 patients followedfor about 6 years who have experienced about 700 majorcardiovascular events Analysis of this data which has
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
Guideline
focused on the short-term and long-term incidence ofstroke in white-coat hypertension and the clinical import-ance of night-time heart rate for predicting cardiovascularevents have been published [166366w]
ACKNOWLEDGEMENTSThe authors are grateful to Dr Grzegorz Bilo and Dr XiaoqiuLiu for their help in reordering and reclassifying the largenumber of references
Conflicts of interestE OrsquoBrien G Parati and GS Stergiou as members of thewriting committee were in receipt of travel support fromthe Hellenic Society of Hypertension University CollegeDublin University of Milano-Bicocca amp Istituto AuxologicoItaliano Milan for meetings in Athens Milan and DublinThe following companies provided unrestricted edu-cational grants for the ABPM Consensus Meeting in MilanAbbott A amp D IEM Microlife Meditech and SuntechMedical
E OrsquoBrien is medical director and a board member ofdabl Ltd Dublin Ireland and has been in receipt of pasthonoraria for lectures with Menarini Ireland and Servier
D Clement A de la Sierra P de Leeuw E Dolan RFagard J Graves Y Imai E Lurbe J-M Mallion M MyersG Ogedegbe P Palatini J Redon and JA Staessen have noconflicts of interest to declare
The following conflicts of interest have been declaredR Asmar consultancy to Servier ndash Fukuda past payment
for lectures Bayer Boehringer and NovartisL Beilin Board member Medical Research Foundation
Royal Perth Hospital competitive national research grantsNHMRC stockstock options CSL Cochlear
G Bilo current grant for BP measuring device validationstudy SENSE AS
GA Head accommodation support ESH current con-sultancy ResMed past consultancy Telemetry Researchcurrent grant NHMRC past lecture payments Novartis Ja-pan traveling expenses Baker Institute
K Kario current consultancies Omron Healthcare Daii-chi Sankyo Teijin Pharma
G Mancia current consultancy Siron BV past lecturepayments Bayer Daicichi Sankyo Menarini RecordatiServier and Takeda current lecture payments NovartisBoehringer Ingeleheim
T Mengden past board membership Actelion consul-tancy Custo med Germany current lecture payment ServierBerlin Chemie past lecture payments Daichi SankyoTakeda payment for manuscript preparation Takeda
T Ohkubo current lecture payments Astellas AstraZeneca Daiichi-Sankyo Dainippon-Sumitomo MerckSharpe and Dohme Novartis Pfizer Takeda Tanabe-Mit-subishi and Omron Health Care
S Omboni current consultancy with Biotechmed LtdLL Ruilope consulting honoraria Astra-Zeneca Bayer
Novartis Menarini Pfizer Daiichi-Sankyo Takeda BMSRelypsa consultancy Astra-Zeneca BMS Bayer Novartisand Relypsa
A Shennan current board membership Hologic Alereand GSK current consultancy GSK and Alere current
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
lecture payments Hologic Alere GSK and Ferring pastpayment development of educational presentations forBBC
G vanMontfrans past lecture payment Merck SharpDohme and Daichii Sankyo past royalty for book chapterBohn Stafleu
P Verdecchia current board membership Stroder Boeh-ringer-Ingelheim current lecture payments Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
B Waeber current board membership Boehringer-Ingelheim Malesci Daiichi-Sankyo Bayer
J Wang current grant A amp D past honorarium Omronpast travel support A amp D Omron current lecture paymentsMSD Novartis Pfizer Servier Takeda
A Zanchetti current lecture payments Menarini Record-ati CVRx
Y Zhang past consultancy Dachi-Sankyo TakedaNovatis Pfizer Sanofi current lecture payments SanofiAstra-Zeneca Novatis Merck Takeda
Co-author affiliationsEoin OrsquoBrien Conway Institute of Biomolecular andBiomedical Research University College Dublin BelfieldDublin Ireland Gianfranco Parati Department of HealthSciences University of Milano-Bicocca and Department ofCardiology S Luca Hospital Istituto Auxologico ItalianoMilan Italy George S Stergiou Hypertension Center ThirdUniversity Department of Medicine Sotiria HospitalAthens Greece Roland Asmar Medical Research InstitutesGeneva Switzerland Laurie Beilin Sydney South West AreaHealth Service Sydney Australia Grzegorz Bilo Depart-ment of Cardiology SLuca Hospital Istituto AuxologicoItaliano Milan Italy Denis Clement University HospitalGhent Belgium Alejandro de la Sierra Hospital MutuaTerrassa University of Barcelona Terrassa Spain Peterde Leeuw Department of Medicine Maastricht UniversityMedical Center Maastricht The Netherlands EamonDolan Royal College of Surgeons Ireland and ConnollyMemorial Hospital Blanchardstown Dublin Ireland Rob-ert Fagard Hypertension amp Cardiovascular Rehab Unit KULeuven University Leuven Belgium John Graves Divisionof Nephrology and Hypertension College of Medicine MayoClinic Rochester Minnesota USA Geoffrey A Head BakerIDI Heart and Diabetes Institute Melbourne VictoriaAustralia Yutaka Imai Tohoku University Graduate Schoolof Pharmaceutical Sciences Sendai Japan Kazuomi KarioDivision of Cardiovascular Medicine Department of Medi-cine Jichi Medical University School of Medicine YakushijiShimotsuke Tochigi Japan Empar Lurbe PediatricsDepartment Consorcio Hospital General UniversitarioUniversity of Valencia Spain Jean-Michel Mallion Cardio-logy and Arterial Hypertension CHU de Grenoble Greno-ble France Giuseppe Mancia Clinica Medica andDipartimento di Medicina Clinica Universita Milano-Bicocca Ospedale San Gerardo di Monza Italy ThomasMengden Kerckhoff-Klinik GmbH Bad NauheimGermany Martin Myers Division of Cardiology Sunny-brook Health Sciences Centre Toronto Canada GbengaOgedegbe Center for Healthful Behavior Change Divisionof Internal Medicine NYU Medical Center New York USATakayoshi Ohkubo Teikyo University School of Medicine
orized reproduction of this article is prohibitedwwwjhypertensioncom 1761
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
OrsquoBrien et al
Tokyo Japan Stefano Omboni Italian Institute ofTelemedicine Varese Italy Paolo Palatini Dipartimentodi Medicina University of Padova Padova Italy JosepRedon University of Valencia INCLIVA Research Instituteand CIBERobn Madrid Spain Luis L Ruilope Hyperten-sion Unit Hospital 12 de Octubre Madrid Spain AndrewShennan Womenrsquos Health Academic Centre KHP Divisionof Womenrsquos Health Kingrsquos College London UK Jan AStaessen Division of Hypertension and CardiovascularRehabilitation KU Leuven Department of CardiovascularSciences University of Leuven Belgium Gert vanMontfransAcademisch Medisch Centrum afd Interne en vasculairegeneeskunde Amsterdam The Netherlands Paolo Verdec-chia Struttura Complessa di Medicina Ospedale di AssisiAssisi PG Italy Bernard Waeber Centre Hospitalier Uni-versitaire Vaudois Division de Physiopathologie CliniqueLausanne Switzerland Jiguang Wang Shanghai Instituteof Hypertension Centre for Epidemiological Studies andClinical Trials Ruijin Hospital Shanghai Jiaotong Univer-sity School of Medicine Shanghai China AlbertoZanchetti Scientifico Istituto Auxologico Italiano MilanoItaly Yuqing Zhang Department of Clinical Epidemiologyand Biostatistics McMaster University Ontario Canada
REFERENCES1 OrsquoBrien E Asmar R Beilin L Imai Y Maillon JM Mancia G et al
European Society of Hypertension recommendations for convention-al ambulatory and home blood pressure measurement J Hypertens2003 21821ndash848
