Embed Size (px)
Citation preview

ETHER ANAESTHESIA1842 - 1900*
ByBARBARA M. DUNCUM, D.Phil.,
Nuffield Department of Anaesthetics, University of Oxford
Pre-anaesthetic HistoryThe first man to give an unequivocal description
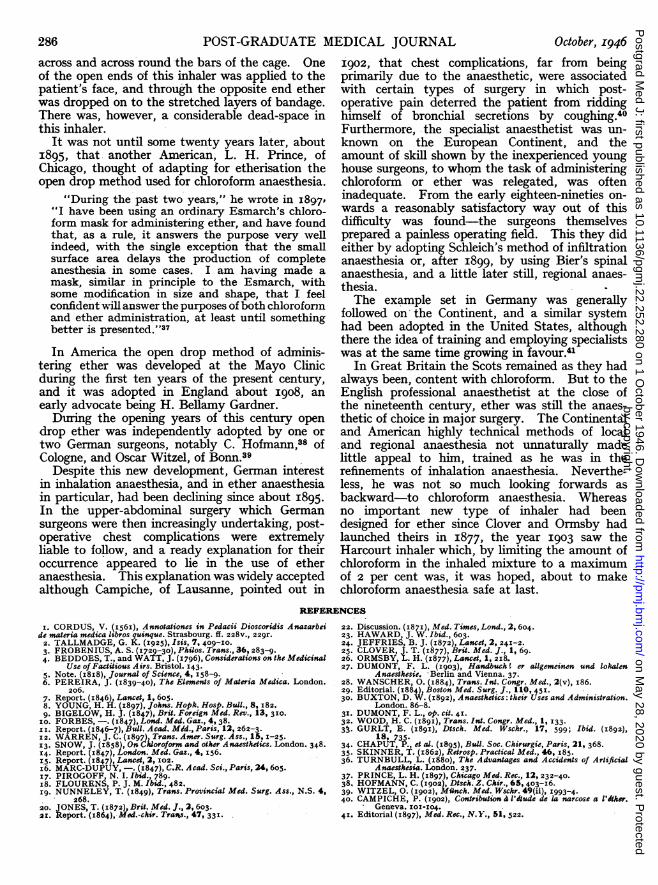
of the distilling of ether from sulphuric acid andalcohol was Valerius Cordus,' about the year I540.Cordus called ether "sweet oil of vitriol," and hisaccount of his method of preparing it and of itsproperties (see Fig. I) has been translated by GuyK. Tallmadge as follows:
"Take six fluid ounces of strong, very biting,thrice purified wine, and the same quantity of souroil of vitriol. Mix in a-Venetian glass, and place ina small gourd with a narrow mouth, and seal themouth with clay. Set aside thus for a wholemonth, or two. Then pour out into a gourd towhich should be immediately connected, and sealedby the heat of the fire, an alembic (that is, ein kolbmit einen angeschmeltzen helm), which we illustratebelow; now place in a small furnace and half coverit with ashes. After this, apply a receiving vesseland carefully close the joint with clay, and extractthe six fluid ounces of strong wine which you added.But, so that this may be done safely, place into abath of Maria: thus the wine alone will ascend,without the oil. WVhen you shall have extractedin the bath the six fluid ounces of strong winewhich had been added, place the residue in thefurnace so that sand is heaped up to the middlepart of the gourd, and, having applied a new, small,empty receiving vessel, carefully seal the joint withclay. Now make a slow fire, and slowly extractall of the moisture which remains in the gourd,until liquid no longer appears in the bottom, alwaysusing the greatest care and watchfulness that youso moderate the fire that the boiling liquid neverreaches the tube of the alembic. . . Whexi youhave completed the slow extraction, at once removethe receptacle, with its liquid, and you will seethat it contains two substances, namely, an aqueousliquid and an oily, fatty one. You should separateone from the other at once, however, so that noaqueous substance remains in the oil, for thatwater spoils the oil. The oil itself generally floatsupon the water, especially if the wine shall havefirst been entirely extracted upon the bath, butyou can easily distinguish the oil from the water
*Some of the material relating to inhalation anaesthesiacontained in this article is based on Dr. Duncum's book,The Development of Inhalation Anaesthesia with SpecialReference to the Years I846-I900, now in course of publi-cation by the Oxford University Press for the WellcomeHistorical Medical Museum.
by touch. For the oil is greasy; the water not atall so. Then preserve the separated oil for furtheruse.
The Properties of the Substance which has been Separated"It has all of the properties of sulphur, but all of
them are more pronounced because it penetratesliquids more easily, and hastens actions, whichsulphur cannot do because it is impeded by itsown solidity and dryness, by which it is less pene-trating. This, indeed, this oil can do better thansulphur, wherefore it is especially valuable for allputrefactions in the body, and particularly for theplague. It draws the pus and mucus from thelung in pleurisy, peripneumonia and hacking cough,for it may be securely taken internally, and withoutany danger. It does not cause stones to form,either in the kidneys or in the urinary bladder; itheals an exulcerated urinary bladder. Its doseis one or two drops, or three mixed in a moderatequantity of wine. It may be mixed, moreover,into pills and electuaries made of sugar. It mustbe carefully preserved, however. For only a littleis got from a pound of sour oil of vitriol, andbecause of the tenuity of its nature it easily eva-porates."2The name cether seems first to have been applied
to the liquid by August Siegmund Frobenius.3He demonstrated various of its properties, realand imaginary, before the Royal Society duringFebruary of the year I730. Among Frobenius'sexperiments on that occasion was one to show"that this Ather may be preserved best . . .
