Embed Size (px)
Citation preview
Last revised 01 April 2010 Review Date 01 April 2011
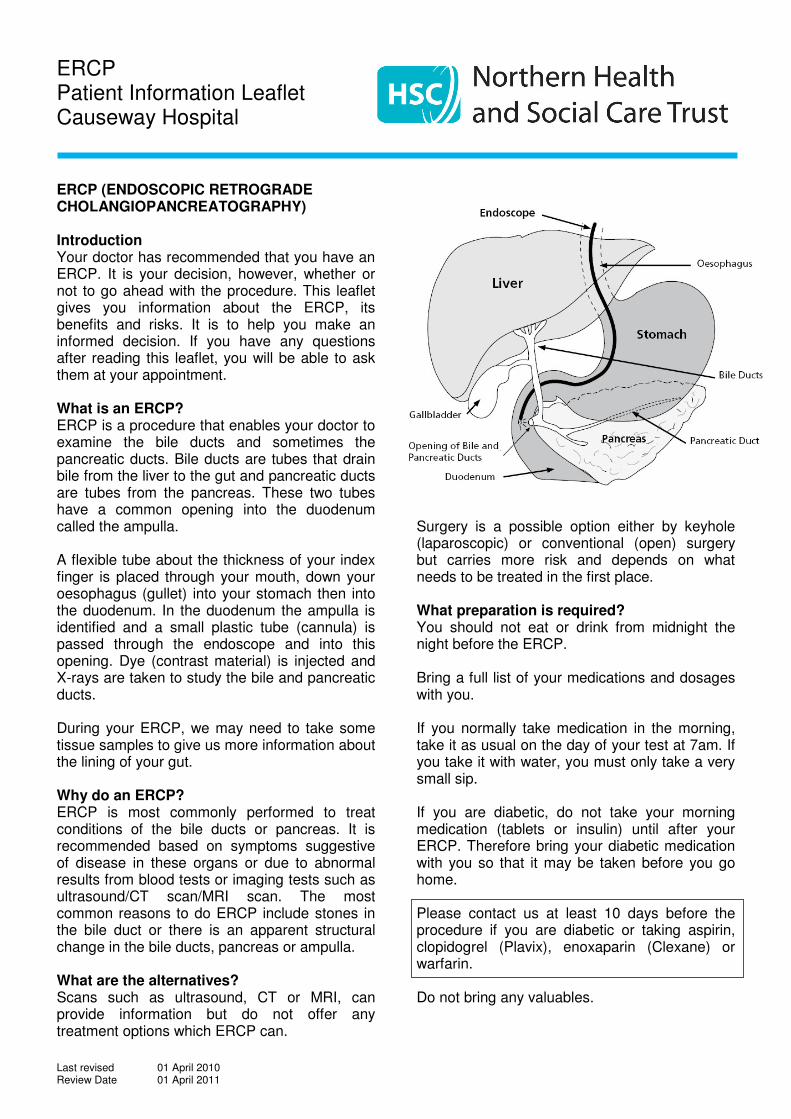
ERCP Patient Information Leaflet Causeway Hospital ERCP (ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY) Introduction Your doctor has recommended that you have an ERCP. It is your decision, however, whether or not to go ahead with the procedure. This leaflet gives you information about the ERCP, its benefits and risks. It is to help you make an informed decision. If you have any questions after reading this leaflet, you will be able to ask them at your appointment. What is an ERCP? ERCP is a procedure that enables your doctor to examine the bile ducts and sometimes the pancreatic ducts. Bile ducts are tubes that drain bile from the liver to the gut and pancreatic ducts are tubes from the pancreas. These two tubes have a common opening into the duodenum called the ampulla. A flexible tube about the thickness of your index finger is placed through your mouth, down your oesophagus (gullet) into your stomach then into the duodenum. In the duodenum the ampulla is identified and a small plastic tube (cannula) is passed through the endoscope and into this opening. Dye (contrast material) is injected and X-rays are taken to study the bile and pancreatic ducts. During your ERCP, we may need to take some tissue samples to give us more information about the lining of your gut. Why do an ERCP? ERCP is most commonly performed to treat conditions of the bile ducts or pancreas. It is recommended based on symptoms suggestive of disease in these organs or due to abnormal results from blood tests or imaging tests such as ultrasound/CT scan/MRI scan. The most common reasons to do ERCP include stones in the bile duct or there is an apparent structural change in the bile ducts, pancreas or ampulla. What are the alternatives? Scans such as ultrasound, CT or MRI, can provide information but do not offer any treatment options which ERCP can.
