Embed Size (px)
Citation preview

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 1
UPDATE – 2/2013 | EuFMD Secretariat
FAO OF
THE UN EuFMD/EC actions funded under MTF/INT/003/EC

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 2

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 3
CONTENTS
Summary .................................................................................................................................................................................... 4
UPDATE : main actions Undertaken between OCTOBER 2012 AND FEBRUARY 2013 ............................................................... 6
Annex I: Iran December report ................................................................................................................................................ 21
Annex II Real Time Training Kenya-Nepal ................................................................................................................................ 32
Annex III Trans-Caucasus Countries: FMD desktop simulation exercise, November 2012; Report by EuFMD consultants. . 36
ANNEX III Trans-Caucasus Countries FMD desktop; Report by C. Danielsson ......................................................................... 56
Annex IV FMD-December report ............................................................................................................................................ 68
The EuFMD .............................................................................................................................................................................. 89

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 4
SUMMARY
This Update is provided to the EuFMD Executive for the 85th
Session of the Executive Committee and should be read
together with the MID-TERM Report (9/2011), Update Report for the 83rd
Session and 84th
Sessions (April and October
2012). Reports to the Executive Committee of the EC are accepted as part of the reporting arrangements to the DG-
SANCO of the European Commission (EC) in fulfillment of the Contract between FAO and the EC relating to funding for the
activities to be conducted by the EuFMD Commission. The current Contract was signed in September 2009 and has a term
of 48 months.
The EuFMD Commission, at the 38th
General Session in April 2009, adopted a four year Strategic Plan of activities,
involving six components, with priorities for in-country actions being to support FMD control in Southeast Europe through
greater management of the FMD risk in countries bordering to Turkey, in West Eurasia. These projects are coordinated
with those of other Directorates of the EC and other funding agencies, to promote progressive control in the West
Eurasian countries along a long term Roadmap.
Following signature of the financing agreement, specific activities of the EuFMD are initiated following response of the EC
to proposals from the Secretariat or decisions of the Executive Committee at which the EC are represented.
The EC support is provided through a Trust Fund (TF), MTF/INT/007/EEC, with a total funding of € 8 million for the four
year period of the current agreement. Since September 2009, the EC has agreed funding of actions in six of the Strategic
Plan components, with by far the largest being for in-country programmes in the Trans-Caucasus and Iran aimed at
reducing the risk of new incursions of FMD into Turkey and Eastern Europe. Funding is also provided for training of
European veterinarians, for surveillance in the African proximity, for short technical studies, and for surveillance for FMD
in Egypt.
In response to FMD outbreaks in Bulgaria in 2011, the TF was used for emergency funding purposes for procurement of
FMD vaccines for re-enforcement of immunity in Turkish Thrace, and thereby protection of the three countries with
common borders. In 2012 emergency missions have been included to Turkey (Asia-1 vaccination effectiveness) and Egypt
and Libya (SAT2 outbreaks). The EC also agreed to supply 500,000 doses of Trivalent A/O/Asia-1 vaccine to the trans-
Caucasus to re-enforce the vaccination campaign in Spring 2012.
At the 39th
Session in April 2011, the EuFMD Commission recommended three additional components. These are
indicated as Components 7-9 below. For two of these, expenditures or activities had not been committed before April
2012, but actions and expenditure has commenced in the current 6 month period (i.e April-September 2012).
In addition, the EC has proposed development of a TRIPARTITE surveillance programme for FMD in Thrace, and the first
activity towards this occurred in September and is reported under Component 1 (Risk reduction in South-East Europe).

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 5
The nine Components summarized in the Update Report are:
1. Risk reduction in South-East Europe through support to FMD control in West Eurasia;
2. Activities to reduce FMD risk in the South and East Mediterranean countries;
3. Field based FMD Training Programme;
4. FMD surveillance in the African proximity;
5. Technical studies;
6. Response to FMD Emergencies.
7. Strengthening FMD laboratories in the Balkan Region;
8. Improved Contingency Planning through use of decision support tools;
9. World Reference Laboratory (WRL) contract – FMD surveillance support activities .
The work under each component is scheduled for completion in 2012 or before completion of the term Funding
Agreement .
Annexes:
Annex I: Iran December report
Annex II: Real-Time Training: Executive Summary of NTC13; Excerpt from Nepal training report
Annex III: Trans-Caucasus Countries: FMD desktop simulation exercise, November 2012; reports by EuFMD
consultants and by external observer.
Annex IV: Monthly report-December2012

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 6
UPDATE : MAIN ACTIONS UNDERTAKEN BETWEEN OCTOBER 2012 AND FEBRUARY 2013
Components 1 to 9 : actions mandated by 39th General Session in 2011 ( EuFMD Workplan for Biennium April 2011-April 2013)
Component Subcomponent Prior (April 2012- September 2012)
Oct 2012-Feb 2013 Reports (examples) Issues /Concerns
[for ExCom awareness]
1. Risk reduction in South-East Europe through support to FMD control in West Eurasia
West Eurasia Roadmap -Secretariat
3rd
Roadmap progress review meeting held in Istanbul, March 2012
Planning for 4th
Roadmap meeting initiated: possible to be held in Baku
Collaboration with: FAO, OIE
Planning and preparation for the 4
th Roadmap Meeting, to
be held in Baku 2-4 April 2013.
Procedure followed for GfTADS labeling of the event; GfTADS Management Committee agreement reached (Jan 2013) that event will be labeled as GfTADS.
Draft agenda is prepared and circulated to GfTADS Regional SC Europe and Mid-East for comments; none received (5
th
Feb).
Report circulated and online (2012 Roadmap meeting)
PCP self-assessment procedure to be followed
[EuFMD PCP experts propose meeting on this in week 10, March4th-)
Funding gaps post- GTFS project to be filled by GTFS extension funds (FAO).
Roadmap Meeting falls 3 weeks before 40
th Session.
Invite AZB as Hosts, to present at 40
th Session ?
Thrace -improved surveillance for early detection of FMD
Support letter from SANCO received.
Workshop held September 18-21
st in
Istanbul (TUR, GRE, BUL)
Surveillance model finalized (AusVet Consultancy).
Invitations issued for Tripartite (TUR,GRE, BG) meeting to finalize surveillance programme for 2013 on 13
th Feb
Report on workshop and surveillance model received. Report to ExCom
Will be identified at TPT Meeting, 13
th Feb.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 7
West Eurasia -Risk assessment
FMD database : transition to EMPRES-i
GEO, ARM, AZER, TURKEY participate in data sharing (monthly)
Collaboration with: EMPRES-i
West Eurasia FMD Database:
Consultation with FMD National consultants (TCC, TUR, Iran) (Istanbul, Dec 2012)on data access. EMPRES-I system software components configured for automated reporting and restricted data access
Turkey: fully participates in data sharing. Mission to resolve GIS mapping of all epi-units and animal demographics.
New participants:
1.MOU with Iran to participate in the database has been drafted and presented to IVO steering committee. 2. Presentation of database to Pakistan (FAO/USAID project) and other potential data-sharing partners during FAO FMD meeting (Rome, Dec 1012)
Monthly FMD vaccination reports (TCC)
Monthly FMD surveillance and vaccination report (Turkey)
Monthly FMD surveillance and vaccination report (Iran).
Lack of animal demographic data and full GIS datasets delayed progress. Resolved after mission to GDPC 1/13.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 8
Component Subcomponent Prior (April 2012- September 2012)
Oct 2012-Feb 2013 Reports (examples) Issues /Concerns
[for ExCom awareness]
West Eurasia- training in progressive control
Practical epidemiology for progressive control (PeP-C) Training course developed and initiated
1st
course (4 weeks over 4 months) delivered, involving 16 trainees from 6 countries (ARM, AZB, GEO, TUR, EGY, IRN)
Ongoing communication with trainees through Wikispace
Reports available from each training week, plus overall report (McLaws BTORs)
Training material on PeP-C Wikispace
Presentation (Prezi) describing course
Excellent collaboration with hosts (Turkey).
Follow-on PEPc courses subject to funding.
How to proceed if other regions/projects wish to “buy” PEPc training.
Relevant Training course for other regions.
WELNET - lab network
Agreement Iraq-Turkey on sample submission to SAP Institute
Activities promoted at no cost to EuFMD/EC:
1. FMDV samples from Iraq transported in RNA later by land route to Turkey, sequenced and analyzed in SAP Institute; results show trans-boundary circulation of A/Iran-05/SIS-10 strain. 2.FMDV sequences shared between Iran and Pirbright. 3.Collaboration with: USAID funded FAO project (Pakistan), on improving capacity for molecular analysis in Pakistan through collaboration with European institutes .
WELNET work programme in 2012 was not funded from EuFMD/EC.
WELNET proposed work programme (March 2012) remains relevant.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 9
Component Subcomponent Prior (April 2012- September 2012)
Oct 2012-Feb 2013 Reports (examples) Issues /Concerns
[for ExCom awareness]
Trans-Caucasus project
Vaccine use assessment mission completed (Krnjaic/Ryan) following EC provision of 500,000 doses of vaccine.
Protocol governing authorization of release of EC-supplied vaccine reserve written.
Project activities on track.
Mission Potzsch (July to GEO, ARM) and project co-ordination mission (Tbilisi).
Final phase activities planned (lab training, Simulation Exercise (lead Consultant: Robert Paul).
Coordination with: USDA & US DTRA activities in Georgia
Activities funded from EC TF:
1.Desktop simulation exercise for Georgia, Armenia and Azerbaijan held in Sighnaghi, Georgia, 6-7 November. Leaders: Carsten Potzsch, Robert Paul, Tsviatko Alexandrov. Observer: C. Danielsson, Swedish Board of Agriculture. 2.Laboratory training course in the use of real-time PCR to detect FMDV held in Tbilisi, 4-8 February, with trainees from all three countries. Trainers: Thomas Bruun Rasmussen, Vesna Milicevic. 3. Transfer of data to EMPRES-i discussed in further detail at PeP-C week 4, Istanbul, with TCC national consultants.
Co-ordination meeting report.
Monthly reports (to December 2012).
Report of vaccine assessment mission circulated to EC.
Reports of the Simulation Exercise, 11/2012 from leaders and from the observer.
TCC programme will officially April 2013.
Future support under a integrated West Eurasia FMD Management Support project?
Representative (AZB) to 40th
Session in April?

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 10
Iran project Major activities on track. Supervision and training mission completed June 2012.
Animal identification and registration study tour to Montenegro completed in June 2012.
Activity plan to 12/2012
Activities supported under EC TF, Iran project Agreement:
1.4 trainees from Iran attended 4 weeks of PeP-C training course; 2. Project meeting – Istanbul Dec 2012, including activity planning through early 2013; 3. L. Bakkali mission 16-22 Nov 2012: progress in the QA system for the subnational FMD laboratory network; 4. Questionnaire survey of animal markets completed Dec 2012 (data entry ongoing); 5.K. van Maanen missions to train staff in cattle challenge (full vaccine potency tests) at Razi Institute in a series of missions in Feb-Mar 2013; 6. Market Swab sampling: initial feasibility study completed, protocol for further work developed
Monthly Disease information reports, Mission Reports.
Proficiency test Results for Central Lab (WRL-PTS)
Implementation arrangements have improved now that the national project coordinator (unsalaried position) back in Iran.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 11
2. Activities to reduce FMD risk in the South and East Med countries
Egypt (see also 6-Emergencies)
1.FMD management Emergency missions to Egypt (April, May). 2.National FMD management workshop, Cairo 2-3
rd
May. 3.Surveillance Programme proposal developed and submitted to EC-SANCO in August for support
Collaboration with: FAO ECTAD, FAO RNE, EMPRES
1.Participation in TAIEX workshop in Cyprus, Sept 2012, covering FMD regional threats; EuFMD chaired session on vaccination strategies.
Coordination with: TAIEX, OIE, FAO Tunis, REMESA.
Funded under EuFMD/EC programme: 1.Diagnostic kits and training for SAT2 diagnosis had been supplied in previous 6 months. 2.Surveillance reports (Egypt): not received as request to EC for surveillance support in previous 6 months had received no answer and FAO/EuFMD national consultants contracts terminated. 3.Action plan developed for surveillance support to Egypt in first 6 months of 2013. Requires ExCom decision. Activities funded by FAO: Workshop on Regional Coordination of Foot and Mouth Disease Surveillance, Diagnosis and Control in the Near East and North Africa, Cairo, Egypt, 4-5/12/12. Keith Sumption and Dimitrios Dilaveris participated with FAO support, assisting in PCP self-assessment and Roadmap construction.
Funded by OIE: Five country meeting (EGY-IRQ-JOR-LEB-SYR) on FMD held in Beirut, 18
th/12. EuFMD
not invited. FAO participated (M Tibbo).
Action plan developed for surveillance support (Bartels, EuFMD).
Requires ExCom decision.
Mission reports.
Cairo FMD Workshop Report (FAO).
Mission report M Tibbo (FAO).
No clear guidance from ExCom or EC on proposals presented for surveillance support in mid-2012 (Egypt).

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 12
Component Subcomponent Prior (April 2012- September 2012)
Oct 2012-Feb 2013 Reports (examples) Issues /Concerns
[for ExCom awareness]
3. Field based FMD Training Programme
Real-Time Training programme (NTC)
One real-time Training Course held in period (September 2012)
New Real-Time training approach piloted (Sept 2012).
Use of smart-phone apps for rapid epidemiological investigations and local risk factor investigations, with knowledge transfer to trainees
Funded under EC-TF: Three real –time training courses held from December to January NTC11- 12-13) training a total of 35 MS vets plus 9 local vets. [Note: in
addition one FAO staff member (H Ormel, NL) and one West African lab expert from RESOLAB FMD network , funded by NL Government and FAO Identify projects at no cost to EuFMD]
-Smart-Phone based epi-data collection implemented in each course for rapid assessment of FMD spread. Implementation of new exercise-centered training approach. -Use of questionnaires to evaluate training experiences (both a standard evaluation form and a survey monkey one), including evaluation of a proposed e-learning module. -Training manual revised. -Photo and Video library expanded. -Collaboration: Improvement to operations through FAO Kenya by greater involvement of FAO Animal health Team (ECTAD) in Kenya.
Each Course reported (Training wikispace).
Very positive feedback- trainees

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 13
4. FMD surveillance in the African proximity
West/Central Africa: via RESOLAB-FMD
FMD-SAT2 laboratory diagnosis course held in ANSES, Paris (May 2012) with North African and Sahelian zone countries. Surveillance plans developed with each country.
Collaboration with: ANSES, FAO Tunis, REMESA
FMD diagnostic course held in Accra, Ghana (funded by USAID IDENTIFY project , EuFMD provided lab trainers and planning).
Nine counties have a new capacity and kits for FMD serotyping, with mainly US funding. Follow up actions identified, to be funded by USAID with technical input from EuFMD.
Collaboration with: USAID IDENTIFY, EMPRES, FAO ECTAD, FAO RAF, RESOLAB
Supported by EC TF :
1.EuFMD consultant (L. Bakkali-Kassimi) supported to attend annual RESOLAB meeting in Dakar in December, for coord/planning 2013 RESOLAB activities. 2.EuFMD consultant provided backstopping for vaccine matching, in Kenya ( at the only lab that conducts vaccine potency and quality tests in East Africa, in Kenya).3.East and West Africa network animators provide Monthly Update reports to EuFMD on outbreaks and lab findings.
Complementary, no cost (to EuFMD/EC) activities:
1.Delivery of FMD diagnostics to East and West African labs: funded by IDENTIFY project (FAO/USAID). 2.EARLN-FMD: publication on East African Lab functions and capacity published (no cost to EuFMD; Uganda/DVI project Lead )
Monthly FMD report of the EuFMD includes input from the Network coordinators.
Regional surveillance report - Annual Meeting.
Some reactions at the 84th
Executive (post-Accra workshop ) were dispiriting to the European and African experts involved, given the success they achieved.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 14
Eastern Africa: EARLN-FMD
Sample shipment Eritrea, Ethiopia and Sudan to WRL
Collaboration with: EMPRES Shipping Service
FMD Manual developed by network.
Vaccine matching capacity - technical advice to establish provided (van Maanen mission).
3. RESOLAB FMD sub-network coordinator (P. Seck, Senegal) participated as a trainee in an EuFMD Kenyan real-time training course in January, with his participation funded by the FAO EMPRES Identify project. He will pass on the knowledge through his role as RESOLAB coordinator. 4. Meeting held with FAO EMPRES (Identify project) and FAO FMD Unit to coordinate activities in support of FMD surveillance. 5. EuFMD consultant (K. van Maanen) provided follow-up technical backstopping to vaccine matching work in Embakasi FMD lab, Kenya, while in Kenya for a real-time training course.
Monthly FMD reports to EuFMD are collated with other regional reports and circulated

