Embed Size (px)
Citation preview
Ethics and Managed Care
Where did it go wrong? (If it did?)
Louis Harris Poll, 1980
97% of HMO enrollees satisfied, would renew
30% of non-members find HMO concept very attractive
WARNING
The following slide contains adult language.
“Fucking HMO bastard pieces of shit!”
--As Good As It Gets (1997)
You know you’ve joined a cheap HMO when….….They give you Viagra tablets in different colors with little “m’s” on them.
--David Letterman
What is managed care?
Same organization combines two functions Insurance Delivery of services
Specified, covered populationProspective financing of services
from a limited budget•Buchanan, 1998
The first HMO’s
1940’sEither labor union-driven or community
cooperative (all non-profit)Payment per member per month
(capitation)Financial incentive to keep people
healthyGroup practice/clinic model
Turning Point: 1970-1980
Health care share of GDP went up from 4% to 10-12% since 1945
Big Three realized they were paying more on a per-car basis for health care than for steel
For first time, HMO’s attractive as a way to cut costs, not as a way to change the direction and quality of care
1980-2000
New Federal legislation encourages creation of HMO’s
Some evidence early that this led to a slow-down in rise of health costs (temporarily)
Suddenly for-profit managed care is the fastest growing segment of industry
Kaiser plan, 1970
Has served same population for 30 yearsVery stable group of physicians and staffMost work there out of choiceWork as team to assure that quality of
care is kept highThe “competition” is very wasteful, so
even a modest trimming of costs makes Kaiser the best deal
Acme HMO, 2000
May have been created yesterdayPhysicians are tied in “virtual”
network, no history of teamworkRapid turnover of patients, no way to
capture savings from preventive care
Competition lean and mean; can’t compete unless costs cut to the bone
Does the term “managed care” specify an entity with a constant, predictable set of ethical problems?
Basic ethical problem
Physician or nurse as “gatekeeper”Gatekeeper may recommend care as
“medically necessary” or not Plan pays for “medically necessary”
careIf less care recommended, staff may
make more money (or may be retained, not fired)
RationingBedside Rationing
RationingThere is a limited amount of resources
availableNeed/demand exceeds the available
resourcesWe must have SOME system to decide who
gets how much Ability to pay Lottery Degree of need Etc.
Where Rationing Occurs
AdministrativeLevel
Bedside Level
Administrative Rationing
Policymakers set very general guidelines based on data of effectiveness and cost
Physicians at bedside merely apply those guidelines with virtually no discretion
Examples: No one over age 70 gets renal dialysis No one gets expensive anti-ulcer medication
for more than 2 months
“[I]t is society, not the individual practitioner, that must make the decision to limit the availability ofeffective but expensive types ofmedical care.”
--Norman Levinsky (p. 102)
Bedside Rationing
Physician/nurse caring for individual patient
Makes a decision not to provide some treatment
Decides on basis of relative need of this patient vs. other patients in “plan”
Trust and Rationing
Levinsky’s argument:If administrative rationing, physician is
still uncompromising in personal dedication to patient welfare
If bedside rationing, physician a double agent-- willing to compromise patient welfare in name of cost saving or service to “society” (= other patients)
Fee-for-service practice
Patient (or insurance company) paid a set amount for each service
Strong financial incentive for physician to recommend or perform unnecessary services Return office visits Unnecessary surgery Unnecessary labs, x-rays
No one has yet designed a way of financing health care that pays the providers when, and only when, they do something beneficial for the patient
--so every plan has some perverse incentives
Is Less Care the Problem?
Assume ethical flaw in managed care is that physician is rewarded for doing less for the patient
Assumes that more care is always better care
If so, should see consistent trend in research for managed care to have worse outcomes (not so)
One Example: ABMTABMT for advanced breast cancer:
thought to provide 10-15% chance of survival when all else has failed
Costs ~ $150,000Many women sued HMOs successfully
when ABMT denied because “experimental”
Latest research-- ABMT adds nothing to survival in advanced breast cancer
The real question
Is gatekeeping ethical?
