Embed Size (px)
Citation preview

Ethics and Professionalism:The Integrity of Medicine
Richard L. Elliott, MD, PhD, FAPAProfessor, Internal Medicine and Psychiatry
Director, Medical EthicsMercer University School of Medicine

Goals• Week one
– Review first year ethics– Three topics on the integrity of the medical profession– Research and ethics
• “The purpose of Community Medicine II is to introduce the concept of evidence-based medicine”
– Small group discussions• Week two• Medicine and the pharmaceutical industry
– Medical student abuse– Impaired colleagues– Exam

Resources
• http://medicine.mercer.edu/Academics/Degree%20Programs/Doctor%20of%20Medicine/medicalethicsprogram

Ethical Principles
• Primum non nocere– First do no harm
• Beneficence• Autonomy• Social justice

USMLE #11. A 72-year-old man was diagnosed with prostate cancer. He
had surgery and felt well for two years before bone metastases were diagnosed. He begins to suffer pain and nausea. He is clear-minded and fully understands his medical condition, prognosis, and treatment options. The patient consistently tells you orally and in writing that he does not want further treatment and wants his physicians to focus on pain relief. With the patient’s agreement, a DNR order is in place. In the hospital, the patient loses the ability to understand questions he is asked about his care. His family requests that the DNR be reversed.

You should:
• Agree with the family and change his DNR status
• Tell the family you cannot change his DNR status
• Advise the family you cannot continue as his physician and ask them to obtain another physician
• Ask for an Ethics Committee consultation

USMLE #2• Ms. Manners is a 39-year-old woman with severe
mental retardation. Her parents have died and no information is available about other living relatives. She lives at a long-term care facility. A court-appointed guardian has been appointed to make health care decisions for her. She has never been able to express preferences of her own concerning these decisions. She has developed leukemia. Treatment involves significant risk and discomfort and only a small chance of prolonging her survival.

Best Interests vs. Substituted Judgment
• What should be done in terms of her medical treatment?– Proceed with the chemotherapy– Withhold chemotherapy– Confer an “expert panel” to determine therapy– Ask the guardian what is in the best interests of
the patient

USMLE #5
• A 73-year-old-man has been brought to a chronic-care facility for long-term ventilator management. The patient has advanced COPD and is unable to be weaned from the ventilator. A tracheostomy has been placed. A nasogastric tube is in place to deliver tube feeding. The patient is fully alert, and understands the situation. He is asking to have the nasogastric tube removed because of discomfort.

You Should:• Document patient’s competence, decision, and
discussion on consequences.• Agree and remove the tube.• Ask to speak with a family member.• Discuss with legal counsel.• Get Ethics Committee consultation.• Check with billing department for proper
reimbursement code for removing tube.

Clinical Research Ethics
• Early history• Tuskegee• Institutional Review Boards





Syphilis
• Widespread• Multiple manifestations• Leading cause of admission to mental
hospitals• Treatment dangerous, questionable is
risk/benefit ration favorable• Previous study of course of syphilis in whites• Study needed to compare outcomes in treated
vs. untreated syphilis






Was Tuskegee An Isolated Incident?
• Nazi experimentation• 1956-70 Hepatitis and Willowbrook State School• 1963 Cancer and Jewish Hospital for Chronic
Diseases• 1960-72 Cincinnati radiation exposure
experiments• Others

Aftermath of Tuskegee
• Widespread distrust among blacks of clinical studies
• National Research Act of 1974• Belmont Report• Institutional Review Boards

National Research Act
• Establishment of IRBs to review all federally funded grants involving human subjects• Common Rule (Title 45 Code of Federal Regulations Par. 46 [45 CFR 46]). • In order for persons (or their legally authorized representatives) to give “legally
effective informed consent,” the researchers seeking participation must disclose eight elements of information about the study:
• 1. a statement that the study involves research, and description of that research and its purposes;
• 2. a description of reasonably foreseeable risks;• 3. a description of reasonably expected benefits;• 4. a disclosure of appropriate alternatives;• 5. a statement about maintenance of confidentiality;• 6. an explanation of possible compensation in case of injury, if the study involves
more than minimal risks;• 7. information about how subjects can have questions answered;• 8. and a statement that participation is voluntary.