2 Parati G Stergiou GS Asmar R Bilo G de Leeuw P Imai Y et al onbehalf of the ESH Working Group on Blood Pressure MonitoringEuropean Society of Hypertension guidelines for blood pressuremonitoring at home a summary report of the Second InternationalConsensus Conference on Home Blood Pressure Monitoring J Hyper-tens 2008 261505ndash1526
3 CMS Centers for Medicare amp Medicaid Services Medicare CoveragePolicyDecisionsABPMMonitoring (CAG-00067N)2001httpwwwcmsgovmedicare-coverage-databasedetailsnca-decision-memoaspxNCAIdU5ampNcaNameUAmbulatorythornBloodthornPressurethornMonitoringampverU9ampfromU252527lmrpstate252527ampcontractorU22ampnameUCIGNAthornGovernmentthornServicesthorn(05535)thorn-thornCarrierampletter_rangeU4ampbcUgCAAAAAAIAAAamp
4 National Institute for Health and Clinical Excellence (NICE) Hyper-tension The clinical management of primary hypertension in adultsClinical Guideline 127 2011 wwwniceorgukguidanceCG127
5 Clement DL (ed) Blood Pressure Variability Proceedings of theInternational Workshop on Blood Pressure Variability held at theUniversity Hospital Ghent on 15ndash16 June 1978 Baltimore MDUniversity Park Press 1978
6 OrsquoBrien E Waeber B Proceedings from a workshop on measurementof blood pressure of the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Milan June 1999 BloodPressure Monit 2000 531ndash32
7 OrsquoBrien E Fitzgerald D The history of indirect blood pressuremeasurement In OrsquoBrien E OrsquoMalley K editors Blood pressuremeasurement In Birkenhager WH Reid JL editors Handbook ofhypertension Amsterdam Elsevier 1991 pp 1ndash54
8 Parati G Mancia G History of blood pressure measurement from thepre-Riva-Rocci era to the twenty-first century In Birkenhager WHReid JL editors Handbook of hypertension The Netherlands ElsevierBV 2004 pp 3ndash32 vol 22
9 OrsquoBrien E Ambulatory blood pressure measurement The case forimplementation in primary care Hypertension 2008 511435ndash1441
10 OrsquoBrien E 24-h ambulatory blood pressure measurement in clinicalpractice and research a critical review of a technique in need ofimplementation J Int Med 2011 269478ndash495
11 Myers MG Godwin M Dawes M Kiss A Tobe SW Kaczorowski JMeasurement of blood pressure in the office recognizing the problemand proposing the solution Hypertension 2010 55195ndash200
Copyright copy Lippincott Williams amp Wilkins Unaut1762 wwwjhypertensioncom
12 Myers MG Reporting bias in self-measurement of blood pressureBlood Press Monit 2001 6181ndash183
13 Omboni S Gazzola T Carabelli G Parati G Clinical usefulness andcost effectiveness of home blood pressure telemonitoring meta-analysis of randomized controlled studies J Hypertens 201331455ndash468
14 Pickering TG Shimbo D Haas D Ambulatory blood pressuremonitoring N Engl J Med 2006 3542368ndash2374
15 Parati G Bilo G Should 24-h ambulatory blood pressure monitoringbe done in every patient with diabetes Diabetes Care 2009 32(Suppl 2)S298ndashS304
16 Dolan E Stanton A Thijs L Hinedi K Atkins N McClory S et alSuperiority of ambulatory over clinic blood pressure measurement inpredicting mortality The Dublin outcome study Hypertension 200546156ndash161
17 Parati G Bilo G Mancia G Prognostic and diagnostic value of ambu-latory blood pressure monitoring In Oparil S Weber MA editorsHypertension Philadelphia PA Elsevier Inc 2005 pp 305ndash317
18 Zaninelli A Parati G Cricelli C Bignamini AA Modesti PA PamparanaF et al MARTE Investigators Office and 24-h ambulatory bloodpressure control by treatment in general practice the lsquoMonitoraggiodella pressione ARteriosa nella medicina TErritorialersquo study J Hyper-tens 2010 28910ndash917
19 Parati G Bosi S Castellano M Cristofari M Di Rienzo M Germano Get al Guidelines for 24 h noninvasive ambulatory blood pressuremonitoring Report from a working group of the Italian Society ofHypertension High Blood Press 1995 4168ndash174
20 Myers MG Haynes RB Rabkin SW Canadian Hypertension Societyguidelines for ambulatory blood pressure monitoring Am J Hypertens1999 121149ndash1157
21 OrsquoBrien E Coats A Owens P Petrie J Padheld P Littler WA et al Useand interpretation of ambulatory blood pressure monitoring recom-mendations of the British Hypertension Society BMJ 2000 3201128ndash1134
22 OrsquoBrien E Owens P Staessen J Imai Y Kawasaki T Kuwajima I Whatare the normal levels for ambulatory blood pressure measurementBlood Press Monit 1998 3131ndash132
23 Verdecchia P Reference values for ABPM and self-measured bloodpressure based on prospective outcome data Blood Press Monit 20016323ndash328
24 Parati G Bilo G Mancia G Blood pressure measurement in researchand clinical practice recent evidence Curr Opin Nephrol Hypertens2004 13343ndash357
25 Kikuya M Hansen TW Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al International Database on Ambulatory bloodpressure monitoring in relation to Cardiovascular Outcomes Investi-gators Diagnostic thresholds for ambulatory blood pressure monitor-ing based on 10-year cardiovascular risk Circulation 2007 242145ndash2152
26 Head GA Mihailidou AS Duggan KA Beilin LJ Berry N Brown MAet al for the Ambulatory Blood Pressure Working Group of the HighBlood Pressure Research Council of Australia Definition of ambulat-ory blood pressure targets for diagnosis and treatment of hyperten-sion in relation to clinic blood pressure prospective cohort study BMJ2010 340c1104
27 Chobanian AV Bakris GL Black HR Cushman WC Green LA Izzo JLJr et al Joint National Committee on Prevention DetectionEvaluation and Treatment of High Blood Pressure National HeartLung and Blood Institute National High Blood Pressure EducationProgram Coordinating Committee Seventh report of the JointNational Committee On Prevention Detection Evaluation and Treat-ment of High Blood Pressure Hypertension 2003 421206ndash1252
28 Mancia G De Backer G Dominiczak A Cifkova R Fagard R GermanoG et al Management of Arterial Hypertension of the EuropeanSociety of Hypertension European Society of Cardiology 2007Guidelines for the Management of Arterial Hypertension the TaskForce for the Management of Arterial Hypertension of the EuropeanSociety of Hypertension (ESH) and of the European Society ofCardiology (ESC) J Hypertens 2007 251105ndash1187
29 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Bohm Met al The Task Force for the management of arterial hypertension ofthe European Hypertension Society (ESH) and of the EuropeanSociety of Cardiology (ESC) 2013 ESHESC Guidelines for the man-agement of arterial hypertension J Hypertens 2013 22193ndash278
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
Guideline
30 Ohkubo T Imai Y Tsuji I Nagai K Ito S Satoh H Hisamichi SReference values for 24-h ambulatory blood pressure monitoringbased on a prognostic criterion the Ohasama study Hypertension1998 32255ndash259
31 OrsquoBrien E The value of 24-h blood pressure monitoring to assess theefficacy of antihypertensive drug treatment Hot Topics in Hypertens2011 47ndash23
32 OrsquoBrien E Why ABPM should be mandatory in all trials of bloodpressure-lowering drugs Drug Inform J 2011 45233ndash239
33 Staessen JA Byttebier G Buntinx F Celis H OrsquoBrien ET Fagard RAntihypertensive treatment based on conventional or ambulatoryblood pressure measurement A randomized controlled trial Ambu-latory Blood Pressure Monitoring and Treatment of HypertensionInvestigators JAMA 1997 2781065ndash1072
