Embed Size (px)
Citation preview

How do service users’ interpersonal sensitivity to dominance and perceptions of staff coercion impact upon self -reported anger and rates of aggression in secure-care
settings?
Jessica Holley
Submitted for the Degree of
Doctor of Psychology
(Clinical Psychology)
School of PsychologyFaculty of Health and Medical Sciences
University of SurreyGuildford, SurreyUnited KingdomSeptember 2019
1

Abstract of empirical paper
Background: Coercive practices – which are used as means to manage violent/aggressive
behaviour in secure forensic settings – have come under scrutiny in recent years due to their
paradoxical effects on provoking further service user aggression and violence. Previous
research has found relationships between increased service user aggression with both service
users’ interpersonal styles and perceptions of staff coercion (i.e. staff limit setting). There is,
however, a gap in the literature which looks at the way in which forensic service users
perceive such coercive practices in relation to interpersonal sensitivities and whether this too
has an impact upon service user aggression.
Aims: To investigate whether forensic service users’ levels of interpersonal sensitivity to
dominance increases levels of self-reported anger and rates of aggression towards staff
through perceptions of staff coercion.
Methods: In a cross-sectional quantitative study design, 70 service users were recruited from
one high and two medium secure forensic hospitals. Standardised measures were completed
by service users and recorded incident data was collected within the past year. Correlation
and mediation analyses were run to investigate the relationship between study variables.
Results: A significant relationship was found between service users’ interpersonal sensitivity
to dominance and self-reported rates of anger, where forensic service users’ who had higher
levels of interpersonal sensitivity to others’ dominance were likely to report higher rates of
anger. No significant relationships were found between all other study variables.
Conclusion: The findings from this study contradict previous research where coercive
practices may not necessarily increase rates of aggression towards staff but, in the context of
service users’ interpersonal sensitivities to dominance, it may be more useful to consider the
way in which coercive practices are implemented. The findings have, however, been
2

interpreted tentatively due to various study limitations. Recommendations have been made
for clinical practice and future research.
3

Acknowledgements
I wish to express my gratitude to the course team for their support during the three years of
training. A special thank you to my clinical tutor, Dr Catherine Huckle, and my associate
clinical tutor, Dr Heinz Kobler, for their invaluable advice and guidance. I would also like to
thank each of my placement supervisors who have provided me with a wealth of clinical
experience – their time and patience both in and outside of supervision was greatly
appreciated and valued.
Thank you to my supportive family, friends, and fellow trainees who, over the past few years,
have provided me with an endless stream of moral support and encouragement. A special
thank you to Matúš who listened patiently and gave me hope during times when I felt just
ever-so-slightly depleted.
Finally, I would like to thank the many service users that I have had the pleasure of working
alongside during these past three years. I have felt humbled by your willingness to share
some of your most difficult of experiences with me whilst also inspired by your resilience
and stories of hope. You are and will continue to drive me to be the best Clinical Psychologist
that I can be.
4

Contents
Part 1: Research – MRP Empirical Paper................................................................................................6Abstract.......................................................................................................................61.0 Introduction...........................................................................................................72.0 Main hypotheses and research questions.........................................................133.0 Method.................................................................................................................154.0 Results..................................................................................................................285.0 Discussion............................................................................................................386.0 Conclusion...........................................................................................................49References..................................................................................................................50MRP Empirical Paper Appendices.........................................................................58Part 2: Research - MRP Literature Review...........................................................95Abstract.....................................................................................................................951.0 Introduction.........................................................................................................962.0 Methods.............................................................................................................1043.0 Results................................................................................................................1094.0 Discussion..........................................................................................................135References................................................................................................................143Part 3: Clinical Experience....................................................................................152Part 4: Assessments..................................................................................................155
5

Part 1: Research – MRP Empirical Paper
How do service users’ interpersonal sensitivity to dominance and perceptions of staff coercion impact upon self -reported anger and rates of aggression and in
secure-care settings?
Abstract
Background: Coercive practices – which are used as means to manage
violent/aggressive behaviour in secure forensic settings – have come under scrutiny
in recent years due to their paradoxical effects on provoking further service user
aggression and violence. Previous research has found relationships between
increased service user aggression with both service users’ interpersonal styles and
perceptions of staff coercion (i.e. staff limit setting). There is, however, a gap in the
literature which looks at the way in which forensic service users perceive such
coercive practices in relation to interpersonal sensitivities and whether this too has an
impact upon service user aggression.
Aims: To investigate whether forensic service users’ levels of interpersonal
sensitivity to dominance increases levels of self-reported anger and rates of
aggression towards staff through perceptions of staff coercion.
Methods: In a cross-sectional quantitative study design, 70 service users were
recruited from one high and two medium secure forensic hospitals. Standardised
measures were completed by service users and recorded incident data was collected
within the past year. Correlation and mediation analyses were run to investigate the
relationship between study variables.
Results: A significant relationship was found between service users’ interpersonal
sensitivity to dominance and self-reported rates of anger, where forensic service
users’ who had higher levels of interpersonal sensitivity to others’ dominance were
6

likely to report higher rates of anger. No significant relationships were found
between all other study variables.
Conclusion: The findings from this study contradict previous research where
coercive practices may not necessarily increase rates of aggression towards staff but,
in the context of service users’ interpersonal sensitivities to dominance, it may be
more useful to consider the way in which coercive practices are implemented. The
findings have, however, been interpreted tentatively due to various study limitations.
Recommendations have been made for clinical practice and future research.
Word Count (excluding Tables, Figures, References and Appendices): 10000
1.0 Introduction
Forensic psychiatric inpatients are often deemed as “dangerous, violent or having
criminal propensities” (Mason, 1993, p. 413) and who have usually “interfaced with
the law at one level or another” (Mason, 2006, p. 3). In Bowers and colleague’s
review (2011) of 424 international studies, the frequency of violent incidents in
secure-care settings were significantly higher compared to general mental health
hospitals (Bowers et al., 2011). For example, in a survey of an independent secure
care facility, 2,137 violent incidents involving 56.4% of service users were recorded
(Dickens et al., 2013). The consequences of workplace violence have been known to
lead to staff absenteeism due to illness, injury and disability (Holmes, 2012). In
addition, these workplace violent incidents can also lead to high staff turnover,
decreased productivity, decreased work satisfaction, and a lack of staff commitment
to work (Holmes, 2012). Not only do these violent incidents have a negative impact
upon staff well-being, but also puts other service users at risk of physical and
7

psychological harm (The National Institute for Health and Care Excellence (NICE),
2015). For those service users committing violence whilst in residing in secure
settings, their stay in secure care can often be extended (e.g. Castro et al., 2002).
Longer lengths of stay in secure care does not only result in high economic burden
on these services (e.g. Vӧllm et al., 2017), but may also impact negatively upon
forensic service users’ quality of life (e.g. Shaw et al., 2001).
Aggressive behaviour in secure care has centrally been managed by the
implementation of coercive measures (NICE, 2015). Although coercive measures are
most commonly associated with short-term management methods of aggression and
violence (through seclusion and restraint), more long-term coercive measures are
also used. Szmukler and Appelbaum (2008) outlined in their ‘sliding scale’, how
coercive measures can take on various forms in forensic secure settings including:
persuasion (e.g. efforts to influence service users’ behaviour by emotional
reasoning); interpersonal leverage (e.g. where service users’ relationship with staff is
used to put pressure on them, such as pointing out dissatisfaction in service user’s
behaviour); inducement (e.g. conditioning ‘good’ behaviour through the use of
positive rewards); threats (e.g. to lose particular benefits); compulsory treatment (e.g.
service users having choice taken away and treatment carried out against their will);
and physical security features (i.e. locked doors and barred windows).
More recently, the use of coercive practice has been scrutinised, particularly with re-
gards to the impact it has upon service users’ personal autonomy and human rights
(Hui et al., 2013). These issues of concern with regards to the use of coercive prac-
tice were raised following several widely reported investigations and scandals that
8

had taken place in mental health care (e.g. Blom-Cooper, 1992; Fallon, 1999; Bubb,
2014). A number of international and national documents have, as such, called for a
review and reduction in restrictive practices in secure and general mental health care
settings (e.g. American Psychiatric Association, American Psychiatric Nurses Asso-
ciation & National Association of Psychiatric Health Systems, 2003; Queensland
Government, 2008; MIND, 2013; Department of Health, 2014; NICE, 2015). The
need to reduce coercive practices in secure-care settings in order to support service
user’s personal recovery may, however, be more problematic than in general mental
health inpatient settings. As highlighted in a national briefing paper on “making re-
covery a reality in forensic settings”, there appeared to be a more complex balance
between the reduction of service users’ risk towards themselves and others whilst
also ensuring they have autonomy and choice over their own recovery (Drennan and
Wooldridge, 2014).
Staff having the ability to understand the way in which service users make sense of
coercive practice within an inpatient setting (i.e. how they react to the demands
placed upon them) may be critical for not only the staff-service user therapeutic rela-
tionship, but may also help to inform more effective ways of reducing and managing
aggressive behaviour (Cookson et al. 2012). As highlighted in previous empirical
evidence, staff placing restrictions on service users through, for example, directing
them to do something and/or being inflexible/rigid with rules, was one of the most
commonly reported triggers of service user aggression (e.g. Bjøkly, 1999; Daffern et
al., 2008; Daffern et al., 2003; Hornsveld et al., 2014; Meehan et al., 2006). Accord-
ing to Kiesler’s (1987) interpersonal theory, in our interactions with others (our inter-
personal behaviour), we are inherently predisposed to establish relationships that re-
9

inforce our sense of self; this is done through our attempts to manoeuvre others’ re-
actions through our own behaviour towards them. All people’s interactions can be
characterised by two dimensions: affiliation (hostile to friendly) and control (domin-
ance to submission). Each person is likely to align more towards one end of these di-
mensions. For example, an individual may more likely have a friendly rather than
hostile disposition whilst be more likely to submit than dominate others; this is
known as their interpersonal style. In addition, an individual’s interactions tend to
complement the interactions of others (i.e. match across the affiliation dimension but
oppose on the control dimension). For example, hostile interpersonal styles may typ-
ically be met with hostility from others whereas submissive interpersonal styles may
typically be met with dominance from others. At times, an individual’s personal
characteristics can often lead to difficulties in their interactions with others. For ex-
ample, individuals with low self-esteem may feel frustrated by those who attempt to
dominant them and in turn, may become overly dominant and rarely submissive
(BjØrkvik et al., 2009). This may be even more problematic for those with personal-
ity disorders with more extreme interpersonal styles who are likely to become ‘stuck’
at one end of the dimensions (e.g. Blackburn, 1998).
Previous research with offenders, confirms the principles of complementarity (i.e.
individuals attempt to manoeuvre others in a way that reinforces their own position)
which reveals how, when committing a violent offence, an offender’s dominant
interpersonal style is likely to elicit victim submission (e.g. Porter and Alison, 2004).
This notion is further supported by previous research studies that have reported
correlations between interpersonal style and aggression where service users in
forensic settings who were more violent were likely to have more dominant,
10

coercive, and hostile interpersonal styles (e.g. Daffern et al., 2010b; Doyle et al.,
2006; Vernham et al., 2016; Smith et al., 2013). According to Cookson and
colleagues (2012), service users with dominant and hostile interpersonal styles are
more likely to encounter problems with psychiatric inpatient treatment. More
specifically, maladaptive interpersonal functioning often reflects persistent and
problematic interpersonal styles and are often associated with aggression and
treatment non-compliance (Daffern et al., 2008).
The rules and regulations of the secure care setting (also known as coercive meas-
ures) “may challenge a service user’s dominance; they may also activate competitive
drives where service users seek to reassert control and mastery over their environ-
ment” (Daffern et al., 2008, p483). In the context of interpersonal functioning, ser-
vice users may react in an acomplementary (e.g. dominant) rather than complement-
ary (e.g. submissive) manner to assert their interpersonal dominance; this can lead to
staff typically responding to aggression by attempting to improve control and order
thus ensuring the integrity and security of the facility (Daffern et al., 2010b). It is
possible that, in turn, service users perceive staff’s attempts to restore order as threat-
ening and exploitative, which thus leads to preventative actions by service users to
restore dominance (Lillie, 2007); this is also known as the ‘aggression-coercion
cycle’ (Goren et al., 2003). Previous research has indicated how conflictful staff–ser-
vice user interactions is a factor leading to aggression on psychiatric wards (Papado-
poulos et al., 2012; Whittington & Richter, 2005). Previous studies have reported
how nurses and other ward staff who, given the time exposed to service users and the
nature of their role, were most likely to be doing the limit setting and were therefore
most likely to be the victims of service user aggression (e.g. Daffern et al., 2010b;
11

Meehan et al., 2006). More specifically, Winje and colleagues (2018) found that ser-
vice users in a secure care setting were more likely to be aggressive due to irritability
that is caused by staff making restrictions over their behaviour. According to Horow-
itz and colleagues (2006), the acomplementary behaviour displayed by service users
can be explained in the context of them viewing staff behaviour as irritating as it
frustrates the service users’ own interpersonal motives. For example, those who
value being in control are likely to be most frustrated by others who are bossy and
act superior (Henderson & Horowitz, 2006). This theoretical notion suggests that
people are differentially sensitive to specific forms of others’ interpersonal behaviour
due to a variance in their own interpersonal styles/motives, also known as interper-
sonal sensitivities. Therefore, it may be possible that some service users residing in
secure care settings may be less sensitive to, for example, the rules and regulations of
the hospital and/or staff limit setting. This, in turn, may result in service users being
less likely to display aggressive behaviour towards staff as there may not be a need to
assert their interpersonal dominance.
As highlighted above, previous research indicates that service users residing in
forensic settings are more likely to have dominant interpersonal styles and, in turn,
may react in an acomplementary manner (aggressively) to staff implementing the
more long-term coercive measures (i.e. persuasion, limit setting). However, there
seems to be a gap in the literature which looks at the way in which service users
make sense of such coercive practices in the context of their interpersonal sensitivit-
ies towards others, and in turn, whether they are more likely to respond aggressively
to such coercion.
12

2.0 Main hypotheses and research questions
2.1 Research question
Do forensic service users’ levels of interpersonal sensitivity to dominance affect
levels of self-reported anger and rates of aggression towards staff through
perceptions of staff coercion?
2.2 Research hypotheses
Hypothesis 1
Interpersonal sensitivity to dominance (sensitivity to control) and cold dominance
(sensitivity to antagonism – which is specifically related to service users’ potential to
feel belittled/provoked by staff as noted by Meehan and colleagues, (2006)) is related
to self-reported anger and recorded rates of aggression towards staff, more
specifically:
1a) Service users who have higher levels of interpersonal sensitivity to dominance
are likely to have higher levels of self-reported anger;
1b) Service users who have higher level of interpersonal sensitivity to dominance are
likely to have higher rates of recorded aggressive incidents towards staff;
1c) Service users who have higher levels of interpersonal sensitivity to cold
dominance are likely to have higher levels of self-reported anger;
1d) Service users who have higher level of interpersonal sensitivity to cold
dominance are likely to have higher rates of recorded aggressive incidents towards
staff.
Hypothesis 2
13

Interpersonal sensitivity to dominance and cold dominance is related to perceptions
of staff coercion, more specifically:
2a) Service users who have higher levels of interpersonal sensitivity to dominance
(sensitivity to control) are likely to have higher levels of perceived staff coercion;
2b) Service users who have higher levels of interpersonal sensitivity to cold
dominance (sensitivity to antagonism) are likely to have higher levels of perceived
staff coercion.
Hypothesis 3
Perceptions of staff coercion are related to self-reported anger and rates of recorded
aggression, more specifically:
3a) Service users who have higher levels of perceived staff coercion are likely to
have higher levels of self-reported anger;
3b) Service users who have higher levels of perceived staff coercion are likely to
have higher rates of recorded aggressive incidents towards staff.
Hypothesis 4
The relationship between interpersonal sensitivity to dominance and cold dominance
and self-reported anger and higher rates of recorded aggressive incidents towards
staff are mediated by perceptions of staff coercion, more specifically:
4a) The relationship between interpersonal sensitivity to dominance and self-reported
anger are mediated by perceptions of staff coercion;
4b) The relationship between interpersonal sensitivity to dominance and rates of
recorded aggressive incidents towards staff are mediated by perceptions of staff
coercion;
14

4c) The relationship between interpersonal sensitivity to cold dominance and self-
reported anger are mediated by perceptions of staff coercion;
4d) The relationship between interpersonal sensitivity to cold dominance and rates of
recorded aggressive incidents towards staff are mediated by staff coercion.
3.0 Method
3.1 Study design
A cross-sectional quantitative study design was used to examine whether the
relationship between service users' levels of interpersonal sensitivity to dominance
and self-reported anger and rates of aggression is mediated through perceptions of
staff coercion. The data were collected through completion of standardised outcome
measures from within a representative sub-sample of service users residing in high
and medium secure-care forensic settings at a specific point in time.
Early in the development of the research proposal, it was discovered that the current
research study was investigating a related/similar research topic to another trainee’s
project on the Clinical Psychology Doctorate. As the two research studies were going
to be undertaken in the same setting and with the same participant sample, it felt
appropriate to share out the task of recruitment and data collection. As such, a joint
ethics research application was conducted whereby the participant information sheet
and consent forms were designed together (with information on both research
projects) (see Appendices B and C for a copy of the participant information sheet and
consent form). Going forward in the conduct of the research, the two researchers
shared equal responsibility of recruitment and data collection (see section 3.5 for
further details).
15

3.2 Setting
Research was conducted at one high-secure and two medium secure forensic
hospitals within a London NHS Trust. The forensic hospitals were specialist services
that provided assessment, treatment, and care for people with mental illness and
personality disorders who had either been convicted of an offence or who was seen
as high risk of harm to staff or public, who had specialist rehabilitation needs, whose
behaviours were challenging, and, in the case of the high-secure service users, who
presented a high degree of risk to themselves and to others. One of the medium-
secure hospitals was a female enhanced medium secure service whereas the high-
secure and other medium-secure hospital housed male forensic service users only.
3.3 Sampling and recruitment
3.3.1 Participants
The sample consisted of male and female adults (18> years) who were forensic
service users detained under the Mental Health Act (Her Majesty’s Stationery Office
[HMSO], 1983) at a U.K. high-security or medium-security hospital.
Service users were recruited using a convenience sampling approach. This
sampling approach was deemed appropriate as it aimed to recruit service users who
were accessible, available and willing to take part in the research study. Due to the
challenging nature of recruiting service users within secure-care settings, this
sampling approach was deemed the most feasible and practical way to achieve the
target sample size.
A priori power analysis was conducted using G*Power (3.1.9.2) to determine the
estimated sample size (Faul et al., 2007). As there was limited information on the
power size calculations used in previous related research studies, a pragmatic
16

approach was used. Assuming we needed a power of 0.8 to detect a medium effect
size of F2=0.15 with alpha = 0.05, a total sample size of 70 service users needed to be
obtained.
3.3.2 Recruitment procedure
An email with participant information sheets attached was sent to the lead
responsible clinician/s, lead clinical psychologist and ward manager from each ward
within the two units (see Appendix B for a copy of the participant information sheet).
A list of all service users was provided in the email with a request for permission to
approach service users to invite them to take part in the research. The lead
responsible clinician or the lead clinical psychologist provided a response detailing
who was appropriate to approach from their ward and who was deemed too unwell
and/or unstable at present to take part in the research. Of those identified (and if there
are no concerns of risk), one of the two researchers followed up the email by visiting
the ward and liaising with the ward manager or nurse in charge before approaching
each of the service users. Service users were provided with a participant information
sheet and were given a brief description of the research. As service users were given
24 hours to decide whether they wanted to take part or not (and assuming the service
user was willing to take part in principle), the researchers liaised with the service
user and the nurse in charge to arrange an appropriate time to visit the service user on
another day to take written informed consent and to complete the questionnaires (see
Appendix C for a copy of the consent form). The written informed consent procedure
ensured that service users were not only willing to participate in the study, but to
confirm that they had: 1) read and understood the participant information sheet; 2)
been given the opportunity to ask further questions about the study; 3) understood
17

their participation was voluntary; 4) the right to withdraw at any time; 5) given
permission for us to have access to their clinical notes. If the service users made a
clear refusal (e.g. “No, I do not want to take part”) no further contact was made and
they were not included in the study. However, some service users declined on the
day (which may have been due to feeling unwell or being too busy) but were open to
taking part some other time in future. As such, these service users were re-
approached on another day and if they declined on this second approach then no
further contact was made.
From a total sample of 267 forensic mental health service users (182 male service
users from 14 wards in a high-secure hospital, 85 male and female service users from
4 male wards and 2 female wards in one medium-secure hospital), 222 were
approached to take part in the study. The 44 not approached (36= high-secure, 9=
medium secure) were deemed by their responsible clinician as either too mentally
unwell or too risky to take part in the research study. Out of the 222 who were
approached, 152(68.5%) declined, leaving 70(31.5%) service users in the final
sample.
3.4 Participant description
The 70 service users who took part in the study were predominantly male (94%) with
a mean age of 38.19 years (SD=11.0, range=23-66 years). Most service users were
White British (41.4%) or Black/Caribbean/African/Black British (27.1%), and a
majority had an index offence of violence including GBH/assault (50%) or homicide
(22.9%). The most prevalent International Statistical Classification of Diseases and
Related Health Problems 10th Revision (ICD-10) (World Health Organisation, 1992)
18

primary diagnoses were paranoid schizophrenia or delusional disorder (44.3%),
personality disorder (antisocial and borderline: 24.3%), or a dual diagnosis of
paranoid schizophrenia/delusional disorder and personality disorder (21.4%).
Fifty-four (77.1%) of the study sample were residing in a high-secure hospital. With
regards to ward types, 40(57.1%) were based in assertive rehabilitation wards,
13(18.6%) were in admission wards, 10(14.3%) were in high dependency wards, and
7(10%) were in hybrid wards. The mean overall length of stay in the current unit was
452.44 days (SD=410.88; range= 15-1909 days, median=303 days). See Table 1 for
full details of the sample’s descriptive statistics.
The sample described in this study is comparable to the general population of service
users residing in high and medium secure units based in the UK, as reported in
previous studies (e.g. Harty et al., 2004; Vӧllm et al., 2017). Most service users
described by both Harty et al. (2004) and Vӧllm et al. (2017) were male (85%) with a
mean age of 40 and 45 years old, respectively. With regards to ethnicity, the samples
were predominantly from a White British background (70%) (Harty et al., 2004) or
were reported to have been born in the UK (91.7%) (Vӧllm et al. (2017). The most
prevalent single diagnosis of service users in both studies was schizophrenia (61%
and 57.9% respectively) followed by personality disorder (45% and 46.7%
respectively). Most service user’s index offence involved some form of violence
against another person (42% and 57.9% respectively) which included homicide and
GBH. However, it is important to note that one study was conducted over ten years
(Harty et al., 2004) and the other study focused specifically on long stay service
users (10 years or more in high secure, 5 years or more in medium secure, or 15
19

years + in a combination of both high and medium secure) (Vӧllm et al., 2017) and
therefore the comparability of these samples to the current study’s sample needed to
be taken with caution.
20

Table 1: Sample description
High-secure unit (52) unit Medium-secure unit (18) Total (70)
Sex (%) Male 52 (100) Male 14(77.8)Female 4(22.2)
Male 66(94)Female 4(6)
Age Mean=37.3SD=10.6Range=23-65
Mean=40.13SD=12.6Range=25-66(Missing=3)
Mean= 38.19SD=11.0Range 23-66(Missing=3)
Ethnicity (%)
White British 27(51.9)Black/African/Caribbean/Black British 12(23.9)Asian/Asian British 2(3.8)Mixed/Multiple ethnic groups 6(11.5)White Other 1(1.9)Other ethnic group 1(1.9)Missing 3(5.8)
White British 2(11)Black/African/Caribbean/Black British 7(38.9)Mixed/Multiple ethnic groups 3(16.7)White Other 1(5.6)Other ethnic group 2(11.1)Missing 3(16.7)
White British 29 (41.4)Black/African/Caribbean/Black British 19(27.1)Asian/Asian British 2 (2.9)Mixed/Multiple ethnic groups 9(12.9)White Other 2(2.9)Other ethnic group 3(4.3)Missing 6(8.6)
Diagnosis (%)
Schizophrenia/Psychosis 21(40.4)Personality Disorder 17(32.7)Mixed PD and Schizophrenia 11(21.2)Mixed with LD 2(3.8)Missing 1(1.9)
Schizophrenia/Psychosis 10(55.5)Mixed PD and Schizophrenia 4(22.2)Depression 1(5.6)Missing 3(16.7)
Schizophrenia/Psychosis 31(44.3)Personality Disorder 17(24.3)Mixed PD and Schizophrenia 15(21.4)Mixed with LD 2(2.9)Depression 1(1.4)Missing 4(5.7)
Index Offence (%)
GBH/assault 25(48.1)Manslaughter 2(3.8)Homicide 14(26.9)Sexual Offence 3(5.8)Damage to Property 3(5.8)Other (robbery)/mixed 4(7.7)Missing 3(5.8)
GBH/assault 10(55.5)Homicide 2(11.1)Damage to Property 3(16.7)Missing 3(16.7)
GBH/assault 35 (50)Manslaughter 2(2.9)Homicide 16(22.9)Sexual Offence 3(4.3)Damage to Property 6(8.6)Other (robbery)/mixed 2(2.8)Missing 6(8.6)
Ward Type (%)
Admissions 9(17.3)High dependency 10(19.2)Assertive rehabilitation 26(50)Hybrid 7(13.5)
Admissions 4(22.2)Assertive rehabilitation 14(77.8)
Admissions 13(18.6)High dependency 10(14.3)Assertive rehabilitation 40(57.1)Hybrid 7(10)
Length of stay in current hospital (days)
0-6 months – 18(34.6)6months-1 year – 9(17.3)1-2 years – 7(13.5)2-3 years – 0(0)3-4 years – 8(15.4)4-5 years – 4(7.7)5-6 years – 1(1.9)Missing – 5(9.6)
0-6 months – 4(22.2)6months-1 year – 3(16.7)1-2 years – 5(27.8)2-3 years – 0(0)3-4 years – 1(5.6)4-5 years – 1(5.6)5-6 years – 0(0)Missing – 4(22.1)
0-6 months – 22 (36.1)6months-1 year – 12 (19.7)1-2 years – 12 (19.7)2-3 years – 0(0)3-4 years – 9(14.8)4-5 years – 5(8.2)5-6 years – 1(1.6)Missing – 9(12.9)
21