under the Receiver in Vacuo, whereas on thecontrary, exposed to the open Air, its Parts soonevaporate, and its whole Bulk . . . vanishes."Upon which the Royal Society's reporter com-mented, "This experiment fail'd remarkably." Inanother experiment with ether Frobenius showedthat "a little of it poured on the Surface of theHand, affects it with a Sense of Cold equal to thatfrom the Contact of Snow, and blow upon it butonce or twice with your Mouth, immediately yourHand becomes dry. Beware however of approachinga lighted candle with your Hand thus wet, lest ittake Fire and burn you"-to which account isappended the comment, "Succeeded."During the last decade of the eighteenth century,
after Lavoisier had elucidated the true nature ofrespiration and had shown the part played in it
by copyright. on M
ay 28, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.22.252.280 on 1 O
ctober 1946. Dow
nloaded from
ETHER ANAESTHESIA, 1842-1900
by oxygen and carbon dioxide, and after Priestleyhad inhaled oxygen, a new therapeutic vogue cameinto being. This was pneumatic medicine, inwhich various gases and vapours-among themsulphuric ether-were inhaled in order to cure notonly physical complaints, particularly pulmonaryones, but also such mental ailments as melancholy.Pneumatic medicine had its origins in part in thevery brilliant circle of learned men centred inBirmingham, of whom Priestley was one. It cul-minated in the founding by Thomas Beddoes, ofthe Pneumatic Institution at Clifton, Bristol.
Describing, for example, the method of inhalingether devised by the physician R. J. Thornton,about I795, Beddoes wrote:
"The manner of inhalation is very simple. Twotea-spoonfuls of ather are put into a tea pot. Thisis held near a candle, and the thumb is put overthe spout. When the vapour begins to press onthe thumb, it [the spout] is transferred to themouth, and air is drawn into the lungs. This isrepeated until the whole be consumed, or easeacquired."4
Beddoes added a warning that "the vapour ofaether is inflammable in air.". After Humphry Davy's demonstrations at thePneumatic Institution (of which he became Super-intendent in I798, at the age of nineteen) thatinhaled nitrous oxide-in addition to other, moreweighty, physiological considerations-was capableof inducing a state which was both pleasurable tothe subject and entertaining to onlookers, the"laughing gas" was very frequently inhaled foramusement's sake.A similarity in the effects of nitrous oxide and
of ether vapour when inhaled was pointed out ini8i8 in the Journal of Science, of which MichaelFaraday was then editor.
"When the vapour of ether mixed with commonair is inhaled, it produces effects very similar tothose occasioned by nitrous oxide. A convenientmethod of ascertaining the effect is obtained byintroducing a tube into the upper part of a bottlecontaining ether, and breathing through it; astimulating effect is at first perceived at the epi-glottis, but soon becomes very much diminished, asensation of fulness is then generally felt in thehead, and a succession of effects similar to thoseproduced by nitrous oxide. By lowering the tubeinto the bottle, more of the ether is inhaled at eachinspiration, the effect takes place more rapidly,and the sensations are more perfect in theirresemblance to those of the gas...."It is necessary to use caution in making experi-
ments of this kind. By the imprudent inspirationof ether, a gentleman was thrown into a verylethargic state, 'which continued with occasionalperiods of intermission for more than thirty hours,
and a great depression of spirits; for many daysthe pulse was so much lowered that considerablefears were entertained for his life."'5
These effects were quoted in I839 by the pharma-cologist, Jonathan Pereira,6 and he recounted alsothat "the chemist Bucquet, who died of schirrhusof the colon, with inflammation of the stomach andof the intestines generally, took, before his death,a pint of ether daily to alleviate his excruciatingpains."
Referring to the inhalation of ether vapour,Pereira noted its use "in spasmodic asthma,chronic catarrh, and dyspnoea, whooping cough,and to relieve the effects caused by the accidentalinhalation of chlorine gas." He stated that thephysiological effects "have not been determined,"and described how, after giving fifteen drops to ayoung rabbit, its death took place within an hour."The symptoms were indisposition to move,apparent tendency to sleep, followed by incapacityof supporting the erect position, occasional con-vulsive movements, grating of the teeth, andinsensibility."
The Trial of Ether as an AnaestheticAt the time when Pereira wrote, and during the
next few years, the inhalation both of nitrous oxideand of ether vapour not for therapeutic reasonsbut as a form of entertainment was extremelypopular, especially in the United States of America.Indeed, in May I846, the Lancet quoted theWestern Journal in which "Dr. Miller calls attentionto the pernicious effects of the inhalation of thisvapour [ether]-a habit which seems to prevailamong young persons in some districts of theUnited States."7Such an ordinary gathering and its very unusual
results were described by the young generalpractitioner Crawford Williamson Long:
"In the month of Dec. I84I, or in Jan. I842, thesubject of the inhalation of nitrous oxide gas wasintroduced in a company of young men assembledat night in the village of Jefferson, Ga., and theparty requested me to prepare them some. I in-formed them I had not the requisite apparatus forpreparing or preserving the gas, but that I had anarticle (sul. ether) which would produce equallyexhilarating effects and was as safe. The companywere anxious to witness its effects, the ether wasintroduced and all present in turn inhaled. Theywere so much pleased with its effects that theyafterwards frequently used it and induced othersto do the same, and the practice soon became quitefashionable in the county and some of the conti-guous counties."On numerous occasions," Long added, "I
inhaled ether for its exhilarating properties, andwould frequently, at some short time subsequent
October, I946 281by copyright.
on May 28, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.22.252.280 on 1 October 1946. D
ownloaded from
POST-GRADUATE MEDICAL JOURNAL
to its inhalation, discover bruised or painful spotson my person which I had no recollection of causingand which I felt satisfied were received whileunder the influence of ether. I noticed my friendswhile etherized ieceived falls and blows which Ibelieved were sufficient to produce pain on aperson not in a state of anaesthesia, and on ques-tioning them they uniformly assured me that theydid not feel the least pain from these accidents.Observing these facts I was led to believe thatanaesthesia was produced by the inhalation ofether, and that its use would be applicable insurgical operations."8
How Long then, in March I842, poured ether onto a folded cloth and caused the boy, JamesVenable, to inhale the vapour so that he becamesufficiently insensible to allow two small tumoursto be painlessly removed from his neck is wellknown. So also is the not dissimilar sequence ofevents which, in December i844, led Horace Wellsto conceive and put into practice the idea ofinhaling nitrous oxide to obtund the pain of dentalextractions. That he should have failed to producesatisfactory anaesthesia in his patient during thedemonstration at the Massachusetts General Hos-pital in Boston, arranged through his former dentalpartner, W. T. G. Morton, was a piece of extremelybad luck.When in the summer of I846 Morton himself
decided to experiment in obtunding the pain oftooth extractions, it is not so very. surprising thathe should have chosen sulphuric ether as hisanodyne agent. Indeed, he had actually usedliquid ether in I844, at the suggestion of hisformer chemistry tutor, C. T. Jackson, -as a localapplication to deaden pain in a tooth.