Surgery is a possible option either by keyhole (laparoscopic) or conventional (open) surgery but carries more risk and depends on what needs to be treated in the first place. What preparation is required? You should not eat or drink from midnight the night before the ERCP. Bring a full list of your medications and dosages with you. If you normally take medication in the morning, take it as usual on the day of your test at 7am. If you take it with water, you must only take a very small sip. If you are diabetic, do not take your morning medication (tablets or insulin) until after your ERCP. Therefore bring your diabetic medication with you so that it may be taken before you go home. Please contact us at least 10 days before the procedure if you are diabetic or taking aspirin, clopidogrel (Plavix), enoxaparin (Clexane) or warfarin. Do not bring any valuables.
Last revised 01 April 2010 Review Date 01 April 2011
What happens when I arrive at the Day Procedure Unit? You will be met by a nurse who will ask you some questions. You will be able to ask the nurse questions if you have any. The nurse will make sure that you understand the ERCP. The nurse will take and record your heart rate and blood pressure. If you are diabetic, the nurse will take and record your blood glucose level. You will be seen by the endoscopist for a quick update. If you are happy to proceed with the ERCP, you will be asked to sign your consent form if you have not already done so. This unit is a training centre for endoscopy. This means that trainees (supervised by qualified staff) may be involved in your care. If you do not want trainees to be present, please inform us when you arrive. Please ask us if you would like information about how we use and store tissue samples and hospital records (including images). What can be expected during ERCP? Your throat will be sprayed with a local anaesthetic before the test begins and you will be given sedative medication intravenously to help you relax during the examination. While you are lying on your stomach on an X-ray table, an endoscope will be gently passed through your mouth, down your oesophagus (gullet), and into your stomach and duodenum. An ERCP can last from 30 to 60 minutes however you should expect to be in the department for most of the day. The endoscope does not interfere with your breathing. It is unlikely that you will experience any sensation of gagging. Most patients fall asleep during the procedure or find it only slightly uncomfortable. You may feel temporarily bloated during and after the procedure due to the air used to inflate the duodenum. What happens after ERCP? You will be monitored in the recovery unit or ward until the effects of the sedatives have worn off. Usually you will be kept nil by mouth for four hours; after this you will be required to remain on clear fluids until the following morning. At this stage you can resume your normal diet. Your throat may be a little sore for a day or two. Your doctor will explain the results of the procedure prior to you returning home. Depending on your health condition or the procedure you underwent, you might be admitted overnight.
What complications can occur? Most ERCPs are done without any problem. The benefit from this procedure needs to be weighed up against the small risk of complications. Any complication could mean you need to stay in hospital for treatment. Abdominal pain due to pancreatitis is the most common complication occurring in approximately 1 in 20 people undergoing ERCP. There are the additional risks of infection (less than 1 in 50 people undergoing ERCP), internal bleeding (less than 1 in 50) or perforation (a hole in the intestine)(less than 1 in 100). Emergency surgery may be required to repair the hole or to stop the bleeding. Blood transfusions are rarely required. It is important for you to report symptoms such as severe abdominal pain, fever, chills, vomiting, or bleeding. A reaction to the sedatives can occur. Pancreatitis and potentially any of the above complications may rarely be extremely severe and may lead to life threatening complications. Delays to your appointment We also deal with emergencies which can arise without warning. These can take priority over your appointment, meaning we may have to ask you to wait or even possibly postpone your ERCP to a later date. What if I need to cancel my ERCP? If you are unable to keep your appointment, please tell us as soon as possible. Aftercare If you are having your ERCP as an Outpatient (i.e. not staying in hospital overnight), you must arrange for somebody to take you home and stay with you overnight. Once home it is important for you to rest for the remainder of the day. Furthermore you should avoid the following activities for at least 24 hours after ERCP:
• Going to work • Driving • Operating machinery • Drinking alcohol • Signing any legally binding documents • Carrying out any activities involving
heights • Caring for young children (sole
responsibility)
Last revised 01 April 2010 Review Date 01 April 2011
If any of the following happen within 72 hours after your ERCP, you need to seek help:
• chest or abdominal/tummy pain that becomes more severe, and is different or more intense than any pains that you would ‘usually’ have
• breathing difficulties • fever (raised temperature) • vomiting blood • passing very black stools.
If this is after you leave hospital, contact us on the number provided, between 9am – 5pm Monday – Friday. Contact your GP or nearest A&E department outside these hours. Say you have had an ERCP. About this information This brochure is not intended to take the place of a discussion with your doctor about your need for an ERCP. If you have any questions about your need for an ERCP, alternative tests, the procedure itself and subsequent follow-up, please make an appointment to see Dr. Lynch by telephoning Miss V. Craig at 028 7034 6326 during office hours. Contact details For further information or in the event of any potential complications: Miss V Craig at 028 7034 6326 between 9am – 5pm Monday – Friday.