Embed Size (px)
Citation preview

Journal of Taibah University Medical Sciences (2012) 7(1), 41–44
Taibah University
Journal of Taibah University Medical Sciences
www.jtaibahumedsc.netwww.sciencedirect.com
Case Report
Etiology of ‘blue toe’ syndrome: Emboli versus
warfarin therapy. Report of a case
Samer Ibrahim Sawalhi, MD, MRCS a,*, Hisham Hamad, MD, FRCS b
a Assistant professor in surgery, College of Medicine- Department of surgery, Taibah University, Almadinah Almunawwarah,Saudi Arabia.b Vascular surgery consultant-Islami Hospital, Amman-Jordan.
Received 12 May 2012; revised 19 June 2012; accepted 27 June 2012
*
Su
A
E
Pe
16
ht
KEYWORDS
Anticoagulant therapy;
Blue toe syndrome
Corresponding author. Ad
rgery, Taibah University,
rabia. Tel.: +966 596832442
-mail address: skyscraper555
er review under responsibilit
Production an
58-3612 ª 2012 Taibah Univ
tp://dx.doi.org/10.1016/j.jtum
dress: A
Almadi
.
@yahoo
y of Taib
d hostin
ersity. P
ed.2012.
Abstract ‘Blue toe syndrome’ presents as a cyanotic toe caused by fibrino-platelet micro-emboli
occlusion of the small digital arteries, with palpable pedal pulses originating from a proximal ath-
eromatous source (cardiac, aortic, femoral or popliteal aneurysm). We report a case in a 43-year-old
woman with a history of hypertension and diabetes. She was taking warfarin for extensive right
deep-vein thrombosis 6 months before her current admission. She presented with sudden onset of
severe pain, parasthaesia and bluish discolouration of the right big, second and third toes, in spite
of palpable distal pulses. Computerized tomography angiography revealed an atheromatous plaque
causing 70% stenosis of the infra-renal aorta. We therefore performed aortotomy, thrombectomy
and endartectomy. Blue toe syndrome is of clinical importance in etiology, diagnosis and treatment.
Our case had blue toe syndrome despite anticoagulant therapy.ª 2012 Taibah University. Production and hosting by Elsevier Ltd. All rights reserved.
Introduction
Blue toe syndrome was first described by Karmody in 1976 asacute digital cyanosis secondary to micro-embolism from a
proximal atheromatous source, despite palpable or audibleDoppler signals.1 Blue toe syndrome can occur spontaneously2
or, rarely, following anticoagulant therapy.3–6 Patients with a
recent history of an invasive vascular procedure or anticoagu-
ssistant Professor in General
nah Almunawwarah, Saudi
.com (S.I. Sawalhi).
ah University.
g by Elsevier
roduction and hosting by Elsevier
07.004
lant therapy are most likely to have cholesterol embolism.7,8
Establishing the source of micro-emboli is vital; therefore,diagnosis is based first on duplex ultrasound of the arteriesof the involved limb and echocardiography to exclude a car-
diac source. Chest and abdominal computerized tomographyand angiography are used to exclude an aortic or iliac sourceof emboli. Surgery should be focused on removal of the em-
bolic source from the proximal circulation, by endartectomy,stent grafting or a bypass procedure.9 We present a case ofblue toe syndrome with an unusual presentation, the etiology
of which was either micro-emboli or warfarin therapy.
Case report
A 43-year-old woman with history of hypertension and diabe-tes mellitus developed extensive right femoro-popliteal deepvenous thrombosis 6 months after trauma. She had been
Ltd. All rights reserved.

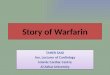
Figure 1: Sharply demarcated bluish discoloration of right first,
second and third toes.
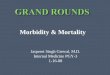
Figure 2: Reformatted sagital image delineates infra-renal aortic
atheromatous plaque causing 70% lumen encroachment.
