Embed Size (px)
Citation preview
Estimating the Costs and Benefits of NewDrug Therapies: Atypical Antipsychotic
Drugs for Schizophreniafry Josephine Mauskopf, Matthew Muroff, P. Joseph Qibson,
and David L. Qrainger
Abstract
This article presents an analytic tool populated withdata from published studies to illustrate the likelyimpacts of a switch from typical to atypical antipsychoticdrugs over a 3-year period on individual, family, andsocietal outcomes for a US. schizophrenia population.Data taken from clinical trials and observational datastudies are used. Changes in annual health care costs,schizophrenia symptom days, extrapyramidal symptom(EPS) days, suicide rates, and employment days are esti-mated. For each 1,000 people treated with typical drugs,the base case scenario gives estimates of annual medicalcare costs of $28.9 million with 80,253 moderate/severeschizophrenia symptom days and 92,006 EPS days. Inthe base case scenario, after switching to atypical drugs,schizophrenia symptom days are estimated to decreaseup to 33 percent, EPS days up to 50 percent, and totalmedical care costs up to 19 percent over the 3-yearperiod. Suicide rates fall and employment rates increase.The direction of the impacts remain the same for a widerange of input parameter values used in sensitivityanalyses. Thus, switching to atypical drugs will likelyreduce total medical care costs and decrease other dis-ease burdens for people with schizophrenia, their fami-lies, and society.
Keywords: Costs, benefits, population, antipsy-chotic, schizophrenia, atypical drugs, typical drugs.
Schizophrenia Bulletin, 28<4):619-635,2002.
Schizophrenia is a chronic mental illness often associatedwith repeated and prolonged admissions to the hospital. Inaddition, people with schizophrenia experience a signifi-cant economic and quality of life impact, as do their fami-lies and society at large (Rupp and Keith 1993). The highuse of the hospital is a key factor in the high costs of med-ical care for schizophrenia, which account for a significantshare of the cost of mental health care in the United States(Addington et al. 1993; Narrow et al. 1993; Rupp and
Keith 1993). Treatments that can reduce hospital admis-sions or the average length of stay in the hospital can resultin significant cost savings. The second generation ofantipsychotic drugs for treating schizophrenia—atypicaldrugs such as clozapine, risperidone, olanzapine, and que-tiapine—effectively treat both positive and negative symp-toms of the disease (Jibson and Tandon 1998), and two,clozapine and olanzapine, have been shown to be effectivein patients who are not responsive to or who are intolerantof the first generation, typical antipsychotic drugs such ashaloperidol, chlorpromazine, or thioridazine (Tollefson etal. 2001). But atypical drugs are considerably more expen-sive than typical drugs. Thus, it is important that decisionmakers have information to help them determine whetherthe safety and efficacy benefits are likely to result ingreater value in terms of health care cost savings, andother population and societal benefits.
The standard method for estimating the populationimpacts of specific diseases is to use large observationaldata bases. Several studies using these data bases to exam-ine the annual costs associated with schizophrenia havebeen published (Wyatt et al. 1995; Dickey et al. 1996; Riceand Miller 1996). These studies present the total annualU.S. medical care costs for people with schizophreniabefore the widespread introduction of atypical drugs. Suchinformation is now becoming available for people treatedwith atypical drugs (Davies et al. 1998). However, suchstudies give information on only costs—not individualhealth and family outcomes. In addition, in observationalstudies, people receiving the newer treatment might besystematically different from those receiving the oldertreatment. Also, such information is often not available atthe time that medical policy makers have to decidewhether to restrict access to the new treatment.
The advantage of developing a model-based approachto estimating the population impacts of a new treatment is
Send reprint requests to Dr. J. Mauskopf, RTI Health Solutions, 3040Cornwallis Road, Research Triangle Park, NC 27709; e-mail:[email protected].
619
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Schizophrenia Bulletin, Vol. 28, No. 4, 2002 J. Mauskopf et al.
that the comparison of treatment with the older drugs totreatment with the newer drugs can be made for differentdisease severity groups and for geographic areas with dif-ferent treatment practice patterns or different unit costs.The model-based approach also allows for estimation ofthe impacts of the new treatment on individual and familyoutcomes not generally included in the observational databases used in the studies cited above. Finally, with themodel-based approach described in this article, prelimi-nary estimates of the population impacts can be obtainedbefore there is widespread use of the new treatment, andthese estimates can be easily updated as more informationbecomes available.
A model has previously been described that estimatesthe burden of schizophrenia when treated with typicaldrugs (Mauskopf et al. 1999). In this article, we extendthis model to estimate the impact of switching from treat-ment with typical drugs to treatment with atypical drugson the annual costs and individual and societal conse-quences in the U.S. schizophrenia population. The analy-sis takes a societal perspective because it includes esti-mates of a broad range of outcomes, including individualsymptoms, medical care costs, employment rates, andsocial service costs.
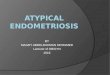
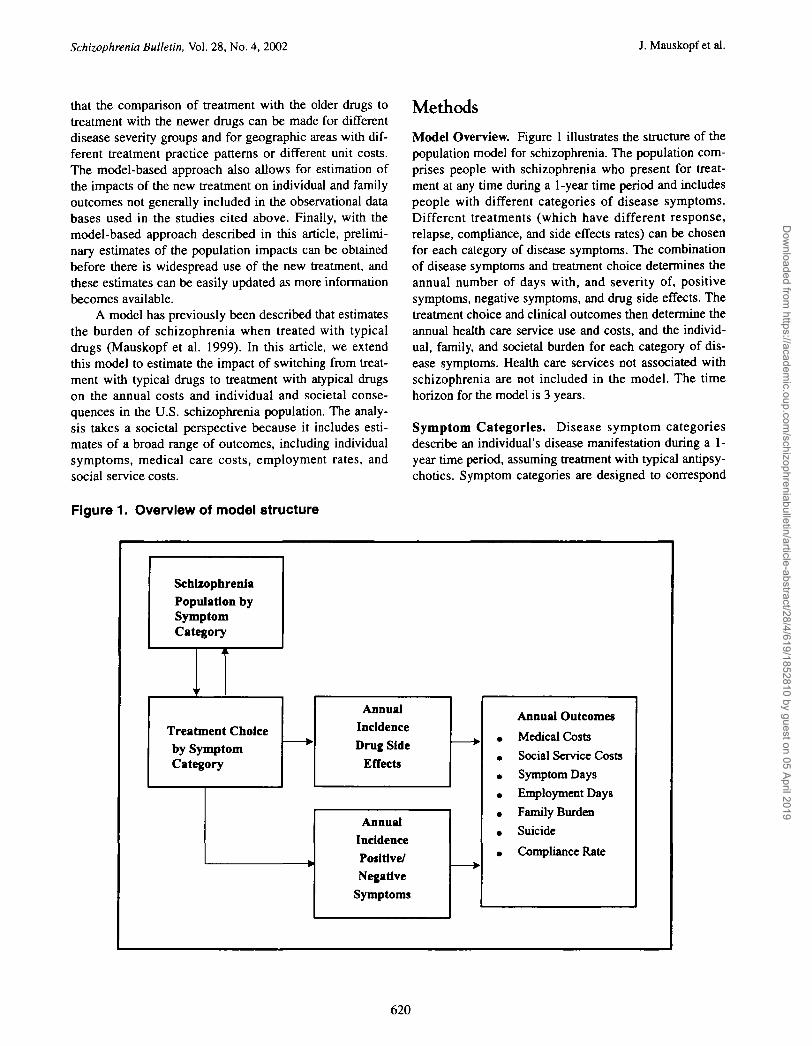
Figure 1. Overview of model structure
Methods
Model Overview. Figure 1 illustrates the structure of thepopulation model for schizophrenia. The population com-prises people with schizophrenia who present for treat-ment at any time during a 1-year time period and includespeople with different categories of disease symptoms.Different treatments (which have different response,relapse, compliance, and side effects rates) can be chosenfor each category of disease symptoms. The combinationof disease symptoms and treatment choice determines theannual number of days with, and severity of, positivesymptoms, negative symptoms, and drug side effects. Thetreatment choice and clinical outcomes then determine theannual health care service use and costs, and the individ-ual, family, and societal burden for each category of dis-ease symptoms. Health care services not associated withschizophrenia are not included in the model. The timehorizon for the model is 3 years.
Symptom Categories. Disease symptom categoriesdescribe an individual's disease manifestation during a 1-year time period, assuming treatment with typical antipsy-chotics. Symptom categories are designed to correspond
SchizophreniaPopulation bySymptomCategory
r
k
Treatment Choiceby SymptomCategory
AnnualIncidence
Drug SideEffects
AnnualIncidencePositive/Negative
Symptoms
•
Annual Outcomes
• Medical Costs
• Social Service Costs
• Symptom Days
• Employment Days
• Family Burden
• Suicide
• Compliance Rate
620
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Costs and Benefits of New Drug Therapies Schizophrenia Bulletin, Vol. 28, No. 4, 2002
to different degrees of individual disability and medicalcare use, to be understandable to decision makers, and tomatch data availability. Except for the "newly diagnosed"category, they differentiate among people with schizo-phrenia according to the amount of hospitalization experi-enced during the year. The five disease symptom cate-gories are:
1. newly diagnosed during the year (newly diagnosed);2. no acute or chronic psychotic episodes requiring hos-
pitalization during the year (no episode);3. one or more acute psychotic episodes during the year
requiring short-term hospitalization, residential care,or both—these are people who are generally respon-sive to and tolerant of typical drugs and include"revolving door" patients (acute episode);
4. extended psychotic episodes during the year requiringprolonged hospitalization, residential care, or both butwith some outpatient care during the year—these arepeople who are probably refractory to or intolerant oftypical drugs (extended episode); and
5. institutionalized for the complete year—these arepeople who are probably refractory to or intolerant oftypical drugs (institutionalized).
For any 1-year time period, an individual can be classifiedin only one of these categories. While individuals maychange category from year to year or even die, we take aprevalence-based perspective and assume that the numberand proportion of schizophrenia patients in each categorystay constant each year.