34 Clement DL De Buyzere M De Bacquer DA de Leeuw PW DuprezDA Fagard RH et al for the Office Versus Ambulatory BP (OvA)Study Investigators Prognostic value of ambulatory blood-pressurerecordings in patients with treated hypertension N Engl J Med 2003348207ndash215
35 Palatini P Dorigatti F Mugellini A Spagnuolo V Van N Ferrara RBertocchi F Ambulatory versus clinic BP for the assessment ofantihypertensive efficacy in clinical trials insights from the Val-SystStudy Clin Ther 2004 261436ndash1445
36 Krakoff LR Cost-effectiveness of ambulatory blood pressure a rean-alysis Hypertension 2006 4729ndash34
37 Fischer MA Avorn J Economic implications of evidence-based pre-scribing for hypertension can better care cost less JAMA 20042911850ndash1856
38 Lovibond K Jowett S Barton P Caulfield M Heneghan C Hobbs FDRet al Cost-effectiveness of options for the diagnosis of high bloodpressure in primary care a modeling study Lancet 2011 3781219ndash1230
39 Zanchetti A Mancia G Longing for clinical excellence a criticaloutlook into the NICE recommendations on hypertension manage-ment ndash is nice always good J Hypertens 2012 30660ndash668
40 Tamaki Y Ohkubo T Kobayashi M Sato K Kikuya M Obara T et alCost-effectiveness of hypertension treatment based on the measure-ment of ambulatory blood pressure Yakugaku Zasshi 2010 130805ndash820
41 Palatini P Mormino P Canali C Santonastaso M De Venuto G ZanataG Pessina AC Factors affecting ambulatory blood pressure reprodu-cibility Results of the HARVEST Trial Hypertension and AmbulatoryRecording Venetia Study Hypertension 1994 23211ndash216
42 OrsquoBrien E Atkins N Stergiou G Karpettas N Parati G Asmar R et alWorking Group on Blood Pressure Monitoring of the EuropeanSociety of Hypertension European Society of Hypertension Inter-national Protocol revision 2010 for the validation of blood pressuremeasuring devices in adults Blood Press Monit 2010 1523ndash38
43 Noninvasive sphygmomanometers Part 2 Clinical validation of auto-mated measurement type American National Standards InstituteANSIAAMIISO 81060-2 2009 httpwebstoreansiorg
44 OrsquoBrien E Petrie J Littler WA De Swiet M Padfield PL Altman D et alThe British Hypertension Society protocol for the evaluation of bloodpressure measuring devices J Hypertens 1993 11 (Suppl 2)S43ndashS63
45 Noninvasive sphygmomanometers clinical validation of automatedmeasurement type International Organization for Standardization(ISO) 81060-2 2009 wwwisoorg
46 Omboni S Costantini C Pini C Bulegato R Manfellotto D Rizzoni Det al PANET International Quality Certification Protocol for bloodpressure monitors Blood Press Monit 2008 13285ndash289
47 Lurbe E Sorof J Daniels S Clinical and research aspects of ambulatoryblood pressure monitoring in children J Pediatr 2004 1447ndash16
48 Natarajan P Shennan AH Penny J Halligan AW de Swiet M AnthonyJ Comparison of auscultatory and oscillometric automated bloodpressure monitors in the setting of preeclampsia Am J Obstet Gynecol1999 1811203ndash1210
49 Duley L The global impact of preeclampsia and eclampsia SeminPerinatol 2009 33130ndash137
50 Shennan A Gupta M Halligan A Taylor DJ de Swiet M Lack ofreproducibility in pregnancy of Korotkoff phase IV as measured bymercury sphygmomanometry Lancet 1996 347139ndash142
51 Clark C Campbell J Evans P Millward A Prevalence and clinicalimplications of the inter-arm blood pressure difference a systematicreview J Hum Hypertens 2006 20923ndash931
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
52 Stergiou GS Kollias A Destounis A Tzamouranis D Automatedblood pressure measurement in atrial fibrillation a systematic reviewand meta-analysis J Hypertens 2012 302074ndash2082
53 Graves JW Prevalence of blood pressure cuff sizes in a referralpractice of 430 consecutive adult hypertensives Blood Press Monit2001 617ndash20
54 Thompson AM Eguchi K Reznik ME Shah SS Pickering TGValidation of an oscillometric home blood pressure monitor in anend-stage renal disease population and the effect of arterial stiffnesson its accuracy Blood Press Monit 2007 12227ndash232
55 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Bloodpressure surge on rising J Hypertens 2004 221113ndash1118
56 Parati G de Buyzere M Evaluating aortic stiffness through an arm cuffoscillometric device is validation against invasive measurementsenough J Hypertens 2010 282003ndash2006
57 Octavio JA Contreras J Amair P Octavio B Fabiano D Moleiro Fet al Time-weighted vs conventional quantification of 24-h averagesystolic and diastolic ambulatory blood pressures J Hypertens 201028459ndash464
58 McGowan N Atkins N OrsquoBrien E Padfield P Computerised reportingimproves the clinical use of ambulatory blood pressure measurementBlood Press Monit 2010 15115ndash123
59 OrsquoBrien E Atkins N Can improved software facilitate the wider use ofambulatory blood pressure measurement in clinical practice BloodPress Monit 2004 9237ndash241
60 Dolan E Thijs L Li Y Atkins N McCormack P McClory S et alAmbulatory arterial stiffness index as a predictor of cardiovascularmortality in the Dublin Outcome Study Hypertension 2006 47365ndash370
61 Kollias A Stergiou GS Dolan E OrsquoBrien E Ambulatory arterial stiff-ness index a systematic review and meta-analysis Atherosclerosis2012 224291ndash301
62 Head GA McGrath BP Mihailidou AS Nelson MR Schlaich MPStowasser M et al Ambulatory blood pressure monitoring in Australia2011 consensus position statement J Hypertens 2012 30253ndash266
63 Nobre F Mion D Jr Is the area under blood pressure curve the bestparameter to evaluate 24-h ambulatory blood pressure monitoringdata Blood Press Monit 2005 10263ndash270
64 White WB Blood pressure load and target organ effects in patientswith essential hypertension J Hypertens Suppl 1991 9S39ndashS41
65 Atkinson G Leary AC George KP Murphy MB Jones H 24-hvariation in the reactivity of rate-pressure-product to everydayphysical activity in patients attending a hypertension clinic Chrono-biol Int 2009 26958ndash973
66 Li Y Wang JG Dolan E Gao PJ Guo HF Nawrot T et al Ambulatoryarterial stiffness index derived from 24-h ambulatory blood pressuremonitoring Hypertension 2006 47359ndash364
67 Schillaci G Parati G Pirro M Pucci G Mannarino MR Sperandini LMannarino E Ambulatory arterial stiffness index is not a specificmarker of reduced arterial compliance Hypertension 2007 49986ndash991
68 Gavish B Ben Dov IZ Bursztyn M Linear relationship betweensystolic and diastolic blood pressure monitored over 24 h assessmentand correlates J Hypertens 2008 26199ndash209
69 Kips JG Vermeersch SJ Reymond P Boutouyrie P Stergiopulos NLaurent S et al Ambulatory arterial stiffness index does not accuratelyassess arterial stiffness J Hypertens 2012 30574ndash580
70 Gosse P Lasserre R Minifie C Lemetayer P Clementy J Arterialstiffness evaluated by measurement of the QKd interval is an inde-pendent predictor of cardiovascular events Am J Hypertens 200518470ndash476
71 Parati G Omboni S Rizzoni D Agabiti-Rosei E Mancia G Thesmoothness index a new reproducible and clinically relevantmeasure of the homogeneity of the blood pressure reduction bytreatment for hypertension J Hypertens 1998 161685ndash1691
72 Parati G Blood pressure variability its measurement and significancein hypertension J Hypertens 2005 23 (Suppl 1)S19ndashS25