In his first clinical trial of etherisation, when onSeptember 30, I846, he painlessly extracted EbenFrost's aching tooth, Morton poured the ether onto a folded cloth. He had for some time pastbeen trying to adapt various pieces of apparatusfor administering ether and, not finding thefolded cloth method entirely satisfactory, heredoubled his efforts to devise a satisfactoryinhaler.At the very last minute before his all-important
demonstration of etherisation at the MassachusettsGeneral Hospital, on October i6th, Morton, withthe assistance of the Boston physitian, AugustusA. Gould, designed and had made "a small two-necked glass globe" to contain an ether-soakedsponge. H. J. Bigelow, who was present at thedemonstration on October i6th, described theworking of the inhaler as follows:
"One aperture admits the air to the interior ofthe globe, whence, charged with vapour, it is drawn.through the second into the lungs. The inspiredair passes throug-h the bottle, but the expiration is
diverted by a valve in the mouthpiece, and escapinginto the apartment is thus prevented from vitiatingthe medicated vapour."9
The fact that this inhaler (which was io cm. indiameter) was held in the administrator's warmpalm, which automatically aided the vaporisationof the ether, was an accidental but a very importantpoint in its favour.Very soon after Morton's public demonstration,
various distinguished men in Boston sent word ofthe great surgical innovation, etherisation, to theirfriends in the Old World.The first to receive the news in England was
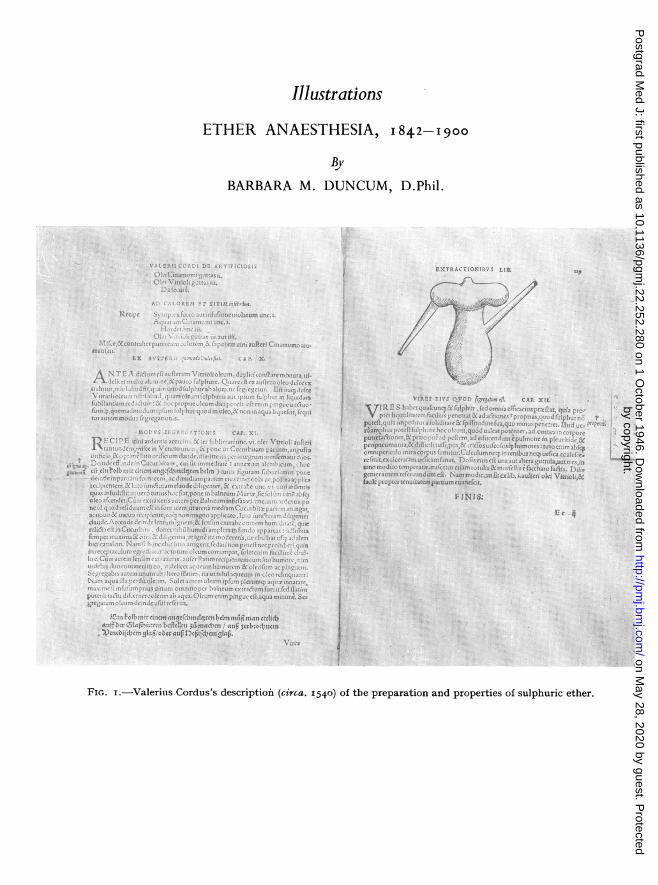
Francis Boott, of Gower Street, London, and heand a dentist named Robinson lost no time inadministering ether to a young lady for the extrac-tioni of a tooth. Boott also passed on the newsto the surgeon, Robert Liston.An eye-witness named Forbes described how,
on December 22, I846,
"in the theatre of University College Hospital,Mr. Liston amputated the thigh of a man previouslynarcotised by inhalation of the ether vapour.Shortly after being placed on the operating tablethe patient began to inhale [from an apparatusprepared by Squire (Fig. 2)], and became apparentlyinsensible in the course of two or three minutes.The operation was then commenced, and the limbwas removed in what seemed to us a marvellouslyshort space of time-certainly less than a minute,the patient remaining, during the incisions and thetying of the arteries, perfectly still and motionless.While the vessels were being secured, on beingspoken to he rose partially up (still showing nosigns of pain) and answered questions pyt to himin a slow drowsy manner. He declared to us thatat no part of the operation had he felt pain, thoughhe seemed partially conscious; he had heard somewords, and felt that something was being done tohis limb. He was not aware, till told, that thelimb was off, and when he knew it, expressed greatgratification at having been saved from pain."iO
In France the first trial of etherisation was madeby the surgeon, J. F. Malgaigne, towards themiddle of January i847. He described at ame.eting of the Academie de Medecine in Paris,how-having no such inhaler as was used inAmerica and England-he took a simple tube intowhich he put some ether and then introduced theend of it into the patient's nostril, the other nostrilbeing plugged. "I took care," said Malgaigne,"that inspiration took place with the mouth closed,expiration with the mouth open."'1" Several ofMalgaigne's colleagues subsequently followed hisexample in making their patients inhale ethervapour through one or both nostrils. Otherspreferred to use the American and English typesof sponge-filled flask.
282 October, I946by copyright.
on May 28, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.22.252.280 on 1 October 1946. D
ownloaded from
ETHER ANAESTHESIA, 1842-1900
In the meantime Morton had taken out a patentto cover the use of etherisation and its adriinistra-tion by any such means as his inhaler. At theMassachusetts General Hospital, John MasonWarren in February I847 decided, in view of thepatent, to abandon the use of any inhaler andinstead to pour t14e ether directly on to a smallbell-shaped sponge which was then held firmlyover the patient's nose and mouth.'2
This procedure proved so simple and so effectivethat it was widely adopted in the United States.Indeed, from that time until the close of thenineteenth century, a sponge or a sponge enclosedin a folded towel was there the method of adminis-tration almost exclusively used.
