Embed Size (px)
Citation preview

2/29/2020
1
Nutrition in Solitary Kidney Care and Kidney Transplantation
“Opportunity to mitigate poor outcomes in individuals who give and persons who take”
Ekamol Tantisattamo, MD, FASN, FASTTransplant nephrologist
Assistant Clinical Professor of Medicine
Division of Nephrology, Hypertension and Kidney Transplantation
Department of Medicine
University of California Irvine School of Medicine
Nutritional and Dietary Management of Kidney Disease:
A Patient Care Approach
Saturday, February 29th, 2020 1
Disclosure
• None
2DO NOT
COPY

2/29/2020
2
Outline• Solitary kidney
– Epidemiology
– Etiology
• Living kidney donor– Complications
– Nutritional management
• Kidney transplant recipient– Outcomes
– Food security
– Nutrition management3
Why only 1 kidney?
4DO NOT
COPY

2/29/2020
3
Epidemiology of adult non-transplant solitary kidney
1McClung et al. J Trauma Acute Care Surg. 1262 2013;75:602–606. 2Hart et al. Kidney. Am J Transplant. 2019;19 Suppl 2:19-123.
3Shuch et al. Cancer. 2013;119:2981–2989. 5
Acquired solitary kidney
Renal traumaKidney
donationRenal cancer
• 126 / y 1 • 5,650 / y 2 • 269 / y 3
Average nephrectomy / year
• 31 y/o M • 35 – 45 y/o F • >60 y/o
Options for ESRD patients
Courtesy from Dr. John Friedewald, Comprehensive Transplant Center Northwestern University 6
End‐stage renal disease
Conservative Dialysis
Hemodialysis
Peritoneal dialysis
Kidney transplant
Living donor
Deceased (Cadaveric)
donor
Tolerance
Artificial kidney
DO NOT
COPY

2/29/2020
4
Living kidney donor
7
“Dedicated to true heroes
Those who give without wanting
Those who receive without forgetting”
UCSF Transplant Center
Care for living kidney donors
8
• Cardiovascular• Psycho‐social• Hypertension• Obesity
• Cardiovascular• Psycho‐social• Hypertension• Obesity
Pre‐donationPre‐donation
• Hypertension• Obesity• CKD (proteinuria),
ESRD• Psycho‐social
• Hypertension• Obesity• CKD (proteinuria),
ESRD• Psycho‐social
Post‐donationPost‐donation
SodiumSodiumProteinProteinDO NOT
COPY

2/29/2020
5
9
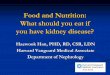
Unilateral native nephrectomy
Renal hemodynamic change Glomerular structural change
⇧ effective renal plasma flow
⇧single nephron GFR
Glomerular hyperfiltration
Glomerular hypertrophy⇧ Intraglomerular pressure
Podocyte injury
ProteinuriaGlomerulosclerosis
Pathways of cell regulation e.g.
• mTOR• IL-10• TGF-β
Secondary FSGS
Tantisattamo E, Dafoe DC, Reddy UG, Ichii H, Rhee CM, Streja E, Landman J, Kalantar-Zadeh K. Current Management of Acquired Solitary Kidney.
Kidney Int Rep: In Press
10
Unilateral nephrectomy
↓ Nephron mass
New GFR =
65 – 70% of pre-donation GFR
Compensatory mechanism
Delanaye et al. Nephrol Dial Transplant. 2012;27:41–50. DO NOT
COPY

2/29/2020
6
Medical complications from Living kidney donation
11
Chronic kidney disease (Proteinuria)
Hypertension
ESRD
Living donation VS. Proteinuria
Garg et al. Kidney Int. 2006;70(10):1801-10.
24‐h protein
Microalbumin
DO NOT
COPY

2/29/2020
7
13
Ref. ESRD(Living kidney donor vs. Controls)
Ibrahim et al., 2009 1 180 cases/million/year vs.
268 cases/million/year
Mjoen et al., 2014 2 Living donor had higher risk of ESRD (HR 11.38 (95% CI 4.37–29.6))
Muzaale et al, 2014 3 30.8 per 10,000 (95% CI, 24.3-38.5) vs.
3.9 per 10,000 (95% CI, 0.8-8.9)
Grams et al., 2016 4 3.5 to 5.3 times greater in living kidney donors compared to age-matched nondonors
1Ibrahim et al. N Engl J Med. 2009;360:459–469; 2Mjoen et al. Kidney Int. 2014;86:162–167. 1238
3Muzaale et al. JAMA. 1240 2014;311:579–586. 1241; 4Grams et al. N Engl J Med. 1243 2016;374:411–421
Risk of end-stage renal disease after kidney donation
Living donation VS. Hypertension
Boudville et al. Ann Intern Med. 2006;145(3):185-96.
SBP
DBP
DO NOT
COPY