3.5 Data collection
Before completing the questionnaires, one of the two researchers went through the
participant information sheet with the service users, providing opportunity for them
to ask any questions about the research. After written informed consent was
obtained, each participant completed six structured questionnaires, two of which
were used specifically for the current research project, three were used specifically
for the other research project, and one was used in both projects (see details of the
three measures used in this research project in the section below). Those service
users who had difficulties with literacy were offered support by the researchers with
reading and writing during the completion of the questionnaires (for example,
reading through the questionnaires with them, helping them to write their response
and/or writing their responses for them). Approximately half of the study sample had
support from the researcher with completing the questionnaire; it was, however,
unclear as to how many of these service users had literacy difficulties as opposed to
how many just wanted the researcher to read the questionnaire out to them.
Completion of questionnaires took between 30-60 minutes. Service users were paid
£5 for their participation in the research study. The money was credited into their
hospital account after they had completed the questionnaires. The two researchers
collected approximately half of the data each (i.e. researchers conducted
questionnaires with around 35 participants each).
With consent from the service users, information was sought from each participant’s
electronic-based clinical notes with regards to age, gender, ethnicity, diagnosis, index
offence, and length of stay in current unit. Permission was also sought to obtain
information from the hospital incident forms (IR1’s) on the amount of times they had
22

been verbally or physically aggressive to staff in the past 12 months working back
from the date in which the participant completed the questionnaire (see outcome
measures for further details). These notes were accessed by the researcher who had
an honorary contract with the Trust for the purposes of data collection.
3.6 Measures
Service users’ interpersonal sensitivities to dominance were measured using the
Interpersonal Sensitivity Circumplex (ISC) dominant (sensitivity to the control) and
cold dominant (sensitivity to antagonism) octant scales (Hopwood et al., 2011).
Ratings of service users’ aggression (in general situations) was measured by asking
service users to complete ‘The Brief Aggression Questionnaire’ (BAQ; Webster et
al., 2014). Service users’ perceptions of staff coercion were rated using ‘The Basic
Psychological Needs Satisfaction ‘Autonomy’ sub-scale (BPNSS; Deci & Ryan
2000). Additionally, data on aggressive behaviour within the past year (this was
calculated from the point of data collection) was collected from online incident
reports and was categorised as either physical, attempted physical, or verbal.
3.6.1 Basic Psychological Needs Satisfaction Scale (BPNSS) (Autonomy subscale)
– This is a 21-item self-report questionnaire, which includes 3 subscales to assess
autonomy (7 items, α = .69), relatedness (6 items, α = .86) and competence (8 items,
α = .71), with the three subscales also forming an index of general need satisfaction
(α = .89) (Deci & Ryan, 2000). General needs satisfaction is innate, psychological
and essential for well-being and all three basic needs of autonomy, relatedness, and
competence must be fulfilled for it to occur (ibid). For the purposes of this research,
autonomy was the only sub-scale used which refers to the need to feel that one’s
23

behaviour and outcomes of the behaviour are self-determined as opposed to being
influenced or controlled by outside forces. Although not explicitly measuring
perceptions of staff coercion (for which there was no measure available), the BPNSS
autonomy sub-scale was thought to be the most appropriate measure to capture the
more long-term coercive measures used in day to day practice (i.e. persuasion,
interpersonal leverage). For example, it would be assumed that those who scored
lower on autonomy would feel more controlled/influenced by outside forces within
their current environment.
Service users were asked to rate how true a statement is for them currently (e.g. “In
my daily life, I frequently have to do what I am told”). These statements were a rated
on a 7-point Likert scale from (1) “Not at all true” to (7) “Very True”. This
questionnaire has not been validated with forensic populations however it has been
used across a wide variety of participant groups and shown to have good external
validity (Johnston & Finney, 2010).
3.6.2 Interpersonal Sensitivity Circumplex (ISC) (Hopwood et al., 2011)
(dominant and cold dominant octant scales) – The Interpersonal Sensitivity
Circumplex is a 64-item self-report questionnaire with content that represents
behaviours that would bother most people to some extent (e.g., “It bothers me when a
person is hostile”). These behaviours were rated on a 7-point Likert-type scale
ranging from (1) “not at all, never bothers me” to (7) “Very much, bothers me most
of the time.” Items cohere into eight 8-item scales (i.e., octant scales) that each
represent an interpersonal sensitivity (e.g., sensitivity to control (dominance) and
antagonism (cold dominance)). The scale has been found by the study authors to
24

show adequate internal consistency (α = .89, Range = .72–.92, dominance: α=.84,
Mean=6.04, SD=1.06; cold dominance: α=.86, Mean=6.17, SD=1.10).
3.6.3 Brief Aggression Questionnaire (BAQ) (Webster et al., 2014) is a brief
version of the Buss-Perry Hostility inventory used to measure trait aggression and
includes 4 sub-scales to assess physical aggression (e.g. “If I have to resort to
violence to protect my rights, I will”), verbal aggression (e.g. “when people annoy
me I may tell them what I think of them”), anger (e.g. “I have trouble controlling my
temper), and hostility (e.g. “When people are especially nice, I wonder what they
want”). These traits were measured on a 7-point response scale ranging from (1)
“extremely uncharacteristic of me” to (7) “extremely characteristic of me”. This
questionnaire has not been validated with forensic populations however has been
used across a wide variety of participant groups. Test–retest reliability correlations
were found by the study authors to show strong and significant total score reliability
(α = .81) with scores ranging from .68 to .81 among the four subscales.
3.7 Ethical considerations
NHS Ethics Approval was obtained from the East of England – Essex Research
Ethics Committee [18/EE/0028]. See Appendix D for the ethics approval letter.
Confidentiality and anonymity of service users were maintained by assigning each
person a study code representing their personal details (example, P1, P2) at the point
of consent. All data was identified by participant study codes from the point of
consent onwards. Hard copies of the data (including consent forms) was stored in
locked filing cabinets at the hospital site. All electronic data was stored under
25

password protected files on an encrypted USB stick. In accordance with the
University policy, all project data related to the administration of the project, (e.g.
consent forms) will be held for at least 6 years and all research data for at least 10
years.
Service users had to have capacity to consent to take part in the research and could
not be of high risk which was the reason for consent to approach each service user
being sought from their responsible clinician first. Some questions included in the
questionnaires could be of a sensitive nature for service users. As such, service users
were offered breaks if necessary and were given an opportunity to discuss any
sensitive and/or difficult issues that may have arisen during the completion of the
questionnaires. In addition, as part of the introduction we explained that we had an
obligation to pass on information regarding any risk or safeguarding concerns raised
during the interview. If any issues raised during the interview indicated that the
participant or others were at risk, the ward manager and/or named nurse linked with
the service user’s care would be informed after completion of the questionnaires.
Given that the research was in a secure-care setting, each participant’s care team
would be available to them 24/7 if they were to become distressed by the research.
3.8 Data analysis
Data was entered into the Statistical Package for the Social Sciences (SPSS) Version
25 (IBM Corp, 2017). Descriptive statistics were carried out on demographic (age,
gender, ethnicity), clinical (diagnosis), and forensic (index offence, length of stay in
current unit) characteristics of the study sample. Descriptive statistics were also used
to calculate the mean, standard deviation, and coefficient alpha (Cronbach, 1951)
26

scores for all study variables. In addition, prior to analysis of study variables, the raw
data was inspected for the presence of non-normal distribution and potential outliers
by a Shapiro-Wilk’s test (p = <0.00) and a visual inspection of histograms and box
plots.
Preliminary associations between variables were investigated through correlation
analysis (hypotheses 1-3). Bivariate Pearson Correlational statistical tests (or non-
parametric equivalents) were used to test for associations between: 1) interpersonal
sensitivity to dominance or cold dominance and perceived staff coercion (levels of
perceived autonomy); 2) interpersonal sensitivity to dominance or cold dominance
and self-reported rates of aggression; 3) interpersonal sensitivity to dominance or
cold dominance levels and rates of recorded aggressive incidents towards staff 4)
perceived staff coercion (levels of perceived autonomy) and self-reported rates of
aggression; 5) perceived staff coercion (levels of perceived autonomy) and rates of
recorded aggressive incidents towards staff. Effect sizes were also determined using
Cohen’s r (1988) standard correlation coefficient.
Mediation analysis was conducted using PROCESS (Version 31) (Hayes, 2012)
through SPSS to investigate the relationship between interpersonal sensitivity to
dominance and self-reported anger and rates of recorded aggressive incidents, with
perceived staff coercion as a mediator (hypotheses 4). For each sub-hypothesis,
mediation analysis was used to look at the direct effect, indirect effect, and the total
effect. The direct effect looks at the effect of the independent variable on the
dependent variable (also known as Pathway c’). The indirect effect looks at the effect
of the independent variable on the dependent variable through the mediating variable
27

(also known as pathway ab). The indirect effect was tested using a bootstrap
estimation approach based on 10000 samples (Preacher & Hayes, 2008). Lastly, the
total effect looks at the sum of the direct effect and the indirect effect (also known as
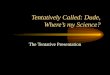
pathway c (ab + c’). See Figure 1 for an example of a basic mediation model.
Figure 1: Diagram of a basic mediation model (taken from Field, 2017)
4.0 Results
4.1 Description of outcome data
Descriptive statistics and tests of normality were run on all study variables. These
findings have been summarised below. See Table 2 for further details on this data for
each of the variables. See also Appendices E- G for the SPSS outputs for the
descriptive statistics, internal consistency, and tests of normality.
4.1.1 Interpersonal sensitivity
Cronbach’s alpha coefficient for each of the ISC dominant and cold dominant
domains ranged from .79 to .87 which indicates adequate internal consistency.
28
Independent Variable (IV)
Mediator Variable
(MV)
Dependent Variable
(DV)
Pathway a Pathway b
Pathway c’= Direct effectPathway ab= Indirect effect
Pathway c= Total effect (ab + c’)

Participants were most sensitive to antagonism (ISC cold dominance domain,
mean=4.89, SD=1.75, α=.87) which was closely followed by sensitivity to control
(ISC dominance domain, Mean=4.59, SD=1.50, α=.79). A Shapiro-Wilk’s test (p =
>0.05) and a visual inspection of histograms and box plots suggested that dominant
and cold dominant domains were normally distributed.
4.1.2 Perceptions of staff coercion (perceived autonomy)
Cronbach’s alpha coefficient for the BPNSS Autonomy sub-scale was .66 indicating
questionable internal consistency. A visual scan of item-total statistics (See
Appendix G) indicated that it would not be possible to increase the alpha coefficient
to an adequate level by the removal of any individual items. The mean BPNSS
Autonomy score in the participant sample was 4.23 (SD=.84). Although the Shapiro-
Wilk’s test (p = <0.05) rejected the null hypothesis, a visual inspection of histograms
and box plots suggested that perceived autonomy scores were normally distributed.
4.1.3 Self-reported anger
Cronbach’s alpha coefficient for BAQ total score reliability was .69 and scores
ranged from .49 to .80 among the four subscales indicating questionable internal
consistency. A visual scan of item-total statistics (see Appendix F) indicated that it
would not be possible to increase the alpha coefficient to an adequate level by the
removal of any individual items. The mean BAQ total score in the participant
sample was 3.33 (SD=.84). With regards to the sub-domains, participants scored
highest on verbal aggression (mean=3.71, SD=1.3, α=.51) which was followed by
physical aggression (mean=3.32, SD=1.7, α=.80) and hostility (mean=3.17, SD=1.5,
α=.60). Participants scored lowest on anger (mean=2.50, SD=1.1, α=.49). Although a
29

Shapiro-Wilk’s test (p = <0.05) rejected the null hypothesis, a visual inspection of
histograms and box plots suggested that self-reported anger mean total scale scores
were normally distributed.
4.1.4 Rates of aggression towards staff
A total of 308 aggressive incidents were recorded against staff within the past year.
A total of 224 (72.7%) of the incidents recorded were verbal assaults against staff, 66
(21.4%) were physical assaults against staff, and 18 (5.8%) were attempted physical
assaults against staff. These offences were committed by 28 (40%) of the 70 service
users who took part in the study. Twenty-one (30%) participants had been the
assailant for more than one incident and one participant was responsible for 81
(26.3%) of the incidents recorded. Incident data was missing for 7 (10%) participants
due to them not giving permission for the research team to access this information. A
Shapiro-Wilk’s test (p<0.001) and a visual inspection of histograms and box plots
suggested that rates of recorded incidents of aggression towards staff were positively
skewed.
30

Table 2: Descriptive statistics of study variables
Measure Domains/ sub-domains
Normative mean scores (SD)
n Mean score (SD)
Range (Median)
Alpha α
ISC (8 items for each sub-domain)
Dominance Cold dominance
Hopwood et al. (2011) n=1,3366.04 (1.06)6.17 (1.10)
70 4.59 (1.50) 4.89 (1.75)
1-8 (4.50)1-8 (4.88)
.79
.87
BAQ (12 items)
PhysicalVerbalAngerHostilityTotal score
Webster et al. (2013) n=1,0003.63 (2.15)1.70 (1.70)3.19 (1.69)3.93 (1.61)4.02 (1.21)
70 3.32 (1.7)3.71 (1.3)2.50 (1.1)3.17 (1.5)3.33 (.84)
1-7 (3.00)1-7 (3.67)1-6 (2.33)1-7 (3.00)2-6 (3.33)
.80
.51
.49
.60
.69BPNSS Autonomy
(7 items)Wei et al. (2005) n=299 5.05 (.82);
Gagne (2003) n=1185.16 (1.05)
70 4.23 (.84) 2-6 (4.14) .66
Rates of aggression towards staff in past year
Verbal Physical Attempted Total
----
63 3.56 (10.53)1.05 (2.59)0.29 (.79)4.89 (12.33)
0-74 (.00) 0-14 (.00) 0-4 (.00)0-81 (.00)
----
4.2 Correlational analysis
Preliminary relationships between variables were investigated through Bivariate
Pearson Correlational statistical analysis. Non-parametric statistical tests
(Spearman’s Rank correlation coefficient) were run on the correlations that involved
the rates of recorded aggressive incidents towards staff due to the non-normal
distribution of the data. See table 3 for the key findings from the correlational
analyses. The findings of these correlational tests have also been summarised below,
31

responding to hypotheses 1-3 outlined in the methods (see section 2.2). See also
Appendix H for the SPSS outputs for the correlational analyses.
4.2.1 Hypothesis 1: Interpersonal sensitivity to dominance, anger and aggression
1a) Interpersonal sensitivity to dominance and self-reported anger – There was a
medium (Cohen, 1988), statistically significant positive correlation between
interpersonal sensitivity to dominance and self-reported anger, r = .42**, p=<.01.
The results suggested that those who were more sensitive to others’ dominance were
likely to report higher levels of anger.
1b) Interpersonal sensitivity to dominance and rates of recorded aggressive incidents
towards staff – There was no correlation between interpersonal sensitivity to
dominance and rates of recorded aggressive incidents towards staff, r = -.05, p=.72.
1c) Interpersonal sensitivity to cold dominance and self-reported anger – There was
a small, but not significant, positive correlation between interpersonal sensitivity to
cold dominance and self-rated anger, r = .16, p= .18.
1d) Interpersonal sensitivity to cold dominance and rates of recorded aggressive
incidents towards staff – There was a small, but not significant, negative correlation
between interpersonal sensitivity to cold dominance and rates of recorded aggressive
incidents toward staff, r =-.11, p= .39.
4.2.2. Hypothesis 2: Interpersonal sensitivity to dominance or cold dominance and
perceptions of staff coercion
2a) Interpersonal sensitivity to dominance and perceptions of staff coercion – There
was no correlation between interpersonal sensitivity to dominance and perceptions of
staff coercion, r = -.08, p= .49.
32

2b) Interpersonal sensitivity to cold dominance and perceptions of staff coercion –
There was no correlation between interpersonal sensitivity to cold dominance and
perceptions of staff coercion, r = -.04, p= .78.
4.2.3 Hypothesis 3: Perceptions of staff coercion, anger and aggression
3a) Perceptions of staff coercion and self-reported anger – There was no correlation
between perceptions of staff coercion and self-reported anger, r = -.04, p= .77.
3b) Perceptions of staff coercion and rate of recorded aggressive incidents towards
staff – There was no correlation between perceptions of staff coercion and recorded
rates of aggressive incidents toward staff, r = -.08, p= .54.
Table 3: Bivariate correlations between variables
Variables Self-rated anger
Rates of recorded aggressive incidents towards staff
Perceptions of staff coercion
Interpersonal sensitivity to dominance
.42** -.05 -.08
Interpersonal sensitivity to cold dominance
.16 -.11 -.04
Perceptions of staff coercion
-.04 -.08 -
Note: **P<.01
4.3 Mediation analysis
Table 4 presents the key findings from the mediation analyses. The findings of the
mediation have also been summarised below, responding to the fourth hypothesis
outlined in the methods (see section 2.2). See also Appendix I for the SPSS outputs
for the mediation analyses.
33

4.3.1 Results for hypothesis 4a: In order to test the mediating effect of perceptions
of staff coercion on the relationship between interpersonal sensitivity to dominance
and self-rated anger, model 1 (hypothesis 4a) was tested (see Figure 1). Interpersonal
sensitivity to dominance did not significantly predict perceptions of staff coercion
and perceptions of staff coercion did not predict self-rated anger. Interpersonal
sensitivity to dominance predicted self-rated anger when perceptions of staff
coercion was or was not in the model, b=.24, 95% CI (.11, .36), p<.001. The indirect
effect confidence interval contained zero (-.02 and .02) which indicates that there
was no evidence to support the idea that perceptions of staff coercion mediates the
relationship between interpersonal sensitivity to dominance on self-rated anger. The
R² value tells us that interpersonal sensitivity to dominance explains 18% (R²=.18) of
the variance in self-rated anger. The positive coefficient (b value) tells us that as
interpersonal sensitivity to dominance increases, self-rated anger also increases.
Figure 2: Mediation model for hypothesis 4a
4.3.2 Results for Hypothesis 4b: In order to test the mediating effect of perceptions
of staff coercion on the relationship between interpersonal sensitivity to dominance
and rates of recorded aggressive incidents toward staff, model 2 (hypothesis 4b) was
34
Interpersonal sensitivity to dominance
Perceptions of staff
coercion
Self-rated anger
(Pathway a) b= -.05, p=.49
(Pathway b) b= -.00, p= .99
(Pathway c’) Direct effect, b= .24, p= .00***(Pathway ab) Indirect effect, b= .00, 95% CI
[-.02, .02]
(Pathway c) Total effect, b= .24, p= .00***

tested (see Figure 2). Interpersonal sensitivity to dominance did not significantly
predict perceptions of staff coercion and perceptions of staff coercion did not predict
rates of recorded aggressive incidents towards staff. Interpersonal sensitivity to
dominance did not predict rates of recorded aggressive incidents towards staff when
perceptions of staff coercion was or was not in the model.
Figure 3: Mediation model for hypothesis 4b
4.3.3 Hypothesis 4c: In order to test the mediating effect of perceptions of staff
coercion on the relationship between interpersonal sensitivity to cold dominance and
self-rated anger, model 3 (hypothesis 3c) was tested (see Figure 3). Interpersonal
sensitivity to cold dominance did not significantly predict perceptions of staff
coercion and perceptions of staff coercion did not predict self-rated anger.
Interpersonal sensitivity to cold dominance did not predict self-rated anger when
perceptions of staff coercion was or was not in the model.
35
Interpersonal sensitivity to dominance
Perceptions of staff
coercion
Recorded rates of
aggression towards staff
(Pathway c’) Direct effect, b= -.69, p= .51(Pathway ab) Indirect effect, b= -.02, 95% CI [-.32, .35]
(Pathway a)b= -.06, p= .38 (Pathway b)
b= .31, p= .87
(Pathway c) Total effect, b= -.71, p= .49

Figure 4: Mediation model for hypothesis 4c
4.3.4 Hypothesis 4d: In order to test the mediating effect of perceptions of staff
coercion on the relationship between interpersonal sensitivity to cold dominance and
rates of recorded aggressive incidents toward staff, model 4 (hypothesis 4d) was
tested (see Figure 4). Interpersonal sensitivity to cold dominance did not significantly
predict perceptions of staff coercion and perceptions of staff coercion did not predict
rates of recorded aggressive incidents towards staff. Interpersonal sensitivity to cold
dominance did not predict rates of recorded aggressive incidents towards staff when
perceptions of staff coercion was or was not in the model.
Figure 5: Mediation model for hypothesis 4d
36
Perceptions of staff coercion
Interpersonal sensitivity to
cold dominance
Self-rated anger
Perceptions of staff coercion
Interpersonal sensitivity to
cold dominance
Rates of recorded
aggression towards staff
(Pathway a) b= .02, p= .77 (Pathway b)
b= .49, p= .79
(Pathway c’) Direct effect, b= -.55, p= .55(Pathway ab) Indirect effect, b= .01, 95% CI
[-.19, .32]
(Pathway a) b= .02, p= .77 (Pathway b)
b= -.04, p= .73
(Pathway c’) Direct effect, b=.08, p=.18 (Pathway ab) Indirect effect, b= -.00, 95% CI
[-.04, .02]
(Pathway c) Total effect, b= .08, p= .18
(Pathway c) Total effect, b= -.54, p= .56

Table 4: Mediation analysis results
Sub-Hypotheses
Regression coefficients(for each pathway)
Measure of indirect effect
Pathway a Pathway b Pathway c’ (Direct effect)
Pathway c(Total effect)
LCI UCI Pm R²
4a) IV: ISD DV: SRA MV: PSC
-.05 -.00 .24 .24 -.02 .02 .00 .18
4b) IV: ISD DV: RRIS MV: PSC
-0.6 .31 -.69 -.71 -.32 .35 .03 .01
4c) IV: ISCDDV: SRA MV: PSC
.02 -0.4 .08 .08 -0.4 .02 -.01 .03
4d) IV: ISCD DV: RRISMV: PSC
.02 .49 -.55 -.54 -.19 .32 -.02 .01
Note: IV=dependent variable; DV= dependent variable; MV= mediating variable; ISD= interpersonal sensitivity to dominance; ISCD= interpersonal sensitivity to cold dominance; SRA= self-rated anger, RRIS= Rates of recorded aggressive incidents towards staff; PSC= perceptions of staff coercion; Pm= the proportion of the direct effect that is explained by the indirect effect.
37

URN: 6455433
5.0 Discussion
5.1 Summary of study results
The results from this study indicated a significant relationship between interpersonal
sensitivity to dominance and self-reported rates of anger, where forensic service
users’ who had higher levels of interpersonal sensitivity to others’ dominance were
likely to report higher rates of anger. There were, however, no significant
relationships found between all other study variables. Furthermore, the relationship
between forensic service users’ interpersonal sensitivity dominance/cold dominance
and self-reported anger/recorded rates of aggression towards staff were not found to
be mediated by their perceptions of staff coercion. I will first discuss these findings
in relation to relevant literature. I will then move on to discuss the findings in the
context of strengths and limitations of the chosen methodology and methods
employed to collect and analyse the data.
5.2 Contextualising the findings within previous research
The significant relationship found between interpersonal sensitivity to dominance
(control of others) and self-reported anger may be associated with the findings of
previous qualitative research whereby the controlling nature of staff was a factor
perceived by service users to contribute to repetitive acts of aggression (Meehan et
al., 2006). These findings simultaneously support and contradict previous empirical
evidence where, although dominant and coercive service user interpersonal styles
have been shown to significantly correlate with aggressive and violent behaviour
(e.g. Daffern et al., 2010a; Doyle et al., 2006; Vernham et al., 2016), in the context of
interpersonal sensitivities, we would also expect to see those who value personal
authority and being in control, to be more frustrated by the coercive behaviours of
38

URN: 6455433
others (Henderson & Horrowitz, 2006). Contrary to sensitivity to dominance, there
was no relationship found between sensitivity to cold dominance (antagonism) and
self-rated anger. Perhaps in the context of secure-care settings, a cold dominant
interpersonal style may be necessary to assert/protect one’s status, particularly when
under threat to others who are competing for a less admiring cold dominant position
(Hopwood, 2018). If we consider this notion in the context of complementarity
(Kiesler, 1987), we would expect to see those who display more cold dominant
interpersonal styles to also be less sensitive to others displaying cold dominance.
Furthermore, it may be that those who align with more cold dominant interpersonal
styles may show anger in a more passive, covert manner (moody disagreeableness,
hostility) (Hopwood et al., 2009) which is perhaps captured less so by the BAQ
compared to those more overt displays of anger (i.e. hitting out at others, losing one’s
temper).
Aside anger and aggression towards staff, in the context of a forensic service user
population, there may be a need to further consider how service users’ maladaptive
behaviours can manifest in such coercive environments. For example, given the re-
percussions for service users who do display increased aggression (i.e. increased re-
strictions such as loss of escorted or unescorted leave), perhaps there is a need to re-
store a sense of control by directing aggression elsewhere, such as bullying towards
other service users who may be considered more weaker and/or vulnerable (e.g. Ire-
land, 2006) or even through acts of self-neglect and/or self-harm (e.g. Jeglic et al.,
2005). This aligns with the current study’s findings where there was no significant
relationship found between actual rates of aggression towards staff and other study
variables; it is therefore possible that actual aggressive incidents may have been dir-
39

URN: 6455433
ected outside of the staff-service user relationship. In addition, aside coercive prac-
tices, perhaps aggressive incidents are provoked by other aversive stimuli such as,
for instance, uncontrollable noises on the ward, and interactions with other service
users (Winje et al., 2018) or the distress caused by delusions or hallucinations (e.g.
Barlow et al., 2000).
The fact that perceptions of staff coercion was not found to be a mediator between
interpersonal sensitivity to dominance and cold dominance and self-reported anger
and/or rates of aggression, challenges previous notions that coercive practices can
have a counter-therapeutic effect upon increased cycles of aggression and violence
(Goren, 1993). The current findings also contrast with previous quantitative research
which have suggested that forensic service users are more likely to respond to coer-
cive practices in an assertive (acomplementarity) manner as opposed to a submissive
(complementary) manner (Daffern et al., 2010b). Consistent with Hopwood and col-
leagues (2011) research into interpersonal sensitivities, service user participants may
have been more sensitive to interpersonal styles that are opposite to their own. For
example, those who have more dominant interpersonal styles may more likely be
sensitive to or bothered by the passivity and submissiveness of others (Hopwood et
al., 2011). As suggested in the previous section, this may be due to the questionable
validity of the questionnaire used to measure perceived coercion (autonomy sub-
scale in the BPNSS) or it may be perhaps that there is no mediating relationship to be
found. Perhaps, as suggested by Lorem and colleagues (2015), it may also be im-
portant to consider service users’ perceptions of ‘good coercion’ which coincide with
their own best interests that acts as an important measure to protect them from their
own impulses.
40