In this way the Americans had found a means ofavoiding the worst difficulties of etherisation; butin Great Britain and on the European Continentanaesthesia was becoming less and less satisfactoryas inhalers grew more conplicated. Summarisingthe common faults of these early inhalers JohnSnow, famous to-day as the first specialist anaes-thetist, wrote:
"When the inhalation of ether was first com-menced, the inhalers employed consisted generallyof glass vases containing sponge, to afford a surfacefor the evaporation of the ether. Both glass andsponge being very indifferent conductors of caloric,the interior of the inhalers became much reducedin temperature, the evaporation of ether was verymuch checked, and the patient breathed air muchcolder than the freezing point of water, and con-taining very little of the vapour of ether. Onthis account, and through other defects in theinhalers, the patient was often very long in becominginsensible, and, in not a few cases, he did notbecome affected beyond a degree of excitement andinebriety."13Inhalers intended to overcome these defects had
been produced, but until the principles laid downby Snow himself began to be appreciated, designersoften showed themselves more remarkable foringenuity than for insight into the problems ofether vaporisation and inhalation.At a meeting of the Westminster Medical Society
on January i6, I847, Snow read a paper on thevaporisation of ether, in which he is reported tohave said that
"the great effect of temperature over relations ofatmospheric air with the vapour of ether, hadapparently been overlooked in the constructionand application of the instruments hitherto used.. . . The operators did not at present know thequantity of vapour they were exhibiting with theair; it would vary immenselyS according to thetemperature of the apartment."Snow gave a table setting out the volumes of
ether vapour which, at different temperatures, onehundred cubic inches of air would contain.
"He (Dr. Snow) was getting an instrument madewhich would enable the surgeon, merely by placingit in a basin of water, warmed or cooled to a giventemperature, to administer an atmosphere of anystrength he wished, and by this means to gaincorrect experience to guide him in future."'l4A week later Snow showed his first ether inhaler
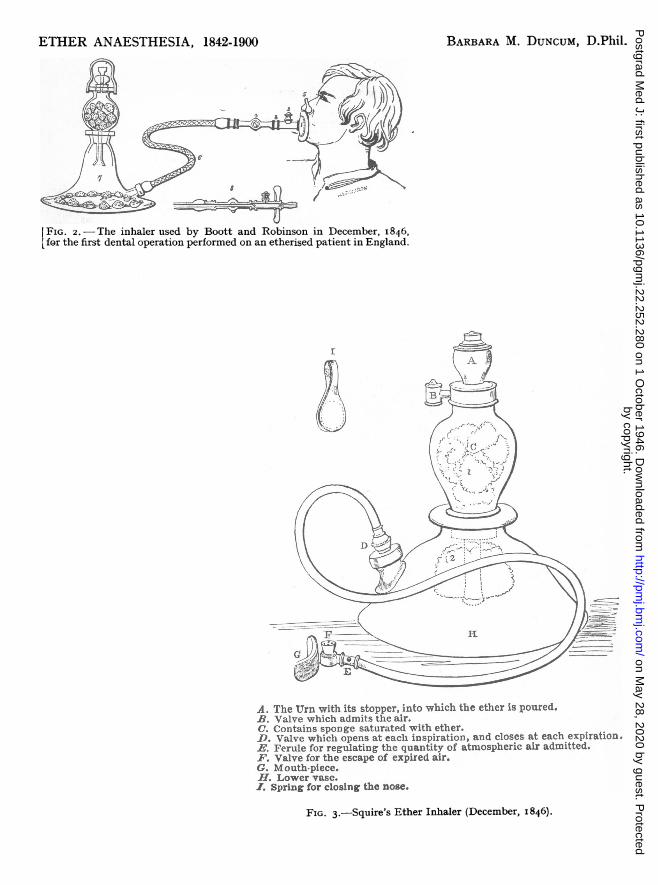
at the Westminster Medical Society; and duringthe spring of I847 he continued to improve it(see Fig. 3a). One of the biggest of these improve-ments was the adoption of a valved facepiece(see Fig. 3b) (based on a valveless facepieceinvented by Francis Sibson) instead of the usualmouth-tube and nose-clip.
Notwithstanding the fact that some adminis-trators were beginning to master the technique ofetherisation, when Professor J. Y. Simpson, inNovember I847, described the simplicity withwhich the far more potent anaesthetic, chloroform,could be administered from a folded cloth, the useof ether was immediately and generally discarded.
In England ether anaesthesia was neglectedduring the next twenty-five years; on the Continentof Europe as a whole, it remained in disreputeuntil the last decade of the nineteeth century; evenin Boston it was for a short time discarded.Besides the Americans in the Northern States ofthe Union, only the surgeons of Lyons-andfollowing their example, the surgeons of Naples-soon returned to the use of etherisation, afterdeaths from chloroform had begun to occur. Inthe Austrian Empire, and in Vienna in particular,a compromise was made, and mixtures containingchloroform and ether in varying proportions, werepreferred to the use of either agent alone.
