Embed Size (px)
Citation preview
Episodic Astigmatism Heralding Generalized Myopathy: Report of a Case Managed with a New Type of Soft Contact Lens LARS FRISEN, MD, CHRISTIAN BLOMSTRAND, MD
Abstract: A 29-year-old woman presented with marked variations in refraction. A few minutes of physical exertion or reading at a close distance induced up to 20 of myopia and 20 of myopic astigmatism, which regressed upon resting with closed eyes. Cycloplegic agents did not affect the refractive changes, which were shown to be due to variations in corneal curvatures. The eyes were otherwise clinically normal. A few months later the patient developed signs of a progressive, generalized myopathy of unknown origin. The muscular disease was resistant to treatment. The refractive changes were effectively controlled by means of a new type of soft contact lens, with a semi-rigid center. [Key words: ametropia, astigmatism, contact lens, myopathy.] Ophthalmology 91 :179-182, 1984
Short-term changes in ocular refraction have been previously reported in sporadic cases of myasthenia gravis. The most common change was towards myopia, usually attributed to an attempt to compensate medial rectus weakness by the use of convergence and concomitant obligate accommodation. I In the unusual case to be reported here, markedly variable myopic astigmatism with normal motility of the eyes and eyelids was a puzzling symptom of a generalized myopathy. The muscular disease was unresponsive to treatment. The changes in refraction were attributable to variations in corneal curvatures and were obviated by means of a new type of soft contact lens with a semi-rigid center.
CASE REPORT
A 29-year-old white woman noticed that her vision would sometimes become dim in both eyes in relation to physical
From the Departments of Ophthalmology and Neurology, University of G6teborg, Sweden.
Reprint requests to Lars Frisen, MD, Ogonkliniken, Sahlgrenska sjukhuset, S-413 45 G6teborg, Sweden.
exertion or reading. This was usually relieved by a period of rest with the eyes closed. A few months later, she noted that her vision tended to blur progressively during the day. This smooth progression was frequently punctuated by bouts of increased blur in relation to physical effort, with partial regression upon rest. Vision was always subjectively normal early in the morning. At the end of the day vision was usually so blurred that the patient found it nearly impossible to drive her car home from work. There were no other eye complaints. Some years previously, the patient had had surgery for gallstones, but she had otherwise enjoyed excellent health. No drugs were used besides a peroral anticonceptive: discarding the pill did not change the variations in vision.
OPHTHALMOLOGICAL EXAMINATIONS
The first eye examinations for this complaint were made about half a year after the onset of symptoms. Previous examinations for ametropia had revealed a refraction of -7.0 sph 00, and -6.5 sph OS; with well tolerated, soft contact lenses acuity had been 1.0 (20/20) OU. In several examinations after the debut of symptoms acuity varied between 0.1 (20/200) and 1.0 with this correction. Full acuity was obtained only after the addition of a variable amount of negative spheres, and negative cylinders with a nearly horizontal axis. Objective refractions using a refractometer under 1 % cyclopentolate cycloplegia on
179
OPHTHALMOLOGY • FEBRUARY 1984 • VOLUME 91 • NUMBER 2
>. .... '3 u o o :;)
VI
>
Q c .2 .... u o L--QI a:
LQI ~ o a.
o CD C L-o U
o.
-cycloplegic 00 c. -7 sph
.,.,05 sphere - -
.......-cycloplegic 05 ........ ",c . -6.5 sph
00 cyl 165·
'" 00 sPher~ -75·
---- ~; ~~~~:
liiiiiliil~f~~=-=-=----~~~~~D~:~05~·~-----~=-=-a i
08 10 12
Time of day
17/16
14 16
different days gave widely divergent readings of both spherical and astigmatic ametropia, with less variability in readings obtained early in the morning than in readings obtained later during the day. Replacement of the contact lenses with spectacles for one week did not change the variability of refraction.
The changes in refraction were monitored in closer detail during I day, after 3 days of cycloplegic treatment of the left eye with 1.0% atropine eyedrops. The right eye remained untreated as a control. In addition to a Rodenstock PR 50 optical refractometer (which determines the total refractive error), a Haag-Streit Javal-Schiotz ophthalmometer was used for determining corneal curvatures. Refraction was also determined subjectively. The intraocular pressures were measured, using the Haag-Streit Goldmann applanation tonometer, and the sagittal positions of the corneal vertices were monitored with a Carl Zeiss Hertel exophthalmometer. In between the examinations, the patient continued her usual daily activities as a radiographer.
