Embed Size (px)
Citation preview

Cancer Treatment Reviews (1979) 6, 107-124
Etoposide (VP-16-213)
B r i a n F. I s s eH a n d S tan l ey T. C r o o k e
Department of Clinical Cancer Research, Bristol Laboratories, Syracuse, New ~'ork 13201, U.S.A.
I n t r o d u c t i o n
Etoposide or VP-16-213 is a semi-synthetic derivative of podophyllotoxin, a natural product extracted from certain plants of the genus Podophyllura (42). Etoposide has been extensively studied in National Cancer Institute (NCI) sponsored clinical trials but it still r emains an investigational agent. A review comparing this compound with its congener V M - 2 6 was written in 1976 (61). However, since then the results of many studies have been published. The purpose of this paper is to update and analyze the available data on etoposide wi th a view to demonstrating its clinical usefulness and optimal method of administration in adult and pediatric oncology.
H i s t o r y
The American Indians and the natives of the Himalayan mountain area independently discovered and used for medicinal purposes the aqueous extracts of the plants Podo- phyllum peltatum and Podophyllum embodi respectively, hundreds Of years ago (43). The extract termed podophyll in was used as a cathartic and anthelmintic. Subsequently the American colonists used podophyllin extracted from: the dried roots and rhizomes of Podophyllum peltatum (also known as the May apple or American mandrake) as an emetic and it was inc luded in the First U.S. Pharmacopoeia (U .S .P . 1820). PodophyUin remained i n the U.S.P. until 1942 when it was removed because of its severe toxicity. Kaplan (41) in i942 reported that podophyllin in oil when applied topically selectively destroyed the venereal war t , condyloma accuminatum and in 1946 the antimitotic properties of podophyllin Were demonstrated (44).
The chemical analysis of podophyllin revealed a number of compounds including podophyllotoxi.n. Although possessing ant i tumor properties they were unacceptable for human usebecause toxicity prevented the i r administration in h i g h enough dosage to give significant clinical activity (35, 46). Since 1963 Sandoz Laboratories have
Address Reprints to: Brian F; Issell, M.D., Bristol Laboratories P.O. Box 657, Syracuse, New York 1320I, U.S.A. 0305-7372/79/020107+ 18 802.00/0 ~ 1979 Academic Press Inc. (London) Ltd.
107

108 B.F. ISSELL AND S. T. CKOOKE
synthesized various podophyll in derivatives (14, 42, 67). The two most successful of these are teniposide or V M - 2 6 and etoposide or VP-16-213.
C h e m i s t r y
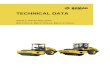
Etoposide is 41 demethyl-epipodophyllotoxin-/~/-D-ethylidene glucoside with a molecular formula of CagHaaOla and molecular weight 588. The structures ofetoposide, its congener teniposide or V M - 2 6 and the natural ly occurring parent compound podophyllotoxin are shown in Figure 1.
OH
H3CO'~'
~ C CH20 oJ
!
OCH 3
OCH3
Podophy l lo tox ln
H
o
(o l | I I It
0 i O
H~CO~OCH;3 H 3 C O ~ O CH 3 OH OH
Tenlposlde ( V M - 2 6 ) Etoposlde ( V M - 16 - 213 )
Figure 1. Structural formula ofpodophyllotoxin and its synflletic derlvativ~ teniposide and etoposide.
In a structure-activity relationship stud>-, Loike and Horwitz (48) tested the ability of various etoposide a n d podophyllotoxin congeners to cleave cellular DNA. They found that a n hydroxyl grouP a t the C ~ 1 position is required for activity and t h a t the configuration oft_he C-4 carbon inf luencesthe activity of a congener.
Etoposide is poorly so luble in water and is supplied for clinical use invials containing

ETOPOSIDE (VP-16-2 I3) 109
I00 mg etoposide, 400 mg Tween 80, 3.25 g polyethylene glycol 300, 10 nag anhydrous citric ac id and absolute alcohol to 5 m l . Desp i t e this complex formulation etoposide is physically unstable in dextrose solutions and should be diluted with sodium chloride injection, USP.
M e c h a n i s m o f a c t i o n
Etoposide when added to chick fibroblast tissue cultures initially causes metaphase arrest, a n effect similar to the spindle poison colchicine and the parent compound podophyllotoxin. However , after 30-60 min two different dose dependent effects are seen. At concentrations of 10 mg]mI or greater, lysis of cells entering mitosis is observed while at concentrations less than 10 mg/ml, cells are prevented from entering mitosis. These effects which are irreversible after drug exposure for 2 h, suggest that etoposide acts in the cell cycle at or before the initiation of mitosis and differentiates this compound from the classical spindle poisons (64). Also supporting this difference is the observation that etoposide does not interfere with microtub~t.qe assembly and it has been postulated that these differences are related to the presence of the glucoside moiety in etoposide (47). Further data suggest ing etoposide has a diffC¢.'ent site of action to the spindle poisons, e.g. vinca alkaloids, have been derived from observing the effect of etoposide on the incorporation of tri t iated thymidine, uridine and leucine in P-815 mastocytoma tissue culture cells (62). Inhibi t ion of thymidine uptake only was observed suggesting inhibit ion of DNA synthesis with no effect on R N A or protein synthesis. However , in H e L a tissue culture cells, inhibit ion ofur idine and to a lesser extent leucine incorporation were found in addi t ion to a reduction in thymidine uptake suggesting that the drug exerted effects on DNA, I~NA and protein syntheses in this human tumor in tissue cu l tu re (47)' In contrast, vincristine, for example, causes inhibition of R N A synthesis through effects of DNA,dependent R N A polymerase (17, 49).
Loike and Horwitz (48) studied the intracellular degradation of DNA in HeLa cells by following the sedimentation profiles of radioactive DNA on alkaline sucrose gradients. Thei r results suggested that etoposide induced single strand DNA breaks.
Cytoflurometric studies have demonstrated that etoposide is cell cycle dependent and phase specific. I n two separate studies using h u m a n lymphoblastic cell lines, the major delay of cell cycle progression and the max imum cell killing, occurred in the S and 82 phases (24, 45).
P r e c l i n i c a l a c t i v i t y
Etoposide was found to be active against the Walker carcinosarcoma in the rat, the Ehrlich ascites sarcoma 37 and 180, and a variety of routine leukemias including L 1210 (20, 26, 64). In addition etoposide activity was detected in the mouse ependymoblastoma system (33).
Marked schedule dependency was demonstrated in the L1210 system. Trea tment intervals o f 2-4 days were superior to dai ly: t reatment for 5 days, t reatment a t 6-8 day intervals, o r t r ea tmen t O n Day 1 alone. Divided t reatments 'every 3 h for 24 h demon- s t ra ted significant super ior i ty over single t rea tments o n tha t day. Etoposide was found to be active by oral administrat ion w h e n given to L1210 bearing mice (64).