1979 Belmont ReportEthical Principles of Research
• Respect for persons– Autonomy
• Informed consent– Protection for vulnerable populations with limited autonomy
• Beneficence– Do no harm– Consider risk/benefits of research– Weigh benefits to society vs individual
• Phase I clinical trial with health volunteers• Justice
– Who should bear the burdens of and benefit from research?– Tuskegee study

IRBs
• Purpose: to assure, both in advance and by periodic review, that appropriate steps are taken to protect the rights and welfare of humans participating as subjects in a research study.
• Mandatory for research conducted in Federal Institutions or Federally supported research

Composition of IRB
• At least 5 members, including one scientist, one non-scientist, one community member.
• If study involves vulnerable population, must have member familiar with this group– Children, pregnant women, prisoners, mentally
disabled• Members must not have conflict of interest

Exempt From IRB Review 45 CFR, Subtitle A, Part 46.101b. • Research conducted in established or commonly accepted educational settings, involving normal
educational practices, such as – research on regular and special education instructional strategies, or – research on the effectiveness of or the comparison among instructional techniques, curricula, or
classroom management methods.
• Research involving the use of educational tests (cognitive, diagnostic, aptitude, achievement), survey procedures, interview procedures or observation of public behavior, unless:
• i. information obtained is recorded in such a manner that human subjects can be identified, directly or through identifiers linked to the subjects; or
• ii. any disclosure of the human subjects' responses outside the research could reasonably place the subjects at risk of criminal or civil liability or be damaging to the subjects' financial standing, employability, or reputation.
• Research involving the collection or study of existing data, documents, records, pathological specimens, or diagnostic specimens, if these sources are publicly available or if the information is recorded by the investigator in such a manner that subjects cannot be identified, directly or through identifiers linked to the subjects.

Groups
• Medical ethics site, Second Year– Ethics of Clinical Research link
• Read cases• Analyze• Discuss• Exam may include questions from cases


Ethics and Professionalism: IIMedical Industry and Medical Practice
Richard L. Elliott, MD, PhD, FAPAProfessor and Director, Medical EthicsMercer University School of Medicine

Week Two
• Feedback on groups?• The integrity of medical research
– Last week – ethics and the protection of research subjects• Tuskegee, IRBs
– Today – another threat to our integrity• Medicine and the medical industry
• Wednesday – threats to our integrity from within– Abuse of trainees– Impaired physicians

Relationships with the Pharmaceutical Industry
• Pervasive influence of industry in medicine– How good is the evidence in Evidence-Based Medicine?
– Publication bias• Negative studies• Adequate review in industry funded journals• Duplicate publications
– What are we teaching?– Influence over content of medical education
• CME talks, lunches
– What are we prescribing?– Influence over prescribing practices
• Free samples• Gifts• Advertising



Similar Effectiveness of Paroxetine, Fluoxetine, and Sertraline in Primary Care• K Kroenke et al. JAMA 2001;286:2947-2955• ARTIST: A Randomized Trial Investigating SSRI
Treatment• 573 depressed adult patients• 37 clinics• 1999• Open label, randomized study• Sponsored by Eli Lilly

ARTIST - Comparative Outcomes per Eli Lilly
• No statistically significant differences in clinical outcomes
• No differences among anxious-depressed patients
• No differences among older patients• No differences in patient satisfaction


Rankings of All Measures at 3 and 9 Months
Paroxetine Fluoxetine Sertraline
Best 7 15 58Middle 27 39 14Worst 39 19 1
p<10-21

ARTIST
• Rare example of reporting a positive study as negative
• What influence did Eli Lilly have on editorial decisions?– Choice of reviewers?– Referral to JAMA statistician?
• Why did JAMA publish this in this fashion?

Big Pharma Scandals
• Vioxx and deaths• Data submitted to FDA concluded no significant risk• Intent-to-treat deaths in RCTs for Alzheimer’s
– Subjects 34/1069– Placebo 12/1078 – Hazard ratio 2.99
• JAMA 2008;299:1813
• SSRI antidepressants and suicide• Vagal nerve stimulation and editorials

Publication Bias• Perlis et al. Am J Psychiatry 2005;162:1957-60• 162 randomized, double-blind, placebo-controlled
clinical trials between 2001-2003• AGP, AJP, J Clin Psych, J Clin Psychopharmacology• 60% received funding from industry• 47% authors reported potential conflict of interest• Those with potential conflict of interest were 4.9
times less likely to report negative results (6/75 vs. 26/87)
• Comparable results in non-psychiatric literature

