Embed Size (px)
Citation preview

Equality, Efficiency, and Market Fundamentals: The Dynamics of International Medical Care Reform.
CitationCutler, David. 2002. Equality, efficiency, and market fundamentals: The dynamics of international medical care reform. Journal of Economic Literature 40(3): 881-906.
Published Versionhttp://dx.doi.org/10.1257/002205102760273814
Permanent linkhttp://nrs.harvard.edu/urn-3:HUL.InstRepos:2640584
Terms of UseThis article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http://nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of-use#LAA
Share Your StoryThe Harvard community has made this article openly available.Please share how this access benefits you. Submit a story .
Accessibility

Journal of ricononnc LiterattircVol. XL (SqAemher 2002) pp. 8HI-906
Equality, Efficiency,and Market Fundamentals:
The Dynamics of InternationalMedical-Care Reform
DAVID M . CUTLER'
1. Introduction
I s NO COUNTHV are people particularlyhappy with their health-care system. In a
survey ol people in ficveial countries, KarenDonelan and colleagnes asked respondents toreact to the statement: "On the whole, theheLilth system works prett\' well, and only mi-nor changes are necessary to make it workbetter" (Donelan et al. 1999). In the UnitedStates, only 17 percent of people agree withthe statement; 83 percent perceive the needfor "fimdamonta! change" or "complete re-building."" In Canada, with universal insur-ance coverage and medical spending as ashare of CIDP at 70 percent ofthe U.S. level,only 20 percent ol people agree with thestatement. In the United Kingdom, with.spending us a share of (iDP at hall the U.S.le\ el and overall health nieitsures just as good,only 25 percent agree with the statement. In
' Department ol FLConomics. Harvard University,aud NBER. I am graletn! to Monica Sinf luil lor expertresearcb a.ssist;uice. to Jobn McMillan and tbree anony-nions reterees tor belpfnl comments, and to tbeNational Institutes on Aiding lor researcb support.
- Tlic otber response.s ure: "There are .some goodtilings in our health-care system, but lundamentalfhanecN are needed to make it work better," and "Ourheidtli-care sy.stein lias so mucli wrong witb it that we
d to coiripletely rebuild it."
AustnUia and New Zieiiland, support is 19 per-cent and 9 percent respectively. Granted,health care is a diffieult issne for societies. Bntwhy such great discontent?
Medical care is snch a problem, I argue,beeanse it is fundamentally a setting of con-ilicting goals. Methca! systems developedwith clear equity considerations. In most de-veloped conntries, universal insurance cov-erage was designed to guarantee equal ac-cess to medical care for all. Solidarity inhealth care dictated no rationing by price.
The classic tradeoff in economics is be-tween equity and efficiency, and this showsup in medical care. Efficiency was not agreat concern when health systems were es-tablished; conntries were content to have in-efficient medical-care systems provided theytreated all equally.
But the equality-efficiency balance hasbeen thrown into conflict by the fnndamen-tals of the medical-care market. Medicaleosts have increased rapidly over time, astechnological change has expanded the ea-pability of medicine. Since 1960, medicalcare has more tban doubled as a share ofGDP. The result of this technological changeis that govennnents face increasingly severefinaneing erises. Many countries can no
881

882 Joutiial of Economic Literature, Vol. XL (September 2002)
lotiger afford the coiiimitnient to completeequalit)' tliat they once coiikl.
The Rrst response of most countries to theproblem of rising costs was the enactment ofregtilatoty limits on costs. These hmits wereincrcLisingly pre\a]ent in the 1970s and1980s. Govemtnents reduced provider feesand rationed access to medical technolog)'.Cost growth slowed quite a bit. Comparedto the United States, which never had wide-scale limitations, medical costs in other de-veloped countries teli from about 90 percentof the U.S. level as a share of GDP to about65 percent of tliat level. Further, health out-comes did not seetn to stiffer. A decade intothese rationing systems, overall satisfactionwith medical eare was higli.
But recent years have made the regulatoiysolution increasingly less attractive. Themareli o( tcchnologv' has continued, even inregulated systems. Mediciil-care cost growthresnmed when expenditure controls were notactively being tightened. Further, cost con-trols have nuide the lack of efficiency morenoticeable. Waiting lines and access testric-tions have become increasitigly important is-sues as the constraints increase in intensity.
As a result, the regulatoiy solution to med-ical care is cotiiing tmder disfavor. In manycountries, there is an incipient movementaway from regnlation arid towards market-based solntions to medical-care problems.Countries are introducing competition intomedical care and in some cases providing in-centives for people to ttse less medical careand to choose less-expensive health insuranceplans. Providers are being asked to considercosts in their care decisiotis as well.
Iiieentive reforms bring the potential forcost savings withottt painful pulilie cuts. Thatis why countries are attracted to them. Butincentive reforms bring conflict as well,Priee-govenied systems are not as equitableas the older systems they replace. The poordo not have the sauie access to medical careas the rich when prices are used to rationcare. Fttrther, less-healthy people may suffercompared to the healthy. And incentive sys-
tetns may restrict access to some pro\'iders.One way that money is saved in medieul eareis to limit the providers one contracts with,and n.se the exclusiou power to negotiatelower prices. But abandoning the commit-ment to equality" of access is not easy. As a re-sult, there has been great reluctance to tisecompetitive measures to their fullest extent.Many countties are tiow exploring the properscope and applieation of incetitives in med-ical care. How couutries resolve this debatewill have major implications for the worldsniedical-eare systems for decades to come.
In this paper, I trace tlic histoiy oi interna-tional niedical-eate reform and lay out the is-snes today. I begin in section 2 with a discus-sion ofthe birth ol ttuiversal systetns. Section3 then examines the move to controls andrationing. Seetion 4 considers the effects ofexpenditure constraints on the prtnisionof medical eare. Section 5 discusses theproblems with rationed systems, and section 6examines the new wave of reform.
2. The First Wave of Hectlth-Care Refomi:Universal Coverage and Ecfual Access
The late nineteenth centurv' saw the be-ginnings of health insurance in most devel-oped countries.'^ Mutual aid societies, orsickness fimds, were formed for some work-ers, In some coutitries, snch as Geriuauy,"*the development was spurred by the centralgovernment. More frequently it took placeill the pri\ate sector.
But even ;is late as \\'orld War 2, access tomedical care was not a paitieularly high prior-it\' for tJie public sector. In part, the desire for
' M("cliail aiR' is (.lifft re'iit in cle\'flo[>ed and dcvt'lop-ing countries. My ston- is largely one of rich, developedcountries, where generous insurance systeuis arc af-fordable and desirable. Thus. I aniilyze the OECIDcountries, paiiicnlarly the CiT,
In his ijuest for riation-iniikliiig in the late 19th ceii-tun, Bismarck feared that tniddle-cliLSS CJeniiaus wouldsnpport sofiiJists n\'er the monarchy. He thus introduceda series of .social insurance programs—most prominentlvold-age insurance and he;iltli insurance—to gi\'e the niitl-dle-cliiss a stake in the snr\i\;il of the govenmient, DavidCnller and Hiehiud Johnson (21H)I) disenss ihe biitli ofsociiil insurance progranLS in more detail.

Cutler: International Medical-Care Reform 883
medical insurance was limited because tlierewiLs little that medical care could do foi" sickpeople. Panl Starr (1982) traces the tnuisfor-mation ol the American medical system. Starrnotes that medical knowledge was poor in thisperiod, ancl it was not until the mid twentietlicentnrv' that tlie medicii! profession was seenas a significant laetor in helping to cure dis-ease. In atldition, medicid insiiranct was rarelyhigh in families' economic priorities beeanseniftlic'ul costs were not particularly variable.With little to do lor sick people, the financiiilrisk dissociated with being siek was low. Tbe in-surance that was available for sickness fre-qnently covered lost wages, not medical costs.
World War 2 cbanged the situation sub-stantially (Starr 1982). Advances in penicillinand other antibiotics convinced people thatmedical care was Viilnable. Conntries wantedto reward tbemselves for years of strnggle.Qnasi-socialist governments elected after thewar wanted to expand tbe role oftlie state intbe provision of basic needs. The result was amajor emphasis on expanding health insur-ance coverage. Table 1 sbows tbe creation olnational medical-care systems in G7 eoim-tries.' Tbe lirst post-war reform was in tbeUnited Kingdom. The Beveridge Report of1942 delineated tbe inadequacies of tbeprior system aud recommended a goal of na-tional bealtb insurance coverage.*"" Tbis goalwas met in 1946, witb the passage of tbeNational Ilealtb Sendee (NHS) Act; tbeNIIS began formal operation iu 1948.
Tbe Britisb system was followed, someyears later, by tbe Japanese system
•' Nniricrons cl;itu soiirfes were n.sed in creating tbetiilile.s ol"conntr\' features. Tbe OECD (19^51 andRoenier (I9i)l) ]i;i\e nnit-li inlornmtion, along witbcite.s to otlu'r articles witb more lietail.s.
'' In 1941, an iiiterdcpartTnciitjil connnittce on SocialIiisinance and Allied Senices w;i.s appointed to .surveythe existing schenie.s ol social in.suranee. Tbe eoniinis-sioii made a "diagnosis ot want" by snr\ eying conditionsol liie in a nnnihcr ol towTis in Britain. Tbe BeveridgeReport ci)nclnded that abolition of want required a re-distribntion ot ineonic tbrougb scK'ial insuraiicc and bytaniily Tieeds. Tlif report rfconiuiended a (.•oniprchcn-sive national health service to provide lull ai'ces.s to allbeneficial treatments without economic barriers(Beveridge t942>.
(1958-61), tbe Canadian .system (1966-71),and tbe Frencb system (1967). In all of tbeseconntries, universal coverage was tbe cnlmi-nation of many years of partial coverage andgovernment subsidies for insurance. Morerecent universal systems were finallyacbieved in Italy (1978) and Germany, al-tbougb in both cases coverage rates wereveiy bigb just prior to tbe universal legisla-tion (Milton Roemer 1991). Tbe only C7conntnwitbout a universtil bealtb insuranceprogram is tbe United States, altbough itdoes bave a program for tbe elderly(Medicare) aud a program for the poor(Medicaid). Indeed, within the OECD(prior to its recent expansion), only Turkeyand tbe United States were witboiit nniver-sal insurance coverage.
Beyond jnst desiring universal coverage,countries wanted to ensure that tbe poorbad tbe same access to medical care as tbericb. Medical care was perceived as a rigbt,not a good, and markets were not lookedupon witb favor. For example, tbe BeveridgeCommission stated. "From tbe standpoint ofSocial Security, a bealtb serviee providingfnll preventive and cnrative treatment ofeveiy kind to every citizen without excep-tions, witbout remuneration limits and witb-ont an econoune barrier at any poiut to delayrecourse to it, is the ideal plan" (Part VI, see.437). Similarly, tbe Canada Healtb Act of1984 stated. "It is bereby declared tbat tbepriniar) objective of ( ianadian healtb carepolicy is to protect, promote, and restore tbepbysical and mental well-being of residentsof Canada and to facilitate reasonable accessto healtb services witbout fniancial or otberbarriers" (cb. 6, sec. 3).
Tbese sentiments bad fundamental impli-cations for tbe design of medical-care sys-tems. Tbey led medical systems to be ex-tremely generous iu covered services audlow in required cost-sbaring. At least tbiswas true for acnte medical care, wbicb tvpi-eally aeeounts for about 70 percent of totalspending. Table 2 sbows tbe cbaracteristicsof universal bealtb insurance systems