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 15
5. Technical studies Completed:
1. Anatolia wild boar surveillance project
2. Implemented:
-Wild boar tracking and non-invasive sampling project -Contracts with IAH and DTU for PCR-typing of African serotypes and methods of transporting samples cheaply -Vaccine effectiveness studies (in Turkey) Contract to develop an “FMD surveillance design and analysis model “
1.Closed Meeting of the Research Group held, identified priorities for further work (October 2012)
2.Technical study funded to apply smart-phone app on data collection to FMD outbreak investigation and risk factor determination; this study is now partially completed, and an interim report is due at the end of February.
3.Wild Boar tracking study: ongoing
4.Wild Boar non-invasive diagnosis study; agreements with FLI and Serbian national laboratory developed for in vivo and in vitro testing
5.FMD Surveillance model finalized and published/online (Ausvet)
6.Project to develop serotyping PCRs for African FMDV: ongoing.
Papers presented at Jerez on
studies commissioned in 2011-
12.
FLI have decided to pull out
(2/2013) of the wild boar
study planned to evaluate
non-invasive sampling. Other
options for in vivo
experiments with infected pigs
being considered.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 16
Component Subcomponent Prior (April 2012- September 2012)
Oct 2012-Feb 2013 Reports (examples) Issues /Concerns
[for ExCom awareness]
6. Response to FMD Emergencies
1. Egypt- emergency
missions in April-June
2. SAT2 diagnostic ELISA kits provided to at risk Mediterranean fringe countries.
3. Surveillance in high risk border zones: workshop Cyprus June 2012 (Israel, PAT, Egypt, Jordan, Cyprus).
4. Surveillance and FMD management regional workshop, Rabat (under UMA/REMESA), funded by EC through EuFMD
5. Asia-1 vaccine effectiveness study, Turkey
No emergency responses in period.
Funded by FAO or national (Libya) funds:
1.EuFMD participated in Cairo workshop in December to evaluate regional PCP progress and control strategies.2. EuFMD participated in two meetings (Rome and Brescia) on a proposed Italian-funded, REMESA-supported project on FMD control in Libya, in coordination with FAO EMPRES and IZSLER. 3.Two Libyan trainees attended EuFMD Kenyan real-time training courses in January. This was fully funded by Libya, and will assist them in developing their outbreak investigation abilities.
The EuFMD rapid response to the SAT2 crisis in Egypt was widely praised by FAO and VS Egypt at the FAO Workshop held in December 2013.
The “ïssues” raised by FAO at the time of the mission appear in retrospect to be communication issues.
The ability for the EuFMD team to act rapidly in response to emergencies remains important. FAO and OIE agreements may clarify communication issues

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 17
7. Strengthening FMD laboratories in the Balkan Region
Gap analysis missions undertaken by IAH for EuFMD, Aug-September (Croatia, Serbia) Meeting held with representative of EC IPA project on rabies & CSF in West Balkans to coordinate epidemiological and laboratory support Coordination with: EC
IPA project
Funded under EC TF, Component 7:
1.Gap analysis missions by IAH for EuFMD, October 2012 – February 2013 (Bosnia and Herzegovina, Kosovo, Montenegro, Albania, FYROM, Moldova). 2. Participation (Eoin Ryan) in IPA Laboratory Networking Workshop held in Belgrade in order to coordinate activities with CSF/rabies Project
NRL assessments(summary tables) available from each mission provided by IAH consultant, Dr J Bashiruddin. Final report and recommendations by IAH expected at ExCom
Report expected at ExCom
Secretariat considers that the gap analysis missions could have been completed by mid-2012 if their proposed implementation arrangements had been followed.
8. Improved Contingency Planning through use of decision support tools
First Workshop held at the CVO Meeting in Denmark, June 2012. Second workshop planned for Vienna, October. Secretary and Chairman of the STC participated in RAPIDD policy/modeling for FMD workshop, September (RAPIDD funded)
Funded under EC TF, Component 8:
1. Workshop on the use of modeling and decision support tools held in Vienna in October. 16 trainees from 8 countries (Austria, Serbia, Croatia, Hungary, Slovakia, Slovenia, Czech Republic, Malta). Very positive feedback.
2.Follow-up plans for further actions discussed with Standing Technical Committee.
Report to ExCom
The difference in needs between MS in this field means tailor made, technical support “on demand” is needed- how to offer and supply this needs discussion.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 18
Component Subcomponent Prior (April 2012- September 2012)
Oct 2012-Feb 2013 Reports (examples) Issues /Concerns
[for ExCom awareness]
9. WRL contract Contract (150,000 per
annum US$) developed with IAH covering surveillance activities 2011-12.
Funded under EC TF, Component 9:
Letter of Agreement (LoA) for services in 2011-12.
Discussions on coordination of EuFMD/WRL activities with overall proposed FAO/WRL global contract held with FAO FMD unit.
Discussion on improved coordination of management of PTS for EuFMD-supported labs held with WRL colleague.
Signed and implemented. First payment made on 21 Dec (USD 91,000).
Proposal by FAO developed for discussion at ExCom.
.
The ”WRL Contract” is now with FAO/OIE to finalize for discussions with the ExCom.
WRL views on this?
Scope of PTS support (European non-EU labs) needed in 2013 defined but decision on funding needed
Note: the monthly reports from each components feed into the MONTHLY EuFMD/EMPRES FMD Surveillance “Global” report produced by 15th of each
Month. An example is provided in Annex IV.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 19

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 20
Annex I
Iran December report
(as sent by the national consultants)

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 21
ANNEX I: IRAN DECEMBER REPORT
Monthly report: Dec. 2012 Iranian calendar: Azar 1391
1.1 Number of outbreaks
Month Nb of outbreaks (2010) Nb of outbreaks prev year (2011) Nb of outbreaks this year (2012)
Total Total Total
Dec 287 203 146
Nov. 108 164 81
Oct. 88 101 95
September 184 52 104
August 182 84 94
July 303 123 127
June 487 169 118
May 1643 176 68
April 1043 108 74
March 331 100 96
February 119 231 119
January 141 448 176
Total 4916 1959 1152

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 22
Outbreak by provinces
Provinces
Large
ruminants
Small ruminants total Total Epi. unit No .of
Outbreak
per 1000
Qom 25 0 25 347 72.05
Kordestan 8 1 9 2024 4.45
Khorasan Razavi 25 1 26 5989 4.34
Qazvin 4 1 5 1538 3.25
Yazd 8 0 8 2658 3.01
Fars 10 9 19 6708 2.83
Markazy 5 0 5 1870 2.67
0
5
10
15
20
25
30
35
0
50
100
150
200
250
300
350
400
450
500
Jan-1
1
Feb-1
1
Ma
r-1
1
Apr-
11
May-1
1
Jun-1
1
Jul-11
Aug-1
1
Sep-1
1
Oct-
11
Nov-1
1
Dec-1
1
Jan-1
2
Feb-1
2
Ma
r-1
2
Apr-
12
May-1
2
Jun-1
2
Jul-12
Aug-1
2
Sep-1
2
Oct-
12
Nov-1
2
Dec-1
2
Num
ber
(Active S
ur.
)
Num
ber
(Passiv
e S
ur.
)
Month
Number of outbreak in Active & Passive survillance reports
during 2011 to 2012 in Iran
Number of outbreak reports
Active Sur. reports

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 23
East Azar 10 0 10 3913 2.56
Ardebil 5 0 5 2131 2.35
North Khorasan 3 0 3 1304 2.30
Hamedan 3 0 3 1707 1.76
Mazandaran 3 3 6 4206 1.43
Kerman 5 0 5 3812 1.31
Tehran 3 0 3 2447 1.23
Hormozgan 2 0 2 1668 1.20
West Azar 4 0 4 3543 1.13
Esfahan 6 0 6 6365 0.94
Kermanshah 1 0 1 3063 0.33
Lorestan 1 0 1 3172 0.32
Sistan Va Blu. 0 0 0 6382 0.00
Khozestan 0 0 0 4163 0.00
South Khorasan 0 0 0 3286 0.00
Gillan 0 0 0 3042 0.00
Golestan 0 0 0 1880 0.00
Kohkilouyeh 0 0 0 1682 0.00
Jiroft 0 0 0 1363 0.00

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 24
P r o v i n c e - g e o . s h p A n i m a l _ D i s e a s e _ m a p
4 0 0 0 4 0 0 8 0 0 M i l e s
N
E W
S
F M D O u t b r e a k s R e p o r t e d D u r i n g
M o u n t h 9 - 9 1 ( D e c . 2 0 1 2 )
Semnan 0 0 0 1219 0.00
Zanjan 0 0 0 1209 0.00
Chaharmahal 0 0 0 1045 0.00
Illam 0 0 0 841 0.00
Bushehr 0 0 0 767 0.00
Total 131 15 146 85344 1.71
* Outbreaks detected during active surveillance.
Qom province is major hot points area in the country.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 25
2. Laboratory diagnosis
FMD Sample results
Positive
negative unsuitable
Total
positive A O
Asia1
Month No samples No. No. No. No. No. No.
Dec (CVL+WA+ Fars) 48 8 3 37 28 9 0
Nov. (CVL+WA) 33 7 3 23 22 1 0
Oct. 2012 (CVL) 57 11 7 39 31 3 5
Sep. 2012 (CVL+ WA) 16+6 0 6 16 9+6 1 0
Aug. 2012(CVL + W.A) 23+13* 7+10 6 10+3 9+3 1+0 0
July 2012 (CVL + W.A) 50 +
27*
14+8 4 +1 36 +18 16 +15 4 +2 12+1
Jun-12 18 8 6 4 1 1 2
May-12 38 12 2 24 6 7 11
Apr. 2012 West
Azerbaijan sNl 16* 6 0 10 0 3 7
Mar-12 52 18 9 25 1 6 18
Feb. 2012 47 17 2 28 7 5 16
Jan. 2012 82 29 12 41 6 15 20
Dec. 2011 115 15 15 85 22 15 48

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 26
Nov. 2011 65 14 8 43 18 13 12
Oct. 2011 35 9 5 21 7 2 12
Sep. 2011 46 13 7 26 14 1 11
FMD Sample result by provinces Oct. 2012 (CVL & W. Azar & Fars)
Province Total Neg. Unsuitable Positive Asia1 A O
Fars* 10 5 0 5 0 3 2
West Azarbaijan (CVL& W.AZAR
sNL)
12 3 1 8
0 4 4
Albourz 5 0 1 4 0 4 0
Semnan 1 0 0 1 0 1 0
Ardebil 2 0 0 2 0 2 0
Esfahan 5 0 1 4 0 4 0
Hamedan 2 0 0 2 0 2 0
Tehran 1 0 0 1 0 1 0
Zanjan 5 0 0 5 0 3 2
Qom 5 0 0 5 0 4 1
total 48 8 3 37 0 28 9
*Samples tested on Fars FMD sNL ,

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 27
Comment:
Serotype A was dominant during Dec. in the country, as according the CVL R1 value results , there were low
matching with A field strain and vaccine Strain (A 05) , it was supposed to have a epidemic condition due to this
serotype, but epidemiological data shows that this serotype induced low virulent outbreaks in affected epi units
but sill induced outbreaks in some recently vaccinated herds. Vaccination of affected dairy farms and around it
with Razi Monovalent vaccine A 05) shows good affects in the farms.
0
20
40
60
80
100
120
140
1-O
ct-1
0
1-N
ov
-10
1-D
ec-1
0
1-J
an
-11
1-F
eb-1
1
1-M
ar-1
1
1-A
pr-
11
1-M
ay
-11
1-J
un
-11
1-J
ul-
11
1-A
ug
-11
1-S
ep-1
1
1-O
ct-1
1
1-N
ov
-11
1-D
ec-1
1
1-J
an
-12
1-F
eb-1
2
1-M
ar-
12
1-A
pr-
12
1-M
ay
-12
1-J
un
-12
1-J
ul-
12
1-A
ug
-12
1-S
ep-1
2
1-O
ct-1
2
1-N
ov
-12
1-D
ec-1
2
Nu
mb
er o
f su
bm
itte
d L
ab
. sa
mp
les
FMD serotyping results in Iran Oct. 2010 - Oct.2012
Asia-1 A O Unsuitable Neg.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 28
Vaccination: During vaccination phase and last 9 month (April – Dec. 2012)
Vaccination
group Provinces
Phase 1 Phase 2 vaccination
on 9 month
Total Epi.
unit
vaccination
converge
Phase1
vaccination
coverage
Phase2
total vac.
Cov.(During
9 month)
Group 1
Illam 68 414 750 841 8% 49% 89%
Bushehr 0 348 673 767 0% 45% 88%
South Khorasan 709 551 1293 3286 22% 17% 39%
Yazd 574 1 1915 2658 22% 0% 72%
Kermanshah 16 1 1697 3063 1% 0% 55%
Hormozgan 0 0 229 1668 0% 0% 14%
Jiroft 270 305 1321 1363 20% 22% 97%
Chaharmahal 490 510 1369 1045 47% 49% 131%
Kohkilouyeh 0 842 904 1682 0% 50% 54%
Group 2
Esfahan 1727 228 4069 6365 27% 4% 64%
Golestan 812 273 1492 1880 43% 15% 79%
Khorasan Razavi 3226 897 6982 5989 54% 15% 117%
North Khorasan 920 75 1688 1304 71% 6% 129%
Khozestan 140 185 3015 4163 3% 4% 72%
Sistan Va Blu. 0 1838 6382 0% 0% 29%
Fars 2117 283 7838 6708 32% 4% 117%
Lorestan 1145 40 2135 3172 36% 1% 67%

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 29
Hamedan 2 516 1794 1707 0% 30% 105%
Kerman 34 3256 3812 1% 0% 85%
Markazy 139 3 479 1870 7% 0% 26%
Group 3
Ardebil 681 12 1300 2131 32% 1% 61%
Zanjan 641 31 751 1209 53% 3% 62%
Semnan 559 56 898 1219 46% 5% 74%
Qazvin 238 134 870 1538 15% 9% 57%
Qom 121 153 426 347 35% 44% 123%
Gillan 1246 84 1340 3042 41% 3% 44%
Mazandaran 902 73 2363 4206 21% 2% 56%
Tehran 646 493 2568 2447 26% 20% 105%
East Azar 1310 25 2704 3913 33% 1% 69%
West Azar 641 422 5052 3543 18% 12% 143%
Kordestan 578 20 802 2024 29% 1% 40%
Since the beginning of this year 1391(Iranian calendar) (April 2012) 32 provinces divided in 3 different
group (according to the density of animal population, FMD risk, outbreaks ...) and it was supposed to
vaccinated dairy farms 3 time a years on group 2 & 3 and villages + dairy farms in group 1, 2 time a
years . Evaluation of vaccination performs during 9 month shows that only in some of provinces
vaccination exceed 100 % of epi units in two vaccination periods. On the other hand in most of
provinces vaccination perform on high density area and less than 50-60 % of epi units vaccinate during
vaccination phase and in most of the provinces vaccination phase take place more than expected
period (2-3 month instead of 1 month).
So vaccination policy should be analyses and revised by the of end this year and appropriate
vaccination program should be define to the country.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 30

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 31
Annex II
Real Time Training
(complete reports are available upon requests and on the EuFMD website
http://www.fao.org/ag/againfo/commissions/eufmd/commissions/eufmd-home/en/)