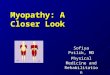
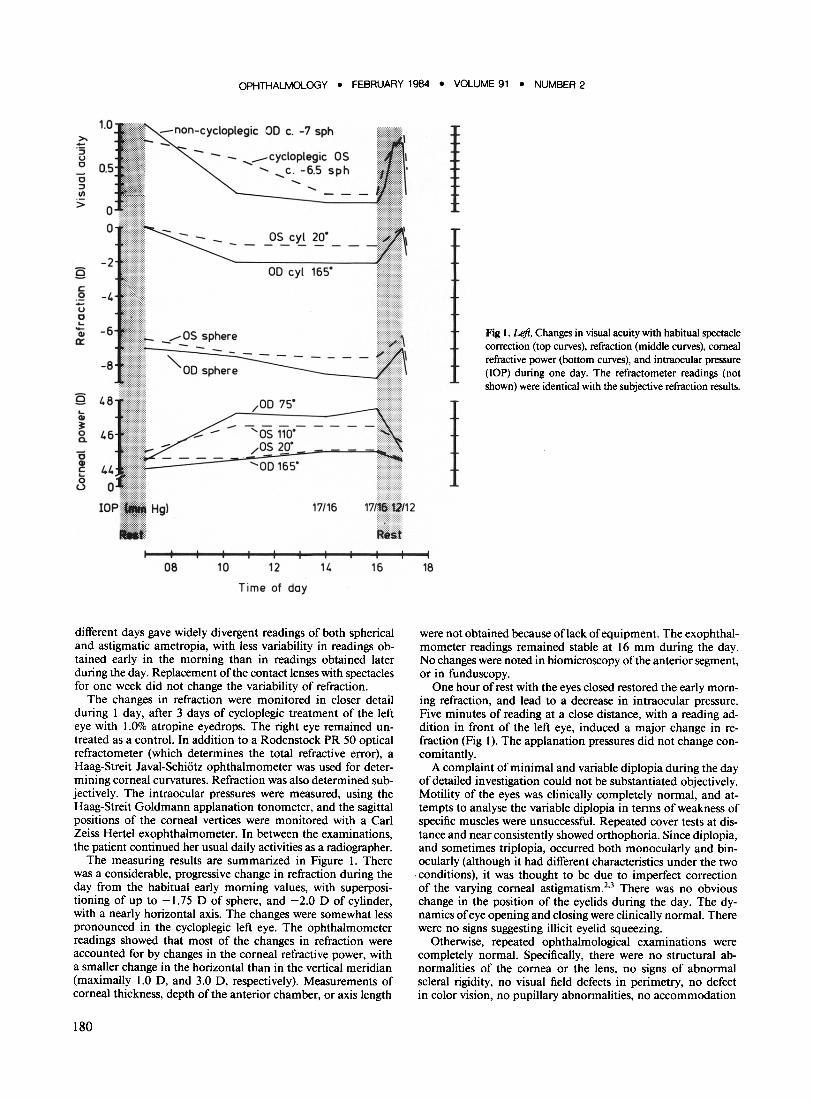
The measuring results are summarized in Figure I. There was a considerable, progressive change in refraction during the day from the habitual early morning values, with superpositioning of up to -1.75 D of sphere, and -2.0 D of cylinder, with a nearly horizontal axis. The changes were somewhat less pronounced in the cycloplegic left eye. The ophthalmometer readings showed that most of the changes in refraction were accounted for by changes in the corneal refractive power, with a smaller change in the horizontal than in the vertical meridian (maximally 1.0 D, and 3.0 D, respectively). Measurements of corneal thickness, depth of the anterior chamber, or axis length
180
18
Fig 1. Leji. Changes in visual acuity with habitual spectacle correction (top curves), refraction (middle curves), corneal refractive power (bottom curves), and intraocular pressure (lOP) during one day. The refractometer readings (not shown) were identical with the subjective refraction results.
were not obtained because oflack of equipment. The exophthalmometer readings remained stable at 16 mm during the day. No changes were noted in biomicroscopy ofthe anterior segment, or in funduscopy.
One hour of rest with the eyes closed restored the early morning refraction, and lead to a decrease in intraocular pressure. Five minutes of reading at a close distance, with a reading addition in front of the left eye, induced a major change in refraction (Fig I). The applanation pressures did not change concomitantly.
A complaint of minimal and variable diplopia during the day of detailed investigation could not be substantiated objectively. Motility of the eyes was clinically completely normal, and attempts to analyse the variable diplopia in terms of weakness of specific muscles were unsuccessful. Repeated cover tests at distance and near consistently showed orthophoria. Since diplopia, and sometimes triplopia, occurred both monocularly and binocularly (although it had different characteristics under the two conditions), it was thought to be due to imperfect correction of the varying corneal astigmatism.2
.3 There was no obvious
change in the position of the eyelids during the day. The dynamics of eye opening and closing were clinically normal. There were no signs suggesting illicit eyelid squeezing.