URN: 6455433
5.3 Strengths and limitations of the research process
The alpha coefficients for both the BPNSS and the BAQ both did not meet satisfact-
ory criteria for internal consistency in the current research study. This means that
there was a lack of coherence between individual questionnaire items in being able to
measure a given construct. Perhaps the items were not worded appropriately or were
not suitable to use in a forensic setting. It is therefore questionable as to how reliable
the measures were in being able to capture service users’ self-reported anger and per-
ceived autonomy.
Interestingly and unexpectedly, the mean score of perceived autonomy in the current
environment was not that dissimilar than those from previous research based within
non-forensic settings (e.g. current study: 4.23 (.84); previous studies: 5.05 (.82) (Wei
et al. 2005); 5.00 (.80) (Gagne, 2003)). Perhaps it is important to consider service
users’ perceptions of autonomy as relative to their experiences within forensic
settings. For example, those who were in assertive rehabilitation wards (wards where
service users work towards lesser security) – which was over half of the sample –
may have perceived higher levels of autonomy due to an increased sense of freedom
compared to when they were first admitted into the secure care system. A large
proportion of the study sample had been residing in secure care where just over one
third (36.1%) of the sample had been in the current unit for under 6 months. As
suggested by Vernham and colleagues (2014), it is possible that those participants
who had more recently been admitted in to secure-care have limited interpersonal
strategies and may more likely act out aggressively as a means of coping compared
to those who had stayed in secure-care for longer. In addition, mean BAQ scores
were similar in current and previous study samples and it is therefore possible that
41

URN: 6455433
forensic service users may be less likely to respond honestly about their levels of
anger due to concerns that this may impact upon their progress whilst in hospital. It
is also important to consider that, compared to the general population, forensic
service users may have limited insight into their aggressive traits, hence the
similarity in mean scores.
Although the target sample size of 70 participants was reached, in consideration of
the small effect sizes shown through some of the statistical outputs (e.g. between in-
terpersonal sensitivity to cold dominance and self-reported anger; between interper-
sonal sensitivity to cold dominance and rates of recorded aggressive incidents), a big-
ger sample size was required to detect statistical power between study variables. In
addition, while common place in inpatient settings, there was a high attrition rate
with only 31.5% of service users approached taking part in the research. It is there-
fore important to consider the representativeness of the final sample. For example,
perhaps those who chose not to take part were less happy within their current envir-
onment due to feeling more coerced and/or restricted. Furthermore, perhaps those
who were more aggressive and/or problematic with members of staff were deemed as
too risky to be included in the study and therefore not approached.
A researcher remained present with the service users whilst they completed the
questionnaires. Although this was done for the purposes of providing support to
service users if required (e.g. outlining instructions and clarifying questions), it also
resulted in all questionnaires being completed fully and as such, there was no
missing data. Over half of the service users requested for the researcher to read out
aloud and complete the questionnaires with them. It was uncertain as to whether
42

URN: 6455433
requests to have the questions read out to them was due to needing extra support with
literacy or whether the service user simply preferred to be more interactive with the
researcher (which was explicitly stated by some service users). This raises issues of
potential interviewer bias where, for example, service users may have been more
suggestible to responding in a desired way when responding directly to the
researcher compared to those who completed the questionnaires by themselves.
Conversely, there may have been a higher chance of service users who completed the
questionnaires on their own misinterpreting and/or making errors when responding to
some of the questions. Furthermore, service users would have needed to accurately
hold in mind the nature of the questionnaire whilst answering each item measure, for
instance, this may have been more problematic when completing some of the longer
outcome measures (e.g. ISC).
The retrospective nature of the recorded aggressive incidents towards staff needs to
be considered with caution. Stated as a limitation in previous research studies (e.g.
Daffern et al., 2008; Vernham et al., 2016), the data collected on the specific nature,
severity and direction of aggression perpetrated by service users may have been
reliant on the limited details of the incident forms and on the member of staff
completing such forms (although Vernham and colleagues did find a good degree of
inter-rater reliability). Furthermore, the aggressive incident may have been indirectly
targeted at the member of staff, in other words, there may have been multiple causes
outside of the staff-service user interaction that led to the aggressive behaviour (see
section below for further discussion). The fact that the recorded incidents were used
alongside service users’ self-reported anger meant that observational (incident) data
could circumvent the problems of impression management – an approach lacking in
43

URN: 6455433
previous studies. Although not reported in the main results, a significant positive
correlation was found between self-reported anger (BAQ mean scores) and rates of
recorded incidents (see Appendix J). Even though the focus of the BAQ was on self-
reported anger in general rather than self-reported anger towards staff, it can still be
assumed that there is some accuracy in the recorded incidents (i.e. verbal aggression
had the highest mean score on the BAQ and was the highest reported incident
towards staff).
When inspecting the raw data, there were some outliers with regards to some
measures (e.g. a small number of service users scored much higher on self-reported
anger and much lower on perceived autonomy than others). Unsurprisingly, these
service users had also been involved in substantially more aggressive incidents
towards staff in the last year, hence the non-normally distributed incident data. As
such, it did not feel appropriate to retract these service users’ data from the data set
as these responses seemed to coincide to the retrospective data collected. As
suggested above, perhaps including those service users who were in seclusion and/or
were more riskier, may reduce the chances of these outliers as it would be anticipated
that their BAQ mean scores (self-rated anger) and their involvement in aggressive
incidents would be higher than the majority of the participants who were included in
the sample who had been involved in no aggressive incidents in the past year. In
addition, those residing in the high dependency (more restricted) wards would also
expect to score lower on perceived autonomy in their current environment compared
to most of our sample who were residing in assertive rehabilitation wards.
44

URN: 6455433
5.4 Implications and Recommendations for policy and practice
As there was a lack of significant findings from the current study, the subsequent im-
plications and recommendations for future clinical practice have been drawn upon
from the wider literature that surrounds interpersonal style and coercive practices in
forensic settings. It is important to stress that this wider literature has been used to
make tentative suggestions of what the study’s findings might mean for clinical prac-
tice.
The findings of this study indicate that, although there was a significant relationship
between interpersonal sensitivity to dominance and self-reported anger, there was no
relationship between interpersonal sensitivity to dominance and cold dominance and
actual acts of aggression towards staff. In future practice, there may be a need to con-
sider the types of behaviours that are recorded as acts of aggression and violence and
furthermore, to try and record more subtle maladaptive behaviours that capture how
service user’s react to coercive practices (i.e. become more demanding towards staff,
bullying other service users, self-harm).
Recommendation: In future clinical practice, it may be useful to consider
the need to collect more detailed information from multiple stakeholder perspectives
about untoward incidents that have taken place. For example, building in to existing
models of practice (e.g. The ‘Safewards’ model) to ask service user/s, and more than
one member of staff on what led to the incident (Royal College of Nursing (RCN),
2016). For example, earlier events that acted as a trigger and possible rationales for
the behaviour.
45

URN: 6455433
In future clinical practice, it may be important to consider autonomy as relative to
service users’ experiences within the secure-care environment where for example,
those residing on assertive rehabilitation wards are likely to feel much less restricted
than when first admitted into hospital. Perhaps coercive practices are respected by
service users where, although they may be interpersonally sensitive to others’ domin-
ance, in the context of staffs’ duty of care, it is understood that rules, boundaries, and
restrictions are in the secure-care environment for a purpose. As suggested by Dren-
nan and Wooldridge (2014), staff and service users need to work together to develop
an organisational culture in which there is a balance between safety and recovery.
Recommendation: Rather than coercive practice being an antithesis to service
users’ autonomy and human rights (Hui et al., 2013), perhaps a more dialectical
stance needs to be taken when conceptualising coercive practices within policy and
practice. There is therefore a need to focus on how coercive practice in secure
settings is not only something that is of benefit for service users but that it also a
responsibility that they can share with staff in ensuring that themselves and others are
kept safe whilst having autonomy in the secure care environment.
Echoing previous research (Hopwood et al., 2011), service users’ interpersonal
sensitivities may be context specific. Therefore, building upon this idea, service users
may only feel bothered by coercion when it does not feel necessary and/or relevant.
For instance, the difference between a member of staff who used coercive practices
for the purposes of service users and staffs’ safety versus a member of staff who was
overly dominant on a consistent (and perhaps unnecessary) basis. The latter may be
what can lead to repetitive acts of aggression and violence by service users as this
type of coercion may be perceived be a way to belittle them. As suggested by the
46

URN: 6455433
findings of this research, whereby most service users perceived some sense of
autonomy in their current environment, it may be that the use of coercive practices
within a secure-care setting is not seen by service users to unnecessarily restrict them
on a day to day basis.
Recommendation: As suggested in a document on ‘Positive and Proactive
Care’ (Royal College of Nursing, 2016), “avoiding assumptions, threats and
provocations adds to positive outcomes” (pp. 7). This approach may respond to the
interpersonal motives of those service users who may be more interpersonally
sensitive to others’ dominance whereby the implementation of coercive practices
within secure-care settings should take place in the context of mutually respected and
positive relationships between staff and service users (DH, 2014). Furthermore, with
collaborative empowerment as central to care, psychosocial interventions such as
persuasion and negotiation should be made a transparent part of everyday
communication between staff and service users. As suggested by Winje and
colleagues (2018), perhaps enhanced methods for communicating restrictions on
service users’ behaviour (e.g. remaining calm with self-assured expressions) needs to
be incorporated into staff training. This coincides with previous research that
suggests good clinical practice cannot be separated from the formal, moral evaluation
of coercion (i.e. was it necessary and was it implemented with open communication
and empathy) (Lorem et al., 2015).
5.5 Recommendations for future research
Future research should attempt to widen the participant sample to those who are pos-
sibly seen as riskier, such as those in seclusion or who are residing on higher depend-
ency wards. This may help to provide more variance and/ or extremities in service
47

URN: 6455433
users’ views of their current environment where, for example, there are lower per-
ceptions of autonomy and higher levels of self-rated anger. Assuming interpersonal
relationships between service user and staff are more problematic (particularly con-
sidering that 40% of the sample had displayed violent behaviour in the past year), it
would also be assumed that interpersonal sensitivities would be more extreme and
possibly directed to their current circumstances.
As indicated in the current study and in previous research (e.g. Chambers et al.,
2009), there is a lack of standardised outcome measures that have been validated
within forensic populations and as such the internal validity of what is being meas-
ured is questionable given their use in non-forensic populations. Therefore, there is a
need for more measures to be validated specifically for forensic service users who
are residing in secure-care settings. More specifically, there is no outcome measure
that adequately captures service users’ perception of staff coercion. As such, the de-
velopment of an outcome measure that explicitly captures either perceptions of coer-
cion and/or autonomy which is specifically designed and validated within a forensic
setting would be beneficial for future research studies. For example, perhaps to
measure actual levels of restriction instead of perceived lack of autonomy, an ordinal
scale of “restrictiveness” could be developed to look at, for instance, perceptions of
seclusion, ward placement, and ground access. Furthermore, it would be useful to
measure self-reported anger specifically towards staff as opposed to general self-re-
ported anger as this may give a more specific indicator as to the extent to which ser-
vice users experience anger towards staff and in turn, whether this is related to per-
ceptions of coercion.
48

URN: 6455433
Given that individuals may be more sensitive to interpersonal styles that are opposite
to their own (Hopwood et al., 2011), future research would benefit from looking
more explicitly at the relationship between interpersonal styles and interpersonal
sensitivities. For example, it would be useful to find out whether, in a forensic
service user population, if service users’ reactions to staff coercion are more
submissive (complementary) or dominant (accomplementary). The complementarity
of their reactions to coercion therefore needs to not only consider whether others’
controlling behaviour is bothering to the person (their interpersonal sensitivity) but
also how they are then predisposed to react to the coercion of others (their
interpersonal style).
In addition, as interpersonal theory relies on the way in which individuals establish
relationships with others (Kiesler, 1997), it may be useful to investigate staff’s own
interpersonal styles and sensitivities. Perhaps some staff members have more
dominant interpersonal styles than others and may be therefore seen as more
coercive. Aside the implementation of hospital rules and regulations that encapsulate
restrictive practice, this would help to shed light on how staff characteristics interact
with service users own sense making and reactions to such coercive measures (i.e. it
may be more about the way in which coercive practices are implemented).
6.0 Conclusion
In conclusion of the study’s findings, perceptions of staff coercion (perceived
autonomy) was not found to mediate the relationship between interpersonal sensitiv-
ity to dominance/cold dominance and self-reported anger and rates of aggression to-
wards staff. Furthermore, although there was a significant relationship found
49

URN: 6455433
between interpersonal sensitivity to dominance and self-reported anger, there was no
relationship between interpersonal sensitivity and actual rates of aggressive incidents
towards staff. It may be important to consider some of the implications that these
non-significant findings have upon clinical practice, where it may not be coercive
practices that are necessarily increasing rates of aggression (as indicated by previous
research) but may be the way in which coercive practices are implemented. These
non-significant findings may also, in part, be due to some of the study’s limitations.
For example, the use of measures which had not been validated in a forensic popula-
tion, the unavailability of measures that accurately captured study variables (i.e. per-
ceptions of staff coercion), and the possible need for a larger sample size. With these
limitations in mind, the conclusions that were drawn from the current study’s find-
ings should be considered under a tentative lens. The conduct of future related re-
search (as discussed in the previous section) should be considered in context of the
study’s limitations and recommendations.
References
American Psychiatric Association, American Psychiatric Nurses Association & National Association of Psychiatric Health Systems. (2003). Learning from each other: Success stories and ideas for reducing restraint/seclusion in behavioural health. Retrieved from WorldCat Website: https://www.worldcat.org/title/learning-from-each-other-success-stories-and-ideas-for-reducing-restraintseclusion-in-behavioral- health/oclc/52758580
Barlow, K., Grenyer, B., & Ilkiw-Lavalle, O. (2000). Prevalence and precipitants of aggression in psychiatric inpatient units. Australian and New Zealand Journal of Psychiatry, 34(6), 967-974. DOI: 10.1080/000486700271
Bjørkly, S. (1999). A ten‐year prospective study of aggression in a special secure unit for dangerous patients. Scandinavian Journal of Psychology, 40(1), 57-63. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/10216464
BjØrkvik, J., Biringer, E.V.A., Eikeland, O.J., & Nielson, G.H. (2009). Self-esteem and interpersonal functioning in psychiatric outpatients. Scandinavian
50

URN: 6455433
Journal of Psychology, 50(3), 259-265. DOI: 10.1111/j.1467-9450.2009.00709
Blackburn, R. (1998). Relationship of personality disorders to observer ratings of interpersonal style in forensic psychiatric patients. Journal of Personality Disorders, 12(1), 77-85. DOI: 10.1521/pedi.1998.12.1.77
Blom-Cooper, L. (1992). Report of the Committee of Inquiry into Complaints about Ashworth Hospital, Cm 2028-1. London: HMSO.
Bowers, L., Stewart, D., Papadopoulos, C., Dack, C., Ross, J., Khanom, H., & Jeffery, D. (2011). Inpatient violence and aggression: a literature. Report from the Conflict and Containment Reduction Research Programme. Retrieved from http://www.kcl.ac.uk/iop/depts/hspr/research/ciemh/mhn/projects/litreview/Li
tRevAgg .pdf
Bubb, S. (2014). Winterbourne view–time for change: transforming the commissioning of services for people with learning disabilities and/or autism. Retrieved from British Library Website: https://www.bl.uk/collection-items/winterbourne-view--time-for-change-transforming-the-commissioning-of-services-for-people-with-learning-disabilities-andor-autism
Castro, M., Cockerton, T., & Birke, S. (2002). From discharge to follow-up: a small-scale study of medium secure provision in the independent sector. British Journal of Forensic Practice, 4, 31-9. DOI: 10.1108/14636646200200019
Chambers, J. C., Yiend, J., Barrett, B., Burns, T., Doll, H., Fazel, S., Jenkinson, C., Kaur, A., Knapp, M., Plugge, E., Sutton, L., & Sutton, L. (2009). Outcome measures used in forensic mental health research: a structured review. Criminal Behaviour and Mental Health, 19(1), 9-27. DOI: 10.1002/cbm.724
Cohen, J. (1988). Statistical power analyses for the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum.
Cookson, A., Daffern, M., & Foley, F. (2012). Relationship between aggression, in-terpersonal style, and therapeutic alliance during short‐term psychiatric hospi-talization. International Journal of Mental Health Nursing, 21(1), 20-29. DOI:10.1111/14470349.2011.00764
Cronbach, L. J. (1951). Coefficient alpha and the internal structure of tests. Psychometrika, 16, 297-334. Retrieved from https://link.springer.com/article/10.1007/BF02310555
Daffern, M., Mayer, M. M., & Martin, T. (2003). A preliminary investigation into patterns of aggression in an Australian forensic psychiatric hospital. Journal of Forensic Psychiatry and Psychology, 14(1), 67–84. DOI: 10.1080/1478994031000074306.
51

URN: 6455433
Daffern, M., Duggan, C., Huband, N., & Thomas, S. (2008). The impact of interpersonal style on aggression and treatment non-completion in patients with personality disorder admitted to a medium secure psychiatric unit. Psychology, Crime & Law, 14(6), 481-492. DOI: 10.1080/10683160801948717
Daffern, M., Duggan, C., Huband, N., & Thomas, S. (2010a). Staff and Patient’s Perceptions of Each Other’s Interpersonal Style Relationship with
Severity of Personality Disorder. International Journal of Offender Therapy and Comparative Criminology, 54(4), 611-624. DOI: 10.1177/0306624X09335111
Daffern, M., Tonkin, M., Howells, K., Krishnan, G., Ijomah, G., & Milton, J. (2010b). The impact of interpersonal style and perceived coercion on aggression and self-harm in personality-disordered patients admitted to a secure psychiatric hospital. The Journal of Forensic Psychiatry & Psychology, 21(3), 426-445. DOI:10.1080/14789940903505951
Deci, E. L., & Ryan, R.M. (2000). The “what” and the “why” of goal pursuits: Human needs and the self-determination of behaviour. Psychological Inquiry, 11, 227-268. DOI: 10.1207/S15327965PLI1104_01
Department of Health. (2014). Positive and proactive care: reducing the need for restrictive interventions. Retrieved from Department of Health Website: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/
attac hment_data/file/300293/JRA_DoH_Guidance_on_RP_web_accessible.pdf
Dickens, G., Picchioni, M., & Long, C. (2013). Aggression in specialist secure and forensic inpatient mental health care: incidence across care pathways. Journal of Forensic Practice, 15, 206-17. DOI: 10.1108/JFP-09-2012-0017
Doyle, M., & Dolan, M. (2006). Evaluating the validity of anger regulation problems, interpersonal style, and disturbed mental state for predicting inpatient violence. Behavioral Sciences & the Law, 24(6), 783-798. DOI: 10.1002/bsl.739
Drennan, G., & Wooldridge, J. (2014). Making recovery a reality in forensic services. Implementing Recovery through Organisational Change (ImROC) briefing paper. Retrieved from the Centre for Mental Health and Mental Health Network NHS Confederation Website: file:///C:/Users/jess/Downloads/ImROC-briefing-10-Making-Recovery-a-Reality-in-Forensic-Settings-final-for-web%20(1).pdf
Fallon, P. (1999). Report of the Committee of Inquiry into the Personality Disorder Unit, Ashworth Specialised Hospital, Cm 4194-1. HMSO, London.
52

URN: 6455433
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175-191. Retrieved from https://link.springer.com/article/10.3758/BF03193146
Field, A. (2017). Discovering statistics using IBM SPSS Statistics. London: Sage Publications Ltd.
Gagne, M. (2003). Autonomy support and need satisfaction in the motivation and well-being of gymnasts. Journal of Applied Sport Psychology, 15(4), 372-390. DOI: 10.1080/714044203
Goren, S., Singh, N. N., & Best, A. M. (1993). The aggression-coercion cycle: Use of seclusion and restraint in a child psychiatric hospital. Journal of Child and Family Studies, 2(1), 61–73. Retrieved from https://link.springer.com/article/10.1007/BF01321301
Harty, M. A., Shaw, J., Thomas, S., Dolan, M., Davies, L., Thornicroft, G., Carlisle, J., Moreno, M., Leese, M., Appleby, L., & Jones, P. (2004). The security, clinical and social needs of patients in high security psychiatric hospitals in England. Journal of Forensic Psychiatry & Psychology, 15(2), 208-221. DOI: 10.1080/14789940410001703967
Hayes, A. F. (2012). PROCESS: A versatile computational tool for observed variable mediation, moderation, and conditional process modelling [White paper]. Retrieved from http://www.afhayes.com/ public/process2012.pdf
Henderson, L., & Horowitz, L. M. (2006). Social allergens and frustrated interpersonal motives, presented at the Society for Interpersonal Theory and Research Conference, Philadelphia, 2006. Philadelphia, PA: Society for Interpersonal Theory and Research.
Her Majesty’s Stationery Office (HMSO). (1983). Mental Health Act 1983, c12. Retrieved from https://www.legislation.gov.uk/ukpga/1983/20/contents
Holmes, D., Rudge T. & Person, A. (2012). Rethinking violence in health care settings. Ashgate, Farnham: Routledge.
Hopwood, C. J. (2018). Interpersonal dynamics in personality and personality disorders. European Journal of Personality, 32(5), 499-524. DOI: 10.1002/per.2155
Hopwood, C. J., Ansell, E. B., Pincus, A. L., Wright, A. G., Lukowitsky, M. R., & Roche, M. J. (2011). The circumplex structure of interpersonal sensitivities. Journal of Personality, 79(4), 707-740. DOI: 10.1111/j.1467-6494.2011.00696
Hopwood, C. J., Morey, L. C., Markowitz, J. C., Pinto, A., Skodol, A. E., Gunderson, J. G., Zanarini, M. C., Shea, T., Yen, S., McGlahsan, T.H., Ansell, E.B., Grilo, C.M., Sanislow, C. A. (2009). The construct validity of
53

URN: 6455433
passive-aggressive personality disorder. Psychiatry: Interpersonal and Biological Processes, 72, 256–268. DOI: 10.1521/psyc.2009.72.3.256
Hornsveld, R. H., Kraaimaat, F. W., Bouwmeester, S., Polak, M. A., & Zwets, A. J. (2014). Behavior on the ward of personality-disordered inpatients and chroni-cally psychotic inpatients during a three-year stay in a Dutch forensic psychiatric hospital. The Journal of Forensic Psychiatry & Psychology, 25(6), 684-704. DOI: 10.1080/14789949.2014.947308
Horowitz, L. M., Wilson, K. R., Turan, B., Zolotsev, P., Constantino, M. J., & Henderson, L. (2006). How interpersonal motives clarify the meaning of interpersonal behavior: A revised circumplex model. Personality and Social Psychology Review, 10, 67–86. DOI: 10.1207/s15327957pspr10014
Hui, A., Middleton, H., & Völlm, B. (2013). Coercive measures in forensic settings: findings from the literature. International Journal of Forensic Mental Health, 12(1), 53-67. DOI: 10.1080/14999013.2012.740649
IBM Corp. (2017). IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.
Ireland, J. L. (2006). Bullying among mentally‐ill patients detained in a high‐secure hospital: an exploratory study of the perceptions of staff and patients into how bullying is defined. Aggressive Behavior: Official Journal of the International Society for Research on Aggression, 32(5), 451-463. DOI: 10.1002/ab.20145
Jeglic, E. L., Vanderhoff, H. A., & Donovick, P. J. (2005). The function of self-harm behavior in a forensic population. International Journal of Offender Therapy and Comparative Criminology, 49(2), 131-142. DOI: 10.1177/0306624X04271130
Johnston, M. M., & Finney, S. J. (2010). Measuring basic needs satisfaction: Evaluating previous research and conducting new psychometric evaluations of the Basic Needs Satisfaction in General Scale. Contemporary Educational Psychology, 35(4), 280-296. DOI: 10.1016/j.cedpsych.2010.04.003
Kiesler, D. (1987). Manual for the Impact Message Inventory. Mountain View, CA: Consulting Psychologists Press.
Kiesler, D. J. (1997). Contemporary interpersonal theory and research: Personality, psychopathology and psychotherapy. The Journal of Psychotherapy Practice and Research, 6(4), 339-341. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3350312/
Lillie, R. (2007). Getting clients to hear: Applying principles and techniques of Kiesler's Interpersonal Communication Therapy to assessment feedback. Psychology and Psychotherapy: Theory, Research and Practice, 80(1), 151-163. DOI: 10.1348/147608306X115198
54

URN: 6455433
Lorem, G. F., Hem, M. H., & Molewijk, B. (2015). Good coercion: Patients' moral evaluation of coercion in mental health care. International Journal of Mental Health Nursing, 24(3), 231-240. DOI: 10.1111/inm.12106
Mason, T. (1993). Seclusion as a cultural practice in a special hospital. Educational Action Research, 1(3), 411–423. DOI: 10.1080/0965079930010307
Mason, T. (2006). Introduction. In T. Mason (Ed.), Forensic psychiatry: Influences of evil (pp.1– 14). New Jersey, NJ: Human Press.
Meehan, T., McIntosh, W., & Bergen, H. (2006). Aggressive behaviour in the high‐secure forensic setting: the perceptions of patients. Journal of Psychiatric and Mental Health Nursing, 13(1), 19-25. DOI: 10.1111/j.1365-
2850.2006.00906
Mezey, G. C., Kavuma, M., Turton, P., Demetriou, A., & Wright, C. (2010). Perceptions, experiences and meanings of recovery in forensic psychiatric patients. The Journal of Forensic Psychiatry & Psychology, 21(5), 683-696. DOI:10.1080/14789949.2010.489953
Mind (2013). Physical Restraint in Crisis: A report on physical restraint in hospital settings in England. Retrieved from Mind Website: https://www.mind.org.uk/media/197120/physical_restraint_final_web_version.pdf
NICE. (2015). Violence and Aggression: short-term management in mental health, health and community settings. Retrieved from National Institute of Clinical Excellence Website: https://www.nice.org.uk/guidance/ng10
Papadopoulos, C., Ross, J., Stewart, D., Dack, C., James, K., & Bowers, L. (2012). The antecedents of violence and aggression within psychiatric in‐patient settings. Acta Psychiatrica Scandinavica, 125(6), 425-439. DOI: 10.1111/j.1600-0447.2012.01827.x
Porter, L.E., & Alison, L.J. (2004). Behavioral coherence in violent group activity: An interpersonal model of sexually violent and gang behavior. Aggressive Behavior, 30, 449–468. DOI: 10.1002/ab.20047
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879-891. Retrieved from https://link.springer.com/article/10.3758/BRM.40.3.879
Queensland Government. (2008). Policy statement on reducing and where possible eliminating restraint and seclusion in Queensland mental health services. Retrieved from http://www.health.gld.gov.uk/mentalhealth/docs/sandrpolicy 081030.pdf.
55