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 32
REAL TIME TRAINING KENYA-NEPAL
Executive Summary from the latest real time training Kenya (January 2013): NTC13
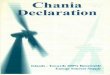
FAO and its EU-FMD Commission held a 4 day real time training course for veterinarians, in field diagnosis and management of FMD in Nakuru, Kenya. The participants included local Kenyanveterinarians and also visiting vets from Libya and several European countries. The course began with an overview from Dr Wanasamba, Deputy provincial Director of Veterinary Services of Kenya. Presentations were then performed by Dr Nick Lyons, Dr Kees van Maanen. Topics covered included procedures for FMD investigations, biosecurity, and sample collection; history of FMD in Kenya; a session on lesion aging; and detailed information on epidemiology, laboratory tests and dangerous contact tracing. Field sessions for practicing biosecurity measures, diagnosing FMD and establishing epidemiological patterns were planned for Day 2, for which the thirteen people were divided into two groups. Both groups visited smallholder subsistence farms. On Day 3 all participants took part in an area survey walk in the same area. Data relating to risk factors for FMD were gathered from short interviews with smallholder farmers. Day 4 was spent writing and collaborating reports, and preparing a summary presentation for the Provincial Director of Veterinary Services and the Director of the Nakuru Veterinary Investigation Laboratory. The area was struck by a recent outbreak of FMD, serotype A. This serotype has not been seen in this area in recent years. A vaccination campaign against serotype A, O and SAT-2 started in the last month.
9 Courses
since 2011;
85 Eur. vets
trained
Exerpt from the report of a real time training Nepal(January 2013): KTC2 DISEASE INVESTIGATION (11 December 2012) Farms with clinical FMD On the 11 December 2012, five properties in an area approximately 20 kilometres south of Kathmandu in the Lalitpur district in the Central region of Nepal were visited to determine if clinical FMD was present (Figure 3). These visits permitted examination of a total of seven cattle and three goats. The age of cattle ranged from adults of 10 years of age to yearling (under 12 months). The small sample of goats included two adults and a single kid all from a single farm.
Clinical & test findings A summary of clinical findings and test results is presented in Table 1. Lesions were estimated to range from one to 6-7 day old.. The most common clinical sign seen was salivation, with lameness only observed in a single cow. It is possible that lameness as a clinical sign is likely to be underreported due the management practice of tethering and the relatively small distances travelled by individual animals. Higher body temperatures appear more commonly

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 33
seen with lesions under 3-4 days. All affected cattle exhibited oral lesions involving either/or tongue, hard palate and gingiva and all but one exhibited feet lesions. If present, foot lesions were most commonly found in the interdigital space between the heels. Two cows exhibited teat lesions which were noticeably less severe than the oral or feet lesions observed. Only one cow with lesions did not show any clinical signs. This animal was determined to have an acute solitary lesion (single site of gingival blanching) so minimum clinical signs were not an unexpected finding. A subsequent interview with the farmer 24 hours following this initial examination revealed that this cow had progressed to exhibit clinical signs. Two of the four cows tested were positive to FMD viral antigen (Ag) using the pen side, Lateral Flow Device (LFD) . Diminishing level of virus with increasing levels of serum antibodies may have resulted in the negative Ag result in one of the remaining two negative cows. The last cow had a single solitary lesion and pyrexia and no clinical signs at the time of sampling. It is possible there was insufficient viral material present at the time to be identified by this test. The new pen side non-structural antibody (NSA) test (not yet validated) failed to detect antibodies in all four samples tested. This is mostly as expected given that the lesions present on three of these animals were early (1-4 days) and NSA are unlikely to be present at this time. One of these samples tested in the laboratory for NSA was suspect but not confirmed positive for NSP. This sample was from a cow with lesions at 6-7 days and therefore it is likely there would be some level of antibodies present. The difference in results between the field and laboratory test for NSA may reflect a difference in sensitivity of these two tests, though it should be noted that this pen side test is still currently unvalidated. Generally the two pen side tests showed good correlation with results obtained from testing from National FMD and TADS Laboratory in Kathmandu, Nepal. This is an encouraging finding in the face of dealing with the initial diagnosis of FMD outbreaks in the field.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 34

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 35
Annex III
Trans-Caucasus Countries FMD desktop
simulation exercise, November 2012-
Report by EuFMD consultants (Carsten Potzsch; Rob Paul; Tsviatko Alexandrov)

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 36
ANNEX III TRANS-CAUCASUS COUNTRIES: FMD DESKTOP SIMULATION EXERCISE,
NOVEMBER 2012; REPORT BY EUFMD CONSULTANTS
Foreword
It is inevitable that a report like this concentrates on the areas for improvement and as a result it might
appear to paint a gloomy picture of the current situation. This would be unfortunate and must be avoided.
It is important to recognize the enormous strides that have been made in recent times in all three Trans
Caucasus Countries (TCC) in developing their plans to control Foot and Mouth Disease (FMD). All three
countries have basically sound plans that contain the essential elements for providing control of FMD. Of
particular note are the policies to differentiate exotic and endemic FMD to allow a targeted and
appropriate response, the processes to detect incursions rapidly through compulsory notification and
immediate investigation, to respond quickly through specific control measures aimed at containment and
elimination, the ability to create structures and put in place processes to support this and, perhaps, most
important of all, the willingness and enthusiasm of all the veterinary services to undertake the not
inconsiderable amount of work that this will require. The recommendations here set out the next steps on
this journey and this report should be viewed in the context of supporting national services in their efforts
to achieve that outcome.
Executive Summary
A desktop simulation exercise for FMD involving all three TCC (Georgia, Armenia, Azerbaijan) was carried
out in Sighnaghi, Georgia between 6 and 7 November 2012 as part of the EuFMD project to support FMD
control in the TCC region. The participants, purpose and objectives for the exercise were agreed with
EuFMD secretariat. From this a scoping document for the exercise was developed (page 5).
A generic scenario containing the key elements (investigation, confirmation and reporting of disease,
movement controls to prevent spread and tracing) that were to be tested was developed. To incorporate
these elements the scenario involved an unusual clinical picture detected and reported in a village one
evening. This occurred shortly after large numbers of small ruminants had returned from summer pasture.
Within a few days similar clinical pictures were detected in more villages in the same district. To generate
tracings a considerable number of animals were moved through markets and/or dealers immediately
before and during the days following reporting of the first case
Key individuals from the veterinary service of each country were invited to take part and provided written
briefing on the exercise (Appendix 1). Participants were told the district in each country for the simulation
in advance but were not given any of the scenario details until the appropriate point during the exercise.
Using the framework document clinical and epidemiological data for each infected premise/village in the
scenario were developed (Appendix 2). For each country a district remote from the capital was selected
and, using local knowledge, the generic scenario was applied to create three detailed but very similar
country specific scenarios (Appendices 3a, 3b & 3c).
To test the agreed key elements three time points in the simulated outbreak were chosen for the exercise -
these were the first disease report (to test rapid investigation through initial response, identification
through sampling, disease reporting, tracing and movement controls), several outbreaks (to test movement
controls, tracing and key decisions likely to have the greatest influence on the later course of the epidemic)

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 37
and the point at which disease is becoming widespread but can still be contained (to test movement
controls, resource constraint, data handling and information systems and prioritization.) To make best use
of the Russian Interpreter and avoid possible language difficulties it was decided at the start of the exercise
to modify the original plans to run open sessions involving all participants. Instead a series of specific
questions based on the objectives were set for each session and translated into Russian. Each country
group worked on the questions before reporting back in plenary session. For each session one country led
the response with others comparing any differences in their responses where appropriate. The exercise
concluded with a discussion to agree with participants the areas for further development after the exercise.
All countries demonstrated an understanding of the disease response requirements and indicated they
would respond immediately to a report of FMD. They would aim to rapidly carry out the initial
investigation, collect, submit and test samples for confirmation of diagnosis, make an epidemiological
investigation and implement disease control measures both in the infected farm/village and more widely.
The exercise demonstrated the need to develop further both the ability to detect disease at an early stage
and to rapidly confirm and identify FMD. Key to this was the need to further develop the ability to collect,
submit and test samples, including where appropriate to an international reference laboratory, to enable
accurate identification of serotypes to be carried as rapidly as possible. It identified the need for more work
to ensure that in the early stages of an outbreak appropriate animal movement controls were put in place
across a large enough geographic area to contain disease. More work was also needed to ensure that all
animals involved in and movements related to an outbreak were identified and traced. Surveillance plays
an important part in controlling an FMD outbreak and here too the need for more development was
identified. To support all these areas further development of epidemiological skills, including carrying out
epidemiological investigations and using tools to assist in communicating findings, for epidemiologists and
more widely across veterinary services would be beneficial.
Contingency planning in all three countries would be further strengthened through the development of
regional and international co-operation and building in the facility to seek external assistance where
appropriate.
Scoping Paper - FMD Exercise Georgia November 2012
This paper set out the basic requirements for the exercise that were agreed with EuFMD secretariat
before the scenario was developed.
Purpose
To identify strengths and weaknesses in existing national plans by testing key sections with the veterinary
services involved.
Objective(s)
Rapidly identify and contain an incursion of an exotic FMD serotype.
Identify serotype accurately and rapidly
Put in place appropriate animal movement and other controls to contain the outbreak and enable
regionalization.
Put in place appropriate disease identification and control measures (including surveillance, tracing and
biosecurity)
If appropriate devise and organize an appropriate emergency vaccination campaign

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 38
Organizers
EuFMD
Observer
Carl Danielson, Swedish Board of Agriculture, Senior Advisor to National Food Agency Georgia (Capacity
Building Agriculture/Georgia (CBA/G) Project)
Players
Veterinary services only – senior and local veterinary surgeons from each country
Project Plan & Timeline
August/September – develop scenario, agree drafts of the Armenian & Georgian plans
October – produce paperwork necessary for participants
November – deliver exercise 6th - 7th in Georgia
November – evaluate and produce report (by end November)
Exercise Risk Register
Not implemented – managed locally by R. A. Paul
Preliminary Preparations
Complete current contingency plans and make available in English to consider by 19 October.
Consider Regional simulation exercise held in 2009
Generate scenario for each country
Create data to support scenario
Write briefing note for attendees
Evaluation
Hot wash up – session held at the end of the exercise to agree areas for development. These are included in
the recommendations.
Questionnaire – questions to participants regarding the exercise itself (did it meet their expectations, what
went well, what could be improved, what they would recommend as follow up to the exercise and any
other comments).
Basic Requirements for the Scenario
The scenario should;
Include primary outbreak and several secondaries, but should not be so complex it would be
unmanageable
Involve large and small ruminants
Have some involvement for pigs and wild boar (as seen in real outbreaks in Bulgaria/Thrace) where
appropriate
Involve movements through local markets and/or dealers.
Examine how the contingency plans deal with animal movements, both legal and illegal.
Create a situation where initial control measures will not be adequate to limit spread and a
containment zone will be needed.
Focus on issues outside the farm.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 39
Draft Programme
Day 1 – Confirmation and setting up a centre
If possible Day 1 should cover;
Initial Report of disease and actions that follow
Sampling and Testing for confirmation
Confirmation of disease
Setting up national and local centres
Establishing a battle rhythm – the running order for gathering data, establishing meetings etc. to
support sound decision making
Establishing processes to control disease
Establishing appropriate control zones – in particular appropriate size, shape and control measures
implemented.
Movement restrictions
Tracing
Surveillance – both passive and active
Epidemiology
Optionally it might include;
Licencing
Helplines
Policies (for instance covering what to do with clinically affected animals, which movements to
restrict and which to allow)
Communication
Day 2– Vaccination, start of emergency vaccination campaign
Establish vaccination strategy and delivery plan
Deploy resources to deliver emergency vaccination in agreed timescale
Scenario Design
To achieve the requirements the scenario;
Must be in an area where containment could be achieved if disease was rapidly and correctly identified –
this needed detailed knowledge of local farming practices including animal movements, risk of fomite
spread and effect of susceptible feral/wildlife (particularly scavenging domestic and feral pigs).
Must be identifiable rapidly and clinically – needed to be in area where clinical disease was not already
present and where farmers were likely to spot, and report, any change to this.
Needed to be set at a point late enough after first introduction to allow some spread but not so late it
would not be possible to prevent creation of epizootic
Would benefit from including movements to/from pasture, animal gatherings and possibly more widely
within each country
Must involve a serotype for which vaccine is available to provide emergency/area/ring vaccination either
immediately or, more likely, readily obtainable.
Must include enough details of animal holdings and movements in the area affected so that the necessary
data to follow outbreak and implement control measures can be created.
To do this a scenario commencing with a single disease report and progressing in several steps to around 7
days after that report was chosen.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 40
Key Learning Points for Scenario
Day 1
All players should be able to;
rapidly detect and report of disease
rapidly collect samples from suspects, convey to laboratory and obtain accurate identification
communicate progress to those needing to know
apply control measures to infected premises
rapidly understand (epidemiology) and control disease processes(biosecurity, movement controls,
tracing)
identify and put in place a containment zone
establish and resource both national and local control centres
Day 2
All players should be able to;
demonstrate ability to deploy appropriate resources to deliver plan
establish processes to begin and sustain an emergency vaccination campaign.
identify and address impact on existing work programmes
develop a suitable vaccination strategy and vaccination delivery plan
consider long term exit strategy from control measures
Exercise Attendees
Origin/Name Occupation Role
EuFMD
Robert A Paul Veterinary Consultant Leader
Carsten Potzsch Veterinary Consultant Leader
Tsviatko Alexandrov Veterinary Consultant Leader
Mzia Kuznetsova Project Regional Secretary Support
Carl Danielsson Contingency Planning, Swedish
Board of Agriculture
Observer
Kate Vachadze-sen Interpreter
Armenia*
Norik Gishyan Inspector of vet. service of
Noyemberyan region of Tovush
Marz
Player
Satenik Kharatyan National Consultant Player
Azerbaijan
Siala Rustamova CVO Player
Kliment Asadov Head of Epidemiological Unit Player
Eldar Hasanov Head of Tovuz Veterinary
Service
Player
Tamilla Aliyeva National Consultant Player

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 41
Georgia
Ioseb Menteshashvili Deputy CVO Player
Lasha Avaliani Head of Epidemiology Unit of
NFA
Player
Lia Bekauri District Veterinarian Player
Zurab Rukhadze National Consultant Player
(*Gevorg Tovmasyan, Head of Veterinary Department of Centre of Veterinary, Food Safety and
Phytosanitary Services (SNCO) and Gagik Vardanyan, Head of Veterinary Department of Division of
Veterinary and Stock Breeding of MoA) were unable to attend at the last minute due to sudden
organisational changes in home country)
Exercise Programme
Day 1
09:00 Introduction and welcome Carsten Potzsch & Rob Paul
Aims of exercise
09:15 Brief Overview of country plans Country Representatives
10:15 Session 1 Day 0 (First Report Case) Plenary Session
(with coffee break at 11:00)
13:00 Lunch Break
14:00 Session 2 Day 4 Plenary session
(with break mid-afternoon)
17:00 Conclusion of Day 1 – scene setting for day 2
Day 2
09:00 Review of day 1 Plenary session
09:15 Continuation of Session 2 Plenary session
10:00 Session 3 Day 6 Plenary session
(with coffee break at 11:00
13:00 Wash up and conclusions Plenary session
14:00 Lunch and Depart
Approach – Session Details
General
To make the exercise manageable separate but similar outbreaks were simulated in each country. Each
one involved a single district far enough from the centre of the country for the central authorities to have
to consider how they would deploy their resources and manage the outbreak. The districts were selected in
advance and the central authorities notified – this had the advantage of making it possible both to invite
the district veterinarian for the district chosen to be at the exercise and to more realistically consider the
resource and other issues that would arise in the chosen district.
A short briefing note was sent to each veterinary authority in advance to enable them to prepare for the
exercise. They were asked to provide the animal demographics and resources available for the chosen
district, along with the maps they would normally use in disease outbreaks. Participants were also offered