42 S.I. Sawalhi, H. Hamad
taking 3 mg warfarin daily for the last 6 months. She had nohistory of hyperlipidaemia, no previous arterial catheterizationor claudication and no family history of hypercoagulation. She
presented to the casuality department with bluish discolour-ation of the right big, second and third toes, which were tenderto the touch, sharply demarcated, with severe pain and parast-
haesia (Figure 1). Her vital signs were stable. Physical exami-nation revealed dusky bluish right big, second and third toeswith moderate to severe tenderness, coldness and delayed cap-illary refill. The bilateral femoral, popliteal, dorsalis pedis and
posterior tibial arteries were palpable, with no features of con-nective tissue or Bahce’t disease. The ankle–brachial index wasnormal.1
Blue toe syndrome was suspected because the peripheralpulses were intact. The initial investigations included electro-cardiography, which showed normal sinus rhythm, a normal
chest X-ray, which showed no cardiomegaly or congested lung,haematological investigations such as for factor von Leiden,proteins C and S and antiphospholipid antibody to excludehypercoagulation. The coagulation profile was: prothrombin
time, 19.2 s; partial thromboplastin time, 28.3 s; internationalnormalized ratio, 1.68. Kidney function tests, lipid profile, fi-brin degradation products and vasculitis screening (nuclear
antibody, DNA and extractable nuclear antigen) were normal.Echocardiography was performed to exclude emboli. The ejec-tion fraction of the heart was 70%, with normal left ventricle
size, trace mitral regurgitation and no pericardial effusion; leftventricular systolic function was normal, and there was noblood clot in the heart chambers. Intravenous heparinization
was started. Abdominal ultrasound showed a non-ulcerated,infra-renal, 3-cm aortic atheromatous plaque causing 70% ste-nosis in the lumen, as confirmed by duplex mode. An abdom-inal computer tomography scan with contrast and reformatted
sagital images of the abdominal aorta confirmed the ultra-sound result (Figure 2).
Surgery is the preferred treatment approach, with good re-
sults,9 and further embolization during anticoagulant therapyshould be treated with immediate surgical intervention.10 Theinfra-renal aorta was approached transperitoneally by aortot-
omy. A non-ulcerated, 3-cm, yellowish atheromatic plaque wasattached to the intima, without calcification or aneurysmaldilatation. Thrombectomy and endartectomy were performed.
Careful manipulation of the artery and clamping were adoptedto avoid plaque disruption. Histopathological examination re-vealed a 3-cm, yellowish atheromatic plaque with a smooth
surface. Microscopically, there were many cholesterol crystalswith lipid-laden macrophages and fibrous material.
The post-operative period was uneventful, with the patienton warfarin and aspirin. Superficial ischaemic changes of theinvolved toes resolved within 1 month of her admission. Thepatient was asymptomatic during 1 year of follow-up.
