Embed Size (px)
Citation preview

In April 2007, all state public health directors sub-mitted their pandemic influenza preparednessplans to the Centers for Disease Control (CDC), in
response to an assignment and template from theNational Strategy for Pandemic Influenza, coordinatedby the Departments of Health and Human Services(HHS) and Homeland Security. Officials wererequired to describe how they will deploy public agen-cies and private sector partners in the event of an out-break, and in coordination with federal agenciesresponsible for surveillance, vaccine development, thedistribution of antiviral medications, and restrictionsaimed at controlling the spread of the virus. The fed-eral agencies will review and score the states’ plans.
In June 2007, the American Journal of Public Healthpublished a survey of the federal and state pandemicplans published to date.1 The authors of this reportnoted that the federal template and scoring criteriadid not require states to be specific about the ethicaldecisions that are integral to pandemic planning andto public health and safety during a crisis. As a result,few plans contain concrete guidance on how offi-cials and first responders can make ethical deci-sions—fair decisions—under immense pressureduring a sustained crisis, or on how to allocate lim-ited resources fairly. While the CDC has publishedrecommendations for rationing vaccines and anti-viralmedicines, these are not the only scarce goods and
Bioethics BackgrounderEthical decisionmaking during an influenza pandemic
The Hastings Center
The Five People You Meet in a Pandemic—and What They Need from You Todayby Nancy Berlinger and Jacob Moses, The Hastings Center
Additional copies of this Bioethics Backgrounder can be downloaded at www.thehastingscenter.org or atwww.providence.org/oregon/Programs_and_Services/Ethics/Default.htm.
Who’s got the plan?
The national Pandemic Influenza Preparednessand Response Plan10 describes the followingresponsibilities of the Federal government during apandemic:
• Surveillance• Epidemiological investigation • Development of lab tests• Vaccine development, testing, evaluation,deployment, safety evaluation; deployment ofantiviral agents in the Strategic National Stockpile • Enacting travel or other quarantines• Facilitating medical and public health communi-cations
The Federal plan requires that state plans cover11 :• Identification of public and private sector part-ners needed for effective planning and response• State coordination with federal efforts aimed atsurveillance and infection control• Integration of pandemic influenza planning withother public health planning activities overseen byfederal agencies, including the CDC’s PublicHealth Preparedness program and the HealthResources and Services Administration (HRSA)’sHospital Preparedness program• Coordination with local authorities, such ascounty and city public health departments, toassist in developing local plans on which stateplan depends• Development of data management systems• Coordination with adjoining jurisdictions, includ-ing other states and regional authorities
This publication was produced incollaboration with The ProvidenceCenter for Health Care Ethics atProvidence Health and Services
and made possible through a generous grant from theProvidence St. Vincent Medical Foundation.

services that will need to be distributed fairly during apandemic.2
The ethical duty to planWhen a wave of influenza deaths begins in a com-
munity, it will be too late to start thinking aboutethics, or to alter public health and medical and othersocial systems so care is organized more ethically.Foreseeable ethical challenges—how a communitywill make fair decisions about using scarce resources,protecting public health, and keeping basic servicesrunning—must be discussed today.3
The ethical duty to develop rules and tools formaking fair decisions
To be fair is to provide individuals and groups withwhat they need: food, water, shelter, health care, safe-ty, information, justice. A public health emergency willrequire rationing of these necessities in the interest ofthe community’s survival. When planners know therewill not be enough of what people will need, they havea duty to create and test the rules and tools that willhelp first responders make fair decisions during a cri-sis. Samples of rules and tools are included in thisdocument. Deciding what “trigger”—such as the dec-laration of a state of emergency by a state’s gover-nor—will alert first responders to the epidemiologicalconditions that authorize them to begin using thesepandemic guidelines and other rules and tools areamong the responsibilities of pandemic planners.
The ethical duty to be accountable to one’s com-munity
Every community member has a stake in its pan-demic plan, because every community member has astake in the community’s survival. Planners have aduty to make their ethical reasoning clear, and toshare it with community members. They can do thisthrough public meetings, by posting draft versions ofrules and tools on websites for public review and com-ment, and by including experts in communication andpublic education in planning activities.
The “five people”The “five people” described in this document are
representative community members who are firstresponders. Each will have particular duties during apandemic. Each will rely on planners to anticipate and
2
Flu FactsGood ethics starts with good facts. Here are the cur-
rent facts, and expert opinions, on the potential for flupandemic:
• International public health experts agree that anew flu pandemic—possibly triggered by a mutat-ed avian flu such as H5N1—is inevitable; that cur-rent vaccine stockpiles are incapable of preventing afuture outbreak; that current antiviral drugs will beeffective only in limited conditions; and that thenation’s hospitals do not have enough ventilators forpatients who will be sick enough to need them.
• According to the CDC, more than 60 countries haveconfirmed cases of H5N1 in animals.12 The WHOreports 319 cases of H5N1 among humans, resultingin 192 deaths from H5N1 to date.13 Although its trans-mission rate among humans is still low, H5N1 has afatality rate of more than 50%. The 1918 flu had afatality rate of just 2%—and killed 50-100 million peo-ple.14, 15
• Reconstructions of the 1918 flu strain (H1N1) sug-gest that flu strains that cause acute inflammation canalso make flu victims vulnerable to opportunistic, con-tagious infections such as bacterial pneumonia. H5N1shares a similar pathology to H1N1.16
• H5N1 is just one flu strain capable of mutating into apandemic-causing virus. It receives much of the scien-tific and public health attention because it has alreadyspread from birds to humans—and in very rare casesfrom humans to humans.17 Failures to control other flustrains within bird populations, and the rapid growth ofpoultry-processing industries worldwide, are increas-ing the likelihood that a pandemic strain will develop.18
• In April 2007, the FDA approved the first vaccineagainst avian flu.19 At this time, the federal govern-ment purchased enough vaccine for the NationalVaccine Stockpile contained enough of the vaccine totreat 6.5 million people: the target is 20 million stock-piled doses for public health workers. However,experts strongly question the vaccine’s usefulnessand effectiveness.20, 21 Effectiveness could be furtherreduced by the rapidly mutating nature of a flu virus:the virology of a pandemic strain would certainly differfrom the H5N1 strain the stockpiled vaccine has beendesigned to combat.22 At most, the stockpile will pro-vide a stopgap in the initial days of an outbreak until amore effective vaccine can be developed from theactual pandemic strain.23 It will take 6-8 months fol-

discuss ethical challenges; to develop ways to makefair rationing decisions; and to be transparent before,during, and after the crisis. Planners can use thesefive people as tools for their own discussions—andmay identify other representative community mem-bers who will rely on them.
