Embed Size (px)
Citation preview

ERCP: A Potential Cause and a ERCP: A Potential Cause and a Potential Cure of PancreatitisPotential Cure of Pancreatitis
Grace H. Elta, MDProfessor of Medicine
Division of GastroenterologyUniversity of Michigan

Complications of ERCPComplications of ERCP
General Considerations: Is the indication for ERCP strong
enough to warrant the risks? Low suspicion: Alternative imaging Death in 0.4 -0.6%
Does the performing physician have adequate case volume?

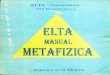
11.1
5.4
8.4
1.2
0
2
4
6
8
10
12
Complications Failed drainage
%
< 1 ES/ wk > 1 ES/ wk
2.30.9
Overall
Severe
*
*
*
*P <0.05
Case Volume of EndoscopistCase Volume of Endoscopist

ERCP ComplicationsERCP Complications
Pancreatitis: 6.7%* Perforation: 0.3% Cholangitis: <1% Cardiopulmonary / sedation: <1% Failed procedure
*Freeman ML et al GIE 2001

Causes of Post-ERCP PainCauses of Post-ERCP Pain
Pancreatitis Transient Pain Cholangitis Perforation

Post-ERCP Pain: What does it mean?Post-ERCP Pain: What does it mean?
Pain at 2 hrs post-ERCP*: 2/3 of pts developed pancreatitis 1/3 of pts who did not get pancreatitis Recovery room pain not very specific
33% of panc. presents >4hrs post-ERCP** Admission required in 12% with >1 risk factor
and 4% without any
*Gottlieb GIE 1996 **Freeman NEJM 1996

Post-ERCP Pancreatitis Post-ERCP Pancreatitis
Definition requires all 3: New or worsened pain amylase 3X ULN > 24 hrs post-ERCP requiring >2 days hospitalization
Severity: Mild: <4 days hospitalization Moderate: 4-10 d. hospitalization Severe: >10 d. hospitalization

Risk Factors for Post-ERCP Risk Factors for Post-ERCP PancreatitisPancreatitis
Patient specific risks Odds ratio
Prior ERCP-induced pancreatitis 5.4
Suspected SOD 2.6
Female gender 2.5
Absence of chronic pancreatitis 1.9
Normal bilirubin 1.9

Risk Factors for Post-ERCP Risk Factors for Post-ERCP PancreatitisPancreatitis
Technique specific risks Odds ratio
Difficult cannulation 3.4
Pancreatic injection (>1) 2.7
Sphincter balloon dilation 4.5
Pancreatic sphincterotomy 3.1

Risks for Pancreatitis: Prospective Risks for Pancreatitis: Prospective US Multi-Center Study*US Multi-Center Study*
Multivariate risk factors Odds RatioMinor sphincterotomy 3.8Suspected SOD 2.6Prior ERCP-pancreatitis 2.0Age <60 1.62 or more pancreatic injections 1.5Trainee involvement 1.5
Not risk factors: female gender, idiopathic pancreatitis,difficult cannulation, major sphincterotomy, SOM
*Cheng AJG 2006

Does SOM Increase Procedure-Induced Does SOM Increase Procedure-Induced Pancreatitis?Pancreatitis?
Suspected SOD pts: ERCP with SOM vs. ERCP alone—No
differences in pancreatitis rates (26%)* Compared to 3% rate in bile duct stone pts Pancreatitis risk increased by ES and
pancreatography
Conclusion: It’s the diagnosis (suspected SOD) not the manometry that increases risk
*Singh GIE 2004

Medications to Lower Medications to Lower Post-ERCP PancreatitisPost-ERCP Pancreatitis
Gabexate mesylate Allopurinol
Somatostatin Glyceryl trinitrate
Octreotide Glucagon
IL-10 Calcitonin
Nifedipine Heparin
Prednisone Beta-carotene
Lidocaine spray*Diclofenac / Indomethacin
N-acetylcysteine **Ulinastatin
*4 positive / 1 negative studies **Single positive study