It seems probable that the reason why thesurgeons of Lyons returned so readily to the useof ether was because, before the introduction ofchloroform anaesthesia, they had been using aneffective methQd of etherisation. This was Roux'ssac, "a bag, made like a lady's reticule, its openingbeing dilated or contracted by the drawing orloosing of the strings around it, and lined by a pig'sbladder. ... In using this apparatus, the mouthand nostrils are both placed in the sac drawn overthem, and inhalation goes on with the ether vapourgiven off from sponges soaked in ether, and placedin the bladder.''l5
Before the inhalation of ether was superseded bythat of chloroform, a few interesting experimentson rectal etherisation were made in the laboratoryand clinically. In France Marc-Dupuy, injectingliquid ether mixed with water into the rectums ofdogs, found that anaesthesia was rapidly estab-lishe,d and caused but slight inflammation of therectal mucous membrane. He came to the con-clusion that this method of rectal administrationwas likely to prove safer than inhalation of the
October,- I946 283by copyright.
on May 28, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.22.252.280 on 1 October 1946. D
ownloaded from
POST-GRADUATE MEDICAL JOURNAL
vapour.16 In Russia, the surgeon, Nikolai Ivano-vich Pirogoff, after experimenting on animals,evolved a satisfactory method of introducing ethervapour into the rectums of his patients. Afterwashing out the rectum, he introduced into it oneend of a rubber catheter, the other end beingconnected to a small container surrounded by awarm water-jacket, so that the liquid ether putinto it should be immediately vaporised. Heclaimed that anaesthesia was established in fromthree to five minutes and that there were noundesirable after effects.17The intravenous injection of ether, also, was
tried on dogs, but the results were not veryencouraging. The physiologist, P. J. M. Flourens,18in I847, found that the dogs became "drunk" butnot insensible, and Thomas Nunneley, of Leeds,two years later reported only that after the injectionof sulphuric and of acetic ether "the symptomspreceding death, and the appearance presentedafterwards, do not differ materially from thosecaused by inhalation."'9 Although P. C. Ore, ofBordeaux, used the intravenous injection of chloralhydrate successfully in a few cases during the earlyeighteen-seventies, it was not until I909, afterLudwig Burkhardt had devised a satisfactorymethod of administering ether intravenously, thatthis method of anaesthesia was adopted in practice.
The Interim PeriodWhile Lyons and Naples remained, during the
eighteen-fifties and sixties, the only two cities inEurope where ether as the sole anaesthetic wasregularly used in preference to chloroform, in i86iThomas Jones gave ether a re-trial at St. George'sHospital in London.Some years afterwards he wrote:
"Although it was administered on a large conicalsponge (a very objectionable mode), I succeeded inalmost all cases in producing the necessary degreeof narcotism. It was given for several capitaloperations, and in cases requiring careful dis-section, such as herniae, with complete success.In the following year I discontinued its use, how-ever, in the operating theatre, on account of theinconvenience occasioned to those present, by thesmell of the vapour, and from the time it took insome cases to get the patient under its influence.
I, however, continued its use in cases whichwere considered unsafe for chloroform, such as forthose in a state of collapse from severe accidents."20
In I864 the committee appointed by the RoyalMedical and Chirurgical Society, to investigatethe physiological action of chloroform anaesthesia,made its report. As a result of comparativeseries of experiments, using chloroform and,ether,the following conclusion was reached: "It is . . .
extremely desirable to obtain an anaesthetic agentwhich shall be capable of producing the requisiteinsensibility, and yet is not so dangerous in itsoperation as chloroform.
"Ether, to a certain extent, fulfils these condi-tions, but its odour is disagreeable, it is slow in itsoperation, and gives rise to greater excitement thanchloroform. The committee therefore concur inthe general opinion which in this country has ledto the disuse of ether as an inconvenient anaes-thetic."As a compromise the committee suggested that
mixtures of chloroform and ether should be used,and in particular recommended the A.C.E. mixturewhich consisted of one part alcohol, two partschloroform, and three parts ether.2'Although such mixtures did not immediately
become popular, a few people began to use achloroform and ether sequence, inducing anaes-thesia with the more easily-manageable agentchloroform, and maintaining it with the saferagent ether. Not long after the introduction ofnitrous oxide into English dental practice in i868,J. T. Clover began to use his famous "gas andether" anaesthesia.22An unsuccessful attempt to arouse English
interest in ether as the sole anaesthetic, adminis-tered by the American method, was made by J.Warrington Haward, in i87I.23 In the followingyear, however, B. Joy Jeffries, an ophthalmicsurgeon from Boston, Massachusetts, came toLondon to attend a conference. He also camedetermined to convince the English chloroformistsof the error of their ways.
Jeffries opened his campaign by reading a paperon "Ether in Ophthalmic Surgery," in which hedescribed the American procedure:
"A towel rolled into a cone, with a napkin orsponge pushed to the top of the inside, is all weneed to pour our ether on, whilst our fingers canmould it over any mouth and nose. .....Nowif the patient is warned that the ether will chokehim, and told when this occurs to take long breathsto relieve it, and not struggle and endeavour topush away the sponge, many will go to sleep quietlyand without trouble to themselves or the surgeon.. . . When the patient, whether old or young,struggles, alid asks for a respite and fresh air, donot yield. Hold them down by main force, ifnecessary, and at any rate, keep the sponge tightover the mouth and nose till they finally take longbreaths and then go off into ether-sleep."24
The London chloroformists were a little startledby Jeffries's methods, but at the same time theywere comeplled to recognise the fact that, given inthis way, ether could be a very efficient anaestheticagent.During the autumn of I872 the British Medical
284 October, 1946by copyright.
on May 28, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.22.252.280 on 1 October 1946. D
ownloaded from
ETHER ANAESTHESIA, 1842-1900
Association, through the medium of its journal,encouraged anaesthetists to make a fresh trial ofetherisation, and by I873 the revival of its use waswell-established in England.
The Use of Ether Anaesthesia Re-established
During the first few months of the revived useof etherisation, variants of the American methodof enclosing a sponge in some kind of cone-made,for example, from a folded towel, from felt, or fromcardboard-were by far the most commonly used,and this was to be expected. But gradually theEnglish preference for mechanical inhalers beganto reassert itself. Unlike the inhalers of I847,which aimed at diluting each breath of ethervapour with atmospheric air, the majority ofinhalers designed during the eighteen-seventiesmade use of re-breathing. Of these inhalers thetwo best-remembered to-day are Clover's "portableregulating inhaler"25 (see Fig. 4), and Ormsby'sinhaler26 (see Fig. 5), which were first described inthe medical joumals early in- I877.At the time when the English were thus en-
thusiastically rediscovering the advantages of etheranaesthesia, France and Germany were recoveringfrom the effects of the Franco-Prussian War, andit seems likely that this was a strong reason whythe general revival of etherisation on the EuropeanContinent was delayed for more than fifteen yearslonger.