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 42
the opportunity to supply any features they wanted to test for inclusion in the scenario though none chose
to do so. The two days were divided into distinct sessions each with its own objective and outcome as
below, the individual sessions building to meet the overall purpose and objectives for the exercise.
During the exercise discussion, thoughts, decisions and outputs were captured on flipcharts and played
back to participants at the end of each session. The absence of Armenian CVO and Head of Epidemiology,
who were unable to attend due to a restructure at home, did affect the skill mix as some of the strategic
capability and policy development capability was missing. Their colleagues did the best they could in their
absence. The original programme was amended when it was discovered that, for security reasons, the
Armenians had to be home before dark on the final day (they were using a UN vehicle). By working straight
through the second day with only a couple of breaks and concluding at 2 p.m. with lunch it was possible to
retain but all but one hour from the original schedule and enable the Armenians to stay right through and
not miss anything.
The original approach was modified to avoid possible language difficulties and to make best use of the
Russian Interpreter. Instead of running open sessions involving all participants a series of specific questions
based on the objectives were set and translated into Russian for each session. (appendix 4) Each country
group worked on the questions before reporting back in plenary session. For each session one country led
the response with others comparing any differences in their responses where appropriate.
Day 1 covered introductions, country presentations on their contingency plans, initial response to a report
case, diagnosis and dealing with 3 confirmed villages on day 4 of an outbreak.
Day 2 concluded the session dealing with 3 confirmed villages on Day 4 of an outbreak, considered 8
confirmed villages on Day 6 of an outbreak and concluded with the hot wash up session for participants.
Country Presentations on Contingency Plans
Each country had previously provided copies of their contingency plans (appendices 5a, 5b & 5c) and gave
an overview and short summary of the key elements of their contingency plans at the start of the exercise
(Appendices 6a, 6b & 6c).
Session 1 Initial Case (Plenary)
Objective was to identify an incursion of an exotic strain of FMD and establish proportionate and
effective measures to control it
The outbreak began with a clinically distinct picture designed to alert the farm/village to an unusual FMD
disease picture and that the central authorities should be informed. An incursion of SAT2 in each country
was used (though the source was never identified as this was not necessary for the exercise). The first case
was not the index case. It involved easily recognisable clinical disease in a large part of the susceptible
group and across all age ranges so should have quickly indicated that this was something different and that
animals were not protected by the routine FMD vaccination programme.
This led to discussions about diagnosis and confirmation (including laboratory tests), introduction of
biosecurity controls, animal movement controls, disease surveillance (patrols) and, perhaps most
important, tracing (both forward and back). It also introduced the first communication questions – what
information would be shared and with whom – locally, nationally and internationally.
Questions addressed in this session;

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 43
- How was presence of different strain recognised at farm/village level
- How did the village vet fulfil his role?
- Who made the report? To whom? How? What information did they report?
- How was suspicion confirmed/negated? (This covered laboratory testing within country and the use
of international reference laboratories etc.)
- How was disease be monitored?
- What was the national picture and how was it captured?
-
Outcome for Session 1 – Participants should have identified an exotic incursion of FMD, confirmed the
serotype, reported its existence and put in place first effective measures to limit further transmission.
In the first report case sessions all players created the right sense of urgency, put in place the structures
and set up the processes necessary to diagnose the cause and begin to control the spread. In some cases
the response times seemed a little optimistic but this was probably partly exercise artefact. The main
concern from this session was a lack of clarity on how the serotype would be identified, given that it was
not one of the endemic serotypes the players are used to dealing with.
This led to a discussion on laboratory diagnosis and sending samples to a reference laboratory. This
appeared to be a key area for improvement for the future. In the end players were told the outbreak was
the result of an incursion of FMD SAT2 from an unknown source.
Overall objectives for Day 1 were largely met.
Session 2 Local Spread of Disease
This session started with a short seminar on creating disease timelines to assist the progress of subsequent
session(s). This took some time but did assist players teasing out the information provided. This also led to
some useful discussion on tracing.
The session itself was set on Day 4 of the outbreak and involved 2 more outbreaks in nearby villages. This
led to discussions on the use of epidemiological tools, including developing a timeline, and the work that
would be needed in the district, including resources, to do this work and try and control the disease. This
session included movements through a relatively small, local market with one or two large traders and/or
dealers plus, given the time of year, movements back from summer pasture of the sheep to consider. It also
involved significant non animal movements and tracing including people, trailers and milk lorries These
were designed to indicate much more widespread dissemination than first thought and suggest that initial
action was now unlikely to contain the outbreak within the district without further control measures.
This session explored international notification – when, who, what etc.
Questions addressed;
- What were next steps (testing/confirming additional cases, surveillance (including patrols),
biosecurity measures, movement controls and further tracing)
- How did players build a full disease picture (timeline)
- What operational structures did they use (local crisis centres? Use of non-veterinarians etc.)
- What data did they use (disease/clinical reports, epidemiology reports and situation (tracing,
district resource and intelligence information) reports
- What did they do about disruption to existing work programmes?
Outcome of Session 2 – structures, processes and data handling established and able to monitor, control
and assist develop additional control measures in developing outbreak
Progress was slower than anticipated due to the challenges of sorting out the strategic approach needed to
make best use of the information provided to develop the appropriate policies. Initially there was a

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 44
tendency to become a little focussed on some less important detail and perhaps lose sight of the bigger
picture. Nevertheless good progress was made and all groups did start to look at the issues strategically. It
also became apparent, even at this stage, that their actions were based around a desire to eliminate the
exotic serotype and avoid any specific/additional vaccination if possible.
This session also led to considerable discussion on tracing. All three countries recognised the need to carry
out tracings but acknowledged that this might be difficult to complete (relying on people’s memories in
many cases) and would generate considerable amounts of data that would be difficult to manage. They also
recognised that carrying out the tracing visits might create more work than existing resources could handle.
This in turn led to discussions about prioritisation, hot and cold tracing etc. and tools to handle the
information but more work is needed in this area.
Session 3 Development of effective containment zone
Objective was development of additional control measures to prevent exotic strain of FMD becoming
endemic. Aim was to protect majority of susceptible domestic livestock and create environment for
ultimate resumption of international trade
Participants were asked to look again at their proposed control measures in light of the emerging disease
information. They were also asked to consider emergency vaccination and to devise a vaccination strategy
and delivery plan. This was based on limited availability of a suitable vaccine around 3 weeks after the
initial report of disease. A large part of the morning was spent working on this, with the emphasis being on
creating and maintaining suitable containment zones by the end of the session. To make life easier a
timeline for all eight cases and a schematic representation of the key movements was provided.
The need for adequate information to make informed decisions and hot & cold tracing dominated the first
part of the discussion in this session. Discussion then moved on to the challenge of scaling up efforts to
match developments and the decisions from session 2 on zone sizes were revisited to review the decisions
in light of developments. Some chose to increase sizes considerably and the epidemiological information
available earlier in the exercise that would have helped make this decision sooner was considered. There
was also considerable discussion on how to select zone boundaries and the disease control measures to be
applied in each zone. This session ended with a look at emergency vaccination. In session 2 there had been
some divergence on whether or not to vaccinate. While there was now agreement it would be the option
of last choice there was discussion on how this decision would be reached in practice and if, instead, a
decision to vaccinate was reached how a vaccination strategy (including matching vaccine availability to
their plan might be developed - for the exercise there was limited availability of a suitable vaccine). Issues
considered included size and shape of vaccination zone, using natural barriers (mountains, rivers, lakes etc)
and restricting vaccination to animals which contributed most to the onward spread. This session also
covered prioritisation of tasks, destruction and disposal of affected animals, establishing local crisis centres,
biosecurity measures, resource management, the role of wildlife and epidemiological investigation. Finally
players began to think ahead and there was a limited amount of time to consider developing an exit
strategy for the measures in place.
Session 4 Wash Up (Plenary)
Objective was to capture their feedback on the exercise and what they have got from it
This session considered and agreed areas for further development on returning home after the exercise.
These included developing contingency plans further to address some of the questions that arise in any
outbreak, early detection and confirmation of serotype, international reporting, strategic thinking from the
outset, building the epidemiological picture both to help this and manage expectation, up scaling early

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 45
enough, resource management (using vets for veterinary roles)information handling (especially tracing) and
developing a vaccination strategy now to use if the situation indicates this is an appropriate control
measure. Players and the observer were asked to provide feedback on the exercise for the final report. This
is attached at Appendices 8a, 8b & 8c. All three countries reported that holding the exercise away from the
normal place of work made it easier to avoid distractions and partake fully in the exercise. Visitors
appreciated the host’s excellent organization which made the event run smoothly. The format of questions
and feedback for each session was recognized as contributing to the useful discussion during the exercise,
as having three countries together contributed to comparing and contrasting different approaches and
decisions. Individual country presentations on their individual contingency plans contributed further to this
benefit from the exercise. Participants felt this increased their overall understanding. Also appreciated was
the use of country specific scenarios which enabled participants to test applied practical skills in a much
more realistic way. They also appreciated having international expertise available to support the discussion.
The exercise helped players both recognise the progress that has been made since 2009 and the further
steps that are needed to maintain this progress. They recognised that early detection and swift response
through good reporting to the national veterinary service, reliable laboratory diagnosis and application of
effective disease control measures will most rapidly bring about effective control. They also recognised that
this requires good investment in not only the veterinary services but also in farmer education, training,
regular exercises, access to international expertise etc.
Conclusions and Recommendations
The aim of the exercise was to test the strengths and weaknesses in all three countries’ Foot and Mouth
Disease (FMD) contingency plans and to identify the next steps in developing them. At this time all the
plans are in draft form and have yet to be validated. They appear as standalone documents though they
cross reference relevant national legislation and other relevant documentation. All contain the essentials
needed and cover the initial response, set out in broad principle the structures that would be established to
manage an outbreak and cover the processes and the roles and responsibilities for doing so. These are very
much works in progress providing the essentials at this stage but needing further development to become
fully functional and integrated plans. All plans would benefit from more detail on strategic and tactical
decision making, operational process, resource management and individual roles and responsibilities. They
would also benefit from being linked to other plans including, where possible, general contingency plans for
civil emergencies and both central and local delivery plans. This would help to ensure that existing
knowledge, currently vested in a relatively small number of experienced individuals, is both shared more
widely and retained. To be effective these plans must be developed and maintained by the individuals who
will be putting them to use in a real outbreak. In practice this means the national veterinary services of
each country. Nevertheless it must be recognized that these services do not have all the skills necessary to
do this at this stage. Initially EuFMD will need to lead this process by providing external expertise advice
and training. As the skills within each veterinary service develop they must increasingly take over the lead
with EuFMD expertise moving to a supporting and advisory role.
To do this the national veterinary services must involve a large cross section of the people, both within and
outside the service, who are given responsibilities in the plans. All these individuals should be trained to
enable them to discharge their responsibility and given the opportunity to take part in regular exercises to
maintain their skills and test their level of readiness. Over time these people should take on the
responsibility for maintaining and developing those parts of the plan that they will deliver in an outbreak.
With the time available and the current state of development it was agreed with EuFMD secretariat that
the exercise would concentrate on the veterinary aspects of the plans at this stage as these are absolutely

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 46
central to any disease control contingency plan operating successfully. Nevertheless a fully effective
response will require much wider participation and this is covered later in the conclusions.
The intention was to test both the national level (by involving Chief/Deputy Chief Veterinary Officer and
lead epidemiologist*) and local level (district vet & national consultant) by looking at three key points in an
outbreak of an exotic serotype of Foot and Mouth Disease (SAT2). These were the first report (to test rapid
investigation through initial response, identification through sampling, disease
(*due to local circumstances Armenia was only able to send the National Consultant and District
Veterinarian on the day)
reporting, tracing and movement controls), several outbreaks in one district (to test movement controls,
tracing and key decisions likely to have the greatest influence on the later course of the epidemic) and the
point at which disease is becoming widespread but can still be contained (to test movement controls,
resource constraint, data handling and information systems and prioritization)
The exercise concentrated on the operational response, looking briefly at strategic and political aspects
where they were significant to the running of the operation. These were not considered in great detail but
simulation exercises to look specifically at strategic planning and including all the players who would be
involved in this would be useful in ensuring the full development of contingency plans. This could be carried
out as part of the wider planning for civil contingencies. The biggest challenge in any outbreak of exotic
FMD is recognizing the presence of disease at an early stage and correctly identifying the serotype(s).
All three countries would activate their national and local structures in the early stages and while awaiting
confirmation of diagnosis. Although not explicit in the early stages of the exercise initial actions suggested
that all three countries would aim to eliminate an incursion of exotic FMD. This was discussed at some
length later in the exercise when this view was confirmed. This suggested that contingency plans must
make this clearer by stating this more explicitly. This would assist in ensuring that all involved in the critical
early decision making were aware of the strategic intent and therefore better able to support fully the
inevitable actions that flowed from it. This in turn would assist in ensuring from the outset that the actions
taken would be more likely to achieve this outcome. This arose again in the second session, when it was not
clear whether or not each country would consider vaccination or, if they did, how they might reach a
decision on whether to do so at that stage, and again in the third session, where the need for an emergency
vaccination strategy was recognized.
The national veterinary authorities should expand the next iteration of the plans to include more
information on strategic intentions when dealing with different scenarios and on the process for deciding
how best to achieve and communicate these on each occasion.
It is important that the central authority within the National Crisis Centre (NCC) concentrate on the bigger
picture while leaving staff in the Local Crisis Centres (LCC) to concentrate on the detail. To achieve this
national contingency plans need to define clearly the different roles and responsibilities and encourage
delegation where possible.
To enable the NCC to build a detailed national picture and develop the necessary overview the plans need
to place more emphasis on gathering the necessary information through reports from the regions.
Combining this with sound epidemiological investigation and analysis and using effective reporting tools
should make strategic and tactical decision making, not to mention international disease reporting,
resource allocation and prioritization much easier and more effective.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 47
The national veterinary authorities should develop their plans to define clearly (and avoid duplication)
the separate roles and responsibilities in the central authority based in the National Crisis Centre and the
local teams based in the Local Crisis Centres
It is also important that full reporting, both nationally and internationally, takes place at a very early stage –
among other things this will facilitate rapid access to international expertise where needed. All countries
confirmed they would meet this commitment. This should be a simple, automatic process but there were
some concerns that in some cases the process used to achieve this may be unclear and/or overly complex
and this could lead in some cases either to delays or, in a worst case scenario, failure to report. This process
could be simplified and the basis for doing so made explicit in the contingency plan. Responsibility for
ensuring this happens should lie with a named senior individual.
National veterinary authorities should amend their plans to make clear the circumstances when disease
must be reported internationally and that the responsibility for doing this lies with one named individual,
ideally the Chief Veterinary Officer.
National veterinary services should develop the capacity to seek international assistance if an outbreak is
identified as an exotic serotype of FMD and/or the size of the outbreak is beyond the national capacity to
deal with it.
During the initial diagnosis session all three countries appeared able to mount an immediate response
irrespective of the time of day. Their approach varied slightly, with 2 (Armenia & Georgia) dispatching
centrally based rapid response teams to do the work, but all seemed able to carry out clinical inspection of
affected and associated animals, impose initial restrictions, collect samples for confirmation of disease and
begin data gathering. There was considerable discussion on how rapidly this could be achieved, with some
overly optimistic estimates initially, but it appeared it should be possible, in most cases, to achieve this
within 24 hours of the initial report. It would be useful to test this through exercises using specific scenarios
to set up the structures such as the NCC & LCC, expert groups, despatch samples etc. and to measure the
time it takes to do so. It would also be useful to estimate how large an outbreak existing resources could
deal with without external assistance.
National veterinary services should carry out exercises using specific scenarios to measure the time
needed to set up the key disease control structures and processes and estimate the maximum size of
outbreak that existing resources could handle in order to assess the current level of preparedness.
In addition to the speed national authorities should consider the scale of the initial response. This will be
particularly important where the aspiration is to contain and ultimately eliminate the incursion. In the early
stages none of the countries considered national movement controls and all were cautious in their
approach to wider movement restrictions. All three countries would quarantine affected villages and
impose protection/buffer zones of approximately 3km radius and surveillance/observation zones of
approximately 10km around each village but there seemed to be an incomplete understanding of the
reasons for doing so. The concern here is that the clinical and epidemiological data provided contained
indications that disease was almost certainly more widespread and that wider movement controls might
have been more appropriate at this point. When this was reviewed after the third session, more
widespread disease, all agreed that with hindsight more extensive geographic restrictions might have been
better. Even then none felt that national restrictions would have been considered.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 48
A precautionary principle should apply here and a bolder initial approach would be beneficial on most
occasions. The longer term benefits for disease control of ‘over restricting’ initially and removing some of
the restrictions as information is gathered to show they are not/no longer necessary is likely to outweigh
the short term disadvantages. The alternative of ‘under restricting’ is likely unwittingly to let disease
continue to spread with the risk that the initial strategic goals will rapidly become unachievable.
National veterinary authorities should look again at their approach to the scale of initial control, and in
particular animal movement controls, and consider the benefits of ‘over restricting’ initially.
It was not possible to consider the legal basis for control measures in depth during the exercise (though all
refer to them in their plans) which concentrated instead on the individual measures that each team would
wish to apply in each zone. This generated considerable discussion, including the controls needed both on
rodents and other susceptible wildlife such as wild boar. There was considerable variation in the detailed
restrictions that would be imposed in each zone with one country even considering locating their local crisis
centre within the quarantine zone. Again there appeared to be an incomplete understanding of the
principles that should be applied in determining specific control measures. All did agree that animal
gatherings, including markets, would be banned. This is an important area and more work needs to be
carried out both to ensure that those involved have the necessary legal authority, understand the principles
that determine the controls to be applied and know how to gather and make full use of the information
needed to consider carefully the most appropriate restrictions for each case. The tendency to simply apply
standard restrictions must be avoided. A full hierarchy of control measures, a process for deciding the most
appropriate in each case and a firm legal basis for doing so is needed. As in other areas working with
experts, holding workshops/seminars and appropriate and targeted exercises would help develop this.
EuFMD should support further training designed to develop the full range of skills necessary to design
and implement disease control measures
National veterinary services should, after training, develop a full hierarchy of control measures, a process
for deciding the most appropriate in each case and make sure a firm legal basis for doing so is in place in
each country.
None of the countries would offer compensation to affected farmers though all have provision to do so and
some have done in similar outbreaks in the past. This is a difficult area. While driving perverse behaviour
and creating dependency on compensation must be avoided this must be set against the natural tendency
of individuals to ‘wait and see’ when disease is first suspected. This can have serious consequences
particularly in the first case, and particularly where the consequences of reporting can be difficult, even if
unintentionally, for the individual doing so. Even a slight delay could more than offset the benefits of a fast
and widespread response once it is detected. While not without its risks a small incentive to encourage
early reporting is a small price in the overall context of disease control. National authorities might want to
consider again the best approach in this area.
National authorities should regularly review, as part of the review of their contingency plans, whether or
not paying some compensation might assist in ensuring early reporting of suspect cases
While all three countries elected to submit samples for analysis at the initial visit the approach to doing so
varied. All three would send samples to their laboratories (the National Laboratory in Armenia, Regional
Laboratories in Georgia and Azerbaijan); Georgia would use its central team and a mobile facility to do so,
Armenia might do likewise but it would depend on the circumstances of the outbreak (location, alternatives

