-
8/13/2019 ES Terapi Hormon 2
1/5
American Journal of Epidemiology
The Author 2009. Published by the Johns Hopkins Bloomberg School
of Public Health.
All rights reserved. For permissions, please e-mail:
[email protected].
Vol. 170, No. 1
DOI: 10.1093/aje/kwp113
Advance Access publication May 25, 2009
Invited Commentary
Invited Commentary: Hormone Therapy Risks and BenefitsThe Womens
Health
Initiative Findings and the Postmenopausal Estrogen Timing
Hypothesis
Emily Banks and Karen Canfell
Initially submitted January 22, 2009; accepted for publication
April 10, 2009.
Worldwide evidence on menopausal hormone therapy shows that it
does not reduce coronary heart disease
(CHD) risk and that it increases the risks of breast cancer,
stroke, and venous thromboembolism. These risks are
not offset by reductions in hip fracture risk. Consequently, the
Food and Drug Administration and other drugregulatory authorities
agree that hormone therapy should be used chiefly for short-term
relief of menopausal
symptoms. Continuing speculation relates to the postmenopausal
estrogen timing hypothesis, which proposes
that hormone therapy initiated soon after menopause will prevent
CHD while therapy started later will have a null
or adverse effect. The detailed analyses of Womens Health
Initiative data reviewed here specifically address the
timing hypothesis. For hormone therapy initiated soon after
menopause versus therapy started later, the findings
demonstrate 1) similar null or adverse effects on CHD risk; 2)
similar adverse effects on the risks of stroke and
venous thrombosis; and 3) possibly greater adverse effects on
breast cancer risk. Therefore, Womens
Health Initiative data do not support the hypothesis of
favorable effects in women starting hormone therapy
soon after menopause. Hence, the overall trial findings,
including net harm for combined estrogen-progestin and
the lack of a net benefit for estrogen-only therapy, also apply
to women initiating hormone therapy soon after
menopause.
clinical trial; cohort studies; estrogens; estrogen replacement
therapy; hormone replacement therapy; medroxy-
progesterone 17-acetate; postmenopause; progestins
Abbreviations: CHD, coronary heart disease; FDA, Food and Drug
Administration; WHI, Womens Health Initiative.
Despite recent substantial declines in use, menopausalhormone
therapy remains among the most commonly usedmedications in
industrialized countries. The availabilityand reliability of
evidence on the risks and benefits ofhormone therapy have improved
markedly over the pastdecade. Synthesis of the worldwide evidence
from ran-
domized trials and observational studies shows that whilehormone
therapy is effective for the relief of menopausalsymptoms, hormone
use leads to no overall beneficial ef-fect on coronary heart
disease (CHD) risk and leads toincreased risks of breast cancer,
stroke, and venous throm-boembolism that are not offset by
reductions in the risk ofhip fracture (13). It is now well
established that the risk ofbreast cancer is increased to a greater
extent in users ofestrogen-progestin preparations than in users of
estrogen-
only preparations (13). In response to results from theWomens
Health Initiative (WHI) clinical trials (3) andin keeping with the
worldwide evidence, the US Foodand Drug Administration (FDA) and
drug regulatory au-thorities in other countries have recommended
that hormonetherapy be used chiefly for short-term relief of
menopausal
symptoms rather than for the prevention of disease (1,
47).Alongside this emerging clarity of evidence and moretargeted
use of hormone therapy, a continuing area of spec-ulation relates
to the postmenopausal estrogen timingor window hypothesis. This
hypothesis proposes thathormone therapy given soon after menopause
will havea beneficial effect on the risk of CHD, whereas
hormonetherapy given later will have a null or adverse effect(8,
9).
Correspondence to Associate Professor Emily Banks, National
Centre for Epidemiology and Population Health, The Australian
National
University, Canberra, ACT 0200, Australia (e-mail:
[email protected]).
24 Am J Epidemiol 2009;170:2428
-
8/13/2019 ES Terapi Hormon 2
2/5
NEW RESULTS FROM THE WHI
In this issue of the American Journal of Epidemiology,Prentice
et al. (8) present results from the most comprehen-sive analysis to
date of WHI data on hormone therapy andclinical outcomes according
to the time between menopauseand initiation of use. These analyses
were designed specif-
ically to address the timing hypothesis. Prentice et al.
pre-sent results from analysis of the WHI clinical trial data,
bothseparately and combined with the observational study data,and
compare a range of health effects in women who initi-ated hormone
therapy soon after menopause with thoseamong women who started
later.