Can gatekeeping be avoided?
What is Gatekeeping?
Physician cares for a population of patients
Limited budgetIf patient #1 gets something, there
is something that the other patients will not get
Comparative judgments of relative priorities of need among patients
Example 1. ICU nurse
Nurse has 2 patientsMr. Smith: Just about ready to transfer
out but has a lot of questionsMrs. Jones: Acutely unstable,
impending multiple organ system failure; unsure of cause
Who will you spend more time with?
Example 2. Primary care office
NP has waiting room full of patientsMrs. Green: Has a 10-min appointment,
starts to complain of several new problems which she has had for years
Mr. White: Has a 10-min appointment; “Oh by the way” chest pain
Will you reschedule or run overtime?
Inevitability of Gatekeeping
Time and not just money is a limited resource
So long as you have more than one patient in your practice, you must always make tradeoffs among needs of different patients
Seems reasonable to make tradeoffs based on best assessment of relative need
Inevitability of Gatekeeping (Morreim)
Policy-makers write clinical guidelines to save money and maintain quality
All guidelines have “wiggle room”Physician must decide whether to
adhere to guideline or try to declare this patient an exception-- both “bedside” decisions impact on resources available to other patients
Eddy’s Argument
Two positionsFirst position: I am generally healthy,
my chances of getting any one particular disease are relatively low
Second position: I already have developed an advanced disease
30yo Healthy Woman
Would rather have lower premiums and put money in kid’s college fund, etc.
Strong interest in funding preventive care e.g. mammograms
Little interest in funding “desperation” care like ABMT
45yo Woman with Metastatic Breast Cancer