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 49
etc.). There was also some discussion on the use of pen side tests with general agreement that use would
depend on circumstances and availability of trained operators to use them.
All three countries are able to offer a range of suitable tests (all 3 would carry out ELISA, Armenia and
Azerbaijan report they would also use CFT and Georgia that it would use PCR) but all are limited to the
endemic serotypes within their country. All recognized the unusual clinical picture in the exercise suggested
this might not be an endemic FMD serotype and that their own laboratories, not surprisingly, might not be
able to confirm what they were dealing with. After considerable discussion the need to make appropriate
rapid use of international reference laboratories at times in order to quickly identify the serotype was
recognized. While all supported this their recent practical experiences suggested that in reality this might
not be easy to achieve.
National veterinary services, supported by EuFMD, must ensure they are able to collect, submit and test
samples, including where appropriate to international reference laboratories, to enable accurate
identification of serotypes to be carried as rapidly as possible.
All countries recognized the need to carry out a detailed epidemiological investigation but their approaches
varied, as did their ability to handle quickly and effectively the large amounts of information this generates,
depending largely on previous experiences. Some time was spent looking at simple tools, such as time lines,
to enable participants to separate out the key elements and communicate their findings rapidly and
effectively to others. Participants made use of this where they could but more training and practice is
needed, both for epidemiologists and more widely across the veterinary services, in using these tools.
There was clearly a great enthusiasm to develop skills further in this area.
EuFMD should support further training and practice, both for epidemiologist and more widely across the
veterinary services, in carrying out epidemiological investigations, gathering and analysing
epidemiological data and, particularly, communicating epidemiological findings.
All three countries indicated that if an exotic serotype of FMD was confirmed they would pursue a
slaughter policy as part of an elimination strategy, at least in the early stages of an outbreak. What was less
clear was the decision on which animals to destroy (clinically affected only, all susceptible animals in a
village where disease has been confirmed or more widespread destruction of susceptible animals) or how
they would be destroyed and disposed. Some favour burning, others burial. Both approaches have
strengths and weaknesses and some time was spent discussing this but it was clear that if slaughter and
disposal is to be included in plans then much more work needs to be done in this area to ensure fully tested
and deliverable policies are developed which can be implemented in a timely manner. A slaughter policy
requires careful consideration of objectives, methods, analysis of costs and benefits, resources required
and achievable response times. In endemic countries, the benefits may not necessarily outweigh the costs.
National veterinary services should carry out work to determine whether a slaughter and disposal policy
might be put in to practice in each country, and if it is, how the stated objectives may best be achieved.
All three countries recognized the need to carry out tracings as part of the disease control process. Two
aspects were recognized – the creation of considerable amounts of data that would be difficult to manage
and the large number of visits that would be needed to follow these up. It was acknowledged that
identifying the tracings might be difficult to complete (relying on people’s memories in many cases) and it
was recognized that following up the tracings with visits to relevant premises might create more work than

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 50
existing resources could handle. This led to some discussion about prioritisation, hot and cold tracing etc.
and tools to handle the information but more work is needed in this area.
EuFMD should support further training in using tracing tools to identify and manage tracing.
National veterinary services should develop their tracing skills further, making use of reliable animal
identification systems wherever possible, and working with the epidemiologists to ensure that the
resulting work can be prioritized correctly during an outbreak.
There was also some discussion on surveillance. All agreed that passive surveillance (responding to disease
reports) would be important and all reports would be investigated. Less clear was the role of active
surveillance (e.g. patrols) in the affected area and where and how this might be implemented. Some felt
that serosurveillance would be the best option, others that animal inspections would be more effective.
Greater clarity and consistency of approach is needed here if best use is to be made of what will by this
stage be limited veterinary resources.
EuFMD should support further training and practice to develop surveillance skills
National veterinary services should ensure that all staff who will be involved in surveillance are trained to
a level to enable them to do so effectively, including training in the importance of good biosecurity to
avoid surveillance teams spreading disease
All these areas will generate large amounts of data which will need to be managed carefully if it is to be
used effectively. Good information, derived largely from this data, will be vital in making sound decisions on
control measures and in communicating these decisions more widely. It was not possible to look at this
aspect in detail during the exercise but discussions suggest that some systems are likely to struggle quite
rapidly if a large outbreak occurs. This needs to be investigated more fully and if any improvements are
identified they must be carried out to ensure that data handling systems can support the approach being
contemplated.
National veterinary services should, with suitable support, review their data handling systems to ensure
they are robust enough to handle the large volumes of data that will be generated and flexible enough to
derive the information needed to manage an outbreak.
National veterinary services should work with EuFMD to develop suitable systems and ensure that
enough staff are trained and familiar with their use to support any future outbreak.
Towards the end of the exercise all the players confirmed their initial view that they would still try to
eliminate the virus and would prefer to avoid emergency vaccination if possible. Emergency vaccination
was considered in the third session as part of containment and all recognised that with limited availability
and time needed to obtain and distribute stocks a clear vaccination strategy and delivery plan would be
needed and that more work was needed in this area.
EuFMD should support further training in developing vaccination strategies and delivery plans
National veterinary services should ensure that once they have the skills they develop emergency
vaccination strategies and delivery arrangements and that they include these in future iterations of their
contingency plans.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 51
During the exercise the issue of biosecurity and cleansing and disinfection (decontamination) arose from
time to time but it was possible to explore this in enough detail to draw meaningful conclusions. This is an
area that will need further consideration. Players recognized that they would be running a fairly large
operation, that resources would start to become limited (particularly but not exclusively veterinary skills)
and that it would be necessary both to work extensively with others and to prioritize effectively. All intend
to work with police, army and local authorities. It would be useful to practice this collaborative working
through regular joint exercises.
National veterinary services, supported initially by EuFMD, should establish a programme of routine joint
exercises with delivery partners, such as the army, police and regional/district authorities to ensure they
are able to collaborate fully in a future outbreak.
Overall the exercise identified a number of areas where development would significantly further
strengthen existing plans but to manage this development it would be beneficial to establish baseline
measures of the current state of readiness in each area in each country and to repeat these measures at
suitable intervals (probably annually). This would assist in prioritising the areas for improvement and
measuring progress towards the agreed level. Schemes to do this that could be tailored to each country’s
needs are readily available and would not be difficult to implement. Initially it might be better to use
independent experienced assessors but part of the process should include training local staff to develop the
necessary expertise in each country to enable them to undertake their own assessments in the longer term.
EuFMD should help identify a suitable existing scheme to assess the current state of readiness in each
country and should support the national veterinary services in its use.
National veterinary services should establish a regular programme of assessing readiness and use the
results to prioritize the areas for improvement and to monitor improvements.
National veterinary services will need external support in developing individual country contingency plans
further and in building capacity. This work will need to co-ordinated and managed to create synergy and
avoid duplication of effort.
EuFMD should assist countries in developing contingency plans further and in building capacity including
working with international donors to create synergy and avoid duplication of work.
Summary and Discussion of Recommendations
Set out below is a summary of recommendations.
1. The national veterinary authorities should expand the next iteration of the plans to include more
information on strategic intentions when dealing with different scenarios and on the process for
deciding how best to achieve and communicate these on each occasion.
2. The national veterinary authorities should develop their plans to define clearly (and avoid
duplication) the separate roles and responsibilities in the central authority based in the National
Crisis Centre and the local teams based in the Local Crisis Centres.
3. National veterinary authorities should amend their plans to make clear the circumstances when
disease must be reported internationally and that the responsibility for doing this lies with one
named individual, ideally the Chief Veterinary Officer

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 52
4. National veterinary services should develop the capacity to seek international assistance if an
outbreak is identified as an exotic serotype of FMD and/or the size of the outbreak is beyond the
national capacity to deal with it.
5. National veterinary services should carry out exercises using specific scenarios to measure the time
needed to set up the key disease control structures and processes and estimate the maximum size
of outbreak that existing resources could handle in order to assess the current level of
preparedness.
6. National veterinary authorities should look again at their approach to the scale of initial control,
and in particular animal movement controls, and consider the benefits of ‘over restricting’ initially.
7. EuFMD should support further training designed to develop the full range of skills necessary to
design and implement disease control measures.
8. National veterinary services should, after training, develop a full hierarchy of control measures, a
process for deciding the most appropriate in each case and make sure a firm legal basis for doing so
is in place in each country.
9. National authorities should regularly review, as part of the review of their contingency plans,
whether or not paying some compensation might assist in ensuring early reporting of suspect
cases.
10. National veterinary services, supported by EuFMD, must ensure they are able to collect, submit and
test samples, including where appropriate to international reference laboratories, to enable
accurate identification of serotypes to be carried as rapidly as possible.
11. EuFMD should support further training and practice, both for epidemiologist and more widely
across the veterinary services, in carrying out epidemiological investigations, gathering and
analyzing epidemiological data and, particularly, communicating epidemiological findings.
12. National veterinary service should carry out work to determine whether a slaughter and disposal
policy might be put in to practice in each country, and if it is, how the stated objectives may best be
achieved.
13. EuFMD should support further training in using tracing tools to identify and manage tracing.
14. National veterinary services should develop their tracing skills further, making use of reliable
animal identification systems wherever possible, and working with the epidemiologists to ensure
that the resulting work can be prioritised correctly during an outbreak.
15. EuFMD should support further training and practice to develop surveillance skills.
16. National veterinary services should ensure that all staff who will be involved in surveillance are
trained to a level to enable them to do so effectively, including training in the importance of good
biosecurity to avoid surveillance teams spreading disease.
17. National veterinary services should, with suitable support, review their data handling systems to
ensure they are robust enough to handle the large volumes of data that will be generated and
flexible enough to derive the information needed to manage an outbreak.
18. National veterinary services should work with EuFMD to develop suitable systems and ensure that
enough staff are trained and familiar with their use to support any future outbreak.
19. EuFMD should support further training in developing vaccination strategies and delivery plans.
20. National veterinary services should ensure that once they have the skills they develop emergency
vaccination strategies and delivery arrangements and that they include these in future iterations of
their contingency plans.
21. National veterinary services should, supported initially by EuFMD, establish a programme of
routine joint exercises with delivery partners, such as the army, police and regional/district
authorities to ensure they are able to collaborate fully in a future outbreak.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 53
22. EuFMD should help identify a suitable existing scheme to assess the current state of readiness in
each country and should train the national veterinary services in its use.
23. National veterinary services should establish a regular programme of assessing readiness and use
the results to prioritize the areas for improvement and to monitor improvements.
24. EuFMD should assist countries in developing contingency plans further and in building capacity
including working with international donors to create synergy and avoid duplication of work.
All three countries recognized that containing and eliminating an outbreak of FMD required a significant
change in approach, a high level of preparedness and involved a large operation that needed to be
maintained for a considerable period of time. To reach this level of preparedness requires a structured
programme of development, training and testing. While players were able to identify areas for
improvement during the exercise it was not possible to make a quantitative assessment of current levels of
preparedness in each area or to measure them against agreed levels. The first step to detecting an exotic
strain of FMD is an effective and functioning system for passive surveillance (reporting of suspicion)
followed by rapid field investigation of suspected FMD cases, with timely and reliable laboratory testing of
samples. It is not possible to differentiate serotypes or strains by clinical signs (although endemic strains
may have less severe signs in vaccinated groups). Therefore improvement is this area will also help detect
non-exotic FMD. Contributing significantly towards this and an obvious priority is the recommendation to
ensure each veterinary service is able to collect, submit and test samples, including where appropriate to
international reference laboratories, to enable accurate identification of serotypes to be carried as rapidly
as possible (recommendation 10). This will be essential if the necessary early confirmation is to be achieved
to enable the appropriate response to be mounted. This should be relatively straightforward to do and,
irrespective of any other improvements, would provide immediate benefit. This will also make it easier to
implement the recommendations relating to international co-operation and support (recommendations 3,
4 & 24). To develop fully effective plans it would be beneficial to widen involvement in the process both
across the veterinary services and further afield. This would lead to wider ownership of the plans, make full
use of all the expertise that already exists and lead to development of locally effective solutions.
To achieve this it would make sense to start by addressing the recommendations on strategic approach and
roles and responsibilities (recommendations 1 & 2) Doing this first would make it much easier to identify
the right individuals and groups to be involved in development of specific areas and it would guide their
work in doing so. The next priority is to develop epidemiological skills (investigations, analysis and
reporting) further and to provide some base lining and routine measuring of current levels of preparedness
in each area identified. (recommendations 5, 11, 22 & 23). Using the results of a structured base lining
exercise would facilitate the prioritisation of the remaining areas. Most of these are operational and would
best be taken forward through training with experts, arranging workshops/seminars and holding specific
exercises both to train and evaluate. The next phase should address the key operational skills – designing
and implementing disease control measures, tracing, surveillance, data handling and emergency
vaccination strategy and delivery plans.(recommendations 7, 8, 13, 14, 15, 16, 17, 18, 19 & 20)
The penultimate phase is for the national veterinary services to look again at some of their policies,
specifically relating to the scale of initial response, payment of (some) compensation and slaughter and
disposal. (recommendations 6, 9 & 12). The final phase, once the bulk of the development is complete, is
the establishment of a programme of routine exercises that would ensure that most individuals that will be
involved in dealing with an outbreak have regular opportunities to refresh and test their skills.
(recommendation 21).