URN: 6455433
Royal College of Nursing. (2016). Proactive and Positive Care: Reducing the need for Restrictive Interventions. London: RCN.
Shaw, J., Davies, J., & Morey, H. (2001). An assessment of the security, dependency and treatment needs of all patients in secure services in a UK health region. The Journal of Forensic Psychiatry, 12(3), 610-637. DOI: 10.1080/09585180127380
Smith, S. T., Edens, J. F., & McDermott, B. E. (2013). Fearless dominance and self-centered impulsivity interact to predict predatory aggression among forensic psychiatric in patients. International Journal of Forensic Mental Health, 12(1), 33-41. DOI: 10.1080/14999013.2012.760186
Szmukler, G., & Appelbaum, P. S. (2008). Treatment pressures, leverage, coercion, and compulsion in mental health care. Journal of Mental Health, 17(3), 233-244. DOI: 10.1080/09638230802052203
Vernham, Z., Tapp, J., & Moore, E. (2016). Observer ratings of interpersonal behavior as predictors of aggression and self-harm in a high-security sample of male forensic inpatients. Journal of Interpersonal Violence, 31(9), 1597-1617. DOI: 10.1177/0886260515569060
Völlm, B., Edworthy, R., Holley, J., Talbot, E., Majid, S., Duggan, C., Weaver, T., & McDonald, R. (2017). A mixed-methods study exploring the characteristics and needs of long-stay patients in high and medium secure settings in England: implications for service organisation. Health Service and Delivery Research, 5(11). Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK424815/
Webster, G. D., DeWall, C. N., Pond, R. S., Jr., Deckman, T., Jonason, P. K., Le, B. M., & Bator, R. J. (2014). The Brief Aggression Questionnaire: Psychometric and behavioural evidence for an efficient measure of trait aggression. Aggressive Behavior, 40, 120–139. DOI:10.1002/ab.21507
Wei, M., Shaffer, P. A., Young, S. K., & Zakalik, R. A. (2005). Adult attachment, shame, depression, and loneliness: The mediation role of basic psychological needs satisfaction. Journal of Counseling Psychology, 52(4), 591. DOI: 10.1037/0022- 0167.52.4.591
Whittington, R., & Richter, D. (2005). Interactional aspects of violent behaviour on acute psychiatric wards. Psychology, Crime & Law, 11(4), 377-388. DOI: 10.1080/10683160500255372
Winje, M., van Mastrigt, S., Gjestad, R., Urheim, R., & Rypdal, K. (2018). Staff members’ evaluation of inpatients’ motivation for aggression–the roles of staff restrictions and aggression severity. The Journal of Forensic Psychiatry & Psychology, 29(3), 419-433. DOI: 10.1080/14789949.2017.1410563
56

URN: 6455433
World Health Organisation. (1992). ICD-10 Classifications of Mental and Behavioural Disorder. Geneva: World Health Organisation.
57

URN: 6455433
MRP Empirical Paper Appendices
List of appendices to the empirical paper
Appendix A – Glossary of terms
Appendix B – Participant information sheet
Appendix C – Consent form
Appendix D – Ethics approval letter
Appendix E – SPSS Outputs: Descriptive statistics
Appendix F – SPSS Outputs: Internal consistency tests
Appendix G – SPSS Outputs: Tests of normality
Appendix H - SPSS Outputs: Correlation analyses for hypotheses 1-3
Appendix I – SPSS Outputs: Mediation analyses
58

URN: 6455433
Appendices to the empirical paper
Appendix A – Glossary of terms
Forensic psychiatric hospitals: secure facilities that treat and rehabilitate individuals who have come in conflict with the law and are deemed unfit to stand trial or not criminally responsible due to mental illness.
High-secure services: high secure services cater for service users who pose a grave and immediate danger.
Medium secure services: medium secure services cater for those service users who present serious danger to the public.
Index offence: Also known as an index crime which includes: murder and non-negligent homicide, rape, robbery, aggravated assault (or grievous bodily harm), burglary, larceny-theft, arson, and auto theft.
The Mental Health Act (1983): main piece of legislation that covers the assessment, treatment, and rights of people with a mental health disorder.
Mental Health Act Section: a case when someone can be detained under the Mental Health Act (1983) and treated without their agreement. People detained under the Mental Health Act and need urgent mental health treatment and are at risk of harm to themselves or others.
Assertive rehabilitation wards: wards where service users are likely to spend most of their time in secure care and is for the purposes of working towards a place of lesser security.
Admission wards: wards set up specifically for service users’ arrival in to hospital. There is a higher ratio of staff to service users on these wards. Service users spend their time being assessed on these wards and depending upon progress, will move to another acute treatment or rehabilitation wards.
High dependency wards: wards set up for service users who are at immediate risk higher level of staffing and physical security.
Hybrid wards: wards set up for service users who have dual diagnosis (personality disorder and mental health).
Risk management: involves the development of flexible strategies aimed at preventing any negative event from occurring or, if this is not possible, minimising the harm caused.
Anger: a strong emotion of annoyance, displeasure, or hostility.
Aggression: feelings of anger that result in hostile or violent behaviour (whether verbal or physical) or readiness to attack or confront.
Violence: behaviour involving physical force intended to hurt, damage, or kill someone or something.
Coercion: the action or practice of persuading someone to do something by using force or threats.
59

URN: 6455433
Coercive/restrictive practice (in mental health settings): including the short-term (e.g, seclusion and restraint) and long-term (e.g. limit setting, persuasion, interpersonal leverage) management of aggression and violence.
Manual restraint: direct contact with service users with an intention to prevent or restrict a person's movement. Used when a person poses an imminent risk of physical harm to self or others and it intended to be the least restrictive intervention that achieves safety.
Rapid tranquilisation: when medicine is given to a person who is very agitated or displaying aggressive behaviour to help quickly calm them.
Seclusion: a type of restraint that involves confining a person in a room from which the person cannot exit freely.
Long-term segregation: a situation where, in order to reduce risk of harm posed by service users to others (which is a continuous feature of their presentation), service users should not be allowed to mix freely with other service users on the ward or unit on a long-term basis.
Paradoxical effects: an effect of treatment which is opposite to the effect that would normally be expected.
Dominance: power or influence over another.
60

URN: 6455433
Appendix B – Participant information sheet
[NHS Trust logo]
Participant information sheet(Version number: 4.0 25/05/2018)
How do service users’ interpersonal style and perceptions of the therapeutic environment impact upon rates of aggression and treatment readiness in secure-
care settings?
IntroductionOur names are [name of trainee] and [name of trainee] and we are Trainee Clinical Psychologists working in the NHS and studying at the University of Surrey. We would like to invite you to take part in a research project. Before you decide you need to understand why the research is being done and what it will involve for you. Please take the time to read the following information carefully. Talk to others about the study if you wish.
Why are we doing the research?We are interested in exploring how people staying in secure care settings view their relationships with staff and in turn, how this impact on rates of aggression and treatment motivation.
Why have I been invited?You have been invited to take part in this research as you are staying in either a medium or high secure hospital.
What will happen to me if I agree to take part? Before you decide to take part you will have the opportunity to ask any questions relating to the study. If you decide to take part we will ask you to sign a consent form, you will receive a copy of this and we will keep a copy in the research file. You will be provided with opportunity to have an Independent Mental Health Advocate or a member of staff present during your participation in the study.
During your participation you will be asked to complete five questionnaires, three will ask about relationship experiences, one will ask about the causes of aggression, and two will ask about treatment motivation. We expect that completion of the questionnaires will take approximately 45 minutes – 1 hour in total, in which you can take a break or discontinue if required. This will be a one-off occasion.
The research team will also ask for your permission to review your clinical notes as part of this research to obtain some additional information on 1) the number (if any) of untoward incidents that you have been involved in over the past month and 2) your engagement in treatment programmes over the past 12 months. We will also collect some basic demographic information (such as age, ethnicity and gender). In
61

URN: 6455433
reviewing your clinical notes, we will only record information about the above things, nothing more. In addition, you will be paid to £5 for your participation in the research study. This money will be credited in to your hospital account after you have completed the questionnaires.
Do I have to participate?No, you do not have to participate. Your participation is voluntary, and you are free to withdraw at any time, without giving any reason, and without your legal rights or clinical care being affected.
Having said this, if you do decide to participate this will also not contribute to any further progression in your care. You have the right to withdraw your data from the project up to the point of data analysis. After this time frame, we may not be able to remove the data from the analysis process.
Who has reviewed the study?All research in the NHS is looked at by independent group of people, called a Research Ethics Committee, to protect your interests. This study has been reviewed and given favourable opinion by the [name of research ethics committee] (18/EE/0028).
Will my Participation be kept confidential?All information which is collected about you during the course of the research will be kept strictly confidential, hard copies of questionnaires and consent forms will be scanned and uploaded on to an encrypted USB stick and the paper copies will be kept in a locked filing cabinet at the hospital site in the office of the research supervisor. Any information about you will be removed (anonymised) and a unique code will be used so that you cannot be recognised from it.
We will let your clinical team know that you have agreed to take part in this research project, but we will not share details with them. However, if you tell us about any criminal offences or things that suggest there is a risk of harm to yourself or others during the interview, we will need to share these with your clinical team, and possibly with other authorities (such as the police). We will talk to you about this if this occurs, so you are aware of what we are sharing.
All project data related to the administration of the project, (e.g. consent form) will be held for at least 6 years and all research data for at least 10 years in accordance with University policy. Your personal data will be held and processed in the strictest confidence, and in accordance with current data protection regulations.
Who is organising and funding this research?This research is a part of our Clinical Psychology Doctorate training programme and is funded by the Psychology department at the University of Surrey.
What will happen to the results of this research?A written report will be prepared with the view to publishing the results. If you would like a copy of the published report please indicate this on the consent form and
62

URN: 6455433
a copy will be sent to you. We will contact your primary nurse about sending this to you, which can be via the post or email. Please note that you will not be identified in any report or publication that arises as result of this study. We may use anonymise direct quotes in reports or publications. We will also be producing a summary of the results which we can send to you after the study is completed.
What if there is a problem?Any complaint or concern about any experience during the course of this will be addressed. Your primary nurse can contact [name of research supervisor], who is supervising this research. He will be able to contact the researchers, who will then arrange to come to the ward to discuss any concerns and answer any questions you may have about the research. If you have a complaint, he will also be able to contact the Programme Director at the University (contact details below). You would also be able to put your complaint into writing (with some help from your primary nurse or the advocacy service if needed) and your primary nurse will be given details of how and where to send this.
Who is handling my data?As researchers on behalf of the University of Surrey will collect information about you for this research study from you directly and your service user notes. We will not provide any identifying information about you to The University of Surrey. We will use this information as explained in the ‘What will happen to me if I agree to take part’ section above. This information will include age, ethnicity, gender, index offence, and length of stay and health information like MHA section which is regarded as a special category of information. We will use this information as explained in the ‘What will happen to me if I agree to take part’ section above.
What will happen to my data? As a publicly-funded organisation, we have to ensure when we use identifiable personal information from people who have agreed to take part in research, this data is processed fairly and lawfully and is done so on the basis of public interest This means that when you agree to take part in this research study, we will use your data in the ways needed to conduct and analyse the research study.
Your rights to access, change or move your information are limited, as we need to manage your information in specific ways in order for the research to be reliable and accurate. If you decide to withdraw your data from the study, we may not be able to do so. We will keep the information about you that we have already obtained. To safeguard your rights, we will use the minimum personally-identifiable information possible.
You can find out more about how we use your information https://www.surrey.ac.uk/information-management/data-protection and/or by contacting [email protected]
What if I want to complain about the way data is handled?
If you wish to raise a complaint on how we have handled your personal data, you can contact our Data Protection Officer [name of officer] who will investigate the matter.
63

URN: 6455433
If you are not satisfied with our response or believe we are processing your personal data in a way that is not lawful you can complain to the Information Commissioner’s Office (ICO) (https://ico.org.uk/). For contact details of the University of Surrey’s Data Protection Officer please visit: https://www.surrey.ac.uk/information-management/data-protection
Further Information
Researchers: [contact details of trainee researchers]
Research supervisor:[contact details of research supervisor]
The University has in force the relevant insurance policies which apply to this study. If you wish to complain, or have any concerns about any aspect of the way you have been treated during the course of this study then you should follow the instructions given above.
Alternative Contact details
[name of programme director]
Independent Mental Health Advocacy ServiceAddress: PO Box 14043, Birmingham, B6 9BLTelephone number: 0300 456 2370Email Address: [email protected]
64

URN: 6455433
Appendix C – Consent form
[NHS Trust logo here]
CONSENT FORM (Version number: 3.0 25/05/18)
Title of Study: Interpersonal style, attachment and perceptions of the secure care environment.
Name of Researcher: Name of Participant:
1. I confirm that I have read and understand the information sheet version number …………dated...................................... for the above study and have had the opportunity to ask questions.
2. I understand that my participation is voluntary and that I am free to withdraw at any time, without giving any reason, and without my medical care or legal rights being affected. I understand that should I can ask for information to be withdrawn at a point before October 2018. After this point, information cannot be erased as it will have been used in the project analysis.
3. I understand that anonymised data collected in the study may be looked at by authorised individuals from the research group where it is relevant to my taking part in this study.
4 I give permission for these individuals to have access to these records and to collect, store, analyse and publish information obtained from my participation in this study. This may include anonymised direct quotes.
5. I understand that my personal details will be kept confidential.
6. I understand that should I disclose any information that puts me or others at imminent risk, my clinical team and/or Responsible Clinician will be informed of this.
7. I agree to my notes being accessed by the research team.
8. I agree to take part in the above study.
9. I would like a summary of the study results.
10. I agree for my special category data (ethnicity) to be collected for the purposes stated in the information sheet.
__________________ ______________ ____________________Name of Participant Date Signature______________ ______________ ____________________Name of Person taking consent Date Signature
65
Please initial box

URN: 6455433
Appendix D – Ethics approval letter
66

URN: 6455433
67

URN: 6455433
68

URN: 6455433
Appendix E – SPSS Outputs: Descriptive statistics
DescriptivesStatistic Std. Error
DOM_mean Mean 4.59 .17995% Confidence Interval for Mean
Lower Bound
4.23
Upper Bound
4.95
5% Trimmed Mean 4.59Median 4.50Variance 2.236Std. Deviation 1.495Minimum 1Maximum 8Range 7Interquartile Range 2Skewness .147 .287Kurtosis -.558 .566
CD_Mean Mean 4.89 .20995% Confidence Interval for Mean
Lower Bound
4.48
Upper Bound
5.31
5% Trimmed Mean 4.90Median 4.88Variance 3.049Std. Deviation 1.746Minimum 1Maximum 8Range 7Interquartile Range 3Skewness -.092 .287Kurtosis -1.005 .566
BAQ_Mean Mean 3.33 .10195% Confidence Interval for Mean
Lower Bound
3.13
Upper Bound
3.53
5% Trimmed Mean 3.29
69

URN: 6455433
Median 3.33Variance .708Std. Deviation .842Minimum 2Maximum 6Range 4Interquartile Range 1Skewness .527 .287Kurtosis .261 .566
Autonomy_Mean
Mean 4.23 .10195% Confidence Interval for Mean
Lower Bound
4.03
Upper Bound
4.43
5% Trimmed Mean 4.21Median 4.14Variance .708Std. Deviation .841Minimum 2Maximum 6Range 4Interquartile Range 1Skewness .494 .287Kurtosis .401 .566
Appendix F – SPSS Outputs: Internal consistency tests
70

URN: 6455433
ISC dominance sub-domain
Reliability Statistics
Cronbach's Al-
pha
Cronbach's Al-
pha Based on
Standardized
Items N of Items
.794 .795 8
Item-Total Statistics
Scale Mean if
Item Deleted
Scale Variance if
Item Deleted
Corrected Item-
Total Correlation
Squared Multiple
Correlation
Cronbach's Al-
pha if Item De-
leted
Dominant 32.16 116.830 .384 .235 .790
Dominant 31.44 109.149 .537 .406 .765
Dominant 31.30 113.865 .507 .334 .770
Dominant 32.43 112.133 .515 .394 .769
Dominant 33.23 112.295 .537 .322 .765
Dominant 31.33 111.122 .506 .289 .770
Dominant 32.09 107.500 .655 .474 .747
Dominant 33.03 119.275 .381 .285 .789
ISC cold dominance sub-domain
Reliability Statistics
Cronbach's Al-
pha
Cronbach's Al-
pha Based on
Standardized
Items N of Items
.870 .869 8
Item-Total Statistics
71

URN: 6455433
Scale Mean if
Item Deleted
Scale Variance if
Item Deleted
Corrected Item-
Total Correlation
Squared Multiple
Correlation
Cronbach's Al-
pha if Item De-
leted
Cold Dominant 34.29 149.251 .711 .576 .844
Cold Dominant 34.61 165.603 .424 .357 .873
Cold Dominant 33.64 150.320 .672 .578 .848
Cold Dominant 33.49 156.137 .545 .405 .862
Cold Dominant 35.06 146.576 .701 .547 .845
Cold Dominant 34.16 146.453 .740 .587 .841
Cold Dominant 34.36 153.334 .556 .382 .862
Cold Dominant 34.40 149.809 .648 .581 .851
BAQ (self-reported anger)
Reliability Statistics
Cronbach's Al-
pha
Cronbach's Al-
pha Based on
Standardized
Items N of Items
.685 .682 12
Item-Total Statistics
Scale Mean if
Item Deleted
Scale Variance if
Item Deleted
Corrected Item-
Total Correlation
Squared Multiple
Correlation
Cronbach's Al-
pha if Item De-
leted
Physical 35.10 94.700 .396 .395 .654
Physical 34.74 88.571 .526 .519 .630
Physical 34.54 89.991 .466 .566 .640
Anger 35.01 104.420 .153 .179 .690
Anger 35.89 98.103 .390 .576 .657
Anger 35.94 103.504 .251 .523 .676
Verbal 33.29 108.845 .032 .455 .706
Verbal 34.07 95.835 .347 .392 .662
Verbal 35.84 98.917 .367 .337 .660
Hostility 34.73 97.766 .296 .249 .670
Hostility 35.63 95.251 .386 .570 .655
Hostility 34.47 98.253 .246 .629 .679
72

URN: 6455433
BPNSS (Autonomy sub-scale) Internal consistency
Reliability Statistics
Cronbach's Al-
pha
Cronbach's Al-
pha Based on
Standardized
Items N of Items
.661 .666 7
Item-Total Statistics
Scale Mean if
Item Deleted
Scale Variance if
Item Deleted
Corrected Item-
Total Correlation
Squared Multiple
Correlation
Cronbach's Al-
pha if Item De-
leted
Autonomy 26.46 41.585 .439 .257 .604
Autonomy 25.66 50.895 .166 .075 .686
Autonomy 25.43 49.582 .328 .315 .638
Autonomy 27.01 47.116 .366 .232 .627
Autonomy 25.99 43.464 .517 .476 .582
Autonomy 25.59 46.101 .453 .407 .604
Autonomy 26.01 45.840 .361 .279 .629
73

URN: 6455433
Appendix G – SPSS Outputs: Tests of normality
Tests of NormalityKolmogorov-Smirnova Shapiro-Wilk
Statistic df Sig. Statistic df Sig.DOM_mean .070 70 .200* .982 70 .401CD_Mean .085 70 .200* .971 70 .098BAQ_Mean .088 70 .200* .963 70 .035Autonomy_Mean
.127 70 .007 .963 70 .036
*. This is a lower bound of the true significance.a. Lilliefors Significance Correction
DOM_mean
74

URN: 6455433
CD_Mean
75

URN: 6455433
BAQ_Mean
76

URN: 6455433
Autonomy_Mean
77

URN: 6455433
Tests of NormalityKolmogorov-Smirnova Shapiro-Wilk
Statistic df Sig. Statistic df Sig.total number of incid-ents on staff
.346 63 .000 .447 63 .000
a. Lilliefors Significance Correction
total number of incidents on staff
78

URN: 6455433
79

URN: 6455433
Appendix H - SPSS Outputs: Correlation analyses for hypotheses 1-3
Correlations
Correlations
DOM_mean CD_Mean BAQ_MeanAutonomy_Me
anDOM_mean Pearson Correlation 1 .778** .419** -.084
Sig. (2-tailed) .000 .000 .489N 70 70 70 70
CD_Mean Pearson Correlation .778** 1 .162 .035Sig. (2-tailed) .000 .180 .775N 70 70 70 70
BAQ_Mean Pearson Correlation .419** .162 1 -.036Sig. (2-tailed) .000 .180 .766N 70 70 70 70
Autonomy_Mean Pearson Correlation -.084 .035 -.036 1Sig. (2-tailed) .489 .775 .766N 70 70 70 70
**. Correlation is significant at the 0.01 level (2-tailed).
80

URN: 6455433
Nonparametric Correlations
Correlations
DOM_mean CD_Mean
total number of incidents on
staffAutonomy_Me
an BAQ_MeanSpearman's rho DOM_mean Correlation Coefficient 1.000 .773** -.046 -.054 .401**
Sig. (2-tailed) . .000 .718 .659 .001N 70 70 63 70 70
CD_Mean Correlation Coefficient .773** 1.000 -.110 .022 .188Sig. (2-tailed) .000 . .392 .857 .119N 70 70 63 70 70
total number of incidents on staff
Correlation Coefficient -.046 -.110 1.000 -.079 .256*
Sig. (2-tailed) .718 .392 . .537 .043N 63 63 63 63 63
Autonomy_Mean Correlation Coefficient -.054 .022 -.079 1.000 -.017Sig. (2-tailed) .659 .857 .537 . .890N 70 70 63 70 70
BAQ_Mean Correlation Coefficient .401** .188 .256* -.017 1.000Sig. (2-tailed) .001 .119 .043 .890 .N 70 70 63 70 70
**. Correlation is significant at the 0.01 level (2-tailed).
*. Correlation is significant at the 0.05 level (2-tailed)81

URN: 6455433
82

URN: 6455433
Appendix I – SPSS Outputs: Mediation analyses
Hypothesis 4 a
Run MATRIX procedure:
**************** PROCESS Procedure for SPSS Version 3.1 ******************
Written by Andrew F. Hayes, Ph.D. www.afhayes.com Documentation available in Hayes (2018). www.guilford.com/p/hayes3
**************************************************************************Model : 4 Y : BAQ_Mean X : DOM_mean M : Autonomy
SampleSize: 70
**************************************************************************OUTCOME VARIABLE: Autonomy
Model Summary R R-sq MSE F df1 df2 p .0841 .0071 .7130 .4843 1.0000 68.0000 .4888
Model coeff se t p LLCI ULCIconstant 4.4478 .3279 13.5633 .0000 3.7934 5.1021DOM_mean -.0473 .0680 -.6959 .4888 -.1830 .0884
83

URN: 6455433
**************************************************************************OUTCOME VARIABLE: BAQ_Mean
Model Summary R R-sq MSE F df1 df2 p .4186 .1752 .6018 7.1156 2.0000 67.0000 .0016
Model coeff se t p LLCI ULCIconstant 2.2490 .5799 3.8781 .0002 1.0915 3.4066DOM_mean .2356 .0627 3.7583 .0004 .1105 .3607Autonomy -.0009 .1114 -.0085 .9932 -.2233 .2214
************************** TOTAL EFFECT MODEL ****************************OUTCOME VARIABLE: BAQ_Mean
Model Summary R R-sq MSE F df1 df2 p .4186 .1752 .5930 14.4434 1.0000 68.0000 .0003
Model coeff se t p LLCI ULCIconstant 2.2448 .2991 7.5065 .0000 1.6481 2.8416DOM_mean .2356 .0620 3.8005 .0003 .1119 .3593
************** TOTAL, DIRECT, AND INDIRECT EFFECTS OF X ON Y **************
Total effect of X on Y Effect se t p LLCI ULCI
84

URN: 6455433
.2356 .0620 3.8005 .0003 .1119 .3593
Direct effect of X on Y Effect se t p LLCI ULCI .2356 .0627 3.7583 .0004 .1105 .3607
Indirect effect(s) of X on Y: Effect BootSE BootLLCI BootULCIAutonomy .0000 .0095 -.0168 .0242
*********************** ANALYSIS NOTES AND ERRORS ************************
Level of confidence for all confidence intervals in output: 95.0000
Number of bootstrap samples for percentile bootstrap confidence intervals: 10000
NOTE: Variables names longer than eight characters can produce incorrect output. Shorter variable names are recommended.
------ END MATRIX -----
Hypothesis 4b
85

URN: 6455433
Run MATRIX procedure:
**************** PROCESS Procedure for SPSS Version 3.1 ******************
Written by Andrew F. Hayes, Ph.D. www.afhayes.com Documentation available in Hayes (2018). www.guilford.com/p/hayes3
**************************************************************************Model : 4 Y : TAI_S X : DOM_mean M : Autonomy
SampleSize: 63
**************************************************************************OUTCOME VARIABLE: Autonomy
Model Summary R R-sq MSE F df1 df2 p .1128 .0127 .7394 .7855 1.0000 61.0000 .3790
Model coeff se t p LLCI ULCIconstant 4.5258 .3471 13.0400 .0000 3.8318 5.2198DOM_mean -.0633 .0714 -.8863 .3790 -.2060 .0795
**************************************************************************OUTCOME VARIABLE:
86