From well-meaning words to real frameworks forreal communities: the regional public healthplanning challenge
An influenza pandemic will force first responders,including health care workers, to think and act differ-ently than they normally do. In a crisis, they needclear protocols to follow. But if these rules seemunfair, or don’t match the situation at hand, the bur-den on first responders will be excruciating. As a soci-ety, we must not shift the burden of deciding how tobe fair onto the same first responders we will rely onto treat the sick and maintain public health and safety.
Pandemics do not respect boundaries. What hap-pens in one city, county, or state will affect its neigh-bors. Yet home-rule traditions are strong: we havenow had 50 separate conversations about pandemicplanning.
We have also had 5,000 other conversations, as thenation’s hospitals developed their own pandemicplans. While some hospitals have collaborated in plan-ning with their competitors, others have worked inisolation. A pandemic will force competitors tobecome collaborators.
We are now having 3,066 more conversations, aseach county public health department grapples withregional planning needs, at the level where state plansand local health and safety resources must meet.Major cities in multi-county and multi-state regionsare also responsible for integrating federal and stateplans with the plans drafted by area hospitals.
Regional planners at the civic, county, multi-county,and multi-state levels must identify gaps in state andfederal plans, including the absence of clear ethicalguidance. They also need to identify gaps in theirlocal hospitals’ plans: are hospitals in the same regionworking from the same epidemiological models, orare they planning for different pandemics? Are somehospitals better prepared or better equipped than oth-ers? How can regional planners encourage collabora-
3
lowing the identification of the outbreak strain for aneffective vaccine to be available.24
• The antiviral Tamiflu is effective only when takenwithin the first 12-48 hours following the onset ofsymptoms.25 Tamiflu-resistant flu strains have beenidentified.26
• When pandemic influenza hits, most hospitals’ venti-lators will already be in use by critically ill patients.Rationing access to available ventilators—and to oxy-gen and staff to operate them—will be an inevitablepart of patient care during a pandemic.
Experts also agree that a pandemic will profound-ly disrupt daily life. If vaccine supplies are limited tothe most essential workers, the most effective publichealth strategy will be restrictions on public gatherings,and quarantine. Few living Americans have ever experi-enced these conditions for sustained periods.
Discussing how compromised communities will func-tion during a prolonged public health emergency, howemergency policies can protect—or harm—vulnerablegroups within communities; and who will be capable ofand responsible for making fair decisions as they ariseduring a prolonged crisis, is part of the ethical duty toplan.
• CDC guidelines released in 2007 recommend clos-ing schools, canceling public gatherings, staggeringworking hours and voluntary quarantine in the event ofan avian flu outbreak.27 According to a report by theTrust for America’s Health report, the US economycould lose three working weeks of productivity fromworkers who are ill, are caring for sick family mem-bers, or are unable to get to work.28
• As normal infrastructure and supply chains are dis-rupted by illness or quarantine, communities may faceshortages of clean water, safe food, utilities, and othernecessities. Hospitals will face the same shortages asthey care for waves of patients and attempt to main-tain safe conditions.29 The secondary consequencesof a pandemic—such as outbreaks of diseases asso-ciated with poor sanitation or with interruptions inaccess to primary care, and the disruption of outpa-tient care for persons with chronic conditions—havethe potential to damage the public’s health beyond theobvious threat of pandemic influenza itself.

4
tion between hospitals with greater resources andthose with fewer resources? And because pandemicplans must describe how basic services will be deliv-ered during a sustained public health crisis, regionalplanners need to know how to create comprehensive,practical plans that are also ethically sound, plans thatfirst responders can trust and the public can support.
In September 2006, The Providence Center forHealth Care Ethics and The Hastings Center part-nered to convene a meeting of public health officials,experts on public health ethics and clinical ethics, andclinicians to discuss the challenge of building pan-demic plans on an ethically sound framework. TheProvidence Center for Health Care Ethics atProvidence Health and Services, a system based inthe Pacific Northwest that includes 26 hospitals, morethan 35 other health care facilities, and 45,000 employ-ees, funded the meeting through a grant from theProvidence St. Vincent Medical Foundation.
This expert group identified several ongoing prob-lems with how pandemic plans, and other disasterplans, handle ethics:
PPllaannss mmaayy iinncclluuddee pprriioorriittyy lliissttss wwiitthhoouutt jjuussttiiffyyiinnggwhy cceerrttaaiinn iinnddiivviidduuaallss oorr ggrroouuppss aarree ggiivveenn pprriioorriittyyaacccceessss ttoo ssccaarrccee rreessoouurrcceess..
