Embed Size (px)
Citation preview

Epileptic Negative Myoclonus in a Newbornwith Hemimegalencephaly
*Francesco Guzzetta, *Domenica Battaglia, *Donatella Lettori, *Federica Deodato,†Emanuela Sani, *Teresa Randò, *Daniela Ricci, *Celeste Acquafondata, and †Carmine Faienza
* Neuropsichiatria Infantile, Catholic University of the Sacred Heart, Roma; and †Neuropsichiatria Infantile,University of Parma, Italy
Summary: Purpose: We report the case of a male newbornwith Ohtahara syndrome and right hemimegalencephaly whopresented epileptic negative myoclonus in the first days of life.
Methods: Prolonged polygraphic studies were performed, aswell as MRI and a full clinical examination.
Results: EEG showed a constant and nonreactive pattern ofburst suppression. There were several kinds of electro-clinicalseizures (generalized myoclonia, short atonias, typical spasmand tonic spasms) at the beginning of the EEG’s burst. The
periods of EMG silence, lasting less than 300 ms, were asso-ciated with stereotyped EEG transients.
Conclusions: Epileptic negative myoclonus can be observedalso in neonatal age. The short transient impairment of motorfunction observed in the newborn seems linked to the slowcomponent of spike-wave discharge, but its mechanism is stillnot clear. Key Words: Epileptic negative myoclonus—Hemimegalencephaly—Early epileptic encephalopathy.
A severe epileptic syndrome often with polymorphicseizures characterizes early epileptic encephalopathies.No epileptic negative myoclonus has been reported. Wepresent one patient with Ohtahara syndrome with hemi-megalencephaly in whom epileptic negative myoclonusoccurred as a neonate.
CASE REPORT
The male infant was born after an uneventful preg-nancy and term delivery. Since the first days of life,frequent startles intermixed with partial tonic seizureslocated at the right limbs with or without secondary gen-eralization. A loading dose of phenobarbital (PB; 20 mg/kg) was administered, followed by maintenance therapyof 4 mg/kg/day.
At clinical examination, there was evidence of jitteri-ness with limb hypertonia and hyperreflexia moremarked at the right side. There was neither fixation noran evident responsiveness. Feeding was made difficultby frequent seizures.
Routine analysis and metabolic as well as microbio-
logic and immunologic examinations were normal.Karyotype was 46, XY.
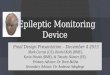
Magnetic resonance imaging (MRI) showed a righthemimegalencephaly (Fig. 1).
Results of the polygraphic studyWe performed prolonged polygraphic studies in the
first days of life, by using electrode placement accordingto the 10/20 International System modified on the basisof the asymmetric MRI data, so that the midline z elec-trodes corresponded roughly to the interhemispheric fis-sure. The examinations showed, during all the states, apattern of constant and nonreactive burst suppression(Fig. 2); even strong stimulations did not provoke anychange of the pattern. Interbursts lasted between 4 and20 s, and short bursts, only 1–3 s, characterized by high-voltage chaotic spikes and slow waves. At the beginningof each burst, high-voltage spike– or polyspike–waveswere usually recorded, coinciding with variable seizures.Consistent with the most dysplastic cortex, higher-voltage spike discharges were often observed at theright frontal region; sometimes they were transmitted tothe contralateral hemisphere. Several kinds of paroxys-mal events were located at the beginning of the bursts:high-voltage slow spikes related to a generalized myo-clonia (Fig. 3a) were the least frequent episodes. Themost usual presentation was a combination of two otherpatterns. The first one (Fig. 3b) consisted of a high-
Accepted March 10, 2002.Address correspondence and reprint requests to Dr. F. Guzzetta at
Neuropsichiatria Infantile, UCSC, Policlinico Gemelli, Largo Gemelli8, I-00168 Rome, Italy
Epilepsia, 43(9):1106–1109, 2002Blackwell Publishing, Inc.© International League Against Epilepsy
1106