Otherwise, repeated ophthalmological examinations were completely normal. Specifically, there were no structural abnormalities of the cornea or the lens, no signs of abnormal scleral rigidity, no visual field defects in perimetry, no defect in color vision, no pupillary abnormalities, no accommodation
FRISEN AND BLOMSTRAND • EPISODIC ASTIGMATISM
defect, no eye motility defects, and no trace of convergenceretraction nystagmus.
CORRECTION OF AMETROPIA
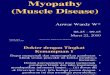
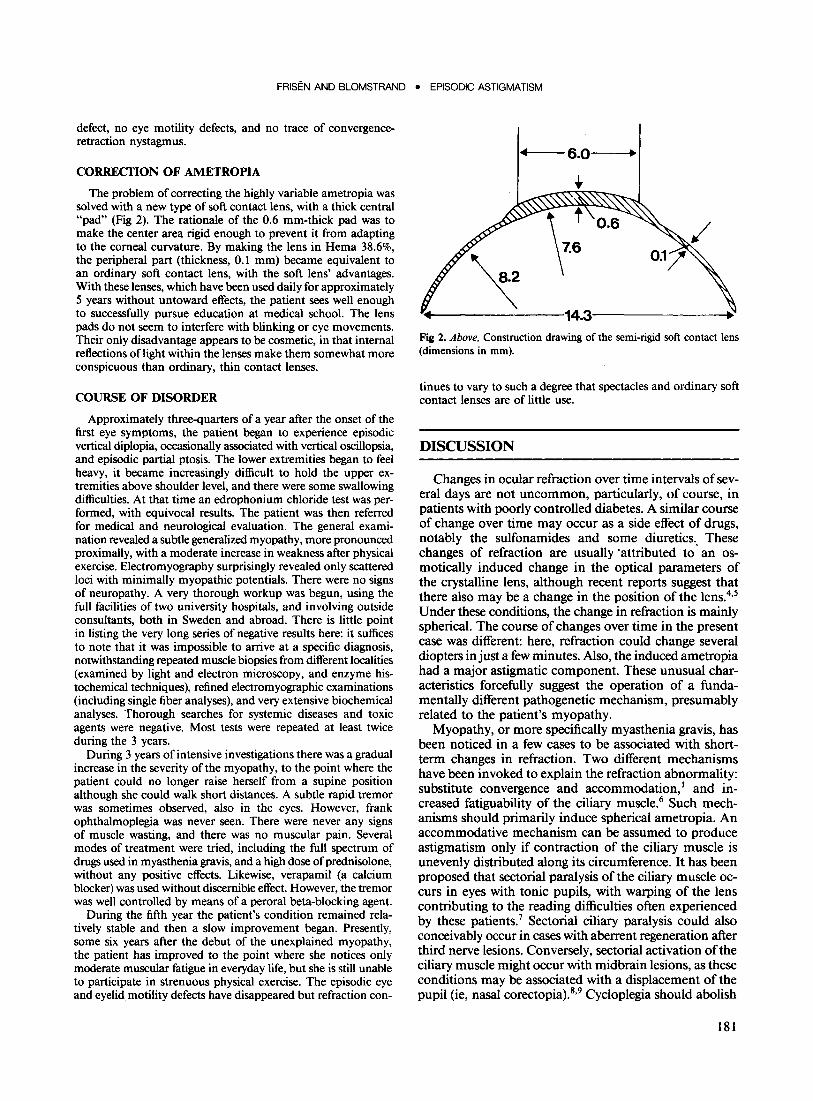
The problem of correcting the highly variable ametropia was solved with a new type of soft contact lens, with a thick central "pad" (Fig 2). The rationale of the 0.6 mm-thick pad was to make the center area rigid enough to prevent it from adapting to the corneal curvature. By making the lens in Hema 38.6%, the peripheral part (thickness, 0.1 mm) became equivalent to an ordinary soft contact lens, with the soft lens' advantages. With these lenses, which have been used daily for approximately 5 years without untoward effects, the patient sees well enough to successfully pursue education at medical school. The lens pads do not seem to interfere with blinking or eye movements. Their only disadvantage appears to be cosmetic, in that internal reflections oflight within the lenses make them somewhat more conspicuous than ordinary, thin contact lenses.