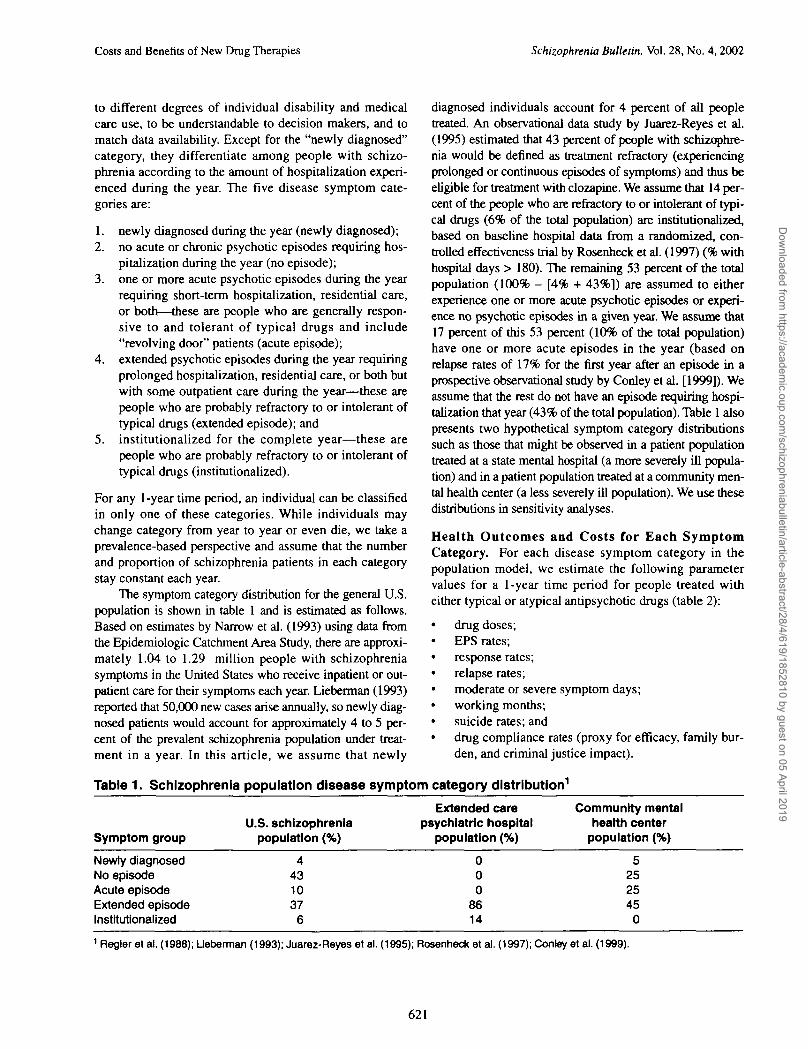
The symptom category distribution for the general U.S.population is shown in table 1 and is estimated as follows.Based on estimates by Narrow et al. (1993) using data fromthe Epidemiologic Catchment Area Study, there are approxi-mately 1.04 to 1.29 million people with schizophreniasymptoms in the United States who receive inpatient or out-patient care for their symptoms each year. Lieberman (1993)reported that 50,000 new cases arise annually, so newly diag-nosed patients would account for approximately 4 to 5 per-cent of the prevalent schizophrenia population under treat-ment in a year. In this article, we assume that newly
diagnosed individuals account for 4 percent of all peopletreated. An observational data study by Juarez-Reyes et al.(1995) estimated that 43 percent of people with schizophre-nia would be denned as treatment refractory (experiencingprolonged or continuous episodes of symptoms) and thus beeligible for treatment with clozapine. We assume that 14 per-cent of the people who are refractory to or intolerant of typi-cal drugs (6% of the total population) are institutionalized,based on baseline hospital data from a randomized, con-trolled effectiveness trial by Rosenheck et al. (1997) (% withhospital days > 180). The remaining 53 percent of the totalpopulation (100% - [4% + 43%]) are assumed to eitherexperience one or more acute psychotic episodes or experi-ence no psychotic episodes in a given year. We assume that17 percent of this 53 percent (10% of the total population)have one or more acute episodes in the year (based onrelapse rates of 17% for the first year after an episode in aprospective observational study by Conley et al. [1999]). Weassume that the rest do not have an episode requiring hospi-talization that year (43% of the total population). Table 1 alsopresents two hypothetical symptom category distributionssuch as those that might be observed in a patient populationtreated at a state mental hospital (a more severely ill popula-tion) and in a patient population treated at a community men-tal health center (a less severely ill population). We use thesedistributions in sensitivity analyses.
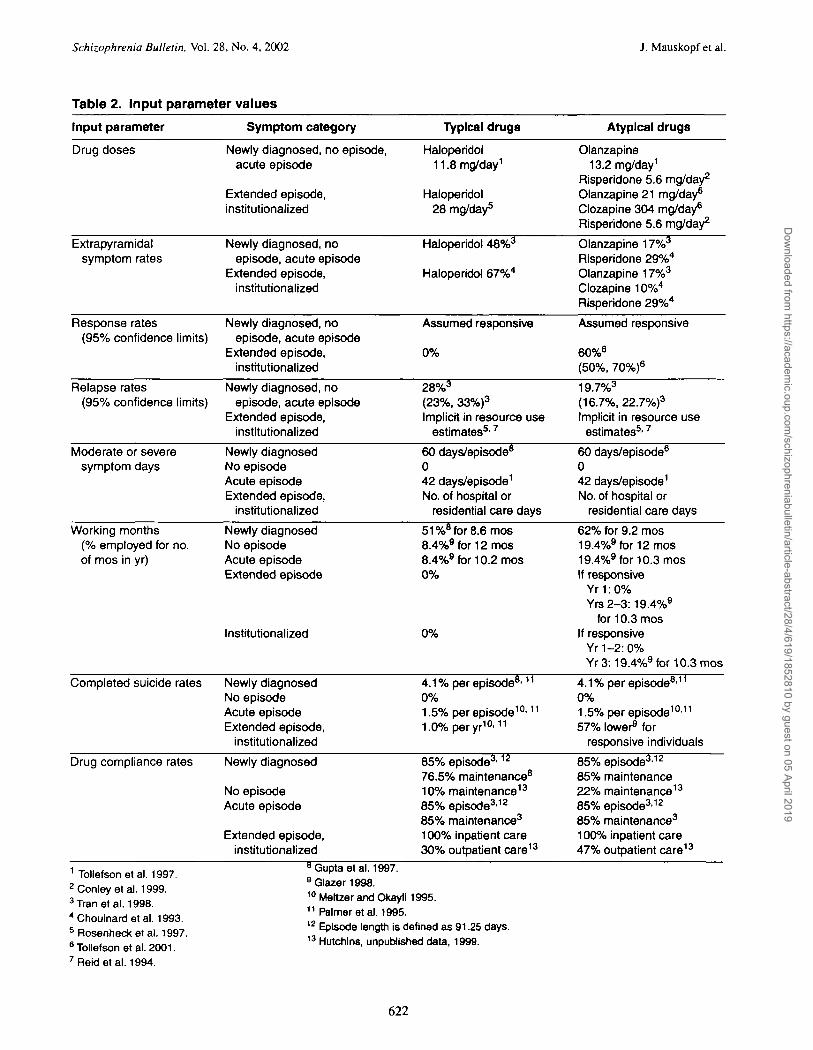
Health Outcomes and Costs for Each SymptomCategory. For each disease symptom category in thepopulation model, we estimate the following parametervalues for a 1-year time period for people treated witheither typical or atypical antipsychotic drugs (table 2):
• drug doses;• EPS rates;• response rates;• relapse rates;• moderate or severe symptom days;• working months;• suicide rates; and• drug compliance rates (proxy for efficacy, family bur-
den, and criminal justice impact).
Table 1. Schizophrenia population disease symptom category distribution1
Symptom group
Newly diagnosedNo episodeAcute episodeExtended episodeInstitutionalized
U.S. schizophreniapopulation (%)
4431037
6
Extended carepsychiatric hospital
population (%)
000
8614
Community mentalhealth center
population (%)
5252545
0
1 Regier el al. (1988); Ueberman (1993); Juarez-Reyes et al. (1995); Rosenheck et al. (1997); Conley et al. (1999).
621
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Schizophrenia Bulletin, Vol. 28, No. 4, 2002 J. Mauskopf et al.
Table 2. Input parameter values
Input parameter
Drug doses
Extrapyramidalsymptom rates
Response rates(95% confidence limits)
Relapse rates(95% confidence limits)
Moderate or severesymptom days
Working months(% employed for no.of mos in yr)
Completed suicide rates
Drug compliance rates
Symptom category
Newly diagnosed, no episode,acute episode
Extended episode,institutionalized
Newly diagnosed, noepisode, acute episode
Extended episode,institutionalized
Newly diagnosed, noepisode, acute episode
Extended episode,institutionalized
Newly diagnosed, noepisode, acute episode
Extended episode,institutionalized
Newly diagnosedNo episodeAcute episodeExtended episode,
institutionalized
Newly diagnosedNo episodeAcute episodeExtended episode
Institutionalized
Newly diagnosedNo episodeAcute episodeExtended episode,
institutionalized
Newly diagnosed
No episodeAcute episode
Extended episode,institutionalized
Typical drugs
Haloperidol11.8 mg/day1
Haloperidol28 mg/day5
Haloperidol 48%3
Haloperidol 67%4
Assumed responsive
0%
28%3
(23%, 33%)3
Implicit in resource useestimates5'7
60 days/episode8
042 days/episode1
No. of hospital orresidential care days
51 %8 for 8.6 mos8.4%9for12mos8.4%9 for 10.2 mos0%
0%
4.1% per episode8'11
0%1.5% per episode10'11
1.0% per yr10'11
85% episode3'12
76.5% maintenance8
10% maintenance13
85% episode3'12
85% maintenance3
100% inpatient care30% outpatient care13
Atypical drugs
Olanzapine13.2 mg/day1
Risperidone 5.6 mg/day2
Olanzapine 21 mg/day6
Clozapine 304 mg/day6
Risperidone 5.6 mg/day2
Olanzapine 17%3
Risperidone 29%4
Olanzapine 17%3
Clozapine 10%4
Risperidone 29%4
Assumed responsive
60%6
(50%, 70%)6
19.7%3
(16.7%, 22.7%)3
Implicit in resource useestimates5'7
60 days/episode6
042 days/episode1
No. of hospital orresidential care days
62% for 9.2 mos19.4%9for12mos19.4%9 for 10.3 mosIf responsive
Yr 1:0%Yrs2-3:19.4%9
for 10.3 mosIf responsive
Yr 1-2:0%Yr3:19.4%9for10.3mos
4.1% per episode811
0%1.5% per episode10'11
57% lower9 forresponsive individuals
85% episode3'12
85% maintenance22% maintenance13
85% episode3'12
85% maintenance3
100% inpatient care47% outpatient care13
1 Tollefson et al. 1997.2 Conley et al. 1999.3Tran et al. 1998.4 Chouinard et al. 1993.5 Rosenheck et al. 1997.6 Tollefson et al. 2001.7 Reideta l . 1994.
Gupta etal. 1997.9Qlazer1998.10 Meltzer and Okayli 1995.11 Palmer etal. 1995.12 Episode length is defined as 91.25 days.13 Hutchins, unpublished data, 1999.
622
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019

Costs and Benefits of New Drug Therapies Schizophrenia Bulletin, Vol. 28, No. 4, 2002
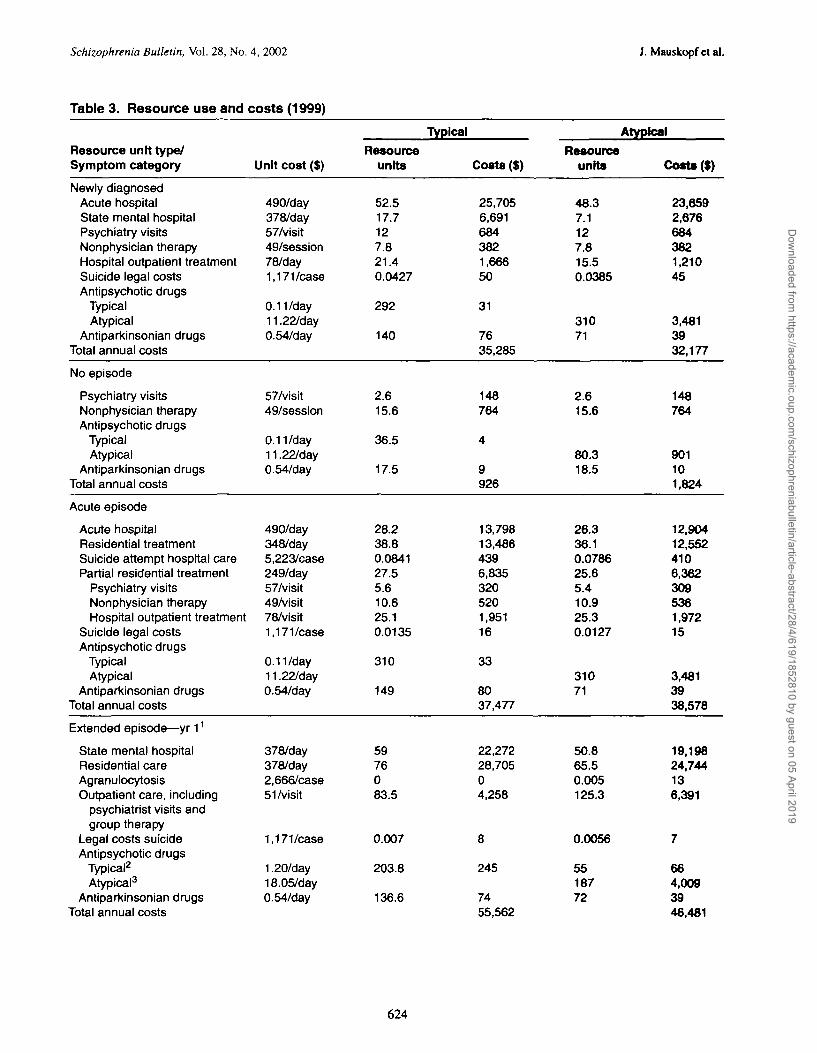
In the model, treatment efficacy, symptom days, sui-cide rates, employment rates, and drug compliance areassumed to differ according to whether the population istreated with typical or atypical drugs but not according towhich atypical drug is used. Among the different atypicaldrugs, only the dose, daily cost, and EPS rates areassumed to differ. Medical care use and costs, includinginpatient and outpatient services and drugs, are also esti-mated for each disease symptom category (table 3). Themedical care use rates (other than drugs) vary dependingon whether typical or atypical drugs are used but are thesame for all atypical drugs. Costs per unit of medical care(except for drugs), such as the cost per acute hospital day,are held constant across treatments and disease symptomcategories. A listing of the key data sources used and asummary of their characteristics (type of study, number ofpatients, location of study) and the parameters taken fromeach study are presented in an appendix. The derivation ofeach parameter value is described below and the valuesare shown in tables 2 and 3.