A pandemic plan that is ethically sound describesdifferent resource allocation scenarios, selects one,justifies this selection in terms of epidemiologicaldata, available resources, the public’s health and wel-fare, and the interests of groups affected by the plan;and is clear about who made these decisions. Itdescribes how this plan will work in practice. It makesthe plan available to the public for review and com-ments. And it identifies the “trigger” that puts the planinto effect. By being clear about the trigger, publicofficials take responsibility for switching the practiceof medicine in their community from “clinically appro-priate” under normal circumstances to “ethicallyappropriate” under emergency rules. New YorkState’s Allocation of Ventilators in an InfluenzaPandemic Guidelines is an example of a resource allo-cation plan that fulfills all of these conditions.4
PPllaannss mmaayy ffaaiill ttoo aacckknnoowwlleeddggee tthhee eexxiissttiinngg ddiissppaarriittiieessooff iinnccoommee,, rreessoouurrcceess,, hheeaalltthh,, aanndd aacccceessss ttoo hheeaalltthh ccaarree,,
Carol Bayley, PhDSenior Vice President for Ethics and JusticeEducationCatholic Healthcare West
Kenneth A. Berkowitz, MD, FCCPChief, Ethics Consultation ServiceVA NY Harbor Medical Center
Nancy Berlinger, PhD, MDivDeputy Director and Research Associate, The Hastings Center
Roger Bernier, PhD, MPHSenior Advisor For Scientific Strategy andInnovationNational Immunization Program, MS E-05Centers For Disease Control and Prevention
Jennifer Gibson, PhDLeader, Clinical and Organizational EthicsStrategic InitiativesCoordinator, Canadian Priority SettingResearch NetworkUniversity of Toronto Joint Centre forBioethics
Amy Haddad, PhD, MSNDirector, Center for Health Policy and EthicsCreighton University Medical Center
L. Lee Hamm, MD, FACPProfessor and Vice Chairman, Department ofInternal MedicineTulane University School of Medicine
Robin Hemphill, MDAssociate Professor of Emergency MedicineVanderbilt University Medical Center
Stephen Ivy, PhD, MDivSenior Vice President, Values, Ethics, SocialResponsibility and Pastoral ServicesClarian Health Partners
Nancy E. Kass, ScDPhoebe R. Berman Professor of Bioethics andPublic HealthJohns Hopkins Bloomberg School of PublicHealth
Thomas H. Murray, PhDPresident, The Hastings Center
Tia Powell, MDDirector, New York State Task Force on Lifeand the Law
Virginia Ashby Sharpe, PhDMedical Ethicist, National Center for EthicsVeterans Health Administration
Daniel Sulmasy, PhD, MD, OFMDirector, Bioethics InstituteNew York Medical College
Sr. Patricia A. Talone, PhD, RSMVice President, Mission ServicesThe Catholic Health Association
Mark Tonelli, MDAssociate Professor of Medicine, Pulmonaryand Critical Care MedicineUniversity of Washington Medical Center
Rev. John Tuohey, PhD, MDivDirector and Endowed Chair, Applied HealthCare EthicsProvidence Center For Health Care Ethics
Matthew Wynia, MD, MPHDirector, The Institute For EthicsAmerican Medical Association
Meeting Participants The Hastings Center, September 25, 2006
Affiliations for identification purposes only.

5
oorr mmaayy ffaaiill ttoo ddeessccrriibbee eeffffoorrttss ttoo aavvooiidd wwoorrsseenniinngg tthheesseeddiissppaarriittiieess..
An ethically sound plan must describe how existingresources will be fairly distributed across communi-ties, and between competitors, during a public healthemergency. Again, New York State’s ventilator alloca-tion plan is a good example of how this can work inpractice. In that state, a standing bioethics task force,reporting to the governor, was available to work withhospitals, experts in bioethics, infectious disease, dis-aster medicine, and legal and public health authoritiesto develop a fair plan for ranking patient access to ven-tilators under the dire circumstances of a pandemic.
However, not all states have a standing bioethicstask force with professional staff, available to helpregional planners and health care institutions analyzecomplex emerging health care problems and theirpotential to worsen health and health care disparities.Public health officials in regions that include bothaffluent suburbs and lower-income cities may havedifficulty getting members of these communities toacknowledge their interdependence, and the infra-structure linking them.
And because chronic health problems, such asasthma or diabetes, may be more common in somepopulations than in others, failure to acknowledgeexisting health disparities now means that membersof these “sicker” populations will likely have lessaccess to scarce resources during a pandemic: theymay be less able to get to a hospital, or less likely tobe high priority for a ventilator should they need it.They may be more likely to die. Health care profes-sionals and community members who deal withendemic chronic disease may ask whether planningfor a disease that is not yet threatening their commu-nities will direct funding and attention away fromthose diseases that already threaten them. Plannersmust acknowledge these concerns.
PPllaannss mmaayy ffaaiill ttoo eexxppllaaiinn hhooww ppuubblliicc hheeaalltthh eetthhiiccss,,wwiitthh iittss eemmpphhaassiiss oonn ffaaiirr ddiissttrriibbuuttiioonn ooff lliimmiitteeddrreessoouurrcceess,, ddiiffffeerrss ffrroomm eevveerryyddaayy cclliinniiccaall eetthhiiccss,, wwiitthh iittsseemmpphhaassiiss oonn pprrootteeccttiinngg tthhee rriigghhttss ooff iinnddiivviidduuaall ppaattiieennttss..
“Ethics” means different things in different healthcare contexts. Behaving ethically in ordinary clinicalcircumstances leads us to focus on individual patientpreferences and values. Behaving ethically in a disas-
ter may shift the balance toward doing what is bestfor the community as a whole. Plans that will go intoeffect during particular types of disaster must antici-pate the particular challenges the community willface, and must offer ethical guidance relevant to thesechallenges.
So, a pandemic plan must describe a fair protocolfor removing a patient from a ventilator after a time-limited trial when clinicians determine that anotherpatient is more likely to benefit from a scarceresource both need. This protocol should describethe palliative care the first patient will be offered if theventilator is removed, and should also describe howclinicians will regularly review the protocol after itgoes into effect to fix problems and prevent abuses.But the protocol cannot rely on individual values andpreferences as a guide to ethical care: many patientsin this situation will—understandably—prefer toremain on the vent.
If clinicians, hospital administrators, ethics commit-tee members, and public health officials involved inpandemic planning are not familiar with public healthethics during a disaster as distinct from everyday clin-ical ethics they will not be able to create plans thatwill help first responders think and act differently, butethically.
The three Rs and the three VsFor physicians and other clinicians whose profes-
sional obligations are based on the duty to care forthe sick, the ethical dilemmas posed by a pandemiccan be summarized in three “Rs”: rationing, restric-tions, responsibilities. These first responders needplans that will give them clear guidance on how tofairly distribute limited resources; that will anticipatethe restrictions that may affect the delivery of healthcare; and that reflect an understanding of their profes-sional responsibilities. First responders also need pub-lic health officials to be responsible for providing aclear set of triggers that will tell first responders whatto do and when to do it.
