Embed Size (px)
Citation preview

, . 183: 287–292 (1997)
EPSTEIN–BARR VIRUS IN B-CELL LYMPHOMASASSOCIATED WITH CHRONIC SUPPURATIVE
INFLAMMATION
-1, 2,3, . 2, 4, 5, . 1, . 6, 4 . 1*1Department of Histopathology, UCL Medical School, University Street, London, U.K.
2Department of Pathology, University of Birmingham, Birmingham, U.K.3Institute for Cancer Studies, University of Birmingham, Birmingham, U.K.
4Laboratoire d’Anatomie et Cytologie Pathologiques, Hôpital Purpan, Toulouse, France5Bone Tumour Service, Royal Orthopaedic Hospital, Birmingham, U.K.
6Cornell University Medical College, The New York Hospital, New York, NY, U.S.A.
SUMMARY
Chronic antigenic stimulation is considered to play an important role in neoplastic lymphoid transformation. This paper describesthree cases of non-Hodgkin lymphomas (NHLs) associated with long-standing chronic suppuration. Two were primary bone lymphomasassociated with long-standing chronic osteomyelitis and one was a primary skin lymphoma associated with chronic venous ulcers with alatent period of 13 years. All were diffuse large B-cell lymphomas, with plasmacytoid differentiation in two cases. Epstein–Barr virus(EBV)-encoded RNAs were demonstrated in virtually all tumour cells in all cases by in situ hybridization. Immunohistochemistryrevealed EBV-encoded latent membrane protein (LMP)-1 expression in one case and BZLF1 protein expression in all three cases, whilstthe EBV-encoded nuclear antigen (EBNA)-2 was not detected. Kaposi’s sarcoma-associated herpesvirus (KSHV) sequences were absentin two cases studied. Our cases show similarities with pyothorax-associated pleural lymphomas reported mainly from Japan and recentlyfrom France, which are invariably associated with EBV. These findings suggest a causal effect of EBV in the development of this typeof lymphoma complicating long-standing chronic suppuration. Localized immunodepression induced by chronic inflammation orimmunosuppressive cytokines may favour the clonal proliferation of EBV-infected B cells. ? 1997 John Wiley & Sons, Ltd.
J. Pathol. 183: 287–292, 1997.No. of Figures: 1. No. of Tables: 4. No. of References: 32.
KEY WORDS—chronic osteomyelitis; chronic venous ulcers; B-cell lymphoma; plasmablastic lymphoma; EBV
INTRODUCTION
Several studies have suggested that chronic in-flammatory stimulation may promote the growth ofneoplastic B cells. This is best illustrated by pyothorax-associated pleural lymphomas (PAPLs), where pleuralinflammation resulting from artificial pneumothorax forthe treatment of pulmonary tuberculosis precedes theonset of the disease with a latent period of 22–55 years.1MALT lymphomas of the salivary glands and of thethyroid gland associated with Sjögren syndrome andHashimoto’s disease, and gastric MALT lymphomasassociated with Helicobacter pylori also constitutegood examples of lymphomas complicating chronicinflammation.2–4 The chronic antigenic stimulationmay be either bacterial or autoimmune in nature, butthe underlying mechanisms for the emergence of amalignant cell clone have not yet been clarified.Previous studies have demonstrated Epstein–Barr
virus (EBV) infection in the tumour cells of all PAPLcases examined so far.5–7 The viral gene expressionpattern detected in most of these cases was similar
to that seen in post-transplant lymphoproliferativedisorders (PTLDs), suggesting that a possibly local-ized immune defect may have contributed to thedevelopment of these lymphomas.Prompted by these studies, we have retrieved from our
files three cases of malignant lymphoma arising in thecontext of chronic suppurative inflammation. Two ofthese were associated with chronic osteomyelitis and onehad developed at the site of a chronic venous ulcer of theskin. To assess if EBV infection may be a contributoryfactor in the development of these lymphomas, we havestudied our cases using the polymerase chain reaction,in situ hybridization, and immunohistochemistry.Because a new member of the herpesvirus family,Kaposi’s sarcoma-associated herpesvirus (KSHV), hasrecently been demonstrated in EBV-positive cases ofbody cavity-based lymphomas in AIDS patients, wehave also studied our cases for the presence of KSHVsequences using the polymerase chain reaction.8,9
MATERIALS AND METHODS
Histological materialThree cases of non-Hodgkin lymphoma (NHL)
associated with long-standing inflammation were
*Correspondence to: Professor P. G. Isaacson, Department ofHistopathology, UCL Medical School, University Street, LondonWC1E 6JJ, U.K.