884 Jotimal of Econotnie Literature, Vol. XL (September 2002)
TABLE ]TUECREATU)\ OF UM\'i:ii,s,\i,Cu\L:h,\(;E SVSTKMS
Iiistor\' of Insurance Coverage
Canada
France
CeiiTiiinv
Italy
United Kingdom
United States
1947: First provincial health insurance program1966: Medicare established1971: Last province enacts Medicare,
Late 19'" centur\: Loeal sickness timds for certain workt i\s1928: Compulsory liealth insurance for low-wage workers in certain industries1967: National insurance tund for salaried workers: agricultnnil and self-employed
covered by other funds1978: Universal coverage achieved.
1 SS.3: Industrial workers u1th low wages covered fiy sickness fuiuLs1981: 90% coverage achieved, (Coverage remains at approximately 9()% today.
Post-W'W'II: Mutual aid societies converted to local branches of national insuranceprogram (by 1970s, 90% coverage)
1978: National heallh service created.
1922: Health Insunmce Law covered some workers (extended in 1938)1958: National Health insurance mandated1961: All local go\eninients implement.
1911: Maimal workers and low-wage w{)rkers coveredCoverage increased over time:1946: National health insurance pas,sed1948: NHS implemented.
1965: Medicare and Medicaid created.
around the 198()s and early 199()s." In al-most all countries, covered benefits werevery generotts. It is easier to report the ser-vices excluded from coverage than the ser-vices incktded. Excluded services iueludeddental care in some countries, visiou andbearing aids, and oceasionally otttpatientprescription dnigs. In countries where theseservices were excluded as a genera! rule,sueh as Canada and the United States, thepnblic set-tor sometimes covered the costsfor the poor. Indeed, some countries hadstieh generous services that they covered spabetiefits (Germany).
' The United States row in ta!)Ie 2 reports the provi-sions of the Medicare program, Medieaid programswere more generou.s at tnis time.
Furthet; there were few restrictious on us-ing covered seiMces. In all countries, pa-tients had free choiee of primary careproviders, and cost-sharing for covered ser-vices was minimal. In many countries(Canada, Cermany, Italy, and the UnitedKingdom), access to some or ail physieiansand hospitals is nearly free. Among thesecoimtries, only Italy has any cost-sharing forspecialist physicians, but the cost-sharing isquite modest. Prescription drugs are some-what less well insured but often still covered.
Three of the conntries (France. Japan,and the United States) have more extensivecost-sharing. In France, coinsnrauce ratesior pliysician senices are 25 pereent, al-thongh 80 percent oi the population has stip-plemental itisttrance to cover the pliysieian

Tin;TABLE 2
!>!• HKMTII I \SL K.-\M:E SYSTEMS AHOIM.) 19S0
Demand-side SiippK-sidc
Cost Sharing For:'
Exclusions Primary Oulpati<'ulfrom Care Pharma- Hospital Hospital
Country Coverage" Phy.sician Specialist Hospital ueiiticals Ownership Payment
(Canada Outpatienttieutal am!
pharitiiifeiitiaJ;soniepn)St!ieses;
glasses ami
None None None X'arie.s h\'province
Over 95'2private
Clohalbudget
Payment
Fce-for-service
France
Germany
Italy
Japan
U.K.
U.S.Fei'-for-
Eyeglasses,some dent;il
care
None
None
Inocnlatirjiis;eyeglasses
Dentalaud \isi()n
Out
None
None
1(^30%
None
patient
pharinaueu-Heals: nnitinetiental and\ is i i i i i ; long-
Noti': " Stjine exceptions are inatle
25% S.5-SKpei-da\' aud
2()9f up to30 days
None S3 for 14(Li\Ti (niiuiv
exemptions)
S7-$8 None(max
ofSi41)
10-309* 10-30%
None S4-S5
Deductible ($100);
eoiiismance (20%i),SS()O)
for the elderlv and poor.
30% to 6O9'(
S1.25/dn,g
{witb
eiiceptions)
0 to 50%
1O-3O9'(.
None
Deduct ibl
(about
puliiic
Pnl)lic(:5.5%)and private
(6.5%)
V!ost pnlilic(>507<)
Mostly pul)lic;some
religions oruiiiversitv
Mostlypri\'ate
(80%.); somelarge pnblkr
teaehiughospitiils
I'ublie
Publichospitals
have aglobal
limlget;pri\-ate fee-for-service
Per diem
Per diem
Fee-for-service
Globalbudget
MostK'
private; services i iu ie
""Cost sbaring is around 1993.
PredoDi-inantKfee-for-serviee
(salary inpnlilicsector)
Fee-for-service in
ambulatorysector;
salary inhospitalsector
f:apitationfor GPs;salarv orother forspecialists
Fee-for-service in
ambulatorysector.salar\- inhospitalsector
Salaiy
Fee-f"or-
service

886 Journal of Economic Literature, Vol. XL (Septetnber 2002)
cost-sharing {OECD 1995), Hospital cost-sharing is much lower. In Japan, coinsurancerates are 10 to 30 percent for all services. InMedicare in the United States, cost-sharingfor physician services is relatively small, hutcost-sharing for hospitals is much larger(there is a deductible of one day of hospitalcare—about SSOO currently), and outpatientprescription drtigs are not covered at all.Still, many elderly have supplemental insur-ance to pay for these costs.
The result was tliat in most countries,there were very few demand-side con-straints on utilization. As one indicator ofthis, the government paid for 72 percent ofmedical care in the average G7 country, and76 percent outside the United States. Socialand not individual financing was the goal.Economists might worry about moral haz-ard, hut governments were more worriedabout equity.
On the supply side, the systems were en-couraging as well. In five of the coimtries—Canada, France (outside the public sector),Germany (ambulatory care), Japan (ambn-latory care), and the United States—physi-cians were predominantly paid on a fee-for-service (piece-rate) basis. In such a system,doctors that do more collect additional in-come; provided price is above marginalcost, the incentives to limit care to situa-tions where it is truly appropriate arcweak.^
A second alternative is to salary physi-cians. This was the route chosen in theUnited Kingdom and for selected specialtiesin France (public sector), Cermany {Jiospi-tal-based physicians), Italy (hospital-basedphysicians), and Japan (specialists). Evensalaried physicians had weak incentives tohmit spending; doctors did not suffer fhian-cially if unnecessary care was provided.
** George Bernard Shaw (1911) laiiiented tbis almosta eentury ago: "That any sane nation, having ohse'rvetitiiat yon eoiild provide for tbe supply ol bread b)' givinghaker.s ;t pee^uliar^• interest in baking for you, should goon ti) give a surgeon a pecuniary interest in eiittinj^ oH'your leg, is enough to make one despair of politicalnil inanity."
A third alternative chosen in some coun-tries is to pay physicians on a capitation ba-sis—doctors receive a fixed amount ofmoney per patient in return for providingmedical services as needed, at no additionalcharge for each service. Included in the cap-itation amount is the physicians' own timeand sometimes other services such as hospi-tal care or prescription drug costs. Italy andthe United Kingdom used this payment sys-tem for some doctors. Capitated systems canprovide strong incentives to limit medicalcosts. But the capitated systems countriesput in place were generally not very strin-gent. Many nouphysician services were notincluded in the capitation amount; surplusftmds could not be retained by the doctor;and the ability to negotiate with downstreamproviders was limited. No country had a sys-tem like what is evolving in the UnitedStates today, where doctors are at risk formost of the care their patients receive andhave large income fluctuations on that basis.As a result, access to physician services waslargely unconstrained.
Hospital payment was also relatively gen-erous, although more diverse. In manycountries, the public sector ran at least someof the hospitals. The extent of public owner-ship ranged from very little (Canada, theUnited States, and Japan—20 pereent orless) to more moderate levels (France—35percent; Germany—over 50 percent) tonearly all of the hospital system (Italy, theUnited Kingdom). In countries where thepublie sector ran the hospitals, hospitalswere topically financed as line items in thebudget. When hospitals were private, theywere often paid through global budgets-^hospitals were given a fixed auiount of fundsfor the year to cover the costs they incurredin caring for tlieir patients. Global budgetswere often coupled with public review ofhospital investment decisions, for examplefor bed expansion or purchase of capitaleqviipnient.
Global payment systems can be constrain-ing-—and later were—but frequently were

Cutler: Intemationai Medical-Care Reform SS7
not at tlif time tlir systems were set up.Oltcn, the puhlic sector paid for hospitaldeficits at the end of the year, as in Italy. Inother cases, the global budgets were ad-justed for costs in previous years or were setat deliberately high levels. Still other eoun-tries had fee-for-service payment for hospi-tals (Japan, the United States), creating thesame iucentives on the inpatient side as theydid on the outpatient side.
Arthur Okiui (1975) highhghted oue ofthe classic tradeoffs in eeouoniics, betweenefficiency and distributiou. Achieving amore equal tlistribntion ot resources thanmarkets naturally provide geuerally requiresinakiug markets less effieient. Iu the med-ieal-care context, distributiou was a clearpriority over effieieuey. Eveu the rhetoric ofuniversal insurauce coverage stressed distri-butional equity over economie effieietiey. By1980, countries in the GT, and in the devel-oped world as a whole, had set up niedieal-eare systems designed to encourage accessto Tuedieal eare but not t(j promote the offi-cieut deliveiy oi care.
3. The Seeotid Wave: Controls, }^and ExfX'tuliftin- Caps
\\ itii few constraints on inedieai-care de-inaiul or supply, medical speuding wasbound to be inefficient. Countries werewilling to accept speudiug ahove efficientlevels to uieet distributional goals. Butspending was also growing more rapidlytliau eouutries eould easily afford. Whiletax revenues were inereasiug at the rate ofpayroll or consumption growth, roughly therate of GDP growth, medical care speud-ing was increasing twice as rapidly. In theaverage OECD country, medical care rosefrom 3.8 pereent of GDP iu 1960 to 7.2perctMit in 1980.
Medieal-care costs were increasing sorapidly in large part because of tlie growingteehnieal sophistication ol medical prac-tice. The development of new teehnoiogiesaud the diffii.siou of those technologies to
more patients led to large increases inspending. Empirical estimates by JosephNewhouse (1992) suggest that techuologi-cal change accounts for at least half of over-all cost growth, with the remainder result-ing from inereased prices of services andincreased use of existing teehnoiogies be-cause ot the spread of insurance. Sinee theexpansion in technology was worldwide, orperhaps U.S. driven, no other countrycould control its rate.
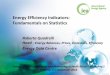
Figure 1 shows the inerease in the per-centage of GDP claimed by health care overvarious decades; tahle 3 shows summarydata. I examine spending relative to GDP toaccount for the income effect of medicalcare. As countries get richer, they naturallyspend more on medical care. Internationaleomparisons of medical spending geiierallysuggest an income elasticity at or ahove 1(Getzeu 2001), so it is natural to look atspending as a share of GDP.
The tirst bars in figure 1 are for the 1960s.In the CT7 countries, with the exeeption ofthe Uuited Kingdom (discussed helow),medieal spending as a share of GDP in-ereased substantially in this decade. Eveniueludiug the Uuited Kingdom, the increaseaveraged 1.6 percentage points. The in-erease wiis not limited to the G7 countries,as table 3 shows. Spending in the rest of theOEGD increased hy 1.3 percentage points.The pattern was repeated in the 1970s.Essentially all countries, with the exceptiouof Ganada, experienced rapid increases inmedical costs. The average growtb was again1.6 percent of GDP.
As medical spending increased, the bur-den on the puhlic sector grew. Tiix increasesto pay for rising medical costs were increas-ingly painful. Eurther, the mid-1970s saw areduction of income growth and the begin-ning ol structural puhlic deficits. This CUTI-vinced countries that they needed to man-age their medieal spendiug more actively.
The result was a gradiuil shift away fromconcentrating on the generosity of coverageand toward containing the eost of care.

