Embed Size (px)
Citation preview

Essential 12-Lead Essential 12-Lead
InterpretationInterpretation
MODULE 1MODULE 1

Essential 12-Lead ECG Essential 12-Lead ECG InterpretationInterpretation
• GoalsGoals
– Recognize and localize Recognize and localize AMI on the ECGAMI on the ECG
– Feel comfortable with Feel comfortable with 12-lead interpretation12-lead interpretation

12-Lead ECG12-Lead ECG

12-Lead ECG12-Lead ECG

12-Lead ECG12-Lead ECG

12-Lead ECG12-Lead ECG

12-lead ECG12-lead ECG

12-Lead ECG12-Lead ECG
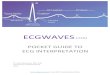
80 milliseconds = 0.08 seconds
0.080 080.0

12-Lead ECG12-Lead ECG

R WaveR Wave

Q WaveQ Wave

S WaveS Wave

QRSQRS
• Q wavesQ waves
– Physiologic Q wavesPhysiologic Q waves
• < .04 sec (40ms)< .04 sec (40ms)
– Pathologic QPathologic Q
• >>.04 sec (40 ms).04 sec (40 ms)

QRSQRS
• Q waveQ wave

QS ComplexQS Complex

J-PointJ-Point

ST SegmentST Segment

PracticePractice
• Find J-points and ST segmentsFind J-points and ST segments

PracticePractice
• Find J-points and ST segmentsFind J-points and ST segments

ST SegmentST Segment
• Compare to TP segmentCompare to TP segment
ST TP

ST Segment AnalysisST Segment Analysis

12-Lead ECG12-Lead ECG
• AMI recognitionAMI recognition
– Two things to knowTwo things to know
• What to look forWhat to look for
• Where you are lookingWhere you are looking

AMI RecognitionAMI Recognition
• What to look forWhat to look for
– ST segment elevation ST segment elevation
• One millimeter or more (one One millimeter or more (one small box)small box)
• Present in two anatomically Present in two anatomically contiguous leadscontiguous leads

ST Segment ElevationST Segment Elevation
• Presumptive Presumptive evidence of AMIevidence of AMI
• Indication for acute Indication for acute reperfusion therapyreperfusion therapy

PracticePractice

Lead “Views”Lead “Views”

Limb Leads Chest Leads
I aVR V1 V4
II aVL V2 V5
III aVF V3 V6
Lead GroupsLead Groups

Lead “Views”Lead “Views”

Inferior WallInferior Wall
• II, III, aVFII, III, aVF
– Left LegLeft Leg
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6

Inferior WallInferior Wall
Inferior Wall
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6

Lateral WallLateral Wall
• I and aVLI and aVL
– Left ArmLeft Arm
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6

Lateral WallLateral Wall
• V5 and V6V5 and V6
– Left lateral chestLeft lateral chest
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6

LateralLateral
Lateral Wall
• I, aVL, V5, V6I, aVL, V5, V6
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6

Anterior WallAnterior Wall
• V3, V4V3, V4
– Left anterior chestLeft anterior chest
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6

Anterior WallAnterior Wall
• V3, V4V3, V4
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6

Septal WallSeptal Wall
• V1, V2V1, V2
• Along sternal bordersAlong sternal borders
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6

SeptalSeptal
• V1,V2V1,V2
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6

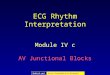
AMI LocalizationAMI Localization
Anterior: Anterior: V3, V4V3, V4Septal: Septal: V1, V2V1, V2Inferior: Inferior: II, III, AVFII, III, AVFLateral:Lateral: I, AVL, V5, V6I, AVL, V5, V6
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6

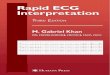
AMI RecognitionAMI Recognition
I Lateral
II Inferior
III Inferior
aVR
aVL Lateral
V1 Septal
aVF Inferior
V2 Septal
V3 Anterior
V4 Anterior
V5 Lateral
V6 Lateral

AMI RecognitionAMI Recognition
• Know what to look forKnow what to look for– ST elevationST elevation
– >> 1mm 1mm
– Two contiguous leadsTwo contiguous leads
• Know where you are lookingKnow where you are looking– Use pocket card as a referenceUse pocket card as a reference
– You will soon have this memorizedYou will soon have this memorized

PracticePractice

PracticePractice

Evolution of AMIEvolution of AMI
• HyperacuteHyperacute

Evolution of AMIEvolution of AMI
• AcuteAcute

Evolution of AMIEvolution of AMI
• AcuteAcute

Evolution of AMIEvolution of AMI
• Age undeterminedAge undetermined

AMI RecognitionAMI Recognition
A normal 12-lead ECG A normal 12-lead ECG
DOES NOTDOES NOT rule out AMI rule out AMI

PracticePractice

PracticePractice

PracticePractice

Reciprocal ChangesReciprocal Changes

Reciprocal ChangesReciprocal Changes
II, III, aVFII, III, aVF I, aVL, V leadsI, aVL, V leads

PracticePractice

PracticePractice

AMI RecognitionAMI Recognition
• Reciprocal changesReciprocal changes
– Not necessary to presume Not necessary to presume infarctioninfarction
– Strong confirming Strong confirming evidence when presentevidence when present

AMI RecognitionAMI Recognition

AMI RecognitionAMI Recognition
• Imitators of infarctImitators of infarct
– LVHLVH
– BBBBBB
– Ventricular beatsVentricular beats
– PericarditisPericarditis
– Early RepolarizationEarly Repolarization
– OthersOthers

SummarySummary
• AMI recognitionAMI recognition
– Know what you are looking forKnow what you are looking for
• 1mm of ST elevation1mm of ST elevation
• Two contiguous leadsTwo contiguous leads
– Know where you are lookingKnow where you are looking
• Positive electrode as an “eye”Positive electrode as an “eye”
• Pocket cardPocket card

SummarySummary
• Reciprocal changesReciprocal changes
– Not necessary to presume Not necessary to presume infarctioninfarction
– Strong confirming Strong confirming evidence when presentevidence when present

SummarySummary
• ST segment elevation is ST segment elevation is presumptive evidence for AMIpresumptive evidence for AMI
• Other conditions may also Other conditions may also cause ST elevationcause ST elevation

SummarySummary
A normal 12-Lead ECG A normal 12-Lead ECG
DOES NOTDOES NOT rule out AMI rule out AMI

ACSACS
AMI is part of a spectrum of
disease know as the
Acute Coronary SyndromesAcute Coronary Syndromes