CCC 0022–3417/97/110287–06 $17.50 Received 18 June 1996? 1997 John Wiley & Sons, Ltd. Accepted 29 May 1997
submitted as primary surgical pathology specimens topathology laboratories in Birmingham, U.K. (case 1);Toulouse, France (case 2); and London, U.K. (case 3),where all cases were collectively studied. The clinicaldata were reviewed. Blocks of tissue were decalcified in 5per cent nitric acid after formalin or Bouin’s solutionfixation when necessary. Tissue was routinely processedand paraffin sections were stained with haematoxylinand eosin for histological examination.
Immunohistochemistry
Immunohistochemistry (IH) was performed using thestreptavidin–biotin peroxidase technique after trypsindigestion or heating in a domestic pressure cooker whereappropriate. The panel of antibodies used is listed inTable I.
Genotypic studies
Genotypic studies were performed on paraffin-embedded material from cases 1 and 3 by the polymer-ase chain reaction (PCR) using standard techniques.Case 2 was fixed in Bouin’s solution, which made itunsuitable for PCR studies. Briefly, single 5 ìm paraffinsections were dewaxed with xylene, rinsed with ethanol,and dried. PCR buffer [100–200 ìl; 10 m Tris (pH 9),50 m KCl, 0·1 per cent Triton X-100; Promega, U.K.],including 200 mg/ml proteinase K (Sigma, U.K.), wasadded to each sample before incubation at 37)C over-night. Digests were heated to 95)C to destroy proteinaseactivity and the resulting supernatants were used in thePCR analysis. Amplification of the immunoglobulinheavy chain gene was performed using the primersdirected to the framework 3 part of the variableregion (FR3A) and to the joining region (LJH andVLJH), using a semi-nested protocol.10 Amplificationof the T-cell receptor ã-chain gene was carried outusing the method of McCarthy et al.11 PCR wasperformed in two separate reactions using the primersVã11+Vã101+Jã12 and Vã11+Vã101+Jp12 as pre-viously described.12
EBV in situ hybridization and polymerase chain reactionstudies
In situ hybridization (ISH) for the detection of EBV-encoded small nuclear RNAs (EBER1 and EBER2) wasperformed on paraffin sections using a publishedmethod.13DNA from cases 1 and 3 was extracted from formalin-
fixed, paraffin-embedded tissue using the method ofWright and Manos.14 Each extract was analysed usingPCR amplification and Southern blotting with primersand probes for Kaposi’s sarcoma herpesvirus (KS330233Bam region) and EBV (EBER region), whose sequenceshave been previously reported.9,15 The conditions for thePCR and hybridization of the KSHV and EBVsequences were as previously described.9,15 PCR prod-ucts were electrophoresed in agarose gel, denatured,neutralized, and transferred to a nitro-cellulose filteraccording to Southern.16 Filters were prehybridized andthen hybridized with a 32-P end-labelled internal oligo-nucleotide probe for 12 h at 42)C, washed at roomtemperature for 15 min in 2#SSPE 0·1 per cent SDS,and at 62)C for 10 min with reduced stringency. Auto-radiography was performed at "70)C with intensifyingscreen for 30 min to 2 h. Appropriate positive andnegative controls were included.
RESULTS
Patients
Case 1—A 49-year-old man sustained an open frac-ture of his right femur 31 years ago which was compli-cated over the years by non-union and recurrent chronicosteomyelitis. He presented to the Bone TumourService, Royal Orthopaedic Hospital, Birmingham, inAugust 1994 with a pathological fracture through thearea of chronic osteomyelitis. He had multiple chronicabscesses and discharging sinuses in his right thigh.Gentamicin-impregnated beads were inserted locally.The patient experienced increasing pain and swellingat the fracture site. A biopsy was performed and a
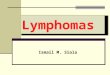
Table I—Antibodies used for immunohistochemistry
CD No. Antibody Source Specificity
CD45 LCA DAKO Lymphoid cellsCD20 L26 DAKO B cellsCD79a CD79a D.Y. Mason (Oxford University, Oxford, U.K.) B cellsCD3 Poly-CD3 DAKO T cellsCD30 BerH2 DAKO Ki-1 activation antigen— Anti-kappa DAKO Kappa light chain— Anti-lambda DAKO Lambda light chain— VS38 D.Y. Mason (Oxford University, Oxford, U.K.) Plasma cell differentiation marker— Anti-bcl 2 D.Y. Mason (Oxford University, Oxford, U.K.) Bcl 2 protein— MNF116 DAKO Epithelial— Anti-LMP-1 DAKO EBV latent membrane protein 1— Anti-EBNA-2 DAKO EBV nuclear antigen 2— Anti-BZLF1 DAKO EBV BZLF1 transactivator protein