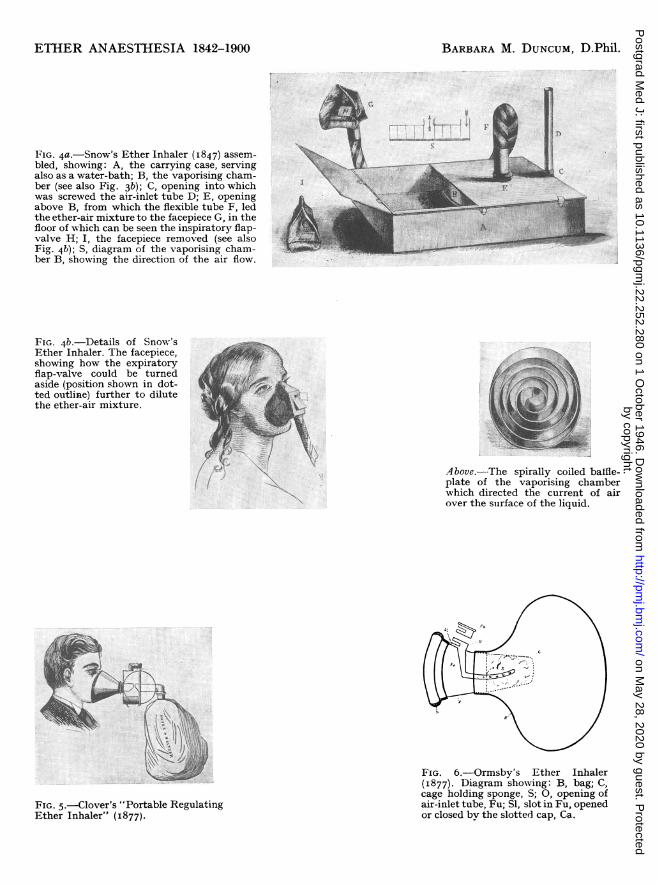
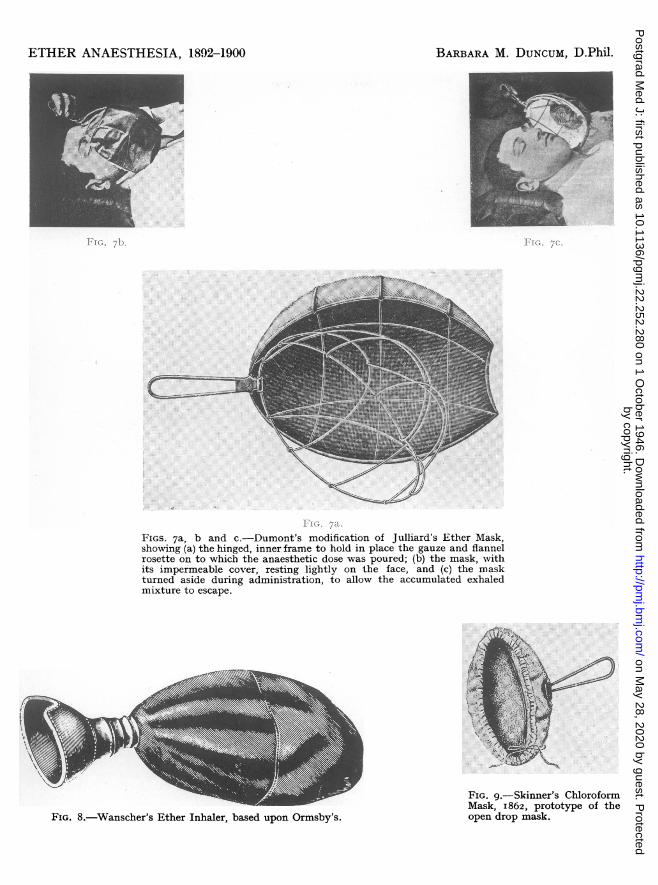
In I877, however, the surgeon, Gustave Julliard,of Geneva, after a death from chloroform hadoccurred in his practice, abandoned the use of thatanaesthetic and adopted ether. He administeredit from a large, wire frame, the outside of whichwas covered with waxed cloth to make it imper-meable to air, the inside with surgical gauze on towhich the ether was poured. This mask wassubsequently modified by F. L. Dumont, of Berne,who added a hinged, inner frame (to allow soiledgauze to be changed more easily) and attached arosette of flannel to the gauze to receive the doseof ether (see Fig. 6). The mask did not fit theface accurately, and when it was desirable todeepen anaesthesia a folded towel was laid roundthe rim to reduce the amount of air filtering in.But as inl any case the carbon dioxide accumulatingunder it was considerable, it was also necessaryto turn the mask aside from the face at intervalsthroughout administration, as is shown in Fig. 6.27The use of Julliard's method of etherisation
slowly spread northward into south Germany,and it was adopted in particular by Bruns andGarre, at Tubingen, during the late eighteen-eighties.At the beginning of the eighteen-eighties ether
anaesthesia had been adopted independently bythe surgeon, Oscar Wanscher, of Copenhagen.He administered ether both rectally,28 by a methodwhich was in principle that used by Pirogoff inI847, and by inhalation, using an inhaler based onOrmsby's, but without any air inlet or sponge, theliquid ether being poured straight into the bag.29A colleague of Wanscher's, Axel Yversen, visiting
Lyons in I884, asked the surgeon, Daniel Molliere,whether he administered ether rectally. Thisprompted Molliere to try the rectal route and hissuccess attracted some attention in the UnitedStates. In a leading article, the Boston Medicaland Surgical Journal in May i884,30 stressed theparticular usefulness of rectal etherisation in leavingthe surgeon a clear field in operations involvingthe head and neck. It was this consideration,also, which led D. W. Buxton to develop his ownmethod of rectal etherisation about i890.31As for Wanscher's method of inhaling ether, his
first convert to it outside Denmark was thegynaecologist Landau, of Berlin, whose clinicWanscher visited during the early part of I890.
