Embed Size (px)
Citation preview

�������� ����� ��
Esophageal button battery ingestions: Decreasing time to operative interven-tion by level I trauma activation
Robert T. Russell, Russell L. Griffin, Elizabeth Weinstein, Deborah F.Billmire
PII: S0022-3468(14)00062-1DOI: doi: 10.1016/j.jpedsurg.2014.01.050Reference: YJPSU 56682
To appear in: Journal of Pediatric Surgery
Received date: 15 October 2013Revised date: 27 January 2014Accepted date: 29 January 2014
Please cite this article as: Russell Robert T., Griffin Russell L., Weinstein Elizabeth,Billmire Deborah F., Esophageal button battery ingestions: Decreasing time to opera-tive intervention by level I trauma activation, Journal of Pediatric Surgery (2014), doi:10.1016/j.jpedsurg.2014.01.050
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Esophageal Button Battery Ingestions: decreasing time to operative intervention by level I
trauma activation
Robert T. Russell, MD, MPH1, Russell L. Griffin, PhD2, Elizabeth Weinstein, MD,3 and Deborah
F. Billmire, MD4
Affiliations: 1University of Alabama at Birmingham, Division of Pediatric Surgery, Children’s
of Alabama, Birmingham, AL; 2University of Alabama at Birmingham, School of Public Health,
Department of Epidemiology, Birmingham, AL; 3Division of Emergency Medicine, JW Riley
Hospital for Children, Indianapolis, IN; 4Division of Pediatric Surgery, JW Riley Hospital for
Children, Indianapolis, IN
Address Correspondence to: Robert T. Russell, Division of Pediatric Surgery, Children’s of
Alabama, 1600 7th Avenue South, Lowder Building Suite 300, Birmingham, AL 35233,
[[email protected]], 205-638-5339, Fax 205-975-4972
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Abstract
Purpose: The incidence of button battery ingestions is increasing and injury due to esophageal
impaction begins within minutes of exposure. We changed our management algorithm for
suspected button battery ingestions with intent to reduce time to evaluation and operative
removal.
Methods: A retrospective study was performed to identify and evaluate time to treatment and
outcome for all esophageal button battery ingestions presenting to a major children’s hospital
emergency room from February 1, 2010 through February 1, 2012. During the first year,
standard emergency room triage (ST) was used. During the second year, the triage protocol was
changed and Trauma I triage (TT) was used.
Results: 24 children had suspected button battery ingestions with 11 having esophageal
impaction. One esophageal impaction was due to 2 stacked coins. Time from arrival in
emergency room to battery removal was 183 minutes in ST group (n=4) and 33 minutes in TT
group (n=7) (p=0.04). One patient in ST developed a tracheoesophageal fistula. There were no
complications in the TT group.
Conclusions: The use of Trauma 1 activations for suspected button battery ingestions has led to
more expedient evaluation and shortened time to removal of impacted esophageal batteries.
Key Words: button battery, level I trauma, esophagus
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Introduction
There are several recent reports of button battery related esophageal injuries, including
erosive esophagitis, tracheoesophageal fistula, hemorrhagic complications, and even death.1-4
From 1990 to 2009, there were an estimated 66,000 battery related emergency department (ED)
visits in the United States in children < 18 years of age. The number and rate of visits increased
significantly during the twenty-year time period, which was due to a significant increase in
battery-related ED visits among children ≤ 5 years.5 A report by Litovitz et al in 2010 also
suggests that fatal and severe button battery ingestions are increasing, and this trend has been
associated with the growing utilization of 3 volt, 20-mm lithium button batteries.6
Recommendations from this report suggest removal of the button battery from the esophagus
within 2 hours from ingestion to limit tissue exposure. Due to the greater voltage and current of
lithium cells, longer impactions can result in more severe tissue damage leading to further
complications. Although time to presentation and duration of procedure are not subject to
control, time from presentation to operative removal may be improved with a standardized
approach. We changed our management algorithm for suspected button battery ingestions with
intent to reduce time to evaluation and operative removal. The goal of this study was to examine
the time to evaluation/treatment and outcomes of patients that were evaluated at our facility one
year prior to and one year after the change of button battery ingestion management algorithm.