288 C. COPIE-BERGMAN ET AL.
? 1997 John Wiley & Sons, Ltd. , . 183: 287–292 (1997)

lymphoma was diagnosed. The right femoral diaphysiscontaining the lymphoma and the fracture site wereexcised and a prosthesis was inserted. Post-operatively,antibiotics were given for 6 weeks. He underwent acourse of chemotherapy. At 5 months post-surgery, heremains clinically well, with no evidence of recurrence oftumour or infection.
Case 2—An 81-year-old man sustained an open frac-ture of his right femur 57 years ago. He developed overthe years a chronic osteomyelitis with a sinus tractopening on to the skin. Recently, a tumour mass aroseadjacent to the sinus, associated with inguinal lympha-denopathy. X-ray examination showed osteosclerosisextending to the distal femur and poorly circumscribedopacities in the surrounding soft tissues. A biopsy wasperformed and the mass was diagnosed as a lymphoma.The patient underwent radiotherapy but died 15 dayslater from multi-organ failure related to diabetes andcirrhosis.
Case 3—An 87-year-old man presented with twochronic venous ulcers of his lower leg. They had recentlybecome more extensive and painful and measured7#3 cm and 3#3 cm at the time of diagnosis. A biopsywas performed and a lymphoma was diagnosed. Theinterval between the onset of the ulcer and thelymphoma was 13 years. The patient underwent localradiotherapy consisting of 20 Gray in five fractions,but responded poorly to the treatment. At 5 monthspost-treatment, the ulcers remain extensive and painfulwithout symptomatic improvement.
PathologyThe gross features were as follows for case 1. The
resected femoral diaphysis showed a tan-colouredtumour with extensive necrosis centred on the fracturesite. Gross findings were not available for cases 2 and 3.Microscopically, all cases were diffuse large cell
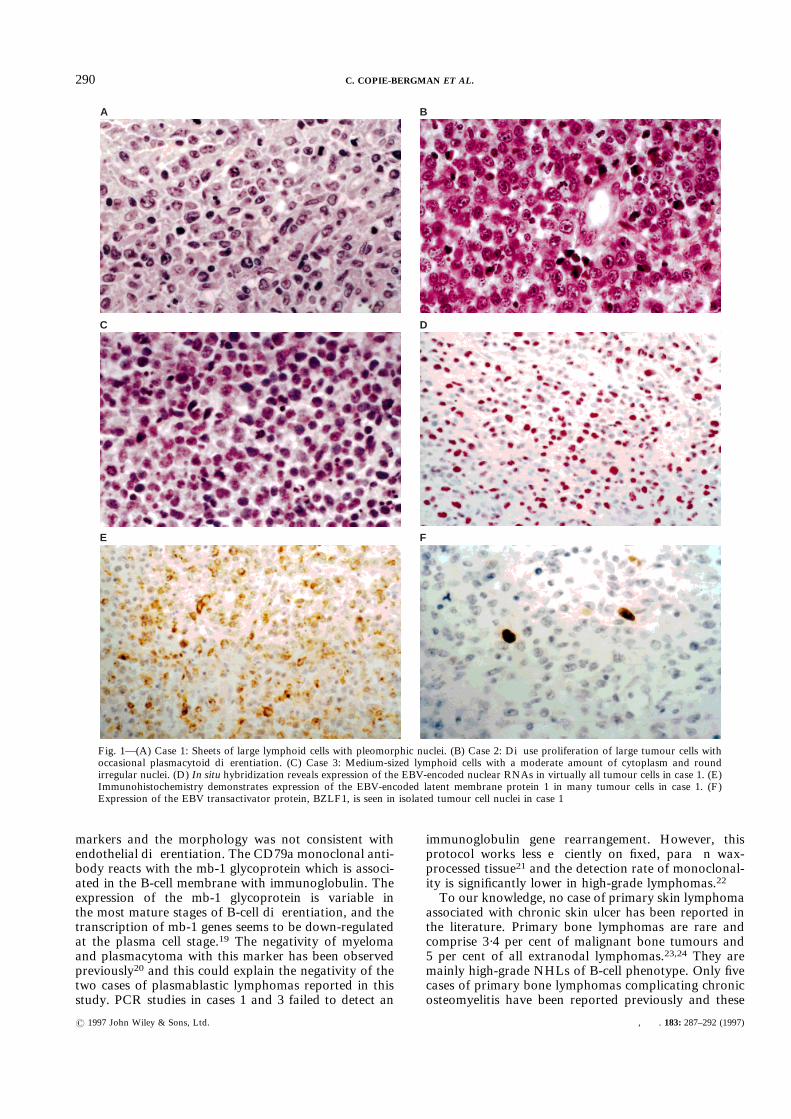
lymphomas. Case 1 was composed of sheets of largelymphoid cells with pale staining cytoplasm, pleomor-phic nuclei with multiple nucleoli, and was considered tobe of centroblastic polymorphous type (Fig. 1A). Cases2 and 3 exhibited plasmacytoid differentiation. Case 2was characterized by a diffuse proliferation of largelymphoid cells, with eosinophilic, often eccentric cyto-plasm and round nuclei containing generally a uniqueprominent nucleolus (Fig. 1B). Case 3 showed deeplyulcerated skin infiltrated by medium to large-sizedlymphocytes with a diffuse and trabecular pattern ofgrowth, containing moderately abundant cytoplasm,round irregular nuclei, and an occasional prominentsingle nucleolus (Fig. 1C).Numerous mitotic figures and prominent apoptosis