I I0 B.F. ISSELL AND S. T. CROOKE
Rivera et al. (60) reported synergism between etoposide and cytonirte arabinoside while Dombernowsky and Nissen (22) reported etoposide synergism with cyclophos- phamide and B C N U in LI210 leukemia.
Precl lnical toxicology
There were difficulties evaluating the acute toxicity of intravenously administered etoposide due to the inherent toxicity of the solvent system (62). The dose, of solvent plus drug, lethal to 50% of animals (LD60), approached that of the solvent alone in mouse, ra t and rabbit species.
Subacute toxicity studies were carried out in monkeys (62). Doses of 0.4, 1.2 and 3.6 mg/kg/day were given i.v. for 4 weeks with a control group receiving solvent alone. The higher doses caused progressive lymphoid and hematologic toxicity. The highest dose produced severe anemia, leukopenia and agranuloeytosis al though no animal died. At this dose pathological abnormalities of the liver and gastrointestinal t ract were also observed.
Pharmacokinet i c s
In the ra t (62), the t~ ~ of tritium-labeled etoposide was found t o range between 28 and 43 rain and the t~ fl was 102 to 128 rain. The drug was shown to be excreted pre- dominant ly in the bile. Concentrations of the compound higher t h a n in the blood were found in the intestine, liver and kidneys, as well as thyroid, adrenals and thymus. For the first three organs this can b e at tr ibuted to the mode of excretion, with the intestinal wall reflecting bile Contents. The lung, stomach, skin and pancreas had drug levels similar to blood, while the brain took u p only low levels of the drug.
Creaven and Al l en (19) investigated the pharmacology of tr i t ium labeled etoposide in nine patients. Four patients received 220 mg/m 2 and five patients received 290 mg/m ~ intravenously as a 1 h infusion. Post-infusion plasma decays were biphasic. The mean terminal ha l f life (t~fl) was nearly I 1.5 h. AlSo unlike the rat, after 72 h, 44% of adminis- tered drug was recovered i n the ~ urine with 2 9 % as unchanged drug and 15% as metabolites. Recovery i n t h e feces ranged from less than 2 to 1 6 % over 3 days. Levels in the cerebrospinal fluid varied from less than 1 to 10~/o of the plasma levels at 2-26 h post infusion. Approximately 74% of the drug was shown to be bound to human serum protein at etoposide concentrations of I0 /~ . /ml (62).
CHnlcal m a x i m u m tolerated doses
Intravenous monotherapy
Nissen et aL (53). performed the initial Phase I studies. They found the maximum tolerated:dose (NfTD) to b e 45 mg/m 2 i r t a d a i l y intravenous schedule for 7 days and 69-86 mg/rrt 2 o n twice weekly schedule fo r 3 weeks.
The M T D Of et0poside~ acc0rding::to the different schedules of administrat ion deter- mined in qater studJes is summarized in Table I. When etoposide was given intra- venously dMIy for: 5 days followed by a 2 w e e k res t cycle i n the : E O R T C study (31) only

ETOPOSIDE (VP-16-213) 111
9 of the 250 cases had severe toxicity and 114 showed no signs of any toxicity. Doses of 60 mg/m ~ daily for 5 days repeated every 3 weeks were considered safe and effective in patients with good bone marrow reserve. Tucker et al. (66) in a Phase I I study found that patients tolerated doses of 60 mg/m2.daily for 5 days intravenously plus 100 mg capsules of etoposide which were administered thrice weekly between the intravenous doses. Etoposide has also been administered by weekly intravenous schedules in which doses of 200--250 mg/m 2 have been tolerated (9, 15) and on Day 1, 3 and 5 every 5 weeks where a dose of 125-140 mg/m 2 was tolerated (26).
Table 1. M a x i m u m to lerated d o s e s (MTD) o f i.v. e t o p o s i d e a c c o r d i n g to s c h e d u l e o f a d m i n i s t r a t i o n
MTD Interval between Total :1o. Dose limiting (mg/m2/day) Schedule courses patients toxicity Reference
60 Day i-5 21 days 250 Leukopenia (53) 60 Day 1-5 14 days 47 Leukopenia (66)
(Plus 100 mg capsules twice weekly p.o.) 200-250 Day 1 7 days 36 Leukopenia (9, 15) 125-140 Day 1, 3, 5 28 days 13 Leukopenia (26)
Oral monotherapy
After etoposide was given orally to 30 patients in a Phase I trial, Nissen et al. (55) recommended a dose of 120 mg/m ~ daily for 5 days with further dose escalation de- pending on toxicity in previously untreated patients. Jungi and Senn (40) using etoposide at doses of 60 mg/m 2 daily for 5 days intravenously and 120 mg/m 2 by the same schedule orally found equivalent satisfactoa3r patient tolerance for both regimens. Hansen et aL (37) found etoposide was tolerated at approximate ly 130 mg/m 2 orally for 5 days repeated every 3 weeks in previously untreated patients and for 4 days in patients who had received prior chemotherapy. After comparing the biologic activity of etoposide given either intravenously or orally, Brunner et al. (7) also found that the oral dose should equal approximately twice the intravenous dose.
Combination therapy Eagan et al. (27) have used etoposide at a dose of 70--75 mg/m 2 on Days 1, 3 and 5 combined with either doxorubicin 40-45 mg/m ~ on D a y 1 or cyclophosphamide 600- 675 mg]m ~ on Day 1 in 4-5 week cycles. As would be ant ic ipa ted at these low doses only mild hematologic toxicities were encountered. Aisner et al. (3) used mor e aggressive therapy administered on a 21 day cycle. This consisted ofetoposide 50 mg/m 2 given on Days 1-5, doxorubicin 45 m g / m ~ given on Day 1 and cyclophosphamide 1000 mg/m ~ given on Day 1. Moderately severe toxicity was encountered especially in patient s with prior radiotherapy. Myelosuppression eventually required some dosage modification in every case but tl~is was not usually necessary until far into therapy. Almost all patients were able to receive their therapy as out-patlents.
C l in i ca l t o x i c i t i e s Hematologic Leukopenia was t h e m a j o r dose limiting toxicity encounte red with etoposide adminis- tration. Thrombocytopenia was also observed but was less frequent. Cumulat ive myelo- suppression has no t been reported. The degree of Ieukopenia and thrombocytopenia

112 B.F. ISSELL AND S. T. CROOKE
encountered after etoposide was given at a dose of 60 mg/m ~ daily for 5 days intravenously or 120 mg/m 2 orally by the same schedule is shown in Table 2. The majority of these patients had received extensive prior therapy.
Table 2. P ropor t ion of pat ients wi th mye losuppress ion following e i ther o r a l o r in t ravenous VP-16 a t equivalent d o s e s
Patients with Patients with Dosage daily for Total leukocyte platelet
5 days (reference) patients nadir < 2000hLl nadir < 50,000/tM
50 mg/m s i.v. (38) 28 7 (25%) 1 (4%) 120regime-p.o. 19 3 (16~/o) 2 (11%)
~ I / l / ! l l l [ ~ l l l ~ I I I ~ ~ I 1 ~ 1 I IIIIIIIIII i i i i i I D U l II ~ ~ ! J i l l IIII I I I I I I I 1 [
Gastrointestinal Nauseaj vomiting and infrequently diarrhea were the major gastrointestinal toxicities, When etoposlde was given either at a dose of 60 nag/m s intravenously or 120 mg]m 2 orally on Days 1-5, 35-42~g of 66 evaluable patients experienced some degree of gastro- intestinal toxicity (37, 40). In tile study of Tucker et al. (66) in which etoposide was given intravenously at 60 mg/mZ/day i.v. for 5 days and I00 nag capsules of etoposide were also given twice weekly between the intravenous courses, nausea was reported to have occurred transiently in 12 of 47 patients (26%), but was easily controlled with supportive antiemetic therapy. Anorexia has also been reported to accompany etoposide therapy (40).
Alopeda
Reversible alopeeia is a common finding after etoposide therapy. In two studies where etoposide was gb,-en either at 60 mg/m ~ i.v. or 120 rag/m-* orally on Days I -5 (35, 41) 35 and 90~/o of patients respectively experienced alopecia. Sometimes complete baldness resulted.
Acute reactions
Acute toxicities, which have been documented, include fever (31, 66), chills (40) and hypotension (18) but these reactions are rare. The rapid infusion of etoposide has been reported to cause hypotension which was subsequently prevented by slowing the infusion rate (15). Severe wheezing and bronch0spasm which responded promptly to cessation of etoposide infiasion and administration of antihistamines have been reported during the U.S.A. clinical trials (70).
.~ducositis
Stomatitis has been reported uncommonly after the oral administration of etoposide (7, 32, 37).
Monotherapy activity
In the ini t iaiPhase I study Nissen etal. (53) noted 8 partial remissions i n 3 3 patients with measurable tumor; Thislincluded :3, of :5 responses ~in patients w i t h H0dgkin's disease, 4 6 f 13:in patients: with o ther malignant lymphomas, 1,of3 patients with car- cinoma Of the esophagus and I of 4 patients with carcinoma ofdae stomach.