A key methodological difference between this and pre-vious
analyses is the investigation of the gap time be-tween menopause
and the first use of hormone therapy (8),rather than the time
between menopause and randomizationinto the trials (10, 11). Hence,
this reclassification takes intoaccount prior use in both the
trials and the observationalstudies and gives a more appropriate
picture of the healtheffects of hormone therapy in relation to the
time between
starting use and menopause. Since 48% and 26% of womenin the
estrogen-only and estrogen-progestin hormone ther-apy trials,
respectively, were prior hormone users (10), thisis important.
Additionally, the authors report on their jointanalysis of the WHI
clinical trial and observational studydata. The large majority of
prior hormone therapy users inboth the clinical trials and the
observational study had firstinitiated hormone therapy within 5
years of menopause.
The main finding from these analyses is that, based onclinical
trial data, the effects of estrogen-only (conjugatedequine
estrogens) and estrogen-progestin (conjugated
equineestrogens/medroxyprogesterone acetate) hormone therapy onthe
risks of CHD, stroke, and venous thromboembolism did
not differ significantly according to how soon after meno-pause
treatment was initiated (8). The findings remainedwhen
observational study data were included in the analyses.
Within the estrogen-progestin trial, the authors identifieda
significantly greater elevation in the risk of invasive
breastcancer among women who initiated use within 5 years
ofmenopause as compared with those who had a longer gaptime to
initiation (Pfor interaction 0.03) (8). Analysis ofcombined data
from the WHI clinical trials and observa-tional studies showed a
significantly greater increase inthe hazard ratio for invasive
breast cancer with a shortergap time (adjusting for duration of
use) for both estrogen-only and estrogen-progestin, which
contributed to greaterrisks of total cancer with shorter gap times
(8). These dataalso showed borderline-significant findings
suggestingworse results for the global index with shorter gap
times(8). Prentice et al. are suitably cautious about
interpretationof the findings for breast cancer, total cancer, and
the globalindex, in view of the large numbers of statistical tests,
theincreased use of observational data, and other methodolog-ical
difficulties. Of particular relevance to the estrogen-onlytrial is
the difficulty of establishing age at menopause, andhence gap time,
accurately in women who have had a hys-terectomy without
oophorectomy prior to menopause (12).However, while it remains to
be seen whether invasivebreast cancer risks are particularly
elevated in women initi-
ating hormone therapy close to menopause, above and be-yond the
already-established overall increase in breastcancer risk, the
trial and observational data do not provideany evidence of a
beneficial effect with early commence-ment of use on this outcome
or on the global index (8).
Prentice et al. conclude that the WHI data . . .providelittle
support for the hypothesis of favorable effects among
women who initiate postmenopausal estrogen use soon
aftermenopause, either for CHD or for health benefits versus
riskindices considered (8, p. 12). They note that, as a
conse-quence, the overall balance of risks and benefits seen in
theWHI trials should be considered to apply to recently
post-menopausal women as well as women who experiencedmenopause in
the more distant past (8).
THE TIMING HYPOTHESIS
The timing hypothesis arose following publication of themain
findings from the WHI, which showed no beneficialeffect of hormone
therapy on CHD risk (3, 9). These find-ings differed from the
expectation of many researchers andclinicians that hormone therapy
would be cardioprotective,and the timing hypothesis was one attempt
to explain thisdifference (9).