and necrosis of tumour cells were observed in all threecases. Admixed with the neoplastic cells were inflam-matory cells consisting either of small reactive lympho-cytes (cases 1 and 3) or of numerous neutrophils (case 2).
ImmunohistochemistryThe immunohistochemistry results are shown in
Table II. Case 1 expressed CD45 and B-cell-associated
antigens (CD20, CD79a) and demonstrated kappaimmunoglobulin light chain restriction and strong uni-form expression of CD30 in most cells. Case 2 failed toexpress B-cell-associated antigens or epithelial markersand showed granular cytoplasmic staining of the tumourcells with the plasma cell differentiation marker VS38.Case 3 was focally positive for CD45, showed stronggranular cytoplasmic staining with the plasma cell dif-ferentiation marker VS38, and demonstrated kappaimmunoglobulin light chain restriction. Expression ofthe cellular bcl 2 protein was not observed in any case.
Gene rearrangement studies
PCR studies performed on cases 1 and 3 were notsuccessful in demonstrating immunoglobulin heavychain gene rearrangement. No rearrangement of theT-cell receptor gamma gene was identified.
Epstein–Barr virus gene expression studies
The EBV status of the three cases is shown in TableIII. EBER-ISH demonstrated an intense nuclear stain-ing in more than 80 per cent of tumour cells in all threecases (Fig. 1D). PCR amplification of the EBER regionof EBV detected the 190 bp fragment in the two casesstudied (cases 1 and 3).Strong cytoplasmic expression of the EBV-encoded
latent membrane protein (LMP)-1 was detected by IH innumerous neoplastic cells in case 1 (Fig. 1E). No expres-sion of the EB nuclear antigen (EBNA)-2 was observed.Nuclear staining for the BZLF1 protein of EBV wasobserved in a small fraction of the tumour cells in allthree cases (Fig. 1F).
PCR amplification of KSHV
PCR amplification and subsequent hybridization toan internal oligonucleotide probe failed to identify thepreviously described 233 bp amplification product ofKSHV in both samples studied (cases 1 and 3).
