Embed Size (px)
Citation preview
Equipment Options and
Positioning Recommendations to
Encourage “Hip Health”
Michele E. Audet, MMSc,PT,ATP/SMS
Children’s Healthcare of Atlanta
Hip – Cerebral Palsy
• Children with cerebral palsy are rarely born with hip dysplasia.
• Developmental hip dysplasia is a very commoncomplication of children with cerebral palsy and canlead to significant disability and pain.
Children’s Healthcare of Atlanta
Hip Development
• Growth of a child’s hip occurs in a sequential process from embryo up to adolescence.
• Cartilage in the acetabulum serves to deepen the hip socket resulting in more complete coverage of the femoral head = More stable hip.
Children’s Healthcare of Atlanta
Hip Development
• Development of the acetabulum is dependent uponarticulation of the femoral head in the acetabulum and is promoted through Weight Bearing.
• Zeng,S., et.al., (2013), Coverage of femoral head at weight-bearing interface of the hip joint in children: an MRI analysis. Open J. of Medical Imaging, 3, 60-64.
Children’s Healthcare of Atlanta
Normal Hip With Cartilage
• (Image removed due to copyright policy)
Children’s Healthcare of Atlanta
Definition Hip Displacement
• Gradual, lateral displacement of the femoral headfrom under the acetabulum.
• Hip displacement often used interchangeably withhip subluxation.
6
Children’s Healthcare of Atlanta
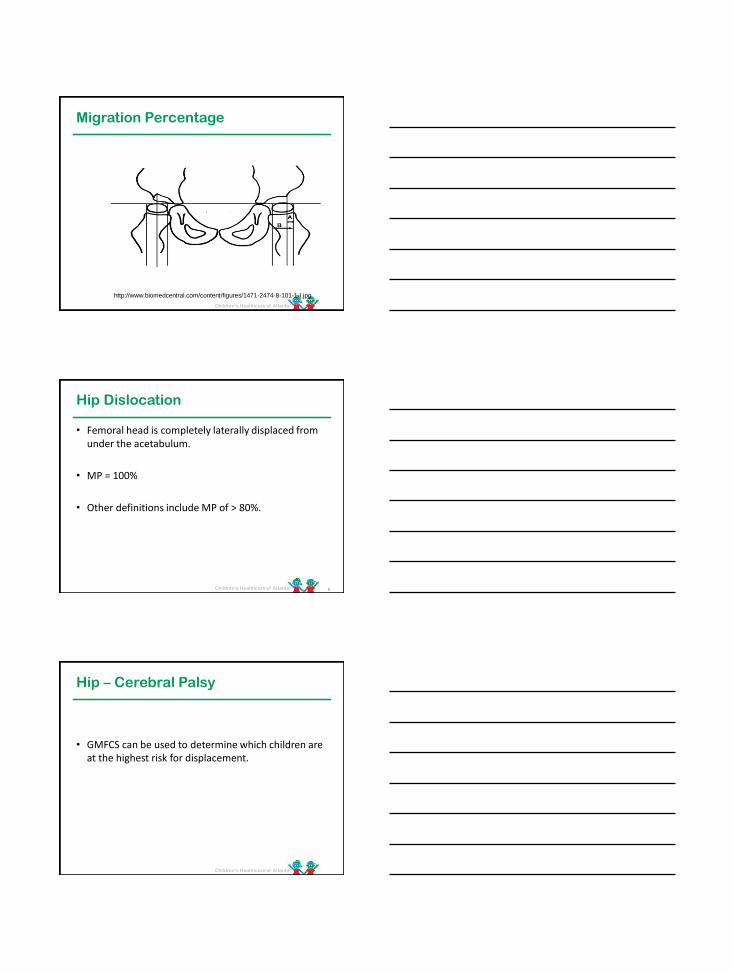
Migration Percentage
http://www.biomedcentral.com/content/figures/1471-2474-8-101-1-l.jpg
Children’s Healthcare of Atlanta
Hip Dislocation
• Femoral head is completely laterally displaced fromunder the acetabulum.
• MP = 100%
• Other definitions include MP of > 80%.
8
Children’s Healthcare of Atlanta
Hip – Cerebral Palsy
• GMFCS can be used to determine which children are at the highest risk for displacement.