73 Omboni S Parati G Mancia G The troughpeak ratio and the smooth-ness index in the evaluation of control of 24 h blood pressure bytreatment in hypertension Blood Press Monit 1998 3201ndash204
74 Parati G Schumacher H Bilo G Mancia G Evaluating 24-h antihy-pertensive efficacy by the smoothness index a meta-analysis of anambulatory blood pressure monitoring database J Hypertens 2010282177ndash2183
orized reproduction of this article is prohibitedwwwjhypertensioncom 1763
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
OrsquoBrien et al
75 Verdecchia P Angeli F Borgioni C Gattobigio R Reboldi G Ambu-latory blood pressure and cardiovascular outcome in relation toperceived sleep deprivation Hypertension 2007 49777ndash783
76 Fagard R Brguljan J Thijs L Staessen J Prediction of the actual awakeand asleep blood pressures by various methods of 24h pressureanalysis J Hypertens 1996 14557ndash563
77 Parati G Rizzoni D Omboni S Bernardi L Mormino P Di Rienzo MThe analysis of blood pressure and heart rate variability methodo-logical aspects and interpretation of results High Blood Press 19954186ndash203
78 Winnicki M Canali C Mormino P Palatini P Ambulatory bloodpressure monitoring editing criteria is standardization needed Hy-pertension and Ambulatory Recording Venetia Study (HARVEST)Group Italy Am J Hypertens 1997 10419ndash427
79 OrsquoBrien E A century of confusion which bladder for accurate bloodpressure measurement J Hum Hypertens 1996 10565ndash572
80 OrsquoBrien E Petrie J Littler WA de Swiet M Padfield PD Dillon MJet al Blood pressure measurement recommendations of the BritishHypertension Society 3rd ed London BMJ Publishing Group 1997
81 Pickering TG Hall JE Appel LJ Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Circulation 2005111697ndash716
82 Bonso E Saladini F Zanier A Benetti E Dorigatti F Palatini PAccuracy of a single rigid conical cuff with standard-size bladdercoupled to an automatic oscillometric device over a wide range of armcircumferences Hypertens Res 2010 331186ndash1191
83 Schell K Bradley E Bucher L Seckel M Lyons D Wakai S et alClinical comparison of automatic noninvasive measurements ofblood pressure in the forearm and upper arm Am J Crit Care2005 14232ndash241
84 Imholz BP Wieling W van Montfrans GA Wesseling KH Fifteenyears experience with finger arterial pressure monitoring assessmentof the technology Cardiovasc Res 1998 38605ndash616
85 Hogan JL Maguire P Farah N Kennelly MM Stuart B Turner MJBody mass index and blood pressure measurement during preg-nancy Hypertens Pregnancy 2011 30396ndash400
86 Verdecchia P OrsquoBrien E Pickering T Staessen JA Parati G Myers MPalatini P European Society of Hypertension Working Group onBlood Pressure Monitoring When to suspect white coat hyperten-sion Statement from the Working Group on Blood Pressure Monitor-ing of the European Society of Hypertension Am J Hypertens 20031687ndash91
87 Williams B Poulter NR Brown MJ Davis M McInnes GT Potter JFet al Guidelines for management of hypertension report of the fourthworking party of the British Hypertension Society 2004-BHS IVJ Hum Hypertens 2004 18139ndash185
88 Pickering TG Hall JE Appel LA Falkner BE Graves J Hill MN et alRecommendations for blood pressure measurement in humans andexperimental animals Part 1 blood pressure measurement inhumans a statement for professionals from the Subcommittee ofProfessional and Public Education of the American Heart AssociationCouncil on High Blood Pressure Research Hypertension 200545142ndash161
89 Alessi A Brandao AA Pierin A Feitosa AM Machado CA de MoraesForjaz CL et al Sociedade Brasileira de Cardiologia SociedadeBrasileira de Hipertensao Sociedade Brasileira de Nefrologia IVGuideline for ambulatory blood pressure monitoring II Guidelinefor home blood pressure monitoring IV ABPMII HBPM Arq BrasCardiol 2005 85 (Suppl 2)1ndash18
90 Parati G Omboni S Palatini P Rizzoni D Bilo G Valentini M et alItalian Society of Hypertension guidelines for conventional andautomated blood pressure measurement in the office at home andover 24h High Blood Press Cardiovasc Prev 2008 15283ndash310
91 Ogihara T Kikuchi K Matsuoka H Fujita T Higaki J Horiuchi Met al Japanese Society of Hypertension Committee The JapaneseSociety of Hypertension Guidelines for the Management of Hyper-tension (JSH 2009) Hypertens Res 2009 323ndash107
92 Canadian Hypertension Education Program (CHEP) Recommen-dations for the Management of Hypertension 2011 httpwwwhypertensioncaimages2012_CHEPRecsFullVersion_EN_HCP1000pdf
Copyright copy Lippincott Williams amp Wilkins Unaut1764 wwwjhypertensioncom
93 Seedat YK Rayner BL Southern African Hypertension Society SouthAfrican Hypertension Guideline S Afr Med J 2012 10257ndash83
94 JCS Joint Working Group Guidelines for the clinical use of 24 hourambulatory blood pressure monitoring (JCS 2010) Circ J 201276508ndash519
95 Pickering TG James GD Boddie C Harshfield GA Blank S LaraghJH How common is white coat hypertension JAMA 1988 259225ndash228
96 Myers MG Valdivieso M Kiss A Use of automated office bloodpressure measurement to reduce the white coat response J Hypertens2009 27280ndash286
97 Hansen TW Li Y Boggia J Thijs L Richart T Staessen JA Predictiverole of nighttime blood pressure Hypertension 2011 573ndash10
98 Hansen TW Kikuya M Thijs L Bjorklund-Bodegard K Kuznetsova TOhkubo T et al IDACO Investigators Prognostic superiority ofdaytime ambulatory over conventional blood pressure in four popu-lations a meta-analasis of 7030 individuals J Hypertens 2007251554ndash1564
99 Fagard RH Cornelissen VA Incidence of cardiovascular events inwhite-coat masked and sustained hypertension versus true normo-tension a meta-analysis J Hypertens 2007 252193ndash2198
100 Mancia G Bombelli M Facchetti R Madotto F Quarti-Trevano F PoloFriz H et al Long-term risk of sustained hypertension in white-coat ormasked hypertension Hypertension 2009 54226ndash232
101 Pierdomenico SD Cuccurullo F Prognostic value of white-coat andmasked hypertension diagnosed by ambulatory monitoring in initiallyuntreated subjects an updated meta analysis Am J Hypertens 20112452ndash58
102 Ugajin T Hozawa A Ohkubo T Asayama K Kikuya M Obara T et alWhite-coat hypertension as a risk factor for the development of homehypertension the Ohasama study Arch Int Med 2005 1651541ndash1546
103 Parati G Ulian L Santucciu C Omboni S Mancia G Differencebetween clinic and daytime blood pressure is not a measure of thewhite coat effect Hypertension 1998 311185ndash1189
104 Myers MG Pseudoresistant hypertension attributed to white-coateffect Hypertension 2012 59532ndash533
105 Calhoun DA Jones D Textor S Goff DC Murphy TP Toto RD et alAmerican Heart Association Professional Education CommitteeResistant hypertension diagnosis evaluation and treatment ndash ascientific statement from the American Heart Association ProfessionalEducation Committee of the Council for High Blood PressureResearch Circulation 2008 117e510ndashe526
106 Mancia G Bertinieri G Grassi G Parati G Pomidossi G Ferrari Aet al Effects of blood pressure measurement by the doctor onpatientrsquos blood pressure and heart rate Lancet 1983 2695ndash698
107 Wing LM Brown MA Beilin LJ Ryan P Reid CM ANBP2 ManagementCommittee and Investigators Second Autralian National Blood Pres-sure Study lsquoReverse white coat hypertensionrsquo in older hypertensivesJ Hypertens 2002 20639ndash644
108 Pickering T Davidson K Gerin W Schwartz JE Masked hypertensionHypertension 2002 40795ndash796