The expectation of cardioprotection was chiefly based ondata
from observational studies of CHD and hormone ther-apy and from
studies of intermediate cardiovascular bio-markers, such as
lipoprotein cholesterol levels, bloodpressure, insulin levels, and
indices of atherosclerosis (9,13). A number of predominantly
US-based observationalstudies published during the 1980s and 1990s
found thatwomen using hormone therapy were at lower risk of CHDthan
nonusers (14, 15). This was interpreted by many asproviding strong
evidence that hormone therapy prevented
CHD (13). However, hormone therapy tends to be pre-scribed
preferentially to women who are at lower risk ofcardiovascular
disease, in terms of known risk factors (16,17) and reduced
preexisting disease (17, 18), and this con-founding was not
accounted for in many studies (19). Be-cause of the complex
interplay of multiple pathways relatingto factors such as clotting,
atherosclerosis, and inflamma-tion, the relation between hormone
therapy and individualintermediate biomarkers is almost impossible
to translateinto an understanding of the overall effect of hormone
ther-apy on CHD (9). Hence, the relation between hormone ther-apy
and clinical endpoints, such as myocardial infarction,must remain
the mainstay for quantifying its effects.
The timing hypothesis is based on the idea that the
WHIparticipants were on average too old to benefit from hor-mone
therapy, because they had existing atherosclerosis, butyounger
women, who are generally closer to menopause andhave less
atherosclerosis, would benefit (9). It supposes thathormone therapy
in women with established atherosclerosismay cause adverse events
when vulnerable plaque is presentbut may prevent atherosclerosis if
begun early enough (9).
The uncertainty surrounding the effects of hormone ther-apy on
CHD prompted the WHI primary prevention trials;the main aim of
these trials was to evaluate the effect ofhormone therapy on
clinical CHD endpoints in healthy post-menopausal women. It is
important to note that the timing
Hormone Therapy Timing and Health Outcomes 25
Am J Epidemiol 2009;170:2428
-
8/13/2019 ES Terapi Hormon 2
3/5
hypothesis was not postulated prior to publication of the
WHIresults, and it was therefore not one of the hypotheses
plannedto be tested in the study. Neither has the proposed pattern
of
effectbenefit in persons who are younger and have lessexisting
coronary damage and null or adverse effects in olderpersonsbeen
observed previously with cardioprotectivemedications, such as
lipid-lowering agents (20), antihyperten-sive agents (21, 22), or
antiplatelet agents (23, 24). Indeed, forthese therapies, benefit
is generally observed regardless ofage, and absolute benefits are
greater in older persons andthose at higher risk of cardiovascular
disease (20, 21, 23, 24).
SUBGROUP ANALYSES
The WHI trials were designed to have sufficient statisticalpower
to examine the overall relation between use of hor-mone therapy and
CHD. There was limited power to investi-gate subgroups, and
examination of subgroups in randomizedcontrolled trials is
generally problematic (25, 26). It is par-ticularly difficult to
meaningfully investigate subgroups thatare defined post hoc,
because their findings appear interest-ing, which is the case for
the timing hypothesis. Evaluation ofwhether effects differ between
subgroups must include for-mal testing for statistical interaction
or effect modifica-tion, according to predefined stringent levels
of significance(26). However, even comparisons of subgroups which
yieldmarginally significant findings must be viewed with caution
ifthey were not specified prior to analysis or if they make upone
of many such comparisons (25, 26). The effect of hor-
mone therapy in a particular subgroup is statistically the
sameas the overall effect in the whole study population, if
nosignificant statistical interaction is present.
THE WAY FORWARD FOR RESEARCH AND CLINICAL
PRACTICE
The current evidence from the WHI regarding the timinghypothesis
is the best available, and it is this that must guidepractice. The
new analysis by Prentice et al. of both the WHIclinical trial data
and the observational data finds no evi-dence of a beneficial
effect on the risk of CHD in womenwho initiate hormone therapy soon
after menopause (8). Theoverall findings on hormone therapy and
cardiovascular dis-ease from randomized controlled trials must
therefore beassumed to apply to women regardless of time
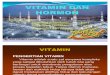
betweenmenopause and commencement of use. Figure 1 showsa summary
of the available data from randomized controlledtrials of the
effect of hormone therapy on CHD risk (1).It demonstrates that
neither estrogen-only nor estrogen-progestin preparations are
protective against CHD, withno significant difference between these
preparations in thiseffect (Pfor heterogeneity 0.1). For outcomes
other thanCHD, the new analysis from the WHI finds no evidence ofa
beneficial effect of initiation of hormone therapy close
tomenopause. Indeed, for breast cancer, the evidence sug-gests, if
anything, that women initiating use closer to men-opause may
experience greater increases in risk. Hence,clinicians cannot
assume that prescription of hormones
Figure 1. Relative risk of coronary heart disease in women
randomized to receive estrogen-only or estrogen-progestin hormone
replacementtherapy (HRT) as compared with placebo in published
randomized trials. Bars, 95% confidence interval (CI). HT, hormone
therapy; ESPRIT,Estrogen in the Prevention of Reinfarction Trial;
HERS, Heart and Estrogen/Progestin Replacement Study; PHASE,
Papworth HRT Atheroscle-rosis Study Enquiry; WAVE, Womens
Angiographic Vitamin and Estrogen Trial; WEST, Womens Estrogen for
Stroke Trial; WHI, Womens HealthInitiative; WISDOM, Womens
International Study of Long Duration Oestrogen after Menopause.