DISCUSSION
We report three cases of high-grade NHL compli-cating long-standing chronic suppuration. Case 1 wasclassified as centroblastic B-cell lymphoma, kappa lightchain-restricted and CD30-positive. Cases 2 and 3 exhib-ited the antigenic profile of plasma cell-related disorders,characterized by partial or complete loss of CD45 andB-cell-associated antigens,17 and were classified asimmunoblastic lymphoma with plasmacytoid differen-tiation, or plasmablastic lymphoma. Light chain stain-ing was unsatisfactory in case 2, due to antigenicdenaturation in Bouin’s fixative, but kappa light chainrestriction was demonstrated in case 3. Both casesexhibited granular cytoplasmic staining of the tumourcells using the VS38 monoclonal antibody,18 which wasconsistent with plasma cell differentiation. This antibodyalso weakly stains epithelial elements and endothelialcells,18 but both cases were negative for epithelial
289EBV IN B-CELL LYMPHOMAS ASSOCIATED WITH CHRONIC SUPPURATIVE INFLAMMATION
? 1997 John Wiley & Sons, Ltd. , . 183: 287–292 (1997)
markers and the morphology was not consistent withendothelial differentiation. The CD79a monoclonal anti-body reacts with the mb-1 glycoprotein which is associ-ated in the B-cell membrane with immunoglobulin. Theexpression of the mb-1 glycoprotein is variable inthe most mature stages of B-cell differentiation, and thetranscription of mb-1 genes seems to be down-regulatedat the plasma cell stage.19 The negativity of myelomaand plasmacytoma with this marker has been observedpreviously20 and this could explain the negativity of thetwo cases of plasmablastic lymphomas reported in thisstudy. PCR studies in cases 1 and 3 failed to detect an
immunoglobulin gene rearrangement. However, thisprotocol works less efficiently on fixed, paraffin wax-processed tissue21 and the detection rate of monoclonal-ity is significantly lower in high-grade lymphomas.22To our knowledge, no case of primary skin lymphoma
associated with chronic skin ulcer has been reported inthe literature. Primary bone lymphomas are rare andcomprise 3·4 per cent of malignant bone tumours and5 per cent of all extranodal lymphomas.23,24 They aremainly high-grade NHLs of B-cell phenotype. Only fivecases of primary bone lymphomas complicating chronicosteomyelitis have been reported previously and these
A B
C D
E F
Fig. 1—(A) Case 1: Sheets of large lymphoid cells with pleomorphic nuclei. (B) Case 2: Diffuse proliferation of large tumour cells withoccasional plasmacytoid differentiation. (C) Case 3: Medium-sized lymphoid cells with a moderate amount of cytoplasm and roundirregular nuclei. (D) In situ hybridization reveals expression of the EBV-encoded nuclear RNAs in virtually all tumour cells in case 1. (E)Immunohistochemistry demonstrates expression of the EBV-encoded latent membrane protein 1 in many tumour cells in case 1. (F)Expression of the EBV transactivator protein, BZLF1, is seen in isolated tumour cell nuclei in case 1
290 C. COPIE-BERGMAN ET AL.
? 1997 John Wiley & Sons, Ltd. , . 183: 287–292 (1997)
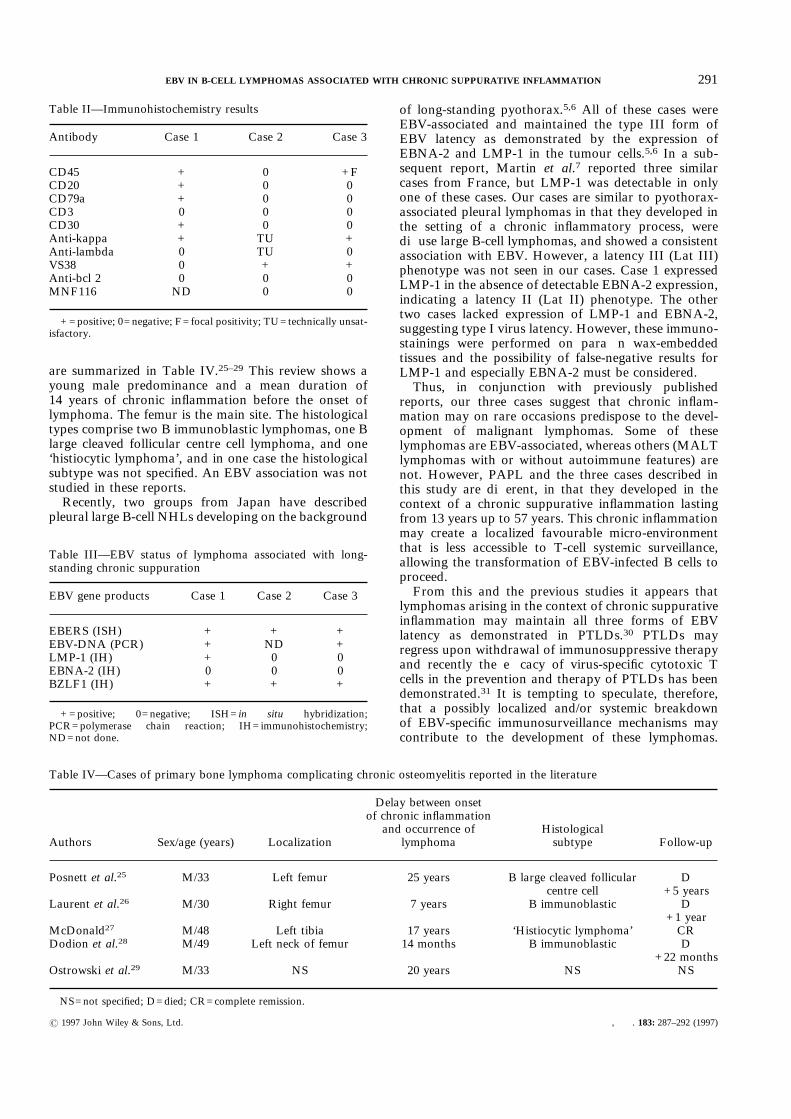
are summarized in Table IV.25–29 This review shows ayoung male predominance and a mean duration of14 years of chronic inflammation before the onset oflymphoma. The femur is the main site. The histologicaltypes comprise two B immunoblastic lymphomas, one Blarge cleaved follicular centre cell lymphoma, and one‘histiocytic lymphoma’, and in one case the histologicalsubtype was not specified. An EBV association was notstudied in these reports.Recently, two groups from Japan have described