Drug doses. We assume that all people treated withtypical drugs receive a dose of 11.8 mg/day of oralhaloperidol (Tollefson et al. 1997) for the acute episode,no episode, and newly diagnosed symptom categories,and a dose of 28 mg/day oral haloperidol (Rosenheck etal. 1997) or 150 mg/month of depot haloperidoldecanoate (Glazer and Ereshefsky 1996) for the extendedcare and institutionalized symptom categories. For peopletreated with atypical drugs, we assume the followingtreatment patterns. For the acute episode, no episode, andnewly diagnosed symptom categories we assume that, inany given year, 50 percent of patients are taking olanza-pine (13.2 mg/day, Tollefson et al. 1997) and 50 percentare taking risperidone (5.6 mg/day, Conley et al. 1999).For extended episode and institutionalized individuals, weassume that 33 percent are taking clozapine (304 mg/day,Tollefson et al. 2001), 33 percent are taking risperidone(5.6 mg/day, Conley et al. 1999), and 33 percent are tak-ing olanzapine (21 mg/day, Tollefson et al. 2001).
EPS rates. EPS rates, which are based on reportsfrom clinical trials, represent the percentage of individu-als needing to take antiparkinsonian drugs or other drugsto treat the EPS while they are taking antipsychotic drugs.The rates are 48 percent for haloperidol (Tran et al. 1998),17 percent for olanzapine (Tran et al. 1998), and 29 per-cent for risperidone (Chouinard et al. 1993) for the acuteepisode(s), no episode, and newly diagnosed symptomcategories. The rates are 67 percent for haloperidol(Chouinard et al. 1993), 10 percent for clozapine (Beasleyet al. 1998), 29 percent for risperidone (Chouinard et al.1993), and 17 percent for olanzapine (Tran et al. 1998)for the extended episode and institutionalized symptomcategories. The cost per day with EPS of $0.54 was taken
from an estimate in a modeling study by Glazer andEreshefsky (1996) that included both monitoring and benz-tropine costs.
Response and relapse rates. Response and relapserates were taken from clinical trials and observationaldata. In our model, we assume that people in the acuteepisode(s) symptom category are equally responsive totypical and atypical drugs. There is no difference in thisefficacy measure. However, the relapse rates for people inthe acute episode(s) symptom category differ by drugtype. We assume a 1-year relapse rate of 28 percent fortypical drugs and of 19.7 percent for atypical drugs (areduction of 30% compared with the typical drugs) basedon a meta-analysis of relapse rates for responsive patientsfrom three olanzapine versus haloperidol randomized,controlled clinical trials (Tran et al. 1998). Response ratesfor the extended episode and institutionalized symptomcategories are assumed to be 60 percent for the atypicaldrugs, based on a randomized, controlled clinical trialcomparing clozapine and olanzapine (Tollefson et al.2001). Similar response rates have been observed for theatypical drugs in other clinical trials (Kane et al. 1988;Owen et al. 1989; Kleiser et al. 1995). The relapse andresponse rates for the newly diagnosed symptom categoryfor the typical drugs were taken from an observationalstudy by Gupta et al. (1997). With treatment with atypicaldrugs, we assume that the percentage of newly diagnosedindividuals who experience an extended episode in theyear of diagnosis is reduced by 60 percent and the relapserate for those experiencing acute episode(s) is 30 percentlower than for those treated with typical drugs.
Moderate or severe symptom days. Days withmoderate or severe symptoms are defined in our analysisas days with a Brief Psychiatric Rating Scale scoregreater than 36 (Overall and Gorham 1962; Tollefson etal. 2001). Moderate or severe symptom days are assumedto be:
• 0 for people not experiencing an episode requiringhospitalization;
• 60 days for each acute episode in newly diagnosed indi-viduals experiencing acute episodes (Gupta et al. 1997);
• 42 days for each acute episode in subsequent years(Tollefson et al. 1997); and
• equal to the number of days in the hospital or otherresidential care facility for newly diagnosed individu-als with extended episodes, extended episode andinstitutionalized individuals.
Working months. Working months are measured asthe product of employment rate and months of employ-ment. The data sources for the employment rate are lim-ited, and thus our estimates are speculative. For newlydiagnosed individuals, Gupta et al. (1997) found that 49
623
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Schizophrenia Bulletin, Vol. 28, No. 4, 2002 J. Mauskopf etal.
Table 3. Resource use and costs (1999)
Resource unit type/Symptom category
Newly diagnosedAcute hospitalState mental hospitalPsychiatry visitsNonphysician therapyHospital outpatient treatmentSuicide legal costsAntipsychotic drugs
TypicalAtypical
Antiparkinsonian drugsTotal annual costs
No episode
Psychiatry visitsNonphysician therapyAntipsychotic drugs
TypicalAtypical
Antiparkinsonian drugsTotal annual costs
Acute episode
Acute hospitalResidential treatmentSuicide attempt hospital carePartial residential treatment
Psychiatry visitsNonphysician therapyHospital outpatient treatment
Suicide legal costsAntipsychotic drugs
TypicalAtypical
Antiparkinsonian drugsTotal annual costs
Extended episode—yr 11
State mental hospitalResidential careAgranulocytosisOutpatient care, including
psychiatrist visits andgroup therapy
Legal costs suicideAntipsychotic drugs
Typical2
Atypical3
Antiparkinsonian drugsTotal annual costs
Unit cost ($)
490/day378/day57/visit49/session78/day1,171/case
0.11/day11.22/day0.54/day
57/visit49/session
0.11/day11.22/day0.54/day
490/day348/day5,223/case249/day57/visit49/visit78/visit1,171/case
0.11/day11.22/day0.54/day
378/day378/day2,666/case51/visit
1,171/case
1.20/day18.05/day0.54/day
Resourceunits
52.517.7127.821.40.0427
292
140
2.615.6
36.5
17.5
28.238.80.084127.55.610.625.10.0135
310
149
5976083.5
0.007
203.8
136.6
Typical
Costs ($)
25,7056,6916843821,66650
31
7635,285
148764
4
9926
13,79813,4864396,8353205201,95116
33
8037,477
22,27228,70504,258
8
245
7455,562
Resourceunits
48.37.1127.815.50.0385
31071
2.615.6
80.318.5
26.336.10.078625.65.410.925.30.0127
31071
50.865.50.005125.3
0.0056
5518772
Atypical
Cost* (I)
23,6592,6766843821,21045
3,4813932,177
148764
901101,824
12,90412,5524106,3623095361,97215
3,4813938,578
19,19824,744136,391
7
664,0093946,481
624
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Costs and Benefits of New Drug Therapies Schizophrenia Bulletin, Vol. 28, No. 4, 2002
Resource unit type/Symptom category
Institutionalized—yr 11
State mental hospitalResidential careAgranulocytosisOutpatient care, including
psychiatrist visits andgroup therapy
Legal costs suicideAntipsychotic drugs
Typical2
Atypical3
AntJparkinsonian drugsTotal annual costs
Unit cost ($)
378/day378/day2,666/case51/visit
1,171
0.25/day18.05/day0.54/day
Resourceunits
365
0
0.007
365
245
Typical
Costs (S)
137,970
8
91
132138,202
Resourceunits
220.294.40.00529.7
0.0056
98240.1110.4
Atypical
Costs ($)
83,23535,696131,516
7
255,13760125,689
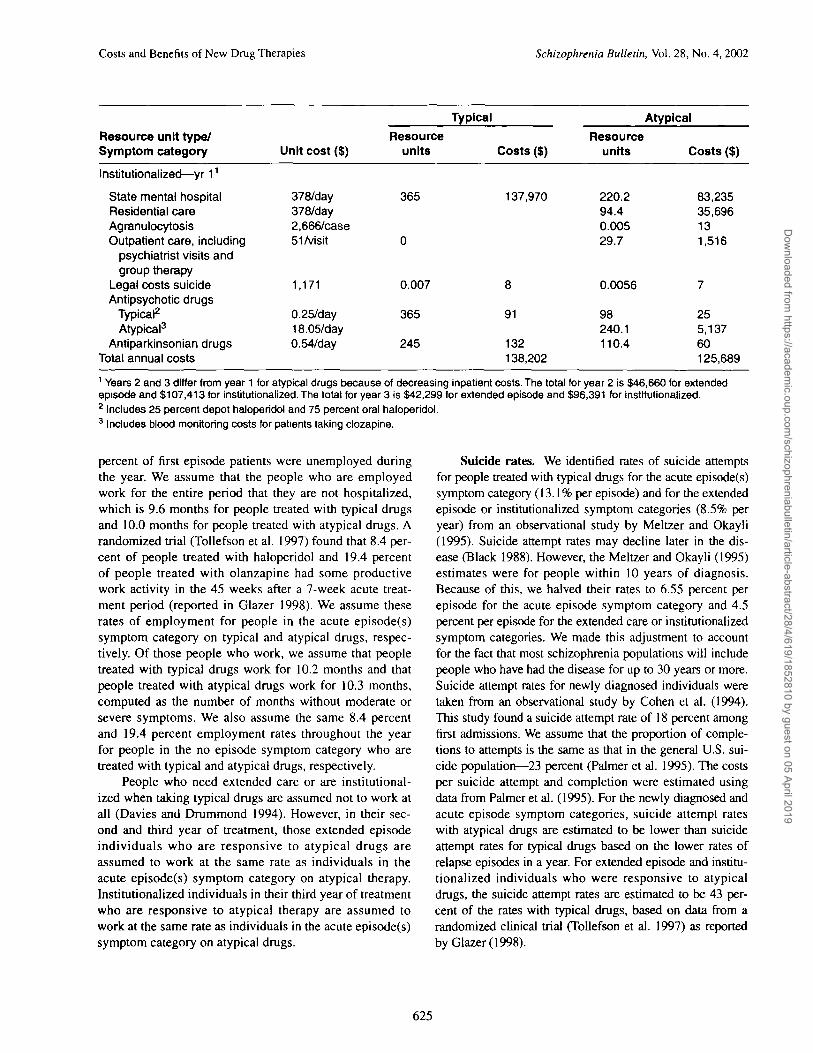
1 Years 2 and 3 differ from year 1 for atypical drugs because of decreasing inpatient costs. The total for year 2 is $46,660 for extendedepisode and $107,413 for institutionalized. The total for year 3 is $42,299 for extended episode and $96,391 for institutionalized.2 Includes 25 percent depot haloperidol and 75 percent oral haloperidol.3 Includes blood monitoring costs for patients taking clozapine.
percent of first episode patients were unemployed duringthe year. We assume that the people who are employedwork for the entire period that they are not hospitalized,which is 9.6 months for people treated with typical drugsand 10.0 months for people treated with atypical drugs. Arandomized trial (Tollefson et al. 1997) found that 8.4 per-cent of people treated with haloperidol and 19.4 percentof people treated with olanzapine had some productivework activity in the 45 weeks after a 7-week acute treat-ment period (reported in Glazer 1998). We assume theserates of employment for people in the acute episode(s)symptom category on typical and atypical drugs, respec-tively. Of those people who work, we assume that peopletreated with typical drugs work for 10.2 months and thatpeople treated with atypical drugs work for 10.3 months,computed as the number of months without moderate orsevere symptoms. We also assume the same 8.4 percentand 19.4 percent employment rates throughout the yearfor people in the no episode symptom category who aretreated with typical and atypical drugs, respectively.