(Reproduced with the permission of the UnitedKingdom Medicines and
Healthcare Products Regulatory Agency (1, p. 43)).
26 Banks and Canfell
Am J Epidemiol 2009;170:2428
-
8/13/2019 ES Terapi Hormon 2
4/5
close to menopause is particularly safe, in terms of therelative
risk of serious disease.
Additional and more independent evidence regarding theCHD timing
hypothesis will be difficult to obtain. The 3primary prevention
trials for hormone therapy, the 2 WHIclinical trials and the WISDOM
trial, were stopped earlybecause it was considered inappropriate to
continue ran-
domizing women to treatment given the evidence of harmand the
lack of benefit (2, 3, 27). It is therefore unlikely thatfurther
trial data of this nature will be forthcoming. Inter-pretation of
data on intermediate cardiovascular endpoints isdifficult.
Judicious interpretation of data from observationalstudies may be a
source of future insights.
CLINICAL IMPLICATIONS: TARGETED USE OF
HORMONE THERAPY
Since 2002, the guidance provided by drug regulatorybodies
internationally has been remarkably consistent. TheFDA (4, 7, 28)
and equivalent agencies elsewhere (1, 5, 6)
have made recommendations that can be summarizedbroadly as
follows.
1. Hormone therapy is indicated only for moderate-to-severe
menopausal symptoms.
2. Women should carefully consider the risks and benefitsof
hormone therapy.
3. Hormones should be used at the lowest effective dose forthe
shortest duration possible.
4. Hormone therapy should not be used for the preventionof
cardiovascular disease or dementia.
5. Use should be reviewed every 36 months (4, 5, 28) or atleast
annually (29).
While the FDA considers hormone therapy an option forthe
prevention of osteoporosis, agencies in Europe, theUnited Kingdom,
and Australia recommend that it not beused as a first-line
treatment for the prevention of osteopo-rosis or osteoporotic
fracture. Hormone therapy has neverbeen approved for the prevention
or treatment of cardiovas-cular disease by the FDA or these other
agencies.
Use of hormone therapy has fallen dramatically since
thepublication of the main results from WHI in mid-2002
andconsequent revision of regulatory guidelines (3). This
re-duction in use has been accompanied by falling breast can-cer
incidence among women aged 50 years or more, but notgenerally in
younger women, in the United States (30),Australia (31), Germany
(32), New Zealand (33), France(34), and Canada (35). Although
multiple factors may affecttrends in breast cancer incidence in
various settings, the dropin breast cancer incidence cannot be
explained fully bychanges in breast cancer risk factors,
mammographicscreening (30, 31, 36), or prescribing of other
medications(31); the rapid decrease in the use of hormone therapy
formenopause is the most likely explanation (37).
The rapid decrease in the use of hormone therapy since2002 and
the substantial declines in breast cancer incidenceindicate that
the availability of evidence on the risks andbenefits of hormone
therapy, and the recommendations for
more cautious and targeted use, are likely to have
alreadyprevented substantial numbers of breast cancers
worldwide(37). These new findings from WHI establish that the
adverseeffects of hormone therapy, seen in the trials in general,
alsoapply to women who initiate use soon after menopause.
