Embed Size (px)
Citation preview

Establishing a Establishing a
Statewide Brain Injury Statewide Brain Injury
ConsortiumConsortium
Daniel Hutton, D.O.Daniel Hutton, D.O.

DisclosuresDisclosures
NoneNone


A Primer on Traumatic A Primer on Traumatic
Brain InjuryBrain Injury

National EpidemiologyNational Epidemiology Traumatic Brain Injury (TBI) is the leading cause of death and disability in Traumatic Brain Injury (TBI) is the leading cause of death and disability in
children and adults from ages 1 to 44.children and adults from ages 1 to 44.
CDC estimates the annual incidence of 1.4 million people in the USCDC estimates the annual incidence of 1.4 million people in the US 50,000 will not survive the trauma50,000 will not survive the trauma
235,000 will be hospitalized235,000 will be hospitalized
1.1 million1.1 million will be treated and released from the ERwill be treated and released from the ER
Men 1.5X greater riskMen 1.5X greater risk
Most common in first three decades of lifeMost common in first three decades of life Although, those over 75 had a 4 fold increase incidence of death related to TBIAlthough, those over 75 had a 4 fold increase incidence of death related to TBI
5.3 million in US alone (2% of population) require assistance with ADLs 5.3 million in US alone (2% of population) require assistance with ADLs secondary to TBIsecondary to TBI 80,00080,000--90,000 added each year due to permanent neurological injury90,000 added each year due to permanent neurological injury
Moderate & severe head injury are associated with a 2.3 and 4.5 times Moderate & severe head injury are associated with a 2.3 and 4.5 times increased risk of Alzheimer’s disease, respectively.increased risk of Alzheimer’s disease, respectively.
Cost of TBICost of TBI $56 Billion$56 Billion per year in direct and indirect costsper year in direct and indirect costs
Alves OL, Bullock R (2001). Excitotoxic damage in traumatic brain injury. in Clark RSB, Kochanek P. Brain injury. Boston: Kluwer Academic Publishers. p. 1.
Crooks CY, Zumsteg JM, Bell KR. Traumatic Brain Injury: A review of practice management and recent advances. Phys Med Rehabil Clin N Am 18 (2007), 681-710.
Langlois, J. ScD, MPH; Rutland-Brown, W. MPH; Wald, M. MLS, MPH; The Epidemiology and Impact of Traumatic Brain Injury: A Brief Overview; Journal of Head
Trauma Rehabilitation, Vol. 21, No. 5, pp. 375378 2006.
MMWR Morb Mortal Wkly Rep. 2007; 56:167-170

National EpidemiologyNational Epidemiology
Falls 28%Falls 28%
Most prevalent 0Most prevalent 0--4 years and >754 years and >75
Motor vehicle 20%Motor vehicle 20%
Most common 15Most common 15--19 years19 years
Struck by object 19%Struck by object 19%
Assault 11%Assault 11%
Bicycle 3%Bicycle 3%
Unknown 9%Unknown 9%

Types and Treatment Types and Treatment
of Traumatic Brain of Traumatic Brain
InjuryInjury

HistoryHistory
Neurosurgical intervention is perhaps one of the Neurosurgical intervention is perhaps one of the
oldest specialtiesoldest specialties
Trepanation performed 5000 BC in EuropeTrepanation performed 5000 BC in Europe
Performed for a multitude of reasons Performed for a multitude of reasons
SpiritsSpirits
EpilepsyEpilepsy
HeadachesHeadaches
OsteomyelitisOsteomyelitis
TraumaTrauma

HistoryHistory
Intracranial PressureIntracranial Pressure
Lundberg 1960Lundberg 1960
Langfitt, Klatzo 1965Langfitt, Klatzo 1965--1967 1967
Cerebral autoregulation and edemaCerebral autoregulation and edema
Rosner and Becker 1984Rosner and Becker 1984
A wavesA waves
Obrist, Bouma, Muizelaar 1986Obrist, Bouma, Muizelaar 1986--19911991
Cerebral ischemia and bloodflow dynamicsCerebral ischemia and bloodflow dynamics
Led to cerebral perfusion pressureLed to cerebral perfusion pressure

HistoryHistory
ClinicalClinical
GCS 1974GCS 1974
Jennett and TeasdaleJennett and Teasdale
Secondary Insults 1977Secondary Insults 1977
Miller and BeckerMiller and Becker
Hypotension 1993Hypotension 1993
ChesnutChesnut