109 Lurbe E Cifkova R Cruickshank JK Dillon MJ Ferreira I Invitti Cet al European Society of Hypertension Management of high bloodpressure in children and adolescents recommendations of the Euro-pean Society of Hypertension J Hypertens 2009 271719ndash1742
110 Stergiou GS Salgami EV Tzamouranis DG Roussias LG Maskedhypertension assessed by ambulatory blood pressure versus homeblood pressure monitoring is it the same phenomenon Am J Hyper-tens 2005 18772ndash778
111 Bobrie G Clerson P Menard J Postel-Vinaya N Chatellier G PlouinPF Masked hypertension a systematic review J Hypertens 2008261715ndash1725
112 Mancia G Facchetti R Bombelli M Grassi G Sega R Long-term risk ofmortality associated with selective and combined elevation in officehome and ambulatory blood pressure Hypertension 2006 47846ndash853
113 Owens P Lyons S OrsquoBrien E Ambulatory blood pressure in thehypertensive population patterns and prevalence of hypertensivesub-forms J Hypertens 1998 161735ndash1743
114 Gomes MAM Pierin AMG Mion D Jr The effect of siesta in parametersof cardiac structure and in interpretation of ambulatory arterial bloodpressure monitoring Arq Bras Cardiol 2000 74314ndash318
115 Staessen J Bulpitt CJ Fagard R Mancia G OrsquoBrien ET Thijs L et alReference values for the ambulatory blood pressure and the blood
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
Guideline
pressure measured at home a population study J Hum Hypertens1991 5355ndash361
116 OrsquoBrien E Sheridan J OrsquoMalley K Dippers and nondippers Lancet1988 2397
117 Ohkubo T Hozawa A Yamaguchi J Kikuya M Ohmori K MichimataM et al Prognostic significance of the nocturnal decline in bloodpressure in individuals with and without high 24-h blood pressure theOhasama study J Hypertens 2002 202183ndash2189
118 Kario K Shimada K Risers and extreme-dippers of nocturnal bloodpressure in hypertension antihypertensive strategy for nocturnalblood pressure Clin Exp Hypertens 2004 26177ndash189
119 Metoki H Ohkubo T Kikuya M Asayama K Obara T Hashimoto Jet al Prognostic significance for stroke of a morning pressor surge anda nocturnal blood pressure decline the Ohasama study Hypertension2006 47149ndash154
120 Fagard RH Dipping pattern of nocturnal blood pressure in patientswith hypertension Expert Rev Cardiovasc Ther 2009 7599ndash605
121 Boggia J Li Y Thijs L Hansen TW Kikuya M Bjorklund-Bodegard Ket al International Database on Ambulatory blood pressure monitor-ing in relation to Cardiovascular Outcomes (IDACO) InvestigatorsPrognostic accuracy of day versus night ambulatory blood pressure acohort study Lancet 2007 3701219ndash1229
122 Fan HQ Li Y Thijs L Hansen TW Boggia J Kikuya M et alInternational Database on Ambulatory Blood Pressure In Relationto Cardiovascular Outcomes Investigators Prognostic value of iso-lated nocturnal hypertension on ambulatory measurement in 8711individuals from 10 populations J Hypertens 2010 282036ndash2045
123 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al European Respiratory Society EU COST ACTION B26 membersPosition paper on the management of patients with obstructive sleepapnea and hypertension joint recommendations by the EuropeanSociety of Hypertension by the European Respiratory Society and bythe members of European COST (COoperation in Scientific andTechnological research) ACTION B26 on obstructive sleep apneaJ Hypertens 2012 30633ndash646
124 Graham SL Drance SM Nocturnal hypotension role in glaucomaprogression Surv Ophthalmol 1999 43 (Suppl 1)S10ndashS16
125 Omboni S Parati G Palatini P Vanasia A Muiesan ML Cuspidi CMancia G Reproducibility and clinical value of nocturnal hypoten-sion prospective evidence from the SAMPLE study J Hypertens 199816733ndash738
126 Staessen JA Thijs L Fagard R OrsquoBrien ET Clement D de Leeuw PWet al Predicting cardiovascular risk using conventional vs ambulatoryblood pressure in older patients with systolic hypertension SystolicHypertension in Europe Trial Investigators JAMA 1999 282539ndash546
127 Ingelsson E Bjorklund-Bodegard K Lind L Arnlov J Sundstrom JDiurnal blood pressure pattern and risk of congestive heart failureJAMA 2006 2952859ndash2866
128 Verdecchia P Schillaci G Guerrieri M Gatteschi C Benemio GBoldrini F Porcellati C Circadian blood pressure changes and leftventricular hypertrophy in essential hypertension Circulation 199081528ndash536
129 Hoshide S Kario K Hoshide Y Umeda Y Hashimoto T Kunii O et alAssociations between nondipping of nocturnal blood pressuredecrease and cardiovascular target organ damage in strictly selectedcommunity-dwelling normotensives Am J Hypertens 2003 16434ndash438
130 Cappuccio FP Cooper D DrsquoElia L Strazzullo P Miller MA Sleepduration predicts cardiovascular outcomes a systematic review andmeta-analysis of prospective studies Eur Heart J 2011 321484ndash1489
131 Castiglioni P Parati G Brambilla L Brambilla V Gualerzi M Di RienzoM Coruzzi P Detecting sodium-sensitivity in hypertensive patientsInformation from 24-h ambulatory blood pressure monitoringHypertension 2011 57180ndash185
132 de la Sierra A Lluch MM Coca A Aguilera MT Sanchez M Sierra CUrbano-Marquez A Assessment of salt sensitivity in essential hyper-tension by 24-h ambulatory blood pressure monitoring Am J Hyper-tens 1995 8970ndash977
133 Kario K Ishikawa J Pickering TG Hoshide S Eguchi K Morinari Met al Morning hypertension the strongest independent risk factor forstroke in elderly hypertensive patients Hypertens Res 2006 29581ndash587
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
134 Head GA Reid CM Shiel LM Jennings GL Lukoshkova EV Rate ofmorning rise in blood pressure is elevated in hypertensives Am JHypertens 2006 191010ndash1017
135 Sega R Corrao G Bombelli M Beltrame L Facchetti R Grassi G et alBlood pressure variability and organ damage in a general populationresults from the PAMELA study (Pressioni Arteriose Monitorate E LoroAssociazioni) Hypertension 2002 39710ndash714
136 Verdecchia P Angeli F Mazzotta G Garofoli M Ramundo E GentileG et al Day-night dip and early-morning surge in blood pressurein hypertension prognostic implications Hypertension 2012 6034ndash42
137 Giles TD Circadian rhythm of blood pressure and the relation tocardiovascular events J Hypertens 2006 24 (suppl 2)S11ndashS16
138 American Academy of Sleep Medicine International classification ofsleep disorders 2nd ed Diagnostic and coding manual WestchesterIL American Academy of Sleep Medicine 2005
139 Coccagna G Mantovani M Brignani F Parchi C Lugaresi E Con-tinuous recording of the pulmonary and systemic arterial pressureduring sleep in syndromes of hypersomnia with periodic breathingBull Physiopathol Respir (Nancy) 1972 81159ndash1172
140 McNicholas WT Bonsigore MR Sleep apnoea as an independent riskfactor for cardiovascular disease current evidence basic mechanismsand research priorities Eur Respir J 2007 29156ndash178
141 Mancia G Laurent S Agabiti-Rosei E Ambrosioni E Burnier MCaulfield MJ et al European Society of Hypertension Reappraisalof European guidelines on hypertension management a EuropeanSociety of Hypertension Task Force document J Hypertens 2009272121ndash2158
142 Nieto FJ Young TB Lind BK Shahar E Samet JM Redline S et alAssociation of sleep-disordered breathing sleep apnea and hyper-tension in a large community-based study Sleep Heart Health StudyJAMA 2000 2831829ndash1836