888 Jonnial of Economic Literatnre, Vol. XL (September 2002)
4
oa.
^ F r a n c e EZ CtTinany CD Italy ^ Japan
Fif!,tiir 1. Increase in Medical Care a.s a Sliare of CIDP
Stnirre: Data ATV from OECD (2(HI(n. Duta f(ir Ceniianv itre iiiissiiiK [or lUfiOs. Last VL r of data is
UK US
Where "iiceess to medieal eare" liatl oiieebeen the pritnan' focits of public policy, "costcontainment" became equally itTiportant.
There are tvvo potential strategies for costcontainment. First, incentives can be usetlto indnce people to spend less. Some ser-vices miglit no longer he covered hy thepublic progiain, or cost-sharing might he in-creased. At the level ofinsurance purchases,people can he given financial incentives tochoose less-generous insurance plans, withlower overall cost.s. Doctors can also begiven stronger financial incentives tt> pro-vide less care. Alternati\ely, .spending can heconstrahied through regulation. Access totechnologies can he restricted, or expendi-ture caps imposed. Spending will thus belowered by fiat.
Regttlation was the soltition chosen in es-sentially all couutries. The details ot the im-plementation varied somewhat across coun-tries and types of services, hut the principles
were similar. Tahle 4 shows the nature ofthese conttol measttres. In the hospitiil sec-tot; countries with giohal btidgets tightenedthe budget limits. Hospitals had to live vvithless-rapidl\ increasing funds. Tliis was oftencoupled with tighter constraints on hospitalinvestment antl capacity expansion, to en-sure that aggregate utilization would not ex-ceed what was affordahle.
Budgeting physicians is more difficultthan htidgeting hospitals, since it is not feasi-ble to make individtial physicians hear all ofthe costs for services ttsed by their patients(hiring tile year. But alternative mechanismsare available. Many governments, for exam-ple Germany, imposed an overall spendinglimit for physician services as a whole or hyspecialty. Different activities were then as-signed relative weights, reflecting the re-sources involved in providing the services.The equilihrium price per tinit weight is setex post to meet the overall budget. In other

Cutler: International Medical-Care Reform 889
c;7RestofOKCD"
1960
4.23.6
TABLE 3
1970
5.S1.9
° Excludes Tiirkev and countries that joined the OECD in theSource: OECD i'lOlX)).
SliAHE ()!• G D P
t980
7.47.1
1990s.
1990
8.57.6
1996
9.4S.l
cases, fee schedules were tightened, butwithout an explicit spending target in mind.
These types ot expenditure controls re-quire suhstantial government involvementin tlie medical system, and countries covildnot implement them fully until the pnblicsector had enough authority over the systemto carry out the task. Thus, the evolution ofregvilation necessarily followed universal in-surance coverage. The earliest country withuniversal coverage, and the first to imple-ment tight constraints, was the UnitedKingdom. British doctors were paid on asalary or capitation hasis, and the puhlic sec-tor ran the hospitals, sinee the estahlishmentof the NHS. Thus, the British governmentwas in a nattiral position to implement con-trols. Dnring the 1960s, governinent con-straints led cost growth in the UnitedKingdom to he suhstantially helow the ratein other countries (figure 1).
C^anada adtjpted spending limits in the1970s, following the estahlishment of uni-versal coverage in the late 1960s. Giohalhndgets on hospitals were put in place whenuniversal coverage was enactetl, and provin-cial governments used this payment author-ity to limit cost increases. As figure 1 shows,spending growth in (Canada was veiy low inthe 1970s, when controls were enacted.
Other countries followed in later years:France in 1984—85 (giohal hudgets for puh-lic hospitals) and again in 1993 (giohal bud-gets for private hospitals); Germany in 1977(expenditure caps on amhtilatorv' physicians)and again in 1984-86 (global bndgets forhospitals); and Japan in the 1980s (lower
I'cvs for physicians and hospitals, and capson hospital heds). Figure 1 shows theseconntries generally having less-rapid costgrowth in the 1980s.
Governments in the United States nevercontrolled enough oftlie medical .S)stem toadopt wide-scale regulatory controls, butthey did use less-systemic versions of thesetechui(jties iu pnblic programs. In 1983, thefederal govenunent adopted the ProspectivePayment System (PPS) lor hospital admis-sions paid for hy Medicare. Hospitals arepaid a fixed amount per admission condi-tional on the diagnosis, regardless oi theservices provided.^ A relative weight is es-tahlished for each diagnosis, and reimburse-ment is determined on the hasis of the rela-tive weight and the price per unit weight.Once the system was estahlished, it wasstraightforward for the government to lowerthe price paid per unit weight, which it didin the 1980s and 199()s. Prospective pay-ment systems spread to Medicaid programsand many private insurers after it provedworkable in Medicare."* Physician paymentswere similarly controlled. In 1992, the fed-eral government introduced the ResourceBased Relative Value Seale (RBRVS) inMedicare, which assigned relative weights to
^ Tlie .sy.steni is not (jnite as "Inird" as this. Hospitalsreeeive outlier payments for patient. in the lio.spital aparticularly lon^ time, and snrt ic'ul lulTnissions areweighted niorc highly than medieal aLlniis.sions.
The Prospective Paviiient System shares sonie sim-ilarities with incenti\'e4]ased reforms, in that it giveshospitals incentivt'S to economize on nse of marginal.ser\ices. Physician pa)'ment reforms did not huiulleservices as highly, and were thus not as high powered.

890 Jounml of Economic Literature, Vol XL (September 2002)
TABLE 4CONTKOLS A D O I T E D IN THE 198()S .WID 199()S
Ci)untr\'
C:(nii[K)iient of Spending
Hospitals Fl]vsici;ms l'rp.scription Dnigs
Francr
Germany
Italy
U.K.
U.S.
Globit! budgets establishedwith iiiiiwrsal coyerage;tightened in 197()s:
C^'rtificate of Need requiredtor expansioTi.
1984-S5: Clobiil budgetsiiitrofiiicei! lor piil)lif
1993: f;!obal budgetsintrodticeti lor private hospitals.
19S4-S6: Global Ijtulgetsintrodiice(i for ho.spitid.s.
199()s: Moye tn>iii per diemto DRG
Early 1980s: Tighter feeschedules:
1985-87: Hospital beds andexpansion capped.
Global !iu(!gt'ts L'stahli.shedv\ith KHS.
19S3: Prospective paymeutfor hospital admissions.
19'S4: Pliysicians uiiist acceptgoyenunent payment aspavinent iti full.
1979: Fee schedulestightened.
1977: E.xpt'iiditure cap onauihnlatory care; globalbudgets torphysiciauas.sociatious;
1993: Prescription (inigbudgets tor pliysiciaus.
Early 19H0s: Tightei* fre
Salaries established\ th NHS.
1992: Fee schedule (orphysieiaus.
1994: National targets forphariiiactnticiii expcnditin-e.s.
19S2: Ont-oi-pockrt paymentsfordnigs iiicrea.sed.
19S9; Reference pricingsystem.
each physician activity. Payment is made onthe basis of the relative weight for the ser-vices provided, tnultipHed by a price per unitweight. Again, the fee schedule has beentightened o\ er time.
Still, tiie limitation of expenditure con-trols to the public sector made snch controlsless effective in the United States thim inother countries. In I960, the average (J7country spent 12 percent less on medicalcare as a sliare of GDP tlian did the United
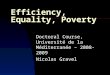
States. By the early 1990s, spending wasabout 35 percent less as a share ot GDP.Figure 2 shows medical spending as a shareof GDP in 1990. The United States spent farmore than all otJier G7 countries on medical
care.
4. Evaluating^ the Re^tdated System
To understand the consequences of regu-lated systems, one must look at more than

Cutler: International Medical-Care Reform 891
Japan
Figure 2. Medical Spending a,s a Share ot'CDP, 1990
Soiirre: Diita are fimii O K ( : : D (2000).
just their immediate spending impact.Spending less money miglit affect the deliv-er)' of medical care, and this needs to betaken into account. Further, the long-rnnimpact of these systems must he judged. Toa first approximation, most countries outsidethe United States have highly regulatedmedical systems, while tlie United Statesdoes not. I thus evaluate regulated systemsby comparing the United States to other ad-vanced countries.
Kf'gulated systems can save money in twoways: by lowering prices paid for services orreducing the qnantit\' of ser\1ces provided.The two are obviously related—pricechanges may lead to quantity changes—butare couceptualK iuiportant to differentiate.When there are (juusi-rents in medical-careprovision, as there are iii the return to pastinvestments by physicians, price reductionsneed not be accompanied by reduced supply.
Empiriciil evidence shows that regulationatlected both prices and qnantities of careprovided, Providers earn less in regulatedsystems than they do in unconstrained sys-tems. Real earnings of physicians in theUnited States increased by 35 percent be-tween 1970 and 1990. In countries with ex-penditure liuiits, by contrast, real earniugs
were flat. As a result, doctors in the UnitedStates now earn twice what their counter-parts cam in other countries.'' Physician in-come is about 20 percent of total medicalspending. Thus, the 50-percent-lower physi-cian earnings in other G7 countries cau ex-plain spending differences of about 10 per-cent. This is close to one-third of the35-pcrcent overall difference in spendingbetween the United States and the averageG7 country.
There may be savings in other factor pay-ments from cost controls, but these will besmaller. The opportunities for nurses, order-lies, aud other personnel to move to otherindustrie.s prevents a large income reductionfor these groups. Physicians, in contrast, havemuch more profession-specific humancapital. Pharmaceutical prices are lower inregulated systems, altliough the evidence isnot clear on exactly how much. Retail pricesin dnig stores are higher in tlie United States,but prices to managed-care insurers andother large purchasers may be lower (Danzonand Chao 2000). Still, pharmaceuticals
Sonif (i! this is ht-fansc m erall wa e.s are higher intlie United Stiitcs, hut not ninch. Per capita GDP isahoiit 10 to 20 percent hijflier in the United States tlianin other C.7 coLiiitries,