Children’s Healthcare of Atlanta
Hip Displacement - CP
• Soo et. al. -374 children with CP in Australia bornbetween 1990 and 1992.
• Mean follow-up 11 years, 8 months.
• Incidence of hip displacement entire group was 35%.
• Incidence GMFCS Level I =0%. Level V = 90%
Soo, B., Howard, J., Boyd, R., et.al. (2006), Hip stability in cerebral palsy. J. Bone Joint Surg AM, Jan (88)1, 121-129.
Children’s Healthcare of Atlanta
Hip Displacement - CP
• Hagglund et.al. – 212 children with cerebral palsy in Sweden.
• Followed using X-rays until age 9-16 years old.
• 27% developed hip displacement > 33% and of these 18% showed displacement > 40%.
Hagglund, G., Lauge-Pederson, H., and Wagner, P., (2007), Characteristics of children with hip displacement in cerebral palsy. BMC Musculoskelet Disord, Oct (26)8,101.
Children’s Healthcare of Atlanta 12
Children’s Healthcare of Atlanta
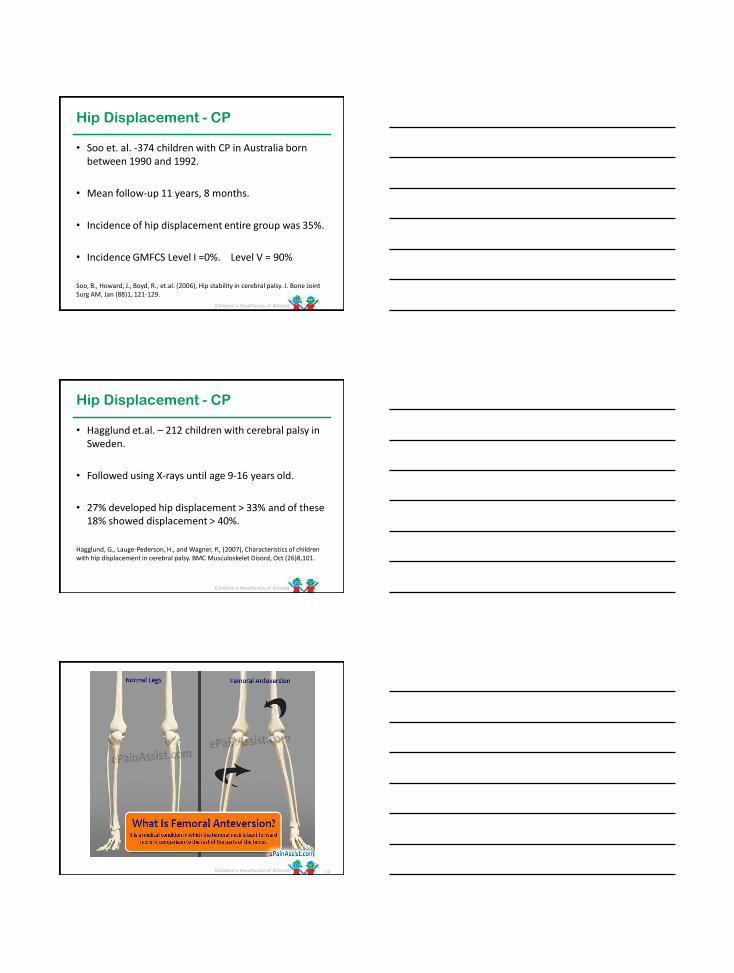
Femoral Anteversion and CP
• 147 children (267 hips) of children with CP studied.
• Early ages, angle of femoral anteversion similar to typically developing peers.
• As age, typical children’s angles decreased to normal adult degrees.
• CP children showed minimal change in degree of anteversion.
Bobroff,ED; Chambers,HG et.al.(1999), Femoral anteversion and neck shaft angle in children with cerebral palsy. Clin Orthop Relat Res, July (364), 194-204.
13
Children’s Healthcare of Atlanta
Coxa Valga
14
(Image removed due to copyright policy)
Children’s Healthcare of Atlanta
Who Is At Risk?
• GMFCS Levels IV and V are highest risk.
• Level III lesser risk but need monitoring.
15
Children’s Healthcare of Atlanta
• 1. Asymmetries:
– Muscle Imbalances
– Range of motion limitations, especially at hips and knees.