ETOPOSIDE (VP-1G-213) 113
T h e c u m u l a t i v e response ra tes for e topos ide as a single a g e n t in s u b s e q u e n t s tudies r e p o r t e d u p to m i d 1978 a re s h o w n in T a b l e 3. W h e n cons ide r ing these responses i t is i m p o r t a n t to n o t e tha t t h e y a r e c o m p i l e d f rom studies u t i l i z ing va r ious doses a n d schedu les o f e topos ide , some o f w h i c h m a y n o t h a v e been o p t i m a l . D a t a ava i lab le p r io r to m i d - 1 9 7 6 h a v e previous ly b e e n r e v i e w e d b y Rosencwe ig et al. (61).
Table 3, Cumulative activity o f etoposide monotherapy according to tumor type
Number cvaluable Number %
Tumor type patients respondcrs responders Refercnce~
Small cell lung 205 88 43 9, 15, 26, 3I, 32, 37, 40, 55, 66
I-Iistiocytic lymphoma 85 26 31 13, 3 I, 32, 39, 50 Lymphocytic and mixed lymphoma 31 3 10 13, 31, 50 I-Iodgkins disease 48 8 17 13, 31, 50 Acute non-lymphocytic leukemia 157 36 23 4, 5, 1 I, 31, 36,
63, 68 Acute lymphoblastic leukemia 30 2 7 5, 31, 36, 50 Won small cell lung 53 5 9 28, 32 Breast 99 5 5 1, 29, 31, 32, 55 Bladder 9 I 11 31, 32 Ovary 40 1 3 30, 31, 32, 40 Testis 20 4 20 10, 31, 52 I-Iepatoma 6 3 50 I0 Colorectal 78 1 1 23, "55, 58 Mdanoma 58 0 0 2, 13 Head and neck 32 0 0 31 Brain 2 0 0 31
i , . i . . i . i . . , _ , , , j , , , , , i i H , , , ,
(Responders = Patients with ~ 505/o measured tumor regression)
O p t i m a l r o u t e a n d s c h e d u l e o f c l i n i c a l a d m i n i s t r a t i o n
As sugges t ed f r o m its t e rmina l half-l ife o f a p p r o x i m a t e l y l l . 5 h (19), its cell cycle d e p e n d e n c y (24), a n d its p rec l in ica l schedu le s tudies (20) e topos ide a p p e a r s to be m o r e ac t ive w h e n g iven in d iv ided dosage ove r several days t h a n b y a s ingle dose. T h e response ra tes in smal l cell l u n g cancer a c c o r d i n g to t he di f ferent schedules a n d rou tes o f admin i s - t r a t i o n a re s h o w n in T a b l e 4. O f the s chedu l e s used in t h e t r e a t m e n t o f smal l cell l ung c a n c e r those us ing r e p e a t e d a d m i n i s t r a t i o n for 3 o r 5 days, a p p e a r to be a m o n g t h e m o s t act ive. H o w e v e r , one m u s t c a u t i o n a d i rec t c o m p a r i s o n o f response rates b e t w e e n s tud ies W i t h o u t cons ide ra t ion o f t h e p r o p o r t i o n o f pa t i en t s in each s t u d y w h o h a d r e c e i v e d p r i o r t h e r a p y , w h o h a d extensive disease a n d w h o h a d a p o o r p e r f o r m a n c e s ta tus . N 0 n e - t h e - l e s s in these s tudies the d i f ferences be tween responses a re un l ike ly to be Solely d u e to differences in p a t i e n t charac ter i s t ics a n d p r o b a b l y r ep re sen t d r u g s c h e d u l i n g effects.
W h e n a specific schedule is cons ide red there is n o e v i d e n c e sugges t ing super io r ac t iv i ty for e i the r the oral or i n t r a v e n o u s r o u t e o f admln i s t r a t i on . Caval l i et al. (9) r e p o r t e d a r a n d o m i z e d s t u d y in w h i c h e topos id e g i v e n ora l ly e i ther b y a 5 d a y s c h e d u l e eve r y 3 w e e l ~ : o r a 3 d a y schedule eve ry week was found to lbe s igni f icant ly supe r io r to a week ly i n t r a v e n o u s schedule . T h e infer ior i ty o f the single d a y i . v . dosage mos t l ikely

114 B.F. ISSELL AND S. T. CIROOKE
represents a schedule r a t h e r t han a rou t e of admin i s t r a t i on difference. I n the oral schedules the d r u g was given in d iv ided dosage 3 t imes da i ly e i the r for 3 or for 5 days. T h e a p p a r e n t super ior i ty of the 3 d a y eve ry week schedule over the 5 d a y every 3 week schedule (Tab le 4) was exp la ined by the au thors as possibly d u e to a h ighe r m e a n total e toposide dosage b y the fo rmer schedu le (9).
Tab le 4. Response r a t e a c c o r d i n g to r o u t e and schedule o f e topos ide a d m i n i s t r a t i o n in s m a l l cell lung c a n c e r
Interval Total Investigator Dose between number Number of (reference) (mglm~/day) i.v./p.o. Schedule courses patients responders
Tucker et al. (1978) 60 i.v. Days 1-5 14 days 47 24 (51%) (66) (Plus 1120 nag capsules twice weekly p.o.)
Jungi and Senn (1975) 60 or 120 i.v. Days 1-5 2I days 16 5 (3I%) (4o) p.o.
Hansen eta/. (1977) (37) 130 p.o. Days I-4 or 5 21 days 40 20 (50%)
Cavalli et al. (1978) (9)
Schedule A 250 i.v. Day 1 7 days 20 4 (20%) Schedule B 166 p.o. Days 1-3 7 days 17 11 (65%) Schedule C 283 p.o. Days 1-5 21 days 19 8 (42%)
Cohen et al. (1977) (15) 200 i.v. Day 1 7 days 16 4 (25%)
Eagan el at. (1976) (26) 125-140 i.v. Days 1, 3, 5 28 days 16 7 (44%)
Overall 191 83 (43%)
(Responders = patients with ~ 50% measured tumor regression)
Activity in specific t u m o r s
Smal l cell lung
Monotherapy
T h e ma jo r i t y of d a t a ava i lab le on e toposide has b e e n o b t a i n e d in small cell b roncho- genie c a r c i n o m a agains t w h i c h e t o p o s i d e appears to be one o f the mos t act ive drugs tes ted t o d a t e . T h e response ra tes for e toposide as a single a g e n t in this d isease are s u m m a r i z e d in T a b l e 4. W h e n d a t a a r e eva lua t ed f rom those studies w h e r e > 1 0 pat ients wi th small ceil lung cance r a r e eva luab le 4 3 % of 191 pat ients eva lua ted ach ieved at least a par t ia l response w h e n t r ea ted wi th etoposide as a single agent .
T u c k e r et aL (66) t rea ted 47 small cell l ung cance r pa t ients wi th e toposide a t 6 0 m g / m ~ da i ly f o r 5 days admin i s t e red every 2 weeks plus oral doses o f 100 nag admin i s t e red twice weekly b e t w e e n the in t ravenous doses. N i n e t e e n pat ients h a d extensive disease a n d 2 6 h a d r e c e i v e d e i ther p r ior c h e m o t h e r a p y o r r a d i o t h e r a p y . T w e n t y . f o u r (51 °/o) o f t h e 4 7 pa t ien ts ach ieved a par t ia l r emiss ion . T h e overa l l m e d i a n surv iva l for the s tudy f rom t h e first d a y i o f t he rapy Was 225 days.
C a v a l l i et a L (9) compared : 31 dose schedules o f e t o p o s i d e in 60 pat ients wi th small cell l ung cancer , 45 of w h o m were previous ly un t r ea t ed . T h e 3 dose schedules were :