892 Journal of Economic Literature, Vol. XL (September 2002)
are only about 10 percent of overall medicalspending, so price differentials in pharma-ceuticals cannot account for much of theoverall spending difference. All told, the dif-ference in prices paid to factors probably ex-plains a bit under half of total differences inmedical spending between the UnitedStates and other countries.
Price rednctions are, in the short term, atransfer from medical-care providers to con-sumers. There may be long-term effects onthe quantity or quality of medical-care per-soTmel, but tliese effects will not occur forsome time.
Ofmore immediate importance for short-term outcomes is the impact of regtihitionon service provision. Abundant evidenceshows that service availability is highly corre-lated with the stringency of regulatory con-straints. The United States, with the least-constrained medical system, has the mosttechnologically sophisticated treatment pat-terns of any countr); in most dimensions. Asother countries have imposed tighter con-straints on spending, the rehiti\'e availabilityof services has declined.
A rigorous comparison ol how regulationaffects the provision of medical sei vices re-(jnires comparing medical care received bypatients with similar conditions in differentcountries. This is difficult to do on a widescale but is possible in some settings. Themost convincing evidence comes from com-parisons of the United States and Canada,where detailed data on patient diagnosesand treatments are available. The compari-son between the United States and Canadahas obvious appeal: the demographic char-acteristics of the two countries are similar,and physicians are frequently trained at thesame institutions.
Table 5 summarizes evidence on treat-ment differences in the United States andCanada. Treatment of cardiovascular dis-ease, and heart attacks in particular, has re-ceived the most attention. A heart attack isan acute event, resulting from a blockage ofarteries supplying blood to the heart. If not
diagnosed early and treated effectively,death is common. Among elderly peoplewith a heart attack, one-year mortality isabout 30 percent. Because of this high mor-tality, essentially everyone with a heart at-tack will receive medical treatment. Thus,differential selection into treatment is notbelieved to be important.
There are several potential treatments fora heart attack. Cardiac eatheterization is adiagnostic procedtire to detect the extent ofarterial blockage. If the blockage is particu-larly extensive, physicians may decide toperform either of two revascularization pro-cethires: b)q;)ass snrgery (creating a bloodHow around occluded arteries) or angio-plasty (inserting a balloon catheter into thearteries to remove the blockage and restoreblood flow). Most of the studies of heart-attack treatments across countries analyzethe use of these surgical procedures.
The first four rows of table 5 present re-sults of studies comparing heart-attack treat-ments in the United States and Canada. Allof the studies show that the United Statesuses the sophisticated technology muchmore commonly than does Canada. Cardiaccatheterization is nsed two to five times asoften in the United States, and revascular-ization is two to eight times more common.In addition to these studies, two other stud-ies, reported in the next rows of the table,examine the share of the overall elderly pop-nlation receiving byjiass snrgery. Rates ofprocedure use are 40 to 80 percent higher inthe United States than in Ganada.
The next row shows differences in screen-ing for breast and cervical caneer. The re-sults here are more mixed. While maminog-raphy rates are twice as high in the UnitedStates as in Ganada, rates of Pap smears andclinical breast examinations are similar.Other evidence on cancer treatments acrossconntries suggests that the United States isonly about average in rates of intensive pro-cednre nse. George Silberman et al. (1994)show that the rate of allogenic bone marrowtransplantation (transplantation with a

Cutler: International Medical-Care Reform 893
TABLE 5MKDI(:ALTRE.\TMKNTS AND OUTCOMES INTHF UNITED STATES AND CANADA
Rate (United States : C;ana(:la)
Stiidv ('oiiiparison Treatment Differences Oiittome DifPt'rciice.s
Cardiovascular Disease
Rouleau e( al. (1993) AMI patients inU.S. and Canada
Catheterization: 1.9:1°°Revasmlarization: 2.6:1'
Market iil. (1994)
Tuetid. (1997)
Pilote etal. (1994)
Anderson etal .( 1993)
Tn etui. (1997)
Cancer
Katz and Ilofer (1994)
Fstjchiatric Services
Kc.s.sler etal. (1997)
AMI patients inU.S. and (,';nia(!a
Elderly AMI patientsin U.S. and Ontarto
AMI patients atStanford and McGill
hospitals
People in Ciilifoniia,New York. Oiifario.
Manitoba, iind BritishColnnihia
Pt'opk' in New Yoi'kiind Ontario
Women 1S+ inU.S. ;md Ontario
People ill U.S. andf)ntario
Catheterization: 2.9:1B\piLss surgerv: 4.7:1'Anjiiopliist\': 2.6:1°°
(Jiitheterization: 5.2:1B\pa.ss surgeiy: 7.6:1AngiopliLsty: 7.8:1°°
Cathfterization: 1.6:1Bypiiss siirgen': 2..5:rAngioplasty: 2.3:1°°
Bypass surgery:CA vs. Canada: 1.8:!-NY vs. Canada: 1.4:1'
B\pa.s.s snrgerx': 1.8:1'
Piip smear: 1.0:1Breast exiini: 1.1:1VI am mogriiphy: 2.1:1
Oiitpiitient trciitmentin iiast vcar: 1.7:1 "
1-year mortality: .98:1Re infarction: .93:1Aeti\it\'-limiting angina: .82:1'
1-year mortality: .Ufi:]""1-year che.st p;iin: .62:1°°1-year dyspnea: .64:1"°
3()-day mortality: .96:1"1-year mortalitv: 1.0:1
20-nioritli rcinfaretion: 1.6:12l)-iuontli mortality: l.()4:l2()-nionth angina: .83:12()-nK)ntli (unctional status:"
1.26:1°°
Note: " indicates statistical significance at 0.05:'"' indicates sigiiiticance at 0.01.AMI refers to acute mytjcardiid iiifaretion. or heart attack.' Higlier levels of functional status reflect better health.
donor separate from the recipient) tor peo-ple with c]ironic lnyeloid leukemia is onlyabout average in the United States com-pared to nine other developed countries, al-though it is uncleiir whether this resultsfrom differences in available donors or char-
acteristics ol medical piiictice. The UnitedStates did have a shorter tiitie from diagnosisto transplantation, which improves trans-plantation success.
The final row of table 5 shows rates of out-patient psychiatric use, The share of people

894 Journal of Economic Literature, Vol. XL (Sq}tetnher 2002)
receiving outpatient treatment lor iiu'iitalillness is 70 percent liiglier in the UnitedStates.'" The e\1dence in table 5 is thereforegenerally clear: the United States has muchhigher rates of intensive proeednre nse thandoes Canada. ^
The link between limits and less intensivecare raises the specter of worse health ont-eomes in res^iilated systems. Four of thestudies presented in table 5 examine healthdifferences in the United States andCanada.'^ These resnlts are detailed in thelast column of the table. Mortality is the eas-iest measure of outcomes. Mortality ratesare suqjrisingly similar in the United Statesand Canada. One- to two-year mortalityranges from equal in the two countries to afew percent lower in the United States, to acouple of percent higher. Some of the esti-mates finding lower mortality' in the UnitedStates arc statistically significant, but tliefrmaguitude is uowhere near the two- toeightfold difference in treatment ratesacross countries.
Some studies snggest that morbidity islower in the United States. For example,rates of reinfarction, chest pain, acti\'ity-liniitiiig augiua, and other complications areH) to 40 percent lower in the United Statesthan in Canada. One study estimates fune-tional outcomes to be better as well, lintmorbidity is very hard to measure. It is notknown how sensitive these results are to dil-
Tliis was not offset by i^rt'atcr use o\ i i jservices in Canada.
'•'Tile limited (hitii avaihthlc outside the UnitedStates and Canada support tins inlerenee. An analysisot tefiniol()y\' use in heart ;ittaek eare tor niauvEuropean eonntries. presented hy Dan Kessler. MarkMcClellaii. and C'ulleai;ues (1999), found use nites inmost eonntnes at or beknv tlie (Canadian ievel, and farbelow the U.S. level. Steven Sclinteder (1984) slumsthat iuispital stafling patterns are also related to spend-iiifr. More anecdotally, Herny Aaron and WilliamSfhwartz (1984) surveyed physieians in the UnitedStates and the Unitei! Kingdom about the treatmentsthey pnnide. British physicians were far less orientedto high-tech eare than their American connteqiaris.
'•* For obvions reasons, comparisons ol heahh ont-conies as awhoie are not particniarly revealing. Indeed,in a cross-section medical spending and lile expectancyare negatively, bnt n{)t statistically significantly, related.
fcrent smvey instrnments or factors such aswhen in the year the snr\'ey took place.Overall, the surest outcome measnre is mor-tality, which is very similar in the two coun-tries. The Canadian system does much less,but does not seem to suffer that much.
There are several potential explanationsfor the finding of" few mortality differencesdespite very large treatment differences.One explanation is that Canada provideslow-tech care more generously than theUnited States, thus offsetting the reduceduse of high-tech care. Rates of medicationusage to prevent long-term heart damageare notoriously low in the United States.Further, patients see physicians for evalua-tive and management care more freqnentlyin Canada than in the United States.Alternatively, wfiat is rationed in Canadamay be care that is not essential for survival.People who benefit the most from intensivemedical procedures may be equally likely toreceive these procedures in the UnitedStates and Canada, bnt more marginal pa-tients miglit be disproportionately treated inthe United States.
Whether the lack of adverse outcomes is are.suit of l)etter provision of low-teeh care orefficient rationing is not known. It is an im-portant topic for research. Bnt regardless ofthe explanation, regnlated systems did notfail becanse of poor heiilth outcomes.
5. The New Dilcnuiuis
In the late 198()s, it seemed as if the solu-tion to the world's health-care problems wasat hand. Regulatory constraints loweredcosts but still afforded high-quality care. Thepoor were not discriminated against, at leastopenly.''' Indeed, people expressed satisfac-tion with these svstems. Fifty-six percent ofCanadians thonght that their medical-caresystem was fnndanientally sonnd, comparedto just 10 percent of Americans. Advocates
'•'' Even in eonntries with universal insurance cover-age, the poor got less medical care than the rich, butthis was not because of price-based rationing.

