Embed Size (px)
Citation preview



Equine Veterinary Nursing


Equine Veterinary Nursing
Second Edition
Karen M CoumbeMA VetMB CertEP CertVA MRCVSBell Equine Veterinary ClinicMereworthNear MaidstoneKentUK
For the BRITISH EQUINE VETERINARY ASSOCIATION
A John Wiley & Sons, Ltd., Publication

This edition first published 2012 © 2001 by Blackwell Science Ltd, 2012 by John Wiley & Sons Ltd
Wiley-Blackwell is an imprint of John Wiley & Sons, formed by the merger of Wiley’s global Scientific, Technical and Medical business with Blackwell Publishing.
Registered office: John Wiley & Sons, Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
Editorial offices: 9600 Garsington Road, Oxford, OX4 2DQ, UK The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK 2121 State Avenue, Ames, Iowa 50014-8300, USA
For details of our global editorial offices, for customer services and for information about how to apply for permission to reuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwell.
The right of the author to be identified as the author of this work has been asserted in accordance with the UK Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by the UK Copyright, Designs and Patents Act 1988, without the prior permission of the publisher.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The publisher is not associated with any product or vendor mentioned in this book. This publication is designed to provide accurate and authoritative information in regard to the subject matter covered. It is sold on the understanding that the publisher is not engaged in rendering professional services. If professional advice or other expert assistance is required, the services of a competent professional should be sought.
Library of Congress Cataloging-in-Publication Data
Equine veterinary nursing / [edited by] Karen M. Coumbe. – 2nd ed. p. ; cm. Rev. ed. of: Equine veterinary nursing manual / edited by Karen M. Coumbe. 2001. Includes bibliographical references and index. ISBN 978-0-470-65655-6 (pbk. : alk. paper) 1. Horses–Diseases. 2. Veterinary nursing. I. Coumbe, Karen. II. British Equine Veterinary Association. III. Equine veterinary nursing manual. [DNLM: 1. Horse Diseases–nursing. 2. Animal Technicians. SF 951] SF951.E68 2012 636.1'089–dc23
2012014813
A catalogue record for this book is available from the British Library.
Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not be available in electronic books.
Cover images: courtesy of Karen Coumbe, Nick Bolas and Bonny MillarCover design by optadesign.co.uk
Set in 9/11.5 pt Sabon by Toppan Best-set Premedia Limited
01 2012

v
Contents
List of contributors, vii
Foreword, ix
Preface to the second edition, x
Abbreviations and Acronyms, xi
1 Basic equine management, 1W. Linnenkohl & D.C. Knottenbelt
2 Anatomy and physiology, 25P.D. Clegg, N. Townsend & R.C. Conwell
3 Genetics, 69G. Munroe
4 Reproduction, 78J.F. Pycock
5 Nutrition, 97P.A. Harris
6 Clinical nutrition, 121P.A. Harris
7 Basic first aid, 134M. Smith & S.J. Haylock
8 General nursing, 153K. Snalune & A. Paton
9 Safety management in the practice, 176A. Jones & A. Barr
10 The equine nurse’s professional responsibilities, 184S. Pullen
11 Medicines and their management, 191C.A. Roberts, L. Loines & K. Tillett
12 Laboratory diagnostics, 201R.J. Naylor, L.L. Hillyer & M.H. Hillyer
13 Fluid therapy, 226V.E.N. Copas & J.C. Boswell
14 Medical nursing, 246J.D. Slater & E.J. Knowles
15 Foal nursing, 286S.J. Stoneham

CONTENTS
vi
16 Equine orthopaedic nursing, 303E.D. Barr & E. Jones
17 Diagnostic imaging, 332M.A. Smith, K. Holmes & N. Turley
18 General surgical nursing, 382S. Boys Smith & B.M. Millar
19 Theatre practice, 407D.P. McHugh
20 Anaesthesia, 432J.C. Murrell & V. Ford-Fennah
Index, 461

vii
List of contributors
Alistair Barr MA VetMB PhD MRCVS DVR DEO DipECVS
Dept of Clinical Veterinary Science, Division of Companion Animals, University of Bristol, Langford, Somerset
Elizabeth Barr BVMS PhD CertES(Orth) DipECVS MRCVS
Bell Equine Veterinary Clinic, Mereworth, Kent
Jane Boswell MA VetMB CertVA CertES(Orth) DipECVS MRCVS
The Liphook Equine Hospital, Liphook, Hampshire
Sarah Boys Smith MA VetMB CertES(Orth) DipECVS MRCVS
Rossdales Equine Hospital & Diagnostic Centre, Newmarket, Suffolk
Peter Clegg MA VetMB PhD CertES DipEVCS MRCVS
University of Liverpool Veterinary School, Liverpool, Cheshire
Rachael Conwell BVetMed, Cert EM (Int Med), DipECEIM, MRCVS
Equimed Referrals Ltd, Tadcaster, North Yorkshire
Victoria Copas MA VetMB CertAVP (EM) MRCVS
The Liphook Equine Hospital, Liphook, Hampshire
Vicky Ford-Fennah BSc RVN VNPA
University of Bristol Veterinary School, Langford, Bristol
Pat Harris MA VetMB PhD DipECVCN MRCVS
Equine Studies Group, WALTHAM Centre for Pet Nutrition, Waltham-on-the-Wolds, Leicestershire
Sophie J. Haylock REVN
Newmarket Equine Hospital, Newmarket, Suffolk
Lynn Hillyer BVSc CertEM (IntMed) MRCVS British Horseracing Authority, London
Mark Hillyer BVSc PhD DipECVS DipECEIM MRCVS
Newmarket Equine Hospital, Newmarket, Suffolk
Katie Holmes BSc REVN EVN
Newmarket Equine Hospital, Newmarket, Suffolk
Alan Jones BSc NEBOSH CertSchool of Veterinary Science, University of Bristol,
Langford, Somerset
Emma Jones MA VetMB VertES(Orth) MRCVS
Abbey Veterinary Centre, Llanover, Monmouthshire
Derek Knottenbelt OBE BVM&S DipECEIM MRCVS
Philip Leverhulme Equine Hospital, University of Liverpool, Liverpool, Cheshire
Edd Knowles MA VetMB MRCVS
Bell Equine Veterinary Clinic, Mereworth, Kent
Whitney Linnenkohl DVM
Department of Clinical Science, Cornell University, Ithaca, New York, USA
Linda LoinesBell Equine Veterinary Clinic, Mereworth, Kent
Dawn McHugh BA DipAVN(Surgical) RVN REVN
Newmarket Equine Hospital, Newmarket, Suffolk

List of contributors
viii
Bonny Millar CVT(USA) REVN EVN
Rossdales Equine Hospital & Diagnostic Centre, Newmarket, Suffolk
Graham Munroe BVSc PhD CertEO DESM DipECVS FRCVS
Flanders Veterinary Services, Greenlaw, Berwickshire
Jo Murrell BVSc PhD DipEVCA CertVA MRCVS
University of Bristol Veterinary School, Langford, Bristol
Rosie Naylor BVetMed DipACVIM MRCVS
Centre for Veterinary Nursing, Royal Veterinary College, North Mymms, Hertfordshire
Anna Paton REVN
Queens Veterinary School Hospital, University of Cambridge, Cambridge, Cambridgeshire
Sophie Pullen BSc(Hons) CertEd RVN
Centre for Veterinary Nursing, Royal Veterinary College, North Mymms, Hertfordshire
Jonathan Pycock BVetMed PhD DESM MRCVS
Equine Reproductive Services, Messenger Farm, Ryton, North Yorkshire
Colin Roberts BVSc MA PhD FRCVS
Sidney Sussex College, Cambridge, Cambridgeshire
Josh Slater BVM&S PhD MRCVS
Equine Medicine & Surgery Group, Royal Veterinary College, North Mymms, Hertfordshire
Matt Smith BVetMed CertES(orth) DEO DipECVS MRCVS
Newmarket Equine Hospital, Newmarket, Suffolk
Meredith Smith MA VetMB PhD CertES DipECVS AECVDI MRCVS
Newmarket Equine Hospital, Newmarket, Suffolk
Katie Snalune BSc MA VetMB CertEM (Int Med) CertES (Soft Tissue) MRCVS
Queens Veterinary School Hospital, University of Cambridge, Cambridge, Cambridgeshire
Sarah Stoneham BVSc CertESM MRCVS
Lone Oak Stud, Hilborough, Norfolk
Kelly Tillett REVN
Bell Equine Veterinary Clinic, Mereworth, Kent
Neil Townsend BSc BVSc CertES (Soft Tissue) MRCVS
University of Liverpool Veterinary School, Liverpool, Cheshire
Nia Turley BSc(Hons)Newmarket Equine Hospital, Newmarket, Suffolk