NSAID Meta-analysisNSAID Meta-analysis
4 RCTs: 879 patients* Diclofenac / indomethacin vs. placebo Relative risk of pancreatitis: 0.35 65% decrease in pancreatitis, 90%
decrease in severe pancreatitis NNT to prevent one episode: 15
*Elmunzer Gut 2008

Techniques to Lower Post-ERCP Techniques to Lower Post-ERCP PancreatitisPancreatitis
Wire cannulation instead of contrast* Temporary PD stenting Not clearly shown to be helpful:
Post-biliary ES botox Pure cut cautery may be safer than blended cut Low osmolality contrast
* Lella GIE 2004

Temporary Pancreatic StentingTemporary Pancreatic Stenting
RCT: Stent lowers risk in biliary SOD pts* Used for other high risk cases Single pigtail flangeless 3F stents appear
safer and more effective** Spontaneous stent passage: 70-85% Successful placement in 4 studies=88%
*Tarnarsky Gastroenterology 1998 ** Rashdan Clin Gastro & Hep 2004

Stenting to Minimize PancreatitisStenting to Minimize PancreatitisMeta-AnalysisMeta-Analysis
Singh P. GIE 2004;60:544.

Problems with Prophylactic PD StentProblems with Prophylactic PD Stent
Technical difficulty in placement Small stents require 0.018 guide wire
Increased risk in failed stent placement May require repeat endoscopy Increased cost Possible stent-induced damage Lack of expert agreement on methods

Survey on PD Stents: Survey on PD Stents: Who should get one? Which one?Who should get one? Which one?
Agreed upon indications: SOD Pancreatic sphincterotomy (minor & major) Ampullectomy
Indications according to some: Pre-cut sphincterotomy (71%) Prior post-ERCP pancreatitis (64%) Suspected SOD / normal or no manometry (60%) Traumatic or difficult cannulation (44%)
No agreement on stent size and length, how long stents left, and retrieval methods
*Brackbill GIE 2006

Post-ERCP Pancreatitis: Post-ERCP Pancreatitis: ConclusionsConclusions
Most common complication, 1/3 pts. take > 4hrs to present
Patient-related and technique-related risk factors are major determinants of risk
Limit pancreatic injection / wire for cannulation
Temporary PD stenting for high risk pts

Endotherapy for the PancreasEndotherapy for the Pancreas
Indications: Acute idiopathic pancreatitis Chronic pancreatitis pain

Idiopathic Acute Pancreatitis:Idiopathic Acute Pancreatitis:Possible EtiologiesPossible Etiologies
Microlithiasis / missed stones in GB / ducts Pancreas divisum Sphincter of Oddi dysfunction Neoplasms Subtle chronic pancreatitis Autoimmune / genetic pancreatitis Missed diagnosis of hypertriglyceridemia or
hypercalcemia

Idiopathic Pancreatitis:Idiopathic Pancreatitis:Possible Additional LabsPossible Additional Labs
Cystic fibrosis genotype Positive in 20% (range: 4-37%)
CA19-9 in suspected cancer ANA and IGG4 subtype Ionized serum calcium / parathormone FH: trypsinogen gene and Spink1 Repeat non-fasting triglyceride

Idiopathic Pancreatitis: Idiopathic Pancreatitis: Diagnostic ChoicesDiagnostic Choices
Diagnostic Choices Wait for second episode EUS MRCP +/- secretin stimulation ERCP with manometry Empiric cholecystectomy
Factors affecting choice Age= >40 years: 21% had neoplasm* Absent gallbladder
*Choudhari AJG 1998

What is the role of Microlithiasis?What is the role of Microlithiasis?
Microlithiasis: small (1-2 mm) stones Sludge: Collection of crystals,
mucin, glycoproteins, and cellular debris
Sludge may contain microlithiasis: terms used interchangeably clinically

Microlithiasis in IAP: Microlithiasis in IAP: Gallbladder in SituGallbladder in Situ
High incidence (60-80%) centers of IAP due to microlithiasis
Low incidence (6-8%) centers
Evaluation/Rx options: Empiric cholecystectomy / trial of Urso Bile crystal analysis: sensitivity 66% EUS: Superior to crystal analysis*
*Dahan Gut 1996