People who need extended care or are institutional-ized when taking typical drugs are assumed not to work atall (Davies and Drummond 1994). However, in their sec-ond and third year of treatment, those extended episodeindividuals who are responsive to atypical drugs areassumed to work at the same rate as individuals in theacute episode(s) symptom category on atypical therapy.Institutionalized individuals in their third year of treatmentwho are responsive to atypical therapy are assumed towork at the same rate as individuals in the acute episode(s)symptom category on atypical drugs.
Suicide rates. We identified rates of suicide attemptsfor people treated with typical drugs for the acute episode(s)symptom category (13.1% per episode) and for the extendedepisode or institutionalized symptom categories (8.5% peryear) from an observational study by Meltzer and Okayli(1995). Suicide attempt rates may decline later in the dis-ease (Black 1988). However, the Meltzer and Okayli (1995)estimates were for people within 10 years of diagnosis.Because of this, we halved their rates to 6.55 percent perepisode for the acute episode symptom category and 4.5percent per episode for the extended care or institutionalizedsymptom categories. We made this adjustment to accountfor the fact that most schizophrenia populations will includepeople who have had the disease for up to 30 years or more.Suicide attempt rates for newly diagnosed individuals weretaken from an observational study by Cohen et al. (1994).This study found a suicide attempt rate of 18 percent amongfirst admissions. We assume that the proportion of comple-tions to attempts is the same as that in the general U.S. sui-cide population—23 percent (Palmer et al. 1995). The costsper suicide attempt and completion were estimated usingdata from Palmer et al. (1995). For the newly diagnosed andacute episode symptom categories, suicide attempt rateswith atypical drugs are estimated to be lower than suicideattempt rates for typical drugs based on the lower rates ofrelapse episodes in a year. For extended episode and institu-tionalized individuals who were responsive to atypicaldrugs, the suicide attempt rates are estimated to be 43 per-cent of the rates with typical drugs, based on data from arandomized clinical trial (Tollefson et al. 1997) as reportedby Glazer (1998).
625
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Schizophrenia Bulletin, Vol. 28, No. 4, 2002 J. Mauskopf et al.
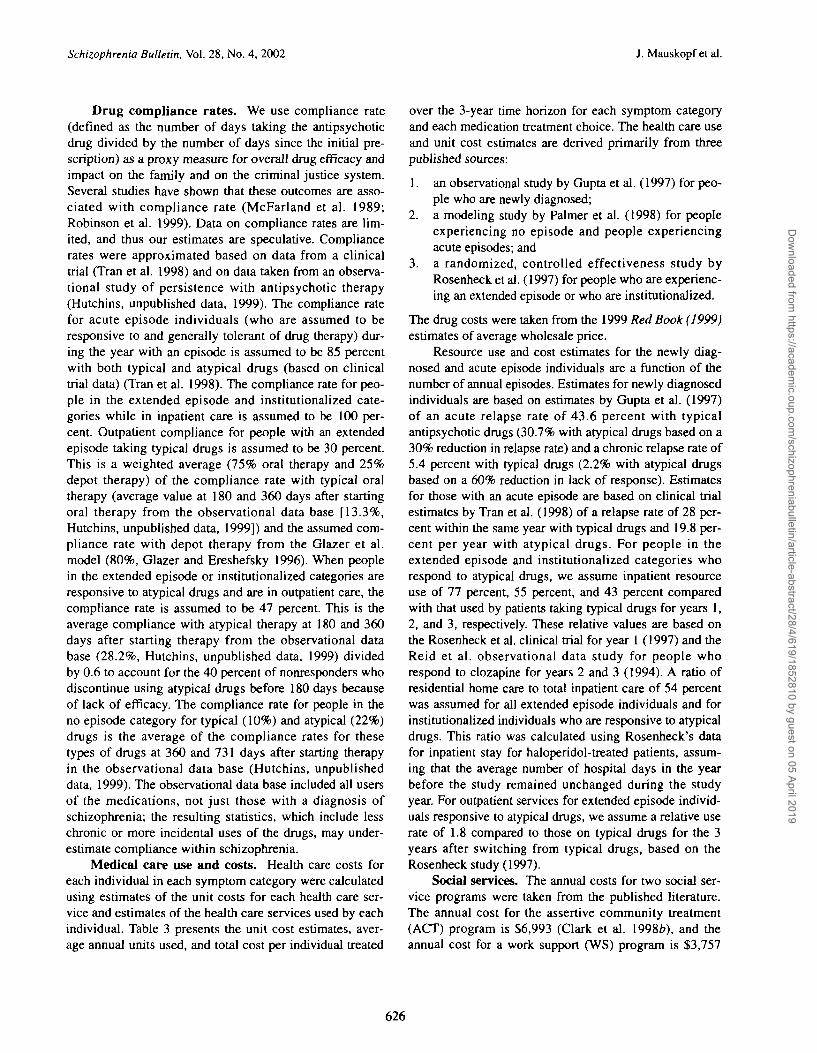
Drug compliance rates. We use compliance rate(defined as the number of days taking the antipsychoticdrug divided by the number of days since the initial pre-scription) as a proxy measure for overall drug efficacy andimpact on the family and on the criminal justice system.Several studies have shown that these outcomes are asso-ciated with compliance rate (McFarland et al. 1989;Robinson et al. 1999). Data on compliance rates are lim-ited, and thus our estimates are speculative. Compliancerates were approximated based on data from a clinicaltrial (Tran et al. 1998) and on data taken from an observa-tional study of persistence with antipsychotic therapy(Hutchins, unpublished data, 1999). The compliance ratefor acute episode individuals (who are assumed to beresponsive to and generally tolerant of drug therapy) dur-ing the year with an episode is assumed to be 85 percentwith both typical and atypical drugs (based on clinicaltrial data) (Tran et al. 1998). The compliance rate for peo-ple in the extended episode and institutionalized cate-gories while in inpatient care is assumed to be 100 per-cent. Outpatient compliance for people with an extendedepisode taking typical drugs is assumed to be 30 percent.This is a weighted average (75% oral therapy and 25%depot therapy) of the compliance rate with typical oraltherapy (average value at 180 and 360 days after startingoral therapy from the observational data base [13.3%,Hutchins, unpublished data, 1999]) and the assumed com-pliance rate with depot therapy from the Glazer et al.model (80%, Glazer and Ereshefsky 1996). When peoplein the extended episode or institutionalized categories areresponsive to atypical drugs and are in outpatient care, thecompliance rate is assumed to be 47 percent. This is theaverage compliance with atypical therapy at 180 and 360days after starting therapy from the observational database (28.2%, Hutchins, unpublished data, 1999) dividedby 0.6 to account for the 40 percent of nonresponders whodiscontinue using atypical drugs before 180 days becauseof lack of efficacy. The compliance rate for people in theno episode category for typical (10%) and atypical (22%)drugs is the average of the compliance rates for thesetypes of drugs at 360 and 731 days after starting therapyin the observational data base (Hutchins, unpublisheddata, 1999). The observational data base included all usersof the medications, not just those with a diagnosis ofschizophrenia; the resulting statistics, which include lesschronic or more incidental uses of the drugs, may under-estimate compliance within schizophrenia.
Medical care use and costs. Health care costs foreach individual in each symptom category were calculatedusing estimates of the unit costs for each health care ser-vice and estimates of the health care services used by eachindividual. Table 3 presents the unit cost estimates, aver-age annual units used, and total cost per individual treated
over the 3-year time horizon for each symptom categoryand each medication treatment choice. The health care useand unit cost estimates are derived primarily from threepublished sources:
1. an observational study by Gupta et al. (1997) for peo-ple who are newly diagnosed;
2. a modeling study by Palmer et al. (1998) for peopleexperiencing no episode and people experiencingacute episodes; and
3. a randomized, controlled effectiveness study byRosenheck et al. (1997) for people who are experienc-ing an extended episode or who are institutionalized.
The drug costs were taken from the 1999 Red Book (1999)estimates of average wholesale price.
Resource use and cost estimates for the newly diag-nosed and acute episode individuals are a function of thenumber of annual episodes. Estimates for newly diagnosedindividuals are based on estimates by Gupta et al. (1997)of an acute relapse rate of 43.6 percent with typicalantipsychotic drugs (30.7% with atypical drugs based on a30% reduction in relapse rate) and a chronic relapse rate of5.4 percent with typical drugs (2.2% with atypical drugsbased on a 60% reduction in lack of response). Estimatesfor those with an acute episode are based on clinical trialestimates by Tran et al. (1998) of a relapse rate of 28 per-cent within the same year with typical drugs and 19.8 per-cent per year with atypical drugs. For people in theextended episode and institutionalized categories whorespond to atypical drugs, we assume inpatient resourceuse of 77 percent, 55 percent, and 43 percent comparedwith that used by patients taking typical drugs for years 1,2, and 3, respectively. These relative values are based onthe Rosenheck et al. clinical trial for year 1 (1997) and theReid et al. observational data study for people whorespond to clozapine for years 2 and 3 (1994). A ratio ofresidential home care to total inpatient care of 54 percentwas assumed for all extended episode individuals and forinstitutionalized individuals who are responsive to atypicaldrugs. This ratio was calculated using Rosenheck's datafor inpatient stay for haloperidol-treated patients, assum-ing that the average number of hospital days in the yearbefore the study remained unchanged during the studyyear. For outpatient services for extended episode individ-uals responsive to atypical drugs, we assume a relative userate of 1.8 compared to those on typical drugs for the 3years after switching from typical drugs, based on theRosenheck study (1997).
Social services. The annual costs for two social ser-vice programs were taken from the published literature.The annual cost for the assertive community treatment(ACT) program is $6,993 (Clark et al. 1998b), and theannual cost for a work support (WS) program is $3,757
626
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019

Costs and Benefits of New Drug Therapies Schizophrenia Bulletin, Vol. 28, No. 4, 2002
(Clark et al. 1998a). To make these programs comparableto other ambulatory services, we assume a service unitcost of $43 (the same as a group therapy session) and usethe annual costs to compute an average annual number ofservice units (163 for ACT and 87 for WS). There are fewdata on the proportion of people with schizophrenia whouse either or both of these programs. Usage rates dependon individual characteristics as well as program availabil-ity. We have made a series of assumptions to include inthe model's base case, but these numbers do not have asound basis in the published literature. Therefore, thesenumbers should be updated as more data become avail-able.