ix
Foreword
I am delighted to have the opportunity to write the foreword to the second edition of this seminal book on Equine Veterinary Nursing. Much has happened in the world of equine nursing since the highly suc-cessful first edition. Perhaps most importantly the Royal College of Veterinary Surgeons (RCVS) has recognised officially the nursing of equidae, and there is now a firmly established direct-entry equine nursing diploma. The RCVS holds a non-statutory register and there is a published Guide to Professional Conduct for Veterinary Nurses, to mirror that for veterinary surgeons. At the time of writing, the RCVS is replacing this Guide with a Code of Professional Conduct for Veterinary Nurses.
Since 2002, the Veterinary Nurses Council has replaced the old Veterinary Nurses Committee and this RCVS council has created a disciplinary and pre-liminary investigation committee to deal specifically with veterinary nurses. The Veterinary Defence Society has therefore established a professional indemnity insurance policy for veterinary nurses, to support registered nurses in any potential action against them. We have seen the first nursing graduates from the courses at the Universities of Bristol and Middlesex. The decade has also seen the appointment of the first Professor of Veterinary Nursing in the UK, at the Royal Veterinary College, and the first qualified equine veterinary nurse to become President of the British Veterinary Nursing Association.
Such changes have afforded veterinary nurses a new professional confidence and a stronger voice to speak on their own behalf. However, with this increase in profile comes an increased responsibility for equine nurses to be correctly trained and to act in a manner becoming to a professional person, rather than merely as an employee, whose actions can only be called to account under the aegis of a veterinary surgeon. I cannot pretend that this has been an easy journey, nor yet that all the ‘i’s have been dotted or the ‘t’s crossed. For example, there is still a major issue regarding
whether such changes require legislation to empower them, or whether they might be enacted under the RCVS Charter.
However, without question, the last decade has seen a visible, real and entirely appropriate increase in the professional status of veterinary nurses. Of course, increasing nursing aspiration must be underpinned by continued progression in educational standards. The current iteration of veterinary nurse training has a modular format and there is now a requirement for every veterinary nurse to study basic equine nursing, even if their ultimate aim is to become a small animal nurse. This book will therefore form an essential part of the general veterinary nursing syllabus, as well as being an essential manual for equine nursing trainees.
The first edition was required to be reprinted almost immediately and this edition, I am certain will be at least as popular. Whilst the chapter headings remain essentially the same, the information has been updated and several new authors have been recruited. Equine medicine and surgery has continued to evolve in the intervening years, and the number of specialist equine clinics and hospitals has also increased. Thus there is a definite need for the equine nursing profes-sion to maintain its position at the cutting edge of equine clinical practice. As an equine surgeon working in an equine hospital, I have become accustomed to the support of top quality equine nurses, and greatly appreciate the benefits that such skilled professionals afford the whole surgical team and, more impor-tantly, our patients.
I would like to congratulate Karen Coumbe on overseeing the production of yet another excellent edition of what in my opinion is the definitive text on equine nursing.
Tim GreetPresident, World Equine Veterinary Association(Honorary member, British Veterinary Nursing
Association)

x
Preface to the second edition
It is amazing that it is over ten years since the first edition of this reference book was published. Much has changed in equine nursing since then, both under the auspices of the Royal College of Veterinary Surgeons and in the wider world.
This second edition has the same intention as the first: to provide a definitive reference for equine vet-erinary nurses. The aim is that it will be practical, useful and educationally informative for all those involved in the veterinary care and professional man-agement of sick horses, ponies and donkeys. The goal is to supply the technical knowledge and essential information on the practical techniques needed by all members of a successful nursing team.
This new and larger volume is very closely based on the ever-expanding nursing syllabus, which encom-passes the breadth and depth of expertise essential for equine veterinary nursing today. It also contains suc-cinct sections suitable for those nurses who may be specialising in other species, yet still wish to acquire some basic equine understanding as part of their training. The information included is designed to update every equine nurse’s skills and I hope the book will become an essential guide, and a worthy succes-sor to the first edition.
Many developments have occurred since I wrote the previous preface to this book and the equine nursing world has made enormous professional progress. This is reflected in the many innovations described in this second edition, which has been completely reworked, with an abundance of new information and clear colour photos. Every chapter has been rewritten, with complete updates throughout the volume and increased emphasis on the various responsibilities of
an equine nurse. Additional artwork (Figs 1.1, 2.8, 2.18, 7.4, 8.5, 11.3, 13.2, 14.3, 16.9, 16.22, 17.22, 17.23 & 20.13) has been accurately and beautifully produced by Samantha Elmhurst of www.livingart.org.uk and I would like to thank both her and the hard-working team at Wiley-Blackwell, especially Anne Bassett, Rupert Cousens, Rebecca Huxley, Lucy Nash, Sue Peter and Justinia Wood. I am very grateful to Deirdre Carson for all her helpful suggestions and support, and for those who helped by providing pho-tographs, especially Peter Clegg, Marcus Head, Derek Knottenbelt, Sarah Mack, Tim Mair, Annie Makin (BCF Technology), Lorraine Palmer and Jess Spanton. I would also like to thank Jo Gregory, Matt Legg, Bonny Millar and Cassie Barber, but most of all Dr Nick Bolas, for their enormous photographic contri-bution, without which this book would have a blank cover! Also huge thanks to my family for allowing me the time to do this and their invaluable editorial input!
I am enormously grateful to all the contributors and thank everyone who has helped me, especially my col-leagues at Bell Equine. I am delighted that, amongst the authors, there are now more qualified equine nurses. I am proud that these include many of the same exceptional individuals who have worked with me over many years, both clinically and in drafting the first syllabus, setting the initial examinations as well as writing several chapters.
It is more obvious now than ever before that good equine vets need good equine nurses. I hope that equine nursing will remain an evolving discipline and that this volume will help speed the progress, to the benefit of the animals under our care. As with the first edition, the credit should go to the authors, any errors are mine.
Feel free to comment and constructively criticise!
Karen CoumbeKent, 2012
“Knowledge is power.”
Sir Francis Bacon,Religious Meditations, Of Heresies, 1597
All images are copyright the authors and/or editor in each and every chapter and Wiley-Blackwell, who retain all rights.

xi
Abbreviations and Acronyms
AB antibodyACD acid–citrate–dextroseACTH adrenocorticotrophichormoneADH antidiuretichormoneAF atrialfibrillationAG antigenAHS AfricanHorseSicknessAHVLA AnimalHealth&Veterinary
LaboratoriesAgencyAI artificialinseminationAL-DDFT accessoryligamentofthedeepdigital
flexortendonAM atypicalmyoglobinuriaAMTRA AnimalMedicinesTrainingRegulatory
AgencyANS autonomicnervoussystemAP alkalinephosphataseATD auditorytubediverticulumASA AmericanSocietyofAnesthesiologyASIF AssociationfortheStudyofInternal
FixationAST aspartateaminotransferaseAVD assistedvaginaldeliveryBAL bronchoalveolarlavageBAR BrightAlertResponsiveBCAA branchedchainaminoacidBCS bodyconditionscoreBEF BritishEquestrianFederationBHA BritishHorseracingAuthorityBP bloodpressurebpm beatsperminuteBUN bloodureanitrogenBVNA BritishVeterinaryNursingAssociationBW bodyweightCA cerebellarabiotrophyCa calciumCBC completebloodcountCCTV closedcircuittelevisionCCDL colourcoatdilutionlethalCD controlleddrugCDE commondigitalextensorCEM contagiousequinemetritis
CEPEF confidentialenquiryintoperi-operativefatalities
CFT complementfixationtestCID combinedimmunodeficiencydiseaseCK creatinekinaseCNS centralnervoussystemCOPD chronicobstructivepulmonary
diseaseCOSHH ControlofSubstancesHazardousto
HealthCP crudeproteinCPD continuingprofessionaldevelopmentCPK creatininephosphokinaseCPR cardiopulmonaryresuscitationCR computedradiographyCRT capillaryrefilltimeCRI continuousrateinfusionCS caesariansectionCSF cerebrospinalfluidCT computedtomographyCVS cervicalvertebralstenosisDAP doseareaproductDCP dynamiccompressionplateDCR directcaptureradiographyDDF deepdigitalflexorDDFT deepdigitalflexortendonDDSP dorsaldisplacementofthesoftpalateDE digestibleenergyDEFRA DepartmentforEnvironment,Food&
RuralAffairsDM drymatterDOD developmentalorthopaedicdiseaseDR digitalradiographyECF extracellularfluideCG equinechorionicgonadotrophinECG electrocardiogramEDTA ethylenediaminetetraaceticacidEED earlyembryonicdeathEGT exuberantgranulationtissueEHM equineherpesvirus1-associated
myeloencephalopathyEHV equineherpesvirus

AbbreviAtions And Acronyms
xii
EIA equineinfectiousanaemiaEIPH exercise-inducedpulmonary
haemorrhageEIV equineinfluenzavirusELISA enzyme-linkedimmunosorbentassayEMEA EuropeanMedicinesEvaluationAgencyERS equinerhabdomyolysissyndromeERV equinerhinovirusET embryotransferEU EuropeanUnionEVA equineviralarteritisEVN equineveterinarynurseFEI FédérationEquestreInternationaleFFA freefattyacidFFD filmfocaldistanceFSH follicle-stimulatinghormoneGBED glycogenbranchingenzymedeficiencyGGE glycerylguaiacolateetherGGT gamma-glutamyltransferaseGIT gastrointestinaltractGLDH glutamatedehydrogenaseGnRH gonadotrophin-releasinghormoneGP gutturalpouchh hourHb haemoglobinhCG humanchorionicgonadotrophinHERDA hereditaryequineregionaldermal
astheniahh handshighHR heartrateHSAWA HealthandSafetyatWorkActHSE HealthandSafetyExecutiveHYPP hyperkalaemicperiodicparalysisICF intracellularfluidICU intensivecareunitILRD infectiouslowerrespiratorytract
diseaseIPPV intermittentpositivepressure
ventilationIRAP Interleukin-1ReceptorAntagonist
ProteinIRU increasedradioisotopeuptakeIURD infectiousupperrespiratorytract
diseaseIM intramuscularIV intravenousJEB junctionalepidermolysisbullosaLCP lockingcompressionplateLDH lactatedehydrogenase
LFS lavendarfoalsyndromeLH luteinisinghormoneLMN lowermotorneuroneMAC minimumalveolarconcentrationMCV meancorpuscularvolumeMDP methylenediphosphonateMRI magneticresonanceimagingMRSA methicillin-resistantStaphylococcus
aureusNILRD non-infectiouslowerrespiratorytract
diseaseNIURD non-infectiousupperrespiratorytract
diseaseNMS neonatalmaladjustmentsyndromeNRC NationalResearchCouncilNSAID non-steroidalanti-inflammatorydrugNSC non-structuralcarbohydrateOCD osteochondrosisdissecansOCLL osseouscyst-likelesionP pharmacymedicineorphosphorusPCR polymerasechainreactionPCV packedcellvolumePG prostaglandinPIVA partialintravenousanaesthesiaPPID pituitaryparsintermediadysfunction
(Cushing’sdisease)PLGE protein-losinggastroenteropathyPML pharmacyandmerchant’slistmedicinePMT photomultipliertubePOM prescription-onlymedicinePSP periodofsupervisedpracticePSSM polysaccharidestoragemyopathyPTH parathyroidhormoneQAR Quiet,Alert,ResponsiveQAU Quiet,Alert,UnresponsiveQP QualifiedPersonRAO recurrentairwayobstructionRBC redbloodcellRCVS RoyalCollegeofVeterinarySurgeonsRDDLC rightdorsaldisplacementoflargecolonREVN RegisteredEquineVeterinaryNurseRIA radioimmunoassayRIDDOR ReportingofInjuries,Diseasesand
DangerousOccurrencesRegulationsRJB RobertJonesbandageRLN recurrentlaryngealneuropathyRPA radiationprotectionadvisorrpm revolutionsperminuteRPS radiationprotectionsupervisor