Methods
Children presenting to a free standing children’s hospital with a level 1 trauma center
who had known or suspected history of button battery ingestion were included. Known patients
included those transferred from an outside facility with radiographic documentation of battery
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
ingestion. Suspected patients included those who presented to the triage desk from home with a
history of possible ingestion. Prior to February 1, 2010, standard triage (ST) was utilized for
initial evaluation of a suspected button battery ingestion in the emergency room. This involved
standard emergency room registration, initial nursing triage for a brief history of the presenting
problem and medical history followed by triage for physician evaluation. Confirmation of button
battery ingestion prompted immediate consultation with a surgical endoscopist (pediatric
surgeon, pediatric gastroenterologist, or pediatric ENT). After February 1, 2010, Trauma I triage
activation (TT) was utilized to facilitate more expedient evaluation of patients with suspected
button battery ingestion. TT entails immediate notification of the pediatric trauma team, the
anesthesia team, the radiology technician, and the operating room charge nurse of the arrival of
trauma patients to the emergency department. This allows immediate response of the pediatric
trauma surgeon and immediate confirmation of presence and site of battery by imaging.
Availability of an operating room for potential operative intervention is also secured. After IRB
approval, a retrospective chart review was performed to identify all button battery ingestions
from February 1, 2010 through February 1, 2012. To ensure complete capture of button battery
ingestions, we searched the medical records utilizing Current Procedural Terminology (CPT)
codes for endoscopic retrieval of foreign body (43215, 43247). We reviewed each chart
associated with these CPT codes and eliminated all foreign bodies that were not suspected button
batteries. We then collected and analyzed data including type of battery or foreign body,
location of impaction, time of ingestion, time to first medical attention, time to arrival to our
facility, time to operative intervention, method of removal, operative findings, post-operative
complications, and follow up.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Cases were divided into two groups for evaluation—standard triage (ST) and Trauma I
triage (TT). To compare the two management algorithms, we calculated the time from arrival to
our facility to the time of arrival to the operating room as a measure to measure improvement in
treatment times. Demographic and clinical characteristics of children treated were compared
between time periods using a Fisher’s exact chi-square test and Wilcoxon rank-sums test for
categorical and continuous variables, respectively.
Results
From February 1, 2010 to January 31, 2012, there were a total of twenty-one patients
