Embed Size (px)
Citation preview

Journal of Mammary Gland Biology and Neoplasia, Vol. 3, No. 1, 1998
Estrogen Responsiveness and Control of Normal HumanBreast Proliferation
Elizabeth Anderson,1,3 Robert B. Clarke,1 and Anthony Howell2
Our understanding of the hormonal control of the proliferation of normal human breast epithe-
lium is still surprisingly meager. However, the results of a number of recent studies have
confirmed that estrogen is the major steroid mitogen for the luminal epithelial cell population
(the usual targets for neoplastic transformation). Estrogen seemingly exerts its effects on cell
division indirectly as there is complete dissociation between the population of luminal epithelial
cells expressing the estrogen receptor (ER)4 and those that proliferate. We suggest that the
ER-negative proliferating cells represent a precursor or stem cell population that differentiates
to ER-containing, nonproliferative cells. In turn, these ER-positive cells act as ` estrogen
sensors’ and transmit positive or negative paracrine growth signals to the precursor cells
depending on the prevailing hormonal environment. As yet there is no direct evidence supporting
this hypothesis but we suggest ways in which it may be obtained. The implication of these
studies is that inhibition of luminal epithelial proliferation with tamoxifen or pure antiestrogens
or by preventing ovarian steroid secretion should be an effective strategy for the prevention
of breast cancer. In addition, we may be able to predict the risk of breast cancer in an individual
by measuring the intrinsic estrogen sensitivity of her breast epithelium. Finally, study of the
paracrine mechanisms of growth control in the normal human breast may provide new, more
specific, therapeutic targets for breast cancer prevention.
KEY WORDS: Human breast; proliferation; estrogen; estrogen receptor.
INTRODUCTION normal breast development, yet we still do not know
exactly how the ovarian steroids exert their effects.In 1984 Jean McManus and Clifford Welsch One reason is that endocrine regulation of breast devel-
wrote, ª The hormonal control of development, growth opment is difficult to study in normal women. Weand differentiation in vivo of the human breast is, cannot obtain normal human tissue at will nor can weunfortunately, still an enigmaº (1). In 1997, our under- manipulate the hormonal environment of the normalstanding of normal human breast growth and develop- breast at will. Consequently, we are reliant on tissuement is still surprisingly incomplete. We accept almost obtained at surgery for the removal of benign lesions oras a fact of life that intact ovaries are required for for breast reduction with attendant reservations about
whether these conditions are really representative of
the normal situation. Because of these constraints,1 Clinical Research Department, Christie Hospital NHS Trust, Wil-important new insights into the effects of ovarian ste-mslow Rd, Manchester M20 4BX.roids on the normal human breast and their underlying2 CRC Department of Medical Oncology, Christie Hospital NHS
Trust, Wilmslow Rd, Manchester M20 4BX. mechanisms are only now emerging.3 To whom correspondence should be addressed. e-mail: The major histological unit of the human breast
[email protected] an.ac.ukis the lobular structure arising from a terminal duct.4 Abbreviations: estrogen receptor (ER); thymidine labeling indexThis structure consists of several small, blind-endingin percent (TLI); epidermal growth factor receptor (EGFR); pro-
gesterone receptor (PR). ductules lined by a continuous layer of luminal epithe-
231083-3021/98/0100-0023$1 5.00/0 q 1998 Plenum Publishing Corporation

24 Anderson, Clarke, and Howell
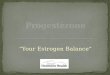
lial cells surrounded by a second layer of myoepithelial the normal human breast throughout the menstrual
cycle (10±16). In these, and all subsequent studies,cells (Fig. 1). The myoepithelial cells are in direct
contact with the basement membrane and the whole our strategy has been to use normal tissue obtained
either at reduction mammoplasty or at operation forstructure is surrounded by delimiting fibroblasts and
a specialized intra-lobular stroma. The lobule in the the removal of a fibroadenoma (with informed con-sent). We chose to study patients with fibroadenomasnon-pregnant, non-lactating woman is a surprisingly
dynamic structure; several studies have shown that because they were the largest source of relatively
young, pre-menopausal breast tissue and, at the timethere is considerable cyclical variation in the morpho-
logical appearance of the epithelium as well as the of initiating these studies, fibroadenomas were thought
not to be associated with an increased risk of breaststroma and components of the surrounding extracellu-
lar matrix (2±6). Our comments will be restricted to cancer. However, more recently, the relationshipbetween the presence of a fibroadenoma and the riskthe cyclical variation and hormone responsiveness of
the luminal epithelial cells where human breast tumors of breast cancer has become less certain with one group
reporting up to an approximately two-fold increase inappear to arise. Careful histological examination
shows that most human breast tumors are morphologi- relative risk (17). This finding clearly demonstrates
the difficulty in obtaining truly normal human breastcally similar to luminal epithelial cells (7). In addition,
most tumors retain the biochemical characteristics of tissue for the study of hormonal control of function.Although the situation is not ideal, we are continuingluminal cells; for example, they express the same
cytokeratin profile (8), steroid receptors and polymor- to use tissue from fibroadenoma patients in addition
to that from reduction mammoplasties because thesephic epithelial mucin (9). Thus, the purpose of the
present article is to review the cyclical changes in the patients represent the largest group in which we can
study pre-menopausal breast function and becauseluminal epithelial cell population of the normal humanbreast together with the evidence for the estrogenic other benign lesions such as hyperplasia are associated
with a much greater risk of breast cancer. Howevercontrol of these changes that has been generated in invitro and in vivo experimental studies. These studies we have ensured that none of the patients we studied
had a family history of breast cancer although aboutare of more than academic interest; we cannot hope
to develop new, more effective strategies for cancer a quarter were using oral contraceptives at the time
of surgery.prevention if we do not understand how the factorsthat increase breast cancer risk affect the development The proliferative activity of normal tissue taken
at different times of the menstrual cycle was measuredof the normal human mammary epithelium.
by incubation with tritiated thymidine ([3H]-dT) and
subsequent calculation of a thymidine labeling indexCYCLICAL VARIATION IN
from autoradiography of tissue sections (TLI; percentPROLIFERATION AND STEROID RECEPTOR
cells labeled with [3H]-dT). We found considerableEXPRESSION IN NORMAL BREAST
inter-individual variation between the TLIs that couldLUMINAL EPITHELIAL CELLS
not be attributed to assay variability (10); nevertheless,
proliferation was clearly elevated in the luteal phaseWe and several other groups have examined theof the cycle. This result is in agreement with those ofproliferative activity of luminal epithelial cells withinthe other groups who have also found the proliferative
activity of normal human breast epithelial cells to behigher in the last half of the cycle (11±16). Detailed
analysis of other kinetic parameters such as the mitotic
and apoptotic indices showed a similar pattern of
change in that they, also, were higher in the second
half of the cycle compared to the first, although theapoptotic index reached a maximum approximately
three days after the peak of proliferative activity (13).