AbbreviAtions And Acronyms
xiii
RQP registeredqualifiedpersonRR respiratoryrateSBC subchondralbonecyst(seeOCLL)SCID severecombinedimmunodeficiency
diseases.c. subcutaneousSDF superficialdigitalflexorSDFT superficialdigitalflexortendonSDH sorbitoldehydrogenaseSL suspensoryligamentSOP standardoperatingprocedureSPL subpalpebrallavageSQP suitablyqualifiedpersonSSC squamouscellcarcinomaSTH somatotrophichormoneTB ThoroughbredTBW totalbodywaterTFT thinfilmtransistorTIVA totalIVtechniqueTL tracheallavage
TPN totalparenteralnutritionTPR temperature,pulseand
respirationTRH thyroid-releasinghormoneTSBA totalserumbileacidestimationTSH thyroid-stimulatinghormoneUMN uppermotorneuroneUSP USPharmacopeiaUV ultravioletVFA volatilefattyacidsVI virusisolationVMD VeterinaryMedicines
DirectorateVMP veterinarymedicalproductVMR VeterinaryMedicinesRegulationsVN veterinarynurseWBC whitebloodcellWNV WestNilevirusWSC water-solublecontentWSW writtensystemofwork


1
1 Basic equine managementW. Linnenkohl1 & D.C. Knottenbelt2
1Cornell University College of Veterinary Medicine, Ithaca, New York, USA; 2Philip Leverhulme Equine Hospital, Liverpool, UK
General horse behaviour
Horses have evolved as a flight species and therefore, whenever a horse is to be handled, it should be remembered that it will try to escape from any uncomfortable or unfamiliar situation by running away. In instances where a horse feels that it is unable to escape, it may resort to kicking or biting as a form of defence. When handling unfamiliar horses, or horses in an unfamiliar or stressful situation (i.e. in a hospital setting), knowledge of how horses might react and proper methods of restraint are imperative for everyone’s safety.
Most horses behave better if handled with confidence, firmness and kindness. Only deliberate bad behaviour should incur reprimand, and this should be immediate; hitting or kicking horses is completely counterproductive. A firm verbal reprimand is usually enough to make a horse pay attention. When persuading horses to do something unfamiliar or frightening, their primitive instincts for food and companionship can be utilised. If a horse is objecting to a particular task it is being asked to perform, it is important to understand whether its actions are motivated by fear or bad behaviour, since punishing a fearful horse will often make the situation worse. When horses flatten their ears, bare their teeth and lunge towards other animals or people, this is usually a sign of aggression rather than fear. A frightened horse may flatten its ears, yet turn away.
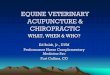
As horses are instinctively creatures of flight, it is important to understand the concept of a flight zone (Fig. 1.1). The flight zone can be thought of as the horse’s personal space. The size of the flight zone is determined by the tameness of the horse; welltrained animals will usually have a small flight zone whilst wild horses invariably have a large one. The point of balance, which determines which direction a horse will flee from an approaching person, is at the shoulder. When the flight zone is entered from the head, the horse will move backward and vice versa. It is important to be aware that it is best to approach a horse from the left, if possible, in a slow and calm manner using your voice to let the animal know you are there.
Vices, stereotypies and redirected behaviour
In the past, certain types of abnormal behaviour were known as vices. We now know that many ‘vices’ are the horse’s attempts to cope with a stressful environment. Their significance to equine health is widely disputed, e.g. the link between colic and cribbiting is a good example of the controversy. Whilst there is a proven correlation between cribbiting and colic caused by epiploic foramen entrapment, the link with flatulent (gassy) colic is much less convincing.
Stereotypies are invariant and repetitive behaviour patterns with no apparent function. Examples of
Equine Veterinary Nursing, Second Edition. Karen M Coumbe.© 2012 John Wiley & Sons, Ltd. Published 2012 by John Wiley & Sons, Ltd.

CHAPTER 1
2
Moredangerous
areas
Moredangerous
areasBODY OF ANIMAL
SaferArea
SaferArea
Safer approach area (left shoulder)in the standing animal
Edge offlight zone
Blind spotshaded gray
Handlersposition to stop
movement
Handlersposition to start
movement
Point of balance
90°
45°
60°A
B
a
b
Fig. 1.1a&b. The flight zone of a horse is the distance at which the horse will choose to flee when approached by a human (or in the wild, a predator). See Box 1.1.

BAsiC EquinE mAnAgEmEnT
3
Box 1.1 The flight zone
• The flight zone can be thought of as a horse’s ‘personal space’. movement into this area is likely to make a horse move away.• The size of the flight zone depends primarily on the familiarity of the horse with the handler. With frequent handling, the flight zone decreases in size and may even disappear.• A horse that is approached head-on has a larger flight zone than if it is approached from the side. A head-on approach by another horse or human is considered threatening.• The edge of the flight zone can be determined by slowly walking up to the horse. The point at which the horse begins to move away is the edge of the flight zone.• When working with a horse, there is a point-of-balance for moving the horse backward or forward.
The point-of-balance is at the shoulder, perpendicular to the length of the body. if you want the horse to move backwards, start in front of the point-of-balance and move into the horse’s flight zone. if you want the horse to move forward, move into the horse’s space from behind the point-of-balance.• if a handler enters the flight zone suddenly, the horse will either bolt and run away or turn back and run over the person.• it is important to be aware of the flight zone and the horse’s response to the handler within and near the flight zone. This will help to ensure safety at all times for the handler.
isfaction’ from the behaviour and so, again, prevention could be viewed as harmful. There is still much debate on the basis of most of these behaviour patterns.
General horse handling
Basic technique
When approaching a horse, and particularly a nervous animal, it is important to always speak to let it know of your presence. Approach from the front and slightly to the side, and walk towards the shoulder. Horses have a blind spot directly behind them. Handle the horse first on the lower neck or shoulder, and then put a lead rope around its neck. At this stage many animals will consider themselves ‘caught’. Difficult individuals should wear a headcollar when turned out or even in the stable until they learn to be caught submissively. Headcollars with leather pieces that break if the headcollar snags on something are ideal to prevent injury (Fig. 1.3).
Food is a useful bribe for most horses, although they should not always come to expect it. Placing the noseband of a headcollar around the inside of a bucket may help when catching a difficult animal.
stereotypies include weaving, boxwalking, and windsucking or cribbiting (Fig. 1.2a,b&c). Redirected behaviour occurs when a certain type of motivational behaviour is prevented. The horse will perform another type of behaviour to replace the missing behaviour pattern. Selfmutilation is a compulsive behaviour that is seen occasionally, particularly in stallions. Psychogenic polydipisia (drinking water for no physiological reason) can be alarming and can result in significant renal physiological compromise.
Certain behaviours, such as pawing, digging or doorkicking, may be reinforced by attention. Stereotypical and redirected behaviours do not consistently cause direct harm to the horse. They are usually considered undesirable and may represent a welfare problem. Recent research has shown that some stereotypies may have a physiological basis. The relationship between gastric ulceration and cribbing is an example of this. It is thought that cribbing in some cases at least starts as a result of gastric discomfort when feeding methods are not natural; the horse cribs to induce salivation which acts as buffer for gastric acidity. Preventing a horse from cribbing can therefore be regarded as a harmful procedure. In addition there is some evidence that horses ‘get some psychological sat

CHAPTER 1
4
Fig. 1.3 a,b &c How to approach a horse and fit a headcollar, all from left (near) side of the horse.
a cb
a
c
b
Fig. 1.2(a) Stereotypical behaviour: horse cribbing or cribbiting on a fence post, which is when a horse holds fixed objects with its teeth, arches the neck as shown and makes a grunting sound, usually as they gulp in air. Windsucking is when they do this without holding onto a fixed object. (b) Worn incisor teeth as a result of cribbiting (USA term = cribbing). (c) A horse boxwalking.