pleural large B-cell NHLs developing on the background
of long-standing pyothorax.5,6 All of these cases wereEBV-associated and maintained the type III form ofEBV latency as demonstrated by the expression ofEBNA-2 and LMP-1 in the tumour cells.5,6 In a sub-sequent report, Martin et al.7 reported three similarcases from France, but LMP-1 was detectable in onlyone of these cases. Our cases are similar to pyothorax-associated pleural lymphomas in that they developed inthe setting of a chronic inflammatory process, werediffuse large B-cell lymphomas, and showed a consistentassociation with EBV. However, a latency III (Lat III)phenotype was not seen in our cases. Case 1 expressedLMP-1 in the absence of detectable EBNA-2 expression,indicating a latency II (Lat II) phenotype. The othertwo cases lacked expression of LMP-1 and EBNA-2,suggesting type I virus latency. However, these immuno-stainings were performed on paraffin wax-embeddedtissues and the possibility of false-negative results forLMP-1 and especially EBNA-2 must be considered.Thus, in conjunction with previously published
reports, our three cases suggest that chronic inflam-mation may on rare occasions predispose to the devel-opment of malignant lymphomas. Some of theselymphomas are EBV-associated, whereas others (MALTlymphomas with or without autoimmune features) arenot. However, PAPL and the three cases described inthis study are different, in that they developed in thecontext of a chronic suppurative inflammation lastingfrom 13 years up to 57 years. This chronic inflammationmay create a localized favourable micro-environmentthat is less accessible to T-cell systemic surveillance,allowing the transformation of EBV-infected B cells toproceed.From this and the previous studies it appears that
lymphomas arising in the context of chronic suppurativeinflammation may maintain all three forms of EBVlatency as demonstrated in PTLDs.30 PTLDs mayregress upon withdrawal of immunosuppressive therapyand recently the efficacy of virus-specific cytotoxic Tcells in the prevention and therapy of PTLDs has beendemonstrated.31 It is tempting to speculate, therefore,that a possibly localized and/or systemic breakdownof EBV-specific immunosurveillance mechanisms maycontribute to the development of these lymphomas.
Table II—Immunohistochemistry results
Antibody Case 1 Case 2 Case 3
CD45 + 0 +FCD20 + 0 0CD79a + 0 0CD3 0 0 0CD30 + 0 0Anti-kappa + TU +Anti-lambda 0 TU 0VS38 0 + +Anti-bcl 2 0 0 0MNF116 ND 0 0
+=positive; 0=negative; F=focal positivity; TU=technically unsat-isfactory.
Table III—EBV status of lymphoma associated with long-standing chronic suppuration
EBV gene products Case 1 Case 2 Case 3
EBERS (ISH) + + +EBV-DNA (PCR) + ND +LMP-1 (IH) + 0 0EBNA-2 (IH) 0 0 0BZLF1 (IH) + + +
+=positive; 0=negative; ISH=in situ hybridization;PCR=polymerase chain reaction; IH=immunohistochemistry;ND=not done.
Table IV—Cases of primary bone lymphoma complicating chronic osteomyelitis reported in the literature
Authors Sex/age (years) Localization
Delay between onsetof chronic inflammation
and occurrence oflymphoma
Histologicalsubtype Follow-up
Posnett et al.25 M/33 Left femur 25 years B large cleaved follicularcentre cell
D+5 years
Laurent et al.26 M/30 Right femur 7 years B immunoblastic D+1 year
McDonald27 M/48 Left tibia 17 years ‘Histiocytic lymphoma’ CRDodion et al.28 M/49 Left neck of femur 14 months B immunoblastic D
+22 monthsOstrowski et al.29 M/33 NS 20 years NS NS
NS=not specified; D=died; CR=complete remission.