– Spasticity
– Adduction contractures can directly lead to changes in the acetabulum and femur.
2. Lack of Normal Weight Bearing
16
Risk Factors
Children’s Healthcare of Atlanta
Intervention
• 1. Tone Management
• 2. Postural management
• 3. Therapy
• Orthoses and Splinting
17
Children’s Healthcare of Atlanta
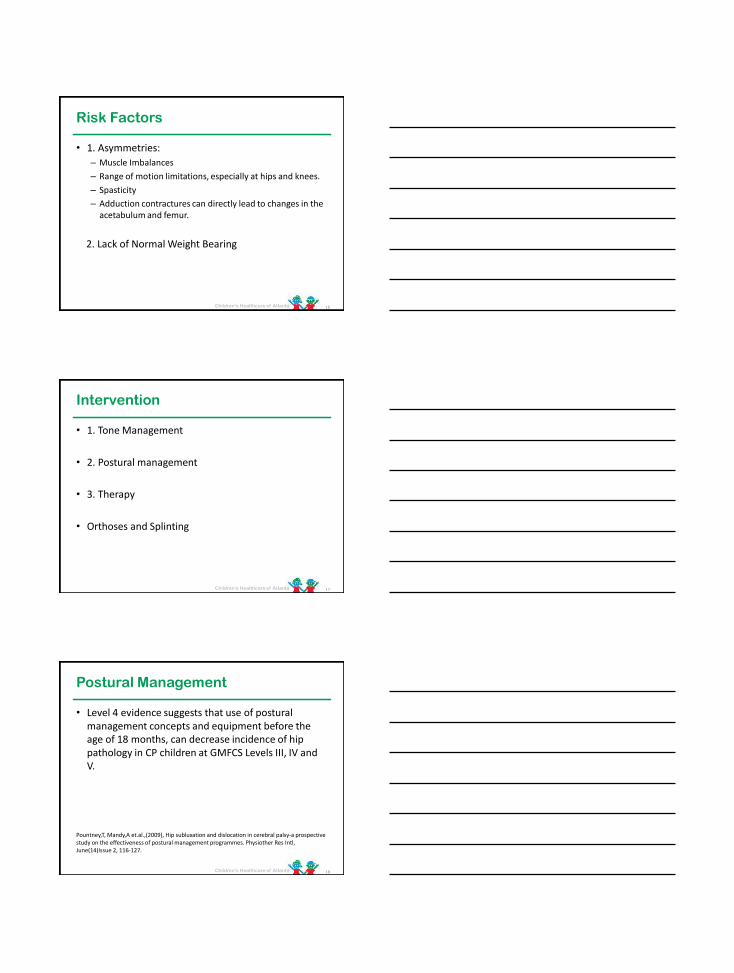
Postural Management
• Level 4 evidence suggests that use of postural management concepts and equipment before the age of 18 months, can decrease incidence of hip pathology in CP children at GMFCS Levels III, IV andV.
Pountney,T, Mandy,A et.al.,(2009), Hip subluxation and dislocation in cerebral palsy-a prospective study on the effectiveness of postural management programmes. Physiother Res Intl, June(14)Issue 2, 116-127.
18
Children’s Healthcare of Atlanta
Positioning
• The following areas need to be addressed:
– Lying Support
– Seating
– Standing
19
Children’s Healthcare of Atlanta
Standing
• Goal:
– Symmetry
– Neutral pelvis in terms of tilt, rotation and obliquity
– Hips in ABDUCTION
– Hips and knees in full extension
20
Children’s Healthcare of Atlanta
Why Abduction?
• (Image removed due to copyright policy)
Children’s Healthcare of Atlanta
Martinsson and Himmelmann
• Non-ambulatory children with CP, GMFCS levels III-V.
• 1 year of straddled weight bearing in maximumtolerated hip extension and abduction.
• Controls matched for age, motor ability and surgery.
Martinsson, C., Himmelmann, K., (2011), Effect of weight bearing in abduction and extension on hip stability in children with cerebral palsy, Pediatr Phys Ther, Summer 23(2), 150-157.
Children’s Healthcare of Atlanta
Dosing
• 1. Bone Mineral Density – 60-90 minutes/day
• 2. Hip Stability – 60 minutes in 30-60 degrees bilateral hip abduction.