Cyclical variation in epithelial expression of other pro-
teins related to the proliferative and apoptotic pro-
cesses has also been shown. For example, Sabourin etFig. 1. The arrangement of epithelial cell types in the lobules
of the normal human breast. al. (18) showed that the anti-apoptotic protein bcl-2

Estrogen Responsiveness and Control of Normal Human Breast Proliferation 25
reached peak levels in the middle of the cycle (days when progesterone levels rise in the early luteal phase
(19). Such observations have led several groups to13±17) and fell to a nadir at the time when apoptosis
was greatest. suggest that, unlike the endometrium, the major steroid
mitogen for breast epithelial cells is progesterone eitherThe pattern of change in breast epithelial prolifer-
ative activity throughout the cycle contrasts directly alone or after estradiol priming. Likewise there appearto be important differences in the control of PR expres-with that seen in the endometrium. In this tissue, prolif-
eration is highest in the follicular phase of the cycle sion between the two tissues; the cyclical variation of
PR expression in the endometrium suggests that it isand falls rapidly at the beginning of the luteal phase;
it is almost undetectable in the later stages of the cycle an estrogen-inducible protein (28) whereas the lack of
variation in PR expression in the breast suggests that(19,20). Despite these differences, we assumed that
the cyclical variation in breast epithelial cell prolifera- it might be constitutively expressed. In order to investi-gate the hormonal control of function further, manytion was related in some way to the changes in ovarian
steroid secretion and we wanted to know whether groups have turned to experimental systems where the
steroid exposure of breast epithelial tissue or cells canexpression of the receptors for estrogen and progester-
one (ER and PR) also varied. We found that approxi- be manipulated. Such systems will be reviewed later
but we also hope to show that novel data on the hor-mately 5% of luminal epithelial cells expressed the
ER as determined immunocytochemically on frozen monal control of human breast function can be gleanedfrom relatively simple observations on tissue obtainedsections of the normal tissue used for the proliferative
studies (21, see also 24). The number of cells express- at operation.
ing ER was highest in the follicular phase of the cycle
and was inversely correlated with the TLI. In contrast,
15±20% of epithelial cells expressed the PR and theproportion did not vary during the cycle when mea- NORMAL HUMAN BREAST EPITHELIALsured immunocytochemically on frozen sections of CELLS IN CULTUREnormal breast tissue. A few other groups have exam-
ined steroid receptor expression in normal human
breast tissue throughout the menstrual cycle. The The establishment of human breast epithelial cell
cultures that replicate and retain their original charac-results of these studies are in agreement with those ofour own investigations and show that ER protein is teristics has proved extraordinarily difficult despite the
development of a number of different strategies formore readily detected in tissue removed in the follicu-
lar phase of the cycle compared to the luteal phase epithelial cell isolation and culture. These include sep-
aration of the luminal and myoepithelial cell popula-(22±24). The other groups were also able to show
that PR expression in the normal breast does not vary tions on the basis of specific cell surface antigens (29),
allowing the cells to immortalise spontaneously (30),appreciably during the cycle.Epithelial cell expression of receptors other than immortalization with the SV40 tumor or human papil-
loma viruses (31±34) or mutated tumor suppressorthose for steroids also varies throughout the cycle. For
example, Gompel et al. (25) showed that epidermal genes (35), culture on or in different extracellular
matrix components (36±39) or combinations of thesegrowth factor receptors (EGFR) are more highly
expressed in the luteal phase of the cycle compared approaches (31,37). Studies on epithelial cells cultured
using these techniques have produced much valuablewith the follicular phase. This finding may not besurprising in the light of studies on human breast and interesting data on, for example, the peptide
growth factors that stimulate growth (40±42) and thetumors showing that EGFR and ER expression are
generally inversely related (26). conditions required for branching morphogenesis and
ductule formation (37,39,43). Almost universally theseThe obvious candidates for the control of cyclical
changes in the breast epithelial cell population are methods have failed to produce cultured luminal epi-thelial cells that express steroid receptors and are capa-estradiol and progesterone since they are produced
cyclically by the ovaries (27). Maximal breast prolifer- ble of responding to ovarian steroids. To date, there
are only two reports of the isolation of steroid receptoration coincides with the mid-luteal phase peaks of
estradiol and progesterone secretion whereas prolifera- expressing human mammary epithelial cells. In the
first study, the cultured epithelial cells expressed bothtion of the endometrium, a ª classicalº estrogen target
organ is highest in the follicular phase and declines the ER and the PR and treatment with estradiol not only

26 Anderson, Clarke, and Howell
increased proliferation but also enhanced expression of NORMAL HUMAN BREAST EPITHELIUMIMPLANTED INTO ATHYMIC NUDEboth types of receptor suggesting that estradiol is theMICEovarian steroid that stimulates luminal epithelial cell
proliferation (44). However, the cells used in this par-Because cultures of primary or immortalizedticular study were obtained at operation for fibrocystic
human breast luminal epithelial cells have proved todisease and may have been derived from the lesionbe poor models for the study of steroid responsiveness,rather than the normal epithelium. In the second study,many researchers, including ourselves, have turned tohuman mammary epithelial cells isolated from reduc-in vivo models of normal human breast tissuetion mammoplasties and immortalised with SV40 wereimplanted into athymic nude mice.found to express a splice variant of the ER (45). This
A system of implanting intact human breast tissueER variant contained a deletion in exon 2 (the DNA-into athymic nude mice was developed in the late 1970sbinding domain) and did not bind to an artificial EREin response to a perceived lack of suitable modelsin gel mobility shift assays. These results imply thatin which the hormonal control of proliferation andthese particular cells were incapable of responding tofunction could be studied (1). In these particular exper-estradiol treatment although this was not shown. Asiments, small pieces of tissue taken from the peripher-far as is known, none of the other studies involvingies of benign breast lesions were implantedisolation of cells from reduction mammoplasties havesubcutaneously into intact female athymic nude mice.produced ER-expressing human luminal epithelialThe mice were subsequently treated with estradiol,cells.progesterone , thyroxine or human placental lactogenThere have been attempts to restore receptoreither singly or in combination and tissue pieces wereexpression in cultures of immortalized human breastretrieved at different time points after the start of treat-epithelial cells by transfection with an ER-expressionment for measurement of proliferative activity by [3H]-vector (46±48). These attempts have successfully pro-dT uptake. This particular study showed, for the firstduced high level ER protein expression but in onlytime, that human breast epithelial cell proliferation
one did subsequent treatment with estradiol stimulatecould be stimulated by estradiol (1). Thyroxine also
proliferation and even then the effect was small (48).stimulated proliferation, human placental lactogen
More often, transfection of ER resulted in the oppositealone was without effect although it enhanced the
effect in that treatment of the transfected cells withactivity of estradiol when given in combination. In
estradiol inhibited proliferation (46,47). One explana-contrast, progesterone did not alter the proliferative
tion for these findings is that the negative effects ofactivity of the breast epithelium either alone or in
estradiol on ER negative cells transfected with ER iscombination with the other agents. At about the same
that the exogenous receptor interferes with ortime, other experiments were being carried out in
` squelches’ the transcriptional factors used to maintainwhich partially enzymatically digested breast tissue
estrogen-independent growth (46). Why over expres-(` organoids’ ) was implanted into intact mammary fat
sion of ER in the MCF-7 cells does not ` squelch’ the pads of athymic nude mice or fat pads that had beentranscriptional factors involved in estrogen-dependent cleared of parenchyma (49±51). In all these reports,growth is not well understood. However, it is becoming the partially digested human tissue re-organized itselfclear that the activity of the ER is highly dependent into primitive glandular structures. Only one groupupon its cellular context and it is possible that the examined the estrogen-responsiveness of such tissueER negative cell lines do not provide the appropriate implants and showed that estradiol did, indeed, stimu-environment in terms of co-factors for correct function late proliferation (50). The other groups concentratedof the exogenous ER (46). At present, it is not known on demonstrating a lactational response in the humanwhy the ER-expressing cells that have been shown to tissue after administration of lactogenic hormones orexist in the luminal epithelial cell population in vivo after mating the xenograft-bearing mice (49,51). Muchdo not survive to grow in vitro. If we could determine later, a response to estrogen treatment was demon-why this happens we might gain valuable new informa- strated in a system where human breast epithelial cells,tion about the steroidal control of proliferation in the dissociated from reduction mammoplasty specimens,normal human breast epithelium as well as an answer were embedded in extracellular matrices (type I colla-to the question of why such a large proportion of breast gen and Matrigel) before being implanted subcutane-
ously into the nude mice (52). Again, the breasttumors contain ER.