HistoryHistory
ImagingImaging CTCT
4 hour window 19814 hour window 1981
SeeligSeelig
Marshall’s Criteria 1991Marshall’s Criteria 1991
Data CollectionData Collection TCDB 1983TCDB 1983
Monitoring TechniquesMonitoring Techniques SJVOSJVO22 19911991
DeardenDearden
PbOPbO22 20042004
Hemedex 2005Hemedex 2005
JaegerJaeger

Grading the InjuryGrading the Injury

Mild TBIMild TBI
GCS 13GCS 13--1515
Difficult to get true numbers, due to the rarity of admission to Difficult to get true numbers, due to the rarity of admission to hospitalhospital
Recovery is rapidRecovery is rapid 15% will have symptoms for greater than 3 weeks 15% will have symptoms for greater than 3 weeks post concussive post concussive
syndromesyndrome
Spectrum of symptoms Spectrum of symptoms Blurred vision, headache, nausea, vomiting, dizziness, Blurred vision, headache, nausea, vomiting, dizziness, emotional emotional
lability/depression, cognitive dysfunctionlability/depression, cognitive dysfunction
3030--40% have depression or anxiety40% have depression or anxiety
Need for early neurorehabilitationNeed for early neurorehabilitation
Lost productivity from MTBI totaled an estimated $12 billion in Lost productivity from MTBI totaled an estimated $12 billion in the United States in 2000 the United States in 2000

Moderate TBIModerate TBI
GCS 9GCS 9--1212
General FeaturesGeneral Features
Similar pathology to severe head injurySimilar pathology to severe head injury
More common in younger age groupsMore common in younger age groups
“Gray Zone” of treatment“Gray Zone” of treatment
90% able to have functional independence90% able to have functional independence

Severe TBISevere TBI
GCS 3GCS 3--88
Multiple etiologies for hemorrhage typeMultiple etiologies for hemorrhage type
Overwhelming indications for ventriculostomyOverwhelming indications for ventriculostomy
40% mortality40% mortality
Less than 20% have functional independenceLess than 20% have functional independence

Biomechanics and Biochemistry of Biomechanics and Biochemistry of
Traumatic Brain InjuryTraumatic Brain Injury

Mechanism of InjuryMechanism of Injury
BiomechanicsBiomechanics Contact injuries cause focal injuriesContact injuries cause focal injuries
No inertial load No inertial load
“coup” injuries“coup” injuries ContusionsContusions
Skull fractures/EDHSkull fractures/EDH
Translational acceleration injuries Translational acceleration injuries Inertial load is highInertial load is high
“contracoup” injuries“contracoup” injuries
Contusions, ICH, SDHContusions, ICH, SDH
Angular acceleration is a combination of translational and Angular acceleration is a combination of translational and rotational accelerationrotational acceleration Most commonMost common
DAI, et al.DAI, et al.

Mechanism of InjuryMechanism of Injury

Mechanism of InjuryMechanism of Injury
CalciumCalcium
Trauma increase causes activation Trauma increase causes activation of phospholipases Aof phospholipases A2 2 and C, and C, resulting in release of free fatty resulting in release of free fatty acids and diacylglycerol.acids and diacylglycerol.
Free fatty acids may further Free fatty acids may further damage the blood brain barrier damage the blood brain barrier and increase cerebral edema.and increase cerebral edema.
May also affect electron transport May also affect electron transport at the inner membrane of the at the inner membrane of the mitochondria, inhibiting ATP mitochondria, inhibiting ATP production and worsening production and worsening anaerobic metabolism and anaerobic metabolism and increasing intracellular lactate. increasing intracellular lactate.
Dhillon HS, Carman HM, Zhang D, et al: Severity of experimental brain injury on lactate and free fatty acid accumulation and
Evans blue extravasation in the rat cortex and hippocampus. J Neurotrauma 16:455-469, 1999.