ETOPOSIDE (VP-16-213) 115
(a) 250 mg/m a i.v. weekly, (b) 500 mg/m °" p.o. in divided doses over 3 days every week, and (c) 850 mg/m a p.o. in divided doses over 5 days every 2-3 weeks. Oral etoposide was supplied as drink ampules. Response rates for the three regimens were 20%, 65% and 42% respectively 1n a total of 56 evaluable patients.
Eagan el al. (26) carried out a randomized study comparing etoposide alone, given i.v. a t the dose of 125-140 mg/m ~ on Days I, 3 and 5 every 4-5 weeks, to the combination of v incr i s t ine+methot rexa te+cyc lophosphamide or v inc r i s t ine+b leomyc in+adr i a - mycin. All patients had extensive disease. Thir teen patients received etoposide as their initial chemotherapy, and three others had received prior therapy. Seven patients, all of w h o m were previously untreated, achieved a partial response making the total response rate 44%. The median survival of the etoposide patients was 229 days (range 77 -515+ days). The presence of brain metastases did not adversely affect survival.
Hansen el aL (37) have evaluated etoposide given as an oral solution (drinking ampule) in 4 0 patients, 10 of whom, all older than 70 years, had not received prior chemotherapy. Patients received I00 rag twice a day (approximately 130 mg/ma/day) for 4 days i f previously treated and for 5 days if previously untreated. Courses were repeated every 3 weeks, and treatment continued until disease progression. A total of 20 patients (50%) achieved a partial response. No difference in response rate was observed between previously treated and untreated patients.
Cohen et al. (15) reported a study of etoposide administered i.v. weekly in previously treated small cell l u n g carcinoma patients. The dose used was 200 mg/m~/week. O f 16 patients evaluated, 4 achieved a partial remission and an additional 9 had stabilization of their disease.
Jungi and Senn (40) reported 5 of 16 responses after two courses of therapy when etoposide was given at a dose of 60 mg/m2/day for 5 days every 2 weeks, followed by etoposide p.o. 60-120 mg/m~/day for 5 days every 3 weeks.
Combination therapy
Due to its h igh activity as a single agent, etoposide has been evaluated in combination with other agents in small cell bronehogenic carcinoma. These studies are summarized in Table 5.
Aisner et al. (3) reported on the use of etoposide, doxorubicin and cyclophosphamide with or without methanol extracted residue of BCG (MER). Each course of chemo- therapy was given every 3 weeks and consisted of etoposide 50 mg]m2/day Day 1-5, doxorubicin 45 mg]m 2 Day 1 and eyclophosphamide !000 mg/m 2 Day 1. O f 27 evaluable patients with measurable .disease, 11 achieved a complete response, 10 a partial response and 3 an objective improvement, f o r a n overall response rate of 89%. All 22 evaluable patients w h o had n o prior t reatment responded. Although the median survival for patients had not been reached at the time of the report the projected median survival for patients with Extensive disease exceeded 30 weeks. The addition of M E R did not appear to affect response and survival at the time of evaluation.
Tenezynski et aL (65) treated 22 small cell lung cancer patients with etoposide (75 mg/m2/day i.v. D a y 1,3), doxorubicin (50 mg/m ~ i.v. Day 1) Ifosfamide 1000 mg/ m2/day Day 1-5) vlncristine (2 nag i.v. D a y I) a n d C . parvum. Therapy was repeated every 3 weeks. N i n e t y per cent of the 22 pa t ien ts treated achieved > 5 0 % measured tumor reduction, and .ha l f of the responders were complete. The median survival time for all patients was in excess of 10.5 months.

Tab
le #
. Eto
posi
de in
com
b|tr
ot|o
n st
udie
s fo
r sm
~ c
ell l
ung
canc
er
' I
......
....
i ot
a N
umbe
r ..
....
. M
cd a
n In
v~tig
ator
e~
aiua
blt:
~tc
miv
e Nu
mber
Num~
%
~ su
rviv
al
(ref
exen
ce)
The
rapy
pa
tien
ts
dise
ase
CR
PR
P
R+
CR
C
R
(mon
ths.
)
Ais
n~ a
~.
(|977
) de
50
mgl
m~l
day D
ay 1
~ i
x.
27
1 !
10
78
41
7+
(3)
Dox
or~t
bick
q 45
mg/
m t
Day
1
|de
10@
3 mg/
m ~ ~
y
l Lv.
+]
-MB
R ir
mzm
~oth
erap
y T
encz
ymki
a d
. (1
978)
75
D
ay I
-3 i.
v.
22
10
10
10
~ 45
10
.5+
(651
ic
in 5
0 ra
g/m
* D
ay i
i.v
. If
osfa
mid
c 10C
,) mg/
m ~ D
ay 1
-5 L
v.
Vin
c~,s
tisc 2
.0 n
ag D
ay I
i.v.
C
. Pw
~'um
ir:a
mun
o~ap
y E
t 13
0 y
Day
8,
!5 i.
v.
14
Proc
a6ba
zine
60
Day
i-1
0 i.v
. ~n
35 mg
/m ~
Day
1
Et
70-7
5 m
D
ay 1
, 3, 5
i.v.
12
~p
ham
ide 600-675 m
g~'n ~ D
ay l
70-7
5 D
ay !
, 3, 5
i.v.
10
ci
~ 40
~5 m
g/m
~ Day
I
Ero
s|d
e 2
~ r
ag/d
ay D
ay l-
$ p.
o.
11
Vhlcrlx~e 0.02 mg
,~g w~ly LV.
t¢ 0
35
wee
kly i
a.
am|d
e 2.0
m#g
i'day
~il
y p.
o.
E.'~
der a
~.
(197
8)
6 6
7 93
43
~n
a ~.
(19
~7)
1 5
50
8 m
east
lred a
fi~
I ~m
~e
(27)
0
2 20
0
m~
ed
afi~
I c
ours
e C
aval
li a
~. (1977)
0 6
56
0
~:~::~:~--':~
:::-
7
:~/"-~: -
/";;~-;-7%:-~:; ......... : ~:~:-::.
~
~,,/~:~,
::~:,:~:::J'~""
:~:;::~-~
-~
¸~¸
~:::::~
;
;
~;
~7:~::'/7::~::::~''--
;:::~:
"~:
":~;~:;/~:~;:~::
~'":'~:'~
~;;
~"'~
~:
::~:: :~:::°"~:':'~
::
:̧̧
::~;~::v~-7
;;;;~:
:;~:-";~;;"--;:~-
(CR
=eo
mpl
etc
r~m
e;
PP. ~
par
tial r
~sp
o~, L
e., >
~3%
m~
ured
tum
or r
~n
)
>
U
0
0 0