Members of the public who are thinking about pan-demics are thinking about three “Vs”: vaccine, venue,ventilator. Will my family be vaccinated? Will we haveaccess to basic health care? Will we have access totechnology if we need it? The public may not yet seethe three Vs as ethical dilemmas, but questions aboutaccess to scarce resources, about restrictions aimed

6
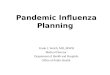
Like other states, Oregon needed an emergency pre-paredness plan to address public health and ethicalissues that would arise in a pandemic. The state’sDirector of Public Health formed a Medical AdvisoryGroup (MAG), which includes representatives fromcounty health departments, health professional organi-zations, insurers, local governments and tribal organiza-tions, plus a health care ethicist and an expert in masscommunications, to develop this plan. MAG membersdeveloped a decision-making matrix as a tool todescribe how to integrate ethical principles into thetypes of decisions that must be made prior to and duringa pandemic or other emergency.
Oregon’s matrix [see illustration, below] is based onthose values MAG members believed to be most at riskduring a pandemic: social solidarity; professional stan-dards; and justice. The matrix lists the characteristics ofthese values: for example, “equality” is one of the char-acteristics of justice, because a just policy or practiceassumes that people are equal, although their needsmay be different. The matrix also lists ethical terms, orprinciples, that may be used when applying these val-ues in a public health crisis: for example, because truth-telling is characteristic of a society that values justice, ajust policy or practice will need to uphold this principle
when communicating with the public or with individualpatients.
The overlapping areas of the matrix show wheredecisionmaking takes place, illustrating how each deci-sion involves different relationships among different prin-ciples in each sphere. Every decision must be account-able to each facet of the matrix: there can be noassumption that any decision will involve only one set ofprinciples. Decisions about public announcements dur-ing a pandemic, for example, must be accountable tothe justice principle of truth telling as well as the socialsolidarity principle of public order and the professionalprinciple of reciprocity.
This approach to decisionmaking anticipates theinformation crises that are likely to occur during a publichealth emergency. Rather than scripting ethical recom-mendations in advance for every possible public-infor-mation scenario, MAG members concluded that chang-ing conditions during a pandemic will require decision-makers to consult with one another on an ongoingbasis, using the matrix to assess the ethics of a givensituation. MAG continues to consult with the Departmentof Public Health on how the matrix will be disseminated,and what will trigger its use.
How Oregon Created an Ethical Decision-Making Matrix by John F. Tuohey, Providence Center for Health Care Ethics
Social Solidarity Professionalism
Justice
InterdependenceAttachmentCommitmentInvolvement
SubsidiarityCommon GoodPublic OrderSafetyReady Access
Evidence basedCompetenceConsensus drivenConsistencyAdaptive
TransparencyDuty to ActReciprocityIntegrity
EqualityEquityDifference PrincipleLibertyDue ProcessProportionality
AutonomyConfidentialityDisclosure/ Truth-TellingInformed Consent/ refusalBeneficenceNonmaleficenceStewardship

7
at infection control, and about the hard choices thatproviders will make concerning who gets access tointensive care, are all ethical questions. The duty toplan includes helping the public to understand theirresponsibilities as well as their rights during a publichealth emergency.
There are many different kinds of first responders:community members whose responsibilities andneeds must be reflected in any pandemic plan that isboth ethical and practical. Here are five of them:
The truck driverThe gatekeeperThe triage officerThe janitorThe public health official
These five “people” are really five groups of people.The “truck driver” represents community membersresponsible for essential non-medical tasks in a publichealth emergency. The “gatekeeper,” the “triage offi-cer,” and the “janitor” represent groups workinginside of hospitals, responsible for a variety of essen-tial tasks and decisions. The “public health official”represents local, state, and federal authorities respon-sible for making or carrying out the rules—laws, reg-ulations, emergency triggers, policies—that communi-ties will follow during an emergency, and that willhelp them to recover after an emergency.
All of these people have interests of their own,including an interest in being protected while doingtheir jobs under difficult, distressing conditions. Andall of these people need to have confidence in the planthey are following: it must make sense to them, and itmust clearly reflect the public’s interest.
The truck driver: community members to think about when mak-ing ethical decisions about vaccine allocation
CDC and NIH estimates continue to warn that wemust plan for an extreme scarcity of effective vaccineat the outbreak of pandemic, due to the impossibilityof predicting which influenza strain (or which muta-tion of which strain) will become pandemic and due tothe time needed to manufacture and distribute the
right vaccine. So every pandemic plan must clearlyanswer this ethical question: Who should be vaccinat-ed first, and why?
One person who will be high on the priority list, forexample, is the truck driver who delivers essentialsupplies that cannot be stockpiled, or when stockpilesrun out: these may include food; medical supplies;fuel, even clean water. Other essential personnelinclude the workers who will load and unload thesetrucks, police, fire fighters, and workers responsiblefor public safety, the factory workers meeting thedemand for vaccines—all of these people, like essen-tial medical personnel, must report for work, andmust work in situations where they may be exposedto pandemic influenza. So, these workers who are pro-tecting the public’s health must first be protected.
In thinking about that vaccination priority list, plan-ners must answer other ethical questions.
Incentives:
• What are appropriate and inappropriate incentivesto offer to essential workers, and why? Extra pay—orother employment-related benefits—is an appropriateincentive: essential workers will work long hoursunder difficult conditions. However, offering vaccineto essential workers’ family members is not appropri-ate, unless these individuals are also at high risk ofinfection. The ethics of fairly rationing scarce medicalresources require that these resources be reservedfor other essential workers charged with protectingthe public’s health.
Medical personnel:
• Physicians are community members, too. Whichphysicians should be vaccinated immediately, andwhy? Which physicians should not be vaccinatedimmediately, and why? Not all physicians who want tohelp in a crisis are professionally qualified to be firstresponders in a pandemic, when the crucial special-ties will be emergency medicine and critical care. Anethically sound pandemic plan will describe theresponsibilities of physicians and other health careproviders in terms of epidemiology and skills, ratherthan relying on the usual professional hierarchies toguide the distribution of scarce resources. In a flupandemic, respiratory technicians outrank neurosur-geons in terms of their value to the public’s health—

and all health care workers may be outranked byworkers responsible for maintaining a community’ssupply lines.