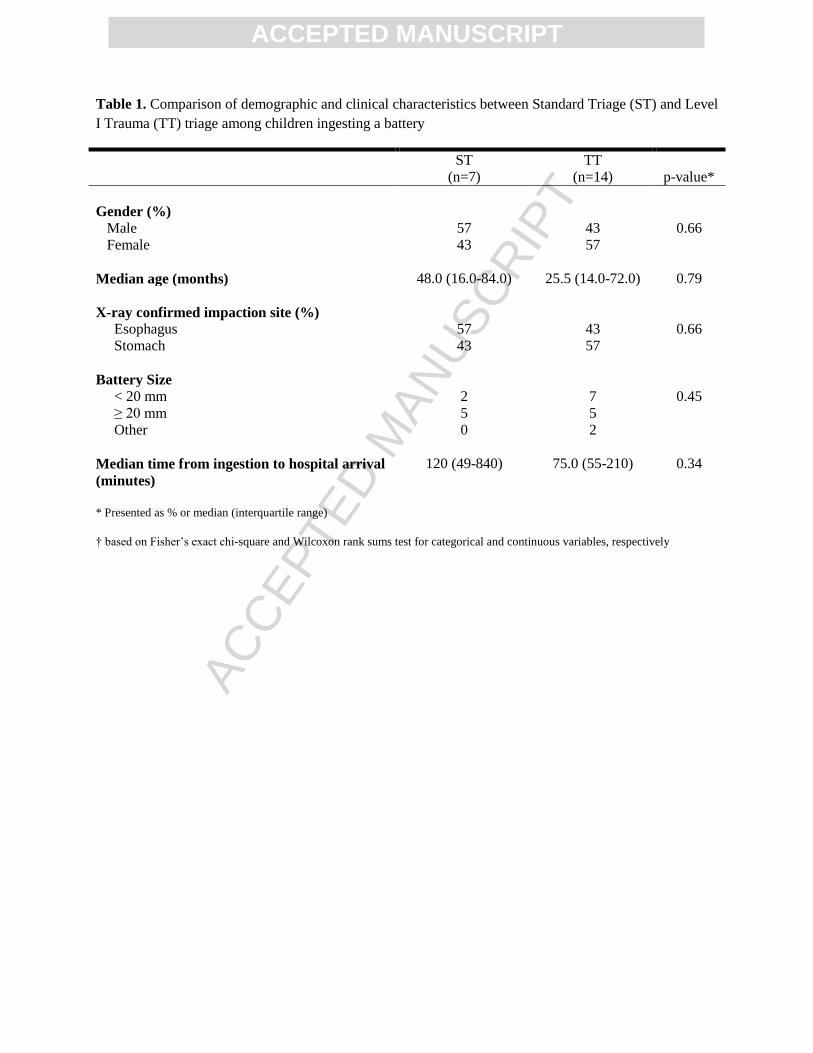
requiring surgical evaluation for button battery ingestion. Table 1 demonstrates the distribution
of all patients during the time periods of standard and trauma triage. There was no difference in
the median age, impaction site, battery type, or median time from suspected ingestion to hospital
arrival between groups. The most common presenting symptoms were vomiting, drooling, or
dysphagia, however this was in a minority of the population. There was a significant difference
in median time from arrival to the operating room between the ST and TT group (169 vs. 50
minutes; p=0.04) One of the ST patients returned seven days later with acute symptoms from a
developing acquired tracheoesophageal fistula (TEF) at the level of the right mainstem bronchus
secondary to battery impaction. He was readmitted to the hospital one week after battery
retrieval and was hospitalized for a total of 53 days with successful non-operative management
of the acquired TEF. None of the patients in the TT group developed complications secondary to
battery ingestion.
Since the most devastating outcomes occur in those patients with impacted esophageal
button batteries, we chose to focus on those patients in with a foreign body impacted in the
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
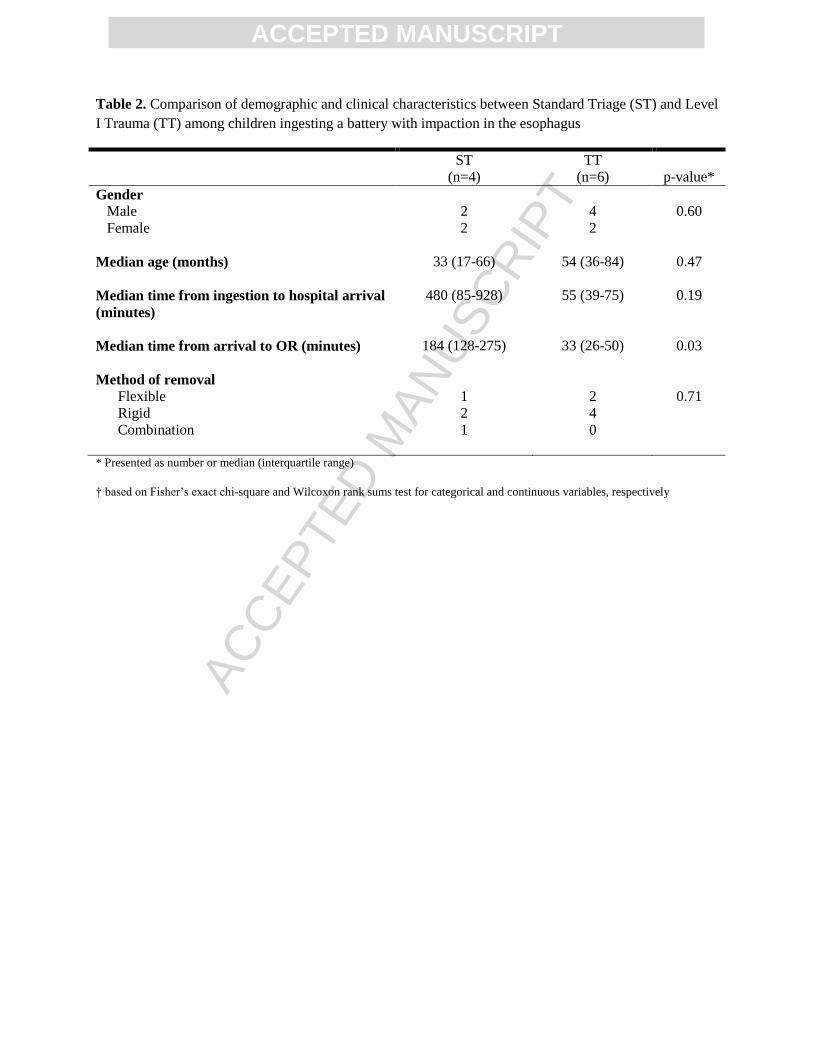
esophagus. This further limited our groups to 4 ST patients and 6 TT patients. However
between these two groups, there was no difference between time periods in regards to gender,
age, impaction site, and time from battery ingestion to hospital arrival (Table 2). 80% of the
impacted objects were 20 mm button batteries. One patient had a 12 mm button battery lodge at
the gastroesophageal junction requiring removal and one patient had two stacked coins removed
from the upper esophagus. There was no difference in retrieval methods of impacted batteries
between time periods. One patient required a combination of flexible and rigid esophagoscopy,
but all other patients were managed with either flexible or rigid esophagoscopy depending on
surgeon preference. The median time from hospital arrival to the OR was significantly decreased
by over two hours in the TT group (median, 184 vs. 33, p=0.04).
Discussion
Esophageal button battery impaction can lead to surrounding tissue injury and further
complications in as little as two hours. These injuries are almost exclusively due to 20mm
lithium batteries as batteries 12 mm and less are easily passed, and even 20 mm batteries will not
cause injury if they are able to reach the stomach without impaction. Several mechanisms
leading to tissue damage have been proposed: (1) generation of an external current causing
electrolysis of tissue fluids when placed in a conductive medium; (2) liquefactive necrosis
secondary to leakage of alkaline electrolyte; and (3) tissue necrosis from pressure phenomenon.7
The first mechanism is the most important for the most dangerous and more prevalent 20-mm