BAsiC EquinE mAnAgEmEnT
5
Speed and technique are always important in such situations but it is also important to avoid sudden (potentially threatening) movements that might frighten the horse.
Horses are trained to respond to pressure cues. A welltrained horse knows to move away from pressure as well as to respect a human’s personal space. Young or untrained horses often do not understand these boundaries, particularly in stressful environments. Care and patience should be maintained when handling these types of horses. It is often better to allow the horse to ‘come’ to the handler. The horse is naturally inquisitive and will usually make an approach to a person standing in the vicinity in a quiet and nonthreatening manner.
When being led, the horse should walk forward freely. Traditionally horses are led from the left (i.e. the ‘near’ side), although they should be trained to accept approaches from both left and right. The lead rope should be held near the horse’s head, with the free end in the other hand. The rope should never be wound around the hand. Ideally gloves should be worn.
Handling mares and foals
When handling mares and foals, the handler must be aware of the mare’s attitude. Even the most wellmannered mares can become aggressive when they have a foal at their side, particularly a maiden mare with her first foal. Conversely, some mares show inadequate maternal behaviour and may even reject their foal.
Young foals often have larger flight zones than mature horses if they are not accustomed to human interaction. The foal has highly developed hearing, good eyesight and is sensitive to touch. If properly handled, a foal will quickly become accustomed to people and will learn to trust them. In recent years, the concept of imprinting has gained popularity. This involves handling foals and accustomising them to human attention shortly after birth. The foal should be gently handled and regularly spoken to in the first few days of life. As soon as the foal is used to being touched and approached it should be fitted with its first headcollar, which is called a foal slip. Gentle handling of the head and ears in the early stages is important in preventing the foal from becoming headshy in later life.
Foals often resent being led by a halter. Foals that are not adequately halter broken should never be pulled as they will usually resist and injure themselves. Leading a foal while it is following the mare is a good way to teach it, accompanied by quiet but firm verbal aids and a hand around its hindquarters to gently push and guide it.
When restraining a foal for examination, one hand should be placed around the chest and one hand should grasp the hind quarters or tailhead. If the foal needs to be removed from the mare for examination, the mare should be sedated.
Handling stallions
Care should always be taken when handling stallions as they can be unpredictable. Proper restraint, using a stallion chain, chifney or bridle, is the safest way to handle these horses. An excited stallion can become very aggressive towards humans by biting, striking or kicking out. Caution should be shown when handling a stallion in the company of mares, particularly if a mare is displaying signs of oestrus (heat) or has a foal at foot. A stallion should always be housed in a safe environment (i.e. appropriate fencing and box design) so that they do not injure themselves or other horses or make attempts to escape.
Handling young horses
When handling young horses, the aim is to be gentle and not frighten the horse; the training process should produce a horse that is calm and confident to ride and handle. Horses, like people, differ in their natural ability and in their capacity for learning. Young horses often differ in their behaviour on being handled, due to differences in their training and temperament. They are rarely aggressive, and most often act out of fear based on inexperience.
Handling nervous horses
When handling a nervous horse, understanding their natural response to fear is the key to successful handling. It is most unwise to stand directly in front of or behind a horse, particularly a nervous animal, as these are the most dangerous areas around a horse. It is best to talk in a soothing voice to reassure it; punishing a nervous horse will often aggravate their behaviour.

CHAPTER 1
6
6–7 mm thick at the end. The loop, which should be 40–50 cm long, is twisted around the horse’s upper lip. The twitch works partially by causing pain and distracting the horse’s attention, so should be used only when absolutely necessary. It also causes the release of natural endorphins, which have a narcotic effect. It can be an extremely useful method of restraint, but modern sedatives are often a more humane solution. On occasion, a horse may react violently and unexpectedly when a twitch is used. The handler must try to observe the behaviour of the horse and in particular try to detect increasing respiratory movements. The twitch must be removed as soon as these develop.
Fig. 1.4 Tying a quickrelease knot.
Fig. 1.5 A chifney bit with identifying tags for hospital.
Handling aggressive or disrespectful horses
Truly aggressive horses are extremely rare. Often a horse’s behaviour is interpreted as aggression, but this is more often fear motivated. An aggressive horse can be very dangerous, so caution must be used at all times. Do not ever handle an aggressive horse alone; appropriate restraint using a bridle or chifney should be used at all times. The aggressive or disrespectful horse should always be handled with confidence but caution.
Appropriate restraint
For most procedures around the stable yard the horse can be restrained using a halter or headcollar. A foal slip, which will break easily, is preferable for very young animals. All horses should be trained to stand quietly when tied up. This should be achieved at an early age. A quickrelease knot (Fig. 1.4) should always be used, and ideally the animal should be tied to a sturdy ring or post via a piece of string that will break if the horse pulls back violently.
For additional control a bridle may be used, but it is not recommended to tie a horse up using either a bridle or a chifney. A chifney, or antirearing bridle, is a useful device fitted with three rings – two for the cheek pieces and one for the lead rein – with a shallow invertedport mouthpiece (Fig. 1.5). In animals that are too young to wear a bit, a lunge cavesson with lunge rein may provide better control. The lead rein or lunge line attaches to the front of the noseband on a lunge cavesson.
Additional restraints
TwitchA traditional twitch (Figs 1.6 & 1.7) is made of a short pole 50–70 cm in length, with a loop of rope

BAsiC EquinE mAnAgEmEnT
7
When using a twitch the handler must stand appropriately when the twitch is in place and should be careful to hold the leading rein correctly. The twitch pole can become a dangerous missile if not held correctly.
Other methods of restraint include the following.• Skin twitch: taking a firm grip of a fold of neck skin can distract some horses.• Ear twitch: similar to a skin twitch; grasping and gently twisting the ear may control some horses, particularly youngsters.• Raising a foreleg: this can be useful to encourage a horse to stand still if you are confident that you can keep the leg up when the horse tries to move.• Stocks will limit horse movement, but must be designed to maximise horse and human safety. It is always important to remember a horse in stocks can still injure you, so caution should be taken.
Basic stable management
medical reasons for stabling
Stabling is often essential for medical management of sick or injured horses, for example in the following situations.• Orthopaedic problems requiring box rest.• Monitoring of sick patients requiring the horse to be stabled.• As a preventative measure for certain conditions such as laminitis, insect bite hypersensitivity (sweet itch or culicoides hypersensitivity)or horses suffering from mud fever or rain scald.• In situations requiring isolation.
Requirements of a stable
Safety and good hygiene are essential. With the large throughput of animals in an equine hospital, there is a significantly increased risk of nosocomial (hospitalacquired) infections. Good examples are salmonellosis and methacillinresistant Staphylococcus aureus (MRSA) infections of wounds. Suspected viral infections, such as influenza and herpes virus, are more difficult to contain since they are airborne.
General considerations• Stables should be easy to clean and disinfect, particularly in hospital situations. The drains are a source
Fig. 1.6 Applying a twitch.
Fig. 1.7 When the twitch is applied to the nose it should not be excessively tight, but its effect does rely on significant pressure. Once it is tightened, the lead rein should be held firmly against the pole (without excessive rope dangling down) and the handler should stand back or to the side. The behaviour of the horse must be observed carefully and the twitch should be released if the horse shows signs of sweating or other discomfort.

CHAPTER 1
8
shoes. Hay nets should be tied with quickrelease knots and attached to twine that will break easily if the horse gets caught and struggles.
Stable fittingsInternal fittings should be minimised and, where possible, should be flush with the walls with no sharp projections. Firmly fixed rings at shoulder level for tying the horse to, and another ring at eye level for a hay net, are the minimum requirements.
VentilationGood ventilation is particularly important for stabled horses.• There is a tendency among horse owners to think large wellventilated stables are too cold. Rugs can provide extra warmth but still permit the horse adequate fresh air.• Windows and top doors are the main source of ventilation. Windows should be arranged so that they can be opened with an inward slant while ideally being protected by bars.• In barns, louvre boards at the apex of the roof are ideal. These consist of two or more overlapping boards separated from each other by a few inches and set at such an angle that wind and rain cannot enter. Wind blowing across the top of buildings will aspirate air from the apex. Heat loss from horses also causes air to rise within the building. These factors contribute to the upward and outward flow of air, called the stack effect. In many barns, large doors at one or both ends allow a good inward movement of air. Wind blowing from side to side and end to end is known as perflation. Yorkshire boarding assists perflation.• Barns often have better ventilation than individual loose boxes. However, there are disadvantages in that a group of horses share the same air space; this can encourage the spread of respiratory disease. In addition, hay and straw are commonly kept in the same air space and this can exacerbate allergic respiratory disease.• Draughts should be avoided, particularly in foal accommodation.• Mechanical ventilation can be employed in long or wide buildings.• In a stable with a monopitch roof, an open top door will provide an adequate inlet for air. A second inlet in the front wall and an outlet in the back wall are ideal. Boxes with peaked roofs ideally should have a fourth opening in the form of a capped chimney.
of disseminated infection and so are particularly important.• Stables should be warm and dry and have adequate drainage.• Adequate ventilation is essential with good air throughput and a lack of draughts and dust.• Lighting is important – a lack of suitable lighting will be a potential danger for a person entering the stable and will necessarily limit the efficiency of any examination and procedure.• Fresh water must be available at all times whether this is delivered by bucket or by automatic drinker.• Food should be placed in areas where there is less chance of faecal or urinary contamination. Some horses may have special requirements, for example, airway disease horses need to be fed off the floor, whilst horses with some orthopaedic disorders may require feeding from an elevated position. Hay nets can be used but are a potential hazard.All necessary precautions should be taken to minimise the risk of fire and suitable firesafety measures must be readily to hand and properly functional.
Water provisionAdequate clean water always should be available.• Automatic water bowls are efficient, but they must be checked regularly to ensure that they are working and a backup supply of buckets should be available. A major drawback of automatic fillers is that monitoring water intake is impossible.• Water buckets should be cleaned and refilled daily. Buckets can be secured in holders, old tyres or on hinged rings off the ground to prevent them being knocked over.
Food provision• Mangers should be easy to clean. Ideally, mangers should be large, broad and have a completely smooth surface with wellrounded corners.• Hay and mangers on the floor mimic the horse’s natural way of eating. For some medical conditions, e.g. sinusitis, it may help the horse to eat from floor level to enable good sinus drainage.• Hay racks fitted above head level oblige the horse to feed at an unnatural level and there is a risk of getting dust and grass seeds in the eyes.• If hay nets are used, they should be tied high enough to prevent the horse getting entangled. This is more of a danger in horses shod with longheeled