• 3. Range of Motion of Hip Knee and Ankle – 45 to 60 minutes.
• 4. Spasticity – 30 to 45 minutes.
Children’s Healthcare of Atlanta
Systematic Review Dosage
Paleg, G., Smith, A., Glickman, L., (2013), Systematic review and evidence-based clinical recommendations for dosing of pediatric supported standing programs. Ped Phys Ther, 25, 232-247.
Paleg, G., Livingstone, R., (2015), Systematic review and clinical recommendations for dosage of supported home-based standing programs for adults with stroke, spinal cord injury and other neurological conditions. BMC Musculoskeletal Disorders, 16:358.
Children’s Healthcare of Atlanta
Sitting
• Goal:
– Symmetry
– Neutral pelvis in terms of tilt, rotation and obliquity.
– Hips in ABDUCTION
25
Children’s Healthcare of Atlanta
Lying
• Symmetry
• Hips in Abduction
• Comfort
26
Children’s Healthcare of Atlanta
When Equipment Considered
• Lying Supports – As soon after birth as possible.
• Sitting programs – About age 6 months.
• Standing – Age 10 to 12 months.
27
Children’s Healthcare of Atlanta 28
Scanned by CamScanner
Children’s Healthcare of Atlanta
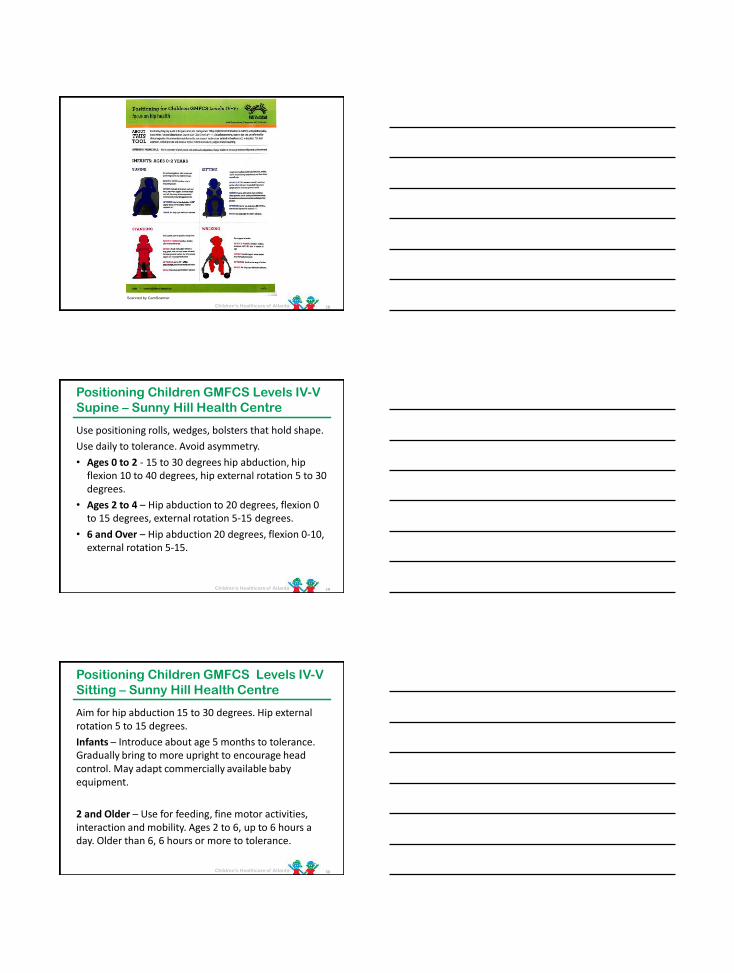
Positioning Children GMFCS Levels IV-V
Supine – Sunny Hill Health Centre
Use positioning rolls, wedges, bolsters that hold shape.
Use daily to tolerance. Avoid asymmetry.
• Ages 0 to 2 - 15 to 30 degrees hip abduction, hip flexion 10 to 40 degrees, hip external rotation 5 to 30 degrees.
• Ages 2 to 4 – Hip abduction to 20 degrees, flexion 0 to 15 degrees, external rotation 5-15 degrees.