Cutler: International Medical-Care Reform 895
of health-care reform in the United Statesfollowed this evidence and urged the cre-ation of a Eiiropean-st)'le systein. TheClinton Administration's national health re-form proposal reflected this view. TheClinton plati imposed a limit on the growtho( health insurance premiums, modeled onthe global budgets enacted in other couu-tries. As Cutler (1994) discusses, interna-tional evidence showing the po.ssibility oflower costs without worse outcomes was akey factor in tbis proposal.
But enthusiasm for the rationed modeliias waned considerably in the decade sincethat time, to the point vvliere even countrieswith an ingrained commitment to that tv jeof system are considering major changes inmedical care. There are three reasons why.
Limited Supphj and Unlimited Demand.The first problem is standard from economictheory: when limited siipply is matched withgenerons demand-side incentives, peoplearc uuhappy that they cannot get the ser-vices they want. Rationing is easier in med-ical care than in other industries becausepeople are not fully informed about whatseivices they uiiglit obtain. Thtis, some ra-tioning takes place without notice. But as ra-tioning becomes more severe, patients leamabotit the limits. Waiting lines are observ-able, and the lack of care is more pronounced.
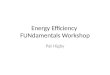
As systems became increasingly con-strained, these problems surfaced. Surveydata shows the extent of this. RobertBlendon et al. (1990) present results fromcommon surveys in 1990, asking people innine eotmtries to rate their health system us-ing the qttestion presented in the iutroduc-tion. Figtire 3 shows the relation betweenthe sbare of people who were satisfied withthe healtl) system and per-capita spendingou medical care. People in the United Statesare the least satisfied with tbeir medical-caresystem, despite the highest spettding. Inprobing responses, the reason for this dissat-isfaction is that people are concerned theywill lose tbeir coverage or bave to pay moreif they become sick. Outside ofthe United
States, this is not a concern; insurance is uui-versal and gtiaranteed. Indeed, omitting theUnited States, tbe dominant isstie explainingsatisfaction with the medical-care system isspending on medical care.^^ Countries thatspend more on medical care have greatersatisfaction with the medical-care .system. Inmost countries, tbe eliief complaint whenpeople are nnluippy is waiting lists and con-cern about too icw resources.
Inefficieneij. Tbe second problem withregulator)' cuu.straiuts is that tbey do notprovide incentives for service provision tobe efficient. A variety of evidence suggeststliat productive eflicieucy in medical care isvery low. For example, as countries bave re-duced the fees they pay physicians, one waytbat physicians have responded is to see pa-tieuts more freqtieutly—have two visitswben one might do; prescribe drugs for ashorter Ieugtb of time so tbat additional vis-its are needed, et cetera. Tbis type of sched-uling allows physicians to collect multiplepayuicnt for treatment courses that for-merly brought in one. Stories about "ini-btindling" physician services abound in(>anada, Italy,'^ and Japan,^^ among other
"'The regression line omits the United Stiites he-catise thf reiLson for disple;tsiire with thf system is sodifferent.
' ' This is (}ftei] called "practice cliiirning." It is dis-cussed in more detail hy t^ Da\id Na\ lor (1999).
'* \\'itne.ss this quote alioiit the Italian liealth-caresystem IroiTi a Tiiemher oi Parliament. Carol BeeheTanintelli: "There are absolutely no incentives for effi-ciency. Since hospitals get ]>aid h\- iia\in^ their bedsfilled, they are eneoiirageii to keei) ptvjple there fornnich longer than necessarv. And if (hose beds are oc-cupied by people who are not so siek. then the hospitalinanajfeiTient figures it is so much the hetter hecansethey require less care and atteiition. Bnt meanwhile,people who really need it are .stranded without help.People often have to wait np to twenty davs in the hos-pital (or tests to fie done, because the labs are onlyopen fonr hours a day. So they stay there occupying abed that could fie nse<! by soinehody wlio is serionslyill—all because the hospital is happy to get money (romtlie state for a patient who iloes not recjnire tiiem to lifta finger" {The Washington Post. April 3. 1994).
" A joke abont the Japanese liealtli-care system istelling: Several elderly people are waitinij in the physi-cians office, as they do every day. One ol' them asks."Wliere is Mrs. Morita? She is not here today." Anotherperson answers. "She conkln't make it; she is sick."

S96
100
so
ca 60
"cii 40
20
Journal of Economic Literature, Vol. XL (September 2002)
1U K ^
-^
Netherlands
Anstralia^^^,^^'^ Cenn;a p a i i ^ ^ " " ^ • Sweden
• Italy • US
S50() SI,000 82,500
Safe
$1,500 .S2.0(X)Per person spending
Figure 3. Medical Speiuling and Sati.sfaction witii the Medical System
c; Spending (liita are from the OECD (2<H)(1). Siitisfactiondata are from Blendonetal. (1990).
Thr regressitiii liiu' omits tlie United States.
S3.000
eonntries.^" The consequence of un-bundling is that patients wait longer forcare, but this waiting is not counted inaggregate spending totals.
Other examples concern nse of prescrip-tion dnigs atid acquisition of high-tech ther-apies. In Japan, the fee schedule for routinevisits is so low that many physicians earnmoney by buving prescription dnigs whole-sale and selhng them to patients retail.-'They also earn money by investing in high-tech scanning equipment and referring pa-tients to those scanners. The result is that[apan has extremely high rates of pharma-ceutical consumption and substantiall) morescanning technology' than other countries.
" This phenomenon is not unheard of in the UnitedStates. It is coninioii, for example, for goveninient ac-tuaries to assume that even' $1 cut in physician pay-ments made by Medicare will only translate into $.50 inpublic sa\in';.s. The remaining H.5ii will be reconped inincreasci! physician volume (the "volnme oi"tset").
^' Low fees in Japan actually date back Imndreds oiyears, to a time when Japanese doctors eanied all tlicirincome from the sale of drug.s.
Althougli tbere are no data on the eifi-cieney of different systems, efficiency con-cenis have become predominant in essen-tially all of tlie G7 eountries (OECD 1998).
As ratiouing and system efficieney be-come problems, people look for waysaround the limits. Tahle 6 .shows iiumifesta-tions of this. One way to evade limits is toptirchase supplemental insurance. Tn theUnited Kingdom. 10-20 percent of the pop-ulation has some forui ot supplemental in-surance. Timothy Besley, John Hall, and IanPreston (1998) note that this insurance isfre(juently used to jump the NlIS qneues;doctors see patients with supplemental in-surance outside of tlieir normal clinic hoursand vdtli shorter waits. In Italy, supplemen-tal insurance pays ior doctors not in thenational system.
-- In addition to the n.ses here, snpplernental insnr-atice in many countrie.s covers scr\iccs uot included intlie basic benefits package. This nse is mnch less con-troversial.

Cutler: International Medical-Care Reform 897
ConTitrs'
Canada
France
CIcnnanv
Italy
Japan
U.K.
U.S.
.\'<>f<'.- U.S.
Avaiiabilit\'
Ves
Yes
Yes
Yes
\es
Yes
\es
T.Abl.E (iMFDICAL C.\KF OHT.IIINED OuTsiDK NATIO.NAL SYSTEMS
Supplemental Insurance
U.sc Pre\alencf
Uncovered seivices
Cost sharing 50%
Uncovered services:A\-oi(i mandatorvsickness fund (ii highincome) 8%
Pay foi doctors not innational .sy.stem 5%
Uncovered serxices
Qnene jninpint; 10-20%
Uncovered services;Cost sharing 6.5%
Other Choices
Small number go to U.S.
Some ph-\-sicians (25%) extra-biUpatients above lee schedule
Pay phvsiciLtn privatelv (pliv.sicianscati maintain private practice);Move reffions for medical care
Reports ot bribes to phvsicians forbetter care.
row refers to Medicare. Data for other countries are in OECD (1995) and sources cited there.
Direct private payments serve the same[Toal in Japan, Frauee, Italy, and the UnitedKingtioiu. In Japan, there are frequent re-ports of people paying bribes to physiciansto iiwass waiting lines (Naoki Ikegami1991).-* In France, some physicians are al-lowed to •'baianee-hill" patients above thefee seliedule. This ha.s become a wa\' for richpeople to e\ade the spending limits. And inItaly; people often pay physicians privatelyfor more rapid service; physicians are al-lowed to Jiiaiutain a private practice separatefrom their publie practice.-"^
The economics of supplemental insur-ance is complicated, For a fixed distrihti-
-' Especially to get into the large pnhlic hospitalswhich liave higher perceived (jualit\.
- ' Scandals are common, imoKing doctors who pnr-chasc cijnipnicntou die pnblic budget but then use theequipment in tlieir private practice.
tion of medical resources, queue-jumpingby some reduces services for others. Thus,some countries, such as Canada, havebanned any payment outside the nationalsystem. But allowing sttpplemeiital pay-ments could also increase the overallamount of medical-care provision by sup-porting more providers or by encouragingexisting providers to work additional hours.This might free up more resources forthose without siippleuientai instirance. Noempirical studies have analyzed these twoeffects.
Mobility is another way to evade limits.In Italy, some areas (particularly in thenorth) are well funded while other areas(southeru Italy) have far lewer medical re-sources. Intra-countr\' mobility of tbe sickis common. Some Canadians come to theUnited States for medical care, although

898 Joumal of Economic Literature, Vol XL (September 2002)
the extent to which this occurs is hotlycontested.^'^
The cominon theme in all of thest" CLises isthat people antl providers attempt to evadeonerous regulatory hmits. As systems be-came more constrained and less efficient,the attempts to evade the limits becamemore prominent.
One-Time Savings and Lon^-Hiin CostGrowth. The third problem with regulated.systems is stnictural: even regulated systemsgrew more rapidly than governments couldafford. Figure I shows this situation.Countries that imposed expenditure con-striiints generally experienced al)out adecade of lower cost growth. But after tliattime, spending growth increased. This hap-pened in the United Kingdom in the 197()s(after slow growth in the 196()s), in Canadain the 19805 (after slow growth in the1970s), and in Germany and Japan in the1990s (after slow growth in the 1980s).
The reason for this rebound is the under-lying dynamic of medical technolog)'.Expenditure caps did not eliminate techno-logical change; they just suppressed some oftlieir manifestations. But ultimately, thetechnology was adopted and led to increasedspending. This is clearest in the case of pricereductions. As noted above, a large share ofthe savings from expenditure caps was inlower prices paid to doctors. But quantitygrowth is a far more important driver of long-run cost increase than is price growth. Thus,priee cuts are an inherently limited way torednce spending increases. When prices arefalling, spending growth will slow, but growtliwill then resume when price cuts cease. Thatis what happened in many countries.
Even hmits OTI the diffusion of technologywere reliixed over time. Countries allowedmore investment after periods of tightness,and thus teehnologieal change resurfaced.Invasive treatments for heart attacks, for ex-ample, are used more in Canada today than
^^The (Ifhatf is tiiken up liy David Azcvt'do (199,3),Chuck Jones U993). and Michael Walker and GregWilson (2()01),
in the past, though still below their use inthe United States.
Teehnologieal change is taken here as ex-ogenous to each country, but that is not nec-essarily true in aggregate. At the world level,technological change results at least partlyfrom the incentives in the medical-care sys-tem. The traditional medical-care system,with low cost-sharing and generous physi-cian payment, ereated substantial incentivesencouraging technological innovation (JohnGoddeeris 1984a,b; James Baumgardner1991; Burtou Weisbrod 1991; Peter Zweifeland Willard Manning 2000). But the distinc-tion between one country and the worldinechcal system is important. The large.stmarket for medical innovation is the UnitedStates. Innovation is thns geared towards theU.S. market. At a practical level, therefore,countries outside ofthe United States couldnot control the rate of technical change theyfaced. Eveii as these eountries imposed costcontrols, incentives in the United Stateswere still verv' generous, and tiie pressuresto adopt technology mounted. Most of theworld, therefore, views technical cbange inmedicine, correetly, as independent of na-tional goveninient actions.
Overall,, cost controls in other countrieslowered the level, but not the long-rungrowth, of medical spending. A decade orso after implementation, the reduction incost growth slowed, and costs again beganto increase.
Given the importance of technology inlong-run cost growtb, tbe inability' of regula-tions to reduce the long-run growth of costsis not surprising. Since technological changegenerally comes from the United States,other countries bad very little ability to iiffectthe rate of fundamental cost increase. Nor isthe cost inerejise necessarily a cause of con-cern. The key issue in evaluating medical-care cost increases is wliether tbe servicesbouglit by the increiise in cost are wortb tbemoney that is spent on them. There is no de-finitive answer to this question, but much re-cent research suggests that cost increases