lithium batteries. These batteries do not contain an alkaline electrolyte, but they do generate
more current due to their increased voltage and capacitance in comparison with other button
batteries. This diagnosis is not always made by history as the symptoms of ingestion and the
age of the population leads to vague symptoms that may lead to a delay in diagnosis. A chest
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
and/or abdominal radiograph are simple diagnostic modalities to confirm diagnosis. Endoscopic
removal from the esophagus by esophagoscopy with visualization of the impaction site should be
performed. Airway evaluation should be considered when esophageal injury is identified or
when the negative pole of the battery faces anteriorly in the esophagus. Complications from
ingestion and esophageal impaction include esophageal stricture, esophageal perforation, vocal
cord paralysis, tracheoesophageal fistula, spondylodicitis, and aortoesophageal fistula.1, 2, 6, 7
Recent literature has highlighted the increasing epidemiologic trends and hazards
associated with button battery ingestions. Sharpe et al. detailed the significant increase in
national battery-related emergency department (ED) visits from 1990 to 2009. There were
almost 66,000 battery-related ED visits in children < 18 years of age in the United States during
this time period. The number and rate of these visits increased significantly during this time
period and the increase was primarily seen in the group of children ≤ 5 years of age.5 Litovitz et
al. reported a 6.7-fold increase in the percentage of button battery ingestions resulting in severe
or fatal outcomes from 1985 to 2009. Outcomes were significantly worse for children who
ingested large-diameter lithium cells (≥ 20mm) and in those children younger than 4 years.6 This
report led to a revised National Battery Ingestion Hotline guideline for management of button
battery ingestions. (www.poison.org/battery/guideline.asp) These guidelines suggest immediate
endoscopic removal of batteries lodged within the esophagus and careful assessment of the
mucosa for the depth and extent of tissue damage. These studies detail important epidemiologic
trends showing increasing number of visits related to button batteries and increasing serious
outcomes related to these ingestions. This highlights the importance of this study to assess an
effort at a “quality improvement” effort to improve evaluation and treatment times in an attempt
to reduce the risk of serious outcomes.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
A Level I trauma center provides the highest level of surgical care to trauma patients. It
has a full range of specialists and resources available 24 hours a day and admits a minimum
required annual volume of severely injured patients. Level I trauma centers utilize specific triage
criteria to designate different levels of expected severity of injury based on mechanism of injury
and certain physiologic criteria. At our center, the trauma activations are categorized in a two-