Estrogen Responsiveness and Control of Normal Human Breast Proliferation 27
epithelial cells were shown to have organized them- The results of our experiments on the effects of
estradiol and progesterone on the proliferation ofselves into primitive branching ductal structures inhuman breast tissue implanted into the athymic nudeboth types of extracellular matrix and there were prolif-mice were described in detail by Laidlaw et al. (53).erative responses to estradiol, cholera toxin and epider-Briefly, when human breast tissue was implanted intomal growth factor (EGF).female, intact, adult mice that received no further treat-These experiments showed that the hormonalment, the TLI of the epithelial cells fell from approxi-environment of normal human breast tissue could, atmately 2% at the time of removal from the patient tolast, be relatively easily manipulated following implan-0.5%, two weeks after implantation. This low level oftation into athymic nude mice. However, very fewproliferation was maintained for at least eight weeksgroups continued to pursue this approach possiblyin the untreated mice as was the structure and integritybecause the experiments were tedious and time-con-of the tissue. Raising the serum estradiol levels suchsuming and because specialist animal facilities werethat they approximated human peak luteal phase levelsrequired. Nevertheless, we decided to revisit the exper-( , 1300 pmol/l) significantly increased the prolifera-iments of McManus and Welsch (1) to further investi-tive activity of the epithelial cells whereas progester-gate the estrogenic response in normal human breastone, also at peak luteal levels, was without effect eithertissue. We decided to implant pieces of intact tissuealone or after priming with luteal phase estradiol levels.into non-ovariectomized adult female mice for severalThe proliferative response to estradiol was dose-depen-reasons, some of them rather pragmatic. Firstly, thedent between median serum estradiol levels of 400 touse of intact pieces of tissue would maintain the archi-1300 pmol/l which were representative of the rangetecture of the normal human breast tissue and the rela-seen during the human menstrual cycle. Raising estra-tionship between the epithelial and stromaldiol levels to those of early pregnancy (a median ofcompartments. Secondly, implantation subcutaneously4400 pmol/l) had no further effect. Thus we confirmedrather than into the mammary fat pad was adoptedthe results of McManus and Welsch (1) and providedbecause it was felt that it would be a less invasivefurther evidence to support the role of estradiol as the
procedure and because the pieces of tissue wouldmajor ovarian steroid mitogen for the normal human
remain easily accessible for serial sampling. Thirdly,breast. Progesterone appeared to be neutral with
implanting intact tissue would be much less time con-respect to its effects on breast epithelial cells in that
suming than using enzymatically disaggregatedit neither stimulated nor inhibited proliferation.
organoids. Finally, we used intact female mice as ovari-We obtained some very interesting results when
ectomy would add another level of complexity to thewe examined steroid receptor expression in the normal
experiments and would be associated with significanthuman breast tissue after estradiol and progesterone
intra- and post-operative mortality. We measured thetreatment. The percentage of normal epithelial cells
endogenous serum estradiol levels in the strain of micethat expressed the ER fell from , 5% when removed
used in our experiments and found them to be lessfrom the patients to , 1% after the two week control
than 100 pmol/l which is equivalent to those found in period and subsequent treatment with estradiol andpost-menopausal women (53). Thus, our first aim was progesterone either alone or in combination had noto confirm the results of McManus and Welsh (1) using further effect. This reduction in the proportion of epi-histologically confirmed normal tissue as opposed to thelial cells expressing the ER may have resulted fromtissue obtained from the periphery of diffuse benign the low levels of circulating estradiol in the untreatedlesions. We also aimed to use calibrated slow-release nude mice ( , 100 pmol/l) or may be related to theestradiol silastic pellets designed to deliver serum lev- immunocytochemical assay used at that time whichels that approximated those in the human menstrual was not very sensitive, especially after it had beencycle instead of the schedule of McManus and Welsch adapted for application to tissue after it had been xeno-(1) which resulted in uncertain amounts of estradiol grafted. The proportion of luminal epithelial cells thatand estrone being administered to the mice. Our third expressed PR was also very small after two weeks inaim was to examine the effects of steroid treatment the untreated mice. However, a 15±20 fold increase inon receptor expression in the breast tissue implants the percentage of cells expressing PR was seen inbecause suitable methods for the immunocytochemical the normal tissue xenografts after 7 and 14 days ofdetection of ER and PR in small tissue samples had, treatment with estradiol at luteal phase levels. Proges-
terone at luteal phase levels was without effect on theby then, been developed.

28 Anderson, Clarke, and Howell
expression of either of the receptors. These results
suggested that the PR is an estrogen-regulated protein
in normal human breast epithelial cells. This finding
was rather surprising given that studies on breast epi-
thelium throughout the menstrual cycle in vivo showedthat PR expression remained high through the men-
strual cycle. These data had, in turn, been interpreted
to mean that synthesis of the receptor might be consti-
tutive (shown earlier). Accordingly, we carried out
more detailed investigations into the control of PR
expression in normal human breast epitheliumimplanted into the athymic mice with the specific aim
of determining why PR expression did not change
throughout the cycle in women in vivo (54).