143 Peppard PE Young T Palta M Skatrud J Prospective study of theassociation between sleep-disordered breathing and hypertensionN Engl J Med 2000 3421378ndash1384
144 Calhoun DA Obstructive sleep apnea and hypertension Curr Hyper-tens Rep 2010 12189ndash195
145 Somers VK Dyken ME Clary MP Abboud FM Sympathetic neuralmechanisms in obstructive sleep apnea J Clin Invest 1995 961897ndash1904
146 Dudenbostel T Calhoun DA Resistant hypertension obstructivesleep apnoea and aldosterone J Hum Hypertens 2012 26281ndash287
147 Parati G Lombardi C Hedner J Bonsignore MR Grote L Tkacova Ret al EU COST Action B26 members Recommendations of themanagement of patients with obstructive sleep apnea and hyperten-sion Eur Respir J 2013 41523ndash538
148 Di Rienzo M Grassi G Pedotti A Mancia G Continuous vs inter-mittent blood pressure measurements in estimating 24-h averageblood pressure Hypertension 1983 5264ndash269
149 Mancia G Bombelli M Facchetti R Madotto F Corrao G Trevano FQet al Long-term prognostic value of blood pressure variability in thegeneral population results of the Pressioni Arteriose Monitorate eLoro Associazioni Study Hypertension 2007 491265ndash1270
150 Kikuya M Ohkubo T Metoki H Asayama K Hara A Obara T et alDay-by-day variability of blood pressure and heart rate at home as anovel predictor of prognosis the Ohasama study Hypertension 2008521045ndash1050
151 Rothwell PM Howard SC Dolan E OrsquoBrien E Dobson JE Dahlof Bet al Prognostic significance of visit-to-visit variability maximumsystolic blood pressure and episodic hypertension Lancet 2010375895ndash905
152 Sander D Kukla C Klingelhofer J Winbeck K Conrad B Relationshipbetween circadian blood pressure patterns and progression of earlycarotid atherosclerosis a 3-year follow-up study Circulation 20001021536ndash1541
153 Pringle E Phillips C Thijs L Davidson C Staessen JA de Leeuw PWet al Systolic blood pressure variability as a risk factor for stroke andcardiovascular mortality in the elderly hypertensive populationJ Hypertens 2003 212251ndash2257
154 Hansen TW Thijs L Li Y Boggia J Kikuya M Bjorklund-Bodegard Ket al Prognostic value of reading-to-reading blood pressure variabilityover 24 h in 8938 subjects from 11 populations Hypertension 2010551049ndash1057
orized reproduction of this article is prohibitedwwwjhypertensioncom 1765
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
OrsquoBrien et al
155 Lemmer B Clinical chronopharmacology of the cardiovascular sys-tem hypertension and coronary heart disease Clin Ter 2006 15741ndash52
156 Eguchi K Hoshide S Schwartz JE Shimada K Kario K Visit-to-visitand ambulatory blood pressure variability as predictors of incidentcardiovascular events in patients with hypertension Am J Hypertens2012 25962ndash968
157 Redon J Roca-Cusachs A Mora-Macia J on behalf of the ACAMPAInvestigators Uncontrolled early morning blood pressure in medi-cated patients the ACAMPA study Blood Press Monit 2002 7111ndash118
158 Ishikawa J Kario K Hoshide S Eguchi K Morinari M Kaneda R et alJ-MORE Study Group Determinants of exaggerated difference inmorning and evening blood pressure measured by self-measuredblood pressure monitoring in medicated hypertensive patients JichiMorning Hypertension Research (J-MORE) study Am J Hypertens2005 18958ndash965
159 de la Sierra A Segura J Banegas JR Gorostidi M de la Cruz JJ ArmarioP et al Clinical features of 8295 patients with resistant hypertensionclassified on the basis of ambulatory blood pressure monitoringHypertension 2011 57898ndash902
160 Redon J Campos C Narciso ML Rodicio JL Pascual JM Ruilope LMPrognostic value of ambulatory blood pressure monitoring in refrac-tory hypertension a prospective study Hypertension 1998 31712ndash718
161 Pierdomenico SD Lapenna D Bucci A Di Tommaso R Di Mascio RManente BM et al Cardiovascular outcome in treated hypertensivepatients with responder masked false resistant and true resistanthypertension Am J Hypertens 2005 181422ndash1428
162 Salles GF Cardoso CR Muxfeldt ES Prognostic influence of office andambulatory blood pressures in resistant hypertension Arch InternMed 2008 1682340ndash2346
163 Muxfeldt ES Cardoso CR Salles GF Prognostic value of nocturnalblood pressure reduction in resistant hypertension Arch Intern Med2009 169874ndash880
164 Grodzicki T Rajzer M Fagard R OrsquoBrien ET Thijs L Clement D et alAmbulatory blood pressure monitoring and postprandial hypoten-sion in elderly patients with isolated systolic hypertension SystolicHypertension in Europe (SYST-EUR) Trial Investigators J Hum Hyper-tens 1998 12161ndash165
165 Pickering TG Miller NH Ogedegbe G Krakoff LR Artinian NT GoffD American Heart Association American Society of HypertensionPreventive Cardiovascular Nurses Association Call to action on useand reimbursement for home blood pressure monitoring executivesummary a joint scientific statement from the American Heart Associ-ation American Society of Hypertension and Preventive Cardiovas-cular Nurses Association Hypertension 2008 521ndash9
166 Verdecchia P Reboldi GP Angeli F Schillaci G Schwartz JE Pick-ering TG et al Short- and long-term incidence of stroke in white-coathypertension Hypertension 2005 45203ndash208
167 Suzuki Y Kuwajima I Aono T Kanemaru A Nishinaga M Shibata HOzawa T Prognostic value of nighttime blood pressure in the elderlya prospective study of 24-h blood pressure Hypertens Res 200023323ndash330
168 Fagard RH Van Den Broeke C De Cort P Prognostic significance ofblood pressure measured in the office at home and during ambu-latory monitoring in older patients in general practice J Hum Hyper-tens 2005 19801ndash807
169 Staessen JA Thijs L OrsquoBrien ET Bulpitt CJ de Leeuw PW Fagard RHet al Syst-Eur Trial Investigators Ambulatory pulse pressure aspredictor of outcome in older patients with systolic hypertensionAm J Hypertens 2002 15835ndash843
170 Verdecchia P Schillaci G Reboldi G Franklin SS Porcellati CDifferent prognostic impact of 24-h mean blood pressure and pulsepressure on stroke and coronary artery disease in essential hyperten-sion Circulation 2001 1032579ndash2584
171 Gorostidi M de la Sierra A Gonzalez-Albarran O Segura J de la CruzJJ Vinyoles E et al Spanish Society of Hypertension ABPM Registryinvestigators Abnormalities in ambulatory blood pressure monitoringin hypertensive patients with diabetes Hypertens Res 2011 341185ndash1189
172 Yano Y Inokuchi T Hoshide S Kanemaru Y Shimada K Kario KAssociation of poor physical function and cognitive dysfunction with
Copyright copy Lippincott Williams amp Wilkins Unaut1766 wwwjhypertensioncom
high nocturnal blood pressure level in treated elderly hypertensivepatients Am J Hypertens 2011 24285ndash291
173 Kario K Matsuo T Kobayashi H Imiya M Matsuo M Shimada KNocturnal fall of blood pressure and silent cerebrovascular damage inelderly hypertensive patients Advanced silent cerebrovascular dam-age in extreme dippers Hypertension 1996 27130ndash135
174 Kario K Pickering TG Matsuo T Hoshide S Schwartz JE Shimada KStroke prognosis and abnormal nocturnal blood pressure falls in olderhypertensives Hypertension 2001 38852ndash857
175 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Night-day blood pressure ratio and dipping pattern aspredictors of death and cardiovascular events in hypertension J HumHypertens 2009 23645ndash653
176 Fagard RH De Cort P Orthostatic hypotension is a more robustpredictor of cardiovascular events than nighttime reverse dipping inelderly Hypertension 2010 5656ndash61