ETOPOSIDE (VP-I 6-213) I 17
Broder el aL (6) carried out a randomized study comparing a combination of cyclo- phosphamide, vincristine, methotrexate and lomustine (COMC) to a regimen abbre- viated APE which consisted of etoposide (130 rag/m"- i.v. Day 8-15) procarbazine (60 mg/m ~ p.o. Day 1-10) and doxorubicin (35 mg/m 2 i.v. Day 1) with courses repeated every 3 weeks. A fixed crossover to the al ternate regimen occurred a t 3 months. In patients with regional disease, radiotherapy was given to the p r imary tumor by a split course technique to a total dose of 5150 tad. Responses were evaluated prior to radio- therapy. The APE combinat ion was given to 8 patients with regional disease, and 4 complete and 3 part ial responses resulted. In 6 patients with extensive disease there were 2 complete and 3 part ial responses. This compared to 4 complete and 3 par t ia l responses in 9 regional disease patients and 1 complete and 4 part ia l responses in 6 extensive disease patients treated with C O M C . O f 5 patients who h a d received C O M C as pr imary chemotherapy, 4 responded to APE, indicating lack of cross resistance. The projected median survival had not been reached after 12 months of follow-up.
Eagan el al. (27) compared etoposide at a dose of 70-75 mg/m 2 on Day 1, 3 and 5 every month either combined with cyclophosphamide (600-675 mg/m 2 i.v. Day 1 monthly) or doxorubicin (40-45 mg/m s i.v. Day 1 monthly). A third group of patients received the combination of cyclophosphamide, doxorubicin and cisplatin. Dur ing the second and thi rd cycle of chemotherapy, radiotherapy was also given. Twelve patients were randomized to receive etoposide and cyclophosphamide and I0 patients to receive etoposide and doxorubicin. After one course of therapy there were 1 complete and 5 partial responders in the etoposide and cyclophosphamide group and 2 part ial responders in the etoposide and doxorubicin group. After completion of the radio therapy there were 4 complete and 2 partial responders in the etoposide and cyclophosphamide group and in the group receiving etoposide and doxorubicin there were 3 complete and 1 partial responders.
Cavalli et aL (12) treated 11 small cell lung cancer patients with a combination con, taining etoposide (200 rag/day Day 1-3 p.o. every week for a total of 8 weeks), vincristine (0.02 mg[kg[week i.v. for a total of 8 weeks), methotrexate (0.75 mg/kg/week i.v. for a total of 8 weeks) and cyclophosphamide (2.0 mg/kg/day p.o. for a total of 8 weeks). They reported that 6 of the 11 patients treated achieved a partial response.
Other encouraging studies where etoposide has been used in the consolidation and maintenance phase of therapy and where the role of etoposide is more difficult to evaluate include those reported by Oldham etaL (57) and Cohen et al. (16).
Lymphomas
As suggested by the initial Phase I study of Nissen et aL (53) etoposide is clearly active in mal ignant lymphoma and Hodgkin 's disease. The results of studies using etoposide monotherapy are summarized in Table 6. The cumulative response rates are 17% in 48 patients with Hodgkin 's disease, 31 ~o in 85 patients with histlocytic lymphoma and 1 0 % i n 31 patients with lymphocytic or mixed lymphoma. Although only occasional complete responses were noted and the durat ion of response was generally short (<~ 6 months), die majori ty of patients had failed extensive prior chemotherapy.
Despite its activity as a single agent in lymphoma there has been very little evaluation of etoposide containing chemotherapy combinations in this disease. O 'Connel l et al. (56) reported on the combination of etoposide (80 mg/m 9 i.v. on Day 1 and 2), doxo- rubieln (30 or 45 mg/m ~ Day 3) and prednisone (100 mg/m e p.o. Day 3-7). O f 15

118 B.F. ISSELL AND S. T. CROOKE
pat ients previously t rea ted wi th c h e m o t h e r a p y and /o r r ad io the r apy , w h o were en te red in to the s tudy, 5 responded .
F u r t h e r studies eva lua t ing the role o f e toposide e i ther as a subst i tute for or in add i t ion to c o m p o u n d s used in c u r r e n t f ront l ine r eg imens for l y m p h o m a seem ind ica ted .
Leukemia
The activity of etoposide monotherapy in acute leukemia is summarized in Table 7. This c o m p o u n d is clearly ac t ive in a c u t e non- lymphoblas t i c l eukemia w h e r e the cumu la - t ive comple t e remission r a t e is 17% i n 157 p re t r ea t ed pat ients . Pat ients wi th myelo- m o n o c y t i c a n d m o n o e y t i e l eukemia have r e s p o n d e d especially well to e toposide a n d it
Table 6. Etoposlde monotherapy l'or l y m p h o m a
Investigator Etoposide (reference) Histology dose and schedule
Total number evaluable Number % patlcnts rcsponders rcspondcrs
Cecil st al. (1978) Hodgkins (I 3) Histiocytic
Lymphocytic or mixed
Jacobs el al . (1975) Histioeytic (39)
Falkson et al. (1975) Histiocytic Math6 el aL (1974) Hodgkins
(50) Histioeytic Lymphocytic
EORTC (1973) Hodgklns
Histiocytic Lymphocytic
~ 1 1 1 _ III iiiiiimm ~ _ ~ i i i i i i I
45 nag/m2/day Day I-5 i.v. 17 3 16 0
60 mg]nat]day Day 1-5 i.v. 19 0 27 17
200 rag/day Day 1-5 p.o. 50 r a g / m S / d a y Day 1-5 i.v.
or 120 nag/m*/day Day 1-5 p.o.
50 nag/mS/day Day I-5 i.v. or 100 nag/mS/day Day I-5 p.o.
7 2
16 2 14 3 4 I
15 3 2] 4 8 2
, ............... ,,,,,,,, ,, ,,t ,,,
18 0
0 63
29
13 21 25
20 19 15
T a b l e 7 , E t o p o s i d e m o n o t h e r a p y i n a c u t e l e u k e m i a = , , , , , , , , , , , , , , , , , , , , , _ ,,,. , , , , , t , , , , , , . . , , , , , , , ,
Total Investigater ]~toposide evaluab]e No. ~o. % (reference) :Leukemia t~uc dose and schedule patients CIL C/t response
Duration CR
(%OR) month
Smith et aJ. (1970) ANLL 50 mg/m~/day Day 1-5 Lv. 20 2 1 15 (63) or 250 mg/m ~ 24 h Infusion
:Mathd et eL (1974) A N L L 50 mg/mZ/day Day 1-5 Lv. 20 7 1 40 (5) or 120 mglrn~day Day 1-5 p.o.
ALL 5 0 0 0 :EORTC (1978) A N L L 50 mg/mZ/day Day 1-5 l.v. 12 4 0 33
(81) or I00 mglm'/day Day 1-5 p.o. ALL 6 0 0 o
Cavall! et ¢d. (1975) ANLL 100-250 mg[rct~/d~y for 3 days 4 1 1 50 (11) each week
Bcrnascont et aI. (1976) ANLL 200 mglday Day 1-5 p.o. 6 3 0 50 (4)
Bleycr et aL(1978) ANLL (Pod) 100-150 mg/m~/day Day 1-5 Lv. 59 5 4 lfi (5)
A L L (Pcd) I I 0 1 9 Hammond (1977) AI~LL (Ped) 125-150 mg[ml/day Day 1-5 Lv. 24 4 Z 25
(86) ALL (Pod) 8 0 1 13
Van Echo (1978) ANLL 200-300 mg/m z by 2 h infusion 12 0 1 8 (68)
(ALL = acute lymphoblastlc l eukcu~ ; A N L L ~= acute non-]ymphoblasUc leukenda; Ped .= pediatric)
(lo)
(o) (s3)
(zs)
(50)
(s)
(tO
(o) (o)
2.5, 8
.°-4

