Embed Size (px)
Citation preview

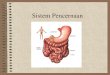
Esophageal varicesFrom Wikipedia, the free encyclopedia
Esophageal varices
Classification and external resources
Gastroscopy image of esophageal varices with prominent cherry-red spots
ICD-10 I 85.
ICD-9 456.0-456.2
DiseasesDB 9177
MedlinePlus 000268
eMedicine med/745 radio/269
MeSH D004932
In medicine (gastroenterology), esophageal varices are extremely dilated sub-mucosal veins in the
lower esophagus. They are most often a consequence of portal hypertension, commonly due to cirrhosis;
patients with esophageal varices have a strong tendency to developbleeding.
Esophageal varices are diagnosed with endoscopy.[1]

Contents
[hide]
1 Pathogenesis
2 Treatment
3 Prevention
4 Histology
5 See also
6 References
7 See also
8 External links
[edit]Pathogenesis
The majority of blood from the esophagus is drained via the esophageal veins, which carry deoxygenated blood
from the esophagus to theazygos vein, which in turn drains directly into the superior vena cava. These veins
have no part in the development of esophageal varices. The remaining blood from the esophagus is drained
into the superficial veins lining the esophageal mucosa, which drain into the coronary vein (left gastric vein),
which in turn drains directly into the portal vein. These superficial veins (normally only approximately 1mm in
diameter) become distended up to 1-2 cm in diameter in association with portal hypertension.
Normal portal pressure is approximately 9 mmHg compared to an inferior vena cava pressure of 2-6 mmHg.
This creates a normal pressure gradient of 3-7 mmHg. If the portal pressure rises above 12mmHg, this gradient
rises to 7-10 mmHg.[2] A gradient greater than 5 mmHg is considered portal hypertension. At gradients greater
than 10 mmHg, blood flow though the hepatic portal system is redirected from the liver into areas with lower
venous pressures. This means that collateral circulation develops in the lower esophagus, abdominal
wall, stomach, and rectum. The small blood vessels in these areas become distended, becoming more thin-
walled, and appear as varicosities. In addition, these vessels are poorly supported by other structures, as they
are not designed for high pressures.
In situations where portal pressures increase, such as with cirrhosis, there is dilation of veins in
the anastomosis, leading to esophageal varices. Splenic vein thrombosis is a rare condition which causes
esophageal varices without a raised portal pressure. Splenectomy can cure the variceal bleeding due to splenic
vein thrombosis. The most common cause of esophageal varices is from aging changes in the vessels.
Varices can also form in other areas of the body, including the stomach (gastric
varices), duodenum (duodenal varices), and rectum (rectal varices). Treatment of these types of varices
may differ.

[edit]Treatment
Esophageal varices seven days post banding, showing ulceration at the site of banding.
In emergency situations, the care is directed at stopping blood loss, maintaining plasma volume, correcting
disorders in coagulation induced by cirrhosis, and appropriate use of antibiotics (usually a quinolone or
ceftriaxone, as infection by gram-negative strains is either concomitant, or a precipitant).
Blood volume resuscitation should be done promptly and with caution. Goal should be hemodynamic stability
and hemoglobin of over 8. Resuscitation of all lost blood leads to increase in portal pressure leading to more
bleeding. Volume resuscitation can also worsen ascites and increase portal pressure. (AASLD guildlines)
Therapeutic endoscopy is considered the mainstay of urgent treatment. Two main therapeutic approaches
exist:
Variceal ligation, or banding
sclerotherapy
In cases of refractory bleeding, balloon tamponade with Sengstaken-Blakemore tube may be necessary,
usually as a bridge to furtherendoscopy or treatment of the underlying cause of bleeding (usually portal
hypertension). Methods of treating the portal hypertension include: transjugular intrahepatic portosystemic
shunt (TIPS), or a distal splenorenal shunt procedure or a liver transplantation.
Nutritional supplementation is not necessary if the patient is not eating for four days or less.[3]
Terlipressin and octreotide (50mcg bolus IV followed by 25-50mcg/h IVF for 1 to 5 days) have also been used.
[4]

