-
ESMO PRECEPTORSHIP PROGRAMME BREAST CANCERScreening
Name
Kristina Lång
Date 9 Nov 2018
-
DISCLOSURE OF INTEREST
Disclosure: • Received speaker’s fee and travel grant from
Siemens
• Siemens Scientific Advisory Board (2017)
• Research collaboration with Philips
-
The aim of screening
• Detect a disease early in an asymptomatic stage
• Give early intervention and management
• Reduce the impact of a disease that has already occurred
(secondary prevention)
Outcome is better because of early detection and
intervention
Kristina Lång, ESMO 9 Nov 2018
-
Guidelines on the principles and practice of screeningaccording
to Wilson and Jungner (WHO 1968)
The disease
• Severe
• High prevalence in a preclinical stage
• The natural history of the disease known
• Long period between between first sign and manifest
disease
• Acceptable sensitivity and specificity
• Simple and cheap
• Safe and acceptable
• Possible treatment
• Effective, safe and acceptable
The test
The treatment
Kristina Lång, ESMO 9 Nov 2018
-
• New York HIP (1963)
• Malmö I and II (1976)
• Swedish Two County (1977)
• Edinburgh (1978)
• Canada I and II (1980)
• Stockholm (1981)
• Göteborg (1982)
• UK Age trial (1991)
www.mskcc.org
5
Early randomized controlled trials
Kristina Lång, ESMO 9 Nov 2018
-
Mammography screening in EUInitiation of a population based
screening programmes
Sweden 1986
Finland 1987
UK 1988
The Netherlands 1988
Ireland 2000
Belgium 2001
Balticum 2002–2008
Hungary 2002
Germany 2005
Polen 2006
Malta 2008
Slovenia 2008
Altobelli and Lattanzi IJO 2014
Participation rate of
>70% acceptable
Kristina Lång, ESMO 9 Nov 2018
-
• Two-view mammography
• Target age 50–69
• Biennial screening intervals
• Double reading
mediolateral oblique craniocaudal
Typical mammography screening programme
Sweden: Age 40–74 with 1.5–2 year interval
UK: Age 50–70 with 3 year interval
Kristina Lång, ESMO 9 Nov 2018
-
The balance in screening
• Reduction in mortality
• Reduced suffering from metastatic disease
• Breast conserving surgery
• Feeling of security
• False positives
• Overdiagnosis
• Anxiety
• False negatives = false sense of security
Benefits Harms
8Kristina Lång, ESMO 9 Nov 2018
-
Reduction in breast cancer deaths
• In age group 40–49: 16% relative risk reduction
• 2057 women needs to be screened regularly to prevent one
breast cancer death
• The effect of screening is lower in younger women:
• In age group 50–74: 23% relative risk reduction
• 760 women needs to be screened regularly to prevent one breast
cancer death
- Lower prevalence
- Lower sensitivity of mammography (dense breasts)
Gotzsche, PC, Nielsen, M. Screening for breast cancer with
mammography. Cochrane database of systematic reviews (2011)
Nationella riktlinjer för screening, Socialstyrelsen (2017)
0.049% absolute risk reduction
0.13% absolute risk reduction • In Europe: 50–69 år
IARC Working Group for Screening. NEJM (2015)
Benefit of screening
9Kristina Lång, ESMO 9 Nov 2018
-
False positives
• 80–90% of recalled women are false positives
• Breast cancer-specific psychological distress that may endure
for up to 3 years
• Recall rates: – prevalence screening
-
Overdiagnosis
• The detection of a cancer that would never have been found
were it not for the screening test
• Two forms of overdiagnoses: 1. The detection of a lesion with
essentially no malignant potential
2. The detection of a lesion that is slow-growing enough that
the individual will go on to die of a competing cause of death
first
• Women become cancer patients with psychological and treatment
side effects
• A breast cancer diagnosis is associated with comorbidity:
increased risk of dying of various causes (pulmonary circulation,
suicide, heart failure, and gastrointestinal disease)
The consequences:
Riihimäki et al. Ann Oncol (2012)
Harm of screening
Kristina Lång, ESMO 9 Nov 2018
-
•
-
• Review of RCTs
• Screening is likely to reduce breast cancer mortality by about
15%
• But 30% overdiagnosis and overtreatment
Cochrane Database of Systematic Reviews 2011
• 2000 invited women screened for 10 years: 1 BC death
prevented
10 women overdiagnosed and overtreated
200 women with FPs
13Kristina Lång, ESMO 9 Nov 2018
-
• Review of the early mammography RCTs
• Reduction of breast cancer mortality about 20% (invited)
• Overdiagnosis rate: 11% (invited), 19% (attending)
• If 10,000 women aged 50 are invited to screening for 20
years:
1 breast cancer death prevented 3 women overdiagnosed and
overtreated
43 breast cancer deaths prevented
129 women overdiagnosed and overtreated
14Kristina Lång, ESMO 9 Nov 2018
-
Can we reduce overdiagnosis and overtreatment?