Does Microlithiasis cause Does Microlithiasis cause IAP Post Cholecystectomy?IAP Post Cholecystectomy?
Bile crystals rare in biliary SOD* No biliary crystals in IAP pts**Conclusion: Bile duct Stones /
microlithiasis are very rare cause of IAP post-cholecystectomy, best diagnosed by EUS***
*Quallich GIE 2001 **Law GIE 2002 ***Scheiman AJG 2001

Acute Idiopathic Pancreatitis Acute Idiopathic Pancreatitis Diagnostic TestsDiagnostic Tests
EUS Accurate for P. divisum, tumors, bile duct or
gallbladder stones Pro: Safe Con: Not therapeutic, miss SOD
MRCP Accurate for P. divisum, variable accuracy for
tumors and missed stones, miss SOD + Secretin: Improve image quality but value of P.
duct dilation / flow is controversial

Diagnostic Yield of EUS in IAPDiagnostic Yield of EUS in IAP
*Yusoff GIE 2004
EUS FindingNo cholecystec.
(n=246)Post-cholecystec.
(n=124)
Stones (GB or BD) 7% 3%
GB Sludge 11% -
Pancreas division 5% 11%
IPMN/neoplasm 2.8% 4.8%
Chronic pancreatitis (≥5 criteria)
31% 27%
Other 4.8% 4.8%

Chronic Pancreatitis Chronic Pancreatitis Presenting as IAPPresenting as IAP
“Small duct” or minimal change Difficult diagnosis
EUS: need > 5 criteria for certainty Panc func tests: Also has accuracy issues
Treatment options: Medical therapy first ? Value to endoscopic therapy Surgery relegated to resection

EUS Diagnostic Accuracy in Chronic EUS Diagnostic Accuracy in Chronic PancreatitisPancreatitis
Number of EUS criteria only weakly correlated with fibrosis score*
>3 criteria: 80% sensitive & specific EUS true cut and FNA also have poor
specificity (65%) Only moderate interobserver
agreement on individual criteria***Chong GIE 2007 **Wallace GIE 2001

EUS in IAP PatientEUS in IAP Patient

Endotherapy for P. DivisumEndotherapy for P. Divisum

Pancreas Divisum Pancreas Divisum TreatmentTreatment
Pancreas divisum as cause of IRP Rx outcome: 127 pts in 8 series81% no
further episodes in mean f/u of 27 mo Long term (61 mos) f/u of 28 IRP pts*
23 cured, 5 better, 3 repeated ERCP NK vs traction sphincterotome?**
Restenosis rate: 13% NK vs 25% TS
*Alsolaiman T1528 GIE 04 **Berkes T1532 GIE 04

Acute pancreatitis can be a Acute pancreatitis can be a neoplastic presentationneoplastic presentation
Ampullary neoplasm Ductal cancer / isolated MPD
stricture IPMN Islet cell / metastatic cancer

Ampullary NeoplasmAmpullary Neoplasm

Pancreatic Duct StricturePancreatic Duct Stricture

EUS of Case: EUS of Case: Early Pancreatic CancerEarly Pancreatic Cancer

Intraductal Papillary Mucinous Intraductal Papillary Mucinous Neoplasm: IPMN Neoplasm: IPMN

SO AnatomySO Anatomy

Does SOD cause Does SOD cause Idiopathic Acute Pancreatitis?Idiopathic Acute Pancreatitis?
Pro: Present in 30-60% of IAP pts Pts with panc. SOD more likely to get
post-ERCP pancreatitis than those with normal SOM (26% vs. 7%)*
60-80% IAP pts improve after sphincter ablation
*Tarnasky Gastroenterology 1998

Does SOD cause Does SOD cause Idiopathic Acute Pancreatitis?Idiopathic Acute Pancreatitis?
Pro: Present in 30-60% of IAP pts Pts with panc. SOD more likely to get
post-ERCP pancreatitis than those with normal SOM (26% vs. 7%)*
60-80% IAP pts improve after sphincter ablation
*Tarnasky Gastroenterology 1998