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 54

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 55
Annex III
Trans-Caucasus Countries FMD desktop
simulation exercise, November 2012-
Report by C. Danielsson
(as sent by C. Danielsson, Senior Adviser to National Food Agency, Georgia (CBA/G Project)

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 56
ANNEX III TRANS-CAUCASUS COUNTRIES FMD DESKTOP; REPORT BY C. DANIELSSON
Swedish Board of Agriculture | SE-551 82 Jönköping www.jordbruksverket.se | [email protected]
Swedish Board of Agriculture 12-11-2012 Division for International Affairs and Contingency
EuFMD Trans Caucasus Countries (TCC) Foot- and Mouth Diseases (FMD) Desktop Simulation Exercise Date: 6-7 November 2012 Location: Signagi, Georgia Participating countries: Georgia, Armenia, Azerbaijan
Mission objective: To participate mainly as an observer and contribute with input from the perspective of CBA/G1 project component of Civil Emergency Planning. Mission output: A supplementary report to the complete report provided by FAO consultant Robert A. Paul. Supplementary report includes full exercise documentation and key conclusions/recommendations. SIGNED C. Danielsson Senior Adviser to National Food Agency, Georgia (CBA/G Project) 1 Capacity Building Agriculture / Georgia implemented in Georgia, National Food Agency 2011-2014. The project is financed by the Swedish Development and Cooperation Agency and is divided into five interrelated work packages targeting the National Food Agency in Georgia.
CBA--‐G

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 57
Introduction This supplementary report is divided into two reporting components, each feeding into the main report provided by FAO consultant Robert A. Paul. The FIRST component includes a set of key observations. For the most part, these are based on the discussion points provided in appendix A. In addition to identifying significant competences that arguably necessitate further strengthening/development, observations may also provide some insight into the broader context of civil emergency planning. Including an understanding of validating contingency plans and capabilities through regular exercises and trainings. Albeit not directly related to the exercise objective, the first component also includes a set of recommendations about possible ways to continue building capacity in the field of contingency planning. Recommendations are general in scope and may apply to circumstances in each participating country. In terms of general capacity-building in the sphere of contingency planning, it is recommended, should FAO express a continued interest in providing support to Georgia, to liaise and coordinate proposed activities with the CBA-G project. Coordination may contribute to valuable synergy effects whilst avoiding unnecessary duplication of work. The SECOND component is attached as an appendix. It is entirely descriptive and summarises the main discussion points during the exercise. It adheres to the structure laid out by the FAO FMD TCC Exercise Questions Sheet. Key conclusions, reflections and recommendations pertaining to FMD TSS Exercise General reflections The exercise provided an excellent opportunity to familiar the participating countries with key issues requiring urgent attention in case of an outbreak of FMD (e.g. Sat2). The set-up of the exercise was well balanced and raised pertinent questions related to each country´s current capability to deal with a cross-border outbreak of EDDs. While the focus of the exercise was predominately operational in character, the question sheets also forced the participants to contemplate relevant strategic and political implications of the scenario. Generally in the trans-caucasus countries, there appears to be a limited experience of using this type of methodology as a tool for validating and/or developing existing or new capabilities including contingency plans. Thus, the need for similar exercises/trainings is well substantiated. Each national delegation delved into the exercise with good empathy and humour. Still it would be understandable if some of the participants experienced the sheer volume of issues raised, at times, as overwhelming. Nevertheless the design of the exercise (overload) generally provides good indicators of what capabilities need further strengthening and/or development.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 58
Key conclusions
Early detection: The scenario highlighted the importance of early detection and diagnostic capability. In particular it emphasises the crucial role played by the local veterinarian. Only Azerbaijan maintains a reliable sampling-capability at the local level. The remaining countries, in the scenario, rely on central capabilities (response team) that are dispatched from the capitol. This amounts to lost time at a crucial stage of disease spread. Neither trainings nor resources are provided to the local level by these countries. In addition there was an important discussion regarding where to send samples following confirmation of FMD-virus. Reference laboratories including the logistics of sending samples and receiving results appears unclear.
Contingency- plans: Each country provided their contingency plans (FMD) to the facilitator of the exercise beforehand. Generally these plans appear immature and inadequately incorporated into the wider emergeny planning context of respective agency. The Plans have only been partially validated. Several actions, for example setting up central- and regional incident response structures have not been tested or validated. Implementing such structures (effectively) may thus prove cumbersome in an urgent situation. Thus delaying important field-activities such as tracing, sampling, vaccination and stamping out. As a general rule, all contingency planning should be multi-hazard in its approach. Making good use of generic structures notwithstanding the character of the scenario is key in effective resource-management. By tailoring incident-response to specific scenarios, there is a risk of succumbing to an overly event-driven approach. Thus ending up in a situation in which the responsible agency cannot deliver an adequately flexible and adaptable response. Many of the actions proposed to manage an outbreak are not documented in specific checklists, routines and so forth. Instead much of the expertise is vested in a limited number of experienced individuals. A culture of dependency on key individuals with elaborate informal networks often overrides (if any) formal institutional competences and processes. This implies poor back-feed from incidents and limited institutional development and memory over time.
Command & control: No strategic decision-makers participated in the exercise, except for the CVO of Azerbaijan and the deputy CVO of Georgia. While the exercise did not apply a strategic focus, it nevertheless revealed the importance of incorporating such elements (and participants) in future exercises. Basic concepts and tools of contingency planning were not applied, used or contemplated by the participants in the exercise. For example establishing a shared situational awareness, information-management, resource-management, forward-looking analyses (alternative scenarios), cost-benefit analyses etc. Only to a limited extent was basic methodology (international standard) in disease-control operationalized.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 59
Legal framework: Each country maintains a legal framework of how to deal with situations similar to that of the scenario. It is unclear however to what extent this legal framework is sufficiently updated and implemented given frequent institutional developments (re-organisation) taking place in the participating countries. Any actions taken by a governmental agency must be based on a legal mandate. Thus, officers in charge must show a good understanding of relevant normative acts. Recommendations
Actively promote a culture of conducting validation exercises in the trans-caucasus countries.
Include strategic decision-makers and other relevant stakeholders in future exercises. This will in addition contribute towards increased awareness and understanding of FMD and related animal diseases among policy-makers.
Build capacity to deal with FMD from a multi-hazard perspective. This means building generic command and control structures (including resources) that are flexible, adaptable and easily scalable notwithstanding the scenario. The entire context of the responsible agency needs to be taken into consideration. Involve professional contingency planners in the process.
Strengthen, and where needed, develop contingency plans. Establish the legal mandate. Define roles and responsibilities as well as the coordination capability (including information-management) between central- and regional/local level. Ensure organisational endurance. Regard contingency plans as invalid if not adequately tested.
Conduct, where relevant analyses to be used as key documentation for making necessary disease-control priorities in urgent situations. For example national standstill decisions, where to establish regional crisis centres, appropriate burial sites, methods of disposal, sampling strategies etc.
Introduce the precautionary principle in strategic disease-control management. Where there are good indicators that the situation may quickly escalate, the response should rather be “exaggerated” in the initial phase of the incident-response.
Create and maintain formal networks and institutional know-how. Apply a process-oriented approach to dealing with FMD.
Introduce and standardise disease-control concepts and tools. Ensure compatibility with corresponding concepts of contingency planning. APPENDIX 1 – Main discussion points Session 1 – National contingency plans for FMD GENERAL NOTE All three countries appear to have a similar set-up and level of maturity of contingency plans (Plan) for FMD. Each Plan is currently in an on-going draftprocess and appears inadequately coordinated with other Plans for animal diseases (EDD). Neither of the countries appears to apply a multi-hazard

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 60
approach to contingency planning. In addition no country seem to have validated their plans through exercise or training, especially the decision-making process and central-regional crisis structures. COUNTRY SPECIFIC GE: The Plan is a draft. Its content concerns contingency planning in all regions (11) and districts (65). The Ministry of Agriculture (MoA) is involved in the elaboration process of the Plan. In terms of reporting of suspicious animal disease, it is compulsory for all stakeholders. This is done to the nearest veterinarian, may he/she be official or private. They in turn must immediately notify a state veterinarian who notifies the National Food Agency (NFA) centrally. The head of the NFA is responsible for notifying the government, neighbouring countries and relevant international bodies such as the OIE of confirmed disease. To swiftly combat an Especially Dangerous Animal Disease (EDA), the NFA may decide to establish a National Crisis Center (NCC). Members of that temporary decision-body includes among others the deputy ministry of agriculture, CVO, head of veterinary department and when needed, international experts. To supplement the NCC, a Regional Crisis Center (RCC) may be operationalized locally. It is headed up by the NFA regional office staff and relevant local authorities. No compensation scheme is in place. AR: Armenian veterinary services are mostly made up by state-employed veterinarians. It is the MoA in Armenia that is responsible for disease-control and setting up of regional/local response structures (committees). Generally the institutional framework for disease-control in Armenia is under development. No compensation scheme is in place. Government may however decide on compensation on a case-by-case basis. This was for instance done in the first year of outbreak of swine fever in the country. AZ: The country is divided into several veterinary structures. There are approximately 65 veterinary districts (corresponds to region), 12 laboratory regions and some 700 veterinary points (corresponds to district). Contingency plans for FMD was initially developed in 2005. It was revised and updated in 2007. A plethora of normative legal acts regulate disease-control, including FMD; CISframework plan, Plan of joint actions etc. There is in addition a list of EDDs which also includes principles of prevention and eradication. While there is no formal compensation scheme in place, there are however “rules” on this issue. In terms of notification, animal owners are obliged to notify its nearest veterinary point. They in turn are responsible for initial epidemiological investigation. They report to higher government levels. In addition to the local veterinary, the regional CVO and an officer from the nearest laboratory visits the site and supports the investigation. Samples are immediately sent to state laboratory in Baku or to Russia. In disease-control, a similar set-up of NCC is used. The incident-response

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 61
organisation is mostly based on the ministerial level. Regional/local crisis centres may be established. It is headed up by the regional veterinary office and populated by among others, local stakeholders. Session 2 – Initial Report to confirmation (Q sheet 1) Q1: Who will make report and are they obliged to do so? AR: The village veterinarian. They are obliged. GE: The village veterinarian (private/state) They are obliged. AZ: The village veterinarian. They are obliged. Q2: Who receives the report? (In the first instance) AR: The regional veterinary body and unnamed “relevant” stakeholders. GE: The district or regional veterinary body and unnamed “relevant” stakeholders. AZ: The district AND central authority. Q3: What actions do they take? ALL: On-site investigation. The farm is put in quarantine pending further investigation and diagnostics. Q4: Who do they inform? ALL: See Q 2 Q5: What are the timings? ALL: Immediately. Despite it being 20.00 in the evening. Q6: What restrictions are imposed and when? ALL: For example number of animals with clinical signs, preliminary diagnosis, last vaccination, number of suspected animals in the region, contacts with others, last movements, vet´s own reflections and comments. Swedish Board of Agriculture 12-11-2012 9(17) Q7-8: What information is required AND how is it recorded? ALL: A specific form is used by the veterinary inspector. It is recorded by hand. Q9: To whom is it provided? ALL: See Q2 Q10: Who decides on next steps HOW? AR: A permanent crisis commission (local) decides on next step. GE: No reply. AZ: First meeting is held by a local committee. Decisions may be taken following a visit of the regional veterinary head has visited the relevant farm. Q11: Are you going to sample, WHY? All: Yes, samples will be obtained. Samples are needed to confirm/disconfirm clinical signs detected by veterinarian and animal owner. Actions taken by AR and GE at this stage includes dispatching a rapid response team centrally. Only this resource has the capability to collect relevant samples. The resource is anticipated to arrive early in the morning the following day. Thus samples are taken in the morning. In AZ, the village veterinarian is capable of collecting relevant samples. Samples may thus be taken already in the evening. Q12-13: What samples and tests?

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 62
AR: ELISA (antigen) and rapid tests from tissue samples. From animals showing clinical signs. Results from antigen test expected in one day. Is diagnosed by national laboratory. GE: ELISA and PCR may be taken in the field but only rapid response team dispatched from the HQ has necessary training. Results may be obtained at the close of day. AZ: ELISA and rapid test. Results expected in the same day. Scans for all 7 FMD serotypes. AR and GE have the capability, through rapid response team, to analyse results on-site. Q14: What laboratories? AR: Collected samples sent to National laboratory GE: Collected samples sent to Regional laboratory AZ: Collected samples sent to Regional laboratory Q15: What are the arrangements for getting samples there? ALL: Samples are collected, packaged and sent according to a pre-established format. The package includes a standardised label with necessary information about the sample Q16: What is the timescale for results and who decides? AR: Laboratory operator informs head of laboratory who in turn informs the Food Safety Service Agency and CVO. GE: Laboratory informs the head of animal department at NFA (CVO). He/she contacts head of NFA and presents the results. The head of agency informs other stakeholders. AZ: The laboratory informs the CVO. He/she informs the National Commission who confirms the outbreak. CVO reports to relevant international bodies. Q17: What actions will be taking place in the meantime? AR: All veterinarians in the affected geographical are informed of the issue. Tracing takes place. Every farmer keeps animals confined. Report on vaccination status. GE: No reply. AZ: Restriction on movements is imposed, clinical signs evaluated and affected animals are isolated. Tracing. A veterinary point of contact is assigned to the farm. Q18: Are actions limited to village if not what actions are taking place in wider area? ALL: No discussion AND no specific measures mentioned in the discussion. Q19: How is wider situation being monitored? ALL: No discussion AND no specific measures mentioned in the discussion. Q20: What structures and processes will you establish (battle rhythm)? ALL: Command and control based on central-regional crisis centres/committes. DISCUSSION ALL: Each country send samples to reference laboratory on confirmation on FMD-virus (notwithstanding serotype) from national laboratory. While AR and AZ send samples to reference laboratory in Russia, GE sends to Pirbright, UK. There was a general uncertainty as to how reference samples are sent, diagnosed and managed. AZ acknowledged they had experienced problems in this area

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 63
(logistical) but that there nowadays are private companies specialising on sample logistics. Session 3 – Several confirmed cases (Q sheet 2) Q1: What additional controls are you going to put in place? GE: Introduces zones (quarantine) in each village. All susceptible animals are stamped out. Carcasses are burnt. Disinfection of premises. Pest control. All animal products destroyed. Measures relate to protection zone. Before measures are implemented, a special group enters the farm and makes a full investigation. Tracing is part of this investigation. Local government is contacted for epizootic burial. Wild animals (hunters) is an issue which is pursued from an epidemiological perspective. Special checkpoints and foot path controls are set up. When carrying out tracing, the outcome of that work is shared with affected villages. Animal markets are closed down. At this point in time, NO COUNTRY introduces a national stand-still. AR: No specific reply. AZ: No specific reply. DISCUSSION ALL: Destroying and disposing of 1200 or so animals will take an elongated period of time. In the UK it took weeks! Discussion about vaccination in surveillance zone. Q2: What restrictions are you placing on movements of animals, products, people and other? No discernible discussion. Q3: What movements are you going to allow? GE: Only rapid response team and veterinarians working in the restriction zone are allowed freedom of movement. Q4: How will you decide, monitor and amend? No discernible discussion. Q5: How are you going to control them? No discernible discussion. Q6: What tracing will you do? No discernible discussion. Q7: How will you do it (animal ID)? No discernible discussion. Q8: What actions will you take when you successfully trace? No discernible discussion. Q9: How will you manage the tracings? No discernible discussion. Q10: What zones will you set up and why? No discernible discussion. Q11: What control measures will apply in those zones? No discernible discussion. Q12: How will you enforce/control? No discernible discussion. Q13: How will you decide which movements you will allow? No discernible discussion.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 64
Q14: Which movements will you allow? No discernible discussion. Q15: How will you manage this (general/specific) No discernible discussion. Q16: What surveillance? (active/passive) ALL: Predominately passive surveillance. Session 4 – Regional control (Q sheet 3) Q1: Do you have full understanding of the disease spread? AZ: Picture is incomplete. For example movement of milk trucks, markets, sources and so forth. DISCUSSION A discussion on tracing ensued. Carsten talked about the difference (and importance) of “hot” tracing and “cold” tracing. Hot tracing such as types of contacts, significance of movement etc. is tracing which should be prioritised. Cold tracing on the other hand such as contacts with e.g. relatives living in urban are with no animal-keeping or similar, should only be pursued pending resources. Q2-3: What further information do you require and how to obtain? ALL: Have to address and investigate movements and transactions of the market and contact veterinarians, driver of milktruck and so forth. Prioritisation is necessary. Q4: What are you major concerns at this stage? AZ: Tracing is a major concern. Farmers and other parties may not recollect past events and transactions. Resources must be made available as well as financial funds, personnel, vehicles and so forth. Q5-9: How are you going to address them? AZ: Will raise relevant issues before the National Commission in which relevant stakeholders are represented. Must involve armed forces resources. This resource will contribute to securing protection zones. In addition, relevant ministries will be approached as well as police forces. In AZ there is such a thing as a special police battalion called the quarantine battalion. This asset is of course activated. It dispose of special biosecurity chambers. Q10: How would you reach a decision on vaccination? AZ: Highest level, the National Commission decides. But vaccination is the last resort. As a preparedness measure, vaccine doses will be purchased. Documentation and recommendation is crucial at this stage. It must maintain good quality for decision-makers. Should vaccination of animals be decided, then its a ring vaccination which is applicable. Thus, first ring vaccinate then destroy. Several strategic decisions will have to be made. Q11: Where will you obtain vaccine? AZ: FAO store 25 000 doses. Q12: When will vaccine be available? AZ: In seven days. Q13: Where will you vaccinate? AZ: Vaccination will take place outside the surveillance zone. Q14: What will you vaccinate?