• Potential overdiagnosed cancer: low-grade DCIS and invasiv
tubular cancer?
• Detection of DCIS has increased with screening (10–20%), 90%
of DCIS do probably not evolve into invasive cancer
• Watchful waiting of low-grade DCIS vs. treatment (ongoing
RCTs, The LORIS trial, the LORD trial mfl.)
Evans A and Vinnivombe S. Breast (2017)Francis A, et al. Clin
Oncol (2015)Elshof LE, et al. Eur J Cancer. (2015)
15Kristina Lång, ESMO 9 Nov 2018
-
Interval cancer
16
• Symptomatic cancers diagnosed in the interval between two
screening examinations
• ”False” or ”true” interval cancers
• More aggressive with poorer prognosis
• Strong indicator on how successful your screening programme
is
Kristina Lång, ESMO 9 Nov 2018
-
S C R E E N I N G B T
S C R E E N I N G D MS C R E E N I N G D M
2 0 1 3 2 0 1 4 2 0 1 4
Söker för knöl 3 månader senare
PAD: 12 mm IDC trippel negative G3
17
3 months later lump in the
breast
-
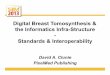
1000 screened women
30 recalls no recalls
true positives
false positives
true negatives
false negatives
clinically relevant cancers
overdiagnosed cancers
970
5 25 969
1 4
1
≈1/3 of all cancers are missed in screening
partly due to the limitation of the mammographic
technique
Birdwell et al. Radiology (2001)
Typical outcome of screening
Kristina Lång, ESMO 9 Nov 2018
-
Tomosynthesis in screening
• Caumo F, et al. Digital Breast Tomosynthesis with Synthesized
Two-Dimensional Images versus Full-Field Digital Mammography for
Population Screening: Outcomes from the Verona Screening Program.
Radiology (2018)
• Hofvind S, et al. Digital Breast Tomosynthesis and Synthetic
2D Mammography versus Digital Mammography: Evaluation in a
Population-based Screening Program. Radiology (2018)
• Skaane P, et al. Performance of breast cancer screening using
digital breast tomosynthesis: results from the prospective
population-based Oslo Tomosynthesis Screening Trial. Breast Cancer
Research and Treatment. (2017)
• Bernardi D, et al. Breast cancer screening with tomosynthesis
(3D mammography) with acquired or synthetic 2D mammography compared
with 2D mammography alone (STORM-2): a population-based prospective
study. Lancet Oncol. (2016)
• Lång K, et al. Performance of one-view breast tomosynthesis as
a stand-alone breast cancer screening modality: results from the
Malmö Breast Tomosynthesis Screening Trial, a population-based
study. Eur. Radiol. (2016)
• Skaane P, et al. Prospective trial comparing full-field
digital mammography (FFDM) versus combined FFDM and tomosynthesis
in a population-based screening programme using independent double
reading with arbitration. Eur. Radiol. (2013)
• Skaane P, et al. Comparison of Digital Mammography Alone and
Digital Mammography Plus Tomosynthesis in a Population-based
Screening Program. Radiology (2013)
• Ciatto S, et al. Integration of 3D digital mammography with
tomosynthesis for population breast-cancer screening (STORM): a
prospective comparison study. Lancet Oncol. (2013)
Prospective population-based screening trial (2013–2018)
19
• Incremental increase in breast cancer detection with
BT:2.2–2.7 per 1000 screens
• Mixed effect on recall rates
Kristina Lång, ESMO 9 Nov 2018
-
14,848 screened womenBT DM
Recall rate (%) 3.6 2.5
Detected cancers (n)* 131 97
CDR** 8.7/1000 6.5/1000
Sensitivity (%) 81 60
Specificity (%) 97 98
PPV (%) 24 26
* Bilateral cancers in two women
** Calculated per woman
+42 cancers (90% invasive)
+8 cancers (50% invasive)
+2.2 women with cancer per 1000 screened (CI: 1.2 to 3.2, p<
0.0001)
Malmö Breast Tomosynthesis Screening TrialOne-view tomosynthesis
vs. two-view mammography
20Kristina Lång, ESMO 9 Nov 2018
-
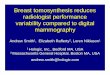
SCREENING DM
-
SCREENING BT
-
DM
PAD: 15 mm IDC G1, LN-
SCREENING DM SCREENING BT
-
• Today; outside rare very-high risk conditions, age is the sole
risk factor considered in screening
• Individualized/risk-based screening may improve benefit/harm
ratio
unsplash.com
‣ Earlier cancer detection and less intensive
treatments in high risk women ‣ Less false positives and
overdiagnoses in
low risk women ‣ Increase the cost-efficacy
Individualized screening
Kristina Lång, ESMO 9 Nov 2018
-
• RCT, 7-year long European H2020 project ststarted 2018,
including 5 countries (France, Italy, UK, Belgium and Israel)
• 85,000 women aged 40–70, 4-years follow-up
• Stratification based on personalized breast cancer risk (risk
model, SNPs and breast density)
• Outcomes:
- Primary: Is risk-based screening non-inferior, and eventually
superior, to conventional screening in terms of reduction of stage
II or higher BC
- Secondary: Biopsy rates for benign breast lesions, rate of
low-risk cancers in low-risk women in both arms,
socio-psychological assessments, cost-effectiveness
MyPEBS (My Personalized Breast Screening)
25
https://cordis.europa.eu/project/rcn/212694_en.html
Personalized breast cancer screening trial
Kristina Lång, ESMO 9 Nov 2018
-
Additional imaging method for dense breasts
MRI
• Advantages: no ionizing radiation, high sensitivity
• Disadvantages: time, FP, cost, accessibility, contrast
agent
• Abbreviated MRI protocol: 3D MIP image and first post-contrast
T1 image (FAST)
• DWI-MRI (without Gd) a good alternative?