URN: 6455433
TAI_S
Model Summary R R-sq MSE F df1 df2 p .0909 .0083 155.8063 .2498 2.0000 60.0000 .7798
Model coeff se t p LLCI ULCIconstant 6.7764 9.8049 .6911 .4922 -12.8364 26.3892DOM_mean -.6923 1.0429 -.6638 .5094 -2.7783 1.3938Autonomy .3094 1.8586 .1665 .8683 -3.4083 4.0272
************************** TOTAL EFFECT MODEL ****************************OUTCOME VARIABLE: TAI_S
Model Summary R R-sq MSE F df1 df2 p .0883 .0078 153.3229 .4796 1.0000 61.0000 .4913
Model coeff se t p LLCI ULCIconstant 8.1769 4.9977 1.6361 .1070 -1.8168 18.1705DOM_mean -.7118 1.0279 -.6925 .4913 -2.7673 1.3436
************** TOTAL, DIRECT, AND INDIRECT EFFECTS OF X ON Y **************
Total effect of X on Y Effect se t p LLCI ULCI -.7118 1.0279 -.6925 .4913 -2.7673 1.3436
Direct effect of X on Y87

URN: 6455433
Effect se t p LLCI ULCI -.6923 1.0429 -.6638 .5094 -2.7783 1.3938
Indirect effect(s) of X on Y: Effect BootSE BootLLCI BootULCIAutonomy -.0196 .1550 -.3159 .3523
*********************** ANALYSIS NOTES AND ERRORS ************************
Level of confidence for all confidence intervals in output: 95.0000
Number of bootstrap samples for percentile bootstrap confidence intervals: 10000
NOTE: Variables names longer than eight characters can produce incorrect output. Shorter variable names are recommended.
------ END MATRIX -----
Hypothesis 4c
88

URN: 6455433
Run MATRIX procedure:
**************** PROCESS Procedure for SPSS Version 3.1 ******************
Written by Andrew F. Hayes, Ph.D. www.afhayes.com Documentation available in Hayes (2018). www.guilford.com/p/hayes3
**************************************************************************Model : 4 Y : BAQ_Mean X : CD_Mean M : Autonomy
SampleSize: 70
**************************************************************************OUTCOME VARIABLE: Autonomy
Model Summary R R-sq MSE F df1 df2 p .0349 .0012 .7172 .0827 1.0000 68.0000 .7745
Model coeff se t p LLCI ULCIconstant 4.1484 .3031 13.6877 .0000 3.5437 4.7532CD_Mean .0168 .0584 .2876 .7745 -.0997 .1333
**************************************************************************
89

URN: 6455433
OUTCOME VARIABLE: BAQ_Mean
Model Summary R R-sq MSE F df1 df2 p .1673 .0280 .7092 .9644 2.0000 67.0000 .3865
Model coeff se t p LLCI ULCIconstant 3.1178 .5840 5.3384 .0000 1.9521 4.2836CD_Mean .0788 .0581 1.3560 .1797 -.0372 .1947Autonomy -.0419 .1206 -.3471 .7296 -.2826 .1988
************************** TOTAL EFFECT MODEL ****************************OUTCOME VARIABLE: BAQ_Mean
Model Summary R R-sq MSE F df1 df2 p .1620 .0262 .7000 1.8319 1.0000 68.0000 .1804
Model coeff se t p LLCI ULCIconstant 2.9442 .2994 9.8325 .0000 2.3467 3.5417CD_Mean .0781 .0577 1.3535 .1804 -.0370 .1932
************** TOTAL, DIRECT, AND INDIRECT EFFECTS OF X ON Y **************
Total effect of X on Y Effect se t p LLCI ULCI .0781 .0577 1.3535 .1804 -.0370 .1932
90

URN: 6455433
Direct effect of X on Y Effect se t p LLCI ULCI .0788 .0581 1.3560 .1797 -.0372 .1947
Indirect effect(s) of X on Y: Effect BootSE BootLLCI BootULCIAutonomy -.0007 .0086 -.0200 .0174
*********************** ANALYSIS NOTES AND ERRORS ************************
Level of confidence for all confidence intervals in output: 95.0000
Number of bootstrap samples for percentile bootstrap confidence intervals: 10000
NOTE: Variables names longer than eight characters can produce incorrect output. Shorter variable names are recommended.
------ END MATRIX -----
91

URN: 6455433
Hypotheses 4d
Run MATRIX procedure:
**************** PROCESS Procedure for SPSS Version 3.1 ******************
Written by Andrew F. Hayes, Ph.D. www.afhayes.com Documentation available in Hayes (2018). www.guilford.com/p/hayes3
**************************************************************************Model : 4 Y : TAI_S X : CD_Mean M : Autonomy
SampleSize: 63
**************************************************************************OUTCOME VARIABLE: Autonomy
Model Summary R R-sq MSE F df1 df2 p .0375 .0014 .7479 .0857 1.0000 61.0000 .7707
Model coeff se t p LLCI ULCIconstant 4.1381 .3438 12.0378 .0000 3.4507 4.8255CD_Mean .0189 .0644 .2927 .7707 -.1100 .1477
**************************************************************************92

URN: 6455433
OUTCOME VARIABLE: TAI_S
Model Summary R R-sq MSE F df1 df2 p .0827 .0068 156.0297 .2065 2.0000 60.0000 .8140
Model coeff se t p LLCI ULCIconstant 5.6196 9.1225 .6160 .5402 -12.6281 23.8674CD_Mean -.5540 .9311 -.5950 .5541 -2.4164 1.3084Autonomy .4898 1.8493 .2648 .7921 -3.2095 4.1890
************************** TOTAL EFFECT MODEL ****************************OUTCOME VARIABLE: TAI_S
Model Summary R R-sq MSE F df1 df2 p .0753 .0057 153.6513 .3482 1.0000 61.0000 .5573
Model coeff se t p LLCI ULCIconstant 7.6463 4.9272 1.5518 .1259 -2.2064 17.4990CD_Mean -.5448 .9233 -.5900 .5573 -2.3910 1.3015
************** TOTAL, DIRECT, AND INDIRECT EFFECTS OF X ON Y **************
Total effect of X on Y Effect se t p LLCI ULCI -.5448 .9233 -.5900 .5573 -2.3910 1.3015
93

URN: 6455433
Direct effect of X on Y Effect se t p LLCI ULCI -.5540 .9311 -.5950 .5541 -2.4164 1.3084
Indirect effect(s) of X on Y: Effect BootSE BootLLCI BootULCIAutonomy .0092 .1200 -.1866 .3241
*********************** ANALYSIS NOTES AND ERRORS ************************
Level of confidence for all confidence intervals in output: 95.0000
Number of bootstrap samples for percentile bootstrap confidence intervals: 10000
NOTE: Variables names longer than eight characters can produce incorrect output. Shorter variable names are recommended.
------ END MATRIX -----
94

URN: 6455433
Part 2: Research – MRP Literature Review
Abstract
Background: Coercive practices have become integral to managing
violent/aggressive behaviour in secure forensic settings. In more recent years, the use
of coercive practice has come under scrutiny due to its paradoxical effects on
provoking further service user aggression and violence. In addition, coercive
practices can also be counter-therapeutic to the staff-service user relationship,
particularly the way in which service users relate and react to such practices used by
staff (also known as service users’ interpersonal style).
Aims: To investigate the extent to which coercive practices and service user
interpersonal style predict service user aggression in secure settings.
Methods: A literature review was conducted using the following databases:
CINAHL; Psychinfo; Psyarticles; P&BSC; Medline. Peer-reviewed journals were
reviewed. Search terms included: “forensic”, “interpersonal”, “coercion”, and
“aggression” were used.
Results: Nine studies were included in the review. All studies included in this
literature review indicated that either interpersonal style (particularly dominance and
coercion) or coercive measures (such as staff limit-setting) were predictors of service
user violence and aggression. Only one study explicitly focused on interpersonal
style, coercion, and aggression, and this was based in the context of service user
admissions.
Conclusion: There is little research that has explicitly looked at the relationship
between both service users’ interpersonal style and coercive practice as possible
predictors of further aggression/violence. Future research should seek to understand
the way in which service user’s make sense and react to coercive practice,
95

URN: 6455433
particularly in relation to their interpersonal styles. This research may help staff to
find alternative ways in engaging with service users that reduces the use of coercive
practice whilst simultaneously promoting service users’ recovery and maintaining a
safe environment.
Key words: Forensic, interpersonal style, coercive measures, aggression.
Word count: 7822
1.0 Introduction
Despite a shortage of beds, service users admitted into acute mental health wards in
England have a longer length of stay compared to several other developed countries
(Care Quality Commission (CQC), 2017). According to the Care Quality
Commission (2017), there was an extreme variation in the length of stay on NHS
high dependency rehabilitation wards, ranging from 45 to 1,744 days in 2015/16,
with an average length of stay of 341 days. This growing attention is due to
increasing pressure for containment of costs within psychiatric care and an ongoing
focus on psychiatric care being delivered in the least restrictive settings possible
(Compton et al., 2006). The Centre for Mental Health UK (2011) noted forensic
beds are more expensive and treat a smaller number of service users compared to
other general psychiatric admission beds. For those residing in high and medium
secure forensic hospitals, concerns have been raised that service users are staying for
too long in too high levels of security (Shaw et al., 2001; Harty et al., 2004).
Extended length of stay in secure care does not only result in high economic burden
on these services (e.g. Vӧllm et al., 2017) but can also have a negative impact on
forensic service users’ quality of life (e.g. Shaw et al., 2001). There have been
several research studies over the past few decades that have investigated possible
96

URN: 6455433
predictors/determinants of longer length of stay in both non-forensic and forensic
settings (e.g. Taylor et al., 1996; Compton et al., 2006; Davoren et al., 2015; Vӧllm
et al., 2016). A major factor found to predict length of stay was the number of
untoward incidents (mainly violence and aggression) that the service user had been
involved in whilst in the institutional settings (e.g. Castro et al., 2002; Mellesdal et
al., 2003; Tulloch et al., 2008; Vӧllm et al., 2016).
1.1 Violence, aggression, and coercive practice in forensic settings
A review of 424 international studies found that the prevalence of violent incidents in
forensic settings was significantly higher compared to general inpatient psychiatric
hospitals (Bowers et al., 2011). A recent survey of a large independent secure care
facility found that 2,137 incidents involving 56.4% service users were reported
(Dickens et al., 2013). In terms of high-secure settings, Uppal and McMurran (2009)
reported 3,565 violent incidents over a 16-month period in just under 400 service
users.
Coercive measures have become integral to managing violent/aggressive behaviour
by use of severe containment methods such as manual restraint, rapid
tranquillisation, seclusion, long-term segregation and withholding parole (NICE,
2016). The definition of coercion is typically seen as an ‘action or practice of
persuading someone to do something by using force or threats’ (Oxford Dictionaries,
2010). As highlighted in the literature, the term ‘coercive measures’ has multiple
definitions that can lead to confusion and difficulty for those who wish to examine it
(e.g. Jarrett et al., 2008). Although coercive measures are mostly thought of in
context of short-term management of aggression and violence (through seclusion and
97

URN: 6455433
restraint), there are also more long-term coercive measures used (Hui et al., 2013).
As outlined by Szmukler and Appelbaum’s (2008) ‘sliding scale’, coercive measures
may take on various forms in forensic psychiatric settings including: persuasion (e.g.
attempts to influence service users actions by emotional reasoning); interpersonal
leverage (e.g. where the service user-professional relationship is used to put pressure
on the service user, such as pointing out disappointment in service user’s behaviour);
inducement (e.g. the use of positive rewards if action suggested by clinician is
accepted by the service user); threats (e.g. to lose particular benefits); compulsory
treatment (e.g. locked doors, bars on windows, choices taken away and treatment
administered against service users’ wishes).
In more recent years, the use of coercive practice has come under scrutiny, particu-
larly with more emphasis having been placed on personal autonomy and human
rights (Hui et al., 2013). Much of this current pressure has come about due to investi-
gations and scandals which have been widely reported (e.g. Blom-Cooper, 1992; Fal-
lon, 1999; Bubb, 2014). Coercive practice has even been found to have paradoxical
effects on provoking further aggression and violence (Daffern et al., 2003; Goren,
Singh, & Best, 1993). For example, Goren (1993) considered how high levels of se-
clusion and restraint used in child psychiatric hospitals to manage aggression and
non-compliance may have led to a pattern of behaviour characterised by an aggres-
sion-coercion cycle exhibited by both staff and service users. Several national and in-
ternational documents have called for review and reduction in restrictive practices in
general and secure-care psychiatric settings (e.g. American Psychiatric Association,
American Psychiatric Nurses Association & National Association of Psychiatric
Health Systems, 2003; Queensland Government, 2008; MIND, 2013; Department of
98

URN: 6455433
Health, 2014; NICE, 2015). Reducing coercive practice in forensic settings to sup-
port service user’s personal recovery may, however, be more problematic than in
general psychiatric settings. As highlighted in the Centre for Mental Health’s brief-
ing paper on “making recovery a reality in forensic settings”, there seems to be a
more complex balance between providing service users with autonomy and choice
over their own care when the reduction of service users’ risk towards themselves and
others is imperative whilst residing in secure-care services (Drennan and
Wooldridge, 2014). It is therefore recommended that staff and service users need to
work together to develop an organisational culture in which there is a balance
between safety and recovery (Drennan and Wooldridge, 2014).
1.2 Research on coercion in forensic settings
There is some empirical literature on coercive practice in forensic settings, but more
often, research is based in general psychiatric settings. In a systematic review
conducted by Hui and colleagues (2013), ten out of the fifteen studies included
conducted retrospective analyses of forensic hospital records to examine the use of
coercive measures in relation to various service user demographic indicators (such as
age, gender, and ethnicity), and clinical indicators (such as diagnosis and length of
admission). Findings suggested that younger service users tended to be secluded over
older service users (e.g. Ahmed & Lepnurm, 2001; Beck et al., 2008). In addition,
service users were likely to be secluded or restrained in their first two months of
admission and that after this period the use of such coercive measures were likely to
reduce (Beck et al., 2008). Findings related to gender, ethnicity and service user
diagnosis were equivocal in the review’s included studies. A smaller number of
qualitative studies included in the review conducted semi-structured interviews with
99

URN: 6455433
staff and/or service users to explore attitudes, perceptions, and experiences of
coercive measures (e.g. Keski-Valkama et al. 2010; Sequiera & Halstead, 2004). In
one study, nursing staff reported feelings of anger and anxiety, low morale, and
conflict between the use of restraint and seclusion techniques and their role as a
nurse (Sequiera & Halstead, 2004). In another study, forensic service users were
likely to view seclusion negatively and as a form of punishment and suggested that
limitations in staff-service user interactions during seclusion often increased feelings
of anxiety and confusion (e.g. Keski-Valkama et al. 2010).
Some research studies have focused on situational/environmental determinants of
aggression in secure-care settings (e.g. Kelly et al. 2015). Coercive practice has not
been explicitly examined in this body of research but has instead, emerged from the
findings as a determinant of aggressive behaviour. For example, in a cross-sectional
survey of service user assaults against staff in a forensic psychiatric hospital, a
sample of three hundred and forty-eight staff participated in an online survey about
their workplace experiences, psychosocial characteristics and well-being (Kelly et
al., 2015). Ninety nine percent of staff reported experiencing conflict with service
users and eighty percent of staff reported using seclusion, restraint, or unscheduled
medication within the last six months. Frequency of service user assaults were
substantially correlated with the frequency of service user-staff conflict (r = 0=54)
concluding that ‘staff who regularly engage in […] in service user containment
procedures, have the highest likelihood of experiencing service user-on-staff assault’
(Kelly et al., 2015: p 1118).
100

URN: 6455433
1.3 Coercion and interpersonal style
It has been suggested that aggressive behaviour may be a result of a complex
interaction between situational factors and individual factors (Anderson & Bushman,
2002). In psychiatric hospital settings, we may therefore need to consider that it is
not just the coercive practices (i.e. the implementation of hospital rules and
regulations (Alexander and Bowers, 2004)) that predicts rates of aggression, but it is
also how these situational factors interact with individual service user characteristics.
According to Kiesler’s (1987) interpersonal theory, when interacting with others (our
interpersonal behaviour), we are inherently predisposed to establish relationships that
reinforce our sense of self, and this is done through the reactions of others. Every
individual's interactions can be characterized by two main dimensions: affiliation
(hostile to friendly) and control (dominance to submission). Our interactions
complement the interactions of others (i.e. usually matching across the affiliation
dimension but opposing on the control dimension). For example, friendly
interpersonal styles are typically met with friendliness from others whereas dominant
interpersonal styles are typically met with submission from others. At times,
individual characteristics may lead to maladaptive behaviours in our interactions
with others where lower self-esteem may be linked to increased frustration that
manifests as an over reliance in becoming overly dominant and rarely submissive
(BjØrkvik et al., 2009). For example, when staff confiscate certain privileges off
service users who act out aggressively (i.e. ground leave taken away), some service
users may stop the aggressive behaviour (complementarity across the control
dimension) whereas others may react with further aggression (acomplementarity
across the control dimension).
101

URN: 6455433
According to Cookson et al. (2012), service users with dominant and hostile
interpersonal styles are more likely to encounter problems with psychiatric inpatient
treatment. Service users’ attempts to maintain their dominance are more often met by
a dominant response from nursing staff, which in the context of coercive practice, is
an attempt to maintain the integrity of the treatment regime and to ensure safety of
service users and staff (Daffern et al., 2010a). Staff’s attempts to restore order may
be perceived by service users as threatening and exploitative, which thus leads to
preventative actions by service users to restore dominance (Lillie, 2007). Therefore,
in the context of some service user’s interpersonal styles, the use of coercive
practices may have a counter-therapeutic effect through escalating cycles of attempts
to secure dominance by staff and service users (Goren, 1993). This coincides with
previous research in psychiatric hospital settings which has suggested that
hostile/dominant/coercive personality styles, in particular, are strong predictors of
service user aggression and violence (e.g. Morrison, 1992; Dolan & Blackburn,
2006; Harris et al., 2014). This highlights that the implementation of coercive
practice, does not take place in a vacuum, but also concerns the way in which service
users make sense of and react to staffs’ use of such practices.
Previous research has indicated that the formation of a therapeutic relationship
between staff and service users is fraught with difficulties in forensic settings
compared to non-forensic settings (Mason et al., 2008). Furthermore, as highlighted
above, previous research has indicated that forensic settings not only have a
significantly higher prevalence of violent incidents (Bowers et al., 2011) but consists
of a more complex balance between providing both a therapeutic and a safe/secure
environment (e.g. Burrows, 1991; Drennan and Wooldridge, 2014). This echoes the
102

URN: 6455433
works of Goffman (1968), where staff working in institutions find themselves
simultaneously trying to care whist enforcing strict regulations that threaten this
caring process. The complex interaction between individual and situational factors in
predicting aggressive behaviour may be further complicated within a forensic setting
where therapeutic efficacy may well be related to issues of maintaining control of a
population of service users who, more often than not, wish to disrupt a hated system
(Peternelj-Taylor & Johnson, 1995). As such, it may be important to investigate the
current evidence base on how service users residing explicitly in secure forensic
settings make sense of coercive practices used by staff, particularly in context of
service users’ interpersonal styles and in turn, how these factors play a role in the
incidence of violence/aggression.
1.4 Literature survey aims
1.4.1 Research question
What is known from the existing literature about the extent to which service users’
interpersonal style and coercive practices predict incidents of aggression and
violence in secure forensic settings?
1.4.2 Research objectives
A common theme that arose from the current empirical evidence, is the paradoxical
effects of coercion on provoking further service user aggression and violence. As an
alternative to focusing on factors that are associated with the use of coercive practice
(e.g. Hui et al., 2013), this literature review aims to identify empirical evidence on:
1) the extent to which coercive practices predict outcomes of service user aggression
in secure forensic settings;
103

URN: 6455433
2) the extent to which service users’ interpersonal style predicts outcomes of service
user aggression in secure forensic settings;
3) the extent to which both coercive practice and interpersonal style predict service
user aggression in secure forensic settings.
2.0 Methods
2.1 Identifying the relevant studies
Peer reviewed journal papers were identified via the relevant health and social care
databases available at Surrey University through a keyword search using terms
relating to coercive practice, service user interpersonal style and aggressive
behaviour in secure forensic settings. In total, five databases were searched:
CINAHL; Psychinfo; Psycharticles; P & BSC; Medline. These databases were
deemed most appropriate as they specifically included articles related to the subjects
of psychology and healthcare. These database searches were run in 01/11/2017 and
re-rerun on 26/01/19.
Searches for ‘grey literature’ were also conducted via online searches (Google
Scholar, Open Grey) and by liaising with authors of included papers. Searching of
key journals (i.e. Journal of Forensic Psychiatry and Psychology) and examination of
retrieved articles’ reference and citation lists (including relevant literature reviews)
were also undertaken.
2.1.1 Search terms
104

URN: 6455433
To search for studies focusing on service user interpersonal style, coercion (either
perceived coercion or coercive practice), and service user aggression in secure
forensic settings the following search terms were used:
Forensic AND (secure OR inpatient)
AND
Aggress* OR Violen*
AND
Interpersonal
OR
Coerci* OR Seclusion OR restraint OR Restrict* OR Constrain* OR force OR threat
Search fields: Set to default: searches in Abstract, Titles and Key Words. No
restrictions over year of publication.
2.1.2 Rationale for search terms
The main search term ‘forensic’ was used in all searches. As suggested by Hui and
colleagues (2013), although distinctions are made between low, medium, and high
secure services in the UK, there is less of a distinction in other countries. As such,
‘forensic’ (and ‘secure’ or ‘inpatient’) felt most appropriate to use as search terms.
Search terms ‘aggression’ or ‘violence’ were included as they were used
interchangeably in the literature and ‘interpersonal’ was used to cover all
eventualities related to interpersonal style. A related review that looked at coercive
measures within a forensic setting (Hui et al., 2013) only used search terms specific
to short-term coercive measures (e.g. coercion, restraint, seclusion, involuntary
105

URN: 6455433
medication). In this review, it was also important to identify articles that focused on
long-term coercive measures as described by Szmukler and Applebaum’s (2008)
‘sliding scale’ (see section 1.1). It therefore felt appropriate to use more broader
terms which captured coercion in forensic settings. As such, an iterative approach
was adopted whereby keywords of relevant retrieved papers were looked at, and any
new relevant keywords were added to the search terms.
2.2 Study selection
2.2.1 Inclusion and exclusion criteria
Inclusion and exclusion criteria were used to eliminate studies that did not answer the
research area of interest. Rather than adhering to a hierarchy of evidence approach,
based on methodology, empirical studies were included (quantitative and qualitative)
most likely to be relevant to the research area of interest (Aveyard, 2014).
Inclusion criteria:
a. Peer-reviewed empirical studies published in peer reviewed journals
addressing the areas in the key research questions;
b. Empirical studies based in forensic, secure-care settings;
c. Service user sample includes adults (18-65 years old);
d. Empirical studies that focus on either service users’ interpersonal style
and/or coercion (whether that be perceived coercion or coercive
/restrictive practices/measures);
e. Empirical studies that focus on service user violence and aggression
as an outcome measure;
106

URN: 6455433
f. Conference papers addressing the areas in the key research questions
published in peer reviewed journals or as ‘grey literature’ conference
proceedings;
g. Both quantitative and qualitative research studies;
h. English language publications.
Exclusion criteria:
a. Duplications;
b. Studies that are not based in forensic psychiatric settings;
c. Studies concerning children, young people (0-18) and older age (65+);
d. Empirical studies that do not focus on either service users’
interpersonal style or coercion (whether that be perceived coercion or
coercive /restrictive practices/measures);
i. Empirical studies that do not focus on service user violence and
aggression as an outcome measure;
e. Commentary pieces; policy and guidance documents; material
published in ‘trade press’ and magazines; conference abstracts;
f. Papers and reports published in a language other than English.
2.2.2 Study screening process
Titles, abstracts, and key words of the retrieved studies were initially screened. Those
that did not meet the inclusion criteria were excluded. The full text of the remaining
articles were reviewed for eligibility. Those studies that did not meet the inclusion
criteria were excluded. A record was kept reporting the reasons why each study was
excluded (e.g. wrong setting). A PRISMA chart has been used to illustrate this
selection process (see Figure 1).
107

URN: 6455433
2.3 Data extraction
Relevant data was extracted from each of the included studies following a similar
approach to Arksey and O’Malley (2005). By using a ‘data extraction table’ (see
Table 1), the following key information was recorded about each study:
Author(s), year of publication, study location
Setting
Study population
Methods (including study design, data collection, data analysis)
Key findings
2.4 Collating, summarizing and reporting the results
By referring to the data extraction table (see Table 1), an initial list of key findings
from each of the included studies were created. The review’s three objectives (see
section 1.4.2) were used to create a ‘thematic framework’ (Ritchie et al., 2003). This
framework was used to classify and organise data from the included studies into key
categories, each comprising of overarching categories subdivided into related sub-
categories. The findings sections of each of the nine original articles were re-checked
to ensure that extracts of data reported on the findings had not been missed thus
further refining the emergent categories and sub-categories within the thematic
framework. The emerging categories/sub-categories from the included studies were
presented to the research supervisor (with examples from the included studies data)
to assess credibility of the coding process. The supervisor read through the results
section of a selection of studies to cross-check whether the categories I had pulled
108

URN: 6455433
from these papers were aligned with their own identified emerging categories/sub-
categories.
2.5 Quality assessment
The quality of the included studies was assessed using appropriate critical appraisal
tools for both quantitative and qualitative methodologies. Quantitative studies were
assessed using the STROBE’s (Strengthening the Reporting of Observational Studies
in Epidemiology) for cohort studies (Von Elm et al., 2007). This checklist was
deemed the most appropriate checklist for the quantitative studies included in the
review as all were cohort study designs. Qualitative studies were assessed using the
critical appraisal skills programme (CASP) qualitative appraisal tool (CASP, 2013).
The checklists were used to assess whether each of the included studies met the
criteria with a rating scale of ‘yes’ (1 point), ‘partly’ (0.5 points), and ‘no’ (0 points).
Each study’s points were added up to give a total quality score which was out twenty
for the quantitative studies (total scores were deducted where quality criteria were
not applicable for the study) and out of eight for the one qualitative study.
3.0 Results
The database, grey literature and previous relevant literature review searches yielded
a total of 573 papers, reducing to 357 after duplicates were removed. 250 articles
were excluded as they did not meet inclusion criteria. A total of 107 full text copies
were obtained and 9 relevant papers were included in the final review (see Figure 1
for the selection process flow diagram).
109