Community leaders:
• Where do community leaders other than officialsresponsible for public health and safety fit on the vac-cination priority list? Clergy, business leaders, andnonprofit executives, among others, may want andexpect to help out in a crisis, but they too may lackthe specific skills of essential workers that justify toppriority for vaccination when vaccine is scarce. Evenwhen vaccine is more widely available, simply show-ing up at the emergency room, ready to volunteer,may add to the burden of first responders without aid-ing those in need of medical evaluation and treatment.In what concrete ways can community leaders beencouraged and prepared to use their constituencies,their financial resources, or their facilities to supportessential workers, as well as families under quaran-tine or other restrictions, and communities experienc-ing illness and death on an unprecedented scale?
The gatekeeper:making ethical decisions about access to acutecare facilities
Community members expect their local hospital tobe open all the time, and the human tendency to go tothe hospital for safety and shelter as well as medicalcare is strong. During a pandemic, epidemiologicalconditions will work against these expectations: oncethe emergency plan is triggered, inpatient care will bereorganized to cope with influenza patients sickenough to be admitted, while ICU personnel continueto care for other patients too sick to be released.Emergency departments will be flooded with waves ofinfluenza patients, even as everyday medical emer-gencies continue. Keeping hospitals open and func-tioning safely with reduced staff is one of the chal-lenges in a disaster: it cannot be taken for granted.Hospitals will need “gatekeepers” to ration access tothese public facilities.
During a pandemic, the gatekeeper role is partlymedical: physicians and other clinicians may volun-teer to support emergency medicine specialists, by
registering patients and keeping the system moving.It is partly communications: administrators, chaplains,and social workers may volunteer for the difficult taskof turning people away, including family memberswho arrive with patients, and individuals who are notill enough to be admitted under emergency rules.And it is partly safety: the hospital’s security staff willbe responsible for keeping patients and staff safe ifthe hospital becomes a target for desperate individu-als.
However, the gatekeeper role begins with planners,and also includes local media, hospital CEOs, andleaders of other local institutions, from corporations tocongregations to nursing homes.
In thinking about the gatekeeper role, and inpreparing to support the individuals who will fulfillthat role during a crisis, planners must answer theseethical questions.
Public education:
• How will the public be educated about its responsi-bilities during a pandemic, including obeying quaran-tine or other restrictions? What clear guidance willthey receive about the symptoms of pandemic influen-za, and about seeking medical attention, at hospital, orother emergency health care facility, should theybecome ill?
Collaboration:
• How will competing hospitals collaborate with oneanother, with public health officials, and with themedia, to plan for and provide information aboutaccess to acute care facilities throughout affectedcommunities, and to prevent any single hospital frombecoming overwhelmed with patients?
Public information:
• Media organizations and individual journalists alsohave ethical obligations to their communities thattrump self-interest—how will planners enlist themedia (television, radio, print, web and other electron-ic communications) to provide accurate informationand prevent panic? How will media organizations,media professionals, and influential nonprofessionalsources of information in a community, such as blog-gers, monitor their own conduct?
8

9
Community health care:
• What is the appropriate gatekeeper role of commu-nity health care providers that are not acute-care facil-ities? Leaders of clinics and physicians in community-based medical practices will need clear information ontheir responsibilities as health care providers in com-munities under quarantine or other restrictions. Toensure fair access to needed medical services andtechnologies while keeping hospitals from being over-whelmed, some of these facilities may also be desig-nated as temporary emergency clinics or even ICUs,requiring that medical professionals be trained to usevents or other equipment. Leaders of sub-acute healthcare facilities, such as nursing homes, will also needclear information on how to protect the health of theirresidents and staff while vaccine stockpiles are limit-ed to essential workers, and on their responsibility toreduce the burden on acute-care facilities by caringfor residents’ medical needs in place whenever possi-ble.
The triage officer:making ethical decisions about access to ventila-tors and other critical care resources
Nationwide, 65.7 percent of ICU beds are occupiedon any given day.5 Should pandemic influenza breakout, some ICU beds will already be occupied bypatients who are critically ill and cannot be moved.Remaining beds will quickly be filled by influenzapatients who are sick enough to be admitted to theICU. Current epidemiological models project that atleast 50 percent of these flu patients will need ventila-tors.6 However, hospitals faced with inadequatestaffing may restrict ICU access to the sickestpatients: in this scenario, fully 100 percent of flupatients in the ICU will be sick enough to need venti-lators.
Pandemic plans must anticipate a shortage of venti-lators, because some ventilators will already be in useby critically ill patients, and because influenza is a res-piratory disease. Who gets access to available ventila-tors, and under what conditions, are rationing ques-tions that planners must address in concrete, action-able, ethically sound terms.
Ethical and clinical guidelines will help frontline
medical staff decide who goes on a ventilator, thelength of time-limited trials, the criteria for removingpatients from ventilators when recovery is uncertainand there are other patients with equal or greaterneeds for ventilator access; and how patients who“fail” the trials will be cared for. These are perhapsthe most distressing situations that medical personnelwill face during a pandemic.
The decision to remove a patient from a ventilatoror other life support can be stressful under normalcircumstances. During an influenza pandemic, somepatients will be removed from ventilators without theirconsent or the consent of a surrogate, in the interestof giving other patients with equivalent claims tothese scarce resources a fair chance to survive. Whatwould be unethical under normal circumstancesbecomes ethical under the emergency rules activatedby the trigger. The act of removing a patient from aventilator when this patient might recover given a bitmore time on the ventilator imposes a terrible burdenon the clinicians with the technical skills to care forcritically ill patients. It is unfair to add to this burdenby demanding that these same clinicians also decidewhich patients will have time-limited trials, and whichpatients should be removed from ventilators. An ethi-cally sound pandemic plan will specify that a seniorsupervising physician act as a triage officer to makethese decisions on behalf of front line clinicians.7
The triage officer is a gatekeeper with very specificduties, focused on ventilators. The triage officer mustbe supported by a rotating shift of administrators,including but not limited to clinical ethicists, who arecapable of assessing clinical situations inside a public-health framework, and of applying clear, consistentrules that acknowledge the rights of individualpatients while also acknowledging that, for the dura-tion of the emergency, the need to be fair to allpatients may trump individual claims.