• The Dense Tissue and Early Breast Neoplasm Screening (DENSE)
trial:
Bickelhaupt, S et al. Radiology (2016)Kuhl CK, et al. Radiology
(2017)
26
Emaus MJ et al. Radiology (2015)
- Women with extremely dense breast- RCT DM vs. DM + MRI-
Primary outcome: proportion of IC rates
Kristina Lång, ESMO 9 Nov 2018
-
• Computer-aided-detection (CAD) has been used in mammography
since the 90s
• To many false positives
• Recent improvements in AI, due to deep learning algorithms, is
closing the gap between humans and computers
Lehman CD, et al. JAMA Intern Med (2015)
Fenton JJ, et al. NEJM (2007)
27
Artificial intelligence in screening
• Multicenter multireader-multicase study, 2,652 exams (653
malignant)
• 101 radiologist vs machine (Transpara)
• The performance of the AI system similar to the average
radiologist
A Rodriguez-Ruiz et al. JNCI (2018)
Kristina Lång, ESMO 9 Nov 2018
-
• 9,588 double-read mammography screening exams (71
screen-detected cancers,187 FP)
• Images were analysed with a deep learning-based software
(Transpara)
• Preselection tool that assigns 10 risk scores with an
increasing likelihood of cancer
• The effect of excluding cases with low risk scores (≤5) from
screen-reading was investigated
28
Can artificial intelligence reduce the workload in
screening?
Kristina Lång, ESMO 9 Nov 2018
-
• Safely reduce the workload by 10%
29
AI score Normal cases (n) False positives (n) Cancer cases (n)1
1004 (10.4%) 6 (3.2%) 0 (0%)1–2 1830 (19.1%) 10 (5.4%) 1 (1.4%)1–3
2724 (28.4%) 19 (10.2%) 3 (4.2%)1–4 3996 (41.7%) 35 (18.7%) 5
(7.0%)1–5 5085 (53.0%) 52 (27.8%) 8 (11.3%)
K Lång et al. (ECR 2019) AI-score
N
• Adapt work effort to risk?
Sin
gle
read
ing
Dou
ble
read
ing
No
hum
an r
eade
rs
Can artificial intelligence reduce the workload in
screening?
Kristina Lång, ESMO 9 Nov 2018
-
Workflow Efficiency.CAT – Computer Assisted Triage
Worklist A Worklist B Worklist C
Result from an AI or CAD solution automatically set on the exam
and visible in the worklist in Sectra PACS.Single
readingDouble reading
AI
-
Breast cancer screeningSummary
31
• Implemented in most countries in Europe
• Screening interval: age 50–69, mammography with 2 year
interval
• RCTs: Reduction in breast cancer mortality by 20%
• Overdiagnosis rate 11%
• False positives is a drawback in screening
• The screening policy will most likely be modified in the
future with new imaging techniques, individualized screening and
with the introduction of AI
Kristina Lång, ESMO 9 Nov 2018
-
Thank you for your attention
ESMO preceptorship programme Breast cancerDisclosure of
interestThe aim of screeningGuidelines on the principles and
practice of screeningaccording to Wilson and Jungner (WHO
1968)Early randomized controlled trialsMammography screening in
EUTypical mammography screening programmeThe balance in
screeningReduction in breast cancer deathsFalse
positivesOverdiagnosisEstimates of overdiagnosis in screeningSlide
Number 13Slide Number 14Can we reduce overdiagnosis and
overtreatment?Interval cancerSlide Number 17Slide Number
18Tomosynthesis in screeningSlide Number 20Slide Number 21Slide
Number 22Slide Number 23Individualized screeningPersonalized breast
cancer screening trialAdditional imaging method for dense
breastsSlide Number 27Can artificial intelligence reduce the
workload in screening?Can artificial intelligence reduce the
workload in screening?Workflow Efficiency. Breast cancer
screeningSlide Number 32