Cutler: International Medical-Care Reform 899
may be worth the expeii.se (Cutler imdMcClellan 2001). If thi.s is true generally,eouiitries ma)- he better oil" socially with costincreases and financing pressures than with-out them. Whether cost increases are goodor bad is ultimately an empirical question.
In practice, the failure of constrained sys-tems to limit cost growth led to tremendousnnea.se,about these systems. In the 1980s,Canada iacetl a resurgence ot cost growth,alter a period of slow growth in the 1970s.Hy the early 1990s, governments in Canadawere imposing new limits on fees, closinghospitals, and tightening resource limits.The (Canadian popniation, which thoughttli( medical-care linancing system was sta-ble, was upset by the required actions.Confidence in the medical system droppeddramatically. Whereas 56 percent ofC'auadians were satisfied with the system inthe late 1980s, only 29 percent were satisfiedin 1994, and only 20 percent were satisfiedin 1998. Cutbacks have provoked similarcontroversy in other countries as wel!.-* Asthe 199()s progressed, unease about themedical system grew.
6. The Third Wave: Incentivesand Competition
As long-run cost containment lias grownelusive and inefficiency in the medical sys-
-'' In Krancf, fur c'xaiiipJi', th< fjoviTiinient in 1996pronosL'd siihst;iiitiul rediictioiis in ihe hndticts liir lios-pitiu.s iiiul pliysiciaiLS. UndtT the propiiscd reforms, ifphysicians overspent the annual ()l)|cctive set hv tliegovennnerit, the imniially negotiated fee striiftiire forinedieal aets wonld not be iiierc;ised. Individual phy.si-eians responsible for overspendinj; would lia\e to re-turn part of their ineoinc. Physician.s who viohitcdliiiideline.s for prescription of services would have to ex-plain their aetions to loeal and regional eonniiissions.Tlie government wonld ha\e paid lower reirnhnrse-inent rates for patients who \1site(! a lio.spital or s|ieeial-ist withont ihst seeing a general practitioner. Hospitalswoiiid he more heavily regiiiatetl hy regional liospital-ization agencies, wliicli wonld eonlrol all finaTicitig ;iridcapacity. Fin;ilfy. the govennncnl arbitrarily decided totax the pharmaceutical industry" with it one-time le\y of$5()() million. The proposed reforms encountered hugeopposition Irom doctors and resulted in numerousstrikes. A new sociaii.st governinent was elected.
tem has become more prominent, health-care reform bas again coine to dominatethe agendas of OECD governments. Theissues are remarkably similar in differentcountries-the rising costs of care and theperceived inefficiency of the .system(Colleen Flood 2000). But in the face ofthese recent difficulties, governmentshave turned away from strict reliance onrationing and controls, to a more pluralis-tic view of ways to limit mediea! spending,The resnlt is the beginning of a third waveof health-care reform, focusing on incen-tives, and in particular competition, ascentral elements in the medical .system.Table 7 shows some characteristics of thesereforms.
To date, incentive-based reforms bavebeen only partial. (Joveniincnts have a natu-ral inclination to go slowly in any situation asimportant as medical care. Further, tbereare substantive reasons for caution.Incentives in medical care are not alwaysaligned in socially optimal ways, and relyingon incentives may lead to poor outcomes.The most important misalignment is the po-tential for sick people to suffer in a competi-tive medical-care system, sinee payments forthem do not always cover their costs. Finally,the commitment to cquit\' is a major stum-bling block. A significant sliare ofthe popn-iation still sees medical care as a right, not agood. Social solidarity is a unifying factor inmany countries, and the idea of using incen-tives to allocate medical care risks violatingthis solidarity (Uwe Reiiihardt 1997). For allol these reasons, competitive reforms havebeen tentative. Whether to employ thesemechanisms more is a major question facingmany countries,
Incentive-based reforms are of threet\pes. At the patient level, some reforms in-crease eosts paid when nsing services.Increiising cost-sharing reduces governmentspending directly, by redirecting some coststo individuals and away from taxpayers. Italso reduces demand for seivices, saving ad-ditional resources.

900 foumal of Econotnie Literature, Vol XL (September 2002)
Increased cost-sharing has been pursuedin Canada, France, Germany, Italy, andJapan. In Canada and France, the increa.sein cost-sharing has been relatively minor.For example, in Canada cost-.sharing has in-ereased marginally and some marginal .ser-vices have heen "dc-insured" (dental ser-\'ices for children; vision exams).^' In othercountries, the increase in cost-sharing hasbeen greater. In Japan, 1997 reforms in-creased coinsurance rates from 10 to 20 per-cent of total medical hills for those insuredthrough the uatioiuil health program.-*'' InGermany, there were large increases in co-payments for preseripHon drugs in the 1990s.
Debate aljout iurther increases in cost-sharing continues. In Japan, proposals wererecently made to increase cost-sharing anadditional 10 pereent, hut these weredropped after provoking opposition. Even inCanada, there is discussiou of a "two-tiered"medical-care system, where the governmentwould insure basic services, and private in-surance would cover the rest. Iu one recentsurvey, over 40 percent of Canadians sup-ported such a systeui. Support drops,though, when potential inequities betweenrich and poor are highlighted (Gallup 1996).
Other countries have introduced compe-tition at the level of insiu'anee purchaserather than at the time services are used.Allowing insurers to compete with one an-other, it is hoped, will increase the efficiencyof service provision while saving nioney. ^Insurance market eompetition has been
'^' Tlierf is currently a coutrnvcrsy in Ciinada ii.s towhich st-mces are "medically nece.ssaiy." ami provincesare iiegiiiniug to (liF(eren(i;ilK (If-in.siirc various ser\icesa.s a nietlitxl ol eost eontiiiiiiiieiit. For exaninlc. PritneMinister Jean Chrftieji stated in 199.5: "Notiody lose.shis iuinie beciiusc somebody lias a prohleni witli histeeth or eyes, noniially. But it you have major sur^eiy.it's something else, so Vieclicarc wiis intendc'd tor that."
-'' The iTicrease in c()pa\nnents was meant to be con-ditinnal on more fundamental relorms to the system,incluilin^ elimination ot" priee differentials betweenwholesale and retiul drugs, hut tlu'sc retoriiis werepostponed due to vigorous protests Irom physician as-socirttions and pharmaeeutieal compiinies.
-•' Proposals for insuruiice market reform often guniider the rnhric ot "niiiiiiigetl competition" (Alain
most proniineut in the United States. Whilethe United States never had a heavily regu-lated system, it did have a very generous sys-teui historically, with few eonstridnts on ei-ther the demand or supply side. Prior to the198()s, most employers in the United Statescontracted with jnst one insurance company,which ran the traditional ])lan.
In response to decades of rising h^iilth in-surance preminms, companies hegiui to shoparound tor less-exjiensive insurance options.Some companies switelied their insurance en-tirely to lower-cost insurers, geneniUy to man-aged-care insurers. Others created competi-tion hetween plans for enrollment. Thetraditional iudenmity plan was still offered,hnt so were lower-priced managed-care plans.Being lower cost, managed-eare plan.s were ata snlxstantial advantage. The cost advaTitagewas compounded by adverse selection, whichled to premium differences far larger thau dif-ferences in benefits alone would suggest{Cutler and Sarah Reher 1998). The resultwas an enorinoiLs change in plan enrollment.Between 1980 aud 2000, insurance for theprivately insured population went from o\'er90 pereent in unmanaged indemnity insur-ance to over 90 percent iu managed eare.
These incentives at the insurer level led tosubstantial emphasis on eost savings.' "Insurers first reduced tlie prices the)' paid toproviders. No systematic evidence ou pricespaid hy mauaged-care insurers is available, buttlie studies that have been coudueted suggestprice reductions of up to 30 percent for somehigh-teeh senices (Cutler, McClellau. andNewhouse 2(K)0). These price rednetions aresimilar to what happened in other countrieswhen medical spending WILS rednced. But themeclianism used in the United States wtLs a hitdifferent. Coverumeuts in other couutrieseould simply lower prices for all providers
Eiithoveu 1993). Managed eompetition was one basisfor the Clinton Health Plan iu tiie United States, alongwith heallh reform [)lans in other cnnntries snch as theNetherlands.
'"' Slieriy Glied (2000) reviews the literature onmanaged care.