Mechanism of InjuryMechanism of Injury
BiochemicalBiochemical
GlutamateGlutamate
Excitatory amino acid Excitatory amino acid (Glutamate and Aspartate)(Glutamate and Aspartate)
Binds NMDA (Binds NMDA (NN--methylmethyl--DD--Aspartate), which normally Aspartate), which normally regulates Naregulates Na++ and Caand Ca2+2+
Regulation is through Regulation is through Magnesium (MgMagnesium (Mg2+2+) binding to ) binding to the receptorthe receptor
Excessive levels of excitatory Excessive levels of excitatory amino acids cause cell death in amino acids cause cell death in two ways:two ways:
Acute increase in NaAcute increase in Na++ and Cland Cl--
cause intracellular edemacause intracellular edema
Increase in intracellular CaIncrease in intracellular Ca2+2+

Mechanism of InjuryMechanism of Injury
Other chemicals implicatedOther chemicals implicated
P53P53 upup--regulationregulation
Free radical damageFree radical damage
Leukotrienes, thromboxane (Arachadonic Acid Leukotrienes, thromboxane (Arachadonic Acid
derivatives)derivatives)
PARPPARP
CalpainCalpain

Management of Traumatic Brain Management of Traumatic Brain
InjuryInjury

Guidelines for the Management Guidelines for the Management
of Severe Traumatic Brain Injuryof Severe Traumatic Brain Injury
33rdrd EditionEditionA Joint Project of theA Joint Project of the
Brai n Trauma Foundat i onBrai n Trauma Foundat i onImprovi ng t he Out come of Brai n Trauma Pat i ent s Worl dwi deImprovi ng t he Out come of Brai n Trauma Pat i ent s Worl dwi de
andand
American Association of Neurological Surgeons (AANS)American Association of Neurological Surgeons (AANS)
Congress of Neurological Surgeons (CNS)Congress of Neurological Surgeons (CNS)
AANS / CNS Joint Section on Neurotrauma and Critical CareAANS / CNS Joint Section on Neurotrauma and Critical Care
New Yor k, 2007New Yor k, 2007

Prehospital Management of TBIPrehospital Management of TBI
Multitude of caregivers Multitude of caregivers FirstFirst--responders, EMTs, RNsresponders, EMTs, RNs
ATLS protocolsATLS protocols ABCDABCD
A and B:A and B: Hypoxia should be avoided Hypoxia should be avoided
and is prognosticand is prognostic
Reliable airway should be Reliable airway should be secured as soon as possiblesecured as soon as possible
CC A single episode of SBP<90 A single episode of SBP<90
doubles mortalitydoubles mortality
Give isotonic fluidsGive isotonic fluids ??Hypertonic??Hypertonic
OO22 satsat MortalityMortality Severe Severe
DisabilityDisability
>90%>90% 14.3%14.3% 4.8%4.8%
6060--90%90% 27.3%27.3% 27.3%27.3%
<60&<60& 50%50% 50%50%

Prehospital Management of TBIPrehospital Management of TBI
ATLS protocol (continued)ATLS protocol (continued) DD
GCSGCS PostresuscitationPostresuscitation GCSGCS
Most widely utilized clinical measurement for TBIMost widely utilized clinical measurement for TBI
GCS of 3GCS of 3--5 has a 70% predictive value of poor outcome5 has a 70% predictive value of poor outcome
Motor component most predictiveMotor component most predictive
Great disparities between medical personnelGreat disparities between medical personnel
40% discrepancy40% discrepancy
PupilsPupils Pupillar asymmetry (Anisicoria) is >1mm difference in diameterPupillar asymmetry (Anisicoria) is >1mm difference in diameter
Examine for orbital trauma, postresuscitationExamine for orbital trauma, postresuscitation
Braakman, et al.Braakman, et al.
Bilateral fixed, dilated pupils has a 91% mortality Bilateral fixed, dilated pupils has a 91% mortality
Unlateral fixed pupil has good outcome in 54%Unlateral fixed pupil has good outcome in 54%
Preponderance of epidural hematomasPreponderance of epidural hematomas
E E (Exposure and other injuries)(Exposure and other injuries) Other injuries….how about the spine?Other injuries….how about the spine?
21% of patients with severe TBI have cervical spine injuries21% of patients with severe TBI have cervical spine injuries
Braakman R, Gelpke G, Hebemma J, et al.: Systemic Selection of Prognostic Features in Patients with Severe Head Injury.
Neurosurg 6: 362-70, 1980.