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 65
AZ: All susceptible animals. Focus on large cattle. Q15: How will you store and distribute vaccine? AZ: Maintain a cooling-chain. AZ has a special department dealing with vaccines. Throughout the country there are cold storage facilities. Q16: Who will do the vaccinating? Is there any flexibility? AZ: Performed by state veterinarians. Q17: What impact till this have on current control measures/your existing vaccination programme? AZ: Q18: How long will it take? AZ: It completely depends on the size of geographical area. Q19: Where will you start? AZ: Vaccinations start beyond the surveillance zone and then progress outward from the zone. Q20: How will you prioritise? AZ: Will depend on several factors, for instance the limited number of vaccination doses available. One must also take into account epidemiological results and incubation periods. Will probably prioritise vaccination of calves. They are more susceptible due to less developed immune system. NOTE: Robert: Not necessarily true. None has immune defence concerning SAT2. It is often the small ruminants that contribute to disease spread the most. Q21: How will you adapt to changing disease spread? AZ: No discernible discussion. DISCUSSION A discussion ensued on what focus one should put on disease spread in the wild population. It was concluded that disease spread in the wild boar population is not a driver for disease spread. Due to lack of density, a potential FMDinfections normally dies out. It can seldom maintain virulence. Thus, don’t get caught up in less important details, e.g. the wild population. Spread is almost always associated with human movements. Session 5 – Conclusions AZ: Desire more collaboration and training on vaccination strategies concerning exotic serotypes of FMD. Propose a workshop centred on this particular issue. AZ: Desire more information on the role of wild life in outbreak and spread of FMD-virus. GE: Desire additional information on vaccination strategy concerning small ruminants. AR: Desire additional information concerning zoning strategies related to exotic
serotypes of FMD.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 66

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 67
Annex IV
FMD Monthly report: December 2012

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 68
ANNEX IV FMD-DECEMBER REPORT
Foot-and-Mouth Disease situation Monthly Report December 2012 I N F O R M A T I O N S O U R C E S U S E D: Databases: *OIE WAHID World Animal Health Information Database* *FAO World Reference Laboratory for FMD (WRLFMD)* Other sources: *FAO/EuFMD supported FMD networks* *FAO/EuFMD projects and field officers* ACKNOWLEDGEMENT: Laboratoire veterinaire de Goma, DRC
The sources for information are referenced by using superscripts. The key to the superscripts is on the last page
Please note that the use of information and boundaries of territories should not be considered to be the view of
the U.N. Please, always refer to the OIE for official information on reported outbreaks and country status.
GENERAL OVERVIEW
Foot-and-mouth disease (FMD) distribution by Serotype and the seven virus pools,
2010-2012 (Map 1)
Pools represent independently circulating and evolving FMDV genotypes; within the pools, cycles of emergence and spread
occur that usually affect multiple countries in the region. In the absence of specific reports, it should be assumed that the
serotypes indicated below are continuously circulating in parts of the pool area and would be detected if sufficient
surveillance was in place (Table 1).

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 69
Map 1: Foot-and-mouth disease virus pools distribution, 2010-2012
Table 1: List of countries representing each virus pool
POOL REGION/COUNTRIES SEROTYPES
1
CENTRAL/EAST ASIA
(Cambodia, China (People's Rep. of), China (Hong Kong, SAR),China (Taiwan
Province), Japan, Korea (DPR), Korea (Rep. of), Lao PDR, Malaysia, Mongolia,
Myanmar, Russian Federation, Thailand, Viet Nam)
O, A, Asia 1
2 SOUTH ASIA
Bangladesh, Bhutan, India, Nepal, Sri Lanka O, A, Asia 1
3
WEST EURASIA & MIDDLE EAST
(Afghanistan, Armenia, Azerbaijan, Bahrain, Bulgaria, Egypt, Georgia, Iran, Iraq,
Israel, Jordan, Kazakhstan, Kuwait, Kyrgyzstan, Lebanon, Libya, Oman, Pakistan,
Palestine Autonomous Territories, Qatar, Saudi Arabia, Syrian Arab Republic,
O, A, Asia 1

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 70
Tajikistan, Turkey, Turkmenistan, Uzbekistan)
4
EASTERN AFRICA
(Burundi, Comoros, Congo D. R., Djibouti, Egypt, Eritrea, Ethiopia, Kenya, Libya,
Rwanda, Somalia, North Sudan, South Sudan, Tanzania, Uganda, Yemen)
O, A, SAT 1, SAT 2
5
WEST/CENTRAL AFRICA
(Benin , Burkina Faso, Cameroon, Cape Verde, Central Afr. Rep., Chad, Congo D. R.,
Congo R., Cote d'ívoire, Equatorial Guinea, Gabon, Gambia, Ghana, Guinea Biss.,
Guinea, Liberia, Mali, Mauritania, Niger, Nigeria, Sao Tome Principe, Senegal,
Sierra Leone, Togo)
O, A, SAT 1*, SAT 2
6
SOUTHERN AFRICA
(Angola, Botswana, Congo D. R., Malawi, Mozambique, Namibia, South Africa,
Zambia, Zimbabwe)
{O, A}**, SAT 1,
SAT 2, SAT3
7 SOUTH AMERICA
(Ecuador, Paraguay, Venezuela) O, A
* NOT CONFIRMED IN THE PAST 30 YEARS IN DOMESTIC ANIMALS
** ONLY IN NORTH ZAMBIA AS OVERSPILL FROM POOL 4
Egypt and Libya are indicated as being in multiple pools, since they have evidence of FMDV originating from 2 or more
pools in the recent past (4 years).
POOL 1: China1 – Serotype O outbreak was reported in Xinbei, Changzhou, Jiangsu; POOL 2: Nepal2 – FMD
serotype O outbreaks in Lalitpur and Kavre districts were reported; POOL 3:Iraq5 – A/ASIA/ Iran-05SIS-10
was
confirmed. Turkey5, 2 –During December, 31 FMD outbreaks were reported. A new incursion of A/ASIA/ Iran-
05SIS-10
was detected in Van region. POOL 4Tanzania5 – Poor vaccine protection against circulating FMDV
strains. POOL 5 Democratic Republic of the Congo14 – During November and December 2012, in Ruzizi plain
and around Uvira city, several FMD outbreaks were reported. POOL 6 Botswana5 – SAT2 serotype, topotype III,
was confirmed in Zone 2. POOL 7 No new events have been reported for this reporting period.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 71
POOL 1
CENTRAL / EAST ASIA
China1 – Serotype O outbreak was reported in Xinbei, Changzhou,
Jiangsu (Map 2). The pig farm got infected after introduction of
new live animals. 338 pigs were destroyed in response to the
disease. This is a reoccurrence of FMD which started in February
2012 in this region. Suspicion was based on clinical signs; FMD
was confirmed in National Laboratory (OIE Reference Laboratory)
by ELISA, virus isolation and PCR.
In response, in Liaoning and Ningxia divisions, emergency
vaccination was conducted (Table 2).
Table 2: Vaccination in response to the outbreak
Map 2: FMD outbreak in Xinbei
Cambodia15 – A recent study has shown that, according to
farmers’ knowledge and perception, and the relative incidence
of FMD from January 2009 to June 2010 in fifty-one villages of Svay Rieng province, FMD is not perceived as a
major animal health problem by farmers. This finding explains why the number of infected villages notified to
veterinary authorities is generally largely underestimated. FMD control in Cambodia would gain by running
more educational campaigns with farmers in its programs in order to promote farmer case reporting.
FMD in most central and eastern Asia countries is endemic (Map 3). Brunei and Japan are the only countries in
this region with the free FMD status where vaccination is not practiced.
There is a zone covering the provinces of Sabah and Sarawak in Malaysia which is designated as FMD free
without vaccination. In China, the main threat comes from O/Mya-98 strain and PanAsia strain. The O/Mya-98
strain mainly affects pigs, although cattle and goat/sheep can also show clinical signs in some field cases.
However, the type O PanAsia strain mainly affects cattle.
CATTLE SHEEP/GOATS SWINE
LIAONING 19584 31506 247141
NINGXIA 6141 8060 305

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 72
Map 3: FMD distribution by serotypes 2010 – 2012
Epidemiological analysis indicates that animal
movements associated with trade are the main
factors for the spread of the FMD and for transmission between provinces in China. Both Mya-98 and PanAsia
strains of FMDV sequences from PR China had a close relationship with those sequences from outbreaks in
Southeast Asian nations6. FMD history in past 2 years is given in Table 3.
Table 3: Pool 1 FMD history 2010-2012
COUNTRY/6 MONTHS
REPORTING TO OIE FMD HISTORY (past 2 years)
LAST OUTBREAK
REPORTED/TYPE OIE FMD STATUS
CAMBODIA, 2011 2011, 2012 – NOT TYPED1 OCT 2012/NOT TYPED
1 DISEASE PRESENT
CHINA (PEOPLE'S REP.
OF), 2011, ½ 2012 2011, 2012 – O
1 DEC 2012/O
1 DISEASE PRESENT
CHINA (HONG KONG,
SAR) , 2011
2011 – O1, 5
2012 – O3
NOV 2012/O3 DISEASE PRESENT
CHINA (TAIWAN
PROVINCE),
NO OIE DATA
2011 - 2011 – O 5
2012 – O1
NOV 2012/O1 UNKNOWN
JAPAN, 2011 2011, 2012 - NO REPORTED
OUTBREAKS1
JULY 2010/O1, 5
FREE WITHOUT
VACCINATION
KOREA (DPR), 2011 2011 – O1, 5
MARCH 2011/O1 ½ 2011-PRESENT

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 73
2/22011 – NOT REPORTED
KOREA (REP. OF), 2011 2011 – O1, 5
APR 2011/O1
½ 2011-PRESENT
2/22011 – NOT REPORTED
LAOS PDR,
NO SUBM. REPORTS
2011, 2012 - NO REPORTED
OUTBREAKS1
OCT 2010/O1 UNKNOWN
MALAYSIA,
2011, ½ 2012
2011 – O, A1, 5
2012 – O, A1, 5
JUN 2012/O1
FMD FREE ZONE WHERE
VACCINATION IS NOT
PRACTISED
MONGOLIA, 2011 2012 - O10
2012/O10
½ 2011 – LIMITED ON ONE
OR MORE ZONES, 2/22011
-NOT REPORTED
MYANMAR, 2011 2011 – O1 FEB2012/O
9 DISEASE PRESENT
RUSSIAN FEDERATION,
2011
2011 – O1
2012 – O1
MAR 2012/O1
½ 2011 – NOT REPORTED,
2/22011 -DISEASE PRESENT
THAILAND,
2011, ½ 2012
2011 – O, A1, 5
2012 – O, A1, 5
OCT 2012/A, O1 DISEASE PRESENT
VIET NAM, 2011
2011 – O1, 5
2012 – O5
MAR 2012/O5 DISEASE PRESENT
P O O L 2
SOUTH ASIA
Nepal2 – FMD outbreaks have been continuing to appear in Godamchaur, Lalitpur district. New outbreak was
reported in Kavre district. FMDV serotype O was confirmed by Ag ELISA. South Asia is known to be an FMD
endemic area but very limited data on serotypes is available (Map 4).
The PD-FMD at Mukteswar (FMD Reference laboratory for South Asia) is active in this region and is requested
to provide information on FMD circulation that will assist improved understanding of virus circulation.
FMD history in past 2 years is given in Table 4.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 74
Map 4: FMD distribution by serotypes 2010 – 2012
Table 4: Pool 2 FMD history 2010-2012
COUNTRY FMD HISTORY (past 2 years) LAST OUTBREAK
REPORTED/TYPE OIE FMD STATUS
BANGLADESH, 2011 2011 – O, A, Asia 16 NOT AVAILABLE
½ 2011DISEASE
PRESENT, 2/22011-
LIMITED TO ONE OR
MORE ZONES
BHUTAN, 2011 2011, 2012 – NO REPORTED
OUTBREAKS1
MAY 2010/NOT TYPED1 DISEASE PRESENT
INDIA, 2011 2011 – O, A, Asia 11 SEP 2012/NOT TYPED
3
LIMITED TO ONE OR
MORE ZONES
NEPAL, 2011 2011 – O, A, Asia 1
1, 6
20122
DEC2012/O2 DISEASE PRESENT
SRI LANKA, 2011 2011 – O1,
5 JUN 2011/O
1
½ 2011 - DISEASE
PRESENT
2/22011 – NOT
REPORTED

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 75
P O O L 3
WEST EURASIA & MIDDLE EAST
Iraq5- four samples from Babil, Diyala, Missan, Baghdad regions, collected in 2012, were sequenced at the SAP
Institute, Ankara, as part of its role as lead laboratory in the West Eurasia Laboratory Network. All isolates were
typed as A/ASIA/ Iran-05SIS-10 and had over 98% identity with viruses recently sampled from Turkey. The Iran-
05SIS-10 lineage is also present in Iran. This highlights two things:
This is evidence of cross-border spread of this virus lineage between Turkey and Iraq.
There is a clear benefit to the region from the a regional approach to surveillance and laboratory analysis.
Turkey5, 2 – During December 2012, 31 FMD outbreaks were reported, bringing the total number of outbreaks
in 2012 to 1038.
Serotype Asia 1 has been dominant over the year causing more than 50% of all outbreaks (Table 5). According
to the significant drop of outbreaks due to this serotype after August, a declining phase and completing of the
evolution cycle of Asia 1 virus could be considered (Figure 1).
Table 5: Distribution of serotypes
SEROTYPE No OF OUTBREAKS (2012) DECEMBER
O 106 3
A 177 13
Asia 1 565 9
not typed 191 6
total 1038 31

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 76
Figure.1. Distribution of outbreaks by month
Serotype O PanAsiaII has been causing limited numbers of outbreaks over the year, showing no spreading
potential.
Serotype A/ASIA/Iran-05 has spread and is dominant in a limited area of inner Anatolia and the middle of Black
Sea region. A new incursion of A/ASIA/ Iran-05SIS-10
was detected in Van region (Map 5). This sublineage has been also detected in Iraq, with sequencing performed by the SAP Institute, Ankara.
Map 5: The locations of samples which were genotyped as the new serotype A lineage virus

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 77
Trans-Caucasian countries (Georgia, Armenia, Azerbaijan)2 - no FMD outbreaks or suspicious cases have been
reported; no samples have been submitted for investigation.
FMD history in past 2 years is given in Table 6 and Map 6.
Map 6: FMD distribution by serotypes 2010 – 2012
Table 6: Pool 3 FMD history 2010-2012
COUNTRY FMD HISTORY (past 2 years) LAST OUTBREAK
REPORTED/TYPE OIE FMD STATUS
AFGHANISTAN, 2011 2011 – O, A, Asia 11, 5
DEC 20111 DISEASE PRESENT
ARMENIA, 2011
MONTHLY REPORTS
REGULARLY SUBMITTED
TO EUFMD
2011, 2012 – NO REPORTED
OUTBREAKS1
NOT AVAILABLE NOT REPORTED IN THIS
PERIOD
AZERBAIJAN, 2011
MONTHLY REPORTS
REGULARLY SUBMITTED
TO EUFMD
2011, 2012 – NO REPORTED
OUTBREAKS1
JUN 20011
NOT REPORTED IN THIS
PERIOD
BAHRAIN, 2011 2011 – O, A, Asia 1
5
2012 – O5
MAR 2012/O5
LIMITED TO ONE OR
MORE ZONES
BULGARIA,
2011, ½ 2012 2011 – O
1, 5 JUN 2011/O
1
½ 2011 – DISEASE
PRESENT, 2/22011, 2012
- NOT REPORTED IN THIS
PERIOD
EGYPT, 2011 – A, O1, 5
JUN 2012/SAT 21
2011 – NOT REPORTED,