BAsiC EquinE mAnAgEmEnT
9
• Colic boxes should have ample deep bedding right up to the door. Alternatively they can be constructed with a rubber floor and walls. Such boxes should have minimal fittings so that the horse does not injure itself if it rolls violently.• Specialised facilities for sick foals should be available. Intensivecare systems for mares and foals should include a separation box, where the foal can be separated to facilitate treatment while the mare can still have some contact.
Biosecurity
Cleaning and disinfection
Stables should be designed and constructed, so they can be cleaned and disinfected readily and routinely. To minimise the risk of microorganisms becoming established in the fabric of stables, there should be a regular programme of depopulating the accommodation and subjecting it to a thorough disinfec tion. It is only possible to do this effectively if all internal surfaces have impervious and easily disinfectable concrete walls and floors. The materials used must withstand pressure cleaners, strong detergents and a full range of disinfectants. Chemical steam cleaners are valuable as they result in a dramatic fall in the bacterial bioburden within the treated environment.
Daily ‘mucking out’ is important and stables should be kept clean and dry with plenty of fresh bedding. As far as possible, horses should keep the same stables; repeated moving of horses from stable to stable is a definite biohazard for both that horse and other horses that follow it into the stables. A routine of removing all the bedding and thorough disinfection should be employed after each horse leaves the stable.
Hygiene
As with any stable yard, hygiene is vital. Hospitals should be organised so that stables are grouped according to the following categories. Notes on cleaning and hygiene are made for each category.• Routine hospital cases: stables should be washed and cleaned between cases.• Intensivecare hospital cases: particular care should be taken with the routine cleaning of intensive care boxes. It is important to observe the amount of faeces and urine produced by horses in intensive care.
Ventilation and respiratory disease The level of dust and spores in the centre of a box is dependent on the rate of release of the contaminant into the air and on the ventilation rate. Release rates depend on the activity in the stable and on the level of contamination of bedding and hay. Good ventilation combined with the use of bedding and hay with inherently low levels of potential antigens is important, because improving the ventilation alone may be insufficient to prevent respiratory disease.
Intensive-care facilitiesIntensivecare facilities are an important part of an equine hospital. They should include the following resources.• Facilities for provision of additional heat and excellent lighting• Facilities for IV fluid administration (Fig. 1.8)
Fig. 1.8 Intensive care facilities: fluid administration, with elevated system to hang multiple bags of fluid, including plasma. It is important that any horse with an IV catheter cannot put its head out through the doorway, so running risk of dislodging the catheter. (See also Table 1.6 page 14).

CHAPTER 1
10
Isolation accommodationThe stable should have no direct or indirect contact with others and should ideally be downwind of other stables so that airborne infection is less likely. Ideally, an isolation box should be at least 35 m away from other animals, regular thoroughfares and from communal feeding and bedding stores. A completely separate set of feeding, watering, tools, grooming and veterinary equipment should be used. Everything must be thoroughly disinfected between horses. The drain away from isolation accommodation should be apart from other animal accommodation or natural watercourses.
All hospital boxes, but particularly isolation boxes, should have floors of roughened concrete or rubber mats with sealed edges. Walls should be impervious with central floor drains. There should be minimal
Fig. 1.9 Hot water or steam and chemical solutions under pressure can be used to improve the disinfection of a stable, where an infectious agent might have been present.
Table 1.1 Indications for isolation
• Individual acutely sick animals• Incontact animals not showing clinical signs. Particular
attention should be paid to animals that may be immunocompromised (e.g. old horses, foals and horses with Cushing’s disease)
• Noncontact unaffected animals in an epidemic• Animals not showing clinical signs but in the recovery
stages of disease (shedders)• Quarantine procedures preceding entry into the herd
Table 1.2 Some equine infectious diseases to be considered in the UK
• Equine influenza• Equine herpes virus infections• Other respiratory virus infections• Streptococcus equi infections (strangles)• Other streptococcal infections (e.g. Streptococcus
pneumoniae)• Infectious enterocolitis (e.g. salmonellosis, clostridial
disease, rotavirus, cryptosporidia)• Ringworm
The following are notifiable & although there have been cases are not endemic• Equine viral arteritis• Equine infectious anaemia
• Isolation boxes: removal of all bedding (with appropriate disposal) should be carried out. Thorough disinfection preferably with hightemperature powerwasher chemical disinfection is essential (Figure 1.9). Ideally the stable should be left vacant for a period of time before being reused. This often depends on the microorganism implicated in the contagious disease, because different microorganisms can survive for differing lengths of time in the environment, even after disinfection.• Quarantine: as with isolation boxes, quarantine boxes should be disinfected thoroughly between occupants. It would be advisable when working in such situations to obtain specific information about where the horse has come from and the nature of potential diseases it may carry.
isolation facilities
Forward planning is vital to good isolation and the control of infectious disease outbreaks. See Tables 1.1 and 1.2 for indications for isolation and some infectious diseases.
Principles of isolationIf a serious infectious disease is suspected, then all movement onto and off the premises should be stopped immediately. If an infectious disease is suspected, the affected animal must be isolated immediately (Table 1.3). Isolate first and confirm the diag-nosis later!

BAsiC EquinE mAnAgEmEnT
11
• Personnel in contact with the isolated horse should wash their hands and other exposed skin thoroughly with a suitable antiseptic detergent such as a surgical scrub immediately after contact.• Fomites (i.e. inanimate objects such as feed buckets) can be a cause of disease transmission. Care should be taken to reduce this risk by ensuring disinfection and avoidance of contact with other horses.• No items taken into an isolation area should return to the hospital without thorough disinfection.
Duration of isolationThe period of isolation will depend on the disease involved. The owner’s willingness to continue with full isolation requirements is likely to be reduced following cessation of clinical signs.
Disinfectants and antiseptics
• Disinfection is the removal or destruction of pathogenic microorganisms. Bacterial and fungal spores may survive normal disinfection processes, but the number of ‘vegetative’ microorganisms can be reduced to a level that is not harmful to health. Disinfection can be achieved using chemical solutions, by heat treatment or by physical removal of microorganisms.• A disinfectant is an agent usually applied to inanimate objects to destroy microorganisms. Many disinfectants are, however, harmful to living tissue. It is therefore important that anyone using disinfectants should be aware of this and take the appropriate precautions by implementing the manufacturer’s instructions regarding concentration and application. It is essential always to read the data sheets and labels carefully and to adhere strictly to the safety instructions.• Antiseptics destroy microorganisms, but not necessarily bacterial spores, on living tissue. They prevent the growth of microorganisms and may usually be applied safely to living tissue.• Sterilisation is the total elimination/destruction of microorganisms and spores.• Contamination is the presence of microorganisms in tissues, which may or may not result in infection.
Principles of disinfectionIt is important to establish whether a disinfectant is bactericidal (i.e. destroys the organisms) or
fittings within the box itself and these should be easy to disinfect. Ledges and windowsills should be minimised because they can support a buildup of debris and potential infection. All waste feed and bedding should be disposed of appropriately, e.g. as clinical waste.
Nursing isolation cases• A single person should look after the nursing and management needs of a patient in isolation. Contact with the animal should be reduced to the minimum necessary level. In situations where a nurse has to deal with normal and isolated horses, the isolated animal must be dealt with last.• Overalls, shoe covers and a head cover should be kept outside the box and used whenever the horse is handled. Latex gloves should also be worn. These protective items should be disposed of in a closed clinical waste bin outside the box.• There should be adequate facilities for staff to wash hands and disinfect at entry/exit to the box. A shoe dip should also be provided outside the box.
Table 1.3 Important questions to ask about an infectious disease
Clinical signs and diagnostic tests:• What samples need to be collected?• What is the incubation period?
Transmission of pathogens between animals:• How does the animal contaminate its environment?• How important are fomites or other animal vectors?• Over what distance can aerosol transmission occur?
Survival of pathogen outside the animal:• How long can the pathogen survive?• What environmental conditions enhance its survival?• Does the pathogen produce resistant spores?• What disinfectants is the pathogen susceptible to?
Protection of susceptible animals:• Will treatment/vaccination help?
During isolation:• What is the incubation period and for how long can
animals shed the pathogen following recovery?• Can asymptomatic carriers be identified (a recognised
problem with strangles)?