291EBV IN B-CELL LYMPHOMAS ASSOCIATED WITH CHRONIC SUPPURATIVE INFLAMMATION
? 1997 John Wiley & Sons, Ltd. , . 183: 287–292 (1997)

This might allow a local unchecked outgrowth of EBV-carrying B lymphocytes. This notion is also supportedby the frequent detection of cells expressing the BZLF1trans-activator protein of EBV. This protein triggers theswitch from latent to replicative infection and precedesthe expression of other virus replication-associated pro-teins. BZLF1 expression is only infrequently observed inlymphomas arising in immunocompetent individuals,but is a regular feature of EBV-associated PTLDs.32 Asin PTLDs, additional genetic alterations may contributeto the development of a fully malignant phenotype.One such event might be co-infection with a recentlyidentified member of the herpesvirus group, Kaposisarcoma-associated herpes-virus (KSHV).9 This possi-bility has been suggested by the recent detection ofKSHV in EBV-associated body cavity-based lympho-mas arising in AIDS patients.8 However, KSHVsequences were not detectable in any of our cases byPCR.In summary, we have described three cases of diffuse
large B-cell NHL arising in the context of chronicosteomyelitis or chronic venous ulcer. All cases wereEBV-associated and displayed type II or type I viruslatency. These cases are similar to previously describedpyothorax-associated pleural lymphomas, which arealso invariably EBV-positive and often display a Lat IIIphenotype. Thus, the features of these lymphomas aresimilar to PTLDs, suggesting that a localized failure inthe EBV-specific immune control mechanisms may be animportant factor in the pathogenesis of lymphomasarising in the setting of long-standing suppurativeinflammation.
ACKNOWLEDGEMENTS
We gratefully acknowledge the technical expertise ofKeith Miller and other staff of the Immunohistochemis-try Laboratory and Angelo Agathanggelou and MrsNalini Singh for the in situ hybridization. CCB is arecipient of a Bourse Lavoisier du Ministère des AffairesEtrangères Français.
REFERENCES1. Iuchi K, Aozasa K, Yamamoto S, et al. Non-Hodgkin’s lymphoma of the
pleural cavity developing from long-standing pyothorax. Summary ofclinical and pathological findings in thirty-seven cases. Jpn J Clin Oncol1989; 19: 249–257.
2. Hyjek E, Smith WJ, Isaacson PG. Primary B cell lymphoma of salivarygland and its relationship to myoepithelial sialadenitis. Hum Pathol 1988;19: 766–776.
3. Hyjek E, Isaacson PG. Primary B cell lymphoma of the thyroid and itsrelationship to Hashimoto’s thyroiditis. Hum Pathol 1988; 19: 1315–1326.
4. Wotherspoon AC, Ortiz-Hidalgo C, Falzon MR, Isaacson PG.Helicobacterpylori-associated gastritis and primary B-cell gastric lymphoma. Lancet1991; 338: 1175–1176.
5. Fukayama M, Ibuka T, Hayashi Y, Ooba T, Koike M, Mizutani S.Epstein–Barr virus in pyothorax-associated pleural lymphoma. Am J Pathol1993; 143: 1044–1049.
6. Sajajima Y, Yamabe H, Kobashi Y, Hirai K, Mori S. High expression of theEpstein–Barr virus latent protein EB nuclear antigen-2 on pyothorax-associated lymphomas. Am J Pathol 1993; 143: 1280–1285.
7. Martin A, Capron F, Liguory-Brunaud MD, De Frejacques C, Pluot M,Diebold J. Epstein–Barr virus-associated primary malignant lymphomas ofthe pleural cavity occurring in longstanding pleural chronic inflammation.Hum Pathol 1994; 25: 1314–1318.
8. Cesarman E, Chang Y, Moore PS, Said JW, Knowles DM. Kaposi’ssarcoma-associated herpesvirus-like DNA sequences in AIDS-related body-cavity-based lymphomas. N Engl J Med 1995; 332: 1186–1191.
9. Chang Y, Cesarman E, Pessin MS, et al. Identification of herpesvirus-likeDNA sequences in AIDS-associated Kaposi’s sarcoma. Science 1994; 266:1865–1869.
10. Wan JH, Trainor KJ, Brisco MJ, Morley AA. Monoclonality in B celllymphoma detected in paraffin wax embedded sections using the polymerasechain reaction. J Clin Pathol 1990; 43: 888–890.
11. McCarthy KP, Sloane JP, Kabarowski JHS, Matutes, Wiedemann LM. Asimplified method of detection of clonal rearrangements of the T-cellreceptor-ã chain gene. Diagn Mol Pathol 1992; 1: 173–179.