PROLIFERATION AND PR EXPRESSIONARE DIFFERENTIALLY SENSITIVE TOESTROGEN
Our first approach to resolving the discrepancy
in PR expression between our experiments on normalhuman breast implanted into athymic mice and the
studies on normal breast throughout the menstrual
cycle was to determine both PR expression and prolif-
erative activity in xenografts removed from mice
treated with different levels of estradiol (54).Fig. 2. Effects of estradiol treatment at differing concentrations onFigure 2A shows the results of the immunocyto-normal human breast tissue implanted into athymic nude mice.chemical detection of PR in sections cut from Carnoy’ s(A) Epithelial cell PR expression. (B) Epithelial cell proliferation
fixed paraffin-embedded specimens of human breastmeasured by the TLI. The columns represent the interquartile ranges
tissue xenografts retrieved from mice after treatment of the measurements whereas the bars indicate the median values.
with follicular or luteal phase levels of estradiol. As P 5 progesterone; Lo 5 follicular phase levels of estradiol; Hi 5luteal phase levels of estradiol; Hi,14 5 14 day treatment withbefore, PR expression was almost undetectable inluteal phase levels of estradiol; * 5 p , 0.001 compared with thebreast tissue removed from untreated mice. However,no treatment value by Mann Whitney U test.
follicular phase levels of estradiol were sufficient to
induce maximal PR expression in the epithelial cells
and the higher luteal phase levels of the steroid had
no further effect. In keeping with the menstrual cycle serum (27) or breast tissue (55) during the cycle are
sufficient to induce maximal PR expression in thedata, the proliferative activity of the breast epithelium
treated with follicular phase levels of estradiol was breast epithelial cells. In contrast, proliferation is onlysignificantly enhanced by much higher serum levelsnot significantly different from that of the control,
untreated tissue (Fig. 2B). But, as expected, treatment of estradiol.
How individual breast epithelial cells might bewith the higher, luteal phase estradiol levels signifi-
cantly increased the proliferative activity of the epithe- differentially sensitive to estradiol is, as yet, unclear.
However, there are data, generated in studies on breastlial cells in the breast tissue implants. These findingsindicated that PR expression was far more sensitive to cancer cells, suggesting that the sensitivity of the ER
may altered by interactions with other intracellularestrogen than proliferation explaining the discrepancy
between the data on PR expression during the men- signaling pathways. In particular, phosphorylation of
the ER by, for example, protein kinase A or mitogen-strual cycle and those obtained from the model of
normal human breast tissue implanted into athymic activated protein kinase has been shown to enhance
DNA binding and transcriptional activity (56). Further-nude mice. Even the lowest levels of estradiol seen in

Estrogen Responsiveness and Control of Normal Human Breast Proliferation 29
more, a plethora of steroid receptor co-activators and dent in very few cells suggesting the existence of two
co-repressors have been identified which appear to separate populations of luminal epithelial cells. Anregulate receptor function in a cell- and context-spe- alternative explanation was that PR synthesis had beencific manner (57). It is not difficult to envisage that down-regulated during the S-phase of the cell cyclechanges in the environment of the receptor by, for (the only phase detected by [3H]-dT labeling). Studiesexample, signaling from cell surface receptors or inter- on breast cancer cells have shown that PR proteinactions with co-factors could enhance or reduce the levels vary throughout the cell cycle and are maximalestrogen sensitivity of individual breast epithelial cells. only at the transition into G2 from the S-phase (59).
In order to confirm that PR expression and proliferation
were, indeed, taking place in separate epithelial cells,
we used fluorescent immunocytochemistry to detectTHE RELATIONSHIP BETWEENthe Ki67 proliferation-associated antigen and steroidPROLIFERATION AND STEROIDreceptor expression simultaneously. The Ki67 antigenRECEPTOR EXPRESSION IN LUMINALhas been reported as being present in cell nuclei at allEPITHELIAL CELLSstages of the cell cycle except G0 (60) and should be
co-localized with PR even if, as suggested previously,These findings raised the question of whetherthe receptor has been down-regulated during the S-PR expression and proliferation occurred in the samephase. Fluorescent dual labeling was carried out onepithelial cell which would have to have been sensitiveformalin-fixed sections of normal breast tissue afterto two different concentrations of estradiol or whethermicrowave antigen retrieval and showed that, as forthe two processes took place in separate cell popula-the previous studies, very few epithelial cells were co-tions each of which was sensitive to a different estrogenlabeled with the anti-PR and anti-Ki67 antibodies (Seelevel. An answer to this question was suggested byFig. 3B). Thus our original conclusion that PR expres-studies in which we used dual labeling techniques forsion and proliferation take place in separate epithelialthe simultaneous detection of steroid receptor expres-cell populations was corroborated.sion and proliferation in sections of human breast tis-
Since both the PR expressing and the proliferatingsue (58).luminal epithelial cells were sensitive to estrogen, weIn the first set of experiments we used sectionsassumed that both populations would contain ER.cut from Carnoy’ s fixed breast tissue samples obtainedAccordingly, we examined the co-incidence of ER andat different times of the menstrual cycle. The sectionsPR expression and of ER and Ki67 expression usingwere stained immunocytochemically to reveal the PR-the same methods and samples as detailed earlier. Aexpressing cells and then dipped in photographic emul-number of interesting points were raised by the datasion to determine [3H]-dT uptake. As shown in Fig.
3A, PR expression and [3H]-dT labeling were co-inci- obtained from these studies. The first was that a larger
Fig. 3. The proportion of PR expressing epithelial cells that are also labeled with (A)
[3H]-dT or (B) an antibody against the Ki67 proliferation associated protein. The results
are presented as the percentage of the total number of cells counted in 25 specimens
of normal human breast. At least 1000 cells were assessed per specimen; the total
number of cells counted is indicated in parentheses.

30 Anderson, Clarke, and Howell
one expressing ER and PR. In addition, the receptor-
expressing cells were distributed relatively evenly
throughout the luminal epithelium. Taken together,
these findings implied that steroid receptor expression
is dissociated from proliferation in the normal humanbreast. They raise some very interesting questions as
to how hormonal control of epithelial growth and func-
tion might be achieved.
A MODEL FOR THE ESTROGENICFig. 4. The proportion of PR expressing cells that were also labeled
CONTROL OF LUMINAL EPITHELIALwith an antibody against the ER. The results are presented as
CELL PROLIFERATIONpercentages of the total number of cells counted (indicated in paren-
theses) across 10 specimens of normal human breast tissue.