CHAPTER 1
12
• Cryptosporidia are a special case and only a minimum of 18 h of fumigation of buildings with formaldehyde or ammonia will disinfect adequately. However, formaldehyde is highly toxic and has noxious fumes, making it impractical to use routinely in a stable environment.
Practical disinfectionTable 1.4 outlines the common disinfectants and their properties. Practically, it is best for a hospital to have one main type of disinfectant to be used for most circumstances. Halogenated peroxides and tertiary amines are highly effective against all bacteria and most viruses, including rotavirus.
Bedding and cleaning of stables
Table 1.5 summarises the basic bedding materials available.
Cleaning and changing of bedding
Deep litter systemsDeep litter stables are maintained by just removing the droppings on a daily basis. This type of management is not suitable for a hospital situation because of the lack of hygiene.
bacteriostatic (i.e. stops bacterial replication and growth). Bactericidal chemicals with activity against spores are preferable, but such substances are more likely to be harmful to the operator. Chemicals that are not inactivated in the presence of organic material (such as pus, blood and faeces) should be chosen. Removal of gross contamination is paramount and pressure hoses can be very useful for this purpose on solid inanimate surfaces (Fig. 1.9). Selection of a chemical that is effective against the pathogens that are most difficult to destroy is appropriate.
Susceptibility of microorganisms• Grampositive bacteria are destroyed most easily by disinfectants. Streptococcal organisms are susceptible to drying and heat but Rhodococcus equi is resistant to drying, heat, acid and alkali under natural conditions.• Gramnegative bacteria, acidfast bacteria and bacterial spores are increasingly resistant.• Rotavirus and cryptosporidia are probably the most difficult organisms to destroy. Rotavirus commonly causes diarrhoea in foals, up to 5 months of age. It is a heatresistant virus that is known to survive in the environment for up to 9 months. Choosing a disinfectant that is effective against rotavirus will also control most other commonly encountered pathogens.
Table 1.4 Disinfectants and their properties
Active ingredients (product name)
Inactivated by organic material (Yes / No)
Effective against rotavirus
Comments
Chlorine compounds (bleaches) Yes No
Quarternary ammonium compounds
Yes No
Phenolic compounds No Yes Generally not utilised due to toxic and irritant properties
Iodophors No Yes Usually utilised more for handwashing during outbreaks
Halogenated tertiary amines (e.g. Trigene)
No Yes Nontoxic and biodegradable. Commonly utilised
Halogenated peroxides (e.g. Virkon)
Yes Yes Commonly utilised. Has fungicidal properties

BAsiC EquinE mAnAgEmEnT
13
and faeces. Regular washing of hands and wearing clean protective clothing daily is important. Gloves and masks are recommended.
Disposal of bedding waste
A ‘muck’ heap should be created in a suitable area some distance from the stables in an area where no animal contact can occur. It should be far enough away from the hospital treatment areas and the stables that flies are not a problem. Rotting mounds of bedding provide a source of potential pathogens and spores. Regular disposal of bedding, at least every third day, should be arranged. In some circumstances bedding waste can become very hot and this is a useful means of limiting infective potential. Burning is no longer an acceptable means of management.
Bedding for special cases
Recurrent airway obstruction (RAO)RAO (previously known as chronic obstructive pulmonary disease, COPD) is an allergic disease caused by inhalation of fungal spores in hay and straw. If this condition is to be controlled it is vital that the horse is not exposed to materials containing spores. The spore content of feed or bedding depends largely on the moisture content. Straw, hay and grains harvested with high moisture contents develop a high mould burden (Figure 1.10). It should be noted that other bedding types that have been allowed to mould will exacerbate RAO. Nonbiological beddings do not provide a base medium for fungal growth.
Orthopaedic and other recumbent casesA deep bed is essential when a horse is recumbent since getting up and lying down are difficult and often uncontrolled. Additionally, pressure from a solid floor can cause significant damage and induce pressure sores (decubitus ulcers).
ConvalescenceRecumbent horses, horses with lung compromise after an anaesthetic or pneumonic foals may inhale millions of spores into an already compromised respiratory system. A clean nondusty bedding material is essential. Warmth may be an additional requirement under some circumstances.
Table 1.5 Summary of bedding materials
Type of bedding Comments
Hay Generally not suitable because it is edible and expensive
Hemp Low dust and mould free. Good for horses with RAO. Some horses try to eat it
Paper Excellent for dustfree environment. May be expensive
Peat moss Inedible. Dust free. Becoming less readily available (peat extraction is an ecological issue)
Straw: barley straw Often cheapest but can be poor quality and cause skin irritation. Not suitable for horses with RAO. Any straw can cause impactions if eaten
Straw: oat straw Often cheaper, but edible. Not suitable for horses with RAO
Straw: treated straw Treated straw to prevent horses eating it is now available. It is more expensive
Straw: wheat straw Generally considered the best straw bedding. Light, durable , not usually eaten. Not suitable for horses with RAO
Sawdust May block drains. If damp, can cause foot problems such as thrush
Wood shavings Less dusty than sawdust, but can also cause foot problems if damp or if hygiene is poor
Other: rubber, peanut hulls, corncobs, etc.
Ensure a fresh clean supply. Easy to muck out
Complete ‘mucking-out’ systemsFaeces and urinesoaked bedding should be removed daily. Ideally bedding should be removed completely between different horses. Personnel involved in the cleaning of stables should be aware of good personal hygiene and the potential problems of handling urine

CHAPTER 1
14
be taken to limit the slack in the lunge line and prevent it from dragging on the ground, where it might tangle in the horse’s legs. A lunge whip is often used to encourage the horse to move forward. Most horses accept lungeing readily and will respond to verbal commands.
Transportation
Loading/unloading horses from transportsHorses may be transported by road in trailers or horse boxes. These come in varying forms and may have side and/or front or rear loading facilities. Many horses are accustomed to travelling and load and unload easily. Some horses can, however, be very difficult. Listed below are some common problems.• Unfamiliarity with the vehicle or trailer (some horses will not travel well in a trailer, but accept a horse box readily and vice versa. Others travel better sideways or rearfacing).• Steep ramps create significant difficulty and some ramps are dangerous if slippery or unstable.• previous bad experiences can cause future problems with loading and unloading.• If the compartment size is narrow (e.g. in endloader trailers) some horses will be reluctant to load, especially if there is no visible exit.• The biggest problems loading are usually with horses that have never loaded, rather than those that have had problems in the past. Lack of suitable training is the cause of most problems.• Reluctance to travel alone: some horses only travel with company and others may not travel with an unfamiliar companion.
General points for loading and transportingThe trailer should be in a safe loading area with a closed gate between the loading area and any road. Many horses load more readily when the vehicle and trailer have been positioned with one side along a solid high wall. Backing the trailer into a barn could be considered for horses that readily run out of either side of the ramp. Many horses will enter more readily if a second ramp is open, so as to create the impression of a thoroughfare.
Ideally, all horses should be loaded in a bridle or with a chifney bit. Where two or more horses are to be transported together, the more sensible horse should be loaded first. Many horses that are nervous
Common hospital procedures
Lungeing
Lungeing is commonly performed for evaluation of lameness, but is also used as a form of training and exercise. A horse should be lunged in a bridle for safety and control. The person undertaking lungeing should wear a safety helmet and gloves. Care should
Table 1.6 Special considerations for equine hospitals
Crosstying facilities
Crossties should be attached to the wall with twine that can break if a horse panics
Intravenous fluid administration
Each stable should have an overhead rope and pulley system to hang fluid, the fluid should be attached to the horse with a spiral coil so the horse can move about the stable
Identification Stables should be marked with the patient’s name, medications, and current active problem; the patient and all equipment with it should also be clearly labelled with the owners name
Fig. 1.10 A magnified picture of mouldy damp straw used for bedding – it is easy to visualise that the spores from this could be inhaled. Similar moulds occur in hay and so this can also be a source of allergens for a horse with RAO.

BAsiC EquinE mAnAgEmEnT
15
be solid walls either side of the ramp to ‘funnel’ the horse in. It is usually necessary to have a lower ramp for trailers and a higher one for horseboxes.
UnloadingAs with loading, safety precautions should be taken. Horses often exit from vehicles with unexpected speed. A bridle or chifney bit should be used, particularly where there is direct access to a road. Loading directly onto a concrete or tarmacadam surface can be dangerous, since the horse may slip and crash to the ground. A firm but yielding surface such as sand or grass is ideal.
Problem horsesThere are many tricks that can help a horse to load. Generally owners should be encouraged to practise loading horses so that the horse does not fear transporters. Lunge lines can be used to encourage a horse from behind to walk forward onto the trailer. Feeding the horse in the trailer can be an excellent method of getting it used to the vehicle. Shy loaders should be rewarded with food when they enter the vehicle but tempting a horse into the trailer with food often leads to longterm problems. The
and reluctant to load will do so much more readily with a companion already in the transporter.
Trailers and horseboxes should be safe and roadworthy. Regular safety checks and compliance with regulations are important, as with any vehicle. This includes safety within the transporter, such as ensuring a strong enough floor and ramp.
TrailersThe following are points that should be considered.• The vehicle always should be attached to the trailer before loading.• When loading the first horse it may be easier to move the central partition across to give the impression of a larger compartment.• It is illegal and extremely dangerous for persons to travel in the back of trailers, no matter how much space there is available.
Loading rampsLoading ramps (Fig. 1.11) decrease the gradient of the transporter ramp in order to make the entrance to the vehicle seem more inviting to the horse. A purposebuilt ramp should have room for boxes with both front and side doors to manoeuvre. There should
Fig. 1.11 Two different height loading ramps at an equine hospital. Difficult horses will often load more readily using a loading ramp.