In thinking about the triage officer role, and inpreparing to support the individuals who will fulfillthat role during a crisis, planners must answer theseethical questions.
Fairness:
• How fair, or unfair, are the criteria that the triageofficer and colleagues will use to ration access to ICUbeds and technology? For example, giving younger
1.2.3.

10
persons priority may not be defensible if current epi-demiological models do not support the claim thatolder persons are less likely to benefit from criticalcare measures. But using “mileage” rather than age—giving priority to persons whose overall state of healthis better—as a rationing rule means that persons withchronic diseases will be low priority for critical careduring a pandemic, which means that the populationswho disproportionately suffer from chronic diseaseswill have less access to scarce resources. The doingof ethics as part of pandemic planning means beingcandid about ethical trade-offs. Creating practicalrules to help frontline workers quickly identify whichpatients are most likely to benefit from scarceresources means acknowledging existing health dis-parities and further acknowledging that these dispari-ties will worsen in a crisis, while making access toscarce health care resources as fair as possible.
Who jumps the queue?
• Does an ER physician who becomes ill go to the topof the ventilator list, as a reward for taking greaterrisk? Or should a critically ill physician, who will notbe able to return to duty quickly, be subject to thesame criteria as any other critically ill patient?
Palliative care:
• What comfort care will be provided to the criticallyill patient who will not have access to life-saving treat-ment—surgery, antibiotics, and other treatments andtechnologies in addition to ventilators—that hospitalsmay not be able to provide during a pandemic? Painmanagement and palliative care specialists are notaccustomed to caring for patients who do not wanttheir services; providing comfort care to patients whowant curative care may be stressful to these medicalpersonnel. And while some of these patients may die,others may recover; the personnel caring for themmust be prepared for both possibilities. What ethicaland clinical guidelines can planners provide to clini-cians caring for these patients so suffering is mini-mized and clinicians understand and are not over-whelmed by their duties?
End of life care:
• What care will be provided to the dying personwhose family cannot be present due to public-health
restrictions? Clinicians who care for dying patientsassume that if the patient has a family, the family willbe at the bedside. During a pandemic, patients will diewithout their families present, and clinicians will besolely responsible for the care of these patients.Providing clear, compassionate ethical and clinicalguidance to these clinicians, and involving them inpandemic planning and preparedness, is yet anotherresponsibility of planners.
Training for triage:
• How will the triage officer and team be recruitedand trained for their responsibilities? What clinicaland ethical training do they need, in advance of a pub-lic health emergency, so they are ready to apply ethi-cal rules more stringently than usual, and to let fair-ness trump individual preferences while ensuringbasic procedural justice for individuals facing life ordeath situations? Which decisions are foreseeable andcan be addressed in guidelines? Who is responsiblefor reviewing these guidelines to ensure that they arefair and useful? How can bad—unjust, inconsistent, orimpractical—decisions be prevented when the triageofficer and team are confronted with a situation theirguidelines do not cover?
The janitor: protecting vulnerable health care workers
Like the truck driver, the hospital janitor is anotheressential worker during a public health emergency.Unlike the truck driver, the janitor is a health careworker, and may be at greater risk of infection due tothe location and nature of the job. In the early weeksand months of a pandemic flu outbreak, vaccine stock-piles may not be sufficient to cover the janitor, thelaundry workers, the orderlies, the staff memberswho deliver meals—all of these workers come intodirect contact with sources of infection and are in dan-ger of becoming ill themselves, whether from the fluvirus or from secondary infections carried by patientsin hospitals that cannot maintain normal sanitary stan-dards.
Do these workers have a duty to come to work dur-ing a pandemic? In ethics, “duty” tends to refer to pro-fessional responsibilities, or to enforceable civic obli-

11
gations, such as a duty to obey the law.Nonprofessional health care workers may identifywith and take pride in the institutions where theywork, or in their role in the care of the sick. Hospitalscannot function without these workers. However,these workers do not enjoy anything like the authorityand status of physicians or senior executives, or evenof much less powerful professionals in the hospitalhierarchy who may recognize a duty, as health careprofessionals, to come to work during an emergency.It is never ethically appropriate to add to the burdenof the most vulnerable members of any society. If low-status workers do not receive a fair share of their soci-ety’s benefits, it is not fair to tell them they have a pro-fessional or civic duty to do dangerous work.
In thinking about the janitor and other vulnerablehealth care workers, planners must answer these ethi-cal questions.
Incentives:
• What are appropriate and inappropriate incentivesto offer to these workers, and why? The answers tothese questions may seem to be the same as for thetruck driver: The janitor’s incentives should reflectthe risk this worker is exposed to, but should notdivert scarce resources from others who have anequivalent claim on these same resources. Howeverhealth care workers may face special risks or burdensduring a health care emergency, and their incentivesshould reflect these risks and burdens. Workers whomay be quarantined in hospitals to avoid becomingvectors of infection may need to make sure that theirfamilies quarantined at home have enough food orcash, or that safe child care is available in their com-munities. Workers who are able to go home after theirshifts may need to know that they can bring foodhome from work, or that they will receive flu medica-tion for family members.
Rationing supplies:
• How will hospitals stockpile and ration food, water,protective gear (masks, gloves), and antiviral andother medications among essential health care work-ers? Hospitals do not maintain supply warehouses,instead using “just in time” practices to order suppliesas needed. Breakdowns in the safe use of protectivegear triggered a second wave of SARS cases in
Toronto in 2002: several nurses died.8 So that thesegoods are not distributed by rank, or according tofirst come, first served, and so that hospitals with lesscash on hand to purchase supplies do not leave theiressential workers unprotected, planners must workwith providers to develop equitable and effective waysto establish, activate, and maintain supply lines andinfection-control procedures during a prolongedemergency.