2/29/2020
8
What is the top asked questions
from potential living kidney donors?
15
Diet in living kidney donor
16
Protein
Sodium
DO NOT
COPY

2/29/2020
9
Dietary protein intake
1717
Amount of protein
Sources of protein
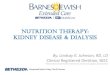
GFR vs. Dietary protein intake
18Cirillo et al. Nephrol Dial Transplant. 2015;30(7):1156-62.DO NOT
COPY

2/29/2020
10
High dietary protein intake in living kidney donor
19
Kidney donationKidney donation High protein dietHigh protein diet
Glomerular hyperfiltrationGlomerular hyperfiltration
↑ Intraglomerular pressure↑ Intraglomerular pressure
Kidney injuryKidney injury
CKDCKD
Ko GJ, Obi Y, Tortorici AR, Kalantar-Zadeh K. Curr Opin Clin Nutr Metab Care. 2017;20(1):77-85.
20
How low is low protein?
CKD
• eGFR <45 ml/min per 1.73 m2 or proteinuria >0.3 g/day
• Protein intake 0.6 –0.8 g/kg/day
Living kidney donor
• ???
• Protein intake ≤ 1 g/kg/day
Kalantar-Zadeh K, Fouque D. N Engl J Med. 2017;377(18):1765-76.DO NOT
COPY

2/29/2020
11
Sources of protein VS. CKD progression
21Haring et al. J Ren Nutr. 2017;27(4):233-42.
Animal protein Plant-based protein
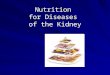
Na diet VS. CKD
22Yoon et al. Kidney Int. 2018;93(4):921-31.
Na 2.93 to 4.03 g/d
<2.08 g/d
Incident CKD was significantly longer in Q3 group then Q1 group.DO NOT
COPY

2/29/2020
12
Daily Na intake ≤ 4 g/day
??? >2 g/day
23Kalantar-Zadeh K, Fouque D. N Engl J Med. 2017;377(18):1765-76.
DO NOT
COPY

2/29/2020
13
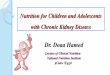
Trends of 10-year all-cause and cause-specific mortality among KTx recipients.
Awan et al. Am J Nephrol. 2018;48(6):472-481. DO NOT
COPY

2/29/2020
14
Mortality in living donor KTx recipients
Hart et al. OPTN/SRTR 2018 Annual Data Report: Kidney. Am J Transplant 2020;20 Suppl s1:20-130.
Risk factors for CVD in KTx recipients
Traditional • Age• Gender• DM• HTN• Smoking• Dyslipidemia• Renal function• Proteinuria
Nontraditional• Metabolic syndrome• Oxidative stress,
inflammation• Hyperparthyroidism• Anemia• Endothelial dysfunction• Hypoalbuminemia
CKD
KTx
Immunosuppression
Single kidney
DO NOT
COPY

2/29/2020
15
Advanced CKD or ESRDAdvanced CKD or ESRD Post-KTxPost-KTx
Diet Pre- vs. Post-KT
Food (in)security
30https://www.scrapehero.com/store/product/mcdonalds-store-locations-usa/
13,863.
(February 25, 2020)
DO NOT
COPY

2/29/2020
16
31
Food security in KTx recipientsFood security in KTx recipients
“All people, at all times, have access to sufficient, safe, nutritious food to maintain a healthy and active life”
World Food Summit, 1996
“All people, at all times, have access to sufficient, safe, nutritious food to maintain a healthy and active life”
World Food Summit, 1996
World Food Summit, 1996 Limb et al. NKF 2018 Spring Clinical Meetings Abstracts #188. AJKD Vol 71 | Iss 4 | April 2018 p562
24‐hour diet recall interview and analyzed using the USDA Supertracker
24‐hour diet recall interview and analyzed using the USDA Supertracker
Living farther from the grocery store Living farther from the grocery store
If food cost influenced food
choices
If food cost influenced food
choices
• ↓ Na, protein, PO4• ↓ Fast food• ↑Carb• ↑Others preparing meal• Not related to calorie, BMI
• ↓ Na, protein, PO4• ↓ Fast food• ↑Carb• ↑Others preparing meal• Not related to calorie, BMI
• ↑Prepared food• ↑ Stress• ↓ Vit D
• ↑Prepared food• ↑ Stress• ↓ Vit D
Nutrition in KTx
Macronutrients
• Fat
• Protein
• Carbohydrate
Micronutrients
• Sodium
• Phosphorus
32DO NOT
COPY