Neurointensive CareNeurointensive Care

Understanding Neurointensive CareUnderstanding Neurointensive Care
It’s all about oxygen delivery!!!!It’s all about oxygen delivery!!!!
Optimize arterial oxygenationOptimize arterial oxygenation
Optimize Oxygen carrying capabilitiesOptimize Oxygen carrying capabilities
Optimize blood pressureOptimize blood pressure
Understand the forces helping or hindering OUnderstand the forces helping or hindering O2 2
deliverydelivery
MAP/CBF (Hemedex)MAP/CBF (Hemedex)
ICPICP
Checking the end productChecking the end product
SjOSjO22
PbOPbO22

Intracranial PressureIntracranial Pressure
How high is too high?How high is too high?
Marmarou (1991) 1030 severe TBI patients found Marmarou (1991) 1030 severe TBI patients found
that an ICP of 20 greatest predictive threshold for that an ICP of 20 greatest predictive threshold for
outcome at 6 months.outcome at 6 months.
Retanalert (2004) evaluated outcome in patients with Retanalert (2004) evaluated outcome in patients with
ICP of 25 vs. 20 and found no differenceICP of 25 vs. 20 and found no difference
CPP>70, SjOCPP>70, SjO22>54%>54%
Only 27 patientsOnly 27 patients
Marmarou A, Anderson RL, Ward JD, et al: Impact of ICP instability and hypotension on outcome in patients with severe head
trauma.J Neurosurg 1991;75:S159-S166.
Ratanalert SN, Phuepathom N, Saeheng S, et al: ICP threshold in CPP management of severe head injury patients. Surg Neurol
2004;61:429-435.

Cerebral Perfusion PressureCerebral Perfusion Pressure
What is it?What is it?
CPP=MAPCPP=MAP--ICPICP
More emphasized than ICPMore emphasized than ICP--guided treatmentguided treatment
Ties into hypotension as poor outcomeTies into hypotension as poor outcome
Rosner and Daughton (1990)Rosner and Daughton (1990)
CPP>70 had superior outcomesCPP>70 had superior outcomes
Serious complications, including ARDSSerious complications, including ARDS
Rosner MJ, Daughton S. Cerebral perfusion pressure management in head injury. J Trauma 1990;10:151-165.

Cerebral Perfusion PressureCerebral Perfusion Pressure
CPP <50CPP <50--60 associated with worse outcomes60 associated with worse outcomes
Usually confounded by severely elevated ICPUsually confounded by severely elevated ICP
Which is more predictive?Which is more predictive?
CPP (Andrews, 2002)CPP (Andrews, 2002)
Therefore, goal CPP is 60Therefore, goal CPP is 60--9090
Newest monitoringNewest monitoring
Licox (Brain tissue pOLicox (Brain tissue pO22))
Hemedex (Cerebral Blood Flow)Hemedex (Cerebral Blood Flow)
Andrews PJ, Sleeman DH, Statham PF, et al: Predicting recovery in patients suffering from traumatic injury by using admission
variables and physiological data: a comparison between decision tree analysis and logistic regresiion. J Neurosug 2002;97:326-336.

Osmotic TherapyOsmotic Therapy
MannitolMannitol
How does it work?How does it work?
Decreases blood viscosityDecreases blood viscosity
Immediate plasma expansion/reduces hematocritImmediate plasma expansion/reduces hematocrit
Improved rheology (deformability of the RBC) and Improved rheology (deformability of the RBC) and
increases oxygen delivery to injured areasincreases oxygen delivery to injured areas
Osmotic EffectOsmotic Effect
Delayed 15Delayed 15--30 minutes after dose30 minutes after dose
Unpredictable duration of treatment (90minUnpredictable duration of treatment (90min--6hrs)6hrs)
Use with caution in patients with hypotension, sepsis, Use with caution in patients with hypotension, sepsis,
nephrotoxic drugs or those with impaired kidney functionnephrotoxic drugs or those with impaired kidney function

Osmotic TherapyOsmotic Therapy
Mannitol (continued)Mannitol (continued)
How to give it?How to give it? No reliable answerNo reliable answer
Marshall, et al. report a faster infusion has a safer and more Marshall, et al. report a faster infusion has a safer and more reliable effect, and possibly longerreliable effect, and possibly longer 1g/kg1g/kg
Effects become less after multiple (3Effects become less after multiple (3--4) doses4) doses
Does it work every time?Does it work every time? NO!NO!
AutoregulationAutoregulation Muizelaar, et al. found Mannitol is effective in those with intact Muizelaar, et al. found Mannitol is effective in those with intact
autoregulation.autoregulation. Rheological effect possibly more important than osmotic effect.Rheological effect possibly more important than osmotic effect.
Marshall LF, Smith RW, Rauscher LA. Mannitol dose requirements in brain injured patients. J Neurosurg. 1978; 48: 169-172.
Muizelaar JP, Lutz HA, Becker DP. Effect of mannitol on ICP and CBF and correlation with pressure autoregulation in severely head
injured patiens. J Neurosurg. 1984; 61:700-706.