COURSE OF DISORDER
Approximately three-quarters of a year after the onset of the first eye symptoms, the patient began to experience episodic vertical diplopia, occasionally associated with vertical oscillopsia, and episodic partial ptosis. The lower extremities began to feel heavy, it became increasingly difficult to hold the upper extremities above shoulder level, and there were some swallowing difficulties. At that time an edrophonium chloride test was performed, with equivocal results. The patient was then referred for medical and neurological evaluation. The general examination revealed a subtle generalized myopathy, more pronounced proximally, with a moderate increase in weakness after physical exercise. Electromyography surprisingly revealed only scattered loci with minimally myopathic potentials. There were no signs of neuropathy. A very thorough workup was begun, using the full facilities of two university hospitals, and involving outside consultants, both in Sweden and abroad. There is little point in listing the very long series of negative results here: it suffices to note that it was impossible to arrive at a specific diagnosis, notwithstanding repeated muscle biopsies from different localities (examined by light and electron microscopy, and enzyme histochemical techniques), refined electromyographic examinations (including single fiber analyses), and very extensive biochemical analyses. Thorough searches for systemic diseases and toxic agents were negative. Most tests were repeated at least twice during the 3 years.
During 3 years of intensive investigations there was a gradual increase in the severity of the myopathy, to the point where the patient could no longer raise herself from a supine position although she could walk short distances. A subtle rapid tremor was sometimes observed, also in the eyes. However, frank ophthalmoplegia was never seen. There were never any signs of muscle wasting, and there was no muscular pain. Several modes of treatment were tried, including the full spectrum of drugs used in myasthenia gravis, and a high dose of prednisolone, without any positive effects. Likewise, verapamil (a calcium blocker) was used without discernible effect. However, the tremor was well controlled by means of a peroral beta-blocking agent.
During the fifth year the patient's condition remained relatively stable and then a slow improvement began. Presently, some six years after the debut of the unexplained myopathy, the patient has improved to the point where she notices only moderate muscular fatigue in everyday life, but she is still unable to participate in strenuous physical exercise. The episodic eye and eyelid motility defects have disappeared but refraction con-
1"·f---6.0--"·
Fig 2. Above. Construction drawing of the semi-rigid soft contact lens (dimensions in mm).
tinues to vary to such a degree that spectacles and ordinary soft contact lenses are of little use.
DISCUSSION
Changes in ocular refraction over time intervals of several days are not uncommon, particularly, of course, in patients with poorly controlled diabetes. A similar course of change over time may occur as a side effect of drugs, notably the sulfonamides and some diuretics. These changes of refraction are usually 'attributed to' an osmotically induced change in the optical parameters of the crystalline lens, although recent reports suggest that there also may be a change in the position of the lens.4
•5
Under these conditions, the change in refraction is mainly spherical. The course of changes over time in the present case was different: here, refraction could change several diopters in just a few minutes. Also, the induced ametropia had a major astigmatic component. These unusual characteristics forcefully suggest the operation of a fundamentally different pathogenetic mechanism, presumably related to the patient's myopathy.
Myopathy, or more specifically myasthenia gravis, has been noticed in a few cases to be associated with shortterm changes in refraction. Two different mechanisms have been invoked to explain the refraction abnormality: substitute convergence and accommodation,l and increased fatiguability of the ciliary muscle.6 Such mechanisms should primarily induce spherical ametropia. An accommodative mechanism can be assumed to produce astigmatism only if contraction of the ciliary muscle is unevenly distributed along its circumference. It has been proposed that sectorial paralysis of the ciliary muscle occurs in eyes with tonic pupils, with warping of the lens contributing to the reading difficulties often experienced by these patients.7 Sectorial ciliary paralysis could also conceivably occur in cases with aberrent regeneration after third nerve lesions. Conversely, sectorial activation of the ciliary muscle might occur with midbrain lesions, as these conditions may be associated with a displacement of the pupil (ie, nasal corectopia).8.9 Cycloplegia should abolish
181

OPHTHALMOLOGY • FEBRUARY 1984 • VOLUME 91 • NUMBER 2
any ametropia attributable to uniform or sectorial ciliary muscle dysfunction. Cycloplegia could prevent neither spherical ametropia, nor astigmatism, in the case reported here. Furthermore, during several years of observation there were never any signs in the present case of either myasthenia gravis, tonic pupils, aberrent regeneration of the third cranial nerves, or a midbrain lesion.