ACKNOWLEDGMENTS
Author affiliations: National Centre for Epidemiology
andPopulation Health, The Australian National University,
Can-berra, Australian Capital Territory, Australia (Emily
Banks);The Sax Institute, Sydney, New South Wales, Australia
(EmilyBanks); Cancer Epidemiology Research Unit, The CancerCouncil
New South Wales, Sydney, New South Wales, Aus-tralia (Karen
Canfell); and The School of Public Health, Uni-versity of Sydney,
NewSouth Wales,Australia(Karen Canfell).
Conflict of interest: none declared.
REFERENCES
1. Medicines and Healthcare Products Regulatory Agency. UKPublic
Assessment Report. Hormone-Replacement Therapy:Safety Update.
London, United Kingdom: Medicines andHealthcare Products Regulatory
Agency; 2007.
(http://www.mhra.gov.uk/home/groups/pl-p/documents/websitere-sources/con2032228.pdf).
(Accessed January 12, 2009).
2. Anderson GL, Limacher M, Assaf AR, et al. Effects of
con-jugated equine estrogen in postmenopausal women with
hys-terectomy: the Womens Health Initiative randomizedcontrolled
trial. JAMA. 2004;291(14):17011712.
3. Rossouw JE, Anderson GL, Prentice RL, et al. Risks
andbenefits of estrogen plus progestin in healthy
postmenopausalwomen: principal results from the Womens Health
Initiativerandomized controlled trial. JAMA.
2002;288(3):321333.
4. Food and Drug Administration, US Department of Health
andHuman Services. Guidance for Industry. NoncontraceptiveEstrogen
Drug Products for the Treatment of VasomotorSymptoms and Vulvar and
Vaginal Atrophy SymptomsRecommended Prescribing Information for
Health Care Pro-viders and Patient Labeling. Draft Guidance.
Revision 4.Rockville, MD: Food and Drug Administration; 2005. (
http://www.fda.gov/cder/guidance/6932dft.pdf). (Accessed January13,
2009).
5. Australian Drug Evaluation Committee.ADEC SummaryStatement on
HRT. Canberra, Australia: Therapeutic GoodsAdministration,
Australian Government Department of Healthand Ageing; 2004.
(http://www.tga.gov.au/docs/html/
hrtadec3.htm). (Accessed January 13, 2009).6. European Agency
for the Evaluation of Medicinal Products.EMEA Public Statement on
Recent Publications RegardingHormone Replacement Therapy. London,
United Kingdom:European Agency for the Evaluation of Medicinal
Products;2003.
(http://www.emea.europa.eu/pdfs/human/press/pus/3306503en.pdf).
(Accessed January 13, 2009).
7. Food and Drug Administration, US Department of Health
andHuman Services. FDA Approves New Labeling and ProvidesNew Advice
to Postmenopausal Women Who Use or Who AreConsidering Using
Estrogen and Estrogen With Progestin.(FDA Fact Sheet). Rockville,
MD: Food and Drug Adminis-tration; 2003.
(http://www.fda.gov/oc/factsheets/WHI.html).(Accessed January 13,
2008).
Hormone Therapy Timing and Health Outcomes 27
Am J Epidemiol 2009;170:2428
http://www.mhra.gov.uk/home/groups/pl-p/documents/websiteresources/con2032228.pdfhttp://www.mhra.gov.uk/home/groups/pl-p/documents/websiteresources/con2032228.pdfhttp://www.mhra.gov.uk/home/groups/pl-p/documents/websiteresources/con2032228.pdfhttp://www.fda.gov/cder/guidance/6932dft.pdfhttp://www.fda.gov/cder/guidance/6932dft.pdfhttp://www.tga.gov.au/docs/html/hrtadec3.htmhttp://www.tga.gov.au/docs/html/hrtadec3.htmhttp://www.emea.europa.eu/pdfs/human/press/pus/3306503en.pdfhttp://www.emea.europa.eu/pdfs/human/press/pus/3306503en.pdfhttp://www.fda.gov/oc/factsheets/WHI.htmlhttp://www.fda.gov/oc/factsheets/WHI.htmlhttp://www.emea.europa.eu/pdfs/human/press/pus/3306503en.pdfhttp://www.emea.europa.eu/pdfs/human/press/pus/3306503en.pdfhttp://www.tga.gov.au/docs/html/hrtadec3.htmhttp://www.tga.gov.au/docs/html/hrtadec3.htmhttp://www.fda.gov/cder/guidance/6932dft.pdfhttp://www.fda.gov/cder/guidance/6932dft.pdfhttp://www.mhra.gov.uk/home/groups/pl-p/documents/websiteresources/con2032228.pdfhttp://www.mhra.gov.uk/home/groups/pl-p/documents/websiteresources/con2032228.pdfhttp://www.mhra.gov.uk/home/groups/pl-p/documents/websiteresources/con2032228.pdf
-
8/13/2019 ES Terapi Hormon 2
5/5
8. Prentice RL, Manson JE, Langer RD, et al. Benefits and risks
ofpostmenopausal hormone therapy when it is initiated soon
aftermenopause. Am J Epidemiol. 2009;170(1):1223.