Discussion
Blue toe syndrome is the spontaneous onset of a painful bluishdiscolouration of the toes caused by fibrino-platelet micro-em-boli from the abdominal aorto-iliac-femoral arterial system,which travels down the arterial tree into the small digital ves-
sels of the foot, where it becomes lodged. The condition canoccur insidiously or may be the result of abdominal surgeryor an invasive vascular procedure (2%)7,8,11,12 that scratches
the luminal surface of the vessels, or rarely following anticoag-ulation.3–6 Acute digital ischaemia caused by the coumarinanticoagulant warfarin was first described by Feder and Auer-
bach.13 It has been suggested4 that use of anticoagulants pre-vents stabilization of the ulcerated plaque surface by clottingand leads to gradual loss of the protective fibrin layer overlyingthe plaque,14 which permits cholesterol-containing debris to be
shed into the circulation. Lodgement of cholesterol clefts insmall arteries results in an inflammatory reaction involvingmacrophage and giant cell infiltration. This inflammatory reac-
tion leads to an endothelial reaction causing intimal prolifera-tion, intravascular fibrosis of the affected vessels andnarrowing or obliteration of the lumen, which may cause tissue
ischaemia. Acute focal digital ischaemia may result fromembolism, thrombosis, mechanical obstruction or inflamma-tion or from a combination of these mechanisms.15 Vasospasm
may also contribute, because endothelial cell damage from any

Etiology of ‘blue toe’ syndrome: Emboli versuswarfarin therapy 43
cause impairs generation of endothelium-derived relaxationfactor and prostacyclin.15
Some reports indicate that blue toe syndrome is induced by
long-term anticoagulant therapy with warfarin, acenocouma-rol or phenindione.5,6,16 Anticoagulant-associated cholesterolembolization has been reported to develop 1 week to 3 years
after initiation of antiocoagulants.5,17,18 Rauh and Spengel re-ported that cholesterol emboli may also occur in patients trea-ted with low-dose oral anticoagulation for 2 months, with no
previous arterial catheterization.3 In patients with no obviousembolic source, systemic abnormalities should be considered,including circulating agglutinins, vasculitis, acrocyanosis, sys-temic lupus erythematosus, polycythemia vera and subacute
bacterial endocarditis, as well as certain drugs such as warfarinand prednisilone.19
The segment most commonly responsible for symptomatic
embolization is the aorta-iliac segment.20 Keen et al. notedthat 85% of emboli arose from aorto-iliac occlusive or anerys-mal disease.20 Untreated blue toe syndrome frequently recurs
and could result in loss of a limb and death.10 Our patienthad extensive aortic atheroma that might have been due tohypertension, atherosclerosis and diabetes mellitus. Hyperco-
agulability in diabetes mellitus can result from abnormal plate-let function, increased blood viscosity or decreased red bloodcell deformability or from disturbances of the coagulationand fibrinolytic systems.21 Moreover, both thromboembolism
and atheroembolism can occur either spontaneously or afteran iatrogenic procedure in the aorta.12 Patients with bilateralblue toe syndrome usually have an embologenic lesion proxi-
mal to an aortic bifurcation, while unilateral lesions are usuallyassociated with an atherosclerotic plaque or aneurysm distal tothe aortic bifurcation.22 Our patient had unilateral blue toe
syndromeeven though the plaque lesion was located proximalto the aortic bifurcation.
Establishing the source of an embolism is vital. Noninva-
sive vascular assessment including ultrasound imaging todetermine the presence of an aneurysm, should be performedin all patients.15 Computerized tomography angiography isthe preferred imaging modality for diagnosis, while angiogra-
phy is reserved for cases in which noninvasive evaluation isnot informative.23 A renal function test is often performed inpatients with bilateral lesions because deterioration in the
suprarenal aorta due to atheroemboli can lead to renal shut-down. The standard treatment for lower limb microemboliza-tion is removal of the embolic source.22 In our case, we used
immediate surgery as the standard treatment approach, withgood results. Further embolization during anticoagulant ther-apy should be treated by immediate surgical intervention,10
especially for plaques located in the infra-renal aorta. Endar-
tectomy with or without patch angioplasty has been estab-lished in the literature and should be considered thetreatment of choice when limb-threatening ischaemia is pres-
ent.10 Several authors have found antiplatelet24 and anticoag-ulant treatment to be ineffective3 and suggested that it mighteven predispose to further embolization.1 There is some evi-
dence that warfarin and heparin might actually promote fur-ther embolization.5
Morris-Jones et al.24 used the antiplatelet drugs acetylsali-
cylic acid and dipyridamole to treat patients with blue toe syn-drome. Treatment with aspirin or warfarin has resulted in anoverall recurrence rate of 75%.20 Therefore, anticoagulantsare generally less effective than surgical intervention.23 If a pa-
tient develops the syndrome, long-term anticoagulation shouldbe withdrawn, if possible.16 Interestingly, it has been reportedthat a patient may be become asymptomatic even if oral anti-
coagulation is continued5 or given at a lower dosesymptomatic.25
Angioplasty with stenting is effective in treating blue toe
syndrome.23 Renshaw and colleagues used percutaneous angi-oplasty with stenting for eight patients with unilateral blue toesyndrome and 12 haemodynamically significant lesions: four in
the superficial femoral artery, six in the common iliac and twoin the external iliac. They concluded on the basis of intermedi-ate results that angioplasty and stenting are a reasonable alter-native to standard operative approaches.23 Treatment with
anticoagulants and delayed angioplasty of the upstream lesion,including in the iliac, femoral and popliteal arteries, may be aneffective alternative to surgery,10 but endovascular stenting for
treatment of aortic and arterial embolism has largely been lim-ited to abdominal aortic and infrainguinal forms of the dis-ease.26 Case reports have suggested a beneficial role of
statins (3-hydroxy-3-methylglutaryl-coenzyme A reductaseinhibitors) in stabilizing the cholesterol-rich atheroscleroticplaque. Statins have not only a cholesterol-lowering effect
but also anti-inflammatory and immunomodulatory proper-ties, which may play a role in plaque stabilization.27
There are limited data on the long-term outcome of medi-cal, surgical or combined management of blue toe syndrome.