Effectiveness of Antidepressants• 74 FDA-registered trials of 12 antidepressants approved between 1987-
2004• 74 trials, 38 positive (statistically significant benefits for drug over placebo)
– 37/38 published• Of 36 FDA-deemed negative trials:
– 22 never published– 11 published in manner to appear positive– Only 3 negative trials published
• Turner et al. NEJM 2008;358:252-60
• Thus, the published evidence for the efficacy of SSRIs is vastly different from the results of all trials:– 48/51 trials positive vs. 38/74

Efficacy of Cardiovascular Drugs
• Results published in NEJM, JAMA, Lancet– 2000-2005
• If study funded by for-profit, 67.2 % favored newer treatment
• If study funded by non-profit, 49% favored newer treatment
• Ridker PM, Torres J: JAMA 2006; 295. 2270-2274

Publication of Clinical Trials
• 451 study protocols submitted to one research committee
• 375 publications resulted from 233 protocols (publication rate 52% - 233/451 protocols)
• Odds ratios for publication:– Non-commercial funding 2.4– Commercial funding 0.7
• Von Elm et al. Swiss Med Weekly

Reducing Publication Bias
• Authors must have submitted trial to clinicaltrials.gov– Negative results would have been available
• Authors must report potential conflicts of interest– But funding sources can be buried in a long list of
honoraria, speakers bureaus, research funding, …• Mandatory reporting of payments from
medical industries

Clinical Equipoise
• Ethical principle in controlled trials• The must be genuine doubt within a community of
experts whether the treatment is beneficial• Once the certainty of benefits (or adverse effects) is
established, the preferred treatment must be offered• Problem: stacking the deck in favor of a sponsored
product – e.g., inadequate dosing of comparator• So, if clinical equipoise is followed, we should reduce
trials unfairly designed to favor a particular treatment

Peer Review
• Peer review – supposed to ensure submission has scientific validity and ethical integrity
• Peer review” is a term used loosely by some.– The editor/symposium chair looked at it

Peer Review
• Reviewers are selected randomly from a pool of pre-qualified experts having no conflicts of interest – avoids preselecting outcome of review– Some studies are so specialized that few experts
exist and cannot be assigned randomly– Conflicts can be buried in a list of funding sources
• Blinded review: Authors are removed from reviewers copies– Not hard to identify some authors based on
references, previous work

Ghost Writing
• Ghost writer – person not identified who was involved in significant data or writing process
• 11-13% of articles – Flanagan et al. JAMA 1998;280:222– Ross JAMA 2008;299:1800
• “Hundreds of articles” The Observer Dec 7, 2003
• Guest author – inclusion of author who had minimal or no involvement in data or writing– Often honorarium– 16% research articles, 26% review articles, 21% editorials
• ARTIST study?

Influence of Industry on Scientific Conclusions
• Effects of passive smoking – harmful?• 106 reviews• 39/106 (37%) of reviews concluded no harm
– 29/39 (74%) of these reviews had tobacco affiliations• 67/106 (63%) of reviews concluded passive smoke harmful
– 2/67 (3%) had tobacco affiliations• Similar results in other biomedical research – affiliation with
industry is best predictor of pro-industry finding (odds ratio 3.60)• Artist study?• Barnes et al. JAMA 1998;279:1556• Bekelman et al. JAMA 2003;289:454

Accuracy of Advertising
• 69 journal advertisements• 50.2% claims provided no source to support• When sources cited, 65% claims supported• Efficacy claims supported 53.2%• Can you believe claims in medical journal ads?
– Flip a coin• Spielman et al. J Nerv Ment Dis 2008;196:267

Physicians and the Pharmaceutical Industry
• Relationship(s) often mutually beneficial• Gifts• Educational funding• Research support• Information• Samples

Gifts from the Pharmaceutical Industry
• Industry spends approximately $10,000/physician/year
• 97% residents carry at least one item with industry logo
• Six gifts/year• 14 meals/year
– Much higher at MCCG• Wazana and Primeau Psych Clin N Am 2002;25:647

Steinman et al. Am J Med 2001;110:551

Industry CME and Prescribing Patterns
• $2.45 billion spent on continuing education for health professionals in 2006– $1.4 billion paid for by industry (57%)
• After event, 4-5x greater prescribing of product

Formulary Requests
• 40 physicians who requested a formulary addition from January 1989 through October 1990. Control physicians were 80 randomly selected physicians who had not made requests.
• Physicians were more likely to have requested that drugs manufactured by specific companies be added to the formulary if they had met with pharmaceutical representatives from those companies (OR, 13.2; 95% CI, 4.8 to 36.3) or had accepted money from those companies (OR, 19.2; 95% CI, 2.3 to 156.9)