CHAPTER 1
16
Equine ambulances Specialist trailers and horseboxes are available for the transport of animals requiring special treatment. Such vehicles are fitted with accessories such as winches, belly support straps and drag mats.
Clipping
Horses are clipped for various management and veterinary reasons.
Management reasons for clippingHorses may be clipped to facilitate evaporative cooling during exercise or to reduce grooming. It is traditional not to clip horses after January, to allow the subsequent summer coat to develop properly. It is also advisable not to clip the lower limbs because this removes the waterproofing of the hair. However, many horses are fully clipped and suffer no recognisable ill effects provided that the legs are adequately cleaned and dried, when necessary.
Veterinary-related reasons for clippingThe following are reason for clipping.• Investigation of trauma sites and wounds.• When cleaning wounds prior to repair.• Preparation of a site for surgery or aseptic techniques, e.g. arthrocentesis.• In pituitary pars intermedia dysfunction (equine Cushing’s disease), as cases often grow a thick curly coat, which they fail to shed in summer. They may be significantly helped by full body clips during the summer months.• Skin diseases: rain scald and mud fever develop in damp microclimates, such as that afforded by long hair. Clipping is used as both a preventative measure and part of treatment.
General pointsThe coat must be clean and dry for clipping. Efficient use of clippers is dependent on clean, sharp, cool blades used at the correct tension. Poorly maintained equipment is noisy, pulls the hair and may burn the animal. Clipper rashes or wounds can occur with poor clipping technique. Clippers need to be lubricated regularly during the process to keep them running smoothly and to cool the blades. This is particularly relevant where horses are being fully clipped for management reasons. After use,
reward should only be given when the horse is actually in the vehicle.
Clothing for transportThere is a wide range of opinion as to how much protective clothing should be worn by the horse during transport. Certainly some form of lower limb protection is advisable; this can be purposemade travelling boots or long stable bandages. Horses that violently raise their heads or rear may benefit from a poll guard. Tail bandages and tail guards may also be useful. Capped hocks are a relatively common result with difficult journeys, so hock boots are commonly used.
Transport of sick or injured horsesSpecial considerations Transportation of sick patients requires additional attention. For example, horses with respiratory problems may experience sudden exacerbation during transport, particularly on long journeys where conditions are hot and dusty. Horses that have been sedated should be fully recovered before they are travelled (although they can usually be loaded safely). Horses that are travelling long distances (over 2 h) should have water offered regularly. Horse ambulances are equipped to deal with most difficult circumstances and the service should be used wherever available for more serious cases.
Colic Horses travelling to a clinic for colic investigation may be extremely restless or violent and some may require sedation to travel safely. People travelling with sick horses should not put themselves in danger if a horse tries to go down in a trailer. If a horse goes down in a trailer, the horse should be taken to a hospital as quickly as possible; attempting to extract a horse from a trailer on the side of a busy road is unwise and may result in dangerous delays.
Fractured limbs With any suspected or diagnosed fracture, a vet must apply proper support and splinting before moving the horse, because travel can exacerbate the injury. Great care should be taken when loading, transporting and unloading animals with limb splints. A horse with a suspected fracture should travel with the affected limb facing the back of the trailer as horses need two good limbs to support themselves during braking.

BAsiC EquinE mAnAgEmEnT
17
care. Conditions such as thrush occur in dirty stable conditions. It should be noted that youngsters and unshod horses turned away to grass still require regular foot care and attention.
To lift a horse’s foot, the handler should stand facing the tail of the horse and run the hand down the back of the leg. Most horses are trained to respond to gentle pressure over the tendons by lifting their leg. The front legs can be held by positioning one leg on either side of the foot and grasping the hoof between your thighs. The hind leg can be held by sliding the cannon bone across your thigh and balancing the hoof between your thighs. (Fig. 1.12)
How frequently a horse is shod depends on the type of work it is doing, how fast its feet grow and are worn, and whether it needs special remedial shoes. Typically a horse is shod every 6–8 weeks.
Removing a shoe
A shoe is removed in three stages.(1) Raising the clenches, by placing the blade of a buffer under each clench and giving it a sharp blow with the shoeing hammer. It is important to fully raise the clenches as otherwise they can tear the hoof wall as the shoe is pulled off.(2) Using the farrier’s pinchers (also referred to as pulloffs), the inside heel of the shoe is pulled away from the foot towards the toe, and to the inside. This is continued alternately along each branch until the shoe is loose.(3) At this point the shoe can be grasped at the toe and pulled backwards across the foot and off. Most
the clippers should be stripped, cleaned and oiled before storage. Since some infectious diseases such as ringworm and staphylococcal dermatitis can be spread by clippers, thorough disinfection between horses is essential. Most clipper lubricants are also disinfectants.
Preparation of sites for ultrasound examination
Skin preparation is a fundamental requirement for any ultrasound examination. Although asepsis is not required, thorough cleaning of the area as for surgical preparation is recommended. This degreases the skin, facilitating better contact between the probe and the skin. Even better contact is afforded if the gel is allowed to soak in for 10 min before scanning.
Bathing horses
Nonmedical reasons include bathing for the removal of sweat, dirt and scurf, and for aesthetic reasons. Horse shampoos can wash away the natural oils of the coat and therefore should not be overused.
When horses suffer from various parasitic infections and skin diseases, bathing with medical preparations may be necessary. Medical bathing should always be with warm water both for the washing process and for the subsequent rinsing. Medical reasons for bathing horses include:• mud fever, rain scald and staphylococcal dermatitis• ringworm (dermatophytosis)• lice infestation (pediculosis).Medicated shampoos or washes are sometimes prescribed by the vet for specific skin conditions.
Basic hoof care
Daily foot care
Daily care of the feet is vital. This involves picking out the horse’s feet and cleaning away debris with a hoof pick and stiff brush. This should be performed at least once daily, and should be performed each time the horse returns from work. Picking out the feet before a horse leaves its stable is sensible and helps to limit the contamination and littering of the yard surfaces. Stable hygiene is also a vital part of foot
Fig. 1.12 How to hold a hind foot to examine it with hoof testers in the other hand.

CHAPTER 1
18
RaspThe rasp is a long, thin rectangular piece of metal that has sets of metal teeth on both sides as well as at the edges. On one side the teeth are longer and angle towards the handle. This side is used for coarse work, such as levelling the foot after trimming. The other side of the rasp usually has a crosshatched pattern that is used for finishing the foot or smoothing off any rough areas of metal. This side of the rasp can be used to remove nail clenches prior to pulling the shoes.
NippersNippers are used for removing larger portions of the outer hoof wall, most commonly when trimming the foot. The handles are opened and closed while perpendicular to the foot in order to maintain a flat weightbearing surface. They should never be used to remove shoes because this will damage the blades.
Cleaning and preparation of the foot
Extensive cleaning and preparation is often required for radiographic investigation of the foot. For a full examination, the shoes must be removed. Dirt will create artefacts on radiographic images so the foot should be well picked out. Putty or ‘play dough’ should be used to pack the frog to reduce artefact. Similar cleaning of the foot (without packing) is often required when horses are taken into the operating theatre, in order to reduce contamination.
General stable equipment
grooming equipment
Grooming is carried out in order to promote good health of the coat and skin, as well as for aesthetic reasons. The key items include brushes, curry combs and hoofcare equipment. Plastic and rubber curry combs are used to remove dried mud, sweat and dead hair. Metal curry combs are used to clean the brushes, not the horse. Dandy brushes are designed to remove heavy dirt from a horse’s coat. Body brushes are softer and are used on the body, mane and tail for the removal of fine dust, scurf and grease from the coat. Mane and tail combs, scissors and sweat scrapers are just some of the many additional items that may be found in a grooming kit.
pinchers have knobs at the ends so they are less likely to be confused with nippers.Alternatively, a nail puller is an effective tool for removing each nail individually after raising the clenches (Fig. 1.13). The nail should be removed by grasping the head of the nail and pulling it towards the toe. It is important that nails are safely disposed of immediately, to reduce the risk of the horse treading on them.
Chaps or a farrier’s apron are very useful for protection while removing shoes and handling feet.
Farrier’s tools
Hoof testersHoof testers are useful in identifying generalised or focal pain in the foot. Generally hoof testers are used prior to paring with hoof knives when an abscess is suspected, because it is important to localise sensitivity within the foot.
Hoof knivesThe basic style has a curved handle with a blade that is gently curved throughout its body, with a sharp hook at the end. There are several sizes and a variety of shapes including a full circle blade; each knife has a different role. Hoof knives are used to remove dead sole from the bottom of the horse’s foot and to trim the frog. These knives are used also to search the foot for abscesses. It is vital that they are kept very sharp. Blunt knives often cause more injuries than very sharp ones as extra force has to be applied.
Fig. 1.13 Common farrier tools include (left to right) a rasp, shoe pullers, nippers, nail pullers, hoof testers, and buffer.

BAsiC EquinE mAnAgEmEnT
19
bandaging is used after strenuous exercise to reduce synovial effusions such as windgalls (digital sheath effusions). Stable bandages are frequently made of nonelastic material. Overtight or fixed bandages (with velcro fastening around the leg) are potentially very dangerous, particularly if the leg swells at all. They must not be left on for longer than necessary
In veterinary situations stable bandages have some specific roles, e.g. a serious limb injury on one leg means that the contralateral (opposite) leg will be bearing extra weight, so a firm stable bandage may help by providing support.
Exercise bandagesExercise bandages are used primarily to protect the digital flexor tendons from injuries such as overreaches and trauma. They are not as impact resistant
All items should be cleaned and disinfected regularly and since they are a potential source of bacteria and fungi, grooming kits should be confined to one horse. Checking brushes after grooming can be a useful diagnostic tool for skin diseases. For example, examining brushings either with the naked eye or under the microscope can reveal mites such as Trom-bicula autumnalis (harvest mites) and lice.
Rugs
Rugs can be important fomites in the transmission of contagious diseases, particularly ringworm. Restricting rugs to one individual is a sensible precaution in controlling infection. There are many types of rugs that are useful in different circumstances including heavy waterproof turnout rugs, stable rugs, cooling sheets, and fly sheets. Rugs must be washed or cleaned regularly.
Bandages
Bandages should be applied with even pressure, so that they do not cross or rub bony prominences. The frequency with which a bandage should be changed depends on the type of bandage and its purpose. A bandaged horse should be checked daily for rubs and sores.
Tail bandagesAny veterinary examination involving the perineal region is greatly facilitated by the application of a tail bandage. This is particularly important during gynaecological work, hind limb lameness investigation or evaluation of traumatic wounds. Full tail bandages for horses with diarrhoea are also very useful in reducing contamination and keeping the perineal area clean. A rectal sleeve over the bandage is also very useful (Fig. 1.14). Full tail bandages should be applied also before a horse enters the operating theatre, in order to reduce contamination. It is very important however that tail bandages are not over tightened or left on for too long.
Stable and travelling bandagesThese bandages require some form of conforming material between the leg and the bandage to ensure even pressure distribution. They provide protection against trauma and support to the limb. Traditionally
Fig. 1.14 Tail bandages and plastic bags or rectal sleeves can be useful when nursing patients with diarrhoea.