tiered system: Level I (severe mechanism, penetrating injury, and/or significantly altered
physiologic criteria) activations, which require an immediate full trauma team response, and
Level II activations, which are initially managed and appropriately triaged based on injuries by
emergency department physicians. We utilized this already existing mechanism of Level I
trauma activation by adding suspected button battery ingestion as one of the Level I triage
criteria to require immediate trauma team evaluation in the emergency department. Those
patients coming from another facility with a known impaction have the team on standby before
arrival. Those patients presenting to the triage desk are immediately placed into a room. The
radiology technician is already present and prompt imaging confirms presence and site of
impaction without need for transport to the radiology department. The operating room nurse
holds a room available until cleared by the trauma surgeon. Although this did result in
overtriage for those found to have no ingestion or a gastric battery, no patient with an esophageal
battery had delay in diagnosis or treatment in our facility. This algorithm change resulted in a
significant decrease in time from presentation to the ED to time to the OR.
Interestingly, however, during the same time frame we noted two trends: an overall
increase in incidence of ingestion, and a decrease in time from suspected ingestion to time to
presentation in the ED. We hypothesize that this decrease in patient response time may be
secondary to increased public awareness and outreach, both nationally and locally. Nationally,
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
efforts by organizations such as the Button Battery Task Force, the National Capitol Poison
Center, and the Consumer Product Safety Commission were ongoing during this time.
Improving product safety standards, voluntary industry efforts, including child resistant
packaging and warning label stickers, and legislative efforts are ongoing to aid in reducing
potential exposures and the hazard related to these batteries.7 During the final portion of our
post-algorithm change time frame, local education and outreach regarding button battery dangers
was conducted by our EMS agency, our state Emergency Medical Services for Children
program, and a regional healthcare coalition. Specifically, these efforts consisted of news
releases, newsletters, and social media blitzes. These modalities were further enhanced by local
media coverage including local news and radio and web distribution. However, though we
believe that this outreach has had impact, the time frame of this outreach is insufficient to
explain the change in response time. Finally, regional EMS Medical direction has subsequently
developed a destination protocol directing transport for known or suspected button battery
ingestion to a facility prepared for emergent removal and can decrease the time spent due to
interfacility transfer.