E T O P O S I D E ( V P - 1 6 - 2 1 3 ) 119
has been suggested that this compound may have a specific role in acute leukemia where monocytoid cells have failed to clear with conventional first line therapy (4, 8, 31, 50). Etoposide does not appear to have significant activity in amate lymphoblast ic leukemia where no complete remissions have been observed in 30 accumulated patients. Rivera et al. (59) have also reported responses in 5 children with acute non-lymphoblast ic and acute lymphoblast ic leukemia when treated with etoposide. However, insufficient data were presented to determine re~ponse rates for each type of leukemia. Activity in chronic myelomonocytic leukemia (34) and chronic myeloid leukemia have also been reported (11~ 32).
Encouraged by its activity as a single agent in acute non-lymphoblast ic leukemia several investigators have combined etoposide with other chemotherapeutic agents in the t reatment of this disease. These studies are summarized in Table 8. I t is impossible to evaluate the contribution ofetoposide to these regimens from these data. As expected the major detmwninant of response was whether patients had failed prior chemotherapy. First line therapy studies compar ing the addi t ion of etoposide to cmwent conventional chemotherapy regimens seem indicated.
T a b l e 8. E t o p o s l d e c o n t a i n i n g c o m b i n a t i o n t h e r a p y i n a c u t e n o n - l y m p h o b l a s t l c l e u k e m i a
Total Investigator evaluable ~o. ~'o. % (reference) Therapy patients CR PR CR Comments
$'an :Echo et at. (1978) (68)
Jacobs et al. (1975) (38)
Cavalll a ag. (1975) (s)
Bernasconl et al. (1976) (4)
~Etoposlde 50 mg/mZ/day Day 1-5 | .v. 15 2 1 14 +5-Azacytldine 150-200 mg/mffi/day
]Day 1-5 L'v. +Vlnblastlne 6 rag/mr/day Day 1, 5 Etoposide 75 rng/rnZ/day Day 1-5 t.v. 5 Azacytidine 150-o_.00 rng/m~]day 14 0 0 0
:Day 1-5 Lv, Etoposide 60 rnglm s Day 6 Lv, +Cytosine Arablnoslde 2 mK/kglday 16 8 0 50
Day 1-5 continuous Lvo +Doxorublcin 40 mg/m z Day 6 Lv. :Etoposide 100 mg/ml/day
Day 2-5 continuous Lv. 4 2 0 50 +VtncrlsUne 2 mg :Day 1 +Doxorublcin 60 mg/m t Day 2 +6-Thioguanine 200 mg/m~/dsy
Day 2-6 :Etopusldo 200 rag/day :Day 1-5 p.o. 8 3 1 38 +Cytosine Arabinoside 3 mg/kg/day
Day 6-10 +pDaunomycln 1.5 mg/kg Day 1
Previously untreated
Previously untreated
.Non-small cell lung cancer
Studies investigating the activity of etoposide in non-small cell lung cancer patients are summarized in Table 9. While the drug given as a single agent does cause definite tumor regressions, with part ial remission achieved in about 10% of patients (28, 32), the place of etoposide in combinat ion therapies is impossible to evaluate based on the single study reported by Cavalli et aL (12). Fur ther studies are required to define the role of etoposide in this disease, which is relatively resistant to chemotherapy.
Breast
The activity of etoposidc monotherapy in breast cancer patients is summarized in Table 10. The cumulative response rate for 99 evaluable patients is only 5 % and suggests disappointing activity. However, almost all patients had extensive disease and had

120 B.,F. ISSELL AND S. T. CROOKE
failed first-line chemotherapy. Eagan et aL (29) compared etoposide monotherapy to vincristine and doxorubicin patients who h a d failed first-line chemotherapy. Etoposide monotherapy resulted in 2 responses in 19 evaluable patients while the doxorubic in- vincristine combination resulted in 4 responses in 20 patients.
T a b l e 9. E t o p o s i d e in n o n - s m a l l - c e l l l u n g c a n c e r
Investigator (reference) Histology Therapy
Re~pouse
l~'umber Number evaluable Number <PR or patients G R + P R unspeelfled
Falkao~ et ale (1975) (S2)
Eaga~ et aL (1078) (.os)
CavMll el at. (1977)
Non-small-cell :Etopostdo 200 rag/day Day 1-5 p.o. 0 1 1 I 1
Adenocarclnoma Etoposlde 140 mg/m=/day D~ty 1, 3, 5 24 2 1 8 Squamous cell Etopostde 140 rag/mS/day 1, 3, 5 20 2 3 10 • N'on-small-eell Etopestde 200 rag/day Day 1-3 p.o. weekly
Vlnerlstlne 0.02 mglkglweek Lv. 19 3 5 16 ~[ethotrexate 0.75 mg/kg/wcek i.e. Cyclophosphamlde 2.0 mg]kg/day p.o.
= m , , , , , , . _ , , , , , , , , .
T a b l e I0 . E t o p o s i d e i n b r e a s t c a r c i n o m a
No. No. ]rivestigator evaluabte No. <PR or (reference) Etoposide dose and schedule patients PR unspecified % PR
EORTC (1973) (31)
Ahmann et al. (1976) (1)
Falkson el aL (1975) 02)
Eagan et al. (1976) (29)
50 mg[m~/day Day 1-5 i.e. 41 3 or I00 mg/ma/day Day I-5 p.o.
100-125 mg/m2/day Day 1, 3, 5 19 0
200 mg/m2/day Day 1-5 20 0
100-125 mg/m2/clay Day 1, 3, 5 19 2
10 7
0 0
4 0
0 10
Genitourinary
Although little information has so far been reported, some studies have suggested etoposide activity in bladder, ovarian and testicular malignancies. ]Further Phase I I studies in these tumors seem indicated.
Bladder
In the E O R T C study (31) 1 of 5 patients achieved a part ial response (PR) and Falkson et al. (32) reported 2 regressions < P R in 4 patients.
Ovary
Jung i and Senn (40) reported i part ial response and 3 regression < P R in 7 patients with ovarian carcinoma. However in the EORTCI study (31) only I of 7 evaluable patients achieved tumor regression < P R in 12 evaluable patients and no responses were reported by Edmonson et al. (30) when they treated 14 patients with advanced ovarian cancer resistant to alkylating agents.