[edit]Prevention
Ideally, patients with known varices should receive treatment to reduce their risk of bleeding.[5] The non-
selective β-blockers (e.g., propranolol 10mg PO TID, timolol or nadolol 20mg PO OD) and nitrates
(e.g. isosorbide mononitrate (IMN) 20mg BD to TID) have been evaluated for secondary prophylaxis. Non-
selective β-blockers (but not cardioselective β-blockers likeatenolol) are preferred because they decrease both
cardiac output by β1 blockade and splanchnic blood flow by blocking vasodilating β2 receptors at splanchnic
vasculature. The effectiveness of this treatment has been shown by a number of different studies.[6]
Unfortunately, non-selective β-blockers do not prevent the formation of esophageal varices.[7]
[edit]Histology
Dilated submucosal veins are the most prominent histologic feature of esophageal varices. The expansion of
the submucosa leads to elevation of the mucosa above the surrounding tissue which is apparent during
endoscopy and is a key diagnostic feature. Evidence of recent variceal hemorrhage includes necrosis and
ulceration of the mucosa. Evidence of past variceal hemorhage includes inflammation and venous thrombosis.
Pathophysiology
The esophagus is more vulnerable than the rest of the alimentary tract due to the lack of a serosal layer, which provides stability through elastin and collagen fibers. Perforation may be due to several mechanisms, including direct piercing, shearing along the longitudinal axis, bursting from radial forces, and thinning from necrosis of the esophageal wall.
Iatrogenic injury through esophageal instrumentation is the leading cause of perforation by either piercing or shearing and may be due to any number of procedures, especially endoscopy and dilatation of strictures. Such tears often occur near the pharyngoesophageal junction where the wall is weakest. Because the esophagus is surrounded by loose stromal connective tissue, the infectious and inflammatory response can disseminate easily to nearby vital organs, thereby making the esophageal perforation a medical emergency and increasing the likelihood of serious sequelae. Underlying esophageal disease (tumor, stricture) predisposes toward perforation with instrumentation, which often occurs distal to the affected area. Perforation during surgery most often occurs in the abdominal esophagus.
Spontaneous esophageal rupture (Boerhaave syndrome) occurs secondary to a sudden increase in intraluminal pressures, usually due to violent vomiting or retching, and often follows heavy food and alcohol intake. In more than 90% of cases, perforation occurs in the lower third of the esophagus; most frequently, the tear is in the left posterolateral region (90%) and may extend superiorly. The predilection for left-side perforation is due to the lack of adjacent supporting structures, thinning of the musculature in the lower esophagus, and anterior angulation of the esophagus at the left diaphragmatic crus. Fifty

percent of ruptures occur in patients with gastroesophageal reflux disease , suggesting that ease of pressure transfer from the abdominal to thoracic esophagus may facilitate rupture.
Shearing forces due to rapid increases in intragastric pressure against a closed pylorus result in a Mallory-Weiss tear (MWT). These longitudinal mucosal lacerations occur most commonly at the gastroesophageal junction or gastric cardia, especially if a hiatal hernia is present, and often present with hematemesis. Ultimately, these tears can perforate if the pressure increases are unrelieved. Further discussion of MWTs is reserved for another section.
The cervical esophagus is the most common site of perforation by several other mechanisms as well, particularly in the region of the pyriform sinus. Trauma, almost uniformly penetrating, shows an affinity for the upper esophagus, while toxic ingestions and foreign bodies can directly damage the cervical esophagus or become lodged and cause insidious erosion of the muscle wall.
Frequency
United States
Boerhaave syndrome is rare, accounting for 15% of all cases of esophageal perforation.
Iatrogenic causes account for 50-75% of esophageal perforations. The actual incidence depends on the procedure; rigid endoscopy carries a perforation rate 0.1-0.4%, while that of flexible endoscopy varies from 0.01-0.06%. Rates increase quickly when interventions are undertaken, such as pneumatic balloon dilatation in achalasia (2-6%) or any procedure involving strictures secondary to radiation or tumor (10%). Furthermore, the rate of perforation is increased in the presence of a large hiatal hernia or esophageal diverticula.
Penetrating trauma to the neck (2-9%), thinning of esophageal membrane secondary to variceal sclerotherapy (1-3%), and foreign body or toxic ingestions (5-15%) make up the bulk of the remaining causes.








![Small Esophageal Varices in Patients with Cirrhosis—Should ... · Varices of medium/large size (>5-mm diameter), or small varices with red spot signs [3†]. According to the](https://img.pdfslide.us/doc/110x75/5fa0286b8b7f711ce374a04d/small-esophageal-varices-in-patients-with-cirrhosisashould-varices-of-mediumlarge.jpg)