We assume that newly diagnosed individuals treatedwith typical or atypical drugs do not use ACT or WS ser-vices. We assume that 20 percent of the people in the acuteand no episode symptom categories use both types of ser-vices when treated with typical drugs, and that 26 percentuse both types of services when treated with atypical drugs(except during time periods when they are experiencingmoderate or severe psychotic symptoms). This differenceis based on the assumption that people who experiencefewer negative symptoms may be more likely to use theseservices if given the option (Weiden et al. 1996). Weassume that extended episode and institutionalized indi-viduals do not use either ACT or WS services when treatedwith typical drugs, or when they are nonresponsive toatypical drugs. For extended episode individuals who areresponsive to atypical drugs, we assume service use rateswhile they are not hospitalized of:
• 10 percent ACT and 0 percent WS in year 1;26 percent ACT and 13 percent WS in year 2; and
• 26 percent ACT and 26 percent WS in year 3.
For institutionalized patients who are responsive to atypi-cal drugs, we assume service use rates while they are nothospitalized of:
• 0 percent ACT and WS in year 1;• 10 percent ACT and 0 percent WS in year 2; and• 26 percent ACT and 13 percent WS in year 3.
Analyses—Base Case and Sensitivity Analyses. Thebase case analysis compares the use of typical drugs andthe use of atypical drugs for 1,000 people with schizo-phrenia with a distribution of disease symptom categoriessimilar to that of the U.S. population. Annual costs andindividual and proxy outcomes are estimated. For the sen-sitivity analyses, we determine the impact of changes inthe following input parameter values on the outcomes:
• distribution of disease symptom categories within theschizophrenia population (e.g., for state mental hospi-tal or community mental health center populations);
• impact of change to atypical drugs on "revolvingdoor" individuals (defined as people experiencing twoacute episodes in a single year);
• upper and lower bounds for differences in antipsy-chotic drug relapse and response rates;
• average daily costs for inpatient residential care;• average daily costs for atypical drugs; and• impact of change to atypical drugs on Medi-Cal
expenditures for people with schizophrenia.
Results
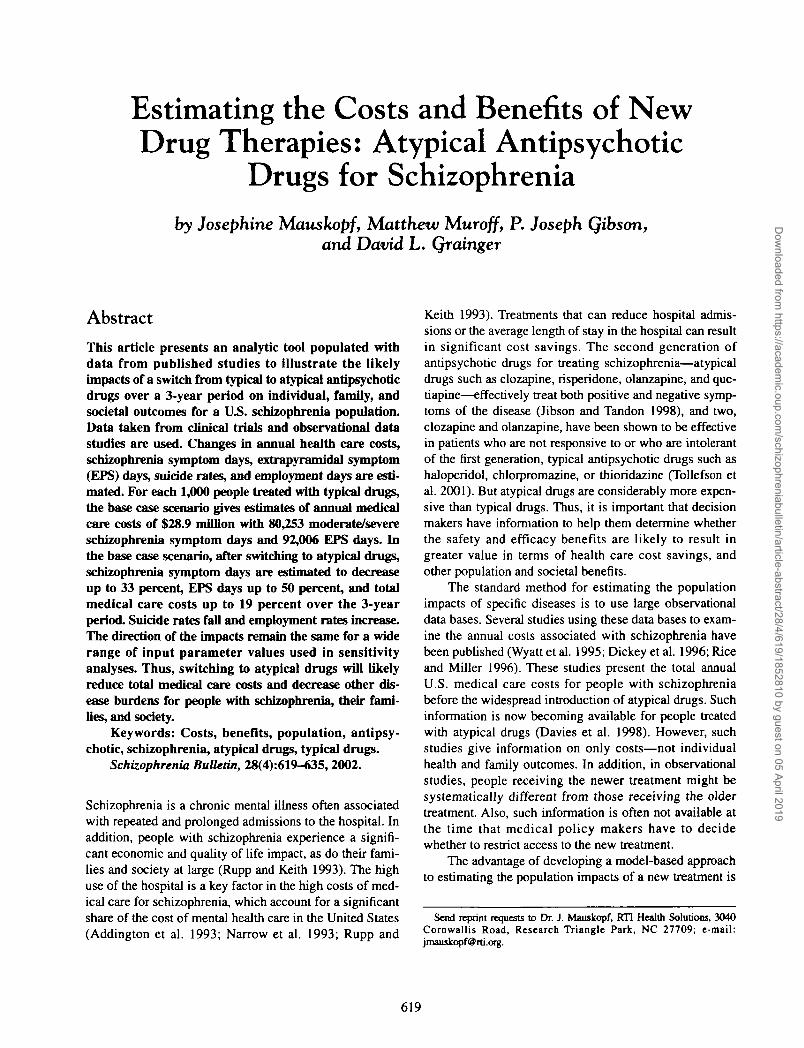
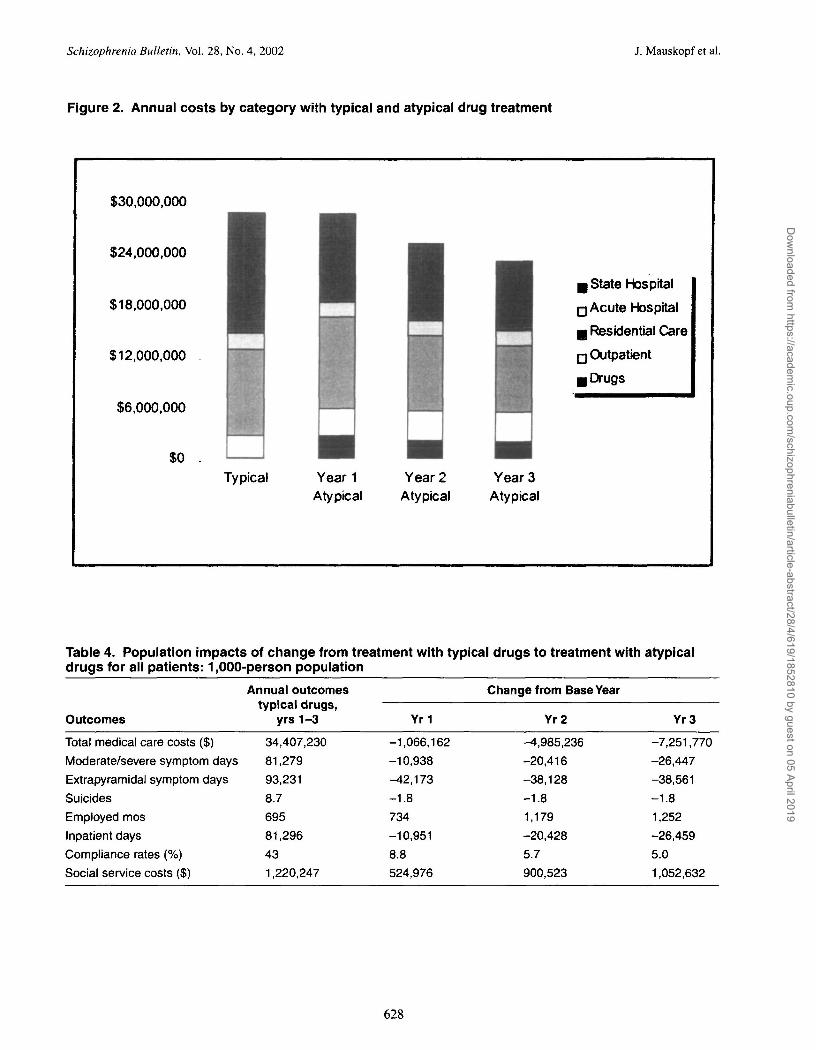
Figure 2 presents the impact of switching to atypical drugson total medical care costs and different cost subcategoriesfor 1,000 people with schizophrenia. In year 1, a decreasein hospital and residential care costs is offset by an increasein medication and outpatient costs, producing a netdecrease of 1 percent compared with treatment with typicaldrugs. In years 2 and 3, following the switch to atypicaldrugs, the drug and outpatient costs remain fairly constant,while the state mental hospital and residential care costscontinue to decline. The result is decreases in total medicalcosts of 13 percent (year 2) and 19 percent (year 3), relativeto costs under treatment with typical drugs.
Table 4 presents the impact of switching to atypicaldrugs on costs as well as on other individual patient out-comes. Relative to treatment with typical drugs, EPS daysare 45 percent lower in year 1 and 41 percent lower in year3. The number of moderate to severe symptom days is 13percent lower in year 1 and 33 percent lower in year 3.Suicides are reduced by 21 percent, compliance isincreased by 12 percent to 21 percent, and inpatient daysare reduced 13 percent in year 1 to 33 percent in year 3.Costs for social services such as vocational rehabilitationare increased by 43 percent in year 1 to 86 percent in year3, as people leave inpatient settings and are able to benefitfrom these services. Employed months increase by 106percent in year 1 to 180 percent in year 3.
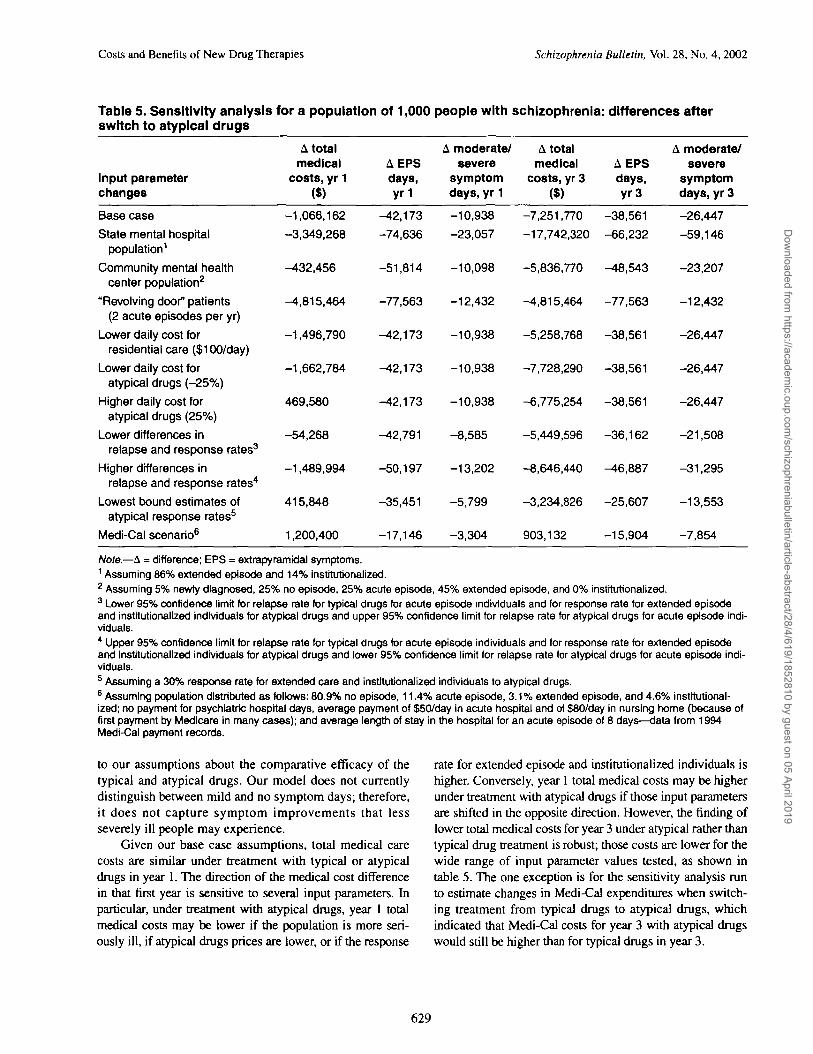
Table 5 presents the results of the sensitivity analysis.The impacts of changes in the parameter values are shownfor years 1 and 3 only. The impacts are shown for totalmedical care cost, EPS days, and moderate/severe symp-tom days as representative of societal and patient out-comes. Under most of our assumptions about drug use pat-terns and unit costs, EPS days and moderate/severesymptom days decrease as more people are treated withatypical drugs. However, because of higher compliancerates expected for people with no episode in a given yeartaking atypical agents, EPS days could be slightly higherin this subgroup if people are treated with atypical drugs,depending on the drug used and the dose prescribed.Reductions in moderate/severe symptom days are sensitiveto the disease severity of the treated population as well as
627
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Schizophrenia Bulletin, Vol. 28, No. 4, 2002 J. Mauskopf et al.