URN: 6455433
Figure 1: PRISMA flow diagram of selection process
110
Titles and abstracts identified through
electronic database search (n = 566)
Screening
Included
Eligibility
Identification
Titles and abstracts identified through other
sources (i.e. grey literature, literature reviews, and
citation and reference lists of relevant articles)
(n = 7)
Duplicates removed(n = 216)
Records screened (titles and abstracts)(n = 357) Records excluded
(n = 250)
Full-text articles retrieved and assessed for eligibility
(n = 107)
Full-text articles excluded, with reasons
(n = 98)
Wrong setting (non-forensic): n=40
Did not look at interpersonal style or coercive/restrictive practice n= 31
Wrong outcome measures (did not look at aggression/violence) n=27
Studies included (n =9)

URN: 6455433
3.1 Description of included studies
Study focus: All nine studies investigated how interpersonal style and/or coercive practices
may have influenced service users’ aggressive behaviour in secure care. Four of these studies
elicited data surrounding the impact of coercive practices on service user aggression (e.g.
limit setting by staff and service user’s responses to these limitations/measures of control)
(Harris & Varney, 1986; Bjøkly, 1999; Meehan et al., 2006; Winje et al., 2018). Four studies
investigated the relationship between service user interpersonal style and aggression (Daffern
et al., 2008; Doyle et al., 2006; Smith et al., 2013; Vernham et al., 2016). The remaining
study looked at the impact of both interpersonal style and perceived coercion on aggression
and self-harm (Daffern et al., 2010b).
Study design/methods: All studies drew on a quantitative methodology, except for Meehan
and colleagues (2006) who used a qualitative methodology. Seven out of the eight
quantitative studies used a range of standardised outcome measures assessing service users’
aggressive behaviour (e.g. Report Form for Aggressive Episodes (REFA); Aggressive
Incident Motivation Evaluation Scale (AIMES); Staff Observation Aggression Scale – Revised
(SOAS-R)) (Bjøkly, 1999; Doyle et al.,2006; Winje et al., 2018) symptom/diagnostic
characteristics (e.g. PCL-R; BPRS) (Daffern et al., 2010b; Smith et al., 2013; Doyle et al.,
2006); personality traits (e.g. TCI; PCIR) (Smith et al., 2013); interpersonal styles (e.g. IMI;
CIRCLE) (Daffern et al., 2008; Daffern et al., 2010b; Doyle et al., 2006; Vernham et al.,
2016); and perceived staff coercion (MAES) (Daffern et al., 2010b). Four out of the eight
quantitative studies retrospectively reviewed incidents of violent and aggressive behaviour in
a past time period (Daffern et al., 2008; Daffern et al., 2010b; Vernham et al., 2016; Winje et
al., 2018). Four studies adopted a prospective approach where incidents were recorded at
baseline and at specific incidents in future time points (Harris & Varney, 1986; Bjøkly, 1999;
111

URN: 6455433
Doyle et al., 2006; Smith et al., 2013). In three out of the eight quantitative studies, outcome
measures were completed by staff and service users (Bjøkly, 1999; Daffern et al., 2010b;
Doyle et al., 2006), in four quantitative studies only staff completed outcome measures on
service users (Daffern et al., 2008; Daffern et al., 2010b; Vernham et al., 2016; Winje et al.,
2018), and in one study, only service users completed outcome measures (Smith et al., 2013).
In one quantitative study, no outcome measures were used but service users and where
possible, staff and witnesses were interviewed about the time, cause and actual events that
had transpired from an assaultive incident (Harris & Varney, 1986). Meehan and colleague’s
(2006) qualitative studies conducted focus groups with service users.
Study settings: In terms of study setting, four out of the nine studies were conducted in a
high-secure forensic hospital (Harris & Varney, 1986; Daffern et al., 2010b; Meehan et al.,
2006; Vernham et al., 2016), two in medium-secure units (Daffern et al., 2008; Doyle et al.,
2006), and three studies conducted outside of the UK were set in ‘specialised secure units’
(Bjøkly, 1999; Smith et al., 2013; Winje et al., 2018). In addition, two out of the nine studies
conducted research in a specialist personality disorder unit (Daffern et al., 2010b; Daffern et
al., 2008).
Study participants: With regards to participant demographics, sample sizes ranged from
nineteen participants to two hundred and fifty-three participants. Five studies samples were
predominantly male (Bjøkly, 1999; Meehan et al., 2006; Doyle et al., 2006; Smith et al.,
2013; Winje et al., 2018) and the sample in the remaining four studies were solely male
(Harris & Varney, 1986; Daffern et al., 2010b; Daffern et al., 2008; Vernham et al., 2016).
The age range of participants in most studies were between 18-65 years old with the mean
age falling between 30-43.45 years old. For those studies that included details on ethnicity,
112

URN: 6455433
most participants were White Caucasian (Doyle et al., 2005; Daffern et al., 2010b; Daffern et
al., 2008; Bjøkly, 1999; Smith et al., 2013; Vernham et al., 2016). Most participants in the
samples of six studies had a diagnosis of schizophrenia or other psychotic-related disorder
(e.g. psychosis) (Harris & Varney, 1986; Meehan et al., 2006; Doyle et al., 2006; Bjøkly,
1999; Vernham et al., 2016; Winje et al., 2018) whereas two studies’ samples only included
those with a diagnosis of personality disorder (due to the studies being set in Personality
Disorder units) (Daffern et al., 2010b; Daffern et al., 2008). See Table 1 for the review’s
extraction table.
113

URN: 6455433
Table 1: Data extraction table
Author/Date/ Country/ Aims
Setting/ study populations
Methods (including relevant outcome measures) Key findings
Study 1
Bjøkly, S. (1999)
Norway
To identify, classify and measure the occurrence of aggressive behaviour, as well as the frequency of events preceding such behaviour.
Setting: Special secure unit, Norway.
Participants: 19 service users who were treated during a 10-year period in the unit.
White, Native Norwegian; 6 females and 13 males; mean age of 30.5 years old; 13 paranoid schizophrenia, 4 paranoid PD, 3 substance abuse, 1 antisocial PD.
Average Length of stay in secure unit during 10-year study was 49.5 months; 6 were still in secure unit after 10-year period.
Design: 10-year prospective study using hospital records (cohort study)
Data collection: Incidents of aggressive behaviour recorded on the Report Form for Aggressive Episodes (REFA) by nursing staff.
After service users had calmed, they were asked for their motives for the aggressive behaviour.
A routine injury form (rating severity) was also completed as close in time to the incident.
Outcome measures/instruments:
The REFA- rating scales - measures aggressive behaviour towards other persons (Bjorkly, 1996). A list of 30 situations/interactions, grouped in seven main categories, to help determine the situations/interactions that precipitated the aggressive episode. The seven main categories are: Physical contact; Limit-setting; Problems of communication; Changes/readjustments; Persons; High risk contact; and Drugs/stimulants.
Data analysis: Descriptive statistics were used to report the data. No specific details on how this was done.
Rates of aggression: During ten-year study period, a total of 2021 aggressive episodes occurred (Mean=106 per service user, Range= 0–694, SD=179) (See Table 1). Twenty-three per cent of the aggressive episodes were physical assaults, 25% were physical threats and around half were verbal.
Precipitants of aggression: Sixty-four per cent of aggressive incidents were precipitated by situations that involved limit-setting. A relatively higher proportion of physical threats (73%) than verbal threats (63%) and physical assaults (58%) had limit-settings as precipitant of aggression. The relative proportion of physical contact that resulted in physical assaults (7%) was higher than in verbal threats (3%) and physical threats (2%).
Victims of aggression: Nursing staff were the main target of service user aggression. There were 229 incidents of service user-to-service user aggression out of a total of 2021 episodes (11%).
114

URN: 6455433
Author/Date/ Country/ Aims
Setting/ study populations
Methods (including relevant outcome measures) Key findings
Study 2Daffern et al. (2008)
UK
To examine the impact of interpersonal style and psychopathy on treatment non-completion and aggressive behaviour.
Setting: Personality Disorder Unit (PDU), a 12-bed service for male service users with personality disorder. Participants: Service users ranged in age from 17 to 41 years old (M=26.82, SD = 6.68) and most were described as Caucasian (49; 96.1%). Their length of stay varied between 30 and 1515 days (M=411.27, SD = 326.15).
Design: Retrospective study using hospital records (cohort study)
Data collection: An electronic database of incident forms was reviewed in September 2006 to determine whether participants had been aggressive during their stay. Incidents categorised as either physical, verbal, or damage to property.
Outcome measures/instruments completed by staff:Psychopathy Checklist – Revised (PCL-R; Hare, 1991)-Two factor scores: Interpersonal and affective characteristics.
International Personality Disorder Examination (IPDE; Loranger et al., 1994); The Impact Message Inventory (IMI, Kiesler, 1987) The IMI Items are grouped into one of 15 interpersonal style scales (six items per scale); a total scale score is the sum of the six items. This was completed by staff.
Data Analysis: Continuous data compared with independent t-tests using an initial significance level of p<0.1. Logistic regression used to check for possible confounding and effect modification.
Aggressive incidents: Twenty-nine (56.9%) service users were aggressive during their stay on the PDU and twenty-one were not. For those who were aggressive, the mean number of incidents was 3.66 (SD 2.57). Individuals ranged from one to nine aggressive incidents overall.
PCL-R- Total score ranged from 6 to 30 (M=18.09, SD = 5.93). The PCL-R Factor 1 score ranged from 1 to 17 (M=5.74, SD = 3.03). The PCL-R Factor 2 score ranged from 2 to 20 (M=10.80, SD = 3.71).
The relationship between psychopathy and interpersonal style and aggression: Service users who were aggressive during the time period scored higher on the Competitive and Dominant sub-scales of the IMI (0.48, p=0.055 and 0.47, p=0.08, respectively). However, PCL-R total scores showed no association between aggressive and non-aggressive service users.
Study 3 Setting: Rampton high- Design: Retrospective study (cohort study). Perceived coercion: The mean MPCS score in the current sample
115

URN: 6455433
Author/Date/ Country/ Aims
Setting/ study populations
Methods (including relevant outcome measures) Key findings
Daffern et al. (2010b)
UK
To explore the impact of interpersonal style and perceptions of staff coercion on aggression and self-harm.
secure hospital; PD service.
Participants: 39 residents (DSPD n =15, PD n = 24) consented to participate in the study.
Mean age 37.95 years. Predominant ethnic group was White-British (n =32). Remaining seven service users were a mixture of White-Other (n = 3), Mixed-White and Black African (n =1), Mixed-White and Asian (n= 1), and Caribbean (n=1).
Data collection: Service users participated in a semi-structured interview using the MacArthur Admission Experience Survey: Short Form 1 (MAES: SF; Gardner et al., 1993).
Two independent members of staff familiar with the service user then completed CIRCLE ratings.
A register of incident forms on an electronic database was reviewed six months after initial interview. Incidents were coded by a research assistant.
Outcome measures: The chart of interpersonal reactions in closed living environments (CIRCLE; Blackburn & Renwick, 1996) – determined service users’ interpersonal style. The MacArthur Admission Experience Survey: Short Form 1 (MAES: SF; Gardner et al., 1993)- an interview that focuses on service users’ perceptions of coercion during hospital admission.
Data Analysis: The hypotheses addressed using descriptive statistics and tests of association (i.e. multiple regression, nonparametric statistics were used wherever continuous MPCS and incident data were included in the analyses).
was 3.03 (SD = 1.87; median =3.00; minimum =0; maximum= 5). Most service users felt they had little influence (n = 27 or 69.2%), control (n= 24 or 61.5%), choice (n=19 or 48.7%) or freedom (n= 25 or 64.1%) over their admission.
What is the relationship between interpersonal style, perceived coercion and subsequent aggression and self-harm?
96 incidents of aggression and 31 incidents of self-harm were recorded. Most aggressive incidents were categorised as verbal aggression (n =70, 72.92%), however, there were several physically aggressive incidents directed at others (n =23, 23.96%). Staff were predominantly the victims of aggressive acts (68.75% of aggressive incidents).
There was a correlation between a coercive interpersonal style and aggression approached statistical significance (p=0.002).
With regards to the overall regression model, coercive interpersonal style made the only statistically significant contribution to the prediction of self-harm and aggression (ß=0.63, F=22.79*). Perceived coercion did not (ß=0.15, F=0.76).
116

URN: 6455433
Author/Date/ Country/ Aims
Setting/ study populations
Methods (including relevant outcome measures) Key findings
Study 4Doyle et al. (2006)
UK
To assess the predictive validity of brief assessment scales with forensic service users to test the hypotheses that anger regulation problems, interpersonal style, and disturbed mental state would be linked to increased violence risk in a forensic hospital during a hospital stay.
Setting: Three adult forensic mental health medium secure units.
Participants: 94 mentally disordered service users. Sample predominately male (91.5%, n = 86). Mean age of the sample was 38 years (SD=9.03 years; range= 21 to 63 years). 83% of the sample were white Caucasian, 16% (n = 15). The majority (90.4%, n =85) had a psychotic-related disorder. Four (4.3%) had a primary diagnosis of personality disorder. Had an index offence of homicide, 31.9% (n = 30) index offence of wounding or grievous bodily harm, and 10.6% (n = 10) had an index offence of a sexual nature.
Design: Prospective study using hospital records (cohort study)
Data collection: Baseline assessments were conducted with participants and their key workers interviewed. Subsequent institutional violence was recorded weekly up to 12 weeks post baseline.
Outcome measures: The Ward Anger Rating Scale (WARS) (Novaco & Renwick, 1998) rating verbal and physical behaviours relating to anger and aggression. And then rating the behaviours’ affective–behavioural attributes (completed by staff).The Novaco Anger Scale (NAS) (Novaco, 2003) - measures cognitive, arousal, and behavioural correlates of anger (completed by service user); Chart of Interpersonal Reactions in Closed Living Environments (CIRCLE) (Blackburn & Renwick, 1996)- assesses interpersonal styles based on ward observations.
Data analysis: Mean scores of the scales were compared to determine whether the violent group scored higher; Mann–Whitney u statistics used to test the significance of the differences; Spearman’s r coefficient used to compare associations between different scales, and between scales and frequency of violence.
Prevalence of violence: Only 5.3% (n = 5) of the sample were physically aggressive in the 12 weeks following baseline assessment, committing a total of 10 acts of physical violence.
The self-report NAS and subscales were only predictive of physical violence (r=.82*, p<0.05).
WARS scales, rated based on behaviour in the preceding week, had relatively high predictive validity for physical violence (r=.79*, p<0.05) and physical and verbal threats of violence (r=.86***, p<0.001).
Interpersonal style and violence: The CIRCLE scale mean scores revealed that violent participants were more likely to have a dominant (r= .69**, p<0.01), coercive (r=.83***, p<0.001), and hostile interpersonal style (r=.71**, p<0.01).
117

URN: 6455433
Author/Date/ Country/ Aims
Setting/ study populations
Methods (including relevant outcome measures) Key findings
Study 5Harris & Varney (1986)
USA
To examine some of the temporal characteristics of physically assaultive behaviour over an extended period in a maximum-security psychiatric unit.
Setting: Maximum security psychiatric unit.
Participants: Forensic service users.
Over a five-year period of the study, only 45 out of 980 service users committed more than 4 assaults over the five-year period. Characteristics of assaulters were compared to 44 non-assaulters.
Characteristics of reported assaulters: All male; mean age 32.07 years old; 53% diagnosed as psychotic.
Design: Prospective study using hospital records (cohort study)
Data collection: Researchers collected data on assaults that occurred in the maximum-security unit between January 1975 to December 1984.
Incidents were classed as assaults if they involved service user- initiating intentional physical contact of a forceful nature.
Researchers examined ward reports of significant incidents daily. Service users, staff and witnesses interviewed about the time, cause and actual events that had transpired from an assaultive incident.
Outcome measures: Number of assaultive incidents between 1975-1984 taken from hospital records.
Analysis: Assaultive behaviour was analysed using descriptive statistics including types of assault (from actual to attempted assault on either staff or service user victims) and other assaultive characteristics (e.g. location of assault; reasons for assault; and details on the assaulters in comparison to an equal sample of non-assaulters).
Prevalence of assaultive behaviour: Attempted assaults on staff was the highest throughout the 10 years.
Key findings from the more detailed 5-year data set on assaults: The vast number of assaults in the ward occurred in the ward corridors (59%) whereas fewer occurred in the service users’ room (13%) (possibly because staff were discouraged from entering upset service users’ rooms).
Reasons for assaults: three categories which were: No reason, Staff/program reasons (e.g. “ordered to do something”, “staff refused a request”, “patient upset by rules”, “staff provocation”, and “other”), and service user reasons (“teased by another patient”, “crowded”, “voices or delusional orders”, “reaction to homosexual advances”, and “building tension”).
Service users were most likely to attribute the assaultive behaviour with being teased or bugged by other service users (20.5%), being provoked by staff (12%), that there was no reason (15.4%) or that they gave no reason/no comment (23.8%). Ward staff were most likely to attribute assaultive behaviour to: No reason (24.6%), unknown reasons (58.6%) followed by the fact that service users had been ordered to do something (16.8%).
Lowest agreement on reasons for assaults were most apparent in which staff were the victims (p<0.001).
118

URN: 6455433
Author/Date/ Country/ Aims
Setting/ study populations
Methods (including relevant outcome measures) Key findings
Study 6Meehan et al. (2006)
Australia
To elicit service user perceptions of 1) the factors leading to aggressive behaviour; and 2) strategies to reduce the risk of such behaviour.
Setting: High Secure Forensic Unit (HSFU) situated on the campus of a large tertiary mental health facility.
Participants: 22 male and 5 female clients. Eighty-five per cent had a diagnosis of schizophrenia and 73% were found not guilty of their crime due to insanity.
Those service users who had spent less than 3 months in either unit and those who were experiencing an exacerbation of their illness at the time of the study were excluded.
Design: Qualitative research
Data collection: Focus groups were conducted with to elicit perceptions of (1) factors that lead to aggressive behaviour; and (2) strategies that can reduce the risk of such behaviour.
Five discussion groups (ranging from 35 to 75 min) with between four and seven participants were conducted.
Data analysis: Content analysis (Morse & Field 1996) was used to guide analysis of the transcripts.
Environment- The lack of personal space was raised frequently and unfavourably. The impact of living in a confined area for long periods of time could lead to aggressive behaviour.
Staff interactions- the way staff interacted with service users was a major source of dissatisfaction. Staff were perceived to adopt superior attitudes and controlling behaviours to enforce a strict sense of authority rather than to care for service users.
Ward procedures -Staff were portrayed as ignoring frequent requests for assistance as ‘you’ve got to beg these people 26 [swear word] times before you get anything’. The inflexible and strict way in which staff enforced ward ‘rules’ was also perceived to cause aggressive behaviour. Frustration was expressed by service users when staff appeared to enforce rules and withdraw service users’ privileges for no real reason.
119

URN: 6455433
Author/Date/ Country/ Aims
Setting/ study populations
Methods (including relevant outcome measures) Key findings
Study 7Smith, Edens & McDermott (2013)
USA
To examine the psychopathic personality inventory subscales’ (fearless dominance (FD) and self-centred impulsivity (SCI) prospective relationship with predatory, impulsive and psychosis-motivated aggression in an inpatient forensic psychiatric facility.
Setting: Forensic hospital
Participants: 200 forensic service users consisting of: 171 men and 29 women; 65% White, 20.5% Black, 7.5 % Hispanic, 7% other; mean age of 43.45 years old (SD-9.83); 67.5% had a diagnosis of schizophrenia spectrum disorder and 26.5% had diagnosis of Antisocial Personality disorder.
Design: Prospective follow-up study with a review of hospital records (cohort study).
Data Collection: Service users voluntarily enrolled in the study. They completed various outcome measures (see below). Aggressive incidents were tracked on each participant prospectively for an average of 4.39 years (SD- 0.99) after initial enrolment. Reports were completed by nurses following an aggressive incident. Researchers screened reports and categorised the aggressive behaviour to either: predatory, impulsive, psychotic, and unclear.
Outcome measures used:
The Psychopathic Personality Inventory Revised (PPIR; Lilienfeld & Widows, 2005) and Psychopathy Checklist-Revised (PCLR; Hare, 2003) were used to measure aspects of the participants’ personality that were thought to be linked to aggressive behaviour.
Data analysis: Bivariate relationships examined between criterion measures and FD and SCI, as well as for the PPI-R total score for comparative purposes. Hierarchical logistical regression tests used to examine moderator effects between sub-scales of the PPI-R and the PCL-R.
Incidents of aggression: 36.5% of participants (n = 73) engaged in at least one documented incident of physical aggression during the study’s prospective follow-up period. Only 9.5% of the total sample committed at least one predatory act of aggression, 24.5% committed at least one impulsive aggressive act, and 9% acted aggressively at least once due to psychotic symptoms.
Key findings: Fearless dominance was marginally related to predatory aggression, AUC = .60, SE = .08, p = .07 (one-tailed), 95% CI [.45, .75] but unrelated to impulsive aggression, psychotic aggression and any aggression (AUCs ranging from .42 to .50, SEs from .04 to .07, all p values = ns).
Study 8 Setting: Male forensic inpatient unit in a high-
Design: Retrospective quasi-experimental and Aggressive incidents: Verbal (n=53) and physical aggression (n=41) were the most commonly reported incidents within 12
120

URN: 6455433
Author/Date/ Country/ Aims
Setting/ study populations
Methods (including relevant outcome measures) Key findings
Vernham et al., (2016)
UK
To investigate the predictive validity of the Chart of Interpersonal Reactions in Closed Living Environments (CIRCLE) for incidents of verbal and physical aggression, and self-harm recorded from 204 high-secure forensic service users.
secure hospital.
Participants: 262 male service users with CIRCLE ratings (58 were excluded because they only had one rating completed). 204 male service users therefore included in the final sample.
Mean age 41.53 years (SD=10.03). Majority were White British (60.8%), and most had an index offence of homicide (62.7% or sexual offence 13.2%). Most prevalent diagnoses were paranoid schizophrenia or delusional disorder (48.0%) and personality disorder (antisocial and borderline 28.5%). Shortest length of stay (below 53.26 months); and longest (above 53.26months).
correlational study design. (cohort study)Procedure: Sample identified from the Centralised Groupwork Service (CGS) based at UK high secure hospital. IR1 used to identify incidents of verbal and physical aggression and self-harm for the study sample between 2004 and 2009. Details collated: date and location, incident category.
Measures: CIRCLE (the chart of interpersonal interactions) (Blackburn and Glasgow, 2006). Data analysis: Descriptive statistics used to collate info on demographics, clinical diagnosis and forensic characteristics. Means comparisons between service users with and without reported incidents of verbal aggression, physical aggression, and self-harm were conducted for dominant, hostile, and coercive scales of the CIRCLE, as directed by the hypotheses. Correlations were conducted between the CIRCLE total scores on the dominant, hostile, and coercive scales and the total frequency of incidents. All statistical analyses were conducted on incident data collected at 12, 24, and 48 months to investigate whether the predictive validity of the CIRCLE scales changed over time.
months.
Significant positive associations between the dominance and coercion scores and the frequency of verbal aggression (DOM: r=.234, p<.001; COER: r= .289, p<.001), and physical aggression (DOM: r=.192, p=.003; COER: r= .245, p<.001). No association found between aggression and violence with hostility.
All associations were consistent at 24 months, whereas at 48 months a further significant association was found between hostility scores and the frequency of verbal aggression (p=.050) and physical aggression (p=.034).
121

URN: 6455433
Author/Date/ Country/ Aims
Setting/ study populations
Methods (including relevant outcome measures) Key findings
Study 9Winje et al. (2018)
Norway
This study investigates staff members’ evaluation of motivation for aggressive incidents, and how such evaluations are influenced by staff restrictions and aggression severity.
Setting: Secure psychiatric unit. One high and one medium security ward.
Participants: Convenience sample used. 108 service users were admitted in the two wards. A total of 67 service users were included in the study.
57 were male (85.1%). Mean age of service users at the first registered aggressive incident was 32 years (SD = 9.63, range 15–62). Mean length of stay for service users was 22.42 months (SD = 3.29, range 0–120). Most common diagnosis was schizophrenia (59.7%).
Design: A cross sectional study.
Procedure: As soon as aggressive incident occurred, one staff member involved in or witnessing the incident was asked to fill out a report form. This data was collected over the period 2006–2015 of all incident reports with information about aggression motivation.
Measures: The Aggressive Incident Motivation Evaluation Scale (AIMES) (Urheim et al., 2014) - assessed motives and mental/emotional states associated with each motivational dimension.The Staff Observation Aggression Scale – Revised (SOAS-R) (Nijman et al., 1999; Palmstierna & Wistedt, 1987) – used to collect information about provocation.The Visual Analog Scale (VAS) - used to assess staff members’ rating of aggression severity (Nijman et al., 1999).Data Analysis: Report forms were registered as individual episodes (according to Participant study ID). Descriptive statistics and internal consistency reliability (Cronbach’s α) tests ran. A confirmatory factor analysis (CFA) with corrected standard errors was specified to confirm the three-factor structure of the AIMES. Multilevel modelling with random intercepts and cross-level interaction used to predict outcome variables.
Key findings: On average service users were involved in 39 (SD = 58) aggressive incidents, with a range from 1 to 292. Approximately 40% of service users had ten or fewer aggressive incidents. In total, 1900 incidents were reported with provocation scored as ‘no observable provocation’ (53.2%) or ‘staff placing restriction on service users’ behaviour’ (46.8%) in the SOAS-R.
Mean rating of aggression motivation- Irritable motivation (47.1% of incidents) instrumental motivation (39.9% of incidents) and defensive motivation (7.5% of incidents).
Staff members placing restrictions on service users’ behaviour was associated with higher levels of irritable (ß=.45, p<.001) and instrumental motivation (ß=.31, p<0.01). Service users with more incidents provoked by staff restrictions were rated higher on irritable (ß=.72, p<.001) and instrumental motivation (ß=.72, p<.001) across aggressive incidents.
122