Conclusion
A careful history and physical examination will often suggest
the cause of blue toe syndrome. For patients on anticoagulanttherapy (warfarin) who complain of toe symptoms, blue toesyndrome should be considered. The distinctions between uni-
lateral and bilateral blue toe syndrome and between the pres-ence or absence of associated systemic or cutaneous findingsare useful.
Surgery should focus on removal of the embolic sourcefrom the proximal circulation. We suggest that further embo-lization during anticoagulant or antiplatelet therapy be treated
by immediate surgical intervention. More cases and clinical tri-als are needed to determine the optimal treatment and to cat-egorize which patients require surgical intervention and whichcan be managed safely by medical therapy or stenting.
Conflict of interest statement
Neither Samer Sawalhi nor Hisham Hamad has a conflict of
interest.
References
1. Matchett WJ, McFarland DR, Eidt JF, Moursi MM. Blue toe
syndrome: treatment with intra-arterial stents and review of
therapies. J Vasc Interv Radiol 2000; 11: 585–592.
2. Kugler CF, Poser M, Mosel F, Ruehm S, Rudofsky G. Sponta-
neous dissection of the popliteal artery in a young man. A rare
cause of the blue toe syndrome. Int Angiol 2006; 25: 93–97.
3. Rauh G, Spengel FA. Blue toe syndrome after initiation of low-
dose oral anticoagulation. Eur J Med Res 1998; 17: 278–280.
4. Oster P, Rieben FW, Waldherr R, Schettler G. Blood clotting and
cholesterol crystal embolization. JAMA 1979; 242: 2070–2071.

44 S.I. Sawalhi, H. Hamad
5. Moll S, Huffman J. Cholesterol emboli associated with warfarin
treatment. Am J Hematol 2004; 77: 194–195.
6. Varis J, Kuusniemi K, Heiro M, Jarvelainen H. Blue toe syndrome
– a rare but possible complication of anticoagulant therapy.
Duodecim 2011; 127: 1154–1157.
7. Ramirez G, O’Neill Jr WM, Lambert R, Bloomer HA. Cholesterol
embolization: a complication of angiography. Arch Intern Med
1978; 138: 1430–1432.
8. Colt HG, Begg RJ, Saporito JJ, Cooper WM, Shapiro AP.
Cholesterol emboli after cardiac catheterization. Eight cases and
a review of the literature. Medicine (Baltimore) 1988; 67:
389–400.
9. Fisher Jr DF, Clagett GP, Brigham RA, Orecchia PM, Youkey
RJ, Aronoff RJ, et al.. Dilemmas in dealing with the blue toe
syndrome: aortic versus peripheral source. Am J Surg 1984; 148:
836–839.