9. Barrett-Connor E. Hormones and heart disease in women:
thetiming hypothesis. Am J Epidemiol. 2007;166(5):506510.
10. Rossouw JE, Prentice RL, Manson JE, et al.
Postmenopausalhormone therapy and risk of cardiovascular disease by
age andyears since menopause. JAMA. 2007;297(13):14651477.
11. Manson JE, Hsia J, Johnson KC, et al. Estrogen plus
progestinand the risk of coronary heart disease. N Engl J Med.
2003;349(6):523534.
12. Collaborative Group on Hormonal Factors in Breast
Cancer.Breast cancer and hormone replacement therapy:
collaborativereanalysis of data from 51 epidemiological studies of
52,705women with breast cancer and 108,411 women without
breastcancer. Lancet. 1997;350(9084):10471059.
13. Manson JE, Bassuk SS. Re: Invited commentary: hormonetherapy
and risk of coronary heart diseasewhy renew thefocus on the early
years of menopause? [letter]. Am J Epi-demiol.
2007;166(12):14811482.
14. Grodstein F, Stampfer MJ, Manson JE, et al.
Postmenopausalestrogen and progestin use and the risk of
cardiovascular dis-ease.N Engl J Med. 1996;335(7):453461.
15. Grodstein F, Stampfer MJ, Colditz GA, et al.
Postmenopausalhormone replacement therapy and mortality. N Engl J
Med.1997;336(25):17691775.
16. Barrett-Connor E, Wingard DL, Criqui MH.
Postmenopausalestrogen use and heart disease risk factors in the
1980s.Rancho Bernardo, Calif, revisited. JAMA.
1989;261(14):20952100.
17. Hunt K, Vessey M. Long-term effects of postmenopausal
hor-mone therapy. Br J Hosp Med. 1987;38(5):450453, 456460.
18. Million Women Study Collaborators. Patterns of use of
hor-mone replacement therapy in one million women in
Britain,19962000. BJOG. 2002;109(12):13191330.
19. Nelson HD, Humphrey LL, Nygren P, et al.
Postmenopausalhormone therapy: scientific review. JAMA.
2002;288(7):872881.
20. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety
ofcholesterol-lowering treatment: prospective meta-analysis ofdata
from 90,056 participants in 14 randomised trials of sta-tins.
Lancet. 2005;366(9493):12671278.
21. Gueyffier F, Boutitie F, Boissel J, et al. Effect of
antihyper-tensive drug treatment on cardiovascular outcomes in
womenand men: a meta-analysis of individual patient data from
ran-domized, controlled trials. The INDANA Investigators. AnnIntern
Med. 1997;126(10):761767.
22. Turnbull F. Blood Pressure Lowering Treatment
TrialistsCollaboration. Effects of different
blood-pressure-loweringregimens on major cardiovascular events:
results ofprospectively-designed overviews of randomised
trials.Lancet. 2003;362(9395):15271535.
23. Antiplatelet Trialists Collaboration. Collaborative
overviewof randomised trials of antiplatelet therapyI: prevention
of
death, myocardial infarction, and stroke by prolonged
anti-platelet therapy in various categories of patients. BMJ.
1994;308(6921):81106.
24. Antithrombotic Trialists Collaboration. Collaborative
meta-analysis of randomised trials of antiplatelet therapy for
pre-vention of death, myocardial infarction, and stroke in high
riskpatients. BMJ. 2002;324(7329):7186.