Contemporary* Classification Contemporary* Classification for Suspected Pancreatic SODfor Suspected Pancreatic SOD
Type I -Pancreatic type pain
-Amylase/lipase elevation
-Dilated Pancreatic duct
Type II -Pancreatic type pain
-Either abnormal pancreas enzymes or duct
dilation
Type III -Pancreatic type pain only*Classic System includes delayed drainage >8 min

Why Pancreatic SOD Why Pancreatic SOD Classification is Not UsefulClassification is Not Useful
Few Type I pts reported, most IAP pts have normal PD caliber
IAP pts fit into Type II category and are primary pts of interest
Type III—an uncertain diagnosis

Pancreatic SOD Therapy ChoicesPancreatic SOD Therapy ChoicesWhat Type of Sphincterotomy?What Type of Sphincterotomy?
Biliary ES: Proposed as safer 1st step* Dual purpose: treats microlithiasis and
lowers panc SO pressure somewhat Efficacy is only 28-50% Higher failure rate than panc or dual ES
*Levy AJG 2001

Pancreatic SOD Therapy ChoicesPancreatic SOD Therapy ChoicesWhat Type of Sphincterotomy?What Type of Sphincterotomy?
Pancreatic ES alone Treats correct portion of SO Creates small biliary ES
Complete dual ES Surgical sphincteroplasty Insufficient data to support clear
superiority for any method

65 yo woman, 3 episodes of 65 yo woman, 3 episodes of IARP in one yearIARP in one year

Idiopathic Acute Pancreatitis↓
R/0 autoimmune / genetic pancreatitis↓
EUS → diagnosis/treatment ↓ no diagnosisERCP with manometry for >1 attack
Algorithm for IARPAlgorithm for IARP

Pancreatic Endotherapy for Chronic Pancreatic Endotherapy for Chronic PancreatitisPancreatitis
Duct disruptions, pancreatic ascites Pseudocyst drainage
Per ampulla-communicating cysts Transluminal stents
Treatment of chronic pain Stone clearance Stricture treatment

Stent for Duct DisruptionStent for Duct Disruption
Resolution: 60-80% Bridge disruption Less success in AP

Rules for Endoscopy of Rules for Endoscopy of Pancreatic PseudocystsPancreatic Pseudocysts
Symptomatic True PP-not acute fluid
collections (<4 wks) EUS to assess wall (<10 mm) &
R/O vessels Antibiotic coverage Surgical back-up

Endotherapy for Endotherapy for Pseudocysts - Outcome*Pseudocysts - Outcome*
Resolution Complication
Chronic PP 92% 17%
Acute PP 74% 19%
Panc necrosis
72% 37%
PFC recurrence=16% with 766 d f/u
*Baron GIE 2002

Endotherapy of MPD Stones & Endotherapy of MPD Stones & Chronic Pancreatitis PainChronic Pancreatitis Pain
Pancreatic duct stones Rx Usually requires ESWL
1.5 sessions / pt Stone clearance:
Complete 40%; partial 40%; failure 20%
Pain relief outcome: 75% with complete clearance 40% with partial clearance

Endotherapy for Chronic Endotherapy for Chronic Pancreatitis PainPancreatitis Pain
Case series:Pain relief: 45-74% RCT surg vs endotherapy in 72 pts*
Initial success similar 5 yr f/u: Pain relief 86% vs 61%
RCT surg vs endotherapy in 39 pts** 2 yr f/u: Pain relief 75% vs 32%
*Dite Endoscopy 2003 **Cahen NEJM 2007

Complications of Pancreatic Complications of Pancreatic EndotherapyEndotherapy

Complications of Pancreatic Complications of Pancreatic EndotherapyEndotherapy
Procedure-induced pancreatitis High risk in IAP--odds ratio=1.9
Stenosis of pancreatic ES: 13-25% Risk greater for traction type
Stent-induced ductal changes Infect a cyst Misc: bleeding, perforation, sedation

Pancreatic EndotherapyPancreatic EndotherapyConclusion Conclusion
Acute & chronic pancreatitis indications
50-80% chance of benefit depending on specific indication
15-20% complication rate RCTs needed