Figure 2. Annual costs by category with typical and atypical drug treatment
$30,000,000
$24,000,000
$18,000,000
$12,000,000
$6,000,000
$0
B State Hospital
Q Acute Hospital
g Residential Care
• Outpatient
• Drugs
Typical Year iAtypical
Year 2Atypical
Year 3Atypical
Table 4. Population impacts of change from treatment with typical drugs to treatment with atypicaldrugs for all patients: 1,000-person population
Outcomes
Total medical care costs ($)
Moderate/severe symptom days
Extrapyramidal symptom days
Suicides
Employed mos
Inpatient days
Compliance rates (%)
Social service costs ($)
Annual outcomes
typical drugs,yrs 1-3
34,407,230
81,279
93,231
8.7
695
81,296
43
1,220,247
Yr1
-1,066,162
-10,938
-42,173
-1.8
734
-10,951
8.8
524,976
Change from Base Year
Yr2
-4,985,236-20,416
-38,128
-1.8
1,179
-20,428
5.7
900,523
Yr3
-7,251,770
-26,447
-38,561
-1.8
1,252
-26,459
5.0
1,052,632
628
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Costs and Benefits of New Drug Therapies Schizophrenia Bulletin, Vol. 28, No. 4, 2002
Table 5. Sensitivity analysis for a population of 1,000 people with schizophrenia: differences afterswitch to atypical drugs
Input parameterchanges
Base case
State mental hospitalpopulation1
Community mental healthcenter population2
"Revolving door" patients(2 acute episodes per yr)
Lower daily cost torresidential care ($100/day)
Lower daily cost foratypical drugs (-25%)
Higher daily cost foratypical drugs (25%)
Lower differences inrelapse and response rates3
Higher differences inrelapse and response rates4
Lowest bound estimates ofatypical response rates5
Medi-Cal scenario6
A totalmedical
costs, yr 1($)
-1,066,162
-3,349,268
-432,456
-4,815,464
-1,496,790
-1,662,784
469,580
-54,268
-1,489,994
415,848
1,200,400
A moderate/ A totalA EPS severe medicaldays, symptom costs, yr 3yr 1 days, yr 1 ($)
A moderate/A EPS severedays, symptomyr 3 days, yr 3
-42,173 -10,938 -7,251,770 -38,561 -26,447
-74,636 -23,057 -17,742,320 -66,232 -59,146
-51,814 -10,098 -5,836,770 -48,543 -23,207
-77,563 -12,432 -4,815,464 -77,563 -12,432
-42,173 -10,938 -5,258,768 -38,561 -26,447
-42,173 -10,938 -7,728,290 -38,561 -26,447
-42,173 -10,938 -6,775,254 -38,561 -26,447
-42,791 -8,585 -5,449,596 -36,162 -21,508
-50,197 -13,202 -8,646,440 -46,887 -31,295
-35,451 -5,799 -3,234,826 -25,607 -13,553
-17,146 -3,304 903,132 -15,904 -7,854Note.—A = difference; EPS = extrapyramidal symptoms.1 Assuming 86% extended episode and 14% institutionalized.2 Assuming 5% newty diagnosed, 25% no episode, 25% acute episode, 45% extended episode, and 0% institutionalized.3 Lower 95% confidence limit for relapse rate for typical drugs for acute episode individuals and for response rate for extended episodeand institutionalized individuals for atypical drugs and upper 95% confidence limit for relapse rate for atypical drugs for acute episode indi-viduals.4 Upper 95% confidence limit for relapse rate for typical drugs for acute episode individuals and for response rate for extended episodeand institutionalized individuals for atypical drugs and lower 95% confidence limit for relapse rate for atypical drugs for acute episode indi-viduals.5 Assuming a 30% response rate for extended care and institutionalized individuals to atypical drugs.6 Assuming population distributed as follows: 80.9% no episode, 11.4% acute episode, 3.1% extended episode, and 4.6% institutional-ized; no payment for psychiatric hospital days, average payment of $50/day in acute hospital and of $80/day in nursing home (because offirst payment by Medicare in many cases); and average length of stay in the hospital for an acute episode of 8 days—data from 1994Medi-Cal payment records.
to our assumptions about the comparative efficacy of thetypical and atypical drugs. Our model does not currentlydistinguish between mild and no symptom days; therefore,it does not capture symptom improvements that lessseverely ill people may experience.
Given our base case assumptions, total medical carecosts are similar under treatment with typical or atypicaldrugs in year 1. The direction of the medical cost differencein that first year is sensitive to several input parameters. Inparticular, under treatment with atypical drugs, year 1 totalmedical costs may be lower if the population is more seri-ously ill, if atypical drugs prices are lower, or if the response
rate for extended episode and institutionalized individuals ishigher. Conversely, year 1 total medical costs may be higherunder treatment with atypical drugs if those input parametersare shifted in the opposite direction. However, the finding oflower total medical costs for year 3 under atypical rather thantypical drug treatment is robust; those costs are lower for thewide range of input parameter values tested, as shown intable 5. The one exception is for the sensitivity analysis runto estimate changes in Medi-Cal expenditures when switch-ing treatment from typical drugs to atypical drugs, whichindicated that Medi-Cal costs for year 3 with atypical drugswould still be higher than for typical drugs in year 3.
629
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Schizophrenia Bulletin, Vol. 28, No. 4, 2002 J. Mauskopf et al.
Discussion
The model base case estimates indicate that switchingpeople from typical drugs to atypical drugs will improveindividual and family well-being with decreased medicalcare costs and increased social service costs. Although thecost and outcome estimates are sensitive to input parame-ter assumptions, for a wide variety of parameter values,medical care costs were shown to decrease by the thirdyear after switching to atypical drugs. The one exception isthe scenario run estimating Medi-Cal expenditures forpeople with schizophrenia. The main reason for the differ-ence in results using this scenario is that Medi-Cal doesnot pay for all of the costs of treating people with schizo-phrenia. Payments for hospitalizations at psychiatric facil-ities are reimbursed through not Medi-Cal but other publicfunds. There is also a substantial portion of people withschizophrenia whose disabled status qualifies them forboth Medicare and Medi-Cal, in which case Medicare isthe primary payer for hospital and physician services,while Medi-Cal pays for medications. The Medi-Cal sce-nario may also overestimate the portion of the populationwith no episode, as some psychiatric hospitalizations maynot be captured in the data. Thus, the Medi-Cal scenarioomits much of the savings in public funds that may resultfrom fewer hospitalizations among those using atypicalantipsychotics. The Medi-Cal scenario might also under-estimate the reductions in symptom and EPS days in theirpopulation. This result illustrates the importance of look-ing at the total costs associated with treatment of schizo-phrenia rather than taking the perspective of a single payer.
A key value of the interactive computer model used togenerate these results is that the input parameter valuescan readily be altered to reflect a specific schizophreniapopulation as well as regional patterns of care and unitcosts. Thus, the outcomes of a switch from typical to atyp-ical drugs can be estimated for the population of interest.
It is very important to develop methods that extrapolatefrom clinical trial data to the population for which a decisionmaker may be responsible. In this article, we have assumedthat the efficacy rates shown in clinical trial and observa-tional study populations are the same as would be observedin normal practice for people with characteristics similar tothose of the people enrolled in the trials. In addition, we haveextrapolated from the types of people typically enrolled inclinical trials to the more general population using data fromepidemiological studies of schizophrenia to determine theactual symptom profile. For example, clinical trials of newschizophrenia drugs often enroll only people who are experi-encing moderate or severe psychotic symptoms requiringhospitalization. A large proportion of the schizophrenia pop-ulation will not experience such severe symptoms in anygiven 1-year time period. If people with no episodes are
switched to atypical antipsychotics, they will likely experi-ence an increase in drug costs, a reduction in negative symp-toms, and a reduction in EPS days. In our analysis, we havebeen conservative and have assumed that there are no healthcare cost savings or quality of life gains (e.g., fewer negativesymptoms) for the no episode individuals switched to atypi-cal drugs (apart from fewer days needing EPS drugs).
Our model also illustrates the importance of the timehorizon chosen. Although what happens in the first year thata new drug is introduced is important to decision makers, thefull impact of switching to a new therapy for a long-term ill-ness such as schizophrenia may not be felt for many years.We chose a 3-year time horizon for this model because thereare published data indicating that health care use continuesto fall for up to 3 years for extended episode and institution-alized individuals who respond to an atypical drug (Reid etal. 1994). Other possible impacts of more tolerable or effec-tive therapy might be an increase in the proportion of thepopulation who experience no episodes during a given yearor a reduction in the proportion of newly diagnosed individu-als who go on to experience extended episodes or to be insti-tutionalized. Over time, these impacts would reduce the pro-portion of acute episode, extended episode, orinstitutionalized individuals in the prevalent population. Ourmodel could be used to estimate the individual, family, andsocietal outcomes associated with such impacts. We have notestimated these outcomes in this article because there arecurrently no data to demonstrate whether such effects occurand what their magnitude might be. Also, these impactswould not become important drivers of the total cost andhealth burdens for a schizophrenia population until severalyears after the introduction of the new drugs.
An important issue that has to be addressed whendeveloping models of the impact of new drugs is the con-flict between the decision makers' need for more detailedinformation and the availability of experimental or obser-vational data to support those estimates. The relapse andresponse rate data used in this study were taken from ran-domized, controlled efficacy or effectiveness trials(Rosenheck et al. 1997; Beasley et al. 1998; Tran et al.1998). However, when we first presented the model todecision makers, they expressed the need to have estimatesof inpatient care broken out by type of inpatient care (e.g.,into acute hospital, state hospital, and nursing home orother residential care facility). The problem was that thesedata were not presented at this level of detail in the pub-lished literature for the extended episode and institutional-ized individuals. To produce the estimates of this break-down, we developed the algorithm described in theMethods section. The decision makers also wanted infor-mation on the use of social services by people with schizo-phrenia and how this might change with the introductionof atypical agents. There were no studies that indicated the
630
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Costs and Benefits of New Drug Therapies Schizophrenia Bulletin, Vol. 28, No. 4, 2002
current magnitude of use—we used a verbal estimate fromNational Alliance for the Mentally 111 personnel—andthere were only anecdotal data that indicated an increasein use of these services by patients taking atypical drugs.Thus, the modeler faces a dilemma when the data are notsufficient to give the decision maker the information at thenecessary level of detail. Our solution was to make all ofour assumptions clear and allow them to be easily changedin an interactive computer model. This method allows theassumptions to be updated as more data become available.