voltage spike-and-waves at the beginning of the bursts;the wave appeared time-locked with an electromyogram(EMG) silent period of ∼150–300 ms; typically, we ob-served these short atonias especially in drowsiness. Thesecond pattern (Fig. 3c) was represented by typicalspasms consisting of a rhombus-shaped (1) EMG pattern,related to a wide high-voltage slow wave. More rarely,tonic spasms were observed. The typical spasm some-times was associated with a previous short EMG silence(Fig. 3d).
In one registration, a partial seizure lasted ∼40 s: theseizure was heralded by a synchronous high-voltagespike wave (SW) followed by a short alpha-like dis-charge at the right frontal region; successively, therewere rhythmic (1.5-Hz) SWs of increasing amplitude atthe frontotemporal right regions, promptly spreading onthe other side. At the end of the partial seizure, after along period (40 s) of depressed activity, a cluster ofspasms began.
DISCUSSION
Our case presented a complex epileptic syndrome in aneonate associated with a right hemimegalencephaly.The association of infantile spasms, myoclonias, and par-
tial epilepsy in newborns is generally found in cases withextensive migration disorders and indicated as Ohtaharasyndrome.
Our case is peculiar because of the presentation of aproteiform array of clinical seizures among which someare characterized by a short (<300 ms) EMG silence,time-locked with a stereotyped EEG transient. This EMGsilence was usually bilateral; rarely there was a preva-lence of the atonia duration on the left side.
Inhibitory motor critical phenomena (atonias) aftermyoclonus have been described in several action myo-clonuses. In these cases, the muscular inhibition is con-sidered a consequence of the myoclonic burst. The samemechanism seems at the base of type II silent period ofasterixis, a phenomenon that is lesional or metabolic inorigin, in which a subclinical EMG discharge related toan EEG transient seems to precede the EMG silence.
Differently, there have been observations (2–5) inwhich the EMG silence appears directly linked to anEEG transient without any previous myoclonic potential.The relation between the EEG pattern and the contralat-eral muscular inhibition suggested that the phenomenonbe called “epileptic negative myoclonus” (5). This typeof epileptic seizure has been described in different het-erogeneous epileptic syndromes in older children, but
FIG. 1. Magnetic resonance imaging: T1-weighted coronal scan showing a right hemi-megalencephaly including typical changes ofboth white matter and cortex, mostly in the pa-rietal region.
NEONATAL EPILEPTIC NEGATIVE MYOCLONUS 1107
Epilepsia, Vol. 43, No. 9, 2002

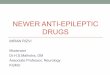
FIG. 3. Paroxysmal events linked to EEG bursts: bilateral synchronous myoclonic jerks related to right high-voltage slow spike (a);deltoid electromyogram (EMG) silence associated with right spike–wave (b); typical spasm linked to a spike–wave; the spasm appearsrelated to the wide high-voltage slow wave (c); short EMG silence followed by a typical spasm (d).
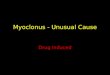
FIG. 2. Suppression burst pattern with more evident spikes on the right hemisphere. Note the atonic events linked to the beginning ofthe bursts.
F. GUZZETTA ET AL.1108
Epilepsia, Vol. 43, No. 9, 2002

never in newborns; there is only one description in anewborn that could fit with this kind of epileptic negativemyoclonus (ENM) (6).
The mechanism of ENM is often supposed to be ashort transient impairment of motor function that canoccur as the result of brief subclinical focal or general-ized SW discharges. Cerebral impairment may concernvarious kinds of functions, including high cortical func-tions (7). Particularly, the postural lapse time-lockedwith a cortical event allowed Guerrini et al. (5) to suggestthat the clinical phenomenon of tonus loss is an expres-sion of transient disruption of cortical function in thesensorimotor cortex. The focal epileptic event that oper-ates through an inhibitory interference on the areas pre-paring the movements or that directly involves a negativemotor area provokes this disruption.
There is good evidence that focal spike-induced cere-bral transitory impairment can be related to the slowcomponent of the SW discharge (8). That is what weobserved in our case, in which the EMG silent periodcorresponds to the middle of the slow wave after thehigh-voltage spike heralding the clinical phenomenon.
An inhibitory large concentric area including the ver-tical dimension is invoked to explain the EEG after slowwaves, induced by the paroxysmal depolarization of thefocal EEG spikes. The subsequent inhibitory potential
can be vertically propagated down to the spinal moto-neurons producing the EMG silence; that is whatCirignotta and Lugaresi (9) showed in some cases withpartial motor epilepsy through the evidence of absent Hreflex associated with the EEG focal spike. However, noclear explanation is available to understand the mecha-nism of this complex phenomenon.
REFERENCES
1. Fusco L, Vigevano F. Ictal clinical electroencephalographic find-ings of spasms in West syndrome. Epilepsia 1993;34:671–8.
2. Tassinari CA. New perspectives in epileptology: Proceedings ofthe International Public Seminar in Epileptology. Tokyo: JapaneseEpilepsy Association, 1981:42–59.
3. Wang PJ, Omori K, Utsumi H, et al. Partial inhibitory seizures: areport on two cases. Brain Dev 1984;6:553–9.
4. Oguni H, Sato F, Hayashi K, et al. A study of unilateral brief focalatonia in childhood partial epilepsy. Epilepsia 1992;33:75–83.
5. Guerrini R, Dravet C, Genton P, et al. Epileptic negative myoclo-nus. Neurology 1993;43:1078–83.
6. Hakamada S, Watanabe K, Hara K, et al. Brief atonia associatedwith electroencephalographic paroxysm in an infant with infantilespasms. Epilepsia 1981;22:285–8.
7. Aarts JIH, Binnie CD, Smit AM, et al. Selective cognitive impair-ment during focal and generalized epileptiform EEG activity.Brain 1984;107:293–308.
8. Shewmon DA, Erwin RJ. Focal spike-induced cerebral dysfunctionis related to the after-coming slow wave. Ann Neurol 1988;23:31–137.
9. Cirignotta F, Lugaresi E. Partial motor epilepsy with “negativemyoclonus.” Epilepsia 1991;32:54–8.
NEONATAL EPILEPTIC NEGATIVE MYOCLONUS 1109
Epilepsia, Vol. 43, No. 9, 2002