Our own data together with those of others sug-
gest a model for the estrogenic control of proliferation
within the human luminal epithelial compartment. Inproportion of luminal cells than expected expressed
the ER compared to our original studies on frozen this model (see Fig. 6), the ER-negative cells are in
close proximity to the ER-positive cells and are stimu-sections cut from samples of the breast tissue that had
been implanted into the athymic nude mice (shown lated to divide by juxtacrine and/or paracrine factorssecreted by the receptor-containing cells in responseearlier). We attributed this to the greater sensitivity of
the immunofluorescent method of detecting the ER to estrogen. The ER-negative cells may represent a
precursor or stem cell population which eventuallywhich included microwave-mediated antigen retrieval
in citrate buffer. Secondly, there was almost complete differentiates to become ER-positive and non-prolifer-
ative. Based on our observations that proliferating cellsco-incidence of ER and PR expression in that 96% of
the cells labeled with the anti-PR antibody also labeled are often immediately adjacent to those expressing thereceptor, we further speculate that the ER-positive cellswith the anti-ER antibody (see Fig. 4). Thirdly, co-
incidence of ER expression and proliferation as mea- might be arranged with their proliferative precursors
into discrete areas of the luminal epithelium or ` prolif-sured by [3H]-dT uptake or by detection of the Ki67
antigen was a very rare event (see Fig. 5). However, erative units’ similar to those described in the epider-
mis (61).almost every proliferating cell was found adjacent to
Fig. 5. The proportion of ER expressing epithelial cells that are also labeled with (A) [3H]-
dT or (B) an antibody against the Ki67 proliferation associated index. The results are
presented as the percentage of the total number of cells counted in (A) 10 specimens or
(B) 25 specimens of normal human breast. At least 1000 cells were assessed per specimen;
the total number of cells counted is indicated in parentheses.

Estrogen Responsiveness and Control of Normal Human Breast Proliferation 31
addition, we have shown that estradiol treatment
enhances expression of type 1 insulin-like growth fac-
tor receptor mRNA in normal human tissue implanted
into athymic nude mice (68). These preliminary studies
suggest the potential for paracrine regulation of prolif-eration of the normal human breast epithelium as sug-
gested in this hypothesis.
Recently Cunha and his colleagues (69) carried
out elegant studies in which mammary gland epithe-
lium isolated from ER knockout mice was implanted
into the mammary fat pads of wild type mice and viceversa. The results of these experiments suggest that,
in the mouse as well as in humans, estradiol stimulates
epithelial cell proliferation indirectly via the secretion
of paracrine growth factors. In the case of the mouse,Fig. 6. A model for indirect estrogenic control of normal human
the ` estrogen sensor’ cells appear to be in the stromalbreast epithelial cell proliferation. In this scheme, the cells capable
compartment as wild type epithelial cells could notof proliferation (the stem cell/early transit cell populations) are ER-respond to estrogen treatment when implanted into thenegative and the receptor is only expressed as the cells become more
differentiated. These differentiated cells control the proliferative fat pads of ER-knock out mice. However, in humans,activity of the stem and early transit cells via positive and negative ER expression in the stromal cells surrounding theparacrine signals depending on the prevailing estrogenic
epithelium has never been reported leading to the con-environment.
clusion that the ` estrogen sensing’ cells in our proposedmodel are situated in the epithelial compartment.
Studies on breast cancer cell lines carried out
some time ago provide indirect support for the above CONCLUSIONSmodel of estrogenic control of normal breast epithelial
cell proliferation. Firstly, conditioned media from ER- The studies reviewed in this article all point tothe normal human breast epithelium being an estrogenpositive breast cancer cell lines treated with estradiol
in culture was shown to stimulate the proliferation of target tissue. Unlike the endometrium, however, human
breast epithelial cells do not appear to be very sensitiveER-negative breast cancer cells both in culture and
when injected into athymic nude mice bearing ER- to estrogen. This would seem logical in that a cyclical
estrogenic response in the breast of the same magnitudenegative breast tumor xenografts (62). Furthermore ,
treatment of ER-positive breast cancer cell lines with and speed of that seen in the endometrium would behighly undesirable. An indirect mechanism of control-antiestrogens enhanced the synthesis and secretion of
peptide growth regulators (63). Transforming growth ling proliferation within the breast luminal epithelium
is one means by which estrogen sensitivity could befactors a and b together with insulin-like growth fac-
tor-I were implicated as the mediators of these para- attenuated. During pregnancy, when extensive epithe-
lial proliferation is required, not only are circulatingcrine effects. Secondly, some evidence has been
generated by studies on breast cancer cell lines that estradiol levels much higher than those of the men-strual cycle but there are large numbers of, as yet,ER-negative cells can give rise to ER-positive ones.
For example, small colonies of MCF-7 cells grown in unidentified factors that could enhance the estro-
genic response.soft agar were shown to be ER-negative when sec-
tioned and stained immunocytochemically with anti- For future studies on estradiol control of normal
breast growth and function, we should like to recapitu-ER antibodies whereas large colonies were ER-posi-tive (64). Fractionation of primary tumor cells on the late in culture the full repertoire of luminal epithelial
cell types that we see in vivo. We would not expectbasis of receptor content produced an ER-negative
fraction that gave rise to ER-positive cells in culture to isolate and culture ER-positive cells from normal
breast tissue de novo as the hypothesis presented earlier(65). Expression of growth factors and their cognate
receptors has been demonstrated in both normal human predicts that these cells represent a differentiated, non-
proliferative population. However, given the correctbreast tissue and cultured epithelial cells (66,67). In

32 Anderson, Clarke, and Howell
culture conditions, we may be able to induce differenti- small replacement doses of estrogens and androgens
to protect the cardiovascular and skeletal systems.ation of the ER-negative precursor cells and use them
as a model in which to study paracrine regulation of Finally, an early first full term pregnancy protects
against breast cancer (70) presumably because a signi-breast epithelial physiology. An alternative strategy
would be to implant isolated ER-negative epithelial ficant proportion of the breast luminal epithelium hasundergone terminal differentiation. A preventativecells embedded in extracellular matrix into athymic
nude mice. Some interesting data have been generated strategy suggested by Russo and colleagues (72) and
tested in rodents is the administration of a differentiat-recently by Kang et al. (45) who showed that splicing
of the ER mRNA to produce the wild type ER protein ing agent (in this case human chorionic gonadotrophin)
at the time when the mammary gland is most suscepti-occurred only when tumor epithelial cells were xeno-
grafted subcutaneously into athymic mice. This sug- ble to carcinogens; i.e., in early reproductive life. Thisstrategy has not been tested using human material orgests that three-dimensional structure and intercellular
interactions are also involved in governing estrogen subjects although the effects of human chorionic
gonadotrophin on proliferation and differentiationresponsiveness. Finally, relatively simple immunocy-
tochemical and/or in situ hybridization surveys of nor- could be tested relatively easily using human tissue
implanted into athymic nude mice.mal human breast tissue under well characterized
estrogenic conditions could still yield interesting data. In conclusion, recent studies on human breastepithelial cells in culture and xenografted into athymicIn addition to providing new insights into the
control of normal breast function, the findings and nude mice have generated new data on the estrogenic
control of proliferation. Future studies of this kindhypothesis presented earlier have important implica-
tions for breast cancer prevention and for predicting may yield new therapeutic targets for breast cancer
prevention or new methods of predicting individualbreast cancer risk. Firstly, we and others, have shownthat there is considerable variation in breast epithelial risk of breast cancer.