In August I890, the Tenth International Con-gress of Medicine was held in Berlin, and in thecourse of the proceedings the American pharma-cologist, Horatio C. Wood, read a paper onanaesthesia, in which he emphasised, with statisticaldetails, the far greater safety of etherisation ascompared with chloroform anaesthesia.32 Thispaper made a great impression upon the Germans,and Ernst Gurlt was commissioned by the GermanSurgical Society to compile independent statisticsrelating to the safety of the two agents. Thesewere published annually.33
Gurlt's results weighed heavily in favour ofether, and by I894, as an outcome of his investi-gation, a number of German surgeons were tryingether anaesthesia either by Julliard's method orby Wanscher's. Following the German example,about I895 a few French surgeons, the Lyonnaisapart, began tentatively to use ether.34The last major development in ether anaesthesia
which had its beginnings during the first fiftyyears of anaesthetic practice was the adoption ofthe open drop method.As long ago as i862 Thomas Skinner,35 of Liver-
pool, had introduced the use of a small, wire face-mask, covered with woollen fabric, on to whichchloroform was dropped from a specially adaptedbottle; and this simple and effective method hadproved popular, particularly in Germany.
In I874 the American, 0. H. Allis, had introducedthe use of what he claimed was an open etherinhaler.36 It consisted of a leather cover, shapedrather like a detachable shirt-cuff, enclosing asimilarly shaped, oval, metal cage, its internalspace being occupied by layers of bandage threaded
285October, I1946by copyright.
on May 28, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.22.252.280 on 1 October 1946. D
ownloaded from
286 POST-GRADUATE MEDICAL JOURNAL October, I946across and across round the bars of the cage. Oneof the open ends of this inhaler was applied to thepatient's face, and through the opposite end etherwas dropped on to the stretched layers of bandage.There was, however, a considerable dead-space inthis inhaler.
It was not until some twenty years later, aboutI895, that another American, L. H. Prince, ofChicago, thought of adapting for etherisation theopen drop method used for chloroform anaesthesia.
"During the past two years," he wrote in. I897,"I have been using an ordinary Esmarch's chloro-form mask for administering ether, and have foundthat, as a rule, it answers the purpose very wellindeed, with the single exception that the smallsurface area delays the production of completeanesthesia in some cases. I am having made amask, similar in principle to the Esmarch, withsome modification in size and shape, that I feelconfident will answer the purposes of both chlorofonnand ether administration, at least until somethingbetter is presented."37
In America the open drop method of adminis-tering ether was developed at the Mayo Clinicduring the first ten years of the present century,and it was adopted in England about I908, anearly advocate being H. Bellamy Gardner.
During the opening years of this century opendrop ether was independently adopted by one ortwo German surgeons, notably C. Hofmann,38 ofCologne, and Oscar Witzel, of Bonn.39
Despite this new development, German interestin inhalation anaesthesia, and in ether anaesthesiain particular, had been declining since about I895.In the upper-abdominal surgery which Germansurgeons were then increasingly undertaking, post-operative chest complications were extremelyliable to follow, and a ready explanation for theiroccurrence appeared to lie in the use of etheranaesthesia. This explanation was widely acceptedalthough Campiche, of Lausanne, pointed out in
I902, that chest complications, far from beingprimarily due to the anaesthetic, were associatedwith certain types of surgery in which post-operative pain deterred the patient from riddinghimself of bronchial secretions by coughing.40Furthermore, the specialist anaesthetist was un-known on the European Continent, and theamount of skill shown by the inexperienced younghouse surgeons, to whom the task of administeringchloroform or ether -was relegated, was ofteninadequate. From the early eighteen-nineties on-wards a reasonably satisfactory way out of thisdifficulty was found-the surgeons themselvesprepared a painless operating field. This they dideither by adopting Schleich's method of infiltrationanaesthesia or, after I899, by using Bier's spinalanaesthesia, and a little later still, regional anaes-thesia.The example set in Germany was generally
followed on' the Continent, and a similar systetnhad been adopted in the United States, althoughthere the idea of training and employing specialistswas at the same time growing in favour.41
In Great Britain the Scots remained as they hadalways been, content with chloroform. But to theEnglish professional anaesthetist at the close ofthe nineteenth century, ether was still the anaes-thetic of choice in major surgery. The Continentaland American highly technical methods of localand regional anaesthesia not unnaturally madelittle appeal to him, trained as he was in therefinements of inhalation anaesthesia. Neverthe-less, he was not so much looking forwards asbackward-to chloroform anaesthesia. Whereasno important new type of inhaler had beendesigned for ether since Clover and Ormsby hadlaunched theirs in I877, the year I903 saw theHarcourt inhaler which, by limiting the amount ofchloroform in the inhaled mixture to a maximumof 2 per cent was, it was hoped, about to makechloroform anaesthesia safe at last.
REFERENCES
i. CORDUS, V. (I561), Annotationes in Pedacii Dioscoridis Anazarbeide materia medica hIbros quinque. Strasbourg. ff. 228v., 22gr.2. TALLMADGE, G. K. (1925), Isis, 7, 409-10.3. FROBENIUS, A. S. (I729-30), Philos. Trans., 36,283-9.4. BEDDOES, T., and WATT, J. (I796), Considerations on the Medicinal
Use of Factitious Airs. Bristol. 143.5. Note. (i8i8), Journal of Science, 4, 158-9.6. PEREIRA, J. (I839-40), The Elements of Materia Medica. London.
2o6.7. Report. (i846), Lancet, 1, 605.8. YOUNG, H. H. (I897), Johns. Hoph. Hosp. Bull., 8, i82,9. BIGELOW, H. J. (1847), Brit. Foreign Med. Rev., 13, 310.
lo. FORBES, -. (i847), Lond. Med. Gaz., 4, 38.ii. Report. (I846-7), Bull. Aced. Mid., Paris, 12, 262-3.12. WARREN, J. C. (I897), Trans. Amer. Surg. Ass., 15, 1-25.13, SNOW, J. (i858), On Chloroform and other Anaesthetics. London, 348.54. Report. (X847), London. Med. Gaz., 4, i56.I.5. Report. (1847), Lancet, 2, os2.I6. MARC-DUPUY, -. (1847), C.R. Acad. Sci., Paris, 24,605.17. PIROGOFF, N. I. Ibid., 789.x8. FLOURENS, P. J. M. Ibid., 482,I9. NUNNELEY, T. (1849), Trans. Provincial Med. Surg. Ass., N.S. 4,
268.jo. JONES, T. (I872), Brit. Med. J., 2, 603.az. Report. ,(864), Mod.-chir. Trais., 47, 331.