URN: 6455433
3.2 Overview of studies key findings
Overview of service user aggression and violence: Incidents reported in all nine
studies included verbal aggression, physical threats, physical assaults/violence. In
three of the studies, more than half of the incidents recorded were verbal aggression
or physical threats (Bjøkly, 1999; Daffern et al., 2010b; Doyle et al., 2006).
Furthermore, in one study sample, 36.5% (n=73) of participants engaged in at least
one incident of physical aggression (Smith et al., 2013). Although Winje and
colleagues (2018) did not report the type of aggressive incident, they did report
whether the aggressive behaviour was motivated by either irritable (47.1% of
incidents), instrumental (39.9% of incidents), or defensive (7.5% of incidents)
means. In four studies, staff (particularly nursing staff) were found to most often be
the victims of service user aggression (Harris & Varney, 1986; Bjøkly, 1999; Daffern
et al., 2010b; Meehan et al., 2006).
Coercive practice and aggression: In relation to coercion, limit setting by staff was
one of the most commonly reported precipitants of service user aggression (Harris &
Verney, 1986; Bjøkly, 1999; Daffern et al., 2008; Meehan et al., 2006; Winje et al.,
2018). For example, Bjøkly (1999) found that 64% of reported incidents of
aggression were preceded by staff limit setting. Staff limit-setting was defined in
several ways which included, for example, demands for activities/ordering service
users to do something, denial or ignoring service user requests, staff provocation,
inflexibility of rules put in place by staff. Furthermore, Winje and colleagues (2018)
found that, out of 1900 incidents recorded, 46.8% were reported to be provoked by
staff placing restrictions on the service users’ behaviour on the SOAS-R measure. In
123

URN: 6455433
the one qualitative study, service user participants described how staff’s limit-setting
was, at times, demeaning (Meehan et al., 2006).
One study reported service users’ interactions with staff as being a major source of
dissatisfaction and a factor that often leads to service users’ aggression (Meehan et
al., 2006). In Meehan and colleagues’ (2006) qualitative study, service users
described staff as adopting a superior attitude and controlling behaviour.
Furthermore, service users described how staff lack of understanding and non-caring
attitude often led service users to retaliate in an aggressive manner.
Interpersonal style and aggression: Four studies reported a correlation between
service user interpersonal styles and aggressive behaviour (Daffern et al., 2010b;
Doyle et al., 2006; Vernham et al., 2016; Smith et al., 2013). Daffern and colleagues
(2010b) found that a coercive interpersonal style correlated with aggression, this
approached a statistical significance (p= .002). Another study found that violent
service users were more likely to have dominant, coercive and hostile interpersonal
styles (Doyle et al., 2006). Vernham and colleagues (2016) also found a significant
relationship between dominant and coercive interpersonal styles with verbal and
physical aggression (dominant and verbal, p=<.001; dominant and physical, p=.003;
coercive and verbal, p=<.001; coercive and physical, p=<.001), but unlike Doyle and
colleagues, they found that hostile interpersonal styles did not significantly predict
either verbal or physical aggression. Contrary to the significant relationship between
dominant interpersonal style and aggression, Smith and colleagues (2013) found that
fearless dominance was marginally related to predatory aggression (p=0.07) and
unrelated to impulsive aggression and psychotic aggression.
124

URN: 6455433
With regards to moderator effects, in Daffern and colleagues (2010b) study neither
hostility nor dominance were independently related to aggression whereas an
elevation in both interpersonal styles was found to increase likelihood of service user
aggression. Similarly, Smith and colleagues, found significant interactive effects
between high levels of fearless dominance and self-centred impulsivity in increasing
the likelihood of predatory aggression (p=<0.05) whereas high levels of one of either
characteristic independent of the other did not increase likelihood of predatory
aggression. Furthermore, Smith and colleagues (2013) found no significant
interactive effects between fearless dominance and self-centred impulsivity in forms
of impulsive or psychotic aggression. Nearly three times more of the included sample
in Smith and colleagues (2013) study took part in impulsive aggressive incidents
compared to predatory aggressive incidents which, in the context of this study’s
findings, suggests that rates of aggressive incidents in forensic settings may not be
related to those who display more dominant interpersonal behaviours.
Doyle and colleagues (2006) findings indicated that compliant interpersonal styles
were a protective factor towards aggressive behaviour. Furthermore, the strongest
inverse relationship was found between dominance and submission (where those
who have dominant interpersonal characteristics are least likely to show submissive
interpersonal characteristics) (Doyle et al., 2006).
With regards to longitudinal follow up, Vernham and colleague’s study (2016), there
was a consistent (but not an increased) association between dominant and coercive
interpersonal styles and aggression from when service users were first admitted into
125

URN: 6455433
the unit, and at 12 and 24 months follow up. There was, however, a significant
positive association between hostile scorings with recorded incidents of verbal and
physical incidents recorded at 48 months follow up (verbal, p=0.05; physical,
p=.034). Furthermore, although not formally assessed, this study found that
predictive validity of interpersonal styles was only applicable to service users who
had been recently admitted who were more likely to see hospital processes as more
coercive compared to those that had been residing in hospital for longer.
Interpersonal style, coercion and aggression: Only one study investigated the
relationship between interpersonal style, perceived coercion and incidents of
aggression during admission (Daffern et al., 2010b). The study’s findings concluded
that there was no statistical significance in the relationship between perceived
coercion and service user interpersonal style. And although coercive interpersonal
style was correlated to aggression, service users’ perceptions of coercion during the
admission process was not related to likeliness of aggression. For example, service
users’ perceptions of the control and restrictions put in place when first admitted into
hospital did not correlate to future aggressive behaviour. There was no attempt to
analyse how interpersonal style interacted with perceived coercion to impact on
aggression and self-harm due to the non-significance in the above findings.
3.3 Quality assessment results of the included studies
Following from the methodological quality assessment, this section will summarise
the main strengths and limitations of the review’s included studies.
With regards to total quality scores, the highest scoring study met 82.5% of
quality criteria (Vernham et al., 2016), four studies met between 60-70% of quality
126

URN: 6455433
criteria (BjØkly, 1999; Doyle & Dolan, 2006; Smith et al., 2013; Winje et al., 2018),
and the remaining four studies scored 50% or lower (Meehan et al., 2006; Daffern et
al., 2008; Daffern et al., 2010b; Harris & Varney, 1986). All nine studies provided in
full or in part, an appropriate/relevant scientific background. In addition, all studies
provided clear study objectives, whereas only two out of the eight quantitative
studies provided study hypotheses (Smith et al., 2013; Vernham et al., 2016).
Two out of the nine studies provided a rationale for the study design (Smith
et al., 2013; Vernham et al., 2016). All studies provided in full or in part, a
description of the study setting. Only one study provided a clear, full description of
the study sampling criteria and recruitment strategy (Smith et al., 2016) and
furthermore, only three out of the eight quantitative studies provided full details on
how study sample size was calculated (BjØkly, 1999; Vernham et al., 2016; Winje et
al., 2018). All, aside one of the eight quantitative studies (Harris & Varney, 1986),
either in full or partly provided details on the methods of assessment/outcome
measures. Only one quantitative study (BjØkly, 1999) did not include any details on
the statistical methods used to analyse the data. The remaining eight quantitative
studies only partly fulfilled the criteria for methods of statistical analysis as they did
not include any details on, for example, sensitivity analyses. The one qualitative
study (Meehan et al., 2006) provided a clear description on data collection and data
analysis (e.g. how focus groups were conducted and how content analysis was used
to analyse the data). This study did not, however, provide detail on researcher
reflexivity (how researcher’s own position impacted upon the collection and analysis
of the data).
All eight quantitative studies only partly met criteria for descriptive data; this
was because, for example, there was no information provided on missing data. Only
127

URN: 6455433
two quantitative studies provided full details of the main results (e.g. including
adjusted estimates for confounding variables) (BjØkly, 1999; Doyle & Dolan, 2006).
The one qualitative study provided a clear description of the five identified themes
(Meehan et al., 2006).
All studies either fully or partly discussed key results in the context of study
objectives, previous research evidence, and study limitations. Those who partly met
these criteria were missing information on, for example, clinical implications (e.g.
Harris & Varney, 1986) or provided no discussion on how confounding variables
may have impacted upon the study findings (e.g. Daffern et al., 2008).
128

URN: 6455433
Table 2: Quality assessment table for quantitative studies
Criteria BjØkly (1999)
Daffern et al. (2008)
Daffern et al. (2010b)
Doyle et al. (2006)
Harris & Varney (1986)
Smith et al. (2013)
Vernham et al. (2016)
Winje et al. (2018)
Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N
Titl
e an
d ab
stra
ct
(i) Was the study’s design a commonly used term in the title or the abstract?
Yes No Partly Partly Yes Partly Partly No
(ii) Did the abstract provide an informative and balanced summary of what was done and what was found?
Yes Yes Partly No Partly Yes Yes Yes
Intr
oduc
tion
i) Background/rationale: Was an appropriate/relevant scientific background and rationale for the investigation reported?
Partly Yes Yes Partly Partly Yes Yes Yes
ii) Objectives: Were specific objectives stated and prespecified hypotheses specified?
Partly Partly Yes Partly Partly Partly Yes Partly
Met
hods
i) Study design: Were key elements of study design presented early in the paper?
No No No No No Yes Yes Partly
ii) Setting: Was there a clear description of the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection?
Partly Partly Partly Partly Partly Partly Yes Yes
129

URN: 6455433
Criteria BjØkly (1999)
Daffern et al. (2008)
Daffern et al. (2010b)
Doyle et al. (2006)
Harris & Varney (1986)
Smith et al. (2013)
Vernham et al. (2016)
Winje et al. (2018)
Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/Niii) Participants: (a) Was eligibility criteria, and the sources and methods of selection of participants provided? Were methods of follow-up described? (b) For matched studies, was matching criteria and number of exposed and unexposed given?
n/a Partly Partly Partly No Yes Partly Partly
iv) Variables: Were outcomes (DV), exposure (IV), predictors (experimental/manipulated variable), potential confounders, and effect modifiers clearly described?
Partly No No Yes Partly Yes Yes Yes
v) Data sources/ measurement: For each variable of interest, were sources of data and details of methods of assessment (measurement) given? Was comparability of assessment methods if there is more than one group described?
Partly Partly Partly Yes No Partly Yes Partly
vi) Bias: Were any efforts to address potential sources of bias provided?
No No No Partly No Partly Yes Partly
130

URN: 6455433
Criteria BjØkly (1999)
Daffern et al. (2008)
Daffern et al. (2010b)
Doyle et al. (2006)
Harris & Varney (1986)
Smith et al. (2013)
Vernham et al. (2016)
Winje et al. (2018)
Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/Nvii) Study size: Was there an explanation on how the study size was arrived at?
Yes n/a No Partly n/a No Yes Yes
Viii) Statistical methods: (a) Were all statistical methods, including those used to control for confounding described? (b) Was there a description of the methods used to examine subgroups and interactions? (c) Was there an explanation for any missing data? (d) If applicable, was there an explanation as to how loss to follow-up was addressed? (e) Were sensitivity analyses included and described?
No Partly Partly Partly Partly Partly Partly Partly
Res
ults
i) Participants: (a) Were numbers of individuals reported at each stage of study? —eg numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed (b) Were reasons given for non-participation at each stage? (c) Was a flow diagram used?
No No Partly Partly Partly Partly Partly Partly
131

URN: 6455433
Criteria BjØkly (1999)
Daffern et al. (2008)
Daffern et al. (2010b)
Doyle et al. (2006)
Harris & Varney (1986)
Smith et al. (2013)
Vernham et al. (2016)
Winje et al. (2018)
Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/Nii) Descriptive data: (a) Were characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential confounders given? (b) Were number of participants with missing data for each variable of interest indicated? (c) Was follow-up time (eg, average and total amount) summarised?
Partly Partly Partly Partly Partly Partly Partly Partly
iii) Outcome data: Were numbers of outcome events or summary measures over time reported?
Yes No n/a n/a Yes Partly Partly Yes
iv) Main results: (a) Were unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence interval) given? Was it clear which confounders were adjusted for and why they were included? (b) Were category boundaries when continuous variables were categorized reported? (c) If relevant, was translating estimates of relative risk into absolute risk for a meaningful time period considered?
Yes No No Yes No Partly Partly Partly
132

URN: 6455433
Criteria BjØkly (1999)
Daffern et al. (2008)
Daffern et al. (2010b)
Doyle et al. (2006)
Harris & Varney (1986)
Smith et al. (2013)
Vernham et al. (2016)
Winje et al. (2018)
Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N Y/P/N
Dis
cuss
ion
i) Key results: Were key results with reference to study objectives summarised?
Yes Yes Yes Yes Partly Yes Yes Yes
ii) Limitations: Were limitations of the study considering sources of potential bias or imprecision discussed? Were both direction and magnitude of any potential bias discussed?
Partly Yes Partly Yes Partly Yes Yes Yes
iii) Interpretation: Was a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence given?
Yes Yes Yes Yes Partly Yes Yes Yes
iv) Generalisability: Was the generalisability (external validity) of the study results given?
Partly Partly Partly Yes No Yes Yes Yes
Total score 11/19(60.5%)
8.5/19(44.7%)
9/19(47.4%)
12/19(63.2%)
7.5/19(39.5%)
14/20 (70%)
16.5/20(82.5%)
11.5/19 (60.5%)
Note: Y= yes, met criteria; P= partly met criteria; N= no, not met criteria.
133

URN: 6455433
Table 3: Quality assessment table for the qualitative study
Criteria Meehan et al. (2006)
Y/P/N1) Was there a clear statement of the aims of the research?
Partly
2) Is the qualitative methodology appropriate? Yes
3) Was the research design appropriate to address the research aims?
Partly
4) Was the recruitment strategy appropriate to the aims of the research?
Partly
5) Was the data collected in a way that addressed the research issue?
Partly
6) Has the relationship between researcher and participants been adequately considered?
No
7) Was the data sufficiently rigorous? Partly
8) Is there a clear statement of findings? Partly
Total quality score 4/8 (50%)
Note: Y= yes, met criteria; P= partly met criteria; N= no, not met criteria
134

URN: 6455433
4.0 Discussion
In this section, the main findings of the included studies will be discussed in the
context of current theory, practice and research whilst presenting potential areas of
focus or specific questions for future research, and potential implications for policy
and practice. Before discussing the findings of the literature review in more detail,
the methodological limitations of the study (following from the quality assessment)
will be discussed. These limitations will provide a critical framework in which to
consider the reliability and validity of the current evidence base on coercive practice,
service user interpersonal style and aggressive behavior in secure forensic settings.
4.1 Methodological limitations of the included studies
In some of the included studies, service user participants may have completed
questionnaires in a socially desirable way or may have been less ‘risky’ than other
service users who refused to participate. In addition, some of the included studies
collected data from specialist secure units which only took those service users who
displayed more challenging behaviour and therefore the sample may have been
skewed by, for example, certain personality traits and interpersonal styles which are
more likely to be correlated with higher incidents of violence and aggression. Aside
service user participants, seven out of the eight quantitative studies used only one
member of staff to complete measures about, for example, service user interpersonal
style, with most studies not reporting who the staff were and/or the nature of their
relationship with the service user. Furthermore, in Meehan and colleague’s (2006)
qualitative study, presumably participants signed themselves up to taking part in the
focus groups (although there is no information reported on this) and it is therefore
questionable as to whether there may have been a biased/skewed view towards staff.
135

URN: 6455433
For example, service users may have been motivated to take part in the research as
they had negative issues, they wanted to vent about staff behaviour, although it is
also important to highlight that this does not make their experience any less real.
Future research should provide more details on how characteristics relevant to the
service user population are represented within the sample and furthermore, consider
the impact of self-completed measures (by staff and service users) on the validity of
the findings.
All eight quantitative studies collected data on violent and aggressive incidents over
specific periods of time. As these incidents are recorded as routine procedure in
hospital settings, the data collected on the specific nature, severity and direction of
aggression perpetrated by the service users may have been reliant on the limited
details of the incident forms. Further to this, most of the studies did not report
specific details on missing data and it was therefore unclear as to which participants’
data was and was not included in the follow up periods. For example, in Harris &
Varney’s (1986) study there was a likelihood that those who were discharged from
the units during the study (possibly to lower secure units) were service users who
were less likely to be involved in violent/aggressive incidents and it is therefore
understandable why incidents of violence and aggression would reduce at follow up.
Future research should consider ways to triangulate routine collected data with other
sources of information. For example, the findings in the only qualitative study
included in the survey, were complementary to and provided further insight into the
quantitative findings on coercive practice and aggression (Meehan et al., 2006). This
suggests a potential need to conduct mixed methods research thus, dovetailing
qualitative service user and/or staff accounts on to the quantitative data. In specific
136

URN: 6455433
reference to the only study that looked at the relationship between both interpersonal
style and perceived coercion on rates of aggression and violence (Daffern et al.,
2010b), it is important to consider that there was a limited variability in perceived
coercion and a narrow and extreme range of interpersonal styles within the study
sample. which may just reflect the nature of those who reside in such services (e.g.,
Blackburn, 1998). This may have been due to the study’s small sample size which
focused only on those who had been recently admitted into hospital. It may have
therefore been useful to include a larger, more varied sample size which included
service users who had been in the secure care system for longer and who’s
perceptions of coercion may be somewhat different to service users who had been
recently admitted.
All included studies reported significant findings that mapped on to the main
research objectives and existing evidence base whilst providing implications and
recommendations for future practice. However, the significance of the findings from
the included studies should be considered with caution due to the limited detail on
the methods of data collection (e.g. sampling and statistical analysis) and the
relatively small sample sizes that were often recruited from specialised units within
one or two hospital settings. For example, Vernham and colleagues (2016) was the
only study included in the review that had included a power size calculation while
also had a large sample size (which reached statistical power). It is therefore
important to consider that the statistical significance of the other studies findings
may have been more vulnerable to Type I errors.
137

URN: 6455433
Lastly, five studies were conducted outside the UK (USA, Norway, Australia) whilst
half the included studies were published over a decade ago. It is therefore important
to consider differences and changes in policies and procedures in secure forensic
hospitals within and between the study settings and the impact that this may have
upon the relevance of the study’s findings for current UK forensic secure-care.
4.2 Discussion of the literature review’s findings
As highlighted in the findings, only one study explicitly looked at the relationship
between coercive practice, interpersonal style and aggression and no significant
relationship was found between perceived coercion of staff and interpersonal style
(Daffern et al., 2010b). However, there was no information about how the sample
size was arrived at and/or whether a power calculation was conducted and therefore
it was not known as to whether there was an appropriate sample size in which a
precise and accurate conclusion could be drawn upon. The authors concluded that
perceived coercion when first admitted into hospital does not correlate to future
aggressive behaviour (Daffern et al., 2010b). Therefore, there is a need for research
that focuses on the use of coercive measures and service users’ perceptions of these
measures that runs outside of the period of admission.
Coercive practice has become integral to managing violent/aggressive/non-compliant
behaviour by use of extreme coercive measures through manual restraint, rapid
tranquillisation and seclusion (NICE, 2014). Surprisingly, although included in the
search terms, none of the studies looked explicitly at seclusion or restraint, which are
the more commonly known coercive measures. Furthermore, studies that have
focused on seclusion, restraint and service user aggression did so in general
138

URN: 6455433
psychiatric inpatient settings and were therefore excluded. This mirrors Hui’s review
of coercive measures in forensic settings, who noted that there was a distinct lack of
research on coercive measures in forensic inpatient settings (Hui et al., 2013).
Dominant and coercive service user interpersonal styles were significantly correlated
with aggressive and violent behaviour (Daffern et al., 2010b; Doyle et al., 2006;
Smith, Edens & McDermott et al., 2013; Vernham et al., 2016). In Doyle and
colleagues (2006) research, an inverse relationship between submission and
compliance with more dominant service user interpersonal styles was found. In the
context of Kiesler’s interpersonal theory (1987) and the complementarity in our
interactions with others, we would expect that service users who scored highly on
dominant and coercive interpersonal styles as being more likely to clash with
coercive practices (which aim to coerce service users into submission). However, as
suggested by Daffern and colleague’s (2010b) findings, there was no significant
relationship between dominant and coercive interpersonal styles and perceptions of
staff coercion (during the period of admission into hospital).
Putting interpersonal style aside, four out of nine studies included in this review
reported staff limit-setting as the most common predictor of service user aggression
(Harris & Varney, 1986; Bjøkly, 1999; Daffern et al., 2008; Meehan et al., 2006;
Winje et al., 2018). This illustrates the relevance of longer-term measures of coercion
used in secure-care settings such as, persuasion, interpersonal leverage and
inducement, as well as the shorter-term, more extreme coercive measures, such as
seclusion and restraint (Applebaum & Szmukler, 2008). Aside the types of status
challenges that arise between staff and service user in the implementation of coercive
measures, and as suggested by the one qualitative study included in the review
139

URN: 6455433
(Meehan et al., 2006), perhaps service users’ vulnerabilities to low self-esteem and
emotional deprivation (e.g. feeling as if staff do not understand or care about them)
may also trigger acts of aggression and violence amongst more dominant/coercive
service users. This notion is supported by previous literature which indicates that
those with lower self-esteem may be more vulnerable to experiencing increased
frustration and often display overly dominant behaviour as a way to cope (BjØrkvik
et al., 2009). There is therefore a need to consider that, in the context of secure-care
settings where coercive measures are being used by staff on a day-to-day basis (i.e.
limit setting/restricting rules), those service users who are vulnerable to low self-
esteem and feelings of emotional deprivation may resort to acts of aggression and
violence (become overly dominant) as a maladaptive coping strategy. Therefore, as
highlighted by the studies included in this review, it may not just be
dominant/coercive interpersonal styles that are more likely to predict service user
aggression but, may also be about the way in which service users perceive the
behaviour of others. Perhaps service users’ perceptions of staff coercion are linked to
individual differences in their interpersonal sensitivities to others where “some
patients may be less likely to be sensitive to others' irritating behaviour” (Hopwood
et al., 2011: p 708). For example, those who value personal authority and being in
control should be most frustrated by others who are arrogant, bossy, and act superior
(Henderson & Horowitz, 2006). This would suggest that people may be differentially
sensitive to specific forms of aversive behaviour of others because their interpersonal
motives vary. Therefore, interpersonal sensitivities may act as a “bridge” between
service users’ interpersonal styles and their perceptions of staff coercion and is an
area which needs further exploration.
140

URN: 6455433
Given the high hits and the small final number of relevant papers, it may be
important to consider the sensitivity and specificity of the review’s search strategy.
This might suggest that the search did not only retrieve the relevant literature but lots
of irrelevant literature as well. In addition, the review only included studies based in
forensic/secure settings and therefore may have excluded several studies from non-
forensic settings which may looked at the link between coercive practices,
interpersonal style, and service user violence/aggression. Furthermore, although the
search terms were carefully selected for the search strategy, they will in turn
ultimately influence those articles retrieved from the literature. For example, Hui and
colleagues (2013) noted that different definitions of coercive measures exist, which
made the selection of search terms for this review even more complex in nature. It is
therefore questionable as to how adequate the criteria were in capturing all measures
of coercion used in forensic settings. With these implications in mind, it would
therefore be advisable for this search strategy to be reviewed in future research.
All studies included in this literature review indicated that either interpersonal style
and/or coercive measures (such as staff limit-setting) were linked to service user
violence and aggression. There was, however, no research that explicitly looked at
the relationship between both service users’ interpersonal sensitivities and perceived
staff coercion as possible predictors of further aggression/violence. A better
understanding in to the way in which service users make sense of coercive practices
in context of their interpersonal sensitivities and in turn, how these impact upon
aggressive incidents, may help to reduce the number of untoward incidents that occur
because of service users feeling frustrated/restricted by staff limit setting. For
example, for staff to have an awareness that some service users may be more
141

URN: 6455433
bothered by inducement (e.g. the confiscation of items) and may act out aggressively
compared to other service users who are not bothered by such coercive measures. In
order to reduce the likelihood of aggressive incidents, alternative approaches to
manage challenging behaviour may need to be considered. Perhaps if staff had a
better understanding of the types of interpersonal behaviours that service users are
sensitive to, this would help aid in their communication with service users with the
aim of maximising service user’s recovery whilst reducing and managing risk. For
example, by interweaving interpersonal sensitivities into the service user’s care plans
(i.e. service user may act out with further aggression when staff make threats to
confiscate items), clinical teams may be more aware of specific triggers related to
their interactions with service users that could precede service user aggression and
furthermore, to consider more appropriate/alternative communication styles. This
may help to break the ‘aggression-coercion cycle’ (Goren, 1993) between staff and
service users and in turn, reduce aggressive incidents, thus helping service users to
move forward in their recovery and through the secure care system. As stated
previously, aggressive behaviour may be a result of a complex interaction between
situational factors and individual factors (Anderson & Bushman, 2002). For example,
some service users may be particularly sensitive to being controlled by others which
can be exacerbated further when placed in a restrictive environment. On a policy
level, perhaps there may be a need to consider not just what coercive measures need
to be in place (i.e. hospital rules and regulations) but how they are implemented, and
how they may or may not predict further acts of aggression and violence in the
context of specific service user characteristics.
142

URN: 6455433
References
Fallon P (1999) Report of the Committee of Inquiry into the Personality Disorder Unit, AshworthSpecial Hospital, Cm 4194-1. London: HMSO.Fallon P (1999) Report of the Committee of Inquiry into the Personality Disorder Unit, AshworthSpecial Hospital, Cm 4194-1. London: HMSO.Fallon P (1999) Report of the Committee of Inquiry into the Personality Disorder Unit, AshworthSpecial Hospital, Cm 4194-1. London: HMSO.Henderson, L., & Horowitz, L. M. (2006, June) Social allergens and frustratedinterpersonal motives. Paper presented at the Society for Interpersonal Theoryand Research, Philadelphia, PA.Henderson, L., & Horowitz, L. M. (2006, June) Social allergens and frustratedinterpersonal motives. Paper presented at the Society for Interpersonal Theoryand Research, Philadelphia, PA.Henderson, L., & Horowitz, L. M. (2006, June) Social allergens and frustratedinterpersonal motives. Paper presented at the Society for Interpersonal Theoryand Research, Philadelphia, PA.Ahmed, A. G. and Lepnurm, M. (2001). Seclusion practice in a Canadian forensic
psychiatric hospital. Journal of the American Academy of Psychiatry and the Law, 29(3), 303–309. Retrieved from https://europepmc.org/abstract/med/11592458
Alexander, J. & Bowers, L. (2004). Acute psychiatric ward rules: A review of the literature. Journal of Psychiatric and Mental Health Nursing, 11, 623-631. DOI: 10.1111/j.1365 2850.2004.00770
American Psychiatric Association, American Psychiatric Nurses Association & National Association of Psychiatric Health Systems. (2003). Learning from each other: Success stories and ideas for reducing restraint/seclusion in behavioural health. Retrieved from WorldCat Website: https://www.worldcat.org/title/learning-from-each-other-success-stories-and-ideas-for-reducing-restraintseclusion-in-behavioral-health/oclc/52758580
Anderson, C. A., & Bushman, B.J. (2002). Human aggression. Annual Review of Psychology, 53, 27-51. DOI: 10.1146/annurev.psych.53.100901.135231
Arksey, H., & O'Malley, L. (2005). Scoping studies: towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19-32. DOI: 10.1080/1364557032000119616
Aveyard, H. (2014). Doing a literature review in health and social care: A practical guide. London: McGraw-Hill Education.
143