25. Peto R. Misleading subgroup analyses in GISSI.Am J
Cardiol.
1990;66(7):771772.26. Gail M, Simon R. Testing for qualitative
interactions between
treatment effects and patient subsets. Biometrics.
1985;41(2):361372.
27. Vickers MV, MacLennan AH, Lawton B, et al. Main morbid-ities
recorded in the Womens International Study of LongDuration
Oestrogen after Menopause (WISDOM): a rando-mised controlled trial
of hormone replacement therapy inpostmenopausal women. BMJ.
2007;335(7613):239.
28. Food and Drug Administration, US Department of Health
andHuman Services. Menopause & Hormones. Rockville, MD:Food and
Drug Administration; 2005.
(http://www.fda.gov/womens/menopause/mht-FS.html). (Accessed
January 19,2008).
29. Medicines and Healthcare Products Regulatory Agency.
Hor-mone Replacement Therapy (HRT)Latest Data From theMillion Women
Study and Womens Health Initiative Trial:MHRA Statement. London,
United Kingdom: Medicines andHealthcare Products Regulatory Agency;
2007.
(http://www.mhra.gov.uk/Safetyinformation/Safetywarningsalertsandrecalls/Safetywarningsandmessagesformedicines/CON2030815).(Accessed
January 19, 2009).
30. Ravdin PM, Cronin KA, Howlader N, et al. The decrease
inbreast-cancer incidence in 2003 in the United States. N Engl
JMed. 2007;356(16):16701674.
31. Canfell K, Banks E, Moa AM, et al. Decrease in breast
cancerincidence following a rapid fall in use of hormone
replacementtherapy in Australia. Med J Aust.
2008;188(11):641644.
32. Katalinic A, Rawal R. Decline in breast cancer incidence
afterdecrease in utilisation of hormone replacement therapy.
BreastCancer Res Treat. 2008;107(3):427430.
33. Johnston M. Breast cancer drop linked to fall in HRT. N
ZHerald. 2006;Dec 20.
(http://www.nzherald.co.nz/nz/news/article.cfm?c_id1&objectid10416198).
(Accessed July 2,2008).
34. Allemand H, Seradour B, Weill A, et al. Decline in
breastcancer incidence in 2005 and 2006 in France: a
paradoxicaltrend.Bull Cancer. 2008;95(1):1115.
35. Kliewer EV, Demers AA, Nugent ZJ. A decline in breast-cancer
incidence. N Engl J Med. 2007;357(5):509510.
36. Kerlikowske K, Miglioretti DL, Buist DS. Declines in
invasivebreast cancer and use of postmenopausal hormone therapy ina
screening mammography population. J Natl Cancer
Inst.2007;99(17):13351339.
37. Kumle M. Declining breast cancer incidence and decreasedHRT
use. Lancet. 2008;372(9639):608610.
28 Banks and Canfell
Am J Epidemiol 2009;170:2428
http://www.fda.gov/womens/menopause/mht-FS.htmlhttp://www.fda.gov/womens/menopause/mht-FS.htmlhttp://www.mhra.gov.uk/Safetyinformation/Safetywarningsalertsandrecalls/Safetywarningsandmessagesformedicines/CON2030815http://www.mhra.gov.uk/Safetyinformation/Safetywarningsalertsandrecalls/Safetywarningsandmessagesformedicines/CON2030815http://www.mhra.gov.uk/Safetyinformation/Safetywarningsalertsandrecalls/Safetywarningsandmessagesformedicines/CON2030815http://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=10416198http://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=10416198http://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=10416198http://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=10416198http://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=10416198http://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=10416198http://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=10416198http://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=10416198http://www.mhra.gov.uk/Safetyinformation/Safetywarningsalertsandrecalls/Safetywarningsandmessagesformedicines/CON2030815http://www.mhra.gov.uk/Safetyinformation/Safetywarningsalertsandrecalls/Safetywarningsandmessagesformedicines/CON2030815http://www.mhra.gov.uk/Safetyinformation/Safetywarningsalertsandrecalls/Safetywarningsandmessagesformedicines/CON2030815http://www.fda.gov/womens/menopause/mht-FS.htmlhttp://www.fda.gov/womens/menopause/mht-FS.html