cell proliferative activity between individuals but we
do not know, as yet, whether high levels of proliferation
are associated with an increased risk of breast cancer.ACKNOWLEDGMENTS
Current theories on the carcinogenic process suggest
that this may well be the case and it is interesting thatThe authors thank Mr. Ian Laidlaw and Professorthe endocrine breast cancer risk factors such as early
C. Potten for their invaluable contributions to the stud-menarche, late menopause and late first full term preg-ies on normal human breast tissue implanted into nudenancy (70) all serve to increase the number of timesmice. We should also like to acknowledge the involve-the breast epithelium undergoes a cyclical increase inment of Mr. K. Spreckley, Mr. A. Rushton, Dr. S.proliferation. It is also not yet known whether muta-Roberts, Dr. A. Wakeling and Dr. J. Coyne. The studiestions in the BRCA 1 and 2 genes alter the estrogencarried out at the Christie Hospital were supported bysensitivity of the normal breast epithelium or whetherthe Endowment Fund of the Christie Hospital NHSthey exert their effects on breast cancer susceptibilityTrust, Zeneca Pharmaceuticals and the Cancerby some other mechanism. If it could be shown thatResearch Campaign.the estrogen sensitivity of the luminal epithelial cell
population is related to the likelihood of developing
breast cancer, then we can envisage individual riskprediction based on measurement of products of estra-
REFERENCESdiol action in samples obtained by relatively non-inva-
sive techniques such as nipple or fine needle aspiration.1. M. J. McManus and C. W. Welsch (1984). The effect of estro-
In terms of prevention, a reasonable strategy would be gen, progesterone, thyroxine and human placental lactogen onDNA synthesis of human breast ductal epithelium maintainedto prevent the luminal epithelial cells from undergoingin athymic nude mice. Cancer 54:1920±1927.cyclical in proliferation increases. This could be
2. H. Fanger and H. J. Ree (1974). Cyclic changes of humanachieved by using tamoxifen as in the current preven- mammary gland epithelium in relation to the menstrual
cycleÐ an ultrastructural study. Cancer 34:574±585.tion trials or, in the future, by using pure antiestrogens.3. P. M. Vogel, N. G. Georgiade, B. F. Fetter, S. Vogel, and K.An alternative strategy suggested by Pike and his col-
S. McCarty, Jr. (1981). The correlation of histologic changesleagues (71) is to inhibit ovarian steroid secretion using in the human breast with the menstrual cycle. Am. J. Pathol.
104:23±34.gonadotrophin releasing hormone agonists with very

Estrogen Responsiveness and Control of Normal Human Breast Proliferation 33
4. T. A. Longacre and S. A. Bartow (1986). A correlative morpho- increases proliferation and decreases oestrogen receptor contentof epithelial cells in the normal human breast. Int. J. Cancerlogic study of human breast and endometrium in the menstrual
cycle. Am. J. Surg. Pathol. 10:382±393. 48:206±210.22. D. Ricketts, L. Turnbull, G. Ryall, R. Bakhshi, N. S. Rawson,5. J. E. Ferguson, A. M. Schor, A. Howell, and M. W. J. Ferguson
(1990). Tenascin distribution in the normal human breast is J. C. Gazet, C. Nolan, and R. C. Coombes (1991). Estrogenand progesterone receptors in the normal female breast. Canceraltered during the menstrual cycle and in carcinoma. Differenti-
ation 42:199±207. Res. 51:1817±1822.23. G. Soderqvist, B. von Schoultz, E. Tani, and L. Skoog (1993).6. J. E. Ferguson, A. M. Schor, A. Howell, and M. W. J. Ferguson
(1992). Changes in the extracellular matrix of the normal human Estrogen and progesterone receptor content in breast epithelialcells from healthy women during the menstrual cycle. Am. J.breast during the menstrual cycle. Cell Tissue Res.
268:167±177. Obstet. Gynecol. 168:874±879.24. M. Boyd, R. H. Hildebrandt, and S. A. Bartow (1996). Expres-7. S. R. Wellings, H. M. Jensen, and R. G. Marcum (1975). An
atlas of subgross pathology of the human breast with special sion of the estrogen receptor gene in developing and adulthuman breast. Breast Cancer Res. Treat. 37:243±251.reference to possible precancerous lesions. J. Natl. Cancer
Inst. 55:231±273. 25. A. Gompel, A. Martin, P. Simon, D. Schoevaert, G. Plu-Bureau,D. Hugol, J. Audouin, E. Leygue, J. B. Truc, and Ph. Poitout8. J. Taylor-Papadimitr iou, M. Stampfer, J. Bartek, A. Lewis, M.
Boshell, E. B. Lane, and I. M. Leigh (1987). Keratin expression (1996). Epidermal growth factor receptor and c-erbB-2 expres-sion in normal breast tissue during the menstrual cycle. Breastin human mammary epithelial cells cultured from normal and
malignant tissue: relation to in vivo phenotypes and influence Cancer Res. Treat. 38:227±235.26. T. van Agthoven, M. Timmermans, J. A. Foekens, L. C. Dors-of medium. J. Cell Sci. 94:403±413.
9. J. Taylor-Papadimitr iou, R. Millis, J. Burchell, R. Nash, L. sers, and S. C. Henzen-Logman s (1994). Differential expressionof estrogen, progesterone and epidermal growth factor receptorsPang, and J. Gilbert (1986). Patterns of reaction of monoclonal
antibodies HMFG-1 and 2 with benign breast tissues and breast in normal, benign and malignant human breast tissues usingdual staining immunohistochem istry. Am. J. Pathol.carcinomas. J. Exp. Pathol. 2:247±260.
10. C. S. Potten, R. J. Watson, G. T. Williams, S. Tickle, S. A. 144:1238±1246.27. R. W. Rebar and S. S. C. Yen (1979). Endocrine rhythms inRoberts, M. Harris, and A. Howell (1988). The effect of age
and menstrual cycle upon proliferative activity of the normal gonadotrophins and ovarian steroids with reference to repro-ductive processes. In D. T. Krieger (ed.), Endocrine Rhythms,human breast. Brit. J. Cancer 58:163±170.
11. J. R. W. Masters, J. O. Drife, and J. J. Scarisbrook (1977). Raven Press, New York, p. 259.28. B. A. Lessey, A. P. Killam, D. A. Metzger, A. F. Haney, G. L.Cyclic variation of DNA synthesis in human breast epithelium.
J. Natl. Cancer Inst. 58:1263±1265. Greene, and K. S. McCarty, Jr. (1988). Immunohistochem icalanalysis of human uterine estrogen and progesterone receptors12. J. S. Meyer (1977). Cell proliferation in normal human breast
ducts, fibroadenomas and other ductal hyperplasia measured by throughout the menstrual cycle. J. Clin. Endocrinol. Meta-bol. 67:334±340.nuclear labeling with tritiated thymidine. Effects of menstrual
phase, age, and oral contraceptive hormones. Hum. Pathol. 29. C. L. Clarke, J. Titley, S. Davies, and M. J. O’ Hare (1994). Animmunomagnetic separation using superparamagneti c (MACS)8:67±81.