Developing models to estimate the annual burden of anillness with and without use of a new therapy can provideimportant information when a decision must be made aboutthe use of the new therapy. Previous studies of the burden ofschizophrenia have taken a retrospective look at large U.S.data bases to derive the estimates (Wyatt et al. 1995; Dickeyet al. 19%; Rice and Miller 19%). While retrospective stud-ies estimate actual costs incurred, they cannot estimate theimpact of new treatments in a timely manner. Once the newtreatments have been widely used for several years (allowing
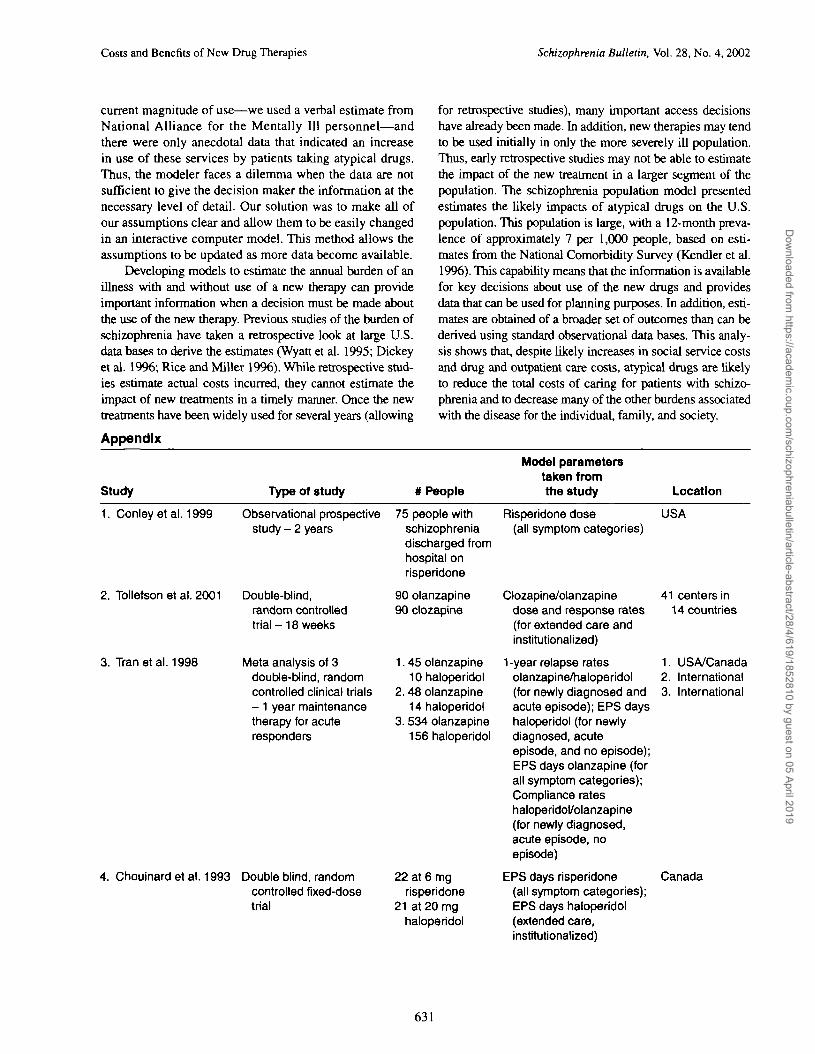
Appendix
for retrospective studies), many important access decisionshave already been made. In addition, new therapies may tendto be used initially in only the more severely ill population.Thus, early retrospective studies may not be able to estimatethe impact of the new treatment in a larger segment of thepopulation. The schizophrenia population model presentedestimates the likely impacts of atypical drugs on the U.S.population. This population is large, with a 12-month preva-lence of approximately 7 per 1,000 people, based on esti-mates from the National Comorbidity Survey (Kendler et al.19%). This capability means that the information is availablefor key decisions about use of the new drugs and providesdata that can be used for planning purposes. In addition, esti-mates are obtained of a broader set of outcomes than can bederived using standard observational data bases. This analy-sis shows that, despite likely increases in social service costsand drug and outpatient care costs, atypical drugs are likelyto reduce the total costs of caring for patients with schizo-phrenia and to decrease many of the other burdens associatedwith the disease for the individual, family, and society.
Study Type of study # People
Model parameterstaken fromthe study Location
1. Conley etal. 1999
2. Tollefson et al. 2001
3. Tran etal. 1998
Observational prospectivestudy - 2 years
Double-Wind,random controlledtrial - 18 weeks
Meta analysis of 3double-Wind, randomcontrolled clinical trials- 1 year maintenancetherapy for acuteresponders
75 people withschizophreniadischarged fromhospital onrisperidone
90 olanzapine90 clozapine
1.45 olanzapine10 haloperidol
2. 48 olanzapine14 haloperidol
3. 534 olanzapine156 haloperidol
4. Chouinard et al. 1993 Double blind, randomcontrolled fixed-dosetrial
22 at 6 mgrisperidone
21 at 20 mghaloperidol
Risperidone dose USA(all symptom categories)
Clozapine/olanzapine 41 centers indose and response rates 14 countries(for extended care andinstitutionalized)
1-year relapse rates 1. USA/Canadaolanzapine/haloperidol 2. International(for newly diagnosed and 3. Internationalacute episode); EPS dayshaloperidol (for newlydiagnosed, acuteepisode, and no episode);EPS days olanzapine (forall symptom categories);Compliance rateshaloperidol/olanzapine(for newly diagnosed,acute episode, noepisode)
EPS days risperidone Canada(all symptom categories);EPS days haloperidol(extended care,institutionalized)
631
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Schizophrenia Bulletin, Vol. 28, No. 4, 2002 J. Mauskopf et al.
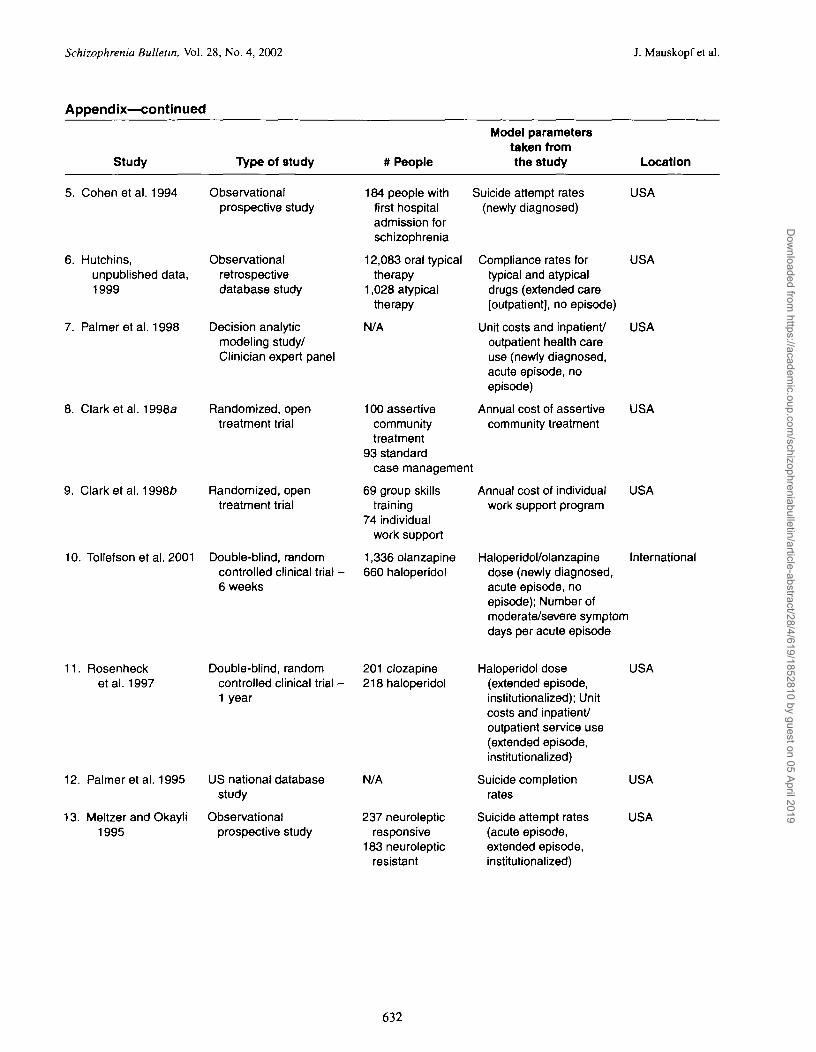
Appendix—continued
Study Type of study # People
Model parameterstaken fromthe study Location
5. Cohen etal. 1994 Observationalprospective study
6. Hutchins,unpublished data,1999
7. Palmer etal. 1998
Observationalretrospectivedatabase study
Decision analyticmodeling study/Clinician expert panel
8. Clark et al. 1998a Randomized, opentreatment trial
9. Clark et al. 1998fc> Randomized, opentreatment trial
10. Tollefson et al. 2001 Double-blind, randomcontrolled clinical trial •6 weeks
184 people withfirst hospitaladmission forschizophrenia
12,083 oral typicaltherapy
1,028 atypicaltherapy
N/A
100 assertivecommunitytreatment
93 standardcase management
69 group skillstraining
74 individualwork support
1,336 olanzapine660 haloperidol
Suicide attempt rates USA(newly diagnosed)
Compliance rates for USAtypical and atypicaldrugs (extended care[outpatient], no episode)
Unit costs and inpatient/ USAoutpatient health careuse (newly diagnosed,acute episode, noepisode)
Annual cost of assertive USAcommunity treatment
Annual cost of individual USAwork support program
Haloperidol/olanzapine Internationaldose (newly diagnosed,acute episode, noepisode); Number ofmoderate/severe symptomdays per acute episode
11. Rosenhecketal. 1997
12. Palmer etal. 1995
13. Meltzer and Okayli1995
Double-blind, randomcontrolled clinical trial -1 year
US national databasestudy
Observationalprospective study
201 clozapine218 haloperidol
N/A
237 neurolepticresponsive
183 neurolepticresistant
Haloperidol dose(extended episode,institutionalized); Unitcosts and inpatient/outpatient service use(extended episode,institutionalized)
Suicide completionrates
Suicide attempt rates(acute episode,extended episode,institutionalized)
USA
USA
USA
632
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Costs and Benefits of New Drug Therapies Schizophrenia Bulletin, Vol. 28, No. 4, 2002
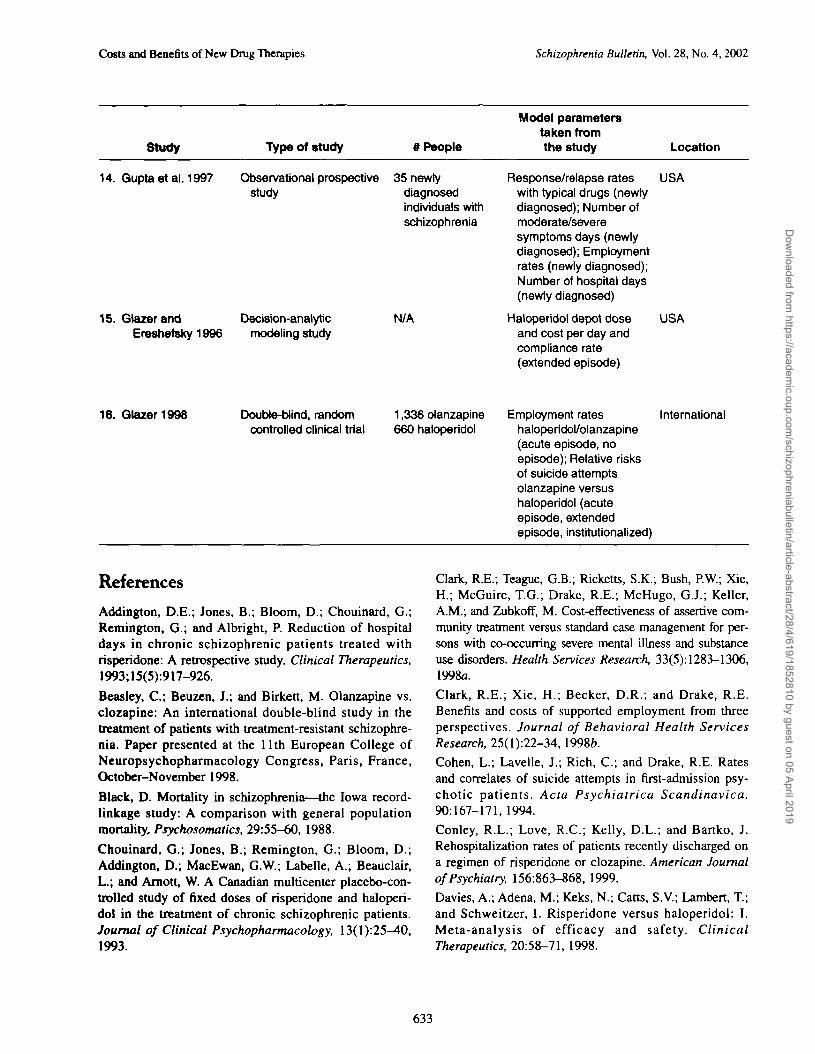
Study Type of study # People
Model parameterstaken fromthe study Location
14. Gupta eta). 1997 Observational prospectivestudy
15. GlazerandEreshefsky1996
Decision-analyticmodeling study
35 newtydiagnosedindividuals withschizophrenia
N/A
Response/relapse rates USAwith typical drugs (newtydiagnosed); Number ofmoderate/severesymptoms days (newlydiagnosed); Employmentrates (newly diagnosed);Number of hospital days(newly diagnosed)
Haloperidol depot dose USAand cost per day andcompliance rate(extended episode)
16. Glazer1998 Double-blind, randomcontrolled clinical trial
1,336 olanzapine660 haloperidol
Employment rateshaloperidol/olanzapine(acute episode, noepisode); Relative risksof suicide attemptsolanzapine versushaloperidol (acuteepisode, extendedepisode, institutionalized)
International
References
Addington, D.E.; Jones, B.; Bloom, D.; Chouinard, G.;Remington, G.; and Albright, P. Reduction of hospitaldays in chronic schizophrenic patients treated withrisperidone: A retrospective study. Clinical Therapeutics,1993;15(5):917-926.
