Embed Size (px)
Citation preview

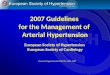
Figure 3. Estimated 1-year mortality rates for CML patients by disease phase and treatment line compared with age-specific US Census (background) mortality
2L = second line; 3L = third-lineYearly death rates = all reported deaths ÷ estimated mean patient-years*2011 US Census estimates by 10-year age band as reported by Centers for Disease Control and Prevention (CDC)15
Cause of Death in Resistant and Advanced Chronic Myeloid Leukemia (CML) Patients Treated with Tyrosine Kinase Inhibitors (TKIs)Lisa J McGarry1, Chakkarin Burudpakdee2, Smeet Gala2, Arpamas Seetasith2, Merena Nanavaty2, Hui Huang1
1ARIAD Pharmaceuticals, Inc., Cambridge, MA; 2MKTXS, LLC., Raritan, NJ
Chronic myelogenous leukemia (CML) was diagnosed in approximately 70,000 patients in 2010, and theprevalence is expected to increase to 112,000 by 2020 in the US alone.1
With recent advances in CML management, newly-diagnosed chronic phase (CP) CML patients may expectnear-normal life expectancy on TKI treatment. However, patients resistant to prior TKIs and those withadvanced disease may face a much poorer prognosis and higher likelihood of CML-related death.
This systematic literature review was undertaken to quantify the proportion of deaths attributed to diseaseprogression, treatment-related adverse events (AEs), and unrelated (background) causes in treatment-resistantand advanced-stage CML.
European School of Haematology (ESH) 16TH Annual John Goldman Conference on Chronic Myeloid Leukemia: Biology and Therapy, Philadelphia, USA, September 4 – 7, 2014
RESULTS
A total of 2,531 citations were screened, of which 13 studies (12 full-text and 1 conference abstract) wereincluded in the final assessment (Figure 1); one study2 contributed data for 2nd line, 3rd line, and AP/BP. The line of treatment was 2nd line in 7 studies, 3rd line in 2 studies, and 6 studies reported AP/BP
Iden
tify
Scre
enEl
igib
leIn
clud
e
Conference proceedings and grey literature (Jan 1999-Jan 2014)
Records screened (n = 2,531)Abstracts excluded (n = 2,399)1.Duplicate studies (n = 49) 2.No relevant data (n = 1,917) 3.Not post 1st-line treatment (n = 360)4.Not CML population (n = 73)
Full-text articles excluded (n = 119)1.No death data (n = 64)2.Reviews used for cross-referencing (n = 6)3.Full-text not available (n = 2)4.Poor data quality (n = 47)
Studies included in qualitative review (n = 13)
Full-text articles assessed for eligibility (n = 132)
PubMed (Jan 1999-Jan 2014)
Figure 1. PRISMA Flow Diagram of Systematic Literature Search
Table 1. Characteristics of the included 13 studies
The drug of evaluation was dasatinib in 8 studies, nilotinib in 2, bosutinib in 1, dasatinib and nilotinib in 1, andGHI (granulocyte colony-stimulating factor + homoharringtonine + standard dose imatinib) regimen in 1 study.
Overall, 5% of 2nd-line, 10% of 3rd-line, and 21% of AP/BP patients died during study follow-up.
Ref # MoleculeMedian
follow-up (years)
Patients evaluated for death
CML-related
mortalityn (%)
Tx-related AE
mortalityn (%)
Tx-unrelated
AE mortality
n (%)
Mortality due to
unspecified AE
n (%)
Unspecified deaths n (%)
Back-ground deathsa
n (%)
Back-ground deaths / PY (%)
Adjusted PYb
2nd line CP-CML
3 DAS 1.2 387 6 (42.9) 0 (0.0) 0 (0.0) 8 (57.1) 0 (0.0) 8 (57.1) 1.7 697.0
4 DAS 2.1 101 1 (50.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0.0 311.2
5 DAS 2.3 36 2 (100.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0.0 119.4
6 DAS 2.0 670 26 (47.3) 2 (3.6) 0 (0.0) 24 (43.6) 3 (5.5) 27 (49.1) 2.0 1933.2
7 DAS 2.0 125 2 (18.2) 0 (0.0) 0 (0.0) 8 (72.7) 1 (9.1) 9 (81.8) 3.6 361.4
8 NIL 1.5 321 1 (11.1) 0 (0.0) 0 (0.0) 8 (88.9) 0 (0.0) 8 (88.9) 1.6 711.3
2 BOS 1.0 286 4 (57.1) 0 (0.0) 3 (42.9) 0 (0.0) 0 (0.0) 3 (42.9) 1.1 410.1
3rd line CP-CML
9 DAS, NIL 1.8 26 8 (88.9) 0 (0.0) 0 (0.0) 1 (11.1) 0 (0.0) 1 (22.2) 2.2 66.2
2 BOS 1.0 118 2 (40.0) 1 (20.0) 2 (40.0) 0 (0.0) 0 (0.0) 2 (40.0) 1.7 169.2
AP/BP CML
10 DAS 0.7 36 2 (50.0) 0 (0.0) 2 (50.0) 0 (0.0) 0 (0.0) 2 (50.0) 8.5 34.1
11 DAS 0.3 109 28 (57.1) 2 (4.1) 0 (0.0) 19 (38.8) 0 (0.0) 19 (38.8) 62.4 43.9
12 DAS 1.2 174 11 (35.5) 1 (3.2) 0 (0.0) 13 (41.9) 6 (19.0) 19 (61.3) 9.4 290.7
13 GHI 1.0 12 3 (50.0) 1 (16.7) 0 (0.0) 2 (33.3) 0 (0.0) 2 (33.3) 16.9 17.1
14 NIL 2.0 137 7 (53.8) 0 (0.0) 0 (0.0) 6 (46.2) 0 (0.0) 6 (46.2) 2.2 389.6
2 BOS 1.0 166 19 (59.4) 2 (6.8) 11 (34.4) 0 (0.0) 0 (0.0) 11 (34.4) 6.7 238.0
CONCLUSIONS Published data suggest the frequency of death due to CML is nearly 10 times that from treatment-related AEs in
patients with resistant and advanced disease. In advanced CML population, the potential benefits of treatment may outweigh potential risks of treatment-
related mortality.