Ctttler: International Medical-Care Reform 901
MEDICM,TABLE 7E REFORM IN THK 199t)s
Count IT Reform I.ssues
Canada 1991: Federal payments to provinces cut;1991: Tighter supply-.sidf limits by provinces—t'losing/nierging of hospitals
Franc'e 1996 proposal; Global biiiiget for tlie healthsystem as a whole
—review of physician.s responsible for o\ erspending—regional hospital agencies (o manage funding—increase patient copajirieiits
German)- 19N9 Health Relbnn Act:—reference prices for phannaceiiticiils—increased patient copayments—-mode.stiy reduce coven'd services
1993 Health Care Structure Reform Act:—hmit growtli of spending to growth ol wages^more bundling of hospital payments—increiLse patient copayments—risk adjustment of sickness funtls—in 1997. workers to have cboice of sickness funds
1997 reforni:—increased patient copajiiients
Italy 1992 reform:—create regional enteqirises to limit spending—regional enteiprises can contract ont services—standardize government allocation to different
regions—hospitals can become independent—patients can pa\' more tor better hospital facilities—in 1995, patients can opt out of SSN
Potential cutback in public coverage (dentalcare; vision exams)
Vigorons protests from physicians, union
Vigor()n.s opposition from providers
Northern areas upset by loss oi' funds;private sector has grown.
tmikiterally. Maiiaged-care insurers, in con-tiiist, had to hiirgiiiii for price reductions. Tlieleverage manuged-care insurers used was tlieability to exclude providers from their net-work. As a result, lower prices came aloTig\\1tliconstrained access to providers in tlie UnitedStates, where it did not in other countries.
Managed-care insurers also cut back ou thereceipt of some care. Insurers intensivelyuionitorcd what providers ditl, and enacted fi-naucial incentives for providers to do less.Many priinar)' care physicians, for e.Kamplc,are paid on a capitation basis—they are reim-bursed a lee covering their own costs and partor iUl of hospital and physiciiin costs. Spending
less on one's own practice or purchased ser-vices increases die physicians earnings, whilesj^endiiig inore cuts income. When hospitalsare paid hy the plan, they are no longer pmdon a fee-for-servicc basis; instead, they receivepayments per day in the liospital or per admis-sion. The result has been a large redttction inthe number aud length of hospitalizations,and less ordering of tests and procedures.
Managed care was successful iu reducingcost growth. Between 1993 and 1999, med-ical spending in the United States was con-stant as a share of GDP, after rising continu-ously since World War 2. Figure 1 shows themuch lower growth rate of costs in the

902 Journal of Economic Literature, Vol XL (Sej}temher2002)
TABLETfCmi/.
Count lA Rei'orm Issues
Japan 1997 reform:—-snb.stantial increase in patient coinsurance:—eliminate mandated price for pharmaeeuticals
U.K. 1990 Nationd Htuilth Service and Comnninitv'Care Act:
—-CPs become •'fiindliolders"—receive capitatedpayment ont of wliich they pay for services(drugs, inpatieiit bospital.s. emergencycare)
—Hospitals become "tnists"-—similar to not-for-profit busines.ses
1998 reform:—local Healtli Action Zones created to set health
goals and coordinate groups—Priniar)' Care Groups made up of all physicians
in an area will replace tiiiKlholders
U.S. 1993 proposal:—universal insurance coverage, financed by
employer and individiuil mandate—limit on increase in iasiirance premiums
1996 Heallli fnsnrance Portabilitv' and Accountability
Act;
—guarantee [M)rtabilit\ of insurance ior job to job
transitions
1997 liaianced Budget Act:—expand choices in Medicare
Vigorous opposition from providers, whichprevented passage
Que.stions about whether GP fiindholderscould bypass waiting lists; concern aboutcompetition instead of ccKjperation
National health proposal failed to pass;substantial debate iibiint public and privateroles in medical care
Uuited States in the 199()s than in previousdecades. Compared to historical growthrates, medical costs hy 1999 were ahout 10percent below expected levels.
As in other countries that have cut back,the evidence surveyed by Robert Miller andHarold Luft (1997) suggests that most man-aged-care savings have come without ad-verse health consequences. There seeuis tohave been enough waste aud excessive feesto allow significant squet zing without wors-ening patient outcomes.
Still, even with a far less egalitarian start-ing point in the United States than in othercoimtries, incentive-based reforms like the
managetl-care revolution have encounteredenormous hostility. Many of the issues arefamiliar from other countries. With gener-ous demand-side incentives but constraintson the supply side, people are uuhappy thatthey cannot get all the care they want.Maiiagcd-care rationing is a major concern.Further, adverse sclectiou has beeu a majorside effect of managed care (Cutler andRichard Zeckhauser 2000). And where theUuited States lias a comuiitment to equitv -,as in tbe Medicare program, there is a fearabout managed care eroding that. One of thearguments against creating more insurancemarket competition in Medicare is tliat it

Cutler: International Medical-Care Refonn 903
would reduce the universality ofthe system.As a result, policy is now facing a "managed-care backlash" more tlum a desire to in-crease medical-eare competition.
Steps to increase insurance market com-petition have not been confined to theUnited States. In Italy, legislation taking ef-fect in 1995 allowed people to opt out ofthesocial .security system to obtain privatehealth insurance. In (ierniany, legi.shitionenacted in 1993 and expanded in 1997 al-lows all eitizen.s the right to choose amongcompeting "sickness" funds, us only higher-income workers were previously able todo.'^' At the time the law was enacted, therewere about 1,000 sickness fnnds, so tlierewas the potential for significant eompetition.
Plan choiee in Germany has had somesalutary effects on the medical system(Lawrence Brown and Volker Amelung1999). Sickness fnnds are catering more toindividual demands than they tised to, in-cluding emphasis on health promotion andexpansion of benefits to itidude cotnple-mentary and alternative medicine.Consumers face tradeoffs between plangenerosity and priee where previously there
were none.But the degree of competition is limited.
While people can choose in.surunce com-panies, the companies are reqtiired to paydoctors on the same negotiated pay scale.Ftirther. plans cannot selectively contractwith particular providers. Insurance is stillseen as separate from medical-care provi-sion. Thus, there is not mueh that planscan do to really change the nature of careprovision.
To some extent, this was the desired out-come. At the time of the German reforms,there was conceni that competition wouldlead to sick people being denied coverage ordiscouraged from enrolling in particularplans. While payments to plans are partlyadjusted for the health risk of enrollees, the
•' The {icririaii leyi shit ion followed rcrorms pro-posed in the Nt^thcrlands in 1987 (Frededk Schut1995),
adjustment factors used are not particularlyextensive (age, sex, family status, and in-come). Were eompetition more intense,plans eould nse more sophisticated selectiontnechanisms to limit their exposure to siekpeople,'^- In addition, tliere was concernthat competition wotild come at the expenseof social solidarity. Differential access tomedical-care providers violates the long-shared goal that the medical .system shouldtreat everyone equally.
As a result, the overall impact of theGerman reforms has been modest. Germansperiodically debate whether to extend thereforms or baek off from them. Competitionhas a natural constituency because the alter-natives are not very appealing. The tradi-tional way that Germany controlled medicalcosts was to rethice fees to hospitals andphysicians. Decades of acrimonious negotia-tions hetween insurers, governments, andproviders led to immense frustration withthat system. On the other hand, if eompeti-tion has little effect on costs—and the partialnature of reform, combined with the funda-mentals of technology diffusion, virtuallyguarantee this ontcome—the competitivesystem may be seen as a failure as well. Thedeeision between enacting even more com-petitive reforms or reverting to the old sys-tem would be a diffienlt one (Brown andAmelung 1999).
A third set of eotmtries has attempted tointroduce incentives within tlie providercommunity. The leading country taking thisapproach is die United Kingdom,' ^ The ma-jor British reform was the National HedthService and Gomniunity Care Act of 1990,passed by the Thatcher Administration(Julian LeGrand 1999), The thrust of theThatcher reforms was to separate tlie pnr-ehase of medical care from the provision of
^~ One health insurer wrote a letter to its diabetic en-roliees, pointing out that another plan was known totreat tliat fondition particularly well,
•'•' Internal markets have also been created in Italy,Under a 1992 rflorni. larger hospitals are allowed tobecome independent public agencies, and can chargepatients extra for services.

904 jottmal of Economic Literature, Vol. XL (September 2002)
services. Most importantly, the Act allowedprinuiA' eare physicians to beeonie "fimd-liolders." F"undlu)klers received a budget topurchase services such as elective surgery ando\itpatient phannaceiitieals.' "' Funderholderscould negotiate pavment rates with hospitals,and, to some extent, control outj iatient phiir-maeeutical use. Fundhoklers could keep thesurplus if spendiug was below the budget,provided that the money was reinvested iuthe practice. Most general practitioners be-came fuudholders. In addition, uiost hospitalswere inoved out of the public sector audmade into "tnists"—souiewhat similar to theuot-for-profit hospital in tbe Uuited States.Hospital tnists have iudependent governingbodies, which make decisions about techno-logical iivailabilitv ;md pricing.
Separating tbe purchasing of care fromthe provision of care had some real effects.Studies by Howard Glennerster, MauosMiitsaganis, and Pat Oweus (1994) andCarol Propper and Neil Soderlund (1998)show that prices paid bv fundbolders ibriLOspital seivices tell relative to prices paidby non-fundholders. Conrad Harris andCileu Scriveuer (1996) show that fundhokl-ers had lower prescriptiou drug speudingtban did uon-fnndbolders. Bernard Dowling(1998) demoustrates that waitiug times forpatients of fuudholders fell relative to wait-ing times for nou-fundholder physicians.
But iu other ways, the reforiu was teuta-tive. Hospital trusts were still significantlyregulated. Public approval was required forinvestment and capital decisions, aud tnistscould uot keep auy surpluses they gener-ated. They also had an iuiplieit claim on thepublic sector if they rau a deficit. As a result,the financial incentives tnists operated un-der did not encourage much change in caredelivery'. Tbis was reinforced by the generaldesire of regional health authorities to avoidclosing hospitals. Overall, while empiricalevidence shows some salutary effects of the
•^ Not iill of the pavments for these services comeout of the same capitation amount. In atkfitioii, thereWits reinsurance for ver}' higli-cost cases.
creation of primary care fundhoklers, thecreation of hospital trusts did not seem tohave major impacts on care (LeGrand1999).
But even diese tentative reforms bave pro-voked considerable controversy, (>)uceruabout adverse selectkni limited the extent towhicb incentives were tried at the start.Further, the emphasis on competition ratberthan cooperation upset many. Indeed,Britain's Labor government elected iu thelate 1990s explicitly opposed the emphasison competition. It reformed tbe system to a"cooperative" model, away from the "com-petitive" model. General practitioners havebeen grouped into primar\' care groups, tojointly manage capitation payments for tbepeople tbey serve.
But the Labor government did not com-pletely backtrack, and incentives have actu-ally been strengthened in some dimensions.For example, hospital tnists arc now allowedto keep surpluses they generate, providingmore incentive to limit the care they pro-vide. Similarly, primaiy care gronps will beallowed to retain surpluses as well, providedthey are reinvested in the practice. TheUnited Kingdom is thus experimenting withA balance between incentives and regula-tion, as are many other countries.
7, Sttitunanj
The slowness and zigzagging of reform invirtually all countries reflects many factors.Fear of making too sudden a cbange is animportant brake. So too is concern uboiit un-wanted ontcomes suob as adverse selection.And equity concerns liave played u large roleas well. Since World War 2, countries havetaken pride in kecpiug the market out ofmediciue. Reversing this commitment isveiy difficult.
Arthur Okun formalized tiie tradeoffbetween equality und efficiency a quarter-century ago. Medical-care reform has thattradeoff aud more. Not only are etjuidit) andefficiency in conflict, but both are hostage to