Osmotic TherapyOsmotic TherapyHypertonic SalineHypertonic Saline
How does it work?How does it work? Direct increase of solute load in vasculatureDirect increase of solute load in vasculature
How to give it?How to give it? Multiple formulationsMultiple formulations
3%, 5%, 7.5%, 23.4%3%, 5%, 7.5%, 23.4%
For increased ICPFor increased ICP Bolus over 10Bolus over 10--20 min20 min
Caution with CHFCaution with CHF
Contraindicated as bolus in hyponatremiaContraindicated as bolus in hyponatremia
Battison, et al. evaluated ICP control in severe TBI in a Battison, et al. evaluated ICP control in severe TBI in a randomized controlled trial of Hypertonic Saline vs. Mannitol vs. randomized controlled trial of Hypertonic Saline vs. Mannitol vs. DextranDextran HS at least as effective as Mannitol for controlling ICPHS at least as effective as Mannitol for controlling ICP
Small sample sizeSmall sample size
Battison C, Andrews PJ, Graham C, et al. Randomized, controlled trial of the effect of 20% mannitol solution and a 7.5% saline/6%
dextran solution on increased intracranial pressure after brain injury. Crit Care Med. 2005;33:196-202.

Secondary InjuriesSecondary Injuries

Secondary InjuriesSecondary Injuries
HypoxiaHypoxia
What is it?What is it?
How often does it occur?How often does it occur?
Survey of firstSurvey of first--responders to patients with severe head responders to patients with severe head
injury found preinjury found pre--intubation hypoxia (SaOintubation hypoxia (SaO22<85) occurred <85) occurred
55% of the time55% of the time
Over 50% of the time, hypotension was also present. Over 50% of the time, hypotension was also present.
In those with SaOIn those with SaO22<60% pre<60% pre--intubation, mortality rate intubation, mortality rate
was 50% and all survivors had severe disability. was 50% and all survivors had severe disability.
Stochetti N, Furlan A, Volta F. Hypoxemia and arterial hypotension at the accident scene in severe head injury. J Trauma
1996; 40:764-767.

Secondary InjuriesSecondary Injuries
HypotensionHypotension
Defined as SBP < 90Defined as SBP < 90
Most powerful predictor of poor outcomeMost powerful predictor of poor outcome
Single episode of hypotension doubles the mortality rate.Single episode of hypotension doubles the mortality rate.
Increased frequency and duration of hypotension has also Increased frequency and duration of hypotension has also
been shown to be an independent predictor of poor been shown to be an independent predictor of poor
outcomeoutcome
More focus should be paid to MAP/CPP, CBF, More focus should be paid to MAP/CPP, CBF,
PbOPbO22 to determine adequate perfusionto determine adequate perfusion
Chestnut RF, Marshall LM, Klauber MR, et al. The role of secondary brain injury in determining outcome from severe head
injury. J Trauma 1993; 34:216-222.

Pediatric Head InjuryPediatric Head Injury
General ConceptsGeneral Concepts
Hypotension should, in kind, be avoidedHypotension should, in kind, be avoided
Defined as systolic blood pressure less than the fifth Defined as systolic blood pressure less than the fifth
percentile for age group or signs of shockpercentile for age group or signs of shock
Quick formula: Hypotension= 70 mm Hg + 2(age in years)Quick formula: Hypotension= 70 mm Hg + 2(age in years)
Hypoxia with worsened outcome (PaOHypoxia with worsened outcome (PaO22<65)<65)
Hypotension + Hypoxia is only slightly worse than Hypotension + Hypoxia is only slightly worse than
hypotension alone.hypotension alone.
Mortality as high as 85% in some reportsMortality as high as 85% in some reports

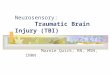
PrognosisPrognosis
GCS scoreGCS score MortalityMortality
33 65%65%
44 45%45%
55 35%35%
66 24%24%
77--1313 1010--15%15%
TBI Mortality
0%
10%
20%
30%
40%
50%
60%
70%
GCS 3 GCS 4 GCS 5 GCS 6 GCS 7-13
GCS
Mo
rtali
ty