ETOPOSIDE (VP- 16--213) 121
Testicular
Tumor regression <7 P R was reported for 1 of 4 patients in the E O R T C study (31). Newlands and Bagshawe (52) reported the results of etoposide administrat ion to 5 patients wi th mal ignant terator~as who had failed prior chemotherapy. Four patients responded both clinically and by a reduction of tumor markers. Two patients with drug-resistant choriocarcinoma were also treated. One failed to respond to etoposide alone but both responded to etoposide given after a bleomycin infusion. Cavalli et al. (10) have also reported that 4 of 7 patients with far advanced mal ignant teratomas achieved short term tumor regressions.
Hepatoma
Cavalli et al. (10) have reported 3 Objective responses in 6 patients wi th mal ignant hepatoma, who received etoposide (180 mg/m2/day Day 1-3 repeated weekly). Although the number of patients is small and no data on response durat ion are available these data are encouraging as mal ignant hepa toma is a tumor in which most chemotherapeutic agents are of limited value.
Coloreclal
Nissen et aL (55) reported 1 of 6 patients with colorectal adenocarcinoma responded to etoposide given daily. Perry et al. (58) carried out a Phase I I study with etoposide in 28 patients with measurable metastatic colorectal adenocarcinoma. Fifteen patients had received prior chemotherapy. Etoposide was given at a dose of 130 mg/m ~ on Days I, 3 and 5 and repeated at 4-5 week intervals. No patient had any objective evidence of response. Two patients h a d stabilization of disease for 13 weeks, one for 18 weeks, and one for 23 weeks. Douglass et aL (23) also failed to demonstrate any objective response when etoposide was given in a similar dosage and schedule to 44 patients with advanced measurable colorectal adenocarcinoma.
&lelanoma
A h m a n n et al. (2) carried out a similar trial to the colorectal study above in 19 patients with mal ignant melanoma. No evidence of any objective response to etoposide was seen. Cecil et al. (13) also found no evidence of response when they tested etoposide in 29 patients with mal ignant melanoma. These data suggest that this compound lacks significant activity in this disease.
Head and neck
In the E O R T C study (3I) all 32 evaluable patients with various head and neck malignancies failed to respond to etoposide (50 mg/m~/day D a y 1-5 i.v. or 100 mg/m~-/ day D a y 1-5 p.o.) suggestingno significant activity by this compound in these tumor types.
Other tumors
Patients wi th other malignancies who have shown measured tumor regression after etoposide therapy include those with thyroid cancer (7, 31), esophageal cancer (31), adul t soft tissue sarcoma (54), mesothelioma (32), prostate cancer (40), Wilms tumors (5, 54) and Ewing's sarcoma (5). However, insufficient data have been reported to determine response rates for these tumors and further studies seem indicated.

122 B.F. ISSELL AND S. T. CROOKE
S u m m a r y and conc lus ion
Etoposide or VP-16-213 is a semi-synthetic derivative of podophyllotoxin, a natural product with ant imitot ic properties. Its mode of action appears to be pre-mitosis inhibition, but rnetaphase arrest has been repor ted at higher drug concentrations. Pre-mitosis inhibi t ion is possibly secondary to an an t i -DNA synthesis effect.
Etoposide appears to be easily managed in the clinic. Its dose l imiting toxicity is myelosuppression (mainly leukopenia) and this appears to be predictable.
Etoposlde is effective when administered orally at approximately twice the effective intravenous dose. Biological activity appears to be schedule dependent with mult iple dosage over 3 or 5 days showing superiority to single dose administrat ion.
Etoposide appears to be one of the most active available drugs for small cell lung cancer. I t is also clearly active in acute non-lymphoblast ic leukemia and lymphoma. Its role ei ther as a substitute for or in addi t ion to compounds used in current front line regimens for these diseases needs to be bet ter defined by comparat ive Phase I I I studies. In non small cell lung cancer where etoposide has shown definite ~lthough modest activity in this relatively chemotherapy resistant disease further Phase I I studies examining the activity of various etoposide containing combinations are required.
Etoposide has demonstra ted encouraging activity in small numbers of patients with mal ignant hepa toma and geni tour inary tumors. The accrual of further patients in Phase I I single agent or combinat ion studies in these malignancies is needed. Also the report ing of sporadic activity in esophageal cancer, s tomach cancer, adul t soft tissue sarcoma and pediatr ic solid tumors requires further Phase I I studies to determine the response rates in these malignancies.
Based on the da ta current ly available, etoposide appears to have only minimal activity in breast cancer and does not seem to be active against colorectal adenocarcinoma, mal ignant melanoma or head and neck cancer.
A c k n o w l e d g e m e n t
The authors wish to thank S. D. Reich, A. W. Prestayko a n d J . D'Aoust for their reviews and Ms Carol Boyd for typing this manuscript .
References
I. Ahmann, D. L., Bisel, H. F., Eagan, R. T., Edmonson, J. H., Hahn, R. G., O'Connell, M.J. & Frytak, S. (1976) Cancer Treatment Reports 60: 633-635.
2. Ahmann, D. L., Bisel, H. F., Edmonson, J. H., Hahn, R. G., O'Connell, ~L J. & Frytak, S. (1976) Cancer Treatment Reports 60: 1681-1682.
3. Aisner, J., Wiernik, P. H. & Esterhay, R.J . (1977) In Adjuvant Thera#.y of Career (Salmon, S. E. & Jones, S. E., Eds). Elsevier/North Holland Biomedical Press, Amsterdam.
4. Bernasconl, C., Lazzarino, M. & Morra, E. (1976) In Erkrankungen der M yelepoese--Leukamien, .~4ryelofroliferative$ Syndrom, Po[.yzythamie (Stacher, Herausgegeben yon Alois & Hocker, Paul, Eds). Urban & Schwarzenberg, Munchen-Berlin. Pp. 224-227.
5. Bleyer, W. A., Chard, R. L., Krivit, W. & Hammond, D. (1978) Proc. Am. Soc. din. Omolo~y 19: 373. 6. Broder, L. E., Selawry, O. S., Bagwell, S. P., Silverman, M. A. & Charyulu, K. N. (1978) Proc. Am.
Assoc. Cancer Res. 19: 71.