Pharmaceutical Research and Manufacturers of America (PhRMA) Guidelines
• Pre-2002– Golf, honoraria for attending presentations, trips, games
• 2002– Meals modest, without guests– Gifts of modest value (<$25-100) and primarily of benefit
to patient care or practice• 2009
– No gifts (pens, notepads, stethoscopes, lights, etc.) which have value independent of patient education
– May have office meals

AMA and the Pharmaceutical Industry
• Gifts should primarily entail a benefit to patients and should not be of substantial value
• Individual gifts of minimal value are acceptable if work-related
• Some are calling for rejection of all gifts, meals, speaking honoraria, GME support
• Supports National Clinical Trials Registry– Trials begun after 7/05 will be considered for publication
only if publicly registered

Marcia Angell
• “It would be naïve to conclude that bias is only a matter of a few isolated instances. It permeates the entire system.”
• “Physicians can no longer rely on the medical literature for valid and reliable information.”
• “Clinicians just do not know anymore how safe and effective prescription drugs really are, but the products are probably nowhere near as good as the published literature indicates.”– Angell M: JAMA 300. 1069-1071.2008

AMSA Scorecard
• Conflict of Interest Policies at Academic Medical Centers (http://amsascorecard.org/)
• Gifts/Industry relationships– Gifts, consulting, speaking, disclosure
• Samples, purchasing, access• Education
– On/off campus, industry support, curriculum• MUSM Grade “C”• `Not widely disseminated to faculty/trainees

Abuse and Impairment of Medical Students and Physicians
Richard L. Elliott, MD, PhD, FAPAProfessor, Internal Medicine
Director, Medical EthicsMercer University School of Medicine

Goals
• Special ethical situations affecting students– Abuse– Role of students and rights of patients– Reporting errors– Boundary issues with faculty
• Physician Impairment• Review of Step One Ethics – Spring 2010?

Can you spot the pimp?

The Art of Pimping
• To pimp: verb. To ask a series of progressively arcane and distantly related questions. The purpose is to establish or confirm power.– Historical, anatomical, physiological, clinical, eponomical,
characterological, hierarchical
• Responses: bluffing, feigned erudition• Brancati FL. The art of pimping. JAMA. 1989;262(1):89-90.• Detsky AS. The art of pimping. JAMA 2009;301:1379-81

Wounded Knee Massacre• Senior resident asked me to tap a knee when I was
an intern• Had tapped bellies, spines, chests, never knee• Didn’t know landmarks, procedure• Many (!!) medical students, nursing students invited
to watch• Improper technique led to extremely painful tap• Resident told group “That’s what you get from a
psychiatrist.”• Later I learned he had never tapped a knee, was
afraid to ask attending

Abuse of Students• Approximately 50% students report significant abuse• Clinical
– Exposure to risk management problems• Informed consent• Improper procedure techniques• Breaches of confidentiality
• Teaching– Humiliation
• 24% first year students, 55% 4th years viewed derogatory comments about patients as appropriate – patient abuse?
– Sexual harassment– See one, do one, teach one – always true?
• Research– Authorship

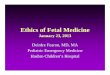
Copyright ©2006 BMJ Publishing Group Ltd.
Frank, E. et al. BMJ 2006;333:682
Proportion of medical students experiencing harassment or belittlement at entry to wards or in senior year

Decline of Ethical Values During Medical School
• Four studies show leveling or decline in moral reasoning during medical school
• Idealism shifts to self-interest– What does this mean for me?– Fear and blame as motivators– Fatigue– Coping with difficult patients– Effects of role models
• Interns and residents as teachers• Most student abuse comes from house staff

Understanding the clinical dilemmas that shape medical students’ ethical development
• Experiences constitute a “hidden ethics curriculum”• May or may not be consistent with desirable ethics
content• Happens frequently
– 61% of students witnessed clinical faculty acting unethically at least occasionally
• What are some of these ethically problematic situations?
• What should you do when faced with problematic ethical situations involving teachers?

Examples of potential abuse?