2/29/2020
17
Fat and Obesity
33
How come I cannot stop eating after KTx?
• 52 y/o White man
• eGFR >60
• BMI 37
https://www.google.com/search?tbm=isch&source=hp&biw=1264&bih=749&ei=Bj23W7TeIrjH0PEPw6-
VmAc&q=obesity&oq=obesity&gs_l=img.3..0l10.1818.2883..3270...0.0..0.87.567.7......2....1..gws-wiz-img.....0..35i39.g_65_1CvtgU#imgrc=XNy8lJzc2uGndM:DO N
OT COPY

2/29/2020
18
Pre- vs. Post-KTx
35
Pre-KTx Post-KTx
MortalityCardiovascular
Nutritional status • Sarcopenia• Malnutrition
• Weight gain- Overweight- Obese
36
Potential contributing factors for post-transplant weight gain and obesity
Tantisattamo E. Adv Obes Weight Manag Control. 2017;7(2):276‒279. DO NOT
COPY

2/29/2020
19
Causes of dyslipidemia post-KTxMedications
• Steroids
• Calcineurin inhibitors
• mTori
Other secondary causes
• Nephrotic syndrome
• Hypothyroidism
• Diabetes mellitus
• Excessive alcohol intake
• Obesity
• Chronic liver disease
• Genetic predisposition
• Low daily exercise
37
Diet recommendation for hyperlipidemic KTx patient
• 6-mo of moderate calorie-restricted AHA step 1 in hyperlipidemic pt with BMI >27
• Mediterranean diet rich in olive oil and polyunsaturated fatty acids
• Soy protein (rich in mono and polyunsaturated fatty acids and protoestrogens) -> ↓ total cholesterol and LDL
38DO NOT
COPY

2/29/2020
20
Fish oil vs. placeboHDL in KT recipient
Lim et al. Cochrane Database Syst Rev. 2016 Aug 18;(8):CD005282.
Total 15 RTC: 5 studies, 178 participants. Mean diff 0.12 mmol/L (95% CI 0.03 to 0.21)↑HDL, ↓Serum Cr (fish oild > 6 mo), ↓DBP
Protein40DO N
OT COPY

2/29/2020
21
41
Negative nitrogen balance during immediate post-KTx
↑ Hepatic gluconeogenesis
2/2 high dose steroids
↑ Hepatic gluconeogenesis
2/2 high dose steroids
Surgery-induced stress
Surgery-induced stress
Wound healingWound healing
Negativenitrogen balance
Negativenitrogen balance
Goral S, Bleicher MB. Handbook of Nutrition and the Kidney. Philadelphia, PA: Lippincott Williams and Wilkins (2010).
Nolte Fong JV and Moore LW. Front Med (Lausanne) 2018;5:302.
Guideline for post-KTx dietary protein intake
Post-KTx conditions Recommendation
Immediate post-KTx • ≥1.4 g/kg/day1
• 1.3-1.52
• 1.3-23
Regular review by a dietitian
Long-term (>4 mo post-KTx) • Female 0.75 g/kg/day1
• Male. 0.84 g/kg/day1
• <1 g/kg/day2
Treatment with high doses of prednisone e.g. acute rejection
• Same as immediate post-KTx1
Chronic renal allograft dysfunction • ? but >0.55 g/kg/day)1
1Chadban et al. Nephrology (Carlton) 2010;15 Suppl 1:S68-71. 2Goral S, Bleicher MB. Handbook of Nutrition and the Kidney. Philadelphia, PA: Lippincott Williams and Wilkins (2010). 3Nolte Fong JV and Moore LW. Front Med (Lausanne) 2018;5:302.DO N
OT COPY

2/29/2020
22
Carbohydrate &
Diabetes
43
44
Transplant-associated hyperglycemia (TAH)
Goral S, Bleicher MB. Handbook of Nutrition and the Kidney. Philadelphia, PA: Lippincott Williams and Wilkins (2010).
Insufficient insulin secretionInsufficient insulin secretion ↑Insulin metabolism(Possible unmasked pre‐KTx DM)
↑Insulin metabolism(Possible unmasked pre‐KTx DM)
TAHTAH
↑Insulin resistance↑Insulin resistance
DO NOT
COPY