Newer NeuromonitoringNewer Neuromonitoring
How do we know if the therapy is effective at How do we know if the therapy is effective at delivering oxygen to the brain?delivering oxygen to the brain? Jugular Venous Saturation Monitoring (SjOJugular Venous Saturation Monitoring (SjO22))
Late 1980s and early 1990s Late 1980s and early 1990s
Gives global cerebral informationGives global cerebral information
Labor intensiveLabor intensive
Brain Tissue Oxygen Monitor (Licox)Brain Tissue Oxygen Monitor (Licox) 20002000--presentpresent
Gives partial pressure of Oxygen in brain parenchymaGives partial pressure of Oxygen in brain parenchyma
Observed levels of ischemiaObserved levels of ischemia
Currently, more of a prognostic tool. However, promising guidelines Currently, more of a prognostic tool. However, promising guidelines are emergingare emerging
Capable of microdialysisCapable of microdialysis
Discernable levels of PBODiscernable levels of PBO22 for ischemia and for ischemia and poorpoor outcomeoutcome

LicoxLicox

HemedexHemedex

Trauma Care in Trauma Care in
OregonOregon

Oregon Trauma SystemOregon Trauma System
1982 1982 –– Dr. Daniel Lowe evaluated 762 trauma cases from 26 Dr. Daniel Lowe evaluated 762 trauma cases from 26 PortlandPortland--area hospitalsarea hospitals He found 25% of the fatalities and 16% of all outcomes were He found 25% of the fatalities and 16% of all outcomes were
“inappropriate” for the severity of the injury“inappropriate” for the severity of the injury
Average response time for trauma surgeon was more than an hourAverage response time for trauma surgeon was more than an hour
1983 1983 –– State Senators Steve Starkovich and John Kitzhaber State Senators Steve Starkovich and John Kitzhaber M.D., introduced Senate Joint Resolution 23, which authorized M.D., introduced Senate Joint Resolution 23, which authorized Oregon Health Services (OHS) to develop a plan for a statewide Oregon Health Services (OHS) to develop a plan for a statewide trauma system. trauma system.
1985 1985 –– Senate bill 147 provided the authority to establish a Senate bill 147 provided the authority to establish a statewide trauma systemstatewide trauma system
1988 1988 –– Oregon Trauma System begins Oregon Trauma System begins

Oregon Trauma SystemOregon Trauma System
It was the first state to develop a system that included It was the first state to develop a system that included
small rural hospitals as well as large urban facilities and small rural hospitals as well as large urban facilities and
that was voluntarily entered into by the hospitals. that was voluntarily entered into by the hospitals.
Oraganized and centralized trauma careOraganized and centralized trauma care
Under the direction of the State Trauma Advisory Under the direction of the State Trauma Advisory
Board (STAB)Board (STAB)
The state is divided by geography and population into The state is divided by geography and population into
nine Area Trauma Advisory Board (ATAB)nine Area Trauma Advisory Board (ATAB)
Report to STABReport to STAB

Oregon Trauma SystemOregon Trauma System

Oregon Trauma SystemOregon Trauma System
Facts about the Oregon Trauma SystemFacts about the Oregon Trauma System
• Since its inception, 133,859 trauma patients have been treated • Since its inception, 133,859 trauma patients have been treated within the Oregon Trauma System, and 21,474 patients have within the Oregon Trauma System, and 21,474 patients have been transferred within the system to a higher level of care. been transferred within the system to a higher level of care.
• Forty• Forty--four hospitals throughout Oregon participate in the four hospitals throughout Oregon participate in the trauma system. trauma system.
• The trauma system includes six hospitals outside of Oregon • The trauma system includes six hospitals outside of Oregon ----four in Washington, one in Idaho and one in California. four in Washington, one in Idaho and one in California.
• Trauma patients are transported by 169 EMS agencies within • Trauma patients are transported by 169 EMS agencies within the trauma system. the trauma system.

Oregon Trauma SystemsOregon Trauma Systems
A few facts about injury prevention A few facts about injury prevention
The unintentional death rate for Oregon children ages The unintentional death rate for Oregon children ages 00--14 has dropped 54 percent since 1996. 14 has dropped 54 percent since 1996.
An Allstate Insurance study ranked the Portland An Allstate Insurance study ranked the Portland metropolitan area as one of the top 10 safest places for metropolitan area as one of the top 10 safest places for teenage drivers. teenage drivers.
Oregon is a leader in the nation for passing safety Oregon is a leader in the nation for passing safety legislation, including primary safety belt use; motorcycle legislation, including primary safety belt use; motorcycle helmet use; bike, skateboard, roller blade and scooter helmet use; bike, skateboard, roller blade and scooter helmet use for children under 16; graduated licensing helmet use for children under 16; graduated licensing laws for teens; and child safety seats and booster seat laws for teens; and child safety seats and booster seat use. use.