STRENGTHS AND LIMITATIONS
This is the first systematic review that studied the causes of death in resistant and advanced CML patients. Inconsistencies existed in reporting of the causes of death in the included studies.
REFERENCES
RESULTS (CONT’D)RESULTS (CONT’D)BACKGROUND
Although we lacked patient-level follow-up data, we estimated overall yearly death rates of 2%, 6% and 13% for2nd-line, 3rd-line and AP/BP, respectively, versus US census estimates of <1% for ages 55-64, indicatingsubstantial excess deaths in these CML populations (Figure 3).
1. Huang X et al. Cancer, 2012; 118(12), 3123-3127.2. Kantarjian HM et al. Blood. 2013:blood-2013-2007-513937.3. Hochhaus A et al. 2008;22(6):1200-1206.4. Kantarjian H et al. Cancer. Sep 15 2009;115(18):4136-4147.5. Khoroshko N et al. Paper presented at: Haematologica 20106. Shah NP et al. Feb 2010;95(2):232-240.7. Latagliata R et al. Leuk Res. Sep 2011;35(9):1164-1169.8. Giles FJ et al. Jan 2013;27(1):107-112.9. Ibrahim AR et al. Blood. 2010;116(25):5497-5500.10. Ottmann O et al. Blood. 2007;110(7):2309-2315.11. Cortes J et al. Leukemia. Dec 2008;22(12):2176-2183.12. Apperley JF et al. Journal of clinical oncology. Jul 20 2009;27(21):3472-3479.13. Fang B et al. Annals of hematology. Nov 2010;89(11):1099-1105.14. Le Coutre P et al. Leukemia. 2012;26(6):1189-1194.15. Hoyert DL, Xu J. National vital statistics reports. 2012;61(6):1-51.
For 2nd-line patients, CML-related was the investigator-reported cause of 44% of deaths, compared with 2% dying of treatment-relatedcauses and the remainder of unrelated (3%) or unspecified (51%) AEs (Figure 2).
In 3rd line, 71% of patients died of CML, versus 7% treatment-related, 14% unrelated and 7% unspecified. For AP/BP patients, death from disease comprised 54%, versus 5% treatment-related (9% unrelated; 31% unspecified).
METHODS
Systematic literature review inclusion criteria:• CML patients in 2nd-line CP, 3rd-line CP or those with accelerated phase (AP) / blast phase (BP)• Published between January 1999 - 2014 • Identified from PubMed, conference proceedings, and grey literature • Reporting cause of death
Exclusion criteria:• No report of disease phase and line of therapy• Poor data quality for investigator-reported cause of death
Two researchers reviewed study titles and abstracts to determine eligibility for full text review; discrepancies resolved by a third researcher
Investigator-reported causes of death was categorized as:• CML-related • Treatment-related AE• Treatment-unrelated AE• Unspecified AE and • Unspecified death
Figure 2. Proportion of deaths among CML patients attributable to each investigator-reported cause, by disease phase and treatment line
AP = accelerated-phase; BP = blast phase; PH+ ALL = Philadelphia chromosome positive acute lymphocytic leukemia; 2L = second line; 3L = third-line; CP-CML = chronicphase chronic myeloid leukemia; Tx = treatment
DAS: dasatinib; NIL: nilotinib; BOS: bosutinib; GHI: granulocyte colony-stimulating factor + homoharringtonine + standard dose imatinib; TX: treatment; PY: patient yearsa Background death = unrelated AE + unspecified AE + unspecified death b Estimated mean follow-up = estimated median patient years ÷ ln(2) (assuming constant attrition)
0.8%
1.8%
2.2%
5.9%
13.3%
0% 2% 4% 6% 8% 10% 12% 14%
55–64 years*
65-74 years*
2L CP-CML
3L CP-CML
AP/BP/Ph+ALL
US population expected mortality, selected age groups
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
AP/BP/Ph+ALL
3L CP-CML
2L CP-CML
CMLTx-relatedUnrelatedUnspecified
54% 5% 9% 31%
71% 7% 14% 7%
44% 2%3% 51%
Please scan the QR code to view the poster