2/29/2020
23
Risk factors E.g.
Non-modifiable • Advanced age• Male• Non-White• Family history
Modifiable • Obesity• Physical inactivity• Weight gain• HCV• Immunosuppressive medications
Risk factors for TAH
Goral S, Bleicher MB. Handbook of Nutrition and the Kidney. Philadelphia, PA: Lippincott Williams and Wilkins (2010).
Diet recommendation for TAH
• Daily CHO 130– 180 g/day
• 1,800 – 2,000 Kcal/day
• Complete avoidance of concentrated sweets
46Goral S, Bleicher MB. Handbook of Nutrition and the Kidney. Philadelphia, PA: Lippincott Williams and Wilkins (2010). DO N
OT COPY

2/29/2020
24
Nutrition in KTx
Macronutrients
• Fat
• Protein
• Carbohydrate
Micronutrients
• Sodium
• Phosphorus
• Magnesium
47
Sodium48DO N
OT COPY

2/29/2020
25
Daily Na intake and on post-KTx HTN
Soypacaci et al. DTransplant Proc 2013;45:940-943.
Dietary Na suggestion• 2,000 mg of Na per day esp. h/o HTN
• Choose fresh, frozen, or canned food items without added salt.
• Limit the amount of salty snacks.
• Avoid adding salt when cooking or at the dinner table.
• Select unsalted or reduced sodium versions of broth, soups, and other processed foods.
• Spices and herbs in place of salt when cooking.
Phillips S and DeMello S. J Ren Nutr 2014;24:e15-17.DO NOT
COPY

2/29/2020
26
Phosphorus
51
Should I drink more Coca Cola after KTx?
• 60 y/o Hispanic man
• eGFR >60
• Serum PO4 2
• On K-PO4-Neutral
kreg.steppe via http://www.flickr.com/photos/spyndle/5047889128/ Creative Commons
DO NOT
COPY

2/29/2020
27
Post-KTx hypophosphatemia
KTx
TacrolimusFGF23 remains
elevatedPTH remains elevated
Hypophosphatemia
• ↑Renal Pi excretion• ↓Intestinal Pi absorption• ↓1-alpha hydroxylation
• ↑Renal Pi excretion• ↓NaPi2a• ↑Renal Pi excretion
Blaine et al. Clin J Am Soc Nephrol 2015;10:1257-1272.
Nolte Fong JV and Moore LW. Front Med (Lausanne) 2018;5:302.
Post-KTx hypophosphathemiaDiet modification
• 3 sources of phosphorus• Organic phosphorus in plant foods
• Organic phosphorus in animal protein
• Inorganic phosphorus
• Phosphate rich foods e.g. whole grains, eggs, poultry, fish, and dairy products
• When good graft functionWickham E. J Ren Nutr 2014;24:pp e1-e4.
Watanabe et al. Clin Nutr ESPEN. 2016 Aug;14:37-41.
Pochineni V and Rondon-Berrios H. Front Med (Lausanne) 2018;5:261.DO NOT
COPY

2/29/2020
28
55Gomes-Neto et al. Clin J Am Soc Nephrol. 2020 Feb 7;15(2):238-246.
Food security in KTx recipients
56
Environment &
Place to live
Environment &
Place to live
Food costPolicy
Regulations
Food costPolicy
Regulations
• Protein, CHO, fat• Na, K, PO4• Protein, CHO, fat• Na, K, PO4
• ↑ Stress• ↓ Vit D• ↑ Stress• ↓ Vit D
Food choicesFood choices
Social & Family support
Social & Family support
• ?Calorie• ?BMI• ?Calorie• ?BMI
• Prepared food• Fast food• Prepared food• Fast food
Education from providers
Education from providers
DO NOT
COPY

2/29/2020
29
Conclusions
• Living kidney donation is the most common cause of acquired solitary kidney in adults.
• Secondary FSGS is pathophysiologic change after unilateral nephrectomy.
• Long-term complications include CKD / ESRD, HTN, and proteinuria.
Conclusions
• Nutrition management should be one of the main strategies for the care after nephrectomy; although, there is a lack of evidence.
• Post-KTx immunological and non-immunological factors leads to complex nutrition-related conditions but provide opportunities to intervene and improve post-KTx outcomes.
• While waiting for evidences of nutritional management in KTxrecipients, secure food with education from all of us should help to mitigate poor renal and patient outcomes.
DO NOT
COPY