10. Brewer ML, Kinnison ML, Perler BA, White Jr RI. Blue toe
syndrome: treatment with anticoagulants and delayed percutane-
ous transluminal angioplasty. Radiology 1988; 166: 31–36.
11. Fukumoto Y, Tsutsui H, Tsuchihashi M, Masumoto A. Choles-
terol Embolism Study (CHEST) investigators. The incidence and
risk factors of cholesterol embolization syndrome, a complication
of cardiac catheterization: a prospective study. J Am Coll Cardiol
2003; 42: 211–216.
12. Tunick PA, Rosenzweig BP, Katz ES, Freedberg RS, Perez JL,
Kronzon I. High risk for vascular events in patients with
protruding aortic atheromas: a prospective study. J Am Coll
Cardiol 1994; 23: 1085–1090.
13. Feder W, Auerbach R. ‘Purple toes’: an uncommon sequela of oral
coumarin drug therapy. Ann Intern Med 1961; 55: 911–917.
14. Warkentin TE. Coumarin-induced skin necrosis and venous limb
gangrene. In: Colman RW, Marder VJ, Clowes AW, George JN,
Goldhaber SZ, editors. Hemostasis and thrombosis: basic principles
and clinical practice. Philadelphia, PA: Lippincott Williams &
Wilkins; 2005. p. 1663.
15. O’Keeffe ST, Woods BO, Breslin DJ, Tsapatsaris NP. Blue toe
syndrome. Causes and management. Arch Intern Med 1992; 152:
2197–2202.
16. Meyrier A. Cholesterol crystal embolism: diagnosis and treatment.
Kidney Int 2006; 69: 1308–1312.
17. Wakabayashi T, Yoshizawa Y, Kawana S. Successful use of
heparin and warfarin in the treatment of cholesterol crystal
embolization. J Dermatol 2008; 35: 111–114.
18. Jucgla A, Moreso F, Muniesa C, Moreno A, Vidaller A.
Cholesterol embolism: still an unrecognized entity with a high
mortality rate. J Am Acad Dermatol 2006; 55: 786–793.
19. Caldwell BD, Marrochello VS. Microembolization from athe-
roembolic disease or aneurysm. A case study. J Am Podiatr Med
Assoc 1996; 86: 249–252.
20. Keen RR, McCarthy WJ, Shireman PK, Feinglass J, Pearce WH,
Durham JR, et al. Surgical management of atheroembolization. J
Vasc Surg 1995; 21:773–80 [discussion, 780–781].
21. Banga JD, Sixma JJ. Diabetes mellitus, vascular disease and
thrombosis. Clin Haematol 1986; 15: 465–492.
22. Kaufman JL, Karmody AM, Leather RP. Atheroembolism and
micro-thrombotic syndromes (the blue toe syndrome and dissimi-
nated atheroembolism). In: Rutherford RB, editor. Vascular
surgery. 3rd ed. Philadelphia, PA: W.B. Saunders; 1989. p.
565–574.
23. Renshaw A, McCowen T, Waltke EA, Wattenhofer SP, Tahara
BT, Baxter BT. Angioplasty with stenting is effective in treating
blue toe syndrome. Vasc Endovascular Surg 2002; 36: 155–159.
24. Morris-Jones W, Preston FE, Greaney M, Chatterjee DK.
Gangrene of the toes with palpable peripheral pulses. Ann Surg
1981; 193: 462–466.
25. Yang YW, Chen CL, Ho WT, Wang KH. Cutaneous reactive
angiomatosis associated with cholesterol embolism. J Cutan
Pathol 2010; 37: 692–696.
26. Wolf PS, Burman HE, Starnes BW. Endovascular treatment of
massive thoracic aortic thrombus and associated ruptured ather-
oma. Ann Vasc Surg 2010; 24: 416.
27. Blanco-Colio LM, Tunon J, Martın-Ventura JL, Egido J. Anti-
inflammatory and immunomodulatory effects of statins. Kidney
Int 2003; 63: 12–23.