22. Discussion. (I87I), Med. Times, Lond., 2, 604.23. HAWARD, J. W. Ibid., 603.24. JEFFRIES, B. J. (I872), Lancet, 2, 24I-2.25. CLOVER, J. T. (I877), Brit. Med. J., 1, 69.26. ORMSBY, L. H. (I877), Lancet, 1, 2I8127. DUMONT, F. L. (1903), Handbuch er aligemeinen und lokalen
Anaesthesie. Berlin and Vienna. 37.28. WANSCHER, 0. (I884), Trans. Int. Congr. Med., 2(v), i86.29. Editorial. (I884) Boston Med. Surg. J., 110, 45I.30. BUXTON, D. W. (I892), Anaesthetics: their Uses and Administration.
London. 86-8.31. DUMONT, F. L., op. cit. 42.32. WOOD, H. C. (I89I), Trans. Int. Congr. Med., 1, 233.33. GURLT, E. (I89I), Dtsch. Med. Wschr., 17, 599; Ibid. (i89z),
18, 735.34. CHAPUT, P., et al. (i895), Bull. Soc. Chirurgie, Paris, 21, 368.35. SKINNER, T. (I862), Retrosp. Practical Med., 46, i85.36. TURNBULL, L. (i88o), The Advantages and Accidents of Artificial
Anaesthesia. London. 237.37. PRINCE, L. H. (i897), Chicago Med. Rec., 12, 232-40.38, HOFMANN, C. (I902), Dtsch. Z. Chir., 65,403-I6.39. WITZEL, 0. (I902), Muinch. Med. Wschr. 49(ii), I993-4.40. CAMPICHE, P. (I902), Contribution d l'dtude de la narcose a l'dther.
Geneva. boI-Io4.4I. Editorial (2897), Med. Rec., N.Y., 51, 522.
by copyright. on M
ay 28, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.22.252.280 on 1 O
ctober 1946. Dow
nloaded from
Illustrations
ETHER ANAESTHESIA, I842-1900
By
BARBARA M. DUNCUM, D.Phil.
..... .. ....... IW
.. ...
......~s ..
.... .....
FIG. i.-Valerius Cordus's description (circa. 1540) of the preparation and properties of sulphuric ether.
by copyright. on M
ay 28, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.22.252.280 on 1 O
ctober 1946. Dow
nloaded from
ETHER ANAESTHESIA, 1842-1900 BARBARA M. DUNCUM, D.Phil.
II
0'
[FIG. 2.-The inhaler used by Boott and Robinson in December, I846,[ for the first dental operation performed on an etherised patient in England.
A-
n\t
*- q$)-\*r
A. The Urn with its stopper, into which the ether is poured.B. Valve which admits the air.C. Contains sponge saturated with ether.D. Valve which opens at each Inspiration, and closes at each expiration.E. Ferule for regulating the quantity of atmospheric air admitted.F. Valve for the escape of expired air.G. Mouth-piece.H. Lower vase.S. Spring for closing the nose.
FIG. 3.-Squire's Ether Inhaler (December, I846).
by copyright. on M
ay 28, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.22.252.280 on 1 O
ctober 1946. Dow
nloaded from
ETHER ANAESTHESIA 1842-1900 BARBARA M. DUNCUM, D.Phil.
...MMCA..
FIG. 4a.-Snow's Ether Inhaler (I847) assem-bled, showing: A, the carrying case, servingalso as a water-bath; B, the vaporising cham-ber (see also Fig. 3b); C, opening into whichwas screwed the air-inlet tube D; E, openingabove B, from which the flexible tube F, ledthe ether-air mixture to the facepiece G, in thefloor of which can be seen the inspiratory flap-valve H; I, the facepiece removed (see alsoFig. 4b); S, diagram of the vaporising cham-ber B, showing the direction of the air flow.
FIG. 4b.-Details of Snow'sEther Inhaler. The facepiece,showing how the expiratoryflap-valve could be turnedaside (position shown in dot-ted outline) further to dilutethe ether-air mixture.
A bove.-The spirally coiled batHe-plate of the vaporising chamberwhich directed the current of airover the surface of the liquid.
..... -: .......... ..... .. ...........
:: ..: :..
FIG. 5.-Clover's "Portable RegulatingEther Inhaler" (I877).
4.,.-.
r,.0
F, I1.
I:-xl.-I.
il8'
FIG. 6.-Ormsby's Ether Inhaler(I877). Diagram showing: B, bag; C,cage holding sponge, S; 0, opening ofair-inlet tube, Fu; SI, slot in Fu, openedor closed bv the slotted cap, Ca.
by copyright. on M
ay 28, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.22.252.280 on 1 O
ctober 1946. Dow
nloaded from
ETHER ANAESTHESIA, 1892-1900 BARBARA M. DUNCUM, D.Phil.
/
FIG. 7a.
FIGS. 7a, b and c.-Dumont's modification of Julliard's Ether Mask,showing (a) the hinged, inner frame to hold in place the gauze and flannelrosette on to which the anaesthetic dose was poured; (b) the mask, withits impermeable cover, resting lightly on the face, and (c) the maskturned aside during administration, to allow the accumulated exhaledmixture to escape.
.9ft
FIG. 7b.
O) .
.: ...
FIG. 7C.
SiPs=FIG. 8.-Wanscher's Ether Inhaler, based upon Ormsby's.
FIG. 9.-Skinner's ChloroformMask, I862, prototype of theopen drop mask.
by copyright. on M
ay 28, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.22.252.280 on 1 O
ctober 1946. Dow
nloaded from