Definitions of Impaired Physician
• “unable to practice medicine with reasonable skill and safety to patients because of physical or mental illness, including deterioration through the aging process or loss of motor skill, or excessive use or abuse of drugs including alcohol.” (AMA)
• “inability to exercise prudent medical judgment and the ability to practice with reasonable skill and safety without jeopardy to patient care” (AAFP)

Examples of Impairment
• Substance abuse• Mental Illness• Cognitive• Personality traits
– Boundary violations• Physical condition
– Motor– Visual

Impaired Physician - Epidemiology
• Overall – 10-15% lifetime risk of becoming impaired
• Substance abuse – 90% of impaired physicians– 8-10% lifetime risk– 2% current
• Mental Illness – 8% of impaired physicians• No greater than general population except 30-100
times greater risk of narcotic addiction

Impaired Physician - Trainees
• Medical students: 11% with excessive alcohol use during at least one 6-month period, 18% with alcohol abuse during first two years
• 30% residents report depression with suicidal ideation in previous two weeks
• 14% students reported suicidal thoughts in previous year
• Only 22% of depressed students received treatment

Medical Student Impairment
• N Engl J Med 353;25 December 22, 2005 2673• 235 physicians disciplined by medical boards matched with
469 physicians who graduated from the same school and year• Students who were described as having unprofessional
conduct during medical school were 3 times more likely to be disciplined, with a risk of 26%.
• Risk factors during medical school for future disciplinary action included irresponsibility (lack of accountability) and lack of capacity for self-improvement

Impaired Physician – Risk Factors
• Problem behaviors, low test scores, drug use in medical school predict problems in residency and later
• Sensation seeking and paternal history predict substance abuse in students
• Sleep – drugs to sleep or stay awake• Access – narcotics• Stress – school, family, burnout• Specialty – anesthesia, ER – x3• Pharmacological optimism, reliance on intellect,
strong willed, high “T”

Impaired Physician - Recognizing
• Personality changes– Patient and staff complaints– Sleep problems– Erratic performance and behavior– Burn out – 50% of physicians– Absences, odd hours– Errors and unusual practices– Irritability, moodiness


Physician Mortality
• 1261 physicians, graduated 1948-1964, studied through 1998
• Overall mortality 56% lower in men, 26% lower in women
• Suicide 82% greater in men, 395% greater in women
• DM Torre et al. Suicide compared to other causes of mortality in physicians. Suicide and Life-Threatening Behavior. 2005;35:146-53

Aid for the Impaired Medical Student (AIMS)
• MUSM Medical Student Handbook • Goals
– Provide assistance before irreversible harm– Protect rights of students to receive treatment in
confidence– To ensure recovered students can continue
education without stigma or penalty– To protect others affected by impaired students– Prevent future cases of impairment

Aid for the Impaired Medical Student (AIMS) II
• Administered by AIMS Council (8 students, 4 professionals)
• Referral to AIMS student representative• Class representatives and professional
member review circumstances, interview student, recommend action
• Professional member monitors follow-up

Impaired Physician - Interventions
• Key is recognition – colleagues must overcome denial, reluctance, desire to be “discrete”
• Personal vs. formal intervention• Thorough assessment – high co-morbidity• Physician-focused treatment (e.g., Ridgeway,
Caduceus)• Anticipate relapse and determine consequences• Long term monitoring• Address specific issues – (e.g., burnout)

Impaired Physician - Reporting
• AMA “Physicians have an ethical obligation to report impaired, incompetent, and/or unethical colleagues in accordance with the legal requirements in each state”– August 29, 2005, AMA E-9.031
• Reporting not mandatory in Georgia

Impaired Physician – Outcomes
• Risk of relapse related to family history, opioid use, co-morbid psychiatric disorder
• California – 73% drug free more than two years• Missouri Physician Health Program –90% recovery• Anesthesia – 56% success, 40% entered another
specialty, 5% mortality within several years

Physician Health Program
• Physicians Well-Being ProgramMedical Association of Georgia
• 339 Tenth Street, NWAtlanta, GA 30318-5681
• (404) 875-1061• Fax (404) 875-3084• email [email protected]• George D. Miller, MD, Medical Director• Types of disease, illness, or conditions monitored:
– Chemical dependency – Mental health – Behavioral health problems – Sexual misconduct and/or boundary violations – Physical illness

Georgia PHP – Chemical Dependency
• Length of contract: 5 years • Random urine drug screen frequency:
– Year 1: 1 time per week – Year 2: 1 time per month – Year 3: 1 time per month – Year 4: 1 time per month – Year 5: 1 time per month
• Support (self help) group requirements:– AA,,NA, Caduceus, Other: IDAA
• Support (self help) group frequency:– Year 1: 3 times per week – Year 2: 3 times per week – To completion: 2 times per week
• Therapy or treatment requirement: peer group required, other Tx as directed by provider• Work or practice monitor requirement: once weekly contact (minimum)• Other provisions: monthly monitoring meeting with program representative