2/29/2020
30
Acknowledgements
• Dr. Kalantar for his advice of his mentorship and preparation for this talk.
• Faculty and staff, Division of Nephrology, Hypertension and Kidney transplantation
• UCI Medical Center and School of Medicine
• Our patient (both give and take) to motive our learning to improve our patient care
59
References
1: Hart A, Smith JM, Skeans MA, Gustafson SK, Wilk AR, Castro S, Foutz J,Wainright JL, Snyder JJ, Kasiske BL, Israni AK. OPTN/SRTR 2018 Annual Data Report: Kidney. Am J Transplant. 2020 Jan;20 Suppl s1:20-130. doi: 10.1111/ajt.15672. PubMed PMID: 31898417.
2: Gomes-Neto AW, Osté MCJ, Sotomayor CG, van den Berg E, Geleijnse JM, Berger SP, Gans ROB, Bakker SJL, Navis GJ. Mediterranean Style Diet and Kidney Function Loss in Kidney Transplant Recipients. Clin J Am Soc Nephrol. 2020 Feb 7;15(2):238-246. doi: 10.2215/CJN.06710619. Epub 2020 Jan 2. PubMed PMID: 31896540.
3: Awan AA, Niu J, Pan JS, Erickson KF, Mandayam S, Winkelmayer WC, NavaneethanSD, Ramanathan V. Trends in the Causes of Death among Kidney Transplant Recipients in the United States (1996-2014). Am J Nephrol. 2018;48(6):472-481.doi: 10.1159/000495081. Epub 2018 Nov 23. PubMed PMID: 30472701; PubMed Central PMCID: PMC6347016.
4: Nolte Fong JV, Moore LW. Nutrition Trends in Kidney Transplant Recipients: the Importance of Dietary Monitoring and Need for Evidence-Based Recommendations. Front Med (Lausanne). 2018 Oct 31;5:302. doi: 10.3389/fmed.2018.00302. eCollection 2018. Review. PubMed PMID: 30430111; PubMed Central PMCID: PMC6220714.
5: Pochineni V, Rondon-Berrios H. Electrolyte and Acid-Base Disorders in the Renal Transplant Recipient. Front Med (Lausanne). 2018 Oct 2;5:261. doi: 10.3389/fmed.2018.00261. eCollection 2018. Review. PubMed PMID: 30333977; PubMed Central PMCID: PMC6176109.
DO NOT
COPY