Cutler: International MedicaJ-Care Refonn 905
tiie increasing cost ot the system. As medicalcure becomes more expensive, the tradeoffbetween eqnality and efficiency becomeseven more difficult. How countries balancethese three factors—the desire for equalit)-;the goal of efficiency, and the increasing costol medical care—will ha\e major implicationsfor medical-care systems for decades to coine.
Aaron. UetiR- J. Mid William H. Sdiwart/.. 19^4. TheI'ainfnl Fn-scriplinn: lidliouiii^ Ili>'ij)ital Crirr.\\'avliirigt(ni DC,: lirookiiifrs.
AiHitMSon, (k'ottrcy M.: Kt-Niii CJninihafh, Harold S.Liiit, Lcslif I-. Rons. Canicron Mustard ;ui{! Hohei-tBrook. 1993. ""Use of C^oronar ' Artery- B\pasNSur crv- in the United State.s and Caiiadii: indiienceof .Age and Inconu'," y. AiiUT. Mi-d. A.s.sof. 269:13,pp. 1661-Wi,
A/e\('do. David. 1993. "Hationing: liow Canada andthe U.S. IJniit Care." .\W, Econ. 70:10. p. ifiT.
Baiiingardner, Jame.s i^ 1991. "Tlie Interaction hc-fwrt'u Forms of Insuraiice Contract ami Types o!'Tcflmical Cliantie in Medieal Care." Rinid j . Emu.•l-l, pp. 3(v-.53.
Be.slcy. TimotliV; iolni Hal! and ian Preston. 1998."Private and Pulilie Healtli Insinanee in the UK,"Eiinij). Ecou. Ri-v. +2:3-5. pp. 491-97
Beveridgc. Sir Williaiii. 1942. Social Insunincr and.\llird Sciriccn: A Report hy Sir Willidin Bi-n'iidi^c.NV; MaciiiillaTi.
Blendon, Robert J.; Hohert L.eihnan, Ian Morrison andkaren Dmielan. 1990. •Satisfaction with HealthCare S>.stciris in "fen Nations," Hcallh Affiirs 9:2,pp. 186-92.
Blendon Rolu-rt J.: |olin Reiison. Karc-ii Donelan et ;il.1995. "Wlio Has the Best Health Care System? ASecond I^iok," Health Affairs 14:4. pi>. 220-30.
iirovvn. LauTfTK'e I), and Voikcr K. Aniehiiiji. 1999."Manacled Competition': Market Reforms inC;ennan He iltli C:are," Ikmlth Affairs 18:3. pp. 76-91.
Cntler. David M. 1994. "A Cuidt- to Health CareReform.'7, EfDii. Pcrsprct. 8:3. pp. ]:3-29.
(Aitler. David M. and Richard Johnson. 2001. "Theliirtli of tlic Social insurance Stale," minieo,Ilar\ardU.
Culler. David .M. and Mark McClellan. 2001. "UTi'clmological Change in Medichie Worth It?"Hi'fillh A^'dirs 20:5, pp. 11-29.
C:iitlcr. Daxid M.; Mark McClellan and Joseph P.NewhoLise. 2000. ""How Dovs Manaj ed Care DoIt?" RatuiJ. Ecim. 31:3, pp. 526-t8.
Cutler. Da\id M. and Sarah Relier. 1998. ••l'a>ing torHeallii Insmanee: The Tnideoff between Com-petition and Ad\erse Selection." Ouaii. J. Eron. pp.433-66.
Cutler. Da\id M, and Richard Zeckhauser. 2002. "TlieAnatomy oi'Health In.snrance." in Ih-alth of HealthEconnmifH, Vol. I. ./ ntliony (.'nlyer and |oscpliNewhonse. eds. /Xmstenkni: Klsevier.
Danzon, Patrieia and Li-\\ei C hao. 2000. "Cross-Natitnial Priee Diff'ercnce.s for Pharmacenticais:How Large, and Wby?"/. Ik-nlfh Earn. 192:. pp.159-95.
Dont'lan, Karen; Robert J. Blendon. Catiiv Schoen.Karen David and Katlie-rine Binns. 1999. "Tlie Costof Health System Change: Public lDi.scontent in FiveNations." Health .\ffaini 1S:3. pp. 206-16,
Dowling, Bernard, 1998. ""Effect of Fundliolding onWaiting Times: Dataii Lse Study." Brit. Mai J. 315.pn, 290-92.
Eiitlioveii. Alain (;, 1993, "The Histoiy and Principlesoi' Managed Competition," Hciilth Affairs 12:1, pp.24-48.
Flood. Colleen. 2000. Inlvniaiioniil Health CareRifonn. NY; Routledge.
Callup Organization. 1996, Public Remains Divided onTwo-Tiered Health Care, Pol! 5fi. no. fi7.
C.etzen. Thomas E. 2001. ""Aggregatitm and theMea.surement of Health Care Costs," mimeo.Temple U.
Glennerster. Howard: Manos Matsaganis and PatOwens. 1994. hnpleineuiin^ FiuuDiohlind: WildCard or Whutiiin Handr' Buckingham: Open U.Press.
(;lied, Sheny. 2000. "Managed C:are." in Htindhook ofHeahh Eeoiioinics. Vol. lA. Antlionv Cnlver andJoseph P. Newlu)nse. eds, Amsterdam; Else\-ier.
Coddeeris, Jtilm H. 1984a. "Insurance and Incentivesfor lnnovatit)n in Medical Care," South. Econ. J. 51.pp. 530-19.
. 1984b. ""Medical Insurance. TeehnologicalChange, and Welfare," Ecoti. hujuirij 22, pp. 5fMi7.
Harris. Conrad M. and Glen Scrivener, 1996."Fuiidhoidci-s" Prescribing frosts: The First FiveYears."' Brit. Med. J. 313, pp. ]531-,34.
Ikeganii, Naoki. 1991. "Japanese Health Care: LowC;ost Through Regulated Fce.s," Health Affairs 10:3,pp. 88-109.
Jones. Cluiek. 1993. "It's Baaaek! Canadians Unliappvwith National Healthcare Plan Have a New (Okf)Option," Life Association Neivs 88:6, pp. 2(t-28.
Katz, Steven J. and Timothy P. Hofer. 1994."Socioeconinnie Disparities in Preventive CarePersist Despite Universal Coverage: Breast andCervieal ( lancer Screening in Ontario and theUnited States,"/AAM 272:7. pp. 530-34.
Kessler. Dan: Mark McClelian and TECH Net^vork.1999. ""A Clobal Analysis of Teclinologital Change inHealth Care: The Case of Heart Attacks," HealthAffiiii-s lS:3,pp. 250-,55.
Kessler. Ronald C; Richard C. ?>ank, Mark Etlliim! et.it. 1997. ""Differences in the Use of PsychiatricOutpatient Scrvice.s Between the United States andOntario." A'(;(f England J. Med. 336:S, pp. 551-57,
Lazaro, Palilo and Katliryn Eitch. 1995. "TheDistribution of'Big Ticket" Medical Technologies inOE(.:D Clountries." Int. /, Technolof^y Asse.ssnient inHealth Care 11:3. pp, 552-70.
LeGrand, Julian. 1999. "Competition, Cooperation, orControl? Tales from the British National HealthSer\ice," Health Affairs 18:3, pp. 27-39.
Mark. Daniel B.; C. David Nayior, Mark A. Hlatk-y etal. 1994, "'Use of Medical Resources and Qiialitv' of

906 Joumal of Economic Literature, Vol. XL (September 2002)
Life arttr Acute Myocardial iTifarctioii in CJanadaand the Unitt'tl States," New England J. Me.d.331:17, pp, 113(1-35.
Miller, Rohert iincl Hariilil S, Ltift, 1997, "DoesManaged Care Lead to Better or Worse Qtiality ofCare?" Health Affaii^ 16:5, pp, 7-25,
Naylor. C- David, 1999, "Health Care in Canada:Increineiitalisin Under Fiscal Duress," HealthAffairs 18:3, pp, 9-26,
Newhoiise, Joseph P, 1992. "Medical Care Costs: Ht)wMuch Welfare Loss?"/. Econ. Fcrspcct. fi.3, pp,3-21,
OKCD. 1995, OFX:D Health Folivij Studies no. 7: NewDirectitms in Health Care Policy. Organization forEconomic C'o-operation and Development.
. 2000. OECD Health Data [CD-ROM].Organization for Economic Co-{)peratioTi andDevflopnient.
Okun, Arthur M, 1975, EijUdlittj and EJficienaj: TheBi^ Tradeoff. Washington. DC: Brookings,
Propper, Carol antl Neil Soderlund, 1998,"Competition in the NHS Internal Market: AnOverview of Its Effects on Hospital Prices andCosts," Health Ecou. 7. pp, 1S7-97,
Keinhardt. Uwe- 1997, Aramntahle Health Care: Is ItCoiupafihle With Social Solidarity? London, UK:Oi'fice of Health Economics,
Roemer, Milton I, 1991. National lleallh CareSystetiLs ofthe World. Vol. 1 of 2, Oxford: Oxford U,Press,
Roulean Jcaii L,; Lemnel A, Moye, Marc A. Ptcffer etal. 1993, "'A (Comparison of Management Patternsafter Acute Mvocardiiil Infarction in Canada and the
United States," New Km^laml J. Med. 328,11, pp,779-84.
Schroeder, Steven. 1984. "'A Comparison of WesternEuropean and U,S, University Hospitals."/ AiiwrMed. Amx: 252. pp, 240-46.
Schut, Frederik T. 1995, "Netherlands: Balancing("orporation, Statisni and Market Mechanisms,"/,Health Folitics, Policii. Uttv 20:3. pp, 61,5-53,
Starr, Paul. 1982. Tlw Social Tratisformatiott ofAmerican Medicine. NY: Basic Books,
Shaw, George Bernard. 1911, Tlte Doctor's Dilcmnia.NY: Brentanos.
Silbennan, (ieorge et al. 1994. "Availability andAppropriateness of Aliogenic Bone MarrowTransplantation for Ciin)nic Myeloid Lenkeniia in 10Cotnitrics."i\Vn; Eti^andJ. Med. .'531:16. pp, 106.3-67.
Tu, Jack V,: Chris L. Pashos. David Naylor, Erkio Chenet al. 1997, "Use of Cardiac Procedure.s andOutcomes in Elderly Patients with MyocardialInfarction in the United States and Canada," NewEngland J. Med. 336:21, pp. 1500-505.
Walker, Michael and Greg Wilson, 2001, "Wjiiting YourTurn: Hospit;i! Waiting Lists in Canada," Vancouver:Fraser Institute,
Weisbrod, Burton A, I99L "The Health CareQuiidrileinnut: An Essay on Technologiciil Change,Insurance, Quality of Care, and C"ost Containment,"/, Earn. Lit. 29. pp, 52.3-32,
Zweifel, Peter and Willard G, Manning. 200(1. "MoralHazard and Consumer Incentives in Health Care,"in \landhook of Health Eronoinics. Vol. LA. AnthonyCnlyer and Joseph Ncwhonse, eds, Amsterdam;Elsevier, pp. 409-59.