13. T. J. Anderson, D. J. P. Ferguson, and G. M. Raab (1982). Cell beads for large scale purification of human mammary luminaland myoepithelial cells. Epith. Cell. Biol. 3:38±46.turnover in the ª restingº human breast: influence of parity,
contraceptive pill, age and laterality. Brit. J. Cancer 30. R. J. Pauley, H. D. Soule, L. Tait, F. R. Miller, S. R. Wolman,P. J. Dawson, and G. H. Heppner (1993). The MCF10 family46:376±382.
14. J. J. Going, T. J. Anderson, S. Battersby, and C. C. A. MacIntyre of spontaneously immortalised human breast epithelial celllines: models of neoplastic progression. Eur. J. Cancer Prev.(1988). Proliferative and secretory activity in human breast
tissue during natural and artificial menstrual cycles. Am. J. 2 (suppl 3):67±76.31. P. S. Rudland, G. E. Ollerhead, and A. M. Platt-Higgins (1991).Pathol. 130:193±204.
15. H. Olssen, H. Jernstrom, P. Alm, H. Kreipe, C. Ingvar, P. Morphogenetic behavior of simian virus 40 transformed humanmammary epithelial stem cell lines on collagen gels. In VitroE. Jonssen, and S. Ryden (1996). Proliferation of the breast
epithelium in relation to menstrual cycle phase, hormonal use Cell Dev. Biol. 27A:103±112.32. C. Y. Kao, C. S. Oakley, C. W. Welsch, and C. C. Changand reproductive factors. Breast Cancer Res. Treat.
40:187±196. (1997). Growth requirements and neoplastic transformation oftwo types of normal human breast epithelial cells derived from16. G. Soderqvist, E. Isaksson, B. von Schoultz, K. Carlstrom, E.
Tani, and L. Skoog (1997). Proliferation of breast epithelial reduction mammoplasty. In Vitro Cell Dev. Biol. 33:282±288.33. J. Bartek, J. Bartkova, N. Kyprianou, E. N. Lalani, Z. Staskova,cells in healthy women during the menstrual cycle. Am. J.
Obstet. Gynecol. 176:123±128. M. Shearer, S. Chang, and J. Taylor-Papadimitr iou (1991).Efficient immortalization of luminal epithelial cells from17. W. D. Dupont, D. L. Page, F. F. Parl, C. L. Vnencak-Jones,
W. D. Plummer, Jr., M. S. Rados, and P. A. Schuyler (1994). human mammary gland by introduction of SV40 large tumorantigen with a recombinant retrovirus. Proc. Natl. Acad. Sci.Long term risk of breast cancer in women with fibroadenoma.
N. Engl. J. Med. 331:10±15. USA 88:3520±3524.34. V. Band, D. Zajchowski, V. Kulesa, and R. Sager (1990).18. J. C. Sabourin, A. Martin, J. Baruch, J. B. Truc, A. Gompel,
and P. Poitout (1994). bcl-2 expression in normal human breast Human papilloma virus DNAs immortalise normal humanmammary epithelial cells and reduce their growth factortissue during the menstrual cycle. Int. J. Cancer 59:1±6.
19. A. Ferenczy, G. Bertrand, and M. M. Gelfand (1979). Prolifera- requirements. Proc. Natl. Acad. Sci. USA 87:463±467.35. L. S. Gollahon and J. W. Shay (1996). Immortalization oftion kinetics of human endometrium during the normal men-
strual cycle. Am. J. Obstet. Gynecol. 133:859±867. human mammary epithelial cells transfected with mutant p53(273his). Oncogene 12:715±725.20. J. C. Felix and S. Farahmand (1997). Endometrial glandular
proliferation and estrogen receptor content during the normal 36. C. A. Smith, H. J. Bunnage, P. Monaghan, and A. M. Neville(1987). Human breast epithelium in vitro: the re-expression ofmenstrual cycle. Contraception 55:19±22.
21. G. Williams, E. Anderson, A. Howell, R. Watson, J. Coyne, structural and functional cellular differentiation in long termculture. Cell Tissue Res. 246:433±440.S. A. Roberts, and C. Potten (1991). Oral contraceptive use

34 Anderson, Clarke, and Howell
37. F. Berdichevsky, D. Alford, B. D’ Souza, and J. Taylor-Papadi- 52. N. K. Popnikolov, J. Yang, R. C. Guzman, and S. Nandi (1995).Reconstituted human normal breast in nude mice using collagenmitriou (1994). Branching morphogenesis of human mammarygel or Matrigel. Cell Biol. Int. 19:539±546.epithelial cells in collagen gels. J. Cell Sci. 107:3557±3568.
53. I. J. Laidlaw, R. B. Clarke, A. Howell, A. W. M. C. Owen, C.38. O. W. Petersen, L. Ronnov-Jessen, A. R. Howlett, and M. J.S. Potten, and E. Anderson (1995). Proliferation of normalBissell (1992). Interaction with basement membrane serves tohuman breast tissue implanted in athymic nude mice is stimu-rapidly distinguish growth and differentiation pattern of normallated by estrogen and not progesterone. Endocrinologyand malignant human breast epithelial cells. Proc. Natl. Acad.136:164±171.Sci. USA 89:9064±9068.
54. R. B. Clarke, A. Howell, and E. Anderson (1997). Estrogen39. J. J. Gomm, R. C. Coope, P. J. Browne, and R. C. Coombessensitivity of normal human breast tissue in vivo and implanted(1997). Separated human breast epithelial and myoepithelialinto athymic nude mice: analysis of the relationship betweencells have different growth factor requirements in vitro but canestrogen-induced proliferation and progesterone receptorreconstitute normal breast lobuloalveolar structures. J. Cell.expression. Breast Cancer Res. Treat. 45:121±133.Physiol. 171:11±19.
55. J. H. H. Thijssen, M. A. Blankenstein, J. Daroszewski, and40. N. P. Perusinghe, P. Monaghan, M. J. O’ Hare, S. Ashley, andA. Milewicz (1990). Steroids in normal and neoplastic breastB. A. Gusterson (1992). Effects of growth factors on prolifera-tissues. Ann. N.Y. Acad. Sci. 595:222±226.tion of basal and luminal epithelial cells in human breast epithe-
56. N. L. Weigel (1996). Steroid hormone receptors and their regu-lial explants in serum-free culture. In Vitro Cell Dev. Biol.lation by phosphorylation. Biochem. J. 319:657±667.28A:90±96.
57. K. B. Horwitz, T. A. Jackson, D. L. Rain, J. K. Richer, G. S.41. B. M. Gabelman and J. T. Emerman (1992). Effects of estrogen,Takimoto, and L. Tung (1996). Nuclear receptor coactivatorsepidermal growth factor and transforming growth factor a onand corepressors. Mol. Endocrinol. 10:1167±1177.the growth of human breast epithelial cells in primary culture.