Oregon Trauma RegistryOregon Trauma Registry
Data PointsData Points Mechanism of injuryMechanism of injury
fall heightfall height
MVA speedMVA speed
composite description of what happened to the patientcomposite description of what happened to the patient
Response timeResponse time 911 call and scene times911 call and scene times
EMS agency was the first responder/ transporter EMS agency was the first responder/ transporter
Mode of transportMode of transport whether pt. arrived by ground or airwhether pt. arrived by ground or air
Field vitalsField vitals at multiple time pointsat multiple time points
GCS GCS
Airway status Airway status number of intubation attempts (ETCO2 values) number of intubation attempts (ETCO2 values)
other field interventions such as IV, IOother field interventions such as IV, IO and Cand C--Collar.Collar.
Intracranial pressure monitor insertion and tracheostomiesIntracranial pressure monitor insertion and tracheostomies
ICUICU length of staylength of stay
Total length of stayTotal length of stay
Outcome Outcome
DispositionDisposition

Sounds great, but how Sounds great, but how
are we doing?are we doing?

American College of Emergency Physicians American College of Emergency Physicians
2008 Report Card2008 Report Card

American College of Emergency American College of Emergency
Physicians 2008 Report CardPhysicians 2008 Report Card

Traumatic Brain Injury Traumatic Brain Injury
in Oregonin Oregon

Oregon TBI EpidemiologyOregon TBI Epidemiology
There were over 681 deaths in Oregon associated with There were over 681 deaths in Oregon associated with TBI in 2007.TBI in 2007.
Over 3,000 hospitalizations associated with TBI in Over 3,000 hospitalizations associated with TBI in 2007.2007. Males have higher rates of TBI associated death and Males have higher rates of TBI associated death and
hospitalization.hospitalization.
Firearms are the most frequent cause of TBI death.Firearms are the most frequent cause of TBI death.
Falls are the most frequent cause of TBI Falls are the most frequent cause of TBI hospitalization.hospitalization.
TBI was associated with over TBI was associated with over $145 million$145 million in in hospitalization charges in 2007.hospitalization charges in 2007.

Oregon TBI StatisticsOregon TBI Statistics
MortalityMortality The ageThe age--adjusted mortality rate due to TBI declined adjusted mortality rate due to TBI declined
between 1999 and 2006, yet increased in 2007 from between 1999 and 2006, yet increased in 2007 from 20062006 Increased public awarenessIncreased public awareness
Improved access to careImproved access to care
?? Helmet Law?? Helmet Law
The rate in 1999 was 20.0 per 100,000, while the 2007 The rate in 1999 was 20.0 per 100,000, while the 2007 rate was 17.5 per 100,000. rate was 17.5 per 100,000.
In total, there were In total, there were 4,506 deaths4,506 deaths in Oregon associated in Oregon associated with TBI between 1999 and 2007.with TBI between 1999 and 2007.

Oregon TBI StatisticsOregon TBI Statistics

Oregon TBI StatisticsOregon TBI Statistics
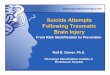
The rate of TBI is higher The rate of TBI is higher
in males than females, in males than females,
typically three times the typically three times the
female rate from year to female rate from year to
year. year.
In 2007, the male rate In 2007, the male rate
was 28.7 per 100,000 was 28.7 per 100,000
compared to the female compared to the female
rate of 7.2 per 100,000rate of 7.2 per 100,000

Oregon TBI StatisticsOregon TBI Statistics
Age and Sex Age and Sex Age distribution of TBI rates shows Age distribution of TBI rates shows
that rates generally increase with age, that rates generally increase with age, and that the highest rates are among and that the highest rates are among males 85 and oldermales 85 and older
The rate for males in this age group is The rate for males in this age group is 137.4 per 100,000 population, while the 137.4 per 100,000 population, while the rate for females in the same age group rate for females in the same age group is 71.0 per 100,000.is 71.0 per 100,000.
The high rate among older men The high rate among older men generally reflects the higher risk and generally reflects the higher risk and mortality due to falls, motor vehicle mortality due to falls, motor vehicle traffic deaths, and firearmstraffic deaths, and firearms
PrePre--existing medical conditions were existing medical conditions were reported for 81.7% of geriatric patientsreported for 81.7% of geriatric patients