Beasley, C ; Beuzen, J.; and Birkett, M. Olanzapine vs.clozapine: An international double-blind study in thetreatment of patients with treatment-resistant schizophre-nia. Paper presented at the 11th European College ofNeuropsychopharmacology Congress, Paris, France,October-November 1998.
Black, D. Mortality in schizophrenia—the Iowa record-linkage study: A comparison with general populationmortality, Psychosomatics, 29:55-60, 1988.
Chouinard, G.; Jones, B.; Remington, G.; Bloom, D.;Addington, D.; MacEwan, G.W.; Labelle, A.; Beauclair,L.; and Amott, W. A Canadian multicenter placebo-con-trolled study of fixed doses of risperidone and haloperi-dol in the treatment of chronic schizophrenic patients.Journal of Clinical Psychopharmacology, 13(1):25—40,1993.
Clark, R.E.; Teague, G.B.; Ricketts, S.K.; Bush, P.W.; Xie,H.; McGuire, T.G.; Drake, R.E.; McHugo, G.J.; Keller,A.M.; and Zubkoff, M. Cost-effectiveness of assertive com-munity treatment versus standard case management for per-sons with co-occurring severe mental illness and substanceuse disorders. Health Services Research, 33(5): 1283-1306,1998a.
Clark, R.E.; Xie, H.; Becker, D.R.; and Drake, R.E.Benefits and costs of supported employment from threeperspectives. Journal of Behavioral Health ServicesResearch, 25(l):22-34, \99%b.
Cohen, L.; Lavelle, J.; Rich, C ; and Drake, R.E. Ratesand correlates of suicide attempts in first-admission psy-chotic patients. Acta Psychiatrica Scandinavica,90:167-171, 1994.
Conley, R.L.; Love, R.C.; Kelly, D.L.; and Bartko, J.Rehospitalization rates of patients recently discharged ona regimen of risperidone or clozapine. American Journalof Psychiatry, 156:863-868, 1999.
Davies, A.; Adena, M.; Keks, N.; Catts, S.V.; Lambert, T;and Schweitzer, I. Risperidone versus haloperidol: I.Meta-analysis of efficacy and safety. ClinicalTherapeutics, 20:58-71, 1998.
633
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019
Schizophrenia Bulletin, Vol. 28, No. 4, 2002 J. Mauskopf et al.
Davies, L.M., and Drummond, M.F. Economics andschizophrenia: The real cost. British Journal ofPsychiatry, 165(Suppl 25): 18-21, 1994.
Dickey, B.; Normand, S.L.; Norton, E.; Azeni, H.; Fisher,W.; and Altaffer, F. Managing the care of schizophrenia:Lessons from a 4-year Massachusetts Medicaid study.Archives of General Psychiatry, 53:945-952, 1996.
Glazer, W. Formulary decisions and health economics.Journal of Clinical Psychiatry, 59(Suppl 19):23-29, 1998.
Glazer, W.M., and Ereshefsky, L. A pharmacoeconomicmodel of outpatient antipsychotic therapy in "revolvingdoor" schizophrenic patients. Journal of ClinicalPsychiatry, 57:337-345, 1996.
Gupta, S.; Andreasen, N.C.; Arndt, S.; Flaum, M.;Hubbard, W.C.; and Ziebell, S. The Iowa longitudinalstudy of recent onset psychosis: One-year follow-up offirst-episode patients. Schizophrenia Research, 23:1-13,1997.
Jibson, M., and Tandon, R. New atypical antipsychoticmedications. Journal of Psychiatric Research,32:215-228, 1998.
Juarez-Reyes, M.G.; Shumway, M.; Battle, C; Bacchetti,P.; Hansen, M.S.; and Hargreaves, W.A. Effects of strin-gent criteria on eligibility for clozapine among publicmental health clients. Psychiatric Services,1995;46(8):801-806.
Kane, J.; Honifeld, G.; Singer, J.; Meltzer, H.; and theClozaril Collaborative Study Group. Clozapine for treat-ment resistant schizophrenia. Archives of GeneralPsychiatry, 45:789-796, 1988.
Kendler, K.S.; Gallagher, T.J.; Abelson, J.M.; and Kessler,R.C. Lifetime prevalence, demographic risk factors, anddiagnostic validity of nonaffective psychosis as assessedin a U.S. community sample. Archives of GeneralPsychiatry, 53:1022-1031, 1996.
Kleiser, E.; Lehmann, E.; Kinzler, E.; Wurthmann, C; andHeinrich, K. Randomized, double-blind, controlled trial ofrisperidone versus clozapine in patients with chronicschizophrenia. Journal of Clinical Psychopharmacology,15(Suppl 1):45S-51S, 1995.
Lieberman, J.A. Prediction of outcome in first-episodeschizophrenia. Journal of Clinical Psychiatry,54(Suppl): 13-17, 1993.
Mauskopf, J.; David, K.; Grainger, D.; and Gibson, P.J.Annual health outcomes and treatment costs for schizo-phrenia populations. Journal of Clinical Psychiatry,60(Suppl 19): 14-19, 1999.
McFarland, B.; Faulkner, L.; Bloom, J.; Hallaux, R.; andBray, J.D. Chronic mental illness and the criminal justice sys-tem. Hospital and Community Psychiatry, 40:718-723,1989.
Meltzer, H.Y., and Okayli, G. Reduction of suicidalityduring clozapine treatment of neuroleptic-resistant schizo-phrenia: Impact on risk-benefit assessment. AmericanJournal of Psychiatry, 152:183-190, 1995.
Narrow, W.; Regier, D.; Rae, D.; Manderscheid, R.W.; andLocke, B.Z. Use of services by persons with mental andaddictive disorders: Findings from the National Instituteof Mental Health epidemiologic catchment area program.Archives of General Psychiatry, 50:95-107, 1993.
Overall, J.E., and Gorham, D.R. The Brief PsychiatricRating Scale. Psychological Reports, 10:799-812, 1962.
Owen, R.R.; Beake, B.J.; Marby, D.; Dessain, E.C.; andCole, J.O. Response to clozapine in chronic psychoticpatients. Psychopharmacology Bulletin, 25:253-256,1989.
Palmer, C.S.; Revicki, D.A.; Genduso, L.A.; Hamilton,S.H.; and Brown, R.E. A cost-effectiveness clinical deci-sion analysis model for schizophrenia. American Journalof Managed Care, 4<3):345-355, 1998.
Palmer, C.S.; Revicki, D.A.; Halpern, M.T.; andHatziandreu, E.J. The cost of suicide and suicide attemptsin the United States. Clinical Neuropharmacology,18(Suppl3):S25-S33, 1995.
Red Book. 1999 Drug Topics Red Book. Montvale, NJ:Medical Economics Company, 1999.
Regier, D.A.; Boyd, J.H.; Burke, J.D.; Rae, D.S.; Myers,J.K.; Kramer, M.; Robins, L.N.; George, L.K.; Karno, M.;and Locke, B.Z. One-month prevalence of mental disor-ders in the United States. Archives of General Psychiatry,45:977-986, 1988.
Reid, W.H.; Mason, M.; and Toprac, M. Savings in hospi-tal bed-days related to treatment with clozapine. Hospitaland Community Psychiatry, 45(3):261-264, 1994.
Rice, D., and Miller, L. The economic burden of schizo-phrenia: Conceptual and methodological issues, and costestimates. In: Moscarelli, M.; Rupp, A.; and Sartorius, N.,eds. Handbook of Mental Health Economics and HealthPolicy, 1996. New York, NY: John Wiley and Sons, 1996.pp. 321-334.
Robinson, D.; Woerner, M.; Alvir, J.; Bilder, R.;Goldman, R.; Geisler, S.; Koreen, A.; Sheitman, B.;Chakos, M.; Mayerhoff, D.; and Liberman, J.A.Predictors of relapse following response from a firstepisode of schizophrenia or schizoaffective disorder.Archives of General Psychiatry, 56:241-247, 1999.
Rosenheck, R.; Cramer, J.; Xu, W.; Thomas, J.;Henderson, W.; Frisman, L.; Fye, C; and Charney, D. Acomparison of clozapine and haloperidol in hospitalizedpatients with refractory schizophrenia. New EnglandJournal of Medicine, 337(12):809-815, 1997.
634
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019

Costs and Benefits of New Drug Therapies Schizophrenia Bulletin, Vol. 28, No. 4, 2002
Rupp, A., and Keith, S.J. The costs of schizophrenia.Psychiatric Clinics of North America, 16X2):413-423, 1993.
Tollefson, G.D.; Beasley, CM.; Tran, P.V.; Street, J.S.;Krueger, J.A.; Tamura, R.N.; Graffeo, K.A.; and Thieme,M.E. Olanzapine versus haloperidol in the treatment ofschizophrenia and schizoaffective and schizophreniformdisorders: Results of an international collaborative trial.American Journal of Psychiatry, 154:457-465, 1997.
Tollefson, G.D.; Birkett, M.A.; Kiesler, G.M.; and Wood,AJ. Double-blind comparison of olanzapine versus cloza-pine in schizophrenic patients clinically eligible for treat-ment with clozapine. Biological Psychiatry, 49:52-63,2001.
Tran, P.V.; Dellva, M.A.; Tollefson, G.D.; Wentley, A.L.;and Beasley, CM. Oral olanzapine versus oral haloperidolin the maintenance treatment of schizophrenia and relatedpsychoses. British Journal of Psychiatry, 172:499-505,1998.
Weiden, P.; Aquila, R.; and Standard, J. Atypical antipsy-chotic drugs and long-term outcome in schizophrenia.Journal of Clinical Psychiatry, 57(Suppl ll):53-60, 19%.
Wyatt, R.; Henter, I.; Leary, M.; and Taylor, E. An eco-nomic evaluation of schizophrenia—1991. SocialPsychiatry and Psychiatric Epidemiology, 30:196-205,1995.
Acknowledgments
Funding for the project was provided to Research TriangleInstitute by Eli Lilly and Company.
The Authors
Josephine Mauskopf, Ph.D., is Global Head, Health Eco-nomics, RTI Health Solutions, Research Triangle Park,NC; Matthew Muroff, B.S., is Programmer, U.S. Airways,Bethesda, MD; P. Joseph Gibson, Ph.D., is Epidemiolo-gist, USMD Outcomes Research, Eli Lilly & Co., Indi-anapolis, IN; and David L. Grainger, B.Sc, is Director,Corporate Affairs and Health Economics, Eli Lilly PtyAustralia, Sydney, Australia.
635
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article-abstract/28/4/619/1852810 by guest on 05 April 2019