177 Kario K Pickering TG Blood pressure variability in elderly patientsLancet 2000 3551645ndash1646
178 Stergiou GS Vemmos KN Pliarchopoulou KM Synetos AG RoussiasLG Mountokalakis TD Parallel morning and evening surge in strokeonset blood pressure and physical activity Stroke 2002 331480ndash1486
179 National High Blood Pressure Education Program Working Groupon High Blood Pressure in Children and Adolescents The FourthReport on the Diagnosis Evaluation and Treatment of High BloodPressure in Children and Adolescents Pediatrics 2004 114 (Suppl 2)555ndash576
180 Urbina E Alpert B Flynn J Hayman L Harshfield GA Jacobson Met al American Heart Association Atherosclerosis Hypertension andObesity in Youth Committee Ambulatory blood pressure monitoringin children and adolescents recommendations for standard assess-ment a scientific statement from the American Heart AssociationAtherosclerosis Hypertension and Obesity in Youth Committee ofthe Council on Cardiovascular Disease in the Young and the Councilfor High Blood Pressure Research Hypertension 2008 52433ndash451
181 Lurbe E Redon J Kesani A Pascual JM Tacons J Alvarez V Batlle DIncrease in nocturnal blood pressure and progression to microalbu-minuria in type 1 diabetes N Engl J Med 2002 347797ndash805
182 Soergel M Kirschstein M Busch C Danne T Gellermann J Holl Ret al Oscillometric twenty-four-hour ambulatory blood pressurevalues in healthy children and adolescents a multicenter trial includ-ing 1141 subjects J Pediatr 1997 130178ndash184
183 Wuhl E Witte K Soergel M Mehls O Schaefer F Kirschstein M et alGerman Working Group on Pediatric Hypertension Distribution of24-h ambulatory blood pressure in children normalized referencevalues and role of body dimensions J Hypertens 2002 201995ndash2007
184 Brown MA Davis GK McHugh L The prevalence and clinicalsignificance of nocturnal hypertension in pregnancy J Hypertens2001 191437ndash1444
185 Bellomo G Narducci PL Rondoni F Pastorelli G Stangoni G AngeliG Verdecchia P Prognostic value of 24-h blood pressure in preg-nancy JAMA 1999 2821447ndash1452
186 Waugh J Perry IJ Halligan AW De Swiet M Lambert PC Penny JAet al Birth weight and 24-h ambulatory blood pressure in non-proteinuric hypertensive pregnancy Am J Obstet Gynecol 2000183633ndash637
187 Higgins JR Walshe JJ Halligan A OrsquoBrien E Conroy R Darling MRCan 24-h ambulatory blood pressure measurement predict the devel-opment of hypertension in primigravidae Br J Obstet Gynaecol 1997104356ndash362
188 Magee LA Helewa M Moutquin JM von Dadelszen P Diagnosisevaluation and management of the hypertensive disorders of preg-nancy JOGC 2008 30 (Suppl1)S1ndash48
189 Higgins JR de Swiet M Blood-pressure measurement and classifi-cation in pregnancy Lancet 2001 357131ndash135
190 Brown MA Robinson A Bowyer L Buddle ML Martin A Hargood JLCario GM Ambulatory blood pressure monitoring in pregnancy whatis normal Am J Obstet Gynecol 1998 178836ndash842
191 Strachan MW Gough K McKnight JA Padfield PL Ambulatory bloodpressure monitoring is it necessary for the routine assessment ofhypertension in people with diabetes Diabet Med 2002 19787ndash789
horized reproduction of this article is prohibitedVolume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013
Guideline
192 OrsquoBrien E Turner R Assessing blood pressure responses to non-cardiovascular drugs the beneficial role of ambulatory blood pres-sure monitoring J Clin Hypertens 2013 1555ndash62
193 Sager P Heilbraun J Turner R Gintant G Geiger MJ Kowey PR et alAssessment of drug-induced increases in blood pressure during drugdevelopment report from the Cardiac Safety Research ConsortiumAm Heart J 2013 165477ndash488
194 Cardoso CR Leite NC Muxfeldt ES Salles GF Thresholds of ambu-latory blood pressure associated with chronic complications in type 2diabetes Am J Hypertens 2012 2582ndash88
195 Gorostidi M Sobrino J Segura J Sierra C de la Sierra A Hernandez delRey R et al Spanish Society of Hypertension ABPM Registry inves-tigators Ambulatory blood pressure monitoring in hypertensivepatients with high cardiovascular risk a cross-sectional analysis ofa 20 000-patient database in Spain J Hypertens 2007 25977ndash984
196 Fagard RH Thijs L Staessen JA Clement DL De Buyzere ML DeBacquer DA Prognostic significance of ambulatory blood pressure inhypertensive patients with history of cardiovascular disease BloodPress Monit 2008 13325ndash332
197 Agarwal R Brim NJ Mahenthiran J Andersen MJ Saha C Out-of-hemodialysis-unit blood pressure is a superior determinant of leftventricular hypertrophy Hypertension 2006 4762ndash68
198 Tripepi G Fagugli RM Dattolo P Parlongo G Mallamaci F Buon-cristiani U Zoccali C Prognostic value of 24-h ambulatory bloodpressure monitoring and of nightday ratio in nondiabetic cardio-vascular events-free hemodialysis patients Kidney Int 2005 681294ndash1302
199 Minutolo R Agarwal R Borrelli S Chiodini P Bellizzi V Nappi F et alPrognostic role of ambulatory blood pressure measurement inpatients with nondialysis chronic kidney disease Arch Intern Med2011 1711090ndash1098
200 Agarwal R Andersen MJ Prognostic importance of ambulatory bloodpressure recordings in patients with chronic kidney disease KidneyInt 2006 691175ndash1180
201 Agarwal R Andersen MJ Light RP Location not quantity of bloodpressure measurements predicts mortality in hemodialysis patientsAm J Nephrol 2008 28210ndash217
202 Agarwal R Blood pressure and mortality among hemodialysispatients Hypertension 2010 55762ndash768
203 Liu M Takahashi H Morita Y Maruyama S Mizuno M Yuzawa Yet al Nondipping is a potent predictor of cardiovascular mortality andis associated with autonomic dysfunction in haemodialysis patientsNephrol Dial Transplant 2003 18563ndash569
204 Redon J Plancha E Swift PA Pons S Munoz J Martinez F Nocturnalblood pressure and progression to end-stage renal disease or death innondiabetic chronic kidney disease stages 3 and 4 J Hypertens 201028602ndash607
205 Farmer CK Goldsmith DJ Quin JD Dallyn P Cox J Kingswood JCet al Progression of diabetic nephropathy is diurnal blood pressurerhythm as important as absolute blood pressure level Nephrol DialTransplant 1998 13635ndash639
206 Timio M Venanzi S Lolli S Lippi G Verdura C Monarca C Guerrini ENondipperrsquo hypertensive patients and progressive renal insufficiencya 3-year longitudinal study Clin Nephrol 1995 43382ndash387
207 Senard JM Blood pressure disorders during idiopathic Parkinsonrsquosdisease Presse Med 2003 321231ndash1237
208 Pathak A Senard JM Blood pressure disorders during Parkinsonrsquosdisease epidemiology pathophysiology and management ExpertRev Neurother 2006 61173ndash1180
209 Imai Y Abe K Sasaki S Minami N Nihei M Munakata M et al Alteredcircadian blood pressure rhythm in patients with Cushingrsquos syndromeHypertension 1988 1211ndash19
210 Fallo F Fanelli G Cipolla A Betterle C Boscaro M Sonino N 24-hblood pressure profile in Addisonrsquos disease Am J Hypertens 199471105ndash1109
211 Fommei E Iervasi G The role of thyroid hormone in blood pressurehomeostasis evidence from short-term hypothyroidism in humansJ Clin Endocrinol Metab 2002 871996ndash2000
212 Zelinka T Pacak K Widimsky J Jr Characteristics of blood pressure inpheochromocytoma Ann N Y Acad Sci 2006 107386ndash93