ETOPOSIDE (VP-16-213) 123
7. Brunner, K. W., Sonntag, R. W., Rysscl, H . J . & Cavalli, F. (1976) Cancer Treatment Reports 60: 1377- 1379.
8. Cavalli, E , Sonntag, R. & Brunner, K. W. (1975) Brit. reed. ft. iv: 227. 9. Cavalll, E , Sonntag, R. W., Jungi, F., Senn, H . J . & Brunner, K. W. (1978) Cancer Treatment Reports
62: 473--475. 10. Cavalli, F., Sonntag, R. W. & Brunncr, K. VV. (1977) Lancet: 362. 11. Cavalll, F., Ryssel, H .J . , Bctz, K., Sonntag, R. W. & B,~anner, K. W. (1975) Schweitz reed. IYochenschr.
105: 250-253. 12. Cavalli, F., Hasler, E., R.yssel, H . J . , Sormtag, R. W. & Brur.ner, K. W. (1977) Tumorl 63: 169-173. 13. Cecil, J. W., Quagliana, J . M., Coltman, C. A., A1-Sarraf, M., Thigpen, T. & Groppe, C. W., Jr.
(1978) Cancer Treatment Reports 62: 801--803. 14. Chakravorty, R., Scrkar, S., Sen, S. & Mukeji, B. (1967) Brit. ~7. Cancer 21 : 33-39. 15. Cohen, 1N~I. H., Broder, L. E., Fossieck, B. E., Ihde, D. C. & Minna, J. D. (1977) Cancer Treatment
Reports 61: 489-490. 16. Cohen, M. H., Ihde, D. C., Fossleek, B. E., Bunn, P. A., Matthcws, M.J . , Shackney, S. E.,Johnston,
A. V. & Minna, J. D. (1978) Proc. Am. Sac. din. Oncology 19: 359. 17. Creasey, W. (1968) Fed. Proc. 27: 760. I8. Crcaven, P. J . , Newman, S .J . , Selawry, O. S., Cohen, M. H. & Primack, A. (1974) Cancer Chemo-
therapy Reports 58: 901-907. 19. Crcaven, P .J . & Allen, L. M. (1975) Clin. Pharm. Therapeutics 18: 221-226. 20. Dombcrnowsky, P. & Nissen, N. I. (1973) Arch. Path. zl~ficrobioL Scand. 81: 715-724. 21. Dombernowsky, P., Nisscn, N. I. & Larsen, V. (1972) Cancer Chemotherapy Reports 56: 71-82. 22. Dombcrnowsky, P. & Nissen, N. I. (1973) Proc. Am. Assoc. Cancer Res. 14: 167. 23. Douglass, H, O., Maelntyre, J. M., Evans, J . T., Kaufman, J. & Carbone, P. P. (1977) Proc. Am.
Sac. clin. Oncolog), 18: 313. 24. Drewlnko, B. & Barlogie, B. (1976) Cancer Treatment Reports 60: 1295-1306. 25. Dubovsky, D. & Jacobs, P. (1975) South African tned. 97. 49: 1904. 26. Eagan, R. T., Carl', D. T., Frytak, S., Rubin, J. & Lcc, R. E. (1976) Cancer Treatment Reports 60:
949-951. 27. Eagan, R. T., Carr, D. T., Lee, 1R.. E., Frytak, S., Rubin, J . & Coles, D. T. (1977) Cancer Treatment
Reports 61: 93-95. 28. Eagan, I~. T., Ingle, J . N., Crcagan, E. T., Frytak, S., Kvols, L. K., Rubin, J . & McMahon, R. T.
(1978) Cancer Treatment Reports 62: 843-844. 29. Eagan, R. T., Ahmann, D. L. & Biscl, H. F. (1976) Ontology 33: 146-148. 30. Edmonson, J. H., Dcckcr, D. G., Malkasian, G. D., Wcbb, M.J . & Jorgenscn, E. O. (1978) Gynecologic
Oncology 6: 7. 31. EOI~TC: (1973) Brit. med. oT. ill: 199-202. 32. Falkson, G., VanDyk, J . J . , VanEden, E. B., Van der ~¢erwe, A. M., Van den Bergh, J. A. & Falkson,
H. C. (1975)Cancer 35: 1141-1144. 33. Geran, R. I., Congleton, G. F., Dudeck, L. E., Abbott, B . J . & Gargus, J . L. (1974) Cancer Chemo-
therapy Pep. Part 2 4: 53-87. 34. Getaz, E. P. & Staplcs, W. G. (1977) South African med. J . 51: 852-853. 35. Grccnspan, E., Leitcr, J. & Shear, M. (1950) .7. nat. Cancer Inst. 10: 1295-I333. 36. Hammond, R. L. (1977) Proc. Am. Sac. clin. Oncol. 18: 352. 37. Hansen, M., Hirsch, F., Dombcrnowsky, P. & Hanscn, H. H. (1977) Cancer 40: 633--637. 38. Jacobs, P., Dubovsky, D., Hougaard, M. & Comay, S. (1975) Brit. reed. J . i: 396. 39. Jacobs, P., King, H. S. & Scaly, G. R. H. (1975) S. African reed. ~7. 49: 483-485. 40. Jungi, W. F. & Senn, H . J . (1975) Cancer Chemotherapy Rep. 59: 737-742. 41. Kaplan, I. (1942) aVew Orleans reed. Surg. 97. 94: 388-390. 42. Kcllcr-Juslin, C., Kuhn, M. & van Wartburg, A. (1971) 97. reed. Chem. 14: 936-940. 43. Kelly, M. & Hart~vell, J. (1954) ft. nat. Cancer Inst. 14: 967-1010. 44. King, L. & Sullivan, M. (1946) Science 104: 244-245. 45. Krishan, A., Palka, K. & Frci, E. (1975)~7. Cell Biol. 66: 521-530. 46. Lclter, J., Downlng, V., HartwcI1, J. & Shear, M. (1950) 97. #Vat. Cancer Inst. 10: 1273--1290. 47. Loike, J. D. & Horwitz, S. B. (1976) Biochemistry 15: 5435-5442. 48. Loikc, J. D. & Horwitz, S. B. (I976) Biochemistry 15: 5443-5448. 49. Marsdcn, J. H. (1972) In Cancer Ctwrnotherapy I[ (Brodsky, I., Kahn, S. & Mayer, J., Eds). Greene and,
Stratton, New York and London. pp. 33-40.

124 B. F. ISSELL AND S.T. CROOKE
50. Math~, G., Schwarzenberg, L., Pouillart, P., Oldham, R., Weiner, R., Jasmin, C., Rosenfeld, C. Hayat, M., Misset, J. L., Mussel, M., Schneider, M., Amiel, J. L. & DeVassal, F. (1974) Cancer 34: 985--992.
51. Muggla, F. M., Selawry, O. S. & Hamen, H. I~/. (1971) Cancer Cl~motl~r. Rep. 55: 575-581. 52. Newlands, E. S. & Bagshawe, K. D. (1977) Lancet ii: 87. 53. Nissen, N. I., Larsen, V., Pedersen, H. & Thomson, K. (1972) Cancer Chemott~r. Rep. 56: 769-777. 54. Nissen, N. I., Hamen, H. H., Pedersen, H., Strayer, I., Dombernowsk¥, P. & Hessellund, M. (1975)
Cancer Chemotherapy Reports 59: 1027-1029. 55. Nissen, N. I., Dombernowsky, P., Hansen, H. H. & Larsen, V. (1976) Cancer Treatment Reports 60:
943-945. 56. O'Connell, M.J. , Silverstein, M. N., Kiely, J. M. & White, W. L. (1977) Cancer Treatment Reports 61:
65-68. 57. Oldham, R. K., Greco, F., Richardson, R. L. & Stroup, S. L. (1978) Proc. Am. Sot. din. Oncology 19:
361. 58. Perry, M. C., Moertel, C. G., Schult, A.J., Reitemeler, R.J . & Hahn, R. G. (1976) Cancer Treatment
Reports 60: 1247-1250. 59. Rivera, G., Avery, T. & Pratt, C. (1975) Cancer Chemother. Re/torts Part 1 59: (4) 743-749. 60. Rivera, G., Avery, T. & Roberts, D. (1975) Eur.J. Canter U: 639-647. 61. Rozencwelg, M., VonHoff, D. D., Henney, J. E. & Muggla, F. (1977) Cancer 40: 334-342. 62. Sandoz Pharmaceuticals (1971) VP-16--213 Preclinlcal Brochure. 63. Smith, I. E., Gerken, M. E., Clink, H. M. & MeClwain, T .J . (1976) Postgrad. reed.ft. 52: 66-70. 64. Stahelin, H. (1972) Europ...7. Cancer 9: 215-221. 65. Tenczynski, T. F., Valdivieso, M., Hersh, E. M., Khalil, K. G., Mountain, C. F. & Bodey, G. P.
(1978) Proc. Am. Soc. din. Ontology 19: 376. 66. Tucker, R. D., Ferguson, A., VanWyk, C., Scaly, R., Hewltson, R. & Levln, W. (1978) Cancer 41:
1710-1714. 67. Vaitkevicius, V. & Reed, M. (1966) Canoe." Chemother. Re/J. 50: 565-571. 68. Van Echo, D. A., Wiernik, P. H. & Aisner, J. (1978) Proc. Am. Assoc. Cancer Research 19. 144. 69. Venditti, J. M. (1971) Cancer Chcmother. Rep. (3) 2: 35-59. 70. Young, C. SV., Ihde, D. C. & Von Stubbe, W. (1973) Pror. Am. Assoc. CancerRes. 14: 60.













![Increased Rate of Adenosine Triphosphate …...(CANCER RESEARCH 55, 4352-4360, October 1, 1995] Increased Rate of Adenosine Triphosphate-dependent Etoposide (VP-16) Efflux in a Murine](https://img.pdfslide.us/doc/110x75/5e7e8d68c5d0407f2447f2a9/increased-rate-of-adenosine-triphosphate-cancer-research-55-4352-4360-october.jpg)