The public official:making good decisions—and preventing “bone-headed” ones—before and during a publichealth emergency
In a public health emergency, members of the pub-lic should believe that their leaders are on their sideand are making good decisions on their behalf.Studies of communities that have endured natural dis-asters and other crises find that if a community’s lead-ers and citizens have a shared sense of social solidarity—of working together for the good of thecommunity—before a crisis, they will function wellduring and after a crisis. In the United States, howev-er, social solidarity at the local level—neighbors help-ing neighbors—does not always extend to trust instate or federal leadership.9
Establishing who is in charge during a publichealth emergency can be a challenge. Governors areresponsible for declaring states of emergency, whichmay be the trigger for local first responders to acti-vate their pandemic plans. As health care providedunder emergency guidelines may not meet normalstandards of care as defined by state law and otherstandards and policies, physicians and other cliniciansfear they could be vulnerable to charges of negligencein the aftermath of a crisis. As pandemic plans will callfor hospitals to cancel elective procedures and releaseall but the most fragile patients, hospitals’ cash flowfrom Medicare and insurance reimbursements will beprofoundly disrupted even as they continue to need tomaintain payroll, pay vendors, and purchase supplies.These are among foreseeable problems that requirethe attention of public officials well in advance of thedeclaration of a public health emergency. Failure toacknowledge and address these problems throughpractical guidelines is an ethical failure as well as a

12
policy failure.
In thinking about elected and appointed public offi-cials, and other individuals whose decisions beforeand during a pandemic will have consequences forthe public health and for the functioning of healthcare facilities, planners must answer these ethicalquestions:
• How can clinicians, health care administrators, andlocal public health officers limit the likelihood thatpublic officials will make bad decisions during a cri-sis? Public officials who are experienced in disastermanagement are more likely to make good decisionsunder pressure than are officials who lack this experi-ence.
First responders at all levels can use case studies ofprevious disasters—including the public-sectorresponses to them—to familiarize themselves withhow decisionmaking authority should, and should not,be exercised during a crisis, and how this authorityshould be distributed within a community. Clearlywritten policies, disseminated and discussed inadvance of a crisis, will reduce the need for crisis-driv-en decisionmaking, as the policies themselves will beauthoritative, giving first responders rules to follow.Having ethically sound policies in place will also helpto limit the effects of bad decisions that will,inevitably, be made during a crisis: officials will needto justify why it is in the public’s interest to departfrom broadly accepted policies.
Transparency:
• How transparent is the pandemic planning process?How are the social values of fairness and equality—the basis of an ethically sound pandemic plan—evi-dent in this process? In what ways do planners callattention to existing, ethically troubling health andhealth care disparities in the communities covered byits plan? To what extent are they listening to commu-nities that do not expect to be well-served during apublic health emergency, as well as from communitiesthat expect to receive quality health care?
Public engagement:
• How are members of the public involved in plan-ning activities, through public hearings or opportuni-ties to read and comment on draft documents? What
is the public education component of the planningprocess? What evidence is there that members of thepublic believe in the plan—believe that it is in theircollective best interests, and that it can be followed?
Private sector:
• How will public officials engage private-sector lead-ers in planning to help communities enduring a pro-longed public health emergency to function, and torecover? Using case studies as part of the planningprocess will help public and private community lead-ers understand what community members are likelyto need during a disaster and how community leaderscan support first responders to meet these needs.
What can planners do today to help these fivepeople do their jobs well during a pandemic?
• Recognize that the duty to plan, the duty todevelop rules and tools for first responders, andthe duty to be accountable to one another, ascivic duties as well as professional duties. Urgestate leaders, regional public health officials, leadersof health care organizations, and media executives tocoordinate their pandemic planning rather than workin isolation. Give private-sector leaders and the publicopportunities to discuss the plan and understand theirroles and responsibilities during a disaster.
• Give ethics a seat at the planning table. Theethicist recruited to participate in pandemic planningmust understand, and be able to explain, public healthethics as well as clinical ethics. The ethicist must begood at asking “why”—in particular, why is aresource-allocation option fair, rather than simplyexpedient? The ethicist should also have experiencedrafting ethical guidelines for practical use: firstresponders need rules and tools, not abstract princi-ples.
All of these decisions are hard decisions. To saythese decisions are too hard to make today is to shirkour duty to plan, and to make the duties of firstresponders even more difficult.
And to say Americans won’t plan, or won’t ration,or won’t care about others—and will no longer trustthe public sector to be on their side—is to allow cyni-

13
cism to triumph over civic responsibility and the pub-lic interest. In considering these five people, pandem-ic planners must show the rest of us how we will carefor one another, as communities and as a society, inperilous times.
References
1. J.C. Thomas, N. Dasgupta and A. Martinot, “Ethics in a pan-demic: A survey of the state pandemic influenza plans,”American Journal of Public Health 97 Suppl 1, (2007): S26.
2. US Department of Health and Human Services, “Pandemicinfluenza plan,” May 2007, at http://www.hhs.gov/pandemicflu/plan/appendixd.html.3. Thomas, S1. Emphasis added.4. NYS DOH/ NYS Task Force on Life & the Law, Workgroupon Ventilator Allocation in an Influenza Pandemic. Allocation ofVentilators in an Influenza Pandemic (2007).5. Organization for Economic Cooperation and Development.Health at A Glance: OECD Indicators 2005 (2005): 171.6. NYS DOH/ NYS Task Force on Life & the Law, Ventilators,10.7. Ibid
Selected ResourcesWebsites and electronic documents
• The New York State Task Force on Life and the Lawis an interdisciplinary, 23-member state commissionwith a standing mandate to develop public policy for therange of ethical issues raised by biomedical advances.The task force’s recommendations for ventilator alloca-tion provide a model for ethical planning. NYS DOH/ NYS Task Force on Life & the Law,Allocation of Ventilators in an Influenza Pandemic(2007), at http://www.health.state.ny.us/diseases/com-municable/influenza/pandemic/ventilators/docs/ventila-tor_guidance.pdf.
• Maryland’s pandemic plan includes an example of adetailed vaccination priority list that includes essentialworkers and members of the public.Maryland Department of Health and Mental Hygiene,Maryland Pandemic Influenza Plan, Version 6,” athttp://bioterrorism.dhmh.state.md.us/docs_and_pdfs/DRAFTFluPlanDec2006Part2.pdf: pages 207 and follow-ing.