58. E. Anderson, R. B. Clarke, and A. Howell (1997). ChangesExp. Cell Res. 201:113±118.in the normal human breast throughout the menstrual cycle:42. R. Sakthivel, M. Hamdan, J. Yang, R. C. Guzman, and S. Nandirelevance to carcinogenesis. Endocrine-Rela ted Cancer,(1993). Effect of TGF a on growth of normal human breast4:23±33.epithelial cells in serum-free primary culture using 3-dimen-
59. P. Rostagno, C. Caldani, and B. Lahlou (1996). Cell cyclesional collagen gels. Cell Biol. Int. 17:387±397.expression of steroid receptors determined by image analysis43. Q. Y. Liu, B. Niranjan, P. Gomes, J. J. Gomm, D. Davies, R.on human breast cancer cell line: A hypothesis on the effectsC. Coombes, and L. Bulawela (1996). Inhibitory effects ofof antiestrogens. Breast Cancer Res. Treat 37:77±87.activin on the growth and morphogenesis of primary and trans-
60. J. Gerdes, H. Lemke, H. Baisch, H. H. Wacker, U. Schwab,formed mammary epithelial cells. Cancer Res. 56:1155±1163.and H. Stein (1984). Cell cycle analysis of a cell proliferation-44. C. Malet, A. Gompel, H. Yaneva, H. Cren, N. Fidji, I Mowszow-associated human nuclear antigen defined by the monoclonalicz, F. Kuttenn, and P. Mauvais-Jarvis (1991). Estradiol andantibody Ki-67. J. Immunol. 133:1710±1715.progesterone receptors in cultured normal human breast epithe-
61. C. S. Potten and R. J. Morris (1988). Epithelial stem cells inlial cells and fibroblasts: immunocytochem ical studies. J. Clin.vivo. J. Cell Sci. Suppl. 10:45±62.Endocrinol. Metabol. 73:8±17.
62. R. Clarke, R. B. Dickson, and M. E. Lippman (1992). Hormonal45. K-S. Kang, I. Morita, A. Cruz, Y. J. Jeon, J. E. Trosko, and C-aspects of breast cancer. Growth factors, drugs and stromalC. Chang (1997). Expression of estrogen receptors in a normalinteractions. Crit. Rev. Oncol. Hematol. 12:1±23.human breast epithelial cell type with luminal and stem cell
63. C. Knabbe, M. E. Lippman, L. M. Wakefield, K. C. Flanders,characteristics and its neoplastically transformed cell lines.
A. Kasid, R. Derynck, and R. B. Dickson (1987). EvidenceCarcinogenesis 18:251±257.that transforming growth factor b is a hormonally regulated
46. D. A. Zajchowski, R. Sager, and L. Webster (1993). Estrogennegative growth factor in human breast cancer cells. Cell
inhibits the growth of estrogen receptor-negative , but not estro-48:417±428.
gen receptor-postive, human mammary epithelial cells express-64. F. Kodama, G. L. Green, and S. E. Salmon (1985). Relation of
ing a recombinant estrogen receptor. Cancer Res.estrogen receptor expression to clonal growth and antiestrogen
53:5004±5011.effects on human breast cancer cells. Cancer Res.
47. B. K. Lundholt, M. W. Madsen, A. E. Lykkesfeldt, O. W.45:2720±2724.
Petersen, and P. Briand (1996). Characterisation of a nontumor-65. O. L. Podhajcer, A. I. Bravo, I. Sorin, N. Guman, R. Cerdeiro,
igenic human breast epithelial cell line stably transfected withand J. Mordoh (1986). Determination of DNA synthesis,
the human estrogen receptor (ER) cDNA. Mol. Cell. Endocri- estrogen receptors, and carcinoembryonic antigen in isolatednol. 119:47±59. cellular subpopulations of human breast cancer. Cancer
48. M. J. Pilat, J. K. Christman, and S. C. Brooks (1996). Character- 58:720±729.ization of the estrogen receptor transfected MCF10A breast 66. S. E. Bates, E. M. Valverius, B. W. Ennis, D. A. Bronzert, J.cell line 139B6. Breast Cancer Res. Treat. 37:253±266. P. Sheridan, M. R. Stampfer, J. Mendelsohn, M. E. Lippman,
49. B. A. Gusterson, J. Williams, H. Bunnage, M. J. O’ Hare, and and R. B. Dickson (1990). Expression of the transformingJ. D. Dubois (1984). Human breast epithelium transplanted growth factor a /epidermal growth factor receptor pathway ininto nude mice. Proliferation and milk protein production in normal human breast epithelial cells, Endocrinologyresponse to pregnancy. Virchows Arch. A Pathol. Anat. Histopa- 126:596±607.thol. 404:325±333. 67. P. Monaghan, C. L. Clarke, N. P. Perusinghe, M. G. Ormerod,
50. L. G. Sheffield and C. W. Welsch (1988). Transplantation of and M. J. O’ Hare (1995). Epidermal growth factor receptorhuman breast epithelia to mammary-gland- free fat pads of expression on human breast luminal and basal cells in vitro.athymic nude mice: influence of mammotrophic hormones on Epithelial Cell Biol. 4:52±62.growth of breast epithelia. Int. J. Cancer 41:713±719. 68. R. B. Clarke, A. Howell, and E. Anderson (1997). Type I
51. J. D. Dubois, M. J. O’ Hare, P. Monaghan, J. Bartek, R. Norris, insulin-like growth factor receptor gene expression in normaland B. A. Gusterson (1987). Human breast epithelial xeno- human breast tissue treated with oestrogen and progesterone.grafts: an immunocytochem ical and ultrastructural study of Brit. J. Cancer 75:251±257.differentiation and lactogenic response. Differentiation 69. G. R. Cunha, P. Young, Y. K. Hom, P. S. Cooke, J. A. Taylor,
and D. B. Lubahn (1997). Elucidation of a role for stromal35:72±82.

Estrogen Responsiveness and Control of Normal Human Breast Proliferation 35
steroid hormone receptors in mammary gland growth and 71. M. C. Pike, J. R. Daniels, and D. V. Spicer (1997). A hormonalcontraceptive approach to reducing breast and ovarian cancerdevelopment using tissue recombination experiments. J. Mam.
Gland Biol. Neoplasia. 2:393±402. risk: an update. Endocrine-Rela ted Cancer 4:125±133.72. J. Russo and I. H. Russo (1997). Role of differentiation in70. T. J. A. Key and M. C. Pike (1988). The role of oestrogens
and progestagens in the epidemiology and prevention of breast the pathogenesis and prevention of breast cancer. Endocrine-Related Cancer 4:7±21.cancer. Eur. J. Cancer Clin. Oncol. 24:29±43.








![Study of Estrogen Receptor, Progesterone Receptor, …...[CANCER RESEARCH 49,4298-4304, August 1. 1989] Study of Estrogen Receptor, Progesterone Receptor, and the Estrogen-regulated](https://img.pdfslide.us/doc/110x75/5f95792bbdbd5e0915333803/study-of-estrogen-receptor-progesterone-receptor-cancer-research-494298-4304.jpg)