2/29/2020
31
References
6: Merhi B, Shireman T, Carpenter MA, Kusek JW, Jacques P, Pfeffer M, Rao M, Foster MC, Kim SJ, Pesavento TE, Smith SR, Kew CE, House AA, Gohh R, Weiner DE, Levey AS, Ix JH, Bostom A. Serum Phosphorus and Risk of Cardiovascular Disease, All-Cause Mortality, or Graft Failure in Kidney Transplant Recipients: An Ancillary Study of the FAVORIT Trial Cohort. Am J Kidney Dis. 2017 Sep;70(3):377-385. doi: 10.1053/j.ajkd.2017.04.014. Epub 2017 Jun 2. PubMed PMID: 28579423; PubMed Central PMCID: PMC5704919.
7: Watanabe MT, Araujo RM, Vogt BP, Barretti P, Caramori JCT. Most consumed processed foods by patients on hemodialysis: Alert for phosphate-containing additives and the phosphate-to-protein ratio. Clin Nutr ESPEN. 2016 Aug;14:37-41. doi: 10.1016/j.clnesp.2016.05.001. Epub 2016 Jun 1. PubMed PMID: 28531397.
8: Pranger IG, Gruppen EG, van den Berg E, Soedamah-Muthu SS, Navis G, Gans RO, Muskiet FA, Kema IP, Joosten MM, Bakker SJ. Intake of n-3 fatty acids and long-term outcome in renal transplant recipients: a post hoc analysis of a prospective cohort study. Br J Nutr. 2016 Dec;116(12):2066-2073. doi: 10.1017/S0007114516004207. Epub 2016 Dec 20. PubMed PMID: 27993180.
9: Lim AK, Manley KJ, Roberts MA, Fraenkel MB. Fish oil for kidney transplant recipients. Cochrane Database Syst Rev. 2016 Aug 18;(8):CD005282. doi: 10.1002/14651858.CD005282.pub3. Review. PubMed PMID: 27535773.
10: Rathi M, Rajkumar V, Rao N, Sharma A, Kumar S, Ramachandran R, Kumar V, Kohli HS, Gupta KL, Sakhuja V. Conversion from tacrolimus to cyclosporine in patients with new-onset diabetes after renal transplant: an open-label randomized prospectivepilot study. Transplant Proc. 2015 May;47(4):1158-61. doi: 10.1016/j.transproceed.2014.12.050. PubMed PMID: 26036543.
References
11: Pirsch JD, Henning AK, First MR, Fitzsimmons W, Gaber AO, Reisfield R, Shihab F, Woodle ES. New-Onset Diabetes After Transplantation: Results From a Double-Blind Early Corticosteroid Withdrawal Trial. Am J Transplant. 2015 Jul;15(7):1982-90. doi: 10.1111/ajt.13247. Epub 2015 Apr 16. PubMed PMID: 25881802.
12: Blaine J, Chonchol M, Levi M. Renal control of calcium, phosphate, and magnesium homeostasis. Clin J Am Soc Nephrol. 2015 Jul 7;10(7):1257-72. doi: 10.2215/CJN.09750913. Epub 2014 Oct 6. Review. Erratum in: Clin J Am Soc Nephrol. 2015 Oct 7;10(10):1886-7. PubMed PMID: 25287933; PubMed Central PMCID: PMC4491294.
13: Phillips S, DeMello S. Nutrition and the kidney donor. J Ren Nutr. 2014 Mar;24(2):e15-7. doi: 10.1053/j.jrn.2013.12.001. PubMed PMID: 24559894.
14: McKane CK, Marmarelis M, Mendu ML, Moromizato T, Gibbons FK, Christopher KB. Diabetes mellitus and community-acquired bloodstream infections in the critically ill. J Crit Care. 2014 Feb;29(1):70-6. doi: 10.1016/j.jcrc.2013.08.019. Epub 2013 Oct 3. PubMed PMID: 24090695.
15: Soypacaci Z, Sengul S, Yıldız EA, Keven K, Kutlay S, Erturk S, Erbay B. Effect of daily sodium intake on post-transplant hypertension in kidney allograft recipients. Transplant Proc. 2013 Apr;45(3):940-3. doi: 10.1016/j.transproceed.2013.02.050. PubMed PMID: 23622593.
DO NOT
COPY

2/29/2020
32
References
16: Pascual J, Royuela A, Galeano C, Crespo M, Zamora J. Very early steroid withdrawal or complete avoidance for kidney transplant recipients: a systematic review. Nephrol Dial Transplant. 2012 Feb;27(2):825-32. doi: 10.1093/ndt/gfr374. Epub 2011 Jul 22. Review. PubMed PMID: 21785040.
17: Chadban S, Chan M, Fry K, Patwardhan A, Ryan C, Trevillian P, Westgarth F, CARI. The CARI guidelines. Protein requirement in adult kidney transplant recipients. Nephrology (Carlton). 2010 Apr;15 Suppl 1:S68-71. doi: 10.1111/j.1440-1797.2010.01238.x. PubMed PMID: 20591048.
18: Woodle ES, First MR, Pirsch J, Shihab F, Gaber AO, Van Veldhuisen P; Astellas Corticosteroid Withdrawal Study Group. A prospective, randomized, double-blind, placebo-controlled multicenter trial comparing early (7 day) corticosteroid cessation versus long-term, low-dose corticosteroid therapy. Ann Surg. 2008 Oct;248(4):564-77. doi: 10.1097/SLA.0b013e318187d1da. PubMed PMID: 18936569.
19: Rettkowski O, Wienke A, Hamza A, Osten B, Fornara P. Low body mass index in kidney transplant recipients: risk or advantage for long-term graft function? Transplant Proc. 2007 Jun;39(5):1416-20. PubMed PMID: 17580151.
20: Vincent AM, Russell JW, Low P, Feldman EL. Oxidative stress in the pathogenesis of diabetic neuropathy. Endocr Rev. 2004 Aug;25(4):612-28. Review. PubMed PMID: 15294884.
References
21: Hasse JM. Nutrition assessment and support of organ transplant recipients. JPEN J Parenter Enteral Nutr. 2001 May-Jun;25(3):120-31. Review. PubMed PMID: 11334061.
22: Terranova A. The effects of diabetes mellitus on wound healing. Plast Surg Nurs. 1991 Spring;11(1):20-5. PubMed PMID: 2034714.
DO NOT
COPY

2/29/2020
33
g{tÇ~ çÉâ
DO NOT
COPY