Prevention is now of no use“I’ve paid my premiums for all those
years; now it’s my turn to get something back”
Strong interest in having funding for “last ditch” measures even if low likelihood of success
Eddy: The Conflict
Should we interpret the ethical question as “the patient vs. society”?
Or is it ourselves at one point in our lives vs. ourselves at another point in our lives?
If the latter, which of the two positions is ethically privileged in terms of taking a moral priority for health policy? Eddy argues: First position
When is Gatekeeping Unethical?
Very generally-- when financial incentives are so intrusive into physician’s thoughts that she is highly likely to place financial concerns ahead of concerns for the well-being of the patient
Bowman Case (TN)
Prisoner died of pneumonia; had known sickle cell disease
For profit prison management firm had capitated contract with physician
By denying care physician could double his annual income
No “carve out” for prisoners with known serious illnesses
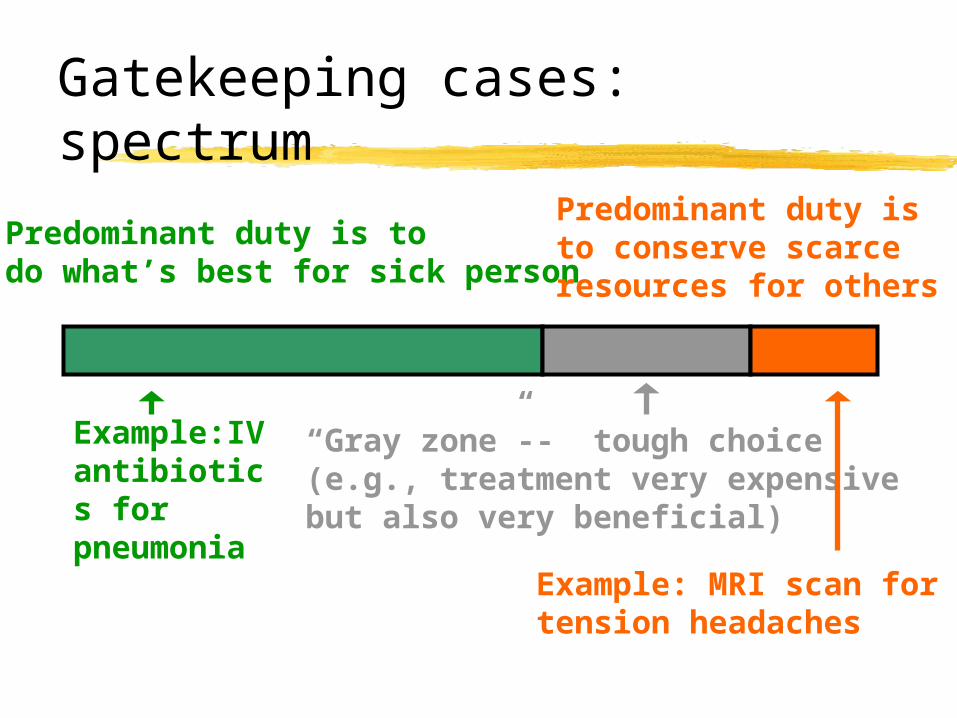
Gatekeeping cases: spectrum
Predominant duty is todo what’s best for sick person
Predominant duty isto conserve scarceresources for others
“Gray zone”-- tough choice(e.g., treatment very expensive but also very beneficial)
Example:IV antibiotics for pneumonia
Example: MRI scan fortension headaches
For-Profit Managed Care
Is this form of financing inherently unethical?
Is a for-profit plan inherently less trustworthy?
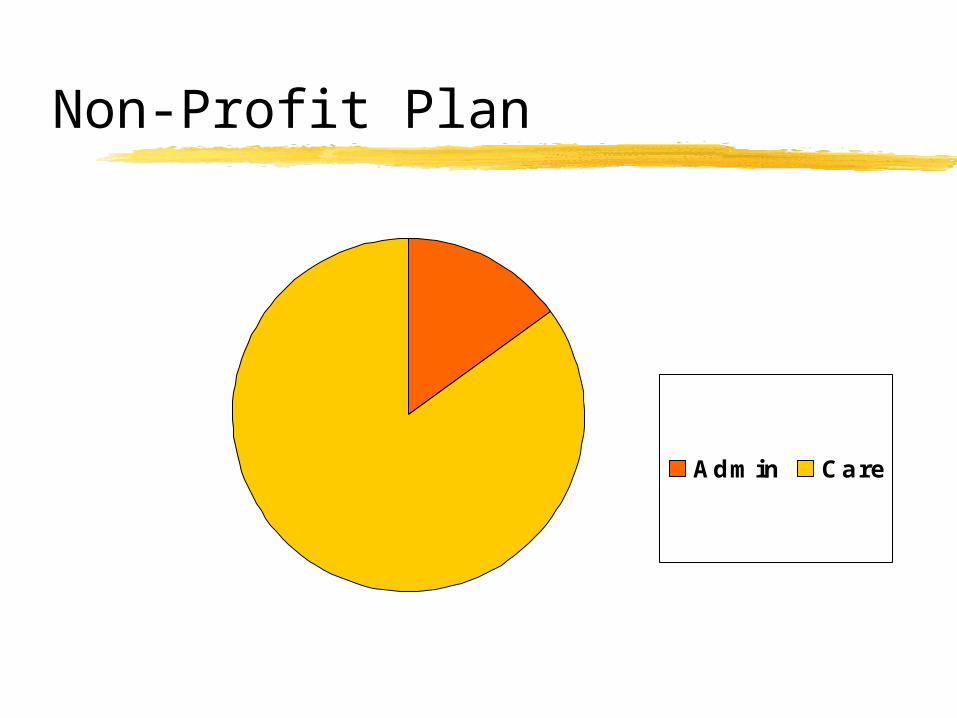
Non-Profit Plan
Admin Care
For-Profit Plan
Admin
Care
Dividends
For-Profit vs. Nonprofit
Unless for-profit plans considerably more efficient, they will have less $ to spend on care No evidence of such efficiency
BUT at least a few non-profit plans spend less on care than a few for-profit plans, tho on average NP spends greater percentage than FP