This study evaluates the importance of improving the efficiency of evaluation and
management of suspected esophageal button battery ingestions at the hospital level. Since this is
a time-sensitive issue, we believed that immediate activation of the trauma team and operating
room staff would lead to improved times to removal of the esophageal foreign body. We have
demonstrated that utilization of this system has led to a more expedient evaluation and operative
removal of suspected esophageal button batteries. Due to our small numbers and low
complication rate in both groups, we were not able to demonstrate a difference in complications
between our two groups.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
This study has several limitations. This is a retrospective study from a single institution
including a small population of patients. We must recognize the unmeasurable “study effect”
that parallels any new change in algorithm and focuses attention on this problem. However, this
also reinforces education of all personnel involved in the process as to the importance and time-
sensitive nature of this problem. The change in management instituted in this study may not be
feasible at all pediatric hospitals depending on the immediate availability of pediatric surgeons,
anesthesia, and operating room staff. Classification of these ingestions as Level I trauma
activations led to a more expedient evaluation prompting quicker transitions to the operating
room for those requiring urgent endoscopy for battery removal. In 2012 the 11th
International
Conference for Injury Prevention and Safety Promotion highlighted the increasing public health
issue surrounding button batteries and the risk for significant and irreversible injury occurring in
as little as 2 hours post ingestion. Participants including the US Consumer Product
Administration and SafeKids international called for a “multi-pronged” solution, including
industry changes and design safety, physician recognition and response and public awareness
campaigns. Our trauma activation algorithm change, in conjunction with community based
outreach and education initiatives and changes in EMS destination protocols represent a novel
and effective response to this growing public health hazard.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
References
1. Gordon AC, Gough MH. Oesophageal perforation after button battery ingestion. Ann R Coll
Surg Engl. Sep 1993;75(5):362-364.
2. Samad L, Ali M, Ramzi H. Button battery ingestion: hazards of esophageal impaction. J
Pediatr Surg. Oct 1999;34(10):1527-1531.
3. Slamon NB, Hertzog JH, Penfil SH, Raphaely RC, Pizarro C, Derby CD. An unusual case of
button battery-induced traumatic tracheoesophageal fistula. Pediatr Emerg Care. May
2008;24(5):313-316.
4. Banerjee R, Rao GV, Sriram PV, Pavan Reddy KS, Reddy DN. Button battery ingestion.
Indian J Pediatr. Feb 2005;72(2):173-174.
5. Sharpe SJ, Rochette LM, Smith GA. Pediatric battery-related emergency department visits in
the United States, 1990-2009. Pediatrics. Jun 2012;129(6):1111-1117.
6. Litovitz T, Whitaker N, Clark L, White NC, Marsolek M. Emerging battery-ingestion hazard:
clinical implications. Pediatrics. Jun 2010;125(6):1168-1177.
7. Jatana KR, Litovitz T, Reilly JS, Koltai PJ, Rider G, Jacobs IN. Pediatric button battery
injuries: 2013 task force update. Int J Pediatr Otorhinolaryngol. Sep 2013;77(9):1392-1399.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Table 1. Comparison of demographic and clinical characteristics between Standard Triage (ST) and Level
I Trauma (TT) triage among children ingesting a battery
ST
(n=7)
TT
(n=14) p-value*
Gender (%)
Male 57 43 0.66
Female 43 57
Median age (months) 48.0 (16.0-84.0) 25.5 (14.0-72.0) 0.79
X-ray confirmed impaction site (%)
Esophagus
Stomach
57
43
43
57
0.66
Battery Size
< 20 mm
≥ 20 mm
Other
2
5
0
7
5
2
0.45
Median time from ingestion to hospital arrival
(minutes)
120 (49-840) 75.0 (55-210) 0.34
* Presented as % or median (interquartile range)
† based on Fisher’s exact chi-square and Wilcoxon rank sums test for categorical and continuous variables, respectively
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Table 2. Comparison of demographic and clinical characteristics between Standard Triage (ST) and Level
I Trauma (TT) among children ingesting a battery with impaction in the esophagus
ST
(n=4)
TT
(n=6) p-value*
Gender
Male 2 4 0.60
Female 2 2
Median age (months) 33 (17-66) 54 (36-84) 0.47
Median time from ingestion to hospital arrival
(minutes)
480 (85-928) 55 (39-75) 0.19
Median time from arrival to OR (minutes)
184 (128-275) 33 (26-50) 0.03
Method of removal
Flexible 1 2 0.71
Rigid 2 4
Combination 1 0
* Presented as number or median (interquartile range)
† based on Fisher’s exact chi-square and Wilcoxon rank sums test for categorical and continuous variables, respectively