URN: 6455433
Beck, N.C., Durrett, C., Stinson, J., Coleman, J., Stuve, P., & Menditto, A. (2008). Trajectories of seclusion and restraint use at a state psychiatric hospital. Psychiatric Services, 59(9), 1027–1032. DOI:
10.1176/ps.2008.59.9.1027
Blackburn, R. (1998). Criminality and the interpersonal circle in mentally disordered offenders. Criminal Justice and Behavior, 25(2), 155-176. DOI: 10.1177/0093854898025002001
Blackburn, R., & Renwick, S.J. (1996). Rating scales for measuring the interpersonal circle in forensic psychiatric patients. Psychological Assessment, 8, 76–84. DOI: 10.1037/1040- 3590.8.1.76
Blom-Cooper, L. (1992). Report of the Committee of Inquiry into Complaints about Ashworth Hospital, Cm 2028-1. London: HMSO.
Bjorkly, S. (1996). Report Form for Aggressive Episodes: Preliminary report. Perceptual and Motor Skills, 83, 1139-1152. DOI: 10.2466/pms.1996.83.3f.1139
Bjørkly, S. (1999). A ten‐year prospective study of aggression in a special secure unit for dangerous patients. Scandinavian Journal of Psychology, 40(1), 57-63. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/10216464
BjØrkvik, J., Biringer, E.V.A., Eikeland, O.J., & Nielson, G.H. (2009). Self-esteem and interpersonal functioning in psychiatric outpatients. Scandinavian Journal of Psychology, 50(3), 259-265. DOI: 10.1111/j.1467-9450.2009.00709
Blackburn, R., & Glasgow, D. V. (2006). Manual for the Chart of Interpersonal Reactions in Closed Living Environments (CIRCLE). Unpublished manuscript, University of Liverpool, UK.
Bowers, L., Stewart, D., Papadopoulos, C., Dack, C., Ross, J., Khanom, H., & Jeffery, D. (2011). Inpatient violence and aggression: a literature. Report from the Conflict and Containment Reduction Research Programme. Retrieved from http://www.kcl.ac.uk/iop/depts/hspr/research/ciemh/mhn/projects/litreview/LitRevAgg.pdf
Bubb, S. (2014). Winterbourne view–time for change: transforming the commissioning of services for people with learning disabilities and/or autism. Retrieved from British Library Website: https://www.bl.uk/collection- items/winterbourne-view--time-for- change-transforming-the-commissioning-of-services-for-people-with-learning-disabilities-andor-autism
Burrows S. (1991). The special hospital nurse and the dilemma of therapeutic custody. Journal of Advances in Health and Nursing Care, 1, 21–38.
144

URN: 6455433
Care Quality Commission. (2017). The state of care in mental health services 2014 to 2017. Retrieved from Care Quality Commission Website: https://www.cqc.org.uk/publications/major-report/state-care-mental-health-services-2014-2017
Castro, M., Cockerton, T., & Birke, S. (2002). From discharge to follow-up: a small-scale study of medium secure provision in the independent sector. British Journal of Forensic Practice, 4, 31-9. DOI: 10.1108/14636646200200019
Centre for Mental Health. (2011). Pathways to unlocking secure mental health care. Retrieved from Centre for Mental Health Website: https://www.centreformentalhealth.org.uk/sites/default/files/2018-09/Pathways_to_unlocking_secure_mental_health_care.pdf
Compton, M. T., Craw, J., & Rudisch, B. E. (2006). Determinants of inpatient psychiatric length of stay in an urban county hospital. Psychiatric Quarterly, 77(2), 173-188. DOI: 10.1007/s11126-006-9005-z
Cookson, A., Daffern, M., & Foley, F. (2012). Relationship between aggression, interpersonal style, and therapeutic alliance during short‐term psychiatric hospitalization. International Journal of Mental Health Nursing, 21(1), 20-29. DOI:10.1111/1447-0349.2011.00764
Critical Appraisal Skills Programme (CASP). (2013). Qualitative Research Checklist. Retrieved from Critical Appraisal Skills Programme Website: http://www.casp-uk.net/wp-content/uploads/2011/11/casp-qualitative-
research-checklist-31.05.13.pdf#!casp-tools-checklists/c18f8
Daffern, M., Mayer, M. M., & Martin, T. (2003). A preliminary investigation into patterns of aggression in an Australian forensic psychiatric hospital. Journal of Forensic Psychiatry and Psychology, 14(1), 67–84. DOI: 10.1080/1478994031000074306
Daffern, M., Howells, K., & Ogloff, J. R. (2007). What’s the point? Towards a methodology for assessing the function of psychiatric inpatient aggression. Behaviour Research and Therapy, 45, 101-111. DOI: 10.1016/j.brat.2006.01.011
Daffern, M., Duggan, C., Huband, N., & Thomas, S. (2008). The impact of interpersonal style on aggression and treatment non-completion in patients with personality disorder admitted to a medium secure psychiatric unit. Psychology, Crime & Law, 14(6), 481-492. DOI: 10.1080/10683160801948717
Daffern, M., Duggan, C., Huband, N., & Thomas, S. (2010a). Staff and Patient’s Perceptions of Each Other’s Interpersonal Style Relationship with
Severity of Personality Disorder. International Journal of Offender Therapy and Comparative Criminology, 54(4),611-624. DOI:10.1177/0306624X09335111
145

URN: 6455433
Daffern, M., Tonkin, M., Howells, K., Krishnan, G., Ijomah, G., & Milton, J. (2010b). The impact of interpersonal style and perceived coercion on aggression and self-harm in personality-disordered patients admitted to a secure psychiatric hospital. The Journal of Forensic Psychiatry & Psychology, 21(3), 426-445. DOI:10.1080/14789940903505951
Davoren, M., Byrne, O., O’Connell, P., O’Neill, H., O’Reilly, K., & Kennedy, H. G. (2015). Factors affecting length of stay in forensic hospital setting: need for therapeutic security and course of admission. BMC psychiatry, 15(1), 301. DOI: 10.1186/s12888-015-0686-4
Department of Health. (2014). Positive and proactive care: reducing the need for restrictive interventions. Retrieved from Department of Health Website: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/
attac hment_data/file/300293/JRA_DoH_Guidance_on_RP_web_accessible.odf
Dickens, G., Picchioni, M., & Long, C. (2013). Aggression in specialist secure and forensic inpatient mental health care: incidence across care pathways. Journal of Forensic Practice, 15, 206-17. DOI: 10.1108/JFP-09-2012-0017
Dolan, M., & Blackburn, R. (2006). Interpersonal factors as predictors of disciplinary infractions in incarcerated personality disordered offenders. Personality and Individual Differences, 40(5), 897-907. DOI: 10.1016/j.paid.2005.10.003
Doyle, M., & Dolan, M. (2006). Evaluating the validity of anger regulation problems, interpersonal style, and disturbed mental state for predicting inpatient violence. Behavioral Sciences & the Law, 24(6), 783-798. DOI: 10.1002/bsl.739
Drennan, G., & Wooldridge, J. (2014). Making recovery a reality in forensic services. Implementing Recovery through Organisational Change (ImROC) briefing paper. Retrieved from the Centre for Mental Health and Mental Health Network NHS Confederation Website: file:///C:/Users/jess/Downloads/ImROC-briefing-10-Making-Recovery-a-Reality-in-Forensic-Settings-final-for-web%20(1).pdf
Fallon, P. (1999). Report of the Committee of Inquiry into the Personality Disorder
Unit, Ashworth Specialised Hospital, Cm 4194-1. London, UK: HMSO.
Gardner, W., Hoge, S. K., Bennett, N., Roth, L. H., Lidz, C. W., Monahan, J., & Mulvey, E. P. (1993). Two scales for measuring patients' perceptions for coercion during mental hospital admission. Behavioral Sciences & the Law, 11(3), 307-321. DOI: 10.1002/bsl.2370110308
Goffman, E. (1968) Asylums Essays on the Social Situation of Mental Patients and Other Inmates. Harmondsworth: Penguin.
146

URN: 6455433
Goren, S., Singh, N. N., & Best, A. M. (1993). The aggression-coercion cycle: Use of seclusion and restraint in a child psychiatric hospital. Journal of Child and Family Studies, 2(1), 61–73. Retrieved from https://link.springer.com/article/10.1007/BF01321301
Hare, R.D. (1991). The Hare Psychopathy Checklist Revised (PCL-R). Toronto, Ontario: MultiHealth Systems.
Harty, M. A., Shaw, J., Thomas, S., Dolan, M., Davies, L., Thornicroft, G., Carlisle, J., Moreno, M., Leese, M., Appleby, L., & Jones, P. (2004). The security, clinical and social needs of patients in high security psychiatric hospitals in England. Journal of Forensic Psychiatry & Psychology, 15(2), 208-221. DOI: 10.1080/14789940410001703967
Harris, G. T., & Varney, G. W. (1986). A ten-year study of assaults and assaulters on a maximum security psychiatric unit. Journal of Interpersonal Violence, 1(2), 173-191. DOI: 10.1177/088626086001002003
Harris, S. T., Oakley, C., & Picchioni, M. M. (2014). A systematic review of the association between attributional bias/interpersonal style, and violence in schizophrenia/psychosis. Aggression and Violent Behavior, 19(3), 235-241. DOI: 10.1016/j.avb.2014.04.009
Henderson, L., & Horowitz, L. M. (2006). Social allergens and frustrated interpersonal motives, presented at the Society for Interpersonal Theory and Research Conference, Philadelphia, 2006. Philadelphia, PA: Society for Interpersonal Theory and Research.
Hopwood, C. J., Ansell, E. B., Pincus, A. L., Wright, A. G., Lukowitsky, M. R., & Roche, M. J. (2011). The circumplex structure of interpersonal sensitivities. Journal of Personality, 79(4), 707-740. DOI: 10.1111/j.1467-6494.2011.00696
Hui, A., Middleton, H., & Völlm, B. (2013). Coercive measures in forensic settings: findings from the literature. International Journal of Forensic Mental Health, 12(1), 53-67. DOI: 10.1080/14999013.2012.740649
Jarrett, M., Bowers, L., & Simpson, A. (2008). Coerced medication in psychiatric inpatient care: Literature Review, Journal of Advanced Nursing, 64(4), 538-548. DOI: 10.111/j.1365-2648.2008.04832.x
Kelly, E.L., Subica, A. M., Fulginiti, A., Brekke, J. S., & Novaco, R.W. (2015). A cross-sectional survey of factors related to inpatient assault of staff in a
forensic psychiatric hospital. Journal of Advanced Nursing, 71(5), 1110–1122. DOI: 10.1111/jan.12609
Keski-Valkama, A., Koivisto, A.M., Eronen, M. and Kaltiala- Heino, R. (2010). Forensic and general psychiatric patients’ view of seclusion: A comparison
147

URN: 6455433
study. Journal of Forensic Psychiatry and Psychology, 21(3), 446–461. DOI: 10.1080/14789940903456569
Kiesler, D. (1979). An interpersonal communication analysis of relationship in psychotherapy. Psychiatry, 42, 299–311. DOI: 10.1080/00332747.1979.11024034
Kiesler, D. (1987). Manual for the Impact Message Inventory. Mountain View, CA: Consulting Psychologists Press.
Kiesler, D. J. (1997). Contemporary interpersonal theory and research: Personality, psychopathology and psychotherapy. The Journal of Psychotherapy Practice and Research, 6(4), 339-341. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3350312/
Lillie, R. (2007). Getting clients to hear: Applying principles and techniques of Kiesler's Interpersonal Communication Therapy to assessment feedback. Psychology and Psychotherapy: Theory, Research and Practice, 80(1), 151-163. DOI: 10.1348/147608306X115198
Lilienfeld, S. O., & Widows, M. R. (2005). Psychopathic Personality Inventory-Revised: Professional manual. Lutz, FL: PAR, Inc.
Loranger, A.W., Sartorius, N., Andreoli, A., Berger, P., Buchheim, P., Channabasavanna, S.M., Coid, B., Dahl, A., Diekstra, R., Ferguson, B., Jacobsberg, L., Mombour, W., Pull, C., Ono, Y., & Regier, D.A. (1994) The International Personality Disorder Examination. The World Health Organization/Alcohol, Drug Abuse, and Mental Health Administration International Pilot Study of personality disorders. Archives of General Psychiatry, 51, 215-224. DOI: 10.1001/archpsyc.1994.03950030051005
Mason, T., Lovell, A., & Coyle, D. (2008). Forensic psychiatric nursing: skills and competencies: I role dimensions. Journal of Psychiatric and Mental Health Nursing, 15(2), 118-130. DOI: 10.1111/j.1365-2850.2007.01191
Meehan, T., McIntosh, W., & Bergen, H. (2006). Aggressive behaviour in the high‐secure forensic setting: the perceptions of patients. Journal of Psychiatric and Mental Health Nursing, 13(1), 19-25. DOI: 10.1111/j.1365-
2850.2006.00906
Meissner, W. (2007). Therapeutic alliance: Theme and variations. Psychoanalytic Psychology, 24, 231–254. DOI: 10.1037/0736-9735.24.2.231
Mellesdal, L. (2003). Aggression on a psychiatric acute ward: a three-year prospective study. Psychological Reports, 92, 1229-1248. DOI: 10.2466/pr0.2003.92.3c.1229
Mind (2013). Physical Restraint in Crisis: A report on physical restraint in hospital settings in England. Retrieved from Mind Website:
148

URN: 6455433
https://www.mind.org.uk/media/197120/physical_restraint_final_web_version.pdf
Morrison, E. F. (1992). A coercive interactional style as an antecedent to aggression in psychiatric patients. Research in Nursing & Health, 15(6), 421-431. DOI: 10.1002/nur.4770150604
Morse J.M. & Field P.A. (1996). Nursing Research: The Application of Qualitative Approaches, 2nd edn. London: Chapman and Hall.
National Institute for Health and Care Excellence. (2005). Violence: The short-term management of disturbed/violent behaviour in inpatient psychiatric settings and emergency departments. Retrieved from NICE Website: https://www.nice.org.uk/guidance/ng10/resources/violence- and aggression-short-term-management-in-mental-health-health-and-community settings-pdf-1837264712389
NICE. (2015). Violence and Aggression: short-term management in mental health, health and community settings. Retrieved from National Institute of Clinical Excellence Website: https://www.nice.org.uk/guidance/ng10
Nijman, H., Muris, P., Merckelbach, H. L. G. J., Palmstierna, T., Wistedt, B., Vos, A. M., Rixtel, A.V., & Allertz, W. (1999). The staff observation aggression scale-revised (SOAS-R). Aggressive Behavior, 25(3), 197–209. Retrieved from http://search.proquest.com.ez.statsbiblioteket. dk:2048/docview/619431198?accountid=14468
Novaco,R. W. (2003). The Novaco Anger Scale and Provocation Inventory (NAS-PI). Los Angeles, LA: Western Psychological Services.
Novaco, R. & Renwick, S. (1998). Anger predictors of the assaultativeness of forensic hospital patients. In E. Sanavio (Ed.), Behavior and cognitive therapy today: Essays in honor of Hans J. Eysenck (pp. 199–208). Oxford: Pergamon.
Oxford Dictionaries. (2010). ‘Coercion’, Oxford Dictionary of English, Oxford University Press, Oxford.
Palmstierna, T., & Wistedt, B. (1987). Staff observation aggression scale, SOAS: Presentation and evaluation. Acta Psychiatrica Scandinavica, 76(6),
657– 663. DOI: 2048/10.1111/j.1600-0447.1987.tb02936
Peternelj‐Taylor C. & Johnson R. (1995). Serving time: psychiatric mental health nursing in corrections. Journal of Psychosocial Nursing, 33, 12–19. DOI: 10.3928/0279-3695- 19950801-06
Queensland Government. (2008). Policy statement on reducing and where possible eliminating restraint and seclusion in Queensland mental health services. Retrieved from http://www.health.gld.gov.uk/mentalhealth/docs/sandrpolicy 081030.pdf.
149

URN: 6455433
Ritchie, J., Spencer, L. & O'Connor, W. (2003). Ritchie, J., and Lewis, J. (eds.) Carrying out Qualitative Analysis, in Qualitative Research Practice: A Guide for Social Science Students and Researchers. London: Sage.
Sequeira, H. & Halstead, S. (2004). The psychological effects on nursing staff of administering physical restraint in a secure psychiatric hospital: “When I go home, it's then that I think about it.”. British Journal of Forensic Practice, 6(1), 3–15. DOI: 10.1108/14636646200400002
Shaw, J., Davies, J., & Morey, H. (2001). An assessment of the security, dependency and treatment needs of all patients in secure services in a UK health
region. The Journal of Forensic Psychiatry, 12(3), 610-637. DOI: 10.1080/09585180127380
Smith, S. T., Edens, J. F., & McDermott, B. E. (2013). Fearless dominance and self-centered impulsivity interact to predict predatory aggression among forensic psychiatric inpatients. International Journal of Forensic Mental Health, 12(1), 33-41. DOI: 10.1080/14999013.2012.760186
Szmukler, G., & Appelbaum, P. S. (2008). Treatment pressures, leverage, coercion, and compulsion in mental health care. Journal of Mental Health, 17(3), 233-244. DOI: 10.1080/09638230802052203
Taylor, P. J., Maden, A., & Jones, D. (1996). Long-term medium secure hospital units: service gap of the 1990s? Criminal Behaviour and Mental Health, 6, 223–239. DOI: 10.1002/cbm.96
Tulloch, A. D., Fearon, P., & David, A. S. (2008). The determinants and outcomes of long-stay psychiatric admissions. Social Psychiatry and Psychiatric Epidemiology, 43(7), 569-574. DOI: 10.1007/s00127-008-0332-2
Uppal, G., & McMurran, M. (2009). Recorded incidents in a high‐secure hospital: A descriptive analysis. Criminal Behaviour and Mental Health, 19, 265-76. DOI: 10.1002/cbm.741
Urheim, R., Rypdal, K., Melkevik, O., Hoff, H. A., Mykletun, A., & Palmstierna, T. (2014). Motivational dimensions of inpatient aggression. Criminal Behaviour and Mental Health, 24(2), 141–150. DOI: 2048/10.1002/cbm.1894
Vernham, Z., Tapp, J., & Moore, E. (2016). Observer ratings of interpersonal behavior as predictors of aggression and self-harm in a high-security sample of male forensic inpatients. Journal of Interpersonal Violence, 31(9), 1597-1617. DOI: 10.1177/0886260515569060
Vӧllm, B. & Nedopil, N. (2016). The use of coercive measures in Forensic Psychiatric Care: Legal, ethical and practical challenges. Switzerland: Springer.
150

URN: 6455433
Völlm, B., Edworthy, R., Holley, J., Talbot, E., Majid, S., Duggan, C., Weaver, T., & McDonald, R. (2017). A mixed-methods study exploring the characteristics and needs of long-stay patients in high and medium secure settings in England: implications for service organisation. Health Service and Delivery Research, 5(11). Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK424815/
Von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., Vandenbroucke, J. P., & Strobe Initiative. (2007). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. International Journal of Surgery, 12(12), 1495-1499. DOI: 10.1016/j.ijsu.2014.07.01
Winje, M., van Mastrigt, S., Gjestad, R., Urheim, R., & Rypdal, K. (2018). Staff members’ evaluation of inpatients’ motivation for aggression–the roles of staff restrictions and aggression severity. The Journal of Forensic Psychiatry & Psychology, 29(3), 419-433. DOI: 10.1080/14789949.2017.14105
151

URN: 6455433
Part 3: Clinical Experience
Community Mental Health Recovery Service (CMHRS) (Year 1: November 2016-
September 2017) – this was a community service offering psychological assessment and
intervention to people (16 years old +) with severe and enduring mental health problems who
were eligible for Secondary Services. In this placement, I conducted 1:1 therapeutic work
with a diverse range of clients, primarily employing disorder-specific cognitive behaviour
therapy (CBT) (e.g. CBT for Psychosis, Bi-Polar Affective Disorder, Depression, and Post-
Traumatic Stress Disorder). Aside the 1:1 psychological work, I co-led a family intervention
for psychosis. With regards to psychological group work, I co-delivered a drop-in CBT skills-
based psychoeducational group and a 10-week dialectical-behaviour therapy group
intervention for those with emotional unstable personality disorder.
Older People’s Recovery & Support Team / Memory Assessment Service (Year 2:
October 2017 – March 2018) – I obtained experience in three different settings on this
placement working alongside older adults (65 years old +). The first setting was an older
people’s recovery and support team where I provided psychological interventions (e.g. CBT
and Acceptance and Commitment Therapy (ACT)) for older adults experiencing depression
and/or anxiety. The second setting was a memory assessment service whereby I undertook
neuropsychological assessments on older adults as well as supporting clients and their
families adjusting to a dementia diagnosis. The third setting was a rehabilitation unit working
with older adults who had been referred to the unit for physical health difficulties (i.e. having
experienced frequent falls/mobility issues and Parkinson’s disease) and who were also likely
to benefit from brief psychological therapy. In addition, I worked within the Care Home
Liaison Service supporting staff of local care homes who were experiencing difficulties
managing the behaviour of residents, predominantly those with advanced dementia.
152

URN: 6455433
Child and Adolescent Community Mental Health Team (Year 2: April 2018-September
2018) –I worked alongside children and young people (from the age of 6-18 years old) with
their families and often, their schools, dividing my time between a tier 2 and tier 3 service. In
the tier 3 service I worked alongside young people with more acute presentations who often
needed both psychological and psychiatric (i.e. medication) input. I provided a range of
psychological interventions including, exposure therapy for panic and developing a PBS plan
for an individual with Attention Deficit Hyperactive Disorder (ADHD)). In the tier 2 service I
predominantly worked in the single point of access (SPA) where my role was to conduct
initial psychological assessments, including risk assessments, with young people and their
families and to signpost these individual on to appropriate services (i.e. tier 2 or tier 3 mental
health services, parenting workshops). I also provided brief CBT interventions for young
people with mild mental health difficulties (i.e. narrative therapy for a child with separation
anxiety).
Low and medium-secure forensic unit (Year 3: October 2018- March 2019) – I chose to
work in a low and medium secure forensic unit for my specialist placement and gained
experience working alongside male and female offenders (aged 18-65 years old) presenting
with mental health difficulties (primarily psychosis-related disorders). Complex
comorbidities that were common in this client population included substance misuse and
personality disorder in addition to difficulties caused by biological factors (e.g. ASD),
psychosocial factors (e.g. traumatic childhood/past experiences), and coping/adaptation to
stressful life events (e.g. bereavements, difficult transitions from adolescence to adulthood).
A main part of my work was conducting psychological assessments which enabled me to
develop psychological formulations for not only the individual’s mental health difficulties but
also their offending behaviour/risk history (i.e. arson, grievous bodily harm) and personality
153

URN: 6455433
and interpersonal functioning. I conducted both 1:1 psychological therapy (i.e. CBT for
Psychosis and solution-focused therapy) whilst also lead on an adapted family therapeutic
intervention. With regards to group work, I co-led an ‘Understanding Mental Health’ group
which was primarily a CBT skills-based psycho-educational intervention for those residing in
the medium secure wards. This also required the supervision of psychology assistants in the
design and delivery of group material.
Community Learning Disability Healthcare Team: (Year 3: April 2019- September
2019) – in this placement I worked with male and female adults (18-65 years old) who had a
diagnosed learning disability typically alongside other comorbidities such as Autism
Spectrum Disorder, Downs Syndrome and Cerebral Palsy. The Psychology team sat within a
wider physical health care team that included, for example, speech and language therapists,
occupational therapists, nurses, and physiotherapists. Reasons for referral to the psychology
team included mild mental health problems (i.e. anxiety), challenging behaviour and life
changes and transitions (i.e. bereavements, moving to independent living). There was a lot of
indirect work with systems, for instance, gathering information and presenting psychological
formulations to social workers and care staff from residential settings. The main
psychological approach/model used in this placement was behavioural, for example,
developing Positive Behaviour Support plans through formal observations and the monitoring
of ABC (antecedent, behaviour, consequence) charts. In addition, I conducted cognitive
assessments (i.e. Weschler Adult Intelligence Scale (WAIS)-IV) and social functioning
assessments (i.e. Adaptive Behaviour Assessment Systems (ABAS)) to assess whether an
individual had a diagnosis of a learning disability in order to access appropriate services.
154

URN: 6455433
Part 4: Assessments
Year I AssessmentsAssessment Title
WAIS WAIS Interpretation (online assessment)
Practice Report of Clinical Activity CBT assessment and formulation of Simon (pseudonym), a male in his 50’s experiencing low mood and rumination.
Audio Recording of Clinical Activity with Critical Appraisal
Audio Recording and Critical Appraisal of Ac-ceptance and Commitment Therapy for Depres-sion and Anxiety.
Report of Clinical Activity N=1 Cognitive Behaviour Therapy with a woman in her early forties with Bipolar Affective Disorder.
Major Research Literature Survey Coercive practice and patient interpersonal style as predictors of patient aggression and violence in secure-care forensic settings: A literature Survey.
Major Research Project Proposal The relationship between interpersonal sensitivity and perceived staff coercion in predicting levels/rates of patient aggression in a secure forensic setting.
Service-Related Project Evaluation of a Trauma and Dissociation Aware-ness Training program for staff in multidisciplin-ary adult mental health teams.
Year II AssessmentsAssessment Title
Report of Clinical Activity – Formal Assessment A neuropsychological assessment with a lady in her early 70s for a suspected Dementia within a Memory Assessment Clinic.
PPD Process Account Personal and Professional Development Group Process Account.
Presentation of Clinical Activity CBT for Depression with a White British Adolescent Boy.
155

URN: 6455433
Year III AssessmentsAssessment TitleMajor Research Project Literature Review Coercive practice and service user interpersonal
style as predictors of service user aggression and violence in secure-care forensic settings: A literature review.
Major Research Project Empirical Paper How do service users’ interpersonal sensitivity to dominance and perceptions of staff coercion impact upon self -reported anger and rates of aggression and in secure-care settings?
Report of Clinical Activity Adapted family therapy with a man in his 30s and his father in the context of a forensic setting.
156