CHAPTER 1
20
be difficult. It is suggested that a decision be based on the colour of the hairs of the muzzle.
BlackThe skin, mane, tail and body hair are black. No other colour is present except that white markings on the face and limbs are permitted.
as boots, but are conforming, which is important for horses in fast work.
Boots
There are many types of boots used to protect equine legs. The most common types of boots include brushing boots, overreach boots, and travelling (or shipping) boots. Brushing boots are used to prevent injury that occurs when the supporting limb is struck by its advancing partner. Over-reach boots prevent injury which is produced by the advancing hindfoot on the back of the forelimb of the same side. Travelling boots are commonly used in place of stable bandages during transport.
Riding tack
A saddle, saddle pad, girth, and bridle are the basic tack required for riding. Proper fitting and regular care are important for the longevity of the equipment as well as the health of the horse. All tack and harnesses have the potential to cause serious rubs and sores. It is critical that it is fitted properly and maintained carefully. See further reading.
Identification
Identifying an individual horse relies on noting their individual natural features (i.e. markings) or using an acquired method of marking, e.g. microchipping or freeze branding. Different marking forms vary slightly in their horse outlines and also in the information required. However, in general the following rules apply:• any white marking on the horse must be shown in red and any other marks shown in black on the form.• the narrative and the completed diagram must agree.Further information is available in the Box 1.2 above and in the booklet entitled Colours and markings of horses, published by the RCVS.
Colours
There are five basic coat colours in horses. These are grey, black, brown, bay and chestnut, but deciding the true colour, particularly of a foal, can sometimes
Box 1.2 Identification of a horse
• Whorls occur where there is a change in direction of flow of the hair, usually radiating from a single point whorls must be indicated by an ‘x’ in the case of simple or tufted whorls. Linear and feathered whorls are indicated by placing an ‘x’ where the whorl starts and a line from this to indicate the direction and extent of the whorl.• White markings are outlined in red and hatched in with red diagonal lines. A few white hairs may be indicated by a few short lines in red. White markings from surgery, freeze branding, etc. should be indicated as for other white markings.• Bordered markings should be indicated using a double line.• Flesh marks. These should be outlined and shaded completely in red. Any spots on the mark should be outlined in black and left unshaded.• The prophets thumb mark. This is a natural dimple in the muscle, usually on the neck, which is shown on the diagram by a black triangle.• Permanent scars should be arrowed.• Others: hairs of a different colour on parts of the coat should be described with accuracy. if the horse has the ears nicked, this should be stated in the description; wall eyes (lack of pigment in the iris, causing the eye to be blue/grey in colour) should be noted. some authorities require that chestnuts (horny deposits on insides of limbs) are marked on the forms for whole coloured or grey animals.

BAsiC EquinE mAnAgEmEnT
21
SkewbaldThe coat consists of large irregular patches of white and any other colour except black. The line of demarcation between the patches is usually well defined.
PiebaldThe coat consists of large irregular patches of white and black. The patches are well defined.
Odd colouredThe coat consists of large irregular patches of white and more than one other colour. In North America, coloured horses are also referred to as ‘paints’ if they are registered or ‘pintos’ if they are not. Paint horses are further classified as overos or tobianos.
AlbinoThere is no pigmentation of the skin or hair (which is therefore white). The eyes are also devoid of pigment and are pink in colour.
gender
The gender of an animal and whether it is neutered should be noted on identification forms. A mature intact male is called a stallion. A castrated mature male horse is called a gelding. A mature female horse is called a mare. An immature male horse is called a colt. An immature female horse is called a filly.
Height
The horse should be measured on level ground from the floor to the height of the withers. A pony measures less than 148 cm at the level of the withers. The height of an animal at the time of completion of the official documents should be stated in centimetres (Fig. 1.15a&b).
Acquired identification marks
TattoosTattoos are rare in the UK, but they are sometimes found on the inside of the upper lip.
Hoof burnsThese are not strictly permanent markings because they grow out with hoof growth. Occasionally hooves
BrownThe skin is dark and the coat hairs are a mixture of black and chocolate. The limbs, mane and tail are brown or black.
BayThe coat is dark red to yellowish brown in colour, while the mane, tail and lower limbs are black. Black on the limbs is referred to as black points.
ChestnutA chestnut horse has red hairs in its coat. The proportion of yellow hair varies to give a coat that ranges in colour from dark reddish brown (liver chestnut) to light reddish brown.
Palamino/cremelloA palamino could be considered a type of chestnut as they have a genetic dilution of the chestnut gene. The body hairs are a bright golden yellow, while the mane and tail are flaxen or white. A cremello is a palamino with a second dilution of the chestnut gene, making its coat a very pale golden colour.
DunDun colours are the result of dilution of the basic coat colour, while the mane and tail remain dark. For example, a yellow dun, which is a dilution of a bay horse, has a dark skin and yellow or tan hair with a black mane and tail. A withers stripe, list (or dorsal stripe) and zebra markings are often present in duns.
RoanA roan horse has a body colour that consists of a mixture of white and coloured hairs in approximately equal quantities. The solid colour tends to predominate on the head and the limbs with white hairs interspersed on the body giving a lightened effect to the colour. Types of roans include blue roan, red roan, and bay roan. A roan differs from a grey horse in that their coat does not become whiter with age.
GreyThe coat of a grey horse is an uneven mixture of white and dark coloured hairs with the skin darkly pigmented. As the animal ages, the coat becomes whiter. Foals are rarely born grey but become grey when they lose their foal coat.

CHAPTER 1
22
these markings to be placed on the back just behind the withers, to the left of the midline. Less commonly they are seen on the neck or shoulder (Fig. 1.16).
Hot brandingRedhot irons are applied to the skin to burn and scar it, so hair growth is affected. Although there are welfare questions asked, this method of identification is still used for certain breeds, particularly mountain and moorland ponies and warmbloods (Fig. 1.17).
MicrochippingThis form of identification is also organised as a national scheme, so that each microchip Code is different. A small chip is implanted on the left side of the middle third of the neck, into the ligamentum nuchae 2.5–3.75 cm from the dorsal midline (1.25 cm in foals). The chip is read using an electronic machine that reads the individual Code (Fig. 1.18).
All foals born in the UK must now be implanted with a microchip by a vet. These are implanted in the same place as other microchips. Microchips are being used increasingly as a means of permanent identification and are part of the equine passport system in the UK.
are still burnt, usually by the farrier, with post Codes or other individual marks.
Freeze brandsThis method of marking is now common. There is a national scheme such that no two horses have the same number and letter combination. Very cold blocks in the shape of letters or numbers are applied to the skin of the animal. This causes a scar, and subsequent hair growth is white. It is common for
Fig. 1.15 Images showing a pony’s height being measured with (a) a traditional stick and (b) a laser device.
a
b
Fig. 1.16 The freeze brand on the right above identifies the horse as the subject of a settled permanent incapacity insurance claim and the other symbol (
Ω
) on left indicates a microchip has been implanted.

BAsiC EquinE mAnAgEmEnT
23
Breeds
There are hundreds of breeds of horses worldwide. Generally horses can be described as being cold, warm, or hotblooded. Coldblooded horses refer to gentle, quiet horses of large build which are draft breeds. A hotblooded horse is a more spirited horse that is fine boned, classically a thoroughbred or Arabiantype horses. A warmblood is a classification of horse that falls in between the previous two, such horses being of medium build and generally quiet temperament.
Fig. 1.17 Some examples of common hot brands. All German Warmbloods used three breeds as foundation stock, with other breeding then being introduced. These
three breeds are the Hanoverian, the Trakehner and the Holstein. The English Thoroughbred (Engl Vollblut) is in the top righthand corner.
WESTFALEN TRAKEHNER (Bundeszucht)HANNOVERANER
ZWEIBRüCKEN RHEINLAND HESSEN
OLDENBURGER HOLSTEINER OSTFRIESE
WüRTTEMBERGER HAUPT- und LANDGESTüTMARBACH
BAYERN
MECKLENBURGER BRANDENBURGER ENGL. VOLLBLUT
ARAB. VOLLBLUT Kleinpf. SCHLESWIG- HOLSTEIN
HAFLINGER
Nord- u. Westd.Kleinpf.u. Ponyu. Pony
Mittel- u.Südd.Kleinpf. Dülmener Brand
Hessen Westfalen Haflinger in Nordhessen
Fig. 1.18 A microchip scanner being used.

CHAPTER 1
24
Henderson C. (2009) Horse Tack Bible, David & Charles PLC, Newton Abbot.
McGreevy P. (2004) Equine Behavior. Saunders, LondonNational Association of State Public Health Veterinarians
(2010) Compendium of Veterinary Standard Precautions for Zoonotic Disease Prevention in Veterinary Personnel. JAVMA 237 (12) 1403–1422.
RCVS, Weatherby’s, BEVA (1930) Identification of Horses (revised 2005). RCVS, London.
Spiers V. (1997) Clinical Examination of Horses. Saunders, Philadelphia.
Further reading
Brazil T.J. (1995) Isolation of infectious equine cases. Equine Vet. Educ. 7 (4) 220–224.
Colles C. & Ware R. (2010) The Principles of Farriery, J.A. Allen, London.
Devereux S. (2006) In: K.M. Coumbe, Ed. The Veterinary Care of the Horse, 2nd edn. J.A. Allen, London
Dwyer R.M. (1992) Practical methods of disinfection and management during outbreaks of infectious disease. Proc. Am. Assoc. Equine Pract. 38, 381–388.
Revised from the first edition of this chapter written by L.C. Marlborough & D.C. Knottenbelt