Embed Size (px)
Citation preview

Essential Health Benefits:Getting Specific, Getting Prepared
Christopher F. KollerHealth Insurance Commissioner, State of RI
NASHP Annual MeetingOctober 3, 2011

Agenda
• What does ACA say about EHB’s?• Let’s set a baseline
– Populations directly affected by EHB definition– Some definitions
• Lessons from IOM Committee• Timelines
• Implications for States: Our Speakers
2

EHB’s in Affordable Care Act
• Intent: Answer the question – What constitutes the health insurance every one is to buy in ACA?
• Relevant Section: 1302
• EHB’s are “to be defined by Secretary of HHS”
3

EHB’s in Affordable Care Act The Statutory Guidance Conflict in 1302:
4
“At least the following categories and the items and services covered with in 1.Ambulatory Patient Services2.Emergency Services3.Hospitalization4.Maternity and newborn care5.Mental Health and Substance Abuse Disorder Services6.Prescription Drugs7.Rehabilitative and habilitative services and devices8.Laboratory Services9.Preventive and wellness services and chronic disease management 10.Pediatric Services, including oral and vision care”
vs
“The Secretary shall ensure that the scope of essential health benefits ..is equal to the scope of benefits under a typical employer plan as determined by the Secretary”

EHB’s in Affordable Care Act “Required Elements for Consideration”
(in Section 1302)
• Appropriate balance between categories• Non discrimination in design and administration of benefits
based on age, disability or life expectancy• Take into account healthcare needs of diverse segments of
population• Ensure the EHB’s are not denied based age, length of life,
present or predicted disability, degree of medical dependency, or quality of life
• Must cover emergency treatment in and out of network• (dental plans and full health plans)• Periodic reviews, reports and updates
5

EHB’s in Affordable Care Act Statutory Strategy
• “The Secretary shall…”• Strategic vagueness and principles (that
appear to conflict in places)• Contrast this to negotiating a list in statute
(Clinton reform strategy)• In hindsight – a little bit of structure and
process in statute would have been helpful…– Federalism?
6

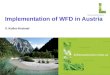
EHB’s: What populations are directly affected by this determination?
Inside the Exchange Outside the Exchange
Individual Market Yes Yes
Small Group Market Yes Yes
Large Group and Self Insured
(N/a) No
Medicaid Only Medicaid Benchmark Plans
Basic Health Plans Yes
7
EHB’s: the floor or the room?
• Employers may always choose to cover more than the EHB package
• But the federal government will only subsidize insurance in the Exchange at the EHB level; and
• The state is fully responsible for the costs of benefits in the Exchange beyond the EHB level for subsidy recipients
• Implications – great pressure on state mandates not in EHB package- Significant influence in EHB definition on market
8

“What’s Covered”:Getting the Language Straight
“Covered Services”
“Benefit Design” “Benefit Administration”
What is it The list of services to be paid for
Terms and conditions of coverage
How those terms and conditions are administered
Examples Usually broad and vague inclusions and very specific exclusions
Medical NecessityCost sharingVisit LimitsNetwork limitationsPrior Authorization
Claims Payment rulesPlan Policies and ProceduresMedical Management guidelinesMedical Necessity determination
Public Oversight Examples
EHB definitionState MandatesMH ParityMedicare and Medicaid
State law – coverage minimumsFederal law – “Precious metals”, external appealsPublic ContractsExchange terms
State Law – UR certification Internal Appeals, prompt paymentFederal Law – External appealsIndustry standards - NCQA
ACA “oppor-tunity”
Standardized, rational, sustainable definitions through EHB process
Standardized oversight through exchanges and Medicaid managed care
QHP certification in exchanges.
9

Institutes of Medicine EHB Committee
• Charge from Assistant Secretary for Planning and Evaluation for HHS:– Recommend to the secretary a process for determining
EHB’s– How to take into account “required elements for
consideration”– Thoughts on medical necessity– Take in public comment on defining and updating EHB’s
• Composition– State officials, industry, academia, providers, consumers
10

IOM Committee: Issues in Defining EHB – from public comment process
1. Balancing generosity and affordability: base line package and changes over time
2. Defining a “typical” employer. 3. Evaluating state mandates 4. Considering specificity and flexibility in EHB guidance. 5. Determining medical necessity 6. Applying evidence and encouraging innovation (in benefit coverage,
design and administration)7. Protecting patients – applying “required elements” 8. Ensuring fair processes—public engagement, independence of
decision makers, and transparency of information used when making benefit decisions were all considered fundamental.
11http://www.iom.edu/Reports/2011/Perspectives-on-Essential-Health-Benefits-Workshop-Report.aspx

EHB Milestones
• Very soon: IOM report to Secretary• Secretary gives draft guidance to states and exchanges• States have to implement
– Commercial Market/ Statutory mandates (2012 legislative session?)
– Medicaid Programs– Exchange Programs (as needed)– Stakeholder education
12

Remainder of Session
• Perspectives for States:–Medicaid Programs–Commercial Markets–Sustainability and Coordination across
Covered Populations
“States should count on a lot of terrifically hard and terribly important work.”
13