• 6 and Over – Hip abduction 20 degrees, flexion 0-10, external rotation 5-15.
29
Children’s Healthcare of Atlanta
Positioning Children GMFCS Levels IV-V
Sitting – Sunny Hill Health Centre
Aim for hip abduction 15 to 30 degrees. Hip external rotation 5 to 15 degrees.
Infants – Introduce about age 5 months to tolerance. Gradually bring to more upright to encourage head control. May adapt commercially available baby equipment.
2 and Older – Use for feeding, fine motor activities, interaction and mobility. Ages 2 to 6, up to 6 hours a day. Older than 6, 6 hours or more to tolerance.
30
Children’s Healthcare of Atlanta
Positioning Children GMFCS Levels IV-V
Standing – Sunny Hill Health Centre
• Use supine, prone, upright or sit to stand standers.
• Under 2 – Introduce about age 10 months. Aim toward 15 + degrees hip abduction. Daily per tolerance.
• Ages 2 and Older – Hip abduction 15 to 30 degrees.Avoid 0 degree hip abduction. Use daily 60 to 90 minutes.
31
Children’s Healthcare of Atlanta
Positioning Children GMFCS Levels IV-V
Walking – Sunny Hill Health Centre
Supportive Walker/Gait Trainer
• Introduce for Level IV children after 10 months as appropriate.
• Provide support where needed from head down.
• Aim for active range of motion.
• Daily as per tolerance.
32
Children’s Healthcare of Atlanta
24 Hour Postural Care
• Literature shows strong correlation between postural asymmetries and hip displacement, scoliosis, kneeflexion contractures.
• At least 1/3 of 24 hour day, is spent lying down/sleeping.
• Basis of this approach is to support the person in comfortable, well aligned, symmetrical positionthroughout day and night.
33
Children’s Healthcare of Atlanta
Montana Postural Care Project
• Pilot program funded by the Montana Council onDevelopmental Disabilities.
• Purpose: “Introduce 24 hour postural care as apractical approach for people with motor impairments in a large rural state with limited special services, while examining the results in the population served.”
Tamara Kittleson-Aldred, (2017), Montana Postural Care project: a 24 hour postural care model, Proceedings of the 33rd International Seating Symposium, Mar 2-4, 2017.
34
Children’s Healthcare of Atlanta
Montana Project
• Participants: 30 people with physical impairments/spasticity.
• Training: 1 day course for all participants including therapists, caretakers, nurses, etc.
• Evaluation: Half day in home for each individual person in study. Included Goldsmith Indices of Bodysymmetry (GIoBS), Pittsburgh Sleep Quality Index, Pediatric Pain Profile or other pain scale.
35
Children’s Healthcare of Atlanta
Montana Project
• Night Time Care Plan formulated.
• Provided: 4 postural supports
– Non-slip mesh
– Pressure relieving airflow mattress pad
– 2 types lateral supports (usually included a leg positionerof some kind)
– Additional household items (rolled towels, stuffed animals, cushions)
Photos Taken --- Ongoing support as needed.
36
Children’s Healthcare of Atlanta
Montana Project
• Results:
– 80% improvement sleep quality vs. 0% controls.
– 80% improved body symmetry vs. 0% controls.
– 50% participants with pain issues, had lower pain scores.
• Anecdotal:
– Most common report was improved day time alertness.
– Several people who did not tolerate the full posturalassessment at initial evaluation, tolerated at final follow up.
37
Children’s Healthcare of Atlanta
Surveillance
• Whole child oriented
– Includes tone management, gross and fine motor development, hip and spine surveillance.
• Levels III to V GMFCS - Ortho
– Radiographs hips annually starting 1 year to 8 years.
– After 8, radiographs as needed.
– MP calculated all radiographs
– CPUP Hip Score
– Hips at risk dislocation, MP > 40% surgery considered early.
38
Children’s Healthcare of Atlanta
Surveillance - Therapy
• Evaluation 2 times/year until age 6, then annually
• Evaluation includes joint range of motion using agoniometer, and clinical evaluation of spine.
• Goal: early detection of contractures and deformities to allow for early non-surgical treatments.
• Treatment includes:
– Postural management
– Orthotics and assistive devices
– Individual training
– Spasticity management
39

Children’s Healthcare of Atlanta
CPUP Program
40