Georgia PHP – Mental Health
• Length of contract: 5 years • Support (self help) group requirements: professionally
facilitated• Support (self help) group frequency: as directed by
participant's psychiatrist of record• Therapy or treatment requirement: as directed by
participant's psychiatrist of record• Work or practice monitor requirement: weekly contact• Other provisions: as needed• Other monitoring services provided: as needed, committee
monitor (quarterly), worksite monitor, therapeutic monitoring groups, hair analysis, naltrexone


Slides from this point on were not part of the presentations

USMLE #3• A 95-year-old woman in a nursing home has had advanced
vascular dementia, severe dysphagia, and a 9-kg (20-lb) weight loss over the past 2 months. Her four children are divided regarding the decision to provide artificial feeding through a gastrostomy tube. There is no living will. The oldest son approaches the physician after a family meeting and says, “You should simply decide what is best for her and tell the others that’s what we should do.” Assuming the physician proceeds in this manner, which of the following best describes the physician’s action?

Best Interest Standard
• Paternalism• Preserving fairness in use of resources• Protecting patient autonomy• Rationing care• Truth-telling

USMLE #4
• You are a psychiatrist and Mr. Moore is your patient. Mr. Moore has been talking to you for some time about his neighbor who, he believes, has it in for him. He tells you that he plans to get his revenge. He tells you he plans to kill his neighbor.

Tarasoff – Duty to Protect
• Which is the best course of action?– Inform the police of this threat.– Inform the patient’s neighbor– Inform both the police and the patient’s neighbor– Inform no one but focus on treating the
underlying illness

USMLE #6
• You are preparing a clinical trial of different doses of a certain medication. This medication has already been proven to be clinically effective and is already approved by the FDA. You are only studying to see whether a higher dose of the medication will lead to enhanced benefit.

Tuskegee• The Tuskegee Study of Untreated Syphilis in the Negro Male
– Do whites and blacks differ in disease course?• Treatment planned, cut due to cost• Participation of Tuskegee Institute, black nurse eased fears among men• Macon County Medical Society, mostly black physicians, agreed to deny
treatment• Treatment – arsenic, mercury, ASA, iron, spinal taps – perceived as far
superior medical care than usually received• Later, men denied free care for syphilis at PHS clinics• Study continued after Nuremberg and Declaration of Helsinki (1964)• Expose 1972 ended the study• $10 million settlement• IRBs established• Legacy of mistrust between blacks and whites in research

Where is Tuskegee Today?
• Vulnerable populations and research• AIDS in Africa
– Is use of a placebo ethical?• Children
– Proxy consents

Mortality and Vioxx
• Data submitted to FDA concluded no significant risk
• Intent-to-treat deaths in RCTs for Alzheimer’s– Subjects 34/1069– Placebo 12/1078 – Hazard ratio 2.99
• JAMA 2008;299:1813

Policy on the rights of patients in medical education (BMJ)
• For educational activities not part of clinical care:– Patients must understand that medical students are not
qualified doctors (and not "young doctors," "my colleagues," or "assistants").
• What about interns? Unlicensed physicians? Non-board certified physicians? Do all patients understand the distinctions?
– Clinical teachers and students must obtain consent from patients before students take their case histories or physically examine them, making sure they understand the primarily educational purpose of their participation.
• What is “primarily educational?” Students are valuable history takers, examiners, etc.

BMJ Patients’ Rights II• Never perform examinations or present cases that are
potentially embarrassing for primarily educational purposes without the patient's consent. When individual students are conducting such examinations a chaperone should usually be present.
• Students should never perform examinations on patients under general anesthetia for primarily educational purposes without patients' consent. Patients who are unconscious or incompetent must be involved in primarily educational activity only with the explicit agreement of their responsible clinician and after consent from parents (children) or consultation with relatives (adults).

BMJ Patients’ Rights III• Clinical teachers should obtain patients' consent for students to
participate in treatment (suturing, taking blood, delivering babies, etc.). Procedures not requiring immediate supervision should be undertaken only if there is recorded evidence of competence. – How, where, and by whom is this recorded? How will this be available
to subsequent attendings? Missions work!• Students must respect the confidentiality of information communicated by
patients. Patients should understand that students may be obliged to inform a responsible clinician about information relevant to their care. – Do we lose placebo (non-specific therapeutic) effect?
• Clinical teachers are responsible for ensuring that these guidelines are followed. If students are asked by anyone to do the contrary, they must politely refuse, referring to these guidelines.
• Anyone want to do research on compliance with these?