213 Polonia J Santos AR Gama GM Barros H Accuracy of twenty-four-hour ambulatory blood pressure monitoring (night-day values) for thediagnosis of secondary hypertension J Hypertens 1995 131738ndash1741
Copyright copy Lippincott Williams amp Wilkins UnauthJournal of Hypertension
214 Muxfeldt ES Fiszman R de Souza F Viegas B Oliveira FC Salles GFAppropriate time interval to repeat ambulatory blood pressuremonitoring in patients with white-coat resistant hypertension Hyper-tension 2012 59384ndash389
215 Ohkubo T Imai Y Tsuji I Nagai K Kato J Kikuchi N et al Homeblood pressure measurement has a stronger predictive power formortality than does screening blood pressure measurement a popu-lation-based observation in Ohasama Japan J Hypertens 199816971ndash975
216 Cappuccio FP Kerry SM Forbes L Donald A Blood pressure controlby home monitoring meta-analysis of randomised trials BMJ 2004329145
217 Agarwal R Bills JE Hecht TJ Light RP Role of home blood pressuremonitoring in overcoming therapeutic inertia and improving hyper-tension control a systematic review and meta-analysis Hypertension2011 5729ndash38
218 Sega R Facchetti R Bombelli M Cesana G Corrao G Grassi G ManciaG Prognostic value of ambulatory and home blood pressures com-pared with office blood pressure in the general population follow-upresults from the Pressioni Arteriose Monitorate e Loro Associazioni(PAMELA) study Circulation 2005 1111777ndash1783
219 Parati G Omboni S Bilo G Why is out-of-office blood pressuremeasurement needed Home blood pressure measurements willincreasingly replace ambulatory blood pressure monitoring in thediagnosis and management of hypertension Hypertension 200954181ndash187
220 Craig MW Kenny D Mann S Balasubramanian V Raftery EB Effect ofonce-daily atenolol on ambulatory blood pressure BMJ 1979 1237ndash238
221 Mancia G Parati G Office compared with ambulatory blood pressurein assessing response to antihypertensive treatment a meta-analysisJ Hypertens 2004 22435ndash445
222 White WB Littlejohn TW Majul CR Oigman W Olvera R Seeber Met al Effects of telmisartan and amlodipine in combination onambulatory blood pressure in stages 1ndash2 hypertension Blood PressMonit 2010 15205ndash212
223 US Food and Drug Administration International Conference onHarmonisation (ICH) Guidance on statistical principles for clinicaltrials Federal Reg 1998 6349583ndash49598 Available from URL httpwwwfdagovdownloadsDrugsGuidanceComplianceRegulatoryInformationGuidancesucm 073147pdf [Accessed 14 January2011]
224 European Medical Agency Committee for Medicinal Products forHuman Use Guideline on clinical investigation of medicinal productsin the treatment of hypertension London 18 November 2010 EMA2381995Rev 3 httpwwwemaeuropaeudocsen_GBdocument_libraryScientific_guideline201012WC500100191pdf
225 Ohkubo T Hozawa A Nagai K Kikuya M Tsuji I Ito S et alPrediction of stroke by ambulatory blood pressure monitoring versusscreening blood pressure measurements in a general population theOhasama study J Hypertens 2000 18847ndash854
226 Khattar RS Senior R Lahiri A Cardiovascular outcome in white-coat versus sustained mild hypertension a 10-year follow-upstudyCirculation 1998 981892ndash1897
227 Myers MG Implications of ambulatory blood pressure monitoringsubstudies on the interpretation of clinical trials in hypertensionshould the threshold for drug therapy be lower in older patientsJ Clin Hypertens 2011 13703ndash705
228 Bulpitt CJ Beckett N Peters R Staessen JA Wang JG Comsa M et alDoes white coat hypertension require treatment over age 80 Resultsof the hypertension in the very elderly trial ambulatory blood pressureside project Hypertension 2013 6189ndash94
229 Mancia G Parati G Bilo G Maronati A Omboni S Baurecht H et alAssessment of long-term antihypertensive treatment by clinic andambulatory blood pressure data from the European Lacidipine Studyon Atherosclerosis J Hypertens 2007 251087ndash1094
230 Mancia G Parati G Bilo G Choi J Kilama MO Ruilope LM TALENTinvestigators Blood pressure control by the nifedipine GITS-telmi-sartan combination in patients at high cardiovascular risk the TALENTstudy J Hypertens 2011 29600ndash609
231 Fagard RH Staessen JA Thijs L Relationships between changes inleft ventricular mass and in clinic and ambulatory blood pressure inresponse to antihypertensive treatment J Hypertens 1997 151493ndash1502
orized reproduction of this article is prohibitedwwwjhypertensioncom 1767
OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013

OrsquoBrien et al
232 ESH Hypertension Excellence Centres a new strategy to combat anold foe Blood Press 2007 16276ndash277
233 Stergiou GS Myers MG Reid JL Burnier M Narkiewicz K Viigimaa MMancia G Setting-up a blood pressure and vascular protection clinicrequirements of the European Society of Hypertension J Hypertens2010 281780ndash1781
234 White WB Kostis JB Leadership message American Society ofHypertension-designated centers of excellence a new initiativeJ Clin Hypertens 2011 13391ndash392
235 Little P Barnett J Barnsley L Marjoram J Fitzgerald-Barron A Mant DComparison of agreement between different measures of bloodpressure in primary care and daytime ambulatory blood pressureBMJ 2002 325254
236 Uallachain GN Murphy G Avalos G The RAMBLER study the role ofambulatory blood pressure measurement in routine clinical practice ndasha cross-sectional study Ir Med J 2006 99276ndash279
237 Banegas JR Segura J Sobrino JRodrıguez-ArtalejoFde laSierraAde laCruz JJ et al Spanish Society of Hypertension Ambulatory BloodPressure Monitoring Registry Investigators Effectiveness of blood pres-sure control outside the medical setting Hypertension 2007 4962ndash68
238 Lee JK Grace KA Taylor AJ Effect of a pharmacy care program onmedication adherence and persistence blood pressure and low-density lipoprotein cholesterol a randomized controlled trial JAMA2006 2962563ndash2571
Copyright copy Lippincott Williams amp Wilkins Unaut
References cited in the text with the letter w asupplementary file httplinkslwwcomHJHA28
1768 wwwjhypertensioncom
239 Green BB Cook AJ Ralston JD Fishman PA Catz SL Carlson J et alEffectiveness of home blood pressure monitoring web communi-cation and pharmacist care on hypertension control A randomizedcontrolled trial JAMA 2008 2992857ndash2867
240 Gliklich RE Dreyer NA editors Registries for evaluating patient out-comes a userrsquos guide 2nd ed [Prepared by Outcome DEcIDE Center(Outcome Sciences Inc dba Outcome) under Contract NoHHSA29020050035I TO3] AHRQ Publication No10-EHC049 Rock-ville MD Agency for Healthcare Research and Quality September2010
241 National disease registries for advancing healthcare Lancet 20113782050
242 Imai Y Nagai K Sakuma M Sakuma H Nakatsuka H Satoh H et alAmbulatory blood pressure of adults in Ohasama Japan Hyperten-sion 1993 22900ndash912
243 Boggia J Thijs L Hansen TW Li Y Kikuya M Bjorklund-Bodegard Ket al on behalf of the International Database on Ambulatoryblood pressure in relation to Cardiovascular Outcomes (IDACO)Investigators Ambulatory blood pressure monitoring in 9357subjects from 11 populations highlights missed opportunities forcardiovascular prevention in women Hypertension 2011 57397ndash405
244 International Ambulatory Blood Pressure Monitoring Registry ndashARTEMIS httpwwwartemisnetorg
horized reproduction of this article is prohibited
fter the reference number are listed in the3 that accompanies this paper
Volume 31 Number 9 September 2013