12. Diss TC, Watts M, Pan LX, Burke M, Lynch D, Isaacson PG. Thepolymerase chain reaction in the demonstration of monoclonality in T celllymphomas. J Clin Pathol 1995; 48: 1045–1050.
13. Pan L, Diss TC, Peng H, et al. Epstein–Barr virus (EBV) in enteropathy-associated T-cell lymphoma (EATL). J Pathol 1993; 170: 137–143.
14. Wright DK, Manos MM. Sample preparation from paraffin-embeddedtissues. In: Innis MA, Gelfand DH, Sninsky JJ, White TJ, eds. PCRProtocols, a Guide to Methods and Applications. San Diego, CA: AcademicPress, 1990; 153–158.
15. Lin JC, Lin SC, De BK, Chan WP, Evatt BL. Precision of genotyping ofEpstein–Barr virus by polymerase chain reaction using three gene loci(EBNA-2, EBNA-3C, and EBER): predominance of type A virus associatedwith Hodgkin’s disease. Blood 1993; 81: 3372–3381.
16. Southern EM. Detection of specific sequences among DNA fragmentsseparated by gel electrophoresis. J Mol Biol 1975; 98: 503–517.
17. Knowles MD. Neoplastic Hematopathology. Baltimore: Williams &Wilkins, 1992; 691.
18. Turley H, Jones M, Erber W, Mayne K, de Waele M, Gatter K. VS38: anew monoclonal antibody for detecting plasma cell differentiation in routinesections. J Clin Pathol 1994; 47: 418–422.
19. Verschuren MCM, Comans-Bitter WM, Kapteijn CAC, et al. Transcriptionand protein expression of mb-1 and B29 genes in human hematopoieticmalignancies and cell lines. Leukemia 1993; 12: 1939–1947.
20. Mason DY, Cordell JL, Brown MH, et al. CD79a: a novel marker for B-cellneoplasms in routinely processed tissue samples. Blood 1995; 86: 1453–1459.
21. Diss TC, Pan L, Peng H, Wotherspoon AC, Isaacson PG. Sources of DNAfor detecting B cell monoclonality using PCR. J Clin Pathol 1994; 47:493–496.
22. Ben-Ezra J. Variable rate of detection of immunoglobulin heavy chainV-D-J rearrangement by PCR: a systematic study of 41 B-cell non-Hodgkin’s lymphomas and leukemias. Leuk Lymphoma 1992; 7: 289–295.
23. Spjut H, Dorfman H, Fechner R, Ackerman L. Tumor or tumor-like lesionsof marrow origin. In: Firminger H, ed. Tumors of Bone and Cartilage. 2ndedn. Atlas of Tumor Pathology, 2nd Ser., Fasc 5. Washington, DC: ArmedForces Institute of Pathology, 1983; 230.
24. Freeman C, Berg J, Cutler S. Occurrence and prognosis of extranodallymphomas. Cancer 1977; 29: 252–260.
25. Posnett DN, Collins RD, Krantz SB. Osteomyelitis and lymphoma. Lancet1979; ii: 1085.
26. Laurent G, Pris J, Delsol G, Familiades J, Fabre J. Immunoblasticlymphoma and osteomyelitis. Lancet 1980; i: 258.
27. McDonald I. Malignant lymphoma associated with internal fixation offractured tibia. Cancer 1981; 48: 1009–1011.
28. Dodion P, Putz P, Amiri-Lamraski MH, Efira A, De Martelaere E,Heimann R. Immunoblastic lymphoma at the site of an infected vitalliumbone plate. Histopathology 1983; 6: 807–813.
29. Ostrowski ML, Unni KK, Banks PM, et al. Malignant lymphoma of bone.Cancer 1986; 58: 2646–2655.
30. Thomas JA, Hotchin NA, Allday MJ, et al. Immunohistology of Epstein–Barr virus-associated antigens in B cell disorders from immunocompro-mised individuals. Transplantation 1990; 49: 944–953.
31. Rooney CM, Smith CA, Ng CYC, et al. Use of gene-modified virus-specificT-lymphocytes to control Epstein–Barr virus related lymphoproliferation.Lancet 1995; 345: 9–13.
32. Pallesen G, Hamilton-Dutoit SJ, Rowe M, et al. Expression of Epstein–Barrvirus replicative proteins in AIDS-related non-Hodgkin’s lymphoma cells.J Pathol 1991; 165: 289–299.
292 C. COPIE-BERGMAN ET AL.
? 1997 John Wiley & Sons, Ltd. , . 183: 287–292 (1997)