The present case appears to demonstrate a totally different mechanism for varying ametropia, viz variations in corneal curvature (Fig 1). Such variations are not uncommon in contact lens users, and are usually attributed to a temporary moulding of the cornea by the contact lens, or changes in corneal hydration. Although the case presented here had used soft contact lenses for a long period of time, a causal role of these lenses is disproved both by the very rapid change in refraction (Fig 1), and the unchanged variability of refraction after 1 week without the lenses. There was no clinically apparent structural abnormality of the corneas to account for their varying curvatures.
It appears likely that the varying ametropia in the present case was causally related to the generalized myopathy. At least two possibilities of explanation on this ground seem to exist. One applies to a generalized loss of tone in the extraocular muscles, the other to a loss of tone in the orbicularis oculi. A combination of both is also conceivable. The lack of clinical signs of ocular myopathy is not incompatible with a generalized decline in extraocular muscle tone, with an associated change in the shape of the eyeball. The hypothesis that the shape of the eyeball is influenced by the state of the extraocular muscles is supported by the finding that the intraocular pressure normally varies with the direction of gaze, 10 and that it increases temporarily in patients with untreated myasthenia gravis upon administration of edrophonium chloride. II A decrease of tone in the orbicularis oculi muscles also could lead to a change in refraction, by reducing the pressure of the eyelids on the cornea, and thereby changing its curvatures. However, the rarity of major refractive changes in patients with facial nerve palsies (unpublished observations) suggests that this mechanism would affect refraction only marginally. In normal individuals, lifting the eyelids off the eyeball usually induces less than 1.0 D of astigmatism. 12 A more direct assessment of the effects of extraocular and orbicularis muscle tone on corneal curvatures might be obtained by sequential anesthetic blocks of the retrobulbar space and the facial nerve, as suggested by an anonymous referee.
The observed variations in corneal curvatures do not account fully for the observed variations in refraction (Fig 1), indicating the operation of additional factors. Presumably, these could involve small changes in depth of the anterior chamber, or in axis length, or both. One or
182
more of these mechanisms may have been marginally influenced by the induced cycloplegia, possibly through mechanical bracing, as the variability of refraction in the left eye decreased somewhat following atropine treatment (Fig 1). Unfortunately, the limitations of the present observations hinder a more detailed analysis in this regard.
Generalized but variable changes in extraocular muscle tone, as part of a generalized, myastheniform myopathy, appear to be the most important factor behind the extreme variations in corneal curvatures occurring in the present case. Irrespective of the actual mechanism, variations in corneal curvatures seem to deserve the same attention as induced convergence-accommodation, I and myasthenic fatiguability of the ciliary muscle,6 when attempting to elucidate short-term variations in refraction in otherwise normal eyes. Recognition of these phenomena may also contribute to the early diagnosis of myopathy.
ACKNOWLEDGMENT
The contact lenses were designed and fitted by Ake Gustafsson, Kontaktlinser AG AB, Goteborg, and manufactured by AB Unilens, AmAI, Sweden.
REFERENCES
1. Romano PE, Stark WJ. Pseudomyopia as a presenting sign in ocular myasthenia gravis. Am J Ophthalmol 1973; 75:872-5.
2. Camey LG, Liubinas J, Bowman KJ. The role of comeal distortion in the occurrence of monocular diplopia. Acta Ophthalmol1981; 59: 271-4.
3. Bowman KJ, Smith G, Carney LG. Comeal topography and monocular diplopia following near work. Am J Optom Physiol Opt 1978; 55:818-23.
4. Eva PR, Pascoe PT, Vaughan DG. Refractive change in hyperglycaemia: hyperopia, not myopia. Br J Ophthalmol 1982; 66:500-5.
5. Bovino JA, Marcus OF. The mechanism of transient myopia induced by sulfonamide therapy. Am J Ophthalmol 1982; 94:99-102.
6. Manson N, Stem G. Defects of near vision in myasthenia gravis. Lancet 1965; 1:935-7.
7. Bell RA, Thompson HS. Ciliary muscle dysfunction in Adie's syndrome. Arch Ophthalmol 1978; 96:638-42.
8. Wilson SAK. Ectopia pupillae in certain mesencephalic lesions. Brain 1906; 29:524-36.
9. Selhorst JB, Hoyt WF, Feinsod M, Hosobuchi Y. Midbrain corectopia. Arch Neuro11976; 33:193-5.
10. Reader AL III. Normal variations of intraocular pressure on vertical gaze. Ophthalmology 1982; 89:1084-7.
11. Glaser JS, Miller GR, Gass JDM. The edrophonium tonogram test in myasthenia gravis. Arch Ophthalmol 1966; 76:368-73.
12. Wilson G, Bell C, Chotai S. The effect of lifting the lids on corneal astigmatism. Am J Optom Physiol Opt 1982; 59:670-4.