Oregon TBI StatisticsOregon TBI Statistics
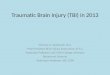
Mechanism of InjuryMechanism of Injury
The leading causes of TBIThe leading causes of TBI--
related death indicate that related death indicate that
firearms were involved in 43% firearms were involved in 43%
29% were the result of MVT 29% were the result of MVT
injuryinjury
17% were due to falls17% were due to falls
10% were due to a variety of 10% were due to a variety of
other causes.other causes.

Oregon TBI StatisticsOregon TBI Statistics
Mechanism of Injury in the ElderlyMechanism of Injury in the Elderly
The most common mechanism wasThe most common mechanism was
ground level fall (31.4%)ground level fall (31.4%)
falls from steps or stairs (19.5%)falls from steps or stairs (19.5%)
increases as the patients’ age increases. increases as the patients’ age increases.
third most common mechanism of injury was a fall from a third most common mechanism of injury was a fall from a
ladder (17.3%), which decreases in frequency as age ladder (17.3%), which decreases in frequency as age
increases. increases.
These three types of falls accounted for 68.2% of the These three types of falls accounted for 68.2% of the
known fall injuries known fall injuries

Oregon TBI StatisticsOregon TBI Statistics
HospitalizationHospitalization
TBITBI--associated associated
hospitalization rates have hospitalization rates have
increased since 1997increased since 1997

Oregon TBI StatisticsOregon TBI Statistics

Oregon TBI StatisticsOregon TBI Statistics

Establishing a Establishing a
Statewide Brain Injury Statewide Brain Injury
ConsortiumConsortium

What is a brain injury consortium?What is a brain injury consortium?
Multiple centers, centralized reportingMultiple centers, centralized reporting
Routine review of trauma statistics and patternsRoutine review of trauma statistics and patterns
Trauma designation/Tertiary referralsTrauma designation/Tertiary referrals
Centralize the careCentralize the care
Directed at extending efficient care to local and rural areasDirected at extending efficient care to local and rural areas
Neurotrauma specialistsNeurotrauma specialists
FullFull--spectrum carespectrum care
PrePre--hospital/transporthospital/transport
Acute careAcute care
RehabilitationRehabilitation

Who is involved?Who is involved?
…..Everyone…..Everyone First RespondersFirst Responders
Emergency DepartmentEmergency Department
Trauma ServiceTrauma Service
NeurosurgeonsNeurosurgeons
IntensivistsIntensivists
NeurologistsNeurologists
PM&RPM&R
PT/OT/STPT/OT/ST
NeuropsychologyNeuropsychology
ICU and floor RNsICU and floor RNs
Many, many moreMany, many more

What are the goals of a brain injury What are the goals of a brain injury
consortium?consortium?
Organized, consistent careOrganized, consistent care
Clear guidelines (algorithms) for decisionClear guidelines (algorithms) for decision--makingmaking
“right patient, right facility, right treatment.”“right patient, right facility, right treatment.”
Timely access to specialty careTimely access to specialty care
Public servicePublic service
Public educationPublic education
Potential for researchPotential for research

What are the resources needed?What are the resources needed?
Multiple sites for care implementationMultiple sites for care implementation
SHRBSHRB
OHSUOHSU
Legacy EmanuelLegacy Emanuel
?Based on ATABs?Based on ATABs
Trauma CoordinatorsTrauma Coordinators
Neurotrauma director & liasonNeurotrauma director & liason
Expansion of data collection points Expansion of data collection points
Cooperation of rehab/longterm care facilitiesCooperation of rehab/longterm care facilities
Funding??Funding??

Are there models in place?Are there models in place?
Current Head injury consortiumsCurrent Head injury consortiums
MassachusettsMassachusetts
Not directed at the acute managementNot directed at the acute management
Focused on Rehab/Long term care Focused on Rehab/Long term care
StateState--based resources for the injuredbased resources for the injured

“No head injury was too “No head injury was too
trivial that it should be trivial that it should be
ignored or too severe that it ignored or too severe that it
be despaired of.”be despaired of.”
Hippocrates, 400 BCHippocrates, 400 BC

Thank youThank you