• The Pandemic Influenza Working Group from theUniversity of Toronto’s Joint Centre for Bioethics recom-mends a 15-point ethical guide for use by planners. R. Upshur, K. Faith, J. Gibson, A. Thompson, C.S.Tracy, K. Wilson and P. Singer, Stand on Guard forThee: Ethical Considerations in Preparedness Planningfor Pandemic Influenza (2005), athttp://www.utoronto.ca/jcb/home/documents/pandemic.pdf.
• The University of Michigan’s Center for InfectiousDisease Research and Policy and Pew Center on theStates have launched an online database to sharepromising practices for pandemic preparedness.CIDRAP, “Promising Practices,” at http://www.pan-demicpractices.org.
• Maintained by the US Department of Health andHuman services, PandemicFlu.gov offers status reports,allocation guidelines and other planning resources fromfederal agencies.US Department of Health and Human Services,“PandemicFlu.gov,” at http://www.pandemicflu.gov.
Articles and reports
D.J. Alexander, “An overview of the epidemiology ofavian influenza,” Vaccine 25, no. 30 (2007): 5637-5644.
J.D. Arras, “Rationing vaccine during an avian influenzapandemic: Why it won’t be easy,” The Yale Journal ofBiology and Medicine 78, no. 5 (2005): 287-300.
V. Colizza, A. Barrat, M. Barthelemy, A. J. Valleron andA. Vespignani. “Modeling the worldwide spread of pan-demic influenza: Baseline case and containment inter-ventions,” PLoS Medicine 4, no. 1 (2007): e13.
J.K. Taubenberger, D.M. Morens, and A.S. Fauci, “Thenext influenza pandemic: Can it be predicted?” JAMA :The Journal of the American Medical Association 297,no. 18 (2007): 2025-2027.
J.C. Thomas, N. Dasgupta and A. Martinot, “Ethics in apandemic: A survey of the state pandemic influenzaplans,” American Journal of Public Health 97 Suppl 1,(2007): S26-31.
E. Toner and R. Waldhorn, “What hospitals should do toprepare for an influenza pandemic,” Biosecurity andBioterrorism : Biodefense Strategy, Practice, andScience 4, no. 4 (2006): 397-402.
R. Wray, J. Rivers, A. Whitworth, K. Jupka and B.Clements, “Public perceptions about trust in emergencyrisk communication: Qualitative research findings,”International Journal of Mass Emerging Disasters 24,no. 1 (2006): 45-75.

8. S. Yox, “SARS in Toronto—Nurses on the Front Lines,” June2003, at http://www.medscape.com/viewarticle/456919.9. R. Wray, J. Rivers, A. Whitworth, K. Jupka and B. Clements,“Public perceptions about trust in emergency risk communica-tion: Qualitative research findings,” International Journal ofMass Emergencies and Disasters 24, no. 1 (2006): 45-75.10. The White House, “National strategy for pandemic influen-za,” November 2005, at http://www.whitehouse.gov/homeland/pandemic-influenza.html.11. US Department of Health and Human Services, “Federaldepartment point of contact letter,” January 2007, athttp://www.pandemicflu.gov/plan/states/stateoperatingplanattach.html.12. M. Leavitt, “Pandemic planning update IV,” July 2007, athttp://www.pandemicflu.gov/plan/panflureport4.html.13. World Health Organization, “Cumulative number of con-firmed human cases of avian influenza A/(H5N1) Reported toWHO,” July 2007, at http://www.who.int/csr/disease/avian_influenza/country/cases_table_2007_07_25/en/index.html14. D. McNeil, “Closings and cancellations top advice on fluoutbreak,” New York Times, February 2, 2007.15. D. McNeil, “Scientists warn that bird-flu virus remains athreat,” New York Times, February 15, 2007.16. D.M. Morens and A.S. Fauci, “The 1918 influenza pandem-ic: Insights for the 21st century,” JID 195 (2007): 1018-1028.17. D.J. Alexander, “An overview of the epidemiology of avianinfluenza,” Vaccine 25 (2007): 5637-5644. 18. Ibid19. FDA News, “FDA approves first US vaccine for humansagainst the avian influenza virus H5N1,” April 2007, athttp://www.fda.gov/bbs/topics/NEWS/2007/NEW01611.html20. A. Pollack, “First vaccine against avian flu is approved as
interim measure,” New York Times, April 18, 2007.21. Associate Press, “Feds weigh future of bird flu vaccine,”New York Times, February 27, 2007.22. J.K. Taubenberger, “The next influenza pandemic,” JAMA297, no. 18 (2007): 2025-2027.23. FDA News, 200724. C. Vittoria, A. Barat, M. Barthelemy, A. Valleron, A.Vespignani, “Modeling the worldwide spread of pandemicInfluenza: Baseline case and containment interventions,” PLoSMed 4, no. 1 (2007): 95-110.25. Roche, “Flu treatment with Tamiflu,” at http://www.tamiflu.com/treat.aspx.26. D. McNeil, “Closings and cancellations”.27. Centers for Disease Control and Prevention, Interim Pre-pandemic Planning Guidance: Community Strategy forPandemic Influenza Mitigation in the United States, February2007, at http://www.pandemicflu.gov/plan/community/community_mitigation.pdf.28. Trust for America’s Health, Pandemic Flu and the Potentialfor US Economic Recession, March, 2007, athttp://healthyamericans.org/reports/flurecession/FluRecession.pdf.29. E. Toner, R. Waldhorn, “What hospitals should do to pre-pare for an influenza pandemic,” Biosecurity and Bioterrorism:Biodefense Strategy, Practice, and Science 4, no. 4 (2006):397-402.
Acknowledgements
The authors wish to thank Tia Powell, John Tuohey, AlisonJost, Erika Blacksher, Arlene Stoller, Mary Crowley, NoraPorter, Charis Torok, and the Providence St. Vincent MedicalFoundation for their assistance.
14
An electronic copy of this Bioethics Backgrounder can be downloaded at:www.thehastingscenter.org or
www.providence.org/oregon/Programs_and_Services/Ethics/Default.htm For more information on the issues addressed in this Bioethics Backgrounder, contact:
Nancy Berlinger, Research Associate, at [email protected].
November 2007