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 78
2011, ½ 2012 2012 – O, A, SAT 21, 5
2012 - DISEASE PRESENT
GEORGIA, 2011
MONTHLY REPORTS
REGULARLY SUBMITTED
TO EUFMD
2011, 2012 – NO REPORTED
OUTBREAKS1
20021
NOT REPORTED IN THIS
PERIOD
IRAN, 2011 2011, 2012 – O, A, Asia 15 NOV 2012/O
5, A
2, Asia 1
5 DISEASE PRESENT
IRAQ, 2011 2011 – O,A
1
2012 – A5
20125/A DISEASE PRESENT
ISRAEL, 2011 2011 – O
1
2012 – O5
MAR 2012/O5 DISEASE PRESENT
JORDAN, 2011 2011, 2012 – NO REPORTED
OUTBREAKS1
20061
NOT REPORTED IN THIS
PERIOD
KAZAKHSTAN, 2011 2011 – O, A
1
2012 – O, A5
MAY 2012/O10
DISEASE PRESENT
KUWAIT, 2011 2011, 2012 – O5 FEB 2012/O
5 DISEASE PRESENT
KYRGYZSTAN, 2011 2011 – O, A1 NOV 2011/O, A
1
LIMITED TO ONE OR
MORE ZONES
LEBANON, 2011 2011, 2012 – NO REPORTED
OUTBREAKS1
03/20101
NOT REPORTED IN THIS
PERIOD
LIBYA,
NO SUBM. REPORTS
2011 – O5
2012 – O, SAT 25
APR 20121, 5
DISEASE PRESENT
OMAN, 2011 2011 - NO DATA AVAILABLE DEC 20111 DISEASE PRESENT
PAKISTAN, 2011 2011 – Asia 1, O
2012 – O, A, Asia 15, 13
JUN 2012/O, Asia 1, A
5, 13
LIMITED TO ONE OR
MORE ZONES

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 79
AUTONOMOUS
TERRITORIES
PALESTINE, 2011
2011 – O, A, Asia 11
2012 – SAT 21, 5
APR 2012/SAT 2
5
LIMETED TO ONE OR
MORE ZONES
QATAR, 2011 NO DATA AVAILABLE
½ 2011 – NOT
REPORTED,
2/22011DISEASE
PRESENT
SAUDI ARABIA, 2011 2012 – O5 JULY 2012/O
5 DISEASE PRESENT
SYRIAN ARAB
REPUBLIC, 2011
2011, 2012 – NO REPORTED
OUTBREAKS1
03/20021
NOT REPORTED IN THIS
PERIOD
TAJIKISTAN, 2011 2011 – Asia 11 NOV 2011/Asia 1
1
½ 2011 – NOT
REPORTED, 2/22011 -
DISEASE PRESENT
TURKEY,
2011, ½ 2012
MONTHLY REPORTS
REGULARLY SUBMITTED
TO EUFMD
2011 – Asia 1, A, O5,1
2012 – Asia 1, A5, O
1
DEC 2012/O, A5, Asia 1
1 DISEASE PRESENT
TURKMENISTAN
NO SUBM. REPORTS NO DATA AVAILABLE UNKNOWN
UZBEKISTAN
NO SUBM. REPORTS NO DATA AVAILABLE UNKNOWN
P O O L 4
EASTERN AFRICA
Tanzania5 – vaccine matching results, using three O type vaccines, 0 4625, O Manisa and OTur
5/09, show poor protection against circulating FMDV strains in Tanzania (Table 7).

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 80
Table 7: Vaccine matching results
r1 value
vaccine
0 4625 O Manisa OTur
5/09
field strain OTan 38/12
(mean) 0.19 0.08 0.26
r1 = > 0.3 Suggests that there is a close relationship between field isolate and vaccine strain. A potent vaccine containing
the vaccine strain is likely to confer protection.
r1 = < 0.3 Suggests that the field isolate is so different from the vaccine strain that the vaccine is unlikely to protect.
Map 7: FMD distribution by serotypes 2010 – 2012
East Africa is known to be FMD endemic area but with
limited available data (Map 7).
FMD history in past 2 years is given in Table 8.
Table 8: Pool 4 FMD history 2010-2012
COUNTRY FMD HISTORY (past 2 years) LAST OUTBREAK
REPORTED/TYPE OIE FMD STATUS
BURUNDI, 2011 2011 – O, A, SAT 1, SAT 27
20117 UNKNOWN
COMOROS, 2011 2011 - DISEASE SUSPECTED
BUT NOT CONFIRMED1
20101
SUSPECTED NOT
CONFIRMED

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 81
CONGO D. R. , 2011 2011, 2012 O, A, SAT 17 2011/2012
7, NO PRECISE
DATA
LIMITED TO ONE OR
MORE ZONES
DJIBOUTI, 2011 2011 – ABSENT1 NOT AVAILABLE
NOT REPORTED IN THIS
PERIOD
EGYPT ,
2011, ½ 2012
2011 – A, O1, 5
2012 – SAT 21, 5
JUN 2012/SAT 2
1
2011 – NOT REPORTED,
2012 - DISEASE PRESENT
ERITREA,
NO SUBM. REPORTS 2011 – O
5 DEC 2011/O
5 UNKNOWN
ETHIOPIA, 2011 2011 – A, SAT 1, O
5, 7
2012 – O5
2012/O5 DISEASE PRESENT
KENYA, 2011 2011 – O, SAT 1, SAT 2
1, 5
2012 – SAT 2, A7
NOV 2012/A, SAT27 DISEASE PRESENT
LIBYA ,
NO SUBM. REPORTS
2011 – O5
2012 – O, SAT 25,7
APR 2012
1, 5 DISEASE PRESENT
RWANDA,
NO SUBM. REPORTS
2011 – ABSENT7
2012 – NOT TYPED2
NOV 2012/NOT TYPED2 UNKNOWN
SOMALIA, 2011 2011 – NO DATA AVAILABLE 20111 DISEASE PRESENT
NORTH SUDAN, 2011 2011 – A, O1
DEC 20111 DISEASE PRESENT
SOUTH SUDAN, 2011 2011, 2012 – O, SAT 1, SAT 2,
A7
20117 DISEASE PRESENT
TANZANIA, 2011
2011 – SAT 1(buffalo), SAT 2
(cattle), O7, SAT3
1, 5
2012 – A, O, SAT 1, SAT 25
MAY-JULY 2012/A, O, SAT 1,
SAT 25
DISEASE PRESENT

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 82
UGANDA, 2011
2011 – O, A, SAT 1, SAT 2,
SAT37, 2, 1
201211
NOV 201211
DISEASE PRESENT
YEMEN,
NO SUBM. REPORTS NO AVAILABLE DATA
P O O L 5
WEST/CENTRAL AFRICA
Democratic Republic of the Congo14 – During November and December 2012, in Ruzizi plain and around Uvira
city, suspected FMD outbreaks were reported.
Morbidity reported in Uvira/Kaborosha was 5.9% and 0.44% in Luberizi during November.
During December suspected FMD outbreaks were reported in bovines in Ruzizi plain(South-Kivu),
Nyamugali/Luberizi and Kitemesho/Luberizi. Morbidity in December was low, 0.29% in Nyamugali/Luberizi and
1.17% in Kitemesho/Luberizi.
No samples has been tested nor sent to Pirbright Laboratory.
More suspicions, but no confirmed nor verified cases, were seen in South-Kivu, North-Kivu and Ituri.
Map 8: FMD distribution by serotypes 2010 – 2012
Foot and mouth disease is endemic in West Africa (Map 8). In Gabon, Sierra Leone, Mauritania, Guinea, Guinea
Biss. FMD has not been reported at least in the last 3 years.
FMD history in past 2 years is given in Table 9.

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 83
Table 9: Pool 5 FMD history 2010-2012
COUNTRY FMD HISTORY (past 2 years) LAST OUTBREAK
REPORTED/TYPE OIE FMD STATUS
BENIN, 2011 2011 – A, O, SAT 1, SAT 24, 1
DEC 2011/O, A, SAT 1, SAT
21
DISEASE PRESENT
BURKINA FASO, 2011 2011, 2012 – O, A, SAT 24
NO PRECISE DATA,
DEC 20111
DISEASE PRESENT
CAMEROON, 2011 2011 – O, A, SAT 24,1
20124 DISEASE PRESENT
CAPE VERDE ,
NO SUBM. REPORTS NO DATA AVAILABLE
CENTRAL AFR. REP.
2011 NO DATA AVAILABLE DISEASE PRESENT
CHAD,
NO SUBM. REPORTS 2011, 2012 – A, SAT 1
4
2011/20124, NO PRECISE
DATA UNKNOWN
CONGO D. R. , 2011 2011, 2012 O, A, SAT 14
DEC 201214
/NOT TYPED LIMITED TO ONE OR
MORE ZONES
CONGO R.,
NO SUBM. REPORTS NO DATA AVAILABLE
COTE D'ÍVOIRE, 2011 2011 – SAT 1, A1, O, SAT 2
4 2011
4
LIMITED TO ONE OR
MORE ZONES
EQUATORIAL GUINEA,
2011 NO DATA AVAILABLE
DISEASE SUSPECTED,
NOT CONFIRMED
GABON, 2011 2011 – ABSENT1 NO IN 2006-2012 PERIOD
1 NEVER REPORTED

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 84
GAMBIA,
NO SUBM. REPORTS 2011, 2012 –O, A, SAT 2
9
2011/20129, NO PRECISE
DATA DISEASE PRESENT
GHANA, 2011 2011 – O, A, SAT 1, SAT 24, 1
DEC 20111 DISEASE PRESENT
GUINEA BISS.,
2011, ½ 2012 2011, 2012 – ABSENT
1 NO IN 2009-2012 PERIOD
1
NOT REPORTED IN THIS
PERIOD
GUINEA,
2011, ½ 2012 2011, 2012 – ABSENT
1 NO IN 2007-2012 PERIOD
1
NOT REPORTED IN THIS
PERIOD
LIBERIA,
NO SUBM. REPORTS 2011, 2012 – A, SAT 2
4
2011/20124, NO PRECISE
DATA UNKNOWN
MALI, 2011 2011/2012 – O, A, SAT 1, SAT
24, 1
2011/20124, NO PRECISE
DATA
LIMITED TO ONE OR
MORE ZONES
MAURITANIA, 2011 2011, 2012 – ABSENT1 NO IN 2007-2012 PERIOD
1
NOT REPORTED IN THIS
PERIOD
NIGER, 2011 2011/2012 – O, A, SAT 1, SAT
24, 1
NO PRECISE DATA,
OCT 20111
LIMITED TO ONE OR
MORE ZONES
NIGERIA ,
2011, ½ 2012 2011/2012 – O, A
4, 1 OCT/NOV 2012/A, O
4 DISEASE PRESENT
SAO TOME PRINCIPE,
NO SUBM. REPORTS NO DATA AVAILABLE
SENEGAL, 2011 2011/2012 – O, A, SAT 24, 1
NO PRECISE DATA,
DEC 20111
DISEASE PRESENT
SIERRA LEONE, 2011 2011, 2012 – ABSENT1 OCT 1958
1
NOT REPORTED IN THIS
PERIOD

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 85
TOGO, 2011 2011, 2012 – O, SAT 11, 4, 1
FEB 20124 DISEASE PRESENT
P O O L 6
SOUTHERN AFRICA
Botswana5 – SAT 2 serotype, topotype III, was detected in 21 samples submitted to WRL. Samples were
collected during May – August 2012 from Matsebe Crush, Spanplek crush, and Nokaneng all within Zone 2
where vaccination is practiced.
Swaziland and Lesotho are free from FMD without vaccination.
Also, there is a zone in both Botswana and Namibia which is
FMD free without, since 2010 and 1997 respectively (Map 9).
FMD history in past 2 years is given in Table 10.
Map 9: FMD distribution by serotypes 2010 – 2012
Table 10: Pool 6 FMD history 2010-2012
COUNTRY FMD HISTORY (past 2 years) LAST OUTBREAK
REPORTED/TYPE OIE FMD STATUS
ANGOLA,
NO SUBM. REPORTS NO REPORTED OUTBREAKS DEC. 2010/ SAT 2
1 UNKNOWN
BOTSWANA, 2011 2011 – SAT 2
5 SAT 2
1
2012 – SAT 21
OCT 2012/ SAT 21
FMD FREE ZONE WHERE
VACCINATION IS NOT
PRACTISED
CONGO D. R. , 2011 2011, 2012 O, A, SAT 14 2011/2012
9, NO PRECISE
DATA
LIMITED TO ONE OR
MORE ZONES
MALAWI, 2011 2011 – SAT 21 OCT 2011
1 DISEASE PRESENT

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 86
MOZAMBIQUE, 2011 2011 – SAT 21 JUN 2011/SAT 2
1 DISEASE PRESENT
NAMIBIA, 2011 2011 – SAT 1
1
2012 – SAT 11
JAN 2012/SAT 11
FMD FREE ZONE WHERE
VACCINATION IS NOT
PRACTISED
SOUTH AFRICA, 2011
2011 – SAT 11
SAT 21
2012 – SAT 21
APR 2012/SAT 21 DISEASE PRESENT
ZAMBIA, 2011 2012 – SAT 21 JAN 2012/SAT 2
1 DISEASE PRESENT
ZIMBABWE, 2011 2011 – SAT 2
1
2012/NOT TYPED12
2012/NOT TYPED
12 DISEASE PRESENT
P O O L 7
SOUTH AMERICA
Most South America countries are FMD free with
(Uruguay)/without (Chile, Guyana) vaccination or
with free zones with/without vaccination. Small
areas of the continent are considered as endemic
but clinical cases are rare (Map 10).
FMD history in past 2 years is given in Table 11.
Map 10: FMD distribution by serotypes 2010 – 2012

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 87
Table 11: Pool 7 FMD history 2010-2012
COUNTRY FMD HISTORY (past 2
years) LAST REPORTED/TYPE
COUNTRY FMD
STATUS1
CONTROL
MEASURES
ECUADOR,
2011, ½ 2012 2011 – O
1 AUG 2011/O
1
2011 – DISEASE
PRESENT, 2012 –
NOT REPORTED
ROUTINE
VACCINATION -
CATTLE
PARAGUAY, 2011 2011 – O1 DEC 2011/O
1
½ 2011 – NOT
REPORTED, 2/22011
- LIMITED TO ONE
OR MORE ZONES
ROUTINE
VACCINATION –
CATTLE,
BUFFALOES
VENEZUELA,
NO SUBM.
REPORTS
2011 – O8
A8
2011/O, A8 UNKNOWN
The key to the superscripts is below:
1. WAHID Interface – OIE World Animal Health Information Database http://web.oie.int/wahis/public.php?page=home 2. Reports from FAO/EuFMD projects and field officers 3. Dr. Esther TO: Foot and Mouth Disease Hong Kong Situation, Update; Animal Management Division Agriculture, Fisheries and Conservation Department, 10 August 2012 4. FAO/EuFMD supported FMD networks (RESOLAB-FMD West Africa) 5. World Reference Laboratory for Foot-and-Mouth Disease (WRLFMD), www.wrlfmd.org 6. Conference on Scientific Developments and Technical Challenges in the Progressive Control of FMD in South Asia, New Delhi, India, 13-15 February 2012. 7. FAO/EuFMD supported FMD networks (EARLN-FMD Eastern Africa) 8. SENASA, Argentina 9. SEAFMD 10. Open session of the EuFMD, Jerez de la Frontera, Spain. 29-31 October 2012. 11. Ministry of Agriculture Animal Industry and Fisheries. National Animal Disease Diagnostics and Epidemiology Centre (NADDEC) P.o. BOX 513, Entebbe, Uganda 12. Dr C Njagu (Division of Veterinary Field Services): Current status of the livestock sector in Zimbabwe, ACWG MEETING OF 31STMAY 2012 13. Pakistan – FMD Bulletin, Vol 1 (1-2), January-June, 2012 14. Laboratorie veterinarie de Goma, DRC 15. C. Bellet, T. Vergne, V. Grosbois, D. Holl, F. Roger, F. Goutard (2012) Evaluating the efficiency of participatory epidemiology to estimate the incidence and impacts of foot-and-mouth disease among livestock owners in Cambodia, Acta Tropica 123 (2012) 31– 38

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 88

85th Executive Committee meeting of the EuFMD, Chania, Crete, 14-15 February 2013 89
THE EUFMD TEAM
Keith Sumption EuFMD Secretary Eoin Ryan Animal Health Officer Nadia Rumich Communications Officer Gregorio Torres Training Support Officer Vesna Milicevic Short term professional officer Dimitrios Dilaveris Short term professional officer Rossana Cecchi Office manager
Rachel Blasi Clerk Leonardo Leon Clerk Manuela Zingales Temporary assistant Melissa Mclaws EuFMD consultant Chris Bartels EuFMD consultant Kees van Maanem EuFMD consultant Carsten Potzsch EuFMD consultant
As well as the SCR, the STC, Naci
Bulut, Theo KnightJones, Nick Lyons, Nick Honhold, Phil
Watson, TCC consultants, Iran
consultants…